
Submitted:
17 July 2024
Posted:
17 July 2024
You are already at the latest version
Abstract
The purpose of this narrative review is to provide an overview of the latest literature on bariatric and metabolic surgery for diabetes mellitus type II and obesity (diabesity) and to discuss its implications for future research and clinical practice.
Keywords:
bariatric surgery
; metabolic surgery
; diabetes mellitus type II
; diabesity
1. Introduction
Type II diabetes mellitus (T2DM) is a chronic metabolic disorder characterized by hyperglycemia, insulin resistance, and relative insulin deficiency [1]. It does affect millions of people worldwide and is associated with significant morbidity and mortality.
The prevalence of T2DM has been steadily increasing over the past few decades, largely due to the rise in obesity rates hence representing a major public health concern at global level [2].
Bariatric surgery is a gastrointestinal surgical treatment focused on achieving weight loss in individuals with obesity [3]. The swift metabolic impacts of these surgeries have justified the shift in terminology from bariatric to metabolic terminology (bariatric and metabolic surgery – BMS) , as improvements in metabolic disorders are frequently seen prior to significant weight loss [4].
Several studies have shown that BMS can lead to significant improvements in glycemic control, insulin sensitivity, and even remission of T2DM in some patients. However, the mechanisms by which BMS exerts its beneficial effects on T2DM have not been fully elucidated yet [5].
The purpose of this narrative review is to provide an overview of the latest literature on BMS for T2DM and obesity. We will discuss the current state of the research field, highlight key publications, and explore controversial and diverging hypotheses. The main aim of this review is to summarize the robust scientific evidence supporting the use of metabolic surgery as a treatment for T2DM and to discuss its implications for future research and clinical practice.
2. Current State of Research
2.1. Established and Emerging Bariatric and Metabolic Surgery Procedures
The most widely performed metabolic surgeries include vertical sleeve gastrectomy (VSG) and Roux-en-Y gastric bypass (RYGBP). VSG involves the removal of ~80% of the stomach along the greater curvature (Figure 1a). By contrast, RYGB entails the creation of a small gastric pouch out of the most cephalad portion of the stomach (gastric restriction) at a close distance from the gastro-esophageal junction and re-routing of the intestinal tract, such that ingested food bypasses 95% of the stomach, the duodenum and proximal jejunum by emptying directly into the jejunum (Figure 1b). The laparoscopic gastric band, that at some point was the most performed procedure, has eventually lost favor over the past decade or so due to serious concerns about its long-term efficacy and complications that have led to a surge of removal and conversion to VSG or others BMS procedures [6].
In recent years, newer BMS procedures have gained widespread acceptance. For instance, the technical difficulty and the risk of developing internal hernias associated with the gold standard RYGB led to the introduction of the much simpler one anastomosis gastric bypass (OAGB) Figure 1c). However, the greater simplicity, potential reversibility, and the non-inferior outcomes of OAGB compared to the RYGB, must be weighed against its main pitfall that is bile reflux [7]. Single anastomosis duodeno-ileal bypass with sleeve gastrectomy (SADI-S) (Figure 1d) has been suggested as alternative to OAGB and RYGBP. This procedure has shown similar metabolic efficacy of OAGB and RYGB with even greater remission of T2DM and without the bile reflux associated with the former or the need to re-reconstruct the bowel continuity between alimentary and biliary limb associated with the latter; moreover, SADI-S retains the principles of biliopancreatic diversion along with pylorus preservation. All the benefits of SADI-S must be weighed against its reported higher rates of early complications and mortality [8]. Thus, further research is needed to determine which will be the next gold standard procedure. Both procedures (OAGB and SADI-S) have been shown to reduce body weight, improve insulin sensitivity, increase insulin secretion, and lead to remission of T2DM in a significant proportion of patients [8].
2.2. Key Scientific Evidence Supporting the Use of Bariatric and Metabolic Surgery
Recent randomized controlled trials and meta-analyses have demonstrated that BMS is more effective than medical therapy alone in achieving long-term glycemic control and weight loss in patients with T2DM and obesity, condition that is being more frequently named as “diabesity”. The randomized, controlled, single-center STAMPEDE trial involved 150 obese patients who were assigned, in a 1:1:1 ratio, to one of the three study groups in which the effects of intensive medical therapy were compared with those of RYGB or VSG. Only 5% of the patients in the medical-therapy group met the primary end point (glycated hemoglobin level ≤ 6.0%) at 3 years as compared with 38% of those in the RYGB group (P<0.001) and 24% of those in the VSG group (P=0.01). Furthermore, patients undergoing BMS had greater mean percentage reductions in weight from baseline, with reductions of 24.5±9.1% in the GBP group and 21.1±8.9% in the VSG group, as compared with a reduction of 4.2±8.3% in the medical-therapy group (P<0.001 for both comparisons). Lastly, quality-of-life rates were significantly better in the BMS groups than in the group being managed with medical-therapy [9]. These differences between the two BMS groups and the medical therapy group persisted at 5 years although the absolute numbers were lower in each group as the criterion for the primary end point was met by 2 of 38 patients (5%) in the medical group vs. 14 of 49 patients (29%) and 11 of 47 patients (23%) who underwent GBP and VSG respectively. Patients who underwent BMS had greater mean percentage reduction from baseline in glycated hemoglobin level than did patients who received medical therapy alone (2.1% vs. 0.3%, P=0.003). At 5 years, changes from baseline observed in the BMS groups were greater to the changes witnessed in the medical-therapy group with respect also to body weight, triglyceride levels, high-density lipoprotein cholesterol levels, use of insulin, and quality-of-life measures (P<0.05 for all comparisons) [10].
