Submitted:
10 August 2024
Posted:
12 August 2024
You are already at the latest version
Abstract
In 2023, approximately 108 million infants worldwide received three doses of the diphtheria-tetanus-pertussis (DTP) vaccine, yet significant disparities persist, particularly in low-resource settings like West Africa. Despite the DPT vaccine's proven efficacy against diphtheria, the region continues to experience high rates of outbreaks for diphtheria, tetanus, and typhoid in 2024. This review aims to highlight the recent diphtheria crisis and analyze the trends and challenges of DTP vaccine coverage in West Africa by shedding light on socio-economic conditions, healthcare facilities and genetic factors. The review seeks to provide insights into improving vaccination rates and public health outcomes in the region, emphasizing the critical role of the DPT vaccine in combating life-threatening diseases. Enhanced surveillance and effective response strategies and development of region specific theraputics by the analysis of genomic variability in Africans, specifically within the human leukocyte antigen (HLA) locus are essential to address the ongoing public health challenges posed by diphtheria and related infections in West Africa.
Keywords:
DPT vaccine
; effective
; re-emergence
; diphtheria outbreak
; West Africa
Introduction
The recent rise of diphtheria cases in West Africa during 2023 and 2024 underscores the critical role of robust immunization programs in controlling vaccine-preventable diseases. Decades of research have undeniably established the efficacy and economic viability of mass vaccination campaigns in significantly reducing morbidity and mortality from infectious diseases including measles, rubella, and diphtheria [1]. Notably, tetanus and diphtheria toxoids remain some of the most widely administered vaccines globally, formulated with aluminium adjuvants to enhance immune response [2]. The World Health Organization (WHO) recommends a standardized childhood vaccination schedule for optimal lifelong protection against diphtheria and tetanus. This regimen entails three primary doses during infancy, followed by three booster doses at specific intervals throughout childhood and adolescence (12-23 months, 4-7 years, and 9-15 years), ensuring a minimum interval of four years between doses [3].
The historical approach to immunizing against diphtheria, tetanus, and pertussis involved the whole-cell pertussis (wP) vaccine combined with tetanus and diphtheria toxoids, forming the DTP vaccine. This regimen served as the mainstay for childhood immunization from the late 1940s to the 1990s [4]. While demonstrably effective in reducing disease burden, DTP faced challenges related to adverse reactions. Local reactions like redness, swelling, and injection site pain were frequent [4]. More concerning were rare but potentially serious systemic side effects.
The evolution of diphtheria, tetanus, and pertussis (DTP) vaccines reflects advancements in safety and targeting specific age groups. The original DTP vaccine, introduced in the late 1940s, contained whole-cell pertussis bacteria, offering protection but also causing side effects [5]. In the 1990s, DTaP replaced DTP, utilizing acellular pertussis, a less reactogenic form, to address safety concerns [6]. Finally, Tdap, created in 2005, is a booster dose aimed at adolescents and adults. It contains reduced diphtheria and pertussis components compared to DTaP, focusing on maintaining immunity for these individuals [7]. This shift in vaccine formulations demonstrates the ongoing effort to balance protection with minimizing adverse reactions.
The Advisory Committee on Immunization Practices (ACIP) recommends a single dose of Tdap vaccination for adults and adolescents in 2005 [8]. This strategy provides a booster against all three components– diphtheria, tetanus, and acellular pertussis. Following the Tdap dose, a booster of the Td vaccine (tetanus and diphtheria toxoids) is recommended every ten years or for wound care situations, ensuring continued protection against these potentially life-threatening illnesses [8].
Adsorbed diphtheria, pertussis, and tetanus (DPT) vaccines have been a topic of much discussion and reported adverse effects [9]. These vaccines combine components targeting diphtheria, pertussis, and tetanus. These antigens, derived from the respective pathogens, are often adsorbed onto an adjuvant, typically aluminum hydroxide or phosphate, to enhance the immune response [10]. While the DPT vaccine has a well-established safety profile and is crucial for preventing potentially life-threatening diseases, there is documented evidence of adverse effects associated with the vaccine [9]. These can range from mild local reactions like injection site pain and redness to more rarely observed systemic effects [9].
Despite knowledge about the potential for adverse reactions with the individual components of the DPT vaccine (pertussis vaccine, aluminum adjuvants, diphtheria, and tetanus toxoids), efforts to completely eliminate these reactions have not been entirely successful [11]. Research continues to explore ways to optimize vaccine formulations and minimize adverse effects while maintaining robust immune protection.
Diphtheria and the DPT Vaccine
Diphtheria, a toxin-mediated disease is a severe respiratory illness manifests with characteristic symptoms like a sore throat, malaise, fever, and a pseudomembrane (greyish patch) in the throat region [12]. Highly contagious, diphtheria spreads through respiratory droplets expelled by coughing or sneezing [13]. The infectious nature of the bacteria arises from the production of a potent exotoxin, which can lead to serious complications: cardiac problems, swallowing difficulties (dysphagia), airway obstruction due to membrane formation, reduced blood platelet count (thrombocytopenia), nerve damage causing paralysis, and even death in severe cases [14].
The cornerstone of diphtheria prevention lies in cost-effective interventions like vaccination [15]. The well-established DPT vaccine, a combination vaccine, effectively protects against diphtheria, tetanus, and pertussis (whooping cough) [16]. This vaccine incorporates whole-cell pertussis bacteria that have been inactivated, alongside tetanus and diphtheria toxoids, all adsorbed onto adjuvants (immune system stimulators) to enhance the immune response [15,16]. The DPT vaccine works by exposing the immune system to inactivated components of the diphtheria bacteria, triggering the production of antibodies specifically targeted against the diphtheria toxin [17]. This process not only neutralizes the toxin’s harmful effects but also creates immunological memory, allowing the immune system to recognize and respond swiftly to future diphtheria encounters [18].
The success of vaccination programs in reducing diphtheria incidence is evident. World Health Organization (WHO) data shows a significant decline in global diphtheria cases from 2000 to 2022, with a decrease from 11,625 to 5856 cases [19]. This reduction underscores the efficacy of vaccines and the importance of improved vaccination coverage worldwide. However, challenges remain. Diphtheria still poses a greater threat in developing countries, where factors like vaccine hesitancy, inadequate vaccine storage and management practices, and communication gaps impede reaching vaccination targets [20].
The Centers for Disease Control and Prevention (CDC) recommends specific DPT vaccination schedules for different age groups asshown in Table 1) Children under seven years old typically receive either DTaP (which includes pertussis protection) or DT (focusing on diphtheria and tetanus) depending on their age [21]. The recommended DTaP schedule for infants and toddlers involves five doses: two months, four months, six months, 15-18 months, and 4-6 years of age [20]. Research has shown that single-dose tetanus and diphtheria vaccinations may not provide long-term protection against diphtheria [22]. Fortunately, additional booster doses have been demonstrated to offer lasting immunity [23]. Completing the recommended DPT or Tdap vaccination schedule is crucial for establishing and maintaining robust immunity against diphtheria throughout life.
A country’s healthcare infrastructure significantly influences its ability to maintain consistent DTP vaccine coverage by ensuring accessible services, efficient supply chains, and well-trained personnel. Robust systems support public health campaigns, effective data monitoring, and integration with other health services, enabling timely interventions in low-coverage areas. Additionally, strong infrastructure allows for swift responses to public health emergencies, ensuring rapid vaccination efforts during outbreaks. Overall, well-developed healthcare infrastructure is essential for sustaining high vaccination rates and improving public health outcomes.
Several factors contribute to the observed fluctuations in DTP vaccine coverage across West African countries, impacting the overall trends in immunization rates. First, the state of healthcare infrastructure plays a crucial role; countries with well-developed systems tend to achieve higher vaccination rates, while those with limited access face challenges. Political stability also significantly influences vaccine coverage, as governance and policy decisions can either support or hinder healthcare delivery. Public awareness and education are vital in driving vaccination efforts, with community engagement leading to increased uptake, while misinformation can result in hesitancy. Epidemiological factors, such as disease outbreaks, may prompt urgent vaccination campaigns, causing temporary spikes in coverage. Additionally, international partnerships and initiatives often provide essential support, enhancing logistics and outreach efforts. Socioeconomic factors, including poverty and education levels, further impact vaccination rates, creating disparities between urban and rural access. Logistical challenges, particularly in remote areas, can hinder service delivery, affecting overall coverage. Understanding these dynamics is essential for addressing barriers and promoting equitable access to immunizations across the region.
The Figure 2 illustrates trends in DTP vaccine coverage from 2000 to 2022 across several West African countries. Overall, most countries exhibit a relatively stable trend in vaccine coverage, with minor fluctuations. This stability suggests ongoing efforts to maintain immunization rates despite potential challenges. However, certain nations may experience peaks in coverage, indicating successful vaccination campaigns or improvements in healthcare access. Conversely, valleys in the data may reflect logistical issues, funding shortages, or public health crises that hinder vaccination efforts. Notably, in the latter years of the graph, a gradual improvement in coverage is observable for several countries, suggesting effective interventions or renewed focus on immunization programs.
