Submitted:
13 February 2024
Posted:
13 February 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background. Moral distress (MD) and Burnout of Health Care Personnel (HCP) were extensively studied during the pandemic. However, little information is available about their prevalence after its decline. This study assesses the prevalence of MD, and burnout after the decline of the pandemic. Methods. The British Medical Association questionnaire referring to MD and the Maslach Burnout questionnaire were addressed to the hospital’s personnel. Results. 516 valid questionnaires were included in the study. Nurses’ participation rate was 67% and doctors 41%. MD was identical among doctors and nurses 73,8%, and in decremental order factors contributing to MD are insufficient staff, mental fatigue, and physical fatigue. Participants believe that more staff, less bureaucracy, and greater emotional support would alleviate MD. Doctors score higher than nurses for lack of time to give sufficient support to patients and public health decisions affecting communities. To alleviate MD, doctors ask for more ethical and legal support, more funding and working fewer hours. Nurses score high on emotional exhaustion and depersonalization. Conclusions. MD and burnout persist among HCP after the decline of the pandemic. Participants believe that institutional and public health decisions would help alleviate MD. Leaders and institutions must provide more supportive environments to moderate MD.
Keywords:
Moral Distress
; Moral Distress Factors
; Moral Injury
; Burnout
; Post-Covid-19
1. Introduction
During the pandemic health care personnel (HCP) faced unprecedented challenges as patient demand overwhelmed the available human and material resources even in wealthy countries. The surge of patients has fundamentally changed both practice and care decisions. Public health ethics and the welfare of the community overruled the well-being of the individual patient [1]. Triage decisions and resource allocation policies, led to life-or-death decisions prioritizing which patients would get access to potentially life-saving resources [2]. Access was denied to families to see their dying relatives in violation of values around death, dying and bereavement [3]. Medical staff experienced a lack of agency/power to make correct decisions for patients, and some were allocated to care of patients outside of their specialty without adequate training or experience [4]. Fear of becoming infected themselves and transmitting the infection to family, relatives, and colleagues put enormous ethical dilemmas both on physicians and nurses [4,5].
Although burnout in HCP during Covid-19 attracted a lot of attention, moral distress (MD) underwent less scrutiny. A quick search at PubMed from 2020 to 2023, entering the words “Moral Distress”, “Covid -19” and “health-care workers” detected 181 results whereas “burnout”, “Covid -19”, and “health-care workers” yielded 1066 results (accessed 27 November 2023). Burnout arises from excessive demands on energy strength and resources in the workplace leading to malaise, fatigue, emotional exhaustion, frustration, cynicism and feeling of inefficacy [6]. There are many definitions concerning MD [7]. According to Jameton, “MD arises when one knows the right thing to do, but institutional constraints make it nearly impossible to pursue the right course of action” [8]. The American Association of Critical Care Nurses states that “MD occurs when you know the ethically appropriate action to take but are unable to act upon it. You act in a manner contrary to your personal and professional values which undermines your integrity and authenticity” [9].
Moral Distress arises where sustained moral distress leads to impaired function or long-term psychological harm. MI produces profound guilt and shame, sense of betrayal, anger and profound “moral disorientation.” Cartolovni et al. emphasized that MI results in long-term emotional damage contributing to permanent numbness, malfunctioning, and social isolation [10].
According to Dean et al. “there is a difference between burnout and MD and MI, and it is important to clarify the terminology and reframe the problem and its solutions”. The same authors suggested that “burnout is a problem that resides inside the individual who lacks the resources or resilience to withstand the work environment” [11]. MD on the other hand focuses on the challenge of knowing what care the patients need but being unable to provide it due to constraints that are beyond our control. In MD the source of distress is in the system not in the individual and solutions demand changes in the business framework of health care. MI is the result of sustained moral distress and that health-care workers have undergone during the pandemic that lasted for almost three years. Rosen et al. emphasized that MI is distinct from MD and burnout, and this remains important for distinguishing methods for intervention and repair [12]. Although MD and MI are not the only causes of burnout, MD can contribute to its core symptoms [13,14,15]. Furthermore, by reframing burnout as downstream of MD and MI, interventions that reduce both may diminish the likelihood of burnout [12,16].
We believe that it is important to investigate both MD and MI, in the post Covid-19 era because of feelings of guilt and frustration that we had not done enough due to personal, institutional, and public health decisions, that emerged during the pandemic may be accentuated in the aftermath. Greece, a country of ca. 10 million people experienced four waves of the epidemic from January 2020 to October 2023 with 5,5 million of cumulative cases and 37,500 cumulative deaths [17]. It is obvious that the health care personnel were exposed over this time to physical and ethical stressors such as overload of patient cases, lack of personnel, lack of resources and inability to provide optimum care to patients in life-threatening situations.
Our study was conducted eight months after the decline of the pandemic because we hypothesised that MD may persist after the stressful situation has receded and individuals have time for reflection and rethinking of what really happened. The primary outcome of our study is to assess the prevalence and the contributing factors to MD of HCP after the decline of the pandemic. The secondary outcomes are 1. To identify the differences between groups of participants in the prevalence and the contributing factors of MD 2. To assess burnout and the relationship between MD and burnout.
2. Methods
2.1. Design
This is a cross-sectional study conducted during the period between the end of August to the end September 2023, eight months after the waning of latest wave of pandemic.
2.2. Setting
The study was conducted at Papageorgiou General Hospital, an 800 beds hospital, one of the largest in northern Greece. During the successive waves of the pandemic HCP faced overwhelming patients’ admissions and profound changes were implemented in the management structures, and the allocation of medical and nursing personnel. During the pandemic the hospital personnel comprised of 600 nurses, 60 midwives, 294 specialty physicians and 250 interns and fellows. The ICU beds increased from 16 to 48 plus 8 beds in the Respirology department were equipped to function as an Intermediate Care Unit. The nurse-to-patient ratio in the ICU was 1:3, in the intermediate care 1:4 and in the Covid-19 wards 1:9. Non-emergency operations were cancelled, and half of the operating rooms were available for Covid-19 patients in the case of lack of ICU beds.
2.3. Instrument and Participants
From August to the end of September 2023, eight months after the waning of the pandemic, two anonymous electronic questionnaires referring to MD, MI and burnout were distributed by email to the hospital nursing and medical personnel. A link from the Business Administration Department - Human resources Management Lab of the University of Macedonia in Thessaloniki was provided to the participants to have access and respond to the questionnaires on-line. Two reminder invitations by email were sent one week apart. Anonymity was especially emphasized, and no incentive was offered for participation in the survey. The questionnaires were accompanied by an explicative letter for the purpose of the study and the definitions of moral distress and moral injury. The definitions provided were these used by the British Medical association (BMA) MD survey breakdown [18]. Additionally, a burnout questionnaire was addressed only to the nursing personnel. The burnout questionnaire was distributed only to the nursing personnel because of the availability of data from a previous study on burnout amongst nurses during the pandemic for comparison [19].
