Submitted:
28 February 2024
Posted:
06 March 2024
You are already at the latest version
Abstract
Background: The study aimed to investigate the association between environmental tobacco smoke exposure and the risk of wheezing among rural and urban preschool children in Mpumalanga province, South Africa, an area associated with poor air quality. Methods: In this study, parents/caregivers of preschool children (n=3145) completed a modified International Study of Asthma and Allergies in Childhood (ISAAC) questionnaire. Data were analysed using multiple logistic regression models. Results: The overall prevalence of Wheeze ever was 15.14%, with a higher prevalence in urban pre-schoolers than rural pre-schoolers (20.71% vs 13.30 %, P<0.000). Moreover, the total prevalence of asthma ever was 2.34%. The prevalence was greater in urban pre-schoolers than in rural pre-schoolers (3.92% vs 1.81%, P<0.001). In the final adjusted model, both urban and rural area children who lived with one or more people who smoked in the same household (WE: OR 1.44, 95% CI 1.11-1.86) (CW: OR 2.09, 95% CI 1.38-3.16) and (AE: OR 2.49, 95% CI 1.12-5.54) were found to have an increased likelihood of having Wheeze Ever, Current Wheeze and Asthma Ever as compared to those who lived with non-smokers. Conclusions: The implementation of smoking limits and prohibition is crucial in areas that are frequented or utilized by children. Hence, it is imperative for healthcare providers to actively champion the rights of those who do not smoke within the society, while also endorsing legislative measures aimed at curtailing the extent of tobacco smoke exposure.
Keywords:
Environmental tobacco smoke exposure
; The risk of wheezing
; Poor air quality
; Preschool children
1. Introduction
Wheeze can be described as a persistent high-pitched sound characterized by a melodic tone that originates from the chest during the act of exhaling [1]. Wheezing throughout early childhood is a prevalent yet intricate symptom characterized by multiple aetiologies and potential consequences. [2,3] It is common for children who exhibit wheezing symptoms before the age of three and persist with wheezing until the age of six to possess atopic tendencies and subsequently develop asthma over the period of eleven to thirteen years [4,5,6]. Moreover, it has been observed that the respiratory capacity of children experiencing wheezing tends to enhance as they grow older; however, their respiratory capacity never reaches the level observed in children who have never experienced wheezing [4].
The association between wheezing and asthma remains uncertain during the early stages of life. Asthma is a persistent inflammatory ailment affecting respiratory passages, exhibiting fluctuating symptoms such as wheezing, dyspnoea, thoracic constriction, and coughing [7]. Asthma has emerged as a significant public health concern on a global scale, with a particular impact on the paediatric population [8,9,10,11,12,13]. Despite the potential for asthma to manifest clinically at a later stage, [14] investigating asthma in young children holds the potential to mitigate and pre-empt the development of established asthma symptoms [14]. Asthma is considered an incurable condition, and recent research has revealed that recurrent asthma attacks can lead to irreversible lung damage. Asthma management can be effectively achieved by the implementation of proper healthcare interventions. Due to the diverse nature of asthma in the paediatric population, several scholars propose that the term "asthma" should not be employed to characterize episodes of wheezing in preschool-aged children. 1
Children's asthma has been linked to frequent indoor exposure to environmental tobacco smoke (ETS) [15,16]. ETS possess comparable toxic components to those found in conventional tobacco smoke, consequently resulting in similar detrimental consequences akin to those observed in individuals who engage in active smoking [17]. The symptoms of asthma may exhibit temporary remission following therapy interventions and/or avoidance of triggers associated with the condition. Hence, it is advisable to enact legislation aimed at the elimination and regulation of children's exposure to ETS.
According to the Tobacco Products Control Act of 1993 in South Africa, specifically Section 2(1)(a)(iii), it is prohibited for individuals to engage in smoking any tobacco product within a motor vehicle in the presence of a child under the age of 12 years. This provision has been subject to amendments. The act of smoking is now prohibited within buildings designated for commercial childcare services. Sweets and toys resembling cigarettes are likewise prohibited. The implementation of new tobacco regulations was officially announced in September 2022 through the publication of Government Gazette Staats koerant, Regulation Gazette No. 11494, Vol. 68729, September No. 469942022. Regulation number R. 2560.
The following are highlights that will be considered in risk for childhood exposure to ETS:
- In the event that a residence is utilized for educational purposes, tutoring services, or commercial childcare, the act of smoking would likewise be prohibited.
- The implementation of a prohibition on smoking within motor vehicles in the presence of a minor under the age of 18, provided that there is more than one individual occupying said vehicle.
- The proposed legislative expansion involves not only traditional cigarettes, but also embraces any devices used in connection with tobacco-related goods and electronic delivery systems, such as pipes, water pipes, and electronic devices.
There is a tendency for asthma prevalence to be lower in rural areas, with some evidence suggesting the presence of an urban-rural gradient. The rural-urban gradient of wheeze in preschool children is examined to determine whether this indicator differs along an urban-rural gradient. A study was undertaken by Lawson et al. to examine the relationship between asthma and its indicators throughout the rural-urban gradient. The findings revealed that the prevalence of children with smoking parents was lower in the large urban center [18].
The current tobacco control laws are introduced in a baseline and impact of the regulations will be seen in later years. This study presents the baseline of prevalence of wheeze and asthma in Mpumalanga where children are exposed to polluted air including ETS. The aim is to evaluate the association between exposure to environmental tobacco smoke and the occurrence of wheezing, a symptom commonly associated with asthma, among preschool children residing in rural and urban areas of Mpumalanga Province, South Africa.
2. Methods
2.1. Study Design and Settings
An analytical cross-sectional survey was conducted between November 2020 and April 2021. The objective of our study was to assess the association between environmental tobacco smoke exposure and the occurrence of wheezing, a common symptom of asthma, among preschool children residing in rural and urban areas. The research was carried out within the Mpumalanga province, specifically in the Gert Sibande district municipality, which is situated within the Highveld Priority Area. In accordance with the National Environmental Management: Air Quality Act, 2004 (Act No. 39 of 2004), the Minister of Environmental Affairs named this region as a priority area for air pollution in 2007.
The Gert Sibande district municipality was purposively selected because it is in the Highveld priority area. The Highveld Priority Area has substandard air quality and heightened levels of pollutants originating from both industrial and non-industrial origins. The district encompasses a diverse range of sectors, such as power generating, petrochemical, primary metallurgy, and open cast mining. The district municipality comprises seven local municipalities, specifically Dipaleseng, Govan Mbeki, Lekwa, Msukukaligwa, DR Pixley ka Seme, all of which are situated within the Highveld priority area. The Chief Albert Luthuli and Mkhondo municipalities are not encompassed under the Highveld priority area. Figure 1 illustrates the geographical distribution of seven local district municipalities, with Gert Sibande being visually distinguished by the use of a light-yellow highlighting.
2.2. Study Population, Sample Size Estimation and Sampling Procedure
The participants in this study consisted of preschool-aged children, ranging from one to eight years old, who resided in and attended preschools located in either rural or urban areas within the Mpumalanga province, specifically in the Gert Sibande district municipality. Based on the data from the 2019 Gert Sibande database, the number of children enrolled in preschool was recorded as 13,485 [19]. The overall sample size required for this study was determined to be 3,900, assuming a response rate of 70%. A study power of 80% was used for the investigation, with a significance level of 5%. The sample size was determined using the sample size calculator in Microsoft Excel.
A probability sample design was employed in order to achieve equitable representation of all preschool children throughout seven local municipalities. Preschools were identified in the northern, southern, eastern, and western regions of each of the seven municipalities within the Gert Sibande district (Figure 1). A representative sample of preschools was chosen from each of the four areas within each municipality. Preschool children were selected in a random manner from a class roster obtained from each designated preschool. Selected pre-schoolers were then given participant information leaflets inviting their parents to be part of the study. Parents, who consented to let their children participate, were then given a questionnaire to complete and return to the preschool. All necessary COVID-19 protocols were implemented.
2.3. Study Tools
Data was collected using the adapted International Study of Asthma and Allergies in Childhood (ISAAC) questionnaire. 9 The questionnaire was divided into two sections: namely demographic data and health outcomes. The questionnaire was in English, which is the common language in a region with multiple local languages. In order to evaluate the data collection procedure and the quality of the survey questions in light of COVID-19 limitations, a pre-test of the instrument was conducted with environmental health practitioners. These professionals were chosen owing to their regular interaction with parents and carers, which provides them with insights into the educational background of these individuals.
2.4. Health Outcomes of the Study
The following central questions on asthma symptoms were used in order to evaluate health outcomes: (1) Has your child ever experienced chest wheezing or whistling in the past? (Wheeze Ever) (2) Has he or she had chest wheezing or whistling in the previous 12 months? (Current Wheeze) (3) How many wheezing episodes did your child have in the last 12 months? (4) How frequently, on average, during the previous 12 months was your child's sleep interrupted by wheezing? (5) Has your child's wheezing ever been sufficiently severe to prevent them from speaking more than a few phrases at any time between breathing in the last 12 months? (6) Did the child ever suffer from asthma? (Asthma Ever) (7) Did a physician or nurse diagnose the asthma? (8) Has your child's chest ever made a wheezy noise while playing or right after? (9) Besides from a cough brought on by a cold or chest illness, has your child experienced a cough that is dry at night in the last 12 months?
The classification of Current Severe Wheeze was determined if parents provided affirmative responses to every one of the subsequent questions: 1) If children have severe wheezing, with a frequency of 4-12 bouts or over 12 episodes throughout the preceding 12-month period. 2) If the children experience disrupted sleep as a result of wheezing at least once a week or more. 3) In the event that children experienced a wheezing episode within the last 12 months, resulting in a restriction of their ability to speak to just a few phrases at a time due to intermittent breaths. 4) If the children have experienced wheezing symptoms during or following physical activity throughout the preceding 12-month period.
2.5. Environmental Tobacco Smoke Exposure
Parents and caregivers were requested to provide responses pertaining to risk factors associated with wheezing, a symptom commonly observed in individuals with asthma. The questions encompassed the following: Does the male parent engage in smoking behaviour? (yes/no), Is the female parent engaged in the act of smoking? (yes/no).
