Submitted:
27 May 2024
Posted:
29 May 2024
You are already at the latest version
Abstract
Leptospirosis is a worldwide zoonotic disease, most common in tropical and rural settings. It's a public health problem in most of the French tropical overseas territories. The primary objective of this study was to describe severe forms of leptospirosis admitted to the intensive care unit (ICU) on Mayotte, a French island in the Indian Ocean. The secondary objective was to compare the characteristics of these patients with those admitted to the ICU in other French tropical territories and in mainland France.
We conducted a retrospective study among adult patients admitted to the ICU of Mayotte hospital between 2009 and 2017. The diagnosis mainly relied on a positive PCR in blood or urine samples. The results were compared to the similar and available studies carried out in mainland France and in the other French tropical overseas territories.
On the study period, 55 patients were admitted in the ICU for leptospirosis (18% of the leptospirosis admitted in the hospital). Among them, 45 (82%) were male and the median age was 44 years (25-75 IQR: 33-55). The median time between first symptoms and ICU admission was 3.5 days (2-5). The median duration for antibiotic treatment, hospital stay, and ICU stay were 7 days (7-8), 9 days (6-13) and 5 days (3-9) respectively. The main acute organ impairments were acute renal failure (87%), followed by circulatory failure (58%), acute liver failure (45%) and neurological failure (22%). The most frequently used supportive cares were: vaso-active drugs (56%) and renal replacement (56%), and mechanical ventilation (27%). The case-fatality rate was low (5%). Genotype identification could be performed on 19 patients’ isolates. The strain L. borgpetersenii serogroup Mini cgMLST CG78 was predominant (n=14), followed by L. interrogans serogroup Pyrogenes cgMLST CG 81 (n=4). No L. interrogans serogroup Icterohemorrhagiae was identified.
We publish here the first series of severe patients admitted in the ICU in Mayotte, a French island with a high incidence rate of leptospirosis but with original strain specificities. Despite very severe clinical pictures, mortality remains rather low.
Keywords:
leptospirosis
; zoonosis
; mayotte
; severe infectious disease
Background
Leptospirosis is a worldwide zoonotic disease, most common in tropical and rural settings. Its significant mortality rate may be related to the lack of medical care infrastructures and inadequate diagnosis as well as other reasons such as strain virulence factors, infecting inoculum dose and host immunopathological responses [1,2,3,4]. France has one of the highest endemicity levels in Europe, 1.10 cases per 100,000 inhabitants per year in 2020-2021 [5]. However, this high incidence doesn’t include the high overseas territories incidences distributed in various tropical areas of the globe, including Mayotte island, located in the northern part of the Mozambique Channel. Leptospirosis is endemic in Mayotte where its incidence is about 80 times higher than in mainland France. Besides, the diversity of leptospiral strains is somewhat atypical [6,7,8,9,10,11]. Indeed, the French National Reference Center for Leptospirosis (FNRCL) reported that strains isolated from human cases of the islands have a high genetic diversity and some belong to a species firstly described: Leptospira mayottensis [4]. However, despite these particularities limited data exist on the severity of leptospirosis cases in this territory, compared to other French tropical settings and mainland France [12,13,14,15,16,17,18,19]. The first objective of the present study was to describe severe forms of leptospirosis in Mayotte. The secondary objectives were to describe the leptospiral strains identified in severe patients and compare the characteristics of these severe patients to those of the other French tropical settings and mainland France.
Methods
Settings
The French overseas territories are divided into 3 main regions: 1. the Indian Ocean territories, comprising Reunion Island, Est of Madagascar in the Mascareignes Archipelago, Mayotte and the French Southern and Antarctic Lands; 2. the French territories of America, with French Guiana, the only continental territory, located between Brazil and Surinam, the French West Indies, in the Lesser Caribbean, Martinique and Guadeloupe and their dependencies and Saint Pierre et Miquelon, islands located in the Atlantic Ocean close to Canada; 3. the Pacific Ocean territories, including French Polynesia, and New Caledonia.
Mayotte is a French island belonging to the French overseas territories and located in the northern part of the Mozambique Channel in the Indian Ocean off the coast of Southeastern Africa, between Northwestern Madagascar and Northeastern Mozambique (Figure 1). Its area covers 374 km2 and has a population of 310,022 inhabitants according to January 2023 official estimates (www.insee.fr). The main hospital, the Centre Hospitalier de Mayotte (CHM), is located in Mamoudzou, the main city of the island. The climate is tropical with maritime trade winds. Average temperatures fluctuate between 23 and 30°C and humidity levels often exceed 85%. There are two main seasons, separated by two shorter inter-seasons: the rainy season, which runs from November to April, and the dry season. It is estimated that three quarters of the population live below the poverty threshold, more than five times higher than in mainland France. Finally, around half of the population is under 18 years old.
Study Design
We conducted a retrospective study among patients admitted to the intensive care unit (ICU) of the CHM, between May 1st 2009 and May 31st 2017.
Inclusion and Exclusion Criteria and Case Definition
Patients with leptospirosis admitted for more than one night in the ICU were included. The diagnosis of leptospirosis relied on a positive PCR or ELISA IgM assay performed on blood or urine. Patients <18 years of age were not included.
The patients were identified through the analysis of laboratory and ICU databases to identify the total number of patients supported in the hospital and the proportion of patients admitted in ICU.
Polymerase Chain Reaction Diagnostics, Culture and Characterisation of the Isolates
The plasma of samples positive for the presence of Leptospira by PCR were inoculed in EMJH culture medium to isolate strains and incubated at 30°C for 2 months [20,21]. Extraction DNA, sequencing and genomic identification of the isolated Leptospira species was performed using a core genome multilocus sequence typing (cgMLST) scheme based on 545 highly conserved loci and clonal groups (CG) were defined using a single linkage clustering threshold of 40 allelic mismatches, as developed by Guglielmini et al. [22]. The data are available on the (https://bigsdb.pasteur.fr/leptospira). The MAT was used for serogroup (sg) characterisation with a standard battery of rabbit antisera against reference serovars representing the 24 serogroups [11].
Data Collect and Analysis
The following variables were collected in the medical records of the CHM, using Microsoft Excel 2013: age, gender, date of onset of the symptoms, date of positive PCR, admission to hospital, admission in the Intensive Care Unit, medical history, activity at risk of leptospirosis (including profession-category and leisure), symptoms, results of radiology and biological exams, and treatment (including vaso-active drugs, mechanical ventilation, dialysis, extracorporeal membrane oxygenation (ECMO)) and outcome. The data analysis was performed using the software Microsoft Excel 2021, and Stata 18.0 (StataCorp, College Station Texas, US). Continuous variables were given in median and interquartile range (IQR) and categorical variable in number and percentage. Several continuous variables, in particular biological variables, were dichotomized into categorical variables, according to the most widely accepted categories in the medical literature, but also according to previous publications on severe leptospirosis in the French overseas territories and mainland France.
Definitions of the Variables
Oligouria was defined by a diuresis of less than 400 ml per 24 hours. Pulmonary involvement was defined by pulmonary auscultation abnormalities and/or interstitial syndrome or alveolar syndrome or pleural effusion on chest radiographic. Intra-alveolar hemorrhage was defined by macroscopically bloody bronchial aspirations associated with alveolar-interstitial syndrome on chest radiography. ARDS was defined according to the Berlin definition [23].Cardiogenic shock was defined as ventricular dysfunction on echocardiography combined with low cardiac output syndrome and/or low blood pressure and/or hyperlactatemia (2008, Reynolds, Circulation, Cardiogenic shock: current concepts and improving outcomes). Sepsis was defined as infection or suspected infection with systemic inflammatory response syndrome.
Comparison to Other Settings
Secondly, we compared the results of the study carried out in Mayotte with the results of similar and available studies carried out in mainland France and in the other French tropical overseas territories, on severe and/or intensive care leptospirosis. Variables were compared with those obtained in the articles cited above two by two, using Fisher’s exact test for categorical variables and Student’s t-test for continuous variables, when means with standard deviation were available. When the result given in the article was exclusively median and interquartile range 25%-75%, the comparison could not be made. As every variable was different from a study to another, the various variables of the patients of our study were described using each study cut-off, especially for biological variable. For example, we created 4 different variables for hemoglobin level, (8, 10, 12 and 12.2 g/dL), to afford comparison to other studies.
Ethical Aspects
This research met the reference methodology for personal data processing not requiring the written consent of patients (MR-004). It was carried out in accordance with the Declaration of Helsinki (full version on: http://www.wma.net/en/30publications/10policies/b3/). A collective information note was hung on the wall in the Intensive Care Unit and the Emergency Room of Centre Hospitalier de Mayotte (CHM).. Furthermore, a personal informative note was sent to all patients identified as candidates for inclusion. If they did not wish their medical data to be used for this study, they were asked to return a notification to the investigators indicating their refusal to participate, within one month.
