
Submitted:
10 July 2024
Posted:
11 July 2024
You are already at the latest version
Abstract
Autosomal Dominant Polycystic Kidney Disease (ADPKD) is a genetic disorder characterized by the development and progression of multiple renal cysts, leading to progressive renal function decline. To date, the only approved treatment for this condition is able to slow down the loss of annual renal function, without stopping the disease progression. Furthermore, this therapy is approved only for patients with rapid disease progression and its compliance is problematic because of the impact of this drug on quality of life. The recent literature suggests that cystic cells are subject to metabolic dysregulation in the glucose pathway (Warburg Effect). This finding paved the way for new lines of research targeting potential therapeutic interventions for ADPKD. In particular, this review highlights the latest studies on the use of ketosis, through ketogenic dietary interventions (daily calorie restriction, intermittent fasting, time-restricted feeding, and ketogenic diets), as a potential strategy for patients with ADPKD, and the possible involvement of microbiota in the ketogenic interventions’ effect.
Keywords:
ADPKD
; ketogenic diet
; ketosis
; kidney cysts
; PKD
; renal function decline
1. Introduction
Autosomal Dominant Polycystic Kidney Disease (ADPKD) is one of the most common genetic disorders, with an estimated prevalence of 3.29 - 3.96/10,000 people in Europe [1,2,3]. The disease is characterized by mutations involving PKD1, PKD2, and a few other genes that cause the formation and enlargement of multiple renal cysts in 1-2% of nephrons [4,5], leading to a progressive renal function decline. According to the European Renal Association (ERA) Registry Annual Report, patients with ADPKD were the youngest among primary renal disease groups to undergo kidney replacement therapy, with 68% being younger than 64 years old. Furthermore, twice as many of these patients received preemptive kidney transplants compared to the other primary renal disease groups [6]. The main manifestations of the disease are glomerular filtration rate (GFR) loss, hypertension, nephrolithiasis, gross haematuria, cyst infection, and acute and chronic pain as a consequence of kidneys’ enlargement and episodes of lithiasis. Extra-renal manifestations of ADPKD include the development of cysts in other organs, especially in liver parenchyma, which may cause pain, early satiety, gastro-oesophageal reflux, and and rarely in the most severe cases portal hypertension with ascites and pleural effusion [4]. To date, the only approved drug for this condition (Tolvaptan) is able to slow down the loss of annual renal function, but it does not stop the disease progression [7]. Furthermore, the drug is approved only in subjects with evidence of rapidly progressing disease [8]. Because of the side effects impacting the quality of life, Tolvaptan is not always accepted by the patients. Recent literature suggests that cystic cells are subject to metabolic dysregulation in the glucose pathway (Warburg effect). This paved the way for new lines of research for potential ADPKD therapeutic targets [9,10]. In particular, in this review, we illustrate the latest studies on the use of ketosis induced by ketogenic dietary interventions (KDIs), as a possible therapeutic strategy for patients with ADPKD.
2. Brief Overview on Glucose Metabolism, Warburg Effect, and Ketosis
Typically, glucose is the main energy source for cells, undergoing metabolism via glycolysis (Figure 1). Facilitative transporters (GLUT1-4) usher glucose into cells, where it undergoes phosphorylation at position 6 by hexokinase enzymes (hexokinases 1 or 2, HKs). Following this, eight enzymatic reactions occur in the cytosol, resulting in the production of 2 pyruvate molecules and a net gain of 2 adenosine triphosphate (ATP) molecules for each glucose. When oxygen is present, pyruvate is typically shuttled into mitochondria for conversion into acetyl coenzyme A (acetyl-CoA), so as to fuel oxidative phosphorylation (OXPHOS) and yielding around 36 molecules of ATP per molecule of glucose. However, in anaerobic conditions, pyruvate is converted to lactate in the cytosol (anaerobic glycolysis), yielding 2 molecules of ATP per molecule of glucose. Hyperproliferative states like cancer often favor this less efficient metabolic process even when oxygen is available: this particular metabolic phenomenon is generally known as “aerobic glycolysis” or “Warburg Effect” (WE). Since aerobic glycolysis yields much less energy (approximately 4 molecules of ATP per molecule of glucose) compared to OXPHOS, cells compensate by upregulating glucose import and cytosolic degradation. The WE, while yielding less ATP per mole of glucose compared to OXPHOS, leaves unexploited carbonic chains available for anabolic processes, thus providing a substantial growth advantage to cancer cells [11,12]. Glucose deprivation in some cancer cell lines, called “glucose sensitive cancers” (GSCs), leads to decreased ATP production and cell death, probably triggered by a failure in ROS regulation by the antioxidant system [13]. Recent literature suggests that kidney cystic cells, similarly to GSCs, are subject to the WE. Moreover, high urinary acetylcarnitine in a PKD mouse model suggests mitochondrial abnormalities, along with diminished OXPHOS and impaired fatty acid oxidation, which is one of the conditions which favor aerobic glycolysis. This has paved the way for new lines of research for potential ADPKD therapeutic targets [8,9].
A drastic reduction in circulating glucose levels occurs during a fast long enough to deplete the body’s glycogen stores. In this condition, ketone bodies (acetone, acetoacetate, and β-hydroxybutyrate - BHB) are synthesized from β-oxidation of fatty acids to become an alternative source of energy, generating 20 and 22.5 ATP per molecule for acetoacetate and BHB, respectively [14,15].
This effect can be achieved by: (i) reducing the energy intake through daily calorie restriction (DCR); (ii) intermittent fasting (IMF); (iii) time-restricted feeding (TRF), a dietary approach that restricts food intake to a specific window of time each day, with fasting periods outside of that window; and (iv) ketogenic diets (KDs) (Table 1).
KDs are low-carb, high-fat diets that mimics fasting and induce ketogenesis, but allowing the subjects to continue feeding and meeting their daily caloric needs [16]. KDs, introduced in 1920 for the treatment of drug-resistant epilepsy, are now used for a variety of other neurological [17], metabolic and non-metabolic diseases [18], and could be potentially used in ADPKD patients to slow down the progression of the disease. Currently, there are five types of KD therapies available: classic KD (cKD), medium-chain triglyceride diet (MCT), modified Atkins diet (MAD), low glycemic index treatment (LGIT), and the very low-calorie KD (VLCKD) a diet conceived for weight loss [17,19]. The cKD consists of a ratio of 4:1 or 3:1 grams of fat to combined protein and carbohydrates. The MCT, MAD and LGIT have been developed as normocaloric diets that allow to achieve a state of ketosis, while reducing fat intake. This modification allows for a higher protein content, necessary for growth, as well as improved tolerability and palatability [17]. Of particular relevance is the use of MAD in the adult population, as it can be initiated in an outpatient setting, requires only monitoring of daily carbohydrate intake (max. 20 g/day) and a preference for lipid-rich foods, while there are no restrictions on proteins, liquids, or calories. These factors make meal planning easier and enhance patient compliance [20].
3. Ketosis in ADPKD Animal Models
In the last 10 years, several preclinical studies involving PKD animal models has been carried out to both understand the pathophysiology of the disease and to identify potential new therapies [5]. In addition to studies exploring possible pharmacological interventions, considering the cysts’ defective metabolism, some authors focused on the possibility of acting through diet manipulation.
