
Submitted:
28 June 2024
Posted:
29 June 2024
You are already at the latest version
Abstract
Background and Objectives: Recent studies have focused on the association between the risk of diabetic retinopathy (DR) and rs1501299 and rs2241766 polymorphisms of the ADIPOQ gene, whereas their results remain inconclusive. Thus, a systematic review and meta-analysis was car-ried out to clarify the role of these polymorphisms in the development of DR.
Materials and Methods: A systematic research of electronic databases (PubMed, Scopus, and Cochrane Library) was conducted until June 16, 2023, and a reference list of relevant articles was collected, which explored the association between rs1501299 and rs2241766 polymorphisms of the ADIPOQ gene and the risk of DR. The pooled odds ratios (OR) and 95% confidence intervals (CI) were estimated via random-effects model and the meta-analysis was implemented by using Review Manager 5.4.
Results: In total, 6 out of 178 studies, with 1,888 cases (DR) and 2,285 controls (without DR), were included in the meta-analysis. A statistically significant association between rs1501299 poly-morphism and DR risk was recorded in G vs. T in the overall analysis (OR=0.84, 95% CI=0.72-0.99, p=
Keywords:
Diabetic retinopathy
; Adiponectin gene
; ADIPOQ gene
; rs2241766
; rs1501299
1. Introduction
Diabetic retinopathy (DR) is a common microvascular and neurodegenerative complication of diabetes mellitus (DM) and remains the leading cause of preventable vision loss in working-aged people (20-74 years) in developed countries [1]. To date, 3 out of 4 people with DM have signs of DR after 15 years of disease duration, reaching 93 million worldwide, while an increase in these cases by 150% is expected by 2040 [2]. According to the severity of the disease, DR is classified into non-proliferative diabetic retinopathy (NPDR) and proliferative diabetic retinopathy (PDR). The signs of NPDR include microaneurysms, cotton wool spots, hard exudates, intraretinal vascular abnormalities and venous beading and this condition can progressively develop into PDR, which is characterized by neovascularization and preretinal or vitreous hemorrhage [3]. As a matter of fact, DR is harmful for individuals and society due to the imposed health, psychological and financial burdens [4].
The etiopathogenesis of DR has been studied thoroughly [5,6], but the precise underlying mechanisms have not been clarified and the currently available therapies are insufficient to prevent or minimize the ocular complications of DM [7]. The main risk factors are DM duration and poor glycemic control, while several other risk factors have been identified, including the presence of arterial hypertension, dyslipidemia, obesity, cardiovascular disease, stroke, nephropathy, smoking, pregnancy, anemia, and cataract surgery [8]. In addition, the prevalence of DR varies significantly between different ethnicity groups and is higher in people with type 1 DM (T1DM) rather than type 2 DM (T2DM), due to the longer duration of the disease [9]. However, there is an important variation in DR risk and the complexity of the disease may be explained by genetic factors, such as gene mutations and abnormal expression, which play a significant role in the onset and progression of DR [10].
Adiponectin, a product of the ADIPOQ human gene, is expressed in adipose tissue and modulates sundry metabolic processes, including glucose regulation and lipid metabolism [11]. This adipokine exerts anti-inflammatory and anti-atherogenic effects, as it can prevent vascular remodeling by inhibiting the proliferation and migration of smooth muscle cells and it can reduce the Tumor Necrosis Factor-a (TNF-a) production to modulate the inflammatory response of endothelial cells In fact, adiponectin can protect the vasculature through its pleiotropic actions on endothelial progenitor cells, endothelial cells, macrophages and smooth muscle cells and it may prevent injury and dysfunction of endothelial cells. The ADIPOQ gene is located on chromosome 3q27 and consists of 3 exons and 2 introns, spanning a 17 kb region [12]. Genetic polymorphisms of this gene may affect the plasma adiponectin levels, and their contribution to the occurrence of DR [13]. Two common single nucleotide polymorphisms (SNPs) in the ADIPOQ gene locus at 276G/T (rs1501299) and 45T/G (rs2241766) have been studied in different ethnic groups and have been found to be associated with T2DM and its complications [14,15,16,17].
Many studies have been carried out to investigate the association between these two SNPs and the risk of DR, but their results were conflicting and inconclusive [18,19,20,21,22,23]. Thus, the aim of this systematic review and meta-analysis is to investigate the association between ADIPOQ polymorphisms rs1501299 and rs2241766 and the development of DR.
2. Materials and Methods
This study was conducted according to a predetermined protocol, which was registered in PROSPERO on 21/09/2022 (ID: CRD42022361770). This systematic review and meta-analysis was performed based on the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines [24]. Study identification and selection, data extraction and quality assessment were carried out independently by two researchers (K. F. and G. M.) and disagreement was settled through discussion. If no consensus was reached, a third researcher made the ultimate decision (G. K.).
2.1. Search Strategy
The online databases of PubMed, Scopus, and Cochrane Library were searched up to June 25, 2024, for all potentially relevant publications in English on the association between ADIPOQ rs2241766 and rs1501299 gene polymorphisms and DR risk. The following algorithm was used for searching: “(Adiponectin OR ADIPOQ) AND (rs2241766 OR rs1501299 OR polymorphism OR single nucleotide polymorphism OR SNP OR variant OR variation OR mutation) AND (Diabetic microangiopathy OR Diabetic retinopathy OR DR)”. The reference list of the retrieved articles was hand-searched.
2.2. Eligibility Criteria
The included studies consisted of case-control and cohort studies on the association between ADIPOQ rs1501299 and rs2241766 gene polymorphisms and DR development and had sufficient published data to estimate an odds ratio (OR) and 95% confidence intervals (95% CI) for each allele or genotype. The genotype distribution of these polymorphisms was determined in cases of diabetic retinopathy of any grade (NPDR or PDR) in T1DM or T2DM and in controls. The control group consisted of healthy controls (HC) or individuals with DM but free of DR (NDR). The study subjects were exclusively humans. A minimum number of participants for a study to be included in the meta-analysis was not defined. Furthermore, all participants of the included studies have provided informed consent for their participation in the original studies and these studies have been approved by the ethics committees of the participating institutions.
The exclusion criteria were: (1) reviews, editorials, abstracts, case reports, animal studies, (2) studies with inadequate or overlapping data on allele and genotype frequencies, (3) studies in which the genotype distribution of the controls deviated from Hardy-Weinberg equilibrium (HWE).
HWE of the genotype distribution of the controls was tested through a χ2 analysis and a p-value>0.05 suggested that the study sample was representative of the population [25].
2.3. Data Extraction
After the selection process, data was extracted regarding the following characteristics of the included articles: name of the first author, year of publication, country, ethnicity of population, study design, genotyping method, DM type, control type, demographic/clinical characteristics, and sample sizes of cases and controls for ADIPOQ rs1501299 and rs2241766 genotypes. The allele frequencies and the genotypic distribution were calculated or extracted for both the case and control group. Moreover, the minor allele frequency (MAF) for ADIPOQ rs1501299 and rs2241766 polymorphisms was calculated, and it was examined whether the distribution of genotypes in the control group in each study was consistent with Hardy-Weinberg equilibrium (HWE) [26].
2.4. Quality Assessment
The Newcastle-Ottawa Scale (NOS) was used to evaluate the quality of the included observational studies. The NOS consists of 3 parts: selection (4 entries), comparability (1 entry) and exposure (3 entries) for case-control studies and selection (4 entries), comparability (1 entry) and outcome (3 entries) for cohort studies. Each entry receives only one star for a quality item in selection and exposure/outcome parts and a maximum of two stars is awarded in the comparability part for each study. The NOS is a semi-quantitative scale, and the score ranges from 0 (worst) to 9 (best) stars for each included study. Studies with 7 or more stars are considered to be of relatively high quality [27].