The most recent pooled analysis ARMMS-T2D (Alliance of Randomized Trials of Medicine vs Metabolic Surgery in Type 2 Diabetes) conducted between May 2007 and August 2013 and including 4 USA-based single-center randomized trials, confirmed the positive findings of prior randomized trials indicating superior glycemic control with fewer diabetes medication and higher rates of diabetes remission in patients originally randomized to undergo BMS compared to patients receiving medical/lifestyle intervention only.
The observational follow-up of the ARMMS-T2D reached through July 2022 and included all participants who had been randomized to undergo medical/lifestyle management or BMS (RYGB, VSG, or adjustable gastric banding respectively) [11]. Change in hemoglobin A1c (HbA1c) from baseline to 7 years was set as the primary outcome for all participants although data are reported for up to 12 years. A total of 262 out of 305 eligible participants (86%) enrolled in long-term follow-up for this pooled analysis. At 7 years, HbA1c decreased by 0.2% (95% CI, -0.5% to 0.2%), from a baseline of 8.2%, in the medical/lifestyle group and by 1.6% (95% CI, -1.8% to -1.3%), from a baseline of 8.7%, in the BMS group. The between-group difference was -1.4% (95% CI, -1.8% to -1.0%; P < .001) at 7 years and -1.1% (95% CI, -1.7% to -0.5%; P = .002) at 12 years. The BMS group required fewer antidiabetic medications. Diabetes remission was greater after BMS (6.2% in the medical/lifestyle group vs 18.2% in the BMS group; P = .02) at 7 years and at 12 years (0.0% in the medical/lifestyle group vs 12.7% in the BMS group; P < .001) [11].
Increases in liver, adipose tissue, and muscle insulin sensitivity and in β-cell function are well known effects of weight loss. However, a large body of scientific evidence has clearly shown that BMS leads to a rapid improvement of glycemic control, enabling discontinuation of insulin and other glucose lowering medications, even before substantial weight loss has ensued (Table 1).
Hence, additional mechanisms might add to both early and sustained metabolic improvements after BMS [12].
With RYGB nutrients enter the intestine very rapidly as there is no pylorus or antrum to slow them down. With VSG the increase of post-prandial gastric pressure leads to faster gastric emptying. These changes in nutrient exposure are believed to affect intestinal structure and function in both surgeries. Intestinal hypertrophy has been demonstrated in both human and rodent studies, with shifts in glucose metabolism towards pathways that support tissue growth and increase in 18F-fluorodeoxyglucose uptake in multiple intestinal segments in correlation with reduced fasting blood levels of glucose [12].
Increased lipid accumulation in the liver is associated with impaired hepatic insulin sensitivity. BMS is highly effective at lowering the levels of hepatic lipids and is an effective treatment for non-alcoholic fatty liver disease [13]. In humans, reductions in hepatic levels of triglycerides and fibrosis occur after BMS that translates in an overall improved hepatic insulin sensitivity [12].
Likewise, both short-term and long-term studies find improvements in whole-body insulin sensitivity that are not correlated with a patient’s weight loss pointing out a bettered adipose and skeletal muscle insulin sensitivity after BMS [12].
Higher circulating levels of glucagon are observed postprandially after BMS compared with pre-BMS status, suggesting that BMS is altering pancreatic α-cell function. However, BMS effects are not limited to the α-cells but relates to the β-cells too. After BMS, rapid increases in postprandial blood levels of glucose related to the rapid entry of nutrients into the intestine are paralleled by rapid surges in insulin secretion that quickly return to baseline. Furthermore, fasting insulin and the total insulin output in response to intravenous glucose are reduced after BMS consistent with enhanced insulin sensitivity and a change of the dynamic response of insulin to nutrient ingestion.
Another major contributor to increased postprandial plasma levels of insulin after BMS is represented by the marked increase in plasma levels of incretin hormones, the gut peptides which are traditionally recognized to be secreted by L cells in the distal gut. The greatest interest has been received so far by the incretin hormone glucagon-like peptide 1 (GLP1) whose levels rise over 10-fold after BMS although there is a whole host of gut peptides that also increase postprandially in patients who underwent BMS and are subject of further investigation. The dramatic increase in post-prandial GLP1 secretion after BMS is widely believed to have a role in mediating the improvements in glucose homeostasis that occur early on after BMS and before significant weight loss has already occurred [14].
Other incretins have also been identified to play a role in generating the beneficial metabolic effects of BMS. For instance, the plasma levels of ghrelin are substantially reduced whilst the plasma levels of cholecystokinin (CCK) and gastric inhibitory peptide (GIP) are markedly increased after VSG [15].
The most prominent metabolic effect of ghrelin is the stimulation of appetite via activation of orexigenic hypothalamic axis and the food-intake independent stimulation of lipogenesis, which both lead to an increase in body weight and adiposity. However, recent scientific evidence is emerging that suggest a therapeutic value of pharmacological inhibition of ghrelin signaling by improving insulin resistance and T2DM. Hence ghrelin may play a role with the regulation of glucose metabolism as well [16].
