Submitted:
11 March 2024
Posted:
11 March 2024
You are already at the latest version
Abstract
This study aimed to evaluate the effectiveness of an intensive care unit (ICU) round checklist, FAST HUGS BID (Feeding, Analgesia, Sedation, Thromboembolic prophylaxis, Head-of-bed elevation, Ulcer prophylaxis, Glycemic control, Spontaneous breathing trial, Bowel regimen, Indwelling catheter removal, and De-escalation of antibiotics) in improving clinical outcomes for patients with severe trauma. Patients admitted to our trauma ICU between 2016 and 2020 were retrospectively analyzed. We divided the participants into two groups: before (before-FD, 2016-2017) and after (after-FD, 2019-2020) the checklist's implementation. We compared patient characteristics and clinical outcomes, including ICU and hospital length of stay (LOS) and in-hospital mortality. Survival analysis was performed using Kaplan–Meier curves and multivariable logistic regression models, and multiple linear regression analysis was used to identify independent factors associated with ICU and hospital LOS. Compared with the before-FD group, the after-FD group had significantly lower in-hospital mortality and complication rates, shorter ICU and hospital LOS, and reduced duration of mechanical ventilation. revealed that the checklist's implementation was a significant independent factor in reducing ICU and hospital LOS and in-hospital mortality. In this before/after study, we observed that the FAST HUGS BID checklist implementation was associated with decreased ICU and hospital LOS and in-hospital mortality.
Keywords:
severe trauma
; outcomes
; checklist
; mortality
; implementation
; quality improvement
1. Introduction
Patients with severe trauma require intensive care unit (ICU) treatment for various complex injuries. However, the intricate nature of the treatment process in trauma care creates an environment prone to medical errors, often referred to as a "perfect storm." Such errors can arise from various factors, including unstable vital signs, incomplete patient histories, and insufficient information. In addition, trauma surgeons face the challenge of making time-critical decisions while simultaneously managing complex teams and collaborating with many disciplines [1]. When managing severely injured patients, trauma surgeons usually play a dual role as both surgical specialists and critical care providers, taking charge of all treatment processes. Therefore, trauma surgeons need to possess the necessary qualifications and capabilities in surgical critical care to manage their patients in the ICU. Moreover, ensuring a seamless continuity of management within the same quality of surgical service contributes to improved outcomes [2]. Furthermore, it is crucial for trauma surgeons to minimize medical errors and provide high-quality critical care, in addition to performing resuscitation in the trauma bay and conducting surgical procedures in the operating room.
Many studies have underscored the significance of appropriate physician staffing and the use of protocols, clinical practice guidelines, and checklists to improve clinical outcomes in modern ICUs [3,4,5]. In particular, some studies showed that the implementation of checklists for organized critical care in ICUs led to improved patients' outcomes [6,7]. In our trauma ICU (TICU), we recently adopted the Feeding, Analgesia, Sedation, Thromboembolic prophylaxis, Head-of-bed Elevation, Ulcer Prophylaxis, Glycemic Control, Spontaneous Breathing Trial, Bowel Regimen, Indwelling Catheter Removal, and De-escalation of antibiotics (FAST HUGS BID) checklist, which is easily remembered by simple mnemonics. This checklist was initially introduced as "FAST HUG" by Vincent in 2005 and later updated to "FAST HUGS BID" by Vincent III and Hatton in 2009 [8,9]. The FAST HUGS BID is a multidisciplinary protocol and checklist that includes essential and evolving components of evidence-based critical care.
In this study, we hypothesized that the implementation of the FAST HUGS BID checklist in the TICU could reduce in-hospital mortality and length of stay (LOS) in the ICU and hospital. Accordingly, we compared clinical outcomes before and after the implementation of the FAST HUGS BID checklist in our TICU. Furthermore, we performed a detailed analysis to assess the effectiveness of each checklist component before and after its implementation.
2. Materials and Methods
2.1. Study Procedure
This retrospective observational study was conducted for the patients admitted to the TICU at Ajou University Hospital from March 2016 to December 2020. Patients who were under 18 years of age, transferred from other hospitals, admitted to the general ward, or classified as immediate non-survivors upon arrival were not eligible for this study. After the exclusion, the patients included in final sample were then divided into two groups based on different time phases: before the implementation of the FAST HUGS BID checklist (before-FD) from March 2016 to December 2017 and after implementation (after-FD) from January 2019 to December 2020. The FAST HUGS BID checklist was implemented at our trauma center in mid-2018. We excluded patients admitted in 2018 because the FAST HUGS BID checklist was being refined through trial and error during that period. It is worth noting that the TICU at Ajou University Hospital operates as a semi-closed ICU, with dedicated trauma surgeons conducting bedside rounds more than twice daily. Furthermore, the FAST HUGS BID checklist was prominently displayed at each patient's bedside and applied to all ICU patients by the trauma staff, nurses, and other team members.
2.2. Definition and Study Outcomes
The FAST HUGS BID is a checklist that highlights the key factors in the general care of critically ill patients. This approach includes the following clinical practices: feeding, analgesia, sedation, thromboembolic prophylaxis, head-of-bed elevation, ulcer prophylaxis, glycemic control, spontaneous breathing trials, bowel regimens, indwelling catheters, and drug de-escalation.
The primary outcomes were the in-hospital mortality, overall complication rate, ICU LOS, hospital LOS, and duration of invasive mechanical ventilation. Secondary outcomes were the incidence of each complication, such as acute kidney injury, acute respiratory distress syndrome, pneumonia, venous thromboembolism, pressure ulcer, surgical site infection, urinary tract infection, catheter-related bloodstream infections, or sepsis. Additionally, we conducted a detailed analysis by comparing the impact of each component of the checklist before and after the intervention.
2.3. Statistical Analysis
Categorical variables were reported as proportions and compared before and after FD using the chi-squared test. Continuous variables were presented as means with standard deviations or medians with interquartile ranges. Continuous variables were compared between the two groups using Student's t-test for those with a normal distribution and the Mann-Whitney U test for those with a non-normal distribution. Kaplan-Meier curves and logistic regression models were employed to perform survival analysis. Multiple linear regression analysis was conducted to identify factors independently associated with ICU and hospital LOS. All variables with a p-value <0.1 in the univariable analysis were included in the multivariable model. The threshold for statistical significance was set at p < 0.05. Statistical analysis was carried out using SPSS 25.0 for Windows (SPSS, Inc., Chicago, IL, USA).
3. Results
3.1. Characteristics of Patients
We reviewed 13,278 patients admitted to the TICU during the study period and excluded 10,862 patients according to the criteria. Of the 2,416 patients included in the final sample, 696 and 1,720 were included in the before-FD and after-FD groups, respectively (Figure 1). Patient characteristics are summarized in Table 1. It was observed that patients in the after-FD group exhibited a higher prevalence of underlying diseases and a greater Injury Severity Score (ISS) than those in the before-FD group (P<0.05).
3.2. Primary Outcomes
Compared with the before-FD group, the after-FD group had lower in-hospital mortality (8.3% vs. 4.8%; P<0.05) and complication rates (23.0% vs. 16.5%; P<0.05). In addition, the after-FD group exhibited shorter ICU LOS (7.8 days vs. 5.1 days; P<0.05), hospital LOS (24.3 days vs. 17.6 days; P<0.05), and duration of invasive mechanical ventilation (9.2 days vs. 5.0 days; P<0.05) (Table 2).
3.3. Secondary Outcomes
The after-FD group had lower complication rates for pressure ulcers (10.9% vs. 5.7%; P<0.05), pneumonia (9.1% vs. 3.4%; P<0.05), and surgical site infections (4.3% vs. 1.3%; P<0.05) than the before-FD group. However, a higher incidence of sepsis was observed in the after-FD group than in the before-FD group (0.4% vs. 1.5%; P<0.05) (Table 3).