2.4. Measures
To assess MD and MI we used the BMA Moral Distress Survey Breakdown that had previously been used to get insight into the general awareness and prevalence of MD and MI among UK doctors [18]. Quoting from this survey, “the BMA questionnaire explores not only the prevalence and the general awareness of MD and MI, but also gathers understanding of what their biggest contributors are, and if there are any clear ways to alleviate them”. The questionnaire asks participants to select from a list of factors those that in their opinion are the five most important contributors to moral distress. We adapted the original questionnaire by omitting questions irrelevant to Greece and this particular hospital such as ethnicity, private practice, retirement etc. The questionnaire was translated by two Greek senior physicians who had worked in the NHS for many years and were equally proficient in both languages. The questionnaire was translated from English to Greek and from Greek to English according to the Brislin model for instrument translation, which is a well-known method for cross-cultural research [20]. The back translation was done by blinding the two second translators (equally ex-NHS physicians) to the original document. Both versions (the original and the back translated document) were compared for accuracy by the research team members and the first two senior physicians. To avoid ambiguity some terms were written in English alongside their Greek translation because all the questionnaire participants had English language qualifications. The final form of the Greek version maintained the structure of the original questionnaire.
We used the Maslach Burnout General Survey (MBI-GS) questionnaire to measure Burnout. [21]. This is a sixteen-item scale, rated on Likert scale from 0 to 6 (0 =never to 6=daily) and contains three subscales: Exhaustion, Cynicism, and Professional efficacy. Scores above 3.2 for emotional exhaustion and 2.4 for cynicism, are considered high. Cynicism and feelings of inefficacy stem from sustained emotional exhaustion, resulting in poor mental and physical health [22,23]. Schaufeli and Bakker proposed that personal efficacy should be seen as a dimension of work engagement rather than burnout, whereas Emotional Exhaustion itself lies at the core of burnout. [24].
2.5. Ethical considerations
The study protocol and the research questionnaires were reviewed and approved by the hospital ethics committee. (Study approval no 24571/31-08-2023). Participation in the study was not compulsory. Anonymity and confidentiality were particularly emphasized to all participants.
2.6. Data analysis
For descriptive statistics we used the statistical software SPSS version 22 (SPSS Inc. IBM Corp., Chicago, Illinois, USA). Normality of values distribution was assessed with the Kolmogorov-Smirnov test. Recorded data are presented as percentage frequency distribution. Our hypothesis that moral distress and injury differs between physicians and nurses and providing care to Covid and non-Covid patients was tested with statistical analysis of comparison of two independent groups. Group comparisons were performed with Chi-square test and p-values lower than 0.05 were considered statistically significant. Sample size was calculated in advance with G. Power 3.1 statistical program. It was therefore determined at 350 participants for an error probability test of 0.05, statistical power of 0.8 and effect size of 0.15 (low).
3. Results
3.1. Demographic data
535 nurses and 382 doctors were invited to participate in the study (917 questionnaires altogether were invoiced). Completed questionnaires missing more than 5 item responses were discarded from the analysis. Finally, 516 valid questionnaires were included in the study (359 from nurses and 157 from doctors). Overall participation rate was 56% (nurses 67%, and doctors’ 41%).
3.2. Results of the entire sample of participants
Table 1 presents the participants gender, age, involvement with Covid-19 patients, the working environment, and their experience in relation to MD and MI. Participants less than 45 years old experienced higher levels of MD compared to participants older than 45 (78,5% vs 69,6% p< 0,05), both groups sharing the same levels of MD 12 months before the pandemic (35,4% vs 36,6% respectively). Additionally, 72,5% stated that during the pandemic the risk of MD had changed. Figure 1 exhibits the factors the hospital HCP identified as top contributors to MD and Figure 2 depicts what the participants believe could help alleviate MD in the workplace.
3.3. Opinion Differences on Moral Distress between Doctors and Nurses
Table 2 demonstrates the differences and their significance between doctors and nurses concerning the factors they believe contribute to MD and Table 3 the differences of what doctors and nurses believe could help alleviate MD in the workplace.
Doctors and nurses share similar ratings concerning 1. The experience of MD during the pandemic (73,9% vs 73,8%), 2. The MI (58% vs 64,9%) and 3. The MD in relation to a colleague’s ability to provide care (81,5% vs 79,7%). Moreover, no differences were found between junior and senior doctors concerning their experience of MD, MI and in relation to a colleague’s ability to provide care (78% vs 79,6%, 59,3% vs 58,2% and 79,7% vs 82,7% respectively).
3.4. Differences in MD between participants providing care to Covid patients and participants involved exclusively with non-Covid patients
Significant differences were found between MD and MI among participants working exclusively with Covid patients and non-Covid patients. 81,2% vs 63,4% (p<0,001) experienced MD, 71.8% vs 48,8% (p<0,01) felt MI, and 82% vs 70,7% (p<0,05) experienced MD in relation to a colleague’s ability to provide care. Interestingly participants working in the ICU with Covid patients, when compared to participants working in rotation (50% of their working time during the pandemic) with Covid patients and non-Covid care providers experienced higher levels of MD (92,4% vs 78,9% vs 63,4% respectively, p<0,001) and MI (74,7 vs 63,7 vs 48,8% respectively, p<0,01), Figure 3.
3.5. Nurses Burnout results
On the emotional scale 64,6% of the nursing personnel rated high (above 3,2) 21,5% rated moderate and 13,8% rated low with an average rating of 3,8 and a median of 4,2. On the cynicism scale 46,4% rated high (above2,4), 31,8% rated moderate and 21,8% rated low with an average rating of 2,4 and a median of 2,2.
4. Discussion
Moral distress during Covid-19 attracted less attention compared to burnout. A quick search at PubMed from 2020 to 2023, using the search terms “Moral Distress”, “Covid -19” and “health-care workers” detected 181 results whereas “burnout”, “Covid -19”, and “health-care workers” yielded 1066 results (accessed 27 November 2023). Our study was conducted eight months after the decline of the pandemic and our findings explore the prevalence of burnout and MD, the contributing and the factors that would alleviate MD. Our HCP had been continuously exposed to physical and moral stressors for almost a three-year period. We consider that it is crucial to assess the post pandemic era because there is evidence that moral injury persists or may even increase when compared to the prevalence during the pandemic.
Primo Levy in his book “The Drowned and the Saved” [25] in the chapter “Shame” describes that most of the Nazi concentration camps inmates surprisingly committed suicide after their liberation due to the “awareness emerged that they had not done anything, or not enough against the system into which they had been absorbed and they have failed in terms of human solidarity”, thus suffering from MI. In support to Primo Levy statement on the late effects of MI, six months after the decline of the pandemic our hospital personnel underwent a profound shock after the self-immolation of the ICU director evidently suffering from profound MI (see acknowledgments).
