
Submitted:
09 July 2024
Posted:
10 July 2024
You are already at the latest version
Abstract
The macular pigment optical density (MPOD) signifies a vital component of macular well-being and high-resolution visual acuity. MPOD can serve as a reliable biomarker for assessing the retinal defense mechanisms against oxidative stress and the deleterious effects of excessive light exposure. Elevated MPOD levels offer robust protection against the onset and progression of age-related macular degeneration (AMD) a prevalent cause of vision impairment among the elderly population. MPOD's implications in diverse ocular conditions, including diabetic retinopathy and glaucoma, have been explored and indicate a real need for clinical measurement of MPOD. This review looks at the potential of MPOD as a modifiable biomarker influencing the progression and onset of these conditions, particularly in the context of oxidative stress and retinal ischemia. The integration of MPOD measurement into routine eye examinations presents an unparalleled opportunity for early disease detection, precise treatment planning, and longitudinal disease monitoring. Emerging technologies and longitudinal investigations promise to elucidate the dynamic nuances of MPOD in the context of age-related ocular diseases.
Keywords:
MPOD
; lutein
; zeaxanthin
; biomarker
; glaucoma
; diabetic retinopathy
1. Introduction
1.1. Structure:
The macular pigment, a yellowish deposit in the central retina, arises from the collective presence of carotenoid pigments strategically accumulated within the macular region [1]. These pigments exhibit distinct absorption spectra, aiding their identification and quantification [2]. Lutein, zeaxanthin, and meso-zeaxanthin compromise the macular pigment [2,3]. Lutein, a xanthophyll carotenoid, is known for its antioxidant abilities and light-filtering properties. Zeaxanthin, a close relative, exhibits similar characteristics and is particularly enriched in the central foveal region of the macula [4]. Meso-zeaxanthin, although structurally akin to zeaxanthin, is found in extremely lower quantities if any from dietary sources but is synthesized from lutein in the retina [1]. This interconversion of lutein to meso-zeaxanthin may be especially advantageous for diets that are dominated by lutein rich sources [1]. Notably however, this conversion is not shown in other locations particularly meso-zeaxanthin is starkly absent in brain [5]. Collectively, these pigments bolster ocular defense mechanisms by using reactive oxygen species and absorbing blue light, thereby protecting against oxidative stress and potential retinal damage [6].
1.2. Nutrition:
The journey of these pigments into the retina begins with dietary intake. Rich sources of lutein and zeaxanthin (L/Z) include leafy green vegetables such as spinach, kale, and collard greens, along with other vibrant fruits and vegetables [3]. However, meso-zeaxanthin's primary origin lies within the retina, where it is synthesized from lutein, as it is not commonly found in substantial quantities within typical diets [1]. The intricate interplay between dietary intake, transport, and metabolism influences the availability of these carotenoids for ocular uptake. Bioavailability studies reveal that factors such as food matrix, cooking methods, and individual genetics can affect the extent to which these carotenoids are absorbed and utilized by the body [7,8,9,10].
To better understand the effects of L/Z intake on the macular pigment density, it is important to know about the dietary sources of L/Z. In the past, nutritional analysis has reported L/Z as one value as analytical procedures had not permitted for the evaluation of them separately. Perry et al., have conducted testing to determine their individual quantities in food [11]. Given that L/Z accumulates in different regions of the retina and that they serve different functions it is important to assess their individual quantity [4,12,13]. As seen in Table 1, there is a stark difference in the foods that contain L/Z, with most foods containing lutein but not zeaxanthin. This in part explains why dietary intake in the standard American diet is lower in zeaxanthin and higher in lutein, despite there being a higher level of zeaxanthin in the central fovea thus emphasizing its importance in health maintenance of the eye.
The bioavailability of carotenoids has been shown to be significantly increased when consumed with foods containing fat [7,8]. Despite eggs having a lower L/Z content, their fat content allows them to significantly increase L/Z levels. A study by Goodrow et al. showed that consuming one egg per day over five weeks increased plasma levels of lutein by 26% and zeaxanthin by 38% [14]. It has also been shown that the bioavailability of carotenoids decreases due to competition for absorption when different carotenoids are consumed in the same meal [10,15]. Heat plays an interesting role as it has been shown to decrease carotenoid content but significantly increases carotenoid bioavailability [8]. Dietary fiber has been shown to have a negative effect on the absorption of carotenoids as seen in Riedl et al. with a 40-74% decrease in plasma levels of lutein when these carotenoids were consumed with water soluble fibers such as pectin, guar, and alginate [10].
2.1. Macular Pigment Optical Density (MPOD):
The carotenoids lutein, zeaxanthin and meso-zeaxanthin form the macular pigment. Macular pigment’s optical density (MPOD) is an assessment of the strength of the presence of these carotenoids in an individual. This metric can be measured clinically, and it can be used as a clinical biomarker for ocular disease, ocular performance, and effects of systemic disease. If the macular pigment were to be used as a clinical biomarker it would be imperative to be able to obtain accurate and consistent measurements of a patients MPOD.
2.2. Measurement of MPOD:
There are several techniques to measure MPOD levels. These techniques can be split into psychophysical vs objective techniques, each with their pros and cons. Psychophysical techniques include methods like Heterochromatic Flicker Photometry (HFP) and Minimum Notion Photometry (MNP). These techniques gauge macular pigment density by exploiting visual perception phenomena in response to specific stimulus conditions. While psychophysical methods offer insights into pigment distribution, they may be affected by individual variations in visual perception. Objective techniques include methods such as Fundus Reflectometry (FR), Fundus Autofluorescence (FAF) and Resonance Raman Spectroscopy (RRS).
Heterochromatic Flicker Photometry (HFP) is the most widely used psychophysical method that relies on color sensitivity modulation. It involves presenting a flickering stimulus comprising two lights with different wavelengths. By varying the intensity of one light, the point at which the flicker disappears is indicative of the macular pigment's absorption [16,17]. Its advantages include directly measuring overall macular pigment density, non-invasiveness, and relative simplicity to perform, as demonstrated by a large body of research [17].
Fundus Reflectometry (FR) is an objective technique that measures the amount of light reflected from the fundus. Light that is reflected from a part of the retina is compared to light reflected from the fovea. Because the fovea absorbs certain wavelengths of light at different wavelengths compared to the retina, the difference in reflected light can be used to determine the MPOD [18,19]. Studies have compared the widely used technique of HFP to FR and found that there was a significant correlation between these techniques, indicating FR as an objective, accurate, and reliable measurement tool for MPOD [12,13,20].
Resonance Raman Spectroscopy (RRS) is a technique that leverages the resonance Raman scattering properties of the macular pigments to assess their concentrations [21]. Laser light of specific wavelengths is directed at the retina causing the pigments to resonate and emit scattered light with altered frequencies [22]. By measuring this altered light, the density of pigments can be quantified [22]. While resonance Raman spectroscopy offers excellent sensitivity to changes in pigment density and allows for precise spatial mapping of MPOD, its complexity and dependence on sensitive, specialized, expensive equipment can pose challenges.
Fundus Autofluorescence (FAF) capitalizes on the phenomenon of autofluorescence exhibited by macular pigments. Pigments, when exposed to specific wavelengths of light, emit light of a longer wavelength [23]. FAF captures this emitted light and uses it as a surrogate marker for macular pigment density [23]. This technique is non-invasive and can be integrated into routine clinical examinations. However, the accuracy of the measurement is limited by variations in autofluorescence across individuals and by factors like aging and retinal health [19]. Davey et al. examined the precision and inter-eye-correlation of MPOD, finding that measurements using HFP had excellent short-term repeatability, and that the MPOD value of one eye could predict the value of the fellow eye with 89% accuracy [24]. MPOD, however, was not correlated with ocular dominance [24].
3.1. MPOD in Ocular and Systemic Disease:
Understanding the intricate relationship between MPOD and various aspects of eye health is paramount for deciphering the potential impact of pigment density on ocular diseases and conditions. This section delves into the multifaceted connection between MPOD and ocular health exploring its protective role against AMD, its potential as a biomarker for AMD risk assessment and progression, and its influence on other ocular conditions such as diabetic retinopathy and glaucoma. Figure 1 illustrates how environmental and disease processes interact to increase or decrease MPOD, demonstrating how MPOD can be used as a clinical biomarker for many ocular and systemic conditions.
3.2. MPOD and Age-Related Macular Degeneration
Age-related macular degeneration (AMD), a leading cause of irreversible vision loss in older adults, underscores the importance of exploring potential protective factors [25]. Early signs of AMD are present in a quarter of the population older than 65, increasing the risk of developing late AMD [26]. Late AMD is the stage of AMD that affects vision and 7% of individuals over 75 years old will develop late AMD over the next 10 years of their life [26]. Modern medical interventions include anti-VEGF monoclonal antibodies and photodynamic therapy. These medical treatments present limitations in delaying and reversing the retinal changes seen in late AMD and are considered invasive by many patients, which can significantly affect patient compliance. No cure is currently present and this, along with the widespread prevalence of AMD, is why it is a leading cause of irreversible blindness [25]. MPOD emerges as a potential guardian against the onset and progression of AMD. Macular pigments, which encompass L/Z, exhibit powerful antioxidant properties that counteract the detrimental effects of oxidative stress and inflammation in the retina [6,27]. By scavenging free radicals and mitigating cellular damage, MPOD contributes to retinal health and reduces the risk of AMD development [6]. Higher MPOD levels are correlated with a decreased risk of both early and late-stage AMD, highlighting the potential of these pigments in preserving visual function [27,28].
The significance of MPOD transcends its protective role, extending to its potential as a biomarker for AMD risk assessment and progression. Lower MPOD levels have been associated with an increased likelihood of late AMD development, serving as an early indicator of susceptibility to the disease. Supplementation with lutein/zeaxanthin has been shown to increase MPOD and lower the progression of patients with wet AMD to the late stages of the disease [29]. It is important to note that people diagnosed with AMD have consistently been found to have lower MPOD [30,31,32]. Bone et al. examined donor eyes of individuals with and without AMD, finding lower concentrations of L/Z in individuals with AMD [33]. Monitoring MPOD over time may provide valuable insights into disease progression by aiding in identifying individuals who may be at higher risk of transitioning to advanced stages of AMD. Tsika et al. showed a significantly higher MPOD in the fellow eyes of patients with wet AMD, with no difference in the fellow eyes of patients with dry AMD [32]. Integrating MPOD measurements into routine clinical assessments can enhance AMD risk stratification, enabling proactive interventions and personalized management strategies. Table 2 below summarizes the findings of the randomized control trial and observational cross-sectional studies that have examined the relationship between MPOD and AMD, supporting the idea of using MPOD as a clinical biomarker of progression in AMD.
3.3. Glaucoma
Glaucoma is the world’s leading cause of irreversible blindness. Glaucoma is characterized by progressive degeneration of the optic nerve head, permanent damage to the retinal nerve fiber layer, and loss of retinal ganglion cells [45]. It results in vision loss that begins peripherally and moves centrally through the course of the disease [45]. In addition to elevated IOP, retinal ischemia, oxidative stress, and damage from ischemia-reperfusion, have been proposed as major factors causing retinal ganglion cell death [46]. It has been well established that increased macular pigment density aids in stopping the progression of AMD through potentially anti-oxidative effects [6]. This raises questions regarding the role of the macular pigment in mitigating the oxidative damage seen in glaucoma.
