
Submitted:
14 June 2024
Posted:
17 June 2024
You are already at the latest version
Abstract
Background: Differentiated thyroid cancer (DTC) patients have an outstanding overall long-term survival rate, certain subsets of DTC patients have a very high likelihood of disease recurrence. Radioactive iodine therapy is a cornerstone in DTC management, but sometimes it became useless when cancer cells develop refractoriness. Radioactive Iodine Refractory DTC (RAIR-DTC) is a condition defined by ATA 2015 guidelines when DTC cannot concentrate RAI ab initio or loses RAI uptake ability after the initial therapy. RAIR condition implies that RAI cannot reveal new met-astatic foci, so RAIR-DTC metabolic imaging needs new tracers. 18F-FDG PET/CT has been widely used, it has a demonstrated prognostic value, but 18F-FDG DTC avidity may remain low. FA-Pi, PSMA, SSTR tracers have been proposed as theragnostic agents in experimental settings and Arg-Gly-Asp (RGD) peptides in diagnostic trial field. Multi-targeted tyrosine kinase inhibitors are relatively new drugs approved in RAIR-DTC therapy. Despite the promising targeted setting, they relate to frequent adverse event onset. Sorafenib and trametinib have been included in re-differentiation protocols aimed to re-induce RAI accumulation in DTC cells. Results appeared promising, despite not excellent. Conclusions: RAIR-DTC yet represent a challenging nosological entity. There are still controversies on RAIR-DTC definition and post-RAI therapy evaluation with post-therapy whole body scan (PT-WBS) is the only validated criterion of response. The recent introduction of multiple diagnostic and therapeutic agents oblige physicians to pursue a multidisciplinary approach aiming to correct drug introduction and timing choice.
Keywords:
Radioactive Iodine
; Therapy
; Theragnostics
; Differentiated Thyroid Cancer
; Refractory DTC
1. Introduction
While differentiated thyroid cancer (DTC) patients have an outstanding overall long-term survival rate, certain subsets of DTC patients have a very high likelihood of disease recurrence [1,2,3]. To evaluate the likelihood of recurrent or chronic illness in DTC patients, the American Thyroid Association (ATA) initial risk classification system has been proposed. Three risk categories (low, middle, and high) are assigned to the patients. Furthermore, the ATA has suggested a dynamic risk categorization approach that considers imaging, biochemical, and clinical data gathered during follow-up. Radioiodine (RAI) diagnostic whole-body scanning (WBS) has been utilized in the past for DTC disease status assessment, but it has been replaced by a combination of neck ultrasonography (US) and serum thyroglobulin (Tg) measurement [1].
The current data demonstrate that patients with undetectable serum Tg levels have a high chance of achieving complete remission, and that a diagnostic workup may not be necessary in these cases [4,5]. Moreover, serum Tg, after some months of detectable levels, can tend to zero with no further actions.
An adequate uptake of RAI in the target tissue, defined as RAI avidity (RAI-A), is mandatory to obtain a successful RAI therapy. A low-risk disease and a post-surgical treatment includes thyroid remnant usually are highly iodine avid targets so ablation can be successful.
The primary tumour size and the eventual lymph node metastases determines the administered radioiodine activity, but RAI-A is not guaranteed, especially in high-risk CDT or in presence of known metastases [6,7,8].
Several factors have been associated with lower RAI-A of metastatic tissue, such as patient age, large tumour size, histological type and high [18F] fluorodeoxyglucose uptake[9,10]. Furthermore, tumors exhibiting BRAF V600E or TERT promoter mutations are less likely to spawn iodine avid metastases and are associated with poorer patient outcomes. The co-occurrence of these two mutational events in papillary thyroid cancer (PTC) has been found to be especially indicative of aggressive tumor features [6,11,12].
2. Defining Radioactive Iodine Refractory Differentiated Thyroid Cancer
Despite iodine uptake may be altered ab initio in CDT [13], RAI therapy is still a cornerstone for the success of medium and high risk CDT treatment [1,2,14]. Iodine uptake may decrease with disease progression, until further RAI administration became ineffective from a clinical point of view. In this condition, DTC can be considered as refractory to RAI. RAIR-DTC is a relatively uncommon condition (4-5 cases/million/year). RAIR-DTC is associated with a bad prognosis, in fact less than 10% of patients survive at 10 years (mean 3-5 years) [15].
Radioactive Iodine Refractory DTC (RAIR-DTC) is defined by the ATA 2015 guidelines as a condition where DTC cannot concentrate radioactive iodine (RAI) at the time of initial treatment or loses its ability to concentrate RAI after initial therapy. RAIR-DTC also includes cases where only the local lesion concentrates RAI, or there is disease progression and metastatic spread after high-dose treatment, despite the ability to concentrate RAI [1].
While the refractory condition of DTC patients who lose the capability to concentrate RAI into the target lesion is well understood, more controversy surrounds cases where RAIR is associated with disease progression despite good RAI uptake. For these patients, evaluating the risk-to-reward ratio is crucial. After a cumulative dose of 600 mCi, the risk of side effects increases, while the likelihood of achieving a cure decreases. Therefore, the decision to continue RAI treatment should be made on a case-by-case basis, considering the patient's previous response to RAI administration.[16,17,18]. Table 1 summarizes all the condition that ATA 2015 guidelines define a DTC as RAIR.
Nevertheless, RAIR categories defined by ATA 2015 may appear over-restrictive in the view of a personalized medicine approach and should not be considered definitive. Martinique principles come in aid in 2019 when some experts proposed that the feasibility of a RAI therapy in DTC patients should be discussed case by case, not excluding it a priori when a DTC patient fall in an ATA 2015 RAIR category. Indeed RAIR definition criteria will be subject to evolution due to recent introduction of re-differentiation therapies [19].
The risk of RAIR-DTC can raise in elderly patients with aggressive histological DTC subtype and with presence of metastatic disease at the time of diagnosis. In these patients, cancer heterogeneity increases with RAI uptake inhomogeneity into target lesions so RAI therapy can be less effective [3,20]. The prevalence of RAIR-DTC approximately amounts of 15% of DTC patients, particularly those with distant metastases at diagnosis and older age.
The molecular mechanisms involved in RAIR onset may include either ERK or mTOR activation pathways that both affect PAX8 transcription factor function. BRAF v600e is the most involved mutation in PTC cells, while in follicular thyroid cancer (FTC) cells RAS is the most involved muted kinase [6,12,21]. The main effects of these alterations are the down-expression of sodium-iodine symporter (NIS) and the over-expression of glucose transporter 1 (GLUT1) [2,22,23]. NIS is essential for RAI uptake, indirectly involved in its organification and so it is involved in its mechanism of action [8,22]. From a functional point of view, DTC cells progressively lose the capability of accumulating iodine, but gain an extra income of energetical substrates that can sustain the increased metabolic requirement of cancer cells.
In this scenario, single-stranded mature microRNAs (miRNAs) role has been investigated. MiRNAs are small sequences of nucleotides that lack a coding capability but are involved in post-transcriptional gene expression. Some miRNAs have been linked in DTC tumorigenesis [24], some others have been proposed as biomarker for relapse detection [24,25] and others, as miR-139-5p, have been suggested in RAIR pathogenesis explanation [26]. When DTC cells take the way of dedifferentiation, this leads to an increased aggressivity, to metastasis onset and worse prognosis [2,27,28].
3. Identifying RAI-R
While post therapy 131I-whole-body scan (PT-WBS) can be considered a good negative detector of RAIR, the same consideration cannot be reserved to diagnostic 131I-whole-body scan (D-WBS). RAI activity, acquisition time, γ-camera model and TSH stimulation play a role in D-WBS accuracy and sensibility. In particular, the low administered RAI activity for the D-WBS acquisition would not allow to detect all the RAI avid foci [29,30,31].
Nevertheless, the added value of performing a 131I-single photon emission computed tomography (SPECT)/computed tomography (CT) has been debated since the introduction of this hybrid method. Some authors put the light on the better detection ability derived from the attenuation correction algorithms and from the morphological imaging acquired simultaneously [32,33,34]. In case of equivocal findings at planar WBS images, PT-131I-SPECT/CT can differentiate remnant thyroid from lymph-nodal accumulation. Indeed focal uptake of uncertain source may be defined as para-physiological or metastatic with the fine body district localization [34,35,36]. Thus, the initial staging of DTC, as long with patient risk assessment, can be corrected by the additional imaging findings.
Patients who present negative imaging of 131I-WBS (despite D-WBS or PT-WBS) and abnormally elevated serum Tg levels should receive adequate attention, because this occurrence always indicate the presence of RAI-refractory disease.
RAIR often occurs in advanced DTC patients, when cancer heterogeneity increases as long with its aggressiveness, additionally, RAI accumulation can vary lesion by lesion [37,38].
Molecular imaging reflects these changes accordingly. RAI accumulation decreases while 18F- Fluorodeoxyglucose (FDG) uptake increases. This is called “flip-flop” phenomenon and it is directly correlated with DTC dedifferentiation and aggressiveness [9,10,39,40].