Figure 2.
Trends in DPT vaccination coverage data in West Africa.
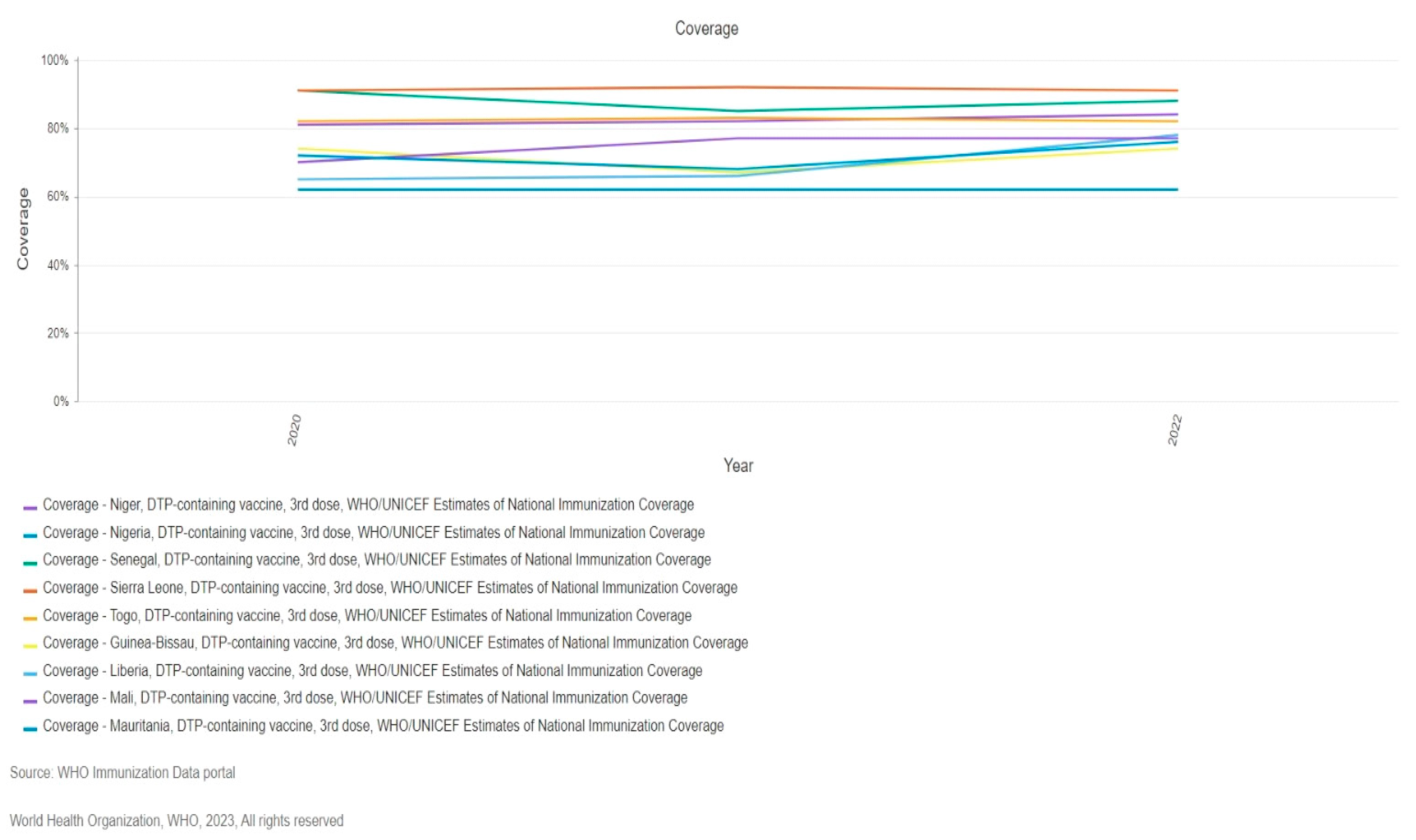
When comparing performance among countries, such as Nigeria and Senegal show higher overall coverage compared to others, indicating more robust targeted vaccination initiatives. In contrast, nations with lower coverage face systemic challenges, including political instability and limited healthcare infrastructure. Consistency in coverage trends suggest that certain countries benefit from stable health policies and funding, while those with fluctuations may experience varying degrees of success in their vaccination campaigns. For instance, Nigeria demonstrates a steady increase in coverage, it could be attributed to better resource allocation and community engagement.
The trends are also be influenced by external factors, such as global health initiatives, partnerships with international organizations, or responses to public health emergencies, such as pandemics. Countries that effectively leverage these partnerships may see better vaccination outcomes. Overall, the analysis indicates that while some countries have made significant strides in DTP vaccine coverage, others still face challenges that need to be addressed to ensure equitable access to immunizations. Continuous monitoring and targeted interventions will be crucial for improving overall vaccination rates in the region.
Over the years, the coverage of DTP (diphtheria, tetanus, and pertussis) vaccines in Nigeria has experienced significant fluctuations. Initially, from 2005 to 2010, there was a notable increase in vaccination rates for both the first and third doses, peaking in 2010 due to successful campaigns and heightened awareness. However, this was followed by a marked decline from 2011 to 2016, likely influenced by changes in health policies, funding challenges, and logistical issues. Despite these setbacks, a gradual recovery in vaccination coverage began after 2016, indicating that corrective measures were implemented to address the previous declines. Additionally, discrepancies between administrative, official, and WHO/UNICEF estimates highlight the importance of diverse data sources in understanding vaccination trends, with WHO/UNICEF data showing more stability over time.
The Figure 3 displays the coverage of DTP (diphtheria, tetanus, and pertussis) vaccines in Nigeria, broken down by dose (first and third) and different data sources, including administrative coverage, official coverage, and WHO/UNICEF estimates. This data provides valuable insights into the trends and effectiveness of vaccination efforts over the years.
In terms of administrative coverage, both the first and third doses show a significant increase around 2006, peaking in 2010. However, after this peak, there are notable fluctuations, with a general downward trend observed until 2016, followed by a gradual recovery. This pattern indicates that while there was initial success in vaccination efforts, subsequent challenges may have impacted coverage rates. The third dose follows a similar trajectory, reflecting the overall trends in vaccination administration.
Official coverage mirrors the administrative data, with significant increases around 2006 and peaks in 2010. Similar to administrative coverage, there is a decline until 2016, suggesting that external factors may have influenced these trends. The WHO/UNICEF estimates also show a steady increase from 2005 to 2010 for both doses, with minor fluctuations afterward. These estimates tend to be more stable, indicating a consistent effort from international health organizations to monitor and support vaccination initiatives. The graph suggests that in 2010 significant efforts were made for all categories to enhance vaccination coverage. However, the notable declines observed around 2015-2016 may be linked to external factors such as changes in health policies, funding constraints, or socioeconomic challenges that affected healthcare delivery. The discrepancies between the various sources of data highlight potential variances in data collection and reporting practices, emphasizing the need for accurate and consistent reporting mechanisms.
The gradual recovery in vaccination coverage after 2016 indicates that corrective measures may have been implemented to address the decline observed in previous years. This recovery suggests a renewed commitment to improving vaccination rates and ensuring that children receive essential immunizations. Overall, the graph presents a complex picture of the efforts in DTP vaccination in Nigeria, illustrating significant improvements followed by challenges and subsequent recoveries. Understanding these trends is crucial for policymakers and health organizations aiming to enhance immunization coverage and protect public health.
The Recent Outbreak 2023 and 2024:
The recent outbreak in West Africa highlights the concerning trend of declining vaccination rates and vaccine hesitancy, which can significantly compromise herd immunity and create fertile ground for the resurgence of previously controlled infectious diseases. Further research is warranted to explore the specific factors contributing to the decline in vaccination coverage in the region and to develop targeted interventions that promote vaccine acceptance and adherence to recommended immunization schedules.
A worrying resurgence of vaccine-preventable diseases is being observed in West Africa. Diphtheria cases have seen a dramatic rise, with approximately 25,000 cases and 800 deaths reported in the region by December 2023, with Guinea being particularly affected [23]. This trend continued into 2024, with the World Health Organization reporting over 34,704 suspected cases across several West African countries by February, with Nigeria experiencing the highest burden [24]. While data for tetanus and pertussis specifically is limited for 2023 and 2024, the resurgence of diphtheria alongside other “vaccine-preventable diseases” in West Africa has been documented [25]. This situation highlights the critical importance of maintaining robust immunization programs and addressing factors like low vaccination rates and vaccine hesitancy that can lead to outbreaks of these potentially fatal diseases.