Results
Baseline Patients’ Characteristics
On the study period, 304 patients were hospitalized in Mayotte hospital with a PCR-confirmed leptospirosis, among whom 55 (18%) were admitted in ICU (Table 1 and Figure 2).
Among the 55 patients admitted in ICU, 45 (82%) were male (male to female sex ratio = 4.5). The median age was 44 years (25-75 IQR: 33-55; range 17-77) (Table 2). There was no significant difference in the proportion of men compared with Reunion, French Guiana, Guadeloupe and mainland France, but there were more men than in the New Caledonia series. The average age of patients was not different from that of patients in French Guiana and New Caledonia, but patients were significantly younger than those in Guadeloupe. A quarter of patients had one or more comorbidities (25%), among which diabetes and hypertension were over-represented (10% and 7%, respectively). The proportion of patients with comorbidities was no different from that of Reunion and French Guiana, except for tobacco consumption, which was much lower in Mayotte than in Reunion. Risk factors were frequently identified among the patients: 64% had a profession exposing to the disease, 46% an exposing leisure activity and 54% reported a contact with rodents, without any significant difference with other studies, when the data were available, except for exposition to rodents, that was more frequent compared to patients from mainland France.
Clinical Patients’ Characteristics at the Admission in ICU ?
The median time between onset of symptoms and hospital admission was 3 days (IQR 25%–75%: 2-5), the median time between first symptoms and initiation of antibiotic therapy was 3 days (2-5), the median time between first symptoms and ICU admission was 3.5 days (2-5) (Table 2). The median duration for antibiotic treatment, hospital stay, and ICU stay were 7 days (7-8), 9 days (6-13) and 5 days (3-9) respectively. The main clinical features found in the patients at the admission in ICU were: temperature > 38°C (65%), myalgia (65%), low systolic blood pressure (<100 mmHg) (65%), oligo-anuria (65%), abdominal pain (62%) and jaundice (58%) (Table 3). Compared to la Reunion, Mayotte’s patients had significantly more abdominal pain (62% vs 36%), but less myalgia (65% vs. 80%), nausea or vomits (25 vs. 48%), hemorrhagic syndrome (4% vs. 54%), hemoptysis (2% vs. 31%) and cough (7% vs. 35%). Compared to French Guiana, they had more jaundice and less diarrhea, compared to Guadeloupe they had more fever >37.7°C (69% vs. 44%), less hypothermia (9% vs. 30%), less hepatosplenomegaly (7% vs. 64%), less hemorrhagic syndrome (4% vs. 21%), and less meningeal syndrome (0% vs. 17%). Compared to French Polynesia, Mayotte’s patients had more frequently fever > 38°C (65% vs. 46%) but less oligo-anuria (65% vs. 93%) and headaches (19% vs. 87%). Among available variables, there was no difference in clinical characteristics with severe patients from Martinique and French Polynesia. At last, there was several differences with the ICU patients from mainland France with more abdominal pain (62% vs. 26%), chest pain (15% vs. 4%), confusion (23% vs. 7%) and less cough (7% vs. 22%).
Biological Patients’ Characteristics at the Admission
On admission, patients had a mean leukocyte count of 11.9 G/L, PNN of 11.0 G/L and CRP of 299 mg/L. Mean thrombocytopenia was 72 G/L, median prothrombin level 69%, mean transaminases 4120 and 152 for AST and ALT respectively, mean total bilirubin 196.1 µmol/L, mean plasma urea 23.0 mmol/L, and creatinine 386 µmol/L. The proportion of patients with thrombocytopenia appeared to be higher than in French Guiana, but with no difference compared with other territories. Liver and kidney damage were more severe in Mayotte patients than in French Guiana patients, but with no significant difference from other territories.
Outcome
The main acute organ impairments were acute renal failure (87%), followed by circulatory failure (58%), acute liver failure (45%) and neurological failure (22%). The most frequently used supportive cares were: vaso-active drugs for shock (56%) and renal replacement for acute renal failure (56%), and mechanical ventilation (27%). Compared to mainland France, circulatory failure (58 vs. 21%), acute kidney failure (87% vs. 15%), central nervous system failure (22 vs. 6%) and acute liver failure (45% vs. 5%) were significantly more frequent in Mayotte than in mainland France. Dialysis was more frequently used in Mayotte than in mainland France (56% vs. 35%). Acute respiratory failure was less frequent in Mayotte than in Reunion Island (11% vs. 57%) and French Guiana (11% vs. 42%). In the same way mechanical ventilation was less often used in Mayotte than in French Guiana (27% vs. 75%), Martinique (27% vs. 67%) and mainland France (27% vs. 36%).
Vaso-active drugs for shock were less often used than in Martinique (56% vs. 89%) and blood transfusion was less frequent than in Martinique and New Caledonia (11% vs. 67% and 11% vs. 32%), respectively.
There was no significant difference in the case-fatality rates between Mayotte (5%) and Martinique (0%), La Réunion (6%), French Polynesia (7%), mainland France (9%), and New Caledonia (14%). However, this mortality was higher in French Guiana (25%, p=0.065) and Guadeloupe (25%, p=0.02).
Identification of the Strains
A core genome MLST (cgMLST) genotyping scheme applicable to identification could be performed on 19 patients’ isolates (Table 5). The strain L. borgpetersenii serogroup Mini cgMLST CG78 was predominant (n=13), followed by L. interrogans sg Pyrogenes cgMLST CG 81(n=4), L. mayottensis sg Mini cgMLST CG79(n=1) and L. kirschneri Mini cgMLST CG63. The FNRCL data, after sequencing of 91 strains from patients hospitalized of varying severity (mild to very severe) during the period from 2007 to 2017 enabled us to define 11 cgMLST GCs (Table 5). The most frequently found strains were L. borgpetersenii Mini SG78 (n=37), L. mayottensis sg Unknown SG82 (n=18) and L. interrogans Pyrogenes SG81. No L. interrogans serogroup Icterohemorrhagiae cgMLST CG6 was identified, which significantly differs from the other tropical overseas French territories where 94%, 92%, 82%, 75% and 56% of cases were L. interrogans serovar Icterohemorrhagiae, for Reunion, Martinique, New Caledonia, Guadeloupe and French Guiana, No information was available for the strains identified in the study on the severe leptospirosis in the French ICUs.
Discussion
This is the first published study of severe cases on the island of Mayotte, a territory characterized by specific bacterial strains and although a more recent publication referred to severe cases in Mayotte, without specifically studying ICU cases [19]. The absence of severe cases linked to the Icterohaemorrhagiae strain was already demonstrated in previous studies. The L. mayottensis strain is also found, as is serogroup Mini, which has been frequently described in previous studies in Mayotte [4,11,24]. However, it is important to note that despite a wide diversity of Leptospira strains circulating in humans in Mayotte, two strains seem to predominate in severe forms, namely L. borgpetersenii sg Mini SG78 and L.interrogans sg Pyrogenes SG81.
The profile of the patients was quite classical, represented by young men of working age, with little prior medical history. Gender distribution was identical in all territories, with an over-representation of males found in most studies worldwide [25]. Only New Caledonia seemed to have a male-female sex ratio inferior to 2 which has already been found in this territory [26]. It was not possible to make a satisfactory statistical comparison of the age of patients from Mayotte with that of patients in the other studies. However, it appears that the average age was broadly comparable to that found in Reunion and French Guiana, whereas it was lower than that found in Guadeloupe and mainland France. This can probably be explained by the age distribution in the various territories, Mayotte and French Guiana being known to have a younger population than the other overseas territories and mainland France [27]. Patients with severe leptospirosis had less prior medical history than in the other territories, including cigarette smoking and chronic alcoholism, an observation probably linked to Islam being largely practiced in the Comoros [28].
There was a fairly long delay in treating these patients, with more than half consulting a doctor more than five days after the onset of signs. This may explain the short delay between admission to intensive care and death.
On the other hand, probably because the disease is relatively well known on the island, the diagnosis of leptospirosis was mentioned in almost four out of five cases on admission, far more frequently than in French Guiana or mainland France [13,18,29]. Thus leptospirosis has been recognized as a frequent cause of fever for less than 10 years in French Guiana, and remains a diagnosis that is rarely evoked in the first instance in France [30,31].