18F-FDG positron emission tomography (PET)/ computed tomography (TC) can be evaluated qualitatively by visual uptake detection and quantitatively by SUV estimation.
4. Current Molecular Imaging and Care Options
Routine RAI imaging in clinical settings involves both regional and planar WBS and SPECT methods. However, there are no standardized quantitative methods for assessing response. Instead, response criteria often rely on visually assessed decreases in tumor uptake during post-treatment follow-up. It is important to consider the potential for functional tumor de-differentiation over the course of the disease when interpreting decreased RAI uptake in follow-up scans. To assess this possibility, 18F-FDG PET/CT scans, which reflect the tumors' glycolytic activity, should be used.
Is now possible to target aberrant cellular pathways and to provide additional treatment options for patients with otherwise poor prognoses due to the identification of multiple molecular alterations in advanced thyroid cancer.
For RAIR-DTC the current standard of care involves treatment with tyrosine kinase inhibitors (TKIs).
The first-line setting includes both sorafenib and Lenvatinib, as established by the National Comprehensive Cancer Network (NCCN) guidelines [46]. However, some patients manifest RET or NTRK fusions and the standard of care has to be changed accordingly. More than half of patients show BRAF mutation, but the efficacy of BRAF inhibitors is not better than Lenvatinib, and they are reserved to later therapy options [47].
Before initiating Lenvatinib blood pressure must be under control, but in case of difficulty, sorafenib should be adopted. Selective RET inhibitors such as Selpercatinib or Larotrectinib should be preferred in patients with fusion detection. However, in case of BRAF positivity, Lenvatinib remains preferable, with BRAF inhibitors reserved for later lines of therapy. In the second-line setting, Cabozantinib is also authorized and considered standard therapy.
The main challenges in managing RAI-Refractory Differentiated Thyroid Cancer (AI-R-DTC include the onset of resistance and adverse events. To extend the efficacy of systemic therapy, local treatments such as surgery or external radiation should be considered for single progressing lesions. Although Sorafenib and Lenvatinib therapies are associated with adverse events, patients may achieve optimal outcomes and should be encouraged to adhere to treatment to avoid unnecessary dose reductions or treatment withdrawal.
5. Future Diagnostic and Therapeutic Perspectives
RAIR DTC biochemical characteristics implies the need to research of alternative targeted imaging tracers other than iodine. Advanced cancer cells show some molecular pathways activation and mechanism similarities, so some tracers yet used in other cancer imaging could be adopted.
Integrin αvβ3 is involved in tumor angiogenesis and can be a potential imaging target for cancer growth, using radiolabeled RGD peptides. 99mTc-3PRGD2 has been used by some authors in DTC patients who had negative 131I-WBS, but elevated Tg levels to perform SPECT/TC images [48,49,50]. It has been demonstrated that, with growing serum Tg levels, both sensitivity and positive predictive value (PPV) remained high and even increased [51]. Additionally, it has been suggested that 99mTc-3PRGD2 uptake can predict the disease progression after initial RAI therapy, in high risk DTC patients [52]. RGD peptides can be labeled also with positron emitting radionuclides for a PET/TC application. Some authors found that 68Ga- DOTA-RGD PET imaging could outperform 18F-FDG PET both in sensitivity and specificity, aiding a precise lesions quantitative analysis [53]. Chernaya et al. reported that BRAF mutation is linked with different expression levels of integrin receptors in DTC, in this scenario RGD imaging can be proposed under individualized conditions [54].
[55] Prostate-specific membrane antigen (PSMA) ligands family are a recent introduction in prostate cancer theragnostic [56,57,58]. PSMA overexpression has also been found in tumor neovasculature in various other tumors [59,60]. The expression of PSMA in thyroid tissue examined by some authors. Bychkov et al. enrolled 267 patients and found that PSMA was expressed in DTC neovasculature, but not in healthy tissue [61]. Similar results were found by Heitkotter and coworkers when comparing PSMA expression in thyroid cancer and benign thyroid diseases [62]. Hence, PSMA imaging in RAIR-DTC should be feasible. Some authors investigated PSMA uptake in a prospective study including 10 patients with 32 DTC metastatic lesions, 68Ga-PSMA PET/TC uptake was consistent (30/32 detected metastasis) and performance was superior to 18F-FDG PET/CT (23/32 detected metastasis) [63]. Verburg et al. in 2015 [64] and Lütje et al. in 2017 [65] demonstrated a possible role of 68Ga-HBED-CC-PSMA PET/CT for staging patients with RAIR- DTC metastases and for select patients eligible for PSMA radioactive labeled therapy. More recently, de Vries and coworkers explored the possible use of 177Lu-PSMA-617 therapy in 5 RAIR-DTC patients that showed 68Ga-PSMA PET/CT uptake in distant metastasis foci. Only 2 of them were considered eligible for a 177Lu-PSMA-617 administration and only one of them established a temporary response [66]. These results need to be used to better define the possible role of PSMA ligands theragnostic putting the basis for future studies.
Somatostatin receptors (SSTR) type 2, 3 and 5 in has been demonstrated in various studies in DTC cells but also in normal thyroid tissue and benign thyroid diseases [67,68,69,70,71]. Radiolabeled somatostatin analogs, such as octreotide and lanreotide marked with 68Ga-DOTA, have discovered a pretty large use in PET/CT SSTR imaging in last years, especially in neuro endocrine tumor (NET) imaging [72,73,74,75,76]. However, the role of SSTR tracers in RAIR-DTC remains unclear. In 2020 Donohoe and colleagues published a document on the appropriate use of the available nuclear medicine methods, including 68Ga-DOTATATE PET/CT and 177Lu-labeled SSTR tracers in RAIR-DTC. The committee stated that there was insufficient evidence to correlate Tg increase with 68Ga-DOTATATE PET/CT imaging positivity. Therefore 177Lu-labeled SSTR tracers should be considered in the therapeutic choices of RAIR-DTC patients that have demonstrated SSTR tracers imaging positivity [77].
Similarly to PSMA, radiolabeled choline PET/CT has found consistency in the diagnosis of prostate cancer. Thyroid uptake has been eventually recorded in some 18F-choline PET/CT done for prostate cancer diagnosis and staging [78,79]. 18F-choline PET/CT has been also investigated in hunting performance of DTC metastases negative on 18F-FDG PET/CT. Piccardo et al. evaluated 25 patients with high risk RAIR-DTC with both 18F-FDG and 18F-choline PET/CT. They found a good correlation with Tg doubling time and 18F-choline uptake. Thus, 18F-choline overperformed 18F-FDG in terms of sensitivity, specificity and negative predictive value [80]. 18F-choline PET/CT should be considered in addition to 18F-FDG PET/CT DTC lesions.
More recently, the attention has moved also to the tumor microenvironment (TME), a complex system composed by extracellular matrix, immune cells, fibroblast, endothelial cells and signaling compounds. It has been demonstrated that TME plays an important role in tumorigenesis and progression [81]. Of note, fibroblast’s function is shifted and promotes tumor growth, so they can be defined cancer associated fibroblasts (CAFs) and express the fibroblast activation protein (FAP) [81,82]. FAP can be targeted by FAP inhibitors (FAPi) and used in nuclear medicine theragnostic applications [83].
A possible RAIR-DTC application for FAPi has been explored by Chen and coworkers that studied a population of 24 patients [84]. All of them performed a 68Ga-DOTA-FAPi-04 PET/CT and the detection rate was fairly good (87.5%). Ballal and co-workers compared 68Ga-DOTA-FAPi-04 PET/CT versus 18F-FDG PET/CT in 117 patients with RAIR-DTC and demonstrated a superior performance in metastasis detection of radiolabeled FAPi over 18F-FDG [85]. After these results Ballal et al. performed a pilot study aimed at evaluating a possible therapeutic use of 177Lu-DOTAGA.(SA.FAPi)2 in 15 RAIR-DTC patients that failed all of the standard options of systemic drugs [86]. At the end of therapy cycles the response rate was 92% and a complete response was achieved in 23% of patients.
177Lu-EB-FAPI was studied by Fu and coworkers in 12 patients with RAIR-DTC in a dose escalation trial. The results, evaluated with RECIST 1.1 criteria [87], were a partial response in 25% of patients, a stable disease in 58% of patients and progression in 17% of patients [88].
