
Submitted:
06 February 2024
Posted:
08 February 2024
You are already at the latest version
Abstract
Background: Cardiovascular diseases (CVDs) are a rising global burden. Preventative strategies such as Cardiac Rehabilitation (CR) have shown a marked reduction of disease burden. Despite this, CR is underutilized worldwide. This study aims to identify the barriers to CR among patients diagnosed with CVD.
Methods: A scoping review of the literature was conducted following the Joanna Briggs Institute (JBI) guidelines. Three major databases including CINAHL, PubMed, EBSCOhost and Scopus were used to obtain studies published between 2010 and 2023. Search terms such as “Cardiac rehab*”, “Barrier*”, “Cardiovascular”, “Disease” And “diagnosis*” Were utilized in order to obtain subject-specific studies relevant to the research question.
Results: From the initial 2098 studies only 14 were included in the final analysis, consisting of both qualitative and quantitative designs. The thematic analysis included “healthcare system-related factors”, “Socioeconomic factors”, and “individual characteristics”. Healthcare system-related factors were mostly related to poor availability of CR programs, lack of proper referral strategies, inadequate knowledge of CR provider and inter-provider communication issues, and lack of alternative methods of CR delivery. Socioeconomic barriers were lack of education, longer distance to CR facilities, high cost of care, unemployment, and poor income status. Identified individual characteristics were female gender, older age, and comorbidities.
Conclusion: Lack of resources, poor access, educational attainment, and high cost of care were some of the barriers to CR, particularly in low and middle-income countries (LMICs). Health policymakers and healthcare providers should implement strategies incorporating issues identified in this scoping review. Systematic reviews may be required to confirm these findings.
Keywords:
Barriers
; Cardiac Rehabilitation
; Cardiovascular Diseases
; prevention
; scoping review
Introduction
Cardiovascular diseases (CVDs) are a range of disorders of the heart and blood vessels. CVDs include Ischemic Heart Diseases (IHD), Cerebrovascular Disease, Peripheral Vascular Disease, Rheumatic Heart Disease, valvular heart diseases, and congenital heart diseases(World Health Organisation, 2021). CVDs are considered the major cause of mortality worldwide. For instance, CVD contributed to 17.9 million deaths in 2019, with heart diseases and stroke contributing to 85% of that. In addition, 38% of the premature deaths attributed to non-communicable diseases are caused by CVD across the world (WHO, 2021). Furthermore, disability-adjusted life years due to IHD and stroke have risen to 182 million and 143 million respectively(Roth et al., 2020). The above trend clearly demonstrates an overall increase of burden of IHD worldwide.
The burden of CVD is highest among low and middle-income countries (LMICs) compared to high-income countries (HICs)(WHO, 2021). Over 75% of CVD deaths occur in LMICs with more premature deaths being attributed to CVD. For instance, in Sub-Saharan Africa over 50% of the deaths due to CVDs are among the age group of 30-69 years (Gheorghe et al., 2018), that is nearly 10 years earlier than HICs, leading to loss of productivity and livelihood. The estimated economic loss due to CVD in LMICs was $3.7 trillion from 2011 to 2015. This was 2% of Gross Domestic Product and contributed nearly 50% of the non-communicable disease burden (Bloom et al., 2011).
Cardiovascular diseases are closely associated with behavioral and socioeconomic factors. The majority of the CVDs can be addressed in the early stages by modifying unhealthy behaviors. For instance, reducing tobacco consumption, modification of dietary risks, and increasing physical activity can be considered. The behavioral factors cause the development of intermediate-risk factors including hypertension, high plasma glucose level, hyperlipidemia, and high BMI. Also, poor governance, inefficient healthcare delivery methods, and insufficient funding to the health systems are major problems associated with poor healthcare delivery in the LMICs leading to a high prevalence of CVD(Gheorghe et al., 2018). Therefore, addressing above mentioned disparities is important to reduce the global CVD burden.
Prevention of CVD remains challenging for healthcare systems worldwide. According to the literature cardiac rehabilitation (CR) stands as a major secondary prevention strategy of CVD(Yuan et al., 2021). Cardiac rehabilitation (CR) is a multidisciplinary intervention recommended for patients with chronic or post-acute cardiovascular events such as, following a myocardial infarction, coronary revascularization, heart transplant, acute or chronic angina, or heart failure. The overall goal of CR is focused on early returning to daily activities and reducing cardiovascular risk factors (Bethell, Lewin, & Dalal, 2008). CR is a multi-interventional prevention method including risk factor modification, patient-tailored exercises, psychosocial counseling, and education (Anderson & Taylor, 2014).