The present study examines the extent of children's exposure to smoking inside their household during the past 30 days, categorized into several frequency levels: never, 1-6 days, 7-10 days, 16-20 days, and more than 20 days. The present study examines the prevalence of children's exposure to smoking inside the school environment over a period of 30 days.
The duration of the observed time intervals ranges from never through 1-6 days, 7-10 days, 16-20 days, and more than 20 days. The present study examines the extent to which children have been exposed to smoking in cars or other modes of transportation within the preceding 30 days. The duration of the event might vary, ranging from less than a week to over three weeks. The present study examines the frequency of children being subjected to smoking within the past 30 days in a restaurant setting. Parents/caregivers were asked to indicate the number of days in which children were exposed to smoking, with response options ranging from never to more than 20 days. In addition, what is the number of individuals residing in the household of your child that engages in smoking?
2.6. Confounders
Parents and caregivers were asked to answer a series of questions about the following topics: Gender of the child (male/female), Location of the child (rural/urban), and How long has the child lived in the area? (6 to 12 months/1 to 2 years/3 years or longer), Was the child born in the area? (Hospital/Clinic/Home/does not apply), What kind of residence does the child live in? (Brick/Mud/Corrugated Iron/Mixture/Other), In the last 12 months, the child used analgesics/antibiotics (Never/At least once a year/At least once per month. What type of fuel is utilized for cooking and heating (electricity/gas/paraffin/coal/wood/other)? How does the child get to and from school? (walks/taxi/bus/motor vehicle/combination/other). How frequently do trucks, buses, and taxis pass through your neighbourhood? (Never/rarely/frequently throughout the day/almost the entire day. Other questions focused on pet ownership, education for parents/caregivers, Job occupation of parents/caregivers and family health history.
2.7. Data Processing and Analysis
The data were captured using EpiData version 3.1[20] for the purpose of ensuring quality and subsequently analysed using STATA 17. Descriptive statistics were computed, utilizing means and standard deviations for continuous data, and frequencies expressed as percentages for categorical data. Observations that were labelled as "not recorded" were designated as missing. Consequently, there were variations in the sample sizes utilized to address each respective question.
In this study, we assessed the association between demographic factors, including gender, age, location, and family history, with four outcome variables: Wheeze Ever, Current Wheeze, Current Severe Wheeze and Asthma Ever. Statistical comparisons were conducted using the chi-square test for independent samples. The researchers employed multiple logistic regression to account for any confounding variables, assessing the strength of the relationship using the odds ratio (OR) and 95% confidence intervals (CI). For outcomes with two categories, binary multiple logistic regression was utilized.
3. Results
Description of Study Participants
We identified 3900 pre-schoolers and invited their parents using participant information leaflets to be part of the study. Three thousand one-hundred and forty-five parents permitted their children and consented to participate, which was a participation rate of 80.6%. The pre-schoolers were, on average, 4.05 (SD=1.22) years old. Most pre-schoolers were within the age range of 3 to 5 years, which fell within the 50th percentile. There were 1 605 (51%) boys and 1 540 (48.9%) girls. Most pre-schoolers (75%) resided in rural areas, while 774 (25%) lived in urban areas. Moreover, a significant majority of pre-school-aged children (87%) were born in hospitals located in suburbs or township areas. Additionally, a substantial proportion of these children (80%) resided in these suburban or township regions for a duration of three years or more.
Table 1 provides a concise overview of the basic characteristics exhibited by children while Table 2 presents the environmental tobacco smoke exposure sources and health outcomes of the study participants. Study findings revealed that 23.56% of pre-school children had male parents who engaged in smoking, whereas just 3.10% of pre-school children had female parents who engaged in smoking. According to Table 2, a total of 28.86% of pre-schoolers resided in households where one or more individuals engaged in smoking activities within the same living space.
The study found that the overall prevalence of wheeze ever among the pre-schoolers was 15.14%, with a greater prevalence observed among urban pre-schoolers compared to their rural counterparts (20.7% vs 13.3%, p<0.001). Moreover, the total prevalence of asthma ever was 2.34% The prevalence was also greater in urban pre-schoolers compared to rural pre-schoolers (3.9% vs 1.8%, P<0.001). The prevalence of Current Wheeze was found to be higher than that of Current Severe Wheeze and Asthma ever, as indicated in Table 2.
The prevalence rates of Wheeze ever, Current wheeze, and Asthma ever among urban pre-schoolers residing in households with one or more individuals who engage in smoking were found to be 23.11%, 14.14%, and 5.97%, respectively. In comparison, their rural counterparts exhibited prevalence rates of 17.15%, 12.93%, and 2.32% for the same respiratory conditions.
Furthermore, urban pre-school children exposed to smoking at restaurants in the past 30 days had a 37.50% prevalence rate of Current wheeze, while their rural counterparts had a prevalence of 11.32% for the same exposure days. Contrary to the above, it was observed that rural pre-school children who had a female parent or caregiver who smoked exhibited a significantly higher prevalence of current wheeze, with a rate of 26.31%. The data presented in Table 3 illustrates the relevant information pertaining to the topic at hand.
The prevalence of wheeze ever in both rural and urban areas combined exhibited a greater incidence among boys (16.73%) compared to girls (13.49%). The data presented in Table 4 and Table 6 indicate that there is a larger prevalence of current severe wheeze among boys (1.75%) compared to girls (0.78%) in both rural and urban areas.
Table 3 shows the multiple logistic regression analysis of risk factors for Wheeze ever, Current Wheeze, Current Severe Wheeze and Asthma ever for rural and urban areas, with their respective odds ratios. Both urban and rural area children who lived with one or more people who smoked in the same house (WE: OR 1.44, 95% CI 1.11-1.86) (CW: OR 2.09, 95% CI 1.38-3.16) and (AE: OR 2.49, 95% CI 1.12-5.54) were found to have an increased likelihood for having Wheeze ever, Current Wheeze and Asthma ever as compared to those who lived with non-smokers. Moreover, those children exposed to smoking at the restaurant for one or more days in the past 30 days (CW: OR 2.27, 95% CI 1.17-4.38) were more likely to present with current wheeze as compared to those who lived with non-smokers.
In the context of combined rural and urban areas, Wheeze Ever and Current Wheeze shared similar ETS risk factors. The occurrence of symptoms was shown to be significantly higher in cases when a female parent or caregiver engaged in smoking behaviour. The crude odds ratios (OR) for Wheeze Ever and Current Wheeze were 3.11 (95% CI 2.00-4.83), and 3.12 (95% CI 1.90-5.12), respectively. In addition, there was a notable relationship between the number of smoking individuals residing in the same household as pre-schoolers and the likelihood of developing Wheeze ever, Current Wheeze, and Current Severe Wheeze. The adjusted odds ratios for these associations were 1.37 (1.08-1.74), 2.09 (1.38-3.16), and 2.46 (1.25-4.85), respectively, as indicated in Table 4, Table 5, and Table 6.
Some of the confounders that showed significant associations with Wheeze Ever in both rural and urban areas were children pre-schoolers using analgesic/antibiotics in the past 12 months at least once a year (adjusted OR 2.29, 95% CI 1.41-3.71) and pre-schoolers using a motorcar as their mode of transportation to school (adjusted OR 1.74, 95% CI 1.27-2.38) (refer to Table 4). The male gender was shown to be associated with a higher probability of experiencing both Wheeze ever (OR 1.35, 95% CI 1.08-1.70) and Current Severe Wheeze (OR 2.30, 95% CI 1.09-4.84) according to the data presented in Table 4 and Table 6. Having a female parent or caregiver who worked in the government sector was shown to be associated with an elevated probability of experiencing Current Wheeze, as indicated by an odds ratio of 1.64 (95% CI 1.06-2.54), as presented in Table 5. The presence of a dog in the household during a period of 12 months has been found to be associated with an increased probability of experiencing both Current Wheeze (OR 1.79, 95% CI 1.28-2.51) according to the crude odds ratios reported in Table 5.
4. Discussion
This study aimed to assess the association between environmental tobacco smoke exposure and the occurrence of wheeze, a common symptom of asthma, among pre-school children residing in rural and urban areas of Mpumalanga province, South Africa. The reported prevalence of wheeze in Mpumalanga is similar to that observed in previous research. Based on the findings of the ISAAC Phase Three study, it was determined that the worldwide prevalence of current wheeze among school-aged children was 11.5%. This prevalence showed significant regional variation, varying from 6.8% in the Indian subcontinent to 21% in Oceania [21]. Furthermore, the prevalence of current wheeze (10%) and lifetime asthma (3.4%) in Africa exhibited a comparable pattern to the outcomes observed in our study [21]. Additionally, the findings of Wichmann et al. [22] who conducted a study on the potential risk factors for asthma symptoms in school-aged children from Polokwane Limpopo province in South Africa, using the ISAAC questionnaire, support our study results. The prevalence of wheeze (11.2%) and severe wheeze (5.7%) observed in their study aligns with the findings of our study.
The potential influence of various factors on the prevalence of asthma symptoms within a given region can be attributed to several key variables, including the age range of children considered in the study, the prevailing climate conditions, the specific timing of the study, the size of the sampled population, the design of the study itself, and the presence or absence of certain risk factors. Research studies that specifically examine children within similar age groups, as well as children residing in a particular place for a duration beyond six months, have found comparable rates of asthma symptom prevalence. Based on the aforementioned findings, it is evident that the management of asthma symptoms poses a persistent problem. Consequently, it may be necessary to formulate and execute strategies aimed at mitigating these symptoms within this specific demographic promptly.