CCK has been traditionally regarded as a peptide with the sole purpose of triggering gallbladder contraction and regulating digestion. On the contrary, recent evidence has emerged that supports a role for CCK in the modulation of insulin secretion. For instance, it does appear that the infusion of pharmacological levels (24 pmol/kg h) of CCK in humans will stimulate insulin secretion. Hence, the pharma industry is currently looking at the development of CCK-based pharmacotherapy to treat T2DM [17]. Lastly, like GLP-1, GIP stimulates glucose-dependent insulin release, and is also known to inhibit beta-cell apoptosis and promote beta-cell proliferation [17].
Plasma levels of both total and specific bile acids increase significantly after BMS [18]. Bile acids are synthesized in the liver and secreted into the intestine and function as signaling molecules at multiple target organs via FXR (expressed in the intestine, liver, adipose tissue, pancreas, and adrenal gland) and TGR5 (expressed in the gall bladder, ileum, colon, adipose tissue, liver, skeletal muscle, and immune cells) receptors. The activation of TGR5 by the bile acids increases GLP-1 secretion. Hence, bile acids represent an attractive target to improve the success of bariatric surgery.
The profound changes of the intestinal anatomy and its function produced by BMS lead to a shift in the composition and diversity of the intestinal microbiome. An improved regulation of bile acids metabolism is among others one of the mechanisms suggested to explain the favorable effect of microbiome changes after BMS that contributes to T2DM control [19].
2.3. Optimal timing of Bariatric and Metabolic Surgery
The optimal timing of surgery during diabetes and the selection criteria for surgery have been matter of debate over the past decade. Some studies have suggested that earlier intervention with surgery may lead to better outcomes, while others have shown that delaying surgery can still result in significant improvements in diabetes control. Additionally, not all patients with diabesity are suitable candidates for metabolic surgery, and careful patient selection is crucial to ensure favorable outcomes.
In October 2022 the two main governing bodies in the field of BMS (International Federation for the Surgery of Obesity and Metabolic Disorders - IFSO and the American Society for Metabolic and Bariatric Surgery - ASMBS) decided it was time to revise the existing 1991 NIH consensus guidelines.
Under the newer IFSO/ASMBS 2022 guidelines all individuals with a BMI>35 kg/m2 may be eligible for surgery, regardless of the presence of underlying health problems, while those with a BMI>30 may be considered for surgery in cases of diabetes (diabesity) or for those who have not been able to maintain long-lasting weight loss [20].
Furthermore, the IFSO and ASMBS agreed that BMI thresholds should be adjusted for the Asian population, since individuals of these ethnicities typically suffer negative health outcomes at a lower BMI.
2.4. Bariatric and Metabolic surgery and Advancements in Pharmacotherapy
In the past few years, we have witnessed some significant advancements in the development of targeted treatments for monogenic obesities that lead to the introduction of a new generation of incretin-based therapies. This novel class of incretin agonist can be grouped in three main categories based on their single or multiple receptor targets (Figure 2) [21].
Single Incretin Agonists
GLP-1 receptor agonists (GLP-1Ras), such as liraglutide and semaglutide, have shown to be effective in weight reduction and improvement of glycemic control by enhancing insulin secretion, delaying gastric emptying, and promoting satiety. Semaglutide can be injected subcutaneously once a week or taken as a once daily tablet. The STEP clinical trials together provide worthy information about semaglutide’s safety, efficacy, and impact on weight loss and cardiovascular outcomes in various patient populations treated with once-weekly subcutaneous administration of semaglutide at a dose of 2.4 mg. Roughly 15% weight loss was observed in overweight and obese, non-diabetic adults across various treatment periods, lasting up to 2 years. Conversely, a smaller but significant 9.6% weight loss was observed in patients with diabesity in the STEP-2 trial [22]. Further light on the efficacy of first generation GLP-1Ras has been shed very recently by an observational, retrospective cohort study based on data obtained from the electronic medical records of largest health care organization in Israel. Dicker et al. study included 6070 subjects aged 24 years or older, who had diabesity and no prior history of ischemic heart disease, ischemic stroke, or congestive heart failure. Patients who underwent BMS and patients who received GLP-1RAs from January 1, 2008, through December 31, 2021, were matched 1:1 by age, sex, and clinical traits and followed for a median of 6.8 years (range 4.1-9.4 years). BMS was associated with greater weight loss and lesser mortality compared with GLP-1RAs among individuals with a diabetes duration of 10 years or less [23]. It is likely that the lower mortality of the surgical group of patients could have been mediated through the significantly greater weight loss achieved in the same.
Dual Incretin Agonists
GLP-1/GIP Agonists: Dual agonists that target both GLP-1 and glucose-dependent insulinotropic polypeptide (GIP) receptors, have displayed improved glycemic control and greater weight loss compared to single agonists in various clinical trials. Tirzepatide was approved in the United States and Europe in 2022 for the treatment of T2DM and is the most widely studied representative of this class of double agonists (DAs).
In the Phase 3 SURPASS-1-5 studies, which included >6000 people with T2DM, tirzepatide was associated with clinically meaningful reductions in HbA1c and weight loss when used as monotherapy, in combination with basal insulin or in comparison to semaglutide, insulin glargine and insulin degludec [24].
