Submitted:
07 May 2024
Posted:
10 May 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The ongoing SARS-CoV-2 pandemic has raised concerns surrounding immunological protection against the virus, particularly for people with inborn errors of immunity (IEI). While COVID-19 vaccination induces robust antibody, memory B-cell, and T-cell responses in healthy individuals, how well vaccination protects people with IEI against infection and severe disease remains unclear – especially in the context of new viral variants and vaccine formulations – leading to anxiety, ongoing self-isolation, and repeated vaccination with limited evidence of increased efficacy. Whilst most people with IEI generate some level of cellular and/or humoral immunity to COVID-19 vaccination, the level of protection and durability of the response are unclear. Alongside vaccination, antibody-based therapeutics are aimed at limiting infection and severe disease in this cohort. Immunoglobulin replacement therapy (IgRT) provides passive immunity in antibody-deficient individuals. However, to successfully prevent SARS-CoV-2 infection, a sufficient number of neutralizing antibodies must be present in product. While antibodies against circulating variants are eventually present in IgRT products (both from natural infection and vaccination of the donors), evidence of their capacity to recognize new variants is limited. Furthermore, while antibody-based pre- and post-exposure prophylaxis can be effective, they are susceptible to decreased efficacy in the context of variant evolution. This review provides an in-depth overview of current knowledge about COVID-19 vaccine efficacy in IEIs, the efficacy of SARS-CoV-2-specific antibody products, and knowledge and technological advances required for continued protection of people with IEI.
Keywords:
COVID-19 vaccination
; SARS-CoV-2-specific antibody therapies
; immune memory
; inborn errors of immunity
; breakthrough infections
; antibodies
; memory B cells
; memory T-cells
; receptor-binding domain
1. Introduction
Since its emergence in November 2019, severe acute respiratory coronavirus-2 (SARS-CoV-2) has caused over 775 million confirmed cases of coronavirus disease 2019 (COVID-19), and over 7 million deaths worldwide [1]. The global fatality rates range across countries and age groups, from <1% in those aged <50 years up to ~4-25% in healthy individuals 60-80 years of age [2,3].
SARS-CoV-2 is an enveloped virus with a linear RNA genome belonging to the Coronaviridae family [4]. The infectious nature of SARS-CoV-2 potentiated quick establishment of a pandemic, rather than the epidemic (SARS-CoV, MERS-CoV) or endemic (seasonal coronaviruses) outbreaks of its predecessors [5,6].
Infection is established when the spike receptor binding domain (RBD) of the SARS-CoV-2 virus engages the angiotensin-converting enzyme 2 (ACE2) receptor on the surface of host T-cells, especially lung, heart, and kidney cells [7,8]. Whilst in most healthy individuals, SARS-CoV-2 infection causes asymptomatic or mild respiratory disease including fever, cough and lethargy, a subset of individuals mount an inappropriately strong inflammatory response to high viral loads resulting in severe illness, hospitalization, respiratory support, and in some cases death [9,10]. This leads to overwhelming concern that people with defective immunity, particularly those with rare inherited immunodeficiencies (approximately 1 in 10,000 people) [11] or more common acquired immunodeficiencies (approximately 1 in 1,200 people) [12], may be at increased risk of severe COVID-19 disease.
Whilst public health measures, such as mask wearing, hand washing, social distancing, and shielding have undoubtedly helped protect people with Inborn Errors of Immunity (IEI), this has posed other issues including feelings of isolation and adverse impacts on quality of life [13,14]. As such, the medical and scientific community rapidly pivoted to combat the global pandemic by providing novel and innovative solutions for SARS-CoV-2 testing, vaccination, and therapies to treat disease and help cover the gap in immunity in an effort to reduce virus transmission and COVID-19 disease severity. We here provide an in-depth overview of the current understanding of COVID-19 vaccine efficacy in people with IEI, efficacy of SARS-CoV-2 specific antibody products, and discuss new insights and technological advances that can enhance protection of people with IEI or other immunocompromised conditions in the changing SARS-CoV-2 landscape [15].
1.1. Inborn Errors of Immunity (IEI)
At present, genetic variants in more than 485 genes are known to cause an IEI. Patients with IEI can be broadly classified into 9 groups capturing the diversity of clinical, genetic, and immunological phenotypes of disease. Groups are defined by the nature of the rare genetic defect identified, the immune cell(s) affected, and infections to which individuals exhibit increased susceptibility [16]. Of these 9 categories, the most prevalent is predominantly antibody deficiency (PAD) [17,18], including patients with Common Variable Immunodeficiency (CVID) and agammaglobulinemia. Other categories include combined immunodeficiencies (CID), and diseases of immune dysregulation known to have defects in multiple immune cell lineages. A common presenting feature in PAD is profound antibody deficiency, poor responses to vaccination, and increased susceptibility to sinopulmonary infections underpinned by defects in B-cell development, differentiation, and function [17,19,20]. It is generally accepted that many of these diseases are accompanied by defects in other immune cells involved in innate and adaptive responses. These include T-cells, which are integral for robust immune generation to infectious agents and may have a key role in vaccine efficacy for some pathogens, particularly those of viral origin. As a result, in people with PAD reduced vaccine efficacy can result in increased susceptibility to vaccine-preventable disease. For these individuals, preventative therapy centers around tackling antibody deficiency including lifelong immunoglobulin replacement therapy (IgRT), annual vaccinations (e.g., for influenza), and prophylactic antibiotics in a complicated attempt to reduce infectious burden [21,22]. Thus, the emergence of the novel SARS-CoV-2 virus presents unprecedented challenges for protecting and treating those with IEI [17,20].
1.2. COVID-19 Infection in People with IEI
Whilst in healthy individuals, SARS-CoV-2 infection generates functional memory B- (Bmem), memory CD4+ T- (CD4+ Tmem) and CD8+ T-cell (CD8+ Tmem) responses, as well as neutralizing antibodies [5,6,23], some of these responses are perturbed in people with IEI resulting in more severe disease outcomes [3]. These have been extensively reviewed elsewhere so will not be described in depth here. Briefly, Tangye et al. recently reported that ~1330 infections with SARS-CoV-2 in IEI had been published to date with 60% of reported individuals diagnosed with antibody deficiency [3]. Among these, a case fatality rate of 8.5% was documented in people with IEI as compared to ~1.1% in the general population. It was noted that the case fatality rate for children 0-19 years old with IEI was up to 100 times higher than that observed for those of the same age in the general population [3].
Within the IEI population, individuals with defects in genes including AIRE (Autoimmune Regulator), IRF7 (Interferon regulatory factor 7) and IFNAR1/2 (Interferon-α/β receptor) had significantly higher COVID-19 case fatality rates, clearly demonstrating that genetics can adversely impact patient outcomes to SARS-CoV-2 infection [3]. In particular, individuals with biallelic variants in AIRE experienced the most severe COVID-19 disease as a consequence of production of neutralizing antibodies to cytokines, including type I interferon (IFN). These anti-IFN antibodies prevent binding of IFN-α or β to its receptor (IFNAR), thereby inhibiting the pivotal role of IFNs in mediating a host response to viruses [24]. Furthermore, SARS-CoV-2 has unmasked undiagnosed IEI in otherwise asymptomatic individuals, with these individuals presenting with life-threatening COVID-19. The first identified genetic cause of severe COVID-19 disease, was published in 2020 by van der Made et al. Here, rare X-linked (XL) loss-of-function (LOF) variants in the gene encoding Toll-like receptor 7 (TLR7), were identified in 4 young males with critical COVID-19 disease [25]. These variants were shown to cause impaired type I and II IFN responses, known to be crucial for immune responses against viruses. Later studies, have additionally revealed novel rare XL LOF variants in TLR7 in young males critically ill with COVID-19, with these defects shown to underlie severe COVID-19 disease in 1-2% men under 60 years of age [25,26,27,28]. Alongside, TLR7 genetic variants in the TLR3 gene has been found to compromise local type I IFN-mediated innate immune responses. Together, variants in these genes are estimated to be the cause of severe COVID-19 in up to 5% of people under 70 years [25,26,29].
Additional studies have identified additional loci where enrichment of rare autosomal recessive (AR), or autosomal dominant (AD) variants in IFNAR1 (AR/AD), IFNAR2 (AD), IRF3 (AD), IRF7 (AR/AD), TBK1 (AD), TICAM1 (AD), TLR3 (AD), and UNC931 (AD), predispose ~3.5% individuals with severe SARS-CoV-2 infection to critical COVID-19 pneumonia [30]. These genes are known to control TLR3 and IRF7-dependent induction and enhancement of type I IFN signaling showing the important role of these pathways in control of SARS-CoV-2 infection. Thus, suggesting that type I IFN administration might reduce disease severity if administered early in disease [30]. These findings were subsequently followed by discovery of additional rare variants in IFNAR1 (AR) [31,32], TNFRSF13B (AD) and TBK1 (AD) underlying severe COVID-19 [33].
Strikingly although only a few individuals have been identified with rare AR IFNAR1 or IFNAR2 variants, COVID-19 lethality rates are 57% in these individuals [30,31,32,34]. IFNAR1 and IFNAR2 encode the α and β chain of the type I interferon (IFN)-α/β receptor (IFNAR) respectively, which along with IFN-I form IFNAR. Upon binding of IFN-α or β to the IFNAR receptor, the IFNAR1 chain binds tyrosine kinase-2 (TYK2) and IFNAR2 interacts with Janus Kinase-1 (JAK1) and Signal transduction and transcription activation (STAT) mediating downstream JAK/STAT (primarily STAT1 and STAT2) signal transduction resulting in the IFN-I induced cellular response [35].
Further to this, an international study has identified recessive defects including XL TLR7 and AR IFNAR1, STAT2 and TYK2 in 10% of pediatric patients hospitalized with COVID-19 pneumonia [36]. Together, the predisposition of individuals with variants in the aforementioned genes to severe COVID-19 disease, demonstrates the critical role of type I IFN in host defense against SARS-CoV-2, whilst this pathway is redundant for other infectious agents. Interestingly, a more recent retrospective cohort study by Ngyuen et al., found that many studies of infection outcomes in IEI did not control for factors classified as social determinants of health, such as race/ethnicity [37]. In their cohort of various combined, humoral, or innate immunodeficiencies, and age (2 months to 69 years), they identified an association between an increased risk of hospitalization and race, ethnicity, obesity, and neurological disease. The authors posit that these findings have important implications for current treatment and COVID-19 disease management guidelines for IEI populations, which center around cellular and genetic mechanisms of severe disease risk.
1.3. SARS-CoV-2 Variants
Over the pandemic, multiple SARS-CoV-2 variants have evolved with the first, Alpha, detected in September 2020 (Table 1). Viral variants contain mutations that are advantageous for viral spread, e.g., increased infectivity, viral fitness or escape from immune responses [38]. Multiple predisposing factors including geographical location, environmental and economic conditions, and access to vaccination favor viral diversification thus leading to emergence of variants in the general population [39]. Indeed, this concern extends to the unvaccinated, and inequitable global vaccine access may play a role in the ongoing development of SARS-CoV-2 variants. There is also evidence that the delayed viral clearance observed in people with immune disorders contributes to the emergence of viral variants [40,41,42,43].
While over 30 different SARS-CoV-2 genetic clades have been identified to date, not all were a cause for heightened concern or attention. Therefore, the World Health Organization (WHO) monitored variants with increased viral transmissibility or virulence or escape from host antibody. For example, the Omicron BA.1 variant which emerged in November 2021 has 37 spike protein mutations resulting in increased ACE2 binding affinity and decreased humoral immune recognition [44]. To date, the Omicron lineage is the most divergent variant, due to the high number of mutations it harbors, with all sublineages maintaining properties of increased immune evasion and preference for binding to ACE2, compared to earlier SARS-CoV-2 variants [45,46] (Table 1).
Due to the ongoing evolution of SARS-CoV-2 variants, there has been a shift in variant predominance from Omicron XBB.1.5 and XBB.1.6. in July 2023, to Omicron E.G.5.1 in December 2023, with the epidemiology differing by geographical locations (Figure 1). The current dominant variants have an immune evasion advantage, but result in less severe infections in the general population [38,47]. Here, more observation is needed to determine how variant transmission impacts the IEI community in terms of infection rates and severity of illness.
2. COVID-19 Vaaccination
The emergence of SARS-CoV-2 and the rapid roll-out of new vaccine formulations have provided a unique opportunity to examine vaccine responses in infection- or vaccine-naïve individuals with or without IEI. This has the capacity to provide novel insights into the immunological defects in individual IEI patients [19], as well as to provide crucial information to direct future vaccination programs.
2.1. Vaccine Formulations for COVID-19
During the pandemic, the WHO evaluated and provided Emergency Use Authorization (EUA)-qualification for COVID-19 vaccines in July 2020 with the initial aim to provide protection from viral transmission, severe disease, hospitalization, and death [48,49]. As viral transmissibility increased (September 2020), focus switched to the latter aspects of vaccine efficacy, as well as the predominance of breakthrough infections [2,50]. To date, more than 13.6 billion doses of COVID-19 vaccine have been administered in the ongoing fight against SARS-CoV-2. This includes receipt of at least one dose of COVID-19 vaccine by 70.6% of the world’s population and 32.9% of people in low-income countries [1]. This in isolation shows the disparity in vaccine access between low and middle/high income countries. Granular data is not available in many regions to assess the extent to which this disparity impacts people with IEI.
The vaccine formulations used for primary dosing in Australia, the UK and USA included mRNA vaccines (Comirnaty (BNT162b2, Pfizer BioNTech), SpikeVax (mRNA-1273, Moderna), viral vector vaccines (Ad26.COV2.S (Johnson & Johnson, Janssen), adenoviral vector based ChAdOx1 nCoV-19 (Oxford/AstraZeneca)), and one protein subunit vaccine (Novavax, Nuvaxovid). All vaccines are generally safe and highly effective at preventing hospitalization in healthy populations. Notable exceptions included the increased incidence of thrombosis with thrombocytopenia syndrome or severe anaphylactic reactions to polyethylene glycol in certain individuals with specific vaccine formulations [51,52]. Importantly, these five authorized COVID-19 vaccines induce a robust humoral response in healthy individuals, with some variation in antibody level identified between different formulations as well as based on timings between doses [50,51,53]. For example, it has been shown that spike RBD-specific IgG antibody levels are higher in healthy individuals who received 2 primary doses of Comirnaty mRNA vaccine compared to those who received 2 primary doses of ChAdOx1 nCOV-19 adenoviral vaccine [5,6,54,55]. The development and rollout of the primary immunization series, and any subsequent boosters are now an indispensable cornerstone of the global response against COVID-19.
In comparison, other authorized vaccination regimens including Coronavac (Sinovac Biotech), Sputnik-V (Gam-COVID-Vac) and BBIBP-CorV (SinoPharm, Beijing Institute Biological Products) produce a substantially reduced antibody response with seropositivity rates of 36.9 – 50%, known to be substantially lower than seen in convalescence. This explains the reduced efficacy of these vaccines both with respect to protection from symptomatic infection and severe infection and hospitalization [56,57,58].
Despite the emergence of SARS-CoV-2 variants as early as May 2021, most COVID-19 vaccine formulations until late 2022/early 2023 exclusively contained spike protein of the ancestral WH1 strain. To combat ongoing viral evolution, bivalent mRNA vaccines were developed and released to further boost immunity to emerging Omicron variants, with the aim of providing protection from severe disease, hospitalization and death. To date, four bivalent vaccines have emerged: the Pfizer bivalent vaccine containing equal amounts of WH-1 and Omicron BA.1 (Comirnaty Original/Omicron BA.1) or Omicron BA.4/BA.5 spike (Comirnaty Original/Omicron BA.4-5) [59], and the Moderna bivalent vaccine containing equal amounts of WH-1 and Omicron BA.1 (Spikevax Bivalent Original/Omicron BA.1) or Omicron BA.4/BA.5 spike (Spikevax Bivalent Original/Omicron BA.4-5). In May 2023, due to increased prevalence of Omicron XBB.1 lineages, the WHO recommended use of the monovalent XBB.1.5 as the antigen for ongoing COVID-19 vaccination. Since then, two monovalent Omicron XBB.1.5 vaccines: Pfizer (Comirnaty) Omicron XBB.1.5. and Moderna (Spikevax) Omicron XBB.1.5. have been approved for use by U.S. Food and Drug Administration (FDA), Australian Technical Advisory Group on Immunization (ATAGI), and the UK medicines regulator [15,60,61].
Due to the sparsity of information regarding the efficacy of bivalent vaccinations in IEI populations, this review summarizes the information to date on the healthy individual and IEI patient response to the original monovalent vaccination formulations.
2.2. The COVID-19 Vaccine-Induced Response in Immunocompetent Individuals
In immunocompetent individuals, COVID-19 vaccination generates neutralizing antibodies, as well as functional SARS-CoV-2-specific B-cell memory (Bmem) and CD4+ and CD8+ T memory (Tmem) responses, namely towards the RBD known to directly bind the ACE2 receptor. These correlates define a protective immune response, emerging 1-2 weeks following vaccination. Whilst specific antibody and neutralizing titers have been shown to wane 1-3 months post vaccination, protection against severe infection has been shown to persist for at least 4-6 months. Importantly, vaccine-induced Bmem and Tmem responses are known to persist longer term, and likely represent a more durable marker of immune protection than antibodies [5,6].
Moreover, it has been shown that booster vaccination can significantly boost Bmem responses specific for ancestral virus and are cross-protective against Omicron subvariant RBD [53,54,55]. It is important to note that vaccine formulation can have a dramatic impact on the magnitude of response, such that individuals who received a 2-dose primary regimen of Pfizer BNT162b2 generated a significantly higher magnitude of ancestral WH1 RBD-specific plasma IgG and Bmem compared to those receiving the 2-dose adenoviral ChAdOx1 vaccine [53,55]. However, upon boosting with a third dose of mRNA vaccine both groups demonstrated a significant increase in ancestral WH1 RBD-specific plasma IgG and Bmem numbers with the magnitude of response now similar between both groups. Furthermore, the mRNA third dose booster increased recognition of the Omicron BA.2 and BA.5 variants both by antibodies and Bmem [53]. This further exemplifies the need to assess these attributes of the immune response in COVID-19 vaccinated IEI patients and determine whether the boosters have the same benefit in this population.
2.3. The COVID-19 Vaccination Response in IEI Patients
Globally, it has been acknowledged that immunocompromised individuals, including those with IEI, may benefit from extra doses of COVID-19 vaccines to generate responses equivalent to those observed in healthy individuals [62,63,64,65]. First, it was recommended by the U.S. FDA, ATAGI, and UK medicines regulator that an additional (third) dose was added to the primary regimen. This differs from the 2-dose regimen (except for Ad26.CoV2.S which comprised of a 1-dose regimen) for the general population [52,64,66]. Vaccines approved by the aforementioned regulatory bodies showed evidence of a high efficacy for protection from infection, as well as protection from severe disease, hospitalization, and death [51,67]. Whilst breakthrough infections with SARS-CoV-2 variants have been documented in patients with IEI, those who have been vaccinated experienced lower disease severity [68].
In contrast to the general population, individuals with IEI have variable immunological responses to vaccination, with responses impaired in some patients [69,70,71,72,73,74] (Figure 2). This section will review the humoral response reported in the literature in a variety of IEIs. For the purposes of this review, we refer to doses 1-3 as the “primary” series for people with IEI, and any additional doses as “boosters”. This differs from healthy individuals where “primary” series refers to doses 1-2, with doses three and onwards qualifying as boosters.
2.3.1. Humoral Response
People with antibody deficiencies generate a particularly poor antibody response to vaccination; indeed, “diagnostic vaccination” is used to clinically evaluate individuals for the presence of humoral IEI [75]. It was therefore an early concern whether these populations would develop any meaningful protection from COVID-19 vaccines, especially those using novel mRNA vaccine platforms. Here, we reviewed 58 papers evaluating the humoral immune response generated by individuals with different IEI to COVID-19 primary vaccines and/or booster doses (Table S1, Figure 2). In many cases [69,76,77,78,79,80,81,82,83], studies age-matched IEI patients to healthy controls to compare the robustness and quality of antibody responses to that of the general population. This is important because otherwise, known age-related changes in the immune system would confound the results of each study. The published study designs varied from observational [71,77,83,84,85,86,87,88,89,90,91,92,93,94,95,96] to interventional studies and clinical trials [80,82,83,97,98]. Furthermore, humoral responses were reported by seroconversion, antibody concentration/titers, and, in some cases, virus neutralization/pseudo-neutralization capacity (Figure 3 and Table 2). Samples were generally collected between approximately 2 weeks to one-month post-vaccination; with a smaller portion of studies collecting samples at 2-, 3-, or 6-months post-vaccination [88,89,99]. These differences in sampling time post vaccination can have dramatic effects on the status of the immune response. For these reasons, care should be taken when comparing studies as variations in sample collection time points and experimental methodology will affect the quantitative ranges etc. (Figure 3 and Table 2).
Overall, seroconversion in populations with IEI was much more variable and at a lower magnitude compared to healthy controls across the primary series and additional doses [74,76,77,78,83,94,99,100,101,102,103,104,105,106,107,108], regardless of methods of measurement differed. This is due to the heterogenous genetic and immunologic phenotype of disease in these individuals. In one study, individuals with IEI overwhelmingly displayed poorer seroconversion rates (ranging from 16.6%-61.4%) compared to healthy controls (90-100%), after two doses of mRNA vaccine (Comirnaty, SpikeVax) [73]. Despite the lower seroconversion rate post dose 2 it is clear that booster doses increased seropositivity (76-100%) in IEI patients after 3 vaccine doses [73,74,77].