2.5. Statistical Analysis
The meta-analysis was conducted using Review Manager 5.4 (The Cochrane Collaboration, Oxford, UK). The following genotype contrasts were assessed for the ADIPOQ rs1501299 polymorphism: homozygotes GG versus a combination of GT and TT [GG vs. (GT + TT), dominant model], a combination of GG and GT versus TT [(GG + GT) vs. TT, recessive model], GG versus TT, GT versus TT, GG versus GT and a combination of GG and TT versus GT [(GG + TT) vs GT, over-dominant model]. The G allelic frequency versus the T allelic frequency was also examined (G versus T). In addition, for the ADIPOQ rs2241766 polymorphism the following genotype contrasts were evaluated: TT versus a combination of TG and GG [TT vs. (TG + GG), dominant model], a combination of TT and TG versus GG [(TT + TG) vs. GG, recessive model], TT versus GG, TG versus GG, TT versus TG, a combination of TT and GG versus TG [(TT + GG) vs GT, over-dominant model], and T allele versus G allele [28].
The summary odds ratio and 95% confidence interval were estimated via random-effects DerSimonian-Laird model [29]. Heterogeneity was assessed through the χ2-based Q statistic test, and it was considered statistically significant for p-value<0.05. The degree of heterogeneity was quantified by the I2 metric which ranges from 0% to 100%, with higher values indicating a greater degree of between-study variability that can be attributed to heterogeneity. Furthermore, subgroup analyses by ethnicity and control type were performed. Additionally, meta-regression analyses were performed to identify the sources of heterogeneity if at least 10 studies were available. Sensitivity analysis was used to examine the stability of the results by gradually removing the included studies one by one. The potential publication bias was assessed using the Begg adjusted rank correlation test and the Egger regression asymmetry test if at least 10 studies were available. Statistical significance was set at p-value<0.05 and all p-values were two-sided [30].
3. Results
3.1. Literature Search
The process of the study selection is presented in Figure 1. In the initial search, a total of 182 citations were identified. After the exclusion of 5 duplicates, another 177 citations were excluded based on title and abstract screening, since they did not meet the inclusion criteria. Then 11 full-text articles were assessed for eligibility and 5 citations were excluded [31,32,33,34,35]. Finally, a total of 6 publications were included in the systematic review involving a total of 1,888 patients and 2,285 controls, 5 of which investigated rs1501299 polymorphism with 1,014 cases and 1,234 controls [18,19,21,22,23], and 4 of which explored rs2241766 polymorphism with 874 and 1,051 respectively [19,20,21,22].
3.2. Study Characteristics and Summary Statistics
The eligible study characteristics and the genotype and allelic distribution of ADIPOQ rs1501299 and rs2241766 SNPs are shown in Table 1. All studies were based on T2DM and in 4 of them the population was Asian [20,21,22,23], while in the other 2 the population was Caucasian [18,19]. All studies had case-control study design [18,19,20,22,23], except for 1 that had a cohort study design [21]. Also, in 1 study the control group consisted of healthy participants [18], in 3 studies consisted of participants with T2DM but without signs of DR (NDR) [19,21,22], and, finally, in 2 studies there were both healthy participants and NDR [20,23], thus two different associations were investigated.
The NOS scores of the included studies ranged from 6 to 8, with a median of 7 (Table 1). Five studies were considered of high-quality [18,19,21,22,23], while the other was of mediocre quality [20]. All studies indicated that the distribution of genotypes in the control group was consistent with HWE (Table 1).

Table 1.
Characteristics of the included studies on ADIPOQ gene polymorphisms and diabetic retinopathy risk.
Table 1.
Characteristics of the included studies on ADIPOQ gene polymorphisms and diabetic retinopathy risk.
| First Author | Year of Publication | Country/Ethnicity | Study Design | Genotyping Method | Control Type | Type of DM | DR grade | Case | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Sample Size | Sex (M/F) | Age (years) | ||||||||
| Aioanei | 2021 | Romania/Caucasian | Case–Control | PCR-RFLP | HC | T2DM | NPDR | 198 | 105/93 | 68.72 ± 11.58 |
| Choe | 2013 | Korea/Asian | Cohort Study | PCR-RFLP | NDR | T2DM | Any DR | 231 | N/A | N/A |
| Gouliopoulos | 2022 | Greece/Caucasian | Case–Control | PCR-RFLP | NDR | T2DM | Any DR | 109 | 74/35 | 67.00 ± 8.00 |
| Li | 2015 | China/Asian | Case–Control | PCR-RFLP | NDR | T2DM | Any DR | 372 | 146/226 | 63.39 ± 10.60 |
| Yoshioka | 2004 | Japan/Asian | Case–Control | PCR-RFLP | HC+NDR | T2DM | Any DR | 104 | 55/49 | 62.05 ± 9.20 |
| Choe | 2013 | Korea/Asian | Cohort Study | PCR-RFLP | NDR | T2DM | Any DR | 225 | N/A | N/A |
| Gouliopoulos | 2022 | Greece/Caucasian | Case–Control | PCR-RFLP | NDR | T2DM | Any DR | 109 | 74/35 | 67.00 ± 8.00 |
| Li | 2015 | China/Asian | Case–Control | PCR-RFLP | NDR | T2DM | Any DR | 372 | 146/226 | 63.39 ± 10.60 |
| Sikka | 2014 | India/Asian | Case–Control | PCR-RFLP | HC+NDR | T2DM | Any DR | 169 | N/A | 58.35 ± 9.01 |
Table 1.
(Continue). Characteristics of the included studies on ADIPOQ gene polymorphisms and diabetic retinopathy risk.
Table 1.
(Continue). Characteristics of the included studies on ADIPOQ gene polymorphisms and diabetic retinopathy risk.
| First Author | Control | Genotype distribution | HWE p-value |
MAF | NOS (Stars) |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sample Size | Sex (M/F) | Age (years) | Case | Control | Control | Case | Control | ||||||
| rs1501299 G/T | |||||||||||||
| GG | GT | TT | GG | GT | TT | ||||||||
| Aioanei | 200 | 143/57 | 58.10 ± 9.00 | 93 | 79 | 26 | 92 | 88 | 20 | 0.876 | 0.33 | 0.32 | 7 |
| Choe | 440 | N/A | N/A | 109 | 102 | 20 | 222 | 178 | 40 | 0.616 | 0.31 | 0.29 | 7 |
| Gouliopoulos | 109 | 75/34 | 66.00 ± 9.00 | 40 | 58 | 11 | 59 | 37 | 13 | 0.069 | 0.37 | 0.29 | 7 |
| Li | 145 | 49/96 | 62.34 ± 10.75 | 164 | 169 | 39 | 82 | 55 | 8 | 0.756 | 0.33 | 0.24 | 8 |
| Yoshioka | 340 | 219/121 | 59.70 ± 10.10 | 50 | 42 | 12 | 163 | 147 | 30 | 0.699 | 0.32 | 0.30 | 7 |
| rs2241766 T/G | |||||||||||||
| TT | TG | GG | TT | TG | GG | ||||||||
| Choe | 442 | N/A | N/A | 111 | 96 | 18 | 213 | 194 | 35 | 0.315 | 0.29 | 0.30 | 7 |
| Gouliopoulos | 109 | 75/34 | 66.00 ± 9.00 | 84 | 23 | 2 | 74 | 32 | 3 | 0.836 | 0.12 | 0.17 | 7 |
| Li | 145 | 49/96 | 62.34 ± 10.75 | 206 | 140 | 25 | 82 | 53 | 10 | 0.720 | 0.26 | 0.25 | 8 |
| Sikka | 355 | N/A | 53.16 ±12.15 | 158 | 9 | 2 | 292 | 58 | 5 | 0.285 | 0.04 | 0.09 | 6 |
ADD Abbreviations: DM, Diabetes Mellitus; DR, Diabetic retinopathy; T2DM, Type 2 Diabetes Mellitus; NPDR, Non-Proliferative Diabetic Retinopathy; HC, Healthy Controls; NDR, Non-Diabetic Retinopathy Diabetes Mellitus, PCR-RFLP, Polymerase Chain Reaction – Restriction Fragment Length Polymorphism; M, Male; F, Female; HWE, Hardy-Weinberg Equilibrium, MAF, Minor Allele Frequency, NOS, Newcastle – Ottawa Scale; N/A, Not Available.
