
Submitted:
11 July 2024
Posted:
12 July 2024
You are already at the latest version
Abstract
The integration of Artificial Intelligence (AI) in healthcare has transformed clinical practices by improving the accuracy of diagnosis, optimizing surgical procedures, improving the patient experience, and accelerating drug development. This article provides a comprehensive overview of the many applications of artificial intelligence (AI) across several industries, including fast diagnostics, where ML algorithms greatly enhance the accuracy and velocity of disease diagnosis. State-of-the-art robotic-assisted minimally invasive surgical procedures that shorten patients' hospitalization and improve their chances of recovery, cutting-edge AI applications in healthcare monitoring, and medication development. The article also looks at the primary challenges that AI in healthcare will inevitably encounter, such as differences in product quality, a shortage of skilled workers, privacy and ethical issues, and the need for improved regulatory frameworks. Despite the challenges, AI contributes significant advantages to the healthcare industry, providing novel and remarkable contributions to the efficiency of medical procedures and the progress of medical outcomes. The paper emphasizes the importance of cooperation in overcoming current challenges and enhancing the acceptability of AI technology in clinical settings. This will ensure that AI-driven innovations continue to enhance the standards of patient care.
Keywords:
Artificial Intelligence
; Healthcare Innovation
; Robotic Surgery
; Medical Diagnostics
; Personalized Medicine
1. Introduction
In recent years, advancements in technology have significantly transformed the field of informatics, particularly in the field of information processing, due to the introduction of cutting-edge technologies. Previously, the primary issue revolved around obtaining information. Ultimately, the scientific community is now benefiting from the advantages of the rapidly developing, readily accessible, and swiftly analyzed datasets that may also be conveniently stored in databases [1]. These technologies and developments have not only enhanced human abilities but also accelerated technological advances.[2]. The term “artificial intelligence” (AI), coined by John McCarthy in 1956, represents the initial concept of replicating human intellect in computers. The concept has revolutionized several domains, enabling significant technical breakthroughs and streamlining problem-solving processes [3,4]. Undoubtedly, AI will significantly impact the future, with the medical industry being at the forefront of experiencing its benefits. This kind of simulation of human intellect in machines is also called AI. This includes the techniques of machine learning (ML), deep learning (DL), and neural networks (NN).
The field of Healthcare AI has made significant advancements since its beginnings, with algorithms now achieving expert-level accuracy in detecting diseases from medical pictures. The rapid advancement of artificial intelligence (AI) will catalyze a revolution across several industries.
Artificial intelligence has the potential to completely transform the field of medical physics [5,6]. Therefore, it is essential for the community to strategize and address upcoming problems and possibilities to lead the way in the new era of the fourth industrial revolution. Despite these progressions, the incorporation of medical AI systems into routine clinical practice is still an important but mostly neglected topic. Furthermore, the medical artificial intelligence community faces the technological, ethical, and interpersonal issues that are difficult to resolve. In order to ensure the secure and effective use of these technologies, it is important to address the challenges they provide [5,6].
Although AI algorithms have proven effective in retrospective medical studies, their application in real-world medical practice has been limited [7,8]. Critics argue that, despite promising data, AI systems may exhibit inadequate speed or complexity for best use in real-world medical settings [8,9]. The challenges may arise from the interactions between people and AI systems [10]. Retrospective in silico datasets frequently undergo rigorous filtering and cleaning procedures, which may reduce their practical relevance in medical practice. AI has been extensively utilized in various areas of modern biology and biomedicine due to its rapid progress and development [11].
Its primary aim is to replicate human-like intelligence in computers, enabling the creation of self-aware intelligent systems. AI applications include vision, robotics, data analytics, problem solving, natural language processing, decision science, and linguistics [12,13,14]. AI’s profound impact on clinical medicine is also evident, enhancing medical practice significantly. AI systems are instrumental in early disease detection, enabling personalized medicine, and improving the efficiency of administrative procedures.
As AI technology progresses, its integration into clinical settings is poised to transform healthcare delivery, significantly improving patient outcomes. AI’s potential extends to revolutionizing diagnosis, treatment planning, drug discovery, personalized treatments, and data analysis. AI, with its advanced algorithms and machine learning abilities, can efficiently analyze vast amounts of medical data to extract important conclusions and offer precise projections. This assists healthcare professionals in making informed decisions, enhancing patient care, and optimizing the use of resources [14]. The evidence for these developments is supported by clinical data obtained from electronic health records (EHR), genomic data derived from whole genome sequencing (WGS) inquiries, and digital imaging data acquired from MRI, ultrasound, biomedical research, and digital pathology systems [14]. AI has an extensive application and receives investments from prominent institutions like as the Mayo Clinic and the Cleveland Clinic, as well as technology heavyweights like Philips, Siemens, and GE [15].
AI also plays a significant role in biotechnology firms like BERG and pharmaceutical companies like Takeda for biomarker discovery and drug development [15,16,17]. Companies such as Google and Apple are investing in AI-powered wearable technologies that monitor health and lifestyle [15]. Additionally, Facebook’s Preventive Health feature offers users access to health resources and recommendations for checkups [18]. These developments illustrate the expansion of American “Big Tech” or “GAFAM” corporations in the healthcare sector, with AI at the forefront of this transformation. Numerous studies have highlighted AI’s transformative impact on medicine and healthcare . This article discusses AI’s immense potential to revolutionize various sides of healthcare delivery, including diagnostics accuracy, Surgical precesion.Patient care , treatment planning, drug discovery, personalized care, and medical imaging
1.1. Enhancing Diagnostic Accuracy with AI:
Artificial Intelligence (AI) can analyze, induce, and organize medical data through electronic information technology, allowing doctors to diagnose diseases more accurately and provide treatment plans.[19] AI encompasses many fields, such as machine learning, evolutionary computing, natural language processing, etc. enabling feasible computations in multi-layer neural networks. Machine learning overcomes the limitations of traditional statistical methods, allowing for the integration and interpretation of complex data[20]. Doctors collect extensive medical data electronically, such as medical records and imaging scan results, and use machine learning algorithms to analyze and make judgments, discovering characteristics and patterns of diseases, thereby enhancing the precision and efficiency of disease diagnosis.[21] For instance, early cancer diagnosis systems, cardiovascular disease (CVD) risk prediction models. Additionally, Google’s DeepMind project has developed an automatic tissue layer segmentation model using AI deep learning, achieving significant results in diagnosing 50 common ophthalmic diseases including retinal disorders, with high accuracy. Intelligent pathology diagnosis utilizes deep learning technology to automatically analyze pathology images, enhancing the accuracy and efficiency of diagnoses. [22]. Applying AI to clinical workflows can also provide valuable insights for nursing decisions. With trained computational methods, clinical doctors can more scientifically and rapidly obtain valuable search results [23]. Thus, based on the patient’s condition and disease characteristics, combined with their professional knowledge and clinical experience, doctors can use intelligent medical systems to generate personalized treatment plans and continuously adjust and optimize them according to changes in the patient’s condition [19]. Some of recent enhancement is expalines in Figure 1.
1.2. AI-Enabled Medical Equipment Innovations:
Current technologies are primarily focused on the increasing integration of complex computer algorithms and equipment modalities. The updates to a new generation of medical examination equipment like X-ray Computer Tomography (CT) and Magnetic Resonance Imaging (MRI) have improved the segmentation, analysis, and diagnosis of medical images [24]. Technologies like deep learning aid clinicians in intelligently evaluating and identifying imaging data, enabling more accurate assessment of disease types and severity, as well as the selection of suitable treatment therapies. For example, the AIRad Companion Organs RT software is an AI-based application used for various clinical analyses [25].Compared to traditional equipment, AI-Rad solutions can generate clinically acceptable contours and save time, thus benefiting the radiotherapy process. Additionally, there are numerous chest X-ray AI tools available on the market for detecting conditions like pneumothorax and pleural effusion, which, as clinical trials have shown, are highly sensitive and assist doctors in their analyses [26,27].
Conventional blood glucose monitoring requires patients to puncture their fingers, a technique that does not offer immediate data. In recent times, there has been a significant increase in the adoption of wearable continuous glucose monitoring (CGM) biosensors [28]. These sensors test using patient’s sweat and saliva and synchronize the results with connected mobile devices via AI algorithms, digitizing diabetes monitoring [29]. Medical care systems based on Wireless Sensor Networks (WSN) used in medical institutions can closely monitor patients’ vital signs in real-time[30]. Sensors can be placed on or around the patient’s body to monitor blood sugar levels, pulse rates, breathing patterns, etc., allowing doctors and nursing staff to remotely monitor these metrics without disrupting the patient’s daily life. This helps in providing more timely treatment to patients and supports the establishment of IoT systems in healthcare institutions[31].
Medical imaging serves as an essential tool for diagnosing and treating various illnesses, including cancer, heart disease, and eye conditions. AI technology, by automatically detecting and interpreting images, enhances the precision and efficiency of medical imaging analysis [[32]. The use of deep learning algorithms, which involve neural networks processing extensive data, represents a notable AI advancement in medical imaging [33]. These algorithms are trained to identify patterns in medically-oriented images, aiding in disease or damage detection and prediction [34].
A significant milestone in AI for medical imaging is the development of deep learning algorithms for skin cancer identification. These algorithms match the accuracy of human dermatologists [35] and are also applied in diagnosing other cancers like breast and lung cancer by analyzing CT and MRI scans [36]. In addition, artificial intelligence (AI) helps in automatically identifying and highlighting regions of importance in photographs, hence decreasing the amount of time and effort needed for manual examination [36]. In eye care, AI algorithms have successfully detected conditions such as glaucoma and diabetic retinopathy with high precision [37].Some of the AI enhanced medical medical equipments are described in Figure 2.