As described in Section 1.1, the immune defects in patients with IEI are highly diverse and likely impact the outcomes of COVID-19 vaccination. Most patients examined in the literature had PAD, in line with this group of diseases being the most prevalent IEI group (42% worldwide IEI diagnoses) [18]. In those receiving an mRNA vaccine, 20.6% to 90.0% of individuals with PAD seroconverted after two doses [71,74,81]. In contrast in a cohort of individuals with primary or secondary antibody deficiencies vaccinated with either Comirnaty or ChAdOx1 nCoV-19, the overall seroprevalence rose from 61.4% to 76.0% after a third dose [73]. Tandon et al. 2023 assessed the differences between an adult (n = 62) and relatively smaller pediatric (n = 13) PADs cohort, finding that antibody levels were higher in the pediatric cohort after a primary series (Comirnaty), as well as after a monovalent booster, but only for those classified as having mild PADs [109]. There was otherwise limited research on pediatric PAD cohorts. A study by Shin et al. specifically investigated the clinical and/or immunological factors in a group of mixed PADs that might predict their COVID-19 vaccination response [110]. They found a lower seroconversion rate and neutralizing antibody levels to vaccination in CVID patients compared to other PAD categories (e.g., IgG deficiency, IgG2 subclass deficiency, and specific antibody deficiency (SpAD)). This was associated with a number of factors including lower baseline IgG, IgA, and proportion of Bmem cells, a higher proportion of CD8+ Tmem cells, and a co-diagnosis of an autoimmune disorder [110]. Mizera et al. also found that in their cohort study of various PADs, that all patients in their CVID subgroup had around 5-fold lower titers than other subgroups [106]. Thus, as stated by Quinti et al., with the high immunological and clinical diversity within CVID, each patient should be assessed individually for their capacity to mount a protective vaccination response [111].
In contrast, several studies report on smaller groups of patients with specific IEI diagnoses. For example, one report of individuals with STAT1-GOF (n=7) found that 57% seroconverted after two doses of vaccine [112]. Another case report on one individual with XMEN/MAGT1 deficiency reported a reactive spike-specific total antibody response after two doses of mRNA vaccine [90]. In addition, Timothy et al. also completed a retrospective chart review of eight patients with CTLA-4 deficiency (two children and six adults). Of those who had their SARS-CoV-2-specific IgG levels tested (n=2), antibody titers were lower (<6.25%) than that of the healthy unvaccinated controls [113]. Multiple studies evaluated antibody responses in individuals with XLA. In all studies patients had nearly nonexistent antibody responses after two doses with either ChAdOx1 nCoV-19 or Comirnaty [81,98]. In fact, in one case study of three people with XLA, only one was able to mount a measurable antibody response post-vaccination [114] (Figure 2). This is consistent with the inherent B-cell defects in these individuals whereby peripheral B cells are low or absent, resulting in an absence of serum immunoglobulins, and an inadequacy in generating a B-cell response to vaccination [16,17]. In this case, the observed post-vaccination antibody response is likely due to the IgRT received by the patient to treat their underlying antibody deficiency (See Section 3.1).
In several studies with more diverse cohorts of IEI, seroconversion differed by subgroup. Van Leeuwen et al. found significantly lower seroconversion rates in those with CVID, XLA, and CID compared to SpAD, undefined antibody deficiency, and phagocytic defects [71]. In studies which evaluated possible predictors of antibody responses in IEI population(s) certain factors, such as condition severity [78,80], previous history of autoimmunity [69], underlying immunosuppressive treatment [78,80] or low numbers of Bmem cells pre-vaccination [81], were associated with poor responses (Figure 2).
This is important as previous studies have established a connection between the humoral and cellular response to infection outcomes in healthy individuals [115].
Interestingly, in some studies which compared both COVID-19 naïve individuals and those with a history of previous SARS-CoV-2 infection, recovery from natural SARS-CoV-2 infection corresponded with a more efficacious antibody response to the vaccination series (i.e., “hybrid immunity”). This includes a more robust seroconversion rate [97,98], higher neutralization capacity [76], and better protection against the Delta variant [116]. Additionally, Abella et al. found that even in the cohort with plasma cell diseases, those with multiple myeloma who had hybrid immunity had a higher plasma neutralization capacity than infection-naïve individuals 3 months post-vaccination [117]. This provides insights in to whether hybrid immunity provides a more robust immune response than vaccination alone, and the capacity of natural infection to shape immunity.
Recently Abo-Helo et al. found that antibody levels remained poor in people with more severe disorders of humoral immunity 5-6 months after vaccination, suggesting the need for additional doses to preserve sufficient protection [82]. Van Leeuwen et al. conducted a large multicenter study of patients with PADs, following them up to 6 months past the primary vaccine series, and a through a third dose for smaller subset of 50 CVID patients. Their cohort all received mRNA-1273 for their primary series, and either BNT16b2 or an unspecified vaccine formulation for a third dose if applicable. At 6 months past the primary series, the decline in antibodies ranged from 5.9 to 11.2-fold, measured in GMT of S-specific IgG. However, seropositivity rates at 6 months ranged from 73% to 98%, with those in the XLA subgroup maintaining a relatively low rate of 24% [118]. Another study of a mixed cohort of more than 50 patients who received at least one dose of any mRNA-based OR inactivated vaccine, or a combination of both, found no significant different in antibody levels across formulations [119].
There remains limited knowledge about the efficacy and durability of responses generated to different COVID-19 vaccine formulations in people with IEI. Leung et al. studied the humoral response to both Comirnaty and CoronaVac (“Sinovac”) formulations in their cohort of mixed IEIs and found that 73% of individuals were seropositive after a full series of either formulation [93]. Some studies found that a full Comirnaty vaccination series was more efficacious than ChAdOx1 nCoV-19 [120], and this superior protection was maintained for about 6 months past the second dose [73]. Overall, most individuals reported had increased neutralizing activity after a partial or full vaccine series [69,70,71,73,83,93,98,116,120]. Furthermore, a follow-up from the COV-AD study using a live virus neutralization assay with Vero cells, found 99.8% of their study subjects had neutralization activity after a booster dose [98]. However, whether these are a bona fide response to vaccination or a consequence of receiving SARS-CoV-2-specific antibody-containing IgRT was not evident, although in at least one study, IgRT did not appear to be significantly associated with either titer or neutralization activity [74]. It is also important to note the sparsity of data surrounding SARS-CoV-2-specific Bmem generation in individuals with IEI both in response to natural infection and SARS-CoV-2 infection, which is necessary to provide information about the generation and durability of the Bmem cells in these populations and their ongoing ability to produce antibody.
Furthermore, to date, some IEI patients may have received five or more vaccine doses; however, information on the efficacy of these later doses is limited. This is likely due to lack of available participants with sufficiently time elapsed since their most recent dose [98], and also insufficient time elapsed to enable sample analysis and reliable reporting of findings.2.3.2. Memory T-cells
Like humoral immunity, cellular immunity in people with IEI is more variable than that of healthy populations. Recent research focuses attention specifically on the mechanisms of Bmem, Tmem, and innate immune cells following COVID-19 vaccination in IEI populations.
As such, we reviewed 43 papers investigating the cellular response overall and its relationship with the humoral response of IEI populations after receiving COVID-19 vaccination (Table S2). As with antibody production, IEI patients demonstrated suboptimal CD4+ and/or CD8+T-cell responses compared to the general population, ranging from ~30-80% of that of healthy controls [70,77,93,98,121,122]. A number of studies found that individuals with IEI could mount measurable CD4+ and/or CD8+T-cell responses [86,104,105,123], measured as percent of IFN-γ-positive T-cells via IFN-γ release assay (IGRA), ELISpot assay, or flow cytometry (Figure 2, Table 2).
Studies that evaluated both cellular and humoral post-vaccination immunity found varying levels of correlation between these two responses, making it difficult to draw definitive conclusions about their relationship [93,96,97]. Sauerwein et al. found an association between intact spike-specific CD4+ T-cell responses and normal IgG responses, defined as a titer of spike protein 3x the limit or more, in individuals with CVID or milder antibody deficiency [100]. Oyaert et al. found a positive and significant correlation between anti-spike IgG and IFN-γ levels in IEI and chronic kidney disease (CKD) subgroups [99]. Notably, Gao et al. were able to confirm a positive correlation between antibodies and spike-specific CD4+ T-cells in all their study groups, both healthy and immunocompromised [124].
Other studies found that a negative humoral response was associated with a poor cellular response. Bergman et al. found that low levels of naïve CD4+ T-cells correlated with a poor antibody response in the CVID participants of their prospective clinical trial [76]. Similarly, Antoli et al. established that low CD4+ and CD8+ T-cell counts were a predictor of poor antibody response specifically in CVID patients [85]. Barmettler et al. also observed a correlation between low CD4+ T-helper cells and low specific antibody responses in their mixed cohort of individuals with secondary and severe primary PADs, including complicated CVID/SpAD, activated P13K-syndrome, TACI deficiency, NFKB1 deficiency, HGG, and IgG subclass deficiency. This observation was evident for both mRNA and the Ad26.CoV.S vaccines [79].
In contrast, several studies reported no association or a discordant relationship between the humoral and cellular responses [93,96,97]. For example, Pulvirenti et al. found nearly no T-cell response in their vaccinated cohort of people with CVID, despite this cohort presenting a positive (albeit suboptimal) IgG response [97]. Findings from a subsequent paper by Pulvirenti et al. demonstrate that T-cell abnormalities resulting from CVID may play a role in lack of specific antibody responses after vaccination [91]. Interestingly, in a separate cohort followed by Goschl et al. had a robust specific CD4+ and CD8+ T-cell response to vaccination, they found no significant correlation between that response and antibody levels [125]. Similarly, a case study of five individuals with PAD by Steiner et al. found a robust cellular response, yet no humoral response in their entire cohort [126]. Mizera et al., in their study on a cohort of individuals with primary antibody deficiencies receiving 2-4 doses, found that anti-SARS-CoV-2 IgG did not correlate with either CD4+ or CD8+ levels, but rather NK cells [106]. This underscores the suggestion made by previous papers to measure both the cellular and humoral response to develop a more complete post-vaccination immune profile in each individual [127,128].
Importantly, some studies evaluated the spectrum of T-cell responses by IEI patients to identify specific characteristics or factors that may predict poor or robust responses. Shin et al. found a correlation between baseline immune profiles as well as comorbidities, where poor vaccine responders among their mixed cohort of PADs had autoimmune diseases, low levels of baseline IgG, low naïve CD8+ T-cells, and higher levels of effector CD8+ Tmem [110]. Gao et al. who looked extensively at T-cell profiles between subgroups of immunocompromised individuals, found overall that specific CD8+ T-cells were generated at a higher rate than CD4+ T-cells. These frequencies were comparable at 35 days after dose 2 between healthy controls, IEI, HIV, and HSCT, but lower in SOT and CLL [124]. This study found that individuals enrolled in the trial generated higher levels of higher frequencies of SARS-CoV-2 specific CD4+ T-cells after two vaccine doses [124]. Similarly, van Leeuwen et al. conducted a multicenter study of different subgroups of IEI compared to healthy controls. Only the CVID subgroup had significantly lower IFN-γ response rates compared to healthy controls. Within this subgroup, lower responses were associated with age and lymphoproliferative diseases [71].
Similarly, we identified case reports of vaccination among less researched IEI, including STAT1-GOF and X-linked SASH3 deficiency, which found that nearly all studied individuals were able to mount both a cellular response and humoral response despite a suboptimal baseline immune profile due to their inborn immune disorders [112,129] (Figure 2). Of note, Bloomfield et al. found that 85% of their STAT1-GOF cohort, including 2 individuals on the JAK inhibitor ruxolitinib, produced a cellular response comparable to healthy controls [112].
Like with post-vaccination antibody levels, exogenous factors such as natural SARS-CoV-2 infection and vaccine formulation appear to impact T-cell responses in certain settings. Some studies found that SARS-CoV-2 infection increased T-cell activity in antibody-deficient individuals [130], while another found poor CD4+ and CD8+ T-cell responses after both previous infection and subsequent vaccination [97]. Other studies have reported that prior SARS-CoV-2 infection results in improved immune response after the first [131] and second [98] vaccine dose. Additionally, other studies have reported the phenomena of pre-existing cross reactive CD4+ T-cells that can recognize SARS-CoV-2 [132]. The COV-AD study follow-up found that receipt of heterologous vaccines by infection-naïve IEI individuals was associated with a significantly higher likelihood of T-cell response generation, compared to homogenous boosting [73]. Lin et al. found that a third dose increased the amount of SARS-CoV-2-specific CD4+ and CD8+ T-cells generated [87], and Goda et al. were able to demonstrate a 30% increase in T-cell activity after a third dose of Comirnaty following two ChAdOx1 n CoV-19 in individuals with CVID [120].
The rise of viral variants has sparked questions about the durability of T-cells, as well as whether strain-specific T-cells are broadly protective against variants in the IEI population. While few studies have been published to date in either healthy populations or individuals with IEI, there is some evidence of sustained reactivity.
In terms of longevity, Hurme et al. conducted a longitudinal cohort study over 22 months in a mixed cohort of primary and secondary antibodies deficiencies, finding a robust cellular response. Specifically, across 1-4 doses of either mRNA-1273, BNT162b2, or ChAdOx1, 95% of their cohort had detectable T-cell responses after the primary series as measured by flow cytometry, dropping down to 78% at 3 months following a fourth dose. In a smaller subset of individuals, they observed that CD4+ cell responses were higher than CD8+ at the same timepoints when stimulated with wildtype SARS-CoV-2 strain [102].
Van Leeuwen et al. extended their investigations to observe cellular responses at 6 months post-primary vaccination in their mixed IEI cohort, finding that while IFN levels decreased significantly in most of their subgroups (XLA, CVID, IgG/SPAD), these responses were still detectable in varying levels [118]. Barouch et al. found that the Ad26.CoV2.S vaccine induces durable cellular immunity with minimal decreases over the course of 8 months in a healthy population [133]. In another healthy individual cohort, Liu et al. found that both the Ad26.CoV2.S and Comirnaty vaccine induced durable spike-specific CD4+ and CD8+ T-cell responses. Here, 82-84% CD8+ T-cell responses were cross-reactive to the Omicron B.1.1.529 variant [122]. Sanchez et al. recently demonstrated that people with XLA had an increased T-cell response to variants compared to healthy controls, while individuals with CVID had a reduced response [134]. More evidence is needed to understand the post-vaccine T-cell response in general as well as its ability to provide protection in the face of future SARS-CoV-2 variants. This coupled with correlation between generation and durability of Tmem and Bmem responses, will provide crucial information about whether, for example, generation of Tmem responses in the absence of Bmem is sufficient for protection from disease.
2.3.3. Memory B Cells & Innate Cells
Very few studies evaluated post-vaccination production of Bmem or those of the innate immune response (Table S3). Those that did tended to concentrate on the correlation between presence of these cells and SARS-CoV-2-specific antibody levels. Most studies reviewed found an association between measures of Bmem and humoral responses. In three studies following individuals with antibody deficiencies, their reduced antibody response correlated with a reduced Bmem count [76,85,110]. However, other studies found little to no correlation between B-cell measurements and humoral response [97,129], likely due to patients receiving IgRT, where antibodies from product are indistinguishable from vaccine-induced antibodies. As with the T-cell response, Lin et al. found a similar effect of a third vaccine dose increasing SARS-CoV-2-specific B-cell responses [87]. The previously mentioned individual with SASH3 deficiency had marked B-cell lymphopenia and reduced switched Bmem cells [129]. Pulvirenti et al. found that SARS-CoV-2 infection produced a more classical Bmem cell response in unvaccinated individuals with CVID, whilst vaccine recipients with CVID had a more atypical [CD19+CD27–CD24–CD38–] Bmem response [97].
At the time of this review, there was limited literature regarding specific innate cell responses to SARS-CoV-2 primary vaccination in individuals with IEI. Of note, Cuapio et al. recently conducted a clinical trial observing natural killer (NK) cells in IEI/SID individuals during COVID-19 vaccination. They found a positive correlation between the frequency of NK cells at baseline and antibody titers taken about a month after vaccination (2.1 T-cell section). Therefore, further elucidation of the innate cell response to vaccination will be important in fully understanding the efficacy of COVID-19 vaccines in these populations [135]. Mortari et al. 2023 conducted a longitudinal study on their cohort of only CVID patients who received 1-4 doses of BNT162b2 and identified 4 functional groups of B cell phenotypes and clinical characteristics. With respect specifically to Bmem cells, they classified their cohort into those with both low and high affinity Bmem cells, those who only had low affinity, neither low nor high affinity Bmem cells, or non-responders (neither Bmem cells nor specific antibodies). Overall, their CVID group had significantly lower levels of low and high affinity Bmem cells compared to healthy volunteers [103]. Steiner et al. 2023, in their smaller cohort of only CVID patients, found that after a primary vaccine series, those who did seroconvert had significantly lower levels of class-switched Bmem cells [105]. Finally, Yam-Puc et al. conducted interesting analyses of the role of age-associated B cells (ABC) in the vaccine responses of those with IEI or cancer, finding that a higher baseline level of ABC is associated with lower levels of specific memory B cells and less neutralizing activity [108].
The reviewed literature highlights the important finding that for certain IEI conditions, solely relying on measurements of antibody response as a proxy for overall immunity may be underestimating the durability and efficacy of COVID-19 vaccines [76]. Given the potential confounding factors of disease, IgRT and other adjunctive therapies (see below), it will be important to devote future research initiatives to specifically evaluating the SARS-CoV-2-specific Tmem, Bmem, and innate immune cell responses to COVID-19 vaccination in IEI to further clarify their efficacy in these populations. Furthermore, it is evident that there is a paucity in information defining what response level of each individual immune correlate is required to confer protection against SARS-CoV-2. This information is urgently needed to accurately discern whether COVID-19 vaccines generate protective responses in people with IEI.
3. Impact of Adjunctive Antibody Therapies on COVID-19 Immunity
Antibodies that are generated against commonly encountered pathogens and vaccine antigens are readily present in IgRT, which reduces infectious burden in the recipient of this therapy [22,24]. Considering the ongoing pandemic, the presence of SARS-CoV-2-specific antibodies in IgRT and its capacity to protect people with IEI from infection and/or severe COVID-19 has been of great interest to patients, clinicians, and the scientific communities. Furthermore, the development and rollout of monoclonal SARS-CoV-2 antibody (mAb)-based therapeutics as preventatives and treatment options for COVID-19 has been extremely pertinent (Table 3), particularly considering the known lag between infection (and, once available, vaccination) of the general population and emergence of these antibodies in IgRT. Here, we review our current understanding regarding the content and functional capacity of SARS-CoV-2 antibody containing products, and their ability to protect against circulating SARS-CoV-2 variants.
3.1. Immunoglobulin Replacement Therapy (IgRT)
IgRT is the cornerstone of treatment for antibody deficient individuals. For over 25 years prophylactic administration either intravenously (IVIg) or subcutaneously (SCIg) has been shown to be safe and tolerable, reducing the incidence and severity of infection [21,22,136]. IgRT is a polyclonal IgG product purified from pooled human plasma (>1000 donors) containing a broad range of antibody specificities directed against commonly encountered pathogens, either because of natural infection or vaccination in the general population (Table 3) [136]. However, when SARS-CoV-2 first emerged, there was a period of multiple months before IgRT products contained IgG against SARS-CoV-2. This gap in protection was problematic due to the reliance of antibody deficient individuals on the protection this product provides to a variety of infections. It was believed that this gap in protection would compound the immune defects already predisposing immune deficient individuals to severe COVID-19 disease.
However, even when SARS-CoV-2-specific antibodies from natural infection and later vaccination in plasma donors emerged in IgRT it was unclear whether they would neutralize virus in recipients. Moreover, early insights into the protective capacity and persistence of SARS-CoV-2-specific neutralizing antibodies (nAbs) in plasma from convalescent COVID-19 patients showed that these antibodies could protect from viral transmission, and remained stable in plasma from 15 months post-infection while retaining their capacity to protect from infection [5,6,23]. This provided an avenue for treatment of at-risk individuals who contracted the virus, including those with IEI, to both limit infection and protect from severe disease. This also provided promise that when antibodies emerged in IgRT they would provide some protection against SARS-CoV-2 [23,137,138]. Despite this, it was necessary to obtain data to prove the retention of antibody function after the IgRT manufacturing process.