Sorafenib and Lenvatinib are multi-targeted tyrosine kinase inhibitors (mTKI), recently approved for use in RAIR DTC [89,90,91,92]. Progression-free survival (PFS) achieved using these drugs is good, but overall survival (OS) nor the quality of life (QOL) would match the patient’s needs. Numerous adverse events have been reported and the treatment is usually prolonged until progression so the development of resistance has to be expected [90,91]. There is expanding evidence that mTKI can induce a sort of re-differentiation in RAIR-DTC cells, promoting NIS exposition on cells membrane and re-inducing a possible RAI sensibility. Iravani et al. studied a re-differentiation protocol in 6 RAIR-DTC patients harboring BRAF v600e mutation. The therapy was targeted to MEK with trametinib and the v600e mutation of BRAF with dabrafenib and trametinib. The RAI uptake was demonstrated in 4/6 patients, and one of them achieved a complete response after therapeutic RAI administration [93]. Leboulleux and coworkers developed a phase II prospective trial based on a re-differentiation therapy with dabrafenib and trametinib, followed by a fixed RAI administration of 5550 MBq. The RAIR-DTC status was demonstrated by a DxWBS prior to mTKI administration [94]. 11 patients were enrolled and 10 of them received RAI therapy. After 6 months, RECIST criteria defined a partial response in 20% of patients and a stable disease in 70% of patients. Unfortunately, 10% of patients showed a progression of the disease. Metabolic assessment was performed with 18F-FDG PET/CT and results were similar to RECIST evaluation (partial response in 25%, stable disease in 63% and progression in 13% of patients) [94]. Balakirouchenane et coworkers studied 22 patients undergoing re-differentiation therapy followed by RAI administration. They found a linkage between lower mTKi plasma concentration and RAI uptake [95]. Leboulleux et al. studied 24 patients with RAIR- DTC (confirmed by DX-WBS) with small metastases that underwent a re-differentiation protocol with dabrafenib-trametinib tandem administration for 42 days [91]. A 5550 MBq RAI therapy was administered at day 28 after rh-TSH stimulation and a first evaluation of response was assessed by RECIST criteria after 6 months. If a partial response was reached, a second RAI could be administered after 6 or 12 months. A progression was diagnosed in 10% of patients, while partial or stable disease was achieved in 38% and 52% of patients respectively. 10 patients received a second RAI administration and one of them obtained a complete response and 6 obtained a partial response at 6 months evaluation. One patient died because of progressive disease within 24 months. Despite the evidence of adverse events was common (96% of patients) the re-differentiation protocol was considered a good option for RAIR-DTC patients with small metastases.
6. A Case of Re-Differentiation
A 59-year-old man underwent total thyroidectomy in 2016 and a subsequently left cervical lymphadenectomy for evidence of papillary thyroid carcinoma with lymph node metastases (pT1b N1b Mx). 5550 MBq of RAI were administered right within 6 months from surgery. Nevertheless, Tg levels returned detectable after some years from the first RAI therapy, so a further dose of 5550 MBq if 131I was administered. The PT-WBS did not show abnormal uptake foci (Figure 1), while Tg blood level was 378 pg/dl after FT4 withdrawal TSH stimulation and there was the evidence of pulmonary nodules at CT examination.
The patient was defined as RAIR and the presence of BRAF v600e mutation was identified by molecular investigation. A re-differentiation protocol was attempted with the administration of dabrafenib and trametinib for 42 days. A 5550 MBq RAI therapy was administered at the 28th day of dabrafenib and trametinib administration, under rhTSH stimulation.
PT-WBS scan demonstrated high RAI uptake in pulmonary area and in a left cervical region (Figure 2).
PT-SPECT/TC demonstrated RAI diffuse uptake in pulmonary parenchyma and left posterior mandibular lymph node (Figure 3). Tg blood levels increased also to 3183 pg/dl after rhTSH stimulation, suggesting that the re-differentiation protocol must have worked at different molecular levels.
7. Conclusions
DTC functional differentiation understanding is linked with its complexity awareness and is necessary to build clear response criterion for response evaluation. Tumor genomics insights are enriching rapidly, and the chimera of individualized therapy becomes more real time to time. Despite that, RAIR-DTC yet represent a challenging nosological entity. There are still controversies on RAIR-DTC definition and post-RAI therapy evaluation with PT-WBS is the only validated criterion of response. Avoiding patients unnecessary RAI radiation exposure and sub-optimal interventions are current concerns. There is a current need of predicting RAIR-DTC before RAI therapy and individualizing therapeutic choices. Thus, molecular imaging is advancing and molecular biochemistry research and should aim for RAIR-DTC prediction, targeted therapy and optimal start timing to select secondary-line treatment strategies.
Author Contributions
Conceptualization, F.V. and C.N.; methodology, F.V.; validation, S.M., E.D. and E.Z.; formal analysis, F.V.; investigation, F.V.; resources, F.V.; data curation, F.V.; writing—original draft preparation, F.V.; writing—review and editing, C.N.; visualization, M.K.; supervision, M.K.; project administration, C.N.; funding acquisition, A.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved on 16 November 2023 by the Institutional Review Committee of the Department of Advanced Biomedical Sciences of the University of Naples Federico II (16114/23).
Informed Consent Statement
“Written informed consent has been obtained from the patient to publish this paper”.
Data Availability Statement
The data presented in this study are available in this article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid Off. J. Am. Thyroid Assoc. 2016, 26, 1–133. [Google Scholar] [CrossRef] [PubMed]
- Klain, M.; Nappi, C.; Zampella, E.; Cantoni, V.; Green, R.; Piscopo, L.; Volpe, F.; Manganelli, M.; Caiazzo, E.; Petretta, M.; et al. Ablation Rate after Radioactive Iodine Therapy in Patients with Differentiated Thyroid Cancer at Intermediate or High Risk of Recurrence: A Systematic Review and a Meta-Analysis. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 4437–4444. [Google Scholar] [CrossRef]
- Worden, F.; Rajkovic-Hooley, O.; Reynolds, N.; Milligan, G.; Zhang, J. Real-World Treatment Patterns and Clinical Outcomes in Patients with Radioiodine-Refractory Differentiated Thyroid Cancer (RAI-R DTC) Treated with First Line Lenvatinib Monotherapy in the United States. Endocrine 2023. [Google Scholar] [CrossRef] [PubMed]
