Submitted:
09 May 2024
Posted:
10 May 2024
You are already at the latest version
Abstract
The prolonged static sitting at the workplace is considered as one of the main risks for development of musculoskeletal disorders (MSDs) and adverse health effects. Factors such as poor posture and extended sitting are perceived to be a reason for conditions such as lumbar hyperlordosis and lower back pain (LBP), even though the scientific explanation of this relationship is still unclear and raises disputes in the scientific community. This publication proposes the low back pain assessment (LBPA) dataset collected through experiment with 100 participants and consisting of photogrammetric images with intentionally placed body markers, calculated postural angles and tags correct and incorrect posture assessed by habilitated rehabilitator, as well as questionnaire-based self-reports regarding the occurrence of LBP and similar symptoms among the participants. Machine learning models trained with this data are employed for recognizing incorrect body postures. Two scenarios have been elaborated for modeling purposes: scenario 1, based on natural body posture tagged as correct and incorrect, and scenario 2, based on incorrect body postures, corrected additionally by the rehabilitator. The achieved accuracies of respectively 75.3% and 85% for both scenarios reveal the potential for future research in enhancing awareness and actively managing posture-related issues that elevate the likelihood of developing lower back pain symptoms.
Keywords:
photogrammetry
; MSDs
; low back pain
; ergonomics
; incorrect sitting posture
; postural angles
; body markers
; self-assessment
; ML models
1. Summary
The seated position is prevalent in the workplace and can exert significant strain on the musculoskeletal system. As an increasing number of occupations involve prolonged static sitting and contribute to a sedentary lifestyle, the prevalence of adverse health effects is on the rise. Ergonomics plays a crucial role in establishing a favorable relationship between individuals and their work, thereby contributing to enhanced worker health [1].
Extended periods of static sitting are associated with the development of musculoskeletal disorders (MSDs), a prevalent issue in Europe [2]. MSDs exert a negative impact on the musculoskeletal system and can lead to severe health problems, particularly when compounded by negative emotions, stress, and heightened cognitive demands. The modern workplace, characterized by widespread use of electronic devices, amplifies the risk of MSDs, especially among students, with up to 65% experiencing such disorders. Contributing factors encompass a lack of rest (85%), passive load (70%), poor body posture (60%), and overwork (30%) [3,4].
A large-scale survey [5] designed to assess the determinants of posture in a large metropolitan area population found that 68.7% of respondents felt that not enough attention is paid to posture in the workplace. Our previous study [6] among 200 prolonged sitting workers showed that 67% of people well-informed about correct working posture suffered from pain in the head, neck, upper or lower back, and waist.
Vertebral segments of the human spine are known to function synergistically to maintain the stability of the human body. Altered vertebral motion has been widely assumed as a biomechanical factor causing spinal pathology [7]. An estimated 7% of all visits to a primary care physician are due exclusively to low-back pain (LBP) [8]. LBP is also the most common musculoskeletal complaint that physiotherapists deal with [9]. Most people (60–70%) experience at least one episode of LBP at some point in their life [10].
Lumbar disc degeneration is among the most common reasons for the development of lower back pain. Causes of physical imbalances, disc degeneration, and lower back pain are complex and multifactorial, caused by processes including aging, abnormal mechanical loads, incorrect sitting, incorrect working posture, and accidental damage. Degenerative disease of the lumbar spine is not only the cause of pain in numerous patients, but it has also become an excessive social burden in various countries [11]. Therefore, understanding the underlying mechanism that causes pain due to the degeneration of lumbar discs is important when analyzing the basic principles of spine biomechanics, and maintaining a correct sitting posture to ensure a healthy spine and pelvis [12].
Inappropriate sitting posture is a prevalent factor in the onset of lower back pain. Extended periods of poor posture, such as slouching or maintaining a bent position, impose biomechanical stress on the lower back, affecting spinal alignment and causing strain on supporting structures. This stress increases the likelihood of conditions like lumbar hyper lordosis, sway-back, round back, flat back, and scoliosis contributing to discomfort and pain [13].
Evaluating spinal posture is crucial in understanding and addressing low back pain, as abnormal postural behavior is identified as a potential risk factor for lumbar injury. Biomechanically, accentuated lumbar lordosis is associated with an increased prevalence of low back pain [14]. Therefore, it is crucial to examine how prolonged sitting affects an individual’s health, specifically whether it leads to musculoskeletal disorders such as lumbar hyper lordosis.
Numerous studies have explored various postures to identify optimal sitting positions. While a consensus on the optimal sitting posture remains elusive, an upright lordotic posture is generally regarded as conducive to spinal health [15].
Ensuring a conducive ergonomic work environment, adopting proper sitting habits, and incorporating regular breaks, along with adequate lumbar support and posture awareness, are crucial in minimizing the risk of musculoskeletal issues and fostering spinal health.
A recommended 90-degree knee angle contributes to lumbar support by minimizing lower back strain and fostering a neutral and comfortable sitting posture. This position offers advantages such as decreased pressure on the knee joints, promoting even weight distribution and averting discomfort associated with extended sitting. Additionally, it facilitates improved blood circulation, reducing the likelihood of leg numbness or tingling.
Numerous studies examining correct sitting postures have employed various methodologies in recent years. The questionnaire approach for assessing good body posture and related musculoskeletal disorders (MSDs) involves the use of structured surveys to gather subjective information from individuals regarding their sitting or standing habits, ergonomic practices, and experiences of discomfort or pain [16,17,18]. These questionnaires typically inquire about the frequency and duration of prolonged sitting or standing, the use of ergonomic furniture, and the presence of any musculoskeletal symptoms. By utilizing this approach, researchers aim to gain insights into participants’ perceptions of their posture and the potential association with MSDs, providing valuable qualitative data for further analysis and understanding.