This study found that there was a higher prevalence of wheeze ever and asthma ever among pre-schoolers living in urban areas compared to those residing in rural areas. Consistent with the results of our study, Chakravarthy et al, [23] Wehrmeister et al, [24] Feng et al, [25] and Kutzora et al [26] conducted research in India, Brazil, China, and Germany respectively, which also indicated a greater prevalence of asthma symptoms among children residing in urban regions compared to those dwelling in rural areas. The present study found that children residing in the Mpumalanga Highveld region were predominantly impacted by wheeze ever, a common symptom of asthma, as well as a history of asthma ever, particularly if they attended an urban pre-school. The results of our study align with the majority of existing literature, which consistently demonstrates that residing in rural areas or on farms, being exposed to livestock, and the hygiene hypothesis confers protective advantages against the development of asthma symptoms in childhood, compared to children residing in urban areas [26,27,28,29,30]. Additionally, our research findings provide support for the notion that children residing in urban areas are more prone to increased exposure and heightened sensitivity to several risk factors associated with asthma symptoms [29,31].
The study outcome indicated above may have been influenced by specific environmental factors. The regions of Mpumalanga Highveld exhibit a notable deterioration in air quality, with heightened levels of pollutants stemming from both industrial and non-industrial origins. The district encompasses a variety of sectors, namely power generating, petrochemical, primary metallurgy, and open-cast mining. Urban environments possess a multitude of modifiable exposures that can impact the prevalence and morbidity of asthma symptoms. In the aggregate of both rural and urban areas, boys had a greater propensity for experiencing wheeze ever at any point and current severe wheeze in comparison to their girls' counterparts.
This observation aligns with previous research indicating that boys consistently have a higher incidence of wheezing and/or asthma symptoms relative to girls [32,33,34].
Risk factors and confounders associated with wheeze, a symptom commonly observed in individuals with asthma, were identified in our study. The risk factors with the highest potential for modification encompassed a female parent who engages in smoking, a male parent who engages in smoking, the number of individuals residing in the same household as a child who engages in smoking, exposure to smoking within the home (within the previous 30 days), exposure to smoking within a motor vehicle or transportation (within the previous 30 days), exposure to smoking within a restaurant (within the previous 30 days), the mode of transportation utilized to commute to school, and ownership of a pet.
This study found that pre-schoolers were more likely to experience wheeze ever and current wheeze in their lives, if they had a female parent or caregiver who smoked and also those who lived in the same household with one or more people who smoked. Those who were exposed to smoking in cars and restaurants in the past 30 days were more likely to present with current wheeze. The results of our study are consistent with existing literature, which indicates that children are primarily exposed to environmental tobacco smoke (ETS) through smoking by adults in environments where children reside and engage in recreational activities. This exposure significantly increases their susceptibility to developing asthma and respiratory symptoms [17,30,35,36].
According to studies conducted by Tsai et.al. [37] and Shahunja et al. [38] there exists a significant relationship between the prevalence of asthma symptoms in children and their exposure to household tobacco smoke. Moreover, Wang et al. [39] conducted a study that revealed a significant relationship between the presence of wheezing symptoms in children and their exposure to second-hand smoke. In addition, Tabuchi et al. [40] and Harju et al. [41] also reported that children who had two smoking parents were more likely to have asthma symptoms and had a greater chance of asthma attacks relative to children with non-smoking parents [42]. Tsai et al [43] provided additional support for the aforementioned results, since they demonstrated that the combined exposure to smoking from both fathers and mothers amplifies the impact of asthma symptoms. According to the findings of Jung et al. [44] there was a notable relationship between parental smoking and an increased incidence of respiratory complaints among children, as compared to those whose parents did not smoke.
Although the presence of second-hand smoke has been identified as a significant indicator of asthma symptoms, there remains a lack of consensus regarding the specific threshold at which exposure to smoking becomes detrimental. It is thus highly advisable to completely refrain from exposure to second-hand smoke and to ensure that household members who smoke confine their smoking activities to isolated areas that are inaccessible to these children [45]. Parents should additionally take into consideration the implementation of a prohibition on smoking within the confines of their residence or its immediate vicinity.
Additionally, our study revealed that preschool-aged children who have been subjected to ETS in cars or transport without a complete physical barrier within the last 30 days were shown to have a higher likelihood of experiencing current wheeze. In addition, our research revealed an association between the utilization of motor vehicles for transportation to school among preschool-aged children and an increased likelihood of experiencing wheeze ever.
The anticipated outcomes of this study are in line with expectations, as the act of parents or caregivers smoking in the car during the transportation of children to school has been found to elevate exposure to ETS and therefore raise the probability of experiencing symptoms associated with asthma. The existing body of literature on the exposure of children to ETS and its impact on the development of respiratory and asthma symptoms provides substantial data that aligns with the findings of the aforementioned study [15,16,17,35,46]. Additionally, the use of motor vehicles may contribute to an increased likelihood of experiencing symptoms associated with asthma. Gasana and colleagues [47] conducted a study that corroborated the aforementioned findings, as they concluded that children who are exposed to elevated amounts of air pollution from motor vehicles are more likely to exhibit symptoms of childhood wheezing. It is advisable to prioritize the avoidance of ETS exposure as a crucial factor in mitigating the onset and facilitating the control of asthma and related symptoms [48].
5. Strength and Limitation of the Study
Firstly, the ISAAC questionnaire is a valid tool for data collection for this investigated population group and has been utilized worldwide in studies investigating asthma symptoms. Secondly, this study had a great participation rate with over 3000 children, which is a requirement by ISAAC centres, thus increasing the study's statistical power. Final: The implementation of a standardized and validated tool facilitates the ability to compare study findings with those of other studies conducted at various levels, including local, regional, and international contexts.
The study outcomes may deviate slightly from the actual prevalence of investigated symptoms due to the presence of missing data. Future research endeavours should prioritize the meticulous completion of questionnaires, aiming to minimize the occurrence of missing data to a significant extent. The study gathered data from the past year by using a parental-completed questionnaire. It was anticipated that these parents, who primarily reside with the children, would be able to accurately recall the information requested. The one-year timeframe was considered sufficient for recollection, without posing significant obstacles.
6. Conclusions
The study found that in Mpumalanga, pre-schoolers living in urban areas had a higher prevalence of wheeze ever, current wheeze, current severe wheeze and asthma ever relative to rural pre-schoolers. The presence of ETS exposure among preschool-aged children in various settings, including their homes, restaurants, and during transportation, increased the probability of experiencing wheezing. The implementation of smoking limits and prohibition is crucial in areas that are frequented or utilized by children. Hence, it is imperative for healthcare providers to actively champion the rights of individuals who do not smoke within the society, while also endorsing legislative measures aimed at curtailing tobacco smoke exposure.
Author Contributions
RM: JS, and KV participated in the study's design, RM was involved in the data collection and statistical analysis, and RM, JS, and KV were involved in interpreting the results and drafting and critically revising the manuscript. The published version of the work has been reviewed and approved by all authors.
Funding
The study was financially supported by the South African Medical Research Council's Division of Research Capacity Development, specifically through the Bongani Mayosi National Health Scholars Programme. The funding for this program was obtained through the Public Health Enhancement Fund, which is administered by the South African National Department of Health. The authors bear sole responsibility for the content herein, and it should be noted that the opinions expressed do not necessarily reflect the official stance of the SAMRC.
Institutional Review Board Statement
The present study received approval from the University of Pretoria Research Ethics Committee (Ethics Number: 766/2019), as well as the Gert Sibande District Municipality - Environmental Health Department and school principals. Consent for participation in the study was obtained from all parents and caregivers of the children.
Informed Consent Statement
Prior to their participation in the study, parental or caregiver agreement was obtained for the children.
Data Availability Statement
We did not receive ethics approval to share raw field data publicly. The data belong to the University of Pretoria (UP). The raw data analysed in the current study are available from UP on reasonable request.
Acknowledgments
The authors would like to thank everybody who participated in the study, the South African Medical Research Council and the University of Pretoria.
Conflicts of Interest
The author(s) declare no potential conflicts of interest concerning this article's research, authorship, and/or publication.
Abbreviations
ETS- environmental tobacco smoke
OR- odds ratio
ISAAC- International study of asthma and allergies in childhood
SD- standard deviation
CI- confidence interval
χ2- chi square
P- P value
References
- Brand PL, Baraldi E, Bisgaard H, Boner A, Castro-Rodriguez J, Custovic A, et al. Definition, assessment and treatment of wheezing disorders in preschool children: An evidence-based approach. Eur Respir J. 2008; 32(4):1096-110. [CrossRef]
- Carlsen KL, Håland G, Devulapalli C, Munthe-Kaas M, Pettersen M, Granum B, et al. Asthma in every fifth child in oslo, norway: A 10-year follow up of a birth cohort study. Allergy. 2006; 61(4):454-60.
- Morgan WJ, Stern DA, Sherrill DL, Guerra S, Holberg CJ, Guilbert TW, et al. Outcome of asthma and wheezing in the first 6 years of life: Follow-up through adolescence. Am J Respir Crit Care Med. 2005; 172(10):1253-8.
- Taussig LM, Wright AL, Holberg CJ, Halonen M, Morgan WJ, Martinez FD. Tucson children's respiratory study: 1980 to present. J Allergy Clin Immunol. 2003; 111(4):661-75.
- Stein RT, Holberg CJ, Morgan WJ, Wright AL, Lombardi E, Taussig L, Martinez FD. Peak flow variability, methacholine responsiveness and atopy as markers for detecting different wheezing phenotypes in childhood. Thorax. 1997; 52(11):946-52. [CrossRef]
- Martinez FD, Wright AL, Taussig LM, Holberg CJ, Halonen M, Morgan WJ, Associates GHM. Asthma and wheezing in the first six years of life. N Engl J Med. 1995; 332(3):133-8. [CrossRef]
- Ferrante G, La Grutta S. The burden of pediatric asthma. Frontiers in pediatrics. 2018; 6:186.
- Castro-Rodriguez JA, Forno E, Rodriguez-Martinez CE, Celedón JC. Risk and protective factors for childhood asthma: What is the evidence? The Journal of Allergy and Clinical Immunology: In Practice. 2016; 4(6):1111-22.
- GINA [Internet]. Global initiative for asthma - global initiative for asthma - gina. 2019 [cited 2019 Sep 07]. Available from: https://ginasthma.org/.