Cardiac rehabilitation programs are mainly supervised by physicians such as cardiologists. Moreover, the team consists of a nurse, physiotherapist, occupational therapist, speech therapist, behavioral therapist, and psychologist, dietician, and family members (Tessler & Bordoni, 2021). Physiotherapists help patients to develop an individual exercise plan and dietitians involve to help a patient maintain healthy eating habits. A social worker or psychologist is helping patients to overcome stress and reduce any type of identified psychological conditions, including smoking cessation programs (Prabhu, Maiya, & Prabhu, 2020).).
Referral to a CR program is based on clinical diagnosis and it involves three phases.
- Phase I: Clinical phase
The first phase of the CR program starts during the hospitalization period, after a cardiovascular event, or after an intervention like revascularization. The aim is to facilitate early ambulation and provide motivation for the rehabilitation process (Tessler & Bordoni, 2021). The CR team needs to pay attention to Activities of Daily Living (ADLs) and train the patient to reduce the stress during the CR process and encourage the patient to remain active until the completion of the rehabilitation program (Prabhu et al., 2020).
- Phase II: Outpatient Cardiac Rehab
The outpatient cardiac rehabilitation begins after identifying the patient is stable by cardiology. Once three weeks are completed in phase I, then phase II is starting between the third to sixth week. Phase II is mainly based on the assessment of individual needs of patients including electrocardiographic monitoring, counseling, and aggressive risk factor management. This phase promotes the healthy lifestyle of the patient and prepares them to return to their normal lives(Tessler & Bordoni, 2021).
- Phase III: Post-Cardiac Rehab
Phase III conducts with minimal supervision or without any supervision by encouraging self-monitoring and periodic medical assessment of disease conditions. Phase III ensures lifelong commitment to maintain healthy behaviors (Bethell et al., 2008).
CR has been recognized as one of the best cost-effective, treatment and secondary prevention methods that improve quality of life(Shields et al., 2018). Evidence shows that CR increases overall prognosis by reducing mortality, morbidity, and re-hospitalization by 20% (Prabhu et al., 2020). According to the literature, the health-related quality of life (HRQoL) of patients after 12 months of engagement of CR has significantly improved. Randomized control trial (RCTs) by Anderson and his colleagues has found that CR has reduced hospitalizations in post-myocardial infarction patients due to heart failure compared to their control groups(Anderson & Taylor, 2014). CR can reduce the probability of mortality within the 5 years following a CVD or bypass surgery by 35% (Yohannes, Doherty, Bundy, & Yalfani, 2010).
Further, CR programs help to increase body functional capacity and decrease associated disabilities and weaknesses by providing patient-tailored physical exercises according to their medical diagnosis(Anderson & Taylor, 2014). In addition to that, reassuring psychological wellbeing is one of the major components of the CR program that help to reduce stress and anxiety after a cardiac event that promotes faster recovery and reduces depression and other mental disorders (Bethell et al., 2008). Moreover, CR programs encourage and monitor adherence to medical management thus improving patients' compliance reducing future mortality and morbidity from cardiac events (Lavie & Milani, 2001).
Despite CR has recognized as a gold standard treatment strategy, it remains under-utilized around the globe (Prabhu et al., 2020). The availability of CR reported significantly low whereas 60% in HICs, 28% in middle-income countries, and 8% in low-income countries respectively. Further, low referral and participation rates and higher dropout rates have been reported globally (Turk-Adawi, Terzic, Bjarnason-Wehrens, & Grace, 2015).
Hence it is crucial to identify the factors that inhibit the referral, participation, and adherence to CR because of its proven benefits in reducing the overall CVD-related burden. The main objective of this scoping review is to identify the barriers to CR among patients diagnosed with CVD from a global perspective. By identifying these barriers, the respective authorities and stakeholders will be able to focus on priority areas and implement sustainable measurements to enhance the CR availability, referrals, and participation thus reducing the global CVD-related mortality and morbidity.
Method
Study Design
A scoping review of the literature was conducted to assess the barriers to cardiac rehabilitation among patients diagnosed with CVD using PRISMA-ScR (PRISMA for scoping reviews). See Figure 1
Data Sources
Extensive literature search was conducted using databases such as CINAHL, SCOPUS, EBSCOHost and PubMed from 2010 to 2023, using the following search term:
(barrier) AND (challenge OR limitation) AND (‘cardiac rehab”) AND (“cardiovascular disease” OR CVD OR “heart disease”). The search was limited to patients diagnosed with CVD and those published in English.