- Diphtheria:
Nigeria: As of December 7, 2023, Nigeria reported 20,602 suspected cases, with 12,481 laboratory-confirmed cases and 553 deaths [23] .
Niger: By November 26, 2023, Niger had 2,300 suspected cases, 2,100 laboratory-confirmed cases, and 128 deaths [24].
Guinea: Guinea faced over 1,200 cases, of which 1,000 were confirmed, resulting in 71 deaths. A major response was initiated in the Siguiri region [25].
- Te0tanus:
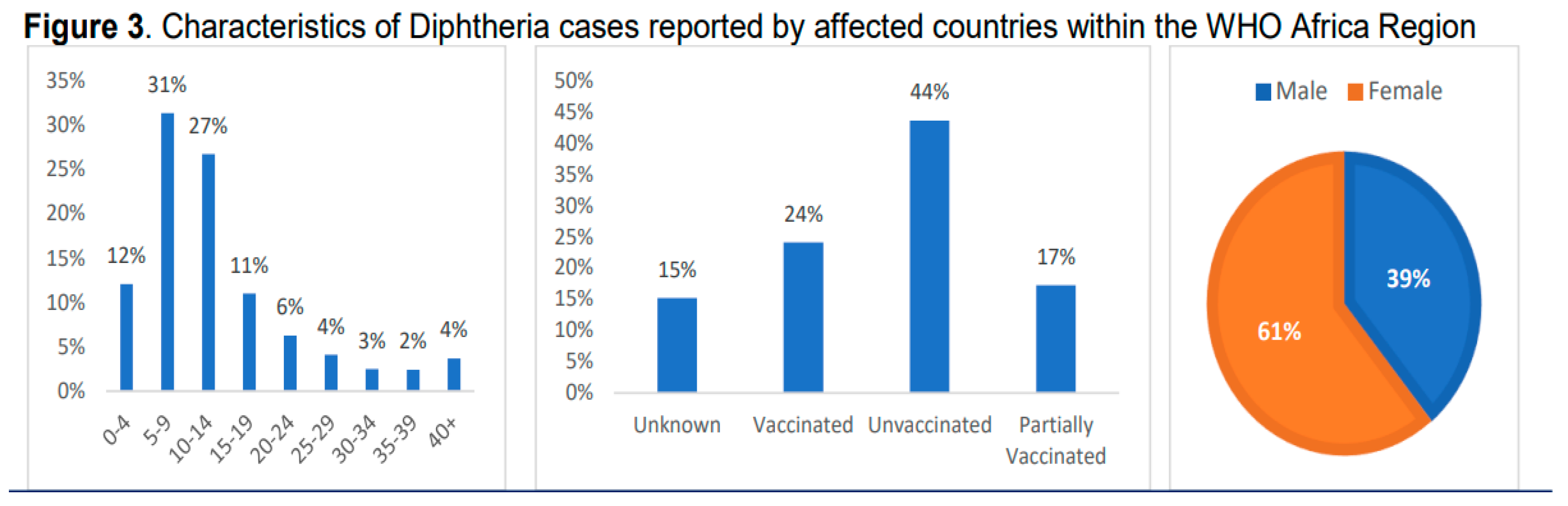
West Africa: Approximately 25,000 cases of diphtheria were reported during this period, leading to 800 deaths. Notably, 90% of cases occurred in children under 5 years old [26].
Republic of Niger: In Niger, 865 cases and 37 deaths were reported across nine regions, primarily in the Matameye district bordering Nigeria [24].
- Pertussis (Whooping Cough):
Guinea: Guinea reported 497 cases, including 14 confirmed and 483 suspected cases, with 58 deaths, mainly in the Kankan region [25].
Factors Influencing Vaccine Effectiveness
Vaccines are sensitive biological materials that can lose effectiveness if not handled properly [24]. Deviations from the recommended storage conditions can adversely affect a vaccine’s ability to protect against infections, such as diphtheria. The inherent sensitivity of vaccines and the necessity to maintain their potency require proper storage and transportation practices to preserve their integrity [25]. Numerous studies have demonstrated that adherence to strict guidelines—such as utilizing temperature-controlled refrigeration units, maintaining a consistent cold chain, employing insulated containers during transportation, avoiding exposure to light or extreme heat, and regularly auditing storage practices—can effectively mitigate and prevent the loss of vaccine efficacy [26,27].
Maintaining the cold chain is critical for preserving the potency and efficacy of vaccinations. Research indicates that the cold chain is a continuous process encompassing the storage, processing, and transportation of vaccines within specified temperature ranges, typically between 2°C and 8°C [28]. The stability and effectiveness of vaccines can be compromised if they are exposed to temperatures that are either too high or too low [29]. For instance, heat can lead to protein denaturation, rendering the vaccine less effective upon administration. Conversely, exposure to freezing temperatures can cause structural damage to the vaccine, further diminishing its efficacy.
Vaccine quality variations, such as low antigen content, can significantly reduce a vaccine’s efficacy and protective capacity [30]. Consequently, strict quality control and potency testing are essential to ensure that DPT vaccines are safe and effective. Studies have indicated that identifying and removing impurities or defects in the vaccine composition throughout the manufacturing and distribution processes ensures that each dose meets established standards and requirements [31]. Similarly, potency testing assesses the vaccine’s ability to effectively induce an immune response and verifies that vaccines contain the appropriate antigens, which are the active components that promote immunity [32,33].
Addressing Vaccine Hesitancy and Strengthening Immunization Programs
Public acceptance of vaccination is essential for the success of vaccination programs [34]. Many individuals exhibit reluctance or refusal to receive vaccinations, despite the proven effectiveness of vaccines in reducing the impact of infectious diseases and preventing vaccine-preventable fatalities [35]. If these concerns persist, there is a risk of resurgence in vaccine-preventable diseases [36]. According to the World Health Organization, the emergence of vaccination hesitancy over several decades has positioned it as one of the primary health risks globally [37].
The World Health Organization’s Strategic Advisory Group of Experts on Immunization (SAGE) has identified three primary factors contributing to vaccine hesitancy: complacency, convenience, and confidence. This framework is commonly referred to as the 3Cs model [38]. In 2018, the model was updated to the 5Cs model, which includes collective responsibility, calculation, complacency, confidence, and limitations [39]. Vaccines have proven to be one of the most effective measures against diseases, saving millions of lives each year [40]. In 1974, the Expanded Programme on Immunization (EPI) was initiated to ensure vaccination against multiple infectious diseases contributing to child mortality worldwide [41]. After four decades, the achievements of vaccination efforts are remarkable [41]. The complete eradication of smallpox and the control of poliomyelitis outbreaks in four World Health Organization zones serve as evidence of the effectiveness of vaccination campaigns [43]. These programs have significantly reduced mortality and morbidity rates from various infectious diseases. To decrease the incidence of vaccine-preventable diseases, vaccination programs must successfully achieve high coverage rates [44].
Healthcare professionals play a crucial role in promoting vaccine acceptance, serving as essential advocates [45]. Healthcare providers are the primary determinants of vaccine acceptance. Public health systems are vital in educating the community about vaccines and vaccine-preventable diseases [46]. The decision of parents to vaccinate their children is influenced by societal norms, including attitudes, behaviors, values, and beliefs [47]. Factors affecting vaccine uptake include safety monitoring, school-entry mandates, vaccine policies, and the development and implementation of vaccination recommendations. The Centers for Disease Control and Prevention oversees the Advisory Commission onImmunization Practices (ACIP), which formulates all vaccination recommendations in the United States. These recommendations provide critical guidance to healthcare providers and parents alike [48].
Health System Challenges in West Africa
Outbreaks of infectious diseases in the past have highlighted significant public health challenges, particularly the resurgence of these diseases and the lack of medical facilities in West Africa. Factors contributing to increased mortality rates, despite the global availability of the DPT vaccine, include insufficient financial support for healthcare improvement, limited vaccination facilities, partial immunization, inadequate vaccine program surveillance, lack of awareness, social stigma, and considerable distances from healthcare facilities. West Africa has a history of severe outbreaks of diphtheria, tetanus, and typhoid. Although recent improvements have been made, healthcare infrastructure remains inadequate.
In contrast, developed countries with expanded and well-managed immunization coverage have not faced sporadic cases of diphtheria, tetanus, or typhoid since the introduction of the DPT vaccine. However, countries in West Africa, including Nigeria, continue to experience high mortality rates due to poor routine immunization coverage for children [49]. The recent diphtheria crisis in Nigeria underscores the lack of robust vaccination coverage, necessitating the initiation of an emergency supplementary immunization program [49,50]. This situation also emphasizes the need for a genomic epidemiology program to determine whether the new outbreak, despite vaccination efforts, is associated with partial immunization, low coverage, or genetic mutations of the pathogen [51]. Early detection and reporting of diphtheria cases are essential for initiating prompt and effective outbreak response measures, including contact tracing, case management, vaccination campaigns, and infection prevention and control [52].
