
Submitted:
09 July 2024
Posted:
11 July 2024
You are already at the latest version
Abstract
Human T-cell lymphotropic virus (HTLV) infection lacks effective treatment. This review describes the virological, immunological and clinical outcomes of antiretroviral therapy (ART) in people with HTLV infection.
This systematic review followed PRISMA reporting guidelines and was registered in PROSPERO: CRD42022350076. The Newcastle-Ottawa Scales, adapted for cross-sectional studies, and Rob-2 were employed to assess the methodological quality of studies. A systematic search was conducted in Medline (PubMed), Scopus (Elsevier), Cochrane Library, and Web of Science (Clarivate Analytics) databases.
We retrieved data from 08 methodologically diverse articles, on treatment of patients infected by HTLV-1 or HTLV-2 alone, or coinfected by HIV-1 with Raltegravir, Tenofovir, Lamivudine and Zidovudine. Proviral load decreased in 3 of 7 studies, during 4 to 48 weeks of antiretrovirals use. Cellular immune response (CD4, CD8, CD25, CD69 and CD71 cells) were evaluated in six studies. There was no significant clinical improvement in the studies but all of them detected clinical stability during treatment.
Despite the demonstrated antiviral activity of ART, in vitro, clinical improvement was not proven. Most studies showed disease stability during ART use, suggesting potential clinical benefits. There is a need of larger, well-controlled trials, to define the role of ART for treatment of HTLV infection.
Keywords:
HTLV
; Antiretroviral
; Treatment
1. Introduction
The Human T-cell Lymphotropic Virus (HTLV) is the second most common retrovirus to infect humans[1]. It can be transmitted through parenteral routes, sexual contact, or vertically from mother to child, similar to HIV[1,2,3]. It is estimated that around 5 to 10 million people are infected worldwide[2] Approximately 10% of the population living with HTLV-1 will develop disease associated with the virus, such as HAM/TSP and ATLL[3]. Unfortunately, there is currently no medication available to control viral replication or prevent transmission.
HTLV-1 infects CD4 and CD8 T lymphocytes, with a preferential tropism for CD4 cells. Its replication is characterized by clonal expansion of infected cells and minimal formation of viral particles for systemic circulation[4]. Replicative activities are modulated by regulatory proteins capable of inducing viral transcription and interfering with host cell’s replicative and repair mechanisms. It is common for HTLV-1 mono-infected or HTLV-1/HIV-1 co-infected patients to have high, dysfunctional, CD4 T cell counts, which may, in the case of coinfection, mask the possible development of opportunistic diseases [5,6]. Therefore, early antiretroviral therapy (ART) is indicated for co-infected patients, even if the CD4 count is elevated, as this would not indicate immunocompetence[7,8].
High proviral load (PVL) of HTLV is one of the main risk factors associated with disease progression[9,10,11]. Studies have shown that individuals with ATL and HAM/TSP, the two most common diseases caused by HTLV, had higher PVL[9,10,11]. Pineda et al.[9] (2019) highlight the importance of other factors such as comorbidities and parasitic infections in lymphocytic clonal expansion, which could consequently lead to an increase in PVL. However, there is no established cutoff reference value of PVL in the literature, as a predictor for the development of diseases or opportunistic manifestations associated with HTLV[9]. Parte superior do formulário
Although HTLV was the first retrovirus to be isolated[11], this infection is considered neglected and still lacks any effective treatment [3]. However, with the evolution of antiretroviral therapy (ART) that targets the replication enzymes present in human retrovirus (proteases, reverse transcriptase, and integrase), studies evaluating the impacts of antiretrovirals use on HTLV infection have been growing. From this perspective, this review aims to describe the results of published studies on the use of ART in HTLV proviral load, as well as clinical and immunological outcomes.
2. Materials and Methods
2.1. Information Sources and Search Strategy
This systematic review was registered with the International Prospective Register of Systematic Reviews (PROSPERO) (registration no. PROSPERO 2022, CRD42022350076).
A comprehensive literature search was performed using the following electronic databases: Medline (PubMed) [229], Scopus (Elsevier) [97], Cochrane Library [3] and Web of Science (Clarivate Analytics) [166]. The search was finalized on 20 July 2022. One article was retrieved from additional literature. No restrictions were placed on the year or location of publication. The search strategies used to obtain the articles are outlined in Table 1.
2.2. Eligibility Criteria
In vivo, studies with humans infected by HTLV, without regard to gender, or ethnicity, and with ART use.
2.3. Exclusion Criteria
Individuals with ATLL, triple non-HIV/HTLV coinfection.
2.4. Main Outcomes
Primary Outcome: Report related changes of proviral load in HTLV 1/2 studies.
Additional outcome(s): Clinical outcomes, count CD4, CD8 and CD4/CD8 ratio, mortality.