Except the study from Martinique, the lethality of severe leptospirosis admitted in ICU in this period was quite low compared to the other territories. Several factors could explain this phenomenon: 1. the extreme youthfulness of the population, with an inverted age pyramid compared with other territories such as Reunion, the French West Indies and mainland France; 2. The absence of Icterohaemorrhagiae strain which is considered as a major risk of severe and lethal forms in some studies [14,32]; 3. The rapid evocation of the diagnosis, with no delay in initiating antibiotic therapy once the patient has been admitted to hospital, thanks to a high level of awareness among the medical profession in Mayotte of the frequency of this disease in cases of fever.
Despite the absence of the Icterohaemorrhagiae strain identified in patients admitted in the ICU, the clinical presentation of intensive care patients in Mayotte seemed more severe than in other territories, with more hepatic and renal damage in particular, but also hemodynamic damage, more often requiring the use of catecholamines, dialysis and mechanical ventilation. On the other hand, it is interesting to note that severe respiratory impairment was more frequently found in patients from the French American territories for which we had information, i.e. Martinique and Guadeloupe [15,18]. This supports the hypothesis of a more pronounced respiratory tropism for New World strains than for Old World strains [33].
The main limitations of this study are its retrospective nature, with missing or uncertain data, and the limited number of strains identified in relation to the total number of cases. Comparison between the different studies was also greatly complicated by differences in definitions of organ damage from one work to another.
Conclusion
We publish here the first series of severe patients admitted in the ICU in Mayotte, a French island with a high incidence rate of leptospirosis but with original strain specificities, with the predominance of strain such as L. borgpetersenii sg Mini and L.interrogans sg Pyrogenes. Despite very severe clinical pictures, more severe in appearance than in other territories, with the exception of respiratory involvement, which is more frequent in French Latin American series, mortality remains rather low. This is possibly due to the youth of the population, the absence of the Icterohaemorrhagiae strain, and antibiotic therapy generally started early in the emergency department.
References
- Picardeau M. Leptospirosis: Updating the Global Picture of an Emerging Neglected Disease. PLoS Negl Trop Dis. 2015;9(9):e0004039.
- Daher EF, Soares DS, de Menezes Fernandes AT, Girao MM, Sidrim PR, Pereira ED, et al. Risk factors for intensive care unit admission in patients with severe leptospirosis: a comparative study according to patients’ severity. BMC Infect Dis. 2016;16:40.
- Lindow JC, Wunder EA, Jr., Popper SJ, Min JN, Mannam P, Srivastava A, et al. Cathelicidin Insufficiency in Patients with Fatal Leptospirosis. PLoS Pathog. 2016;12(11):e1005943.
- Bourhy P, Collet L, Brisse S, Picardeau M. Leptospira mayottensis sp. nov., a pathogenic species of the genus Leptospira isolated from humans. Int J Syst Evol Microbiol. 2014;64(Pt 12):4061-7.
- Centre National de Référence de la Leptospirose, Santé publique France. Rapport annuel d’activité - Année d’exercice 2020-2021. 2022.
- Pagès F, Collet L, Henry S, Margueron T, Achirafi A, Bourhy P, et al. Leptospirose à Mayotte : apports de la surveillance épidémiologique, 2008-2015. Bull Epidemiol Hebdo. 2017;8-9:147-56.
- Subiros M, Brottet E, Solet JL, LeGuen A, Filleul L. Health monitoring during water scarcity in Mayotte, France, 2017. BMC Public Health. 2019;19(1):288.
- Bourhy P, Collet L, Brisse S, Picardeau M. Leptospira mayottensis sp. nov., a pathogenic species of the genus Leptospira isolated from humans. Int J Syst Evol Microbiol. 2014;64(Pt 12):4061-7.
- Desvars A, Michault A, Bourhy P. Leptospirosis in the western Indian Ocean islands: what is known so far? Veterinary research. 2013;44(1):80.
- Desvars A, Naze F, Vourc’h G, Cardinale E, Picardeau M, Michault A, et al. Similarities in Leptospira serogroup and species distribution in animals and humans in the Indian ocean island of Mayotte. Am J Trop Med Hyg. 2012;87(1):134-40.
- Bourhy P, Collet L, Lernout T, Zinini F, Hartskeerl RA, van der Linden H, et al. Human leptospira isolates circulating in Mayotte (Indian Ocean) have unique serological and molecular features. J Clin Microbiol. 2012;50(2):307-11.
- Delmas B, Jabot J, Chanareille P, Ferdynus C, Allyn J, Allou N, et al. Leptospirosis in ICU: A Retrospective Study of 134 Consecutive Admissions. Crit Care Med. 2017.
- Miailhe AF, Mercier E, Maamar A, Lacherade JC, Le Thuaut A, Gaultier A, et al. Severe leptospirosis in non-tropical areas: a nationwide, multicentre, retrospective study in French ICUs. Intensive Care Med. 2019;45(12):1763-73.
- Tubiana S, Mikulski M, Becam J, Lacassin F, Lefèvre P, Gourinat A-C, et al. Risk factors and predictors of severe leptospirosis in New Caledonia. PLoS Negl Trop Dis. 2013;7(1).
- Hochedez P, Theodose R, Olive C, Bourhy P, Hurtrel G, Vignier N, et al. Factors Associated with Severe Leptospirosis, Martinique, 2010-2013. Emerg Infect Dis. 2015;21(12):2221-4.
- Herrmann-Storck C, Saint-Louis M, Foucand T, Lamaury I, Deloumeaux J, Baranton G, et al. Severe leptospirosis in hospitalized patients, Guadeloupe. Emerg Infect Dis. 2010;16(2):331-4.
- Doudier B, Garcia S, Quennee V, Jarno P, Brouqui P. Prognostic factors associated with severe leptospirosis. Clin Microbiol Infect. 2006;12(4):299-300.
- Epelboin L, Le Turnier P, Mosnier E, Schaub R, Fontaine E, Houcke S, et al. Severe leptospirosis in Morocco: comparative data from the Amazonian area. Intensive Care Med. 2017.
- Rajaonarivelo JA, Desmoulin A, Maillard O, Collet L, Baudino F, Jaffar-Bandjee MC, et al. Clinical manifestations of human leptospirosis: bacteria matter. Frontiers in cellular and infection microbiology. 2023;13:1259599.
- Ellinghausen HC, Jr., McCullough WG. Nutrition of Leptospira pomona and growth of 13 other serotypes: fractionation of oleic albumin complex and a medium of bovine albumin and polysorbate 80. Am J Vet Res. 1965;26:45-51.
- Johnson RC, Harris VG. Differentiation of pathogenic and saprophytic letospires. I. Growth at low temperatures. J Bacteriol. 1967;94(1):27-31.
- Guglielmini J, Bourhy P, Schiettekatte O, Zinini F, Brisse S, Picardeau M. Genus-wide Leptospira core genome multilocus sequence typing for strain taxonomy and global surveillance. PLoS Negl Trop Dis. 2019;13(4):e0007374.
- Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, et al. Acute respiratory distress syndrome: the Berlin Definition. Jama. 2012;307(23):2526-33.
- Bourhy P, Collet L, Clement S, Huerre M, Ave P, Giry C, et al. Isolation and characterization of new Leptospira genotypes from patients in Mayotte (Indian Ocean). PLoS Negl Trop Dis. 2010;4(6):e724.
- Costa F, Hagan JE, Calcagno J, Kane M, Torgerson P, Martinez-Silveira MS, et al. Global Morbidity and Mortality of Leptospirosis: A Systematic Review. PLoS Negl Trop Dis. 2015;9(9):e0003898.
- Klement-Frutos E, Tarantola A, Gourinat AC, Floury L, Goarant C. Age-specific epidemiology of human leptospirosis in New Caledonia, 2006-2016. 2020;15(11):e0242886.
- Institut National des Statistiques et des Etudes Economiques (INSEE). Evolution et structure de la population. Tableau de bord de l’économie française2023.
- Daveluy A, Haramburu F. Consommation de substances psychoactives à la Réunion et à Mayotte, départements français de l’Océan Indien. Thérapie. 2018;73(5):419-27.
- Le Turnier P, Mosnier E, Schaub R, Bourhy P, Jolivet A, Cropet C, et al. Epidemiology of Human Leptospirosis in French Guiana (2007-2014): A Retrospective Study. Am J Trop Med Hyg. 2018.
- Epelboin L, Bourhy P, Le Turnier P, Schaub R, Mosnier E, Berlioz-Arthaud A, et al. La leptospirose en Guyane francaise et sur le bouclier des Guyanes. Etat des connaissances en 2016. Bull Soc Pathol Exot. 2017;110(3):165-79.
- Picardeau M. Diagnosis and epidemiology of leptospirosis. Med Mal Infect. 2013;43(1):1-9.
- Sokolova M, Marshall JC, Benschop J. Risk Factors for Hospitalisation amongst Leptospirosis Patients in New Zealand. Trop Med Infect Dis. 2021;6(4).