WHO Strategies and Initiatives in the Control and Prevention of Diphtheria
Diphtheria represents a significant global health issue. The World Health Organization (WHO) plays a crucial role in combating diphtheria outbreaks through various plans and activities. Immunization is essential for preventing diphtheria. WHO supports the Expanded Program on Immunization (EPI) to ensure that children receive the DTP (diphtheria, tetanus, and pertussis) vaccine as part of their routine vaccination schedules worldwide, in collaboration with UNICEF and other partners [53]. This initiative significantly reduces the prevalence of diphtheria.
To monitor cases and outbreaks of diphtheria, the WHO emphasizes the importance of effective surveillance systems. The Global Diphtheria Surveillance Network (GDSN) facilitates data collection, analysis, and reporting, enabling rapid responses to outbreaks [54]. Ensuring a consistent supply of diphtheria vaccines is a critical component of prevention. WHO collaborates with vaccine manufacturers, such as the Serum Institute of India, to guarantee a sufficient global supply of affordable, high-quality vaccines [53]. Controlling epidemics requires prompt action, case management, and contact tracing [55,56]. Additionally, WHO promotes research to enhance diphtheria treatments, screening methods, and vaccine development, including programs aimed at creating more affordable and widely accessible vaccines.
Recent Diphtheria Outbreak in West Africa
Overview of the recent diphtheria outbreak in West Africa.
On 26 May, 2024, WHO reported 40,929 suspected cases of diphtheria have been since 2023 across Gabon, Mauritania, Guinea, Nigeria, Niger, Cameroon and South Africa. A recent report from the World Health Organization (WHO) African Region (as of May 26, 2024) offers cautiously optimistic insights into the ongoing diphtheria outbreak. While Nigeria remains the epicenter, accounting for a substantial 78% of confirmed cases and 70% of fatalities [57], positive developments are evident.
Encouragingly, several countries have successfully contained the outbreak. Mauritania, South Africa, and Cameroon have reported no new cases since late 2023 and early 2024, respectively [57]. This underscores the effectiveness of targeted control measures in these regions and the potential for successful outbreak mitigation.
However, continued vigilance is paramount. Guinea and Niger have shown a slight uptick in weekly cases, highlighting the need for sustained interventions in these areas. Guinea remains classified as a Grade 2 outbreak by the WHO, indicating ongoing transmission risk. While other affected countries demonstrate declining case trends, close monitoring is still necessary.
These findings suggest a potential turning point in the outbreak trajectory. However, further investigation and sustained interventions are crucial to solidify these gains and ensure complete control across all affected regions. Close collaboration between national health authorities, international organizations, and local communities is essential to achieve this goal.
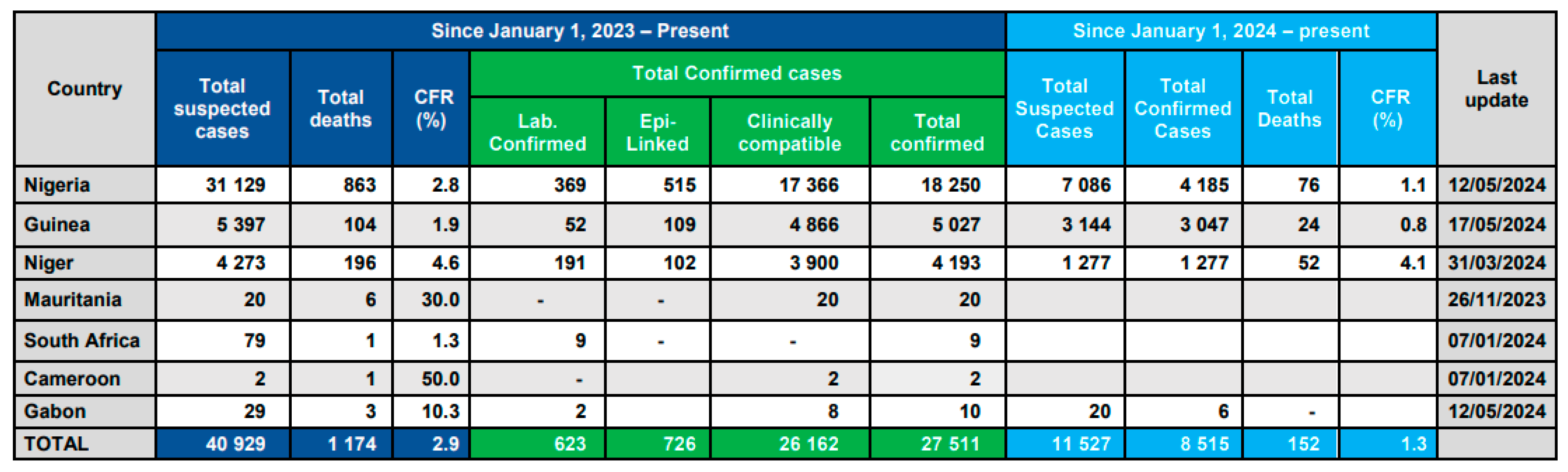
World Health Organization. (2024). WHO African Consolidated Regional Situation Report #008 – As of May 26, 2024.
Diphtheria cases reported by African countries within the WHO Africa Region, as of 15 May 2024
In previous Year, diphtheria cases have increased significantly in the Federal Republic of Nigeria; as of October 5, 2023, there have been 13,145 cases and 493 deaths. Eight federal states have reported experiencing the outbreak; Kano State has been hardest hit because of low immunization rates for the pentavalent vaccine [58]. On August 17, 2023, the Republic of Niger proclaimed an outbreak. Nine areas, including the Matameye district bordering Nigeria, reported 865 cases and 37 deaths [58]. There have been 497 cases recorded in Guinea, mostly in the Kankan region; these cases include 14 confirmed cases and 483 suspected cases, along with 58 deaths [59]. In recent years, extensive vaccination efforts have reduced diphtheria cases in Nigeria and West African countries, but the disease still affects low- and middle-income countries like Senegal, Ghana, Ivory Coast, and Mali.
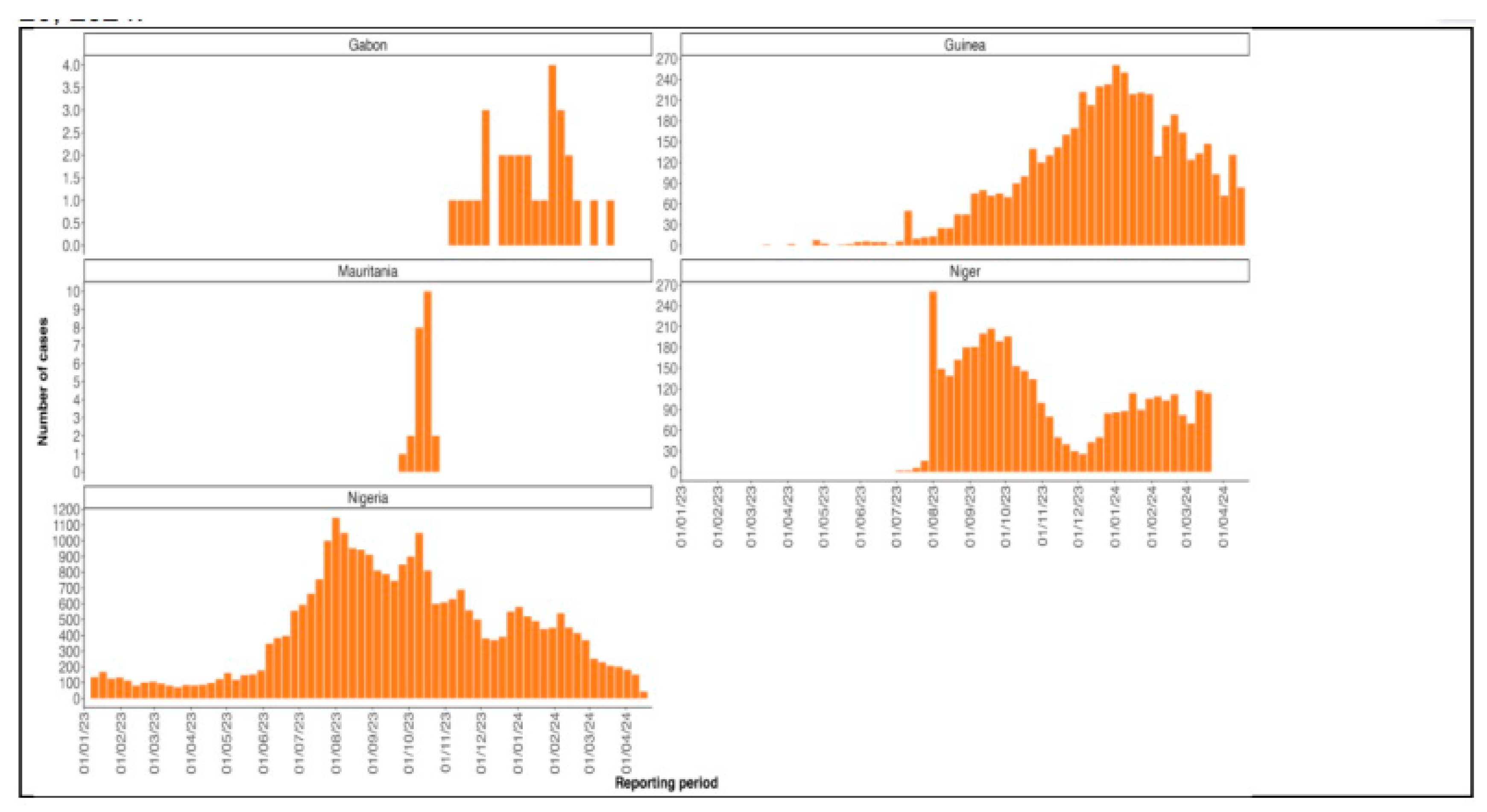
Figure 3.