In 2016, Warner et al. [21] induced a 40% DCR for 6 months compared to a standard ad libitum (AL) diet in an ADPKD mouse model. After the treatment period, the nearly complete inhibition of cyst development was observed due to DCR. The authors also found that kidney inflammation decreased to the level of normal wild-type controls kidneys. In addition, by histological analysis and evaluation of acute and chronic kidney markers of integrity, a decrease in fibrosis and kidney injury was observed in DCR compared to AL. Finally, DCR mice showed a decrease in both markers of cellular proliferation and apoptosis. The reduction of cystogenesis was confirmed even with a mild DCR (10 and 20%), result confirmed by the study by Kipp et al. [22] on ADPKD mice fed on average 77% of the food consumed by the AL controls. The same group, then, confirmed in animal models that the inhibitory effects on ADPKD progression, obtained through DCR, were cause by the induction of ketosis, that impacted the cystic cells because they are metabolically inflexible and thus unable to adapt to alternative fuel sources. The researchers measured BHB levels in the ADPKD mice used for the DCR study and found significantly higher values compared to those in the control group, suggesting that mice underwent IMF leading to ketosis. To test this hypothesis, the group placed PKD rats on a TRF regime wherein they had access to food for an 8-h period [23]. After five weeks, animals on the TRF diet showed significantly less renal cystic disease progression than those on the AL diet. TRF-treated animals had fewer and smaller cysts, improved kidney function, and increased levels of BHB, indicating the induced ketosis. The research team then explored the use of a KD, by giving PKD mice ad libitum access to a high-fat, very-low-carbohydrate KD. In juvenile mice threated with KD, the progression of renal cystic disease was significantly inhibited compared to those on AL. Additionally, KD feeding led to improved kidney function and inhibited both cyst formation and expansion. In adult specimens, the overall number of cysts per animal remained unchanged with KD; nonetheless, there was a significant decrease in cyst size, suggesting that KD feeding prevents cyst enlargement in animals of that age. Torres et al. [23] subsequently subjected Persian PKD cats to a 72-hour fast, resulting in an average reduction of total kidney volume (TKV) by 15%, suggesting fluid drainage during fasting. Considering that KD increases ketonemia, the authors finally attempted to administer BHB to mice fed AL with normal chow. After 5 weeks, the kidneys of treated PKD animals resembled those of wild-type animals in appearance and structure. BHB-treated PKD rats showed notable reductions in kidney size and cystic area compared to controls. BHB treatment also led to improved kidney function and reduced fibrosis, myofibroblast presence, and cell proliferation. This result was likely mediated by mTOR signalling inhibition [23]. Studies have shown that mTOR inhibitors can effectively reduce cyst growth and preserve kidney function in animal models of ADPKD [24]. However, the use of mTOR inhibitors in ADPKD patients was not successful[25]. Recently, Torres group found that the simultaneous administration of BHB and citrate not only significantly decelerated the progression of PKD in juvenile rats, but also partially reversed the established cystic disease in adult rats [26]. Hopp et al. [27] conducted a study to compare DCR, IMF and TRF in PKD mice. In their study, only the DCR regimen proved effective in slowing the progression of cystic kidney disease. However, contrary to expectations, the lack of benefit observed with TRF does not align with Torres et al. findings. This discrepancy could be attributed to differences in the PKD gene variant, disease progression timing, species background, or intervention duration. Moreover, the absence of a therapeutic effect in animals on IMF may be attributed to compensatory overeating on non-fasting days. In this study, the authors observed that the therapeutic effect was evident solely in animals who followed a dietary regimen leading to weight loss. This presents another inconsistency compared to the studies by Torres and Kipp, where DCR and TRF achieved effectiveness in slowing PKD progression without a significant change in body weight (BW) compared to the control group. Once more, the choice of model or the timing of disease progression might elucidate the discordant outcomes [27].
4. Ketosis in ADPKD Patients
The first study evaluating tolerability and safety of ketosis in ADPKD patients was the GREASE single arm interventional pilot study [20]. Three patients with ADPKD were enrolled to follow a MAD for three months. Tolerability was assessed by a 29 items questionnaire on satisfaction, compliance and wellness, that reported overall positive reviews. Patients reported no difficulties with food quality or quantity, nor did they find their taste challenged or experience trouble in purchasing or preparing it. The greatest difficulty regarding compliance was reported by a patient who mentioned difficulties related to the social implications of a restrictive diet and complained about the discomfort of monitoring glycaemia and ketonemia. Finally, it is worth noting that the wellness area received the highest overall satisfaction scores in the questionnaire. The MAD had few predictable side effects (keto-flu), mostly occurring during the initial phase, such as fatigue, muscle cramps, and constipation. Patients in the study experienced an increase in total cholesterol over the follow-up period and a decrease in blood pressure values, aligning with existing literature.
Following this first trial, Strubl et al. conducted a retrospective study to assess safety, feasibility, and effects of KDIs in ADPKD patients. Through questionnaires, they gathered information from ADPKD patients who had previously undergone KDs and TRDs for at least 6 months [28]. The majority of participants reported an overall enhancement in their quality of life and well-being, including a reduction in disease-related pain (such as hip and/or back pain, abdominal swelling, and early satiety). Weight loss was reported by approximately 90% of the participants, a noteworthy result since adiposity, particularly visceral adiposity, is independently linked to accelerated kidney growth and reduces Tolvaptan effectiveness [29,30]. More than half of the patients reported improved blood pressure control, and approximately 15% reported reducing antihypertensive medication. Some participants experienced eGFR improvements, however, reliability was limited due to single, uncontrolled values and eGFR fluctuations. A slight increase might imply stabilized renal function, but glomerular hyperfiltration due to increased protein intake s ,which could affect kidney health negatively, cannot be ruled out [28,31]. As already emphasized, a well-designed KD includes an adequate content of protein [16]. However, little we know about the actual composition of the diets followed by the interviewed patients and their adherence to these protocols [32]. Most participants found KDIs manageable, with minimal impact on food preparation time. The majority described the diet as easy to follow and would recommend it. While half adhered daily, over 40% skipped occasionally due to practical difficulties, particularly with the KD. Despite challenges, KDIs appeared feasible for PKD patients, with manageable implementation and adherence. The side effects reported in the data collection were consistent with those found in the GREASE study. These preliminary evaluations demonstrated that KDIs are safe and feasible in ADPKD, clearing the path for controlled studies with larger patient numbers and longer duration. On safety, it is necessary to emphasize that these nutritional protocols entail significant metabolic changes and are not balanced; therefore, they require formulation by an experienced dietitian. Supplementing the KD with vitamins, minerals, and, if necessary, fiber prevents nutritional deficiencies and intestinal issues. A common misconception is that these diets must be high in protein, while a well-formulated KD is characterized by a high-fat and low-carbohydrate intake, while protein content ranges from normal to moderate [16]. Moreover, the use of a diet with moderate protein content is not currently contraindicated in ADPKD patients. The latest guidelines for the nutritional treatment of ADPKD patients with chronic kidney disease (CKD) suggest considering personalized nutritional plans for these patients, as studies suggest that they may not benefit from protein restriction [33].