4.1. Moral Distress
It is difficult to determine with certitude the level of MD and MI during the pandemic on the health care workers population. In essence MD refers to a situational problem due to the circumstances an individual finds themselves in, while MI represents an experience of the problem which can cause serious harm to an individual [10,26]. In the many studies that explored MD during the pandemic several different questionnaires were used with different ratings and questions addressed in a variety of samples of health care populations and settings and with different proportions of working time with infected people [27]. Many studies focus on the distress induced by, the lack of personal protective equipment, the fear of getting infected, fear of contaminating others including family members or social isolation [5,15,28]. Hines at al. found that in the first wave of the pandemic in early 2020, three months after its peak and contrary to their hypothesis that MD and MI would increase, MD actually decreased whereas MI remained stable demonstrating a permanent effect of the sustained MD [29]. Alimoradi et al. in a systematic review and meta-analysis conducted between October 2021 and February 2022 surprisingly found that MD decreased during the pandemic when compared to the pre-pandemic period [27]. However, the study population was exclusively nurses, and among the 86 papers included in the study only 9 studies had been conducted after the onset of Covid-19 and 15 in the early part of the pandemic. Andersson et al. [30] suggested that contrary to studies early in the pandemic [31,32] the factors contributing to MD shifted from systemic issues such as poor teamwork to patient associated factors such as inability to offer person-centered care. Our study highlights that both systemic and patient factors contribute to MD. As we can see in Figure 1 the first two factors of MD refers to the system (increased mental fatigue due to understaffing within the system) and the following two refer to patients cares (inability to provide timely treatment and lack of time to give sufficient emotional support to patients). Lake et al. early in the pandemic reported that the largest effect on MD was associated with the volume of care for infected patients [5]. Our data confirm this finding. High levels of MD were recorded (92,4%) in participants working in the ICU thus exclusively with Covid-19 patients, compared to participants working in rotation with Covid patients (78,9%) and to participants working with non-Covid patients (63,4%), Figure 3.
On June 2021, the BMA conducted a survey on the prevalence of MD and MI in UK doctors and their contributing factors [18]. We used the same questionnaire for our hospital doctors and nursing population eight months after the decline of the pandemic to detect if there were changes in the prevalence of MD and MI, the contributing factors of MD, the differences between doctors and nurses and the differences between the personnel heavily involved with Covid-19 and non-Covid 19 patients. Some differences and many similarities can be noted between the BMA and our study. The same proportion of participants were involved with the treatment of COVID and non-Covid patients (64,7 vs 68,7% respectively), however; only 3,7% were involved exclusively with Covid patients compared to 15,3% in our study. In both studies the same proportion (78,4 % vs 78,5% respectively) report that they experienced MD at work but there is a difference concerning the experience of MD before the Covid-19 pandemic (59,6% in the BMA study vs 35,9% in our study). Both studies report that the risk of MD has changed during the pandemic (82,7% vs 72,5%), moreover; they share, in decremental order, the same opinion that insufficient staff to properly treat all patients, mental fatigue, lack of time to give sufficient emotional support to patients, and inability to provide timely treatment are the most important factors contributing to MD.
Concerning the factors that would help alleviate the risks of MD, both studies emphasize that above all, adequate staff and streamlined bureaucracy are of primary concern. An interesting difference between the two studies is the demand for more training. 39,5% of our participants believe that more training would alleviate MD compared to 6,3% in the BMA study. Norman et al. found, in a large sample of health care workers with 76,8% of them directly treating Covid patients, a strong association between MD and the worry about not having enough competencies to provide adequate care [28]. Moreover, our participants asked for more emotional and psychological support and more access to ethical and legal support when faced with challenging decisions Figure 2.
4.2. Moral Injury
MI is a stressor-linked problem. The definition of MI concept is problematic because there are currently widely varying uses of the term without concensus about what MI is, and is not, in addition to imprecise terminology used in published empirical studies as well as the lack of a gold standard of measurement [26]. People who are exposed to morally stressful situations do not fully recover from the distress they experience. Epstein and Hamric suggested the term moral residue for this phenomenon [33]. When MD persists and develops into moral residue then the MI syndrome is manifested with important emotional, biological, psychological, behavioral, and spiritual dimensions [26,34,35]. In addition to Litz’s [26] perspective on MI which focuses on the individual, Shay highlights the social environmental component by defining MI as a betrayal by authority figures in high-stakes situations [36]. This perspective focuses on the feeling of being let down by a legitimate social authority in the sociocultural context. This perception of betrayal can occur due to organizational and leadership malpractice receiving immoral orders or witnessing transgressive decisions. These two aspects, individual and environmental of MI are demonstrated by our study even at eight months after the decline of the pandemic. 63 % of the participants experienced MI during the pandemic and among the distressing factors leading to MI they emphasize both organizational and personal level factors (Figure 1). Moreover, when we focus on the factors that would help alleviate the risks of MD, participants primarily refer to the organizational level, (Figure 2). Shale early in the pandemic emphasized that MI should be acknowledged by leaders and appropriate actions taken [35]. She proposes seven central actions, among them acknowledging the injury, acknowledging the responsibility, and acknowledging that remedy is due.
4.3. Differences between doctors and nurses
In the early phase of the pandemic, it has been reported that doctors experienced higher levels of MD compared to the nurses [4]. This difference was explained by the inclusion of a cohort of doctors who had to perform tasks outside their usual range clinical duties (e.g., dermatologists and pediatricians redeployed to treat Covid-19 infected patients). In the ICU setting no difference was found in MD levels between intensivists, nurses, and supporting staff [37]. Our study did not show differences in MD and MI between doctors and nurses however, significant differences were detected concerning the factors that contribute and would alleviate MD and MI. Specifically, doctors felt distressed about their inability to provide timely treatment, the public health decisions affecting communities, the lack of beds and deprioritizing certain patients. On the contrary, nurses were more distressed compared to doctors, by the lack of time to give emotional support to patients (Table 2). Concerning the factors that would help alleviate the risks of MD, doctors and nurses completely agree that more staff are necessary, however, 55,4% of the doctors asked for more access to ethical and legal support when faced with challenging decisions compared to 27,9% of the nurses. It has been reported that exposure to verbal or physical medical violence from patients or relatives represents a risk factor for developing MI [37]. In fact, during the pandemic doctors faced difficult triage and priority dilemmas due to shortages of human and material resources and were exposed to aggressive patients and relatives denying treatments and invasive procedures and threatening of lawsuits in cases with unfavourable outcomes. Additionally, doctors believe that MD could be alleviated by more funding, reduced working hours, access to multidisciplinary teams and more time for reflection. On the contrary nurses prioritize emotional and psychological support (Table 3). Interestingly, both doctors and nurses believe that MD is promoted by insufficient training to provide necessary treatment and support (35,7% and 30,6% respectively, Table 2) and that more training would alleviate the risk of MD (38,9% and 39,8% respectively, Table 3). Our data are supported by the Maffoni’s results that showed that appropriate training decreased the levels of MD [4].