Additionally, tirzepatide significantly reduced weight in obese T2DM patients in a dose-dependent manner; by weeks 40–52 of the trials, the 5 mg dose of tirzepatide resulted in a weight loss of 6.2–7.8 kg, the 10 mg dose led to a weight loss of 7.8–10.7 kg, and the 15 mg dose caused a weight loss of 9.5–12.9 kg [24].
A comparison between tirzapatide and BMS can be extrapolated from a mathematical modeling study that simulated mean weight- and fat-loss trajectories in response to diet restriction, semaglutide 2.4 mg, tirzepatide 10 mg, and Roux-en-Y gastric bypass (RYGB). All interventions except diet restriction substantially weakened the appetite feedback control circuit, resulting in an extended period of weight loss prior to the plateau. However, the simulated BMS intervention resulted in a persistent magnitude more than three-fold greater than diet restriction and two-fold than tirzepatide and semaglutide. Nevertheless, no comparative data on the effect of the three simulated interventions over T2DM amelioration or remission in obese patients were generated by this study [25].
GLP-1/Glucagon Agonists: Glucagon reduces appetite and food intake whilst favorably altering lipid metabolism and energy expenditure, making it an attractive option for the treatment of T2DM and obesity, especially when combined with the insulinotropic effects of GLP-1. In recent years, two GLP-1/Glucagon agonists underwent phase II clinical trials in human experiments but only one of the two (cotadutide) has so far completed its development. Cotadutide effectively improved glycemic control and reduced weight in patients with diabesity whilst increasing insulin secretion and delaying gastric emptying; with the most common side effects being dose-dependent nausea and vomiting [26]. Furthermore, a multicenter study evaluated the effects of subcutaneously administered cotadutide in 834 participants in daily doses of 100 µg, 200 µg, and 300 µg compared with placebo and 1.8 mg liraglutide daily [27]. The study lasted for 54 weeks and assessed liver abnormalities and metabolic parameters in patients with diabesity. Every dose of cotadutide and liraglutide significantly reduced HbA1c levels compared to placebo. The highest dose of cotadutide resulted in a significantly greater reduction in weight compared to liraglutide and placebo and significant improvement in liver enzyme levels and parameters indicative of liver fibrosis compared to liraglutide setting the basis for a possible use of cotadutide towards the treatment of MAFLD. No comparative studies between cotadutide and BMS have so far been implemented.
Triple Incretin Agonists: Emerging therapies that target GLP-1, GIP, and glucagon receptors hold promise to further strengthen metabolic benefits of single and dual therapies. A phase 1b, multicenter, double blind, placebo controlled and randomized trial investigating the novel triple agonist retatrutide in patients with T2DM, showed significant reductions in body weight and HbA1c by the end of the 12th week compared to baseline values whilst exhibiting a safety and tolerability profile like other incretin formulations [28]. No comparative data between retatrutide and BMS are currently available.
Altogether peptide-based therapies (single-, double- or triple-agonists) hold promise for the treatment of diabesity thank to their ability to effectively regulate glucose metabolism and body weight. However, peptides often display poor stability and are susceptible to rapid degradation, which limits their therapeutic and clinical applications potential.
Even though the preliminary results of the clinical trials investigating the efficacy of these novel anti-obesity medications are encouraging long-term data on safety, efficacy, and cardiovascular outcomes are to be gathered yet [21]. As of right now, the reported weight loss (greater than 10% of overall bodyweight in more than two-thirds of clinical trial participants) are far from reaching the durable weight loss of 25% reported by the long-term studies of BMS that are also associated with rapid, sustained improvements in complications of obesity.
Likewise, future research and development will have to address some concerns about the safety profile of these medications as the relatively benign and most common side effects associated with their use (gastrointestinal disturbances, severe nausea and/or vomiting) may be exaggerated by the much more concerning and severe hypoglycemia due to excessive lowering of blood sugar levels [29]. On the other side, BMS carries the risk of gastro-intestinal disturbances both peri-operatively and on the long-term (nutritional deficiencies) and although its associated mortality has been steadily decreasing overtime is not and unlikely will ever be nihil due to the inherent risk associated with a surgical intervention under general anesthesia.
In the next future we will likely assist to a rising number of comparative studies exploring the efficacy of these new-generation anti-obesity medications against BMS. There is certainly a great need for this kind of comparative research.
Meanwhile a mounting body of research is suggesting a novel role of the pharmacotherapy not as alternative but as complementary therapy to BMS. Medications such as sodium-glucose cotransporter 2 (SGLT2) inhibitors, GLP-1 receptor agonists, and combination therapies, are showing potential for maximizing weight loss, improving metabolic outcomes, and lowering the risk of weight regain after BMS. However, optimal timing, duration, and which combinations of pharmacotherapy to use altogether with BMS are still to be elucidated. Nonetheless, the integration of BMS with pharmacotherapy is emerging as a promising approach to managing diabesity and does provide patients with added options for achieving sustainable weight loss and bettering their metabolic well-being [30,31].
3. Discussion
Overall, the evidence supporting the use of metabolic surgery for diabesity is strong and continues to grow. Several long-term studies have shown that BMS can lead to sustained improvements in glycemic control, reduce the need for diabetes medications, and lower the risk of diabetes-related complications. In some cases, BMS has even resulted in complete remission of T2DM, with normalization of blood sugar levels without the need for medication.