We reviewed 21 papers (Table S4) documenting the occurrence of SARS-CoV-2-specific antibodies in products derived from plasma donations mainly from Europe and the USA. At the time of printing information regarding SARS-CoV-2-specific antibody content in other countries including Australia was not available. Observational studies showed that products generated from pre-pandemic plasma contained antibodies cross-reactive to seasonal coronaviruses and SARS-CoV, however none demonstrated the capacity to neutralize the SARS-CoV-2 virus [139,140,141,142,143]. A study by Farcet et al. first detected SARS-CoV-2-specific antibodies in product generated from USA donated plasma in September 2020 [144], and Romero et al. documented the first positive pools from donations in Spain and the USA in July through September of the same year [145]. A later update by Farcet et al. showed that neutralization towards the ancestral WH1 strain plateaued in product between May 2021 and April 2022, with the drop in titers in European plasma being slower compared to the USA [146], likely due to changes in infections rates in these locations. Importantly, antibody titers in IgRT product steadily increased longitudinally with increasing incidence of SARS-CoV-2 infection; with 93% of IgRT lots containing SARS-CoV-2-specific antibodies by January 2021 [144,147]. A later study by Raphael et al. documented a two-fold increase in SARS-CoV-2-spike-specific IgG antibodies in product between February and March 2021. Importantly, this paper associated products with high antibodies titers with donations from countries with a high prevalence of COVID-19 infection and those with low titers produced from countries with low infection rates [148]. Additionally, while the published studies clearly document the emergence of anti-spike SARS-CoV-2 IgG levels [138,139,140,141,142,144,145,146,147,149,150,151,152], in a few cases nucleocapsid-specific IgG was also observed, resulting from natural infection of the donors prior to plasma donation [146,149,152]. This clearly demonstrates the association between geographical location, timing of plasma donations and natural infection and vaccination rates at the time of donation, with the subsequent emergence and levels of SARS-CoV-2 antibody in commercial IgRT.
Additionally, ongoing assessment of IgRT demonstrated that whilst recognition of ancestral WH1 remained high, cross-reactivity towards variants decreased incrementally with continued mutation of the RBD of SARS-CoV-2. Here, Omicron variant cross-recognition levels were lowest [153,154,155], mirrored by decreased neutralization capacity and reduced inhibition of ACE2 receptor binding [153,155]. This is in line with observations in healthy donor plasma post vaccination [53,54,55].
Neutralization capacity of antibody in IgRT to the ancestral SARS-CoV-2 strain was assessed in 11 publications, although multiple assays (Table 3) were utilized making definitive comparisons between the neutralizing capacity of products between studies difficult [137,138,139,142,143,144,146,147,149,150,156]. Despite the continuing emergence of SARS-CoV-2 variants, few of these studies assessed presence or neutralization capacity of antibodies to these variants. In one study in April 2022, all lots derived from US plasma could neutralize Omicron B.1.1.529, albeit at a 12-fold lower level compared to the ancestral strain, and a 22-fold lower level in European donated plasma [146]. A second study showed 32-fold lower Omicron neutralization compared to the ancestral strain [147]. A third study demonstrated neutralization of Omicron BA.1, BA.4/5, BQ.1.1. and XBB, with these antibodies retaining neutralization capacity in the plasma of patients receiving these products [154]. Notably, the latter study is the only one to date that tested the product administered to each patient alongside their plasma, pre and post infusion. This enabled dissection of whether detected antibodies were endogenously produced in response to vaccination, or were due to antibodies contained in IgRT. Importantly, this tracks the IgRT products capacity to retain its function within recipients and infers that these products play a role in limiting severe COVID-19 disease. Additionally, neutralization of ancestral and omicron variants was boosted after receipt of product, further supporting the importance of this treatment for protection against SARS-CoV-2 infection. This again reflects the dynamics of the timing and levels of natural infection and vaccination in different geographical locations, where plasma is donated. It also shows the decreased antibody recognition of variants, which has also been documented in studies examining antibody induced by COVID-19 vaccination [54,55]. This observed reduction in RBD-specific antibody binding to the Omicron B.1.1.529 variant was also observed in serum from convalescent COVID-19 patients, and COVID-19 vaccinated individuals [157]. These observations lead to concerns regarding the ongoing efficacy of antibody-based therapies in the treatment of COVID-19.
The progressive loss of variant recognition and reduced neutralization potency is indicative of viral evasion from antibodies. These variables make it difficult to infer the level of protection IgRT confers towards breakthrough infection, much less the clinical dose that is efficacious in preventing severe disease. These facets will require further examination to provide valuable information to clinicians regarding clinical dosing with IgRT and the clinical need for other supportive treatments including mAbs and antivirals for treatment of COVID-19.
3.2. Prophylactic Monoclonal Antibody (mAb) Therapies to Prevent Severe COVID-19 in IEI
Monoclonal antibodies were developed as a treatment option for immunocompromised individuals who were deemed highly susceptible to severe COVID-19, including individuals with IEI and those who had received solid organ or hematopoietic stem cell transplant. Up to April 2022, a dozen mAbs targeting the RBD spike protein, were rapidly developed and deployed for clinical use as a preventative against SARS-CoV-2 infection, or for treating those infected or recently exposed to SARS-CoV-2 to reduce the chance of severe disease, hospitalization and death [158].
mAbs consisted of either single (e.g., sotrovimab or bebtelovimab) or combination therapies (e.g., Evusheld) aimed at reducing or limiting infection by preventing spike protein binding to the ACE2 receptor and targeting the virus for elimination either by direct neutralization, antibody-dependent-cellular phagocytosis, antibody-dependent T-cell-mediated cytotoxicity or complement activation. Whilst antibodies targeting other domains of the spike protein or other viral proteins are in development, here we will review literature surrounding the efficacy of sotrovimab and Evusheld (Table S5) the mAb modalities most prominently used as preventatives or therapeutics for SARS-CoV-2 in Australia, the UK, and the USA. We discuss their efficacy towards the ancestral WH-1 virus and VOC, and future iterations currently in development to combat the ongoing emergence of VOC.
3.2.1. Sotrovimab
Sotrovimab (Xevudy, VUR Biotechnology GlaxoSmith Kline) is a single dose mAb administered intravenously for the treatment of SARS-CoV-2, and was first authorized for emergency use by the FDA in May 2021 (Table 3) [159]. In people treated with sotrovimab, antibody titers of the drug have been proven to be high at three months post-infusion [160]. This mAb has proven efficacy to the ancestral WH-1 strain of SARS-CoV-2 and the strains preceding Omicron, as evidenced by reduced COVID-19 hospitalization rates in individuals receiving treatment [161,162]. Separately, modelling studies have shown that sotrovimab efficacy could be predicted by the clinical stage of disease at treatment, with early disease yielding better therapeutic efficacy [163]. However, emergence of Omicron sublineages have been suggested to reduce mAb efficacy. Sotrovimab has been shown to maintain efficacy in reducing progression of breakthrough infection with Omicron BA.1 and BA.2, as evidence by reduced hospitalization and/or death rates within 28-30 days of mAb administration [161,164,165,166,167,168]. Importantly, both subvariants showed a similar risk of hospital admission [167,169]. In contrast, a separate study showed no protective effect of sotrovimab against BA.2 [170]. Here, measurement of sotrovimab-treated individuals showed that neutralization of BA.1 was 4-fold lower than for BA.2, demonstrating a dramatic loss in spike protein recognition [169]. Furthermore, in murine models, sotrovimab administration to mice expressing the ACE2 receptor showed reduced lung infection with either Omicron BA.1 and BA.2. This illustrates that despite reduced in vitro neutralization capacity, this mAb retained protective capacity against severe lung disease [171].
Continuous evolution of Omicron has been associated with ongoing immune evasion [5,6]. Here, the progressive loss of neutralization efficacy of sotrovimab has been observed starting with the Omicron BA.1 lineage, with full loss in efficacy predicted from BA.4.6 [171,172,173,174,175,176,177]. To date, Omicron BQ.1.1.10, BA.4.6.3. XBB.1.1, XBB.1.5 and CH.1.1. are the most antibody-evasive strains, with sotrovimab exhibiting reduced neutralization and binding to ACE2 resulting in increased viral transmissibility [178,179,180]. This demonstrated loss in efficacy resulted in retraction of authorization of sotrovimab use in the treatment of COVID-19 [181]. It is important to note that as for cell lines used for neutralization varied in their expression of ACE2 making comparison of neutralization data between studies difficult (Figure 3, Table 2).
3.2.2. Evusheld
Evusheld (AZD7442) is a mAb combination of cilgavimab and tixagevimab, which both bind to non-overlapping epitopes on the SARS-CoV-2 RBD causing direct neutralization of virus [182]. These antibodies, initially isolated from previously infected individuals, were engineered to extend their half-life (Table 3). Phase I trials showed that intramuscular administration of 300mg Evusheld resulted in 10-fold higher levels of neutralization 3 months post-administration, with levels remaining above those of convalescent serum at 9 months. Furthermore, antibody was detectable in nasal mucosa, a SARS-CoV-2 infection site, which might help limit infection [182]. Further to this, non-human primate models of SARS-CoV-2 showed that infection was prevented by prophylactic administration of Evusheld, while accelerated viral clearance was achieved by therapeutic administration [182]. Therefore, while this mAb combination was the only approved pre-exposure prophylaxis for COVID-19 in some countries [160,177,183], other countries including Europe and Japan approved Evusheld solely as a treatment of COVID-19. This demonstrates regulators’ dogmatic focus of not licensing COVID-19 mAbs for simultaneous prophylactic and treatment purposes [177].
Antibody levels in individuals receiving Evusheld were high 3 months post-administration, with breakthrough infections rare in recipients [160]. As of the Delta surge, increased serum antibody levels and efficient neutralization of the Delta variant was observed in all individuals receiving Evusheld [184]. In comparison, neutralization was decreased 344-fold to Omicron BA.1 and 9-fold to BA.2, with 13.8% of Evusheld recipients exhibiting breakthrough infections with these subvariants [184]. This was confirmed in vitro, where neutralization capacity was shown to be significantly reduced to Omicron BA.1, with a high rate of BA.1 breakthrough infections observed in kidney transplant recipients treated with Evusheld [183,185]. In comparison, Evusheld retains strong neutralization capacity against BA.2 in vitro for at least 8 weeks post administration [160,183]. This shows the importance of ongoing testing of mAb therapeutics to emerging variants.
What was evident for Evusheld is that cilgavimab demonstrated a better efficacy against both BA.1 and BA.2 than tixagevimab, accounting for Evusheld’s retained efficacy [173,184]. The ongoing evolution of variants has resulted in progressive loss of variant recognition by Evusheld, reducing its capacity to neutralize SARS-CoV-2 virus, and protect from infection. As of January 2023, the FDA has rescinded authorization for emergency use of Evusheld as a pre-exposure prophylaxis for COVID-19 in the US [186]. In response to the ongoing threat from variants, AstraZeneca has now registered and is recruiting for a Phase I/III study to test a new pre-exposure prophylaxis in the SUPERNOVA (Study Understanding Pre-Exposure pRophylaxis of NOVel Antibodies; NCT05648110) trial. It is noted that Phase I will investigate the therapy in healthy adults, with extension in to immunocompromised adults and adolescents in phase III [187,188].
Together, this highlights the importance of ongoing assessment of mAb recognition of emerging viral variants to determine neutralization capacity, and thus efficacy of these therapeutics.
4. Discussion and Future Directions
The SARS-CoV-2 pandemic has shed light on the role that cellular and humoral immunity play in the control of SARS-CoV-2 infection and elicitation of robust vaccination responses. Importantly, it has shown that solely assessing antibody responses to natural infection and/or COVID-19 vaccination is insufficient for monitoring the efficacy and longevity of SARS-CoV-2-specific immunity, especially in people with IEI [189], particularly as spike-specific antibody levels wane over time [5,6,23,54,55]. Additionally, IgRT and other antibody-based therapeutics confound the measurement of endogenous infection- or vaccination-induced antibodies. This highlights the urgent need for strategies to easily detect antigen-specific Bmem and Tmem responses, particularly as assessment of antibody responses traditionally used to measure vaccine responses is confounded by IgRT administration. These facets of immunity work in concert to provide robust protection against infection, severe disease, and death. Thus, measurement of their quantity, quality and longevity is paramount in assessing vaccine efficacy and their potential to protect from severe disease in both healthy individuals and those with conditions impacting immune function [167,168].
At present, assays examining these compartments are varied and only available in the research setting, making it difficult to compare findings between individual studies. Translating these assays to the diagnostic setting requires dedication of resources including funding, and further refinement and testing of methodology to ensure they are robust, standardized and high-throughput . Availability of these assays are particularly important for IEI; as the genetic and immunological complexity of these diseases make it difficult to draw clear conclusions for immune deficient individuals collectively. As such, individualized assessment is urgently needed to uncover the depth of the defect, the role of the cellular response in the absence of humoral immunity, and the level of protection that may be afforded by each correlate of immune function, thus imparting information regarding the efficacy of COVID-19 vaccination. A prime example of this is in XLA, where T-cell responses play a more prominent role due to the absence of both antibodies and B cells. Comparatively, in disorders with both a T-cell and a B-cell defect (e.g., CVID) it is crucial for immunity to be generated by both compartments to account for defects in both arms of the immune system. Future studies should focus on more than one facet of the immune system to understand and correlate responses generated in different compartments, and provide a more holistic picture of each individual patient’s response to vaccination. Additionally, analyses such as those from Ngyuen et al., bring attention to the importance of population-level factors such as social determinants of health in determining patient outcome and disease risk. Future investigations should consider adding these key factors into the assessment of IEI population response to COVID-19 infection and vaccination, to provide a more wholistic understanding of what drives disease and protection in these populations.
There is currently a paucity in information regarding the number, function, and phenotype of Bmem and Tmem generated in response to COVID-19 vaccination in people with IEI, as well as the capacity of these cells to bind and neutralize SARS-CoV-2 variants. This is important in the ever-evolving landscape of viral mutation, where even in healthy individuals, antibodies and Bmem cells exhibit reduced recognition of variants. In the context of IEI, reduced efficacy could render these populations more susceptible to severe disease and possibly death.
Finally, to date assessments of vaccine responses in IEI patients have only been published up to 3-4 doses of COVID-19 vaccine [73,79,84,87,91,93,120]. While this has provided critical information on early post-vaccination immune responses, immune deficient individuals were recommended to receive boosters every 3-6 months. Thus, at present some IEI patients have received six or more doses of vaccine compared to 4-5 in the general population. Therefore, information regarding the efficacy of these later doses, especially those with the bivalent formulations, and protein-based vaccines (e.g., NovaVax) is required to determine whether certain vaccine platforms elicit a superior immune response, and whether individuals with humoral deficiencies may benefit from a formulation such as NovaVax that specifically induces a T-cell response. This information is urgently needed to ascertain the benefit of continued vaccination and novel formulations in IEI populations. Together, this knowledge will inform future COVID-19 vaccine recommendations for people with IEI, and more widely other immunodeficient populations. Additionally, these insights might also have implications for the regimens for other vaccines currently administered (e.g., influenza) and for pathogenic threats that may emerge in the future.
In summation, there is much that is left to understand about COVID-19 vaccinations in people with IEI. These complex issues require intensive research to provide robust recommendations concerning timing between doses, vaccine formulations for individual disorders, and whether vaccines provide sufficient protection to allay the anxiety brought
by increased transmission of SARS-CoV-2. In addition, it is important to generate continued evidence of the capacity of IgRT and mAb treatments to bind and neutralize emerging variants to inform clinical care of people with IEI, both as prophylactic and treatment options for COVID-19. This ongoing pandemic is known to affect those with IEI physically, mentally, and socioeconomically. We hope the information in this review and that of ongoing and future studies benefit individuals with IEI, ultimately improving their quality-of-life post-pandemic.
Disclaimer
The opinions and assertions expressed herein are those of the author(s) and do not reflect the official policy or position of the Uniformed Services University of the Health Sciences, the National Institutes of Health, the US Department of Health and Human Services, or the US Department of Defense. References to non-Federal entities or products do not constitute or imply a Department of Defense or Uniformed Services University of the Health Sciences endorsement. This work was prepared by a military or civilian employee of the US Government as part of the individual’s official duties and therefore is in the public domain and does not possess copyright protection (public domain information may be freely distributed and copied; however, as a courtesy it is requested that the Uniformed Services University and the author be given an appropriate acknowledgement).
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Antibody responses; Table S2: Memory T-cell responses, Table S3: Bmem& Innate responses; Table S4: IgRT; Table S5: Therapeutic mAbs.
Author Contributions
Conceptualization E.S.J.E and E.E.R; Writing – original draft, E.E.R., E.C.R, E.S.J.E; Writing – review and editing, All authors.
Funding
This work was funded in part by the Division of Intramural Research, National Institute of Allergy and Infectious Diseases, National Institutes of Health, USA (E.E.R, E.C.R.), an Allergy and Immunology Foundation of Australasia (AIFA) Primary Immunodeficiency Clinical Research Grant (supported by CSL Behring (Australia), E.S.J.E), an Australasian Government Medical Research Future Fund (MRFF, Project no. 2016108, M.C.v.Z) and the Jeffrey Modell Foundation (M.C.v.Z).
Institutional Review Board Statement
Not applicable.
Acknowledgments
The authors would like to acknowledge the ongoing support and mentorship of Robyn E. O’Hehir, Luigi D. Notarangelo, Michail S. Lionakis, and Steven M. Holland.
Conflicts of Interest
The authors declare no conflicts of interest. Neither the authors nor their family members have a financial interest in any commercial product, service, or organization providing financial support for this research.
References
- Organisation, W.H. WHO Coronavirus (COVID-19) Dashboard.
- COVID-19 Data Explorer - Our World in Data. Available online: https://ourworldindata.org/explorers/coronavirus-data-explorer?zoomToSelection=true&time=2020-03-01..latest&facet=none&pickerSort=asc&pickerMetric=location&Metric=Case+fatality+rate&Interval=7-day+rolling+average&Relative+to+Population=true&Color+by+test+positivity=false&country=JPN~USA~GBR~ITA~DEU~FRA~CAN (accessed on 5 January 2023).
- Tangye, S.G. ; COVID Human Genetic Effort consortium Impact of SARS-CoV-2 Infection and COVID-19 on Patients with Inborn Errors of Immunity. J Allergy Clin Immunol 2023, 151, 818–831. [Google Scholar] [CrossRef]
- Chiu, S.S.; Hung Chan, K.; Wing Chu, K.; Kwan, S.W.; Guan, Y.; Man Poon, L.L.; Peiris, J.S.M. Human Coronavirus NL63 Infection and Other Coronavirus Infections in Children Hospitalized with Acute Respiratory Disease in Hong Kong, China. Clinical Infectious Diseases 2005, 40, 1721–1729. [Google Scholar] [CrossRef]
- Hartley, G.E.; Edwards, E.S.J.; O’Hehir, R.E.; van Zelm, M.C. New Insights into Human Immune Memory from SARS-CoV -2 Infection and Vaccination. Allergy 2022, 77, 3553–3566. [Google Scholar] [CrossRef]
- Fryer, H.A.; Hartley, G.E.; Edwards, E.S.J.; O’Hehir, R.E.; van Zelm, M.C. Humoral Immunity and B-Cell Memory in Response to SARS-CoV-2 Infection and Vaccination. Biochemical Society Transactions 2022, 50, 1643–1658. [Google Scholar] [CrossRef]
- Yi, C.; Sun, X.; Ye, J.; Ding, L.; Liu, M.; Yang, Z.; Lu, X.; Zhang, Y.; Ma, L.; Gu, W.; et al. Key Residues of the Receptor Binding Motif in the Spike Protein of SARS-CoV-2 That Interact with ACE2 and Neutralizing Antibodies. Cell Mol Immunol 2020, 17, 621–630. [Google Scholar] [CrossRef]
- Jiang, S.; Hillyer, C.; Du, L. Neutralizing Antibodies against SARS-CoV-2 and Other Human Coronaviruses. Trends in Immunology 2020, 41, 355–359. [Google Scholar] [CrossRef]
- Folegatti, P.M.; Ewer, K.J.; Aley, P.K.; Angus, B.; Becker, S.; Belij-Rammerstorfer, S.; Bellamy, D.; Bibi, S.; Bittaye, M.; Clutterbuck, E.A.; et al. Safety and Immunogenicity of the ChAdOx1 nCoV-19 Vaccine against SARS-CoV-2: A Preliminary Report of a Phase 1/2, Single-Blind, Randomised Controlled Trial. The Lancet 2020, 396, 467–478. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N Engl J Med 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Meyts, I.; Bousfiha, A.; Duff, C.; Singh, S.; Lau, Y.L.; Condino-Neto, A.; Bezrodnik, L.; Ali, A.; Adeli, M.; Drabwell, J. Primary Immunodeficiencies: A Decade of Progress and a Promising Future. Front. Immunol. 2021, 11, 625753. [Google Scholar] [CrossRef]
- Szepanowski, F.; Warnke, C.; Meyer Zu Hörste, G.; Mausberg, A.K.; Hartung, H.-P.; Kleinschnitz, C.; Stettner, M. Secondary Immunodeficiency and Risk of Infection Following Immune Therapies in Neurology. CNS Drugs 2021, 35, 1173–1188. [Google Scholar] [CrossRef]
- Pulvirenti, F.; Cinetto, F.; Milito, C.; Bonanni, L.; Pesce, A.M.; Leodori, G.; Garzi, G.; Miglionico, M.; Tabolli, S.; Quinti, I. Health-Related Quality of Life in Common Variable Immunodeficiency Italian Patients Switched to Remote Assistance During the COVID-19 Pandemic. J Allergy Clin Immunol Pract 2020, 8, 1894–1899.e2. [Google Scholar] [CrossRef] [PubMed]
- Sowers, K.L.; Galantino, M.L. Living with Primary Immunodeficiency Disease during the Covid-19 Pandemic. J Public Health (Berl.) 2022, 30, 2753–2760. [Google Scholar] [CrossRef] [PubMed]
- Care, A.G.D. of H. and A. About Coronavirus (COVID-19). Available online: https://www.health.gov.au/topics/covid-19/about (accessed on 2 January 2024).