4.4. Moral distress and Burnout
There is a substantial variability in estimates of prevalence of burnout among doctors. In a systematic review of 182 studies involving 109628 individuals in 45 countries, 85,7% of them using a version of the Maslach Burnout Inventory, Rotenstein et al. found an overall burnout prevalence ranging from 0% to 80,5% [39]. The prevalence on the burnout subscales, emotional exhaustion, depersonalization, and personal accomplishment ranged from 0% to 86,3%, 0% to 89,9% and 0% to 87,1% respectively. Dzeng stated that burnout amongst doctors is approximately 50% due to the fact they feel unable to exercise ethical agency that is so central to their professional identity as ethical care providers [40]. This phenomenon is described by Dean et al. as MI. He emphasizes that doctors suffer from MI and not burnout because they know what care patients need but they are unable to provide it due to constraints that are beyond their control [11]. Rosen during the Covid-19 era agrees with Dean’s opinion that doctors are suffering from MI and not burnout because if they were burned out, they would no longer be distressed at the violation of their deeply held moral beliefs. An individual suffering from detachment and depersonalization associated with burnout is beyond feeling [12]. However, she recognizes that burnout is downstream of MD and MI since sustained MD is a cause of MI and MI if unchecked leads to burnout.
On the contrary, to the doctor’s controversy on burnout, studies on nurse’s burnout are more straightforward and evidence of the relationship with MD during the pandemic is abundant. Our study provides data on our hospital nurses eight months after the decline of the pandemic. We conducted a study during the pandemic, March-July 2021, and it is interesting to compare the levels of burnout during and after the pandemic in the same population [19]. During the pandemic the hospital nurses rated the two burnout main core subscales, emotional exhaustion, and depersonalization-cynicism at the top of moderate: 3,1 (high >3,2) and 2,3 (High >2,4) respectively. In the present study the same participants rated high for emotional exhaustion and on depersonalization, 3,8 and 2,5 respectively. Interestingly 64,6% of the nurses rated high on emotional exhaustion and 73,8% of them declare experiencing MI at work. If we embrace the idea of Rosen that burnout is downstream of MI [12], we can assume that the emotional exhaustion of the hospital nurses is the consequence of a repetitive MD leading to MI and thus burnout. Our data are supported by the findings of longitudinal study demonstrating that burnout, both amplifies MD and is increased by MD [15].
5. Limitations
There are some limitations of our study. First, it is a single hospital survey and not a national survey. Nevertheless, some of our results are very close to the findings of the BMA national survey in the UK medical workforce, indicating that the repercussions of the pandemic on MD are similar across different hospitals and countries.
Second, this is not a longitudinal study because we lack data on MD measured during the pandemic. An attempt to assess MD in the middle of the pandemic had failed due to a very low response rate, suggesting that HCP was too busy and too stressed to complete questionnaires at the time. Moreover, we believe that assessment of Moral Injury and Moral Distress is more accurate when done in retrospect, when an amount of time has passed, facilitating reflection on the events from a safe distance [25]. In favor of this explanation is that in the present post-pandemic study, HCP believes that reduced working hours may alleviate the risks of MD.
Moreover, doctor’s burnout was not assessed in this survey. However, there is evidence in the literature that physicians often confuse the terms “burnout” and “MI”. When they are referring to suffering from burnout, in reality they tend to describe moral injury [11].
Third, the doctors’ participation rate was only 41%. This suggests a possible response bias though ignoring 59% of the medical workforce. Responders of our study perhaps are over reporting their MD factors expressing their disappointment to the institutions regarding inadequate ethical and legal support, too much bureaucracy, and limited access to funding. However, this bias is questionable because nurses with a much higher participation rate score quite the same percentage on the three major causes of MD, more staff, mental fatigue, and physical fatigue.
Finally, the questionnaire items did not cover all the aspects of MD experienced by the participants. However, a more detailed questionnaire would risk an even lower response rate from a mentally and physically tired medical workforce.
6. Conclusions
Our study demonstrates that the terms Moral Distress and Moral Injury were new to our study participants, confirming similar findings from the BMA survey. Although MD had been present among our staff before, it greatly increased during the pandemic, and doctors and nurses, eight months later, still have not recovered from the distress they experienced. MD and MI, persist and burnout even increased. Respondents believe that mainly institutional and public health decisions would help alleviate MD, like more staff, more ethical and legal support, less bureaucracy, and more training. The risk of MD cannot completely be removed from the medical and nursing workplace; however, leaders and institutions must provide more supportive environments to moderate its effects.
Author Contributions
Conceptualization, D.M. M.P, I.S.; Methodology, M.P, I.S, Ch. N; Software, D.M; Validation, M.P, I.S, Th. B.; Formal Analysis, Ch. N, Th. B, D.M.; Investigation, M.P, I.S Resources, M.P, I.S.; Data Curation, Ch. N, Th. B, M.P; Writing – Original Draft Preparation, M.P, Th. B, Ch. N .; Writing – Review & Editing, M.P, D.M ; Visualization, M.P, Ch. N.; Supervision, D.M.; Project Administration, M.P.; Funding Acquisition. M.P, I.S. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research authorship. Funding for the publication costs of this article will be provided by the Papageorgiou Foundation.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Papageorgiou Hospital Ethics Committee, Study approval no 24571/31-08-2023.
Informed Consent Statement
Participants consent was waived since this study is an anonymous, non-compulsory Survey.
Data Availability Statement
The data of our study are available from the corresponding author on reasonable request.