The diphtheria epidemic curve in Nigeria, from epi-week 19 in 2022 to epi-week 14 in 2023, broken down by year and epi-week.
Figure 3.
The diphtheria epidemic curve in Nigeria, from epi-week 19 in 2022 to epi-week 14 in 2023, broken down by year and epi-week.
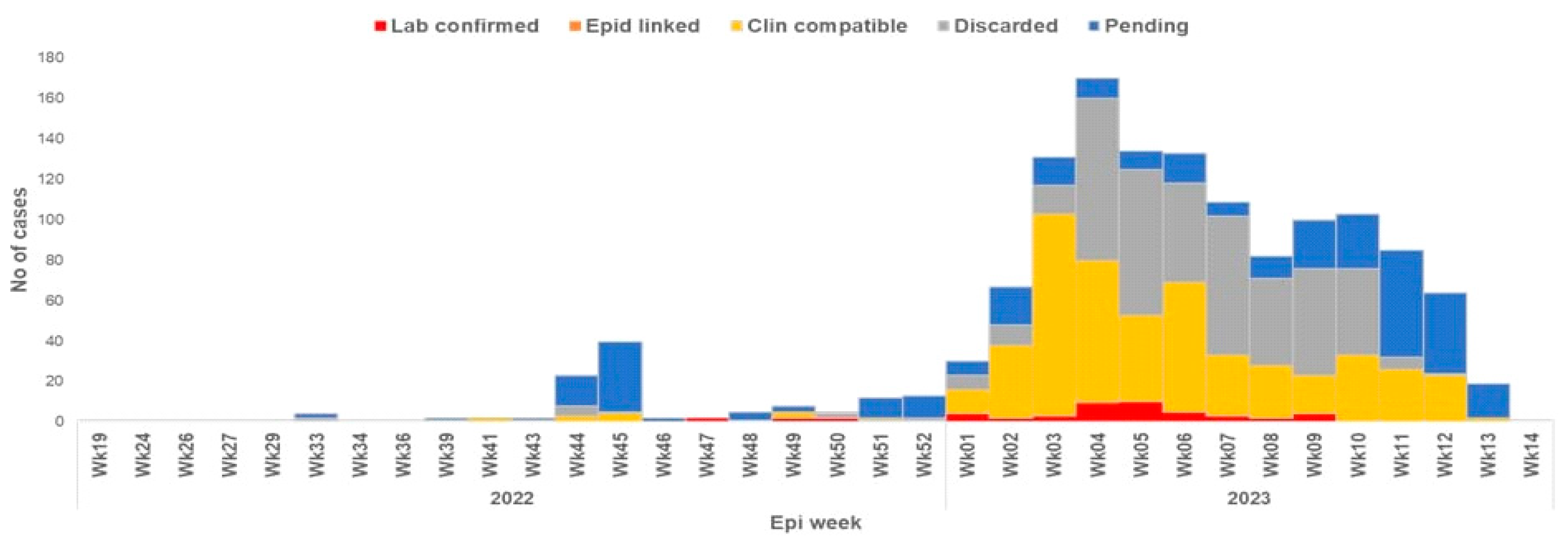
Factors Contributing to the Outbreak.
Understanding that outbreaks of diphtheria, especially those in West Africa, are impacted by a complex interaction of several factors is key [60]. It is also crucial to address these underlying issues that have contributed to this recent outbreak. In West Africa, particularly Nigeria, diphtheria epidemics have been connected to deplorable socioeconomic conditions [61], low vaccination rates, and ineffective surveillance and response systems, according to a 2014 report. Previous studies have also noted that logistics and insufficient finance were significant obstacles to the implementation of successful immunization programs in Nigeria.
Government and Healthcare Response to the Outbreak.
Public health responses to the outbreak included enhanced surveillance for early case discovery, case management, and risk communication, as well as vaccination interventions [62] are being applied under the coordination of the NCDC [63], in coordination with WHO and additional partners. To combat the diphtheria outbreak in Nigeria, the NCDC, Primary Health Care Development Agency (PHCDA), and WHO worked together, particularly in ensuring that infected individuals were isolated to prevent further spread. They enhanced routine immunization coverage and surveillance systems and offered technical assistance for case management [64], laboratory testing, and active surveillance.
Global Efforts in Diphtheria Control and Prevention: International Collaborations and Support for West African Countries
People continue to contract diphtheria worldwide, with the highest prevalence occurring in regions with limited access to medical care and immunization programs. The countries of West Africa present unique challenges that have garnered global attention. International agencies, including the WHO, UNICEF, and Médecins Sans Frontières (MSF), have played a significant role in controlling diphtheria in this region. These organizations collaborate with national governments and local healthcare professionals to develop and implement effective preventive and control measures [65]. One of the primary strategies involves vaccination campaigns. International organizations work with West African nations to ensure the accessibility and equitable distribution of diphtheria vaccines. Immunization coverage has improved significantly, largely due to WHO’s Expanded Program on Immunization (EPI) [57,66].
Unique Challenges by Country in the West African Diphtheria Outbreak (Source: WHO African Region Health Emergency Situation Report, May 2024)
| Country | Challenges |
| Nigeria | - Delays in reporting cases - Limited supplies of medical equipment and testing reagents - Security issues hindering response efforts in some regions - Limited capacity for diphtheria testing at sub-national laboratories |
| Niger | - Insufficient funding for vaccination campaigns and logistics - Security concerns restricting access to affected areas - Inadequate training of healthcare workers in diphtheria management - Challenges in monitoring diphtheria antitoxin usage |
| Gabon & Cameroon | - Lack of in-country infrastructure and resources for diphtheria testing, requiring samples to be shipped to South Africa for confirmation (delays diagnosis and response) |
| Guinea | - Incomplete vaccination coverage leaving the population vulnerable - Inadequate capacity in treatment centers to isolate and treat all patients - Ongoing challenges following MSF withdrawal (expertise and resources) - Funding delays hindering response efforts - Unmet performance indicators (delayed case isolation and investigation) |
Global Re-emergence of Diphtheria cases:
Although, the burden of Diphtheria heaviest in West Africa, other countries have also reported cases in reemergence of Diphtheria cases. Bangladesh, Venezuela and England have reported cases of diphtheria outbreak. A concerning outbreak of diphtheria emerged in Rohingya refugee camps located in Cox’s Bazar district, Bangladesh. This outbreak, documented in 2020, resulted in 19 confirmed cases and tragically, 1 death [70]. The precarious living conditions within the refugee camps likely contributed to the outbreak’s spread. Moreover, diphtheria cases plagued Venezuela between 2018 and 2020, particularly impacting children under the age of 5. While the exact number of cases remains unclear due to limitations in reporting, this outbreak underscores the difficulties of maintaining robust immunization programs in resource-constrained settings [71]. A devastating diphtheria outbreak swept through Madagascar during 2019 and 2020. This outbreak, characterized by over 8,000 suspected cases and a staggering 200 deaths, highlighted the consequences of low vaccination coverage and vaccine hesitancy [72].
The World Health Organization reported 17,248 diphtheria cases globally in 2021, with the highest burden concentrated in low- and middle-income countries [73,74]. This data reinforces the need for strengthened global vaccination programs to prevent diphtheria outbreaks.
It’s important to note that diphtheria outbreaks are not limited to developing countries. In 2019, England reported 10 cases of diphtheria, primarily among asylum seekers with recent arrival, highlighting the importance of maintaining strong vaccination programs even in developed nations [75].
While DTP vaccination is a cornerstone of diphtheria prevention, recent studies suggest a potential link between human genetic diversity, particularly in Africa, and variable vaccine efficacy[76]. Genomic variability in Africans, specifically within the human leukocyte antigen (HLA) locus, has been associated with lower vaccine efficacy for certain diseases, like. Similar studies have shown that genetic variation in the HLA locus can influence antibody responses to vaccines like DTP in African infants.