Study Selection
We have included articles in the following criteria: 1) studies with patients diagnosed with CVD who referred and/or participated and/or benefitted with CR programs and 2) studies that observe the individual characteristics, hospital system-related factors, and socioeconomic factors as barriers to CR referral and/or participation and/or drop out among study population and 3) studies that compare the barriers in a global context, HICs, and LMICs. Also, we have included both qualitative (cohort, case-control, cross-sectional and systematic review) and quantitative studies in this review. We have excluded articles before 2010 and that studied a small sample size(n=<50).
Data Synthesis and Analysis
Data from selected studies were extracted according to the standardised approach and were sorted into tables. The study characteristics were recorded according to study design, author, year, country, study subjects, barriers, and parameters (Table 1). Results were analysed using thematic analysis. Then the results were categorized into three main themes including healthcare system-related factors, socio-economic factors, and individual characteristics (Table 2). Extracted data under three main themes were categorized into subthemes for further interpretation.
Table 2 illustrates the barriers to CR identified in the selected 13 studies that were included in this scoping review. Overall, 3 main barriers; healthcare system-related factors, socioeconomic factors, and individual characteristics were identified and further analyzed according to subthemes.
Ethical Consideration
As this study used secondary data from literature, there were no ethical concerns.
Results
Identification and Selection of Literature
The main three databases were divided among three researchers who searched in electronic databases separately using key terms and a total of 2098 were found. Then 1012 duplicates were removed. After that articles were filtered according to titles and abstract and 803 were excluded. The final 14 articles were selected after excluding 269 articles by reading the full text. Fourteen studies were included in the scoping review. Characteristics of the included studies are summarized in Table 1. One study was a systematic review(Gaalema, Cutler, Higgins, & Ades, 2015), four studies were prospective cohort studies(Bachmann et al., 2017; Grace et al., 2011; Krishnamurthi, Schopfer, Shen, & Whooley, 2019; Parashar et al., 2012), three studies were retrospective cohort studies(Borg et al., 2019; Chamosa et al., 2015; Rodrigo et al., 2021) five studies were cross-sectional studies(Moradi, Maleki, Esmaeilzadeh, & Abkenar, 2011; Pesah et al., 2019; Soroush, Heydarpour, Komasi, Saeidi, & Ezzati, 2018; Turk-Adawi et al., 2019 ; Fraser et al., 2022) and one qualitative study(Schopfer et al., 2016). Two globally conducted studies were analysed in the scoping review. Other studies were from the United States, Canada, Iran, Netherland, Sweden, and Spain. Most of the participants were either patients diagnosed with CVD or CR providers including cardiologists, physicians, and CR managers.
Healthcare System Related Factors
Availability of Cardiac Rehabilitation Programs
Three studies have examined the availability of cardiac rehabilitation worldwide(Pesah et al., 2019; Schopfer et al., 2016; Turk-Adawi et al., 2019). Turk-Adwai and colleagues conducted a cross-sectional study across the globe including 98 countries to determine the availability, capacity, and density of the cardiac rehabilitation programs. The study identified that 54.7% of the countries worldwide had cardiac rehabilitation programs. Furthermore, disparities of availability were identified across the regions. For instance, cardiac rehabilitation programs were available in 80.7% of the European countries compared to 17.0% African countries (p < 0.001). Moreover, 5735 CR programs were identified, and they could facilitate only 1,655,083 patients out of 20,279,651 annual IHD patients worldwide(Turk-Adawi et al., 2019). Another cross-sectional study was conducted by Pesah and colleagues from 55 countries to identify the barriers to the delivery of cardiac rehabilitation in LMICs. According to their study, cardiac rehabilitation programs are available in 16.7% of LICs, 47.1% of MICs and 86.2% in HICs ((χ2 =37.3, p<0.001). Moreover, in LMICs only one spot in cardiac rehabilitation was available for 66 IHD patients( Pesah et al., 2019).