3.4. Comparisons of Each Component of the FAST HUGS BID Checklist
Each component of the checklist was compared between the before-FD and after-FD groups (Table 4). For Feeding, the after-FD group exhibited a faster time to the first start of enteral nutrition and greater body weight gain than the before-FD group (P<0.05). For Analgesia, the after-FD group had a shorter duration of intravenous (IV) fentanyl use, higher usage of IV nefopam, and increased use of per oral (PO) painkillers compared with the before-FD group (P<0.05). For Sedation, the after-FD group showed a lower rate of IV midazolam, IV propofol, and IV vecuronium use and a higher rate of IV dexmedetomidine use than the before-FD group (P <0.05). For Thromboembolic prophylaxis, the after-FD group had a higher rate of SC enoxaparin use and a shorter time to the first use of enoxaparin than the before-FD group (P<0.05). For Head-of-bed elevation, the after-FD group had a shorter time to the first start of head-of-bed elevation than the before-FD group (P<0.05). For Ulcer prophylaxis, the after-FD group exhibited a lower rate of ulcer medication and pantoprazole use than the before-FD group (P<0.05). For Spontaneous breathing trial, the after-FD group showed a shorter time to extubation and a higher rate of unplanned intubation events than the before-FD group (P<0.05). For Bowel regimen, the after-FD group demonstrated a lower rate of diarrhea than the before-FD group (P<0.05). For Indwelling catheter removal, the after-FD group showed a shorter time to central venous catheter removal and urinary catheter removal than the before-FD group (P<0.05). For Drug de-escalation, the after-FD group had a lower rate of restricted antimicrobial use and a shorter duration of antimicrobial use (P<0.05).
3.5. Factors Associated with In-hospital Mortality and LOS in the ICU and Hospital
Multivariable logistic regression analysis showed that the implementation of the FAST HUGS BID checklist was an independent contributing factor for in-hospital mortality (adjusted OR=0.434; P=0.008). Other factors associated with in-hospital mortality included the initial Glasgow Coma Scale (GCS), ISS, and complications (Table 5). The Kaplan-Meier curve for the comparison of the 90-days in-hospital mortality indicated that the after-FD group had a significantly higher survival rate than the before-FD group (P =0.002) (Figure 2).
In addition, multivariate linear regression analysis revealed that the implementation of the FAST HUGS BID checklist was an independent contributing factor for LOS in the ICU (B=-0.118; P <0.001) and hospital (B=-0.063; P =0.002). The initial GCS score, ISS, and complications were also found to be associated with ICU and hospital LOS (Table 6 and Table 7).
4. Discussion
In this study, we observed that the implementation of the FAST HUGS BID checklist improved the clinical outcomes of trauma patients in the ICU. Although patients with after-FD were characterized by higher severity of injuries, as indicated by a greater ISS, they exhibited lower rates of in-hospital mortality and complications, shorter ICU and hospital LOS, and reduced duration of invasive mechanical ventilation. Furthermore, multivariate logistic and linear regression analyses revealed that the implementation of the FAST HUGS BID checklist was an independent factor associated with shorter LOS in the TICU and hospital and lower in-hospital mortality.
The assertion that the implementation of the FAST HUGS BID checklist substantially affects the TICU population is well-supported by the following evidence. First, the implementation of the checklist resulted in a decrease in medical errors due to its concise and easily memorable format, which included the fundamental components of care involving all members of the trauma team. Second, the trauma team was able to make a care plan for each day and assess its completion using the checklist during daily ICU rounds. Several studies have endorsed our approach. For example, Stahl et al. showed that a structured checklist could reduce medical errors in the management of trauma patients [6], Barcellos et al. reported a reduction in the duration of mechanical ventilation and ICU stay with the implementation of a checklist [10], and Pronovost et al. revealed a decrease in the rate of catheter-related bloodstream infections through checklist utilization [11]. Additionally, some studies demonstrated a reduction in the rate of ventilator-associated pneumonia (VAP) following the use of a checklist [12,13], and Haynes et al. documented a decrease in mortality and complications following the implementation of a checklist during surgery [14,15].
Our literature review indicates a scarcity of comparative studies evaluating the impact of the FAST HUG or its updated version since its initial proposal by Vincent [8,9]. Those studies have primarily focused on comparing outcomes of specific diseases or individual components, such as VAP reduction. In contrast, in this study, we selected indicators that could assess the effect of each element within the FAST HUGS BID, collected data, and compared their applications. In addition, we specifically compared LOS in the ICU and hospital and in-hospital mortality using the Kaplan-Meier curve, which are considered quality indicators for critical care treatment. Furthermore, we employed multivariate logistic regression analysis to demonstrate the association between the application of the FAST HUGS BID and other relevant factors. Our findings indicate that the application of the FAST HUGS BID, along with other factors, has a significant impact on clinical outcomes.
F for Feeding. Many studies have reported that malnutrition or weight loss increases complications and worsens outcomes in severely ill patients [16]. Li et al. found that early enteral feeding in patients with trauma in the ICU was associated with lower mortality and shorter hospital LOS [10]. Additionally, Ortiz-Reyes et al. suggested that compared to delayed enteral nutrition, early enteral nutrition improved clinical outcomes in mechanically ventilated patients [17]. Moreover, many studies have demonstrated that early enteral nutrition is associated with lower mortality, shorter LOS, and improved clinical outcomes in mechanically ventilated patients, especially in trauma patients [18]. These findings align with the results observed in our study, where the after-FD group exhibited a shorter time to initiate enteral nutrition. It is worth noting that feeding represents one of the most important advantages of the FAST HUGS BID, considering that patients with sepsis or trauma may require nearly double the amount of energy during the acute phase [19].
A for Analgesia. Pain can affect a patient's psychological and physiological recovery, and adequate pain relief is an integral part of effective intensive care management. Critically ill patients commonly experience pain because of not only their underlying illness but also routine procedures, such as turning, suctioning, and dressing changes [20]. After applying the FAST HUGS BID checklist at our center, we observed a decrease in the use of narcotic analgesics and an increase in the utilization of nefopam. Despite maintaining a pain scale of three points in both groups, pain was effectively managed without excessive use of narcotic analgesics, which has been considered a positive effect [21,22,23]. In light of such emerging evidence, it can be argued that the elimination of disadvantages associated with the misuse and abuse of narcotic analgesics should be prioritized over the concerns about the potential side effects arising from the increased use of nefopam.
S for Sedation. Although the after-FD period exhibited a higher rate of dexmedetomidine and propofol usage and a lower rate of benzodiazepine usage, there were similar sedation levels in both periods; this was evidenced by Richmond Agitation-Sedation Scale scores consistently falling within the target range throughout this study. Previous studies have shown that dexmedetomidine or propofol offers advantages (e.g., reduced ventilation days and LOS in the ICU) over benzodiazepines in sedating critically ill patients [24,25]. It may be difficult and controversial to conclude that the use of dexmedetomidine or propofol instead of benzodiazepines directly affects survival in critically ill patients [24]. However, based on the findings of our study, it can be inferred that reducing benzodiazepine usage while increasing the utilization of dexmedetomidine or propofol contributed to a decrease in ventilation days and LOS in the ICU, as well as overall mortality. It is worth noting that a recent meta-analysis by Ng et al. reported the effectiveness of dexmedetomidine in reducing the incidence of delirium or agitation in the ICU [26]. However, because of the retrospective nature, there was a limitation in comparing the occurrence of delirium between the before and after periods in this study.