- Tangye, S.G.; Al-Herz, W.; Bousfiha, A.; Cunningham-Rundles, C.; Franco, J.L.; Holland, S.M.; Klein, C.; Morio, T.; Oksenhendler, E.; Picard, C.; et al. Human Inborn Errors of Immunity: 2022 Update on the Classification from the International Union of Immunological Societies Expert Committee. J Clin Immunol 2022, 42, 1473–1507. [Google Scholar] [CrossRef] [PubMed]
- Edwards, E.S.J.; Bosco, J.J.; Ojaimi, S.; O’Hehir, R.E.; van Zelm, M.C. Beyond Monogenetic Rare Variants: Tackling the Low Rate of Genetic Diagnoses in Predominantly Antibody Deficiency. Cell Mol Immunol 2021, 18, 588–603. [Google Scholar] [CrossRef]
- Quinn, J.; Modell, V.; Orange, J.S.; Modell, F. Growth in Diagnosis and Treatment of Primary Immunodeficiency within the Global Jeffrey Modell Centers Network. Allergy Asthma Clin Immunol 2022, 18, 19. [Google Scholar] [CrossRef]
- Hartley, G.E.; Edwards, E.S.J.; Bosco, J.J.; Ojaimi, S.; Stirling, R.G.; Cameron, P.U.; Flanagan, K.; Plebanski, M.; Hogarth, P.M.; O’Hehir, R.E.; et al. Influenza-Specific IgG1+ Memory B-Cell Numbers Increase upon Booster Vaccination in Healthy Adults but Not in Patients with Predominantly Antibody Deficiency. Clin Transl Immunology 2020, 9, e1199. [Google Scholar] [CrossRef]
- Edwards, E.S.J.; Bosco, J.J.; Aui, P.M.; Stirling, R.G.; Cameron, P.U.; Chatelier, J.; Hore-Lacy, F.; O’Hehir, R.E.; van Zelm, M.C. Predominantly Antibody-Deficient Patients With Non-Infectious Complications Have Reduced Naive B, Treg, Th17, and Tfh17 Cells. Front Immunol 2019, 10, 2593. [Google Scholar] [CrossRef] [PubMed]
- Durandy, A.; Kracker, S.; Fischer, A. Primary Antibody Deficiencies. Nat Rev Immunol 2013, 13, 519–533. [Google Scholar] [CrossRef]
- Lucas, M.; Lee, M.; Lortan, J.; Lopez-Granados, E.; Misbah, S.; Chapel, H. Infection Outcomes in Patients with Common Variable Immunodeficiency Disorders: Relationship to Immunoglobulin Therapy over 22 Years. Journal of Allergy and Clinical Immunology 2010, 125, 1354–1360.e4. [Google Scholar] [CrossRef]
- Hartley, G.E.; Edwards, E.S.J.; Aui, P.M.; Varese, N.; Stojanovic, S.; McMahon, J.; Peleg, A.Y.; Boo, I.; Drummer, H.E.; Hogarth, P.M.; et al. Rapid Generation of Durable B Cell Memory to SARS-CoV-2 Spike and Nucleocapsid Proteins in COVID-19 and Convalescence. Sci. Immunol. 2020, 5, eabf8891. [Google Scholar] [CrossRef]
- Puel, A.; Bastard, P.; Bustamante, J.; Casanova, J.-L. Human Autoantibodies Underlying Infectious Diseases. Journal of Experimental Medicine 2022, 219, e20211387. [Google Scholar] [CrossRef] [PubMed]
- Asano, T.; Boisson, B.; Onodi, F.; Matuozzo, D.; Moncada-Velez, M.; Maglorius Renkilaraj, M.R.L.; Zhang, P.; Meertens, L.; Bolze, A.; Materna, M.; et al. X-Linked Recessive TLR7 Deficiency in ~1% of Men under 60 Years Old with Life-Threatening COVID-19. Sci. Immunol. 2021, 6, eabl4348. [Google Scholar] [CrossRef]
- Mantovani, S.; Daga, S.; Fallerini, C.; Baldassarri, M.; Benetti, E.; Picchiotti, N.; Fava, F.; Gallì, A.; Zibellini, S.; Bruttini, M.; et al. Rare Variants in Toll-like Receptor 7 Results in Functional Impairment and Downregulation of Cytokine-Mediated Signaling in COVID-19 Patients. Genes Immun 2022, 23, 51–56. [Google Scholar] [CrossRef]
- Fallerini, C.; Daga, S.; Mantovani, S.; Benetti, E.; Picchiotti, N.; Francisci, D.; Paciosi, F.; Schiaroli, E.; Baldassarri, M.; Fava, F.; et al. Association of Toll-like Receptor 7 Variants with Life-Threatening COVID-19 Disease in Males: Findings from a Nested Case-Control Study. eLife 2021, 10, e67569. [Google Scholar] [CrossRef]
- Solanich, X.; Vargas-Parra, G.; Van Der Made, C.I.; Simons, A.; Schuurs-Hoeijmakers, J.; Antolí, A.; Del Valle, J.; Rocamora-Blanch, G.; Setién, F.; Esteller, M.; et al. Genetic Screening for TLR7 Variants in Young and Previously Healthy Men With Severe COVID-19. Front. Immunol. 2021, 12, 719115. [Google Scholar] [CrossRef] [PubMed]
- Van Der Made, C.I.; Simons, A.; Schuurs-Hoeijmakers, J.; Van Den Heuvel, G.; Mantere, T.; Kersten, S.; Van Deuren, R.C.; Steehouwer, M.; Van Reijmersdal, S.V.; Jaeger, M.; et al. Presence of Genetic Variants Among Young Men With Severe COVID-19. JAMA 2020, 324, 663. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Bastard, P.; Liu, Z.; Le Pen, J.; Moncada-Velez, M.; Chen, J.; Ogishi, M.; Sabli, I.K.D.; Hodeib, S.; Korol, C.; et al. Inborn Errors of Type I IFN Immunity in Patients with Life-Threatening COVID-19. Science 2020, 370, eabd4570. [Google Scholar] [CrossRef]
- Abolhassani, H.; Landegren, N.; Bastard, P.; Materna, M.; Modaresi, M.; Du, L.; Aranda-Guillén, M.; Sardh, F.; Zuo, F.; Zhang, P.; et al. Inherited IFNAR1 Deficiency in a Child with Both Critical COVID-19 Pneumonia and Multisystem Inflammatory Syndrome. J Clin Immunol 2022, 42, 471–483. [Google Scholar] [CrossRef]
- Khanmohammadi, S.; Rezaei, N.; Khazaei, M.; Shirkani, A. A Case of Autosomal Recessive Interferon Alpha/Beta Receptor Alpha Chain (IFNAR1) Deficiency with Severe COVID-19. J Clin Immunol 2022, 42, 19–24. [Google Scholar] [CrossRef]
- Schmidt, A.; Peters, S.; Knaus, A.; Sabir, H.; Hamsen, F.; Maj, C.; Fazaal, J.; Sivalingam, S.; Savchenko, O.; Mantri, A.; et al. TBK1 and TNFRSF13B Mutations and an Autoinflammatory Disease in a Child with Lethal COVID-19. npj Genom. Med. 2021, 6, 55. [Google Scholar] [CrossRef]
- Duncan, C.J.A.; Skouboe, M.K.; Howarth, S.; Hollensen, A.K.; Chen, R.; Børresen, M.L.; Thompson, B.J.; Stremenova Spegarova, J.; Hatton, C.F.; Stæger, F.F.; et al. Life-Threatening Viral Disease in a Novel Form of Autosomal Recessive IFNAR2 Deficiency in the Arctic. Journal of Experimental Medicine 2022, 219, e20212427. [Google Scholar] [CrossRef] [PubMed]
- Platanias, L.C. Mechanisms of Type-I- and Type-II-Interferon-Mediated Signalling. Nat Rev Immunol 2005, 5, 375–386. [Google Scholar] [CrossRef]
- Zhang, Q.; Matuozzo, D.; Le Pen, J.; Lee, D.; Moens, L.; Asano, T.; Bohlen, J.; Liu, Z.; Moncada-Velez, M.; Kendir-Demirkol, Y.; et al. Recessive Inborn Errors of Type I IFN Immunity in Children with COVID-19 Pneumonia. Journal of Experimental Medicine 2022, 219, e20220131. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, A.A.; Habiballah, S.B.; LaBere, B.; Day-Lewis, M.; Elkins, M.; Al-Musa, A.; Chu, A.; Jones, J.; Fried, A.J.; McDonald, D.; et al. Rethinking Immunological Risk: A Retrospective Cohort Study of Severe SARS-Cov-2 Infections in Individuals With Congenital Immunodeficiencies. The Journal of Allergy and Clinical Immunology: In Practice 2023, 11, 3391–3399.e3. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Tracking SARS-CoV-2 Variants. Available online: https://www.who.int/activities/tracking-SARS-CoV-2-variants (accessed on 24 January 2023).
- Parra-Lucares, A.; Segura, P.; Rojas, V.; Pumarino, C.; Saint-Pierre, G.; Toro, L. Emergence of SARS-CoV-2 Variants in the World: How Could This Happen? Life 2022, 12, 194. [Google Scholar] [CrossRef] [PubMed]
- Van Egeren, D.; Novokhodko, A.; Stoddard, M.; Tran, U.; Zetter, B.; Rogers, M.S.; Joseph-McCarthy, D.; Chakravarty, A. Controlling Long-Term SARS-CoV-2 Infections Can Slow Viral Evolution and Reduce the Risk of Treatment Failure. Sci Rep 2021, 11, 22630. [Google Scholar] [CrossRef]
- Wilkinson, S.A.J.; Richter, A.; Casey, A.; Osman, H.; Mirza, J.D.; Stockton, J.; Quick, J.; Ratcliffe, L.; Sparks, N.; Cumley, N.; et al. Recurrent SARS-CoV-2 Mutations in Immunodeficient Patients. Virus Evolution 2022, 8, veac050. [Google Scholar] [CrossRef] [PubMed]
- Halfmann, P.J.; Minor, N.R.; Haddock, L.A.; Maddox, R.; Moreno, G.K.; Braun, K.M.; Baker, D.A.; Riemersa, K.K.; Prasad, A.; Alman, K.J.; et al. Evolution of a Globally Unique SARS-CoV-2 Spike E484T Monoclonal Antibody Escape Mutation in a Persistently Infected, Immunocompromised Individual; Infectious Diseases (except HIV/AIDS), 2022.
- Scherer, E.M.; Babiker, A.; Adelman, M.W.; Allman, B.; Key, A.; Kleinhenz, J.M.; Langsjoen, R.M.; Nguyen, P.-V.; Onyechi, I.; Sherman, J.D.; et al. SARS-CoV-2 Evolution and Immune Escape in Immunocompromised Patients. New England Journal of Medicine 2022, 386, 2436–2438. [Google Scholar] [CrossRef] [PubMed]
- McCallum, M.; Czudnochowski, N.; Rosen, L.E.; Zepeda, S.K.; Bowen, J.E.; Walls, A.C.; Hauser, K.; Joshi, A.; Stewart, C.; Dillen, J.R.; et al. Structural Basis of SARS-CoV-2 Omicron Immune Evasion and Receptor Engagement. Science 2022, 375, 864–868. [Google Scholar] [CrossRef]
- Enhancing Response to Omicron SARS-CoV-2 Variant. Available online: https://www.who.int/publications/m/item/enhancing-readiness-for-omicron-(b.1.1.529)-technical-brief-and-priority-actions-for-member-states (accessed on 3 July 2023).
- Panja, A.; Roy, J.; Mazumder, A.; Choudhury, S.M. Divergent Mutations of Delta and Omicron Variants: Key Players behind Differential Viral Attributes across the COVID-19 Waves. VirusDis. 2023. [Google Scholar] [CrossRef]
- Ao, D.; He, X.; Hong, W.; Wei, X. The Rapid Rise of SARS-CoV-2 Omicron Subvariants with Immune Evasion Properties: XBB.1.5 and BQ.1.1 Subvariants. MedComm 2023, 4, e239. [Google Scholar] [CrossRef] [PubMed]
- Commissioner, O. of the FDA Takes Key Action in Fight Against COVID-19 By Issuing Emergency Use Authorization for First COVID-19 Vaccine. Available online: https://www.fda.gov/news-events/press-announcements/fda-takes-key-action-fight-against-covid-19-issuing-emergency-use-authorization-first-covid-19 (accessed on 31 January 2024).
- Commissioner, O. of the FDA Approves First COVID-19 Vaccine. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-first-covid-19-vaccine (accessed on 31 January 2024).
- McIntyre, P.B.; Aggarwal, R.; Jani, I.; Jawad, J.; Kochhar, S.; MacDonald, N.; Madhi, S.A.; Mohsni, E.; Mulholland, K.; Neuzil, K.M.; et al. COVID-19 Vaccine Strategies Must Focus on Severe Disease and Global Equity. The Lancet 2022, 399, 406–410. [Google Scholar] [CrossRef] [PubMed]
- Chirico, F.; Teixeira Da Silva, J.; Tsigaris, P.; Sharun, K. Safety & Effectiveness of COVID-19 Vaccines: A Narrative Review. Indian J Med Res 2022, 155, 91. [Google Scholar] [CrossRef] [PubMed]
- Commissioner, O. of the Coronavirus (COVID-19) Update: FDA Limits Use of Janssen COVID-19 Vaccine to Certain Individuals. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-limits-use-janssen-covid-19-vaccine-certain-individuals (accessed on 15 February 2023).
- Hartley, G.E.; Fryer, H.A.; Gill, P.A.; Boo, I.; Bornheimer, S.J.; Hogarth, P.M.; Drummer, H.E.; O’Hehir, R.E.; Edwards, E.S.J.; Van Zelm, M.C. Third Dose COVID-19 mRNA Vaccine Enhances IgG4 Isotype Switching and Recognition of Omicron Subvariants by Memory B Cells after mRNA but Not Adenovirus Priming; Immunology, 2023.
- Hartley, G.E.; Edwards, E.S.J.; Varese, N.; Boo, I.; Aui, P.M.; Bornheimer, S.J.; Hogarth, P.M.; Drummer, H.E.; O’Hehir, R.E.; van Zelm, M.C. The Second COVID -19 mRNA Vaccine Dose Enhances the Capacity of Spike-specific Memory B Cells to Bind Omicron BA.2. Allergy 2022, all.15624. [Google Scholar] [CrossRef]
- Fryer, H.A.; Hartley, G.E.; Edwards, E.S.J.; Varese, N.; Boo, I.; Bornheimer, S.J.; Hogarth, P.M.; Drummer, H.E.; O’Hehir, R.E.; Van Zelm, M.C. COVID-19 Adenoviral Vector Vaccination Elicits a Robust Memory B Cell Response with the Capacity to Recognize Omicron BA.2 and BA.5 Variants. J Clin Immunol 2023. [Google Scholar] [CrossRef] [PubMed]
- Ikegame, S.; Siddiquey, M.N.A.; Hung, C.-T.; Haas, G.; Brambilla, L.; Oguntuyo, K.Y.; Kowdle, S.; Chiu, H.-P.; Stevens, C.S.; Vilardo, A.E.; et al. Neutralizing Activity of Sputnik V Vaccine Sera against SARS-CoV-2 Variants. Nat Commun 2021, 12, 4598. [Google Scholar] [CrossRef] [PubMed]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing Antibody Levels Are Highly Predictive of Immune Protection from Symptomatic SARS-CoV-2 Infection. Nat Med 2021, 27, 1205–1211. [Google Scholar] [CrossRef] [PubMed]
- Marta, R.A.; Nakamura, G.E.K.; De Matos Aquino, B.; Bignardi, P.R. COVID-19 Vaccines: Update of the Vaccines in Use and under Development. Vacunas 2022, 23, S88–S102. [Google Scholar] [CrossRef] [PubMed]
- Comirnaty® COVID-19 Vaccines (COVID-19 Vaccines) | Pfizer Medical Information - Australia. Available online: https://www.pfizermedicalinformation.com.au/en-au/pfizer-biontech-covid-19-vaccine (accessed on 3 July 2023).
- Statement on the Antigen Composition of COVID-19 Vaccines. Available online: https://www.who.int/news/item/13-12-2023-statement-on-the-antigen-composition-of-covid-19-vaccines (accessed on 31 January 2024).
- Care, A.G.D. of H. and A. ATAGI Recommendations on Use of the Moderna and Pfizer Monovalent Omicron XBB.1.5 COVID-19 Vaccines. Available online: https://www.health.gov.au/news/atagi-recommendations-on-use-of-the-moderna-and-pfizer-monovalent-omicron-xbb15-covid-19-vaccines (accessed on 31 January 2024).
- Edwards, E.; Quinn, K. Why Is a Third COVID-19 Vaccine Dose Important for People Who Are Immunocompromised? Available online: http://theconversation.com/why-is-a-third-covid-19-vaccine-dose-important-for-people-who-are-immunocompromised-166569 (accessed on 3 July 2023).
- Gernez, Y.; Murugesan, K.; Cortales, C.R.; Banaei, N.; Hoyte, L.; Pinsky, B.A.; Lewis, D.B.; Pham, M.N. Immunogenicity of a Third COVID-19 Messenger RNA Vaccine Dose in Primary Immunodeficiency Disorder Patients with Functional B-Cell Defects. The Journal of Allergy and Clinical Immunology: In Practice 2022, 10, 1385–1388.e2. [Google Scholar] [CrossRef]
- Care, A.G.D. of H. and A. ATAGI Recommendations on the Use of a Third Primary Dose of COVID-19 Vaccine in Individuals Who Are Severely Immunocompromised. Available online: https://www.health.gov.au/resources/publications/atagi-recommendations-on-the-use-of-a-third-primary-dose-of-covid-19-vaccine-in-individuals-who-are-severely-immunocompromised?language=en (accessed on 3 July 2023).
- Commissioner, O. of the Coronavirus (COVID-19) Update: FDA Authorizes Additional Vaccine Dose for Certain Immunocompromised Individuals. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-additional-vaccine-dose-certain-immunocompromised (accessed on 4 July 2023).
- Joint Committee on Vaccination and Immunisation (JCVI) Advice on Third Primary Dose Vaccination. Available online: https://www.gov.uk/government/publications/third-primary-covid-19-vaccine-dose-for-people-who-are-immunosuppressed-jcvi-advice/joint-committee-on-vaccination-and-immunisation-jcvi-advice-on-third-primary-dose-vaccination (accessed on 3 July 2023).