This variability underscores the importance of considering human genetic diversity in vaccine design and development, particularly for populations in Africa. Tailored vaccination approaches that account for this diversity might improve vaccine effectiveness and public health outcomes.
Conclusion and Recommendations
To make progress in the fight against diphtheria, targeted actions are required in light of the recent rise in reported cases. The lack of comprehensive, case-based diphtheria data hampers effective intervention, and many national immunization programs loiter behind current recommendations. Increasing routine vaccination coverage with DTP3 and administering recommended booster doses will help reduce susceptibility among children while addressing the loss of immunity in adolescents and adults. High rates of booster vaccinations for adolescents are essential to prevent outbreaks of this disease. Improving immunization rates in West Africa is critically important. Continued school vaccination campaigns are necessary until every region achieves a minimum of 80% vaccine coverage.
Further research is needed to identify specific barriers to vaccination uptake in various communities, assess the effectiveness of current immunization strategies, and evaluate the impact of socio-economic factors on vaccine accessibility. Additionally, studies focusing on the genomic epidemiology of diphtheria in West Africa could provide insights into the resurgence of cases, informing more targeted interventions. Moreover research is needed to unveil other unexplored factors such as potential genetic variations in West African populations that might influence DPT vaccine response.
Funding
The manuscript was not supported financially.
Abbreviations
| DPT: Diphtheria Pertussis Tetanus |
| NCDC: Nigerian Centre for Disease Control |
| WHO: World Health Organization |
| CDC: Center for Disease Control and Prevention |
| EPI: Expanded Program on Immunization |
| GDSN: Global Diphtheria Surveillance Network |
| ACIP: Advisory Commission on Immunization Practices |
Declaration:
Conflict of interest: There were no disclosed conflicts of interest by any of the authors.
Acknowledgement: None
AI Usage: Open AI is used for grammar and language editing services due to unavailability of funds for editing services.
Publication Consent: Not Applicable
Competing Interest: None
Approval of Ethics: Not Applicable
Writing of Manuscript: All Authors
Final Manuscript Approval: All Authors
Author Contributions: Javeria Hamraa: Conceptualization, project design and administration, investigation, writing – Original draft, writing – Review & Editing, supervision. Levi Tuwleh: writing – Original draft, data assembly, writing – Review & Editing– Review & Editing, supervision.
Tolulope Sharon Rumide: Writing – Original draft, writing – Review & editing
Adebayo Taiwo Emmanuel: Writing – Original draft, writing – Review & Editing
Josiah Talee Bropleh: Writing – Original draft, writing – Review & Editing
Hassan Ali: Writing – Original draft, writing – Review & Editing
References
- Wichmann, O., & Ultsch, B. (2013). Effektivität, Populationseffekte und Gesundheitsökonomie der Impfungen gegen Masern und Röteln. Bundesgesundheitsblatt - Gesundheitsforschung - Gesundheitsschutz, 56, 1260–1269. [CrossRef]
- World Health Organization. (2018). Diphtheria vaccine: WHO position paper, August 2017 – Recommendations. Vaccine, 36, 199–201. [CrossRef]
- Desai S, Scobie HM, Cherian T, Goodman T. Use of tetanus-diphtheria (Td) vaccine in children 4–7 years of age: World Health Organization consultation of experts. Vaccine. 2020 May;38:3800–7. [CrossRef]
- Liang, J. L., Tiwari, T., Moro, P., Messonnier, N. E., Reingold, A., Sawyer, M., & Clark, T. A. (2018). Prevention of pertussis, tetanus, and diphtheria with vaccines in the United States: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recommendations and Reports, 67, 1. [CrossRef]
- Centers for Disease Control and Prevention (CDC). (1991). Pertussis vaccination: Use of acellular pertussis vaccines for all childhood immunization programs. MMWR. Morbidity and mortality weekly report, 40(RR-1), 1 (Editorial).
- American Academy of Pediatrics. (1991). Immunization practices committee. Pertussis immunization: Use of acellular pertussis vaccines for all childhood immunization programs. Pediatrics, 88(5), 1090-1096.
- Centers for Disease Control and Prevention (CDC). (2005). Tdap vaccine for adolescents and adults. MMWR. Morbidity and mortality weekly report, 54(RR-7), 1-8.
- Tafreshi, S. Y. H. (2020). Efficacy, safety, and formulation issues of the combined vaccines. Expert Review of Vaccines, 19(10), 949-958. [CrossRef]
- Kretsinger, K., Broder, K. R., Cortese, M. M., Joyce, M. P., Ortega-Sanchez, I., Lee, G. M., Tiwari, T., Cohn, A. C., Slade, B. A., Iskander, J. K., Mijalski, C. M., Brown, K. H., Murphy, T. V., Centers for Disease Control and Prevention, Advisory Committee on Immunization Practices, & Healthcare Infection Control Practices Advisory Committee. (2006). Preventing tetanus, diphtheria, and pertussis among adults: Use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccine recommendations of the Advisory Committee on Immunization Practices (ACIP) and recommendation of ACIP, supported by the Healthcare Infection Control Practices Advisory Committee (HICPAC), for use of Tdap among health-care personnel. MMWR. Recommendations and Reports: Morbidity and Mortality Weekly Report. Recommendations and Reports, 55(RR-17), 1–37.
- Gattás, V. L., Luna, E. J. A., Sato, A. P. S., Fernandes, E. G., Vaz-de-Lima, L. R., Sato, H. K., & Castilho, E. A. D. (2020). Adverse event occurrence following use of tetanus, diphtheria and acellular pertussis adsorbed vaccine–Tdap–, São Paulo, SP, Brazil, 2015-2016. Epidemiologia e Serviços de Saúde, 29, e2019280.
- Van Der Zee, A., Schellekens, J. F. P., & Mooi, F. R. (2015). Laboratory Diagnosis of Pertussis. Clinical Microbiology Reviews, 28(4), 1005–1026. [CrossRef]
- Plotkin, S. A., Offit, P. A., DeStefano, F., Larson, H. J., Arora, N. K., Zuber, P. L., ... & Glanz, J. (2020). The science of vaccine safety: summary of meeting at Wellcome Trust. Vaccine, 38(8), 1869-1880. [CrossRef]
- Nwinyi, O. C., & Ajani, O. O. (2010). Identification, and Clinical Relevance of Gram–Positive Spore Formers.
- Doley, R. M., Mahanta, B. N., & Kakati, S. (2016). Diphtheria–An Overview. Assam Journal of Internal Medicine, 6(1), 19.
- Martin, C. J., Donahue, A. S., & Meyer, J. D. (2016). Bacteria. Physical and Biological Hazards of the Workplace, 347-410.
- Greenwood, B. (2014). The contribution of vaccination to global health: past, present and future. Philosophical Transactions of the Royal Society B: Biological Sciences, 369(1645), 20130433.
- Kour, I., Singhal, L., & Gupta, V. (2023). Diphtheria: A Paradigmatic Vaccine-Preventable Toxigenic Disease with Changing Epidemiology. In Recent Advances in Pharmaceutical Innovation and Research (pp. 749-759). Singapore: Springer Nature Singapore.
- Amara, A. A. (2016). Vaccines against Pathogens: A Review and Food For Thought. SOJ Biochem 2 (2), 20. Vaccines against Pathogens: A Review and Food For Thought. [CrossRef]
- Kolybo, D. V., Labyntsev, A. A., Korotkevich, N. V., Komisarenko, S. V., Romaniuk, S. I., & Oliinyk, O. M. (2013). Immunobiology of diphtheria. Recent approaches for the prevention, diagnosis, and treatment of disease. Biotechnologia Acta, 6(4), 043-062.
- World Health Organisation. Diphtheria reported cases and incidence (Internet). WHO. 2023.
- Jain A, Samdani S, Meena V, Sharma MP. Diphtheria: It is still prevalent!!! International Journal of Pediatric Otorhinolaryngology. 2016 Jul;86:68–71.
- CDC. Diphtheria, Tetanus, and Pertussis Vaccine Recommendations (Internet). CDC. 2023. Available from: https://www.cdc.gov/vaccines/vpd/dtap-tdap-td/hcp/recommendations.html.
- Grasse M, Meryk A, Schirmer M, Grubeck-Loebenstein B, Weinberger B. Booster vaccination against tetanus and diphtheria: insufficient protection against diphtheria in young and elderly adults. Immunity & ageing : I & A. 2016 Sep 5;13(1):26. [CrossRef]
- Desai S, Scobie HM, Cherian T, Goodman T. Use of tetanus-diphtheria (Td) vaccine in children 4–7 years of age: World Health Organization consultation of experts. Vaccine. 2020 May;38(21):3800–7. [CrossRef]
- Bajaj, S. (2024, January 12). Why diphtheria is making a comeback. WUSF https://news.wgcu.org/2024-01-23/why-diphtheria-is-making-a-comeback.