- Chou, R.; Dana, T.; Brent, G.A.; Goldner, W.; Haymart, M.; Leung, A.M.; Ringel, M.D.; Sosa, J.A. Serum Thyroglobulin Measurement Following Surgery Without Radioactive Iodine for Differentiated Thyroid Cancer: A Systematic Review. Thyroid Off. J. Am. Thyroid Assoc. 2022, 32, 613–639. [Google Scholar] [CrossRef] [PubMed]
- Schlumberger, M.; Leboulleux, S. Current Practice in Patients with Differentiated Thyroid Cancer. Nat. Rev. Endocrinol. 2021, 17, 176–188. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Liu, R.; Shen, X.; Zhu, G.; Li, B.; Xing, M. The Genetic Duet of BRAF V600E and TERT Promoter Mutations Robustly Predicts Loss of Radioiodine Avidity in Recurrent Papillary Thyroid Cancer. J. Nucl. Med. 2020, 61, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Nakanishi, K.; Kikumori, T.; Miyajima, N.; Takano, Y.; Noda, S.; Takeuchi, D.; Iwano, S.; Kodera, Y. Impact of Patient Age and Histological Type on Radioactive Iodine Avidity of Recurrent Lesions of Differentiated Thyroid Carcinoma. Clin. Nucl. Med. 2018, 43, 482–485. [Google Scholar] [CrossRef] [PubMed]
- Simões-Pereira, J.; Mourinho, N.; Ferreira, T.C.; Limbert, E.; Cavaco, B.M.; Leite, V. Avidity and Outcomes of Radioiodine Therapy for Distant Metastasis of Distinct Types of Differentiated Thyroid Cancer. J. Clin. Endocrinol. Metab. 2021, 106, e3911–e3922. [Google Scholar] [CrossRef] [PubMed]
- Pace, L.; Klain, M.; Salvatore, B.; Nicolai, E.; Zampella, E.; Assante, R.; Pellegrino, T.; Storto, G.; Fonti, R.; Salvatore, M. Prognostic Role of 18F-FDG PET/CT in the Postoperative Evaluation of Differentiated Thyroid Cancer Patients. Clin. Nucl. Med. 2015, 40, 111. [Google Scholar] [CrossRef] [PubMed]
- Salvatore, B.; Klain, M.; Nicolai, E.; D’Amico, D.; De Matteis, G.; Raddi, M.; Fonti, R.; Pellegrino, T.; Storto, G.; Cuocolo, A.; et al. Prognostic Role of FDG PET/CT in Patients with Differentiated Thyroid Cancer Treated with 131-Iodine Empiric Therapy. Medicine (Baltimore) 2017, 96, e8344. [Google Scholar] [CrossRef] [PubMed]
- Celik, M.; Bulbul, B.Y.; Ayturk, S.; Durmus, Y.; Gurkan, H.; Can, N.; Tastekin, E.; Ustun, F.; Sezer, A.; Guldiken, S. The Relation between BRAFV600E Mutation and Clinicopathological Characteristics of Papillary Thyroid Cancer. Med. Glas. Ljek. Komore Zenicko-Doboj. Kantona 2020, doi:10.17392/1086-20. [CrossRef]
- Wu, Y.; Shi, L.; Zhao, Y.; Chen, P.; Cui, R.; Ji, M.; He, N.; Wang, M.; Li, G.; Hou, P. Synergistic Activation of Mutant TERT Promoter by Sp1 and GABPA in BRAFV600E-Driven Human Cancers. Npj Precis. Oncol. 2021, 5, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Schlumberger, M.; Lacroix, L.; Russo, D.; Filetti, S.; Bidart, J.-M. Defects in Iodide Metabolism in Thyroid Cancer and Implications for the Follow-up and Treatment of Patients. Nat. Clin. Pract. Endocrinol. Metab. 2007, 3, 260–269. [Google Scholar] [CrossRef] [PubMed]
- Namwongprom, S.; Dejkhamron, P.; Unachak, K. Success Rate of Radioactive Iodine Treatment for Children and Adolescent with Hyperthyroidism. J. Endocrinol. Invest. 2021, 44, 541–545. [Google Scholar] [CrossRef] [PubMed]
- Shogbesan, G.; Muzahir, S.; Bridges, A. Radioiodine Refractory Differentiated Thyroid Cancer: Albatross of Patients and Physicians. J. Nucl. Med. 2022, 63, 2693–2693. [Google Scholar]
- Schlumberger, M.; Brose, M.; Elisei, R.; Leboulleux, S.; Luster, M.; Pitoia, F.; Pacini, F. Definition and Management of Radioactive Iodine-Refractory Differentiated Thyroid Cancer. Lancet Diabetes Endocrinol. 2014, 2, 356–358. [Google Scholar] [CrossRef] [PubMed]
- Finessi, M.; Liberini, V.; Deandreis, D. Definition of Radioactive Iodine Refractory Thyroid Cancer and Redifferentiation Strategies. In Integrated Diagnostics and Theranostics of Thyroid Diseases; Giovanella, L., Ed.; Springer International Publishing: Cham, 2023; pp. 143–156. ISBN 978-3-031-35213-3. [Google Scholar]
- Kiyota, N.; Robinson, B.; Shah, M.; Hoff, A.O.; Taylor, M.H.; Li, D.; Dutcus, C.E.; Lee, E.K.; Kim, S.-B.; Tahara, M. Defining Radioiodine-Refractory Differentiated Thyroid Cancer: Efficacy and Safety of Lenvatinib by Radioiodine-Refractory Criteria in the SELECT Trial. Thyroid 2017, 27, 1135–1141. [Google Scholar] [CrossRef] [PubMed]
- Van Nostrand, D. Selected Controversies of Radioiodine Imaging and Therapy in Differentiated Thyroid Cancer. Endocrinol. Metab. Clin. North Am. 2017, 46, 783–793. [Google Scholar] [CrossRef]
- Deandreis, D.; Rubino, C.; Tala, H.; Leboulleux, S.; Terroir, M.; Baudin, E.; Larson, S.; Fagin, J.A.; Schlumberger, M.; Tuttle, R.M. Comparison of Empiric Versus Whole-Body/-Blood Clearance Dosimetry–Based Approach to Radioactive Iodine Treatment in Patients with Metastases from Differentiated Thyroid Cancer. J. Nucl. Med. 2017, 58, 717–722. [Google Scholar] [CrossRef] [PubMed]
- Mu, Z.-Z.; Zhang, Y.-Q.; Sun, D.; Lu, T.; Lin, Y.-S. Effect of BRAFV600E and TERT Promoter Mutations on Thyroglobulin Response in Patients With Distant-Metastatic Differentiated Thyroid Cancer. Endocr. Pract. Off. J. Am. Coll. Endocrinol. Am. Assoc. Clin. Endocrinol. 2022, 28, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Sgouros, G.; Bodei, L.; McDevitt, M.R.; Nedrow, J.R. Radiopharmaceutical Therapy in Cancer: Clinical Advances and Challenges. Nat. Rev. Drug Discov. 2020, 19, 589–608. [Google Scholar] [CrossRef] [PubMed]
- Dotinga, M.; Vriens, D.; van Velden, F.H.P.; Stam, M.K.; Heemskerk, J.W.T.; Dibbets-Schneider, P.; Pool, M.; Rietbergen, D.D.D.; de Geus-Oei, L.-F.; Kapiteijn, E. Reinducing Radioiodine-Sensitivity in Radioiodine-Refractory Thyroid Cancer Using Lenvatinib (RESET): Study Protocol for a Single-Center, Open Label Phase II Trial. Diagnostics 2022, 12, 3154. [Google Scholar] [CrossRef] [PubMed]
- Rosignolo, F.; Sponziello, M.; Giacomelli, L.; Russo, D.; Pecce, V.; Biffoni, M.; Bellantone, R.; Lombardi, C.P.; Lamartina, L.; Grani, G.; et al. Identification of Thyroid-Associated Serum microRNA Profiles and Their Potential Use in Thyroid Cancer Follow-Up. J. Endocr. Soc. 2017, 1, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Celano, M.; Rosignolo, F.; Maggisano, V.; Pecce, V.; Iannone, M.; Russo, D.; Bulotta, S. MicroRNAs as Biomarkers in Thyroid Carcinoma. Int. J. Genomics 2017, 2017, 6496570. [Google Scholar] [CrossRef] [PubMed]
- Pecce, V.; Sponziello, M.; Verrienti, A.; Grani, G.; Abballe, L.; Bini, S.; Annunziata, S.; Perotti, G.; Salvatori, M.; Zagaria, L.; et al. The Role of miR-139-5p in Radioiodine-Resistant Thyroid Cancer. J. Endocrinol. Invest. 2023, 46, 2079–2093. [Google Scholar] [CrossRef]