The benefits of BMS extend beyond glycemic control to include improvements in cardiovascular risk factors, such as hypertension, dyslipidemia, and obstructive sleep apnea. Weight loss after surgery can also lead to improvements in quality of life, physical function, and mental health. However, it is important to note that BMS is not without risks, and patients must be carefully evaluated and monitored both before and after surgery to minimize complications.
Future research directions in the field of BMS for diabesity should focus on elucidating the underlying mechanisms of action, identifying biomarkers for predicting which patients are most likely to benefit from surgery, optimizing surgical techniques to maximize outcomes, and developing personalized treatment approaches. Long-term studies are needed to assess the durability of the metabolic benefits of BMS and to evaluate the impact of surgery on diabetes-related microvascular and macrovascular complications.
The latest generation of anti-obesity medications has so far produced very promising results. Paradoxically, the great enthusiasm generated around these pharmacological interventions has somehow limited their potential spectrum of clinical applications meaning that so far, they have been developed and are being investigated as a potential replacement for the more invasive BMS. This blunt parting is hard to comprehend especially in consideration of the fact that the two therapeutic options (pharmacotherapy and BMS) share common mechanistic actions and have both some limitations and thus they could benefit from each other. For instance, an area of special interest for the surgical community is represented by those patients who did well or very well after BMS, but overtime eventually regained some weight. The newer anti-obesity and anti-diabesity medications should be a critical component of the therapeutic armamentarium at the hand of the bariatrician and endocrinologist who these patients should be referred to by the BMS team. This focus on integrative and combined approaches, could represent the ultimate solution to some of the longstanding challenges in achieving lasting weight loss and could virtually eliminate or greatly reduce the need for revisional BMS, which is associated by definition to a significantly higher risk of peri- and post-operative complications in comparison to the initial BMS.
4. Conclusions
BMS is a valuable treatment option for patients with diabesity, offering significant improvements in glycemic control, weight loss, and overall health. While more research is needed to fully understand the mechanisms of action and long-term effects of surgery, the current evidence supports the use of BMS as an effective and sustainable treatment for T2DM. Further studies are warranted to refine patient selection criteria, optimize surgical techniques, evaluate the impact of surgery on diabetes outcomes in diverse populations and to better define the role of novel pharmacotherapy in conjunction and/or in comparison with BMS.
Author Contributions
Conceptualization, A.G. and P.B.; methodology, A.G..; writing—original draft preparation, A.G..; writing—review and editing, A.G; P.B.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Petersen MC, Shulman GI. Mechanisms of Insulin Action and Insulin Resistance. Physiol Rev. 2018 Oct 1;98(4):2133-2223. [CrossRef] [PubMed] [PubMed Central]
- Jervell J. Diabetes i et internasjonalt perspektiv [Diabetes in international perspective]. Tidsskr Nor Laegeforen. 2000 Sep 20;120(22):2686-9. Norwegian. [PubMed]
- Buchwald H, Avidor Y, Braunwald E, Jensen MD, Pories W, Fahrbach K, Schoelles K. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004 Oct 13;292(14):1724-37.
- Cummings DE, Rubino F. Metabolic surgery for the treatment of type 2 diabetes in obese individuals. Diabetologia. 2018 Feb;61(2):257-64.
- Russel SM, Valle V, Spagni G, Hamilton S, Patel T, Abdukadyrov N, Dong Y, Gangemi A. Physiologic Mechanisms of Type II Diabetes Mellitus Remission Following Bariatric Surgery: a Meta-analysis and Clinical Implications. J Gastrointest Surg. 2020 Mar;24(3):728-741. Epub 2020 Jan 2. [CrossRef] [PubMed]
- Gangemi A, Russel S, Patel K, Khalaf H, Masrur M, Hassan C. Conversion to laparoscopic sleeve gastrectomy after failure of laparoscopic gastric band: A systematic review of the literature and cost considerations. Obes Res Clin Pract. 2018 Sep-Oct;12(5):416-420. Epub 2018 Feb 13. [CrossRef] [PubMed]
- Ferrer-Márquez M, García-Redondo M, Maturana-Ibáñez V, Estébanez-Ferrero B, Fernández-Alonso A, Rubio-Gil F, Zamora Soler JA, Ferrer-Ayza M. Bile reflux and marginal ulcers after one-anastomosis gastric bypass (OAGB). A narrative review. Cir Esp (Engl Ed). 2023 Oct;101 Suppl 4:S69-S75. Epub 2023 Apr 19. [CrossRef] [PubMed]