Referral Strategies
Two studies have studied the impact of referral strategies on utilisation rates of cardiac rehabilitation(Grace et al., 2011; Turk-Adawi et al., 2019). A prospective cohort study was conducted by Grace and colleagues with 1809 participants has concluded that automated referral strategies led to a 70% referral rate and 60% enrolment in cardiac rehabilitation (OR, 3.27; CI, 1.52-7.04). The Liaison referral strategy resulted in a 59% referral rate and 50.6% enrolment in cardiac rehabilitation (OR, 3.35; CL, (1.54-7.29). Moreover, combined use of automated and liaison referral strategies has shown 85.8% referral rates and 73.5% enrolment (OR, 8.41; CI, 3.57-19.85) compared to traditional referral strategies which only resulted in 32.2% referral rate and 29% enrolment( Grace et al., 2011). Similar results were identified by a cross-sectional study conducted by Turk-Adwai and colleagues regarding the availability and density of cardiac rehabilitation programs worldwide. They have also identified higher referral rates where systematic referral strategies were used compared to programs where traditional referral strategies were used(Turk-Adawi et al., 2019).
Providers' knowledge of CRTwo studies have shown the effect of cardiac rehabilitation providers’ knowledge on referral rates to cardiac rehabilitation(Moradi et al., 2011; Schopfer et al., 2016). A qualitative study conducted by Schopfer and colleagues found that 73% of cardiac rehabilitation providers were unfamiliar with indications and referral strategies of cardiac rehabilitation leading to less referral rates(Schopfer et al., 2016). Moradi and colleagues conducted a cross-sectional study among 122 cardiologists to observe the physician-related factors affecting cardiac rehabilitation. 79.5% of cardiologists have reported that lack of physician's knowledge including benefits, program attributes, and referral strategies acts as a barrier to cardiac rehabilitation(Moradi et al., 2011).
Inter-Provider Communication
Inter-provider communication methods and delivery modes or settings are found to have an impact on referral rates and participation rates of cardiac rehabilitation (Schopfer et al., 2016; Turk-Adawi et al., 2019). A qualitative study conducted by Schopfer and colleagues to identify the patient and provider level barriers and facilitators to cardiac rehabilitation has shown that poor inter-provider communication has resulted in fewer referral rates. 18% of CR providers and 17% of CR managers have perceived poor communication among clinicians and providers as a barrier to cardiac rehabilitation(Schopfer et al., 2016). Turk-Adwai and colleagues' cross-sectional study which was conducted to observe the availability and density of the cardiac rehabilitation programs have found that mode/setting of delivery affects participation rates (OR = 1.05, 95%CI = 1.04–1.06).
Socio-Spatial Factors
Accessibility to Cardiac Rehabilitation Facilities
Seven studies have found the association of accessibility to CR facilities and patients’ enrollment and participation(Bachmann et al., 2017; Chamosa et al., 2015; Rodrigo et al., 2021; Schopfer et al., 2016; Soroush et al., 2018; Borg et al., 2019). Borg and his colleagues have conducted a retrospective cohort study to identify the factors related to non-attendance in center-based CR programs using the data of 31,297 post-AMI patients covering six years period(Borg et al., 2019). They have identified the distance to CR facility as the strongest predictor for non-attendance (OR 1.75 [95% CI: 1.64–1.86]) where patients who lived >16km away from facilities have 25% higher non-attendance compared to their counterparts. Also, the prospective cohort study conducted by Bachman and his colleagues has found that when distance increase to CR centers was significantly reduced the CR participation by 29% (OR 0.71, 95% CI, 0.59–0.84, P<0.001)(Bachmann et al., 2017). Chamosa and his colleagues also conducted a retrospective cohort study on 756 patients with myocardial infarction from 2009 to 2012. According to the study they have found that patients who are living >50km away from CR units have 3 folds higher chance of non-enrollment( Chamosa et al., 2015). Also, Rodrigo and his colleagues have conducted a similar study on 469 patients who were hospitalized for acute coronary syndrome in 2017 and evaluated the predictors for their CR referral and participation(Rodrigo et al., 2021). They have found that patients who have >20km distance have higher referral (OR 4.0, CI 1.26–13.0) but less participation (OR 0.2, CI 0.07–0.79) compared to patients who <5km distance to CR centers. Moreover, a cross-sectional study conducted on 312 CABG patients by Soroush and colleagues to assess the predictors for CR referral has found that long distances to CR facilities significantly reduce the referral(p<0.042) among CABG patients(Soroush et al., 2018). A qualitative study has conducted by Schopfer and his colleagues on a total of 56 participants including patients, CR providers, and program managers to assess the barriers to CR utilization and according to their results most perceived barrier was problems with transportation and distance to CR centers(68%) thus limit the CR utilization(Schopfer et al., 2016).