2.5. Assessment of Risk of Bias in Included Studies
The risk of bias in the study was rated as “moderate” by using NOS scale, NOS scale adaptation for cross sectional studies, and Rob-2 for clinical trial, obtaining as a mean final score: Moderate (clinical trial), 6.8 (cohort), and 7 (cross sectional).
2.6. Selection of Studies
After using the search strategy described in the methods section, we identified a total of 494 articles, later duplicates were removed (n=77), and reports retrieval (n=1). 417 articles were eligible for title and abstract reading. By using PICO criteria, we selected 19 articles for full-text reading, subsequently additional 11 full-text articles were excluded, and final were considered to this systematic review 8 articles, as presented on the flowchart (Figure1). The types of article design included were clinical trial (n=1), longitudinal prospective cohort (n=2), longitudinal retrospective cohort (n=3), transversal (n=1), and pilot study (n=1).
2.7. Data Extraction and Management
The review will be conducted in accordance with the "Preferred Reporting Items for Systematic Reviews and Meta-analyzes" protocol (PRISMA, http://prisma-statement.org).
The Rayyan Intelligent Systematic Review (https://www.rayyan.ai/) software was used during the screening process; in this step worked three reviewers who selected articles for inclusion as a blinded form. The full texts of any articles identified as being potentially eligible were then retrieved and independently assessed for inclusion/exclusion, this step was worked with Microsoft Excel; disagreements between the reviewers over the eligibility of any particular studies were resolved through discussion with a fourth reviewer. The risk of bias of all included studies was analyzed with The Newcastle-Ottawa Scale (NOS) and Rob2.0 for analysis of clinical trials studies. All the included studies of this review were summarized in Table 2.
3. Results
In this review, we present the data retrieved from 08 articles(12–19). The population of the selected studies was very diverse. Five were HTLV-1 or HTLV-2 mono-infected patients. Two studies were with HIV/HTLV-2 co-infected patients. One study used HTLV-1 mono-infected and HIV/HTLV-1 co-infected. Other characteristics of the studies´ population are available in table 2.
3.1. Antiretroviral Therapy
Most of the selected articles used only one drug: Raltegravir (RAL) (17–19), Tenofovir (TDF) [16] or Lamivudine (3TC) [12]. Taylor et al.,[14] (2006), in their placebo-controlled study, used the combination of Zidovudina (AZT) and 3TC. In two studies, the protocol did not provide data about the ART used, which was at the discretion of the assistant physician (13,15).
3.2. Proviral Load
The quantification of HTLV proviral load (PVL) in the use of ART was analyzed in seven studies [12,14,15,16,17,18,19]; Zeheinder et al.,[13](2002), described LPV in only one patient who developed myelopathy and no significant changes were observed during follow-up. In another study, Taylor et al.,[12] (1999) observed a reduction in PVL in patients who received 3TC (median reduction of 1.1 log10), with a PVL nadir varying from 4 to 24 weeks. Three studies showed no association between PVL and antiretroviral use[14,15,16]. In the study by Treviño et al.,[17] (2012), a transient decline in PVL was observed in the first 6 months of RAL use, followed by a return to baseline values. In addition, Enoose-Akahata et al.,[19] (2021) did not observe significant changes in proviral load with the use of RAL, but when they performed a subgroup analysis, 08 participants with HAM/TSP showed a reduction in PVL in PBMC and 05 participants with HAM/TSP had a reduction in PVL in the CSF after 6 months of ART use, although it did not reach statistical significance. On the other hand, Abad-Fernández et al.,[18] (2014) carried out a generalized estimating equation model for PVL in relation to time and observed a significant decline in this between the period of 24 to 48 weeks in those who received RAL.
3.3. Immunological Outcomes
The immunological status of patients was analyzed in 6 of the 8 articles [13,14,15,16,18,19]. Taylor et al.,[12] (1999) performed analysis of lymphocyte quantification, half-life and phenotype in only one patient. Treviño et al.,[17] (2012) did not evaluate immunological status. Zehender et al.,[13] (2002) identified a lower CD4+ cells count in patients coinfected with HIV/HTLV-2 than in patients monoinfected with HIV-1. Enoose-akahata et al.,[19] (2021) and Taylor et al.,[14] (2006) also observed that individuals on ART tended to have lower lymphocyte counts. On the other hand, Macchi et al.,[16] (2011) observed ain increase in lymphocyte counts following the use of ART, caused by an increase in CD4+ and CD8+ cells count. Abad-Fernández et al.,[18](2014) found no significant variation in CD4+ or CD8+ cells in placebo or in ART group. One study evaluated the CD4+/CD8+ cells ratio and did not detect any statistical difference between groups [19].