Despite these advancements, AI in medical imaging faces challenges, including the need for high-quality data for training and validating algorithms and potential biases in these algorithms, requiring ongoing monitoring and revision [38] Issues such as inconsistent imaging protocols and the diversity of clinical scenarios add complexity, while privacy regulations and data sharing restrictions complicate AI development and application [38,39]
Predictive analytics in healthcare, powered by AI, improves patient outcomes by identifying those at risk of chronic diseases and tailoring interventions accordingly. This process involves analyzing data from EHRs and other sources using various statistical models and machine learning techniques[40,41]. AI’s ability to predict patient readmission rates and response to treatments helps optimize healthcare delivery[42]. However, the effectiveness of these tools is often limited by the diversity and size of training datasets, which affects their applicability across different patient demographics and disease types [43].
To address these challenges, enhancing data representation, increasing dataset diversity, and improving model interpretability are crucial. These steps aim to develop more accurate, reliable, and equitable predictive analytics tools in healthcare.
1.3. Al driven robotic Surgical Precision
Today, artificial intelligence medical robots have become instrumental in the field of medical services, assisting surgeons in performing various surgeries, primarily minimally invasive spine surgeries (MIS) [44] Robot-Assisted Surgical Systems (RASS) use highly precise instruments for minimally invasive operations, which can speed up recovery, thereby reducing hospital stays and lowering patient treatment costs[45]. For example, a study compared the results of robot-assisted rectal resection with traditional laparoscopic surgery, finding that robot-assisted surgery resulted in less blood loss, fewer surgical site infections, shorter hospital stays, and lower rates of reoperation [46]. During surgery, robots can monitor the patient’s condition and perform operations automatically according to the doctor’s commands. This reduces the risk of medical incidents and enhances the precision and stability of the surgery [47]. Surgical robot technology can reduce human error by using visual and motion sensing technology to sense and adjust the position and force of surgical instruments in real-time, which is essential for surgeries requiring high precision [48].some of the application of Al is illustrated in the Figure 3.
Surgical robot technology also enables remote surgeries. Through the internet and remote control technology, specialists can remotely operate surgical robots, monitor the surgical process in real-time, and provide guidance[49]. Remote surgical systems can reduce occupational hazards faced by surgeons, including radiation exposure and spinal injuries caused by prolonged use of lead aprons, or potential infectious diseases transmission (such as COVID-19)[50]. In one study on robot-assisted coronary intervention, radiation exposure was reduced by 95% compared to traditional surgical positions. Moreover, it can reduce physician fatigue, thereby minimizing errors during surgery. With further development and refinement of surgical robot systems, there is hope that patients in remote areas can receive timely surgical services in a shorter timeframe, potentially saving lives[51].

Table 1.
AI Enhanced Surgical Assesment.
| Sample | AI Tecniques | Stages | Phase of opration | Performance | References |
|---|---|---|---|---|---|
| 8 surgeons; 3 tasks (from 20 to 24 trials for each task); JIGSAWS (all 3 tasks) | CNN | Pre-operative | Knot tyationing, suturing, and needle passage on inanimate models | RMSE: 7.0 s for one task | [52] |
| JIGSAWS Data base for all 3 tasks(knot tying , suturing needle passage ) | 3D CNN + TSN | Pre-operative | Knot tying, suturing, and needle passage on inanimate models | Accuracy: 95.1%–100.0%; Sensitivity: 94.2%–100.0% | [53] |
| JIGSAWS all 3 tasks (knot tying , suturing needle passage ) | CNN | Pre-operative | Knot tying, suturing, and needle passage on inanimate models | Accuracy: 91.3%–95.4% | [54] |
| JIGSAWS Data base forall 3 tasks (knot tying , suturing needle passage ) | PCA, kNN, SVR | Pre-operative | Knot tying, suturing, and needle passage on inanimate models | Accuracy: 77.4%–100.0% | [55] |
| JIGSAWS Data base for 2 tasks(Knoting , suituning) | kNN, LR, SVM | Pre-operative | Knot tying, suturing, and needle passage on inanimate models | Accuracy: 77.9%–82.3% (knot tying); 79.8%–89.9% (suturing) | [56] |
| JIGSAWS Dtabase all 3 tasks (knot tying , suturing needle passage | FCN | Pre-operative | Knot tying, suturing, and needle passage on inanimate models | Accuracy: 92.1%–100.0% | [57] |
| JIGSAWS (all 3 tasks); 9 surgeons; 5 tasks | Clustering and PCA; Temporal clustering: HACA, ACA, SC, GMM | Pre-operative; Post-operative | Knot tying, suturing, and needle passage on inanimate models; Various surgical tasks on porcine model | Sensitivity: 71.2%–83.3%; Precision 72.6%–81.2%; Accuracy: 50.6%–88.0% (HACA) | [58],[59] |
| 3 tasks; 10 trials for circle cutting, 28 trials for needle passage, and 39 trials for suturing | GMM | Pre-operative | Circle cutting, needle passage, and suturing on inanimate model | Comparison of transition accuracy with JIGSAWS: 73.0%–83.0% | [60] |
| 2 urologists and 1 engineer; 2 tasks; Trajectories for drawing and peg transfer | kNN, SVM | Pre-operative | Drawing of ‘R’ letter and peg transfer on inanimate model | Accuracy for gesture classification: 97.4% (kNN), 96.2% (SVM) | [61] |
| 20,000 COCO images, endoscopic images and videos from MICCAI EndoVis 2017 | U-Net and conditional GAN | Post-operative | Tools segmentation in nephrectomies and laparoscopic surgeries | DSC: 65.0%–68.0% | [62] |
| 225 frame sequences from 8 surgeries of MICCAI EndoVis 2017 | GAN | Post-operative | Tools segmentation in operations on porcine model | DSC: 91.6% (binary segmentation); 73.8% (parts segmentation) | [63] |
| Atlas (86 videos by 10 surgeons); MICCAI EndoVis 2015 videos | CNN | Post-operative | Tool detection in surgical training and procedures | mAP: 98.5% (Atlas Dione), 100.0% (EndoVis) | [64] |
| 24 procedures | CNN | Post-operative | Surgical procedure recognition | Recognition metrics not detailed | [65] |
1.4. Elevating Patient Care with AI Technologies
In recent years, artificial intelligence has been applied in multiple medical fields, and AI technology can also enhance patients’ medical experiences[66]. By analyzing patients’ genomic data and other biomarkers, AI can tailor personalized treatment plans, offering more precise treatment guidance. This not only improves treatment outcomes and patients’ quality of life but also saves on treatment time and costs[67]. Studies show that up to 65% of patients are dissatisfied with the waiting times at clinics, and difficulty in accessing healthcare has always been a problem for the public[68]. The application of intelligent medical appointment and payment systems allows patients to more conveniently seek medical advice, make appointments, undergo treatment, make payments, pick up medications, and check medical records, thus improving the efficiency of hospital management and providing more convenient services for patients[69].
Additionally, AI can also optimize the allocation and utilization of medical resources. In situations where medical resources are scarce, AI can help healthcare institutions optimize queuing, ward allocation, and other processes to enhance resource utilization efficiency[70]. With AI-driven remote monitoring systems, patients can track and monitor their vital signs and alert healthcare providers to any potential issues. This can lead to earlier detection and improvement of treatment outcomes, and reduce the need for in-person visits to medical facilities. Furthermore, it allows for effective medical services to be provided to patients far from hospitals through technologies like remote monitoring and telecare[71]. Virtual consultations offered by remote medical systems mean that patients do not need to visit medical facilities to receive treatment, which is particularly beneficial for those living in remote areas or with mobility issues[72]. Healthcare workers can also track the health status and lifestyle habits of discharged patients through intelligent health management systems, analyze patients’ health risks, and provide targeted advice, thereby improving the doctor-patient relationship.[73]
In the field of drug development, artificial intelligence can assist scientists in analyzing chemical data and accelerating the process of developing new drugs. Deep learning technology, as a data mining method, has shown tremendous prospects in the field of drug design.[74] AI learning methods ensure a systematic assessment of physicochemical properties, toxicity, side effects, biological activity, and pharmacokinetics at a conjectural level. Additionally, multi-target refined computational methods can be used to reduce the failure rate of preclinical lead molecules by decreasing the number of synthetic compounds tested in in vitro or in vivo systems, thus reducing loss rates and research and development expenditures[75]. A critical part of the drug development process is the synthesis of selected molecules; AI technology can optimize the sorting of molecules, thereby selecting the most effective synthesis pathways.[76] Moreover, machine learning techniques and predictive modeling software also help identify target-specific virtual molecules, as well as the associations between molecules and their targets, while optimizing safety and efficacy attributes[77].
Based on patients’ genomic and clinical data, artificial intelligence can provide personalized medication selections and dosages. By analyzing patients’ genotypes, medical histories, and other relevant information, machine learning algorithms can predict the efficacy and side effects of specific drugs, helping doctors devise the most suitable treatment plans for patients[78]. Major pharmaceutical corporations such as Bayer, Roche, and Pfizer have initiated partnerships with information technology companies. Insilico Medicine has utilized artificial intelligence to develop a pharmaceutical therapy to treat idiopathic pulmonary fibrosis [79]. Recently, AI has played a significant role in the development of new anti-cancer therapies. For instance, a group of novel medications has been successfully developed using AI techniques. These drugs have demonstrated the ability to effectively inhibit the growth of tumor cells, relax the pain of patients, and prolong their life expectancy [80].
AI robots are revolutionizing healthcare by automating repetitive tasks and delivering personalized treatments, thereby enhancing patient outcomes and reducing costs. These robots vary widely, from exoskeletons to mobile and humanoid forms. In rehabilitation, AI robots are pivotal, assisting patients with physical therapy exercises tailored to improve their functional and motor skills [81,82] Furthermore, AI robots are used for physically demanding or precision tasks such as tele-surgery, where surgeons operate remotely using robotic arms, achieving greater precision and flexibility than traditional methods. This technology proves particularly beneficial for complex or otherwise impossible surgeries using conventional techniques.