Recently, there has been a growing trend in utilizing sensor-based recognition systems that collect data through accelerometers, pressure sensors, or ultrasonic sensors. For instance, Tsai et al. [19] proposed an automated pressure sensor-based sitting posture recognition system designed to facilitate users in reviewing historical data and addressing potential health risks associated with poor posture. However, the implementation of pressure sensors mounted on a chair complicates the experimental setup.
Alternatively, some researchers have explored using postural angles as measurable variables to evaluate posture correctness [20,21]. These angles are assessed through methods such as goniometry, photography, photogrammetry, and radiography, with photogrammetry standing out as a widely adopted noninvasive approach that eliminates the risk of radiation exposure associated with radiography.
A comprehensive review of machine learning (ML) algorithms focused on Musculoskeletal Disorders (MSD) prevention was presented in [22], outlining some of the most frequently used techniques: Artificial Neural Networks (ANN), Decision Tree, Random Forest and Support Vector Machines (SVM). Notably, about one fourth of the research papers, had been published in 2020.
A recent study proposed a sitting posture monitoring system using electromyographic (EMG) sensors and ML algorithms [23]. Support vector machine (SVM), K-nearest neighbors (KNN), decision tree (DT), random forest (RF), and multi-layer perceptron (MLP), were used for detection of improper posture. A binary classification was performed (distinguishing between proper and improper posture) and multi-class classification (including some frequent deviations from the correct posture). The results outlined KNN as best performing algorithm with accuracy reaching 91%. In [24] the authors utilized a hybrid sensor system and K-nearest neighbors (KNN) model for recognition of correct posture with accuracy of up to 92%. Another research paper [19] presented successfully captured and recognized ten common sitting postures. The ML methods employed included SVM, KNN, DT, RF, and logistic regression (LR).
In this study, we investigated the relationship between improper sitting posture (in the context of prolonged working in front of computer) and respectively the occurrence of low back pain. The main goal was creation of resources allowing further investigation and creation of models for recognition of incorrect posture. The primary target were young people occupied with sedentary jobs with the specific aim of early-stage risk assessment of the probability of MSDs development. The experiment was implemented in the framework of a project entitled “Ergonomic research on work-related health problems by innovative computer models with a focus on the prevention of Musculoskeletal Disorders”.
2. Data Description
The data was collected from one hundred participants. The LBPA (Low Back Pain Assessment) dataset consists of left-side view pictures with markers (natural sitting posture and corrected sitting posture), a file with postural angle calculations and tags, a file based on the questionnaire, representing the self-assessment of the respondents. The description of the data is as follows:
- Pictures with markers – Pictures in .jpg with markers ready to use (ten markers corresponding to body map). File name format is “ID.X”, where ID corresponds to Participant ID numbers and “X” denotes the natural sitting posture (5) and the corrected posture (6). Photo IDs correspond to Questionnaire IDs;
- Postural angle calculations – Angle.csv file containing in each column postural angle calculations (angle 2, angle 6, angle 7)
- a file with questionnaire responses
Additional information about our research and the presented dataset can be found on Data Availability Statement.
3. Methods
3.1. Experimental Design
The experimental procedure comprised several sequential steps. Initially, volunteers filled out a self-perception questionnaire regarding their work habits, ergonomic practices, and instances of discomfort or pain. Subsequently, left lateral view photographs of the body were captured while volunteers seated in their natural position in front of a computer, occupied with a game-like standard cognitive task. Thirdly, statistical analysis and postural angle calculations were executed. Finally, the angle values along with tags for incorrect posture, provided by habilitated specialist in the area of MSDs were collected in dataset and used for machine learning purposes, aiming to construct a model for recognizing improper sitting postures related to occurrence of low back pain risk.
3.2. Participants
The study encompassed a total of 100 volunteers, with a gender distribution of 64% males (n=64) and 36% females (n=36). The mean age of the participants was 28.38 (±11.19), height 174.31 (±10.20), and weight 75.27 (±17.50). The survey was conducted in Bulgaria during the months of November and December 2021.
It was ensured that the participants had no structural spinal curvature, neurological disease, chronic inflammatory disease, joint-related conditions, or ongoing pregnancies. The participants were informed of the procedure and signed informed consent declaration before their involvement.
3.3. Experimental Procedure
The data collection commenced following the acquisition of informed consent. Participants were summoned at the designated time. In essence, the data collection session was initiated with a procedural explanation, completion of the questionnaire, and capturing photographs of the subject in relaxed postures. The measurement of sagittal spine posture during computer task was conducted through digital photogrammetry.
The self-assessment questionnaire utilized in this study was specifically developed as outlined in [6]. It aimed to assess the levels of discomfort and pain arising from extended periods of computer work characterized by infrequent changes in body posture and suboptimal ergonomic organization of the workplace.
Left lateral view photographs of the body were captured to assess the sagittal alignment of the spine. The angular measurement method employed in this study was adapted from our previous research. The participants were instructed to sit in their usual comfortable position while gazing at a computer monitor. A digital camera (Panasonic Lumix G80) on a tripod, positioned 2.5 m away from the participant, was used for taking photographs. Additionally, a second photograph was taken after the volunteer’s posture had been corrected by habilitated medical specialist with MSDs specialization.