3.4. Clinical Outcomes
Clinical outcomes were evaluated in six articles [12,13,14,16,17,19]. Zehender et al.,[18] (2002) observed that the development of peripheral polyneuropathy (PN) was greater in HIV/HTLV-2 co-infected patients and that the use of HAART promoted a reduction in the incidence of this outcome. In articles that evaluated clinical outcomes associated with HTLV-related diseases, Taylor et al.,[12] (1999) found clinical improvement in a patient with HAM/TSP while the proviral load had decreased with the use of 3TC. Macchi et al.,[16] (2011) demonstrated that participants who received TDF for a longer time had improvement in pain and/or gait. Finally, the study by Enose-Akahata et al.,[19](2021), concluded that patients experienced subjective improvement with RAL use, but no significant objective improvements were observed.
4. Discussion
In our review we identified that only two classes of antiretrovirals have already been tested in humans: nucleoside reverse transcriptase inhibitors and integrase inhibitors. AZT began the era of antiretrovirals in HTLV infection [20] and is the only antiretroviral drug used in clinical practice, as an adjuvant treatment of adult T-cell leukemia. Although there is no evidence to support its use in patients monoinfected with HTLV, in 2013 a case report was published on a HIV/HTLV co-infected patient diagnosed with HAM/TSP and who experienced progressive clinical improvement after using combined therapy ( AZT+3TC) [21]. Studies with AZT+3TC or AZT monotherapy in HAM/TSP were designed based on a small sample of participants.
HTLV-1 is considered to be highly resistant to 3TC [22,23]. As a consequence, the use of this antiretroviral for studies with the purpose of evaluating the control of replication of the HTLV virus has been discouraged, despite conflicting results in the literature (22–24). In our review, Taylor et al., [12] (1999) used 3TC as monotherapy and demonstrated a reduction in PVL in relation to baseline levels, despite subsequent oscillation in the participants' PVL, that could be explained by cellular clonal expansion. TDF is another drug already tested in vitro, which has been shown to inhibit HTLV-1 infection (EC50 = 17.78 ± 7.16 nM)[25]. In vitro, AZT and TDF appear to be the most potent nucleoside reverse transcriptase inhibitors against HTLV (TDF: IC50 5.4nmol/L versus AZT: IC50 0.11 µmol/L)[24]. In our review, the study in which patients received TDF showed good drug safety, but no significant reduction in PVL nor clinical improvement [16]
Currently, integrase inhibitors are considered the first line of treatment for HIV because they are safe and effective. Few studies regarding this class of antiretroviral and HTLV have been published to date. An in vitro study demonstrated that RAL can inhibit HTLV transmission, both through cell-free and cell-to-cell mechanisms [26]. Another in vitro study described that second-generation integrase inhibitors and Elvitegravir were superior in inhibiting HTLV when compared to RAL[25]. Despite this, to date only RAL has been studied in human beings and with still conflicting results, which can be justified by the reduced number of participants and observation time[17,18,19]. Dolutegravir (DTG) is the most used integrase inhibitor in the world, however there are no publications involving people infected with HTLV in use of DTG.
Only three out the seven studies analyzed detected a PVL decline between 4 and 48 weeks [14,17,18] and an association between presence of symptoms and higher PVL. Beilke et al.[15] (2007) attributes this PVL increase as a response to immune reconstitution caused by ART use. However, four studies related here [12,16,17,19] reported a PVL variability in both groups over time independent of ART use, a fact already detected in other studies that followed HTLV-1 individuals without ART use [27,28]. Although some researchers considered the PVL increase in HTLV-1 as one of the main risk factors for symptomatic patients, PVL alone cannot determine and predict the progression of the disease, and other factors involved in modulation of immune response may be involved, like the increase in Tax expression and the imbalance between pro - and anti-inflammatory cytokines (IFN-γ and IL-10) [29,30]. Nevertheless, it is likely that proviral load in association with other factors can be a predictor of HTLV -1/2 [31].
The CD4+ cells count in HIV-1/HTLV-2 co-infected participants studied by Zehender et al.,[13] (2002) tended to be lower compared to HIV-1 monoinfected participants, like the data found by Beilke et al.[15] (2007) showing the CD4+ cells count of HIV-1/HTLV-1 patients tended to be higher than those with HIV-1/HTLV-2. The target cells of HTLV-2 infection are TCD8 lymphocytes, which are naturally capable of modulating an immune response to HIV-1 infection and have a higher inhibitory effect on HIV-1 in individuals co-infected by HIV-HTLV-2 than in HIV-1 monoinfected ones[32]. However, this characteristic was not reported among the articles in the review that worked with HTLV-2. Abad-Fernández et al,[18] (2014) were also unable to identify such a large clone expansion in CD4+ and CD8+ cells of HIV-1/HTLV-2 participants in their results. No explanation was given for this finding by the authors.
Taylor et al., [14] (2006) reported an increase in CD4 in the groups that were and were not using the combined therapy of AZT and 3TC, as did Macchi et al.,[16] (2011) who reported an increase in both CD4 and CD8 in patients using TDF. Although antiretrovirals can elicit immune reconstitution, there is still no clarification as to the action of these drugs in monoinfected HTLV-1 patients, nor why the number of these lymphocytes increases or decreases in some groups of patients.