- Hedlin G, Bush A, Carlsen KL, Wennergren G, De Benedictis F, Melén E, et al. Problematic severe asthma in children, not one problem but many: A ga2len initiative. Eur Respiratory Soc; 2010. [CrossRef]
- Cutrera R, Baraldi E, Indinnimeo L, Del Giudice MM, Piacentini G, Scaglione F, et al. Management of acute respiratory diseases in the pediatric population: The role of oral corticosteroids. Italian journal of pediatrics. 2017; 43(1):31. [CrossRef]
- Pedro CR, Freitas PP, Papoila AL, Dias SS, Caires I, Martins P, Neuparth N. Respiratory diseases in children attending kindergartens: Health-related variables and mothers’ psychological, parental, and marital functioning. Health psychology open. 2017; 4(2):2055102917724334.
- Zar HJ, Ferkol TW. The global burden of respiratory disease—impact on child health. Pediatric pulmonology. 2014; 49(5):430-4. [CrossRef]
- Carraro S, Scheltema N, Bont L, Baraldi E. Early-life origins of chronic respiratory diseases: Understanding and promoting healthy ageing. Eur Respiratory Soc; 2014. [CrossRef]
- Morkjaroenpong V, Rand CS, Butz AM, Huss K, Eggleston P, Malveaux FJ, Bartlett SJ. Environmental tobacco smoke exposure and nocturnal symptoms among inner-city children with asthma. J Allergy Clin Immunol. 2002; 110(1):147-53. [CrossRef]
- Cheraghi M, Salvi S. Environmental tobacco smoke (ets) and respiratory health in children. Eur J Pediatr. 2009; 168:897-905. [CrossRef]
- CHAN-YEUNG M, DIMICH-WARD H. Respiratory health effects of exposure to environmental tobacco smoke. Respirology. 2003; 8(2):131-9. [CrossRef]
- Lawson JA, Rennie DC, Cockcroft DW, Dyck R, Afanasieva A, Oluwole O, Afsana J. Childhood asthma, asthma severity indicators, and related conditions along an urban-rural gradient: A cross-sectional study. BMC Pulm Med. 2017; 17(1):1-9. [CrossRef]
- Municipality GSD [Internet]. Database. 2020.
- Epidata [Internet]. Data analytics solutions. 2023 [cited 2021 14 August 2021].
- Lai CK, Beasley R, Crane J, Foliaki S, Shah J, Weiland S, Group IPTS. Global variation in the prevalence and severity of asthma symptoms: Phase three of the international study of asthma and allergies in childhood (isaac). Thorax. 2009; 64(6):476-83. [CrossRef]
- Wichmann J, Wolvaardt JE, Maritz C, Voyi KV. Household conditions, eczema symptoms and rhinitis symptoms: Relationship with wheeze and severe wheeze in children living in the polokwane area, south africa. Maternal and child health journal. 2009; 13:107-18. [CrossRef]
- Sibi Chakravarthy K, Singh RB, Swaminathan S, Venkatesan P. Prevalence of asthma in urban and rural children in tamil nadu. Natl Med J India. 2002; 15(5):260-3.
- Wehrmeister FC, Menezes AMB, Cascaes AM, Martínez-Mesa J, Barros AJ. Time trend of asthma in children and adolescents in brazil, 1998-2008. Rev Saude Publica. 2012; 46:242-50.
- Feng M, Yang Z, Pan L, Lai X, Xian M, Huang X, et al. Associations of early life exposures and environmental factors with asthma among children in rural and urban areas of guangdong, china. Chest. 2016; 149(4):1030-41. [CrossRef]
- Kutzora S, Weber A, Heinze S, Hendrowarsito L, Nennstiel-Ratzel U, von Mutius E, et al. Asthmatic/wheezing phenotypes in preschool children: Influential factors, health care and urban-rural differences. Int J Hyg Environ Health. 2018; 221(2):293-9. [CrossRef]
- Von Mutius E. Asthma and allergies in rural areas of europe. Proc Am Thorac Soc. 2007; 4(3):212-6.
- Milligan KL, Matsui E, Sharma H. Asthma in urban children: Epidemiology, environmental risk factors, and the public health domain. Curr Allergy Asthma Rep. 2016; 16:1-10. [CrossRef]
- Milligan KL, Matsui E, Sharma H. Asthma in urban children: Epidemiology, environmental risk factors, and the public health domain. Curr Allergy Asthma Rep. 2016; 16(4):33. [CrossRef]
- Xing Y, Leung ASY, Wong GWK. From preschool wheezing to asthma: Environmental determinants. Pediatr Allergy Immunol. 2023; 34(11):e14049.
- Meireles-Neto I, Pimentel AM, Parreira JN, Fontoura M-SH, Nascimento-Carvalho CM, editors. Recurrent wheezing, allergic rhinitis, and maternal asthma as predictors of asthma in children. Allergy Asthma Proc; 2020. [CrossRef]
- Almqvist C, Worm M, Leynaert B, ‘Gender’ wgoGLW. Impact of gender on asthma in childhood and adolescence: A ga2len review. Allergy. 2008; 63(1):47-57. [CrossRef]
- Chen Y, Stewart P, Johansen H, McRae L, Taylor G. Sex difference in hospitalization due to asthma in relation to age. J Clin Epidemiol. 2003; 56(2):180-7.
- Yung JA, Fuseini H, Newcomb DC. Sex hormones, gender and asthma. Annals of allergy, asthma & immunology: official publication of the American College of Allergy, Asthma, & Immunology. 2018; 120(5):488.
- Dai S, Chan KCC. Household environmental tobacco smoke exposure in healthy young children in hong kong: Prevalence and risk factors. PLoS One. 2020; 15(1):e0227733. [CrossRef]
- Blázquez ML, Moreno JP, Vázquez SV, Fernández RR. Impact of passive smoking on lung function and asthma severity in children. Arch Bronconeumol. 2018; 54(8):436-7. [CrossRef]
- Tsai C-H, Huang J-H, Hwang B-F, Lee YL. Household environmental tobacco smoke and risks of asthma, wheeze and bronchitic symptoms among children in taiwan. Respir Res. 2010; 11(1):1-10. [CrossRef]
- Shahunja K, Sly PD, Chisti MJ, Mamun A. Trajectories of asthma symptom presenting as wheezing and their associations with family environmental factors among children in australia: Evidence from a national birth cohort study. BMJ open. 2022; 12(6):e059830. [CrossRef]
- Wang Z, May SM, Charoenlap S, Pyle R, Ott NL, Mohammed K, Joshi AY. Effects of secondhand smoke exposure on asthma morbidity and health care utilization in children: A systematic review and meta-analysis. Annals of Allergy, Asthma & Immunology. 2015; 115(5):396-401. e2. [CrossRef]
- Tabuchi T, Fujiwara T, Nakayama T, Miyashiro I, Tsukuma H, Ozaki K, Kondo N. Maternal and paternal indoor or outdoor smoking and the risk of asthma in their children: A nationwide prospective birth cohort study. Drug Alcohol Depend. 2015; 147:103-8. [CrossRef]
- Harju M, Keski-Nisula L, Georgiadis L, Heinonen S. Parental smoking and cessation during pregnancy and the risk of childhood asthma. BMC Public Health. 2016; 16(1):1-7. [CrossRef]
- Dai R, Miliku K, Gaddipati S, Choi J, Ambalavanan A, Tran MM, et al. Wheeze trajectories: Determinants and outcomes in the child cohort study. J Allergy Clin Immunol. 2022; 149(6):2153-65. [CrossRef]
- Akinbami LJ, Kit BK, Simon AE. Impact of environmental tobacco smoke on children with asthma, united states, 2003–2010. Acad Pediatr. 2013; 13(6):508-16. [CrossRef]
- Jung JW, Ju YS, Kang HR. Association between parental smoking behavior and children's respiratory morbidity: 5-year study in an urban city of south korea. Pediatr Pulmonol. 2012; 47(4):338-45.
- DiFranza JR, Aligne CA, Weitzman M. Prenatal and postnatal environmental tobacco smoke exposure and children’s health. Pediatrics. 2004; 113(Supplement 3):1007-15.
- Dai S, Chan KC. Associations of household environmental tobacco smoke exposure with respiratory symptoms and utilisation of medical services in healthy young children in hong kong. Tob Induc Dis. 2020; 18. [CrossRef]
- Gasana J, Dillikar D, Mendy A, Forno E, Vieira ER. Motor vehicle air pollution and asthma in children: A meta-analysis. Environ Res. 2012; 117:36-45. [CrossRef]
- Halterman JS, Fagnano M, Conn KM, Szilagyi PG. Do parents of urban children with persistent asthma ban smoking in their homes and cars? Ambul Pediatr. 2006; 6(2):115-9.
Figure 1.
Geographical distribution of preschools within the Gert Sibande District Municipality. a) Provides a visual representation of the global location of the preschools within the Gert Sibande municipality. b) Present the spatial distribution of the Gert Sibande municipality in the province of Mpumalanga within the broader context of the nine provinces of South Africa. c) An illustration depicting the inclusion of all seven local municipalities within the Gert Sibande district, wherein preschools were identified, highlighted in a light-yellow colour. Source: https://en.wikipedia.org/wiki/List_of_municipalities_in_Mpumalanga.
Figure 1.
Geographical distribution of preschools within the Gert Sibande District Municipality. a) Provides a visual representation of the global location of the preschools within the Gert Sibande municipality. b) Present the spatial distribution of the Gert Sibande municipality in the province of Mpumalanga within the broader context of the nine provinces of South Africa. c) An illustration depicting the inclusion of all seven local municipalities within the Gert Sibande district, wherein preschools were identified, highlighted in a light-yellow colour. Source: https://en.wikipedia.org/wiki/List_of_municipalities_in_Mpumalanga.