- Guégan JF, Epelboin L, Douine M, Le Turnier P, Duron O, Musset L, et al. Emerging infectious diseases and new pandemics: dancing with a ghost! Lessons in inter- and transdisciplinary research in French Guiana, South America. Int J Infect Dis. 2023;133:9-13.
Figure 1.
Map of the French tropical overseas territories. World map showing the various French tropical overseas territories. In light green, the French tropical territories of America (French Guiana, Guadeloupe and Martinique), in dark green those of the Indian Ocean (Mayotte and Réunion), in light blue the territories of the Pacific Ocean (French Polynesia and New Caledonia) and in purple, mainland France.
Figure 1.
Map of the French tropical overseas territories. World map showing the various French tropical overseas territories. In light green, the French tropical territories of America (French Guiana, Guadeloupe and Martinique), in dark green those of the Indian Ocean (Mayotte and Réunion), in light blue the territories of the Pacific Ocean (French Polynesia and New Caledonia) and in purple, mainland France.
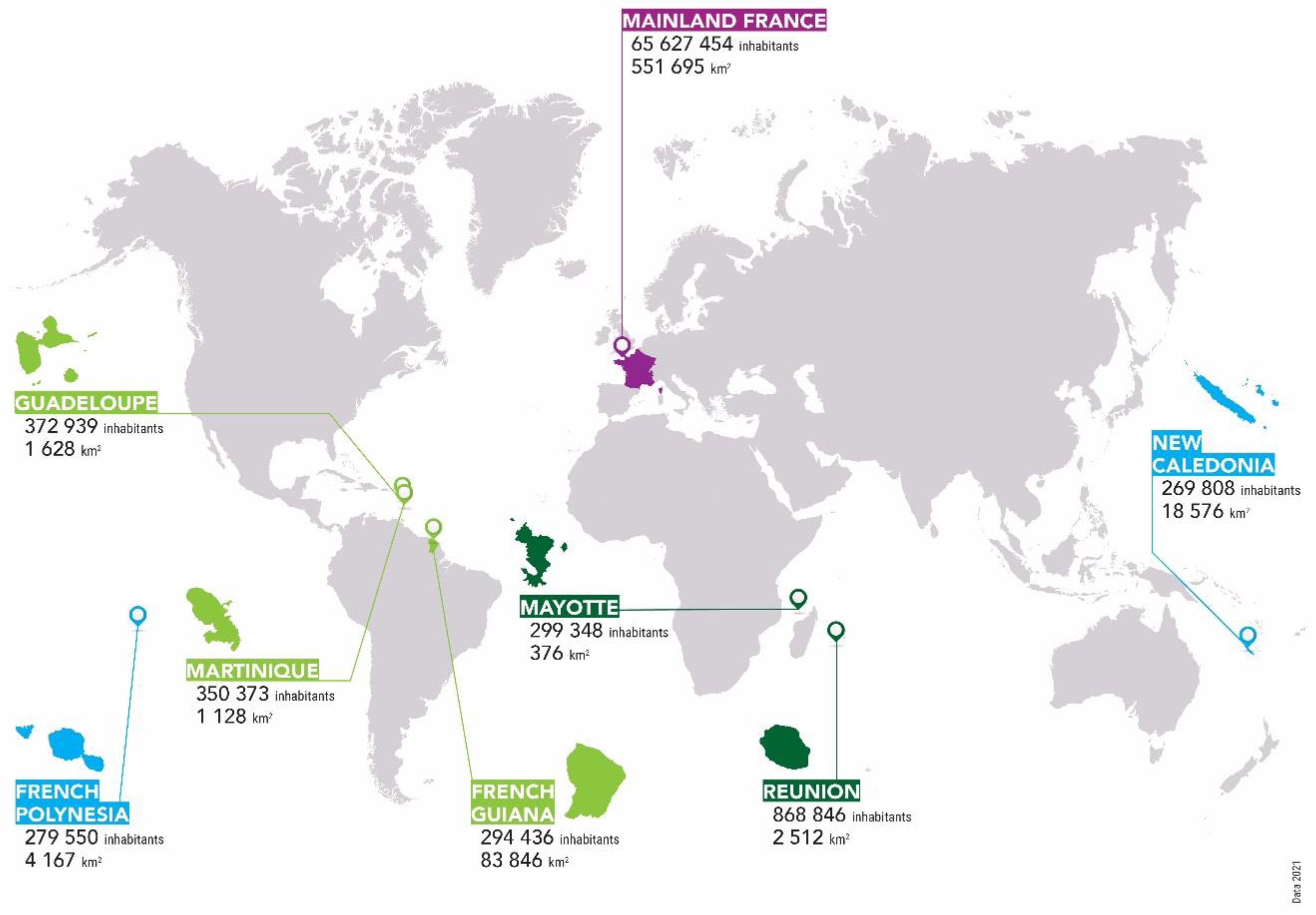
Figure 2.
Histogram showing the number of patients admitted for leptospirosis in the hospital and the ICU.
Figure 2.
Histogram showing the number of patients admitted for leptospirosis in the hospital and the ICU.
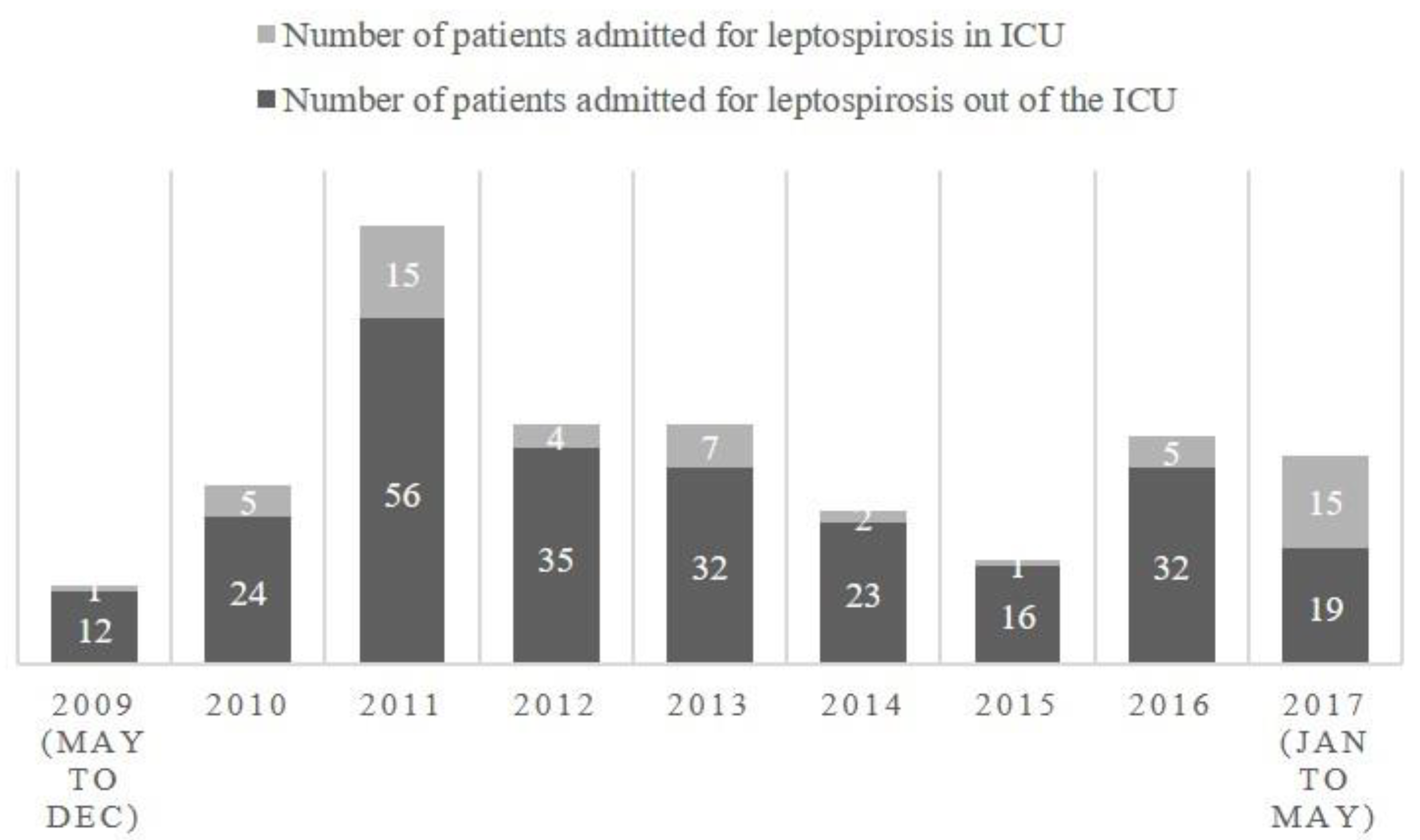

Table 1.