Enose-Akahata [19] (2021) reported that the frequency of TCD4+/CD25+ cells was much higher in PBMC and cerebrospinal fluid samples from patients with HAM/TSP before the start of RAL therapy compared to the same samples collected from healthy participants. However, 15 months after the start of therapy, the frequency of these cells decreased in patients with HAM/TSP, with the same drop seen in TCD8+/CD25+ cells, although only in peripheral blood samples. Other cells profiles were also analyzed, such as T memory lymphocytes and natural killer populations, but without significant changes. CD4+/CD25+ cells are the main reservoirs of the virus and, as they also show high levels of Tax mRNA in the CSF of patients with HAM-TSP, they may be the target of investigations into their possible role as a biomarker of response to antiretroviral drugs [33,34]
In this review, seven studies showed clinical-related results, main of them focused on neurological manifestations such as HAM/TSP, bladder dysfunction, polyneuropathy, functional impairment, and gate. All showed no worsening (clinical stability) during the treatment and follow-up, most of the studies included patients with more than 8 years since the diagnosis of HTLV, the follow-up time ranged from 6 months-10 years, and the n of patients from 4 to 90 patients. The study with the largest number of patients and the longest follow-up[12] showed a transient improvement in one patient during proviral load reduction. No studies reported clinical decline during treatment.
Although the articles included in this review did not show significant clinical improvement, some of them attributed the possibility of no improvement to irreversible nerve damage caused in patients with a long-term medical history [14]. Chronic neuronal dysfunction, both in the central and peripheral nervous systems, leads to cell death and consequent irreversible damage to the nervous system. In the case of infections with known neurotropism, the immune response against infected cells can cause the release of inflammatory cytokines and viral proteins that indirectly damage nervous system cells [35]
The improvement in antiretroviral treatment overtime in people with HIV, was followed by a significant decrease in the incidence rates of dementia, vacuolar myelopathy, polyneuropathy, and myositis [35,36]. By analogy, a population of interest for new studies of HTLV and ART, are patients with recent diagnosis and/or oligosymptomatic patients, given that all studies demonstrated the non-progression of disability, and/or clinical stability during the use of antiretrovirals. Early initiation of antiretroviral therapy could prevent the long-term neuronal damage caused by the infection, minimizing symptoms already present and preventing their progression.
5. Conclusions
Although it has been demonstrated that the use of antiretrovirals inhibits HTLV replication in vitro, the results are still conflicting in clinical practice. Few studies have shown a clear improvement in clinical manifestations and the small sample size and methodological differences between the existing trials limit the understanding of the relevance of ART for treatment of HTLV infection. However, an important finding could be the non-progression of symptoms during the use of antiretrovirals, which was shown in most published studies. Larger, well-controlled trials, with longer follow-up time, are needed to demonstrate the real role of ART for treatment of HTLV infection.
Author Contributions
CB: study design, overview, writing; TF, CSCM, IM-C, and FD: data collection, analysis, writing.
Institutional Review Board Statement
not required.
Conflicts of Interest
Authors declare no conflict of interest regarding this work.
References
- de-Mendoza C, Pérez L, Rando A, Reina G, Aguilera A, Benito R, et al. HTLV-1-associated myelopathy in Spain. Journal of Clinical Virology. 2023 Dec;169:105619. [CrossRef] [PubMed]
- Gessain A, Cassar O. Epidemiological Aspects and World Distribution of HTLV-1 Infection. Front Microbiol. 2012;3. [CrossRef] [PubMed]
- Eusebio-Ponce E, Anguita E, Paulino-Ramirez R, Candel FJ. HTLV-1 infection: an emerging risk. Pathogenesis, epidemiology, diagnosis and associated diseases. Revista Española de Quimioterapia. 2019;32(6):485–95.
- Zane L, David Sibon, Franck Mortreux, Eric Wattel. Clonal expansion of HTLV-1 infected cells depends on the CD4 versus CD8 phenotype. Frontiers in Bioscience. 2009;Volume(14):3935.
- Beilke MA, Theall KP, Megan O, Clayton JL, Benjamin SM, Winsor EL, et al. Clinical Outcomes and Disease Progression among Patients Coinfected with HIV and Human T Lymphotropic Virus Types 1 and 2. Clinical Infectious Diseases. 2004 Jul 15;39(2):256–63. [CrossRef]
- Vandormael A, Rego F, Danaviah S, Carlos Junior Alcantara L, Boulware D, de Oliveira T. CD4+ T-cell Count may not be a Useful Strategy to Monitor Antiretroviral Therapy Response in HTLV-1/HIV Co-infected Patients. Curr HIV Res. 2017 Jul 3;15(3).