One potential side effect of long-term KDs may be an increased risk of developing kidney stones [34]. Uric acid stones are the most frequent type observed in KD patients, followed by calcium-based and mixed uric acid-calcium stones. The exact mechanism behind kidney stone formation on this diet remains uncertain but could be associated with conditions like hypocitraturia and acidosis, typical in individuals adhering to a high-protein, low-alkali diet. Consequently, urine alkalization with oral potassium citrate, a strategy already employed in patients with drug-resistant epilepsy using KDs, should be considered in patients with ADPKD to prevent uric acid precipitation [34]. Lastly, another concern regarding the KD is its impact on cardiovascular disease (CVD) risk. To date, the long-term effects of the ketogenic diet on dyslipidemia, hypertension and overall cardiovascular risk are still uncertain, with conflicting findings in research [35,36,37,38]. This lack of consensus depends on several factors: heterogeneity across studies, small number of studies in certain populations (e.g., normal-weight adults), KD composition and control diets, KD fat sources, patient’s adherence, and ketone concentration [35,36,39].
There are few published uncontrolled clinical studies on the use of KDIs in ADPKD: some who have primarily assessed the feasibility and safety of the therapy [20,27], while others have evaluated its impact in small groups of patients [40,41,42,43]. Moreover, to our knowledge, two studies are on-going [44,45] and one interventional study with no control group is not yet recruiting [46].
The 16-week duration Ren.nu program [40] adopted a plant-focused KD, with 30-40 g net carbohydrates, designed to avoid some renal stressors (oxalate, inorganic phosphate, and purines/uric acid). The diet included a moderate intake of fish, eggs, and full-fat dairy to achieve a protein intake of ≤ 0.8 g/kg BW. Patients were also administered a supplement containing BHB, citrate, potassium, calcium, and magnesium. The study involved training patients to monitor ketosis levels alongside nutrition management. Twenty participants concluded the trial, which commenced with a one-day modified fast comprising 500–600 kcal, including moderate levels of protein and carbohydrates, followed by the actual KD. After 8 weeks of treatment, participants were advised to follow a TRF regimen for an additional 4 weeks. At the end of the program, patients reported that the program improved their PKD symptoms, in particular regarding flank pain and fatigue. The diet was appreciated and deemed feasible, except for the already known initial keto-flu and meals eaten outside the home. Anthropometric measures, blood tests, and kidney function were analyzed post-trial, revealing weight loss, blood sugar reduction, and kidney function improvements. However, kidney function assessment was limited to creatinine measurement and estimated glomerular filtration rate. The same authors agree that the study obviously has limitations, primarily due to the lack of a control group and the acquisition of data mainly through self-measurements and questionnaires from highly motivated individuals. Long-term, randomized clinical trials involving larger patient groups are certainly necessary to evaluate these initial findings.
5. Ketosis in ADPKD Patients: RCTs
Table 2 summarizes the completed and ongoing RCTs on KDIs in ADPKD.
In addition to their investigation on PKD mice model, Hopp et al. carried out a parallel study on weight loss via DCR or IMF in a cohort of overweight or obese patients with ADPKD [27]. The study was based on the premise that epidemiological observation suggests that ADPKD progression is significantly faster with increased BMI [29]. Based on previous animal studies by Warner and Torres [21,23], the authors expected a greater slowdown in pathology in IMF patients compared to DCR ones. Surprisingly, researchers found that both groups exhibited a similar annual kidney growth rate, which was notably lower compared to historical controls. Moreover, participants who achieved clinically significant weight loss showed, on average, a cessation of kidney growth. Intriguingly, they also noticed a correlation between weight loss, decreased abdominal fat, and slower kidney growth. The findings suggest that weight loss might play a crucial role in slowing cyst growth in overweight or obese ADPKD patients. However, it is not yet possible to determine whether the decrease in BW is merely a secondary effect of the therapeutic efficacy of metabolic reprogramming achieved through dietary manipulation. Indeed, the researchers were unable to assess BHB levels and thus ketosis induction due to sample instability and limitations related to COVID-19, which hindered obtaining fresh samples. [27]. Given these premises, the research group subsequently pursued studies on the use of TRF and DCR in overweight and obese ADPKD patients [42,45]. During these interventions it is crucial to avoid the risk of malnutrition or dehydration, that in the long term may lead to bone loss, anaemia, and other consequences. Furthermore, little is known about the long-term risks associated with these approaches. Recently, an abstract presented at the American Heart Association’s scientific conference indicated that 8-hour TRF might increase mortality from CVDs [47]. This study involved 20,000 adults in the U.S. who completed two 24-hour dietary recall questionnaires and were followed for a median of 8 years. The main limitations of the study are its reliance on self-reported dietary information, the lack of consideration for other health factors beyond the daily eating duration, and cause of death. Therefore, it is advisable to regard these KDIs as formally therapies, and thus, it is necessary to provide the patient with medical follow-up and dietary support throughout the entire process.
Following a small pilot trial on short-term ketogenic intervention of KD vs water fasting (WF) (RESET-PKD) [36], the first RCT examining KD interventions was conducted on 63 patients [41,43]. The study included randomization into 3 study arms for 3 months: a KD group (< 30 g/day carbohydrates and 0.8 g/kg BW/day protein), a group undergoing monthly 3-day WF, and a control group receiving routine dietary counselling for ADPKD patients. Consistent with previous studies, almost all patients in the KETO-ADPKD trial rated the KDs as feasible. The primary feasibility endpoint, which assessed both patient-reported feedback and objective evidence of ketosis (BHB ≥ 0.8 mmol/L at 75% of the in-person visits), was achieved only by the WF group, raising concerns about the feasibility of KD. However, the KD group’s failure to reach its threshold was attributed to a high predefined BHB threshold and the limited number of visits on the diet. Despite this, the KD group had significant impacts on outcomes, suggesting that lower BHB target values may still be effective. While WF and control groups showed an increase in TKV, the KD group showed a potential reduction, although this change did not reach statistical significance, possibly due to the limited duration of the study. Additionally, a variation in total liver volume (TLV) has been noticed, although it was likely due to glycogen depletion induced by the KD. Finally, the study revealed a statistically significant decrease in body fat mass and a statistically significant improvement of kidney function (as determined by serum creatinine and cystatin C) in the KD group.
The ongoing studies have leveraged the experiences of these preliminary studies to proceed with the long-term evaluation of larger patient groups. The Nowak group’s study focuses on weight loss through DCR [45]. Investigators are conducting a RCT involving overweight or obese adults with ADPKD. Their aim is to compare the effectiveness of a weight loss intervention based on DCR to a control group in slowing kidney growth over time. Secondary outcomes include changes in abdominal fat, and the effects of weight loss on biological pathways to gain mechanistic insight. Finally, GREASE2 is a 24-month RCT comparing a MAD to a balanced normocaloric diet (BND) on 92 non-obese ADPKD patients [44]. This study will assess the effect on TKV, safety, and tolerability of the MAD, and as a secondary objective, renal function decline (based on serum creatinine and cystatin C), along with the dietary impact on the variation of exploratory prognostic biomarkers. Both studies will evaluate changes in TKV and abdominal adiposity through Magnetic Resonance Imaging (MRI). Moreover, GREASE2 will assess changes in TLV after a 30-day return to the BND to allow for glycogen replenishment.