3.3. Quantitative and Subgroup Analyses
3.3.1. Association between rs1501299 Polymorphism and DR Risk
The estimated results of the association between rs1501299 polymorphism and DR risk are shown in Table 2. In the overall analysis, a statistically significant association was observed in G vs. T (OR=0.84, 95% CI=0.72-0.99, p<0.05) (Figure 2) and a sensitivity analysis through deletion of one study at a time was conducted to reflect the influence of the individual dataset to the pooled OR and a minor change was observed when excluding the studies (Figure 3). The other genetic comparisons reported no significant difference.
Subgroup analysis was performed according to ethnicity and control type. The results of the analysis performed on Asian populations showed no statistically significant association in any genetic model, as well as on Caucasian populations (Table 2).
The pooled results in DR versus DM control type revealed a statistically significant association in G vs. T: OR=0.81, 95% CI= 0.67-0.97, p=<0.05; GG vs. GT: OR=0.72, 95% CI=0.53-0.98, p=<0.05; GG vs. (GT + TT): OR=0.73, 95% CI=0.55-0.96, p=<0.05 (Figure 4). The other genetic models in this analysis presented no significant association. The pooled results in DR versus HC showed no significant association in any genetic model (Table 2).
3.3.2. Association between rs2241766 Polymorphism and DR Risk
Furthermore, the pooled results indicated a non-association between rs2241766 ADIPOQ gene polymorphism and susceptibility to DR in the overall or subgroup analyses (ethnicity, control type) in any genetic model (Table 3). However, the Caucasian population subgroup and the DR versus HC subgroup consisted of 1 study each, hence meta-analysis was not feasible.
4. Discussion
The present meta-analysis of 5 studies for the rs1501299 polymorphism, including 1,014 cases and 1,234 controls, provided an elucidative analysis on the association of this SNP with DR risk. The results indicated that the rs1501299 polymorphism demonstrated a statistically significant association with DR risk in the overall studied population in the allelic contrast, probably since the minor allele (T) is associated with a decrease in plasma adiponectin levels [13]. This estimate is consistent with all the included studies in the meta-analysis [18,19,21,22,23]. Hence, it is possible that the rs1501299 polymorphism plays a role in the development of DR. In the subgroup analysis according to ethnicity, no significant association was recorded in Asian and Caucasian populations in all genetic models, due to the small sample especially in the second case, presenting that the genetic background and the environment play no role in the association between rs1501299 polymorphism and DR risk. As a result, further studies are needed to examine whether the rs1501299 polymorphism may confer a risk of DR between different ethnicities.
In the subgroup analysis according to the control type, statistically significant associations were observed, when the control group was consisted of patients with DM but without signs DR, in the allelic contrast, in the dominant genetic model and in GG vs.GT. This may take place because a comparison between a group with DR and a group with DM but without DR may reduce the confounding factor of the common background disease and possibly uncover any responsible genetic predisposition [19,21,22,23]. Thus, the presence of the T allele in the genotype increases the risk of DR, when a patient is suffering from DR and this SNP may be used as a target for intervention, contributing to new and safe gene therapies.
The meta-analysis of 4 studies for the rs2241766 polymorphism of the ADIPOQ gene, including 874 cases and 1,051 controls, found no statistically significant association with the risk of DR, in the overall or the subgroup analyses, in any genetic model. This may be partly explained due to the small number of included studies and the relatively small sample sizes. The leave-one-out sensitivity analyses showed that the results were stable and unaffected by single studies.
DR is the most serious ocular complication of DM and is the most common vascular disease of the retina, that can lead to vision loss if left untreated [36,37]. The prevalence of DR varies depending on several factors, such as genetic background and the duration of diabetes and the level of glycemic control [38]. The global prevalence of diabetic retinopathy among people with diabetes is estimated to be around 27%, with the highest prevalence rates reported in low- and middle-income countries due to late diagnoses of DM leading to untreated disease [39].
Previous studies documented that rs1501299 GT genotype could be recognized as an independent risk factor of DR, while no association between rs2241766 and DR was identified in a Caucasian population [19]. On the other hand, a higher risk of DR is indicated in rs2241777 TT genotype in an Asian population [20]. Hence, a systematic review and meta-analysis was carried out to elucidate the association between ADIPOQ polymorphisms rs1501299 in intron 2 and rs2241766 in exon 2 and DR risk.
In previous studies, the rs1501299 polymorphism of the ADIPOQ gene has been correlated with T2DM, cardiovascular diseases, metabolic syndrome, hepatocellular carcinoma, and endometrial cancer [40,41,42,43,44]. The rs2241766 genetic polymorphism has been associated with T2DM, hypercholesterolemia, obesity, metabolic syndrome, and cardiovascular diseases [41,45,46,47,48,49]. In fact, these two SNPs are associated with the background disease and with risk factors of DR, contributing, also, indirectly to the onset of DR. Therefore, their targeted intervention may reduce the burden of the disease for the patient and for the health system, through effective and efficient gene therapy.
This study had some limitations that should be taken into consideration when interpreting the results. Firstly, only published studies in English were included in the quantitative analysis, while potential studies in other languages could have been omitted. However, most studies were in Asian populations, so the potential for missing studies is reduced. Secondly, the meta-analysis was based predominantly on Asian studies, while only 2 studies of Caucasian population were included and no study from other part of the world was identified and the number of study participants was limited. Consequently, this may hinder the generalizability of the results, whereas sub-group analysis based on the ethnicity of the participants was conducted and the OR did not differ significantly. Thirdly, confounding exogenous factors such as, age, sex and lifestyle factors were not adjusted in all studies, since one study matched the participants by age and gender [19], and another study matched them by ethnicity and gender [20], although their effect on the SNPs expression is of minor importance. Last but not least, the OR and 95% CI of the included studies were estimated based on the genotype distribution, since these data were not present in all of the studies. Despite these limitations, this systematic review and meta-analysis provides a better understanding of the association between rs1501299 and rs2241766 polymorphisms of the ADIPOQ gene and the risk of DR in T2DM.
5. Conclusions
To summarize, the current meta-analysis provides evidence that the rs1501299 polymorphism may be an independent risk factor for DR in patients with T2DM, while the rs2241766 polymorphism showed no association with the development of DR. Considering the limitations of this study, further larger studies with different ethnic populations are required to verify these findings.