One study injected lutein into a transient ischemia model of high IOP in rats [47]. Rats injected with lutein showed significantly decreased levels of oxidative markers and decreased ischemia-induced retinal cell death compared to controls [47,48]. Research has demonstrated that administering lutein through intravitreal injections to rats suffering from ischemia-reperfusion injuries led to a significant reduction in oxidative markers, an increase in anti-oxidative markers, and a significant decrease in retinal ganglion cell death [49,50]. Müller cells fulfill a dual role by offering homeostatic and metabolic support to retinal neurons while also serving as key mediators of inflammation within the retina [51,52]. A Cross-sectional analysis assessed the MPOD of patients with glaucomatous eyes and found that MPOD was lower in eyes that had a thinner ganglion cell complex, a thinner retinal nerve fiber layer, and an increased cup-to-disc ratio, ultimately indicating a correlation between MPOD and glaucoma severity [53]. Studies have primarily focused on assessing the impact of MPOD and L/Z concentration in animal models, yielding promising results [47,48,49,50]. A recent review paper has suggested that carotenoid vitamin therapy provides synergic neuroprotective benefits and has the capacity to serve as adjunctive therapy in the management of glaucoma [54]. However, further research involving human subjects is essential to understand the mechanism and explore the potential anti-oxidative effects, particularly in the context of a high oxidation disease like glaucoma. Table 3 below summarizes the findings of the randomized control trial and observational cross-sectional studies that have examined the relationship between MPOD and glaucoma supporting the idea of using MPOD as a clinical biomarker of progression in glaucoma.
3.4. Systemic Disease
The assessment of MPOD could be used to gauge the risk of developing ocular and/or systemic disease. At the same time, maintenance or enhancement of MPOD could prevent the onset or advancement of associated co-morbidities. The theorized pathogenic mechanisms and metabolic co-morbidities to explain the lower MP levels reported in diabetes include a process of increased oxidative stress, inflammation, hyperglycemia, insulin resistance or deficiency, obesity, dyslipidemia, and vascular dysfunction/neovascularization [65,66]. In addition to possibly depleting potent antioxidants, such as macular carotenoids lutein, zeaxanthin, and meso-zeaxanthin that are pertinent for retinal protection, these factors may have related and/or independent relationships with MP that warrant further study [65,66]. A significant inverse correlation between MPOD and HbA1C was found and decreased MPOD is evident in type II diabetes with or without retinopathy [67]. Currently, there is robust evidence and early clinical trials supporting the use of carotenoid vitamin supplementation in diabetics with and without retinopathy. A trial on mice demonstrated promising effects on the prevention of diabetic retinopathy with MPOD-bolstering supplements; by reducing apoptosis of retinal ganglion cells, astaxanthin may prevent oxidative stress from causing retinal neurodegeneration [68]. Table 4 below summarizes the findings of the randomized control trial and observational cross-sectional studies that have examined the relationship between MPOD and diabetes, supporting the idea of using MPOD as a clinical biomarker of progression in diabetes and diabetic retinopathy.
3.4.1. Diabetic Retinopathy
Retinopathy is a common ocular complication of uncontrolled type I and type II diabetes. People recently diagnosed with diabetes have been shown to have significantly lower L/Z plasma concentrations [79]. Studies have commonly examined the effects of carotenoids on the development of diabetes but there is limited research examining the effects of carotenoids on diabetic retinopathy. An animal study conducted by Kowluru et al., examined the effects of zeaxanthin supplementation on the retina in diabetic rats and results showed significant inhibition of diabetes-induced retinal oxidative damage [80]. A study conducted by Chous et al., showed that compared to placebo, subjects taking a xanthophyll multicomponent nutritional supplement demonstrated a 27% increase in MPOD after six months which correlated with an improvement in visual function, serum lipids and a decrease in peripheral neuropathy [81]. As discussed earlier, increased MPOD has been shown to mitigate oxidative processes in the retina, studies have shown that type II diabetes patients have lower levels of MPOD [70]. MPOD levels have also been correlated with HbA1C levels [67]. Evidence regarding MPODs effect on the treatment and development of diabetic retinopathy is limited. Early studies and animal models suggest a potential protective role of MPOD in the development of diabetic retinopathy [67,80,81]. Figure 2 provides conceptual framework for the processes leading to reduced macular pigment in diabetes, including oxidative stress and metabolic issues, and their impact on antioxidants. It highlights the relationship between MPOD and HbA1C, as well as the potential role of carotenoid supplementation in the prevention of retinopathy.
3.5. Visual Performance
MPOD's influence on visual performance resonates with its role as a natural optical filter. Higher pigment density corresponds to enhanced light absorption, which aids in optimizing contrast sensitivity – the ability to discern subtle differences in light and dark areas [82,83,84,85]. Studies have demonstrated a positive correlation between MPOD and contrast sensitivity, particularly in conditions of low light and reduced contrast [67,80,81]. This correlation underscores the potential of MPOD to fine-tune visual acuity, translating to improved day-to-day activities such as reading, driving, and recognizing facial expressions.
Glare, often experienced as visual discomfort caused by intense light sources, can significantly impede visual function. MPOD's protective role against glare becomes evident as the pigments selectively filter high-energy blue light, thus reducing glare's impact on visual perception [82,86].
Moreover, MPOD aids in hastening recovery from photostress – the temporary blinding effect experienced after exposure to bright light [82,86]. The pigments’ capacity to absorb excess light and dissipate its energy contributes to quicker recovery times, enhancing visual comfort in challenging lighting conditions [82,86].
Increasing MPOD has been linked to a noteworthy enhancement in best corrected visual acuity (BCVA), as indicated by a study by Loughman et al., revealing a significant positive association (r=0.237) between MPOD levels and BCVA [84]. This finding suggests that interventions aimed at increasing MPOD levels could be promising in enhancing visual acuity, offering a potential avenue for improving the eyesight of individuals with less-than-optimal BCVA [87].
MPOD’s beneficial effects on disability glare, photo stress recovery time, and contrast sensitivity are seen across diverse demographics, including certain professional athletes and individuals with low vision. A one year randomized, double-blind placebo-controlled trial in truck drivers showed that 20mg of daily lutein supplementation resulted in increased MPOD, contrast sensitivity, and decreased disability glare [88]. This underlines the potential commercial uses of increasing and measuring MPOD. There is evidence to support that MPOD can potentially be used as a clinical biomarker for ocular health in the setting of increased screen time and associated short-wavelength light exposure [89]. One study examined the effects of carotenoid supplementation versus placebo and found that carotenoid supplementation increased MPOD, which was also associated with improvements in headache frequency, eye strain, eye fatigue, and all measured visual performance variables [85]. Richer et al., conducted an RCT to assess the impact of increasing MPOD on night vision in elderly drivers [90]. They found that over a six-month period, participants who took a 14 mg Z + 7 mg L supplement experienced significant improvements in MPOD, glare recovery, contrast sensitivity, and preferred luminance, suggesting that carotenoid supplementation can enhance visual functions important for night driving [90]. In the realm of sports, where visual acuity and contrast sensitivity are paramount, higher MPOD levels could confer a competitive advantage. Improved contrast sensitivity could enhance an athlete's ability to discern critical visual cues, thereby refining their performance. Conversely, individuals with low vision may experience perceptual deficits due to compromised contrast sensitivity and glare discomfort. Modulating MPOD offers a potential avenue for ameliorating these challenges, enhancing the visual experiences of those with impaired vision, and improving visual performance in those in visually demanding fields. See Table 5 below for a summary.
3.7. MPOD and Cognitive Function
It has been well established that a higher level of serum and brain carotenoids are associated with improved cognitive function [107,108,109,110]. It is important to note that the carotenoids present in the macular pigment are also widely present in the brain [111]. One study investigated the relationship between MPOD and cognitive function in 4,453 adults aged >50 years and found that lower MPOD was associated with poorer performance on the Mini-Mental State Examination and on the Montreal Cognitive Assessment [109]. Lower MPOD was also associated with poorer prospective memory and slower reaction times [109]. As seen in Table 6, MPOD and cognitive function have been positively correlated across various mental processes in various age groups, strongly supporting the use of MPOD as a clinical biomarker for cognitive function.
4. Discussion
MPOD assessment, once confined to research settings, is finding its stride as a pivotal component of routine eye examinations. Including MPOD measurement within these examinations provides clinicians with a comprehensive snapshot of a patient's macular health. This insight extends beyond mere pigment quantification, unveiling potential susceptibility to AMD and other ocular conditions. By integrating MPOD assessment into the standard ocular assessment paradigm, clinicians can gain a deeper understanding of an individual's visual health trajectory, enabling proactive interventions and tailored recommendations.
The potential of MPOD as a predictive marker revolutionizes the landscape of treatment planning. As our understanding of the relationship between pigment density and ocular health deepens, MPOD emerges as a prognostic tool that guides personalized interventions. For instance, individuals with lower MPOD values may benefit from proactive strategies aimed at enhancing pigment density to mitigate AMD risk. Furthermore, MPOD assessment can aid in identifying individuals likely to respond favorably to specific treatments, optimizing therapeutic outcomes, and minimizing potential side effects.
The longitudinal monitoring of disease progression and treatment efficacy is essential in ocular health management. MPOD's potential in this realm is significant, offering insights into the evolution of macular health over time. By tracking changes in MPOD, clinicians can gauge dietary inadequacies and disease progression in conditions such as AMD and assess the impact of interventions on pigment density. This enables timely adjustments to treatment and management plans, ensuring that patients receive the most effective care. Additionally, MPOD measurements provide an objective parameter for assessing treatment efficacy, supplementing traditional subjective measures of visual function.
Current clinically available technologies for measuring macular pigment optical density (MPOD) lack the ability to estimate lutein and zeaxanthin optical densities, limiting personalized carotenoid supplementation therapies. The introduction of new biomarkers like lutein and zeaxanthin optical densities through technologies such as the Macular Pigment Reflectometer (MPR) could revolutionize precision medicine by providing repeatable MPOD and carotenoid optical density measurements [12]. Unlike heterochromatic flicker photometers (HFP), the MPR objectively measures MPOD and individual lutein and zeaxanthin components, offering a faster and more precise method that addresses the limitations of current technologies. The MPR utilizes controlled light beams and internal spectrometers to quantify lutein and zeaxanthin optical densities, providing reliable measurements for personalized supplementation strategies [13]. The current market and consumers are not ready for prophylactic personalized vitamin and nutritional therapies; nor do we have clinically available devices that can objectively measure MPOD and its individual components. The cost is the major prohibiting factor in the implementation of such strategies. The current conditions further emphasize the importance, dominance, and need for HFP devices in the measurement of MPOD.
Integrating MPOD measurement into clinical applications is not merely an addition to the diagnostic toolkit; it's a paradigm shift that empowers clinicians to provide personalized, proactive, and precise ocular care. The ability to predict risk, tailor treatments, and monitor changes in pigment density imbues ocular health management with unprecedented depth. By harnessing MPOD's potential, clinicians are poised to elevate the standard of care, ensuring that patients receive interventions that are not only evidence-based but also finely tuned to their individual ocular profiles.
