
Submitted:
21 March 2024
Posted:
22 March 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Introduction: The emergency of the SARS-CoV-2 virus spread and its subsequent global pan-demic have raised significant concerns regarding its impact on pregnancy outcomes. This review aims to summarize the emerging data on the risk of preterm delivery in pregnant women infected with SARS-CoV-2.
Materials and Methods: A systematic search was conducted from March 2020 to December 2023 using PubMed, following PRISMA guidelines. Studies correlating maternal COVID-19 infection with preterm birth were included.
Results: Thirteen studies were analyzed, indicating a higher incidence of preterm birth in SARS-CoV-2 positive pregnant women compared to controls. The average incidence rate of pre-term birth in infected patients was 18.5%, with a median of 12.75%, while non infected women showed an average incidence of preterm birth of 10% with a median of 8.2%.
Discussion: Studies suggest an association between SARS-CoV-2 infection during pregnancy and increased risk of preterm birth and cesarean section. Severity of symptoms and underlying comorbidities further elevate this risk. Notably, infections during the third trimester pose the highest risk of preterm birth.
Conclusion: Preventing SARS-CoV-2 infection during pregnancy is crucial to mitigate adverse obstetric outcomes. Close monitoring and tailored interventions for infected pregnant women, particularly those in later trimesters and with comorbidities, are imperative to reduce the risk of preterm birth and improve maternal-fetal outcomes.
Keywords:
SARS-CoV-2
; COVID-19
; preterm birth
; pregnancy outcomes
; obstetric outcomes
1. Introduction
SARS-CoV-2 infection has given rise to a global pandemic in 2020, infecting about 700 million people of all age groups and causing about 6.5 million deaths. The infected population is evenly distributed across age groups, with a broad involvement of pregnant women. An increase in preterm deliveries in pregnant women infected by the virus was registered from several working groups. In fact, more preterm births (PTB) have been reported in pregnant women infected with SARS-CoV-2 (14%-25%), especially in high-income countries [1,2,3,4,5]. One of the main reasons why the preterm delivery showed a higher incidence in infected women was the occurrence of severe maternal respiratory infections such that the fetus had to be extracted to safeguard the health of the mother [6,7,8]. However, a retrospective analysis was conducted in France that demonstrated a high incidence of spontaneous preterm delivery in pregnant women infected with SARS-CoV-2 [9]. The objective of our review was to summarize emerging data on the risk of preterm delivery in pregnant women with infection. An online search from 20th March 2020 to 8th December 2023 was conducted, in order to identify studies about pregnancy outcome in women infected with SARS-CoV-2. The search strategy was implemented according to PRISMA guidelines, in order to conduct an adequate review of published studies. By examining a wide range of studies, this review provides a look at the correlation between Sars-Cov-2 infection and PTB.
2. Materials and Methods
A search on PubMed was carried out with the following keywords: "preterm birth" and "Covid19 infection". All articles published from March 2020 to December 2023 that reflected the following eligibility criteria were included: correlation studies between maternal Covid-19 infection and PTB, article written in English. Review and meta-analysis articles have been excluded, to exclude the risk of including the same study multiple times in this review.
The protocol for this review was prepared using the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) guidelines.
The study selection process is shown in Figure 1. Three independent reviewers reviewed the titles and abstracts of the articles. Of the 114 articles found, 13 were selected that met the inclusion criteria. Studies were included only if the following criteria were met: case-control, comparative or cohort retrospective studies, cohort studies, cross-sectional studies, prospective observational studies, conducted in human participants, available in English. We included studies that measured exposure to Sars-Cov2 infection, by rapid antigen test or molecular polymerase chain reaction (PCR) test, and that had PTB as their primary or secondary outcome. Many articles investigating the incidence of PTB during the Covid era were excluded, as the goal of our study was to investigate the exposure-outcome correlation.
Three investigators (G.P, A.S, M.B) worked independently to extract data from the selected articles. Data were collected in Table 1. In particular, data on the prevalence of PTB in women with Sars-Cov2 infection and the prevalence of PTB in control groups were extracted. All the studies under review based the diagnosis of Sars-Cov2 infection on the result of the PCR-test or antigen test. In addition, all articles considered PTB to have occurred before 37 weeks, as defined by the World Health Organization (WHO).
We also conducted a correlation study, calculating the Pearson coefficient.
3. Results
A total of 13 studies were selected. From these studies, data on the incidence of PTB in enrolled patients with Sars-Cov-2 infection in pregnancy (diagnosed by PCR-test or antigen test) were extracted and compared with the control groups of each study.
Figure 1 shows the incidence rates of PTB in pregnant Sars-Cov-2 infected patients for each study. On average, the incidence rate of PTB in the Sars-Cov-2 positive class of patients is 18.5%, with a median of 12.75%. The relationship coefficient calculated using Pearson's formula was 0.97. In the control groups (patients without Sars-Cov-2 infection), the incidence of PTB averaged 10%, with a median of 8.2%.
All the considered studies suggest that patients with Sars-Cov-2 infection are more likely to experience PTB than women who do not have such an infection.
Some limiting factors could be: the accidental inclusion of patients in the paucisymptomatic control groups and with a false negative test for Covid-19, the small sample size in some cases, not all studies included stillbirth in their outcomes (underestimating an important adverse outcome).
All studies obtained similar results, regardless of the country in which they took place, showing a concordance of results, regardless of geographical area and/or socio-economic characteristics.
For example, a hospital-based retrospective analysis carried out in Mumbai, India, demonstrated a high rate of PTB in pregnancies with Covid-19 infection, as well as a higher rate of maternal complications requiring ICU access [10]. Similarly, a multicenter case-control study confirmed the same finding in the United States [11].
Numerous studies have shown that the rate of PTB in patients with Sars-Cov-2 infection is more represented by medically indicated induced delivery for unfavorable maternal or fetal conditions.
Ferrara A. et al report in their study a percentage of iatrogenic PTB in the women of the study group equal to 62.24% versus 37.76% of spontaneous PTB [12]. Other studies also confirm these data, noting that the severity of Covid-19 infection or the presence of associated complications significantly affects iatrogenic PTB. Bahado et al in their multicenter study point out that a significant number of iatrogenic PTBs in the control group are due to preeclampsia, particularly in women with symptomatic Covid-19 (11%) compared to 7.4% of iatrogenic PTB for other causes in Covid-19 patients [11].