- Ticona E, Huaman MA., Yanque O, Zunt JR. HIV and HTLV-1 Coinfection: The Need to Initiate Antiretroviral Therapy. Journal of the International Association of Providers of AIDS Care (JIAPAC). 2013 Nov 12;12(6):373–4. [CrossRef] [PubMed]
- Montaño-Castellón I, Marconi C, Saffe C, Brites C. Clinical and Laboratory Outcomes in HIV-1 and HTLV-1/2 Coinfection: A Systematic Review. Front Public Health. 2022 Mar 7;10. [CrossRef] [PubMed]
- Pineda MV, Bouzas MB, Remesar M, Fridman A, Remondegui C, Mammana L, et al. Relevance of HTLV-1 proviral load in asymptomatic and symptomatic patients living in endemic and non-endemic areas of Argentina. PLoS One. 2019 Nov 22;14(11).
- Akbarin MM, Rahimi H, Hassannia T, Shoja Razavi G, Sabet F, Shirdel A. Comparison of HTLV-I Proviral Load in Adult T Cell Leukemia/Lymphoma (ATL), HTLV-I-Associated Myelopathy (HAM-TSP) and Healthy Carriers. Iran J Basic Med Sci. 2013 Mar;16(3):208–12.
- Olindo S, Lézin A, Cabre P, Merle H, Saint-Vil M, Edimonana Kaptue M, et al. HTLV-1 proviral load in peripheral blood mononuclear cells quantified in 100 HAM/TSP patients: A marker of disease progression. J Neurol Sci. 2005 Oct;237(1–2):53–9. [CrossRef]
- Taylor GP, Hall SE, Navarrete S, Michie CA, Davis R, Witkover AD, et al. Effect of Lamivudine on Human T-Cell Leukemia Virus Type 1 (HTLV-1) DNA Copy Number, T-Cell Phenotype, and Anti-Tax Cytotoxic T-Cell Frequency in Patients with HTLV-1-Associated Myelopathy. J Virol. 1999 Dec;73(12):10289–95. [CrossRef]
- Zehender G, Colasante C, Santambrogio S, De Maddalena C, Massetto B, Cavalli B, et al. Increased Risk of Developing Peripheral Neuropathy in Patients Coinfected With HIV-1 and HTLV-2. JAIDS Journal of Acquired Immune Deficiency Syndromes. 2002 Dec;31(4):440–7. [CrossRef] [PubMed]
- Taylor GP, Goon P, Furukawa Y, Green H, Barfield A, Mosley A, et al. Zidovudine plus lamivudine in Human T-Lymphotropic Virus type-I-associated myelopathy: a randomised trial. Retrovirology. 2006 Dec 19;3.
- Beilke MA, Dorge VLT, Sirois M, Bhuiyan A, Murphy EL, Walls JM, et al. Relationship between Human T Lymphotropic Virus (HTLV) Type 1/2 Viral Burden and Clinical and Treatment Parameters among Patients with HIV Type 1 and HTLV-1/2 Coinfection. Clinical Infectious Diseases. 2007 May 1;44(9):1229–34. [CrossRef] [PubMed]
- Macchi B, Balestrieri E, Ascolani A, Hilburn S, Martin F, Mastino A, et al. Susceptibility of Primary HTLV-1 Isolates from Patients with HTLV-1-Associated Myelopathy to Reverse Transcriptase Inhibitors. Viruses. 2011 May 5;3(5):469–83. [CrossRef] [PubMed]
- Trevino A, Parra P, Bar-Magen T, Garrido C, de Mendoza C, Soriano V. Antiviral effect of raltegravir on HTLV-1 carriers. Journal of Antimicrobial Chemotherapy. 2012 Jan 1;67(1):218–21. [CrossRef] [PubMed]
- Abad-Fernández M, Cabrera C, García E, Vallejo A. Transient increment of HTLV-2 proviral load in HIV-1-co-infected patients during treatment intensification with raltegravir. Journal of Clinical Virology. 2014;59(3):204–7. [CrossRef] [PubMed]
- Enose-Akahata Y, Billioux BJ, Azodi S, Dwyer J, Vellucci A, Ngouth N, et al. Clinical trial of raltegravir, an integrase inhibitor, in HAM/TSP. Ann Clin Transl Neurol. 2021 Oct 25;8(10):1970–85. [CrossRef] [PubMed]
- Marino-Merlo F, Balestrieri E, Matteucci C, Mastino A, Grelli S, Macchi B. Antiretroviral Therapy in HTLV-1 Infection: An Updated Overview. Pathogens. 2020 May 1;9(5):342. [CrossRef] [PubMed]
- Hassan S, Amer S, Zervos M. Tropical spastic paraparesis treated with Combivir (lamivudine–zidovudine). Journal of Clinical Neuroscience. 2013 May;20(5):759–60. [CrossRef]
- Balestrieri E, Forte G, Matteucci C, Mastino A, Macchi B. Effect of Lamivudine on Transmission of Human T-Cell Lymphotropic Virus Type 1 to Adult Peripheral Blood Mononuclear Cells In Vitro. Antimicrob Agents Chemother. 2002 Sep;46(9):3080–3. [CrossRef]
- García-Lerma J, Nidtha S, Heneine W. Susceptibility of Human T Cell Leukemia Virus Type 1 to Reverse-Transcriptase Inhibitors: Evidence for Resistance to Lamivudine. J Infect Dis. 2001 Aug 15;184(4):507–10. [CrossRef]
- Hill SA, Lloyd PA, McDonald S, Wykoff J, Derse D. Susceptibility of Human T Cell Leukemia Virus Type I to Nucleoside Reverse Transcriptase Inhibitors. J Infect Dis. 2003 Aug;188(3):424–7. [CrossRef] [PubMed]
- Barski M, Minnell J, Maertens G. Inhibition of HTLV-1 Infection by HIV-1 First- and Second-Generation Integrase Strand Transfer Inhibitors. Front Microbiol. 2019 Aug 13;10.