Advances in technology are poised to revolutionize how MPOD is measured and interpreted. Emerging techniques, such as adaptive optics imaging and multi-wavelength fundus autofluorescence, offer enhanced spatial resolution and the ability to quantify pigment distribution across the macula with unprecedented detail. These technologies enable researchers to unravel nuances in pigment density and distribution, potentially linking specific pigment patterns to ocular health outcomes. As these methods become more affordable and accessible, the precision and granularity of MPOD assessment are set to soar, enhancing our understanding of its role in visual health.
The trajectory of ocular and systemic health is a marathon rather than a sprint, necessitating long-term studies to unravel the intricacies of MPOD's relationship with well-being. Longitudinal investigations are key to deciphering the dynamic interplay between MPOD and age-related ocular diseases, tracking changes in pigment density as individuals age and potentially developing early predictive markers for disease onset. These studies also illuminate the temporal dynamics of MPOD alterations due to lifestyle changes, ethnicities [127], interventions, and genetic predispositions. As we venture into the future, long-term studies will anchor our understanding of MPOD's enduring influence on ocular health.
Author Contributions
Conceptualization, B.V. and P.G.D.; methodology, A.M., K.I., B.V.; data curation, A.M.; writing—original draft preparation, B.V., A.M., M.A., K.I. and P.G.D.; writing—review and editing, B.V., A.M., M.A. K.I., D.L.G and P.G.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Dataset available on request from the authors.
Conflicts of Interest
Abdul Masri, none; Mohammed Armanazi, none; Keiko Inouye, none; Dennis L. Gierhart is the Chairman of EyePromise, manufacturer of various nutritional supplements and Zx Pro none of these products have been mentioned in the paper; Pinakin Davey is an Employee of EyePromise; Balamurali Vasudevan, none.
References
- Bone, R.A., Landrum, J.T., Hime, G.W., Cains, A., Zamor, J. Stereochemistry of the human macular carotenoids. Invest Ophthalmol Vis Sci. 1993;34(6):2033-2040.
- Bone, R.A, Landrum, J.T., Tarsis, S.L. Preliminary identification of the human macular pigment. Vision Res. 1985;25(11):1531-1535. [CrossRef]
- Handelman, G. J., Dratz, E. A., Reay, C. C., & van Kuijk, J. G. Carotenoids in the human macula and whole retina. Invest Ophthalmol Vis Sci. 1988;29(6):850-855.
- Bone, R. A., Landrum, J. T., Friedes, L. M., Gomez, C. M., Kilburn, M. D., Menendez, E., Vidal, I., & Wang, W. Distribution of lutein and zeaxanthin stereoisomers in the human retina. Exp Eye Res. 1997;64(2):211-218.
- Dorey CK, Gierhart D, Fitch KA, Crandell I, Craft NE. Low Xanthophylls, Retinol, Lycopene, and Tocopherols in Grey and White Matter of Brains with Alzheimer's Disease. J Alzheimers Dis. 2023;94(1):1-17. [CrossRef] [PubMed] [PubMed Central]
- Krinsky, N.I. Carotenoid protection against oxidation. Pure Appl Chem, 1979;51:649-660.
- Brown, M. J., Ferruzzi, M. G., Nguyen, M. L., Cooper, D. A., Eldridge, A. L., Schwartz, S. J., & White, W. S. Carotenoid bioavailability is higher from salads ingested with full-fat than with fat-reduced salad dressings as measured with electrochemical detection. Am J Clin Nutr. 2004;80(2):396-403.
- Reboul, E., Thap, S., Tourniaire, F., André, M., Juhel, C., Morange, S., Amiot, M. J., Lairon, D., & Borel, P. Differential effect of dietary antioxidant classes (carotenoids, polyphenols, vitamins C and E on lutein absorption. Br J Nutr. 2007;97(3):440-446.
- Hornero-Méndez, D., Mínguez-Mosquera, M.I. Bioaccessibility of carotenes from carrots: Effect of cooking and addition of oil. Innov Food Sci Emer Tech. 2007;8(3):407-412.
- Riedl, J., Linseisen, J., Hoffmann, J., Wolfram, G. Some dietary fibers reduce the absorption of carotenoids in women. J Nutr. 1999;129(12):2170-2176. [CrossRef]
- Perry, A., Rasmussen, H., Johnson, E. Xantophyll (lutein, zeaxanthin) content in fruits, vegetables and corn and egg products. J Food Composition Analysis. 2009;22:9-15.
- Sanabria, J.C., Bass, J., Spors, F., Gierhart, D.L., Davey, P.G. Measurement of Carotenoids in Perifovea using the Macular Pigment Reflectometer. J Vis Exp. 2020 Jan 29;(155).
- Davey, P.G., Rosen, R.B., Gierhart, D.L. Macular Pigment Reflectometry: Developing Clinical Protocols, Comparison with Heterochromatic Flicker Photometry and Individual Carotenoid Levels. Nutrients. 2021 Jul 26;13(8):2553.
- Goodrow, E. F., Wilson, T. A., Houde, S. C., Vishwanathan, R., Scollin, P. A., Handelman, G., & Nicolosi, R. J. Consumption of one egg per day increases serum lutein and zeaxanthin concentrations in older adults without altering serum lipid and lipoprotein cholesterol concentrations. J Nutr. 2006;136(10):2519-2524.
- Müller, H. [Daily intake of carotenoids (carotenes and xanthophylls) from total diet and the carotenoid content of selected vegetables and fruit. Z Ernahrungswiss. 1996;35(1):45-50. [CrossRef]
- Bone, R,A, Landrum, J,T. Heterochromatic flicker photometry. Arch Biochem Biophys 2004; 430:137–142.
- Stringham, J. M., Hammond, B. R., Nolan, J. M., Wooten, B. R., Mammen, A., Smollon, W., & Snodderly, D. M. The utility of using customized heterochromatic flicker photometry (cHFP) to measure macular pigment in patients with AMD. Exp Eye Res. 2008; 87:445–453.
- van de Kraats, J., Berendschot, T. T., Valen, S., & van Norren, D. Fast assessment of the central macular pigment density with natural pupil using the macular pigment reflectometer. J Biomed Opt, 2006; 11:064031.
- Bone, R. A., Brener, B., & Gibert, J. C. Macular pigment, photopigments, and melanin: distributions in young subjects determined by four-wavelength reflectometry. Vision Res 2007; 47:3259–3268.
- Morita, H., Matsushita, I., Fujino, Y., Obana, A., & Kondo, H. Measuring MPOD using reflective images of confocal scanning laser system. Jpn J Ophthalmol, 2024; 68(1), 19–25.
- Wooten, B. R., & Hammond, B. R., Jr. Spectral absorbance and spatial distribution of macular pigment using heterochromatic flicker photometry. Optom Vis Sci 2005; 82:378–386.
- Bernstein, P. S., Yoshida, M. D., Katz, N. B., McClane, R. W., & Gellermann, W. Raman detection of macular carotenoid pigments in intact human retina. Invest Ophthalmol Vis Sci 1998; 39:2003–2011.
- Delori F. C. Spectrophotometer for noninvasive measurement of intrinsic fluorescence and reflectance of the ocular fundus. Appl Opt 1994; 33:7439–7452.
- Davey, P. G., Alvarez, S. D., & Lee, J. Y. Macular pigment optical density: repeatability, intereye correlation, and effect of ocular dominance. Clin Ophthalmol. 2016;10:1671-1678.
- National Society to Prevent Blindness Vision Problems in the US: Data Analyses. New York: National Society to Prevent Blindness, 1980;1–46.
- Klein, R., Klein, B. E., Tomany, S. C., Meuer, S. M., & Huang, G. H. Ten-year incidence and progression of age-related maculopathy: the Beaver Dam Eye Study. Ophthalmol 2002; 109(10):1767–1779.
- Lem DW, Davey PG, Gierhart DL, Rosen RB. A Systematic Review of Carotenoids in the Management of Age-Related Macular Degeneration. Antioxidants (Basel). 2021 Aug 5;10(8):1255. [CrossRef] [PubMed] [PubMed Central]
- Age-Related Eye Disease Study 2 Research Group. Lutein + Zeaxanthin and Omega-3 Fatty Acids for AMD: The Age-Related Eye Disease Study 2 (AREDS2) Randomized Clinical Trial. JAMA Ophthalmol. 2013;309(19):2005–2015.
- Chew, E. Y., Clemons, T. E., Agrón, E., Domalpally, A., Keenan, T. D. L., Vitale, S., Weber, C., Smith, D. C., Christen, W., & AREDS2 Research Group. JAMA Ophthalmol. 2022; Jul 1;140(7):692-698.
- Age-Related Eye Disease Study 2 (AREDS2) Research Group, Chew, E. Y., SanGiovanni, J. P., Ferris, F. L., Wong, W. T., Agron, E., Clemons, T. E., Sperduto, R., Danis, R., Chandra, S. R., Blodi, B. A., Domalpally, A., Elman, M. J., Antoszyk, A. N., Ruby, A. J., Orth, D., Bressler, S. B., Fish, G. E., Hubbard, G. B., Klein, M. L., Bernstein, P. Lutein/zeaxanthin for the treatment of age-related cataract: AREDS2 randomized trial report no. 4. JAMA Ophthalmol. 2013; Jul;131(7):843-50.
- Beatty, S., Murray, I. J., Henson, D. B., Carden, D., Koh, H., & Boulton, M. E. Arch Ophthalmol 1999; 113:1518–1523.
- Tsika, C., Tsilimbaris, M. K., Makridaki, M., Kontadakis, G., Plainis, S., & Moschandreas, J. Assessment of MPOD (MPOD) in patients with unilateral wet AMD (AMD). Acta Ophthalmol. 2011;89(7):e573-e578.
- Bone, R. A., Landrum, J. T., Mayne, S. T., Gomez, C. M., Tibor, S. E., & Twaroska, E. E. Macular pigment in donor eyes with and without AMD: a case-control study. Invest Ophthalmol Vis Sci 2001; 42(1):235–240.
- Beatty, S., Chakravarthy, U., Nolan, J. M., Muldrew, K. A., Woodside, J. V., Denny, F., & Stevenson, M. R. Secondary outcomes in a clinical trial of carotenoids with coantioxidants versus placebo in early age-related macular degeneration. Ophthalmol. 2013;120(3):600-606.
- Dawczynski, J., Jentsch, S., Schweitzer, D., Hammer, M., Lang, G. E., & Strobel, J. Long term effects of lutein, zeaxanthin and omega-3-LCPUFAs supplementation on optical density of macular pigment in AMD patients: the LUTEGA study. Graefes Arch Clin Exp Ophthalmol. 2013;251(11):2711-2723.
- Murray, I. J., Makridaki, M., van der Veen, R. L., Carden, D., Parry, N. R., & Berendschot, T. T. Lutein supplementation over a one-year period in early AMD might have a mild beneficial effect on visual acuity: The CLEAR Study. Invest Ophthalmol Vis Sci. 2013;54(3):1781-1788.