Another study conducted by Smith et al [13] highlights how symptomatic forms of Sars-Cov-2 are more at risk of iatrogenic PTB than mild/moderate forms, with prevalence rates of asymptomatic forms almost comparable to Covid negative patients. However, the total prevalence of iatrogenic PTB in the study group was 38% compared to 61.84% for spontaneous PTB. This data suggest that it is not only maternal clinical conditions and complications of Covid-19 that determine medical indication for delivery, but that evidently the very effect of Sars-Cov-2 infection induces the onset of spontaneous labor/pPROM.
Among the most common symptoms that have necessitated iatrogenic delivery are: respiratory distress, severe pulmonary involvement, need for oxygen therapy, preeclampsia, deep vein thrombosis, tachypnea, hypoxia, intravascular coagulopathy, pulmonary edema, and the need for mechanical ventilation [11,13,14,15,16,17]. Severe COVID-19 contracted late in pregnancy may significantly increase the risk of preterm delivery, predominantly through medically indicated preterm deliveries, but also potentially affecting spontaneous PTB rates [13].
A study conducted by Bahado et al. [11] demonstrated that there is a dose-response relationship between COVID-19 disease severity and gestational age at delivery. The study found that women with more severe COVID-19 disease tended to deliver earlier, and medically-indicated PTB, primarily caused by preeclampsia, were major contributors to the higher rate of prematurity in COVID-19 cases.
Data that emerged from some studies is interesting. According to these studies, the highest probability of PTB is associated with Sars-Cov-2 infection during the third trimester of pregnancy. The risk is particularly high within the first four days of infection [18,19]. In the study by Darling et al., the authors found that infections during the second trimester increased the risk for provider-initiated PTB, whereas infections during the third trimester increased the risk for both subtypes of PTB [20].
According to the study conducted by Bobei et al., certain laboratory indices may increase the risk of PTB in pregnant women who are also positive for Covid. The study highlights that high levels of CRP and low levels of lymphocytes are considered to be risk factors for PTB [18].
Research has shown that pregnant women who have contracted Sars-Cov-2 are at a higher risk of requiring a cesarean section, particularly if they are experiencing fetal distress or maternal and respiratory complications. Studies have confirmed that women with Covid-19 symptoms are more likely to undergo cesarean sections [8,15,18,21,22]. One study found that the cesarean rate in the Sars-Cov-2 group was 82%, compared to 6% in the control group. Most cesareans were due to fetal distress, worsening of maternal symptoms, or dystocia in labor. Additionally, the severity of Covid-19 symptoms has been observed to increase the rate of cesarean sections [18].
Similarly, in a study by Epelboin [9], the percentage of cesarean sections in the study group was 33%, which was higher than the control group's 20.2%. The observational cohort study conducted by Metz et al [15]confirms the trend of increased risk of cesarean delivery in pregnant women with Covid-19. The percentage of cesarean sections in the Covid-19 positive group was 59.6%, compared to 34% in the control group (aRR 1.57). According to a multinational prospective observational cohort study carried out by Giuliani et al [8], newborns born by caesarean section to women who test positive for Sars-Cov-2 are more vulnerable to acquiring the infection. The study provides compelling evidence to support this claim, highlighting the potential risks associated with caesarean delivery in such cases.
The neonatal outcomes reported in various studies included in this review reveal disparities. Mahajan et al. [10] observed no significant differences in neonatal’s Apgar score and birth weight between the study and control groups. Likewise, Trahan's study [16] found no major differences in obstetrical and newborn outcomes associated with SARS-CoV-2 when compared to uninfected patients.
On the other hand, Bobei's [18] study reported that severe maternal symptoms such as respiratory distress had an adverse impact on newborn outcomes (p = 0.001). Additionally, Giuliani's study [15] showed that the length of in utero exposure to COVID-19 had a direct correlation with the risk of newborns testing positive for the virus. Furthermore, when newborns born to COVID-19 positive mothers also tested positive, they had worse outcomes, including higher rates of NICU admission, fever, gastrointestinal and respiratory symptoms, and even death (after adjusting for prematurity). Respiratory signs and NICU admission were also more prevalent among newborns born to all women with COVID-19 diagnosis. These findings demonstrate a direct impact of maternal COVID-19 infection on newborns, independent of neonatal test results.
Vouga et al [24] highlight with their study an 8-11% occurrence of severe outcomes in infected pregnant women, a rate which surpasses the general population at a similar age. Vascular and hemodynamic changes, alongside altered immunity and reduced respiratory capacity in pregnant women, contribute significantly to these outcomes. Moreover, the potential of vertical transmission from mother to fetus/newborn cannot be overlooked, with instances of placental infection raising concerns for the unborn child's health.
The study of Blitz et. AL compared the rate of PTBs in women with symptomatic or asymptomatic coronavirus infection. Specifically, adjusting for maternal age, race-ethnicity, parity, history of PTB, body mass index, marital status, medical co-morbidities, month of delivery, and pandemic wave, it was seen that patients with symptomatic COVID-19 at the time of delivery had a higher risk of PTB (19.0%) compared to women with asymptomatic infection (8.8%) or no infection (7.1%). [25]
Finally, in the article by Gulersen et al. [26] it was seen that, during the Omicron wave, SARS-CoV-2 infection in pregnancy has been associated with an increased risk of PTB compared to uninfected cases. This risk has not been changed by vaccination or the status of the SARS-CoV-2 antibodies in subgroup analyses. Although the association between SARS-CoV-2 infection and PTB was well characterized during the early part of the COVID-19 pandemic, the risk of PTB also increased during the most advanced phase of the pandemic. These results confirm that SARS-CoV-2 infection in pregnancy is a risk factor for PTB, despite evidence of lower virulence of emerging variants. [26]
Data emerging from all studies suggest that symptomatic Sars-Cov-2 infection during pregnancy is associated with increased maternal morbidity and negative maternal outcomes. In particular, infected women have a higher risk of being admitted to the ICU, developing complications such as preeclampsia, hypertensive disorders, coagulation disorders, DIC, respiratory failure, shock, organ failure [10,11,15,17,23].