6. Kidney Disease, Ketosis, and Microbiota
It is worth noting that recent studies demonstrated that in renal pathologies the gut microbiota (GM) is significantly altered, showing proliferation of pathogenic bacteria [48,49,50,51,52,53]. The gut-kidney axis describes a two-way interaction between the kidneys and the gut microbiota: changes in gut bacteria can affect kidney function and vice versa, contributing to systemic inflammation and disease progression [54,55,56]. An eubiotic GM includes bacteria mainly from Firmicutes, Bacteroidetes, and Actinobacteria phyla [57]. These gut bacteria produce a variety of metabolites that significantly affect kidney health. Beneficial compounds like short-chain fatty acids (SCFA), including butyrate, acetate, and propionate, help lower colonic pH, inhibit harmful pathogens, and enhance the absorption of minerals and water, indirectly supporting kidney function. Vitamins produced by gut bacteria enhance immune function and cell health. However, some gut bacterial derived toxins can negatively impact the kidneys in case of dysbiosis [58]. Yacoub et al. conducted the first study on GM in PKD patients, considering different degrees of renal insufficiency [59]. The study strengthens the link between renal function alterations and GM composition. Specifically, researchers observed an increase in the Lactobacillaceae family and decreases in Oscillospira species in patients with decreased eGFR, which contrasts with previous reports showing a decrease in Lactobacillaceae and Prevotellaceae families in CKD patients. This discrepancy may be due to the confounding effects of comorbid conditions like diabetes in other studies. It also identified key metabolic pathways altered in CKD, emphasizing the role of uremic toxins produced by microbial protein catabolism, such as p-cresol sulfate and indoxyl sulfate. These toxins contribute to adverse cardiac outcomes and are elevated in advanced kidney disease [59]. A recent study on 25 ADPKD patients highlighted a shift towards gut dysbiosis also in PKD patients, which may influence disease progression. Healthy control subjects had a significantly higher presence of Actinobacteria, whereas ADPKD patients had increased levels of potentially harmful Enterobacteriaceae, as previously seen on chronic kidney disease patients [60,61]. PKD patients with advanced disease stages (Mayo Classes 1D and 1E) showed notably higher levels of Streptococcaceae. Early hypertension in ADPKD patients was associated with a rise in dysbiotic Proteobacteria and a reduction in probiotic Tannerelleaceae from the Bacteroidetes phylum. Elevated serum uremic toxins in ADPKD patients strongly correlated with lower eGFR and showed a positive trend with Peptococcaceae abundance [62].
Dietary manipulation is known to be one of the factors that can most influence the balance between bacteria [50,63,64]. Evaluating the GM in KDIs is challenging due to the limited number of studies and the significant variation in diet composition across different studies. The review by Kern et al. evaluated the impact of DCR, IMF and TRF in vivo and in human GM [65]. Studies suggest that these KDIs may alter gut microbiota diversity, increasing beneficial bacteria, while reducing harmful ones [65,66,67]. Notably, severe DCR (60%) can cause liver inflammation and increase harmful metabolites like trimethylamine N-oxide (TMAO): similar microbiota changes are seen in anorexia nervosa patients and severely calorie-restricted individuals, with reduced carbohydrate-utilizing bacteria and increased mucin-degrading bacteria [65]. On KD, most studies focus on cKD in pediatric epileptic population and VLCKD in obese patients. Both diets drastically decrease the polysaccharide intake by limiting the consumption of vegetables and fruit, while other KDs allow a higher content of these two foods. Overall, these studies suggest cKD and VLCKD may harm the gut mucus barrier due to microbial changes, by increasing harmful pathogens, such as Desulfovibrio spp. and E. Coli, and decreasing Bifidobacteria [63,68,69,70,71,72]. To date, we do not have sufficient data to assess the actual changes in the gut microbiota in KDIs. Large clinical randomized trials are needed to understand gut microbiota changes during different KDIs, in particular in those KDs that allows more polysaccharide intake than cKD and VLCKD.
7. Conclusions
The potential role of therapies inducing ketosis in managing ADPKD is supported by evidence from animal models and early clinical studies. These therapies, in particular KDs, appear to have a positive impact on the progression of ADPKD, reducing renal cyst sizes and improving kidney function. However, further large-scale clinical studies are needed to confirm these preliminary findings and evaluate their long-term safety and effects on GM. Many studies have focused on overweight or obese patients requiring weight loss, but research is also needed in normal-weight individuals, where either maintaining weight or achieving a minimal weight loss is desirable. It is crucial to carefully formulate KDs to avoid nutritional deficiencies, reduce side effects, prevent the formation of kidney stones, and mitigate the risk of long-term cardiovascular effects. Furthermore, careful medical monitoring of patients and dietitian support to improve adherence during the implementation of these therapies is necessary.
Author Contributions
Conceptualization, C.P., G.B. and R.M.; resources, C.P., G.B. and R.M.; writing—original draft preparation, C.P.; writing—review and editing, C.P., G.B. and R.M.; visualization, C.P.; supervision, G.B. and R.M.; funding acquisition, R.M. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Italian Ministry of Health within the framework of the “Bando della Ricerca Finalizzata 2021”, financial years 2020-2021, Change Promoting” project type, Project No. RF-2021-12374522.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Cordido A, Besada-Cerecedo L, García-González MA. The Genetic and Cellular Basis of Autosomal Dominant Polycystic Kidney Disease—A Primer for Clinicians. Front Pediatr. 2017;5. doi:10.3389/fped.2017.00279. [CrossRef]
- Willey CJ, Blais JD, Hall AK, Krasa HB, Makin AJ, Czerwiec FS. Prevalence of autosomal dominant polycystic kidney disease in the European Union. Nephrology Dialysis Transplantation. 2017;32(8):1356-1363. [CrossRef]
- Solazzo A, Testa F, Giovanella S, et al. The prevalence of autosomal dominant polycystic kidney disease (ADPKD): A meta-analysis of European literature and prevalence evaluation in the Italian province of Modena suggest that ADPKD is a rare and underdiagnosed condition. PLoS One. 2018;13(1):e0190430. [CrossRef]
- Cornec-Le Gall E, Alam A, Perrone RD. Autosomal dominant polycystic kidney disease. The Lancet. 2019;393(10174):919-935. [CrossRef]
- Magistroni R, Boletta A. Defective glycolysis and the use of 2-deoxy-d-glucose in polycystic kidney disease: from animal models to humans. J Nephrol. 2017;30(4):511-519. [CrossRef]
- Astley ME, Boenink R, Abd ElHafeez S, et al. The ERA Registry Annual Report 2020: a summary. Clin Kidney J. 2023;16(8):1330-1354. [CrossRef]
- Torres Vicente E., Chapman Arlene B., Devuyst Olivier, et al. Tolvaptan in Patients with Autosomal Dominant Polycystic Kidney Disease. New England Journal of Medicine. 2012;367(25):2407-2418. [CrossRef]
- Gansevoort RT, Arici M, Benzing T, et al. Recommendations for the use of tolvaptan in autosomal dominant polycystic kidney disease: a position statement on behalf of the ERA-EDTA Working Groups on Inherited Kidney Disorders and European Renal Best Practice. Nephrol Dial Transplant. 2016;31(3):337-348. [CrossRef]
- Padovano V, Podrini C, Boletta A, Caplan MJ. Metabolism and mitochondria in polycystic kidney disease research and therapy. Nat Rev Nephrol. 2018;14(11):678-687. [CrossRef]
- Rowe I, Boletta A. Defective metabolism in polycystic kidney disease: potential for therapy and open questions. Nephrology Dialysis Transplantation. 2014;29(8):1480-1486. [CrossRef]
- Schiliro C, Firestein BL. Mechanisms of Metabolic Reprogramming in Cancer Cells Supporting Enhanced Growth and Proliferation. Cells. 2021;10(5):1056. [CrossRef]
- Vander Heiden MG, Cantley LC, Thompson CB. Understanding the Warburg Effect: The Metabolic Requirements of Cell Proliferation. Science. 2009;324(5930):1029-1033. [CrossRef]
- 13. Kang M, Kang JH, Sim IA, et al. Glucose Deprivation Induces Cancer Cell Death through Failure of ROS Regulation. International Journal of Molecular Sciences. 2023;24(15):11969. [CrossRef]
- Dhillon KK, Gupta S. Biochemistry, Ketogenesis. In: StatPearls. StatPearls Publishing; 2024. Available online: http://www.ncbi.nlm.nih.gov/books/NBK493179/ (accessed on 2 April, 2024).