- Richer, S., Stiles, W., Statkute, L., Pulido, J., Frankowski, J., Rudy, D., Pei, K., Tsipursky, M., & Nyland, J. Double-masked, placebo-controlled, randomized trial of lutein and antioxidant supplementation in the intervention of atrophic age-related macular degeneration: the Veterans LAST study (Lutein Antioxidant Supplementation Trial). Optometry. 2004;75:216-230.
- Trieschmann, M., Beatty, S., Nolan, J. M., Hense, H. W., Heimes, B., Austermann, U., Fobker, M., & Pauleikhoff, D. Changes in macular pigment optical density and serum concentrations of its constituent carotenoids following supplemental lutein and zeaxanthin: the LUNA study. Exp Eye Res. 2007;84(4):718-728.
- Richer, S. P., Stiles, W., Graham-Hoffman, K., Levin, M., Ruskin, D., Wrobel, J., Park, D. W., & Thomas, C. Randomized, double-blind, placebo-controlled study of zeaxanthin and visual function in patients with atrophic age-related macular degeneration: The Zeaxanthin and Visual Function Study (ZVF). Optometry. 2011;82(11):667-680.
- Weigert, G., Kaya, S., Pemp, B., Sacu, S., Lasta, M., Werkmeister, R. M., Dragostinoff, N., Simader, C., Garhöfer, G., Schmidt-Erfurth, U., & Schmetterer, L. Effects of lutein supplementation on macular pigment optical density and visual acuity in patients with age-related macular degeneration. Invest Ophthalmol Vis Sci. 2011;52(11):8174-8178.
- Sabour-Pickett, S., Beatty, S., Connolly, E., Loughman, J., Stack, J., Howard, A., Klein, R., Klein, B. E., Meuer, S. M., Myers, C. E., Akuffo, K. O., & Nolan, J. M. Supplementation with three different macular carotenoid formulations in patients with early age-related macular degeneration. Retina. 2014;34(10):1757-1766.
- Huang, Y. M., Dou, H. L., Huang, F. F., Xu, X. R., Zou, Z. Y., & Lin, X. M. Effect of supplemental lutein and zeaxanthin on serum, macular pigmentation, and visual performance in patients with early age-related macular degeneration. Biomed Res Int. 2015;2015:564738.
- Davey, P. G., Henderson, T., Lem, D. W., Weis, R., Amonoo-Monney, S., & Evans, D. W. Visual function and macular carotenoid changes in eyes with retinal drusen—An open label randomized controlled trial to compare a micronized lipid-based carotenoid liquid supplementation and AREDS-2 formula. Nutrients. 2020;12:3271.
- Ma, L., Yan, S. F., Huang, Y. M., Lu, X. R., Qian, F., Pang, H. L., Xu, X. R., Zou, Z. Y., Dong, P. C., Xiao, X., Wang, X., Sun, T. T., Dou, H. L., & Lin, X. M. Effect of lutein and zeaxanthin on macular pigment and visual function in patients with early age-related macular degeneration. Ophthalmol. 2012;119(11):2290-2297.
- Weinreb, R. N., Aung, T., & Medeiros, F. A. The pathophysiology and treatment of glaucoma: A review. JAMA Ophthalmol. 2014; 311, 1901–1911.
- Kumar, D. M., & Agarwal, N. Oxidative Stress in Glaucoma: A Burden of Evidence. J Glaucoma, 2007; 16 (3), 334-343.
- Choi, J. S., Kim, D., Hong, Y. M., Mizuno, S., & Joo, C. K. Inhibition of nNOS and COX-2 expression by lutein in acute retinal ischemia. Nutrition 2006; 22, 668–671.
- Fung, F. K., Law, B. Y., & Lo, A. C. Lutein Attenuates Both Apoptosis and Autophagy upon Cobalt (II) Chloride-Induced Hypoxia in Rat Muller Cells. PLoS ONE 2016; 11, e0167828.
- Dilsiz, N., Sahaboglu, A., Yildiz, M. Z., & Reichenbach, A. Protective effects of various antioxidants during ischemia-reperfusion in the rat retina. Graefes Arch. Clin. Exp. Ophthalmol. 2006; 244, 627–633.
- Li, S. Y., Fu, Z. J., Ma, H., Jang, W. C., So, K. F., Wong, D., & Lo, A. C. Effect of lutein on retinal neurons and oxidative stress in a model of acute retinal ischemia/reperfusion. Invest Ophthalmol Vis Sci. 2009; 50, 836–843.
- Bignami A, Dahl D. The radial glia of Müller in the rat retina and their response to injury. An immunofluorescence study with antibodies to the glial fibrillary acidic (GFA) protein. Exp Eye Res. 1979 Jan;28(1):63-9.
- Bringmann A, Pannicke T, Grosche J, Francke M, Wiedemann P, Skatchkov SN, Osborne NN, Reichenbach A. Müller cells in the healthy and diseased retina. Prog Retin Eye Res. 2006 Jul;25(4):397-424.
- Siah, W. F., Loughman, J., & O'Brien, C. Lower macular pigment optical density in foveal-involved glaucoma. Ophthalmol. 2015;122(10):2029-2037.
- Lem DW, Gierhart DL, Davey PG. Carotenoids in the Management of Glaucoma: A Systematic Review of the Evidence. Nutrients. 2021 Jun 6;13(6):1949.
- Fikret, C., & Ucgun, N. I.Macular pigment optical density change analysis in primary open-angle glaucoma and pseudoexfoliation glaucoma. Int Ophthalmol. 2021;41(6):2235-2240.
- Bruns, Y., Junker, B., Boehringer, D., Framme, C., & Pielen, A. Comparison of macular pigment optical density in glaucoma patients and healthy subjects – a prospective diagnostic study. Clin Ophthalmol. 2020;14:1011-1017.
- Loughman, J., Loskutova, E., Butler, J. S., Siah, W. F., & O'Brien, C. Macular pigment response to lutein, zeaxanthin, and meso-zeaxanthin supplementation in open-angle glaucoma: a randomized controlled trial. Ophthalmol Sci. 2021;1(3):100039.
- Ji, Y., Zuo, C., Lin, M., Zhang, X., Li, M., Mi, L., Liu, B., & Wen, F. Macular pigment optical density in Chinese primary open angle glaucoma using the one-wavelength reflectometry method. J Ophthalmol. 2016;2016:2792103.
- Arnould, L., Seydou, A., Binquet, C., Gabrielle, P. H., Chamard, C., Bretillon, L., Bron, A. M., Acar, N., & Creuzot-Garcher, C. Macular pigment and open-angle glaucoma in the elderly: The Montrachet population-based study. J Clin Med. 2022;11(7):1830.
- Daga, F. B., Ogata, N. G., Medeiros, F. A., Moran, R., Morris, J., Zangwill, L. M., Weinreb, R. N., & Nolan, J. M. Macular pigment and visual function in patients with glaucoma: the San Diego Macular Pigment Study. Invest Ophthalmol Vis Sci. 2018;59(11):4471-4476.
- Lawler, T., Mares, J. A., Liu, Z., Thuruthumaly, C., Etheridge, T., Vajaranant, T. S., Domalpally, A., Hammond, B. R., Wallace, R. B., Tinker, L. F., Nalbandyan, M., Klein, B. E. K., Liu, Y., Carotenoids in Age-Related Eye Disease Study Investigators, & Second Carotenoids in Age-Related Eye Disease Study Research Group Association of macular pigment optical density with retinal layer thicknesses in eyes with and without manifest primary open-angle glaucoma. BMJ Open Ophth. 2023;8(1):e001331.
- Igras, E., Loughman, J., Ratzlaff, M., O'Caoimh, R., & O'Brien, C.. Evidence of lower macular pigment optical density in chronic open angle glaucoma. Br J Ophthalmol. 2013;97(8):994-998.
- Siah, W. F., O'Brien, C., & Loughman, J. J. Macular pigment is associated with glare-affected visual function and central visual field loss in glaucoma. Br J Ophthalmol. 2018;102(7):929-935.
- Eraslan, N., Yilmaz, M., & Celikay, O. Assessment of macular pigment optical density of primary open-angle glaucoma patients under topical medication. Photodiagnosis Photodyn Ther. 2023;42:103585.
- Lem, D. W., Gierhart, D. L., & Davey, P. G. A systematic review of carotenoids in the management of diabetic retinopathy. Nutrients, 2011; 13(7), 2441.
- Scanlon, G., Loughman, J., Farrell, D., & McCartney, D. A review of the putative causal mechanisms associated with lower macular pigment in diabetes mellitus. Nutrition research reviews, 2019; 32(2), 247-264.
- Lima, V. C., Rosen, R. B., Maia, M., Prata, T. S., Dorairaj, S., Farah, M. E., & Sallum, J. MPOD measured by dual-wavelength autofluorescence imaging in diabetic and nondiabetic patients: a comparative study. Invest Ophthalmol Vis Sci., 2010; pp. 5840–5845.
- Dong, L. Y., Jin, J., Lu, G., & Kang, X. L. Astaxanthin attenuates the apoptosis of retinal ganglion cells in db/db mice by inhibition of oxidative stress. Marine Drugs, 2013; 11(3), 960-974.
- Lima, V. C., Rosen, R. B., & Farah, M. Macular pigment in retinal health and disease. Int J Retina Vitreous. 2016;2:19.
- Scanlon, G., McCartney, D., Butler, J. S., Loskutova, E., & Loughman, J. Identification of Surrogate Biomarkers for the Prediction of Patients at Risk of Low Macular Pigment in Type 2 Diabetes. Curr Eye Res. 2019;44(12):1369-1380.
- Bikbov, M.M., Fayzrakhmanov, R.R., Yarmukhametova, A.L., Zainullin, R.M. Structural and functional analysis of the central zone of the retina in patients with diabetic macular edema. Сахарный диабет. 2015;18(4):99-104.
- Scanlon, G., Connell, P., Ratzlaff, M., Foerg, B., McCartney, D., Murphy, A., OʼConnor, K., & Loughman, J. Macular pigment optical density is lower in type 2 diabetes, compared with type 1 diabetes and normal controls. Retina. 2015;35:1808–1816.
- She, C. Y., Gu, H., Xu, J., Yang, X. F., Ren, X. T., & Liu, N. P. Association of macular pigment optical density with early stage of non-proliferative diabetic retinopathy in Chinese patients with type 2 diabetes mellitus. Int J Ophthalmol. 2016;9(10):1433-1438.
- Bikbov, M.M., Zainullin, R.M., Faizrakhmanov, R.R.. Macular pigment optical density alteration as an indicator of diabetic macular edema development. Sovremennye Tehnologii v Medicine. 2015;7(3):73-75. [CrossRef]
- Chous, A. P., Richer, S. P., Gerson, J. D., & Kowluru, R. A. The Diabetes Visual Function Supplement Study (DiVFuSS). Br J Ophthalmol. 2016;100:227–234.
- Zagers, N. P., Pot, M. C., & van Norren, D. Spectral and directional reflectance of the fovea in diabetes mellitus: photoreceptor integrity, macular pigment and lens. Vision Res. 2005;45(13):1745-1753.
- Varghese, M., & Antony, J. Assessment of macular pigment optical density using fundus reflectometry in diabetic patients. Middle East African J Ophthalmol. 2019;26(3):145-150.