- Mohammed, I.; Nauman, A.; Paul, P.; Ganesan, S.; Chen, K.-H.; Jalil, S.M.S.; Jaouni, S.H.; Kawas, H.; Khan, W.A.; Vattoth, A.L.; et al. The Efficacy and Effectiveness of the COVID-19 Vaccines in Reducing Infection, Severity, Hospitalization, and Mortality: A Systematic Review. Human Vaccines & Immunotherapeutics 2022, 18, 2027160. [Google Scholar] [CrossRef]
- DeSantis, S.M.; Yaseen, A.; Hao, T.; León-Novelo, L.; Talebi, Y.; Valerio-Shewmaker, M.A.; Pinzon Gomez, C.L.; Messiah, S.E.; Kohl, H.W.; Kelder, S.H.; et al. Incidence and Predictors of Breakthrough and Severe Breakthrough Infections of SARS-CoV-2 After Primary Series Vaccination in Adults: A Population-Based Survey of 22 575 Participants. The Journal of Infectious Diseases 2023, 227, 1164–1172. [Google Scholar] [CrossRef]
- Arroyo-Sánchez, D.; Cabrera-Marante, O.; Laguna-Goya, R.; Almendro-Vázquez, P.; Carretero, O.; Gil-Etayo, F.J.; Suàrez-Fernández, P.; Pérez-Romero, P.; Rodríguez de Frías, E.; Serrano, A.; et al. Immunogenicity of Anti-SARS-CoV-2 Vaccines in Common Variable Immunodeficiency. J Clin Immunol 2022, 42, 240–252. [Google Scholar] [CrossRef]
- Hagin, D.; Freund, T.; Navon, M.; Halperin, T.; Adir, D.; Marom, R.; Levi, I.; Benor, S.; Alcalay, Y.; Freund, N.T. Immunogenicity of Pfizer-BioNTech COVID-19 Vaccine in Patients with Inborn Errors of Immunity. J Allergy Clin Immunol 2021, 148, 739–749. [Google Scholar] [CrossRef]
- van Leeuwen, L.P.M.; GeurtsvanKessel, C.H.; Ellerbroek, P.M.; de Bree, G.J.; Potjewijd, J.; Rutgers, A.; Jolink, H.; van de Veerdonk, F.; van Gorp, E.C.M.; de Wilt, F.; et al. Immunogenicity of the mRNA-1273 COVID-19 Vaccine in Adult Patients with Inborn Errors of Immunity. J Allergy Clin Immunol 2022, 149, 1949–1957. [Google Scholar] [CrossRef]
- Fernandez Salinas, A.; Piano Mortari, E.; Terreri, S.; Milito, C.; Zaffina, S.; Perno, C.F.; Locatelli, F.; Quinti, I.; Carsetti, R. Impaired Memory B-Cell Response to the Pfizer-BioNTech COVID-19 Vaccine in Patients with Common Variable Immunodeficiency. J Allergy Clin Immunol 2022, 149, 76–77. [Google Scholar] [CrossRef]
- Shields, A.M.; Faustini, S.E.; Hill, H.J.; Al-Taei, S.; Tanner, C.; Ashford, F.; Workman, S.; Moreira, F.; Verma, N.; Wagg, H.; et al. Increased Seroprevalence and Improved Antibody Responses Following Third Primary SARS-CoV-2 Immunisation: An Update From the COV-AD Study. Front Immunol 2022, 13, 912571. [Google Scholar] [CrossRef]
- Zendt, M.; Bustos Carrillo, F.A.; Kelly, S.; Saturday, T.; DeGrange, M.; Ginigeme, A.; Wu, L.; Callier, V.; Ortega-Villa, A.; Faust, M.; et al. Characterization of the Antispike IgG Immune Response to COVID-19 Vaccines in People with a Wide Variety of Immunodeficiencies. Science Advances 2023, 9, eadh3150. [Google Scholar] [CrossRef]
- Hlongwa, L.; Peter, J.; Mayne, E. Value of Diagnostic Vaccination in Diagnosis of Humoral Inborn Errors of Immunity. Human Immunology 2023, 84, 337–341. [Google Scholar] [CrossRef]
- Bergman, P.; Wullimann, D.; Gao, Y.; Wahren Borgström, E.; Norlin, A.-C.; Lind Enoksson, S.; Aleman, S.; Ljunggren, H.-G.; Buggert, M.; Smith, C.I.E. Elevated CD21low B Cell Frequency Is a Marker of Poor Immunity to Pfizer-BioNTech BNT162b2 mRNA Vaccine Against SARS-CoV-2 in Patients with Common Variable Immunodeficiency. J Clin Immunol 2022, 42, 716–727. [Google Scholar] [CrossRef]
- Amodio, D.; Ruggiero, A.; Sgrulletti, M.; Pighi, C.; Cotugno, N.; Medri, C.; Morrocchi, E.; Colagrossi, L.; Russo, C.; Zaffina, S.; et al. Humoral and Cellular Response Following Vaccination With the BNT162b2 mRNA COVID-19 Vaccine in Patients Affected by Primary Immunodeficiencies. Front Immunol 2021, 12, 727850. [Google Scholar] [CrossRef]
- Bitzenhofer, M.; Suter-Riniker, F.; Moor, M.B.; Sidler, D.; Horn, M.P.; Gschwend, A.; Staehelin, C.; Rauch, A.; Helbling, A.; Jörg, L. Humoral Response to mRNA Vaccines against SARS-CoV-2 in Patients with Humoral Immunodeficiency Disease. PLoS One 2022, 17, e0268780. [Google Scholar] [CrossRef]
- Barmettler, S.; DiGiacomo, D.V.; Yang, N.J.; Lam, T.; Naranbhai, V.; Dighe, A.S.; Burke, K.E.; Blumenthal, K.G.; Ling, M.; Hesterberg, P.E.; et al. Response to Severe Acute Respiratory Syndrome Coronavirus 2 Initial Series and Additional Dose Vaccine in Patients With Predominant Antibody Deficiency. J Allergy Clin Immunol Pract 2022, 10, 1622–1634.e4. [Google Scholar] [CrossRef] [PubMed]
- Bergman, P.; Blennow, O.; Hansson, L.; Mielke, S.; Nowak, P.; Chen, P.; Söderdahl, G.; Österborg, A.; Smith, C.I.E.; Wullimann, D.; et al. Safety and Efficacy of the mRNA BNT162b2 Vaccine against SARS-CoV-2 in Five Groups of Immunocompromised Patients and Healthy Controls in a Prospective Open-Label Clinical Trial. EBioMedicine 2021, 74, 103705. [Google Scholar] [CrossRef]
- Salinas, A.F.; Mortari, E.P.; Terreri, S.; Quintarelli, C.; Pulvirenti, F.; Di Cecca, S.; Guercio, M.; Milito, C.; Bonanni, L.; Auria, S.; et al. SARS-CoV-2 Vaccine Induced Atypical Immune Responses in Antibody Defects: Everybody Does Their Best. J Clin Immunol 2021, 41, 1709–1722. [Google Scholar] [CrossRef] [PubMed]
- Abo-Helo, N.; Muhammad, E.; Ghaben-Amara, S.; Cohen, S. Specific Antibody Response of 14 Patients with Common Variable Immunodeficiency to 3 BNT162b2 Messenger RNA Coronavirus Disease 2019 Vaccinations. Ann Allergy Asthma Immunol 2022, 129, 108–109. [Google Scholar] [CrossRef]
- Erra, L.; Uriarte, I.; Colado, A.; Paolini, M.V.; Seminario, G.; Fernández, J.B.; Tau, L.; Bernatowiez, J.; Moreira, I.; Vishnopolska, S.; et al. COVID-19 Vaccination Responses with Different Vaccine Platforms in Patients with Inborn Errors of Immunity. J. Clin. Immunol. 2022, 43, 271–285. [Google Scholar] [CrossRef]
- Nielsen, B.U.; Drabe, C.H.; Barnkob, M.B.; Johansen, I.S.; Hansen, A.K.K.; Nilsson, A.C.; Rasmussen, L.D. Antibody Response Following the Third and Fourth SARS-CoV-2 Vaccine Dose in Individuals with Common Variable Immunodeficiency. Front. Immunol. 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Antolí, A.; Rocamora-Blanch, G.; Framil, M.; Mas-Bosch, V.; Navarro, S.; Bermudez, C.; Martinez-Yelamos, S.; Dopico, E.; Calatayud, L.; Garcia-Muñoz, N.; et al. Evaluation of Humoral and Cellular Immune Responses to the SARS-CoV-2 Vaccine in Patients With Common Variable Immunodeficiency Phenotype and Patient Receiving B-Cell Depletion Therapy. Front Immunol 2022, 13, 895209. [Google Scholar] [CrossRef]
- Pham, M.N.; Murugesan, K.; Banaei, N.; Pinsky, B.A.; Tang, M.; Hoyte, E.; Lewis, D.B.; Gernez, Y. Immunogenicity and Tolerability of COVID-19 Messenger RNA Vaccines in Primary Immunodeficiency Patients with Functional B-Cell Defects. J Allergy Clin Immunol 2022, 149, 907–911. [Google Scholar] [CrossRef]
- Lin, F.J.; Doss, A.M.A.; Davis-Adams, H.G.; Adams, L.J.; Hanson, C.H.; VanBlargan, L.A.; Liang, C.-Y.; Chen, R.E.; Monroy, J.M.; Wedner, H.J.; et al. SARS-CoV-2 Booster Vaccination Rescues Attenuated IgG1 Memory B Cell Response in Primary Antibody Deficiency Patients. Front. Immunol. 2022, 13. [Google Scholar] [CrossRef]
- Abo-Helo, N.; Muhammad, E.; Ghaben-Amara, S.; Panasoff, J.; Cohen, S. Specific Antibody Response of Patients with Common Variable Immunodeficiency to BNT162b2 Coronavirus Disease 2019 Vaccination. Ann Allergy Asthma Immunol 2021, 127, 501–503. [Google Scholar] [CrossRef]
- Liu, L.; Iketani, S.; Guo, Y.; Chan, J.F.-W.; Wang, M.; Liu, L.; Luo, Y.; Chu, H.; Huang, Y.; Nair, M.S.; et al. Striking Antibody Evasion Manifested by the Omicron Variant of SARS-CoV-2. Nature 2022, 602, 676–681. [Google Scholar] [CrossRef]
- Jalil, M.; Rowane, M.; Rajan, J.; Hostoffer, R. Successful Anti-SARS-CoV-2 Spike Protein Antibody Response to Vaccination in MAGT1 Deficiency. Allergy�Rhinol (Providence) 2021, 12, 215265672110562. [Google Scholar] [CrossRef]
- Pulvirenti, F.; Di Cecca, S.; Sinibaldi, M.; Piano Mortari, E.; Terreri, S.; Albano, C.; Guercio, M.; Sculco, E.; Milito, C.; Ferrari, S.; et al. T-Cell Defects Associated to Lack of Spike-Specific Antibodies after BNT162b2 Full Immunization Followed by a Booster Dose in Patients with Common Variable Immune Deficiencies. Cells 2022, 11, 1918. [Google Scholar] [CrossRef]
- Sheward, D.J.; Kim, C.; Ehling, R.A.; Pankow, A.; Dopico, X.C.; Martin, D.; Reddy, S.; Dillner, J.; Karlsson Hedestam, G.B.; Albert, J.; et al. Variable Loss of Antibody Potency against SARS-CoV-2 B.1.1.529 (Omicron); Immunology, 2021.
- Leung, D.; Mu, X.; Duque, J.S.R.; Cheng, S.M.S.; Wang, M.; Zhang, W.; Zhang, Y.; Tam, I.Y.S.; Lee, T.S.S.; Lam, J.H.Y.; et al. Safety and Immunogenicity of 3 Doses of BNT162b2 and CoronaVac in Children and Adults with Inborn Errors of Immunity. Front. Immunol. 2022, 13. [Google Scholar] [CrossRef]
- Illes, P.; Csomos, K.; Ujhazi, B.; Dasso, J.; Nagy, B.; Alas, E.; Gordon, S.; Timothy, P.; Miranda, M.A.; Sullivan, S.; et al. The Humoral Immune Response To SARS-CoV-2 Infection And/or Immunization in Immunocompromised Versus Immunocompetent Individuals. J. Allergy Clin. Immunol. 2022, 149, AB21. [Google Scholar] [CrossRef]
- Obeid, M.; Suffiotti, M.; Pellaton, C.; Bouchaab, H.; Cairoli, A.; Salvadé, V.; Stevenel, C.; Hottinger, R.; Pythoud, C.; Coutechier, L.; et al. Humoral Responses Against Variants of Concern by COVID-19 mRNA Vaccines in Immunocompromised Patients. JAMA Oncology 2022, 8, e220446. [Google Scholar] [CrossRef] [PubMed]
- Lucane, Z.; Slisere, B.; Ozola, L.; Rots, D.; Papirte, S.; Vilne, B.; Gailite, L.; Kurjane, N. Long-Term Immunological Memory of SARS-CoV-2 Is Present in Patients with Primary Antibody Deficiencies for up to a Year after Vaccination. Vaccines 2023, 11, 354. [Google Scholar] [CrossRef]
- Pulvirenti, F.; Fernandez Salinas, A.; Milito, C.; Terreri, S.; Piano Mortari, E.; Quintarelli, C.; Di Cecca, S.; Lagnese, G.; Punziano, A.; Guercio, M.; et al. B Cell Response Induced by SARS-CoV-2 Infection Is Boosted by the BNT162b2 Vaccine in Primary Antibody Deficiencies. Cells 2021, 10, 2915. [Google Scholar] [CrossRef]
- Shields, A.M.; Faustini, S.E.; Hill, H.J.; Al-Taei, S.; Tanner, C.; Ashford, F.; Workman, S.; Moreira, F.; Verma, N.; Wagg, H.; et al. SARS-CoV-2 Vaccine Responses in Individuals with Antibody Deficiency: Findings from the COV-AD Study. J Clin Immunol 2022. [Google Scholar] [CrossRef]
- Oyaert, M.; De Scheerder, M.-A.; Van Herrewege, S.; Laureys, G.; Van Assche, S.; Cambron, M.; Naesens, L.; Hoste, L.; Claes, K.; Haerynck, F.; et al. Evaluation of Humoral and Cellular Responses in SARS-CoV-2 mRNA Vaccinated Immunocompromised Patients. Front Immunol 2022, 13, 858399. [Google Scholar] [CrossRef]
- Sauerwein, K.M.T.; Geier, C.B.; Stemberger, R.F.; Akyaman, H.; Illes, P.; Fischer, M.B.; Eibl, M.M.; Walter, J.E.; Wolf, H.M. Antigen-Specific CD4+ T-Cell Activation in Primary Antibody Deficiency After BNT162b2 mRNA COVID-19 Vaccination. Front Immunol 2022, 13, 827048. [Google Scholar] [CrossRef]
- Murray, C.E.; O’Brien, C.; Alamin, S.; Phelan, S.H.; Argue, R.; Kiersey, R.; Gardiner, M.; Naughton, A.; Keogh, E.; Holmes, P.; et al. Cellular and Humoral Immunogenicity of the COVID-19 Vaccine and COVID-19 Disease Severity in Individuals with Immunodeficiency. Front Immunol 2023, 14, 1131604. [Google Scholar] [CrossRef]
- Hurme, A.; Jalkanen, P.; Marttila-Vaara, M.; Heroum, J.; Jokinen, H.; Vara, S.; Liedes, O.; Lempainen, J.; Melin, M.; Julkunen, I.; et al. T Cell Immunity Following COVID-19 Vaccination in Adult Patients with Primary Antibody Deficiency – a 22-Month Follow-Up. Front Immunol 2023, 14, 1146500. [Google Scholar] [CrossRef]
- Piano Mortari, E.; Pulvirenti, F.; Marcellini, V.; Terreri, S.; Salinas, A.F.; Ferrari, S.; Di Napoli, G.; Guadagnolo, D.; Sculco, E.; Albano, C.; et al. Functional CVIDs Phenotype Clusters Identified by the Integration of Immune Parameters after BNT162b2 Boosters. Front Immunol 2023, 14, 1194225. [Google Scholar] [CrossRef] [PubMed]
- La Civita, E.; Zannella, C.; Brusa, S.; Romano, P.; Schettino, E.; Salemi, F.; Carrano, R.; Gentile, L.; Punziano, A.; Lagnese, G.; et al. BNT162b2 Elicited an Efficient Cell-Mediated Response against SARS-CoV-2 in Kidney Transplant Recipients and Common Variable Immunodeficiency Patients. Viruses 2023, 15, 1659. [Google Scholar] [CrossRef]
- Steiner, S.; Schwarz, T.; Corman, V.M.; Jeworowski, L.M.; Bauer, S.; Drosten, C.; Scheibenbogen, C.; Hanitsch, L.G. Impaired B Cell Recall Memory and Reduced Antibody Avidity but Robust T Cell Response in CVID Patients After COVID-19 Vaccination. J Clin Immunol 2023, 43, 869–881. [Google Scholar] [CrossRef]
- Mizera, D.; Dziedzic, R.; Drynda, A.; Gradzikiewicz, A.; Jakieła, B.; Celińska-Löwenhoff, M.; Padjas, A.; Matyja-Bednarczyk, A.; Zaręba, L.; Bazan-Socha, S. Cellular Immune Response to SARS-CoV-2 in Patients with Primary Antibody Deficiencies. Front Immunol 2023, 14, 1275892. [Google Scholar] [CrossRef]
- Nourizadeh, M.; Feizabadi, E.; Mirmoghtadaei, M.; Mohammadi, A.; Fazlollahi, M.R.; Moradi, L.; Pourpak, Z. Antibody Production after COVID-19 Vaccination in Patients with Inborn Errors of Immunity. Iranian Journal of Immunology 2023, 20, 400–409. [Google Scholar] [CrossRef]
- Yam-Puc, J.C.; Hosseini, Z.; Horner, E.C.; Gerber, P.P.; Beristain-Covarrubias, N.; Hughes, R.; Lulla, A.; Rust, M.; Boston, R.; Ali, M.; et al. Age-Associated B Cells Predict Impaired Humoral Immunity after COVID-19 Vaccination in Patients Receiving Immune Checkpoint Blockade. Nat Commun 2023, 14, 3292. [Google Scholar] [CrossRef]
- Tandon, M.; DiGiacomo, D.V.; Zhou, B.; Hesterberg, P.; Rosenberg, C.E.; Barmettler, S.; Farmer, J.R. Response to SARS-CoV-2 Initial Series and Additional Dose Vaccine in Pediatric Patients with Predominantly Antibody Deficiency. Front Immunol 2023, 14, 1217718. [Google Scholar] [CrossRef]
- Shin, J.J.; Par-Young, J.; Unlu, S.; McNamara, A.; Park, H.-J.; Shin, M.S.; Gee, R.J.; Doyle, H.; Afinogenova, Y.; Zidan, E.; et al. Defining Clinical and Immunological Predictors of Poor Immune Responses to COVID-19 mRNA Vaccines in Patients with Primary Antibody Deficiency. J Clin Immunol 2022. [Google Scholar] [CrossRef]
- Quinti, I.; Locatelli, F.; Carsetti, R. The Immune Response to SARS-CoV-2 Vaccination: Insights Learned From Adult Patients With Common Variable Immune Deficiency. Front Immunol 2021, 12, 815404. [Google Scholar] [CrossRef]
- Bloomfield, M.; Parackova, Z.; Hanzlikova, J.; Lastovicka, J.; Sediva, A. Immunogenicity and Safety of COVID-19 mRNA Vaccine in STAT1 GOF Patients. J Clin Immunol 2022, 42, 266–269. [Google Scholar] [CrossRef]
- Timothy, P.; Illes, P.; Ujhazi, B.; Gordon, S.; Nagy, B.; Alas, E.; Sullivan, S.; Miranda, M.A.; Duff, C.; Farmer, J.; et al. Effects Of The COVID-19 Pandemic On A Group Of Patients With Pathogenic Variant of Cytotoxic T-Lymphocyte Associated Protein 4 (CTLA-4) in a Tertiary Center in Florida. J. Allergy Clin. Immunol. 2022, 149, AB28. [Google Scholar] [CrossRef]
- Squire, J.D.; Joshi, A.Y. Response to mRNA COVID-19 Vaccination in Three XLA Patients. Vaccine 2022. [Google Scholar] [CrossRef]
- Sette, A.; Crotty, S. Adaptive Immunity to SARS-CoV-2 and COVID-19. Cell 2021, 184, 861–880. [Google Scholar] [CrossRef]
- Zimmerman, O.; Altman Doss, A.M.; Kaplonek, P.; Liang, C.-Y.; VanBlargan, L.A.; Chen, R.E.; Monroy, J.M.; Wedner, H.J.; Kulczycki, A.; Mantia, T.L.; et al. mRNA Vaccine Boosting Enhances Antibody Responses against SARS-CoV-2 Omicron Variant in Individuals with Antibody Deficiency Syndromes. Cell Reports Medicine 2022, 3, 100653. [Google Scholar] [CrossRef]