- Balamurugan G, Leo SJ, Sivagnanam ST, Balaji Prasad S, Ravindra C, Rengan V, Arora E, Bindal V. Comparison of Efficacy and Safety Between Roux-en-Y Gastric Bypass (RYGB) vs One Anastomosis Gastric Bypass (OAGB) vs Single Anastomosis Duodeno-ileal Bypass with Sleeve Gastrectomy (SADI-S): a Systematic Review of Bariatric and Metabolic Surgery. Obes Surg. 2023 Jul;33(7):2194-2209. Epub 2023 May 4. [CrossRef] [PubMed]
- Schauer PR, Bhatt DL, Kirwan JP, Wolski K, Brethauer SA, Navaneethan SD, Aminian A, Pothier CE, Kim ES, Nissen SE, Kashyap SR; STAMPEDE Investigators. Bariatric surgery versus intensive medical therapy for diabetes--3-year outcomes. N Engl J Med. 2014 May 22;370(21):2002-13. Epub 2014 Mar 31. [CrossRef] [PubMed] [PubMed Central]
- Schauer PR, Bhatt DL, Kirwan JP, Wolski K, Aminian A, Brethauer SA, Navaneethan SD, Singh RP, Pothier CE, Nissen SE, Kashyap SR; STAMPEDE Investigators. Bariatric Surgery versus Intensive Medical Therapy for Diabetes - 5-Year Outcomes. N Engl J Med. 2017 Feb 16;376(7):641-651. [CrossRef] [PubMed] [PubMed Central]
- Courcoulas AP, Patti ME, Hu B, Arterburn DE, Simonson DC, Gourash WF, Jakicic JM, Vernon AH, Beck GJ, Schauer PR, Kashyap SR, Aminian A, Cummings DE, Kirwan JP. Long-Term Outcomes of Medical Management vs Bariatric Surgery in Type 2 Diabetes. JAMA. 2024 Feb 27;331(8):654-664. [CrossRef] [PubMed] [PubMed Central]
- Sandoval DA, Patti ME. Glucose metabolism after bariatric surgery: implications for T2DM remission and hypoglycaemia. Nat Rev Endocrinol. 2023 Mar;19(3):164-176. Epub 2022 Oct 26. [CrossRef] [PubMed] [PubMed Central]
- Baldwin D, Chennakesavalu M, Gangemi A. Systematic review and meta-analysis of Roux-en-Y gastric bypass against laparoscopic sleeve gastrectomy for amelioration of NAFLD using four criteria. Surg Obes Relat Dis. 2019 Dec;15(12):2123-2130. Epub 2019 Sep 18. [CrossRef] [PubMed]
- Dirksen C. et al. Exaggerated release and preserved insulinotropic action of glucagon-like peptide-1 underlie insulin hypersecretion in glucose-tolerant individuals after Roux-en-Y gastric bypass. Diabetologia 56, 2679–2687 (2013).
- Nosso G. et al. Comparative effects of Roux-en-Y gastric bypass and sleeve gastrectomy on glucose homeostasis and incretin hormones in obese type 2 diabetic patients: a one-year prospective study. Horm. Metab. Res 48, 312–317 (2016).
- Poher AL, Tschöp MH, Müller TD. Ghrelin regulation of glucose metabolism. Peptides. 2018 Feb;100:236-242. [CrossRef] [PubMed] [PubMed Central]
- Pathak V, Flatt PR, Irwin N. Cholecystokinin (CCK) and related adjunct peptide therapies for the treatment of obesity and type 2 diabetes. Peptides. 2018 Feb;100:229-235. [CrossRef] [PubMed]
- Patti M-EE et al. Serum bile acids are higher in humans with prior gastric bypass: potential contribution to improved glucose and lipid metabolism. Obesity 17, 1671–1677 (2009).
- Fouladi F. et al. The role of the gut microbiota in sustained weight loss following Roux-en-Y gastric bypass surgery. Obes. Surg 29, 1259–1267 (2019).
- Eisenberg D, Shikora SA, Aarts E, Aminian A, Angrisani L, Cohen RV, de Luca M, Faria SL, Goodpaster KPS, Haddad A, Himpens JM, Kow L, Kurian M, Loi K, Mahawar K, Nimeri A, O’Kane M, Papasavas PK, Ponce J, Pratt JSA, Rogers AM, Steele KE, Suter M, Kothari SN. 2022 American Society of Metabolic and Bariatric Surgery (ASMBS) and International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO) Indications for Metabolic and Bariatric Surgery. Obes Surg. 2023 Jan;33(1):3-14. doi:10.1007/s11695-022-06332-1. Erratum in: Obes Surg. 2023 Jan;33(1):15-16. [CrossRef] [PubMed] [PubMed Central]
- Sztanek F, Tóth LI, Pető A, Hernyák M, Diószegi Á, Harangi M. New Developments in Pharmacological Treatment of Obesity and Type 2 Diabetes-Beyond and within GLP-1 Receptor Agonists. [Biomedicines. 2024 Jun 13;12(6):1320. [CrossRef] [PubMed] [PubMed Central]
- Davies, M.; Færch, L.; Jeppesen, O.K.; Pakseresht, A.; Pedersen, S.D.; Perreault, L.; Rosenstock, J.; Shimomura, I.; Viljoen, A.; Wadden, T.A.; et al. Semaglutide 2·4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2): A randomised, double-blind, double-dummy, placebo-controlled, phase 3 trial. Lancet 2021, 397, 971–984.
- Dicker D, Sagy YW, Ramot N, Battat E, Greenland P, Arbel R, Lavie G, Reges O. Bariatric Metabolic Surgery vs Glucagon-Like Peptide-1 Receptor Agonists and Mortality. JAMA Netw Open. 2024 Jun 3;7(6):e2415392. [CrossRef] [PubMed] [PubMed Central]
- De Block, C.; Bailey, C.; Wysham, C.; Hemmingway, A.; Allen, S.E.; Peleshok, J. Tirzepatide for the treatment of adults with type 2 diabetes: An endocrine perspective. Diabetes Obes. Metab. 2023, 25, 3–17.