- Judge A, Dodd MS. Metabolism. Essays in Biochemistry. 2020;64(4):607-647. [CrossRef]
- Masood W, Annamaraju P, Khan Suheb MZ, Uppaluri KR. Ketogenic Diet. In: StatPearls. StatPearls Publishing; 2024. Available online: http://www.ncbi.nlm.nih.gov/books/NBK499830/ (accessed on 2 April, 2024).
- deCampo DM, Kossoff EH. Ketogenic dietary therapies for epilepsy and beyond. Current Opinion in Clinical Nutrition & Metabolic Care. 2019;22(4):264. [CrossRef]
- Galali Y, Zebari SMS, Aj. Jabbar A, Hashm Balaky H, Sadee BA, Hassanzadeh H. The impact of ketogenic diet on some metabolic and non-metabolic diseases: Evidence from human and animal model experiments. Food Sci Nutr. 2024;12(3):1444-1464. [CrossRef]
- Caprio M, Infante M, Moriconi E, et al. Very-low-calorie ketogenic diet (VLCKD) in the management of metabolic diseases: systematic review and consensus statement from the Italian Society of Endocrinology (SIE). J Endocrinol Invest. 2019;42(11):1365-1386. [CrossRef]
- Testa F, Marchiò M, Belli M, et al. A pilot study to evaluate tolerability and safety of a modified Atkins diet in ADPKD patients. PharmaNutrition. 2019;9:100154. [CrossRef]
- Warner G, Hein KZ, Nin V, et al. Food Restriction Ameliorates the Development of Polycystic Kidney Disease. Journal of the American Society of Nephrology. 2016;27(5):1437. [CrossRef]
- Kipp KR, Rezaei M, Lin L, Dewey EC, Weimbs T. A mild reduction of food intake slows disease progression in an orthologous mouse model of polycystic kidney disease. American Journal of Physiology-Renal Physiology. 2016;310(8):F726-F731. [CrossRef]
- Torres JA, Kruger SL, Broderick C, et al. Ketosis Ameliorates Renal Cyst Growth in Polycystic Kidney Disease. Cell Metabolism. 2019;30(6):1007-1023.e5. [CrossRef]
- Shillingford JM, Piontek KB, Germino GG, Weimbs T. Rapamycin ameliorates PKD resulting from conditional inactivation of Pkd1. J Am Soc Nephrol. 2010;21(3):489-497. [CrossRef]
- Weimbs T, Shillingford JM, Torres J, Kruger SL, Bourgeois BC. Emerging targeted strategies for the treatment of autosomal dominant polycystic kidney disease. Clin Kidney J. 2018;11(Suppl 1):i27-i38. [CrossRef]
- Torres JA, Holznecht N, Asplund DA, et al. A combination of β-hydroxybutyrate and citrate ameliorates disease progression in a rat model of polycystic kidney disease. Am J Physiol Renal Physiol. 2024;326(3):F352-F368. [CrossRef]
- Hopp K, Catenacci VA, Dwivedi N, et al. Weight loss and cystic disease progression in autosomal dominant polycystic kidney disease. iScience. 2022;25(1):103697. [CrossRef]
- Strubl S, Oehm S, Torres JA, et al. Ketogenic dietary interventions in autosomal dominant polycystic kidney disease—a retrospective case series study: first insights into feasibility, safety and effects. Clinical Kidney Journal. 2022;15(6):1079-1092. [CrossRef]
- Nowak KL, You Z, Gitomer B, et al. Overweight and Obesity Are Predictors of Progression in Early Autosomal Dominant Polycystic Kidney Disease. J Am Soc Nephrol. 2018;29(2):571-578. [CrossRef]
- Nowak KL, Moretti F, Bussola N, et al. Visceral Adiposity and Progression of ADPKD: A Cohort Study of Patients From the TEMPO 3:4 Trial. American Journal of Kidney Diseases. Published online April 10, 2024. 10 April. [CrossRef]
- Schwingshackl L, Hoffmann G. Comparison of High vs. Normal/Low Protein Diets on Renal Function in Subjects without Chronic Kidney Disease: A Systematic Review and Meta-Analysis. PLoS One. 2014;9(5):e97656. [CrossRef]
- Capelli I, Lerario S, Aiello V, et al. Diet and Physical Activity in Adult Dominant Polycystic Kidney Disease: A Review of the Literature. Nutrients. 2023;15(11):2621. [CrossRef]
- Ikizler TA, Burrowes JD, Byham-Gray LD, et al. KDOQI Clinical Practice Guideline for Nutrition in CKD: 2020 Update. American Journal of Kidney Diseases. 2020;76(3):S1-S107. [CrossRef]
- Acharya P, Acharya C, Thongprayoon C, et al. Incidence and Characteristics of Kidney Stones in Patients on Ketogenic Diet: A Systematic Review and Meta-Analysis. Diseases. 2021;9(2):39. [CrossRef]
- Dyńka D, Kowalcze K, Charuta A, Paziewska A. The Ketogenic Diet and Cardiovascular Diseases. Nutrients. 2023;15(15):3368. [CrossRef]
- Nasser S, Vialichka V, Biesiekierska M, Balcerczyk A, Pirola L. Effects of ketogenic diet and ketone bodies on the cardiovascular system: Concentration matters. World J Diabetes. 2020;11(12):584-595. [CrossRef]
- Pirola L, Ciesielski O, Balcerczyk A. Fat not so bad? The role of ketone bodies and ketogenic diet in the treatment of endothelial dysfunction and hypertension. Biochemical Pharmacology. 2022;206:115346. [CrossRef]
- Popiolek-Kalisz J. Ketogenic diet and cardiovascular risk – state of the art review. Current Problems in Cardiology. 2024;49(3):102402. [CrossRef]
- Joo M, Moon S, Lee YS, Kim MG. Effects of very low-carbohydrate ketogenic diets on lipid profiles in normal-weight (body mass index <25 kg/m2) adults: a meta-analysis. Nutrition Reviews. 2023;81(11):1393-1401. [CrossRef]
- Bruen DM, Kingaard JJ, Munits M, et al. Ren.Nu, a Dietary Program for Individuals with Autosomal-Dominant Polycystic Kidney Disease Implementing a Sustainable, Plant-Focused, Kidney-Safe, Ketogenic Approach with Avoidance of Renal Stressors. Kidney and Dialysis. 2022;2(2):183-203. [CrossRef]
- Oehm S, Steinke K, Schmidt J, et al. RESET-PKD: a pilot trial on short-term ketogenic interventions in autosomal dominant polycystic kidney disease. Nephrology Dialysis Transplantation. 2023;38(7):1623-1635. [CrossRef]
- University of Colorado, Denver. Time Restricted Feeding in Overweight and Obese Adults With Autosomal Dominant Polycystic Kidney Disease. clinicaltrials.gov; 2023. Available online: https://clinicaltrials.gov/study/NCT04534985 (accessed on 1 January, 2024).