Similarly, Fraser et al., 2022 in their cross-sectional study emphasized the factor of geographic location of a cardiac patient significantly affecting the completion or uptake of cardiac rehabilitation (CR) programs. Participants in their cross-sectional survey reported the barriers to attending cardiac rehabilitation classes include lack of resource allocation within the remote areas such as poor of provider support, inconvenient commute options and long waiting times to be contacted for the CR rehab, while some participants in this study felt the need to take responsibility for their own rehabilitation due to limited number of rehab services provided within the disadvantaged areas.
Employment Status/Income
Four studies have found the association between employment status and enrolment and attendance to CR programs(Bachmann et al., 2017; Borg et al., 2019; Chamosa et al., 2015; Soroush et al., 2018). The study conducted by Borg and his colleagues has found that retired patients compared to employed patients were 14% less likely to attend CR programs(OR 0.86; CI,0.80-0.93)(Borg et al., 2019). According to the prospective cohort study by Bachmann et al., household income >$25,000 per year has 64% higher participation (OR 1.68, 95% CI, 1.17–2.42, P<0.01) compared to a household with < $15,000 per year(Bachmann et al., 2017). Also, Soroush and his colleagues have found that there was higher CR referral among patients who are employed(24%) compared to retired(12%) and unemployed(4%)patients(Soroush et al., 2018). But the study conducted by Chamosa and his colleagues has found no significant difference between the rate of enrollment among self-employed (OR = 1.56; 95% CI: 0.62-3.92) and retired workers (OR = 1.33; 95% CI: 0.62-2.77)( Chamosa et al., 2015).
Level of Education
Three studies have found the association between level of education and CR participation (Bachmann et al., 2017; Parashar et al., 2012; Soroush et al., 2018). According to Bachmann and his colleagues, they have found that people who have completed college have a higher participation rate (OR 1.61, 95% CI, 1.06–2.44, P<0.05)compared to those who have completed high school education(Bachmann et al., 2017). According to the study conducted by Soroush and colleagues, illiterate patients were less likely to refer to CR programs compared to patients who have a higher educational level (7% and 16% respectively). Also, Parashar and colleagues conducted a prospective cohort study on 1568 patients with AMI to look at the CR participation within one month and 6 months post-MI( Parashar et al., 2012). They have found that patients who have completed at least high school education have higher participation at the first month after post-MI (OR, 1.38; 95% CI, 1.04–1.84) and after 6 months of MI event (OR, 1.81; 95% CI, 1.42–2.30).
Affordability and Access to Care
Three studies have found the association between cost of care and CR participation( Parashar et al., 2012; Pesah et al., 2019). Pesha and his colleagues have conducted a cross-sectional study collecting data from all available CR programs globally and analyzing the relation between cost of care and CR participation and dropout( Pesah et al., 2019). According to their study, in LMICs 65% of CR cost was out-of-pocket expenditure and it was 24% in HICs. Also, the prospective cohort study of Parashar et al., has found that uninsured patients (OR, 0.39; 95% CI, 0.21–0.71) 60% less likely to participate in CR at the first month of the post-MI period but insurance status of the patient (both uninsured and insured, p<0.001) did not predict CR participation at 6 months( Parashar et al., 2012). In addition to that patients who have economic burden have less participation in CR programs after 6 months (OR, 0.56; 95% CI, 0.38–0.81) compared to the first month (OR, 1.48; 95% CI, 0.97-2.26).