T for Thromboembolic Prophylaxis. According to the recently published American Association for the Surgery of Trauma and the American College of Surgeons Committee on Trauma clinical guidelines, patients with severe trauma face a high risk of venous thromboembolism, and prioritizing prophylaxis is crucial in preventing potentially lethal complications [27]. Indeed, appropriate thromboembolic prophylaxis for critically ill patients with severe trauma who are unable to move or walk is an important factor in achieving favorable outcomes [27]. In this study, we confirmed that thromboembolic prophylaxis was more actively administered after the implementation of the FAST HUGS BID approach, and there were a higher utilization rate of low molecular weight heparin and enoxaparin and a shorter time to the initial administration of enoxaparin in the after-FD period. It can be inferred that these factors contribute to improved clinical outcomes.
H for Head-of-Bed Elevation. Since the 1990s, head-of-bed elevation has been reported to reduce the incidence of gastroesophageal reflux and VAP in ventilated patients [28]. A recent systematic review indicated that head-of-bed elevation to 30°–60° resulted in a reduced occurrence of VAP (with an absolute risk reduction of 25.7%) compared with supine (0°-10°) positioning. However, the analysis did not reveal any improvement in other outcomes, including microbiologically proven VAP, length of ICU and hospital stay, or duration of mechanical ventilation [29]. There are various opinions regarding the optimal degree of head-of-bed elevation (30°–60°), but it is unclear which degree is most effective in reducing VAP [30]. After the implementation of the FAST HUGS BID checklist, we uniformly applied an elevation of 30° in all patients, except for those with cerebrospinal fluid leakage due to unstable spinal cord injury or skull base fracture before fixation. We kept the angle for head-of-bed elevation at 30° in the TICU because we observed an increase in incidents of unplanned tube removal (e.g., endotracheal tube, central venous catheter, and chest tube) when the elevation exceeded 30°. Furthermore, we witnessed an increase in pressure sores resulting from back maceration, primarily caused by the patient sliding down the bed. Moreover, we verified that after-FD patients had a shorter time to initiate head-of-bed elevation, and the incidence of pneumonia was significantly reduced. While other elements were also affected, it can be inferred that the uniform and systematic implementation of head-of-bed elevation contributed to the reduction in the incidence of VAP.
U for Ulcer Prevention. Before 2020, routine prophylaxis against stress ulcers in the ICU was not well justified, and the advantages and disadvantages of stress ulcer prevention were not clearly verified [31,32]. However, a recent review paper published in 2022 concluded that prophylaxis should be considered for critically ill patients with risk factors for stress ulcers. Nonetheless, frequent reassessment and de-escalation of therapy are required when patients have a lower risk of bleeding [33]. In our study, we observed a lower rate of utilization of ulcer medication, including proton pump inhibitors, among after-FD patients. This phenomenon can be attributed to the selective use of medications and the de-escalation of stress ulcer prevention therapy through regular re-evaluation in the TICU following the implementation of the FAST HUGS BID checklist.
G for Glucose Control. A recent systematic review highlighted that intensive glucose control is related to an increased risk of severe hypoglycemic events, but it also leads to reduced ICU LOS, sepsis, and mortality [34]. In this study, blood glucose levels were within the optimal range in both the before-FD and after-FD groups. However, the average blood sugar level was lower in the after-FD group than in the before-FD group, suggesting that blood sugar was controlled more efficiently in the after-FD group. Although this study had limitations in directly confirming whether better-controlled blood glucose levels were associated with reduced ICU and hospital LOS, sepsis incidence, or mortality, it can be inferred that these factors might have indirectly influenced clinical outcomes.
S for Spontaneous Breathing Trial. A randomized controlled trial published in 2008 demonstrated a significant reduction in ventilation days, ICU and hospital LOS, and mortality when spontaneous awakening and breathing trials were implemented daily [35]. Additionally, Robertson et al. showed that the implementation of a daily spontaneous breathing trial protocol resulted in improved extubation rates [36]. In this study, we observed that the after-FD group had a shorter time to extubation but a higher rate of unplanned intubation. Herein, we need to interpret with caution that the before-FD group exhibited an unusually lower rate (0.9%) of unplanned intubation. Since the rate was exceptionally low compared to the optimal range for failed extubation (5%–10%) [37], these findings suggest paradoxically that the absence of daily spontaneous awakening or breathing trials before the implementation of the checklist might have contributed to prolonged ventilator care.
B for Bowel Regimen. Diarrhea is common in ICU and has been found to be associated with increased mortality rates and prolonged ICU and hospital LOS [38]. In this study, we observed a decrease in the incidence of diarrhea events in the after-FD group. It can be inferred that the ICU staff checked for the presence and frequency of diarrhea daily, changed the feeding solution and diet, or prescribed symptom-relieving medications more aggressively following the checklist's implementation. These efforts, either directly or indirectly, might have contributed to the decrease in ICU and hospital LOS, as well as the mortality rate, among patients in the after-FD group.
I for In Indwelling Catheter Removal. Central venous and urinary catheters are necessary for massive transfusion, drug administration, total parenteral nutrition, and close monitoring of critically ill patients in the ICU. However, the risk of infection associated with these catheters is a critical concern. Therefore, many studies, including recent systematic reviews, have underscored the importance of promptly removing unnecessary central venous and urinary catheters to prevent catheter-associated infections [39,40,41,42]. In our study, we found that the indwelling periods of the central and urinary catheters significantly decreased after-FD. This observation indicates that the condition of the catheter was checked more closely, and unnecessary catheters were removed earlier in each round after the implementation of the checklist. Consequently, these efforts might have reduced the LOS in the ICU and hospital and improved mortality.
D for Drug De-escalation of Antibiotics. Empirical antibiotic therapy is widely employed in the ICU due to the high prevalence of infections, and appropriate antimicrobial therapy is crucial for critically ill patients. However, caution must be exercised as it may cause the development of drug-resistant organisms. Consequently, Masterton emphasized the importance of antibiotic de-escalation and discontinuation at the earliest possible time [43]. A recent systematic review demonstrated that antibiotic de-escalation therapy can be both safe and effective for most infections [44]. Consistently, our study also showed a significant decrease in the number of antibiotics used, particularly restricted antimicrobials typically reserved for drug-resistant organisms, and a shorter duration of antibiotic use after-FD. These results suggest that antibiotic utilization was managed more closely and effectively after the checklist's implementation.
To the best of our knowledge, this study is the first to evaluate the effectiveness of the implementation of the ICU round checklist, FAST HUGS BID, in severe trauma patients. Notably, our study differs from previous studies in that we analyzed each component of the checklist separately to identify potential improvements following its implementation. In addition, this study has several strengths, including the quantitative assessment of how much the checklist contributed to reducing ICU and hospital LOS and improving in-hospital mortality through the construction of a multivariable logistic regression model with adjustment for various confounding factors. However, this study has limitations owing to its retrospective observational nature. Regarding the evaluation of performance and outcome improvement, various factors other than the checklist's introduction might have influenced the results. Additionally, the presence of a time gap between the before- and after-FD periods might have introduced a limitation in terms of conducting a fair comparison. The difference in group sizes might have increased the possibility of selection bias. Moreover, because the study was conducted at a single center exclusively for patients with trauma, the generalizability of our results to other ICU settings may be limited.
5. Conclusions
The implementation of the ICU round checklist, FAST HUGS BID, has proven to be a valuable tool in enhancing communication and minimizing the risk of vital information being overlooked during discussions regarding the care of patients with severe trauma. In this study, we confirmed improvements in each component of the checklist following its introduction in the TICU. Moreover, we observed that its implementation was associated with decreases in in-hospital mortality and ICU and hospital LOS. These findings highlight the potential of utilizing a round checklist in an intensive care setting for severely injured patients, as it effectively reduces risks and improves clinical outcomes.