- World Health Organization. (2024, February 25). WHO African Region Health Emergency Situation Report: Multi-country Outbreak of Diphtheria - Consolidated Regional Situation Report 006.
- ReliefWeb. (2024, January 11). Guinea: Diphtheria Outbreak Spreads to 33 Prefectures. https://www.who.int/emergencies/disease-outbreak-news/item/2023-DON492.
- Nigeria Centre for Disease Control and Prevention (NCDC). (2023). Diphtheria Situation Report Serial Number 01 Data as of Epi-week 03 2023.
- Niger Ministry of Public Health. (2023). Epidemiological Weekly Report No. 47, 2023 (Report).
- World Health Organization (WHO). (2023, December 12). Diphtheria - Guinea (2023). (Online). Available from: https://reliefweb.int/report/nigeria/who-african-region-health-emergency-situation-report-multi-country-outbreak-diphtheria-consolidated-regional-situation-report-006-january-14-2024.
- Yakum MN, Ateudjieu J, Walter EA, Watcho P. Vaccine storage and cold chain monitoring in the North West region of Cameroon: a cross-sectional study. BMC Research Notes. 2015 Apr 14;8(1). [CrossRef]
- Kartoglu U, Ames H. Ensuring quality and integrity of vaccines throughout the cold chain: the role of temperature monitoring. Expert Review of Vaccines. 2022 Apr 8;21(6):799–810. [CrossRef]
- Barnes, A. The development of a plan for a comprehensive review of the vaccine storage and handling practices in the general practice setting. Memorial University of Newfoundland; 2015.
- Das A, Ilango K. Challenges Of Storage And Transport Of Covid-19 Vaccines–A Review. Journal of Pharmaceutical Negative Results. 2022;4164–72.
- Hunt, GD. Development of an Improved Backpack Container to Enhance Vaccine Distribution in the Cold Chain Systems of Rural Southeast Asia. LeTourneau University; 2019.
- Kartoglu U, Milstien J. Tools and approaches to ensure the quality of vaccines throughout the cold chain. Expert Review of Vaccines. 2014 May 28;13(7):843–54. [CrossRef]
- Swayne DE, Suarez DL, Spackman E, Jadhao S, Dauphin G, Kim-Torchetti M, et al. Antibody Titer Has Positive Predictive Value for Vaccine Protection against Challenge with Natural Antigenic-Drift Variants of H5N1 High-Pathogenicity Avian Influenza Viruses from Indonesia. Journal of Virology. 2015 Apr;89(7):3746–62. [CrossRef]
- Janani M, Venkatesh ND. Clinical evaluation of vaccines. Journal of Pharmaceutical Sciences and Research. 2019;11(5):1775–80.
- Verch T, Trausch JJ, Shank-Retzlaff M. Principles of vaccine potency assays. Bioanalysis. 2018 Feb;10(3):163–80. [CrossRef]
- Sanyal G. Development of functionally relevant potency assays for monovalent and multivalent vaccines delivered by evolving technologies. npj Vaccines. 2022 May 5;7(1). [CrossRef]
- Peretti-Watel, P., Seror, V., Cortaredona, S., Launay, O., Raude, J., Verger, P., Fressard, L., Beck, F., Legleye, S., L’Haridon, O., Léger, D., & Ward, J. K. (2020). A future vaccination campaign against COVID-19 at risk of vaccine hesitancy and politicisation. The Lancet Infectious Diseases, 20(7), 769–770. [CrossRef]
- Dubé, E. (2017). Addressing vaccine hesitancy: The crucial role of healthcare providers. Clinical Microbiology and Infection, 23(5), 279–280. [CrossRef]
- Hou, Z., Tong, Y., Du, F., Lu, L., Zhao, S., Yu, K., Piatek, S. J., Larson, H. J., & Lin, L. (2021). Assessing COVID-19 Vaccine Hesitancy, Confidence, and Public Engagement: A Global Social Listening Study. Journal of Medical Internet Research, 23(6), e27632. [CrossRef]
- World Health Organization (WHO). (2020). Diphtheria vaccine: WHO position paper, August 2017.
- MacDonald, N. E. (2015). Vaccine hesitancy: Definition, scope and determinants. Vaccine, 33(34), 4161–4164. [CrossRef]
- Betsch, C., Schmid, P., Heinemeier, D., Korn, L., Holtmann, C., & Böhm, R. (2018). Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLOS ONE, 13(12), e0208601. [CrossRef]
- Tetanus vaccines: WHO position paper, February 2017 – Recommendations. (2018). Vaccine, 36(25), 3573–3575. [CrossRef]
- Larson, H. J., Schulz, W. S., Tucker, J. D., & Smith, D. M. D. (2015). Measuring Vaccine Confidence: Introducing a Global Vaccine Confidence Index. PLoS Currents. [CrossRef]
- Ozawa, S., Clark, S., Portnoy, A., Grewal, S., Stack, M. L., Sinha, A., Mirelman, A., Franklin, H., Friberg, I. K., Tam, Y., Walker, N., Clark, A., Ferrari, M., Suraratdecha, C., Sweet, S., Goldie, S. J., Garske, T., Li, M., Hansen, P. M., … Walker, D. (2017). Estimated economic impact of vaccinations in 73 low- and middle-income countries, 2001–2020. Bulletin of the World Health Organization, 95(9), 629–638. [CrossRef]
- Grassly, N. C. (2013). The final stages of the global eradication of poliomyelitis. Philosophical Transactions of the Royal Society B: Biological Sciences, 368(1623), 20120140.
- Dubé, E., Laberge, C., Guay, M., Bramadat, P., Roy, R., & Bettinger, J. A. (2013). Vaccine hesitancy: An overview. Human Vaccines & Immunotherapeutics, 9(8), 1763–1773. [CrossRef]
- Allison, M. A., Dunne, E. F., Markowitz, L. E., O’Leary, S. T., Crane, L. A., Hurley, L. P., Stokley, S., Babbel, C. I., Brtnikova, M., Beaty, B. L., & Kempe, A. (2013). HPV Vaccination of Boys in Primary Care Practices. Academic Pediatrics, 13(5), 466–474. [CrossRef]
- Opel, D. J., Heritage, J., Taylor, J. A., Mangione-Smith, R., Salas, H. S., DeVere, V., Zhou, C., & Robinson, J. D. (2013). The Architecture of Provider-Parent Vaccine Discussions at Health Supervision Visits. Paediatrics, 132(6), 1037–1046. [CrossRef]
- Brunson, E. K. (2013). How parents make decisions about their children’s vaccinations. Vaccine, 31(46), 5466–5470. [CrossRef]
- Jacobson, R. M., Targonski, P. V., & Poland, G. A. (2007). A taxonomy of reasoning flaws in the anti-vaccine movement. Vaccine, 25(16), 3146–3152. [CrossRef]
- Ophori, Endurance A., Musa Y. Tula, Azuka V. Azih, Rachel Okojie, and Precious E. Ikpo. 2014. “Current Trends of Immunization in Nigeria: Prospect and Challenges.” Tropical Medicine and Health 42 (2): 67–75. [CrossRef]
- Oluwadare, Christopher. 2009. “The Social Determinants of Routine Immunisation in Ekiti State of Nigeria.” Studies on Ethno-Medicine 3 (1): 49–56. [CrossRef]
- World Health Organization. (2006). The world health report 2006: working together for health. World Health Organization.
- Rosana, Y., Lusiana, D. I. G., & Yasmon, A. (2022). Genetic characterization of diphtheria tox B to evaluate vaccine efficacy in Indonesia. Iranian Journal of Microbiology, 14(4), 606.
- Lee, Min Hye, Gyeoung Ah Lee, Seong Hyeon Lee, and Yeon-Hwan Park. 2020. “A Systematic Review on the Causes of the Transmission and Control Measures of Outbreaks in Long-Term Care Facilities: Back to Basics of Infection Control.” PLOS ONE 15 (3): e0229911. [CrossRef]
- World Health Organization. (2021). Diphtheria vaccine: WHO position paper. Weekly Epidemiological Record, 96(49), 609-620.
- World Health Organization. “Global antimicrobial resistance and use surveillance system (GLASS) report: 2021.” (2021).
- World Health Organization (WHO). (2022). Diphtheria vaccine: WHO position paper, August 2017.
- Idris, I., Ibrahim, I. and Umar, B.A., 2023. Re-emergence of diphtheria in Kano State, Nigeria: Current effort and challenges. Tropical Doctor, 1, p.2.
- Adepoju, V.A. , 2023. An Epidemic in the Making: The Urgent Need to Address the Diphtheria Outbreak in Nigeria: An Outbreak of Diphtheria in Nigeria. Nigerian Medical Journal, 64(1), pp.1-3.