In geriatric care, AI robots support the elderly with daily activities like dressing and bathing and provide companionship [83]. Although their adoption in eldercare is limited due to high costs, such robots are more prevalent in countries like Japan, which has a significant aging population [84]. AI robots are also useful in hazardous environments, such as contaminated areas or emergency situations, where they can navigate dangers, assess conditions, and relay real-time information to response teams [85].
Despite the potential for increased efficiency and reduced medical errors, the cost of implementing and maintaining robotic technologies remains a major barrier, particularly in developing countries like India [86]. A Canadian study on the financial impact of robotic urology highlighted substantial costs, with the initial setup for robot-assisted prostatectomy exceeding $2 million USD, and total expenses over seven years reaching $3.5 million CAD for prostatectomy alone. This includes costs for operation, maintenance, and training, with each robotic procedure costing considerably more than traditional surgeries [87,88]. However, the long-term benefits could offset these costs through increased procedural volume [88], and short-term gains have been noted in reduced hospital stays, less blood loss, and improved surgical margins, enhancing postoperative outcomes like continence and sexual function [88,89].
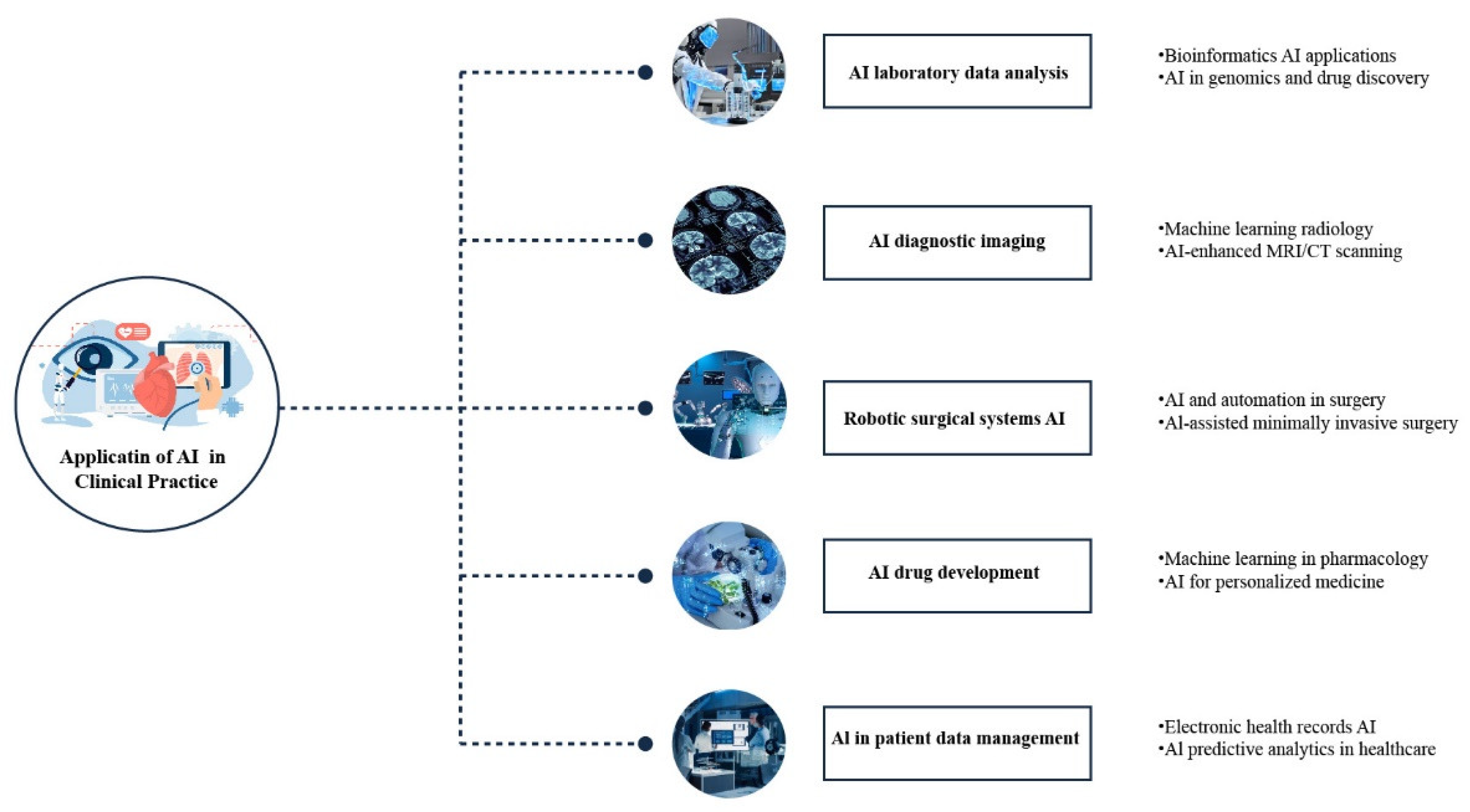
Artificial intelligence (AI) is poised to revolutionize the process of drug development by significantly decreasing the time and expenses involved in bringing novel medications to the market.AI algorithms analyze diverse data sources, including scientific publications, clinical trials, and chemical databases, to identify potential drug targets and assess the efficacy and safety of new compounds [90]. In virtual screening, AI examines vast compound databases to find candidates likely to bind to specific protein targets [91]. AI further aids in analyzing genetic data to pinpoint new therapeutic targets for personalized treatments, such as in cancer [92]. Additionally, by reviewing clinical trial data and electronic health records, AI helps predict potential drug side effects, enhancing safety and reducing adverse events in new drugs [93].The different application of AI has shown in Figure 4.
2. Strategies for Effective AI Adoption
2.1. Standardizing AI Technologies for Better Medical Outcomes
The widespread development and entry of artificial intelligence hardware and software into the medical market have brought about quality issues[94]. AI in the medical field requires a large amount of data, but many data sources are unreliable and vary greatly in quality, negatively impacting the accuracy of diagnoses and treatments, leading to inaccurate results[95]. The inconsistency in product standardization and quality also affects the accuracy of AI systems. AI devices are not all-powerful; for example, robots using precise surgical instruments make operations more precise but cannot perform surgeries involving sensitive nerves[96]. Moreover, their costs are significantly higher than traditional surgeries, and they may also have unknown safety issues. To address the problem that surgical robots cannot handle all types of surgeries, researchers have developed robots for specific surgical operations, but these still present issues of high costs [97].
2.2. Addressing the Skills Shortage in AI Development
Currently, there is a shortage of talent in the research and application of artificial intelligence technology [98]. AI requires human operation and implementation, and due to issues with the education system, clinical professionals lack engineering knowledge, and those involved in device development are not familiar with clinical medicine, which is a bottleneck issue [99]. Healthcare workers’ acceptance of AI-assisted medicine still needs improvement[66]. However, so far, AI has not eliminated any jobs in the healthcare field, but full integration of AI into clinical work and electronic medical record systems remains challenging [100]. We should accelerate the training of medical staff in AI medical knowledge to quickly master advanced science and technology. Schools should also reform their educational models to speed up the training of interdisciplinary talent combining medicine and engineering [101]. Additionally, it is important to enhance public awareness of scientific knowledge so that everyone can consciously accept the benefits brought by AI [102].
2.3. Navigating Ethical and Privacy Challenges in AI Applications
Literature reports on the risks of artificial intelligence in terms of privacy and ethics, mainly focusing on the following aspects: patient agency and oversight, technological robustness and safety, privacy of patient identity and confidentiality of medical data, transparency and diversity in diagnosis and treatment, non-discrimination and fairness, accountability for medical harm, etc [103]. With AI-assisted diagnostics and treatment, patients have the right to know about the system’s limitations, the rationality of decisions, and other related issues [104]. However, in reality, patients are unable to communicate effectively in medical settings, severely challenging their medical autonomy, leaving them no choice but to passively accept the involvement of AI [105]. It is believed that smart medicine, based on AI technology, complicates the protection of information security and individual privacy, and shows indifference to medical humanitarian care, thus becoming a complex of risks[106]. It is proposed to cultivate humanitarian care in AI and to use ethical review to help improve the governance system of technology[107]. Ethical issues in the medical application of AI are increasingly gaining attention, and while problems are inevitable, we need to explore solutions. Before using AI, any potential theoretical problems should be adequately addressed and resolved to eliminate negative impacts and resolve ethical risks. This is the responsibility and duty that ethicists should undertake[108].
2.4. AI Regulatory Challenges
The absence of relevant laws and regulations and the inadequacy of policy management are also key factors restraining the application of artificial intelligence technology in the healthcare industry[109]. Currently, there is a lack of laws and regulations that align with practical circumstances and policy management measures to ensure the legal, standardized, and safe application of technology in the healthcare sector[110]. Moreover, in the actual operations of hospitals at various levels, there is also a lack of corresponding regulations and operational procedures to ensure the practical effectiveness and social benefits of the technology[111].
Fortunately, many countries around the world have enacted numerous laws and regulations regarding the application of artificial intelligence in healthcare, gradually establishing a comprehensive legal system for medical intelligence [112]. Furthermore, artificial intelligence (AI) assists in automatically identifying and highlighting regions of significance within photographs, hence decreasing the amount of time and effort needed for manual examination [113].
The EU AI Act, approved in 2023, is the first and entire legal framework designed to govern AI technology [114]. It categorizes systems based on their risk level and imposes necessary standards for high-risk AI in areas such as data and documentation, transparency, human oversight, accuracy, and cybersecurity. As stated in the legislation, national authorities will track compliance. The US AI Bill of Rights, introduced in 2023, presents an optional framework of principles aimed at directing the development and utilization of AI. It primarily emphasizes the importance of addressing algorithmic discrimination, safeguarding data privacy, providing transparency and explanations for AI systems, and ensuring human alternatives and supervision [115].