Author Contributions
Conceptualization: Seo D, Jung K. Data curation: Seo D, Heo I, Moon J, Kwon J, Huh Y, Kang BH, Song S, Kim S, Jung K. Formal analysis: Seo D, Moon J, Kwon J, Huh Y, Kang BH, Jung K. Investigation: Seo D, Heo I, Moon J, Kwon J, Huh Y, Kang BH, Song S, Kim S, Jung K. Methodology: Seo D, Jung K. Supervision: Jung K. Validation: Seo D, Jung K. Visualization: Seo D, Heo I, Jung K. Writing - original draft: Seo D, Heo I, Jung K. Writing - review & editing: Seo D, Heo I, Moon J, Kwon J, Huh Y, Kang BH, Song S, Kim S, Jung K.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was approved by the Institutional Review Board of Ajou University (AJOUIRB-DB-2023-390).
Informed Consent Statement
The requirement for written informed consent was waived due to the retrospective observational characteristic of the study.
Data Availability Statement
The data and materials that support the study findings are available upon reasonable request from the corresponding author (Kyoungwon Jung, MD, PhD, Division of Trauma Surgery, Department of Surgery, Ajou University School of Medicine, 164 World cup-ro, Yeongtong-gu, Suwon 16499, Korea, Tel: +82-31-219-7491, Fax: +82-31-219-7781, E-mail: jake98@ajou.ac.kr, jake98@daum.net).
Acknowledgments
The authors would like to acknowledge the team of trauma nursing and quality improvement in Ajou University Hospital Gyeonggi South Regional Trauma Center for its support to carry out the study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Gruen, R.L.; Jurkovich, G.J.; McIntyre, L.K.; Foy, H.M.; Maier, R.V. Patterns of errors contributing to trauma mortality: Lessons learned from 2,594 deaths. Ann Surg. 2006, 244, 371–380. [Google Scholar] [CrossRef] [PubMed]
- Michetti, C.P.; Fakhry, S.M.; Brasel, K.; Martin, N.D.; Teicher, E.J.; Newcomb, A. Trauma ICU Prevalence Project: The diversity of surgical critical care. Trauma Surg Acute Care Open. 2019, 4, e000288. [Google Scholar] [CrossRef] [PubMed]
- Adams, C.D.; Brunetti, L.; Davidov, L.; Mujia, J.; Rodricks, M. The impact of intensive care unit physician staffing change at a community hospital. SAGE Open Med. 2022, 10, 20503121211066471. [Google Scholar] [CrossRef]
- Duclos, G.; Zieleskiewicz, L.; Antonini, F.; Mokart, D.; Paone, V.; Po, M.H.; Vigne, C.; Hammad, E.; Potié, F.; Martin, C.; Medam, S.; Leone, M. Implementation of an electronic checklist in the ICU: Association with improved outcomes. Anaesth Crit Care Pain Med. 2018, 37, 25–33. [Google Scholar] [CrossRef]
- Pronovost, P.J.; Young, T.L.; Dorman, T.; Robinson, K.; Angus, D.C. Association between icu physician staffing and outcomes: A systematic review. Crit Care Med. 1999, 27, A43. [Google Scholar] [CrossRef]
- Stahl, K.; Palileo, A.; Schulman, C.I.; Wilson, K.; Augenstein, J.; Kiffin, C.; McKenney, M. Enhancing patient safety in the trauma/surgical intensive care unit. J Trauma. 2009, 67, 430–433, discussion 3-5. [Google Scholar] [CrossRef]
- Byrnes, M.C.; Schuerer, D.J.; Schallom, M.E.; Sona, C.S.; Mazuski, J.E.; Taylor, B.E.; McKenzie, W.; Thomas, J.M.; Emerson, J.S.; Nemeth, J.L.; Bailey, R.A.; Boyle, W.A.; Buchman, T.G.; Coopersmith, C.M. Implementation of a mandatory checklist of protocols and objectives improves compliance with a wide range of evidence-based intensive care unit practices. Crit Care Med. 2009, 37, 2775–2781. [Google Scholar] [CrossRef]
- Vincent, J.L. Give your patient a fast hug (at least) once a day. Crit Care Med. 2005, 33, 1225–1229. [Google Scholar] [CrossRef]
- Vincent, W.R., 3rd; Hatton, K.W. Critically ill patients need "FAST HUGS BID" (an updated mnemonic). Crit Care Med. 2009, 37, 2326–2327, author reply 7. [Google Scholar] [CrossRef]
- Barcellos, R.A.; Chatkin, J.M. Impact of a multidisciplinary checklist on the duration of invasive mechanical ventilation and length of ICU stay. J Bras Pneumol. 2020, 46, e20180261. [Google Scholar] [CrossRef] [PubMed]
- Pronovost, P.; Needham, D.; Berenholtz, S.; Sinopoli, D.; Chu, H.; Cosgrove, S.; Sexton, B.; Hyzy, R.; Welsh, R.; Roth, G.; Bander, J.; Kepros, J.; Goeschel, C. An intervention to decrease catheter-related bloodstream infections in the ICU. N Engl J Med. 2006, 355, 2725–2732. [Google Scholar] [CrossRef]
- Dubose, J.; Teixeira, P.G.; Inaba, K.; Lam, L.; Talving, P.; Putty, B.; Plurad, D.; Green, D.J.; Demetriades, D.; Belzberg, H. Measurable outcomes of quality improvement using a daily quality rounds checklist: One-year analysis in a trauma intensive care unit with sustained ventilator-associated pneumonia reduction. J Trauma. 2010, 69, 855–860. [Google Scholar] [CrossRef]
- Ferreira, C.R.; de Souza, D.F.; Cunha, T.M.; Tavares, M.; Reis, S.S.; Pedroso, R.S.; de Brito Röder, D.V.D. The effectiveness of a bundle in the prevention of ventilator-associated pneumonia. Braz J Infect Dis. 2016, 20, 267–271. [Google Scholar] [CrossRef] [PubMed]
- Haynes, A.B.; Weiser, T.G.; Berry, W.R.; Lipsitz, S.R.; Breizat, A.H.; Dellinger, E.P.; Herbosa, T.; Joseph, S.; Kibatala, P.L.; Lapitan, M.C.; Merry, A.F.; Moorthy, K.; Reznick, R.K.; Taylor, B.; Gawande, A.A. ; Safe Surgery Saves Lives Study Group. A surgical safety checklist to reduce morbidity and mortality in a global population. N Engl J Med. 2009, 360, 491–499. [Google Scholar]
- Writing Group for the CHECKLIST-ICU Investigators and the Brazilian Research in Intensive Care Network (BRICNet); Cavalcanti, A.B.; Bozza, F.A.; Machado, F.R.; Salluh, J.I.; Campagnucci, V.P.; Vendramim, P.; Guimaraes, H.P.; Normilio-Silva, K.; Damiani, L.P.; Romano, E.; Carrara, F.; Lubarino Diniz de Souza, J.; Silva, A.R.; Ramos, G.V.; Teixeira, C.; Brandão da Silva, N.; Chang, C.C.; Angus, D.C.; Berwanger, O. Effect of a quality improvement intervention with daily round checklists, goal setting, and clinician prompting on mortality of critically ill patients: A randomized clinical trial. JAMA. 2016, 315, 1480–1490. [Google Scholar]
- Studley, H.O. Percentage of weight loss: Basic indicator of surgical risk in patients with chronic peptic ulcer. JAMA. 1936, 106, 458–460. [Google Scholar] [CrossRef]
- Ortiz-Reyes, L.; Patel, J.J.; Jiang, X.; Coz Yataco, A.; Day, A.G.; Shah, F.; Zelten, J.; Tamae-Kakazu, M.; Rice, T.; Heyland, D.K. Early versus delayed enteral nutrition in mechanically ventilated patients with circulatory shock: A nested cohort analysis of an international multicenter, pragmatic clinical trial. Crit Care. 2022, 26, 173. [Google Scholar] [CrossRef]
- Giner, M.; Laviano, A.; Meguid, M.M.; Gleason, J.R. In 1995 a correlation between malnutrition and poor outcome in critically ill patients still exists. Nutrition. 1996, 12, 23–29. [Google Scholar] [CrossRef]
- Reid, C.L. Nutritional requirements of surgical and critically-ill patients: Do we really know what they need? Proc Nutr Soc. 2004, 63, 467–472. [Google Scholar] [CrossRef] [PubMed]