Acknowledgments
The authors would like to thank all hospital medical and nursing personnel for participating. Moreover, the authors acknowledge Priede Monty, Professor Emeritus of the University of Aberdeen, and Dimitrios Matamis for their precious editorial assistance and questionnaires translation.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Williams, D. R, Brundage, A. J, Williams, B. E. (2020). Moral Injury in Times of COVID-19. Journal of health service psychology, 46(2): 65–69. [CrossRef]
- Truog, D. R. , Mitchell, C., Daley, Q. G. (2020). The Toughest Triage - Allocating Ventilators in a Pandemic. New England Journal of Medicine, 21; 382(21):1973-1975. [CrossRef]
- Vittone, S., Sotomayor, R. C. (2021). Moral Distress Entangled: Patients and Providers in the COVID-19 Era. HEC forum : an interdisciplinary journal on hospitals’ ethical and legal issues, 33(4):415-423. [CrossRef]
- Maffoni, M., Fiabane, E., Setti, I., Martelli, S., Pistarini, C., Sommovigo, V. (2022). Moral Distress among Frontline Physicians and Nurses in the Early Phase of COVID-19 Pandemic in Italy. International Journal of Environmental Research and Public Health, 19 (15): 9682. [CrossRef]
- Lake, E.T., Narva, A.M., Holland, S., Smith, J.G., Cramer, E., Rosenbaum, K.E.F. (2022). Hospital nurses’ moral distress and mental health during COVID-19. Journal of Advanced Nursing, 78(3):799–809. [CrossRef]
- Freudenberger, H. J. (1975). The staff burn-out syndrome in alternative institutions. Psychotherapy: Theory, Research & Practice, 12(1), 73-82. [CrossRef]
- Morley, G., Ives, J., Bradbury-Jones, C., Irvine, F. (2019). What is ‘moral distress’? A narrative synthesis of the literature. Nursing Ethics, 26(3):646-662. [CrossRef]
- Jameton, A. (1984). Nursing Practice: The Ethical Issues. 1st Edition. Englewood Cliffs, NJ: Prentice-Hall. 331 p.
- American Association of Critical-Care Nurses A. AACN Public Policy Position Statement: Moral Distress. Aliso Viejo, CA: American Association of Critical-Care Nurses (AACN) 2006.
- Cartolovni, A., Stolt, M., Scott, P. A., Suhonen, R. (2021). Moral injury in healthcare professionals: A scoping review and discussion. Nursing Ethics, Vol. 28(5) 590-602. [CrossRef]
- Dean, W., Talbot, S., Dean, A. (2019). Reframing Clinician Distress: Moral Injury Not Burnout. Federal Practitioner, 36(9): 400–402.
- Rosen, A., Cahill, M. J., Dugdale, S. L. (2022). Moral Injury in Health Care: Identification and Repair in the COVID-19 Era. Journal of general internal medicine, 37(14): 3739–3743. [CrossRef]
- Guttormson, L.J., Calkins, K., McAndrew, N., Fitzgerald, J., Losurdo, H., Loonsfoot, D. (2022). Critical Care Nurse Burnout, Moral Distress, and Mental Health During the COVID-19 Pandemic: A United States Survey. Heart Lung. 55: 127–133. [CrossRef]
- Fumis, R. L. R., Amarante, G. A . J., Nascimento, A. F., Vieira, J. J. M. (2017). Moral distress and its contribution to the development of burnout syndrome among critical care providers. Annals of Intensive Care, 7: 71. [CrossRef]
- Maunder, G. R., Heeney, D. N., Greenberg, A. R., Jeffs, P. L., Wiesenfeld, A. L., Johnstone, J., Hunter, J. J. (2023). The relationship between moral distress, burnout, and considering leaving a hospital job during the COVID-19 pandemic: a longitudinal survey. BMC Nursing, 26;22(1):243. [CrossRef]
- Hossain, F., Clatty, A. (2021). Self-care strategies in response to nurses’ moral injury during COVID-19 pandemic. Nursing Ethics, 28(1):23-32. [CrossRef]
- https://covid19.who.int/region/euro/country/gr.
- https://www.bma.org.uk/media/4209/bma-moral-distress-injury-survey-report-june-2021.pdf.
- Papatheodorou, M., Kloutsiniotis, P., Michail, D. (2023) The Influence of Leadership on Structural Empowerment and Work-Life Balance on Nurses’ Burnout and Patients’ Assessed Quality of Care During the Covid-19 Pandemic. Medical Research Archives, 11: 7.1. [CrossRef]
- Brislin, W. R. Back-Translation for Cross-Cultural Research. Journal of Cross -Cultural Psychology, Volume 1, Issue 3. [CrossRef]
- Mashlach, C, Jackson, S.E., Leiter, M. (1986). Mashlach Burnout Inventory Manual. Third Edition Mind Garden publisher.
- Melamed, S., Shriom, A. (2005) Does burnout affect physical health? A review of the evidence. Research Companion to Organizational Health Psychology, 599-622. [CrossRef]
- Maslach, C., Leiter, M. (2004). Areas of work life: a structured approach to organizational predictors of job burnout. Research in Occupational Stress and Well-Being, 3:91–134. [CrossRef]