- Seegulam M, Ratner L. Integrase Inhibitors Effective against Human T-Cell Leukemia Virus Type 1. Antimicrob Agents Chemother. 2011 May;55(5):2011–7. [CrossRef] [PubMed]
- Demontis M, Hilburn S, Taylor G. Human T Cell Lymphotropic Virus Type 1 Viral Load Variability and Long-Term Trends in Asymptomatic Carriers and in Patients with Human T Cell Lymphotropic Virus Type 1-Related Diseases. AIDS Res Hum Retroviruses. 2013 Feb;29(2):359–64. [CrossRef]
- Matsuzaki T, Nakagawa M, Nagai M, Usuku K, Higuchi I, Arimura K, et al. HTLV-I proviral load correlates with progression of motor disability in HAM/TSP: Analysis of 239 HAM/TSP patients including 64 patients followed up for 10 years. J Neurovirol. 2001 Jan;7(3):228–34. [CrossRef]
- Ferraz S, Costa G, Carneiro Neto J, Hebert T, de Oliveira C, Guerra M, et al. Neurologic, clinical, and immunologic features in a cohort of HTLV-1 carriers with high proviral loads. J Neurovirol. 2020 Aug;26(4):520–9. [CrossRef]
- Tarokhian H, Taghadosi M, Rafatpanah H, Rajaei T, Azarpazhooh MR, Valizadeh N, et al. The effect of HTLV-1 virulence factors (HBZ, Tax, proviral load), HLA class I and plasma neopterin on manifestation of HTLV-1 associated myelopathy tropical spastic paraparesis. Virus Res. 2017 Jan;228:1–6. [CrossRef] [PubMed]
- Saffari M, Rahimzada M, Mirhosseini A, Ghezaldasht SA, Valizadeh N, Moshfegh M, et al. Coevolution of HTLV-1-HBZ, Tax, and proviral load with host IRF-1 and CCNA-2 in HAM/TSP patients. Infection, Genetics and Evolution. 2022 Sep;103.
- Abad-Fernández M, Hernández-Walias FJ, Ruiz de León MJ, Vivancos MJ, Pérez-Elías MJ, Moreno A, et al. HTLV-2 Enhances CD8+ T Cell-Mediated HIV-1 Inhibition and Reduces HIV-1 Integrated Proviral Load in People Living with HIV-1. Viruses. 2022 Nov 9;14(11).
- Matavele Chissumba R, Silva-Barbosa SD, Augusto Â, Maueia C, Mabunda N, Gudo ES, et al. CD4+CD25High Treg cells in HIV/HTLV Co-infected patients with neuropathy: high expression of Alpha4 integrin and lower expression of Foxp3 transcription factor. BMC Immunol. 2015 Sep 2;16.
- Yamano Y, Takenouchi N, Li H, Tomaru U, Yao K, Grant CW, et al. Virus-induced dysfunction of CD4+CD25+ T cells in patients with HTLV-I–associated neuroimmunological disease. Journal of Clinical Investigation. 2005 May 2;115(5):1361–8. [CrossRef]
- Wouk J, Rechenchoski DZ, Rodrigues BCD, Ribelato EV, Faccin-Galhardi LC. Viral infections and their relationship to neurological disorders. Arch Virol. 2021 Mar 27;166(3):733–53. [CrossRef]
- Paruk HF, Bhigjee AI. Review of the neurological aspects of HIV infection. J Neurol Sci. 2021 Jun;425. [CrossRef] [PubMed]
Figure 1.
PRISMA 2020 Structured search strategy flow diagram.