- Huang, I.-C.; Chou, F.-F.; Liu, R.-T.; Tung, S.-C.; Chen, J.-F.; Kuo, M.-C.; Hsieh, C.-J.; Wang, P.-W. Long-Term Outcomes of Distant Metastasis from Differentiated Thyroid Carcinoma. Clin. Endocrinol. (Oxf.) 2012, 76, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Klain, M.; Zampella, E.; Piscopo, L.; Volpe, F.; Manganelli, M.; Masone, S.; Pace, L.; Salvatore, D.; Schlumberger, M.; Cuocolo, A. Long-Term Prognostic Value of the Response to Therapy Assessed by Laboratory and Imaging Findings in Patients with Differentiated Thyroid Cancer. Cancers 2021, 13, 4338. [Google Scholar] [CrossRef] [PubMed]
- Jeong, E.; Yoon, J.-K.; Lee, S.J.; Soh, E.Y.; Lee, J.; An, Y.-S. Risk Factors for Indeterminate Response After Radioactive Iodine Therapy in Patients With Differentiated Thyroid Cancer. Clin. Nucl. Med. 2019, 44, 714–718. [Google Scholar] [CrossRef] [PubMed]
- Tramontin, M.Y.; Nobre, G.M.; Lopes, M.; Carneiro, M.P.; Alves, P.A.G.; de Andrade, F.A.; Vaisman, F.; Corbo, R.; Bulzico, D. High Thyroglobulin and Negative Whole-Body Scan: No Long-Term Benefit of Empiric Radioiodine Therapy. Endocrine 2021, 73, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Rosario, P.W.; Mineiro Filho, A.F.C.; Lacerda, R.X.; dos Santos, D.A.; Calsolari, M.R. The Value of Diagnostic Whole-Body Scanning and Serum Thyroglobulin in the Presence of Elevated Serum Thyrotropin during Follow-up of Anti-Thyroglobulin Antibody-Positive Patients with Differentiated Thyroid Carcinoma Who Appeared to Be Free of Disease after Total Thyroidectomy and Radioactive Iodine Ablation. Thyroid Off. J. Am. Thyroid Assoc. 2012, 22, 113–116. [Google Scholar] [CrossRef] [PubMed]
- Al Hatmi, A.; Jain, A.; Mittal, A.K.; Hussain, S. Evaluation of Diagnostic Value of SPECT/CT Imaging in Post-Radioiodine Therapy in Thyroid Cancer. Sultan Qaboos Univ. Med. J. 2022, 22, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Spanu, A.; Nuvoli, S.; Marongiu, A.; Gelo, I.; Mele, L.; Piras, B.; Madeddu, G. Neck Lymph Node Metastasis Detection in Patients with Differentiated Thyroid Carcinoma (DTC) in Long-Term Follow-up: A 131I-SPECT/CT Study. BMC Cancer 2020, 20, 239. [Google Scholar] [CrossRef] [PubMed]
- Zilioli, V.; Peli, A.; Panarotto, M.B.; Magri, G.; Alkraisheh, A.; Wiefels, C.; Rodella, C.; Giubbini, R. Differentiated Thyroid Carcinoma: Incremental Diagnostic Value of 131I SPECT/CT over Planar Whole Body Scan after Radioiodine Therapy. Endocrine 2017, 56, 551–559. [Google Scholar] [CrossRef] [PubMed]
- Blum, M.; Tiu, S.; Chu, M.; Goel, S.; Friedman, K. I-131 SPECT/CT Elucidates Cryptic Findings on Planar Whole-Body Scans and Can Reduce Needless Therapy with I-131 in Post-Thyroidectomy Thyroid Cancer Patients. Thyroid Off. J. Am. Thyroid Assoc. 2011, 21, 1235–1247. [Google Scholar] [CrossRef] [PubMed]
- Jiang, L.; Xiang, Y.; Huang, R.; Tian, R.; Liu, B. Clinical Applications of Single-Photon Emission Computed Tomography/Computed Tomography in Post-Ablation 131iodine Scintigraphy in Children and Young Adults with Differentiated Thyroid Carcinoma. Pediatr. Radiol. 2021, 51, 1724–1731. [Google Scholar] [CrossRef] [PubMed]
- Jannin, A.; Lamartina, L.; Moutarde, C.; Djennaoui, M.; Lion, G.; Chevalier, B.; Vantyghem, M.C.; Deschamps, F.; Hadoux, J.; Baudin, E.; et al. Bone Metastases from Differentiated Thyroid Carcinoma: Heterogenous Tumor Response to Radioactive Iodine Therapy and Overall Survival. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 2401–2413. [Google Scholar] [CrossRef] [PubMed]
- Zhu, C.; Zhang, M.; Wang, Q.; Jen, J.; Liu, B.; Guo, M. Intratumor Epigenetic Heterogeneity-A Panel Gene Methylation Study in Thyroid Cancer. Front. Genet. 2021, 12, 714071. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Dai, H.; Li, Q.; Shen, G.; Shi, L.; Tian, R. Investigating 18F-FDG PET/CT Parameters as Prognostic Markers for Differentiated Thyroid Cancer: A Systematic Review. Front. Oncol. 2021, 11, 648658. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Dondi, F.; Mazzoletti, A.; Bellini, P.; Rodella, C.; Bertagna, F. Prognostic Role of 2-[18F]FDG PET/CT Metabolic Volume Parameters in Patients Affected by Differentiated Thyroid Carcinoma with High Thyroglobulin Level, Negative 131I WBS and Positive 2-[18F]-FDG PET/CT. Diagn. Basel Switz. 2021, 11, 2189. [Google Scholar] [CrossRef]
- Terroir, M.; Borget, I.; Bidault, F.; Ricard, M.; Deschamps, F.; Hartl, D.; Tselikas, L.; Dercle, L.; Lumbroso, J.; Baudin, E.; et al. The Intensity of 18FDG Uptake Does Not Predict Tumor Growth in Patients with Metastatic Differentiated Thyroid Cancer. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 638–646. [Google Scholar] [CrossRef] [PubMed]
- Singh, I.; Bikas, A.; Garcia, C.A.; Desale, S.; Wartofsky, L.; Burman, K.D. 18F-FDG-PET SUV as a Prognostic Marker of Increasing Size in Thyroid Cancer Tumors. Endocr. Pract. Off. J. Am. Coll. Endocrinol. Am. Assoc. Clin. Endocrinol. 2017, 23, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Klain, M.; Maurea, S.; Gaudieri, V.; Zampella, E.; Volpe, F.; Manganelli, M.; Piscopo, L.; De Risi, M.; Cuocolo, A. The Diagnostic Role of Total-Body 18F-FDG PET/CT in Patients with Multiple Tumors: A Report of the Association of Thyroid Cancer with Lung or Renal Tumors. Quant. Imaging Med. Surg. 2021, 11, 4211–4215. [Google Scholar] [CrossRef] [PubMed]
- Santhanam, P.; Khthir, R.; Solnes, L.B.; Ladenson, P.W. The Relationship of Brafv600e Mutation Status to Fdg Pet/Ct Avidity in Thyroid Cancer: A Review and Meta-Analysis. Endocr. Pract. Off. J. Am. Coll. Endocrinol. Am. Assoc. Clin. Endocrinol. 2018, 24, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.W.; Park, K.W.; Heo, J.H.; Jung, S.-N.; Liu, L.; Kim, S.M.; Kwon, I.S.; Koo, B.S. Relationship Between 18F-Fluorodeoxyglucose Accumulation and the BRAF V600E Mutation in Papillary Thyroid Cancer. World J. Surg. 2018, 42, 114–122. [Google Scholar] [CrossRef] [PubMed]
- Haddad, R.I.; Bischoff, L.; Ball, D.; Bernet, V.; Blomain, E.; Busaidy, N.L.; Campbell, M.; Dickson, P.; Duh, Q.-Y.; Ehya, H.; et al. Thyroid Carcinoma, Version 2.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2022, 20, 925–951. [Google Scholar] [CrossRef] [PubMed]
- Cortas, C.; Charalambous, H. Tyrosine Kinase Inhibitors for Radioactive Iodine Refractory Differentiated Thyroid Cancer. Life 2024, 14, 22. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Liu, P.; Yu, Y.; Zhi, J.; Zheng, X.; Yu, J.; Gao, M. Comparison of Diagnostic Methods for the Detection of a BRAF Mutation in Papillary Thyroid Cancer. Oncol. Lett. 2019. [Google Scholar] [CrossRef] [PubMed]
- Solomon, J.P.; Hechtman, J.F. Detection of NTRK Fusions: Merits and Limitations of Current Diagnostic Platforms. Cancer Res. 2019, 79, 3163–3168. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Li, Y.; Lin, Z.; Chen, W. Can 99 Tc m -3PRGD 2 (α ν β 3 ) and 18 F-FDG Dual-Tracer Molecular Imaging Change the Therapeutic Strategy for Progressive Refractory Differentiated Thyroid Cancer: Case Report. Medicine (Baltimore) 2023, 102, e32751. [Google Scholar] [CrossRef] [PubMed]