4. Discussion
Two questions about pregnant women have arisen because of previous viral epidemics:
Is there a risk associated with COVID-19 for expectant mothers? Is this risk increased by the entity of symptoms or underlying health conditions? This review aimed to address the question of whether COVID-19 is associated with risk of adverse obstetrical outcomes among pregnant women, in particular with increased risk of spontaneous or induced PTB and cesarean section, considering also that the rate of cesarean section is challenging in current obstetrical panorama [27].
Many investigations have examined the relationship between PTB rates and Sars-Cov-2 infection during pregnancy, and there are also many case reports that testify the correlation between severe maternal illness and iatrogenic PTB [28]. While some studies have not yet attained statistic levels of significance, all of these research concur that there is a strong association between the two occurrences, and other review studies corroborate this finding. This correlation seems to be present not only between primary Covid-19 infection and the risk of PTB, but also between the severity of infectious symptoms and the risk of caesarean section [5,12,18,21]. Various comparative studies have made it possible to effectively correlate populations of symptomatic and paucisymptomatic infected pregnant women with uninfected pregnant women, providing data on the correlation between symptom severity and the overall risk of PTB. In fact, it was shown that paucisymptomatic or asymptomatic patients reflected a lower risk of both PTB and caesarean section. Moreover, a recent study showed a statistically significant difference in birth weight between symptomatic and asymptomatic pregnant women [29]. All this may be related to the association between symptom severity and organ damage, mainly of a vascular and respiratory nature, resulting from covid 19 infection [13,20].
In particular, some authors have analyzed and highlighted, with statistically significant results, data relating to the primary cause determining the decision for caesarean section in patients with primary COVID 19 infection. The main cause would be preeclampsia not only for cesarean section but also for medical induced PTB, only secondarily would be fetal compromise and respiratory complications [19,30].
Not of secondary importance is the investigation of the underlying conditions of the pregnant patient affected by symptomatic COVID 19 infection. In fact, an increased risk of both spontaneous or induced PTB and cesarean section has been shown in patients with multiple underlying comorbidities. Thus, the overall risk factor for preterm delivery and cesarean section is not only determined by the intensity of the infection's symptoms, but also by the general health and underlying pathologies of the pregnant patient who is infected. Consistently, increased maternal age, high BMI, chronic hypertension, high cholesterole levels, preexisting diabetes were reported to be associated with severe COVID-19 in pregnant women, and preexisting maternal comorbidity described as a risk factor for admission to an ICU and invasive ventilation [22].
Notably, the highest incidence of PTB occurred within the first four-thirty days following a positive PCR test for SARS-CoV-2. Furthermore, an inverse correlation was found between lymphocyte count and the symptom severity of Covid-19, as well as the need for preterm delivery. Similarly, elevated inflammation indices, such as C-reactive protein (CRP), increased the likelihood of PTB. These findings may inform clinical practice by enabling healthcare professionals to proactively mitigate risk factors for PTB in pregnant women with Covid-19. Researchers in Massachusetts [20] conducted a study that specifically examined the relationship between exposure time to Sars-Cov-2 and the onset of PTB, with similar results. Elevated hazard ratios were observed for both types of PTB when infections were detected within 3 days of delivery or, although with a slightly reduced risk, between 4 and 30 days of delivery. In addition, it has revealed that the timing of contracting Sars-Cov-2 infection during pregnancy can have an impact on the risk of PTB. Specifically, if the infection occurs during the second trimester of pregnancy, it is associated with a higher risk of medically induced PTB. However, if the infection occurs during the third trimester, the risk of PTB is the same for both spontaneous and medically induced PTB.
Even if various studies suggest that Covid-related maternal complications are the primary factor contributing to a significant increase in premature births, it is crucial to recognize that the risk of spontaneous PTB should not be disregarded. Actually, the incidence of premature rupture of membranes (PROM) in this population is roughly twice as high as that in the general population [31].
The current body of research suggests that the adverse effects of Covid19 on pregnancy, such as PTB and adverse maternal and fetal outcomes, may be attributed to a significant immunological dysregulation. Studies have shown that CRP and lymphocyte counts are important risk factors for PTB, providing further evidence to support this observation.
Unique maternal immune responses to SARS-CoV-2 have been observed, with altered inflammatory responses, such as increased levels of various interleukins (IL-8, IL-6, IL-10, IL-15) in the blood. IL-6, in particular, may be a biomarker for predicting disease severity and prognosis. The immune system undergoes various changes that lead to a high inflammatory state. This state can be responsible for several adverse events, including preeclampsia. It's worth noting that Covid-19 infection also causes a hyperinflammatory state that damages the endothelial cells, similar to what happens in preeclampsia. This may be why preeclampsia is a common complication in Covid-19 patients [32].
In light of all the evidence emerging from this review, it is mandatory to prevent adverse outcomes due to Sars-Cov-2 infection. The first step in this direction is undoubtedly vaccination, to prevent serious complications from Covid19 in pregnant women. Since the spread of SARS-CoV2 infection, there has been a great hesitancy about vaccination among pregnant women. In the study of Maranto et al., about a third of pregnant women were still hesitant about the anti-SARS-CoV2 vaccine, probably because conflicting information received from media, friends and health institutions [33]. However, an Italian survey conducted by Cavaliere et al. demonstrated that COVID-19 experience raised the awareness to the role of vaccines in pregnancy, such as flu and Tdap (Tetanus, diphtheria, acellular pertussis) vaccination [34], and the common data among many studies is that vaccination hesitancy can be minimized through healthcare providers vaccine advice [33,35]. A recent review has highlighted the effects of anti-Sars-Cov-2 vaccines. The conclusion drawn from the study is that getting a COVID-19 vaccination while pregnant doesn't significantly increase the risk of PTB. This information is crucial in providing reassurance to healthcare providers and pregnant women regarding the safety of COVID-19 vaccines. It reinforces their use in public health strategies, particularly since COVID-19 infection during pregnancy has been shown to increase the risk of PTB and severe illness [36].