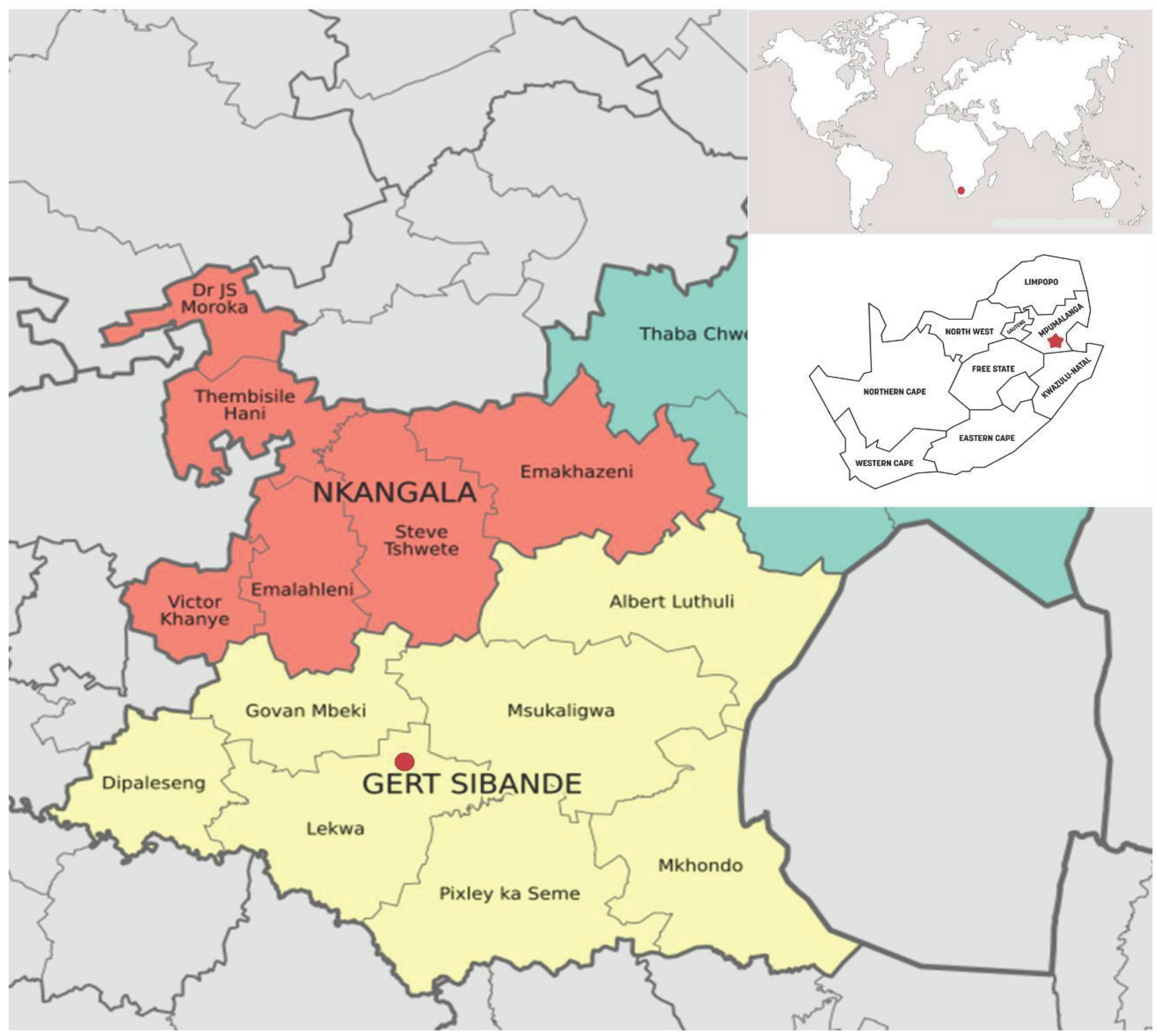

Table 1.
The demographic characteristics of the participants in the study (n=3145).
| Variables | N | Percentage (%) |
|---|---|---|
|
1. Gender of the child Female Male |
1540 1605 |
48.97 51.03 |
|
2. Age group of children < 3 years 3-5 years ≥ 5 years |
414 1779 952 |
13.16 56.57 30.27 |
|
3. Child location Rural Urban |
2372 773 |
75.42 24.58 |
|
4. Time lived in Suburb/township Less than 6 months 6 to 12 months 1 to 2 years 3 years or longer Missing |
107 99 408 2450 81 |
3.40 (3.49) 3.14 (3.23) 12.9 (13.32) 77.90 (79.96) 2.57 |
|
5. Type of house the child lives ina Brick Mud Corrugated iron Combination Other Missing |
2547 116 255 93 81 53 |
80.98 (82.37) 3.68 (3.75) 8.10 (8.25) 2.95 (3.01) 2.57 (2.62) 1.68 |
|
6. Fuel used for cooking in the houseb Electricity Gas Paraffin Coal WoodOther Missing |
2476 100 19 254 292 2 2 |
78.72 (78.78) 3.17 (3.18) 0.60 (0.60) 8.07 (8.08) 9.28 (9.29) 0.06 (0.06) 0.06 |
| 7. Fuel used for heating in the housec Electricity Gas Paraffin Coal Wood Other Missing |
2008 198 27 484 380 19 29 |
63.84 (64.44) 6.29 (6.35) 0.85 (0.87) 15.38 (15.53) 12.08 (12.20) 0.60 (0.61) 0.92 |
|
8. Child used Analgesic/antibiotic in the past 12 months Never At least once a year At least once per month Missing |
445 921 1683 96 |
14.14 (14.59) 29.28 (30.21) 53.51 (55.20) 3.05 |
|
9. How does the child get to schoold Walk Taxi/bus Motor car Combination Other Missing |
1666 848 525 57 23 26 |
52.97 (53.41) 26.96 (27.19) 16.69 (16.83) 1.81 (1.83) 0.73 (0.74) 0.82 |
|
10. How often has your child been absent from school (past 6 months) Never or occasionally Once or twice per week Three or more times a week Missing |
1854 904 256 131 |
58.95 (61.51) 42.14 (29.99) 8.13 (8.49) 4.1 |
|
11. Child Ever Breastfed No Yes Missing |
974 2125 46 |
30.96 (31.43) 67.46 (68.57) 1.46 |
|
12. Truck traffic pass through the street on weekend Never Seldom Frequent through the day Almost all day Missing |
518 735 713 1083 96 |
16.47 (16.99) 23.37 (24.11) 22.67(23.38) 34.43 (35.52) 3.0 |
|
13. Female parent: Highest level of school completed Primary Secondary University Other Missing |
246 1884 454 422 139 |
7.82 (8.18) 59.90 (62.67) 14.43 (15.10) 13.41 (14.04) 4.41 |
|
14. Female parent job industry Government sector Private sector Self-employed Not employed Missing |
351 580 308 1745 161 |
11.16 (11.76) 18.44 (19.44) 9.79(10.32) 55.48 (58.48) 5.11 |
|
15. Female parent ever asthma No Yes Missing |
2487 79 579 |
79.09 (96.92) 2.51 (3.08) 18.41 |
|
16.Cat inside the house No Yes Missing |
2885 223 37 |
91.17 (92.82) 7.09 (7.18) 1.17 |
|
17.Dog inside the house No Yes Missing |
2780 331 34 |
88.39 (89.36) 10.52 (10.64) 1.08 |
( ) Missing data was excluded from the data analysis. a Combination includes Brick & Corrugated iron: Other includes wood. b Other include generator. c Other include Solar energy/electricity. d Combination includes motorcar and Taxi/bus: Other includes animal cart.
Table 2.
Environmental tobacco smoke exposure sources and health outcomes of the study participants (n=3145).
Table 2.
Environmental tobacco smoke exposure sources and health outcomes of the study participants (n=3145).
| Variables | N | Percentages (%) |
|---|---|---|
|
1. Female parent smokes Yes No Missing |
94 2934 117 |
2.98 (3.10) 93.29 (96.90) 3.72 |
|
2. Male parent smokes Yes No Missing |
451 1463 1231 |
14.34 (23.56) 46.51 (76.44) 39.14 |
|
3. How many people living in the same house as your child smoke? Zero One or more Missing |
2051 832 262 |
65.21 (71.14) 26.45 (28.86) 8.33 |
|
4. Child exposure to smoking at home (past 30 days) Never One or more days* Missing |
1947 396 802 |
61.90 (83.10) 12.59 (16.90) 25.50 |
|
5. Child exposure to smoking at school (past 30 days) Never One or more days* Missing |
1444 40 1661 |
45.91 (97.30) 1.27 (2.70) 52.81 |
|
6. Child exposure to smoking in car/transport (past 30 days) Never One or more days* Missing |
1390 70 1685 |
44.19 (95.21) 2.25 (4.79) 53.57 |
|
7. Child exposure to smoking at the restaurant (past 30 days) Never One or more days* Missing |
1387 79 1678 |
44.10 (94.61) 2.51 (5.39) 53.35 |
|
8. Wheeze ever Yes No Missing |
467 2617 61 |
14.8 (15.14) 83.2 (84.86) 1.9 |
|
9. Current wheeze Yes No Missing |
292 2799 54 |
9.2 (9.45) 88.9 (90.55) 1.7 |
|
10. Current severe wheeze Yes No Missing |
40 3076 29 |
1.27 (1.28) 97.8 (98.72) 0.92 |
|
11. Ever had asthma Yes No Missing |
66 2810 269 |
2.09 (2.34) 89.34 (97.65) 8.55 |
|
12. Wheeze attack in the past 12 months Yes No Missing |
274 2815 56 |
8.71(8.87) 89.50 (91.13) 1.78 |
|
13. Sleep disturbed due to wheeze in the past 12 months Yes No Missing |
199 2888 58 |
6.32 (6.45) 91.82 (93.55) 1.82 |
|
14. Wheeze severe enough to limit speech in the past 12 months Yes No Missing |
59 3016 75 |
1.87 (1.92) 95.89 (98.08) 2.38 |
|
15. Asthma diagnosed by a medical Doctor or Nurse Yes No Missing |
54 2929 162 |
1.71 (1.81) 93.13 (98.19) 5.15 |
|
16. Chest ever sounded wheezy during/after playing Yes No Missing |
232 2398 515 |
7.37 (8.82) 76.24 (91.18) 16.37 |
|
17. Dry cough at night apart from cough associated with cold or chest infection Yes No Missing |
650 2229 266 |
20.66 (22.58) 70.87 (77.42) 8.45 |
( ) Missing data was excluded from the data analysis. * One or more days include the following days range:1-6 days;7-10 days;16-20 days; more than 20 days.