- Gao, R.; Zhang, G.-J.; Wang, Y.-B.; Liu, Y.; Wang, F.; Jia, X.; Liang, Y.-Q.; Yang, A.-M. Clinical Value of 99mTc-3PRGD2 SPECT/CT in Differentiated Thyroid Carcinoma with Negative 131I Whole-Body Scan and Elevated Thyroglobulin Level. Sci. Rep. 2018, 8, 473. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Jia, X.; Wang, Y.; Liu, Y.; Yao, X.; Bai, Y.; Han, P.; Chen, S.; Yang, A.; Gao, R. Evaluation of Integrin Avβ3-Targeted Imaging for Predicting Disease Progression in Patients with High-Risk Differentiated Thyroid Cancer (Using 99mTc-3PRGD2). Cancer Imaging 2022, 22, 72. [Google Scholar] [CrossRef] [PubMed]
- Parihar, A.S.; Mittal, B.R.; Kumar, R.; Shukla, J.; Bhattacharya, A. 68 Ga-DOTA-RGD 2 Positron Emission Tomography/Computed Tomography in Radioiodine Refractory Thyroid Cancer: Prospective Comparison of Diagnostic Accuracy with 18 F-FDG Positron Emission Tomography/Computed Tomography and Evaluation Toward Potential Theranostics. Thyroid 2020, 30, 557–567. [Google Scholar] [CrossRef] [PubMed]
- Chernaya, G.; Mikhno, N.; Khabalova, T.; Svyatchenko, S.; Mostovich, L.; Shevchenko, S.; Gulyaeva, L. The Expression Profile of Integrin Receptors and Osteopontin in Thyroid Malignancies Varies Depending on the Tumor Progression Rate and Presence of BRAF V600E Mutation. Surg. Oncol. 2018, 27, 702–708. [Google Scholar] [CrossRef] [PubMed]
- Coerts, H.I.; De Keizer, B.; Verburg, F.A. Advances in the Development of Positron Emission Tomography Tracers for Improved Detection of Differentiated Thyroid Cancer. Cancers 2024, 16, 1401. [Google Scholar] [CrossRef] [PubMed]
- Volpe, F.; Nappi, C.; Piscopo, L.; Zampella, E.; Mainolfi, C.G.; Ponsiglione, A.; Imbriaco, M.; Cuocolo, A.; Klain, M. Emerging Role of Nuclear Medicine in Prostate Cancer: Current State and Future Perspectives. Cancers 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Hofman, M.S.; Emmett, L.; Sandhu, S.; Iravani, A.; Joshua, A.M.; Goh, J.C.; Pattison, D.A.; Tan, T.H.; Kirkwood, I.D.; Ng, S.; et al. [177Lu]Lu-PSMA-617 versus Cabazitaxel in Patients with Metastatic Castration-Resistant Prostate Cancer (TheraP): A Randomised, Open-Label, Phase 2 Trial. Lancet Lond. Engl. 2021, 397, 797–804. [Google Scholar] [CrossRef] [PubMed]
- Alan-Selcuk, N.; Beydagi, G.; Demirci, E.; Ocak, M.; Celik, S.; Oven, B.B.; Toklu, T.; Karaaslan, I.; Akcay, K.; Sonmez, O.; et al. Clinical Experience with [225Ac]Ac-PSMA Treatment in Patients with [177Lu]Lu-PSMA–Refractory Metastatic Castration-Resistant Prostate Cancer. J. Nucl. Med. 2023, 64, 1574–1580. [Google Scholar] [CrossRef] [PubMed]
- Demirci, E.; Ocak, M.; Kabasakal, L.; Decristoforo, C.; Talat, Z.; Halaç, M.; Kanmaz, B. (68)Ga-PSMA PET/CT Imaging of Metastatic Clear Cell Renal Cell Carcinoma. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1461–1462. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.S.; Reuter, V.E.; Heston, W.D.; Bander, N.H.; Grauer, L.S.; Gaudin, P.B. Five Different Anti-Prostate-Specific Membrane Antigen (PSMA) Antibodies Confirm PSMA Expression in Tumor-Associated Neovasculature. Cancer Res. 1999, 59, 3192–3198. [Google Scholar] [PubMed]
- Bychkov, A.; Vutrapongwatana, U.; Tepmongkol, S.; Keelawat, S. PSMA Expression by Microvasculature of Thyroid Tumors – Potential Implications for PSMA Theranostics. Sci. Rep. 2017, 7, 5202. [Google Scholar] [CrossRef] [PubMed]
- Heitkötter, B.; Steinestel, K.; Trautmann, M.; Grünewald, I.; Barth, P.; Gevensleben, H.; Bögemann, M.; Wardelmann, E.; Hartmann, W.; Rahbar, K.; et al. Neovascular PSMA Expression Is a Common Feature in Malignant Neoplasms of the Thyroid. Oncotarget 2018, 9, 9867–9874. [Google Scholar] [CrossRef] [PubMed]
- Verma, P.; Malhotra, G.; Agrawal, R.; Sonavane, S.; Meshram, V.; Asopa, R.V. Evidence of Prostate-Specific Membrane Antigen Expression in Metastatic Differentiated Thyroid Cancer Using 68Ga-PSMA-HBED-CC PET/CT. Clin. Nucl. Med. 2018, 43, e265–e268. [Google Scholar] [CrossRef]
- Verburg, F.A.; Krohn, T.; Heinzel, A.; Mottaghy, F.M.; Behrendt, F.F. First Evidence of PSMA Expression in Differentiated Thyroid Cancer Using [68Ga]PSMA-HBED-CC PET/CT. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1622–1623. [Google Scholar] [CrossRef] [PubMed]
- Lütje, S.; Gomez, B.; Cohnen, J.; Umutlu, L.; Gotthardt, M.; Poeppel, T.D.; Bockisch, A.; Rosenbaum-Krumme, S. Imaging of Prostate-Specific Membrane Antigen Expression in Metastatic Differentiated Thyroid Cancer Using 68Ga-HBED-CC-PSMA PET/CT. Clin. Nucl. Med. 2017, 42, 20–25. [Google Scholar] [CrossRef] [PubMed]
- de Vries, L.H.; Lodewijk, L.; Braat, A.J.A.T.; Krijger, G.C.; Valk, G.D.; Lam, M.G.E.H.; Borel Rinkes, I.H.M.; Vriens, M.R.; de Keizer, B. 68Ga-PSMA PET/CT in Radioactive Iodine-Refractory Differentiated Thyroid Cancer and First Treatment Results with 177Lu-PSMA-617. EJNMMI Res. 2020, 10, 18. [Google Scholar] [CrossRef]
- Pishdad, R.; Treglia, G.; Mehta, A.; Santhanam, P. Somatostatin Receptor Imaging of Thyroid Tissue and Differentiated Thyroid Cancer Using Gallium-68-Labeled Radiotracers—a Review of Clinical Studies. Endocrine 2024. [Google Scholar] [CrossRef]
- Sancak, S.; Hardt, A.; Singer, J.; Klöppel, G.; Eren, F.T.; Güllüoglu, B.M.; Sen, L.S.; Sever, Z.; Akalin, N.S.; Eszlinger, M.; et al. Somatostatin Receptor 2 Expression Determined by Immunohistochemistry in Cold Thyroid Nodules Exceeds That of Hot Thyroid Nodules, Papillary Thyroid Carcinoma, and Graves’ Disease. Thyroid Off. J. Am. Thyroid Assoc. 2010, 20, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Pisarek, H.; Stepień, T.; Kubiak, R.; Borkowska, E.; Pawlikowski, M. Expression of Somatostatin Receptor Subtypes in Human Thyroid Tumors: The Immunohistochemical and Molecular Biology (RT-PCR) Investigation. Thyroid Res. 2009, 2, 1. [Google Scholar] [CrossRef] [PubMed]
- Klagge, A.; Krause, K.; Schierle, K.; Steinert, F.; Dralle, H.; Fuhrer, D. Somatostatin Receptor Subtype Expression in Human Thyroid Tumours. Horm. Metab. Res. Horm. Stoffwechselforschung Horm. Metab. 2010, 42, 237–240. [Google Scholar] [CrossRef] [PubMed]
- Teunissen, J.J.M.; Kwekkeboom, D.J.; Kooij, P.P.M.; Bakker, W.H.; Krenning, E.P. Peptide Receptor Radionuclide Therapy for Non-Radioiodine-Avid Differentiated Thyroid Carcinoma. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2005, 46 Suppl 1, 107S–14S. [Google Scholar]