Number of patients admitted with a diagnosis of leptospirosis in the Centre Hospitalier de Mayotte from May 2009 to May 2017.
Table 1.
Number of patients admitted with a diagnosis of leptospirosis in the Centre Hospitalier de Mayotte from May 2009 to May 2017.
| Year | Number of patients admitted for leptospirosis at the CHM including ICU | Number of patients admitted for leptospirosis in ICU | Percentage of patients admitted in ICU |
| 2009 (may to dec) | 13 | 1 | 8% |
| 2010 | 29 | 5 | 17% |
| 2011 | 71 | 15 | 21% |
| 2012 | 39 | 4 | 10% |
| 2013 | 39 | 7 | 18% |
| 2014 | 25 | 2 | 8% |
| 2015 | 17 | 1 | 6% |
| 2016 | 37 | 5 | 14% |
| 2017 (jan to may) | 34 | 15 | 44% |
| Total | 304 | 55 | 18% |
CHM : Centre Hospitalier de Mayotte ; ICU : intensive care unit ;.
Table 2.
Baseline characteristics of patients admitted for leptospirosis in the ICU of Centre Hospitalier de Mayotte from May 2009 to May 2017 compared to previous literature in other French tropical settings and mainland France.
Table 2.
Baseline characteristics of patients admitted for leptospirosis in the ICU of Centre Hospitalier de Mayotte from May 2009 to May 2017 compared to previous literature in other French tropical settings and mainland France.
| Setting | Mayotte | La Réunion | p Mayotte vs. Réunion | French Guiana | p Mayotte vs. French Guiana | Guadeloupe | p Mayotte vs. Guadeloupe | Martinique | p Mayotte vs. Martinique | New Caledonia | p Mayotte vs. New-Caledonia | French Polynesia | p Mayotte vs. French Polynesia | Mainland France | p Mayotte vs. Mainland France |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Reference | Tantet et al. | Delmas et al., Crity Care Med, 2018 | Epelboin et al. Int Care Med, 2016 | Herrmann-Storck et al. Emerg Inf Dis, 2010 | Hochedez et al. Emerg Inf Dis, 2015 | Tubiana et al., PLoS NTD, 2013 | Doudier et al. Clin Microb Inf 2006 | Miailhe et al., Int Care Med, 2019 | |||||||
| Characteristics of patients | ICU patients | ICU patients | p | dialysis, vasopressor agents, mechanical ventilation and/or death during hospitalization | severe cases = dialysis in case of oliguria, mechanical ventilation or death | Severe leptospirosis = vasoactive drugs or dialysis, or blood transfusion or mechanical ventilation or death | severe leptospirosis : dialysis, or vasoactive drugs, alveolar hemorrhage, blood transfusion, mechanical ventilation or death | Severe leptospirosis (no details) | leptospirosis requiring ICU admission (79 ICU in France) | ||||||
| Microbiological diagnosis | PCR | MAT, ELISA or PCR | PCR, MAT, Elisa IgM | EIA IgM, blood culture, MAT | qPCR | RT-PCR + MAT | MAT or ELISA, PCR, or dark field microscopy. | ||||||||
| Study period | 05/2009-05/2017 | 01/2004-01/2015 | 01/2007-09/2014 | 01/2003-12/2004 | 12/2010-02/2013 | 01/2008-06/2011 | 2 years | 01/2012 - 09/2016 | |||||||
| Number of patients | 55 | 134 | 12 | 24 | 12 (among 23 admitted in ICU) | 71 | 71 | 160 | |||||||
| n/N (%) or median, IQR 25%–75% and/or mean ± standard deviation) | n/N (%) or median, IQR 25%–75% and/or mean ± standard deviation) | n/N (%) or median, IQR 25%–75% and/or mean ± standard deviation) | n/N (%) or median, IQR 25%–75% and/or mean ± standard deviation) | n/N (%) or median, IQR 25%–75% and/or mean ± standard deviation) | n/N (%) or median, IQR 25%–75% and/or mean ± standard deviation) | n/N (%) or median, IQR 25%–75% and/or mean ± standard deviation) | n/N (%) or median, IQR 25%–75% and/or mean ± standard deviation) | ||||||||
| Demographic caracteristics | |||||||||||||||
| Male gender | 45/55 (82) | 125 (93) | 0.32 | 11/12 (92) | 0.41 | 18 (75) | 0.55 | NA | NA | 45/71 (63.4) | 0.029 | NA | NA | 146 (91) | 0.43 |
| Male to female sex ratio | 4.5 | 13.8 | 11,0 | 3.0 | NA | 1.7 | NA | 10.4 | |||||||
| Age (years, median, IQR 25%–75%,mean ± standard deviation) | 44 (33-55) / 43,7 ± 14.9 | 40 (30-52) | - | 46.8 ± 17.2 | 0.26 | 52.7 ± 6.5 | 0.003 | 49 (37–57) | - | 42.6 ± 17.8 | 0.64 | NA | NA | 54 (38–65) | - |
| Age>60 years | 6/55 (11) | NA | NA | 3/12 (25) | 0.35 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Age category<3030-59≥60 | 13 (24) 35 (64) 7 (13) |
- | NA | 2 (17) 7 (58) 3 (25) |
- | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Medical history | |||||||||||||||
| Liver disease | 1/54 (2) | 1 (1) | 0.49 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 4 (3) | 1 |
| Cancer or immune deficiency | 0/55 (0) | 0 (0) | 1 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 2 (1) | 1 |
| Diabetes mellitus | 7/55 (13) | 14 (10) | 0.62 | NA | NA | 3/22 (134) | 1 | NA | NA | 8/70 (11.4) | 1 | NA | NA | 9 (6) | 0.13 |
| Chronic hypertension | 6/55 (11) | 10 (7) | 0.57 | NA | NA | 9/22 (41) | 0.18 | NA | NA | 8/70 (11.4) | 1 | NA | NA | NA | NA |
| Respiratory insufficiency | 0/55 (0) | 0 (0) | 1 | NA | NA | NA | NA | NA | NA | 2/70 (2.9) | 0.5 | NA | NA | 0 (0) | 1 |
| Chronic kidney disease | 0/55 (0) | 0 (0) | 1 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 0 (0) | 1 |
| Cardiovascular disease | 0/55 (0) | 4 (3) | 0.32 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 0 (0) | 1 |
| Chronic alcoholism | 3/55 (5) | 34 (25) | 0.17 | NA | NA | 11/22 (50) | <0.001 | NA | NA | 18/70 (25.0) | 0.003 | NA | NA | 29 (18.2) | 0.027 |
| Current cigarette smoking | 2/55 (4) | 45 (34) | <0.001 | NA | NA | NA | NA | NA | NA | 37/70 (52.9) | 0.035 | NA | NA | 49 (31.2) | <0.001 |
| Underlying comorbidities | 14/55 (25) | 47 (35) | 0.23 | 3/11 (27) | 1 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Risk factors | |||||||||||||||
| Exposure to occupational risk‡ | 24/38 (64) | NA | NA | 8/9 (89) | 0.24 | 12/20 (60) | 1 | NA | NA | NA | NA | NA | NA | NA | NA |
| Activity at risk for contamination | 25/54 (46) | NA | NA | 6/12 (50) | 1 | NA | NA | NA | NA | NA | NA | NA | NA | 98 (65) | 0.058 |
| Contact with water at risk for contamination | 4/54 (7) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 101 (68) | 0.047 |
| Contact with rodents | 29/54 (54) | NA | NA | 1/2 (50) | 1 | 3/9 (33) | 0.30 | NA | NA | NA | NA | NA | NA | 44 (31) | <0.001 |
| Contact with animals | 28/54 (52) | NA | NA | 1/2 (50) | 1 | NA | NA | NA | NA | NA | NA | NA | NA | 79 (56) | 0.88 |
| Durations | |||||||||||||||
| Time between first symptoms and biological diagnosis (days) | 3 (2-5) | NA | NA | 4 (4–5.75) | - | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Time between first symptoms and biological diagnosis >5 days | 27/53 (51) | NA | NA | 3/10 (30) | 0.31 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Time between beginning of symptoms and hospital admission (days) | 3 (2-5) | 5 (4–6) | - | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Time between first symptoms and hospital admission > 3 days | 25/53 (47) | NA | NA | NA | NA | NA | NA | NA | NA | 37/70 (52.9) | 0.59 | NA | NA | NA | NA |
| Time between first symptoms and initiation of antibiotic treatment (days) | 3 (2-5) | 5 (4–6) | - | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 5 (4–6) | - |
| Time between first symptoms and antibiotic treatment > 2 days | 35/53 (66) | NA | NA | NA | NA | NA | NA | NA | NA | 51/69 (73.9) | 0.42 | NA | NA | NA | NA |
| Time between first symptoms and antibiotic treatment >10 days | 2/53 (4) | NA | NA | NA | NA | 7/22 (31.8) | 0.089 | NA | NA | NA | NA | NA | NA | NA | NA |
| Time between first symptoms and occurrence of severity criteria (days) | 3 (2-5) | NA | NA | NA | NA | 3 (3-4) | - | 3 (3-4) | - | NA | NA | NA | NA | NA | NA |
| Time between first symptoms and and ICU admission (days) | 3.5 (2-5) | 5 (4-6) | - | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 5 (4–6) | - |
| Antibiotic treatment duration (days) | 7 (7-8) | 7 (7–9.5) | - | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 10 (8–12) | - |
| Length of hospital stay (days) | 9 (6-13) | 12 (8–16) | - | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 11 (8–20) | - |
| Length of ICU stay (days) | 5 (3-9) | 6 (4-9) | - | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 5 (2–10) | - |
| Time between admission and death (days) | 1 (1-5) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 3 (2–20). | - |
NA : not available.