Prevously, several countries also makind policies for promoting and regulating the development of Health Medical Big Data Application [116] for a New Generation of Artificial Intelligence which outlined the development directions and regulatory policies for smart hospital construction, surgical robots, intelligent diagnostics, intelligent physiological monitoring, image recognition, new drug development, pharmaceutical regulation, and intelligent epidemic monitoring and prevention [117]. These policies have promoted the healthy development of the medical AI technology industry and will effectively improve the efficiency of medical resource allocation and the quality of medical services [118].
3. Conclusion:
The research on AI in the field of health industry has led to a new era of medical innovation, which is characterized by notable progress and challenges. The given review has proven how artificial intelligence is changing healthcare services by enhancing the diagnosis, the surgeon’s accuracy, the patient’s experience, and the new medication development speed. Through the swiftness of AI’s diagnosis, healthcare may not only be more efficient but also more accurate, thus, playing a great role in the early detection and better medical care. Besides, the artificial intelligence has turned into a necessary part of surgery, by giving precision, which leads to the elimination of human error, thus, patients can recover faster. On the contrary, the incorporation of AI into the healthcare too has some difficulties. The main difficulties are the quality of the AI products, the shortage of qualified persons with the training in both AI and clinical applications, and the ethical and privacy issues. Besides, the current legal structure cannot keep up with the fast pace of the technical progress, thus, the process of the widespread adoption is limited.
We are on the edge of a medical revolution, hence we should adopt a contemporary perspective that directly addresses these matters. This involves improving educational programmes to help students understand the relationship between engineering and clinical practice, establishing stringent regulations for AI systems to ensure compliance with laws in the field, and creating a regulatory framework that safeguards patients while also fostering innovation and success. Despite its limitations, the implementation of artificial intelligence (AI) in healthcare will play a crucial role in advancing patient outcomes and operational efficiency. In order for AI to become a complementary tool for human knowledge in the pursuit of achieving high-quality care, it is imperative that stakeholders from various domains, including physicians, technologists, politicians, and ethicists, collaborate to address the challenges that will arise during the advancement of AI in this field.
References
- Athanasopoulou, K.; Daneva, G.N.; Adamopoulos, P.G.; Scorilas, A. Artificial Intelligence: The Milestone in Modern Biomedical Research. BioMedInformatics 2022, 2, 727–744. [Google Scholar] [CrossRef]
- Rong, G.; Mendez, A.; Assi, E.B.; Zhao, B.; Sawan, M. Artificial Intelligence in Healthcare: Review and Prediction Case Studies. Engineering 2020, 6, 291–301. [Google Scholar] [CrossRef]
- Keskinbora, K.H. Medical ethics considerations on artificial intelligence. J. Clin. Neurosci. 2019, 64, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Solomonoff, R. The time scale of artificial intelligence: Reflections on social effects. Hum. Syst. Manag. 1985, 5, 149–153. [Google Scholar] [CrossRef]
- Xing, L.; Krupinski, E.A.; Cai, J. Artificial intelligence will soon change the landscape of medical physics research and practice. Med Phys. 2018, 45, 1791–1793. [Google Scholar] [CrossRef] [PubMed]
- Rajpurkar, P.; Chen, E.; Banerjee, O.; Topol, E.J. AI in health and medicine. Nat. Med. 2022, 28, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Wiens, J.; Saria, S.; Sendak, M.; Ghassemi, M.; Liu, V.X.; Doshi-Velez, F.; Jung, K.; Heller, K.; Kale, D.; Saeed, M.; et al. Do no harm: a roadmap for responsible machine learning for health care. Nat. Med. 2019, 25, 1337–1340. [Google Scholar] [CrossRef] [PubMed]
- Kanagasingam, Y.; Xiao, D.; Vignarajan, J.; Preetham, A.; Tay-Kearney, M.-L.; Mehrotra, A. Evaluation of Artificial Intelligence–Based Grading of Diabetic Retinopathy in Primary Care. JAMA Netw. Open 2018, 1, e182665–e182665. [Google Scholar] [CrossRef] [PubMed]
- Beede, E.; Baylor, E.; Hersch, F.; Iurchenko, A.; Wilcox, L.; Ruamviboonsuk, P.; Vardoulakis, L.M. “A human-centered evaluation of a deep learning system deployed in clinics for the detection of diabetic retinopathy,” in Proceedings of the 2020 CHI conference on human factors in computing systems, 2020, pp. 1-12.
- Kiani, A.; Uyumazturk, B.; Rajpurkar, P.; Wang, A.; Gao, R.; Jones, E.; Yu, Y.; Langlotz, C.P.; Ball, R.L.; Montine, T.J.; et al. Impact of a deep learning assistant on the histopathologic classification of liver cancer. npj Digit. Med. 2020, 3, 23. [Google Scholar] [CrossRef]
- Leite, M.L.; Costa, L.S.d.L.; Cunha, V.A.; Kreniski, V.; Filho, M.d.O.B.; da Cunha, N.B.; Costa, F.F. Artificial intelligence and the future of life sciences. Drug Discov. Today 2021, 26, 2515–2526. [Google Scholar] [CrossRef]
- P. Hamet and J. Tremblay, “Artificial intelligence in medicine,” Metabolism, vol. 69, pp. S36-S40, 2017.
- Bhardwaj, A.; Kishore, S.; Pandey, D.K. Artificial Intelligence in Biological Sciences. Life 2022, 12, 1430. [Google Scholar] [CrossRef] [PubMed]
- Hulsen, T.; Jamuar, S.S.; Moody, A.R.; Karnes, J.H.; Varga, O.; Hedensted, S.; Spreafico, R.; Hafler, D.A.; McKinney, E.F. From Big Data to Precision Medicine. Front. Med. 2019, 6, 34. [Google Scholar] [CrossRef] [PubMed]
- T. Hulsen, “Literature analysis of artificial intelligence in biomedicine,” Annals of translational medicine, vol. 10, no. 23, 2022.
- Tolstikov, V.; Moser, A.J.; Sarangarajan, R.; Narain, N.R.; Kiebish, M.A. Current Status of Metabolomic Biomarker Discovery: Impact of Study Design and Demographic Characteristics. Metabolites 2020, 10, 224. [Google Scholar] [CrossRef] [PubMed]
- Savage, N. The race to the top among the world’s leaders in artificial intelligence. Nature 2020, 588, S102–S104. [Google Scholar] [CrossRef]
- Kaul, V.; Enslin, S.; Gross, S.A. History of artificial intelligence in medicine. Gastrointest. Endosc. 2020, 92, 807–812. [Google Scholar] [CrossRef] [PubMed]
- Haick, H.; Tang, N. Artificial Intelligence in Medical Sensors for Clinical Decisions. ACS Nano 2021, 15, 3557–3567. [Google Scholar] [CrossRef] [PubMed]
- Y. R. Shrestha, V. Y. R. Shrestha, V. Krishna, and G. von Krogh, “Augmenting organizational decision-making with deep learning algorithms: Principles, promises, and challenges,” Journal of Business Research, vol. 123, pp. 588-603, 2021.
- Willemink, M.J.; Koszek, W.A.; Hardell, C.; Wu, J.; Fleischmann, D.; Harvey, H.; Folio, L.R.; Summers, R.M.; Rubin, D.L.; Lungren, M.P. Preparing Medical Imaging Data for Machine Learning. Radiology 2020, 295, 4–15. [Google Scholar] [CrossRef] [PubMed]
- Topol, E.J. High-performance medicine: the convergence of human and artificial intelligence. Nat. Med. 2019, 25, 44–56. [Google Scholar] [CrossRef] [PubMed]
- Sandhu, S.; Lin, A.L.; Brajer, N.; Sperling, J.; Ratliff, W.; Bedoya, A.D.; Balu, S.; O'Brien, C.; Sendak, M.P. Integrating a Machine Learning System Into Clinical Workflows: Qualitative Study. J. Med Internet Res. 2020, 22, e22421. [Google Scholar] [CrossRef]
- Almeida, G.; Tavares, J.M.R.S. Versatile Convolutional Networks Applied to Computed Tomography and Magnetic Resonance Image Segmentation. J. Med Syst. 2021, 45, 1–10. [Google Scholar] [CrossRef]
- Abnet, C.C.; Arnold, M.; Wei, W.-Q. Epidemiology of Esophageal Squamous Cell Carcinoma. Gastroenterology 2018, 154, 360–373. [Google Scholar] [CrossRef]
- Hu, Y.; Nguyen, H.; Smith, C.; Chen, T.; Byrne, M.; Archibald-Heeren, B.; Rijken, J.; Aland, T. Clinical assessment of a novel machine-learning automated contouring tool for radiotherapy planning. J. Appl. Clin. Med Phys. 2023, 24, e13949. [Google Scholar] [CrossRef]
- Zeadally, S.; Bello, O. Harnessing the power of Internet of Things based connectivity to improve healthcare. Internet Things 2019, 14, 100074. [Google Scholar] [CrossRef]
- Lado-Baleato, M. Matabuena, C. Díaz-Louzao, and F. A: Gude, “Optimal Cut-Point Estimation for functional digital biomarkers: Application to Continuous Glucose Monitoring; arXiv:2404.09716, 2024.