- Puntillo, K.A.; White, C.; Morris, A.B.; Perdue, S.T.; Stanik-Hutt, J.; Thompson, C.L.; Wild, L.R. Patients' perceptions and responses to procedural pain: Results from Thunder Project II. Am J Crit Care. 2001, 10, 238–251. [Google Scholar] [CrossRef]
- Chou, R.; Turner, J.A.; Devine, E.B.; Hansen, R.N.; Sullivan, S.D.; Blazina, I.; Dana, T.; Bougatsos, C.; Deyo, R.A. The effectiveness and risks of long-term opioid therapy for chronic pain: A Systematic Review for a National Institutes of Health Pathways to Prevention Workshop. Ann Intern Med. 2015, 162, 276–286. [Google Scholar] [CrossRef]
- Girard, P.; Chauvin, M.; Verleye, M. Nefopam analgesia and its role in multimodal analgesia: A review of preclinical and clinical studies. Clin Exp Pharmacol Physiol. 2016, 43, 3–12. [Google Scholar] [CrossRef]
- Moran, B.L.; Myburgh, J.A.; Scott, D.A. The complications of opioid use during and post-intensive care admission: A narrative review. Anaesth Intensive Care. 2022, 50, 108–126. [Google Scholar] [CrossRef] [PubMed]
- Fraser, G.L.; Devlin, J.W.; Worby, C.P.; Alhazzani, W.; Barr, J.; Dasta, J.F.; Kress, J.P.; Davidson, J.E.; Spencer, F.A. Benzodiazepine versus nonbenzodiazepine-based sedation for mechanically ventilated, critically ill adults: A systematic review and meta-analysis of randomized trials. Crit Care Med. 2013, 41 Suppl 1, S30–S38. [Google Scholar] [CrossRef] [PubMed]
- Jakob, S.M.; Ruokonen, E.; Grounds, R.M.; Sarapohja, T.; Garratt, C.; Pocock, S.J.; Bratty, J.R.; Takala, J. Dexmedetomidine for Long-Term Sedation Investigators. Dexmedetomidine vs Midazolam or Propofol for Sedation During Prolonged Mechanical Ventilation: Two Randomized Controlled Trials. JAMA. 2012, 307, 1151–1160. [Google Scholar] [CrossRef] [PubMed]
- Carver, D.; Kirkpatrick, A.W.; D'Amours, S.; Hameed, S.M.; Beveridge, J.; Ball, C.G. A Prospective Evaluation of the Utility of a Hybrid Operating Suite for Severely Injured Patients: Overstated or Underutilized? Ann Surg. 2020, 271, 958–961. [Google Scholar] [CrossRef] [PubMed]
- Yorkgitis, B.K.; Berndtson, A.E.; Cross, A.; Kennedy, R.; Kochuba, M.P.; Tignanelli, C.; Tominaga, G.T.; Jacobs, D.G.; Marx, W.H.; Ashley, D.W.; Ley, E.J.; Napolitano, L.; Costantini, T.W. American Association for the Surgery of Trauma/American College of Surgeons-Committee on Trauma Clinical Protocol for inpatient venous thromboembolism prophylaxis after trauma. J Trauma Acute Care Surg. 2022, 92, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Torres, A.; Serra-Batlles, J.; Ros, E.; Piera, C.; Puig de la Bellacasa, J.; Cobos, A.; Lomeña, F.; Rodríguez-Roisin, R. Pulmonary aspiration of gastric contents in patients receiving mechanical ventilation: The effect of body position. Ann Intern Med. 1992, 116, 540–543. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Li, X.; Yang, Z.; Tang, X.; Yuan, Q.; Deng, L.; Sun, X. Semi-recumbent position versus supine position for the prevention of ventilator-associated pneumonia in adults requiring mechanical ventilation. Cochrane Database Syst Rev. 2016, 2016, Cd009946. [Google Scholar] [CrossRef] [PubMed]
- Keeley, L. Reducing the risk of ventilator-acquired pneumonia through head of bed elevation. Nurs Crit Care. 2007, 12, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Quenot, J.P.; Thiery, N.; Barbar, S. When should stress ulcer prophylaxis be used in the ICU? Curr Opin Crit Care. 2009, 15, 139–143. [Google Scholar] [CrossRef]
- Barbateskovic, M.; Marker, S.; Jakobsen, J.C.; Krag, M.; Granholm, A.; Anthon, C.T.; Perner, A.; Wetterslev, J.; Møller, M.H. Stress ulcer prophylaxis in adult intensive care unit patients - a protocol for a systematic review. Acta Anaesthesiol Scand. 2018, 62, 744–755. [Google Scholar] [CrossRef] [PubMed]
- Saeed, M.; Bass, S.; Chaisson, N.F. Which ICU patients need stress ulcer prophylaxis? Cleve Clin J Med. 2022, 89, 363–367. [Google Scholar] [CrossRef]
- Yao, R.Q.; Ren, C.; Wu, G.S.; Zhu, Y.B.; Xia, Z.F.; Yao, Y.M. Is intensive glucose control bad for critically ill patients? A systematic review and meta-analysis. Int J Biol Sci. 2020, 16, 1658–1675. [Google Scholar] [PubMed]
- Girard, T.D.; Kress, J.P.; Fuchs, B.D.; Thomason, J.W.; Schweickert, W.D.; Pun, B.T.; Taichman, D.B.; Dunn, J.G.; Pohlman, A.S.; Kinniry, P.A.; Jackson, J.C.; Canonico, A.E.; Light, R.W.; Shintani, A.K.; Thompson, J.L.; Gordon, S.M.; Hall, J.B.; Dittus, R.S.; Bernard, G.R.; Ely, E.W. Efficacy and safety of a paired sedation and ventilator weaning protocol for mechanically ventilated patients in intensive care (Awakening and Breathing Controlled trial): A randomised controlled trial. Lancet. 2008, 371, 126–134. [Google Scholar] [CrossRef]
- Robertson, T.E.; Sona, C.; Schallom, L.; Buckles, M.; Cracchiolo, L.; Schuerer, D.; Coopersmith, C.M.; Song, F.; Buchman, T.G. Improved extubation rates and earlier liberation from mechanical ventilation with implementation of a daily spontaneous-breathing trial protocol. J Am Coll Surg. 2008, 206, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Krinsley, J.S.; Reddy, P.K.; Iqbal, A. What is the optimal rate of failed extubation? Crit Care. 2012, 16, 111. [Google Scholar] [CrossRef]
- Taito, S.; Kawai, Y.; Liu, K.; Ariie, T.; Tsujimoto, Y.; Banno, M.; Kataoka, Y. Diarrhea and patient outcomes in the intensive care unit: Systematic review and meta-analysis. J Crit Care. 2019, 53, 142–148. [Google Scholar] [CrossRef]
- Bell, T.; O'Grady, N.P. Prevention of central line-associated bloodstream infections. Infect Dis Clin North Am. 2017, 31, 551–559. [Google Scholar] [CrossRef]
- Xiong, Z.; Chen, H. Interventions to reduce unnecessary central venous catheter use to prevent central-line-associated bloodstream infections in adults: A systematic review. Infect Control Hosp Epidemiol. 2018, 39, 1442–1448. [Google Scholar] [CrossRef]
- Clarke, K.; Hall, C.L.; Wiley, Z.; Tejedor, S.C.; Kim, J.S.; Reif, L.; Witt, L.; Jacob, J.T. Catheter-associated urinary tract infections in adults: Diagnosis, treatment, and prevention. J Hosp Med. 2020, 15, 552–556. [Google Scholar] [CrossRef] [PubMed]
- Nollen, J.M.; Pijnappel, L.; Schoones, J.W.; Peul, W.C.; Van Furth, W.R.; Brunsveld-Reinders, A.H. Impact of early postoperative indwelling urinary catheter removal: A systematic review. J Clin Nurs. 2023, 32, 2155–2177. [Google Scholar] [CrossRef] [PubMed]
- Masterton, R.G. Antibiotic de-escalation. Crit Care Clin. 2011, 27, 149–162. [Google Scholar] [CrossRef] [PubMed]
- Ohji, G.; Doi, A.; Yamamoto, S.; Iwata, K. Is de-escalation of antimicrobials effective? A systematic review and meta-analysis. Int J Infect Dis. 2016, 49, 71–79. [Google Scholar] [CrossRef]
Figure 1.