Leading scientific societies have conflicting indications on the use of Coronavirus drugs in pregnancy. In particular, a review by Chourasia et al. on the use of Paxlovid showed that although human studies are promising, their number is too few. [37]
Further studies are needed to determine whether patients with Sars-Cov-2 infection can benefit from fetal-safe antiretroviral therapy to prevent complications such as preterm delivery, vertical transmission, and the onset of severe maternal symptoms. Previous studies for other maternal viral infections, such as HIV, have shown positive results for maternal and fetal health, highlighting how multidisciplinary management and increasingly personalised therapy can improve maternal-fetal outcomes. [38]
Another interesting question concerns the vertical transmission (VT) of Sars-Cov-2. Various studies demonstrate in utero fetal and placental infections and possible vertical and/or horizontal viral transfer to the newborn detected among women with nasal SARS-CoV-2 infection. This could corroborate the thesis of a hypothetical chorio-placental damage by the virus such as to favor unfavorable obstetric outcomes [5,19,21,22].
The study of the placentas of women infected with Covid does not show unambiguous data on the possibility of vertical transmission of the virus. Several studies have analyzed the placenta, amniotic fluid and umbilical cord to evaluate the transmission of the virus, but the data obtained are conflicting, which is why it is not justified to schedule a cesarean section in this class of women if there are no other obstetric or clinical reasons that make it necessary. [36]. A systematic review noted that the risk of VT and its effects can be influenced by the timing during pregnancy. According to studies, earlier viral infections, such as those contracted during the first and second trimesters, can have more serious consequences. Another recent review also found that the transmission rate from mother to neonate was relatively low, with an estimated rate of 3.2%. The authors concluded that while vertical transmission of COVID-19 is possible, it appears to be rare and the majority of neonates have a favorable prognosis. Moreover, it has been demonstrated that newborns “inherit” passive immunity from mothers infected by SARS-CoV2 during pregnancy through the transplacental transfer of specific IgG [39,40], and this may represent an important mechanism that protects the neonate.
Considering the lack of data about neonatal consequences, it has been recommended for a long time (and in some countries it is still done today) to test pregnant women admitted for delivery [41]. Thanks to the screening test, the organization of dedicated pathways for pregnant women and a good local territorial health management of pregnancy, some realities contributed to a containment of the spread of SARS-CoV2 in pregnant women [42].
As with other recent epidemics [43] it is crucial to know the key aspects of this disease to ensure early diagnosis and to further improve management strategies for this disease.
5. Conclusions
Lastly, the findings of this literature review highlight the importance of first preventing Sars-Cov-2 infection during pregnancy, to avoid all the related unfavorable outcomes. Pregnant patients infected with the virus must be monitored closely, especially if they contracted the infection in the second or third trimester and even more so if they have important risk factors for Sars-Cov-2 complications in their clinical history. Attention must be paid to the management of the infection to prevent a worsening of the symptoms and consequently limit the risk of PTB, whether spontaneous or induced. Understanding the mediating factors such as maternal comorbidities, cytokine dysregulation, and placental pathology is crucial for the development of targeted interventions and tailored antenatal care strategies.
Author Contributions
Conceptualization, A.F.C. and G.C.; Methodology, V.G. and R.F. ; Software, A.S.; Validation, F.P. and A.V.; Formal Analysis, G.P.; Investigation, G.P. and A.S.; Resources, M.B.; Data Curation, M.P.; Writing – Original Draft Preparation, G.P., M.B., A.S., A.S., A.L.; Writing – Review & Editing, F.P., V.G and A.V.; Visualization, G.G.; Supervision, F.P., G.G., A.F.C., G.C.; Project Administration, G.C and A.F.C.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The original data presented in the study are available on PubMed.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Knight M, Bunch K, Vousden N, et al. Characteristics and outcomes of pregnant women admitted to hospital with confirmed SARS- CoV-2 infection in UK: national population based cohort study. BMJ. 2020;369:m2107. [CrossRef]