- Cennamo, G, Montorio, D, Santoro, G, Cennamo, G. Evaluation of choroidal and retinal thickness changes measured by swept-source optical coherence tomography in patients with prediabetes and type 2 diabetes. Retina. 2019;39(4):702-707.
- Ford, E. S., Will, J. C., Bowman, B. A., & Narayan, K. M. Diabetes mellitus and serum carotenoids: findings from the Third National Health and Nutrition Examination Survey. Am J Epidemiol 1999; 149(2):168–176.
- Kowluru, R. A., Menon, B., & Gierhart, D. L. Beneficial effect of zeaxanthin on retinal metabolic abnormalities in diabetic rats. Invest Ophthalmol Vis Sci. 2008; Apr;49(4):1645-51.
- Chous, A. P., Richer, S. P., Gerson, J. D., & Kowluru, R. A. The Diabetes Visual Function Supplement Study (DiVFuSS). Br J Ophthal. 2016;100:227-234.
- Hammond, B. R., Jr, Fletcher, L. M., & Elliott, J. G. Glare disability, photostress recovery, and chromatic contrast: relation to macular pigment and serum lutein and zeaxanthin. Invest Ophthalmol Vis Sci. 2013;54:476–81.
- Kvansakul, J., Rodriguez-Carmona, M., Edgar, D. F., Barker, F. M., Köpcke, W., Schalch, W., & Barbur, J. L. Supplementation with the carotenoids lutein or zeaxanthin improves human visual performance. Ophthalmic Physiol Opt. 2006;26:362–71.
- Loughman, J., Akkali, M. C., Beatty, S., Scanlon, G., Davison, P. A., O'Dwyer, V., Cantwell, T., Major, P., Stack, J., & Nolan, J. M. The relationship between macular pigment and visual performance. Vis Res. 2010;50:1249–56.
- Stringham, J. M., O'Brien, K. J., & Stringham, N. T. Contrast sensitivity and lateral inhibition are enhanced with macular carotenoid supplementation. Invest Ophthalmol Vis Sci. 2017;58:2291–5.
- Stringham, J. M., Garcia, P. V., Smith, P. A., McLin, L. N., & Foutch, B. K. Macular pigment and visual performance in glare: benefits for photostress recovery, disability glare, and visual discomfort. Invest Ophthalmol Vis Sci. 2011;52:7406–15.
- Bone R.A., Davey, P.G., Roman, B.O., Evans, D.W. Efficacy of Commercially Available Nutritional Supplements: Analysis of Serum Uptake, Macular Pigment Optical Density and Visual Functional Response. Nutrients. 2020 May 6;12(5):1321.
- Yao, Y., Qiu, Q. H., Wu, X. W., Cai, Z. Y., Xu, S., & Liang, X. Q. Lutein supplementation improves visual performance in Chinese drivers: 1-year randomized, double-blind, placebo-controlled study. Nutrition. 2013; Jul-Aug;29(7-8):958-64.
- Stringham, J. M., Stringham, N. T., & O'Brien, K. J. Macular Carotenoid Supplementation Improves Visual Performance, Sleep Quality, and Adverse Physical Symptoms in Those with High Screen Time Exposure. Foods. 2017;6(7):47.
- Richer, S., Novil, S., Gullett, T., Dervishi, A., Nassiri, S., Duong, C., Davis, R., & Davey, P. G. Night Vision and Carotenoids (NVC): A Randomized Placebo Controlled Clinical Trial on Effects of Carotenoid Supplementation on Night Vision in Older Adults. Nutrients. 2021;13(9):3191.
- Engles, M., Wooten, B., Hammond, B. Macular pigment: A test of the acuity hypothesis. Invest Ophthalmol Vis Sci. 2007;48(6):2922-2931.
- Tudosescu, R., Alexandrescu, C. M., Istrate, S. L., Vrapciu, A. D., Ciuluvică, R. C., & Voinea, L. Correlations between internal and external ocular factors and macular pigment optical density. Romanian J Ophthalmol. 2018;62(1):42-47.
- Patryas, L., Parry, N. R., Carden, D., Aslam, T., & Murray, I. J. The association between dark adaptation and macular pigment optical density in healthy subjects. Graefes Arch Clin Exp Ophthalmol. 2014;252(4):657-663.
- Bovier, E. R., Renzi, L. M., & Hammond, B. R. A double-blind, placebo-controlled study on the effects of lutein and zeaxanthin on neural processing speed and efficiency. PLoS ONE. 2014;9(9):e108178.
- Kvansakul, J., Rodriguez-Carmona, M., Edgar, D. F., Barker, F. M., Köpcke, W., Schalch, W., & Barbur, J. L. Supplementation with the carotenoids lutein or zeaxanthin improves human visual performance. Ophthalmic Physiol Opt. 2006;26(4):362-371.
- Putnam, C. M., & Bassi, C. J. Macular pigment spatial distribution effects on glare disability. J. Optom. 2015;8(4):258-265.
- Stringham, J. M., & Hammond, B. R. Macular pigment and visual performance under glare conditions. Optom Vis Sci. 2008;85(2):82-88.
- Stringham, J. M., O'Brien, K. J., & Stringham, N. T. Contrast sensitivity and lateral inhibition are enhanced with macular carotenoid supplementation. Invest Ophthalmol Vis Sci. 2017;58(4):2291-2295.
- Nolan, J. M., Power, R., Stringham, J., Dennison, J., Stack, J., Kelly, D., Moran, R., Akuffo, K. O., Corcoran, L., & Beatty, S. Enrichment of macular pigment enhances contrast sensitivity in subjects free of retinal disease: central retinal enrichment supplementation trials – report 1. Invest Ophthalmol Vis Sci. 2016;57(7):3429-3439.
- Hammond, B. R., Fletcher, L. M., Roos, F., Wittwer, J., & Schalch, W.A double-blind, placebo-controlled study on the effects of lutein and zeaxanthin on photostress recovery, glare disability, and chromatic contrast. Invest Ophthalmol Vis Sci. 2014;55(12):8583-8589.
- Hammond, B. R., Jr, Fletcher, L. M., & Elliott, J. G. Glare disability, photostress recovery, and chromatic contrast: Relation to macular pigment and serum lutein and zeaxanthin. Invest Ophthalmol Vis Sci. 2013;54(1):476.
- Stringham, J. M., O'Brien, K. J., & Stringham, N. T. Macular carotenoid supplementation improves disability glare performance and dynamics of Photostress Recovery. Eye and Vision. 2016;3(1).
- Hammond, B. R., Jr, Wooten, B. R., & Snodderly, D. M. Preservation of visual sensitivity of older subjects: association with macular pigment density. Invest Ophthalmol Vis Sci. 1998;39(2):397-406.
- Estévez-Santiago, R., Olmedilla-Alonso, B., & Beltrán-de-Miguel, B. Assessment of lutein and zeaxanthin status and dietary markers as predictors of the contrast threshold in 2 age groups of men and women. Nutr Res. 2016;36(7):719-730.
- Nolan, J. M., Loughman, J., Akkali, M. C., Stack, J., Scanlon, G., Davison, P., & Beatty, S. The impact of macular pigment augmentation on visual performance in normal subjects: COMPASS. Vision Res. 2011;51(5):459-469.
- Loughman, J., Akkali, M. C., Beatty, S., Scanlon, G., Davison, P. A., O'Dwyer, V., Cantwell, T., Major, P., Stack, J., & Nolan, J. M. The relationship between macular pigment and visual performance. Vision Res. 2010;50(13):1249-1256.
- Johnson, E. J., Vishwanathan, R., Johnson, M. A., Hausman, D. B., Davey, A., Scott, T. M., Green, R. C., Miller, L. S., Gearing, M., Woodard, J., Nelson, P. T., Chung, H. Y., Schalch, W., Wittwer, J., & Poon, L. W. Relationship between serum and brain carotenoids, α-tocopherol, and retinol concentrations and cognitive performance in the oldest old from the Georgia Centenarian Study. J. Aging Res. 2013;2013:951786.
- Feeney, J., O'Leary, N., Moran, R., O'Halloran, A. M., Nolan, J. M., Beatty, S., Young, I. S., & Kenny, R. A. Plasma lutein and zeaxanthin are associated with better cognitive function across multiple domains in a large population-based sample of older adults: Findings from the Irish Longitudinal Study on Aging. J. Gerontol. A Biol. Sci. Med. Sci. 2017;72:1431–1436.
- Power, R., Coen, R. F., Beatty, S., Mulcahy, R., Moran, R., Stack, J., Howard, A. N., & Nolan, J. M. Supplemental retinal carotenoids enhance memory in healthy individuals with low levels of macular pigment in a randomized, double-blind, placebo-controlled clinical trial. J. Alzheimer’s Dis. 2018;61:947–961.
- Lindbergh, C. A., Mewborn, C. M., Hammond, B. R., Renzi-Hammond, L. M., Curran-Celentano, J. M., & Miller, L. S. Relationship of lutein and zeaxanthin levels to neurocognitive functioning: An fMRI study of older adults. J. Int. Neuropsychol. Soc. 2017;23:11–22.
- Feeney, J., Finucane, C., Savva, G. M., Cronin, H., Beatty, S., Nolan, J. M., & Kenny, R. A. Low macular pigment optical density is associated with lower cognitive performance in a large, population-based sample of older adults. Neurobiology Aging. 2013;34(11):2449-2456.
- Khan, N. A., Walk, A. M., Edwards, C. G., Jones, A. R., Cannavale, C. N., Thompson, S. V., Reeser, G. E., & Holscher, H. D. Macular Xanthophylls Are Related to Intellectual Ability among Adults with Overweight and Obesity. Nutrients. 2018;10(4):396.
- Saint, S. E., Renzi-Hammond, L. M., Khan, N. A., Hillman, C. H., Frick, J. E., & Hammond, B. R.. The Macular Carotenoids are Associated with Cognitive Function in Preadolescent Children. Nutrients. 2018;10(2):193.
- Renzi-Hammond, L. M., Bovier, E. R., Fletcher, L. M., Miller, L. S., Mewborn, C. M., Lindbergh, C. A., Baxter, J. H., & Hammond, B. R. Effects of a Lutein and Zeaxanthin Intervention on Cognitive Function: A Randomized, Double-Masked, Placebo-Controlled Trial of Younger Healthy Adults. Nutrients. 2017;9(11):1246.
- Barnett, S. M., Khan, N. A., Walk, A. M., Raine, L. B., Moulton, C., Cohen, N. J., Kramer, A. F., Hammond, B. R., Jr, Renzi-Hammond, L., & Hillman, C. H. Macular pigment optical density is positively associated with academic performance among preadolescent children. Nutr Neurosci. 2018;21(9):632-640.
- Lindbergh, C. A., Renzi-Hammond, L. M., Hammond, B. R., Terry, D. P., Mewborn, C. M., Puente, A. N., & Miller, L. S. Lutein and Zeaxanthin Influence Brain Function in Older Adults: A Randomized Controlled Trial. J Int Neuropsychol Soc. 2018;24(1):77-90.