Flow chart of patient selection.
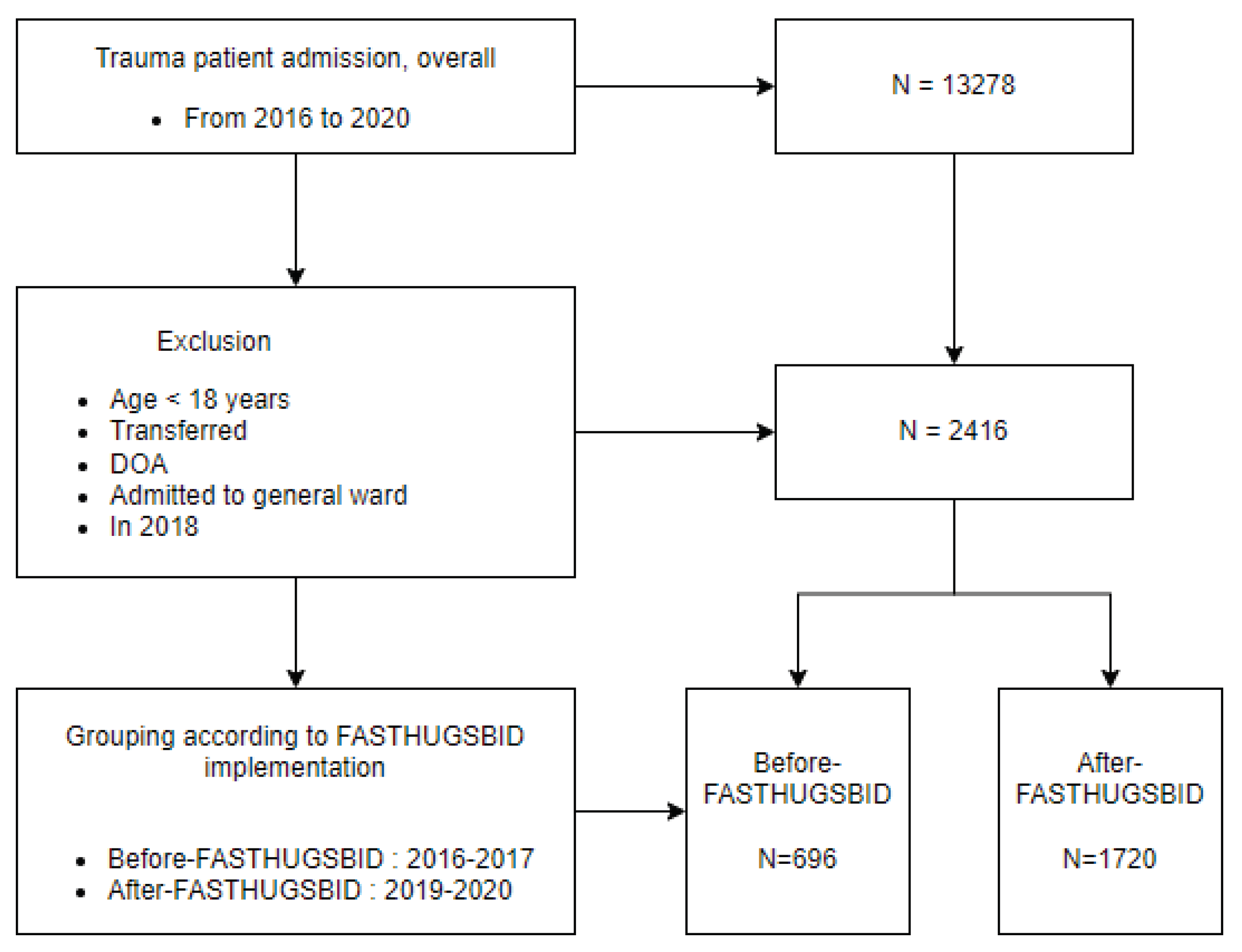
Figure 2.
Kaplan-Meier curve for comparison of 90 days in-hospital mortality before and after implementation of the FAST HUGS BID program.
Figure 2.
Kaplan-Meier curve for comparison of 90 days in-hospital mortality before and after implementation of the FAST HUGS BID program.
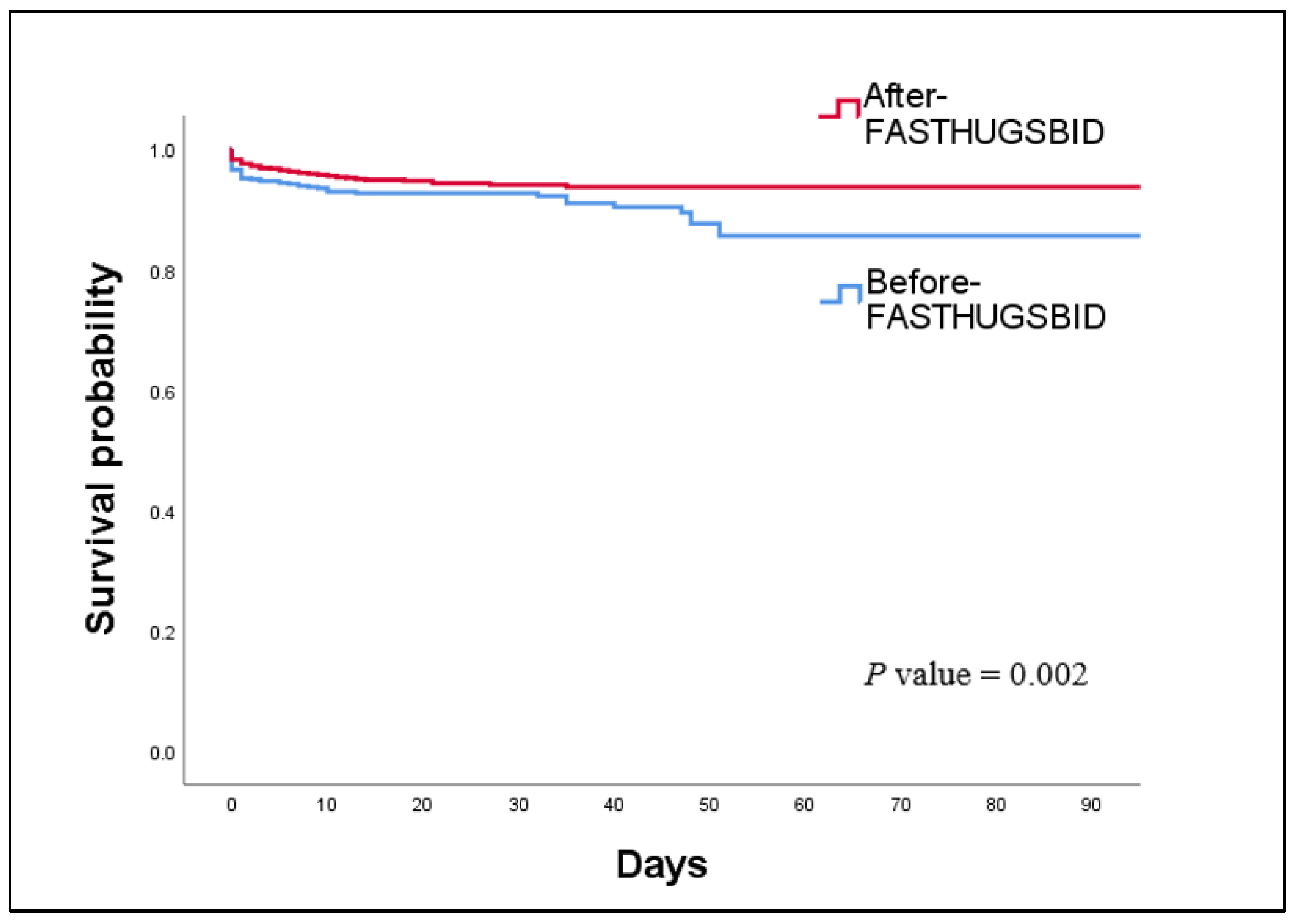

Table 1.