- Martinez-Perez, O., Prats Rodriguez, P., Muner Hernandez, M., Encinas Pardilla, M. B., Perez Perez, N., Vila Hernandez, M. R., Villalba Yarza, A., Nieto Velasco, O., Del Barrio Fernandez, P. G., Forcen Acebal, L., Orizales Lago, C. M., Martinez Varea, A., Muñoz Abellana, B., Suarez Arana, M., Fuentes Ricoy, L., Martinez Diago, C., Janeiro Freire, M. J., Alférez Alvarez-Mallo, M., Casanova Pedraz, C., Alomar Mateu, O., Spanish Obstetric Emergency Group (2021). The association between SARS-CoV-2 infection and preterm delivery: a prospective study with a multivariable analysis. BMC pregnancy and childbirth, 21(1), 273. [CrossRef]
- Al-Matary, A., Almatari, F., Al-Matary, M., AlDhaefi, A., Alqahtani, M. H. S., Alhulaimi, E. A., AlOtaiby, S., Almehiny, K., John, L. S., Alanazi, F. S., Ali, A. M., & Aldandan, F. K. (2021). Clinical outcomes of maternal and neonate with COVID-19 infection - Multicenter study in Saudi Arabia. Journal of infection and public health, 14(6), 702–708. [CrossRef]
- Ayed, A., Embaireeg, A., Benawadh, A., Al-Fouzan, W., Hammoud, M., Al-Hathal, M., Alzaydai, A., Ahmad, A., & Ayed, M. Maternal and perinatal characteristics and outcomes of pregnancies complicated with COVID-19 in Kuwait. BMC pregnancy and childbirth. BMC Pregnancy Childbirth. 2020 Dec 2;20(1):754. [CrossRef]
- Figueiro-Filho EA, Yudin M, Farine D. COVID-19 during pregnancy: an overview of maternal characteristics, clinical symptoms, mater- nal and neonatal outcomes of 10,996 cases described in 15 coun- tries. J Perinat Med. 2020;48:900-911. [CrossRef]
- Allotey, J., Chatterjee, S., Kew, T., Gaetano, A., Stallings, E., Fernández-García, S., Yap, M., Sheikh, J., Lawson, H., Coomar, D., Dixit, A., Zhou, D., Balaji, R., Littmoden, M., King, Y., Debenham, L., Llavall, A. C., Ansari, K., Sandhu, G., Banjoko, A., PregCOV-19 Living Systematic Review Consortium (2022). SARS-CoV-2 positivity in offspring and timing of mother-to-child transmission: living systematic review and meta-analysis. BMJ 2022 Mar 16:376:e067696. [CrossRef]
- Wang, H., Li, N., Sun, C., Guo, X., Su, W., Song, Q., Liang, Q., Liang, M., Ding, X., Lowe, S., Bentley, R., & Sun, Y. (2022). The association between pregnancy and COVID-19: A systematic review and meta-analysis. The American journal of emergency medicine, 56, 188–195. [CrossRef]
- McClymont, E., Albert, A. Y., Alton, G. D., Boucoiran, I., Castillo, E., Fell, D. B., Kuret, V., Poliquin, V., Reeve, T., Scott, H., Sprague, A. E., Carson, G., Cassell, K., Crane, J., Elwood, C., Joynt, C., Murphy, P., Murphy-Kaulbeck, L., Saunders, S., Shah, P., CANCOVID-Preg Team (2022). Association of SARS-CoV-2 Infection During Pregnancy With Maternal and Perinatal Outcomes. JAMA, 327(20), 1983–1991. [CrossRef]
- Epelboin, S., Labrosse, J., De Mouzon, J., Fauque, P., Gervoise-Boyer, M. J., Levy, R., Sermondade, N., Hesters, L., Bergère, M., Devienne, C., Jonveaux, P., Ghosn, J., & Pessione, F. (2021). Obstetrical outcomes and maternal morbidities associated with COVID-19 in pregnant women in France: A national retrospective cohort study. PLoS medicine, 18(11), e1003857. [CrossRef]
- Mahajan NN, Pednekar R, Gaikwad C, More P, Pophalkar M, Kesarwani S, Jnanananda B, Mahale SD, Gajbhiye RK. Increased spontaneous preterm births during the second wave of the coronavirus disease 2019 pandemic in India. Int J Gynaecol Obstet. 2022 Apr;157(1):115-120. Epub 2021 Nov 5. PMID: 34674259; PMCID: PMC9087695. [CrossRef]
- Bahado-Singh, R., Tarca, A. L., Hasbini, Y. G., Sokol, R. J., Keerthy, M., Goyert, G., Jones, T., Thiel, L., Green, P., Youssef, Y., Townsel, C., Vengalil, S., Paladino, P., Wright, A., Ayyash, M., Vadlamud, G., Szymanska, M., Sajja, S., Turkoglu, O., Sterenberg, G. Southern Michigan Regional COVID-19 Collaborative (2023). Maternal SARS-COV-2 infection and prematurity: the Southern Michigan COVID-19 collaborative. The journal of maternal-fetal & neonatal medicine : the official journal of the European Association of Perinatal Medicine, the Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstetricians, 36(1), 2199343. [CrossRef]
- Ferrara, A., Hedderson, M. M., Zhu, Y., Avalos, L. A., Kuzniewicz, M. W., Myers, L. C., Ngo, A. L., Gunderson, E. P., Ritchie, J. L., Quesenberry, C. P., & Greenberg, M. (2022). Perinatal Complications in Individuals in California With or Without SARS-CoV-2 Infection During Pregnancy. JAMA internal medicine, 182(5), 503–512. [CrossRef]