- Abella, E.; Trigueros, M.; Pradenas, E.; Muñoz-Lopez, F.; Garcia-Pallarols, F.; Ben Azaiz Ben Lahsen, R.; Trinité, B.; Urrea, V.; Marfil, S.; Rovirosa, C.; et al. Efficacy of SARS-CoV-2 Vaccination in Patients with Monoclonal Gammopathies: A Cross Sectional Study. Life Sci Alliance 2022, 5, e202201479. [Google Scholar] [CrossRef]
- Van Leeuwen, L.P.M.; Grobben, M.; GeurtsvanKessel, C.H.; Ellerbroek, P.M.; De Bree, G.J.; Potjewijd, J.; Rutgers, A.; Jolink, H.; Van De Veerdonk, F.L.; Van Gils, M.J.; et al. Immune Responses 6 Months After mRNA-1273 COVID-19 Vaccination and the Effect of a Third Vaccination in Patients with Inborn Errors of Immunity. J Clin Immunol 2023, 43, 1104–1117. [Google Scholar] [CrossRef]
- Karabiber, E.; Atik, Ö.; Tepetam, F.M.; Ergan, B.; İlki, A.; Karakoç Aydıner, E.; Özen, A.; Özyer, F.; Barış, S. Clinical and Immunological Outcomes of SARS-CoV-2 Infection in Patients with Inborn Errors of Immunity Receiving Different Brands and Doses of COVID-19 Vaccines. Tuberk Toraks 2023, 71, 236–249. [Google Scholar] [CrossRef] [PubMed]
- Goda, V.; Kriván, G.; Kulcsár, A.; Gönczi, M.; Tasnády, S.; Matula, Z.; Nagy, G.; Bekő, G.; Horváth, M.; Uher, F.; et al. Specific Antibody and the T-Cell Response Elicited by BNT162b2 Boosting After Two ChAdOx1 nCoV-19 in Common Variable Immunodeficiency. Front Immunol 2022, 13, 907125. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Agrawal, S.; Sandoval, A.; Su, H.; Tran, M.; Demirdag, Y. SARS-CoV-2-Specific and Functional Cytotoxic CD8 Cells in Primary Antibody Deficiency: Natural Infection and Response to Vaccine. J Clin Immunol 2022. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Chandrashekar, A.; Sellers, D.; Barrett, J.; Jacob-Dolan, C.; Lifton, M.; McMahan, K.; Sciacca, M.; VanWyk, H.; Wu, C.; et al. Vaccines Elicit Highly Conserved Cellular Immunity to SARS-CoV-2 Omicron. Nature 2022, 603, 493–496. [Google Scholar] [CrossRef] [PubMed]
- Barrios, Y.; Franco, A.; Alava-Cruz, C.; Cuesta-Martin, R.; Camara, C.; Matheu, V. Easy Approach to Detect Cell Immunity to COVID Vaccines in Common Variable Immunodeficiency Patients. Allergol Immunopathol (Madr) 2022, 50, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Cai, C.; Wullimann, D.; Niessl, J.; Rivera-Ballesteros, O.; Chen, P.; Lange, J.; Cuapio, A.; Blennow, O.; Hansson, L.; et al. Immunodeficiency Syndromes Differentially Impact the Functional Profile of SARS-CoV-2-Specific T Cells Elicited by mRNA Vaccination. Immunity 2022, S1074-7613(22)00338-7. [Google Scholar] [CrossRef] [PubMed]
- Göschl, L.; Mrak, D.; Grabmeier-Pfistershammer, K.; Stiasny, K.; Haslacher, H.; Schneider, L.; Deimel, T.; Kartnig, F.; Tobudic, S.; Aletaha, D.; et al. Reactogenicity and Immunogenicity of the Second COVID-19 Vaccination in Patients with Inborn Errors of Immunity or Mannan-Binding Lectin Deficiency. Front. Immunol. 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Steiner, S.; Schwarz, T.; Corman, V.M.; Gebert, L.; Kleinschmidt, M.C.; Wald, A.; Gläser, S.; Kruse, J.M.; Zickler, D.; Peric, A.; et al. SARS-CoV-2 T Cell Response in Severe and Fatal COVID-19 in Primary Antibody Deficiency Patients Without Specific Humoral Immunity. Front. Immunol. 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Ameratunga, R.; Woon, S.-T.; Jordan, A.; Longhurst, H.; Leung, E.; Steele, R.; Lehnert, K.; Snell, R.; Brooks, A.E.S. Perspective: Diagnostic Laboratories Should Urgently Develop T Cell Assays for SARS-CoV-2 Infection. Expert Review of Clinical Immunology 2021, 17, 421–430. [Google Scholar] [CrossRef]
- Ameratunga, R.; Woon, S.-T.; Steele, R.; Lehnert, K.; Leung, E.; Edwards, E.S.J.; Brooks, A.E.S. Common Variable Immunodeficiency Disorders as a Model for Assessing COVID-19 Vaccine Responses in Immunocompromised Patients. Front Immunol 2021, 12, 798389. [Google Scholar] [CrossRef]
- Labrador-Horrillo, M.; Franco-Jarava, C.; Garcia-Prat, M.; Parra-Martínez, A.; Antolín, M.; Salgado-Perandrés, S.; Aguiló-Cucurull, A.; Martinez-Gallo, M.; Colobran, R. Case Report: X-Linked SASH3 Deficiency Presenting as a Common Variable Immunodeficiency. Front. Immunol. 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, H.; Durkee-Shock, J.; Jensen-Wachspress, M.; Kankate, V.; Lang, H.; Lazarski, C.A.; Keswani, A.; Webber, K.; Montgomery-Recht, K.; Walkiewicz, M.; et al. Robust Antibody and T Cell Responses to SARS-CoV-2 in Patients with Antibody Deficiency. 2021. [Google Scholar] [CrossRef]
- Reynolds, C.J.; Pade, C.; Gibbons, J.M.; Butler, D.K.; Otter, A.D.; Menacho, K.; Fontana, M.; Smit, A.; Sackville-West, J.E.; Cutino-Moguel, T.; et al. Prior SARS-CoV-2 Infection Rescues B and T Cell Responses to Variants after First Vaccine Dose. Science 2021, 372, 1418–1423. [Google Scholar] [CrossRef]
- Braun, J.; Loyal, L.; Frentsch, M.; Wendisch, D.; Georg, P.; Kurth, F.; Hippenstiel, S.; Dingeldey, M.; Kruse, B.; Fauchere, F.; et al. SARS-CoV-2-Reactive T Cells in Healthy Donors and Patients with COVID-19. Nature 2020, 587, 270–274. [Google Scholar] [CrossRef]
- Barouch, D.H.; Stephenson, K.E.; Sadoff, J.; Yu, J.; Chang, A.; Gebre, M.; McMahan, K.; Liu, J.; Chandrashekar, A.; Patel, S.; et al. Durable Humoral and Cellular Immune Responses 8 Months after Ad26.COV2.S Vaccination. N Engl J Med 2021, 385, 951–953. [Google Scholar] [CrossRef]
- Sanchez, D.; Radigan, L.; Cunningham-Rundles, C. Assessing SARS-CoV-2 Antigen Specific T-Cell Responses After mRNA Vaccination and/or Omicron Variant COVID-19 Infection in Patients with Primary Humoral Immunodeficiencies. Journal of Allergy and Clinical Immunology 2023, 151, AB195. [Google Scholar] [CrossRef]
- Cuapio, A.; Boulouis, C.; Filipovic, I.; Wullimann, D.; Kammann, T.; Parrot, T.; Chen, P.; Akber, M.; Gao, Y.; Hammer, Q.; et al. NK Cell Frequencies, Function and Correlates to Vaccine Outcome in BNT162b2 mRNA Anti-SARS-CoV-2 Vaccinated Healthy and Immunocompromised Individuals. Mol Med 2022, 28, 20. [Google Scholar] [CrossRef] [PubMed]
- Orange, J.; Hossny, E.; Weiler, C.; Ballow, M.; Berger, M.; Bonilla, F.; Buckley, R.; Chinen, J.; Elgamal, Y.; Mazer, B. Use of Intravenous Immunoglobulin in Human Disease: A Review of Evidence by Members of the Primary Immunodeficiency Committee of the American Academy of Allergy, Asthma and Immunology. Journal of Allergy and Clinical Immunology 2006, 117, S525–S553. [Google Scholar] [CrossRef] [PubMed]
- Romero, C.; Díez, J.M.; Gajardo, R. Anti-SARS-CoV-2 Antibodies in Healthy Donor Plasma Pools and IVIG Products. The Lancet Infectious Diseases 2021, 21, 765–766. [Google Scholar] [CrossRef]
- Volk, A.; Covini-Souris, C.; Kuehnel, D.; De Mey, C.; Römisch, J.; Schmidt, T. SARS-CoV-2 Neutralization in Convalescent Plasma and Commercial Lots of Plasma-Derived Immunoglobulin. BioDrugs 2022, 36, 41–53. [Google Scholar] [CrossRef]
- Ahn, T.S.; Han, B.; Krogstad, P.; Bun, C.; Kohn, L.A.; Garcia-Lloret, M.I.; Damoiseaux, R.; Butte, M.J. Commercial Immunoglobulin Products Contain Cross-Reactive but Not Neutralizing Antibodies against SARS-CoV-2. Journal of Allergy and Clinical Immunology 2021, 147, 876–877. [Google Scholar] [CrossRef] [PubMed]
- Dalakas, M.C.; Bitzogli, K.; Alexopoulos, H. Anti-SARS-CoV-2 Antibodies Within IVIg Preparations: Cross-Reactivities With Seasonal Coronaviruses, Natural Autoimmunity, and Therapeutic Implications. Front. Immunol. 2021, 12, 627285. [Google Scholar] [CrossRef] [PubMed]
- Díez, J.-M.; Romero, C.; Gajardo, R. Currently Available Intravenous Immunoglobulin Contains Antibodies Reacting against Severe Acute Respiratory Syndrome Coronavirus 2 Antigens. Immunotherapy 2020, 12, 571–576. [Google Scholar] [CrossRef]
- Manian, D.V.; Jensen, C.; Theel, E.S.; Mills, J.R.; Joshi, A. Non-Neutralizing Antibodies and Limitations of Serologic Testing for Severe Acute Respiratory Syndrome Coronavirus 2 in Patients Receiving Immunoglobulin Replacement Products. Annals of Allergy, Asthma & Immunology 2021, 126, 206–207. [Google Scholar] [CrossRef]
- Schwaiger, J.; Karbiener, M.; Aberham, C.; Farcet, M.R.; Kreil, T.R. No SARS-CoV-2 Neutralization by Intravenous Immunoglobulins Produced From Plasma Collected Before the 2020 Pandemic. The Journal of Infectious Diseases 2020, 222, 1960–1964. [Google Scholar] [CrossRef] [PubMed]
- Farcet, M.R.; Karbiener, M.; Schwaiger, J.; Ilk, R.; Kreil, T.R. Rapidly Increasing Severe Acute Respiratory Syndrome Coronavirus 2 Neutralization by Intravenous Immunoglobulins Produced From Plasma Collected During the 2020 Pandemic. The Journal of Infectious Diseases 2022, 226, 1357–1361. [Google Scholar] [CrossRef]
- Romero, C.; Díez, J.-M.; Gajardo, R. Anti-SARS-CoV-2 Antibodies in Healthy Donor Plasma Pools and IVIG Products—an Update. The Lancet Infectious Diseases 2022, 22, 19. [Google Scholar] [CrossRef]
- Farcet, M.R.; Karbiener, M.; Knotzer, S.; Schwaiger, J.; Kreil, T.R. Omicron Severe Acute Respiratory Syndrome Coronavirus 2 Neutralization by Immunoglobulin Preparations Manufactured From Plasma Collected in the United States and Europe. The Journal of Infectious Diseases 2022, 226, 1396–1400. [Google Scholar] [CrossRef]
- Lindahl, H.; Klingström, J.; Da Silva Rodrigues, R.; Christ, W.; Chen, P.; Ljunggren, H.-G.; Buggert, M.; Aleman, S.; Smith, C.I.E.; Bergman, P. Neutralizing SARS-CoV-2 Antibodies in Commercial Immunoglobulin Products Give Patients with X-Linked Agammaglobulinemia Limited Passive Immunity to the Omicron Variant. J Clin Immunol 2022, 42, 1130–1136. [Google Scholar] [CrossRef]
- Raphael, A.; Shamriz, O.; Lev, A.; Simon, A.J.; Tal, Y.; Somech, R.; Eisenberg, R.; Toker, O. SARS-CoV-2 Spike Antibody Concentration in Gamma Globulin Products from High-Prevalence COVID-19 Countries Are Transmitted to X-Linked Agammaglobulinemia Patients. Front. Immunol. 2023, 14. [Google Scholar] [CrossRef]
- Hirsiger, J.R.; Weigang, S.; Walz, A.-C.; Fuchs, J.; Daly, M.-L.; Eggimann, S.; Hausmann, O.; Schwemmle, M.; Kochs, G.; Panning, M.; et al. Passive Immunization against COVID-19 by Anti-SARS-CoV-2 Spike IgG in Commercially Available Immunoglobulin Preparations in Severe Antibody Deficiency. J. Allergy Clin. Immunol. Pract. 2022, 10, 2452–2455.e3. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.L.; Rider, N.L.; Pyles, R.B.; Judy, B.; Xie, X.; Shi, P.-Y.; Ksiazek, T.G. The Arrival of SARS-CoV-2–Neutralizing Antibodies in a Currently Available Commercial Immunoglobulin. Journal of Allergy and Clinical Immunology 2022, 149, 1958–1959. [Google Scholar] [CrossRef] [PubMed]
- Stinca, S.; Barnes, T.W.; Vogel, P.; Meyers, W.; Schulte-Pelkum, J.; Filchtinski, D.; Steller, L.; Hauser, T.; Manni, S.; Gardiner, D.F.; et al. Modelling the Concentration of Anti-SARS-CoV-2 Immunoglobulin G in Intravenous Immunoglobulin Product Batches. PLoS ONE 2021, 16, e0259731. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Gada, S. SARS-CoV-2 Antibody Profile of Immune Globulin Preparations. Journal of Allergy and Clinical Immunology 2022, 149, AB65. [Google Scholar] [CrossRef]
- Lindahl, H.; Chen, P.; Åberg, M.; Ljunggren, H.-G.; Buggert, M.; Aleman, S.; Smith, C.I.E.; Bergman, P. SARS-CoV-2 Antibodies in Commercial Immunoglobulin Products Show Markedly Reduced Cross-Reactivities Against Omicron Variants. J Clin Immunol 2023, 43, 1075–1082. [Google Scholar] [CrossRef] [PubMed]
- Upasani, V.; Townsend, K.; Wu, M.Y.; Carr, E.J.; Hobbs, A.; Dowgier, G.; Ragno, M.; Herman, L.S.; Sharma, S.; Shah, D.; et al. Commercial Immunoglobulin Products Contain Neutralizing Antibodies Against Severe Acute Respiratory Syndrome Coronavirus 2 Spike Protein. Clinical Infectious Diseases 2023, 77, 950–960. [Google Scholar] [CrossRef] [PubMed]
- Cousins, K.; Sano, K.; Lam, B.; Röltgen, K.; Bhavsar, D.; Singh, G.; McRae, O.; Jeong, S.; Aboelregal, N.; Ho, H.; et al. Detection of SARS-CoV-2 Antibodies in Immunoglobulin Products. The Journal of Allergy and Clinical Immunology: In Practice 2023, 11, 2534–2541. [Google Scholar] [CrossRef] [PubMed]
- Karbiener, M.; Farcet, M.R.; Schwaiger, J.; Powers, N.; Lenart, J.; Stewart, J.M.; Tallman, H.; Kreil, T.R. Highly Potent SARS-CoV-2 Neutralization by Intravenous Immunoglobulins Manufactured from Post-COVID-19 and COVID-19-Vaccinated Plasma Donations. The Journal of Infectious Diseases 2021, jiab482. [Google Scholar] [CrossRef] [PubMed]
- Schubert, M.; Bertoglio, F.; Steinke, S.; Heine, P.A.; Ynga-Durand, M.A.; Maass, H.; Sammartino, J.C.; Cassaniti, I.; Zuo, F.; Du, L.; et al. Human Serum from SARS-CoV-2-Vaccinated and COVID-19 Patients Shows Reduced Binding to the RBD of SARS-CoV-2 Omicron Variant. BMC Med 2022, 20, 102. [Google Scholar] [CrossRef]
- Cox, M.; Peacock, T.P.; Harvey, W.T.; Hughes, J.; Wright, D.W.; COVID-19 Genomics UK (COG-UK) Consortium; Willett, B.J.; Thomson, E.; Gupta, R.K.; Peacock, S.J.; et al. SARS-CoV-2 Variant Evasion of Monoclonal Antibodies Based on in Vitro Studies. Nat Rev Microbiol 2023, 21, 112–124. [Google Scholar] [CrossRef]
- Commissioner, O. of the Coronavirus (COVID-19) Update: FDA Authorizes Additional Monoclonal Antibody for Treatment of COVID-19. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-additional-monoclonal-antibody-treatment-covid-19 (accessed on 25 April 2023).
- Totschnig, D.; Augustin, M.; Niculescu, I.; Laferl, H.; Jansen-Skoupy, S.; Lehmann, C.; Wenisch, C.; Zoufaly, A. SARS-CoV-2 Pre-Exposure Prophylaxis with Sotrovimab and Tixagevimab/Cilgavimab in Immunocompromised Patients—A Single-Center Experience. Viruses 2022, 14, 2278. [Google Scholar] [CrossRef]
- Martin-Blondel, G.; Marcelin, A.-G.; Soulié, C.; Kaisaridi, S.; Lusivika-Nzinga, C.; Dorival, C.; Nailler, L.; Boston, A.; Melenotte, C.; Gaube, G.; et al. Outcome of Very High-Risk Patients Treated by Sotrovimab for Mild-to-Moderate COVID-19 Omicron, a Prospective Cohort Study (the ANRS 0003S COCOPREV Study). J Infect 2022, 84, e101–e104. [Google Scholar] [CrossRef]
- Gupta, A.; Gonzalez-Rojas, Y.; Juarez, E.; Crespo Casal, M.; Moya, J.; Rodrigues Falci, D.; Sarkis, E.; Solis, J.; Zheng, H.; Scott, N.; et al. Effect of Sotrovimab on Hospitalization or Death Among High-Risk Patients With Mild to Moderate COVID-19: A Randomized Clinical Trial. JAMA 2022, 327, 1236–1246. [Google Scholar] [CrossRef]
- Stadler, E.; Chai, K.L.; Schlub, T.E.; Cromer, D.; Polizzotto, M.N.; Kent, S.J.; Beecher, C.; White, H.; Turner, T.; Skoetz, N.; et al. Determinants of Passive Antibody Efficacy in SARS-CoV-2 Infection; Infectious Diseases (except HIV/AIDS), 2022.
- Zheng, B.; Green, A.C.A.; Tazare, J.; Curtis, H.J.; Fisher, L.; Nab, L.; Schultze, A.; Mahalingasivam, V.; Parker, E.P.K.; Hulme, W.J.; et al. Comparative Effectiveness of Sotrovimab and Molnupiravir for Prevention of Severe Covid-19 Outcomes in Patients in the Community: Observational Cohort Study with the OpenSAFELY Platform. BMJ 2022, e071932. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.; Yarwood, M.J.; Levick, B.; Gibbons, D.C.; Drysdale, M.; Kerr, W.; Watkins, J.D.; Young, S.; Pierce, B.F.; Lloyd, E.J.; et al. Characteristics and Outcomes of Patients with COVID-19 at High-Risk of Disease Progression Receiving Sotrovimab, Oral Antivirals or No Treatment in England; Infectious Diseases (except HIV/AIDS), 2022.
- Zheng, B.; Tazare, J.; Nab, L.; Mehrkar, A.; MacKenna, B.; Goldacre, B.; Douglas, I.J.; Tomlinson, L.A. Comparative Effectiveness of Paxlovid versus Sotrovimab and Molnupiravir for Preventing Severe COVID-19 Outcomes in Non-Hospitalised Patients: Observational Cohort Study Using the OpenSAFELY Platform; Epidemiology, 2023.