- Schaufeli, W.B., Bakker, A.B. (2004). Job demands, job resources, and their relationship with burnout and engagement: a multi-sample study. Journal of Organizational Behavior, 25: 293-315. [CrossRef]
- Primo Levy. The drowned and the saved. Page 70-81. 1989 Edition. Vintage books, New York.
- Litz, T. B., Kerig, K. P. (2019). Introduction to the Special Issue on Moral Injury: Conceptual Challenges, Methodological Issues, and Clinical Applications. Journal of Traumatic Stress, 32(3):341-349. [CrossRef]
- Alimoradi, Z. , Jafari, E., Pakpour, H. A. (2023). Estimation of moral distress among nurses: A systematic review and meta-analysis. Nursing Ethics, Volume 30, Issue 3. [CrossRef]
- Norman, B. S., Feingold H J, Kauderer H K, Kaplan A C, Hurtado A, Kachadourian L, Feder, A., Murrough, W. J., Charney, D., Southwick, M. S., Ripp, J., Peccoralo, L., Pietrzak, H. R. (2021). Moral distress in frontline healthcare workers in the initial epicenter of the COVID-19 pandemic in the United States: Relationship to PTSD symptoms, burnout, and psychosocial functioning. Depression & Anxiety Journal, 38(10):1007-1017. [CrossRef]
- Hines, E.S., Chin, H. K, Glick, R. D, Wickwire, M. E. (2021). Trends in Moral Injury, Distress, and Resilience Factors among Healthcare Workers at the Beginning of the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 18 (2), 488. [CrossRef]
- Andersson, M., Fredholm, A., Nordin, A., Engström, Å. (2023). Moral Distress, Health and Intention to Leave: Critical Care Nurses’ Perceptions During COVID-19 Pandemic. SAGE Open Nursing, 9: 1–10. [CrossRef]
- Petrișor, C., Breazu, C., Doroftei, M., Mărieș, I., Popescu, C. (2021). Association of Moral Distress with Anxiety, Depression, and an Intention to Leave among Nurses Working in Intensive Care Units during the COVID-19 Pandemic.Healthcare, 9(10),1377. [CrossRef]
- Rodriguez-Ruiz, E. , Campelo-Izquierdo, M. , Veiras, P.B. , Rodríguez, M.M., Estany-Gestal A. , Hortas A.B., Rodríguez-Calvo M.S., Rodríguez-Núñez A. (2022). Moral distress among healthcare professionals working in intensive care units in Spain. Medicina Intensiva, Volume 46, Issue 7, 383-391. [CrossRef]
- Epstein, E. G., Hamric, A B. (2009). Moral Distress, Moral Residue, and the Crescendo Effect . The Journal of Clinical Ethics, Volume 20, Nο 4:330-42. [CrossRef]
- Riedel, P.L., Kreh, A., Kulcar, V., Lieber, A., Juen B. (2022). A Scoping Review of Moral Stressors, Moral Distress and Moral Injury in Healthcare Workers during COVID-19. International Journal of Environmental Research and Public Health 1; 19 (3):1666. [CrossRef]
- Shale, S. (2020). Moral injury and the COVID-19 pandemic: reframing what it is, who it affects and how care leaders can manage it. British Medical Journal Leaders, vol. 4, no. 4, https://bmjleader.bmj.com/content/4/4/224. [CrossRef]
- Shay, P.D., (2014). More Than Just Hospitals: An Examination of Cluster Components and Configurations. Virginia Commonwealth University Pro Quest Dissertations Publishing, 3619675. [CrossRef]
- Donkers, A. M., Gilissen, J. H. S. V., Candel. J. J. M. M., van Dijk, M.N., Kling, H., Heijnen-Panis, R., Pragt, E., van der Horst, I., Pronk, A.S., van Mook, N. K. A. W. (2021). Moral distress and ethical climate in intensive care medicine during COVID-19: a nationwide study. BMC Medical Ethics, 17;22(1):73. [CrossRef]
- Wilson, A. C., Metwally, H., Heavner, S., Kennedy, A. B., Britt, W. T. (2022). Chronicling moral distress among healthcare providers during the COVID-19 pandemic: A longitudinal analysis of mental health strain, burnout, and maladaptive coping behaviours. International journal of mental health nursing, 31(1):111-12. [CrossRef]
- Rotenstein, S. L., Torre, M., Ramos, A. M., Rosales, C. R., Guille, C ., Sen, S. , Mata, A. D. (2018). Prevalence of Burnout Among Physicians: A Systematic Review. JAMA, 18; 320 (11):1131-1150. [CrossRef]
- Dzeng, E., Wachter, R. M. (2020). Ethics in Conflict: Moral Distress as a Root Cause of Burnout. Journal of general internal medicine, 35 (2):409-411. [CrossRef]
Figure 1.
Participants’ answers concerning the factors contributing to moral distress, in decremental order.
Figure 1.
Participants’ answers concerning the factors contributing to moral distress, in decremental order.
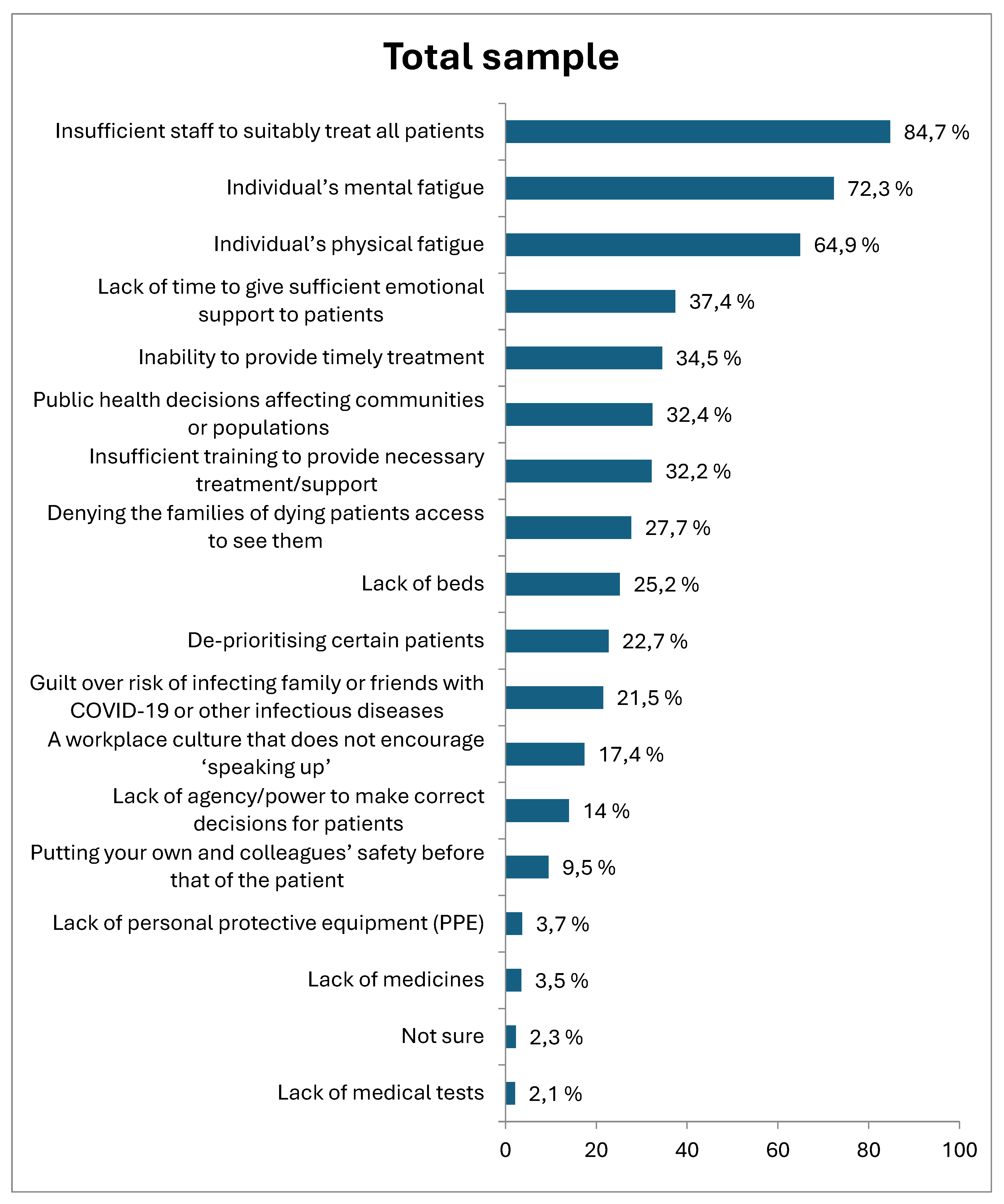
Figure 2.
Participants’ answers concerning the factors they believe would help alleviate the risks of moral distress, in decremental order.
Figure 2.
Participants’ answers concerning the factors they believe would help alleviate the risks of moral distress, in decremental order.