- Smith LH, Dollinger CY, VanderWeele TJ, Wyszynski DF, Hernández-Díaz S. Timing and severity of COVID-19 during pregnancy and risk of preterm birth in the International Registry of Coronavirus Exposure in Pregnancy. BMC Pregnancy Childbirth. 2022;22(1):775. Published 2022 Oct 18. [CrossRef]
- Metz, T. D., Clifton, R. G., Hughes, B. L., Sandoval, G., Saade, G. R., Grobman, W. A., Manuck, T. A., Miodovnik, M., Sowles, A., Clark, K., Gyamfi-Bannerman, C., Mendez-Figueroa, H., Sehdev, H. M., Rouse, D. J., Tita, A. T. N., Bailit, J., Costantine, M. M., Simhan, H. N., Macones, G. A., & for the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) Maternal-Fetal Medicine Units (MFMU) Network (2021). Disease Severity and Perinatal Outcomes of Pregnant Patients With Coronavirus Disease 2019 (COVID-19). Obstetrics and gynecology, 137(4), 571–580. [CrossRef]
- Giuliani, F., Oros, D., Gunier, R. B., Deantoni, S., Rauch, S., Casale, R., Nieto, R., Bertino, E., Rego, A., Menis, C., Gravett, M. G., Candiani, M., Deruelle, P., García-May, P. K., Mhatre, M., Usman, M. A., Abd-Elsalam, S., Etuk, S., Napolitano, R., Liu, B., Villar, J. (2022). Effects of prenatal exposure to maternal COVID-19 and perinatal care on neonatal outcome: results from the INTERCOVID Multinational Cohort Study. American journal of obstetrics and gynecology, 227(3), 488.e1–488.e17. [CrossRef]
- Trahan, M. J., Malhamé, I., O'Farrell, P., Mitric, C., Desilets, J., Bastrash, M. P., El-Messidi, A., & Abenhaim, H. A. (2021). Obstetrical and Newborn Outcomes Among Patients With SARS-CoV-2 During Pregnancy. Journal of obstetrics and gynaecology Canada : JOGC = Journal d'obstetrique et gynecologie du Canada : JOGC, 43(7), 888–892.e1. [CrossRef]
- Cosma, S., Carosso, A. R., Cusato, J., Borella, F., Carosso, M., Gervasoni, F., Stura, I., Preti, M., Ghisetti, V., Di Perri, G., & Benedetto, C. (2021). Preterm birth is not associated with asymptomatic/mild SARS-CoV-2 infection per se: Pre-pregnancy state is what matters. PloS one, 16(8), e0254875. [CrossRef]
- Bobei, T. I., Haj Hamoud, B., Sima, R. M., Gorecki, G. P., Poenaru, M. O., Olaru, O. G., & Ples, L. (2022). The Impact of SARS-CoV-2 Infection on Premature Birth-Our Experience as COVID Center. Medicina (Kaunas, Lithuania), 58(5), 587. [CrossRef]
- Litman EA, Yin Y, Nelson SJ, Capbarat E, Kerchner D, Ahmadzia HK. Adverse perinatal outcomes in a large United States birth cohort during the COVID-19 pandemic. Am J Obstet Gynecol MFM. 2022;4(3):100577. [CrossRef]
- Darling AM, Shephard H, Nestoridi E, Manning SE, Yazdy MM. SARS-CoV-2 infection during pregnancy and preterm birth in Massachusetts from March 2020 through March 2021. Paediatr Perinat Epidemiol. 2023;37(2):93-103. [CrossRef]
- Binte Masud, S., Zebeen, F., Alam, D. W., Hossian, M., Zaman, S., Begum, R. A., Nabi, M. H., & Hawlader, M. D. H. (2021). Adverse Birth Outcomes Among Pregnant Women With and Without COVID-19: A Comparative Study From Bangladesh. Journal of preventive medicine and public health = Yebang Uihakhoe chi, 54(6), 422–430. [CrossRef]
- Mohanty, S., Tita, A. T., Varner, M., Stockwell, M. S., Newes-Adeyi, G., Battarbee, A. N., Reichle, L., Morrill, T., Daugherty, M., Mourad, M., Silverio Francisco, R. A., Woodworth, K., Wielgosz, K., Galang, R., Maniatis, P., Semenova, V., & Dawood, F. S. (2023). Association between SARS-CoV-2 infections during pregnancy and preterm live birth. Influenza and other respiratory viruses, 17(9), e13192. [CrossRef]
- Deruelle, P., & Sentilhes, L. (2021). Coronavirus disease 2019 in pregnancy was associated with maternal morbidity and preterm birth. American journal of obstetrics and gynecology, 224(5), 551. [CrossRef]
- Vouga, M., Favre, G., Martinez-Perez, O., Pomar, L., Acebal, L. F., Abascal-Saiz, A., Hernandez, M. R. V., Hcini, N., Lambert, V., Carles, G., Sichitiu, J., Salomon, L., Stirnemann, J., Ville, Y., de Tejada, B. M., Goncé, A., Hawkins-Villarreal, A., Castillo, K., Solsona, E. G., Trigo, L., Panchaud, A. (2021). Maternal outcomes and risk factors for COVID-19 severity among pregnant women. Scientific reports, 11(1), 13898. [CrossRef]
- Blitz MJ, Gerber RP, Gulersen M, Shan W, Rausch AC, Prasannan L, Meirowitz N, Rochelson B. Preterm birth among women with and without severe acute respiratory syndrome coronavirus 2 infection. Acta Obstet Gynecol Scand. 2021 Dec;100(12):2253-2259. [CrossRef]
- Gulersen M, Alvarez A, Rochelson B, Blitz MJ. Preterm birth and severe maternal morbidity associated with SARS-CoV-2 infection during the Omicron wave. Am J Obstet Gynecol MFM. 2022 Nov;4(6):100712. [CrossRef]