- Harman, K.; Nash, S.G.; Webster, H.H.; Groves, N.; Hardstaff, J.; Bridgen, J.; Blomquist, P.B.; Hope, R.; Ashano, E.; Myers, R.; et al. Comparison of the Risk of Hospitalisation among BA.1 and BA.2 COVID-19 Cases Treated with Sotrovimab in the Community in England. Influenza and Other Respiratory Viruses 2023, 17, e13150. [Google Scholar] [CrossRef]
- Cheng, M.M.; Reyes, C.; Satram, S.; Birch, H.; Gibbons, D.C.; Drysdale, M.; Bell, C.F.; Suyundikov, A.; Ding, X.; Maher, M.C.; et al. Real-World Effectiveness of Sotrovimab for the Early Treatment of COVID-19 During SARS-CoV-2 Delta and Omicron Waves in the USA. Infect Dis Ther 2023, 12, 607–621. [Google Scholar] [CrossRef] [PubMed]
- Martin-Blondel, G.; Marcelin, A.-G.; Soulié, C.; Kaisaridi, S.; Lusivika-Nzinga, C.; Dorival, C.; Nailler, L.; Boston, A.; Melenotte, C.; Cabié, A.; et al. Sotrovimab to Prevent Severe COVID-19 in High-Risk Patients Infected with Omicron BA.2. J Infect 2022, 85, e104–e108. [Google Scholar] [CrossRef]
- Zaqout, A.; Almaslamani, M.A.; Chemaitelly, H.; Hashim, S.A.; Ittaman, A.; Alimam, A.; Rustom, F.; Daghfal, J.; Abukhattab, M.; AlMukdad, S.; et al. Effectiveness of the Neutralizing Antibody Sotrovimab among High-Risk Patients with Mild-to-Moderate SARS-CoV-2 in Qatar. Int J Infect Dis 2022, 124, 96–103. [Google Scholar] [CrossRef]
- Case, J.B.; Mackin, S.; Errico, J.M.; Chong, Z.; Madden, E.A.; Whitener, B.; Guarino, B.; Schmid, M.A.; Rosenthal, K.; Ren, K.; et al. Resilience of S309 and AZD7442 Monoclonal Antibody Treatments against Infection by SARS-CoV-2 Omicron Lineage Strains. Nat Commun 2022, 13, 3824. [Google Scholar] [CrossRef]
- Takashita, E.; Kinoshita, N.; Yamayoshi, S.; Sakai-Tagawa, Y.; Fujisaki, S.; Ito, M.; Iwatsuki-Horimoto, K.; Halfmann, P.; Watanabe, S.; Maeda, K.; et al. Efficacy of Antiviral Agents against the SARS-CoV-2 Omicron Subvariant BA.2. N Engl J Med 2022, 386, 1475–1477. [Google Scholar] [CrossRef]
- Takashita, E.; Yamayoshi, S.; Halfmann, P.; Wilson, N.; Ries, H.; Richardson, A.; Bobholz, M.; Vuyk, W.; Maddox, R.; Baker, D.A.; et al. In Vitro Efficacy of Antiviral Agents against Omicron Subvariant BA.4.6. N Engl J Med 2022, 387, 2094–2097. [Google Scholar] [CrossRef]
- Takashita, E.; Yamayoshi, S.; Simon, V.; van Bakel, H.; Sordillo, E.M.; Pekosz, A.; Fukushi, S.; Suzuki, T.; Maeda, K.; Halfmann, P.; et al. Efficacy of Antibodies and Antiviral Drugs against Omicron BA.2.12.1, BA.4, and BA.5 Subvariants. N Engl J Med 2022, 387, 468–470. [Google Scholar] [CrossRef]
- Imai, M.; Ito, M.; Kiso, M.; Yamayoshi, S.; Uraki, R.; Fukushi, S.; Watanabe, S.; Suzuki, T.; Maeda, K.; Sakai-Tagawa, Y.; et al. Efficacy of Antiviral Agents against Omicron Subvariants BQ.1.1 and XBB. N Engl J Med 2023, 388, 89–91. [Google Scholar] [CrossRef]
- Park, Y.-J.; Pinto, D.; Walls, A.C.; Liu, Z.; De Marco, A.; Benigni, F.; Zatta, F.; Silacci-Fregni, C.; Bassi, J.; Sprouse, K.R.; et al. Imprinted Antibody Responses against SARS-CoV-2 Omicron Sublineages. Science 2022, 378, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.Y.; Carr, E.J.; Harvey, R.; Mears, H.V.; Kjaer, S.; Townsley, H.; Hobbs, A.; Ragno, M.; Herman, L.S.; Adams, L.; et al. WHO’s Therapeutics and COVID-19 Living Guideline on mAbs Needs to Be Reassessed. The Lancet 2022, S0140673622019389. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Jian, F.; Wang, J.; Yu, Y.; Song, W.; Yisimayi, A.; Wang, J.; An, R.; Chen, X.; Zhang, N.; et al. Imprinted SARS-CoV-2 Humoral Immunity Induces Convergent Omicron RBD Evolution. Nature 2022. [Google Scholar] [CrossRef] [PubMed]
- Yue, C.; Song, W.; Wang, L.; Jian, F.; Chen, X.; Gao, F.; Shen, Z.; Wang, Y.; Wang, X.; Cao, Y. ACE2 Binding and Antibody Evasion in Enhanced Transmissibility of XBB.1.5. The Lancet Infectious Diseases 2023, 23, 278–280. [Google Scholar] [CrossRef]
- Wang, Q.; Iketani, S.; Li, Z.; Liu, L.; Guo, Y.; Huang, Y.; Bowen, A.D.; Liu, M.; Wang, M.; Yu, J.; et al. Alarming Antibody Evasion Properties of Rising SARS-CoV-2 BQ and XBB Subvariants. Cell 2023, 186, 279–286.e8. [Google Scholar] [CrossRef]
- Research, C. for D.E. and FDA Updates Sotrovimab Emergency Use Authorization. FDA 2022. [Google Scholar]
- Loo, Y.-M.; McTamney, P.M.; Arends, R.H.; Abram, M.E.; Aksyuk, A.A.; Diallo, S.; Flores, D.J.; Kelly, E.J.; Ren, K.; Roque, R.; et al. The SARS-CoV-2 Monoclonal Antibody Combination, AZD7442, Is Protective in Nonhuman Primates and Has an Extended Half-Life in Humans. Sci. Transl. Med. 2022, 14, eabl8124. [Google Scholar] [CrossRef]
- Stiasny, K.; Weseslindtner, L.; Heinzel, A.; Camp, J.V.; Oberbauer, R.; Reindl-Schwaighofer, R. SARS-CoV-2 Omicron BA.1/BA.2 Neutralization up to 8 Weeks After PrEP With Sotrovimab or Cilgavimab/Tixagevimab. Transpl Int 2022, 35, 10906. [Google Scholar] [CrossRef] [PubMed]
- Bruel, T.; Hadjadj, J.; Maes, P.; Planas, D.; Seve, A.; Staropoli, I.; Guivel-Benhassine, F.; Porrot, F.; Bolland, W.-H.; Nguyen, Y.; et al. Serum Neutralization of SARS-CoV-2 Omicron Sublineages BA.1 and BA.2 in Patients Receiving Monoclonal Antibodies. Nat Med 2022, 28, 1297–1302. [Google Scholar] [CrossRef] [PubMed]
- Benotmane, I.; Velay, A.; Gautier-Vargas, G.; Olagne, J.; Obrecht, A.; Cognard, N.; Heibel, F.; Braun-Parvez, L.; Keller, N.; Martzloff, J.; et al. Breakthrough COVID-19 Cases despite Prophylaxis with 150 Mg of Tixagevimab and 150 Mg of Cilgavimab in Kidney Transplant Recipients. American Journal of Transplantation 2022, 22, 2675–2681. [Google Scholar] [CrossRef] [PubMed]
- Research, C. for D.E. and FDA Announces Evusheld Is Not Currently Authorized for Emergency Use in the U.S. FDA 2023. [Google Scholar]
- AstraZeneca A Phase I/III Randomized, Double Blind Study to Evaluate the Safety and Neutralizing Activity of AZD5156/AZD3152 for Pre Exposure Prophylaxis of COVID 19 in Participants With Conditions Causing Immune Impairment; clinicaltrials.gov, 2023.
- First Participant Dosed in SUPERNOVA Phase I/III Trial Evaluating AZD5156, a next-Generation Long-Acting Antibody Combination, for Prevention of COVID-19. Available online: https://www.astrazeneca-us.com/media/statements/2022/first-participant-dosed-in-supernova-phase-I-III-trial-evaluating-azd5156-a-next-generation-long-acting-antibody-combination-for-prevention-of-covid-19.html (accessed on 26 April 2023).
- Delmonte, O.M.; Bergerson, J.R.E.; Burbelo, P.D.; Durkee-Shock, J.R.; Dobbs, K.; Bosticardo, M.; Keller, M.D.; McDermott, D.H.; Rao, V.K.; Dimitrova, D.; et al. Antibody Responses to the SARS-CoV-2 Vaccine in Individuals with Various Inborn Errors of Immunity. J Allergy Clin Immunol 2021, 148, 1192–1197. [Google Scholar] [CrossRef]
- Davies, N.G.; Abbott, S.; Barnard, R.C.; Jarvis, C.I.; Kucharski, A.J.; Munday, J.D.; Pearson, C.A.B.; Russell, T.W.; Tully, D.C.; Washburne, A.D.; et al. Estimated Transmissibility and Impact of SARS-CoV-2 Lineage B.1.1.7 in England. Science 2021, 372, eabg3055. [Google Scholar] [CrossRef]
- SARS-CoV-2 Variants of Concern as of 9 March 2023. Available online: https://www.ecdc.europa.eu/en/covid-19/variants-concern (accessed on 20 March 2023).
- Davies, N.G.; Jarvis, C.I.; Group, C.C.-19 W.; Edmunds, W.J.; Jewell, N.P.; Diaz-Ordaz, K.; Keogh, R.H. Increased Mortality in Community-Tested Cases of SARS-CoV-2 Lineage B.1.1.7. Nature 2021, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Tegally, H.; Wilkinson, E.; Giovanetti, M.; Iranzadeh, A.; Fonseca, V.; Giandhari, J.; Doolabh, D.; Pillay, S.; San, E.J.; Msomi, N.; et al. Detection of a SARS-CoV-2 Variant of Concern in South Africa. Nature 2021, 592, 438–443. [Google Scholar] [CrossRef] [PubMed]
- Cele, S.; Gazy, I.; Jackson, L.; Hwa, S.-H.; Tegally, H.; Lustig, G.; Giandhari, J.; Pillay, S.; Wilkinson, E.; Naidoo, Y.; et al. Escape of SARS-CoV-2 501Y.V2 from Neutralization by Convalescent Plasma. Nature 2021, 593, 142–146. [Google Scholar] [CrossRef] [PubMed]
- Madhi, S.A.; Baillie, V.; Cutland, C.L.; Voysey, M.; Koen, A.L.; Fairlie, L.; Padayachee, S.D.; Dheda, K.; Barnabas, S.L.; Bhorat, Q.E.; et al. Efficacy of the ChAdOx1 nCoV-19 Covid-19 Vaccine against the B.1.351 Variant. N Engl J Med 2021, 384, 1885–1898. [Google Scholar] [CrossRef]
- Planas, D.; Veyer, D.; Baidaliuk, A.; Staropoli, I.; Guivel-Benhassine, F.; Rajah, M.M.; Planchais, C.; Porrot, F.; Robillard, N.; Puech, J.; et al. Reduced Sensitivity of SARS-CoV-2 Variant Delta to Antibody Neutralization. Nature 2021, 596, 276–280. [Google Scholar] [CrossRef] [PubMed]
- Faria, N.R.; Mellan, T.A.; Whittaker, C.; Claro, I.M.; Candido, D. da S.; Mishra, S.; Crispim, M.A.E.; Sales, F.C.S.; Hawryluk, I.; McCrone, J.T.; et al. Genomics and Epidemiology of the P.1 SARS-CoV-2 Lineage in Manaus, Brazil. Science 2021, 372, 815–821. [Google Scholar] [CrossRef] [PubMed]
- Dejnirattisai, W.; Zhou, D.; Supasa, P.; Liu, C.; Mentzer, A.J.; Ginn, H.M.; Zhao, Y.; Duyvesteyn, H.M.E.; Tuekprakhon, A.; Nutalai, R.; et al. Antibody Evasion by the P.1 Strain of SARS-CoV-2. Cell 2021, 184, 2939–2954.e9. [Google Scholar] [CrossRef]
- Shiehzadegan, S.; Alaghemand, N.; Fox, M.; Venketaraman, V. Analysis of the Delta Variant B.1.617.2 COVID-19. Clinics and Practice 2021, 11, 778–784. [Google Scholar] [CrossRef]
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Stowe, J.; Tessier, E.; Groves, N.; Dabrera, G.; et al. Effectiveness of Covid-19 Vaccines against the B.1.617.2 (Delta) Variant. N Engl J Med 2021, 385, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, A.; McMenamin, J.; Taylor, B.; Robertson, C. ; Public Health Scotland and the EAVE II Collaborators SARS-CoV-2 Delta VOC in Scotland: Demographics, Risk of Hospital Admission, and Vaccine Effectiveness. Lancet 2021, 397, 2461–2462. [Google Scholar] [CrossRef]
- Stowe, J.; Andrews, N.; Kirsebom, F.; Ramsay, M.; Bernal, J.L. Effectiveness of COVID-19 Vaccines against Omicron and Delta Hospitalisation, a Test Negative Case-Control Study. Nat Commun 2022, 13, 5736. [Google Scholar] [CrossRef]
- Nextstrain / Ncov / Open / Global / 6m. Available online: https://nextstrain.org/ncov/open/global/6m (accessed on 20 March 2023).
- Fan, Y.; Li, X.; Zhang, L.; Wan, S.; Zhang, L.; Zhou, F. SARS-CoV-2 Omicron Variant: Recent Progress and Future Perspectives. Sig Transduct Target Ther 2022, 7, 141. [Google Scholar] [CrossRef]
- He, X.; Hong, W.; Pan, X.; Lu, G.; Wei, X. SARS-CoV-2 Omicron Variant: Characteristics and Prevention. MedComm 2021, 2, 838–845. [Google Scholar] [CrossRef]
- Hui, K.P.Y.; Ho, J.C.W.; Cheung, M.-C.; Ng, K.-C.; Ching, R.H.H.; Lai, K.-L.; Kam, T.T.; Gu, H.; Sit, K.-Y.; Hsin, M.K.Y.; et al. SARS-CoV-2 Omicron Variant Replication in Human Bronchus and Lung Ex Vivo. Nature 2022, 603, 715–720. [Google Scholar] [CrossRef]
- Rössler, A.; Knabl, L.; von Laer, D.; Kimpel, J. Neutralization Profile after Recovery from SARS-CoV-2 Omicron Infection. N Engl J Med 2022, 386, 1764–1766. [Google Scholar] [CrossRef] [PubMed]
- Altarawneh, H.N.; Chemaitelly, H.; Hasan, M.R.; Ayoub, H.H.; Qassim, S.; AlMukdad, S.; Coyle, P.; Yassine, H.M.; Al-Khatib, H.A.; Benslimane, F.M.; et al. Protection against the Omicron Variant from Previous SARS-CoV-2 Infection. N Engl J Med 2022, 386, 1288–1290. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Yisimayi, A.; Jian, F.; Song, W.; Xiao, T.; Wang, L.; Du, S.; Wang, J.; Li, Q.; Chen, X.; et al. BA.2.12.1, BA.4 and BA.5 Escape Antibodies Elicited by Omicron Infection. Nature 2022, 608, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Outbreak.Info SARS-CoV-2 Data Explorer. Available online: https://outbreak.info/ (accessed on 20 March 2023).
- Zappa, M.; Verdecchia, P.; Angeli, F. Severe Acute Respiratory Syndrome Coronavirus 2 Evolution: How Mutations Affect XBB.1.5 Variant. European Journal of Internal Medicine 2023, 112, 128–132. [Google Scholar] [CrossRef] [PubMed]
- Uriu, K.; Ito, J.; Zahradnik, J.; Fujita, S.; Kosugi, Y.; Schreiber, G.; Sato, K. Enhanced Transmissibility, Infectivity, and Immune Resistance of the SARS-CoV-2 Omicron XBB.1.5 Variant. The Lancet Infectious Diseases 2023, 23, 280–281. [Google Scholar] [CrossRef] [PubMed]
- Qu, P.; Faraone, J.N.; Evans, J.P.; Zheng, Y.-M.; Carlin, C.; Anghelina, M.; Stevens, P.; Fernandez, S.; Jones, D.; Panchal, A.; et al. Extraordinary Evasion of Neutralizing Antibody Response by Omicron XBB.1.5, CH.1.1 and CA.3.1 Variants; Microbiology, 2023.
- Luoma, E.; Rohrer, R.; Parton, H.; Hughes, S.; Omoregie, E.; Taki, F.; Wang, J.C.; Akther, S.; Amin, H.; Chang, C.; et al. Notes from the Field: Epidemiologic Characteristics of SARS-CoV-2 Recombinant Variant XBB.1.5 — New York City, November 1, 2022–January 4, 2023. MMWR Morb. Mortal. Wkly. Rep. 2023, 72, 212–214. [Google Scholar] [CrossRef] [PubMed]
- 215. COVID XBB 1.16, Nicknamed as Arcturus, Is Spreading Faster than Its Ancestral Variants: Know More. The Times of India.
- SARS-CoV-2 Variants of Concern as of 17 May 2023. Available online: https://www.ecdc.europa.eu/en/covid-19/variants-concern (accessed on 29 May 2023).
- Tracking SARS-CoV-2 Variants. Available online: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/ (accessed on 17 March 2023).
- Giardino, G.; Milito, C.; Lougaris, V.; Punziano, A.; Carrabba, M.; Cinetto, F.; Scarpa, R.; Dellepiane, R.M.; Ricci, S.; Rivalta, B.; et al. The Impact of SARS-CoV-2 Infection in Patients with Inborn Errors of Immunity: The Experience of the Italian Primary Immunodeficiencies Network (IPINet). J. Clin. Immunol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Schulz, E.; Hodl, I.; Forstner, P.; Hatzl, S.; Sareban, N.; Moritz, M.; Fessler, J.; Dreo, B.; Uhl, B.; Url, C.; et al. CD19+IgD+CD27- Naïve B Cells as Predictors of Humoral Response to COVID 19 mRNA Vaccination in Immunocompromised Patients. Front. Immunol. 2021, 12, 803742. [Google Scholar] [CrossRef]
- Sokal, A.; Bastard, P.; Chappert, P.; Barba-Spaeth, G.; Fourati, S.; Vanderberghe, A.; Lagouge-Roussey, P.; Meyts, I.; Gervais, A.; Bouvier-Alias, M.; et al. Human Type I IFN Deficiency Does Not Impair B Cell Response to SARS-CoV-2 mRNA Vaccination. J Exp Med 2022, 220, e20220258. [Google Scholar] [CrossRef]
- Evusheld (Tixagevimab and Cilgavimab) Dosing, Indications, Interactions, Adverse Effects, and More. Available online: https://reference.medscape.com/drug/evusheld-tixagevimab-cilgavimab-4000251 (accessed on 10 August 2023).
- Zhang, J.; Zhang, H.; Sun, L. Therapeutic Antibodies for COVID-19: Is a New Age of IgM, IgA and Bispecific Antibodies Coming? mAbs 2022, 14, 2031483. [Google Scholar] [CrossRef]
- Zost, S.J.; Gilchuk, P.; Case, J.B.; Binshtein, E.; Chen, R.E.; Nkolola, J.P.; Schäfer, A.; Reidy, J.X.; Trivette, A.; Nargi, R.S.; et al. Potently Neutralizing and Protective Human Antibodies against SARS-CoV-2. Nature 2020, 584, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Pinto, D.; Park, Y.-J.; Beltramello, M.; Walls, A.C.; Tortorici, M.A.; Bianchi, S.; Jaconi, S.; Culap, K.; Zatta, F.; De Marco, A.; et al. Cross-Neutralization of SARS-CoV-2 by a Human Monoclonal SARS-CoV Antibody. Nature 2020, 583, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Tuccori, M.; Ferraro, S.; Convertino, I.; Cappello, E.; Valdiserra, G.; Blandizzi, C.; Maggi, F.; Focosi, D. Anti-SARS-CoV-2 Neutralizing Monoclonal Antibodies: Clinical Pipeline. MAbs 2020, 12, 1854149. [Google Scholar] [CrossRef] [PubMed]
- Administration (TGA), T.G. Evusheld. Available online: https://www.tga.gov.au/resources/auspmd/evusheld (accessed on 10 August 2023).
- Coronavirus Disease (COVID-19) Situation Reports. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed on 10 July 2023).
- CoVariants: Per Country. Available online: https://covariants.org/per-country (accessed on 10 July 2023).
Figure 1.
Shifting predominance of SARS-CoV-2 variants over time and in different geographical locations worldwide. SARS-CoV-2 variant predominance in different countries and globally (A) as at July 10th 2023 and (B) December 18th 2023. Global data from [227] and individual country data from [228].
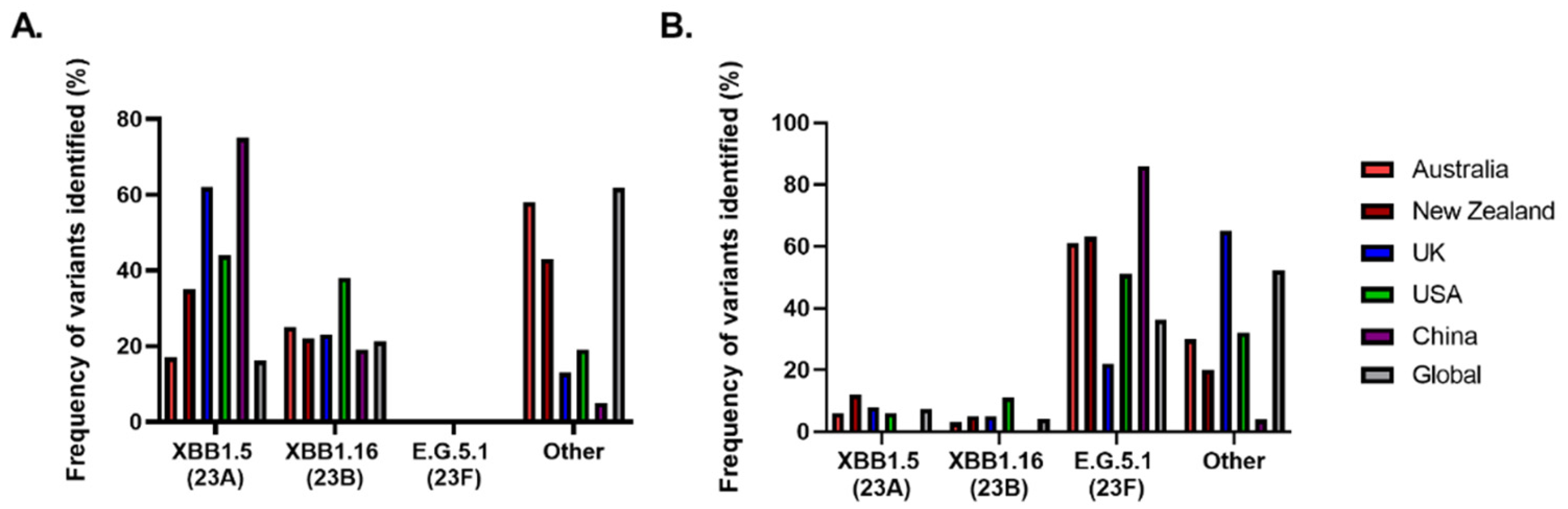
Figure 2.
Generation of SARS-CoV-2-specific immunity in responses to COVID-19 vaccination in IEI patients. In healthy individuals, after administration of the COVID-19 vaccination, naive B and T-cells are primed and expand to generate long-lived memory specific for the SARS-CoV-2 spike protein contained in the vaccine. This includes spike-specific antibodies, memory B cells and memory T-cells that are ready for action upon re-exposure to antigen either because of booster vaccination or natural infection. In contrast, IEI patients are reported to generate a variable and, in some cases, poor response to COVID-19 vaccination which is dependent upon the genetic defect they possess. In most studies, COVID-19 vaccination of IEI patients can result in reduced COVID-19 specific antibody, memory B-cell, and/or memory T-cell responses dependent upon the nature of the genetic lesion and the arm of the immune system affected. Above we indicate IEIs for which IEIs perturbed COVID-19 vaccination responses have been reported in the literature. Additionally, innate cells play a pivotal role in the first line of defense against viruses. However, the responses of these cells to vaccination are currently unknown. Figure generated with BioRender.
Figure 2.