Circular markers were carefully positioned on specific vertebrae (12, L5, and S1), as well as on the hip joint, knee joint, and ankle joint, as shown in Figure 2. Additionally, Figure 2 includes photographs of a participant demonstrating their natural posture before (labeled as ‘a’) and after (labeled as ‘b’) corrections were made.
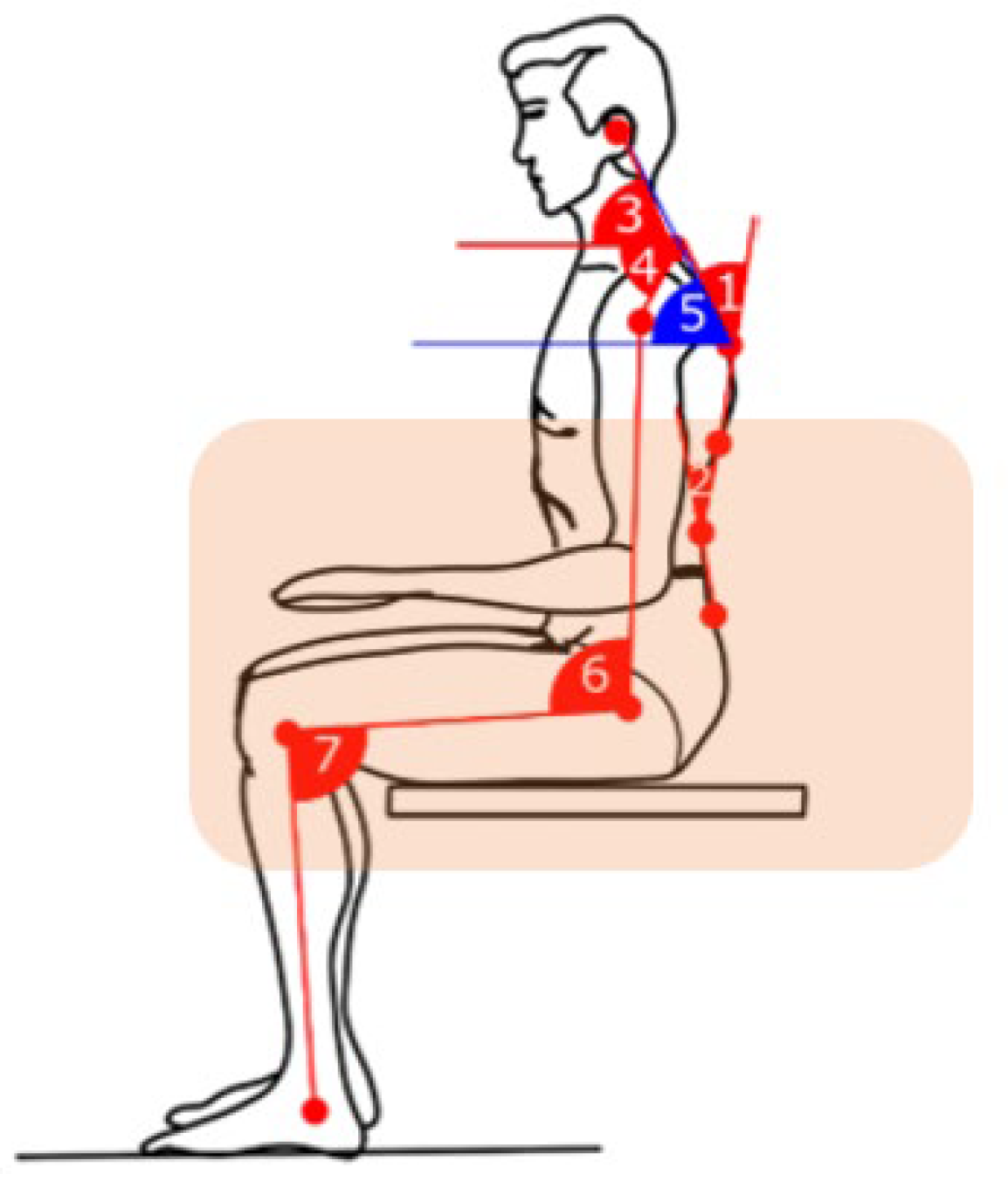
A dedicated software application, developed specifically for this study, was utilized to identify circular markers, and calculate the coordinates of their centers as numerical points in the image (Figure 1). These centers (points) served as the basis for constructing necessary straight lines to measure angles between intersecting lines, including those connecting the points. According to the applied methodology, angles 2, 6 and 7 (Figure 2) were calculated, having a direct relationship with determining the sagittal imbalance and low back pain.
- Angle 2 - Lumbar lordosis (LL), defined as the angle between tangential lines to the lower plateau of L5 and the top of L1.
- Angle 6 - Hip joint angle measurement - sitting position. This is an angle obtained by the intersection of two lines in the region of the greater trochanter of the femur. One line is vertical and parallel to the trunk, and the other line is parallel to the long axis of the femur in line with the lateral femoral condyle.
- Angle 7 – Bent knee angle when sitting. This is an angle obtained by the intersection of two lines in the region of the lateral epicondyle of the femur. One line is horizontal and parallel to the femur to the greater trochanter, and the other line is parallel to the fibula to the lateral malleolus.
Figure 2.
Postural angles with focus on those related to higher risk of low back pain development.
3.4. Data Processing and Statistics
In this experimental study, participants predominantly engaged in prolonged computer work were involved. The research design encompassed general questions addressing ergonomic considerations in the workplace as well as specific ones aimed at understanding the influence of distinct sitting postures on lumbar curvature and associated discomfort. The self-perception survey adhered to the Nordic questionnaire methodology [6].