Author Contributions
Conceptualization: K.F. and M.M.; methodology: G.M. and K.T.; software: G.M.; validation: K.F., G.M. and G.K.; formal analysis: A.C.; investigation: K.F.; data curation: M.G.; writing—original draft preparation, K.F.; writing—review and editing, K.F. and G.M.; supervision: M.M. and G.K.; project administration, K.T. and G.K.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
Data available upon request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Cheung, N.; Mitchell, P.; Wong, T. Y. Diabetic Retinopathy. Lancet (London, England) 2010, 376 (9735), 124–136. [CrossRef]
- Sabanayagam, C.; Banu, R.; Chee, M. L.; Lee, R.; Wang, Y. X.; Tan, G.; Jonas, J. B.; Lamoureux, E. L.; Cheng, C.-Y.; Klein, B. E. K.; Mitchell, P.; Klein, R.; Cheung, C. M. G.; Wong, T. Y. Incidence and Progression of Diabetic Retinopathy: A Systematic Review. lancet. Diabetes Endocrinol. 2019, 7 (2), 140–149. [CrossRef]
- Heng, L. Z.; Comyn, O.; Peto, T.; Tadros, C.; Ng, E.; Sivaprasad, S.; Hykin, P. G. Diabetic Retinopathy: Pathogenesis, Clinical Grading, Management and Future Developments. Diabet. Med. 2013, 30 (6), 640–650. [CrossRef]
- Vujosevic, S.; Aldington, S. J.; Silva, P.; Hernández, C.; Scanlon, P.; Peto, T.; Simó, R. Screening for Diabetic Retinopathy: New Perspectives and Challenges. Lancet Diabetes Endocrinol. 2020, 8 (4), 337–347. [CrossRef]
- Capitão, M.; Soares, R. Angiogenesis and Inflammation Crosstalk in Diabetic Retinopathy. J. Cell. Biochem. 2016, No. April 2016, 2443–2453. [CrossRef]
- Ghamdi, A. H. Al. Clinical Predictors of Diabetic Retinopathy Progression; A Systematic Review. Curr. Diabetes Rev. 2019, 16 (3), 242–247. [CrossRef]
- Simó-Servat, O.; Hernández, C.; Simó, R. Diabetic Retinopathy in the Context of Patients with Diabetes. Ophthalmic Res. 2019, 62 (4), 211–217. [CrossRef]
- Lin, K.-Y.; Hsih, W.-H.; Lin, Y.-B.; Wen, C.-Y.; Chang, T.-J. Update in the Epidemiology, Risk Factors, Screening, and Treatment of Diabetic Retinopathy. J. Diabetes Investig. 2021, 12 (8), 1322–1325. [CrossRef]
- Fung, T. H.; Patel, B.; Wilmot, E. G.; Amoaku, W. M. Diabetic Retinopathy for the Non-Ophthalmologist. Clin. Med. 2022, 22 (2), 112–116. [CrossRef]
- Sharma, A.; Valle, M. L.; Beveridge, C.; Liu, Y.; Sharma, S. Unraveling the Role of Genetics in the Pathogenesis of Diabetic Retinopathy. Eye 2019, 33 (4), 534–541. [CrossRef]
- Xian, L.; He, W.; Pang, F.; Hu, Y. ADIPOQ Gene Polymorphisms and Susceptibility to Polycystic Ovary Syndrome: A HuGE Survey and Meta-Analysis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 161 (2), 117–124. [CrossRef]
- Han, Q.; Geng, W.; Zhang, D.; Cai, G.; Zhu, H. ADIPOQ Rs2241766 Gene Polymorphism and Predisposition to Diabetic Kidney Disease. J. Diabetes Res. 2020, 2020, 5158497. [CrossRef]
- Fang, H.; Judd, R. L. Adiponectin Regulation and Function. Compr. Physiol. 2018, 8 (3), 1031–1063. [CrossRef]
- Al-Nbaheen, M. S. Effect of Genetic Variations in the ADIPOQ Gene on Susceptibility to Type 2 Diabetes Mellitus. Diabetes. Metab. Syndr. Obes. 2022, 15, 2753–2761. [CrossRef]
- Alfaqih, M. A.; Al-Hawamdeh, A.; Amarin, Z. O.; Khader, Y. S.; Mhedat, K.; Allouh, M. Z. Single Nucleotide Polymorphism in the ADIPOQ Gene Modifies Adiponectin Levels and Glycemic Control in Type Two Diabetes Mellitus Patients. Biomed Res. Int. 2022, 2022. [CrossRef]
- Chung, H. F.; Long, K. Z.; Hsu, C. C.; Mamun, A. Al; Chiu, Y. F.; Tu, H. P.; Chen, P. S.; Jhang, H. R.; Hwang, S. J.; Huang, M. C. Adiponectin Gene (ADIPOQ) Polymorphisms Correlate with the Progression of Nephropathy in Taiwanese Male Patients with Type 2 Diabetes. Diabetes Res. Clin. Pract. 2014, 105 (2), 261–270. [CrossRef]
- Isakova, J.; Talaibekova, E.; Vinnikov, D.; Saadanov, I.; Aldasheva, N. ADIPOQ, KCNJ11 and TCF7L2 Polymorphisms in Type 2 Diabetes in Kyrgyz Population: A Case-Control Study. J. Cell. Mol. Med. 2019, 23 (2), 1628–1631. [CrossRef]
- Aioanei, C. S.; Ilies, R. F.; Bala, C.; Petrisor, M. F.; Porojan, M. D.; Popp, R. A.; Catana, A. The Role of Adiponectin and Toll-like Receptor 4 Gene Polymorphisms on Non-Proliferative Retinopathy in Type 2 Diabetes Mellitus Patients. A Casecontrol Study in Romanian Caucasians Patients. Acta Endocrinol. (Copenh). 2019, 15 (1), 32–38. [CrossRef]
- Gouliopoulos, N.; Siasos, G.; Bouratzis, N.; Oikonomou, E.; Kollia, C.; Konsola, T.; Oikonomou, D.; Rouvas, A.; Kassi, E.; Tousoulis, D.; Moschos, M. M. Polymorphism Analysis of ADIPOQ Gene in Greek Patients with Diabetic Retinopathy. Ophthalmic Genet. 2022, 43 (3), 326–331. [CrossRef]
- Sikka, R.; Raina, P.; Matharoo, K.; Bandesh, K.; Bhatia, R.; Chakrabarti, S.; Bhanwer, A. J. S. TNF-α (g.-308 G > A) and ADIPOQ (g. + 45 T > G) Gene Polymorphisms in Type 2 Diabetes and Microvascular Complications in the Region of Punjab (North-West India). Curr. Eye Res. 2014, 39 (10), 1042–1051. [CrossRef]
- Choe, E. Y.; Wang, H. J.; Kwon, O.; Kim, K. J.; Kim, B. S.; Lee, B. W.; Ahn, C. W.; Cha, B. S.; Lee, H. C.; Kang, E. S.; Mantzoros, C. S. Variants of the Adiponectin Gene and Diabetic Microvascular Complications in Patients with Type 2 Diabetes. Metabolism. 2013, 62 (5), 677–685. [CrossRef]
- Li, Y.; Wu, Q. H.; Jiao, M. L.; Fan, X. H.; Hu, Q.; Hao, Y. H.; Liu, R. H.; Zhang, W.; Cui, Y.; Han, L. Y. Gene-Environment Interaction between Adiponectin Gene Polymorphisms and Environmental Factors on the Risk of Diabetic Retinopathy. J. Diabetes Investig. 2015, 6 (1), 56–66. [CrossRef]
- Yoshioka, K.; Yoshida, T.; Takakura, Y.; Umekawa, T.; Kogure, A.; Toda, H.; Yoshikawa, T. Adiponectin Gene Polymorphism (G276T) and Diabetic Retinopathy in Japanese Patients with Type 2 Diabetes. Diabetic medicine : a journal of the British Diabetic Association. England October 2004, pp 1158–1159. [CrossRef]
- Page, M. J.; McKenzie, J. E.; Bossuyt, P. M.; Boutron, I.; Hoffmann, T. C.; Mulrow, C. D.; Shamseer, L.; Tetzlaff, J. M.; Akl, E. A.; Brennan, S. E.; Chou, R.; Glanville, J.; Grimshaw, J. M.; Hróbjartsson, A.; Lalu, M. M.; Li, T.; Loder, E. W.; Mayo-Wilson, E.; McDonald, S.; McGuinness, L. A.; Stewart, L. A.; Thomas, J.; Tricco, A. C.; Welch, V. A.; Whiting, P.; Moher, D. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372. [CrossRef]