Individual Characteristics
Comorbidities
Five studies have found the association between comorbidities and less participation in CR program (Bachmann et al., 2017; Borg et al., 2019; Chamosa et al., 2015; Gaalema et al., 2015; Parashar et al., 2012). Borg and colleagues found that smoking (OR, 1.63; 95% CI,1.54-1.74), history of stroke (OR,1.37;CI,1.21-1.550 percutaneous coronary intervention (PCI) (OR, 1.28;CI,1.16-1.42) coronary artery bypass graft (OR,1.31;CI,1.16-1.42, AMI (OR,1.19;CI,1.08-1.31) or diabetes (OR,1.20; 95% CI, 1.13-1.28) as predictors for nonattendance in CR (Borg et al., 2019). The prospective cohort study by Parashar and colleagues found that lesser participation rates were reported after one month by the patients with hypertension (OR, 0.58; CI, 0.43-0.78), peripheral arterial disease (OR, 0.43; CI.0.22-0.850). Smokers were less likely to participate after six months (OR, 0.59; CI, 0.44-0.80)( Parashar et al., 2012). Bachmann and colleagues found that patients who were smoking were less likely to participate in CR (OR, 0.65; CI, 0.49-0.85) (Bachmann et al., 2017). Gaalema and colleagues conducted a systematic review using 56 peer-reviewed articles to look for the association between smoking and referral, attendance and adherence to CR. They found that smokers are more likely to refer to CR but smoking is associated with less participation and non-adherence (Gaalema et al., 2015). Different results were found by Krishnamurthy and colleagues. They conducted a prospective cohort study to look for an association between mental health conditions and participation in CR by conducting a prospective cohort study on 86537 patients. The above study found that patients with post-traumatic stress disorder (PTSD) and depression are more likely to participate in CR (OR, 1.57; CI, 1.43-1.74) ( Krishnamurthi et al., 2019).
Generic Factors
Two studies found an association between older age and less participation rate in CR ( Chamosa et al., 2015; Parashar et al., 2012). Chamosa and colleagues found that the older age group has higher non-enrollment and with every year of age there was a 5% chance of rising non-enrollment(OR, 1.05; 95% CI: 1.02-1.09) ( Chamosa et al., 2015). The cohort study by Parashar et al (2012) found that older patients are 15% less likely to participate in CR (OR, 0.85 for each 10-year increment; CI, 0.74–0.97) (Parashar et al., 2012).
Two studies showed the relationship between female gender and less participation rate ( Chamosa et al., 2015; S. Parashar et al., 2012). The cohort study by Chamosa et al (2015) found that women with previous MI were less likely to participate (OR: 6.35; 95% CI: 2.53-11.81). Further, they found that females are less likely to refer to CR whereas referral for men was 35.9% and women 20.8% respectively. Conversely, one study found male gender as a predictor for non-attendance in CR(Borg et al., 2019).
Discussion
This scoping review was conducted to identify the barriers to cardiac rehabilitation among patients diagnosed with CVD from a global perspective. Although further studies are needed for more robust evidence, the results of the current study suggest that healthcare system-related factors, socio-economic factors, and individual characteristics have a significant impact on referral, enrolment, and participation in cardiac rehabilitation programs.
Healthcare system-related factors including poor availability of CR programs, lack of proper referral strategies, inadequate knowledge of CR providers, inter-provider communication issues, and lack of alternative methods of CR delivery were identified as barriers to CR.
Despite CR has been recognised as an important intervention in CVD management, the review identified the disparities in the availability of CR programs across the globe, particularly in LMICs. The need for establishing more rehabilitation services for both communicable and non-communicable diseases has been identified worldwide. For example, a study conducted to estimate the need for rehabilitation services has identified that 2.41 billion people could benefit from rehabilitation programs(Cieza et al., 2020).
Traditional referral strategies resulted in fewer referral rates and enrollment rates compared to systematic referral strategies. Similarly, a study conducted by Gravely-Witte and colleagues has identified that automatic and liaison referral strategies could considerably increase the referral and participation rates(Gravely et al., 2009). Furthermore, proper communication among CR providers including in-patient cardiologists, follow-up specialty clinics, or primary care and CR services can lead to more referral rates to rehabilitation. In addition, CR programs delivered in alternative modes such as home-based rehabilitation and telerehabilitation resulted in higher patient compliance in rehabilitation. According to Ozemek and colleagues, CR services can be delivered remotely using alternative methods to increase CR participation(Ozemek, Babu, Arena, & Bond, 2021).
According to this study, socioeconomic factors like lack of accessibility to CR facilities, low level of education, unemployment or poor income, and high cost of care were identified as the barriers to referral and participation of CR.
The Longer distance to CR facilities has been identified as a major barrier to CR referral and participation. Several contributing factors like unavailability of proper transportation methods, cost of transportation, and time constraints may cause more reluctance to travel long distances(Syed, Gerber, & Sharp, 2013). Therefore proper access to healthcare has a great impact on health outcomes especially for non-communicable chronic diseases like CVD where follow-up and prevention methods such as CR are crucial. Moreover, a systematic review done by Starbird and his colleagues has found the association between establishing transport interventions and an increase in services of chronic care management(Starbird, DiMaina, Sun, & Han, 2019). Also, encouraging home-based CR programs will resolve the problems with access to care thus increasing participation and adherence(Ge et al., 2019).