- Kelly, D., Coen, R. F., Akuffo, K. O., Beatty, S., Dennison, J., Moran, R., Stack, J., Howard, A. N., Mulcahy, R., & Nolan, J. M. Cognitive Function and Its Relationship with Macular Pigment Optical Density and Serum Concentrations of its Constituent Carotenoids. J Alzheimers Dis. 2015;48(1):261-277.
- Power, R., Coen, R. F., Beatty, S., Mulcahy, R., Moran, R., Stack, J., Howard, A. N., & Nolan, J. M. Supplemental Retinal Carotenoids Enhance Memory in Healthy Individuals with Low Levels of Macular Pigment in A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. J Alzheimers Dis. 2018;61(3):947-961.
- Ajana, S., Weber, D., Helmer, C., Merle, B. M., Stuetz, W., Dartigues, J. F., Rougier, M. B., Korobelnik, J. F., Grune, T., Delcourt, C., & Féart, C. Plasma Concentrations of Lutein and Zeaxanthin, Macular Pigment Optical Density, and Their Associations With Cognitive Performances Among Older Adults. Invest Ophthalmol Vis Sci. 2018;59(5):1828-1835.
- Vishwanathan, R., Iannaccone, A., Scott, T. M., Kritchevsky, S. B., Jennings, B. J., Carboni, G., Forma, G., Satterfield, S., Harris, T., Johnson, K. C., et al. Macular pigment optical density is related to cognitive function in older people. Age Ageing. 2014;43(2):271-275.
- Renzi, L. M., Dengler, M. J., Puente, A., Miller, L. S., & Hammond, B. R., Jr. Relationships between macular pigment optical density and cognitive function in unimpaired and mildly cognitively impaired older adults. Neurobiol Aging. 2014;35(7):1695-1699.
- Feeney, J., Finucane, C., Savva, G. M., Cronin, H., Beatty, S., Nolan, J. M., & Kenny, R. A. Low macular pigment optical density is associated with lower cognitive performance in a large, population-based sample of older adults. Neurobiol Aging. 2013;34(11):2449-2456.
- Stringham, N. T., Holmes, P. V., & Stringham, J. M. Effects of macular xanthophyll supplementation on brain-derived neurotrophic factor, pro-inflammatory cytokines, and cognitive performance. Physiol Behav. 2019;211:112650.
- Hassevoort, K. M., Khazoum, S. E., Walker, J. A., Barnett, S. M., Raine, L. B., Hammond, B. R., Renzi-Hammond, L. M., Kramer, A. F., Khan, N. A., Hillman, C. H., & Cohen, N. J. Macular Carotenoids, Aerobic Fitness, and Central Adiposity Are Associated Differentially with Hippocampal-Dependent Relational Memory in Preadolescent Children. J Pediatr. 2017;183:108-114.e1.
- Edwards, C. G., Walk, A. M., Cannavale, C. N., Thompson, S. V., Reeser, G. E., Holscher, H. D., & Khan, N. A. Mol Nutr Food Res. 2019;63(15):e1801059.
- Mewborn, C. M., Lindbergh, C. A., Robinson, T. L., Gogniat, M. A., Terry, D. P., Jean, K. R., Hammond, B. R., Renzi-Hammond, L. M., & Miller, L. S. Lutein and Zeaxanthin Are Positively Associated with Visual-Spatial Functioning in Older Adults: An fMRI Study. Nutrients. 2018;10(4):458.
- Davey, P.G., Lievens, C., Ammono-Monney, S. Differences in macular pigment optical density across four ethnicities: a comparative study. Ther Adv Ophthalmol. 2020 Jun 15;12:2515841420924167.
Figure 2.
MPOD Model of Inflammation.
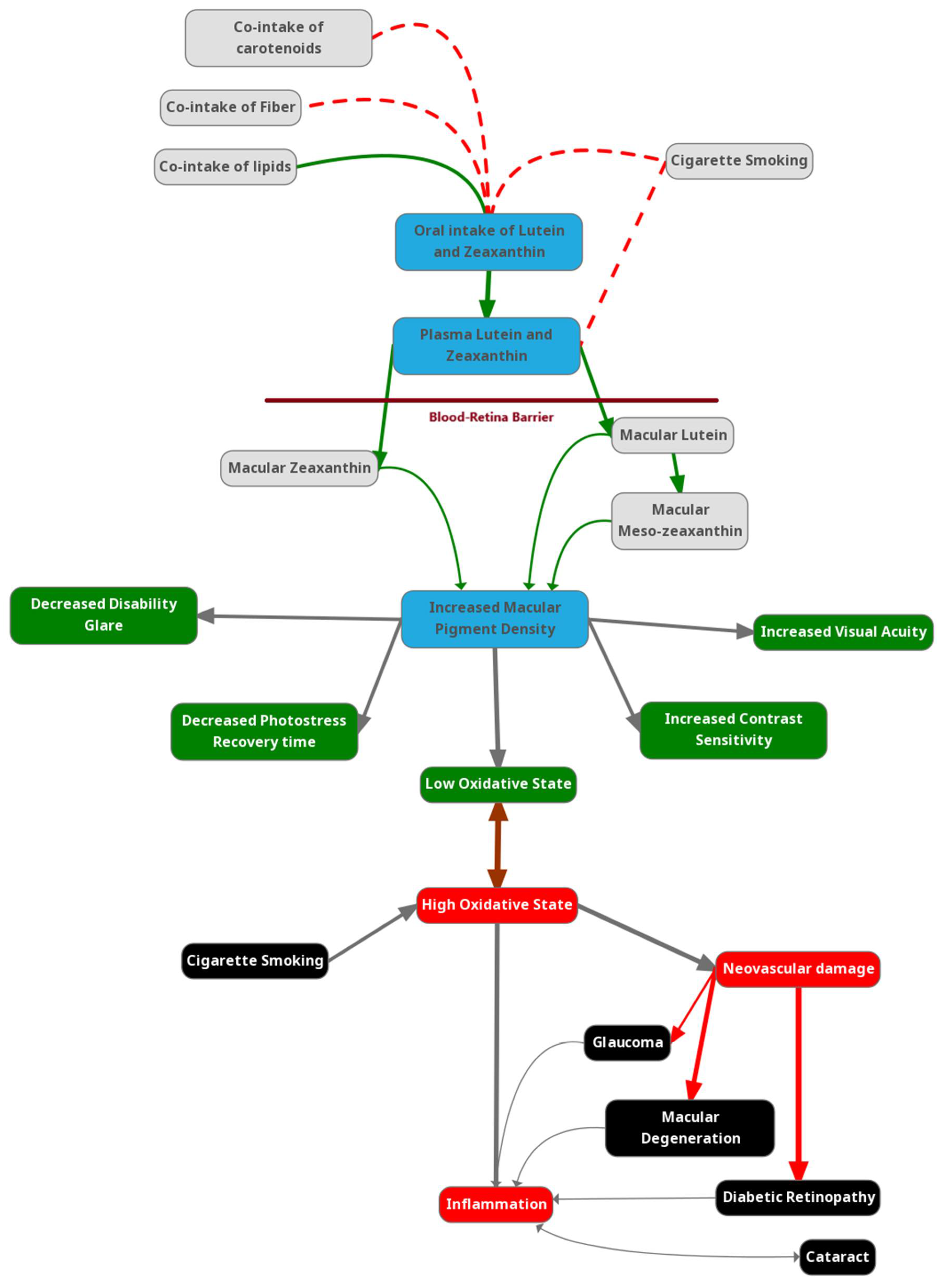
Figure 2.
MPOD and Diabetic Retinopathy.
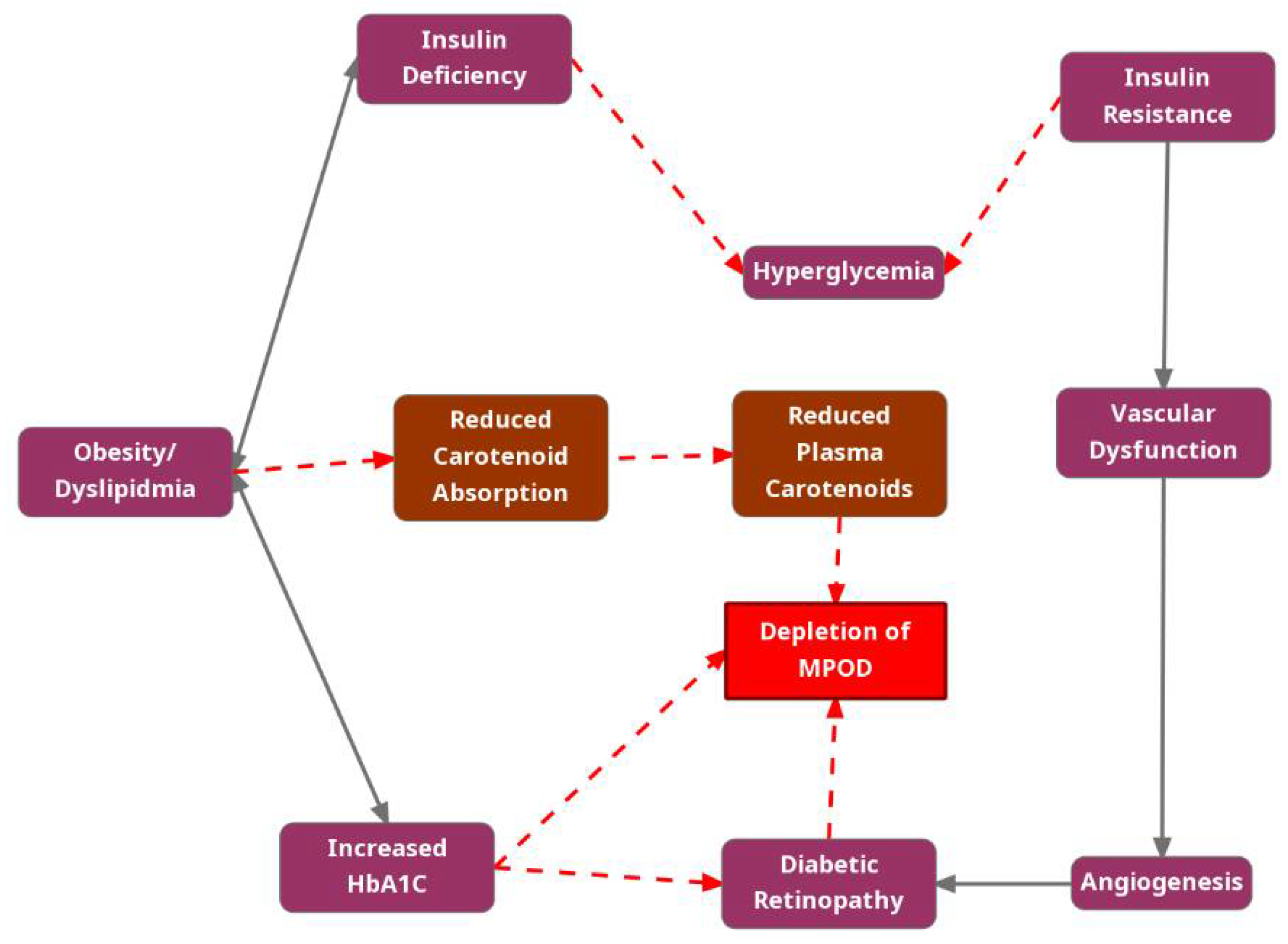

Table 1.