- Piscopo, L.; Zampella, E.; Pellegrino, S.; Volpe, F.; Nappi, C.; Gaudieri, V.; Fonti, R.; Vecchio, S.D.; Cuocolo, A.; Klain, M. Diagnosis, Management and Theragnostic Approach of Gastro-Entero-Pancreatic Neuroendocrine Neoplasms. Cancers 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Subramaniam, R.M. Diagnosis and Treatment of Lung Neuroendocrine Neoplasms: Somatostatin Receptor PET Imaging and Peptide Receptor Radionuclide Therapy. PET Clin 2023, 18, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Gallicchio, R.; Giordano, A.; Milella, M.; Storto, R.; Pellegrino, T.; Nardelli, A.; Nappi, A.; Tarricone, L.; Storto, G. Ga-68-Edotreotide Positron Emission Tomography/Computed Tomography Somatostatin Receptors Tumor Volume Predicts Outcome in Patients With Primary Gastroenteropancreatic Neuroendocrine Tumors. Cancer Control 2023, 30, 10732748231152328. [Google Scholar] [CrossRef] [PubMed]
- Fortunati, E.; Bonazzi, N.; Zanoni, L.; Fanti, S.; Ambrosini, V. Molecular Imaging Theranostics of Neuroendocrine Tumors. Semin. Nucl. Med. 2023, 53, 539–554. [Google Scholar] [CrossRef] [PubMed]
- Duan, H.; Ferri, V.; Fisher, G.; Shaheen, S.; Davidzon, G.; Moradi, F.; Nguyen, J.; Franc, B.; Iagaru, A.; Aparici, C.M. Evaluation of Interim 68Ga-Dotatate PET after Two Cycles of Peptide Receptor Radionuclide Therapy (PRRT) in Neuroendocrine Tumors (NET). Clin. Nucl. Med. 2023, 48, e276. [Google Scholar]
- Donohoe, K.J.; Aloff, J.; Avram, A.M.; Bennet, K.G.; Giovanella, L.; Greenspan, B.; Gulec, S.; Hassan, A.; Kloos, R.T.; Solórzano, C.C.; et al. Appropriate Use Criteria for Nuclear Medicine in the Evaluation and Treatment of Differentiated Thyroid Cancer. J. Nucl. Med. 2020, 61, 375–396. [Google Scholar] [CrossRef] [PubMed]
- Bertagna, F.; Albano, D.; Giovanella, L.; Giubbini, R.; Treglia, G. F18-Choline/C11-Choline PET/CT Thyroid Incidentalomas. Endocrine 2019, 64, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Durmo, R.; Bertagna, F.; Giubbini, R. 18F-Choline PET/CT Incidental Thyroid Uptake in Patients Studied for Prostate Cancer. Endocrine 2019, 63, 531–536. [Google Scholar] [CrossRef] [PubMed]
- Piccardo, A.; Trimboli, P.; Puntoni, M.; Foppiani, L.; Treglia, G.; Naseri, M.; Bottoni, G.L.; Massollo, M.; Sola, S.; Ferrarazzo, G.; et al. Role of 18F-Choline Positron Emission Tomography/Computed Tomography to Detect Structural Relapse in High-Risk Differentiated Thyroid Cancer Patients. Thyroid Off. J. Am. Thyroid Assoc. 2019, 29, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Fozzatti, L.; Cheng, S. Tumor Cells and Cancer-Associated Fibroblasts: A Synergistic Crosstalk to Promote Thyroid Cancer. Endocrinol. Metab. 2020, 35, 673–680. [Google Scholar] [CrossRef]
- Dvorak Harold, F. Tumors: Wounds That Do Not Heal. N. Engl. J. Med. 1986, 315, 1650–1659. [Google Scholar] [CrossRef] [PubMed]
- Kratochwil, C.; Flechsig, P.; Lindner, T.; Abderrahim, L.; Altmann, A.; Mier, W.; Adeberg, S.; Rathke, H.; Röhrich, M.; Winter, H.; et al. 68Ga-FAPI PET/CT: Tracer Uptake in 28 Different Kinds of Cancer. J. Nucl. Med. 2019, 60, 801. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Zheng, S.; Zhang, J.; Yao, S.; Miao, W. 68Ga-DOTA-FAPI-04 PET/CT Imaging in Radioiodine-Refractory Differentiated Thyroid Cancer (RR-DTC) Patients. Ann. Nucl. Med. 2022, 36, 610–622. [Google Scholar] [CrossRef] [PubMed]
- Ballal, S.; Yadav, M.P.; Roesch, F.; Satapathy, S.; Moon, E.S.; Martin, M.; Wakade, N.; Sheokand, P.; Tripathi, M.; Chandekar, K.R.; et al. Head-to-Head Comparison of [68Ga]Ga-DOTA.SA.FAPi with [18F]F-FDG PET/CT in Radioiodine-Resistant Follicular-Cell Derived Thyroid Cancers. Eur. J. Nucl. Med. Mol. Imaging 2023. [CrossRef]
- Ballal, S.; Yadav, M.P.; Moon, E.S.; Rösch, F.; ArunRaj, S.T.; Agarwal, S.; Tripathi, M.; Sahoo, R.K.; Bal, C. First-in-Human Experience With 177Lu-DOTAGA.(SA.FAPi)2 Therapy in an Uncommon Case of Aggressive Medullary Thyroid Carcinoma Clinically Mimicking as Anaplastic Thyroid Cancer. Clin. Nucl. Med. 2022, 47, e444–e445. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New Response Evaluation Criteria in Solid Tumours: Revised RECIST Guideline (Version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Fu, H.; Huang, J.; Zhao, T.; Wang, H.; Chen, Y.; Xu, W.; Pang, Y.; Guo, W.; Sun, L.; Wu, H.; et al. Fibroblast Activation Protein-Targeted Radioligand Therapy with 177Lu-EB-FAPI for Metastatic Radioiodine-Refractory Thyroid Cancer: First-in-Human, Dose-Escalation Study. Clin. Cancer Res. 2023, 29, 4740–4750. [Google Scholar] [CrossRef] [PubMed]
- Schlumberger, M.; Tahara, M.; Wirth, L.J.; Robinson, B.; Brose, M.S.; Elisei, R.; Habra, M.A.; Newbold, K.; Shah, M.H.; Hoff, A.O.; et al. Lenvatinib versus Placebo in Radioiodine-Refractory Thyroid Cancer. N. Engl. J. Med. 2015, 372, 621–630. [Google Scholar] [CrossRef] [PubMed]
- Porcelli, T.; Luongo, C.; Sessa, F.; Klain, M.; Masone, S.; Troncone, G.; Bellevicine, C.; Schlumberger, M.; Salvatore, D. Long-Term Management of Lenvatinib-Treated Thyroid Cancer Patients: A Real-Life Experience at a Single Institution. Endocrine 2021, 73, 358–366. [Google Scholar] [CrossRef] [PubMed]
- Wirth, L.J.; Durante, C.; Topliss, D.J.; Winquist, E.; Robenshtok, E.; Iwasaki, H.; Luster, M.; Elisei, R.; Leboulleux, S.; Tahara, M. Lenvatinib for the Treatment of Radioiodine-Refractory Differentiated Thyroid Cancer: Treatment Optimization for Maximum Clinical Benefit. The Oncologist 2022, 27, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Lieberman, L.; Worden, F. Novel Therapeutics for Advanced Differentiated Thyroid Cancer. Endocrinol. Metab. Clin. North Am. 2022, 51, 367–378. [Google Scholar] [CrossRef] [PubMed]
- Iravani, A.; Solomon, B.; Pattison, D.A.; Jackson, P.; Ravi Kumar, A.; Kong, G.; Hofman, M.S.; Akhurst, T.; Hicks, R.J. Mitogen-Activated Protein Kinase Pathway Inhibition for Redifferentiation of Radioiodine Refractory Differentiated Thyroid Cancer: An Evolving Protocol. Thyroid 2019, 29, 1634–1645. [Google Scholar] [CrossRef] [PubMed]
- Leboulleux, S.; Benisvy, D.; Taieb, D.; Attard, M.; Bournaud, C.; Terroir, M.; Ghuzlan, A.A.; Lamartina, L.; Schlumberger, M.J.; Godbert, Y.; et al. MERAIODE: A Redifferentiation Phase II Trial with Trametinib Followed by Radioactive Iodine for Metastatic Radioactive Iodine Refractory Differentiated Thyroid Cancer Patients with a RAS Mutation. Ann. Oncol. 2021, 32, S1204. [Google Scholar] [CrossRef]
- Balakirouchenane, D.; Seban, R.; Groussin, L.; Puszkiel, A.; Cottereau, A.S.; Clerc, J.; Vidal, M.; Goldwasser, F.; Arrondeau, J.; Blanchet, B.; et al. Pharmacokinetics/Pharmacodynamics of Dabrafenib and Trametinib for Redifferentiation and Treatment of Radioactive Iodine-Resistant Mutated Advanced Differentiated Thyroid Cancer. Thyroid® 2023, 33, 1327–1338. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
No evidence of pathological RAI uptake foci. A) PT-WBS anterior view; B) PT-WBS posterior view.
Figure 1.
No evidence of pathological RAI uptake foci. A) PT-WBS anterior view; B) PT-WBS posterior view.
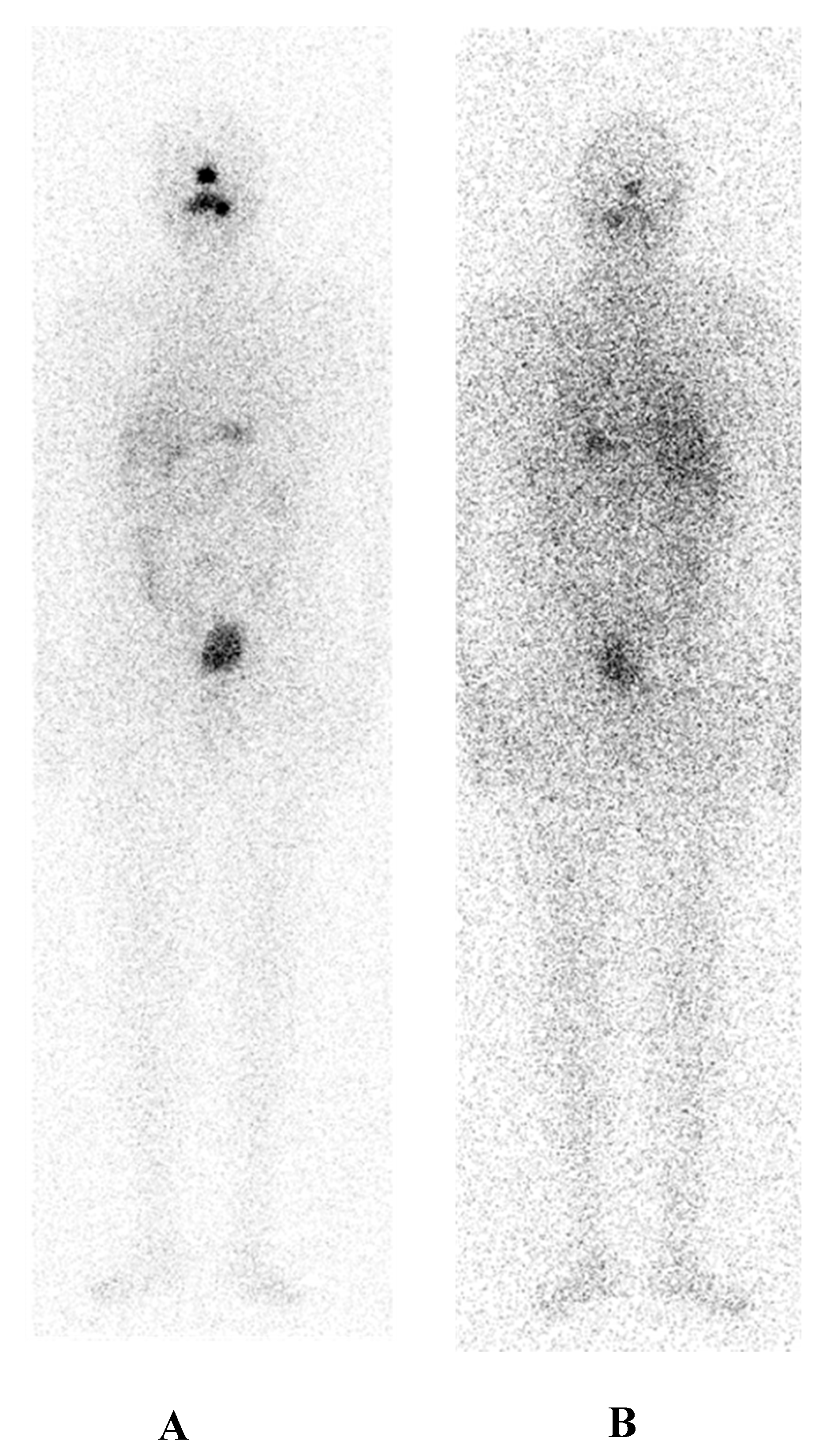
Figure 2.