We elaborated two scenarios for data processing and modelling. The first of them was based on the initial photographs of naturally sitting volunteers (100 cases in total) after their assessment of correct and incorrect postures. The second scenario encompassed only the volunteers sitting improperly with two photographs of each one – before and after posture correction (120 cases in total) in order a balanced dataset to be achieved.
4. Experimental Results
4.1. Questionnaire-Based Analysis
The findings revealed that 37.5% of participants utilized a computer for over 4 hours daily for 6 to 12 years. Additionally, 54% reported experiencing discomfort or pain in the lower back during prolonged computer use, with 20% specifying such occurrences at least once daily. The degree of pain assessed by the participants is presented in Table 1. More than half of the responders (53%) reported a severe degree of pain or discomfort, while 46% reported experiencing a moderate level of discomfort, with 5% indicating a high intensity of pain in the back.
4.2. Photogrametric Analysis
To assess the pelvic position and spinal load during the seated body’s working position, a photogrammetric analysis was conducted on photographs of 100 individuals. This approach involved calculating specific angles, namely the angle 2, angle 6, and angle 7, providing insights into the biomechanics of the seated posture.
The box plot depicted in Figure 3 presents the statistical distribution of data about postural angles 2, 6, and 7 for all participants. Notably, the recommended angle of 90 degrees in the knee joint (7) during seated work is observed in less than 25% of individuals. This indicates that many participants place undue stress on their knee joints, leading to uneven weight distribution. Furthermore, this improper posture hinders blood circulation and elevates the risk of numbness in the extremities. It is imperative to note that incorrect sitting posture is correlated with increased discomfort and pain.
Additionally, we used the data separated in the two scenarios, explained in section 3.4. in order to create detectors of improper posture through machine learning algorithms. We developed distinct detectors for each scenario through experiments involving established classification algorithms, including Decision Tree, Naive Bayes, Logistic Regression, Generalized Linear Model and Deep learning. The classification experiments were carried out using RapidMiner Studio (© 2024 RapidMiner, Inc (Troy, Michigan, USA). All Rights Reserved. Documentation available at https://docs.rapidminer.com/latest/studio/index.html, 5 April 2024) (version 10.2)), employing the 10-fold cross-validation methodology with automated optimization of classifier parameters, ensuring consistency across all experiments. In addition, fine tuning of hyper parameters was conducted to the best performing classifiers.
4.2.1. Natural Postures-Based Scenario
Table 2 displays the experimental results, showcasing the classifiers with the highest accuracy for each of the four feature setups. Across all investigated cases, the Naïve Bayes classifier performed with the highest accuracy of 75.3%.
Since the difference in the accuracy between the first and the second (SVM) ranked clarifiers was too large (above 10%), additional fine tuning with Laplacian correction was performed only to the Naïve Bayes classifier, which did not change its accuracy.
4.2.2. Corrected Postures-Based Scenario
Comparison of the performance of all classifiers with automatic optimization in the corrected postures-based scenario is presented in Table 3.
In this scenario the random forest classifier outperformed the rest of the algorithms with achieved accuracy of 80%. Notably, the second (Deep Learning) and the third (Gradient Boosted Trees) ranked classifiers achieved accuracies very close to the first one, respectively 79.5% and 78.6%. The optimal parameters of the first three classifiers set automatically were as follows: Random Forrest – number of trees: 100; maximal depth: 2; Deep Neural Network - four-layer feed forward architecture 3/50/50/2 as the first three layers consist of neurons with ReLU activation function and the last layer consists of two neurons with SoftMax activation function; Gradient Boosted Trees: number of trees 100; maximal depth: 2; learning rate: 0.001.
These three algorithms were additionally finetuned for improvement of their accuracies. The results and the respective optimal parameters are shown in Table 4.
The results achieved after the finetuning of hyperparameters were considerably improved, both with regard the accuracy and the standard deviation reaching accuracy of 85.00% (resp. standard deviation of ± 12.30%) for the top-rated classifier.
5. Discussion
The causal relationship between improper sitting habits and LBP is still controversial and probably it will take additional time and efforts a consensus on that topic to be established. Two polar positions could be outlined with regard to the understanding about such causality. On the first side are supporters of the strong correlation between the sedentary life-style and the risk of LBP. Several recent studies [25,26,27] confirm this relationship. On the opposite side are studies that either reject the link between the (working) posture and LBP [28] or at least cannot find satisfying scientific evidence about it [29,30,31], underscoring the influence of other personal characteristics, such as age, gender, height, weight etc. The supporters of the first point of view weigh out the influence of different factors, such as the prolonged sitting or the improper posture as more harmful for people’s health. Contrary to this, [28] even argue that there is no such thing as improper posture.
While we do not directly take side into this discussion and considering the arguments of each of the mentioned research studies, we do believe that people exposed to both prolonged sitting and improper posture are in risk of development of MSDs and LBP in particular, without underestimating the rest of the factors.
The aim of the collected LBPA dataset was to contribute to the research devoted to the occurrence of LBP in a way that can prevent young people from developing MSDs on an elder age. This was also the main reason to employ students with computer science profiles for volunteers as they were exposed to prolonged static sedentary work, often accompanied with poor body posture.
The results from the conducted self-report survey proved the relevance of the research, even though the average age of the participants was quite young (28.38 years) and not expected to show occurrence of MSDs. In that context we consider the efforts for data collection and modeling as important with regard to the opportunities for prevention from LBP and similar symptoms.