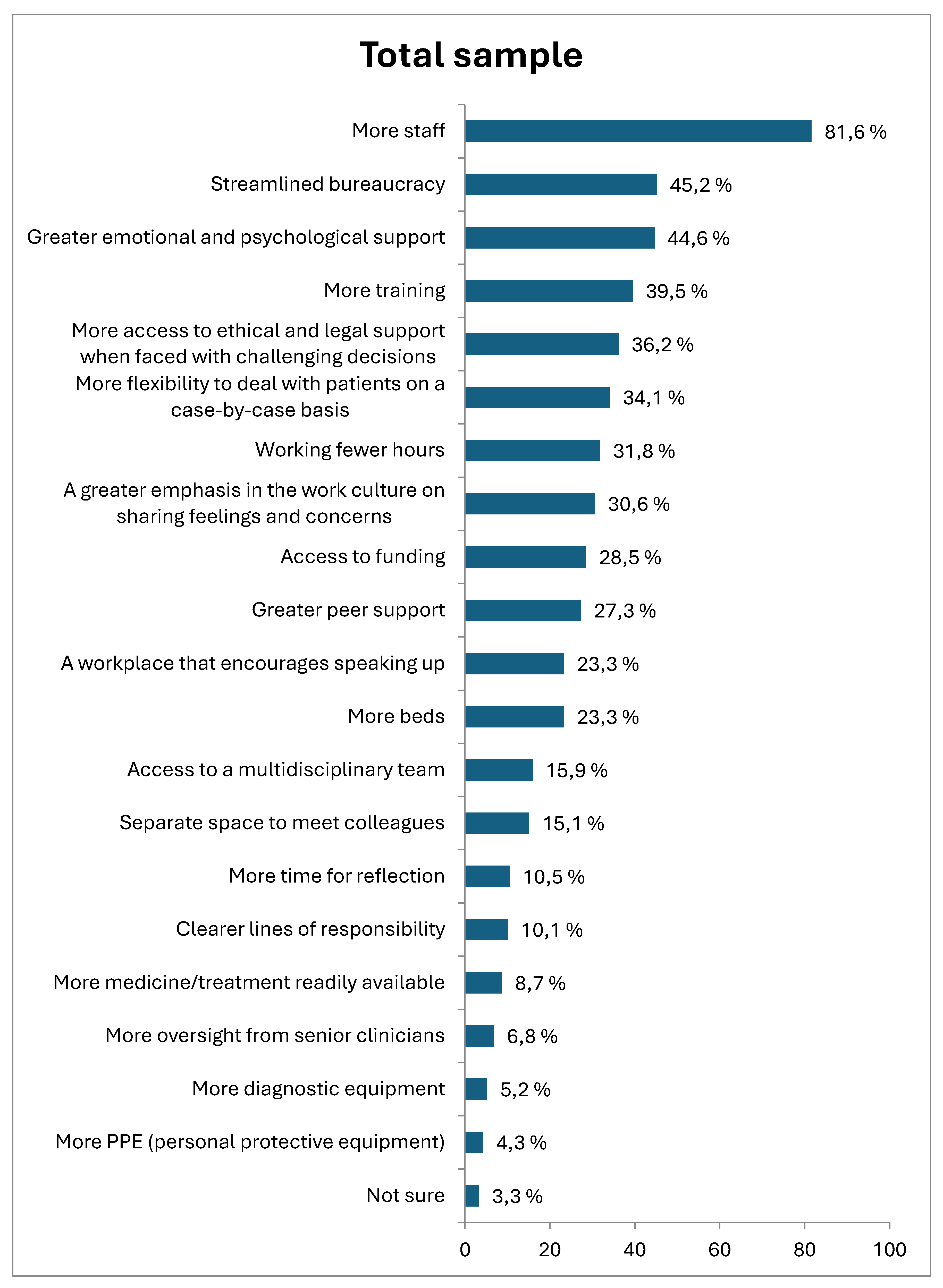
Figure 3.
Differences of moral distress and moral injury between participants working in the ICU, working in rotation with Covid patients and working with non-Covid patients.
Figure 3.
Differences of moral distress and moral injury between participants working in the ICU, working in rotation with Covid patients and working with non-Covid patients.
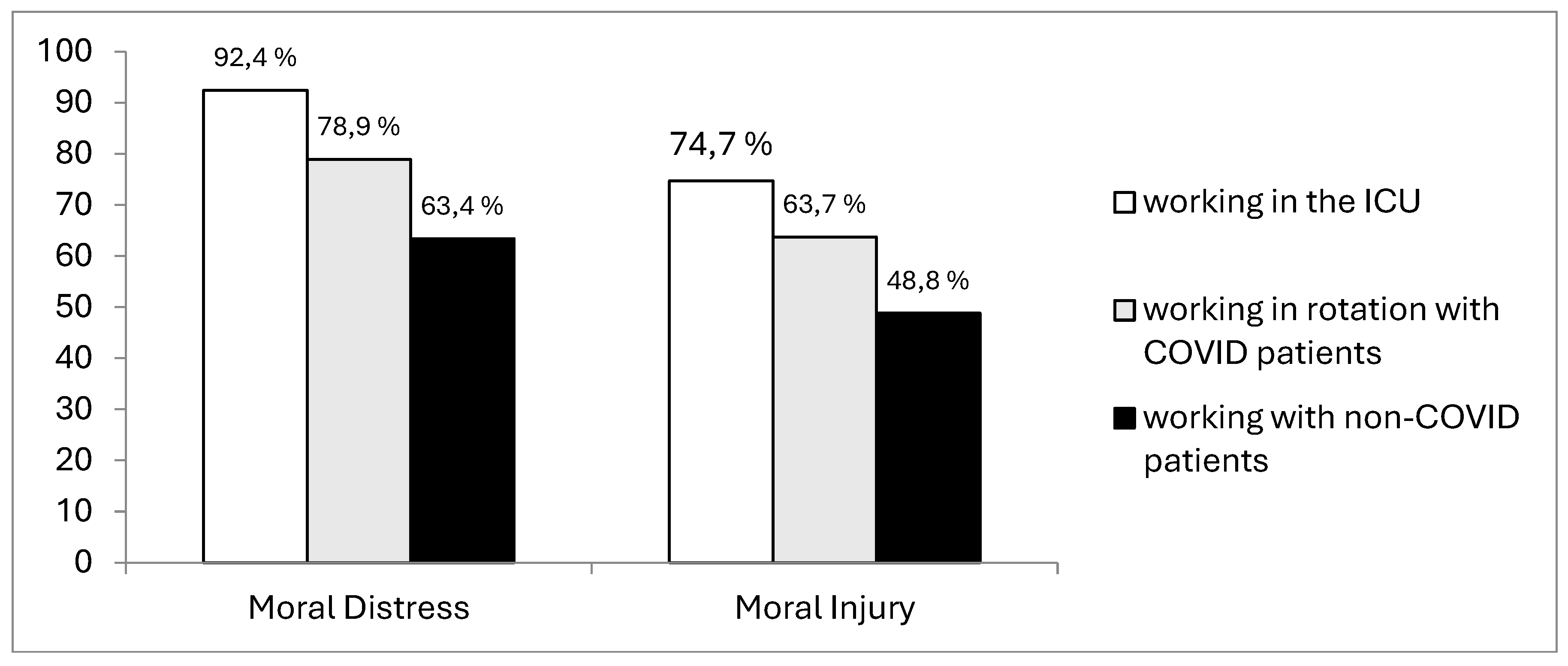

Table 1.