- Cukoski S, Lindemann CH, Arjune S, et al. Feasibility and impact of ketogenic dietary interventions in polycystic kidney disease: KETO-ADPKD—a randomized controlled trial. Cell Reports Medicine. 2023;4(11):101283. [CrossRef]
- Testa F, Marchiò M, D’Amico R, et al. GREASE II. A phase II randomized, 12-month, parallel-group, superiority study to evaluate the efficacy of a Modified Atkins Diet in Autosomal Dominant Polycystic Kidney Disease patients. PharmaNutrition. 2020;13:100206. [CrossRef]
- University of Colorado, Denver. Daily Caloric Restriction in Overweight and Obese Adults With ADPKD. clinicaltrials.gov; 2024. Available online: https://clinicaltrials.gov/study/NCT04907799 (accessed on 1 January, 2024).
- Ohio State University. Feasibility and Efficacy of a Well-Formulated Ketogenic Diet in Delaying Progression of Polycystic Kidney Disease in Patients at Risk for Rapid Progression. clinicaltrials.gov; 2024. Available online: https://clinicaltrials.gov/study/NCT06325644 (accessed on 1 January, 2024).
- 8-hour time-restricted eating linked to a 91% higher risk of cardiovascular death. American Heart Association. Accessed May 20, 2024. Available online: http://newsroom.heart.org/news/8-hour-time-restricted-eating-linked-to-a-91-higher-risk-of-cardiovascular-death (accessed on 2 April, 2024).
- Mosterd CM, Kanbay M, Van Den Born BJH, Van Raalte DH, Rampanelli E. Intestinal microbiota and diabetic kidney diseases: the Role of microbiota and derived metabolites inmodulation of renal inflammation and disease progression. Best Practice & Research Clinical Endocrinology & Metabolism. 2021;35(3):101484. [CrossRef]
- Ma L, Zhang L, Li J, et al. The potential mechanism of gut microbiota-microbial metabolites-mitochondrial axis in progression of diabetic kidney disease. Molecular Medicine. 2023;29(1):148. [CrossRef]
- David LA, Maurice CF, Carmody RN, et al. Diet rapidly and reproducibly alters the human gut microbiome. Nature. 2014;505(7484):559-563. [CrossRef]
- Vasileva VY, Sultanova RF, Sudarikova AV, Ilatovskaya DV. Insights Into the Molecular Mechanisms of Polycystic Kidney Diseases. Front Physiol. 2021;12:693130. [CrossRef]
- Cao C, Zhu H, Yao Y, Zeng R. Gut Dysbiosis and Kidney Diseases. Front Med (Lausanne). 2022;9:829349. [CrossRef]
- Li N, Wang Y, Wei P, et al. Causal Effects of Specific Gut Microbiota on Chronic Kidney Diseases and Renal Function—A Two-Sample Mendelian Randomization Study. Nutrients. 2023;15(2):360. [CrossRef]
- Rukavina Mikusic NL, Kouyoumdzian NM, Choi MR. Gut microbiota and chronic kidney disease: evidences and mechanisms that mediate a new communication in the gastrointestinal-renal axis. Pflugers Arch - Eur J Physiol. 2020;472(3):303-320. [CrossRef]
- Caldarelli M, Franza L, Rio P, Gasbarrini A, Gambassi G, Cianci R. Gut–Kidney–Heart: A Novel Trilogy. Biomedicines. 2023;11(11):3063. [CrossRef]
- Evenepoel P, Poesen R, Meijers B. The gut–kidney axis. Pediatr Nephrol. 2017;32(11):2005-2014. [CrossRef]
- Hou K, Wu ZX, Chen XY, et al. Microbiota in health and diseases. Sig Transduct Target Ther. 2022;7(1):1-28. [CrossRef]
- Lambert K, Rinninella E, Biruete A, et al. Targeting the Gut Microbiota in Kidney Disease: The Future in Renal Nutrition and Metabolism. Journal of Renal Nutrition. 2023;33(6):S30-S39. [CrossRef]
- Yacoub R, Nadkarni GN, McSkimming DI, et al. Fecal microbiota analysis of polycystic kidney disease patients according to renal function: A pilot study. Exp Biol Med (Maywood). 2019;244(6):505-513. [CrossRef]
- Wang F, Jiang H, Shi K, Ren Y, Zhang P, Cheng S. Gut bacterial translocation is associated with microinflammation in end-stage renal disease patients. Nephrology (Carlton). 2012;17(8):733-738. [CrossRef]
- Wong J, Piceno YM, DeSantis TZ, Pahl M, Andersen GL, Vaziri ND. Expansion of urease- and uricase-containing, indole- and p-cresol-forming and contraction of short chain fatty acid-producing intestinal microbiota in ESRD. Am J Nephrol. 2014;39(3):230-237. [CrossRef]
- Strubl S, Woestmann F, Todorova P, et al. #395 Gut dysbiosis in ADPKD patients: a controlled pilot study. Nephrology Dialysis Transplantation. 2024;39(Supplement_1):gfae069-0255-0395. [CrossRef]
- Rinninella E, Cintoni M, Raoul P, et al. Food Components and Dietary Habits: Keys for a Healthy Gut Microbiota Composition. Nutrients. 2019;11(10):2393. [CrossRef]
- Walker AW, Ince J, Duncan SH, et al. Dominant and diet-responsive groups of bacteria within the human colonic microbiota. The ISME Journal. 2011;5(2):220-230. [CrossRef]
- Kern L, Kviatcovsky D, He Y, Elinav E. Impact of caloric restriction on the gut microbiota. Current Opinion in Microbiology. 2023;73:102287. [CrossRef]
- Zhang Z, Chen X, Loh YJ, Yang X, Zhang C. The effect of calorie intake, fasting, and dietary composition on metabolic health and gut microbiota in mice. BMC Biology. 2021;19(1):51. [CrossRef]
- Popa AD, Niță O, Gherasim A, et al. A Scoping Review of the Relationship between Intermittent Fasting and the Human Gut Microbiota: Current Knowledge and Future Directions. Nutrients. 2023;15(9):2095. [CrossRef]
- Tagliabue A, Ferraris C, Uggeri F, et al. Short-term impact of a classical ketogenic diet on gut microbiota in GLUT1 Deficiency Syndrome: A 3-month prospective observational study. Clin Nutr ESPEN. 2017;17:33-37. [CrossRef]
- Lindefeldt M, Eng A, Darban H, et al. The ketogenic diet influences taxonomic and functional composition of the gut microbiota in children with severe epilepsy. NPJ Biofilms Microbiomes. 2019;5(1):5. [CrossRef]
- Xie G, Zhou Q, Qiu CZ, et al. Ketogenic diet poses a significant effect on imbalanced gut microbiota in infants with refractory epilepsy. World J Gastroenterol. 2017;23(33):6164-6171. [CrossRef]
- Linsalata M, Russo F, Riezzo G, et al. The Effects of a Very-Low-Calorie Ketogenic Diet on the Intestinal Barrier Integrity and Function in Patients with Obesity: A Pilot Study. Nutrients. 2023;15(11):2561. [CrossRef]
- Attaye I, van Oppenraaij S, Warmbrunn MV, Nieuwdorp M. The Role of the Gut Microbiota on the Beneficial Effects of Ketogenic Diets. Nutrients. 2021;14(1):191. [CrossRef]
Figure 1.