Considering the patients' level of education, it has played a significant role in CR participation and enrollment. Individual level of education plays a crucial role in literacy of the person. Acquired knowledge of individuals is used to understand and make positive decision related to health outcome, to acquire health-related information, health promotion, and providing care(Liu et al., 2020). For example, a cohort study conducted by Demmler and his colleagues has found that children who have successful education attainments have less health risks behaviors at adolescence period proving the positive influence of education on health(Demmler et al., 2017). Therefore with adequate education and capability to understand the benefits of prevention programs like CR will enhance the patients' participation and reduce the overall burden associated with CVD.
Other factors that affect CR participation and referral are poor income status, unemployment, and the high cost of rehabilitation sessions. Health outcomes of individuals highly depend on income status as income is the major indicator for acquiring all resources in daily life like food, medicine, housing, healthcare services, and education(Darin-Mattsson, Fors, & Kåreholt, 2017). Therefore it will affect individual health-related choices.
Also, comorbidities such as the history of stroke, PCI, AMI, CABG, diabetes, hypertension, low physical function smoking, and female gender and older age were identified as the individual characteristics associated with less enrollment and participation in CR. In line with the literature, lack of patient's desire and lack of willingness to participate in CR was found as barriers. After the revascularization procedure, patients think they will be cured and some patients do not trust that CR will be beneficial (Schopfer et al., 2016). Comorbidities reduced one’s functional capacity and tailored CR programs can be used to improve participation rates (Beckie & Beckstead, 2010). According to the literature, smoking stands as a strong barrier to enrolment and participation. Special considerations should be given to smokers following a cardiac problem and Smoking cessation in CR programs should be reviewed while providing additional support (Gaalema et al., 2015). In contrast with literature, Krshnamurthi et al (2019) mentioned that patients with comorbid depression and PTSD showed higher participation rates. This may be due to CR providing more mental health support to these patients that would be more beneficial ( Krishnamurthi et al., 2019).
The female gender showed disparities in referral, enrolment, and participation. Women's health-seeking behaviors for their symptoms are postponed compared to men and their exercise tolerance is lower than men especially following a cardiac event (Davidson et al., 2008). Gender-specific cardiac health needs for women are recognized as an effective intervention for women. In line with the literature gender tailored CR programs showed improved attendance by 31% (Beckie & Beckstead, 2010). Gender disparity in referral enrolment and participation in CR can be addressed by planning gender-tailored programs that are planned according to the unique needs of females. Different results were shown by Borg et al (2019) where female participation is higher. However, their study was limited to exercise-based CR programs and the study was based on Sweden which is not a male dominate country.
Despite the gender older patient's enrolment and participation were reported lower. When compare with younger patients, generally older patients have low income and they may not perceive CR as a beneficial method. As older people's physical capacity is lower and their rehabilitation requirements could be different from younger patients. To achieve the expected benefits of CR, it should be adapted to individual capacity and outcome goals should be planned according to age groups (Chamosa et al., 2015). However, according to recent literature the younger patients and the male participation becoming lower (Bachmann et al., 2017; Borg et al., 2019) whereas CR achievements should be planned for both sex and all aged groups by addressing other influencing factors.
Limitations
This review has a few limitations. Even though the study was conducted at a global level, studies were limited to a few countries including the USA, Canada, Netherland, Sweden, Spain, and Iran. Therefore, evidence from LMICs was limited and outcomes of the scoping review were mostly based on HICS.
Due to time constraints, scoping review was used to conduct the analysis. However, if a systematic review with meta-analysis was conducted, a more robust global level evidence could have been analysed and a better understanding could be obtained of the barriers to CR.
Recommendation
More global level studies should be conducted to identify barriers to CR in-depth, particularly in LMICs. Governments should allocate more funding to establish home-based and community-based cardiac rehabilitation services to enhance participation and adherence. Also, the government should consider increasing more public-funded programs to reduce out-of-pocket expenditure in CR. Further, introducing advanced technologies to increase the utilization of automated referral strategies and to promote telehealth services is recommended. Additionally, continuous provision of regular training to healthcare professionals to increase the efficacy of CR delivery and review the patient's understanding of CR and incorporate education sessions to CR to increase patient compliance is highly recommended.