- Africa CDC, 2023. https://africacdc.org/news-item/diphtheria-outbreak-in-africa-strengthening-response-capacities/.
- Cooper, S. and Wiysonge, C.S., 2023. Towards a More Critical Public Health Understanding of Vaccine Hesitancy: Key Insights from a Decade of Research. Vaccines, 11(7), p.1155.
- da Cunha, O.M.G. , 2020. Ruth’s Books: Creating Additional Lives. In The Things of Others: Ethnographies, Histories, and Other Artefacts (pp. 467-535). Brill.
- Medugu, N., Musa-Booth, T.O., Adegboro, B., Onipede, A.O., Babazhitsu, M. and Amaza, R., 2023. A review of the current diphtheria outbreaks. African Journal of Clinical and Experimental Microbiology, 24(2), pp.120-129.
- Oduoye, M.O., Musa, Z.M., Tunde, A.M., Nazir, A., Cakwira, H., Abdulkareem, L., Biamba, C., Akilimali, A., Kibukilza, F. and Nyakio, O., 2023. The recent outbreak of diphtheria in Nigeria is a public health concern for all. IJS Global Health, 6(5), p.e0274.
- Abubakar, M.Y., Lawal, J., Dadi, H. and Grema, U.S., 2020. Diphtheria: a re-emerging public health challenge. International Journal of Otorhinolaryngology and Health and Neck Surgery, 6(1), pp.191-193.
- Pan American Health Organization. (2020). Diphtheria in the Americas.
- Liu, J., Ng, T., Islam, M. A., Mahmud, S. M., Faruque, A. S. G., & Mahmud, S. M. (2021). Diphtheria outbreak in Rohingya refugee camps in Bangladesh, 2020. Clinical Infectious Diseases, 72(12), e832-e834. [CrossRef]
- Ranaivo, A., Randrianasolo, L., Rakotonirina, L. P., Ramanantsoa, A., Herindrainy, P., & Andriantsitohaina, R. (2021). Diphtheria outbreak in Madagascar, 2019-2020: Lessons learned. Vaccine, 39(10), 1422-1427. [CrossRef]
- Diphtheria in asylum workers: forgotten but not gone!. International Journal of Surgery, (2023). [CrossRef]
- Martina, Esposito., Francesca, Minnai., M., Copetti., Giuseppe, Miscio., Rita, Perna., Ada, Piepoli., G., De, Vincentis., Mario, Benvenuto., Paola, D’Addetta., Susanna, Croci., Margherita, Baldassarri., Mirella, Bruttini., Chiara, Fallerini., Raffaella, Brugnoni., Paola, Cavalcante., Fulvio, Baggi., E., Corsini., Emilio, Ciusani., Francesca, Andreetta., Tommaso, A, Dragani., Maddalena, Fratelli., Massimo, Carella., Renato, E, Mantegazza., Alessandra, Renieri., Francesca, Colombo. Human leukocyte antigen variants associate with BNT162b2 mRNA vaccine response. Communications medicine, (2024). [CrossRef]
Figure 3.
Trends in DPT vaccination coverage data in West Africa.
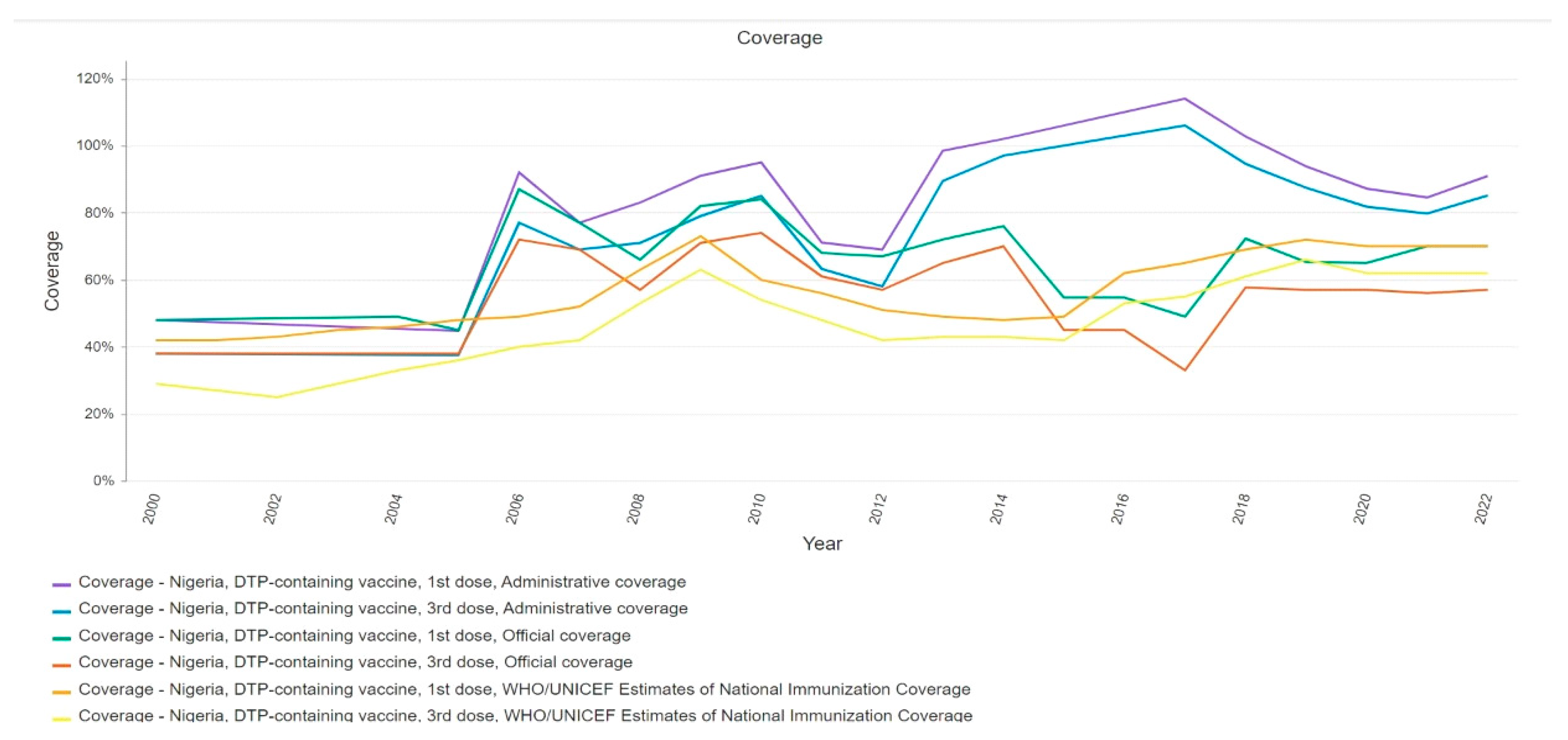

Table 1.
Vaccine types and Schedule.
| Vaccine Type | Description | Age Group | Primary Series Schedule | Booster Dose Schedule | Key References |
|---|---|---|---|---|---|
| DTP (Whole-cell) | Contains inactivated whole cells of Bordetella pertussis, along with diphtheria and tetanus toxoids | Infants and young children | 2, 4, 6 months | 15-18 months, 4-6 years | Cherry M, et al. J Infect Dis. 1980;142(6):563-572. Greco P, et al. N Engl J Med. 1996;334(6):341-348. |
| DTaP (Acellular) | Contains purified antigens of Bordetella pertussis, diphtheria, and tetanus toxoids | Infants and young children | 2, 4, 6 months | 15-18 months, 4-6 years | Klein ES, et al. Pediatrics. 2001;108(3):1-9. Schmitt B, et al. Pediatrics. 1998;101(1):1-7. |
| DT (Pediatric) | Contains diphtheria and tetanus toxoids, used when pertussis component is contraindicated | Children with contraindications to pertussis vaccine | 2, 4, 6 months | 15-18 months, 4-6 years | Healy JC, et al. Pediatrics Rev. 1998;19(2):70-77. |
| Td (Adult) | Contains lower doses of diphtheria and tetanus toxoids, used as a booster for adults | Adolescents and adults | - | Every 10 years after the initial Tdap dose | Zeigler PE, et al. JAMA. 2002;288(6):665-670. Plotkin LC, et al. Clin Infect Dis. 2003;35(2):246-252. |
| Tdap (Adult/Pediatric) | Contains lower doses of diphtheria, tetanus toxoids, and acellular pertussis, used as a booster for older children, adolescents, and adults | Adolescents (11-12 years) and adults | - | 11-12 years (single dose), then Td every 10 years | Quinn MJR, et al. Vaccine. 2006;24(33-34):5686-5694. Cohn SP, et al. J Infect Dis. 2015;212(3):S10-S17. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