L/Z quantities in commonly consumed food.
| Figure 100. | Trans-Lutein (ug per 100g) | Trans-Zeaxanthin (ug per 100g) | L/Z Ratio |
|---|---|---|---|
| Asparagus, cooked | 991 | 0 | - |
| Broccoli, cooked | 772 | 0 | - |
| Cucumber | 361 | 0 | - |
| Spinach, cooked | 12,640 | 0 | - |
| Spinach, raw | 6,603 | 0 | - |
| Tomato, raw | 32 | 0 | - |
| Lettuce, romaine | 3,824 | 0 | - |
| Lettuce, iceberg | 171 | 12 | 14.3 |
| Green beans, cooked from frozen | 306 | 0 | - |
| Kale, cooked | 8,884 | 0 | - |
| Pepper, orange | 208 | 1,665 | 0.1 |
| Pepper, green | 173 | 0 | - |
| Bread, white | 15 | 0 | - |
| Egg (yolk + white), cooked | 237 | 216 | 1.1 |
| Egg yolk, cooked | 645 | 587 | 1.1 |
| Pistachio, shelled | 1405 | 0 | - |
| Grapes, green | 53 | 6 | 8.8 |
| Cilantro | 7703 | 0 | - |
| Lima beans, cooked | 155 | 0 | - |
| Olive, green | 79 | 0 | - |
| Parsley, raw | 4326 | 0 | - |
| Squash, yellow, cooked | 150 | 0 | - |
| Zucchini, cooked with skin | 1355 | 0 | - |
* Abbreviations: L/Z= Lutein/Zeaxanthin, ug= microgram; Data obtained from: [11].
Table 2.
Randomized control trial studies examining the relationship between MPOD and AMD.
| Author (Year) | Study Design | Inclusion Criteria | Sample Size | Interventions | Duration | Relation between MPOD & AMD | MPOD Technique | |
|---|---|---|---|---|---|---|---|---|
| Beatty study (2013) [34] | RCT | Adults ≥55 years with early or late-stage AMD. | 433 | Group 1: L and Z, Vitamin C, Vitamin E, Copper, Zinc.Group 2: Placebo. | Minimum 12 months, up to 36 months | Supplementation with L, Z, and antioxidants showed functional and morphologic benefits in early AMD. MPOD increased in the active group and decreased in the placebo group. | RS | |
| LUTEGA study (2013) [35] | RCT | Adults 60-80 years with non-exudative AMD. | 172 | Group 1: L, Z, Omega-3, antioxidants. Group 2: Placebo |
12 months | Supplementation resulted in a considerable increase in MPOD and improvement/stabilization in BCVA. No difference in MPOD accumulation between dosages. | FA | |
| CLEAR study (2013) [36] | RCT | Adults 50-80 years with early AMD. | 72 | Group 1: L (10 mg) Group 2: Placebo | 12 months | Lutein supplementation increased MPOD and may have a mild beneficial effect on visual acuity. No change in MPOD found in the placebo group. | HFP | |
| LAST study (2004) [37] | RCT | Adults 55-80 years with atrophic AMD. | 90 | Group 1: L (10 mg) Group 2: L (10 mg) with antioxidants Group 3: Placebo |
12 months | Lutein alone or with antioxidants improved MPOD, glare recovery, and contrast sensitivity. No significant change in placebo group. | HFP | |
| LUNA study (2007) [38] | RCT | Adults ≥55 years with or without AMD. | 120 | Group 1: L (6 mg) Group 2: Placebo |
6 months | Lutein supplementation increased MPOD and improved visual function. No change in placebo group. | FA | |
| ZVF study (2011) [39] | RCT | Early and moderate AMD retinopathy, symptoms of visual deficits. | 60 | Group 1: Z (8 mg) Group 2: Z (8 mg) + L (9 mg), Group 3: Placebo |
12 months | MPOD increased in the intervention groups compared to the placebo group | HFP | |
| Weigert (2011) [40] | RCT | Adults 50-90 years with AREDS stages 2, 3, and 4. | 126 | Group 1: L (20 mg for first 3 months, then 10 mg) Group 2: Placebo |
6 months | Lutein significantly increased MPOD by 27.9%. No significant effect on macular function or visual acuity. | HFP | |
| Sabour-Pickett (2014) [41] | RCT | Adults 50-79 years with early AMD. | 52 | Group 1: L (20 mg) and Z (2 mg) Group 2: MZ (10 mg), L (10 mg), Z (2 mg) Group 3: MZ (17 mg), L (3 mg), Z (2 mg) |
12 months | Statistically significant increase in MPOD was observed in Group 2 and Group 3. Improvements in letter contrast sensitivity were seen in all groups, with the best results in Group 3. | HFP | |
| Huang (2015) [42] | RCT | Adults 50-79 years with early AMD. | 112 | Group 1: L (10 mg) Group 2: L (20 mg) Group 3: L (10 mg) and Z (10 mg) |
2 years | All active treatment groups showed a significant increase in MPOD. The 20 mg lutein group was the most effective in increasing MPOD and contrast sensitivity at 3 cycles/degree for the first 48 weeks. | FA | |
| Davey (2020) [43] | RCT | Adults 50-79 years with retinal drusen. | 56 | Group 1: Lumega-Z softgel Group 2: PreserVision AREDS2 softgel |
6 months | Both groups demonstrated statistically significant improvements in contrast sensitivity function (CSF) in both eyes at six months. | HFP | |
| Ma (2012) [44] |
RCT | Ages 50-79, Early AMD. | 108 | Group 1: L (10 mg) Group 2: L (20 mg) Group 3: L (10 mg) plus Z (10 mg) |
48 weeks | Significant increase in MPOD in the high-dose lutein and lutein plus zeaxanthin groups, with improvements in contrast sensitivity at certain spatial frequencies. | FA | |
*Abbreviations: RCT = Randomized Control Trial, AMD = Age-related Macular Degeneration, L = Lutein, Z = Zeaxanthin, MZ = Meso-zeaxanthin, BCVA = Best Corrected Visual Acuity, RS = Raman Spectroscopy, HFP = Heterochromatic flicker photometry, FA = Fundus Autofluorescence.
Table 3.
Cross-sectional and randomized control trial studies examining the relationship between MPOD and Glaucoma
Table 3.
Cross-sectional and randomized control trial studies examining the relationship between MPOD and Glaucoma
| Author (Year) | Study Design | Inclusion Criteria | Sample Size | Intervention(s) | Duration | Relation between MPOD and Glaucoma | MPOD Technique |
|---|---|---|---|---|---|---|---|
| Fikret (2021) [55] |
CS | Age not mentioned. Patients with POAG, PEX and controls. | 79 | None | N/A | Higher MPOD values in patients with PEX glaucoma; no significant differences in POAG compared to controls. There was no correlation between MPOD values and RNFL or GCL. | FR |
| Bruns (2020) [56] |
CS | Adults 34-87 years; Patients with POAG and controls. | 86 | None | N/A | No significant difference in MPOD values between POAG patients and controls. | DWA |
| Loughman (2021) [57] | RCT | Adults >18 years. Patients with POAG and controls. | 62 | Group 1: L (10mg) + Z (2mg) + MZ (10mg). Group 2: Placebo. |
18 months | Supplementation led to a significant increase in MPOD volume. No clinically meaningful changes were noted in glaucoma parameters. | DWA |
| Siah (2015) [53] |
CS | Adults 36-84 years. Patients with POAG and controls. | 88 | None | N/A | Lower MPOD was observed in glaucomatous eyes compared to control. Worse glaucomatous parameters were observed in patients with lower MPOD. | HFP |
| Ji (2016) [58] |
CS | Adults 20-76 years. Patients with POAG and controls. | 82 | None | N/A | MPOD was significantly lower in POAG patients compared to controls, and correlated positively with GCC thickness. | FR |
| Arnould (2022) [59] | CS | Adults >75 years. Patients with POAG and controls. | 1153 | None | N/A | No significant differences in MPOD were found between the POAG group and the control group. | DWA |
| Daga (2018) [60] |
CS | Adults 20-76 years. Patients with POAG and controls. | 107 | None | N/A | No significant association was found between MPOD volume and glaucoma status. | DWA |
| Lawler (2023) [61] | CS | Adults 55-81 years. Patients with POAG and controls. | 379 | None | N/A | MPOD was positively associated with GCC, GCL, among POAG and controls. | HFP |
| Igras (2013) [62] |
CS | Adults 58-80 years. Patients with POAG and controls. | 40 | None | N/A | MPOD was significantly lower in POAG patients compared to controls. | HFP |
| Siah (2018) [63] |
CS | Adults 36-84 years. Patients with POAG and controls. | 88 | None | N/A | MPOD was associated with improved glare-affected visual function and less central visual field loss in POAG patients. | HFP |
| Eraslan (2023) [64] | CS | Adults >55 years. Patients with POAG currently receiving topical medication and controls. |
52 | None | N/A | MPOD levels were higher in POAG patients compared to controls, suggesting a possible protective effect of topical therapies. | FR |
*Abbreviations: RCT = Randomized Control Trial, CS = Cross-sectional, POAG = Primary open angle glaucoma, L = Lutein, Z = Zeaxanthin, MZ = Meso-zeaxanthin, BCVA = Best Corrected Visual Acuity, RS = Raman Spectroscopy, HFP = Heterochromatic flicker photometry, FR = Fundus Reflectance, DWA = Dual-wavelength autofluorescence. RNFL = retinal nerve fiber layer, GCL = Ganglion cell layer thickness, PEX = Pseudoexfoliative, GCC = Ganglion cell complex.
Table 4.
Cross-sectional and randomized control trial studies examining the relationship between MPOD and Diabetes
Table 4.