- Mansour, M.; Darweesh, M.S.; Soltan, A. Wearable devices for glucose monitoring: A review of state-of-the-art technologies and emerging trends. Alex. Eng. J. 2024, 89, 224–243. [Google Scholar] [CrossRef]
- Huang, X.; Yao, C.; Huang, S.; Zheng, S.; Liu, Z.; Liu, J.; Wang, J.; Chen, H.-J.; Xie, X. Technological Advances of Wearable Device for Continuous Monitoring of In Vivo Glucose. ACS Sensors 2024, 9, 1065–1088. [Google Scholar] [CrossRef] [PubMed]
- S. F. Ahmed, M. S. B. S. F. Ahmed, M. S. B. Alam, S. Afrin, S. J. Rafa, N. Rafa, and A. H. Gandomi, “Insights into Internet of Medical Things (IoMT): Data fusion, security issues and potential solutions,” Information Fusion, vol. 102, p. 102060, 2024.
- Tang, X. The role of artificial intelligence in medical imaging research. BJR|Open 2020, 2, 20190031. [Google Scholar] [CrossRef] [PubMed]
- Manco, L.; Maffei, N.; Strolin, S.; Vichi, S.; Bottazzi, L.; Strigari, L. Basic of machine learning and deep learning in imaging for medical physicists. Phys. Medica 2021, 83, 194–205. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Padhy, S.K.; Takkar, B.; Chawla, R. Artificial intelligence in diabetic retinopathy: A natural step to the future. Indian J. Ophthalmol. 2019, 67, 1004. [Google Scholar] [CrossRef]
- Papachristou, I.; Bosanquet, N. Improving the prevention and diagnosis of melanoma on a national scale: A comparative study of performance in the United Kingdom and Australia. J. Public Heal. Policy 2019, 41, 28–38. [Google Scholar] [CrossRef]
- Espinoza, J.L.; Dong, L.T. Artificial Intelligence Tools for Refining Lung Cancer Screening. J. Clin. Med. 2020, 9, 3860. [Google Scholar] [CrossRef]
- Huang, X.; Wang, H.; She, C.; Feng, J.; Liu, X.; Hu, X.; Chen, L.; Tao, Y. Artificial intelligence promotes the diagnosis and screening of diabetic retinopathy. Front. Endocrinol. 2022, 13, 946915. [Google Scholar] [CrossRef] [PubMed]
- Prakash, S.; Balaji, J.N.; Joshi, A.; Surapaneni, K.M. Ethical Conundrums in the Application of Artificial Intelligence (AI) in Healthcare—A Scoping Review of Reviews. J. Pers. Med. 2022, 12, 1914. [Google Scholar] [CrossRef] [PubMed]
- Nia, N.G.; Kaplanoglu, E.; Nasab, A. Evaluation of artificial intelligence techniques in disease diagnosis and prediction. Discov. Artif. Intell. 2023, 3, 1–14. [Google Scholar] [CrossRef]
- Wong, J.; Horwitz, M.M.; Zhou, L.; Toh, S. Using Machine Learning to Identify Health Outcomes from Electronic Health Record Data. Curr. Epidemiology Rep. 2018, 5, 331–342. [Google Scholar] [CrossRef] [PubMed]
- S. Dash, S. K. S. Dash, S. K. Shakyawar, M. Sharma, and S. Kaushik, “Big data in healthcare: management, analysis and future prospects,” Journal of big data, vol. 6, no. 1, pp. 1-25, 2019.
- Ozonoff, A.; E Milliren, C.; Fournier, K.; Welcher, J.; Landschaft, A.; Samnaliev, M.; Saluvan, M.; Waltzman, M.; A Kimia, A. Electronic surveillance of patient safety events using natural language processing. Heal. Informatics J. 2022, 28. [Google Scholar] [CrossRef]
- Van Calster, B.; Wynants, L.; Timmerman, D.; Steyerberg, E.W.; Collins, G.S. Predictive analytics in health care: how can we know it works? J. Am. Med Informatics Assoc. 2019, 26, 1651–1654. [Google Scholar] [CrossRef] [PubMed]
- Haidegger, T.; Speidel, S.; Stoyanov, D.; Satava, R.M. Robot-Assisted Minimally Invasive Surgery—Surgical Robotics in the Data Age. Proc. IEEE 2022, 110, 835–846. [Google Scholar] [CrossRef]
- J. S. Lee et al., “Robotic-Assisted Spine Surgery: Role in Training the Next Generation of Spine Surgeons,” Neurospine, vol. 21, no. 1, p. 116, 2024.
- Chen, Z.-L.; Du, Q.-L.; Zhu, Y.-B.; Wang, H.-F. A systematic review and meta-analysis of short-term outcomes comparing the efficacy of robotic versus laparoscopic colorectal surgery in obese patients. J. Robot. Surg. 2024, 18, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Ou, H.-C.; Marian, L.; Li, C.-C.; Juan, Y.-S.; Tung, M.-C.; Shih, H.-J.; Chang, C.-P.; Chen, J.-T.; Yang, C.-H.; Ou, Y.-C. Robot-Assisted Radical Prostatectomy by the Hugo Robotic-Assisted Surgery (RAS) System and the da Vinci System: A Comparison between the Two Platforms. Cancers 2024, 16, 1207. [Google Scholar] [CrossRef] [PubMed]
- Z. Li et al., “Design and application of multi-dimensional force/torque sensors in surgical robots: A review,” IEEE Sensors Journal, 2023.
- Hou, C.; Wang, K.; Wang, F.; Li, H.; Lou, L.; Zhang, S.; Gu, Y.; Liu, H.; Chen, T.; Sun, L. A Highly Integrated 3D MEMS Force Sensing Module With Variable Sensitivity for Robotic-Assisted Minimally Invasive Surgery. Adv. Funct. Mater. 2023, 33. [Google Scholar] [CrossRef]
- Saber, H.; Beaman, C.; Morales, J.; Kimball, D.; Kaneko, N.; Tateshima, S. Full robotic endovascular treatment for various head and neck hemorrhagic lesions. Interv. Neuroradiol. 2023. [Google Scholar] [CrossRef]
- Sachan, S.; Swarnkar, P. Intelligent Fractional Order Sliding Mode Based Control for Surgical Robot Manipulator. Electronics 2023, 12, 729. [Google Scholar] [CrossRef]
- Zhang, D.; Wu, Z.; Chen, J.; Gao, A.; Chen, X.; Li, P.; Wang, Z.; Yang, G.; Lo, B.P.L.; Yang, G.-Z. Automatic Microsurgical Skill Assessment Based on Cross-Domain Transfer Learning. IEEE Robot. Autom. Lett. 2020, 5, 4148–4155. [Google Scholar] [CrossRef]
- Funke, I.; Mees, S.T.; Weitz, J.; Speidel, S. Video-based surgical skill assessment using 3D convolutional neural networks. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 1217–1225. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Fey, A.M. Deep learning with convolutional neural network for objective skill evaluation in robot-assisted surgery. Int. J. Comput. Assist. Radiol. Surg. 2018, 13, 1959–1970. [Google Scholar] [CrossRef] [PubMed]
- Zia and, I. Essa, “Automated surgical skill assessment in RMIS training,” International journal of computer assisted radiology and surgery, vol. 13, pp. 731-739, 2018.
- Fard, M.J.; Ameri, S.; Ellis, R.D.; Chinnam, R.B.; Pandya, A.K.; Klein, M.D. Automated robot-assisted surgical skill evaluation: Predictive analytics approach. Int. J. Med Robot. Comput. Assist. Surg. 2017, 14. [Google Scholar] [CrossRef] [PubMed]
- Fawaz, H.I.; Forestier, G.; Weber, J.; Idoumghar, L.; Muller, P.-A. Accurate and interpretable evaluation of surgical skills from kinematic data using fully convolutional neural networks. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 1611–1617. [Google Scholar] [CrossRef] [PubMed]
- Fard, M.J.; Ameri, S.; Chinnam, R.B.; Ellis, R.D. Soft Boundary Approach for Unsupervised Gesture Segmentation in Robotic-Assisted Surgery. IEEE Robot. Autom. Lett. 2016, 2, 171–178. [Google Scholar] [CrossRef]
- Zia, A.; Zhang, C.; Xiong, X.; Jarc, A.M. Temporal clustering of surgical activities in robot-assisted surgery. Int. J. Comput. Assist. Radiol. Surg. 2017, 12, 1171–1178. [Google Scholar] [CrossRef]
- S. Krishnan et al., “Transition state clustering: Unsupervised surgical trajectory segmentation for robot learning,” The International journal of robotics research, vol. 36, no. 13-14, pp. 1595-1618, 2017.
- Despinoy, F.; Bouget, D.; Forestier, G.; Penet, C.; Zemiti, N.; Poignet, P.; Jannin, P. Unsupervised Trajectory Segmentation for Surgical Gesture Recognition in Robotic Training. IEEE Trans. Biomed. Eng. 2015, 63, 1280–1291. [Google Scholar] [CrossRef]
- Ross, T.; Zimmerer, D.; Vemuri, A.; Isensee, F.; Wiesenfarth, M.; Bodenstedt, S.; Both, F.; Kessler, P.; Wagner, M.; Müller, B.; et al. Exploiting the potential of unlabeled endoscopic video data with self-supervised learning. Int. J. Comput. Assist. Radiol. Surg. 2018, 13, 925–933. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.; Atputharuban, D.A.; Ramesh, R.; Ren, H. Real-Time Instrument Segmentation in Robotic Surgery Using Auxiliary Supervised Deep Adversarial Learning. IEEE Robot. Autom. Lett. 2019, 4, 2188–2195. [Google Scholar] [CrossRef]
- Malpani, A.; Lea, C.; Chen, C.C.G.; Hager, G.D. System events: readily accessible features for surgical phase detection. Int. J. Comput. Assist. Radiol. Surg. 2016, 11, 1201–1209. [Google Scholar] [CrossRef] [PubMed]
- Zhao, B.; Waterman, R.S.; Urman, R.D.; Gabriel, R.A. A Machine Learning Approach to Predicting Case Duration for Robot-Assisted Surgery. J. Med Syst. 2019, 43, 32. [Google Scholar] [CrossRef] [PubMed]
- H. A. Younis et al., “A Systematic Review and Meta-Analysis of Artificial Intelligence Tools in Medicine and Healthcare: Applications, Considerations, Limitations, Motivation and Challenges,” Diagnostics, vol. 14, no. 1, p. 109, 2024.