The models for detection of improper posture developed in two scenarios show the potential for technological support of the ergonomic organization of the working place for professions related to sedentary working posture. Scenario 1 employs ML algorithms trained with natural proper and improper postures as assessed by an expert. In Scenario 2 the models are trained with improper and post intentionally corrected postures. We acknowledge that these postures are momentary pictures which cannot lead to general conclusions with regard to development of LBP. The detection of improper posture, however, implemented in real time applications and combined with dynamic monitoring of the working process could make sense in the context of increased awareness of the seated workers with regard to the spinal tension they bear, as well as the related adverse health consequences that they could face in the future.
6. Conclusion
The evaluation of seated work posture holds paramount importance due to its association with the risk of development of lower back pain, a prevalent issue affecting significant part of the population. Enhancing our understanding and optimizing sitting posture can serve as a preventive measure against musculoskeletal strain, diminishing the likelihood of chronic back problems and fostering overall occupational well-being. Addressing and refining sitting posture not only enhances the comfort but also mitigates the risk of pain, thereby contributing to the long-term health of the spine.
In the current paper we presented the LBPA dataset collected through experiment and consisting of photogrammetric images with markers, calculated posture angles with tags for correct posture and self-reports of respondents based on questionnaire. The presented results revealed the relevance of such studies as well as a considerable potential for future work in the course of improved awareness and dynamic control on the posture related issues increasing the risk of occurrence of future LBP symptoms.
Supplementary Materials
The following supporting information can be downloaded at: https://www.wwwsensornetworkslab.com/projects/ergo-research, The LBPA dataset.
Author Contributions
Conceptualization, V.M. and S.F.; methodology, V.M.; software, M.M.; validation, Z.P., M.M. and V.M.; formal analysis, Z.P. and V.M.; investigation, V.M., M.M, Z.P. and S.F.; resources, V.M., S.F. and M.M.; data curation, V.M. and Z.P.; writing—V.M and M.M.; writing—review and editing, M.M.; visualization, M.M, V.M. and Z.P.; supervision, V.M. and S.F.; project administration, V.M.; funding acquisition, V.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by BULGARIAN NATIONAL SCIENCE FUND (BNSF), grant number KP-06-N37/1 from 6 December 2019, entitled “Ergonomic research on work-related health problems by innovative computer models with a focus on the prevention of Musculoskeletal Disorders”.
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The LBPA dataset supporting reported results can be downloaded from the website link: https://www.wwwsensornetworkslab.com/projects/ergo-research.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Soares C, Shimano SGN, Marcacine PR, Fernandes LFRM, de Castro LLPT, de Walsh IAP. Ergonomic interventions for work in a sitting position: an integrative review. Rev Bras Med Trab. 2023, 18;21(1): e2023770.
- European agency for safety and health at work, Musculoskeletal disorders. Available online: URL https://osha.eu- ropa.eu/en/themes/musculoskeletal disorders (accessed on 01 Mart 2024). (accessed on 01 Mart 2024).
- Jacquier-Bret, J., Gorce, P. Effect of day time on smartphone use posture and related musculoskeletal disorders risk: a survey among university students. BMC Musculoskeletal Disorder 24, 725 (2023). [CrossRef]
- Sharan D. Musculoskeletal disorders in 115 students due to overuse of electronic devices: Risk factors and clinic. In Proceedings of the 20th Congress of the International Ergonomics Association (IEA 2018), Florence, Italy, August 26-30, 2018.
- Montuori P, Cennamo LM, Sorrentino M, Pennino F, Ferrante B, Nardo A, Mazzei G, Grasso S, Salomone M, Trama U, Triassi M, Nardone A. Assessment on Practicing Correct Body Posture and Determinant Analyses in a Large Population of a Metropolitan Area. Behavioral Sciences. 2023, vol.13, issue 2. [CrossRef]
- Vachinska S., Markova V., Ganchev T. A Risk Assessment Study on Musculoskeletal Disorders in Computer Users Based on A Modified Nordic Musculoskeletal Questionnaire. Lecture Notes in Networks and Systems. 2022, Vol. 374. [CrossRef]
- Shin JH, Wang S, Yao Q, Wood KB, Li G. Investigation of coupled bending of the lumbar spine during dynamic axial rotation of the body. Eur Spine J. 2013 Dec;22(12):2671-7. Epub 2013 Apr 28. PMID: 23625336; PMCID: PMC3843802. [CrossRef]
- Bernstein IA, Malik Q, Carville S, Ward S. Low back pain and sciatica: summary of NICE guidance. BMJ. 2017 Jan 6;356: i6748. Erratum in: BMJ. 2021 Jul 14;374: n1627. PMID: 28062522. [CrossRef]
- Tousignant-Laflamme Y, Martel MO, Joshi AB, Cook CE. Rehabilitation management of low back pain - it’s time to pull it all together! J Pain Res. 2017 Oct 3; 10:2373-2385. PMID: 29042813; PMCID: PMC5633330. [CrossRef]