Table 3.
Participants’ prevalence of wheeze ever, current wheeze, current severe wheeze and asthma ever for rural and urban areas with their respective odds ratios.
Table 3.
Participants’ prevalence of wheeze ever, current wheeze, current severe wheeze and asthma ever for rural and urban areas with their respective odds ratios.
| Rural | Urban | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Totala | Prevalence (%) | Crude ORb | Adjusted ORb | Totala | Prevalence (%) | Crude ORb | Adjusted ORb | ||||
| (95% CI) | P | (95% CI) | P | (95% CI) | P | (95% CI) | P | |||||
|
Wheeze everc Child ever breastfed No Yes |
736 1557 |
13.99 13.10 |
1 1.01 (0.82-1.26) |
0.869 | 1 1.27 (0.96-1.67) |
0.082 | 221 529 |
18.09 21.92 |
1 1.01 (0.82-1.26) |
0.869 | 1 1.27 (0.96-1.67) |
0.082 |
|
How often have you given your child medication (past 12 months)? Never At least once a year At least once per month |
351 611 1300 |
4.55 12.43 16 |
1 2.78 (1.75-4.41) 3.98 (2.56-6.17) |
0.000 0.000 |
1 2.24 (1.32-3.81) 2.83 (1.70-4.49) |
0.003 0.000 |
84 298 350 |
8.33 18.45 36.18 |
1 2.78 (1.75-4.41) 3.98 (2.56-6.17) |
0.000 0.000 |
1 2.24 (1.32-3.81) 2.83 (1.70-4.49) |
0.0030.000 |
|
People living in the same house as your child smoke? Zero One or more |
1500 618 |
11.4 17.15 |
1 1.46 (1.17-1.82) |
0.001 | 1 1.44 (1.11-1.86) |
0.006 | 511 199 |
20.15 23.11 |
1 1.46 (1.17-1.82) |
0.001 | 1 1.44 (1.11-1.86) |
0.006 |
|
Truck traffic where your child lives on weekdays Never Seldom Frequently Almost all day |
389 492 517 854 |
13.11 12.19 14.89 12.99 |
1 1.05 (0.76-1.46) 1.32 (0.95-1.81) 1.07 (0.78-1.45) |
0.76 0.08 0.65 |
1 1.10 (0.73-1.64) 1.40 (0.94-2.07) 1.10 (0.75-1.63) |
0.636 0.092 0.601 |
120 237 187 199 |
15.83 21.09 25.13 19.59 |
1 1.05 (0.76-1.46)1.32 (0.95-1.81)1.07 (0.78-1.45) |
0.76 0.08 0.65 |
1 1.10 (0.73-1.64) 1.40 (0.94-2.07) 1.10 (0.75-1.63) |
0.6360.0920.601 |
|
Cat inside the house (past 12 months) No Yes |
2143 156 |
13.06 16.02 |
1 1.54 (1.09-2.17) |
0.012 | 1 1.39 (0.90-2.15) |
0.136 | 687 64 |
19.65 34.37 |
1 1.54 (1.09-2.17) |
0.012 | 1 1.39 (0.90-2.15) |
0.136 |
|
Female parent level of school completion Primary Secondary University Other |
222 1523 212 286 |
18.01 11.81 16.50 15.73 |
1 0.59 (0.41-0.84) 1.03 (0.68-1.55) 0.82 (0.54-1.24) |
0.004 0.871 0.354 |
1 0.76 (0.46-1.25) 1.64 (0.97-2.80) 0.99 (0.59-1.73) |
0.284 0.064 0.982 |
19 323 237 127 |
23.31 16.09 28.27 21.25 |
1 0.59 (0.41-0.84)1.03 (0.68-1.55)0.82 (0.54-1.24) |
0.004 0.871 0.354 |
1 0.76 (0.46-1.25) 1.64 (0.97-2.80) 0.99 (0.59-1.73) |
0.284 0.064 0.982 |
|
Female parent ever had Asthma No Yes |
1852 43 |
12.41 25.58 |
1 3.65 (2.28-5.85) |
0.000 | 1 3.25 (1.97-5.35) |
0.000 | 599 36 |
18.19 55.55 |
1 3.65 (2.28-5.85) |
0.000 | 1 3.25 (1.97-5.35) |
0.000 |
|
Current wheezed Female parent ever had Asthma No Yes |
1853 43 |
8.04 23.25 |
1 3.82 (2.26-6.45) |
0.000 | 1 5.59 (2.77-11.26) |
0.000 | 600 36 |
9.33 30.55 |
1 3.82 (2.26-6.45) |
0.000 | 1 5.59 (2.77-11.26) |
0.000 |
|
Child used Analgesic/antibiotic in the past 12 months Never At least once a year At least once per month |
354 609 1307 |
1.97 7.38 11.40 |
1 3.85 (1.82-8.12) 7.94 (3.89-16.22) |
0.000 0.000 |
1 3.41 (1.17-9.95) 4.74 (1.68-13.40) |
0.024 0.003 |
86 297 349 |
1.16 6.06 18.33 |
1 3.85 (1.82-8.12) 7.94 (3.89-16.22 |
0.000 0.000 |
1 3.41 (1.17-9.95) 4.74 (1.68-13.40) |
0.024 0.003 |
|
Truck traffic where your child lives on weekdays Never Seldom Frequently Almost all day |
388 489 516 865 |
8.76 8.58 10.07 8.43 |
1 0.99 (0.66-1.48) 1.40 (0.95-2.06) 1.02 (0.70-1.48) |
0.978 0.084 0.905 |
1 1.04 (0.55-1.94) 1.13 (0.60-2.11) 0.86 (0.45-1.64) |
0.902 0.695 0.653 |
120 238 186 199 |
8.33 9.24 16.66 10.05 |
1 0.99 (0.66-1.48) 1.40 (0.95-2.06) 1.02 (0.70-1.48) |
0.978 0.084 0.905 |
1 1.04 (0.55-1.94) 1.13 (0.60-2.11) 0.86 (0.45-1.64) |
0.902 0.695 0.653 |
|
Female parent job industry Government sector Private sector Self-employed Not employed |
183 371 199 1476 |
11.47 7.27 9.04 9.01 |
1 0.62 (0.40-0.96) 0.76 (0.46-1.25) 0.73 (0.50-1.06) |
0.034 0.292 0.103 |
1 0.72 (0.38-1.36) 0.85 (0.42-1.71) 0.50 (0.28-0.87) |
0.317 0.660 0.016 |
164 196 102 245 |
14.63 10.20 11.76 10.20 |
1 0.62 (0.40-0.96) 0.76 (0.46-1.25) 0.73 (0.50-1.06) |
0.034 0.292 0.103 |
1 0.72 (0.38-1.36) 0.85 (0.42-1.71) 0.50 (0.28-0.87) |
0.317 0.660 0.016 |
|
Dog inside the house (past 12 months) No Yes |
2103 205 |
8.13 15.60 |
1 1.74 (1.24-2.44) |
0.001 | 1 1.27 (0.70-2.32) |
0.419 | 639 115 |
10.79 13.04 |
1 1.74 (1.24-2.44) |
0.001 | 1 1.27 (0.70-2.32) |
0.419 |
|
Female parent smoke No Yes |
2186 76 |
8.26 26.31 |
1 3.19 (1.94-5.24) |
0.000 | 1 0.65 (0.20-2.12) |
0.488 | 698 17 |
11.31 11.76 |
1 3.19 (1.94-5.24) |
0.000 | 1 0.65 (0.20-2.12) |
0.488 |
|
People living in the same house as your child smoke? Zero One or more |
1497 626 |
7.34 12.93 |
1 1.77 (1.36-2.30) |
0.000 | 1 2.09 (1.38-3.16) |
0.000 | 511 198 |
9.39 14.14 |
1 1.77 (1.36-2.30) |
0.000 | 1 2.09 (1.38-3.16) |
0.000 |
|
Child exposure to smoking at the restaurant (past 30 days) Never One or more days |
984 53 |
8.23 11.32 |
1 2.35 (1.29-4.26) |
0.005 | 1 2.27 (1.17-4.38) |
0.014 | 381 24 |
11.81 37.5 |
1 2.35 (1.29-4.26) |
0.005 | 1 2.27 (1.17-4.38) |
0.014 |
|
Child ever breastfed No Yes |
738 1561 |
8.40 9.22 |
1 1.14 (0.87-1.49) |
0.312 | 1 1.40 (0.88-2.23) |
0.154 | 221 529 |
9.50 11.72 |
1 1.14 (0.87-1.49) |
0.312 | 1 1.40 (0.88-2.23) |
0.154 |
|
Current severe wheezee Female parent ever had Asthma No Yes |
1866 43 |
0.96 0.0 |
1 2.34 (0.53-10-19) |
0.256 | 1 2.40 (0.19-29.90) |
0.494 | 603 36 |
1.16 5.55 |
1 2.34 (0.53-10-19) |
0.256 | 1 2.40 (0.19-29.90) |
0.494 |
|
Child used Analgesic/antibiotic in the past 12 months Never At least once a year At least once per month |
355 617 1315 |
0.28 1.45 1.36 |
1 4.8 (0.61-37.98) 6.95 (0.94-51.42) |
0.134 0.057 |
1 1.43 (0.33-6.09) - |
0.624 | 85 300 351 |
0.0 0.33 0.02 |
1 4.8 (0.61-37.98) 6.95 (0.94-51.42) |
0.134 0.057 |
1 1.43 (0.33-6.09) - |
0.624 |
|
Dry cough at night apart from cough associated with cold or chest infection No Yes |
1664 492 |
0.30 4.06 |
1 16.75 (6.90-40.64) |
0.000 | 1 53.19 (7.64-370.0) |
0.000 | 564 156 |
0.17 5.12 |
1 16.75 (6.90-40.64) |
0.000 | 1 53.19 (7.64-370.0) |
0.000 |
|
Truck traffic where your child lives on weekdays Never Seldom Frequently Almost all day |
392 493 522 869 |
1.53 1.01 0.57 1.72 |
1 0.59 (0.19-1.77) 0.82 (0.29-2.28) 1.24 (0.51-3.00) |
0.348 0.707 0.626 |
1 0.04 (0.00-0.57) 1.19 (0.20-7.09) 0.32 (0.05-1.84) |
0.018 0.847 0.204 |
121 238 187 201 |
0.82 0.42 2.67 1.49 |
1 0.59 (0.19-1.77) 0.82 (0.29-2.28) 1.24 (0.51-3.00) |
0.348 0.707 0.626 |
1 0.04 (0.00-0.57) 1.19 (0.20-7.09) 0.32 (0.05-1.84) |
0.018 0.847 0.204 |
|
Male parent job industry Government sector Private sector Self-employed Not employed |