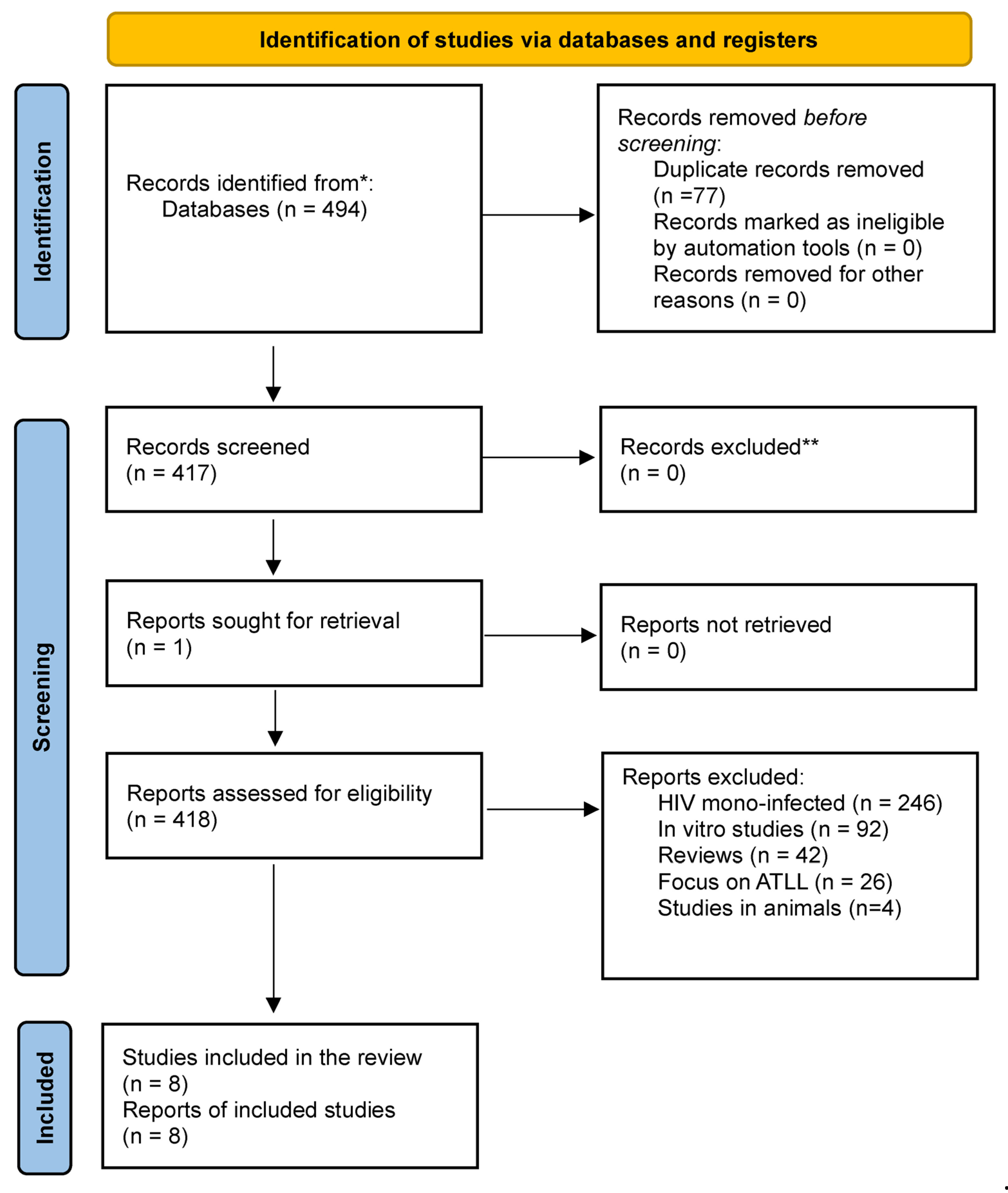

Table 1.
Databases accessed with corresponding search strategies.
| Database (company) | Keywords (MeSH) term and text word search | |
|---|---|---|
| 1 | Medline (PubMed) | ("Human T-lymphotropic virus 1"[Mesh] OR "HTLV-I Infections"[Mesh] OR "HTLV-II Infections"[Mesh] OR "HTLV-1"[tiab] OR "HTLV-2"[tiab] OR "HTLV-I"[tiab] OR "HTLV-II"[tiab] OR "HTLV"[tiab]) AND ("Anti-Retroviral Agents" OR "dolutegravir" OR "raltegravir" OR "Isentress" OR "elvitegravir" OR "bictegravir" OR "zidovudine" OR "efavirenz") NOT ("ATL") |
| 2 | Cochrane Library | ( "HTLV" OR " Human T-lymphotropic virus 1" OR "HTLV-I Infections" OR "HTLV-II Infections" OR "HTLV-1" OR "HTLV-2" OR "HTLV-I" OR "HTLV-II" ) AND (“Anti-HIV Agents” OR ‘HIV Protease inhibitors” OR “HIV Integrase Inhibitors” OR “Anti-Retroviral Agents” OR “HIV/drug effects” OR “”Drug Ressistance”) NOT ("ATL") |
| 3 | Scopus (Elsevier) | ( ( ALL ( "HTLV" OR " Human T-lymphotropic virus 1" OR "HTLV-I Infections" OR "HTLV-II Infections" OR "HTLV-1" OR "HTLV-2" OR "HTLV-I" OR "HTLV-II" ) ) AND ( ALL ("Paraparesis, Tropical Spastic" OR "HAM/TSP" OR "Paraparesis, Tropical Spastic/therapy" ) OR TITLE-ABS-KEY ( "Paraparesis, Tropical Spastic" OR "HAM/TSP" ) ) ) AND ( ALL ( "Anti-HIV Agents" OR "dolutegravir" OR "raltegravir" OR "Anti-Retroviral Agents" OR "elvitegravir" OR "bictegravir" OR "zidovudine" OR "efavirenz" ) NOT ALL("ATL") ) |
| 4 | Web of Science (Clarivate Analytics) | ALL=("HTLV" OR " Human T-lymphotropic virus 1" OR "HTLV-I Infections" OR "HTLV-II Infections" OR "HTLV-1" OR "HTLV-2" OR "HTLV-I" OR "HTLV-II") AND ALL=("Anti-Retroviral Agents" OR "dolutegravir" OR "raltegravir" OR "Isentress" OR "elvitegravir" OR "bictegravir" OR "zidovudine" OR "efavirenz") NOT ALL=("ATL") |
Table 2.