Metabolic Pathways in Normal and Highly Proliferative Cells Under Different Conditions. The image illustrates the different metabolic pathways of normal differentiated cells and highly proliferative cells under three conditions: oxidative phosphorylation - OXPHOS (in the presence of oxygen), anaerobic glycolysis (in the absence of oxygen), and ketosis. In normal cells in the presence of oxygen, glucose is metabolized through glycolysis, producing pyruvate which enters the mitochondria to be converted into acetyl-CoA, initiating the tricarboxylic acid (TCA) cycle and ATP production via oxidative phosphorylation, yielding around 36 molecules of ATP per molecule of glucose. In the absence of oxygen, pyruvate is converted into lactate, yielding around 2 molecules of ATP per molecule of glucose. During ketosis, the scarcity of glucose and the presence of ketone bodies lead to a suppression of glycolysis, with acetyl-CoA derived from ketone bodies entering the TCA cycle to produce around 20 ATP molecules. In contrast, in highly proliferative cells, even in the presence of oxygen, pyruvate is preferentially converted into lactate (aerobic glycolysis or Warburg Effect), which yields much less energy (approximately 4 molecules of ATP per molecule of glucose) compared to OXPHOS. Under ketosis conditions, these cells show suppression of both glycolysis and OXPHOS, highlighting the distinctive metabolic phenotype of highly proliferative cells compared to normal cells. OXPHOS: oxidative phosphorylation; ATP: adenosine triphosphate; Acetyl-CoA: acetyl coenzyme A; TCA: tricarboxylic acid cycle.
Figure 1.
Metabolic Pathways in Normal and Highly Proliferative Cells Under Different Conditions. The image illustrates the different metabolic pathways of normal differentiated cells and highly proliferative cells under three conditions: oxidative phosphorylation - OXPHOS (in the presence of oxygen), anaerobic glycolysis (in the absence of oxygen), and ketosis. In normal cells in the presence of oxygen, glucose is metabolized through glycolysis, producing pyruvate which enters the mitochondria to be converted into acetyl-CoA, initiating the tricarboxylic acid (TCA) cycle and ATP production via oxidative phosphorylation, yielding around 36 molecules of ATP per molecule of glucose. In the absence of oxygen, pyruvate is converted into lactate, yielding around 2 molecules of ATP per molecule of glucose. During ketosis, the scarcity of glucose and the presence of ketone bodies lead to a suppression of glycolysis, with acetyl-CoA derived from ketone bodies entering the TCA cycle to produce around 20 ATP molecules. In contrast, in highly proliferative cells, even in the presence of oxygen, pyruvate is preferentially converted into lactate (aerobic glycolysis or Warburg Effect), which yields much less energy (approximately 4 molecules of ATP per molecule of glucose) compared to OXPHOS. Under ketosis conditions, these cells show suppression of both glycolysis and OXPHOS, highlighting the distinctive metabolic phenotype of highly proliferative cells compared to normal cells. OXPHOS: oxidative phosphorylation; ATP: adenosine triphosphate; Acetyl-CoA: acetyl coenzyme A; TCA: tricarboxylic acid cycle.
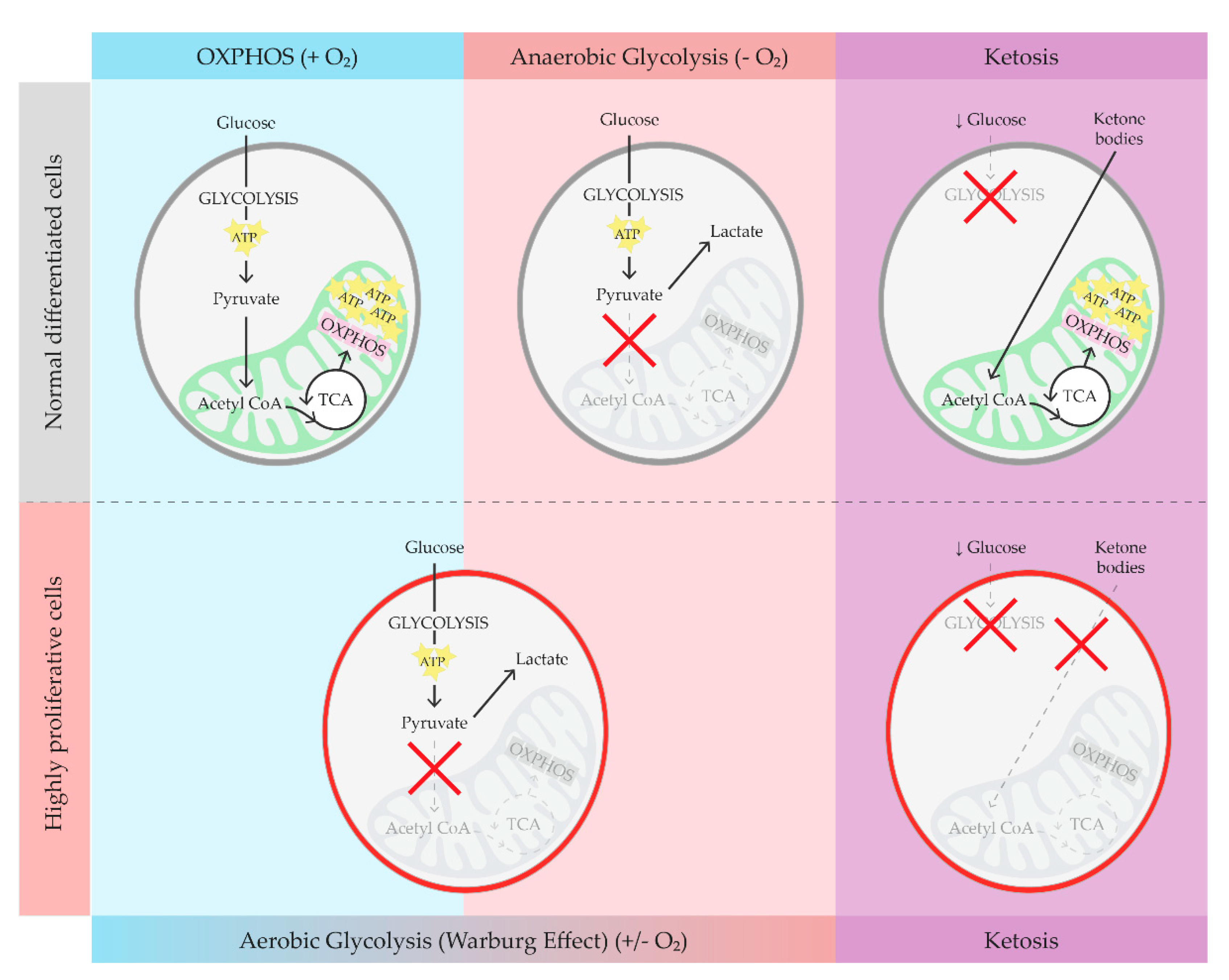

Table 1.