153 505 189 473 |
0.65 1.18 1.05 2.11 |
1 1.96 (0.43-8.95) 1.56 (0.25-9.51) 2.66 (0.56-12.64) |
0.381 0.625 0.217 |
1 3.07 (0.40-23-15) 1.84 (0.17-19.07) 0.23 (0.14-4.01) |
0.276 0.606 0.319 |
126 282 80 61 |
0.79 1.77 1.25 0.0 |
1 1.96 (0.43-8.95) 1.56 (0.25-9.51) 2.66 (0.56-12.64) |
0.381 0.625 0.217 |
1 3.07 (0.40-23-15) 1.84 (0.17-19.07) 0.23 (0.14-4.01) |
0.276 0.606 0.319 |
|
Dog inside the house (past 12 months) No Yes |
2119 209 |
1.13 2.39 |
1 2.60 (1.21-5.55) |
0.014 | 1 2.62 (0.38-18.03) |
0.326 | 642 116 |
0.93 3.44 |
1 2.60 (1.21-5.55) |
0.014 | 1 2.62 (0.38-18.03) |
0.326 |
|
Male parent smoke NoYes |
1017 321 |
0.98 2.49 |
1 2.57 (1.15-5.70) |
0.020 | 1 1.52 (0.28-8.11) |
0.624 | 431 128 |
0.92 2.34 |
1 2.57 (1.15-5.70) |
0.020 | 1 1.52 (0.28-8.11) |
0.624 |
|
People living in the same house as your child smoke? Zero One or more |
1515 628 |
0.99 2.22 |
1 2.23 (1.17-4.24) |
0.014 | 1 2.58 (0.55-11.95) |
0.225 | 513 199 |
0.97 2.01 |
1 2.23 (1.17-4.24) |
0.014 | 1 2.58 (0.55-11.95) |
0.225 |
|
Child exposure to smoking at the restaurant (past 30 days) Never One or more days |
994 54 |
1.20 3.70 |
1 2.67 (0.77-9.21) |
0.119 | 1 1.54 (0.10-21.38) |
0.748 | 383 24 |
2.08 4.16 |
1 2.67 (0.77-9.21) |
0.119 | 1 1.54 (0.10-21.38) |
0.748 |
|
Child exposure to smoking at the car (past 30 days) Never One or more days |
990 47 |
1.11 6.38 |
1 3.03 (0.87-10.50) |
0.079 | 1 9.44 (0.86-102.93) |
0.065 | 390 22 |
2.30 0.00 |
1 3.03 (0.87-10.50) |
0.079 | 1 9.44 (0.86-102.93) |
0.065 |
|
Child exposure to smoking at the home (past 30 days) Never One or more days |
1406 295 |
1.20 1.69 |
1 1.13 (0.46-2.77) |
0.783 | 1 0.33 (0.04-2.65) |
0.302 | 523 100 |
1.72 1.00 |
1 1.13 (0.46-2.77) |
0.783 | 1 0.33 (0.04-2.65) |
0.302 |
|
Child exposure to smoking at the school (past 30 days) Never One or more days |
1045 30 |
1.24 3.333 |
1 1.82 (0.23-13.95) |
0.562 | 1 0.13 (0.00-6.36) |
0.311 | 389 10 |
1.79 0.00 |
1 1.82 (0.23-13.95) |
0.562 | 1 0.13 (0.00-6.36) |
0.311 |
|
Child ever breastfed No Yes |
742 1575 |
1.21 1.33 |
1 1.20 (0.60-2.42) |
0.596 | 1 2.11 (0.35-12.251) |
0.408 | 221 533 |
0.90 1.50 |
1 1.20 (0.60-2.42) |
0.596 | 1 2.11 (0.35-12.251) |
0.408 |
|
How does the child get to schoolg Walk Taxi/bus Motor car Combination Other |
1527 554 201 39 14 |
1.50 0.72 1.49 0.00 0.00 |
1 0.62 (0.27-1.45) 0.84 (0.32-2.23) 1.16 (0.15-8.87) - |
0.276 0.738 0.883 |
1 0.46 (0.08-2.50) 0.31(0.05-1.87) 27.48 (1.47-511.9) |
0.375 0.203 0.026 |
126 283 320 18 9 |
0.79 1.41 1.25 5.55 0.00 |
1 0.62 (0.27-1.45) 0.84 (0.32-2.23) 1.16 (0.15-8.87) - |
0.276 0.738 0.883 |
1 0.46 (0.08-2.50) 0.31(0.05-1.87) 27.48 (1.47-511.9) |
0.375 0.203 0.026 |
|
Asthma everf People living in the same house as your child smoke? Zero One or more |
1364 558 |
1.31 2.32 |
1 175 (1.03-2.98) |
0.036 | 1 2.49 (1.12-5.54) |
0.024 | 479 184 |
3.54 5.97 |
1 175 (1.03-2.98) |
0.036 | 1 2.49 (1.12-5.54) |
0.024 |
|
Child exposure to smoking at the car (past 30 days) Never One or more days |
915 45 |
1.85 0.00 |
1 0.56 (0.07-4.21) |
0.577 | 1 0.58 (0.07-4.53) |
0.605 | 371 21 |
4.31 4.76 |
1 0.56 (0.07-4.21) |
0.577 | 1 0.58 (0.07-4.53) |
0.605 |
|
Child ever breastfed No Yes |
683 1393 |
1.75 1.86 |
1 1.22 (0.70-2.12) |
0.465 | 1 1.13 (0.48-2.68) |
0.769 | 212 485 |
2.83 4.32 |
1 1.22 (0.70-2.12) |
0.465 | 1 1.13 (0.48-2.68) |
0.769 |
|
Child used Analgesic/antibiotic in the past 12 monthsNever At least once a year At least once per month |
314 557 1176 |
0.31 1.97 0.22 |
1 3.14 (0.71-13.85) 6.14 (1.48-25.42) |
0.130 0.012 |
1 1.35 (0.14-12.40) 4.03 (0.53-30.7) |
0.788 0.178 |
76 277 328 |
1.31 1.44 6.40 |
1 3.14 (0.71-13.85) 6.14 (1.48-25.42) |
0.130 0.012 |
1 1.35 (0.14-12.40) 4.03 (0.53-30.7) |
0.788 0.178 |
|
Truck traffic where your child lives on weekdays Never Seldom Frequently Almost all day |
351 452 480 755 |
2.56 1.32 2.29 1.58 |
1 0.49 (0.22-1.07) 0.86 (0.43-1.72) 0.63 (0.32-1.26) |
0.075 0.680 0.201 |
1 0.63 (0.18-2.15) 1.05 (0.34-3.24) 0.55 (0.163-1.89) |
0.464 0.921 0.350 |
110 222 175 184 |
5.45 2.70 4.57 3.80 |
1 0.49 (0.22-1.07) 0.86 (0.43-1.72) 0.63 (0.32-1.26) |
0.075 0.680 0.201 |
1 0.63 (0.18-2.15) 1.05 (0.34-3.24) 0.55 (0.163-1.89) |
0.464 0.921 0.350 |
|
Cat inside the house (past 12 months) No Yes |
1937 145 |
1.70 3.44 |
1 2.7 (1.44-5.25) |
0.002 | 1 1.44 (0.38-5.34) |
0.584 | 636 62 |
3.30 11.29 |
1 2.7 (1.44-5.25) |
0.002 | 1 1.44 (0.38-5.34) |
0.584 |
|
Female parent level of school completion Primary Secondary University Other |
171 338 178 1321 |
3.50 1.47 2.24 1.66 |
1 0.54 (0.24-1.23) 1.03 (0.45-2.36) 0.54 (0.27-1.09) |
0.146 0.930 0.090 |
1 1.06 (0.22-5.04) 1.16 (0.21-6.47) 1.48 (0.27-7.96) |
0.936 0.858 0.647 |
149 185 101 224 |
4.69 3.24 6.93 2.67 |
1 0.54 (0.24-1.23) 1.03 (0.45-2.36) 0.54 (0.27-1.09) |
0.146 0.930 0.090 |
1 1.06 (0.22-5.04) 1.16 (0.21-6.47) 1.48 (0.27-7.96) |
0.936 0.858 0.647 |
|
Female parent ever had Asthma No Yes |
1730 39 |
1.56 15.3 |
1 7.63 (3.72-15.66) |
0.000 | 1 4.05 (1.25-13.15) |
0.020 | 560 35 |
3.21 14.28 |
1 7.63 (3.72-15.66) |
0.000 | 1 4.05 (1.25-13.15) |
0.020 |
aThe Totals for each risk factor are different due to difference in missing values. bThe Values that are statistically significant for the crude OR and less than 0.05 for the adjusted OR are highlighted. c,The Model was adjusted for: people living in the same house as your child smoke, child ever breastfed, use of analgesic/antibiotics, Truck traffic during weekdays, cat in the house, female parent education & female parent ever had asthma. dThe Model was adjusted for: female parent ever had asthma, use of analgesic/antibiotics, Truck traffic during weekdays, female parent job, dog in the house, female parent smoke, Child exposure to smoking in the restaurant & child ever breastfed. eThe Model was adjusted for: female parent ever had asthma, use of analgesic/antibiotics, dry cough at night, Truck traffic during weekdays, male parent job, dog in the house, male parent smoke, people living in the same house as your child smoke, Child exposure to smoking in the restaurant, Child exposure to smoking in the car/transport, child ever breastfed, How the child get to school, Child exposure to smoking at home, Child exposure to smoking at school. f The Model was adjusted for: people living in the same house as your child smoke, Child exposure to smoking in the car/transport, child ever breastfed, use of analgesic/antibiotics, Truck traffic during weekdays, Cat in the house, female parent education, female parent ever had asthma. g Combination includes motorcar and Taxi/bus: Other includes animal cart. -: variable contains !=0, which predicts failure perfectly. Therefore, were omitted and observations not used.