Patient characteristics in the before- and after-FD groups.
| Variables | Before-FD1 (n=696) | After-FD2 (n=1720) | P values |
|---|---|---|---|
| Age (year), mean ± SD3 | 48.7 ± 17.5 | 48.7 ± 16.8 | 0.97 |
| Sex, n (%) | 0.09 | ||
| Female | 171 (24.6) | 368 (21.4) | |
| Male | 525 (75.4) | 1352 (78.6) | |
| Mechanism of injury | 0.539 | ||
| Blunt, n (%) | 618 (89.3) | 1545 (90.1) | |
| Penetrating, n (%) | 74 (10.7) | 169 (9.9) | |
| Underlying disease, yes (%) | 263 (38.3) | 734 (42.9) | <0.05 |
| Injury Severity Score, median (IQR4) | 13 (5-22) | 17 (10-24) | <0.05 |
| Initial physiologic parameters | |||
| Systolic blood pressure (mm Hg), mean ± SD | 131.2 ± 26.9 | 136.0 ± 26.7 | <0.05 |
| Diastolic blood pressure (mm Hg), mean ± SD | 82.2 ± 20.9 | 89.2 ± 21.1 | <0.05 |
| Mean arterial pressure (mm Hg), mean ± SD | 98.5 ± 21.4 | 104.8 ± 21.2 | <0.05 |
| Pulse rate (per min), mean ± SD | 90.7 ± 19.9 | 89.2 ± 20.4 | 0.09 |
| Respiratory rate (per min), mean ± SD | 20.4 ± 5.8 | 21.1 ± 5.9 | <0.05 |
| Body temperature (℃), mean ± SD | 36.4 ± 0.7 | 36.5 ± 0.7 | 0.25 |
| Glasgow Coma Scale, median (IQR) | 15 (13-15) | 15 (14-15) | 0.07 |
1 Before-FD, before implementation of the FAST HUGS BID checklist; 2 After-FD, after the implementation of the FAST HUGS BID checklist; 3 SD, standard deviation; 4 IQR, interquartile range.
Table 2.
Comparisons of primary outcomes between the before- and after-FD groups.
| Primary outcomes | Before-FD1 (n=696) | After-FD2 (n=1720) | P values |
|---|---|---|---|
| In-hospital mortality, n (%) | 58 (8.3) | 83 (4.8) | <0.05 |
| Complications, n (%) | 160 (23.0) | 283 (16.5) | <0.05 |
| ICU3 length of stay (days), mean ± SD | 7.8 ± 13.3 | 5.1 ± 10.4 | <0.05 |
| Hospital length of stay (days), mean ± SD | 24.3 ± 24.6 | 17.6 ± 16.0 | <0.05 |
| Duration of mechanical ventilation (days), mean ± SD | 9.2 ± 13.3 (n=315) | 5.0 ± 8.4 (n=682) | <0.05 |
1 Before-FD, before implementation of the FAST HUGS BID checklist; 2 After-FD, after the implementation of the FAST HUGS BID checklist; 3 ICU, intensive care unit; 4 SD, standard deviation.
Table 3.
Comparisons of secondary outcomes between the before- and after-FD groups.
| Complications | Before-FD1 (n=696) | After-FD2 (n=1720) | P values | OR3 (95% CI4) |
|---|---|---|---|---|
| Total, n (%) | 160 (23) | 283 (16.5) | <0.05 | 0.66 (0.53-0.82) |
| Acute kidney injury, n (%) | 9 (1.3) | 26 (1.5) | 0.68 | 1.17 (0.54-2.51) |
| Acute respiratory distress syndrome, n (%) | 4 (0.6) | 9 (0.5) | 1.00 | 0.91 (0.28-2.97) |
| Pressure ulcer, n (%) | 76 (10.9) | 98 (5.7) | <0.05 | 0.49 (0.36-0.67) |
| Venous thromboembolism, n (%) | 8 (1.1) | 24 (1.4) | 0.63 | 1.21 (0.54-2.72) |
| Pneumonia, n (%) | 63 (9.1) | 59 (3.4) | <0.05 | 0.38 (0.25-0.52) |
| Surgical site infection, n (%) | 30 (4.3) | 23 (1.3) | <0.05 | 0.30 (0.17-0.52) |
| Urinary tract infection, n (%) | 8 (1.1) | 18 (1.0) | 0.82 | 0.91 (0.39-2.10) |
| Catheter related blood stream infection, n (%) | 2 (0.3) | 9 (0.5) | 0.74 | 1.83 (0.39-8.47) |
| Sepsis, n (%) | 3 (0.4) | 25 (1.5) | <0.05 | 3.40 (1.02-11.32) |
1 Before-FD, before implementation of the FAST HUGS BID checklist; 2 After-FD, after the implementation of the FAST HUGS BID checklist; 3 OR, odds ratio; 4 CI, confidence interval.
Table 4.
Comparisons of each component of the FAST HUGS BID checklist before and after implementation.
Table 4.
Comparisons of each component of the FAST HUGS BID checklist before and after implementation.