- Ding, Y.; Hu, Z.; Yuan, S.; Xie, P.; Liu, Q. Association between Transcription Factor 7-like 2 Rs7903146 Polymorphism and Diabetic Retinopathy in Type 2 Diabetes Mellitus: A Meta-Analysis. Diabetes Vasc. Dis. Res. 2015, 12 (6), 436–444. [CrossRef]
- Jiao, J.; Li, Y.; Xu, S.; Wu, J.; Yue, S.; Liu, L. Association of FokI, TaqI, BsmI and ApaI Polymorphisms with Diabetic Retinopathy: A Pooled Analysis of Case-Control Studies. Afr. Health Sci. 2018, 18 (4), 891–899. [CrossRef]
- Luo, S.; Wang, F.; Shi, C.; Wu, Z. A Meta-Analysis of Association between Methylenetetrahydrofolate Reductase Gene (MTHFR) 677C/T Polymorphism and Diabetic Retinopathy. Int. J. Environ. Res. Public Health 2016, 13 (8). [CrossRef]
- Horita, N.; Kaneko, T. Genetic Model Selection for a Case-Control Study and a Meta-Analysis. Meta Gene 2015, 5, 1–8. [CrossRef]
- DerSimonian, R.; Laird, N. Meta-Analysis in Clinical Trials. Control. Clin. Trials 1986, 7 (3), 177–188. [CrossRef]
- Li, X. F.; Jiang, G. Bin; Cheng, S. Y.; Song, Y. F.; Deng, C.; Niu, Y. M.; Cai, J. W. Association between PPAR-Γ2 Gene Polymorphisms and Diabetic Retinopathy Risk: A Meta-Analysis. Aging (Albany. NY). 2021, 13 (4), 5136–5149. [CrossRef]
- Montesanto, A.; Bonfigli, A. R.; Crocco, P.; Garagnani, P.; De Luca, M.; Boemi, M.; Marasco, E.; Pirazzini, C.; Giuliani, C.; Franceschi, C.; Passarino, G.; Testa, R.; Olivieri, F.; Rose, G. Genes Associated with Type 2 Diabetes and Vascular Complications. Aging (Albany. NY). 2018, 10 (2), 178–196. [CrossRef]
- Huang, Y. C.; Chang, Y. W.; Cheng, C. W.; Wu, C. M.; Liao, W. L.; Tsai, F. J. Causal Relationship between Adiponectin and Diabetic Retinopathy: A Mendelian Randomization Study in an Asian Population. Genes (Basel). 2021, 12 (1), 1–11. [CrossRef]
- Rudofsky, G.; Schlimme, M.; Schlotterer, A.; von Eynatten, M.; Reismann, P.; Tafel, J.; Grafe, I.; Morcos, M.; Nawroth, P.; Bierhaus, A.; Hamann, A. No Association of the 94T/G Polymorphism in the Adiponectin Gene with Diabetic Complications. Diabetes, Obes. Metab. 2005, 7 (4), 455–459. [CrossRef]
- Zietz, B.; Buechler, C.; Kobouch, K.; Neumeier, M.; Schölmerich, J.; Scäffler, A. Serum Levels of Adiponectin Are Associated with Diabetic Retinopathy and with Adiponectin Gene Mutations in Caucasian Patients with Diabetes Mellitus Type 2. Exp. Clin. Endocrinol. Diabetes 2008, 116 (9), 532–536. [CrossRef]
- Liao, W. L.; Chen, Y. H.; Chen, C. C.; Huang, Y. C.; Lin, H. J.; Chen, Y. T.; Ban, B.; Wu, C. M.; Chang, Y. W.; Hsieh, A. R.; Tsai, F. J. Effect of Adiponectin Level and Genetic Variation of Its Receptors on Diabetic Retinopathy A Case-Control Study. Med. (United States) 2019, 98 (11), 1–7. [CrossRef]
- Tan, T. E.; Wong, T. Y. Diabetic Retinopathy: Looking Forward to 2030. Front. Endocrinol. (Lausanne). 2023, 13 (January), 1–8. [CrossRef]
- Lightman, S.; Towler, H. M. A. Diabetic Retinopathy. Clin. Cornerstone 2003, 5 (2), 12–21. [CrossRef]
- Al-Shabrawey, M.; Zhang, W.; McDonald, D. Diabetic Retinopathy: Mechanism, Diagnosis, Prevention, and Treatment. Biomed Res. Int. 2015, 2015. [CrossRef]
- Stitt, A. W.; Lois, N.; Medina, R. J.; Adamson, P.; Curtis, T. M. Advances in Our Understanding of Diabetic Retinopathy. Clin. Sci. 2013, 125 (1), 1–17. [CrossRef]
- Alimi, M.; Goodarzi, M. T.; Nekoei, M. Association of ADIPOQ Rs266729 and Rs1501299 Gene Polymorphisms and Circulating Adiponectin Level with the Risk of Type 2 Diabetes in a Population of Iran: A Case-Control Study. J. Diabetes Metab. Disord. 2021, 20 (1), 87–93. [CrossRef]
- Zhao, N.; Li, N.; Zhang, S.; Ma, Q.; Ma, C.; Yang, X.; Yin, J.; Zhang, R.; Li, J.; Yang, X.; Cui, T. Associations between Two Common Single Nucleotide Polymorphisms (Rs2241766 and Rs1501299) of ADIPOQ Gene and Coronary Artery Disease in Type 2 Diabetic Patients: A Systematic Review and Meta-Analysis. Oncotarget 2017, 8 (31), 51994–52005. [CrossRef]
- De Luis, D. A.; Izaola, O.; De La Fuente, B.; Primo, D.; Ovalle, H. F.; Romero, E. Rs1501299 Polymorphism in the Adiponectin Gene and Their Association with Total Adiponectin Levels, Insulin Resistance and Metabolic Syndrome in Obese Subjects. Ann. Nutr. Metab. 2017, 69 (3–4), 226–231. [CrossRef]
- Cai, X.; Gan, Y.; Fan, Y.; Hu, J.; Jin, Y.; Chen, F.; Chen, T.; Sun, Y.; Wang, J.; Qin, W.; Tu, H. The Adiponectin Gene Single-Nucleotide Polymorphism Rs1501299 Is Associated with Hepatocellular Carcinoma Risk. Clin. Transl. Oncol. 2014, 16 (2), 166–172. [CrossRef]
- Bieńkiewicz, J.; Smolarz, B.; Malinowski, A. Association Between Single Nucleotide Polymorphism +276G > T (Rs1501299) in ADIPOQ and Endometrial Cancer. Pathol. Oncol. Res. 2016, 22 (1), 135–138. [CrossRef]
- Tu, Y.; Yu, Q.; Fan, G.; Yang, P.; Lai, Q.; Yang, F.; Zhang, S.; Wang, W.; Wang, D.; Yu, X.; Wang, C. Y. Assessment of Type 2 Diabetes Risk Conferred by SNPs Rs2241766 and Rs1501299 in the ADIPOQ Gene, a Case/Control Study Combined with Meta-Analyses. Mol. Cell. Endocrinol. 2014, 396 (1–2), 1–9. [CrossRef]
- Leon-Cachon, R. B. R.; Salinas-Santander, M. A.; Aguilar-Tamez, D. A.; Marianavaldez-Ortiz, P.; Rios-Ibarra, C. P.; Cepeda-Nieto, A. C.; Suarez-Valencia, V. de J.; Morlett-Chavez, J. A. ADIPOQ-Rs2241766 Polymorphism Is Associated with Changes in Cholesterol Levels of Mexican Adolescents. J. Appl. Biomed. 2022, 20 (4), 146–153. [CrossRef]
- Liu, Y.; Kanu, J. S.; Qiu, S.; Cheng, Y.; Li, R.; Kou, C.; Gu, Y.; Bai, Y.; Shi, J.; Li, Y.; Liu, Y.; Yu, Y. Associations between Three Common Single Nucleotide Polymorphisms (Rs266729, Rs2241766, and Rs1501299) of ADIPOQ and Cardiovascular Disease: A Meta-Analysis. Lipids Health Dis. 2018, 17 (1), 1–21. [CrossRef]
- ZHOU, J. M.; ZHANG, M.; WANG, S.; WANG, B. Y.; HAN, C. Y.; REN, Y. C.; ZHANG, L.; ZHANG, H. Y.; YANG, X. Y.; ZHAO, Y.; HU, D. S. Association of the ADIPOQ Rs2241766 and Rs266729 Polymorphisms with Metabolic Syndrome in the Chinese Population: A Meta-Analysis. Biomed. Environ. Sci. 2016, 29 (7), 505–515. [CrossRef]
- Wu, J.; Liu, Z.; Meng, K.; Zhang, L. Association of Adiponectin Gene (ADIPOQ) Rs2241766 Polymorphism with Obesity in Adults: A Meta-Analysis. PLoS One 2014, 9 (4). [CrossRef]
Figure 1.