Table 3.
Clinical and outcome variables of patients admitted for leptospirosis in the ICU of Centre Hospitalier de Mayotte from May 2009 to May 2017 compared to previous literature in other French tropical settings and mainland France.
Table 3.
Clinical and outcome variables of patients admitted for leptospirosis in the ICU of Centre Hospitalier de Mayotte from May 2009 to May 2017 compared to previous literature in other French tropical settings and mainland France.
| Setting | Mayotte | La Réunion | p Mayotte vs. Réunion | French Guiana | p Mayotte vs. French Guiana | Guadeloupe | p Mayotte vs. Guadeloupe | Martinique | p Mayotte vs. Martinique | New Caledonia | p Mayotte vs. New-Caledonia | French Polynesia | p Mayotte vs. French Polynesia | Mainland France | p Mayotte vs. Mainland France |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Reference | Tantet et al. | Delmas et al., Crity Care Med, 2018 | Epelboin et al. Int Care Med, 2016 | Herrmann-Storck et al. Emerg Inf Dis, 2010 | Hochedez et al. Emerg Inf Dis, 2015 | Tubiana et al., PLoS NTD, 2013 | Doudier et al. Clin Microb Inf 2006 | Miailhe et al., Int Care Med, 2019 | |||||||
| Number of patients | 55 | 134 | 12 | 24 | 12 (among 23 admitted in ICU) | 71 | 71 | 160 | |||||||
| n/N (%) or median, IQR 25%–75% and/or mean ± standard deviation) | n/N (%) or median, IQR 25%–75% and/or mean ± standard deviation) | n/N (%) or median, IQR 25%–75% and/or mean ± standard deviation) | n/N (%) or median, IQR 25%–75% and/or mean ± standard deviation) | n/N (%) or median, IQR 25%–75% and/or mean ± standard deviation) | n/N (%) or median, IQR 25%–75% and/or mean ± standard deviation) | n/N (%) or median, IQR 25%–75% and/or mean ± standard deviation) | n/N () or median, IQR 25–75 and/or mean ± standard deviation) | ||||||||
| Signs and symptoms, n (%) | |||||||||||||||
| Fever reported by patient | 36/55 (65) | 116 (86) | 0.002 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 135 (84) | 0.74 |
| Temperature >37,7 °C | 38/55 (69) | NA | NA | 7/12 (58) | 0 | 10/23 (44) | 0.043 | NA | NA | NA | NA | NA | NA | NA | NA |
| Temperature >38 °C | 36/55 (65) | NA | NA | 6/12 (50) | 0.51 | NA | NA | 9/12 (75) | 0.73 | 31/67 (46) | 0.044 | NA | NA | NA | NA |
| Temperature ≥ 38.5 °C | 28/55 (51) | NA | NA | 6/12 (50) | 1 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Hypothermia (<36.5°C) | 5/55 (9) | NA | NA | 2/12 (17) | 0.60 | 7/23 (30) | 0.033 | NA | NA | NA | NA | NA | NA | NA | NA |
| Hypotension, SBP <100 mm Hg | 30/55 (55) | NA | NA | 4/12 (33) | 0.22 | 7/20 (35) | 0.45 | NA | NA | NA | NA | NA | NA | NA | NA |
| Hypotension, SBP <90 mm Hg | 20/55 (36) | NA | NA | 3/12 (25) | 0.52 | NA | NA | 5 (42) | 1 | NA | NA | NA | NA | NA | NA |
| Myalgia | 36 (65) | 108 (80) | 0.038 | NA | NA | 12/13 (92) | 0.16 | NA | NA | 68/71 (96) | 0.085 | NA | NA | 95 (59) | 0.52 |
| Arthralgia | 17 (31) | 42 (31) | 1 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 35 (22) | 0.20 |
| Jaundice | 32 (58) | 108 (80) | 0.0019 | 3/12 (25) | 0.055 | 9/12 (75) | 0.089 | 9 (75) | 0.34 | 61/71 (86) | 0.11 | NA | NA | 74 (46) | 0.16 |
| Oligoanuria | 36 (65) | 69 (51) | 0.11 | 5/8 (63) | 1 | 10/23 (44) | 0.083 | ‡<500 mL urine/day 5 (41.7) | 0.19 | 66/71 (93) | <0.001 | NA | NA | NA | NA |
| Hepatosplenomegaly | 4/55 (7) | 25 (18) | 0.077 | NA | NA | 7/11 (64) | <0.001 | NA | NA | NA | NA | NA | NA | NA | NA |
| Abdominal pain | 34/55 (62) | 49 (36) | 0.002 | 10/12 (83) | 0.20 | 14/18 (78) | 0.26 | 5 (42) | 0.22 | NA | NA | NA | NA | 41 (26) | <0.001 |
| Digestive disorders (diarrhea, vomiting) | 16/55 (29) | NA | NA | NA | NA | 12/15 (80) | 0.74 | NA | NA | NA | NA | NA | NA | NA | NA |
| Nausea/vomiting | 14/55 (25) | 65 (48) | 0.0036 | 5/12 (42) | 0.30 | NA | NA | 5 (42) | 0.30 | NA | NA | NA | NA | 50 (31) | 0.50 |
| Diarrhea | 10/55 (18) | NA | NA | 8/12 (67) | 0.0017 | NA | NA | 3 (25) | 0.69 | NA | NA | NA | NA | NA | NA |
| Gastrointestinal bleeding | 1 (2) | 8 (6) | 0.45 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Hemoptysis | 1 (2) | 42 (31) | <0.001 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 11 (7) | 0.30 |
| Dyspnea | 17 (31) | 37 (27) | 0.72 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 42 (26) | 0.60 |
| Cough | 4 (7) | 47 (35) | <0.001 | NA | NA | NA | NA | 3 (25) | 0.10 | NA | NA | NA | NA | 35 (22) | 0.015 |
| Chest pain | 8/55 (15) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 6 (4) | 0.0095 |
| Abnormalities at chest auscultation | 16/54 (30) | NA | NA | NA | NA | 8/17 (47) | 0.24 | 4 (33) | 0.74 | NA | NA | NA | NA | 43 (27) | 0.73 |
| Chest radiologic abnormalities | 24/52 (46) | NA | NA | NA | NA | 6/16 (38) | 0.58 | NA | NA | NA | NA | NA | NA | NA | NA |
| Alveolar infiltrate | 10/52 (19) | NA | NA | NA | NA | 5/16 (31) | 0.32 | NA | NA | NA | NA | NA | NA | NA | NA |
| Headache | 9/47 (19) | NA | NA | 5/12 (42) | 0.13 | 5/7 (71) | 0.10 | NA | NA | 61/70 (87) | 0.037 | NA | NA | 47 (29) | 0.19 |
| Confusion | 11/47 (23) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 11 (7) | 0.0027 |
| Meningeal syndrome | 0 (0) | 4 (3) | 0.32 | NA | NA | 2/12 (17) | 0.030 | NA | NA | NA | NA | NA | NA | NA | NA |
| Specific organ involvment | |||||||||||||||
| Pulmonary involvement | 23/53 (43) | NA | NA | 6/12 (50) | 0.75 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Intra-alveolar hemorrhage | 4/55 (7) | 53 (40) | <0.001 | NA | NA | NA | NA | NA | NA | 39/70 (56) | <0.001 | NA | NA | 23 (14) | 0.24 |
| ARDS | 9/55 (16) | 28 (21) | 0.55 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 58 (36) | 0.0067 |
| Macrophage activation syndrome | 0/55 (0) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 5 (3) | 0.33 |
| Meningitis | 1/55 (2) | 2 (1) | 1 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 4 (2) | 1 |
| Encephalitis | 1/55 (2) | 4 (3) | 1 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Myocarditis | 8/55 (15) | 30 (22) | 0.32 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 4 (2) | 0.0025 |
| Pericarditis | 1/55 (2) | 3 (2) | 1 | NA | NA | 2/24 (8) | 0.22 | NA | NA | NA | NA | NA | NA | NA | NA |