Summary of studies included in this review.
| Study | design, Country | Population Characteristic | Infection | ART use | Outcomes |
|---|---|---|---|---|---|
| Taylor et al., 1999[12] | Cohort, United Kingdon | N=5; female: 4(80%); mean age: 46,6 | HTLV-1 with HAM/TSP: 5 (100%) | 3TC* *A patient who had a recent diagnosis of HAM/TSP received AZT for 3 months and then switched to 3TC |
HTLV- PVL reduced in all patients. Clinical improvement was only observed in one patient with recent onset HAM/TSP during the period in which lamivudine reduced PVL. |
| Zehender et al, 2002 [13] | Retrospective cohort, Italy | N = 90; male: 80%; mean age HIV group: 32 (26-50) mean age HIV/HTLV-2 group: 33 (23-55). |
HIV/HTLV-2: 30 (33,3%) HIV: 60 (66,6%). |
It was not controlled by the study protocol | There was no difference between the monoinfected and coinfected groups for mortality and CD4+ cells count. HLTV-2 infection was an independent predictor for developing PN, during ART PN incidence considerably decreased |
| Taylor et al., 2006 [14] | RCT, United Kingdon | N=16, male: 5 (31%); mean age: 57,4 | HTLV-1 with HAM/TSP: 16 (100%) | AZT + 3TC | There was a tendency for to decreasing CD8+ cells count with the use of ART. There was no significant change in PVL and CD4+ cells count. No significant changes in pain score, urinary frequency or nocturia. A patient with recent-onset HAM/TSP, had an improvement which persisted only during the period of ART use. |
| Beilke et al., 2007 [15] | Cross-section, USA | N=72, male: 59 (76%) Age: >45 years (72%) | HIV/HTLV-1: 20 (27,7%) HIV/HTLV-2: 52 (72,3%) |
Any triple ART | Participants' PVL were higher in HIV/HTLV-1 than in HIV/HTLV-2 and in cases with positive PBMC cultures. |
| Macchi et al., 2011 [16] | Cohort, United Kingdon | N=5 Female: 4(80%); mean age: 44.8 (±15) | HTLV-1 with HAM/TSP: 5 (100%) | TDF | There was an increase in CD4 and CD8+ cells count. No significant clinical improvement was seen, except in those who received TDF for a longer period of time and experienced improvement in pain and gait. There was no significant change in PVL |
| Treviño et al., 2012[17] | Pilot study, Spain | N=5; Female: 3 (60%); median age: 52 | HTLV-1 without HAM/TSP: 2(40%) HTLV-1 with HAM/TSP: 2 (40%) HIV/HTLV-1: 1(20%) |
RAL | There was a transient reduction in PVL in the two symptomatic patients. No clinical improvements were observed. |
| Abad-Fernandez et al., 2014 [18] | Cohort, Spain | RAL group: N=4; male:4(26,6%); median age: 51(48-54). Control group: N=11(73,4), median age: 50 (46-56) |
HIV/HTLV-2: 15 (100%) | Intervention: ART with RAL Control: ART whitout RAL |
There was an initial increase followed by a reduction in PVL in the RAL group. This was not observed in the control group. There were no changes in CD4 and CD8+ cells count in both groups |
| Enose-Akahata et al., 2021 [19] | Clinical trail, USA? | RAL group: N=16 (28,6%); famale: 10(62,5%); mean age: 53,5 Control group: HAM/TSP: N=13(23,2%) People without infection: N=27(48,2) age and gender not described |
HTLV-1 with HAM/TSP:29 (51,8%) People without infection: 27 (48,2%) |
Intervention:ART with RAL Control group: without ART |
There was a subjective improvement in symptoms with the use of RAL, but not in objective clinical measurements. PVL in CSF and PBMC remained stable throughout the study. There was a reduction in CD4 and CD8 in peripheral blood after using RAL. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