- Parasiliti M, Vidiri A, Perelli F, Scambia G, Lanzone A, Cavaliere AF. Cesarean section rate: navigating the gap between WHO recommended range and current obstetrical challenges. J Matern Fetal Neonatal Med. 2023 Dec;36(2):2284112. [CrossRef]
- Gullo G, Cucinella G, Tumminello M, Renda B, Donzelli M, Lo Bue V, Termini D, Maranto M, De Tommasi O, Tarantino F. Convalescent plasma use in pregnant patients with COVID-19 related ARDS: a case report and literature review. Italian JOG. Vol. 34 (No. 3) 2022 September, 228-234. [CrossRef]
- Maranto M, Zaami S, Restivo V, Termini D, Gangemi A, Tumminello M, Culmone S, Billone V, Cucinella G, Gullo G. Symptomatic COVID-19 in Pregnancy: Hospital Cohort Data between May 2020 and April 2021, Risk Factors and Medicolegal Implications. Diagnostics (Basel). 2023 Mar 7;13(6):1009. [CrossRef]
- Egloff C, Roques P, Picone O. Impact of COVID-19 on pregnant women's health: Consequences in obstetrics two years after the pandemic. J Reprod Immunol. 2023 Aug;158:103981. [CrossRef]
- Hudak, ML. Consequences of the SARS-CoV-2 pandemic in the perinatal period. Curr Opin Pediatr. 2021;33(2):181-187. [CrossRef]
- Uta M, Craina M, Marc F, Enatescu I. Assessing the Impact of COVID-19 Vaccination on Preterm Birth: A Systematic Review with Meta-Analysis. Vaccines. 2024; 12(1):102. [CrossRef]
- Maranto M, Gullo G, Bruno A, Minutolo G, Cucinella G, Maiorana A, Casuccio A, Restivo V. Factors Associated with Anti-SARS-CoV-2 Vaccine Acceptance among Pregnant Women: Data from Outpatient Women Experiencing High-Risk Pregnancy. Vaccines (Basel). 2023 Feb 16;11(2):454. [CrossRef]
- Cavaliere AF, Zaami S, Pallottini M, Perelli F, Vidiri A, Marinelli E, Straface G, Signore F, Scambia G, Marchi L. Flu and Tdap Maternal Immunization Hesitancy in Times of COVID-19: An Italian Survey on Multiethnic Sample. Vaccines (Basel). 2021 Sep 29;9(10):1107. [CrossRef]
- Vilca LM, Sarno L, Cesari E, Vidiri A, Antonazzo P, Ravennati F, Cavaliere AF, Guida M, Cetin I. Differences between influenza and pertussis vaccination uptake in pregnancy: a multi-center survey study in Italy. Eur J Public Health. 2021 Dec 1;31(6):1150-1157. [CrossRef]
- Al-Kuraishy HM, Al-Gareeb AI, Albezrah NKA, et al. Pregnancy and COVID-19: high or low risk of vertical transmission. Clin Exp Med. 2023;23(4):957-967. [CrossRef]
- Chourasia, P.; Maringanti, B.S.; Edwards-Fligner, M.; Gangu, K.; Bobba, A.; Sheikh, A.B.; Shekhar, R. Paxlovid (Nirmatrelvir and Ritonavir) Use in Pregnant and Lactating Woman: Current Evidence and Practice Guidelines—A Scoping Review. Vaccines 2023, 11, 107. [Google Scholar] [CrossRef] [PubMed]
- Pinnetti, Carmela; Tintoni, Mauro; Ammassari, Adriana; Tamburrini, Enrica; Bernardi, Stefania; Liuzzi, Giuseppina; Scambia, Giovanni; Perno, Carlo Federico; Floridia, Marco; Antinori, Andrea; Cavaliere, Anna Franca (2015). Successful prevention of HIV mother-to-child transmission with dolutegravir-based combination antiretroviral therapy in a vertically infected pregnant woman with multiclass highly drug-resistant HIV-1. AIDS, 29(18), 2534–2537. [CrossRef]
- Marchi L, Vidiri A, Fera EA, Pallottini M, Perelli F, Gardelli M, Brunelli T, Poggetto PD, Martelli E, Straface G, Signore F, Fusco I, Vasarri PL, Scambia G, Cavaliere AF. SARS-CoV-2 IgG "heritage" in newborn: A credit of maternal natural infection. J Med Virol. 2023 Jan;95(1):e28133. [CrossRef]
- Cavaliere AF, Marchi L, Aquilini D, Brunelli T, Vasarri PL. Passive immunity in newborn from SARS-CoV-2-infected mother. J Med Virol. 2021 Mar;93(3):1810-1813. [CrossRef]
- Cavaliere AF, Carabaneanu AI, Perelli F, Matarrese D, Brunelli T, Casprini P, Vasarri PL. Universal screening for SARS-CoV-2 in pregnant women admitted for delivery: how to manage antibody testing? J Matern Fetal Neonatal Med. 2022 Aug;35(15):3005-3006. [CrossRef]
- Cavaliere AF, Vasarri PL, Scatena E, Vidiri A, Santicchia MS, Bordoni Vicini I, Gardelli M, Bressan F, Matarrese D, Perelli F. SARS-CoV2 containment during pregnancy: single Center experience and the unique Chinese reality in Prato. Italian JOG. Vol. 32 (No. 3) 2020 September, 163-165. [CrossRef]
- Fratelli N, Prefumo F, Maggi C, Cavalli C, Sciarrone A, Garofalo A, Viora E, Vergani P, Ornaghi S, Betti M, Vaglio Tessitore I, Gullo, G.; Scaglione, M.; Cucinella, G.; Riva, A.; Coldebella, D.; Cavaliere, A.F.; Signore, F.; Buzzaccarini, G.; Spagnol, G.; Laganà, A.S.; et al. Congenital Zika Syndrome: Genetic Avenues for Diagnosis and Therapy, Possible Management and Long-Term Outcomes. J. Clin. Med. 2022, 11, 1351. [CrossRef]
Figure 1.
study selection process.
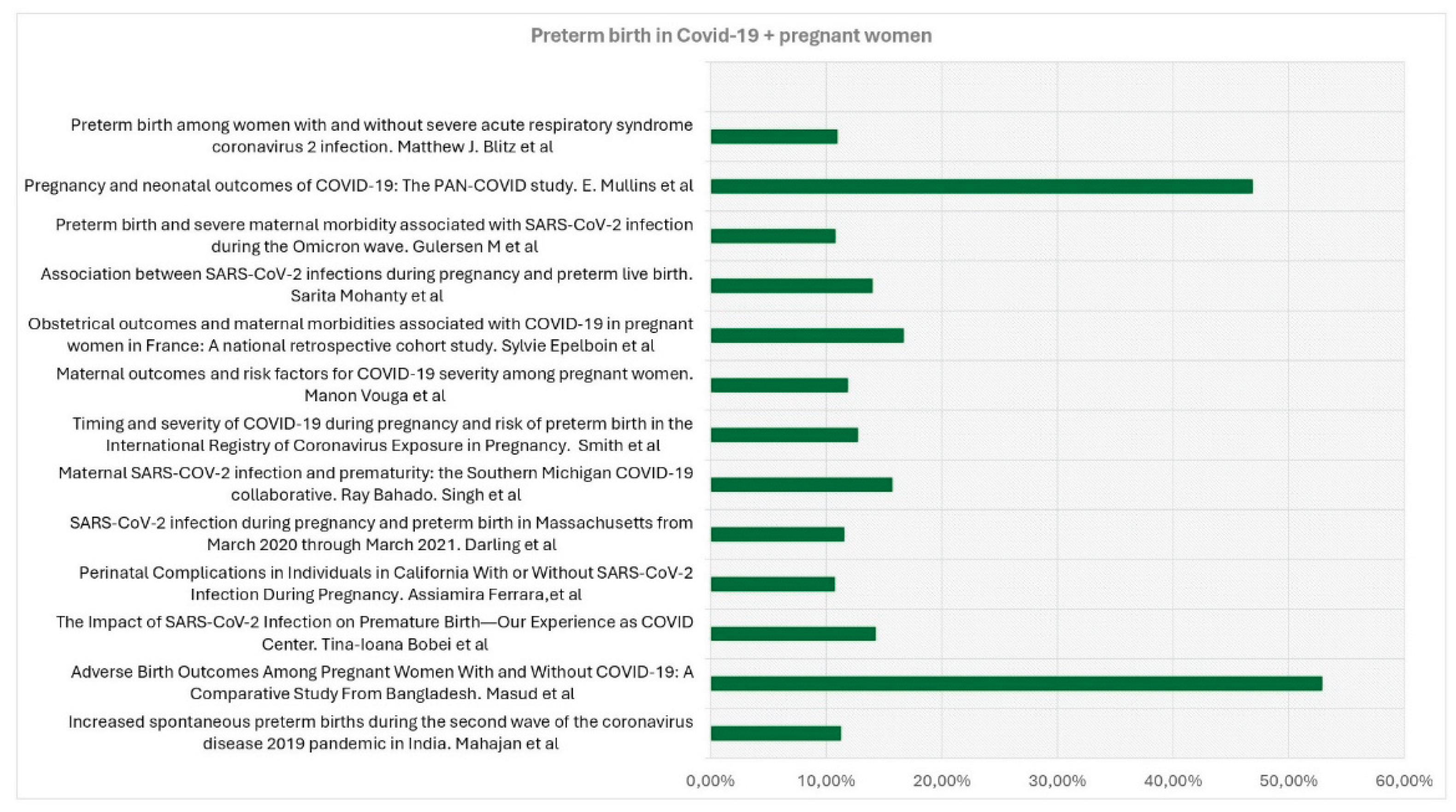

Table 1.