| Cardiac arrest | 4/55 (7) | 3 (2) | 20 | NA | NA | 2/24 (8) | 1 | NA | NA | NA | NA | NA | NA | NA | NA |
| Cardiogenic shock | 10/55 (18) | 11 (8) | 0.072 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Sepsis | 17/55 (31) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 40 (22) | 0.38 |
| Organ failure | |||||||||||||||
| Circulatory failure | 32/55 (58) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 33 (21) | <0.001 |
| Acute kidney failure | 48/55 (87) | 127 (95) | 0.12 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 24 (15) | <0.001 |
| Acute respiratory failure | 6/53 (11) | 76 (57) | <0.001 | 5/12 (42) | 0.024 | NA | NA | NA | NA | NA | NA | NA | NA | 14 (9) | 0.59 |
| Central nervous system failure | 12/55 (22) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 9 (6) | 0.0012 |
| Acute liver failure | 25/55 (45) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 8 (5) | <0.001 |
| Multiorgan failure | 12/55 (22) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 30 (19) | 0.69 |
| Hemorrhagic syndrome | 2 (4) | 72 (54) | 0.033 | 2/12 (17) | 0.14 | 5/24 (21) | 0.024 | 1 (8.3) | 0.45 | NA | NA | NA | NA | 11 (7) | 0.51 |
| Supportive care | |||||||||||||||
| Shock treated with vaso-active drugs | 31/55 (56) | NA | NA | 10/12 (83.3) | 0.11 | NA | NA | 9/12 (75) | 0.33 | 62/70 (89) | <0.001 | NA | NA | 92 (57) | 1 |
| Pulmonary involvement needing mechanical ventilation | 15/55 (27) | 41 (31) | 0.73 | 9/12 (75.0) | <0.001 | NA | NA | 8/12 (67) | 0.017 | 29/71 (41) | 0.13 | NA | NA | 58 (36) | <0.001 |
| Non-invasive ventilation | 10/55 (18) | 13 (10) | 0.14 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 32 (20) | 0.85 |
| ExtraCorporeal Membrane Oxygenation | 0/55 (0) | 5 | 1 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 3 (2) | 0.57 |
| Use of neuromuscular blocking agent (curare) | 10/55 (18) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 33 (20) | 0.85 |
| Prone position | 1/55 (2) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 9 (6) | <0.001 |
| Bleeding requiring blood transfusion | 6/55 (11) | NA | 1/11 (9) | 1 | NA | NA | NA | 8/12 (67) | <0.001 | 23/71 (32) | 0.0053 | NA | NA | NA | NA |
| Acute renal failure with dialysis | 31/55 (56) | 75 (56) | 1 | 7/12 (58) | 1 | NA | NA | 7/12 (58) | 1 | 23/71 (32) | 0.011 | NA | NA | 56 (35) | 0.0067 |
| Outcome | |||||||||||||||
| Diagnosis of leptospirosis suspected at admission | 43/55 (78) | NA | NA | 2/12 (17) | <0.001 | NA | NA | NA | NA | NA | NA | NA | NA | 8 (5) | <0.001 |
| Simplified Acute Physiology Score (SAPS II) | 41 (25.5-50.5) | 38 (27-50) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 40 (28–58) | ||
| Case-fatality rate | 3/55 (5) | 8/134 (6) | 1 | 3/12 (25) | 0.065 | 6/24 (25) | 0.020 | 0/12 (0) | 1 | 10/71 (14) | 0.15 | 5/71 (7) | 1 | 14/160 (9) | 0.57 |
Table 4.
Clinical and outcome variables of patients admitted for leptospirosis in the ICU of Centre Hospitalier de Mayotte from May 2009 to May 2017 compared to previous literature in other French tropical settings and mainland France.
Table 4.
Clinical and outcome variables of patients admitted for leptospirosis in the ICU of Centre Hospitalier de Mayotte from May 2009 to May 2017 compared to previous literature in other French tropical settings and mainland France.
| Setting | Mayotte | La Réunion | p Mayotte vs. Réunion | French Guiana | p Mayotte vs. French Guiana | Guadeloupe | p Mayotte vs. Guadeloupe | Martinique | p Mayotte vs. Martinique | New Caledonia | p Mayotte vs. New-Caledonia | French Polynesia | p Mayotte vs. French Polynesia | Mainland France |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Reference | Tantet et al. | Delmas et al., Crity Care Med, 2018 | Epelboin et al. Int Care Med. 2016 | Herrmann-Storck et al. Emerg Inf Dis. 2010 | Hochedez et al. Emerg Inf Dis, 2015 | Tubiana et al., PLoS NTD, 2013 | Doudier et al. Clin Microb Inf 2006 | Miailhe et al., Int Care Med, 2019 | ||||||
| Number of patients | 55 | 134 | 12 | 24 | 12 (among 23 admitted in ICU) | 71 | 71 | 160 | ||||||
| n/N (%) or median, IQR 25%–75% and/or mean ± standard deviation) | n/N (%) or median, IQR 25%–75% and/or mean ± standard deviation) | n/N (%) or median. IQR 25%–75% and/or mean ± standard deviation) | n/N (%) or median. IQR 25%–75% and/or mean ± standard deviation) | n/N (%) or median, IQR 25%–75% and/or mean ± standard deviation) | n/N (%) or median, IQR 25%–75% and/or mean ± standard deviation) | n/N (%) or median, IQR 25%–75% and/or mean ± standard deviation) | n/N (%) or median, IQR 25%–75% and/or mean ± standard deviation) | |||||||
| L. interrogans serovar Icterohemorrhagiae | 0/21 | 17/18 (94) | <0.001 | 5/9 (56) | <0.001 | 6/8 (75) | <0.001 | 11/12 (92) | <0.001 | 54/66 (82) | <0.001 | NA | NA | NA |
| pH | 7.40 (7.36-7.44) | 7.42 (7.38-7.45) | - | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Leukocyte count ( G/L) | 11.9 (8-17) / 13,2 ± 6,6 | 12 (8-16) | - | 12.1 ± 10.1 | 0.64 | NA | NA | 10.3 (9.1-11.4) | NA | NA | NA | NA | NA | 10.2 (7–14) |
| >15 | 17/55 (31) | NA | NA | 1/12 (8) | 0.16 | NA | NA | NA | NA | 18/71 (25) | 0.55 | NA | NA | NA |
| >10 | 38/55 (69) | NA | NA | 6/12 (50) | 0.31 | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| PMN count (G/L) | 9.7 (6.8-14.0) / 11,0 ± 6,4 | NA | NA | 10.3 ± 9.4 | 0.75 | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| > 7.5 | 33/50 (66) | NA | NA | 7/12 (58) | 0.73 | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| > 12 | 17/50 (34) | NA | NA | 2/12 (16) | 0.31 | 10/23 (44) | 0.45 | NA | NA | NA | NA | NA | NA | NA |
| Platelet count (G/L) | 49 (27-79) / 72,0 ± 109 | 45 (26-84) | - | 146.8 ± 142.4 | 0.046 | NA | NA | 70.5 (32.5-115) | NA | NA | NA | NA | NA | 40 (26–76) |
| < 20 | 9/55 (16) | 17 (13) | 0.49 | 0/12 (0) | 0.20 | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| <50 | 28/55 (51) | NA | NA | 3/12 (25) | 0.12 | 8/23 (35) | 0.15 | NA | NA | 31/71 (44) | 0.47 | NA | NA | 89 (57%) |
| <92 | 43/55 (78) | NA | NA | 6/12 (50) | 0.07 | NA | NA | 7/12 (58.3) | 0.16 | NA | NA | NA | NA | NA |
| < 100 | 47/55 (85) | NA | NA | 7/12 (58) | 0.046 | NA | NA | NA | NA | NA | NA | NA | NA | 138 (89%) |