| Component of FAST HUGS BID checklist | Before-FD1 (n=696) |
After-FD2 (n=1720) |
P values | OR (95%CI) |
|---|---|---|---|---|
| Feeding | ||||
| Time to enteral nutrition (days), mean ± SD | 2.7 ± 3.7 | 1.5 ± 1.9 | <0.05 | - |
| Time to parenteral nutrition (days), mean ± SD | 7.9 ± 8.9 (n=161) | 9.2 ± 9.5 (n=209) | 0.165 | - |
| Body weight difference (kg), mean ± SD | 0.46 ± 6.3 | 0.52 ± 3.9 | <0.05 | - |
| Analgesia | ||||
| IV3 Fentanyl use, n (%) | 508 (73.0) | 1225 (71.2) | 0.382 | 0.91 (0.75-1.11) |
| Duration of IV Fentanyl use (days), mean ± SD | 5.8 ± 7.6 (n=508) | 2.5 ± 2.9 (n=1225) | <0.05 | - |
| IV Nefopam use, n (%) | 421 (60.5) | 1407 (81.8) | <0.05 | 2.94 (2.41-3.57) |
| PO4 painkillers use, n (%) | 456 (65.5) | 1382 (80.3) | <0.05 | 2.15 (1.77-2.61) |
| PO opioids use, n (%) | 72 (10.3) | 654 (38.0) | <0.05 | 5.31 (4.09-6.91) |
| TD5 Fentanyl patch use, n (%) | 196 (28.2) | 550 (32.0) | 0.66 | 1.20 (0.99-1.46) |
| Pain scale, median (IQR) | 1 (0.1-2.0) | 1.2 (0.5-2.1) | <0.05 | - |
| Sedation | ||||
| IV Midazolam use, n (%) | 201 (28.9) | 113 (6.6) | <0.05 | 0.17 (0.13-0.22) |
| IV Propofol use, n (%) | 205 (29.5) | 434 (25.2) | <0.05 | 0.80 (0.66-0.98) |
| IV Dexmedetomidine use, n (%) | 138 (19.8) | 452 (26.3) | <0.05 | 1.44 (1.16-1.79) |
| IV Vecuronium use, n (%) | 69 (9.9) | 83 (4.8) | <0.05 | 0.46 (0.33-0.64) |
| RASS6 score, median (IQR) | -0.4 (-1.5-0.0) | -0.3 (-1.0-0.0) | <0.05 | - |
| Thromboembolic prophylaxis | ||||
| SC7 LMWH use, n (%) | 165 (23.7) | 690 (40.1) | <0.05 | 2.16 (1.77-2.63) |
| Time to the first use of LMWH8 (days), mean ± SD | 4.8 ± 4.8 (n=165) | 2.8 ± 2.8 (n=690) | <0.05 | - |
| Head of bed elevation | ||||
| Time to first head of bed elevation (days), mean ± SD | 8.8 ± 16.8 | 4.8 ± 12.0 | <0.05 | - |
| Ulcer prophylaxis | ||||
| H2-blocker use, n (%) | 640 (92.0) | 1476 (85.8) | <0.05 | 0.53 (0.39-0.72) |
| Proton pump inhibitor use, n (%) | 64 (9.2) | 86 (5.0) | <0.05 | 0.52 (0.37-0.72) |
| Glycemic control | ||||
| Average level of blood sugar (mg/dL), mean ± SD | 137.1 ± 32.6 | 134.5 ± 31.3 | 0.07 | - |
| Hypoglycemic event, n (%) | 29 (4.2) | 67 (3.9) | 0.76 | 0.93 (0.59-1.46) |
| Spontaneous breathing trial | ||||
| Time to extubation (days), mean ± SD | 6.4 ± 7.2 (n=308) | 4.8 ± 5.5 (n=594) | <0.05 | - |
| Unplanned intubation, n (%) | 6 (0.9) | 37 (2.2) | <0.05 | 2.53 (1.06-6.02) |
| Bowel movement | ||||
| Diarrhea event, n (%) | 142 (20.4) | 277 (16.1) | <0.05 | 0.75 (0.60-0.94) |
| Vomiting event, n (%) | 108 (15.5) | 242 (14.1) | 0.36 | 0.89 (0.70-1.14) |
| Indwelling catheter | ||||
| Time to removal of CVC9 (days), mean ± SD | 11.9 ± 16.5 | 7.6 ± 11.0 | <0.05 | - |
| Time to removal of urinary catheter (days), mean ± SD | 8.5 ± 16.3 | 5.8 ± 12.5 | <0.05 | - |
| Drug de-escalation | ||||
| Restricted antimicrobials use, n (%) | 175 (25.1) | 333 (19.4) | <0.05 | 0.71 (0.58-0.88) |
| Duration of antimicrobials use (days), mean ± SD | 18.0 ± 22.1 | 8.2 ± 13.6 | <0.05 | - |
1 Before-FD, before implementation of the FAST HUGS BID checklist; 2 After-FD, after the implementation of the FAST HUGS BID checklist; 3 IV, intravenous; 4 PO, per oral; 5 TD, transdermal; 6 RASS, Richmond Agitation & Sedation Scale; 7 SC, subcutaneous; 8 LMWH, low-molecular-weight heparin; 9 CVC, central venous catheter.
Table 5.
Factors associated with in-hospital mortality identified by logistic regression analysis.
| Variables | Univariable analysis | Multivariable analysis | ||
|---|---|---|---|---|
| Adjusted OR | P values | Adjusted OR | P values | |
| Age | 1.018 | <0.001 | 1.040 | <0.001 |
| Sex | 0.864 | 0.499 | ||
| Mechanism of injury | 0.601 | 0.148 | ||
| Underlying disease | 0.933 | 0.713 | ||
| Initial systolic blood pressure | 0.985 | <0.001 | 0.898 | 0.538 |
| Initial diastolic blood pressure | 0.976 | <0.001 | 0.764 | 0.441 |
| Initial mean arterial pressure | 0.977 | <0.001 | 1.445 | 0.482 |
| Initial pulse rate | 1.025 | <0.001 | 1.010 | 0.103 |
| Initial respiratory rate | 1.019 | 0.244 | ||
| Initial body temperature | 0.458 | <0.001 | 1.048 | 0.789 |
| Initial Glasgow Coma Scale | 0.673 | <0.001 | 0.748 | <0.001 |
| Injury Severity Score | 1.088 | <0.001 | 1.066 | <0.001 |
| FAST HUGS BID | 0.551 | 0.001 | 0.434 | 0.008 |
| Complications | 4.215 | <0.001 | 2.080 | 0.016 |
| Nagelkerke =0.450 Hosmer-Lemeshow Chi-square test = 9.753, df= 8, P value =0.283 | ||||
Table 6.
Multiple linear regression for factors associated with ICU length of stay.
| Variables | β1 | 95% CI2 | Βeta3 | P value |
| Mechanism of injury | 0.502 | -0.840~1.843 | 0.014 | 0.464 |
| Underlying disease | 0.897 | 0.102-1.691 | 0.042 | 0.027 |
| Initial systolic blood pressure | -0.409 | -0.887~0.069 | -1.018 | 0.094 |
| Initial diastolic blood pressure | -0.791 | -1.747~0.164 | -1.566 | 0.104 |
| Initial mean arterial pressure | 1.203 | -0.229~2.636 | 2.385 | 0.100 |
| Initial pulse rate | 0.015 | -0.008~0.037 | 0.027 | 0.202 |
| Initial respiratory rate | 0.003 | -0.069~0.076 | 0.002 | 0.934 |
| Initial body temperature | -0.335 | -0.923~0.254 | -0.022 | 0.265 |
| Initial Glasgow Coma Scale | -0.682 | -0.841~-0.522 | -0.171 | <0.001 |
| Injury Severity Score | 0.194 | 0.150~0.238 | 0.196 | <0.001 |
| FAST HUGS BID | -2.742 | -3.645~-1.839 | -0.118 | <0.001 |
| Complications | 8.212 | 7.049~9.374 | 0.285 | <0.001 |
| R= 0.500, =0.25, adj.=0.246 | ||||
1 Β, unstandardized coefficients; 2 CI, confidence interval; 3 Beta, standardized coefficients.
Table 7.
Multiple linear regression for factors associated with hospital length of stay.
| Variables | β | 95%CI | βeta | P value |
| Initial systolic blood pressure | -40.431 | -124.612~43.749 | -0.597 | 0.346 |
| Initial diastolic blood pressure | -97.933 | -266.144~70.278 | -1.144 | 0.254 |
| Initial mean arterial pressure | 135.708 | -116.528~387.944 | 1.597 | 0.292 |
| Initial pulse rate | -0.534 | -4.176~3.108 | -0.006 | 0.774 |
| Initial body temperature | 58.948 | -42.239~160.135 | 0.023 | 0.253 |
| Initial Glasgow Coma Scale | -189.064 | -214.394~-163.734 | -0.309 | <0.001 |
| Injury Severity Score | 28.164 | 20.962~35.367 | 0.175 | <0.001 |
| FASTHUGSBID | -251.928 | -409.369~-94.487 | -0.063 | 0.002 |
| Complications | 398.987 | 200.615~597.359 | 0.083 | <0.001 |
| R= 0.430, =0.185, adj.=0.182 | ||||
1 Β, unstandardized coefficients; 2 CI, confidence interval; 3 Beta, standardized coefficients.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