Collected Data.
| Title, Authors | Country, duration of observation | Type of Study | Aim of the study | Covid + patients | Covid - patients | Preterm birth in Covid+ patients | Preterm Birth in Covid- patients |
|---|---|---|---|---|---|---|---|
| Obstetrical outcomes and maternalmorbidities associated with COVID-19 inpregnant women in France: A nationalretrospective cohort study -Epelboin et al [9] | France. January to June 2020 | Prospective Cohort Multicentric Study | Investigation on whether maternal morbidities were more frequent in pregnant women with COVID-19 diagnosis compared to pregnant women without COVID- 19 diagnosis during the first wave of the COVID-19 pandemic. | 874 | 243771 | 146 (16.7%) | 17,215 (7.1%) |
| Increased spontaneous preterm births during the second wave of the coronavirus disease 2019 pandemic in India - Mahajan et al [10] | Covid hospital Mumbai, India. April 4, 2020 and July4, 2021. | Hospital-based, retrospective cohort study | To compare spontaneous preterm birth (SPTB) and iatrogenic preterm birth (IPTB) rates during both waves of the coronavirus disease 2019 (COVID-19)pandemic | 1136 | 3463 | 128 (11,3%)) | 259 (13.8%) |
| Maternal SARS-COV-2 infection and prematurity:the Southern Michigan COVID-19 collaborative - Bahado-Singh et al [11] | Michigan, USA, from March 2020 till October1st, 2020. | Multicentre case-control study | Determinate the impact of COVID-19 disease on PTB overall, as well as related subcategories such as early prematurity, spontaneous, medically indicated PTB, and preterm labor. | 369 | 1090 | 58 (15,72%) | 96 (8.81%) |
| Perinatal complications in Individuals in California With or Without SARS-CoV-2 Infection During Pregnancy - Ferrara et al [12] | Northern California, March 1, 2020, and March 16, 2021. | Cohort study | Examinate the risk for perinatal complications in pregnant individuals withSARS-CoV-2 infection. | 1332 | 42554 | 143 (10.74%) | 3438 (8.08%) |
| Timing and severity of COVID-19 during pregnancy and risk of preterm birth in the International Registry of CoronavirusExposure in Pregnancy - Smith et al [13] | USA. June 2020-July 2021 | International internet-based retrospective cohort study | Estimate the risk of PTB (overall, spontaneous, and indicated) after COVID-19 during pregnancy, while considering different levels of disease severity and timing. | 1192 | 4692 | 152 (12,75%) | 414 (8.82%) |
| Preterm birth is not associated withasymptomatic/mild SARS-CoV-2 infection per se: Pre-pregnancy state is what matters – Cosma et al [17] | Italy. 20 September 2020 and 9 January 2021. | Case-control study | To determine the real impact of asymptomatic/mild SARS-CoV-2 infection onPTB not due to maternal respiratory failure. | 53 | 176 | 21 (39,62%) | 81 (46,02%) |
| The Impact of SARS-CoV-2 Infection on Premature Birth—Our Experience as COVID Center - Bobei et al [18] | Romania. from March 2020 to June 2021 | Prospective observational study in a COVID-only hospital | Determination of the impact of SARS-CoV-2 infection on PTB pregnancies | 238 | 33 (14.28%) | 8.2% | |
| SARS-CoV-2 infection during pregnancy and preterm birth in Massachusetts from March 2020 through March 2021 - Darling et al [20] | Massachusetts , from 1 March 2020 to31 March 2021 | Retrospective cohort study | Examinate the association between SARS-CoV- 2 infection and spontaneous and provider-initiated PTB, and how timing of infection, andrace/ethnicity as a marker of structural inequality, may modify this association | 2195 | 66076 | 254 (11.57%) | 4655 (7.04%) |
| Adverse Birth Outcomes Among Pregnant Women With and Without COVID-19: A Comparative Study From Bangladesh - Masud et al [21] | Bangladesh, from March to August 2020 | Cross-sectional study | Compare birth outcomes related to COVID-19 between Bangladeshi pregnant women with and without COVID-19 | 70 | 140 | 37 (52,9%) | 42 (30.0%) |
| Association between SARS-CoV-2 infections during pregnancyand preterm live birth – Mohanty et al [22] | USA. August 2020–October 2021 | Prospective cohort study. | Examinate associations between mild or asymptomatic prenatal SARS-CoV-2 infection and preterm live birth | 185 | 769 | 26 (14%) | 97 (13%) |
| Maternal outcomes and risk factors for COVID-19 severity among pregnant women Vouga et al [24] | COVI-Preg internationalregistry. March 24 and July 26, 2020. | Retrospective comparative Monocentric | Insight into the maternal outcomes and risk factors associated with COVID-19 severity in pregnant women | 926 | 107 | 110 (11,88%) | 8% |
| Preterm birth among women with and without severe acute respiratory syndrome coronavirus 2 infection - Blitz et al [25] | New York City and Long Island. March 2020 and June 2021 | Retrospective cohort study | To establish potential risks determined by a COVID-19-positive pregnancy towards the mother and the newborn. | 1261 | 30289 | 138 (10,98%) | 2140 (6,78%) |
| Preterm birth and severe maternal morbidityassociated with SARS-CoV-2 infection duringthe Omicron wave - Gulersen M et al [26] | Nwe Tork. December 1, 2021 and February 7, 2022. | Retrospective cohort study | Evaluate the risk of PTB and severe maternal morbidity (SMM) in pregnant patients with SARS-CoV-2 infection during the most recent wave of the COVID-19 pandemic. | 631 | 4107 | 68 (10,8%) | 329 (8,0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