- Crawford J. O., R. Graveling, A. Davis, E. Giagloglou, et al.: European Risk Observatory Report, Work-related musculoskeletal disorders: from research to practice. What can be learnt? EU-OSHA, 2020. [CrossRef]
- Machado, Gustavo C., Maher G., Ferreira P., Harris Ian A., Deyo R., McKay D., Li Qiang, Ferreira M. Trends, Complications, and Costs for Hospital Admission and Surgery for Lumbar Spinal Stenosis. SPINE, 2017, vol. 42, pp. 1737-1743. [CrossRef]
- Lee DE, Seo SM, Woo HS, Won SY. Analysis of body imbalance in various writing sitting postures using sitting pressure measurement. J Phys Ther Sci. 2018, vol.30, issue 2. [CrossRef]
- Du SH, Zhang YH, Yang QH, Wang YC, Fang Y, Wang XQ. Spinal posture assessment and low back pain. EFORT Open Rev. 2023 Sep 1;8(9):708-718. PMID: 37655847; PMCID: PMC10548303. [CrossRef]
- Fatemi R, Javid M, Najafabadi EM. Effects of William training on lumbosacral muscles function, lumbar curve, and pain. Back Musculoskeletal Rehabilitation. 2015;28(3):591-7. PMID: 25736954. [CrossRef]
- Korakakis V., O’Sullivan K., O’Sullivan P. B., Evagelinou V., Sotiralis Y., Sideris Al., Sakellariou K., Karanasios S., Giakas G., Physiotherapist perceptions of optimal sitting and standing posture. Musculoskeletal Science and Practice, Vol.39, pp. 24-31, 2019. [CrossRef]
- Bayar B., Güp A., Oruk D., Dongaz Ö., Doğu E, Bayar K. Development of the postural habits and awareness scale: a reliability and validity study. International Journal of Occupational Safety and Ergonomics, 2022. [CrossRef]
- Debora Soccal Schwertnera, Raul Alexandre Nunes da Silva Oliveirab, Alessandra Swarowskya, Érico Pereira Gomes Feldenc, Thais Silva Beltramec and Micheline Henrique Araújo da Luz Koericha, Young people’s low back pain and awareness of postural habits: A cross-sectional study. Journal of Back and Musculoskeletal Rehabilitation 35 (2022) 983–992 983. [CrossRef]
- Jia, N., Li, T., Hu, S. et al. Prevalence and its risk factors for low back pain among operation and maintenance personnel in wind farms. BMC Musculoskelet Disord 17, 314 (2016). [CrossRef]
- Tsai, M.-C.; Chu, E.T.-H.; Lee, C.-R. An Automated Sitting Posture Recognition System Utilizing Pressure Sensors. Sensors 2023, 23, 5894. [CrossRef]
- Furlanetto TS, Sedrez JA, Candotti CT, Loss JF. Photogrammetry as a tool for the postural evaluation of the spine: A systematic review. World J Orthop. 2016 Feb 18;7(2):136-48. PMID: 26925386; PMCID: PMC4757659. [CrossRef]
- G. Kandasamy, J. Bettany-Saltikov, and P. van Schaik, ‘Posture and Back Shape Measurement Tools: A Narrative Literature Review’, Spinal Deformities in Adolescents, Adults and Older Adults. IntechOpen, Apr. 14, 2021. [CrossRef]
- Victor C.H. Chan, Gwyneth B. Ross, Allison L. Clouthier, Steven L. Fischer, Ryan B. Graham. (2021). The role of machine learning in the primary prevention of work-related musculoskeletal disorders: A scoping review, Applied Ergonomics,vol. 98,2022. [CrossRef]
- Laidi R., L. Khelladi, M. Kessaissia and L. Ouandjli. 92023). Bad Sitting Posture Detection and Alerting System using EMG Sensors and Machine Learning. 2023 International Conference on Artificial Intelligence in Information and Communication (ICAIIC), Bali, Indonesia, 2023, pp. 324-329. [CrossRef]
- Jeong H., W. Park. (2021). Developing and Evaluating a Mixed Sensor Smart Chair System for Real-Time Posture Classification: Combining Pressure and Distance Sensors. IEEE Journal of Biomedical and Health Informatics, vol. 25, no. 5, pp. 1805-1813, May 2021. [CrossRef]
- Bontrup C., Taylor W. R., Fliesser М., Visscher Р., Green Т., Pia-Maria Wippert, Zemp R., Low back pain and its relationship with sitting behaviour among sedentary office workers, Applied Ergonomics, Vol. 81, 2019, . [CrossRef]
- Keskin Y., Ürkmez B., Öztürk F., Kepekçi M., Aydın T., Correlation Between Sitting Duration and Position and Lumbar Pain among Office Workers, Haydarpasa Numune Med J, vol.61, n1, pp 1-6, 2021. [CrossRef]
- Kett, A.R.; Sichting, F., Milani, T.L. The Effect of Sitting Posture and Postural Activity on Low Back Muscle Stiffness. Biomechanics, vol1, pp.214-224, 2021. [CrossRef]
- Slater D, Korakakis V, O’Sullivan P, Nolan D, O’Sullivan K. “Sit Up Straight”: Time to Re-evaluate. Journal of Orthopedic and Sports Physical Therapy, vol. 49, issue 8, pp.562-564, 2019. PMID: 31366294. [CrossRef]
- Swain CTV, Pan F, Owen PJ, Schmidt H, Belavy DL. No consensus on causality of spine postures or physical exposure and low back pain: A systematic review of systematic reviews. Journal of Biomechanic. Vol.102, 2020. [CrossRef]
- O’Sullivan K., McCarthy R., White A., O’Sullivan L., Dankaerts W., Can we reduce the effort of maintaining a neutral sitting posture? A pilot study, Manual Therapy, Vol 17, Issue 6, pp. 566-571, 2012., . [CrossRef]
- Schmidt H., Bashkuev M., Weerts J., Graichen F., Altenscheidt J., Maier Ch., Reitmaier S., How do we stand? Variations during repeated standing phases of asymptomatic subjects and low back pain patients,Journal of Biomechanics,Vol 70, pp. 67-76, 2018. [CrossRef]
Figure 1.
Participant’s posture with body markers: natural sitting posture (a) and corrected sitting posture (b).
Figure 1.
Participant’s posture with body markers: natural sitting posture (a) and corrected sitting posture (b).