Cross-sectional and randomized control trial studies examining the relationship between MPOD and Diabetes
| Author (Year) | Study Design | Inclusion Criteria | Sample Size | Intervention(s) | Duration | Relation between MPOD and DR | MPOD Technique |
|---|---|---|---|---|---|---|---|
| Lima (2010) [69] | CS | Adults 56-63; BCVA ≤20/40. | 43 | None | N/A | MPOD was lower in diabetic patients, with significant inverse correlation with HbA1C levels. | DWA |
| Scanlon (2019) [70] | CS | Adults 50+; BCVA ≤20/40. | 2782 | None | N/A | MPOD was found to be lower in individuals with T2D compared to healthy controls. | HFP |
| Bikbov (2015) [71] | CS | Adults 55-71; BCVA ≤20/40. | 52 | None | N/A | Significant reduction of MPOD in patients with diabetic macular edema compared to controls. | FR |
| Scanlon (2015) [72] | CS | Adults 36-73; BCVA ≤20/25. | 150 | None | N/A | MPOD was significantly lower in T2D compared to T1D and controls. Diabetes control was not associated with MPOD. | HFP |
| She (2016) [73] | CS | Adults over 55-71; BCVA ≤20/25. | 401 | None | N/A | No significant difference in MPOD levels among groups with or without early-stage non-proliferative DR | HFP |
| Bikbov (2015) [74] | CS | Adults 54-69; BCVA ≤20/25. | 31 | None | N/A | Significant reduction of MPOD in DME patients, strong inverse correlation between retinal thickness and MPOD | FR |
| Chous (2016) [75] | RCT | Adults 43-69; BCVA ≥20/30; no or mild to moderate DR. | 67 | Group 1: Carotenoid supplement Group 2: placebo | 6 months | Supplemented group showed significant improvements in visual functions which correlated with increased MPOD compared to placebo | HFP |
| Zagers (2005) [76] | CS | Adults 23-61; BCVA ≤20/32. | 14 | None | N/A | No significant difference in MPOD density between diabetic patients and healthy controls. | FR |
| Varghese (2019) [77] | CS | Adults 49-54 years. | 150 | None | N/A | MPOD was similar across diabetic patients with and without DR, suggesting no significant difference due to DR. | FR |
| Cennamo (2019) [78] | CS | Adults 31-38 years; T1D and controls. | 59 | None | N/A | MPOD and vessel density were both significantly lower in diabetic patients compared to controls. Moderate correlation between vessel density and MPOD. | FR |
*Abbreviations: RCT = Randomized Control Trial, CS = Cross-sectional, DR = Diabetic retinopathy, L = Lutein, Z = Zeaxanthin, MZ = Meso-zeaxanthin, BCVA = Best Corrected Visual Acuity, T1D = Type 1 diabetic, T2D = Type 2 diabetic, HFP = Heterochromatic flicker photometry, DWA = Dual-wavelength autofluorescence, FR = Fundus Reflectance.
Table 5.
Cross-sectional and randomized control trial studies examining the relationship between MPOD and Visual Function
Table 5.
Cross-sectional and randomized control trial studies examining the relationship between MPOD and Visual Function
| Author (Year) | Study Design | Demographic | Sample Size | Interventions | Duration | Relation between MPOD and Visual Function | MPOD Technique |
|---|---|---|---|---|---|---|---|
| Stringham (2011) [86] | CS | Adults 23-50; BCVA ≤20/25. | 26 | None | N/A | MPOD was associated with faster photo stress recovery, lower disability glare thresholds, and reduced visual discomfort. | HFP |
| Engles (2007) [91] | CS | Adults 18-40; BCVA ≤20/40. | 80 | None | N/A | No significant correlation found between MPOD and measures of visual acuity. | HFP |
| Tudosescu (2018) [92] | CS | Adults 18-65 years; BCVA ≤20/125. | 83 | None | N/A | No significant correlation between MPOD and blue-light exposure from computers, iris color, refractive errors, or glare sensibility was found. | HFP |
| Patryas (2014) [93] | CS | Adults 18-68 years; BCVA ≤20/32. | 33 | None | N/A | MPOD was weakly associated with rod-mediated recovery, not with cone-mediated recovery. | HFP |
| Bovier (2014) [94] | RCT | Adults 18-32 years; BCVA ≤20/60. | 92 | Group 1: Z - 20mg Group 2: Mixed (Z - 26mg, L - 8mg, Omega-3 - 190mg) Group 3: Placebo |
4 months | MPOD increased with supplementation and led to significant improvements in visual processing speed and motor reaction time. | HFP |
| Kvansakul – (2006) [95] | RCT | Adults 18-40 years; BCVA ≤20/60. | 92 | Group 1: L - 10mg Group 2: Z - 10mg Group 3: Combination (L - 10mg, Z - 10mg) Group 4: Placebo |
12 months | Supplementation with L or Z increases MPOD improved contrast acuity thresholds at high mesopic levels, thus enhancing visual performance at low illumination. | HFP |
| Putnam (2015) [96] | CS | Adults 18-35 years; BCVA ≤20/25. | 33 | None | N/A | Increased MPOD correlates with reduced glare disability, significantly at higher spatial frequencies. | HFP |
| Stringham (2008) [97] | RCT | Adults 17-41 years. | 40 | Group 1: L - 10mg, Z - 2mg Group 2: Placebo |
6 months | Supplementation led to increased MPOD, which significantly improved performance in glare disability and photostress recovery tasks. | HFP |
| Stringham (2017) [98] | RCT | Adults 18–25 years. | 59 | Group 1: L - 6mg and Z - 6mg Group 2: L - 12mg and Z - 12mg Group 3: Placebo |
12 months | Increases in MPOD led to improved contrast sensitivity | HFP |
| Nolan (2016) [99] | RCT | Adults with mean age of 21.5 years. | 105 | Group 1: L - 10 mg, Z - 2mg, and MZ - 10 mg Group 2: Placebo |
12 months | MPOD increased with supplementation and was significantly correlated with improvements in contrast sensitivity in the active group compared to placebo. | DWA |
| Hammond (2014) [100] | RCT | Adults 20-40 years. | 115 | Group 1: L - 10mg, Z - 2mg. Group 2: Placebo |
12 months | Supplementation increased MPOD significantly, improving chromatic contrast and photostress recovery time, but glare disability improvements were not statistically significant. | HFP |
| Hammond Jr (2013) [101] | CS | Adults 20-40 years. | 150 | None | N/A | MPOD density significantly correlated with positive outcomes in glare disability, photostress recovery time, and chromatic contrast thresholds. | HFP |
| Stringham (2016) [102] | RCT | Adults 18-25 years, BCVA ≤20/20. | 59 | Group 1: L - 10mg + Z - 2mg. Group 2: L - 20mg + Z - 4mg. Group 3: Placebo |
12 months | Supplementation led to significant increases in MPOD, which in turn resulted in improvements in photostress recovery, and disability glare. | HFP |
| Hammond Jr. (1998) [103] | CS | Adults 60-84 years; ≤20/32 visual acuity. | 37 | None | N/A | Higher MPOD was associated with preserved visual sensitivity in older ages. | HFP |
| Estévez-Santiago (2016) [104] | CS | Adults 20-35 and 45-65 years; BCVA ≤20/20. | 108 | None | N/A | Contrast threshold inversely correlated with MPOD, particularly in the older group. | HFP |
| Nolan (2011) [105] | RCT | Adults 18-41 years; BCVA ≤20/20. | 121 | Group 1: L - 12mg + Z - 1mg. Group 2: Placebo. |
12 months | Statistically significant increase in MPOD in the active group was not generally associated with improvement in visual performance. | HFP |
| Loughman (2010) [106] | CS | Adults 18-41 years; BCVA ≤20/20. | 142 | None | N/A | MPOD was positively associated with BCVA and contrast sensitivity, while photostress recovery and glare sensitivity were unrelated to MPOD. | HFP |
*Abbreviations: RCT = Randomized Control Trial, CS = Cross-sectional, L = Lutein, Z = Zeaxanthin, MZ = Meso-zeaxanthin, BCVA = Best Corrected Visual Acuity, HFP = Heterochromatic flicker photometry, DWA = Dual-wavelength autofluorescence.
Table 6.
Cross-sectional and randomized control trial studies examining the relationship between MPOD and Cognitive Function.
Table 6.
Cross-sectional and randomized control trial studies examining the relationship between MPOD and Cognitive Function.
| Author (Year) | Study Design | Inclusion Criteria | Sample Size | Intervention(s) | Duration | Relation between MPOD and Cognitive Function | MPOD Technique |
|---|---|---|---|---|---|---|---|
| Khan (2018) [112] | CS | Adults 25-45 years with BMI ≥ 25 kg/m². | 114 | None | N/A | MPOD positively associated with IQ and fluid intelligence, but not with crystallized intelligence | HFP |
| Saint (2018) [113] | CS | Children 7-13 years. | 51 | None | N/A | MPOD positively associated with reasoning skills and executive mental processes | HFP |
| Renzi-Hammond (2017) [114] | RCT | Adults 18-30 years. | 51 | Group 1: L (10mg) + MZ (2mg). Group 2: Placebo |
1 year | MPOD positively associated with improvements in spatial memory, reasoning ability, and complex attention tasks | HFP |
| Barnett (2018) [115] | CS | Preadolescent children 8-9 years. | 56 | None | N/A | MPOD positively associated with overall academic achievement, mathematics, and written language | HFP |
| Lindbergh (2018) [116] | RCT | Adults 64-86 years. | 44 | Group 1: L (10mg) + MZ (2mg). Group 2: Placebo |
1 year | L and Z supplementation increased MPOD and was associated with enhanced signals in prefrontal regions, suggesting a potential mechanism for improved cognitive performance | HFP |
| Kelly (2015) [117] | CS | Group 1: Adults 35-74 years with low MPOD, Group 2: Adults 35-74 years with early AMD. | 226 | None | N/A | MPOD positively associated with phonemic fluency, attention switching, visual and verbal memory, and learning | HFP and DWA |
| Power (2018) [118] | RCT | Adults 33-57 years with low MPOD. | 91 | Group 1: L (10mg) + MZ (10mg) + Z (2mg). Group 2: Placebo |
12 months | Supplementation improved MPOD which positively associated with episodic memory and overall cognitive function | DWA |
| Ajana (2018) [119] | CS | Adults 75-93 years with low MPOD. | 184 | None | N/A | Higher MPOD significantly associated with better global cognitive performance, visual memory, and verbal fluency | DWA |
| Vishwanathan (2014) [120] | CS | Adults 75-80 years. | 108 | None | N/A | MPOD levels significantly positively associated with better global cognition, verbal learning and fluency, recall, processing speed, and perceptual speed | HFP |
| Renzi (2014) [121] | CS | Adults 65-83 years with mild cognitive impairment. | 53 | None | N/A | In unimpaired adults, higher MPOD was associated with better visuospatial and constructional abilities. In mildly impaired adults, higher MPOD was associated with better performance in multiple cognitive domains including memory, language, and attention | HFP |
| Feeney (2013) [122] | CS | Adults 50+ years. | 4453 | None | N/A | Lower MPOD was associated with poorer performance on the MMSE and MoCA, prospective memory, and executive function | HFP |
| Stringham (2019) [123] | RCT | Adults 18-25 years. | 59 | Group 1: MZ (13 mg), Group 2: MZ (27 mg), Group 3: Placebo. |
6 months | Supplementation improved cognitive performance in composite memory, verbal memory, sustained attention, psychomotor speed, and processing speed | HFP |
| Hassevoort (2017) [124] | CS | Children 7-10 years. | 40 | None | N/A | MPOD negatively associated with relational memory errors | HFP |
| Edwards (2019) [125] | CS | Adults 25-45 years with BMI ≥ 25 kg/m². | 101 | None | N/A | MPOD positively associated with improvements attentional resource allocation and information processing speed | HFP |
| Mewborn (2018) [126] | CS | Adults 64-77 years. | 51 | None | N/A | Higher MPOD positively associated with better neural efficiency in visual–spatial processing | HFP |
*Abbreviations: RCT = Randomized Control Trial, AMD = Age-related Macular Degeneration, L = Lutein, Z = Zeaxanthin, MZ = Meso-zeaxanthin, BCVA = Best Corrected Visual Acuity, MMSE = Mini-mental state examination, MoCA = Montreal cognitive assessment, HFP = Heterochromatic flicker photometry, DWA = Dual-wavelength autofluorescence.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