| < 150 | 50/55 (91) | 124 (93) | 0.77 | 7/12 (58) | 0.012 | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Hemoglobin (g/dL) | 10.7 (8.8-12.2) / 10,5 ± 2,9 | 11.7 (10.3-12.8) | - | 11.9 ± 3.0 | 0.14 | 11.1 ± 2.0 (23) | 0.36 | 12.2 (11.6. 13) | NA | NA | NA | NA | NA | NA |
| ≤ 8 | 11/54 (20) | NA | NA | 1/12 (8) | 0.44 | NA | NA | NA | NA | 7/71 (10) | 0.12 | NA | NA | NA |
| < 10 | 21/54 (39) | NA | NA | 2/12 (16) | 0.19 | 5/23 (22) | 0.19 | NA | NA | NA | NA | NA | NA | NA |
| < 12 | 37/54 (69) | NA | NA | 6/12 (50) | 0.31 | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| < 12,2 | 40/54 (74) | NA | NA | 6/12 (50) | 0.16 | NA | NA | 6/12 (50) | 0.16 | NA | NA | NA | NA | NA |
| Creatinine (µmol/L) | 277 (169-439) / 386,3 ± 416,9 | 308 (184-521) | - | 339.2 ± 256.4 | 0.71 | 246.4 ± 220 (21) | 0.13 | 169.5 (132.5-217.5) | NA | NA | NA | NA | NA | 323 (191–483) |
| > 110 | 48/55 (87) | 127 (95) | 0.12 | 11/12 (92) | 1 | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| > 132 | 45/55 (82) | NA | NA | 10/12 (83) | 1 | 11/21 (52) | 0.18 | NA | NA | NA | NA | NA | NA | NA |
| > 154 | 42/55 (76) | NA | NA | 9/12 (75) | 1 | NA | NA | 7/12 (58) | 0.28 | NA | NA | NA | NA | NA |
| > 200 | 36/55 (65) | NA | NA | 8/12 (67) | 1 | NA | NA | NA | NA | 36/67 (54) | 0.20 | NA | NA | NA |
| Urea (mmol/L) | 18.3 (10.0-28.9) / 23,0 ± 20,2 | 16 (10–24) | 13.9 ± 9.1 | 0.13 | 14.3 ± 12.7 (23) | 0.23 | 10.1 (8-18.5) | NA | NA | NA | NA | NA | NA | |
| > 9.3 | 45/55 (82) | NA | NA | 8/12 (67) | 0.26 | NA | NA | 4/8 (50) | 0.065 | NA | NA | NA | NA | NA |
| > 15 | 32/55 (58) | NA | NA | 4/12 (33) | 0.20 | NA | NA | NA | NA | NA | NA | NA | NA | 97 (61%) |
| ASAT (IU/L) | 124 (70-266) / 419,9 ± 1260 | 148 (89-234) | - | 138.0 ± 145.0 | 0.44 | NA | NA | 73.5 (59-126.5) | NA | NA | NA | NA | NA | 112 (64–181) |
| >102 | 35/55 (64) | NA | NA | 4/11 (36) | 0.11 | 17/23 (74) | 0.44 | NA | NA | NA | NA | NA | NA | NA |
| > 150 | 25/55 (45) | NA | NA | 3/11 (27) | 0.33 | NA | NA | NA | NA | 18/66 (27) | 0.056 | NA | NA | NA |
| ALAT (IU/L) | 69 (37-125) / 151,5 ± 326,2 | 77 (52-107) | - | 116.8 ± 224.4 | 0.73 | NA | NA | NA | NA | NA | NA | NA | NA | 81 (50–128) |
| >119 | 15/55 (27) | NA | NA | 3/12 (25) | 1 | 6/23 (26) | 1 | NA | NA | NA | NA | NA | NA | NA |
| ASAT and/or ALAT > 10 N | 30/55 (55) | NA | NA | 2/12 (17) | 0.025 | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Total bilirubin (µmol/L) | 107 (24-286) / 196,1 ± 215,7 | 152 (46-293) | - | 101.7 ± 163.5 | 0.16 | 258.4 ± 199 (18) | 0.055 | 56.5 (35.5-103) | NA | NA | NA | NA | NA | 80 (33–186) |
| > 20 | 43/55 (78) | 120 (90) | 0.061 | 7/12 (58) | 0.16 | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| > 49 | 34/55 (62) | NA | NA | 6/12 (50) | 0.52 | NA | NA | 7/12 (58) | 1 | NA | NA | NA | NA | NA |
| > 50 | 34/55 (62) | NA | NA | 6/12 (50) | 0.52 | NA | NA | NA | NA | 38/66 (58) | 0.71 | NA | NA | NA |
| > 119 | 27/55 (49) | NA | NA | 3/12 (25) | 0.20 | 13/18 (72) | 0.11 | NA | NA | NA | NA | NA | NA | NA |
| > 150 | 26/55 (47) | NA | NA | 2/12 (16) | 0.06 | NA | NA | NA | NA | NA | NA | NA | NA | 50 (32%) |
| Prothrombin ratio (%) | 69 (53-87) | 82 (72-90) | - | NA | NA | NA | NA | 66.5 (56-74.5) | NA | NA | NA | NA | NA | NA |
| < 68 | 26/54 (48) | NA | NA | NA | NA | NA | NA | 7/12 (58) | 0.75 | NA | NA | NA | NA | NA |
| < 70 | 29/54 (54) | NA | NA | NA | NA | 5/21 (24) | 0.022 | NA | NA | 21/57 (37) | 0.088 | NA | NA | NA |
| CRP (mg/L) | 293 (228-388) / 299 ± 140,3 | 220 (155-313) | - | 263.4 ± 126.4 | 0.42 | NA | NA | 338.5 (197.5-464.5) | NA | NA | NA | NA | NA | 237 (166–301) |
| > 150 | 47/55 (85) | NA | NA | 9/12 (75) | 0.40 | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| > 282 | 32/55 (58) | NA | NA | 7/12 (58) | 1 | NA | NA | 7/12 (58) | 1 | NA | NA | NA | NA | NA |
| Kalemia (mmol/L) | 3.6 (3.3-4.1) | 3.5 (3.1–3.5) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | |
| < 3,5 | 19/54 (35) | 62 (46) | 0.009 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Lactate (mmol/L) | 3.6 (2-6) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | 1.7 (1.1–2.6) |
| > 2.5 | 24/41 (59) | 16 (18) | <0.001 | NA | NA | NA | NA | NA | NA | 30/50 (60) | 1 | NA | NA | NA |
| CPK (IU/L) (median IQR 25-75) | 232 (65-646) | 2085 (1010–4875) | NA | NA | NA | NA | 953 (204-1332) | NA | NA | NA | NA | NA | 94 (55–192) | |
| > 443 | 13/41 (32) | NA | NA | NA | NA | NA | NA | 5/9 (56) | 1 | NA | NA | NA | NA | NA |
| >1000 | 8/41 (20) | NA | NA | NA | NA | 5/18 (28) | 0.50 | NA | NA | NA | NA | NA | NA | NA |
| LDH (IU/L) (median IQR 25-75) | 950 (462-6123) / 2294,6 ± 1744,9 | NA | NA | 576.0 ± 579.6 | 0.0013 | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| > 500 | 24/34 (71) | NA | NA | 3/7 (43) | 0.20 | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| > 800 | 16/34 (47) | NA | NA | 1/7 (14) | 0.21 | 3/17 (18) | 0.065 | NA | NA | NA | NA | NA | NA | NA |
| Lipase (IU/L) | 164 (69-543) | 54 (28–150) | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| >60 | 25/31 (81) | NA | NA | NA | NA | 2/8 (25) | 0.0056 | NA | NA | NA | NA | NA | NA | NA |
| Base excess < –5 mmol/L | 26/54 (48) | 18 (16) | <0.001 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA |
Table 5.
Identification leptospira isolates strains of patients in Mayotte 2009-2017.
| ID reference (BIGSdb) | Species | Serogroup | Number CGs of cgMLST in BIGSdb | Genus human strains in data base BIGdb (n=91) | Genus human strains in this study (n=19) |
| 148 | borgpetersenii | Mini | 78 | 37 (41%) | 13 (68%) |
| 150 | borgpetersenii | Pomona | 80 | 5 (5%) | 0 |
| 729 | borgpetersenii | Unknown | 145 | 1 (1%) | 0 |
| 159 | interrogans | Pyrogenes | 81 | 13 (14%) | 4 (21%) |
| 174 | kirschneri | Grippotyphosa | 85 | 8 (9%) | 0 |
| 112 | kirschneri | Mini | 63 | 5 (5%) | 1 (5%) |
| 113 | kirschneri | Unknown | 64 | 3 (3%) | 0 |
| 175 | kirschneri | Mini | 83 | 1 (1%) | 0 |
| 172 | kirschneri | Mini | 84 | 1 (1%) | 0 |
| 178 | mayottensis | Unknown | 82 | 16 (18%) | 0 |
| 149 | mayottensis | Mini | 79 | 1 (1%) | 1 (5%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