Flow diagram of the study selection process.
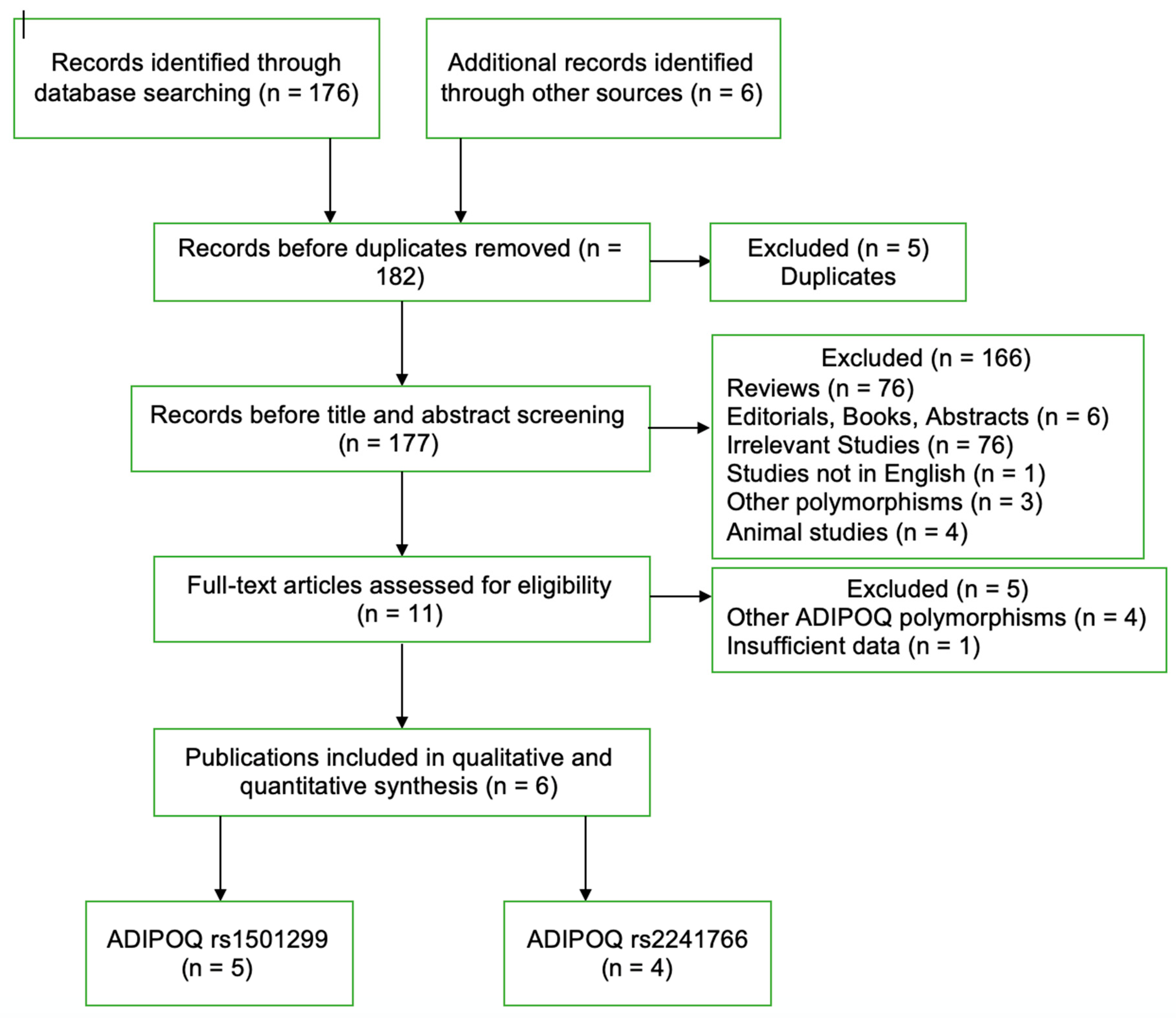
Figure 2.
Forest plot of rs1501299 polymorphism and DR risk in overall analysis in the allelic contrast.
Figure 2.
Forest plot of rs1501299 polymorphism and DR risk in overall analysis in the allelic contrast.
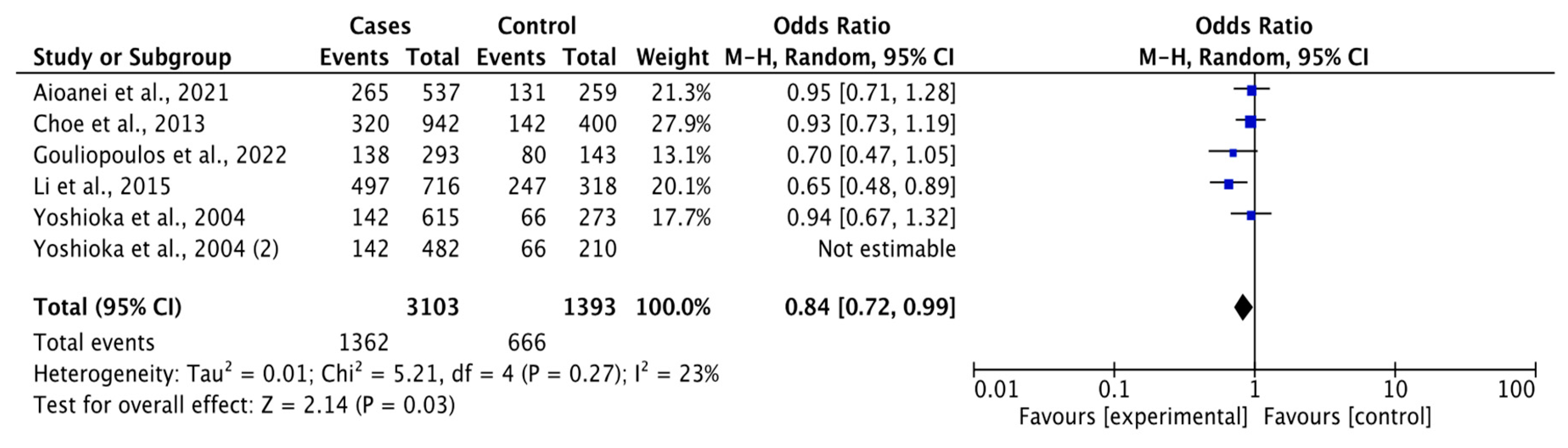
Figure 3.
Sensitivity analysis through deletion of one study at a time for rs1501299 polymorphism and DR risk association in overall comparison in the allelic contrast.
Figure 3.
Sensitivity analysis through deletion of one study at a time for rs1501299 polymorphism and DR risk association in overall comparison in the allelic contrast.