- Bertolaccini, L.; Casiraghi, M.; Uslenghi, C.; Maiorca, S.; Spaggiari, L. Recent advances in lung cancer research: unravelling the future of treatment. Updat. Surg. 2024, 1–12. [Google Scholar] [CrossRef]
- Nor, M.Z.M.; Said, A.H.; Man, M.C.; Yusof, M.Z. Patient's satisfaction towards healthcare services and its associated factors at the highest patient loads government primary care clinic in Pahang. . 2024, 79, 34–41. [Google Scholar]
- Breen, J.; Allen, K.; Zucker, K.; Adusumilli, P.; Scarsbrook, A.; Hall, G.; Orsi, N.M.; Ravikumar, N. Artificial intelligence in ovarian cancer histopathology: a systematic review. npj Precis. Oncol. 2023, 7, 1–14. [Google Scholar] [CrossRef]
- Wahl, B.; Cossy-Gantner, A.; Germann, S.; Schwalbe, N.R. Artificial intelligence (AI) and global health: how can AI contribute to health in resource-poor settings? BMJ Glob. Heal. 2018, 3, e000798. [Google Scholar] [CrossRef]
- Noah, B.; Keller, M.S.; Mosadeghi, S.; Stein, L.; Johl, S.; Delshad, S.; Tashjian, V.C.; Lew, D.; Kwan, J.T.; Jusufagic, A.; et al. Impact of remote patient monitoring on clinical outcomes: an updated meta-analysis of randomized controlled trials. npj Digit. Med. 2018, 1, 20172. [Google Scholar] [CrossRef]
- Caffery, L.A.; Muurlink, O.T.; Taylor-Robinson, A.W. Survival of rural telehealth services post-pandemic in Australia: A call to retain the gains in the ‘new normal’. Aust. J. Rural. Heal. 2022, 30, 544–549. [Google Scholar] [CrossRef]
- Zhou, R.; Zhang, X.; Wang, X.; Yang, G.; Guizani, N.; Du, X. Efficient and Traceable Patient Health Data Search System for Hospital Management in Smart Cities. IEEE Internet Things J. 2020, 8, 6425–6436. [Google Scholar] [CrossRef]
- Bhattamisra, S.K.; Banerjee, P.; Gupta, P.; Mayuren, J.; Patra, S.; Candasamy, M. Artificial Intelligence in Pharmaceutical and Healthcare Research. Big Data Cogn. Comput. 2023, 7, 10. [Google Scholar] [CrossRef]
- Patel, L.; Shukla, T.; Huang, X.; Ussery, D.W.; Wang, S. Machine Learning Methods in Drug Discovery. Molecules 2020, 25, 5277. [Google Scholar] [CrossRef] [PubMed]
- Walters, W.P.; Barzilay, R. Critical assessment of AI in drug discovery. Expert Opin. Drug Discov. 2021, 16, 937–947. [Google Scholar] [CrossRef] [PubMed]
- Hessler, G.; Baringhaus, K.-H. Artificial Intelligence in Drug Design. Molecules 2018, 23, 2520. [Google Scholar] [CrossRef] [PubMed]
- Tan, B.K.J.; Teo, C.B.; Tadeo, X.; Peng, S.; Soh, H.P.L.; Du, S.D.X.; Luo, V.W.Y.; Bandla, A.; Sundar, R.; Ho, D.; et al. Personalised, Rational, Efficacy-Driven Cancer Drug Dosing via an Artificial Intelligence SystEm (PRECISE): A Protocol for the PRECISE CURATE.AI Pilot Clinical Trial. Front. Digit. Heal. 2021, 3. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Liu, X.; Zhang, S.; Chen, S. Artificial intelligence for drug discovery: Resources, methods, and applications. Mol. Ther. - Nucleic Acids 2023, 31, 691–702. [Google Scholar] [CrossRef] [PubMed]
- Sirajudeen, F.; Malhab, L.J.B.; Bustanji, Y.; Shahwan, M.; Alzoubi, K.H.; Semreen, M.H.; Taneera, J.; El-Huneidi, W.; Abu-Gharbieh, E. Exploring the Potential of Rosemary Derived Compounds (Rosmarinic and Carnosic Acids) as Cancer Therapeutics: Current Knowledge and Future Perspectives. Biomol. Ther. 2024, 32, 38–55. [Google Scholar] [CrossRef] [PubMed]
- Yuan, F.; Klavon, E.; Liu, Z.; Lopez, R.P.; Zhao, X. A Systematic Review of Robotic Rehabilitation for Cognitive Training. Front. Robot. AI 2021, 8. [Google Scholar] [CrossRef] [PubMed]
- M. Asada et al., “Cognitive developmental robotics: A survey,” IEEE transactions on autonomous mental development, vol. 1, no. 1, pp. 12-34, 2009.
- Kachouie, R.; Sedighadeli, S.; Khosla, R.; Chu, M.-T. Socially Assistive Robots in Elderly Care: A Mixed-Method Systematic Literature Review. Int. J. Human–Computer Interact. 2014, 30, 369–393. [Google Scholar] [CrossRef]
- Denecke, K.; Baudoin, C.R. A Review of Artificial Intelligence and Robotics in Transformed Health Ecosystems. Front. Med. 2022, 9, 795957. [Google Scholar] [CrossRef] [PubMed]
- Kyrkou, C.; Kolios, P.; Theocharides, T.; Polycarpou, M. Machine Learning for Emergency Management: A Survey and Future Outlook. Proc. IEEE 2022, 111, 19–41. [Google Scholar] [CrossRef]
- Deo, N.; Anjankar, A. Artificial Intelligence With Robotics in Healthcare: A Narrative Review of Its Viability in India. Cureus 2023, 15, e39416. [Google Scholar] [CrossRef] [PubMed]
- C. Ho et al., “Robot-assisted surgery compared with open surgery and laparoscopic surgery: clinical effectiveness and economic analyses,” 2013.
- C. R. Piccininni, “Cost-Effectiveness of Robotics and Artificial Intelligence in Healthcare: Focus on Robot-Assisted Prostatectomy,” University of Western Ontario Medical Journal, vol. 87, no. 2, pp. 49-51, 2018.
- Ahmed, K.; Ibrahim, A.; Wang, T.T.; Khan, N.; Challacombe, B.; Khan, M.S.; Dasgupta, P. Assessing the cost effectiveness of robotics in urological surgery – a systematic review. BJU Int. 2012, 110, 1544–1556. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Luo, M.; Wu, P.; Wu, S.; Lee, T.-Y.; Bai, C. Application of Computational Biology and Artificial Intelligence in Drug Design. Int. J. Mol. Sci. 2022, 23, 13568. [Google Scholar] [CrossRef] [PubMed]
- Carracedo-Reboredo, P.; Liñares-Blanco, J.; Rodríguez-Fernández, N.; Cedrón, F.; Novoa, F.J.; Carballal, A.; Maojo, V.; Pazos, A.; Fernandez-Lozano, C. A review on machine learning approaches and trends in drug discovery. Comput. Struct. Biotechnol. J. 2021, 19, 4538–4558. [Google Scholar] [CrossRef] [PubMed]
- M. Batool, B. M. Batool, B. Ahmad, and S. Choi, “A structure-based drug discovery paradigm,” International journal of molecular sciences, vol. 20, no. 11, p. 2783, 2019.
- Basile, A.O.; Yahi, A.; Tatonetti, N.P. Artificial Intelligence for Drug Toxicity and Safety. Trends Pharmacol. Sci. 2019, 40, 624–635. [Google Scholar] [CrossRef] [PubMed]
- Mirzaei, S.; Mao, H.; Al-Nima, R.R.O.; Woo, W.L. Explainable AI Evaluation: A Top-Down Approach for Selecting Optimal Explanations for Black Box Models. Information 2023, 15, 4. [Google Scholar] [CrossRef]
- Isgut, M.; Gloster, L.; Choi, K.; Venugopalan, J.; Wang, M.D. Systematic Review of Advanced AI Methods for Improving Healthcare Data Quality in Post COVID-19 Era. IEEE Rev. Biomed. Eng. 2022, 16, 53–69. [Google Scholar] [CrossRef]
- Yang, Y.C.; Islam, S.U.; Noor, A.; Khan, S.; Afsar, W.; Nazir, S. Influential Usage of Big Data and Artificial Intelligence in Healthcare. Comput. Math. Methods Med. 2021, 2021, 1–13. [Google Scholar] [CrossRef]
- Sanders, R.; Bustin, S.; Huggett, J.; Mason, D. Improving the standardization of mRNA measurement by RT-qPCR. Biomol. Detect. Quantif. 2018, 15, 13–17. [Google Scholar] [CrossRef]
- Islam, M.; Rahman, M.; Taher, A.; Quaosar, G.M.A.A.; Uddin, A. Using artificial intelligence for hiring talents in a moderated mechanism. Futur. Bus. J. 2024, 10, 1–16. [Google Scholar] [CrossRef]
- Amaya, J.; Holweg, M. Using algorithms to improve knowledge work. J. Oper. Manag. 2024, 70, 482–513. [Google Scholar] [CrossRef]
- Bužančić, *!!! REPLACE !!!*; et al. , “Clinical decision-making in benzodiazepine deprescribing by healthcare providers vs. AI-assisted approach,” British Journal of Clinical Pharmacology, vol. 90, no. 3, pp. 662-674, 2024.