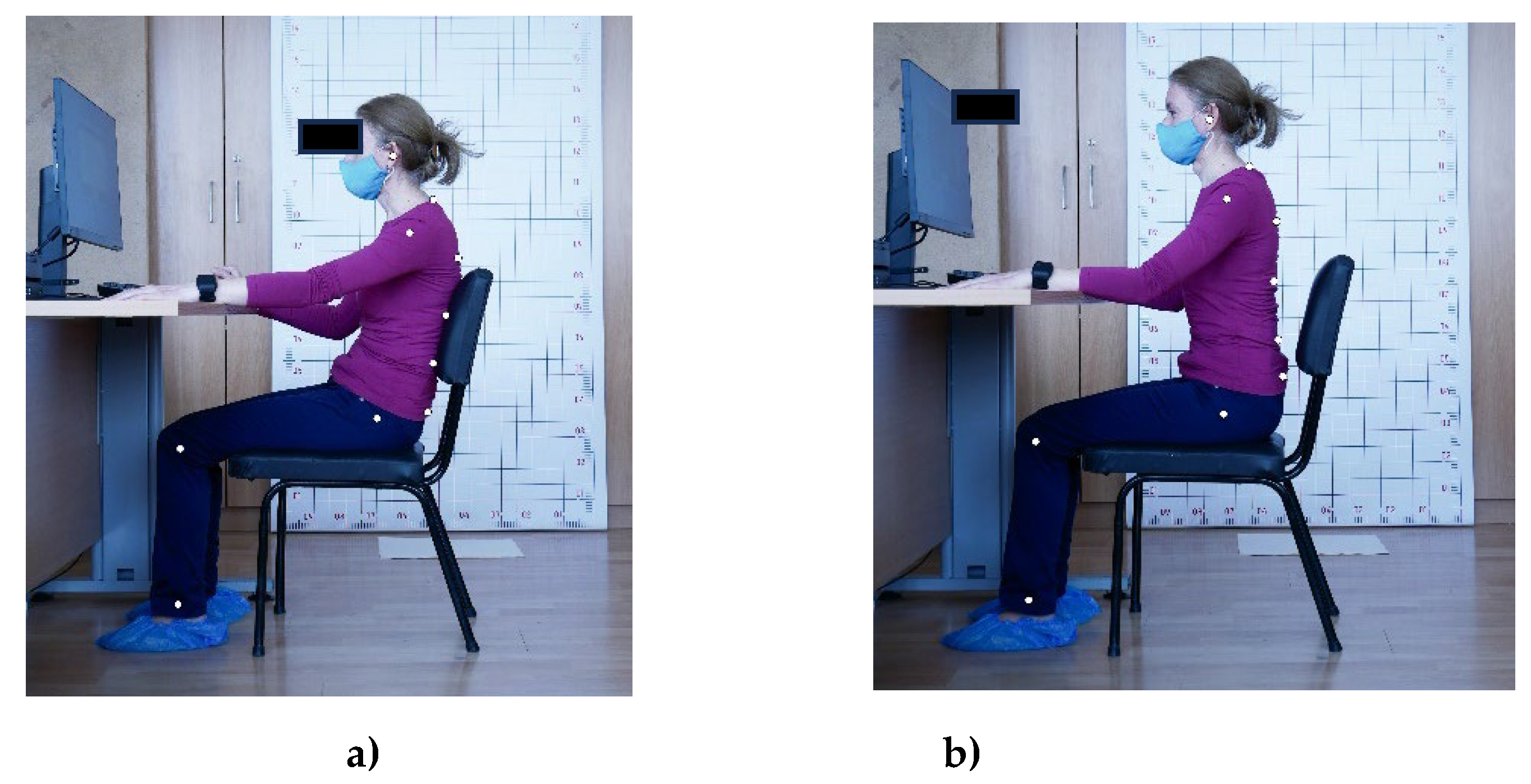
Figure 3.
Box plot representation of distributions of the postural angles (2,6,7) for 100 participants.
Figure 3.
Box plot representation of distributions of the postural angles (2,6,7) for 100 participants.