- Hall KD. Physiology of the weight-loss plateau in response to diet restriction, GLP-1 receptor agonism, and bariatric surgery. Obesity (Silver Spring). 2024 Jun;32(6):1163-1168. Epub 2024 Apr 22. [CrossRef] [PubMed] [PubMed Central]
- Parker VER, Robertson D, Wang T, Hornigold DC, Petrone M, Cooper AT, Posch MG, Heise T, Plum-Moerschel L, Schlichthaar H, Klaus B, Ambery PD, Meier JJ, Hirshberg B. Efficacy, Safety, and Mechanistic Insights of Cotadutide, a Dual Receptor Glucagon-Like Peptide-1 and Glucagon Agonist. J Clin Endocrinol Metab. 2020 Mar 1;105(3):dgz047. [CrossRef] [PubMed]
- Nahra R, Wang T, Gadde KM, Oscarsson J, Stumvoll M, Jermutus L, Hirshberg B, Ambery P. Erratum. Effects of Cotadutide on Metabolic and Hepatic Parameters in Adults With Overweight or Obesity and Type 2 Diabetes: A 54-Week Randomized Phase 2b Study. Diabetes Care 2021;44:1433-1442. Diabetes Care. 2022 Dec 1;45(12):3112. doi:10.2337/dc22-er12. Erratum for: Diabetes Care. 2021 Jun;44(6):1433-1442. [CrossRef] [PubMed] [PubMed Central]
- Urva S, Coskun T, Loh MT, Du Y, Thomas MK, Gurbuz S, Haupt A, Benson CT, Hernandez-Illas M, D’Alessio DA, Milicevic Z. LY3437943, a novel triple GIP, GLP-1, and glucagon receptor agonist in people with type 2 diabetes: a phase 1b, multicentre, double-blind, placebo-controlled, randomised, multiple-ascending dose trial. Lancet. 2022 Nov 26;400(10366):1869-1881. Epub 2022 Oct 27. [CrossRef] [PubMed]
- Perdomo CM, Cohen RV, Sumithran P, Clément K, Frühbeck G. Contemporary medical, device, and surgical therapies for obesity in adults. Lancet. 2023 Apr 1;401(10382):1116-1130. Epub 2023 Feb 9. [CrossRef] [PubMed]
- Bailey CJ. Glucose-lowering therapies in type 2 diabetes: Opportunities and challenges for peptides. Peptides. 2018 Feb;100:9-17. [CrossRef] [PubMed]
- Alabduljabbar K, le Roux CW. Pharmacotherapy before and after bariatric surgery. Metabolism. 2023 Nov;148:155692. Epub 2023 Sep 18. [CrossRef] [PubMed]
Figure 1.
a. Vertical Sleeve Gastrectomy (VSG) b. Roux-en-Y gastric bypass (RYGBP) c. One anastomosis gastric bypass (OAGB) d. Single anastomosis duodeno-ileal bypass with sleeve gastrectomy (SADI-S). © Dr Levent Efe, courtesy of IFSO.
Figure 1.
a. Vertical Sleeve Gastrectomy (VSG) b. Roux-en-Y gastric bypass (RYGBP) c. One anastomosis gastric bypass (OAGB) d. Single anastomosis duodeno-ileal bypass with sleeve gastrectomy (SADI-S). © Dr Levent Efe, courtesy of IFSO.
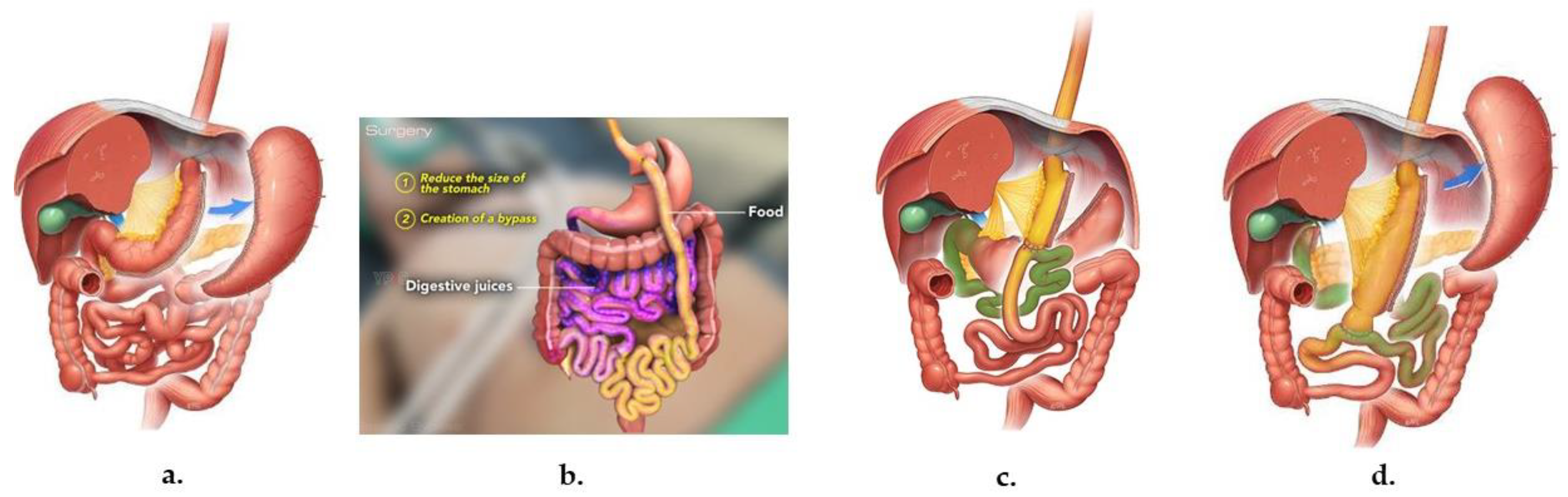
Figure 2.