Table 4.
Participants (combined Rural and Urban areas) prevalence of wheeze ever with their respective odds ratios.
Table 4.
Participants (combined Rural and Urban areas) prevalence of wheeze ever with their respective odds ratios.
| Variable | Totala | Prevalence (%) | Crude ORb | Adjusted ORb,c | ||
|---|---|---|---|---|---|---|
| (95% CI) | P | (95% CI) | P | |||
|
People living in the same house as your child smoke? Zero One or more |
2011 817 |
13.60 18.60 |
1 1.44 (1.16-1.40) |
0.001 | 1.37 (1.08-1.74) | 0.009 |
|
Female parent smoke No Yes |
2878 92 |
14.62 34.78 |
1 3.11 (2.00-4.83) |
0.000 | 1 2.58 (1.57-4.23) |
0.000 |
|
Sex of child Female Male |
1512 1572 |
13.49 16.73 |
1 1.28 (1.05-1.57) |
0.012 | 1 1.35 (1.08-1.70) |
0.008 |
|
Child ever breastfed No Yes |
957 2086 |
15.10 15.34 |
1 1.03 (0.83-1.27) |
0.777 | 1 1.10 (0.86-1.40) |
0.436 |
|
Child used Analgesic/antibiotic in the past 12 months Never At least once a year At least once per month |
435 909 1650 |
5.28 14.41 18.24 |
1 3.01 (1.90-4.77)3.99 (2.57-6.19) |
0.000 0.000 |
1 2.29 (1.41-3.71) 3.04 (1.92-4.81) |
0.001 0.000 |
|
Truck traffic where your child lives on weekdays NeverSeldom Frequently Almost all day |
509 729 704 1053 |
13.75 15.08 17.61 14.24 |
1 1.11 (0.80-1.54) 1.34 (0.97-1.84) 1.04 (0.76-1.41) |
0.512 0.071 0.793 |
1 1.00 (0.69-1.45) 1.22 (0.85-1.75) 1.00 (0.71-1.42) |
0.966 0.270 0.960 |
|
Cat in the house (past 12 months) No Yes |
2830 220 |
17.18 21.36 |
1 1.58 (1.12-2.21) |
0.008 | 1 1.83 (0.65-5.12) |
0.246 |
|
Female parent level of school completion Secondary University Other Primary |
1846 449 413 241 |
12.56 22.71 17.43 18.67 |
1 2.04 (1.57-2.65) 1.46 (1.10-1.96) 1.59 (1.12-2.27) |
0.000 0.009 0.009 |
1.84 (1.36-2.49) 1.30 (0.94-1.80) 1.39 (0.90-2.16) |
0.000 0.106 0.129 |
|
How does the child get to schoolg Walk Taxi/bus Motor car Combination Other |
1633 828 518 57 23 |
13.16 15.57 21.62 12.28 4.34 |
1 1.21 (0.96-1.54) 1.81 (1.41-2.34) 0.92 (0.41-2.06) 0.29 (0.04-2.23) |
0.103 0.000 0.846 0.240 |
1 1.31 (1.00 -1.71) 1.74 (1.27-2.38) 1.07 (0.46-2.49) 0.32 (0.04-2.48) |
0.048 0.000 0.863 0.279 |
a The Totals for individual risk factors differ owing to the absence of values. b The statistically significant values for the crude OR and less than 0.05 for the adjusted OR are highlighted. c Model adjustments were made for all the variables in the table. 1: Unless declared in another manner, the referent category for individual risk factors is the lack of the risk factor.
Table 5.
Participants (combined Rural and Urban areas) prevalence of current wheeze with their respective odds ratios.
Table 5.
Participants (combined Rural and Urban areas) prevalence of current wheeze with their respective odds ratios.
| Variables | Totala | Prevalence (%) | Crude ORb | Adjusted ORb,c | ||
|---|---|---|---|---|---|---|
| (95% CI) | P | (95% CI) | P | |||
|
Female parent ever asthma No Yes |
2453 79 |
8.35 26.58 |
1 3.97 (2.36-6.67) |
0.000 | 1 5.59 (2.77-11.26) |
0.000 |
|
Child used Analgesic/antibiotic in the past 12 months Never At least once a year At least once per month |
440 906 1656 |
1.81 6.95 12.86 |
1 4.03 (1.91-8.49) 7.97 (3.90-16.27) |
0.000 0.000 |
1 3.41 (1.17-9.95) 4.74 (1.68-13.40) |
0.024 0.003 |
|
Truck traffic where your child lives on weekdays Never Seldom Frequently Almost all day |
508 727 702 1064 |
8.66 8.80 11.82 8.74 |
1 1.01 (0.68-1.52) 1.41 (0.96-2.07) 1.01 (0.69-1.47) |
0.931 0.078 0.958 |
1 1.04 (0.55-1.94) 1.13 (0.60-2.22) 0.86 (0.45-1.64) |
0.902 0.695 0.653 |
|
Female parent job industry Private sector Government sector Self-employed Not employed |
567 347 301 1721 |
8.28 12.96 9.96 9.18 |
1 1.64 (1.06-2.54) 1.22 (0.75-1.98) 1.11 (0.79-1.57) |
0.024 0.409 0.519 |
1 1.38 (0.73-2.60) 1.18 (0.73-2.32) 0.69 (0.41-1.17) |
0.317 0.629 0.177 |
|
Dog in the house (past 12 months) No Yes |
2742 320 |
8.75 14.68 |
1 1.79 (1.28-2.51) |
0.001 | 1 1.27 (0.70-2.32) |
0.419 |
|
Female parent smoke No Yes |
2884 93 |
9.01 23.65 |
1 3.12 (1.90-5.12) |
0.000 | 1 0.65 (0.20-2.15) |
0.488 |
|
People living in the same house as your child smoke? Zero One or more |
2008 823 |
7.86 13.12 |
1 1.78 (1.36-2.29) |
0.000 | 1 2.09 (1.38-3.16) |
0.000 |
|
Child exposure to smoking at the car (past 30 days) Never One or more days |
1368 69 |
9.50 11.59 |
1 2.37 (1.31-4.30) |
0.004 | 1 2.27 (1.17-4.38) |
0.014 |
|
Child ever breastfed No Yes |
959 2090 |
8.65 8.65 |
1 1.15 (0.88-1.50) |
0.293 | 1.40 (0.88-2.23) | 0.154 |
a The Totals for individual risk factors differ owing to the absence of values. b The statistically significant values for the crude OR and less than 0.05 for the adjusted OR are highlighted. c Model adjustments were made for all the variables in the table. 1: Unless declared in another manner, the referent category for individual risk factors is the lack of the risk factor.
Table 6.
Participants (combined Rural and Urban areas) prevalence of current severe wheeze with their respective odds ratios.
Table 6.
Participants (combined Rural and Urban areas) prevalence of current severe wheeze with their respective odds ratios.
| Variable | Totala | Prevalence (%) | Crude ORb | Adjusted ORb,c | ||
|---|---|---|---|---|---|---|
| (95% CI) | P | (95% CI) | P | |||
|
People living in the same house as your child smoke? Zero One or more |
2028 827 |
0.98 2.17 |
1 2.23 (1.17-4.24) |
0.014 | 1 2.46 (1.25-4.85) |
0.009 |
|
Sex of child Female Male |
1524 1592 |
0.78 1.75 |
1 2.25 (1.14-4.45) |
0.019 | 1 2.30 (1.09-4.84) |
0.027 |
|
Child plays with dogs/cats No Yes |
2535 556 |
1.18 1.61 |
1 1.27 (0.64-2.91) |
0.407 | 1 0.95 (0.41-2.22) |
0.919 |
|
Child used Analgesic/antibiotic in the past 12 months Never At least once a year At least once per month |
440 917 1666 |
0.22 1.09 1.56 |
1 4.84 (0.61-37.92) 6.95 (0.94-51-42) |
0.133 0.057 |
1 4.34 (0.54-34.68) 6.14 (0.82-45-75) |
0.166 0.077 |
|
Truck traffic where your child lives on weekdays Never Seldom Frequently Almost all day |
513 731 709 1070 |
1.36 0.82 1.12 1.68 |
1 0.59 (0.19-1.79) 0.83 (0.29-2.28) 1.23 (0.51-2.98) |
0.358 0.712 0.636 |
1 0.46 (0.14-1.48) 0.65 (0.23-1.85) 0.89 (0.35-2.23) |
0.196 0.428 0.808 |
|
Child ever breastfed No Yes |
964 2108 |
1.14 1.37 |
1 1.20 (0.60-2.42) |
0.595 | 1 1.16 (0.55-2.45) |
0.690 |
|
Female parent job industry Private sector Government sector Self-employed Not employed |
571 349 303 1736 |
0.87 2.29 1.98 1.15 |
1 2.65 (0.86-8.18) 2.28 (0.69-7.55) 1.31 (0.49-3.53) |
0.089 0.175 0.581 |
1 2.20 (0.68-7.08) 2.23 (0.66-7.47) 1.09 (0.39-3.00) |
0.185 0.192 0.859 |
a The Totals for individual risk factors differ owing to the absence of values. b The statistically significant values for the crude OR and less than 0.05 for the adjusted OR are highlighted. c Model adjustments were made for all the variables in the table. 1: Unless declared in another manner, the referent category for individual risk factors is the lack of the risk factor.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