- Pruski, M. AI-Enhanced Healthcare: Not a new Paradigm for Informed Consent. J. Bioethical Inq. 2024, 1–15. [Google Scholar] [CrossRef]
- Cao, B.; Huang, S.; Tang, W. AI triage or manual triage? Exploring medical staffs’ preference for AI triage in China. Patient Educ. Couns. 2024, 119, 108076. [Google Scholar] [CrossRef]
- M. 10 2317, 2024.
- Wang, W.; Wang, Y.; Chen, L.; Ma, R.; Zhang, M. Justice at the Forefront: Cultivating felt accountability towards Artificial Intelligence among healthcare professionals. Soc. Sci. Med. 2024, 347, 116717. [Google Scholar] [CrossRef]
- Lakkimsetti, M.; Devella, S.G.; Patel, K.B.; Dhandibhotla, S.; Kaur, J.; Mathew, M.; Kataria, J.; Nallani, M.; E Farwa, U.; Patel, T.; et al. Optimizing the Clinical Direction of Artificial Intelligence With Health Policy: A Narrative Review of the Literature. Cureus 2024, 16, e58400. [Google Scholar] [CrossRef]
- F. Pesapane and P. Summers, “Ethics and regulations for AI in radiology,” in Artificial Intelligence for Medicine: Elsevier, 2024, pp. 179-192.
- N. Ferruz et al., “Anniversary AI reflections,” Nature Machine Intelligence, vol. 6, no. 1, pp. 6-12, 2024.
- M. M. Soliman, E. M. M. Soliman, E. Ahmed, A. Darwish, and A. E. Hassanien, “Artificial intelligence powered Metaverse: analysis, challenges and future perspectives,” Artificial Intelligence Review, vol. 57, no. 2, p. 36, 2024.
- N. Singh, M. N. Singh, M. Jain, M. M. Kamal, R. Bodhi, and B. Gupta, “Technological paradoxes and artificial intelligence implementation in healthcare. An application of paradox theory,” Technological Forecasting and Social Change, vol. 198, p. 122967, 2024.
- Palaniappan, K.; Lin, E.Y.T.; Vogel, S. Global Regulatory Frameworks for the Use of Artificial Intelligence (AI) in the Healthcare Services Sector. Healthcare 2024, 12, 562. [Google Scholar] [CrossRef] [PubMed]
- Habbal, A.; Ali, M.K.; Abuzaraida, M.A. Artificial Intelligence Trust, Risk and Security Management (AI TRiSM): Frameworks, applications, challenges and future research directions. Expert Syst. Appl. 2024, 240. [Google Scholar] [CrossRef]
- Mensah, G.B.; Dutta, P.K. Evaluating if Ghana's Health Institutions and Facilities Act 2011 (Act 829) Sufficiently Addresses Medical Negligence Risks from Integration of Artificial Intelligence Systems. Mesopotamian J. Artif. Intell. Heal. 2024, 2024, 35–41. [Google Scholar] [CrossRef]
- Chen, Y.; Esmaeilzadeh, P. Generative AI in Medical Practice: In-Depth Exploration of Privacy and Security Challenges. J. Med Internet Res. 2024, 26, e53008. [Google Scholar] [CrossRef]
- Malgieri, G.; Pasquale, F. Licensing high-risk artificial intelligence: Toward ex ante justification for a disruptive technology. Comput. Law Secur. Rev. 2024, 52. [Google Scholar] [CrossRef]
- W. House, Blueprint for an ai bill of rights: Making automated systems work for the american people. Nimble Books, 2022.
- Beccia, F.; Di Marcantonio, M.; Causio, F.A.; Schleicher, L.; Wang, L.; Cadeddu, C.; Ricciardi, W.; Boccia, S. Integrating China in the International Consortium for Personalised Medicine: a position paper on innovation and digitalization in Personalized Medicine. BMC Public Heal. 2024, 24, 1–11. [Google Scholar] [CrossRef]
- Jin, J.; Du, H. Research on the identification and evolution of health industry policy instruments in China. Front. Public Heal. 2024, 12, 1264827. [Google Scholar] [CrossRef]
- Singh, B.; Jevnikar, A.M.; Desjardins, E. Artificial Intelligence, Big Data, and Regulation of Immunity: Challenges and Opportunities. Arch. Immunol. et Ther. Exp. 2024, 72. [Google Scholar] [CrossRef]
Figure 1.
The figure illustrates the structure for integrating artificial intelligence (AI) into medical diagnostics, consisting of four primary components. AI application is closely associated with important medical domains like as ophthalmology, cancer diagnosis, and cardiovascular risk prediction. Artificial intelligence has the potential to enhance diagnosis accuracy by analyzing data and recognizing trends. The primary components are machine learning algorithms, high computational capacity, and natural language processing. Additionally, there is a continous integration of clinical applications to provide specific treatment.
Figure 1.
The figure illustrates the structure for integrating artificial intelligence (AI) into medical diagnostics, consisting of four primary components. AI application is closely associated with important medical domains like as ophthalmology, cancer diagnosis, and cardiovascular risk prediction. Artificial intelligence has the potential to enhance diagnosis accuracy by analyzing data and recognizing trends. The primary components are machine learning algorithms, high computational capacity, and natural language processing. Additionally, there is a continous integration of clinical applications to provide specific treatment.
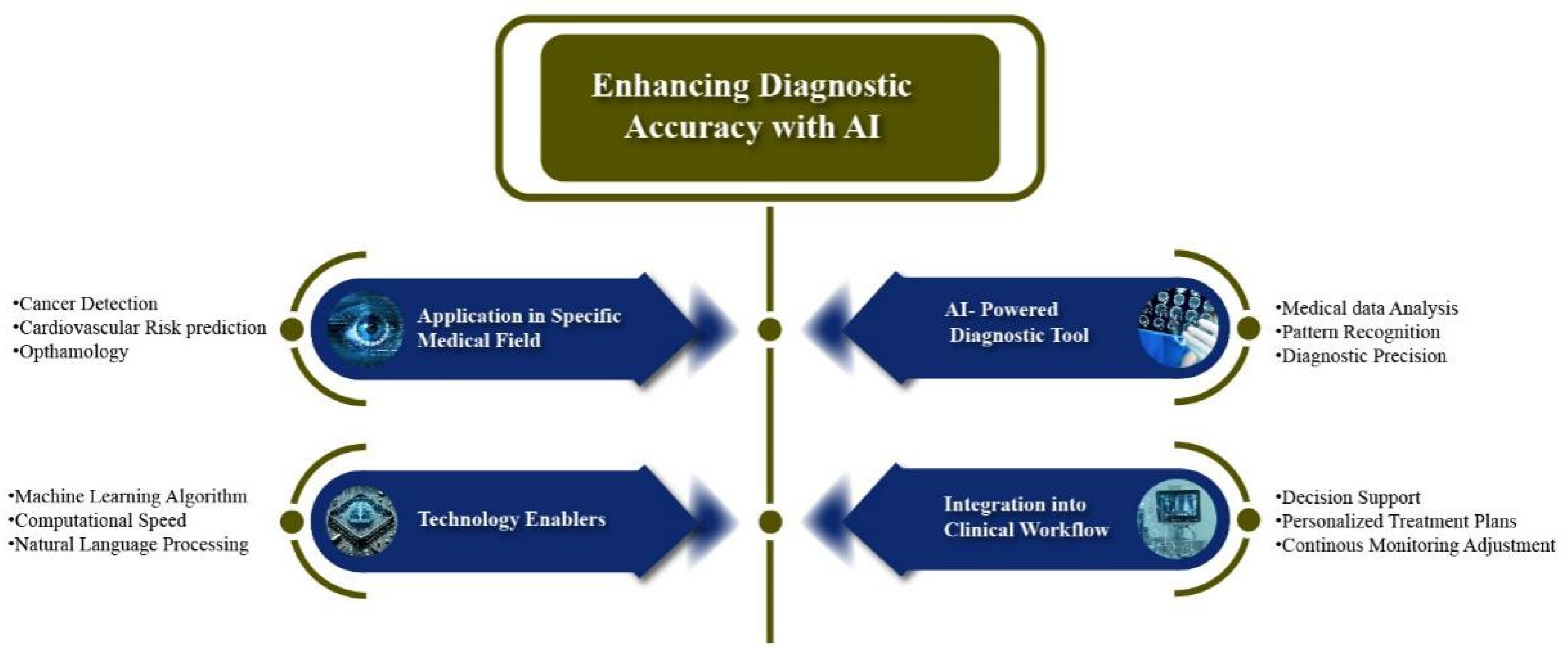
Figure 2.
The image illustrates the application of AI-augmented medical instruments in the radiology workplace. It highlights the major functions, such as image reconstruction, pathology identification, and treatment prognosis. These capabilities are integrated with smart medical devices such as blood pressure monitors and an artificial pancreas. This combination aims to improve diagnostic precision while also enhancing treatment efficiency for patients.
Figure 2.
The image illustrates the application of AI-augmented medical instruments in the radiology workplace. It highlights the major functions, such as image reconstruction, pathology identification, and treatment prognosis. These capabilities are integrated with smart medical devices such as blood pressure monitors and an artificial pancreas. This combination aims to improve diagnostic precision while also enhancing treatment efficiency for patients.