Generation of SARS-CoV-2-specific immunity in responses to COVID-19 vaccination in IEI patients. In healthy individuals, after administration of the COVID-19 vaccination, naive B and T-cells are primed and expand to generate long-lived memory specific for the SARS-CoV-2 spike protein contained in the vaccine. This includes spike-specific antibodies, memory B cells and memory T-cells that are ready for action upon re-exposure to antigen either because of booster vaccination or natural infection. In contrast, IEI patients are reported to generate a variable and, in some cases, poor response to COVID-19 vaccination which is dependent upon the genetic defect they possess. In most studies, COVID-19 vaccination of IEI patients can result in reduced COVID-19 specific antibody, memory B-cell, and/or memory T-cell responses dependent upon the nature of the genetic lesion and the arm of the immune system affected. Above we indicate IEIs for which IEIs perturbed COVID-19 vaccination responses have been reported in the literature. Additionally, innate cells play a pivotal role in the first line of defense against viruses. However, the responses of these cells to vaccination are currently unknown. Figure generated with BioRender.
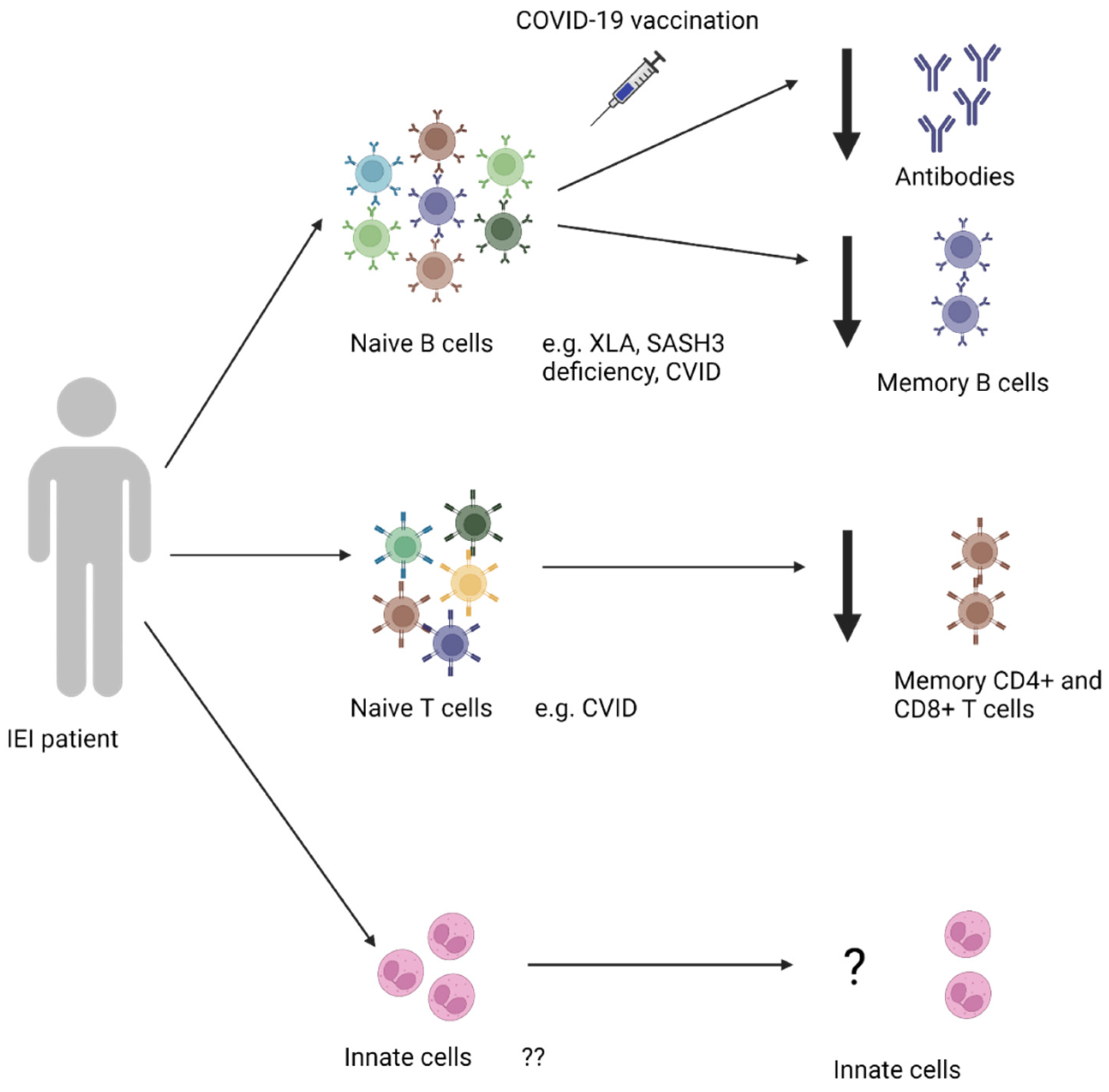
Figure 3.
Main methods for the in vitro detection of SARS-CoV-2-specific humoral and cellular immunity in the peripheral blood of humans. (A) SARS.CoV-2 specific antibodies can be detected by ELISA or immunoblot, whilst SARS-CoV-2 virus neutralization is most frequently quantified using pseudovirus or authentic virus neutralization assays. (B) SARS-CoV-2-specific memory B cells (Bmem) can be identified either by the capture of IgG after antigenic stimulation in an ELISPOT or using fluorescently labelled SARS-CoV-2 antigen containing fluorochromes. (C) SARS-CoV-2-specific memory T-cells (Tmem) can either be identified by binding to fluorescently tagged peptide loaded MHC tetramers, or after stimulation with whole protein or overlapping peptide pools. Here, SARS-CoV-2-specific Tmem are enumerated by either the production of cytokines such as IFN-γ in ELISPOTs or ELISAs, or intracellular detection of cytokines coupled with cell surface expression of activation-induced markers (AIM) such as CD69, CD134, CD137. Together, multiple methods have been used to assess immune responses to vaccination preventing robust comparison between various published reports (Table 2). Figure generated with BioRender.
Figure 3.
Main methods for the in vitro detection of SARS-CoV-2-specific humoral and cellular immunity in the peripheral blood of humans. (A) SARS.CoV-2 specific antibodies can be detected by ELISA or immunoblot, whilst SARS-CoV-2 virus neutralization is most frequently quantified using pseudovirus or authentic virus neutralization assays. (B) SARS-CoV-2-specific memory B cells (Bmem) can be identified either by the capture of IgG after antigenic stimulation in an ELISPOT or using fluorescently labelled SARS-CoV-2 antigen containing fluorochromes. (C) SARS-CoV-2-specific memory T-cells (Tmem) can either be identified by binding to fluorescently tagged peptide loaded MHC tetramers, or after stimulation with whole protein or overlapping peptide pools. Here, SARS-CoV-2-specific Tmem are enumerated by either the production of cytokines such as IFN-γ in ELISPOTs or ELISAs, or intracellular detection of cytokines coupled with cell surface expression of activation-induced markers (AIM) such as CD69, CD134, CD137. Together, multiple methods have been used to assess immune responses to vaccination preventing robust comparison between various published reports (Table 2). Figure generated with BioRender.
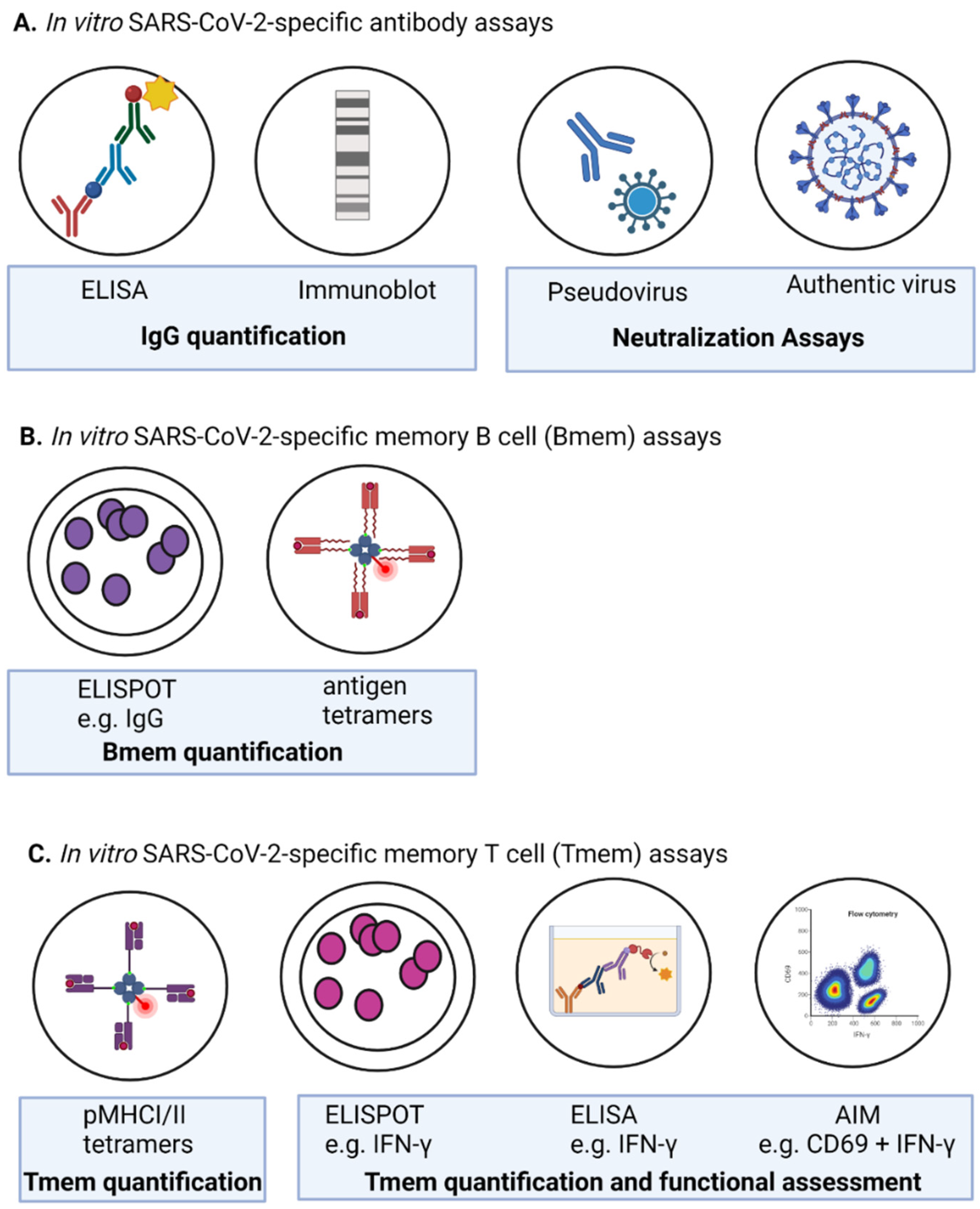

Table 1.
Current and previous SARS-CoV-2 variants and their characteristics.
| WHO label | Earliest documented samples | Date designated as a variant by WHO | Pango lineage (Nextstrain Clade) |
Sublineage | RBD mutations compared to Wuhan (AA #319-541) | Other proteins harboring mutations | Rationale for designation as a variant of interest |
|---|---|---|---|---|---|---|---|
| Alpha | UK, September 2020 | December 18 2020 – March 9 2022 | B.1.1.7 (20I) |
- | N501Y [190] | N, ORF1ab, ORF8 [191] | Increased transmissibility, immune evasion and disease severity [190,192]. |
| Beta | South Africa, September 2020 | December 18 2020 - March 9 2022 | B.1.351 (20H) |
- | K417N, E484, N501Y [193] | E, N, ORF1ab, ORF3a, ORF8 [191] | Increased transmissibility, immune evasion and disease severity [190,193,194,195]. |
| Gamma | Brazil November 2020 | January 11 2021 – March 9 2022 | P.1 (20J) |
- | K417T, E484, N501Y [196] | N, ORF1ab, ORF3a, ORF8 [191] | Increased transmissibility, immune evasion and disease severity [190,197,198]. |
| Delta | India, October 2020 | May 11 2021 – June 7 2022 | B.1.617.2 (21I/21J) |
- | L452R, T478K [199] | M, N, ORF1ab, ORF3a, ORF7a [191] | Increased transmissibility, immune evasion and disease severity [200,201,202]. |
| Omicron | Multiple countries incl. South Africa, November 2021 | November 26 2021 – March 2023 | B.1.1.529 (21K) |
BA.1 | G339D, S371L, S373P, S375F, K417N, N440K, G446S, S477N, T478K, E484A, Q493R, Q498R, N501Y, Y505H [191,203,204,205] | E, M, N, ORF1ab, ORF3a [191] | High transmissibility and immune evasion ability, reduced disease severity [206,207,208]. |
| South Africa, November 2021 | ? – March 2023 | (21L) | BA.2 | G339D, S371L, S373P, S375F, T376A, D405N, R408S, K417N, N440K, S477N, T478K, E484A, Q493R, Q498R, N501Y, Y505H and reversion to Wuhan G446 and G496 [191,204]. | E, M, N, ORF1ab, ORF3a, ORF6 [191] | Enhanced transmissibility and immune evasion ability, reduced disease severity [209]. | |
| South Africa, January and February 2022 respectively | ? – March 2023 | (22A/22B) | BA.4/5 | BA.2 variants plus L452R, F486V and reversion to Wuhan R493Q revertant [210] | E, M, N, ORF1ab, ORF3a (+ORF6 for BA4 and ORF7a, ORF8 for BA5 respectively) [191] | Impact on transmissibility and disease severity unclear, increased immune evasion capacity [209]. | |
| February 2022 | October 2022 | (22E) | BQ.1.1. (descendent of BA.5) |
BA.5 variants plus R346T, K444T, N460K | N, ORF1ab, ORF9b [191] | Unknown. | |
| United States, October 2022 | January 2023 | (23A) | XBB.1.5 |
G339H, R346T, L368I, S371F, S373P, S375F, T376A, D405N, R408S, K417N, N440K, V445P, G446P, N460K, S447N, T478K, E484A, F490P, F490S, Q498R, N501Y, Y505H [211] | E, M, N, ORF1ab, ORF3a, ORF6, ORF8, nsp1 [211] | Enhanced transmissibility, and impact on immunity. Disease severity similar to baseline [179,212,213,214]. | |
| Unknown, January 2023 | April 2023 | (23B) | XBB.1.16 |
BA.2.10.1 and BA.2.75 plus K478R, F486P [215] | E, M, N, ORF1ab, ORF3a, ORF6, ORF8, nsp1 [211] | No evidence of impact on transmissibility, immunity or disease severity [216]. | |
| Unknown, February 2023 |
August 2023 | (23F) | E.G.5.1 | G339H, R346T, L368I, S371F, S373P, S375F, T376A, D405N, R408S, K417N, N440K, V445P, F456L, G446P, N460K, S447N, T478K, E484A, S486P, F490S, Q498R, N501Y, Y505H [217] | ? | No evidence of impact on transmissibility, immunity or disease severity [216]. | |
| Unknown, July 2023 | November 2023 | (23I) | BA.2.86 | G339D, S371L, S373P, S375F, T376A, D405N, R408S, K417N, N440K, S477N, T478K, E484A, Q493R, Q498R, N501Y, Y505H and reversion to Wuhan G446 and G496 [191,204] | Some evidence that the variant evades antibodies. No evidence of changes in clinical severity [38]. | ||
| Unknown, August 2023 | February 2024 | (not assigned) | JN.1 | G339D, S371L, S373P, S375F, T376A, D405N, R408S, K417N, N440K, S477N, T478K, E484A, Q493R, Q498R, N501Y, Y505H and reversion to Wuhan G446 and G496, L5455S [38,191,204] | ORF1a, ORF7b [38] | Some evidence that the variant evades antibodies. No evidence of changes in clinical severity [38]. |
E, Envelope; M, Membrane; N, Nucleocapsid; N/A, not applicable; ORF, Open Reading Frame; PANGO, Phylogenetic Assignment of Named Global Outbreak; RBD, Receptor Binding Domain; WHO, World Health Organization, Unless otherwise stated all variant information compiled from [38,39,217]. All data correct as at 01/03/2024.
Table 2.
Methods used for the evaluation of cellular and humoral immune responses.
| Assay | References | |
|---|---|---|
| Studies investigating | ||
| IEI patient responses to COVID-19 vaccination | Quantity and quality IgG antibodies in IgRT | |
| SARS-CoV-2 binding IgG Antibodies | ||
| SARS-CoV-2 IgG II Quant Assay | [84] | - |
| Luciferase immunoprecipitation | [189] | - |
| ELISA | [79,80,81,83,89,91,94,99,101,102,104,105,106,109,110,111,112,113,114,115,116,117] | [137,138,139,140,141,142,149,150] |
| Abbott/Phadia ELiA SARS-CoV-2-Sp1 IgG assay | - | [147,151] |
| Roche Elecsys immunoassay | [77,79,80,101,125,219] | [154] |
| DiaSorin IgG immunoassay | [77,78,85,99,120,219] | - |
| Microblot assay | [112] | - |
| Abbot nucleoprotein assay | [78] | - |
| His-tagged spike and RBD binding probes | [87] | - |
| Abbott IgG assay | [82,88] | - |
| Luminex Ab binding | [95,149] | - |
| Extracted cell free DNA sequenced by DNBSEQ | [89] | - |
| Abbott Quant chemiluminescent microparticle immunoassay | - | [156] |
| Abbot AdviseDx SARS-CoV-2 IgG II assay | - | |
| V-PLEX SARS-CoV-2 10-plex IgG | [153] | |
| SARS-CoV-2 neutralizing antibodies | ||
| SARS-CoV-2 Neutralization Antibody Detection Kit | [100,110,149] | - |
| Pseudovirus Neutralization assay | [71,79,83,87,89,92,117,120,133] | [139,143,144,145,146,150,156] |
| ELISA | [69,70,86,93] | - |
| Live neutralization assays using Vero cells | [73,98,125] | [147] |
| B-cell measurement | [81] | - |
| Luminex based assays | [95] | [154] |
| SARS-CoV-2-specific B cells | ||
| SARS-CoV-2-specific tetramers | [70,81,87,97,220] | - |
| SARS-CoV-2-specific T-cells | ||
| AIMS (cell surface + intracellular cytokines) | [76,83,91,100,110,124] | - |
| Intracellular cytokine staining | [89,93,121,133] | - |
| Interferon-y ELISA | [85,86,98,99,123] | - |
| Interferon-y ELISPOT | [70,73,76,81,83,89,97,120,125,134] | - |
| Whole blood IGRA | [71,96,112] | - |
| Tetramers/multimers pMHCI |
[121] |
|
| pMHCII | [87] | |
AIMS, Activation induced markers; DNBSEQ, DNA nanoballs sequencing; Elia, Enzyme fluoroimmunoassay; ELISA, Enzyme-Linked Immunosorbent Assay; ELISPOT, Enzyme-linked immunosorbent spot; IgG, Immunoglobulin G; IGRA, IFN-γ release assay; pMHCI, peptide major histocompatibility complex I; pMHCII, peptide major histocompatibility complex I; SARS-CoV-2, Severe Acute Respiratory Syndrome Coronavirus-2.
Table 3.
Adjunctive therapies for prophylaxis or treatment of SARS-CoV-2 infection.
| Monoclonal | Polyclonal | ||
| Example | Evusheld (AZD7442) | Xevudy (sotrovimab) | IgRT (IVIg or SCIg) |
| Company | AstraZeneca | VUR Biotechnology GlaxoSmithKline | Various |
| Pre or Post Exposure Prophylaxis | Pre | Post | N/A |
| Antibody Isotype | Hu IgG1κ | Hu IgG1κ | Various |
| SARS-CoV-2 Target | RBD | RBD | Broad range including NCP and RBD |
| Origin/Platform | Isolated from B cells of convalescent patients | Natural antibody from convalescent patient with SARS-CoV-2 | Purified antibodies from plasma of >1000 donors/product batch |
| Half life | ~6months | LS mutation of Fc increases half life | ~28 days |
| Doses required | 1* | 1 | ongoing |
| Dosage | 150mg of tixagevimab + 150mg cilgavimab |
500mg | Dependent on factors including weight and IgG trough levels |
| Frequency of redosing | Every 6 months | N/A | Every week to every month depending on IgG trough levels |
| Route of Administration | IM | IV | IV or SC |
| Approved recipients Age COVID-19 exposure Clinical disease |
>12 years weighing at least 40kg Not infected and no recent exposure Moderate to severe immunocompromised state |
>12 years weighing at least 40kg COVID-19+ PCR Moderate to severe immunocompromised state |
Dependent on established clinical guidelines |
| Neutralization Omicron BA.1 BA.2 |
344-fold decrease 9-fold decrease |
Unknown Unknown |
Unknown Unknown |
| Emergency Authorization US FDA Australian TGA |
12/21-1/23 11/21-1/22 |
05/21-3/22 08/21-3/22 |
N/A |
| Emergency approval for use in | Australia, UK and USA | Australia, UK and EU | N/A |
| References | [221,222,223] | [52,222,224,225] | [136] |
COVID-19, coronavirus 19; FDA, Food and Drugs Administration; Hu, human; IgRT, Immunoglobulin Replacement Therapy; IM, Intramuscular; IVIg, Intravenous Immunoglobulin; Subcutaneous Immunoglobulin, SCIg; N/A, not applicable; Nucleoprotein, NCP; Receptor binding-domain, RBD; Severe acute respiratory coronavirus-2, SARS-CoV-2; TGA, Therapeutic Goods Administration. (*Dose increased to 300mg each antibody in 12/22 due to emergence of Omicron BA.1 and BA.1.1 [226])
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