Incretin-based agents that are commonly used in routine medical practice and are currently under clinical development [21].
Figure 2.
Incretin-based agents that are commonly used in routine medical practice and are currently under clinical development [21].
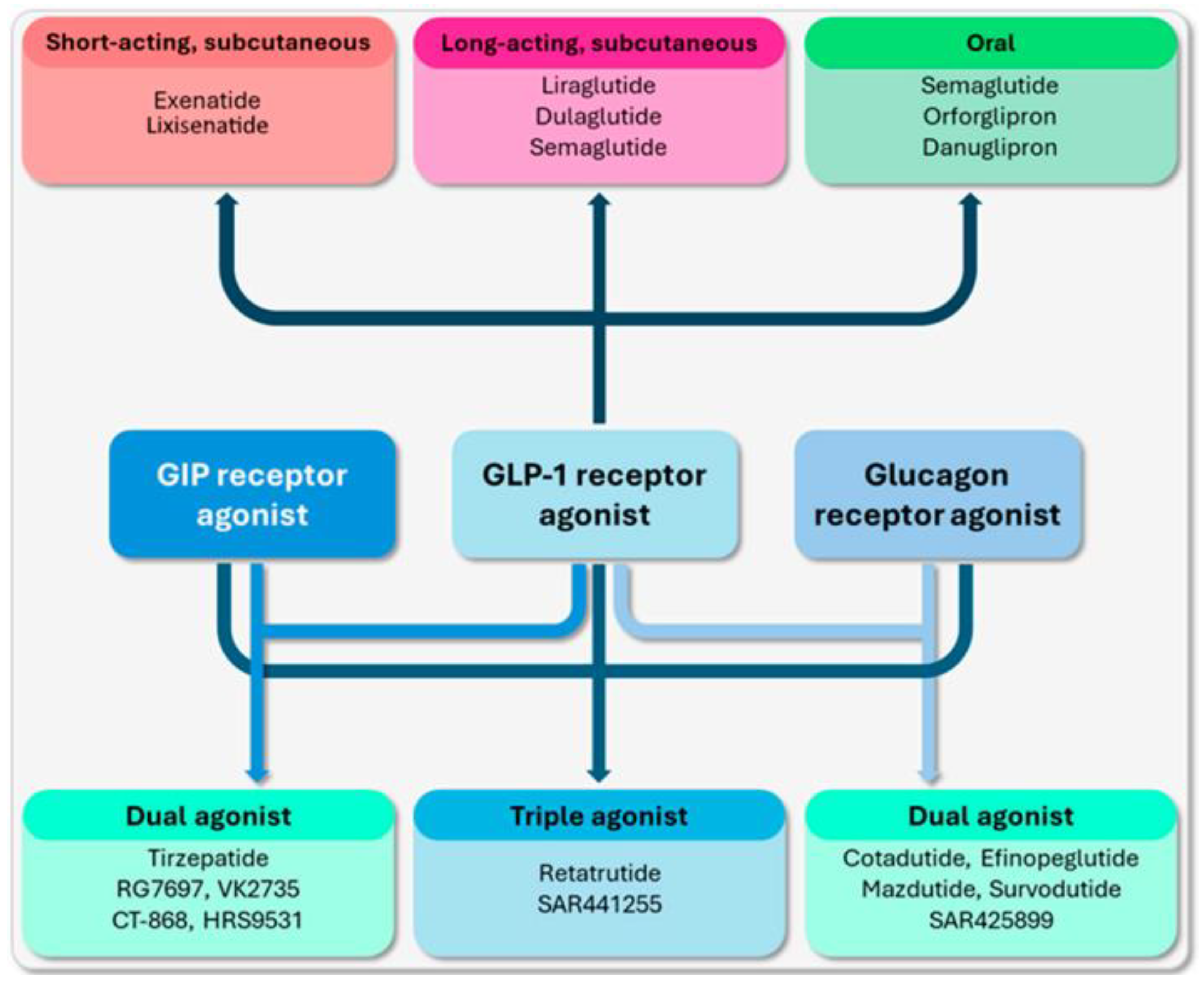

Table 1.
Mechanisms sustaining metabolic improvements after BMS.
| Weight loss-dependent | Weight loss-independent |
|---|---|
| ↑Skeletal muscle insulin sensitivity | ↑Hepatic insulin sensitivity |
| ↑Adipose insulin sensitivity | |
| ↑Postprandial gut peptides including GLP1 | |
| ↑Hepatic insulin sensitivity | ↑Bile acids |
| ↑Fibroblast Growth Factor 19 (FGF 19) | |
| ↑Whole-body insulin sensitivity | |
| ↑ Differentiation towards the enteroendocrine cell lineages (EEC) | |
| ↓Fasting insulin levels | |
| ↓Hepatic glucose production | |
| ↓ Hepatic triglycerides and fibrosis | ↓Hepatic triglycerides and fibrosis |
| Skeletal muscle changes for proteins involved with insulin signaling and ribosomal pathways | Intestinal cell proliferation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