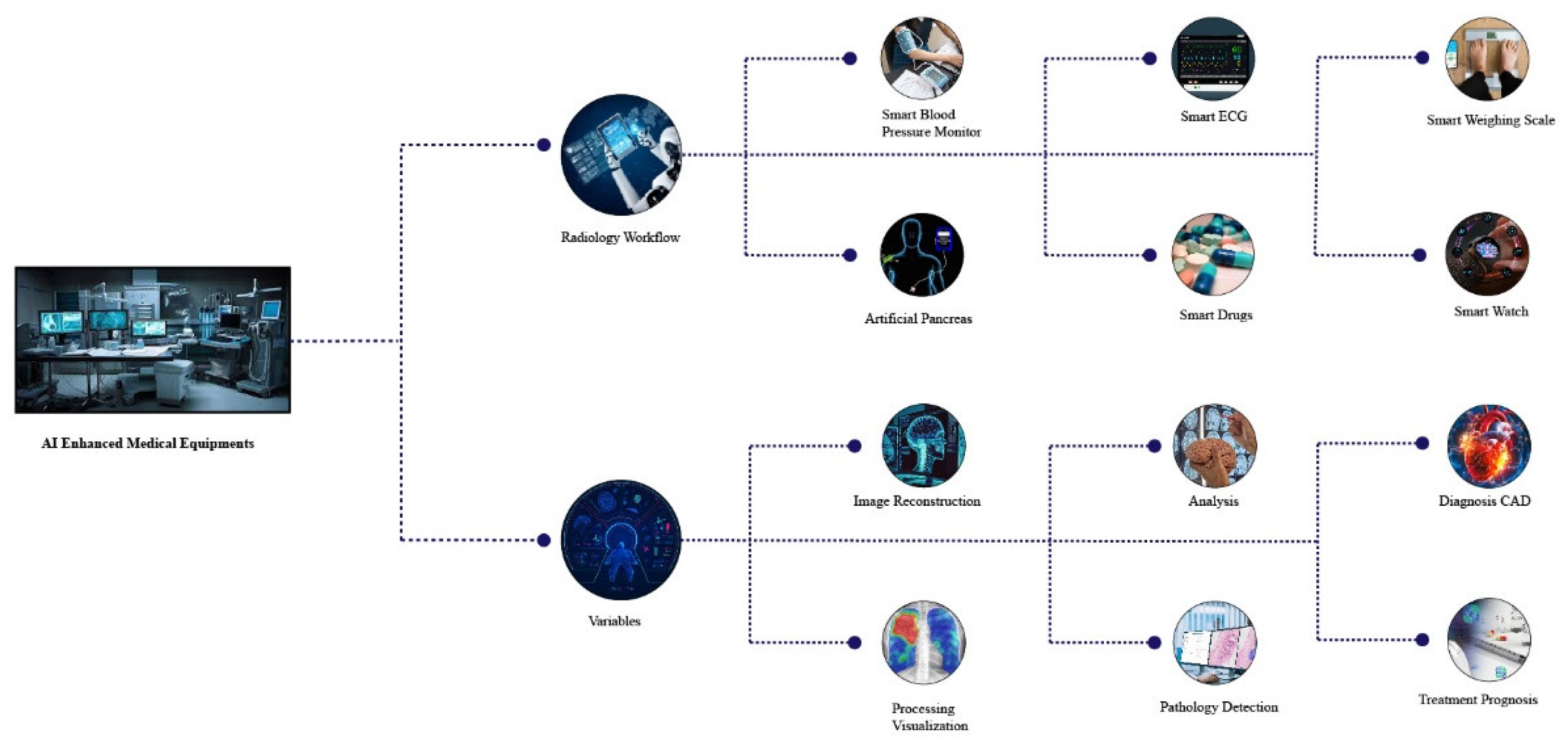
Figure 3.
The figure summarizes three critical aspects of enhancing the role of artificial intelligence in surgery. On the one hand, visual and motion technology relies on various sensors, adaptive movements as well as enhanced visualization to achieve surgical precision. On the other hand, robot-assisted surgery utilizes AI for the exact percutaneous and minimal invasive technique, which is directed only by the surgeon for the best outcome. Finally, the control of remote surgery applies communication technology helps for global reach and collaborates experts which provides surgeons with the ability to perform and supervise surgeries from a remote location. In brief, the picture illustrates how AI can improve the accuracy of surgery, extend the capabilities and bring together globe experts for knowledge-sharing.
Figure 3.
The figure summarizes three critical aspects of enhancing the role of artificial intelligence in surgery. On the one hand, visual and motion technology relies on various sensors, adaptive movements as well as enhanced visualization to achieve surgical precision. On the other hand, robot-assisted surgery utilizes AI for the exact percutaneous and minimal invasive technique, which is directed only by the surgeon for the best outcome. Finally, the control of remote surgery applies communication technology helps for global reach and collaborates experts which provides surgeons with the ability to perform and supervise surgeries from a remote location. In brief, the picture illustrates how AI can improve the accuracy of surgery, extend the capabilities and bring together globe experts for knowledge-sharing.
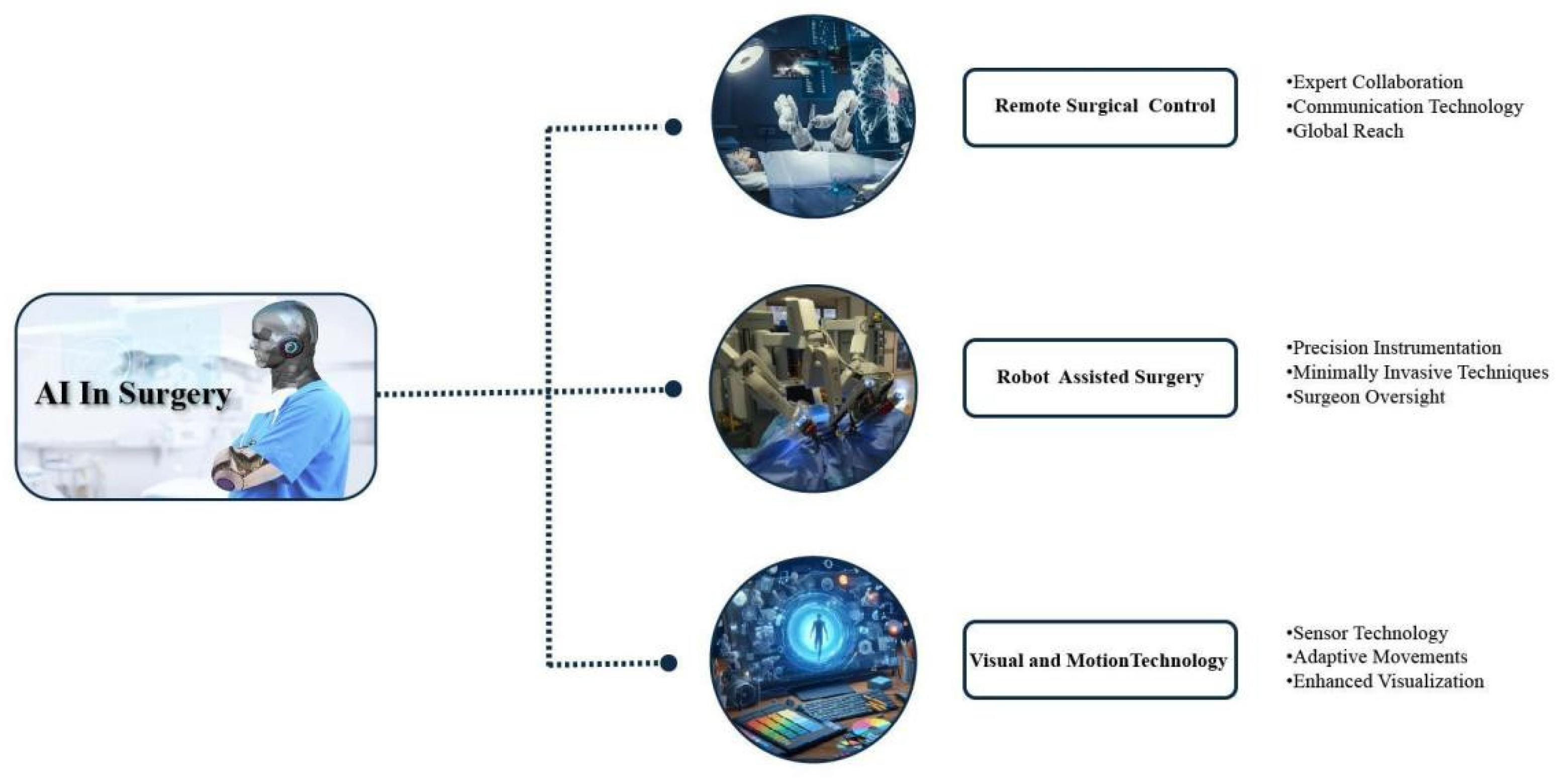
Figure 4.
This image depicts the diverse uses of artificial intelligence (AI) in clinical practice, emphasizing five crucial domains: Artificial intelligence (AI) is utilized in diagnostic imaging to enhance the precision and efficiency of medical diagnoses. AI is also employed in laboratory data analysis to reduce the time needed for comprehension, drug discovery, and identification of biomarkers. Additionally, AI is used in managing patients’ data, allowing for continuous monitoring of their health and personalized treatment. AI is further utilized in medication development, offering predictive modeling for rapid medication creation and personalization. Lastly, AI is employed in robotic surgery. The applications collectively illustrate that AI plays a distinctive role in enhancing service delivery and patient care to unprecedented levels.
Figure 4.
This image depicts the diverse uses of artificial intelligence (AI) in clinical practice, emphasizing five crucial domains: Artificial intelligence (AI) is utilized in diagnostic imaging to enhance the precision and efficiency of medical diagnoses. AI is also employed in laboratory data analysis to reduce the time needed for comprehension, drug discovery, and identification of biomarkers. Additionally, AI is used in managing patients’ data, allowing for continuous monitoring of their health and personalized treatment. AI is further utilized in medication development, offering predictive modeling for rapid medication creation and personalization. Lastly, AI is employed in robotic surgery. The applications collectively illustrate that AI plays a distinctive role in enhancing service delivery and patient care to unprecedented levels.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