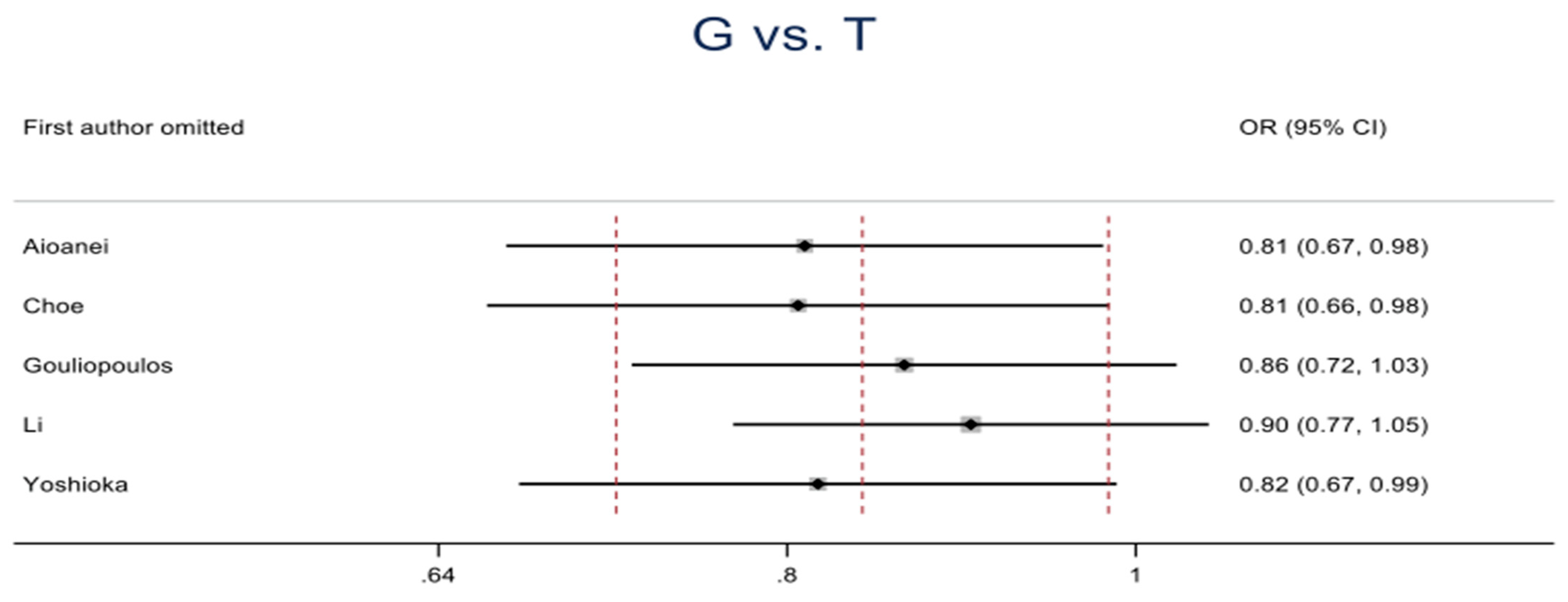
Figure 4.
Forest plot of rs1501299 polymorphism and DR risk in subgroup comparison based on DR versus DM control type in the dominant genetic model.
Figure 4.
Forest plot of rs1501299 polymorphism and DR risk in subgroup comparison based on DR versus DM control type in the dominant genetic model.
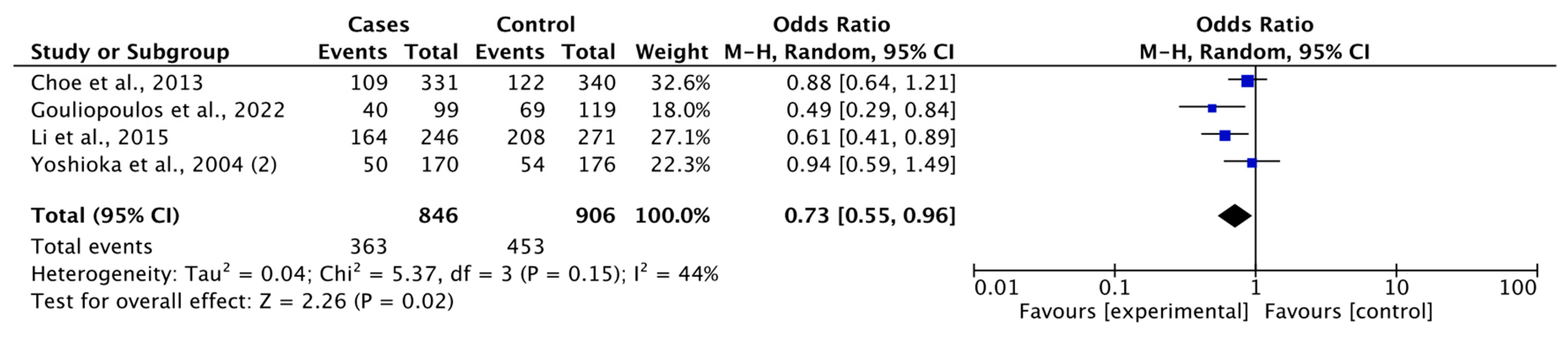
Table 2.
Meta-analysis of the association of ADIPOQ rs1501299 polymorphism and diabetic retinopathy risk.
Table 2.
Meta-analysis of the association of ADIPOQ rs1501299 polymorphism and diabetic retinopathy risk.
| rs1501299 | Study | Sample size | Studies (n) | Test of association | Test of heterogeneity | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Cases | Controls | OR (95% CI) | Z | p-value | χ2 | p-value | I2 (%) | T2 | |||
| G vs. T | Overall | 3103 | 1393 | 5 | 0.84 (0.72-0.99) | 2.14 | 0.03 | 5.21 | 0.27 | 23 | 0.01 |
| Asian | 2273 | 991 | 3 | 0.84 (0.66-1.05) | 1.51 | 0.13 | 3.76 | 0.15 | 47 | 0.02 | |
| Caucasian | 830 | 402 | 2 | 0.84 (0.63-1.13) | 1.14 | 0.25 | 1.44 | 0.23 | 31 | 0.01 | |
| DR vs DM | 2433 | 1071 | 4 | 0.81 (0.67-0.97) | 2.28 | 0.02 | 4.13 | 0.25 | 27 | 0.01 | |
| DR vs HC | 812 | 388 | 2 | 0.97 (0.76-1.24) | 0.21 | 0.83 | 0.07 | 0.79 | 0 | 0.00 | |
| GG vs. TT | Overall | 1074 | 219 | 5 | 0.76 (0.55-1.04) | 1.73 | 0.08 | 3.02 | 0.55 | 0 | 0.00 |
| Asian | 790 | 149 | 3 | 0.72 (0.44-1.18) | 1.32 | 0.19 | 2.99 | 0.22 | 33 | 0.06 | |
| Caucasian | 284 | 70 | 2 | 0.79 (0.46-1.33) | 0.90 | 0.37 | 0.00 | 0.96 | 0 | 0.00 | |
| DR vs DM | 846 | 165 | 4 | 0.75 (0.52-1.08) | 1.55 | 0.12 | 3.01 | 0.39 | 0 | 0.00 | |
| DR vs HC | 278 | 66 | 2 | 0.78 (0.45-1.34) | 0.91 | 0.36 | 0.00 | 1.00 | 0 | 0.00 | |
| GT vs. TT | Overall | 955 | 219 | 5 | 0.90 (0.63-1.29) | 0.56 | 0.57 | 4.82 | 0.31 | 17 | 0.03 |
| Asian | 693 | 149 | 3 | 0.87 (0.58-1.30) | 0.70 | 0.48 | 1.70 | 0.43 | 0 | 0.00 | |
| Caucasian | 262 | 70 | 2 | 1.08 (0.41-2.81) | 0.15 | 0.88 | 3.00 | 0.08 | 67 | 0.32 | |
| DR vs DM | 741 | 165 | 4 | 1.00 (0.66-1.52) | 0.01 | 0.99 | 3.64 | 0.30 | 18 | 0.03 | |
| DR vs HC | 256 | 66 | 2 | 0.66 (0.38-1.14) | 1.49 | 0.14 | 0.06 | 0.81 | 0 | 0.00 | |
| GG vs. GT | Overall | 1074 | 955 | 5 | 0.80 (0.60-1.08) | 1.44 | 0.15 | 9.55 | 0.05 | 58 | 0.07 |
| Asian | 790 | 693 | 3 | 0.83 (0.64-1.08) | 1.40 | 0.16 | 2.60 | 0.27 | 23 | 0.01 | |
| Caucasian | 284 | 262 | 2 | 0.71 (0.28-1.82) | 0.71 | 0.48 | 6.94 | 0.008 | 86 | 0.39 | |
| DR vs DM | 846 | 741 | 4 | 0.72 (0.53-0.98) | 2.06 | 0.04 | 5.85 | 0.12 | 49 | 0.05 | |
| DR vs HC | 278 | 256 | 2 | 1.18 (0.84-1.66) | 0.97 | 0.33 | 0.16 | 0.69 | 0 | 0.00 | |
| GG vs. GT+TT | Overall | 1074 | 1174 | 5 | 0.79 (0.61-1.03) | 1.76 | 0.08 | 8.15 | 0.09 | 51 | 0.04 |
| Asian | 790 | 842 | 3 | 0.81 (0.61-1.07) | 1.48 | 0.14 | 3.34 | 0.19 | 40 | 0.02 | |
| Caucasian | 284 | 332 | 2 | 0.73 (0.35-1.52) | 0.83 | 0.40 | 4.81 | 0.03 | 79 | 0.22 | |
| DR vs DM | 846 | 906 | 4 | 0.73 (0.55-0.96) | 2.26 | 0.02 | 5.37 | 0.15 | 44 | 0.04 | |
| DR vs HC | 278 | 322 | 2 | 1.09 (0.79-1.50) | 0.50 | 0.61 | 0.14 | 0.71 | 0 | 0.00 | |
| GG+GT vs.TT | Overall | 2031 | 219 | 5 | 0.82 (0.61-1.12) | 1.26 | 0.21 | 3.31 | 0.51 | 0 | 0.00 |
| Asian | 1485 | 149 | 3 | 0.78 (0.51-1.19) | 1.14 | 0.26 | 2.38 | 0.30 | 16 | 0.02 | |