Ketogenic Dietary Interventions.
| KDI | DESCRIPTION | MAIN COMPOSITION | RESEARCH FOCUS | NOTE |
|---|---|---|---|---|
| DCR | Reducing energy intake through DCR while maintaining nutritional adequacy. | Reduced overall calorie intake, balanced macronutrients. | Weight loss, metabolic health. | Requires consistent daily caloric reduction, can be challenging to maintain long-term. |
| IMF | Alternating periods of fasting and eating, aimed at inducing ketosis during fasting periods. | Varied depending on fasting schedule, generally low carbohydrate during eating periods. | Weight loss, metabolic health, improved insulin sensitivity. | Different fasting schedules (e.g., 16/8, 5:2) can be used. |
| TRF | Eating all daily calories within a specific time window each day to promote ketosis during fasting periods. | Low carbohydrate during eating window, balanced macronutrients. | Weight loss, metabolic health, improved circadian rhythm. | Typical windows are 8-12 hours; requires consistency in eating times. |
| cKD | Traditional ketogenic diet with a strict ratio (typically 4:1) of fats to combined carbohydrates and proteins. | High fat (about 90%), low carbohydrate, moderate protein. | Refractory epilepsy, some metabolic disorders. | Requires the use of specifically calculated recipes measured in grams to meet the patient’s needs. |
| MCT | Uses medium-chain triglycerides (MCTs) to enhance ketosis with greater carbohydrate tolerance. | Moderate fat including MCTs, more carbohydrates than cKD. | Refractory epilepsy, some metabolic disorders. | As cKD, requires the use of specifically calculated recipes measured in grams. Allows for greater food variety compared to cKD. |
| MAD | Low carbohydrate, high fat diet, less restrictive than cKD and MCT. | High fat, limited carbohydrates (about 20g per day), moderate protein. | Refractory epilepsy, migraine, weight loss (if low calorie). | Food can be measured using standard household measurements. |
| LGIT | Limits carbohydrates to those with a low glycaemic index to maintain stable blood glucose levels. | Low glycaemic index carbohydrates, moderate protein, moderate fats. | Refractory epilepsy, migraine, weight loss (if low calorie), blood glucose management. | Food can be measured using standard household measurements. |
| VLCKD | Very low-calorie diet primarily designed for weight loss while maintaining ketosis. | Very low in calories, low to moderate fat, low carbohydrate, moderate protein. | Weight loss, obesity. | Used under medical supervision, can have rapid weight loss effects but requires monitoring to avoid nutritional deficiencies. |
cKD: Classic Ketogenic Diet; DCR: Daily Caloric Restriction; IMF: Intermittent Fasting; KDIs: Ketogenic Dietary Interventions; MAD: Modified Atkins Diet; MCT: Medium-Chain Triglyceride Diet; TRF: Time Restricted Feeding; VLCKD: Very Low-Calorie Ketogenic Diet.
Table 2.
Ketogenic Diet Interventions (KDIs) in Autosomal Dominant Polycystic Kidney Disease (ADPKD) ongoing and completed RCTs.
Table 2.
Ketogenic Diet Interventions (KDIs) in Autosomal Dominant Polycystic Kidney Disease (ADPKD) ongoing and completed RCTs.
| Study name | Intervention | Study design | Duration (months) | Patients (n) | Bmi (kg/m^2) | Weight loss | Kidney outcomes |
|---|---|---|---|---|---|---|---|
|
Daily Caloric Restriction and Intermittent Fasting in Overweight and Obese Adults With Autosomal Dominant Polycystic Kidney Disease NCT03342742 (completed) |
DCR and IMF both with similar (~34%) targeted weekly energy deficit | Randomized, parallel assignment, 2 experimental arms, masked (Inv, OA) | 12 | 29 | 25 - 45 | Changes in BW | TKV (MRI) |
|
Time Restricted Feeding in Autosomal Dominant Polycystic Kidney Disease NCT04534985 (completed) |
TRF (8-hr window) and normal healthy eating recommendations | Randomized, parallel assignment, 1 experimental arm, 1 control arm (healthy eating), masked (Inv, OA) | 12 | 29 | 25 - 45 | Changes in BW, abdominal adiposity (MRI), body composition (DEXA) | TKV (MRI) |
|
Ketogenic Dietary Interventions in Autosomal Dominant Polycystic Kidney Disease (ADPKD) NCT04680780 (completed) |
KD (carbohydrate < 30 g/day, 0.8 g/kg BW protein intake) and 3-days WF | Randomized, parallel assignment, 2 experimental arms, 1 control arm (AL diet), no masking | 3 | 63 | 18.6 - 34.9 | Changes in BMI | TKV (MRI), serum creatinine, cystatin C |
|
Daily Caloric Restriction in Overweight and Obese Adults With ADPKD NCT04907799 (recruiting) |
DCR (30%) and increased physical activity | Randomized, parallel assignment, 1 experimental arm, 1 control arm (a single nutrition consultation), masked (Inv, OA) | 24 | 126 | 25 - 45 | Changes in BW, subcutaneous/visceral/total abdominal fat (MRI), % body fat in a sub-set of patients (DEXA) | TKV (MRI) |
|
GREASE II. A phase II randomized, 24-month, parallel-group, superiority study to evaluate the activity of a Modified Atkins Diet in ADPKD patients (recruiting) |
KD (MAD: < 20 g/day of carbohydrates) | Randomized, parallel assignment, 1 experimental arm, 1 control arm (balanced normocaloric diet), masked (Inv, OA) | 24 | 92 | 20 - 30 | BW stability, waist circumference, body composition (BIA), subcutaneous/visceral/total abdominal fat (MRI) | TKV (MRI), serum creatinine, cystatin C |
AL: Ad Libitum; BIA: Bioelectrical Impedance Analysis; BMI: Body Mass Index; BW: Body Weight; DCR: Daily Caloric Restriction; DEXA: Dual-Energy X-ray Absorptiometry; IMF: Intermittent Fasting; Inv: Investigator; KD: Ketogenic Diet; MAD: Modified Atkins Diet; MRI: Magnetic Resonance Imaging; OA: Outcomes Assessor; TKV: Total Kidney Volume; TRF: Time Restricted Feeding; WF: Water Fasting.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