Focal RAI accumulation in upper left cervical region; diffuse and intense RAI uptake in pulmonary field. A) PT-WBS anterior view; B) PT-WBS posterior view.
Figure 2.
Focal RAI accumulation in upper left cervical region; diffuse and intense RAI uptake in pulmonary field. A) PT-WBS anterior view; B) PT-WBS posterior view.
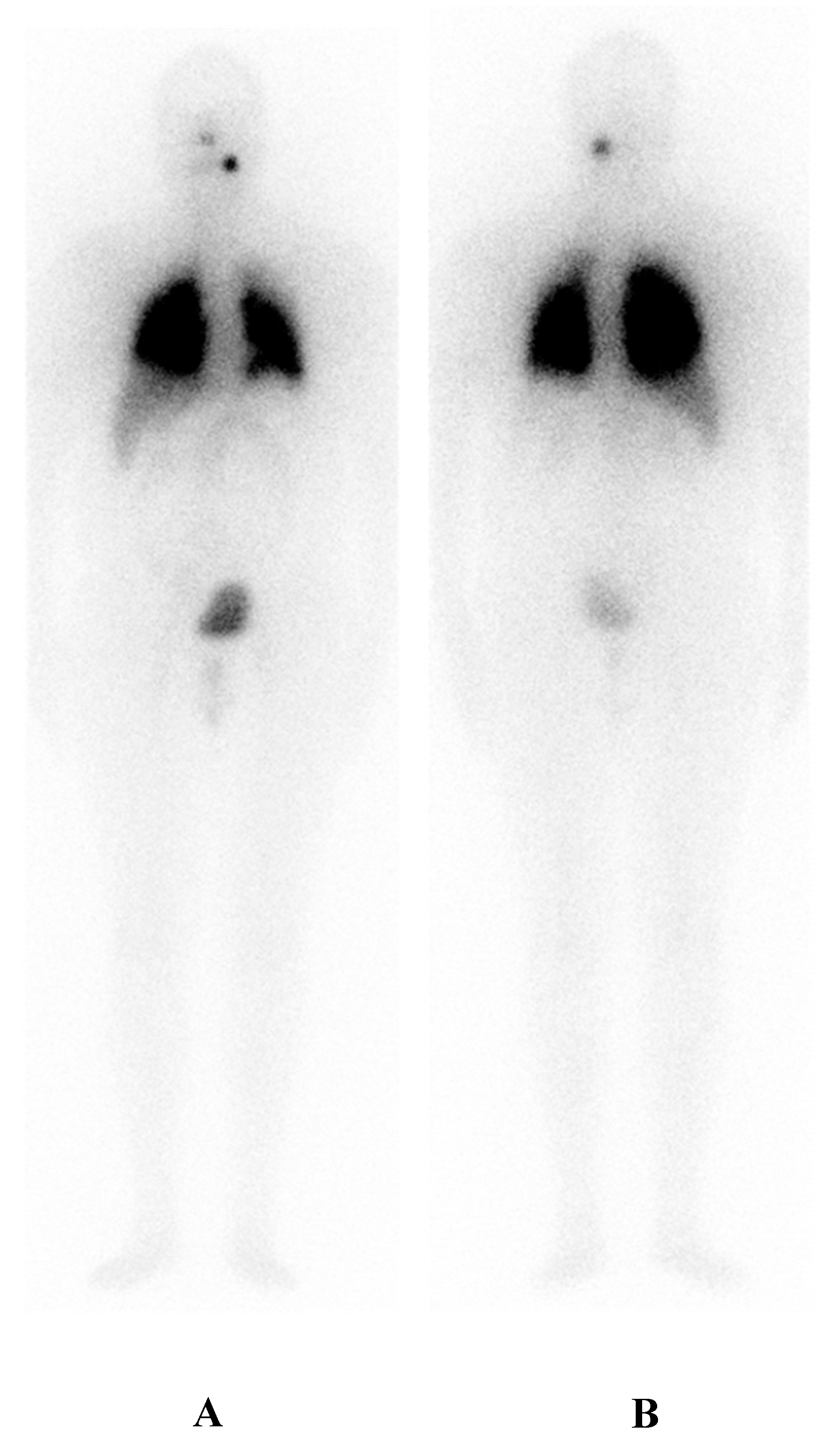
Figure 3.
A) High RAI accumulation in posterior mandibular lymph node. B) Diffuse, intense and bilateral RAI uptake in pulmonary tissue.
Figure 3.
A) High RAI accumulation in posterior mandibular lymph node. B) Diffuse, intense and bilateral RAI uptake in pulmonary tissue.
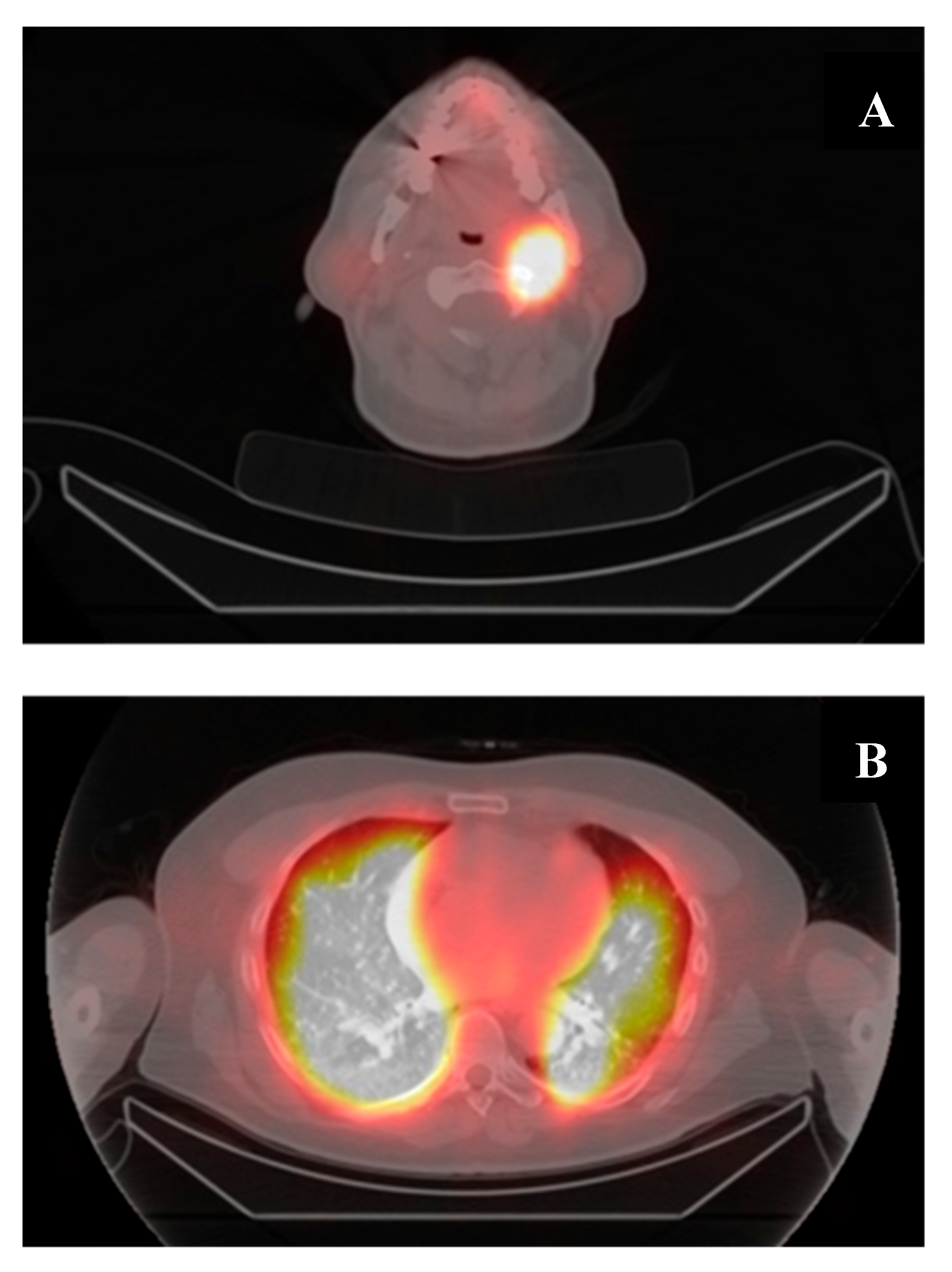

Table 1.
ATA 2015 RAIR categories.
| I. | Malignant/metastatic tissue cannot concentrate RAI on a diagnostic radioiodine scan. |
| II. | Malignant tissue cannot concentrate RAI on a post-131I therapy scan. |
| III. | The tumor loses the ability to concentrate RAI after previous evidence of RAI-avid disease. |
| IV. | RAI is concentrated in some lesions only. |
| V. | Metastasis progression even with significant RAI uptake. |
| VI. | > 600 mCi of cumulated 131I therapy. |
Radioactive Iodine Refractory (RAIR); Radioactive Iodine (RAI).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