| Caucasian | 546 | 70 | 2 | 0.87 (0.53-1.44) | 0.53 | 0.59 | 0.85 | 0.36 | 0 | 0.00 | |
| DR vs DM | 1587 | 165 | 4 | 0.86 (0.60-1.23) | 0.81 | 0.42 | 3.06 | 0.38 | 2 | 0.00 | |
| DR vs HC | 534 | 66 | 2 | 0.72 (0.43-1.21) | 1.25 | 0.21 | 0.02 | 0.90 | 0 | 0.00 | |
| GG+TT vs. GT | Overall | 1293 | 955 | 5 | 0.85 (0.63-1.13) | 1.13 | 0.26 | 9.80 | 0.04 | 59 | 0.06 |
| Asian | 939 | 693 | 3 | 0.87 (0.70-1.08) | 1.23 | 0.22 | 1.99 | 0.37 | 0 | 0.00 | |
| Caucasian | 354 | 262 | 2 | 0.75 (0.29-1.91) | 0.61 | 0.54 | 7.78 | 0.005 | 87 | 0.40 | |
| DR vs DM | 1011 | 741 | 4 | 0.76 (0.57-1.02) | 1.82 | 0.13 | 5.72 | 0.13 | 48 | 0.04 | |
| DR vs HC | 344 | 256 | 2 | 1.24 (0.90-1.72) | 1.30 | 0.19 | 0.16 | 0.69 | 0 | 0.00 | |
ADD Abbreviations: DM, Diabetes Mellitus, DR, Diabetic Retinopathy; HC, Healthy-based Controls.
Table 3.
Meta-analysis of the association of ADIPOQ rs2241766 polymorphism and diabetic retinopathy risk.
Table 3.
Meta-analysis of the association of ADIPOQ rs2241766 polymorphism and diabetic retinopathy risk.
| rs2241766 | Study | Sample size | Studies (n) | Test of association | Test of heterogeneity | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Cases | Controls | OR (95% CI) | Z | p-value | χ2 | p-value | I2 (%) | T2 | |||
| T vs. G | Overall | 3045 | 805 | 4 | 1.30 (1.00-2.09) | 1.42 | 0.15 | 10.03 | 0.02 | 70 | 0.09 |
| Asian | 2674 | 740 | 3 | 1.27 (0.82-1.96) | 1.06 | 0.29 | 8.93 | 0.01 | 78 | 0.11 | |
| DR vs DM | 2681 | 763 | 4 | 1.21 (0.90-1.64) | 1.27 | 0.20 | 6.76 | 0.08 | 56 | 0.05 | |
| TT vs. GG | Overall | 1220 | 100 | 4 | 1.34 (0.87-2.07) | 1.31 | 0.19 | 1.74 | 0.63 | 0 | 0.00 |
| Asian | 1062 | 95 | 3 | 1.32 (0.84-2.07) | 1.21 | 0.23 | 1.66 | 0.44 | 0 | 0.00 | |
| DR vs DM | 1056 | 97 | 4 | 1.33 (0.86-2.07) | 1.28 | 0.20 | 1.74 | 0.63 | 0 | 0.00 | |
| TG vs. GG | Overall | 605 | 100 | 4 | 0.94 (0.60-1.49) | 0.26 | 0.79 | 1.06 | 0.79 | 0 | 0.00 |
| Asian | 550 | 95 | 3 | 0.93 (0.58-1.50) | 0.29 | 0.77 | 1.03 | 0.60 | 0 | 0.00 | |
| DR vs DM | 569 | 97 | 4 | 0.96 (0.60-1.52) | 0.18 | 0.86 | 0.70 | 0.87 | 0 | 0.00 | |
| TT vs. TG+GG | Overall | 1220 | 705 | 4 | 1.38 (0.89-2.15) | 1.45 | 0.15 | 10.61 | 0.01 | 72 | 0.14 |
| Asian | 1062 | 645 | 3 | 1.35 (0.78-2.35) | 1.07 | 0.28 | 9.69 | 0.008 | 79 | 0.18 | |
| DR vs DM | 1056 | 666 | 4 | 1.29 (0.89-1.87) | 1.35 | 0.18 | 7.21 | 0.07 | 58 | 0.08 | |
| TT vs. TG | Overall | 1220 | 605 | 4 | 1.41 (0.88-2.25) | 1.43 | 0.15 | 10.92 | 0.01 | 73 | 0.16 |
| Asian | 1062 | 550 | 3 | 1.39 (0.76-2.53) | 1.08 | 0.28 | 10.13 | 0.006 | 80 | 0.22 | |
| DR vs DM | 1056 | 569 | 4 | 1.31 (0.88-1.95) | 1.33 | 0.18 | 7.54 | 0.06 | 60 | 0.09 | |
| TT+TG vs. GG | Overall | 1845 | 100 | 4 | 0.99 (0.64-1.54) | 0.03 | 0.97 | 0.33 | 0.95 | 0 | 0.00 |
| Asian | 1632 | 95 | 3 | 0.97 (0.62-1.52) | 0.14 | 0.88 | 0.11 | 0.95 | 0 | 0.00 | |
| DR vs DM | 1645 | 97 | 4 | 0.99 (0.63-1.53) | 0.06 | 0.95 | 0.30 | 0.96 | 0 | 0.00 | |
| TT+GG vs. TG | Overall | 1320 | 605 | 4 | 1.40 (0.88-2.21) | 1.42 | 0.16 | 10.91 | 0.01 | 72 | 0.15 |
| Asian | 1157 | 550 | 3 | 1.38 (0.77-2.49) | 1.08 | 0.28 | 10.14 | 0.006 | 80 | 0.21 | |
| DR vs DM | 1153 | 569 | 4 | 1.30 (0.88-1.92) | 1.31 | 0.19 | 7.51 | 0.06 | 60 | 0.09 | |
ADD Abbreviations: DM, Diabetes Mellitus, DR, Diabetic Retinopathy.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