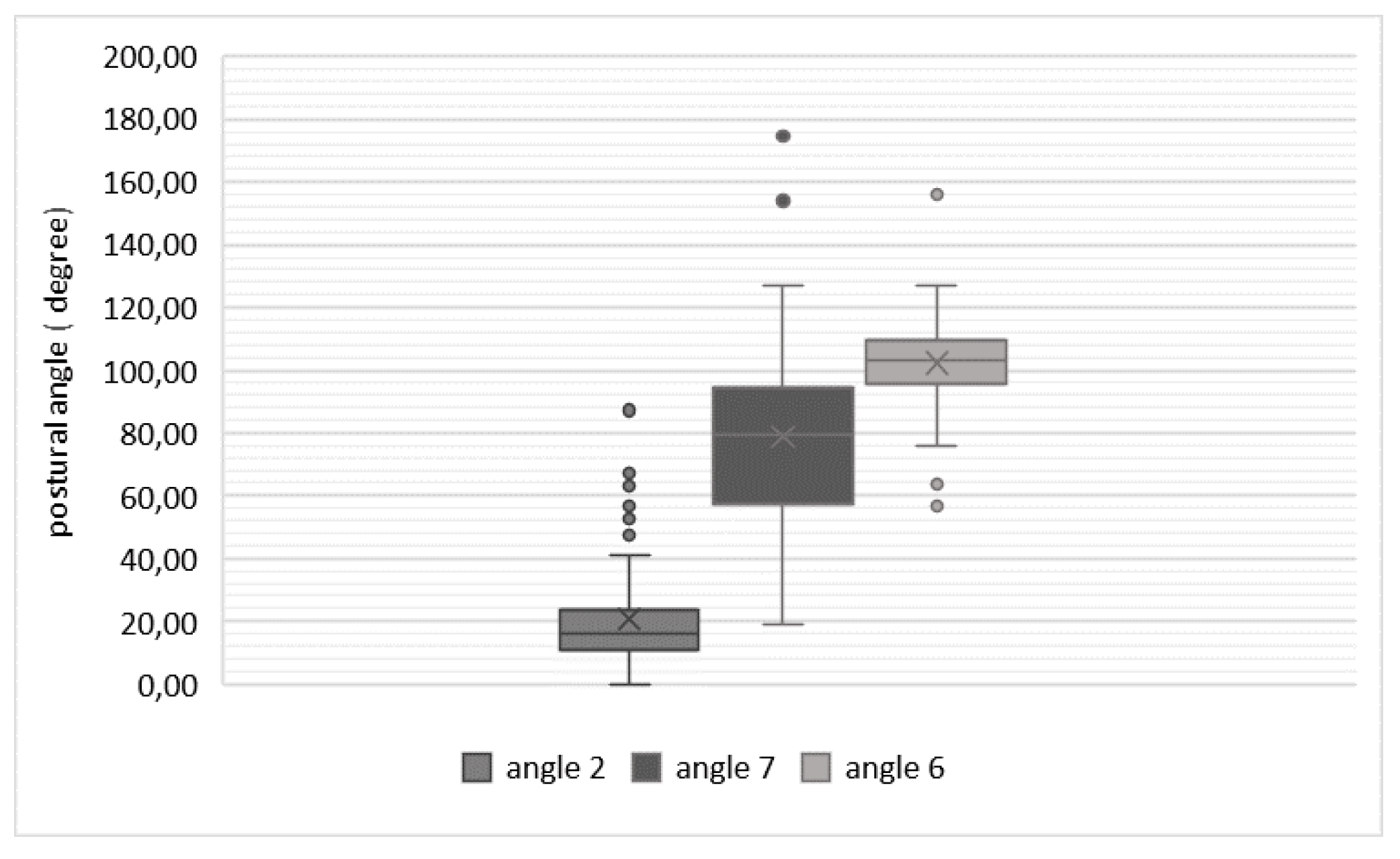

Table 1.
Self-Reported Discomfort or Pain Among Participants Resulting from Prolonged Computer Work.
Table 1.
Self-Reported Discomfort or Pain Among Participants Resulting from Prolonged Computer Work.
| Degree of pain/discomfort | Mild pain | Moderate pain | Severe pain | Very severe | Worst pain possible |
|---|---|---|---|---|---|
| Back pain | 12 | 18 | 20 | 4 | 2 |
| Low back pain | 9 | 16 | 21 | 7 | 1 |
| Pain in the buttock | 10 | 11 | 12 | 2 | 2 |
| Total people with pain or discomfort (%) | 31% | 45% | 53% | 13% | 5% |
Table 2.
Correct sitting posture detection accuracy in percentage in natural postures-based scenario.
Table 2.
Correct sitting posture detection accuracy in percentage in natural postures-based scenario.
| Classifier type | Accuracy, [%] | Standard deviation |
|---|---|---|
| Naïve Bayes | 75.3% | ± 11.2% |
| Generalized Linear Model | 57.3% | ± 18.2% |
| Logistic Regression | 60.7% | ± 13.6% |
| Fast Large Margin | 60.7% | ± 13.6% |
| Deep Learning | 63.3% | ± 22.9% |
| Decision Tree | 59.3% | ± 18.9% |
| Random Forest | 61.3% | ± 16.8% |
| Gradient Boosted Trees | 59.3% | ± 25.2% |
| SVM | 64.7% | ± 19.5% |
Table 3.
Correct sitting posture detection accuracy in percentage in corrected postures-based scenario.
Table 3.
Correct sitting posture detection accuracy in percentage in corrected postures-based scenario.
| Classifier type | Accuracy, [%] | Standard deviation |
|---|---|---|
| Naïve Bayes | 73.3% | ± 7.2% |
| Generalized Linear Model | 76.7% | ± 7.2% |
| Logistic Regression | 76.7% | ± 7.2% |
| Fast Large Margin | 74.3% | ± 6.4% |
| Deep Learning | 79.5% | ± 7.5% |
| Decision Tree | 72.9% | ± 14.6% |
| Random Forest | 80.0% | ± 16.3% |
| Gradient Boosted Trees | 78.6% | ± 18.9% |
| SVM | 73.3% | ± 12.4% |
Table 4.
Correct sitting posture detection accuracy in percentage in corrected postures-based scenario after finetuning of the hyperparameters of the first three ranked classifiers.
Table 4.
Correct sitting posture detection accuracy in percentage in corrected postures-based scenario after finetuning of the hyperparameters of the first three ranked classifiers.
| Classifier type | Optimal parameters | Accuracy, [%] | Standard deviation, [%] |
|---|---|---|---|
| Random Forest | number of trees 100; criterion Gain Ratio; max depth 10; voting strategy: majority vote |
85.00% | ± 12.30% |
| Deep Learning | 3/ 100/100/2 architecture; the first three layers – neurons with Maxout activation functions, and the two output neurons have SoftMax activation functions. |
82.50% | ± 12.08% |
| Gradient Boosted Trees | number of trees: 50; max depth: 3; learning rate: 0.01 |
81.67% | ± 16.57% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