Participants’ characteristics and their experience in relation to moral distress and moral injury.
Table 1.
Participants’ characteristics and their experience in relation to moral distress and moral injury.
| Total n (%) | Doctors n (%) | Nurses n (%) | |
| Branch of practice | 516 (100%) | 157 (30,4 %) | 359 (69,6 %) |
| Gender | |||
| Male | 131 (25,4%) | 77 (49%) | 54 (15%) |
| Female | 385 (74,6%) | 80 (51%) | 305 (85%) |
| Age (years) | |||
| 25-34 | 95 (18,4%) | 50 (31,8%) | 45 (12,5%) |
| 35-44 | 151 (29,3%) | 29 (18,5%) | 122 (34%) |
| 45-54 | 192 (37,2%) | 41 (26,1%) | 151 (42,1%) |
| >55 | 78 (15,1%) | 37 (23,6%) | 41 (11,4%) |
| Group of patients | |||
| COVID patients | 85 (16,5%) | 16 (10,2%) | 69 (19,2%) |
| Non-COVID patients | 82 (15,9%) | 21 (13,4%) | 61 (17%) |
| In rotation | 349 (67,6%) | 120 (76,4%) | 229 (63,8%) |
| Working environment | |||
| Inside the ICU | 43 (8,3%) | 11 (7%) | 32 (9%) |
| Outside the ICU | 437 (84,7%) | 131 (83,4%) | 306 (85,2%) |
| In rotation (50% of working time) | 36 (7 %) | 15 (9,6%) | 21 (5,8%) |
| Have you heard of the terms “moral distress” and “moral injury” before? | |||
| Yes | 160 (31%) | 49 (31,2%) | 111 (30,9%) |
| No | 356 (69%) | 108 (68,8%) | 248 (69,1%) |
| During the pandemic, have you experienced moral distress in relation to your ability to provide care? | |||
| Yes | 381 (73,8%) | 116 (73,9%) | 265 (73,8%) |
| No | 135 (26,2%) | 41 (26,1%) | 94 (26,2%) |
| During the pandemic, have you experienced moral distress in relation to a colleague’s ability to provide care? | |||
| Yes | 414 (80,2%) | 128 (81,5%) | 286 (79,7%) |
| No | 102 (19,8%) | 29 (18,5%) | 73 (20,3%) |
| Thinking specifically about the 12 months before the COVID-19 pandemic, did you have experience of moral distress at work? | |||
| Yes | 185 (35,9%) | 58 (36,9%) | 127 (35,4%) |
| No | 147 (28,5%) | 43 (27,4%) | 104 (29%) |
| Not sure | 108 (20,9%) | 29 (18,5%) | 79 (22%) |
Table 2.
Differences in decremental order between doctors and nurses concerning the factors they believe contribute to moral distress.
Table 2.
Differences in decremental order between doctors and nurses concerning the factors they believe contribute to moral distress.
| Factors that contribute to moral distress | Doctors (%) | Nurses (%) | p value |
|---|---|---|---|
| Insufficient staff to suitably treat all patients | 82,8 | 84,7 | 0,685 |
| Individual’s mental fatigue | 73,2 | 71,9 | 0,829 |
| Individual’s physical fatigue | 61,1 | 66,6 | 0,276 |
| Inability to provide timely treatment | 42 | 31,2 | <0,001 |
| Public health decisions affecting communities or populations | 41,4 | 28,4 | 0,005 |
| Lack of beds | 37,6 | 19,8 | <0,001 |
| Insufficient training to provide necessary treatment/support | 35,7 | 30,6 | 0,307 |
| Lack of time to give sufficient emotional support to patients | 34,4 | 38,7 | <0,001 |
| De-prioritising certain patients | 28,7 | 20,1 | 0,042 |
| Denying the families of dying patients access to see them | 24,2 | 29,2 | 0,284 |
| Guilt over risk of infecting family or friends with COVID-19 or other infectious diseases | 21 | 21,7 | 0,949 |
| A workplace culture that does not encourage ‘speaking up’ | 20,4 | 16,2 | 0,299 |
| Lack of agency/power to make correct decisions for patients | 16,6 | 12,8 | 0,321 |
| Putting your own and colleagues’ safety before that of the patient | 8,9 | 9,7 | 0,894 |
| Lack of personal protective equipment (PPE) | 4,5 | 3,3 | 0,715 |
| Lack of medicines | 3,8 | 3,3 | 0,99 |
| Lack of medical tests | 1,9 | 2,2 | 1,000 |
| Not sure | 1,3 | 2,8 | 0,465 |
Table 3.
Differences in decremental order of what doctors and nurses believe could help alleviate moral distress in the workplace.
Table 3.
Differences in decremental order of what doctors and nurses believe could help alleviate moral distress in the workplace.
| Factors that would help alleviate the risks of moral distress | Doctors (%) | Nurses (%) | p value |
|---|---|---|---|
| More staff | 83,4 | 80,8 | 0,553 |
| More access to ethical and legal support when faced with challenging decisions | 55,4 | 27,9 | <0,001 |
| Streamlined bureaucracy | 45,2 | 45,1 | 1,000 |
| Access to funding | 40,8 | 23,1 | <0,001 |
| Working fewer hours | 40,1 | 28,1 | 0,010 |
| More training | 38,9 | 39,8 | 0,911 |
| Greater emotional and psychological support | 35,7 | 48,5 | 0,009 |
| More beds | 34,4 | 18,4 | <0,001 |
| More flexibility to deal with patients on a case-by-case basis | 32,5 | 34,8 | 0,679 |
| A greater emphasis in the work culture on sharing feelings and concerns | 28,7 | 31,5 | 0,593 |
| Greater peer support | 27,4 | 27,3 | 1,000 |
| Access to a multidisciplinary team | 26,8 | 11,1 | <0,001 |
| A workplace that encourages speaking up | 21 | 24,2 | 0,495 |
| Separate space to meet colleagues | 17,2 | 14,2 | 0,460 |
| More time for reflection | 16,6 | 7,8 | 0,005 |
| More medicine/treatment readily available | 12,1 | 7,2 | 0,103 |
| Clearer lines of responsibility | 12,1 | 9,2 | 0,395 |
| More oversight from senior clinicians | 8,9 | 5,8 | 0,278 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