Conclusion
The burden of CVD is rising worldwide. Despite CR being considered as the most cost-effective treatment strategy of CVD, it is grossly underutilized. Various factors related to the healthcare system, socioeconomic status, and individual characteristics were identified as key barriers to cardiac rehabilitation. These findings should be the focus of healthcare planning and healthcare policies as an attempt to improve outcomes of cardiovascular rehabilitation programs. Further studies are recommended to identify the barriers in-depth especially in CVD high prevalence areas like LMICs.
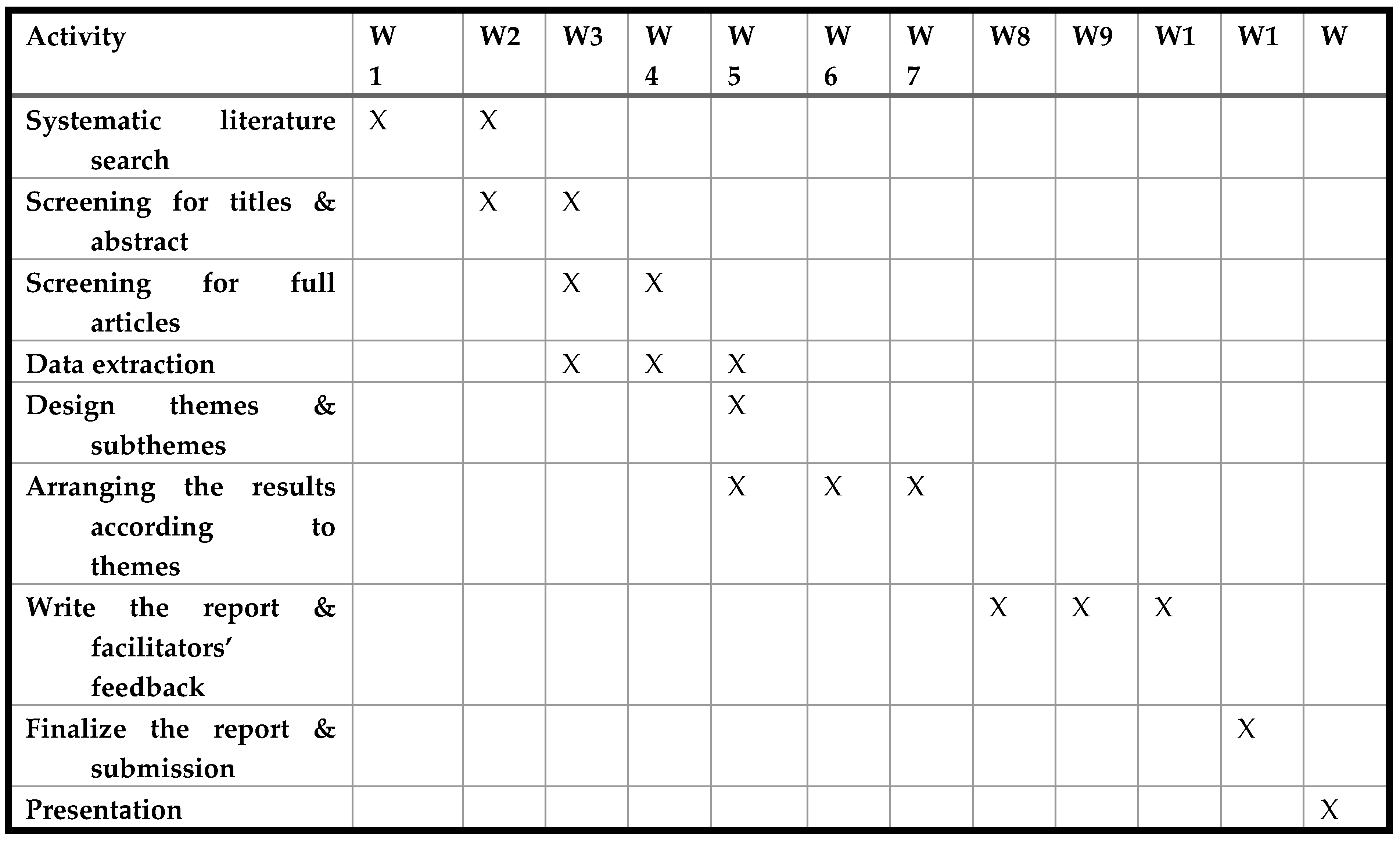
Gantt Chart
Contributions
FH: GP: PA, and PS participated in research concept and design and data collection, PI, WU, GP, PA, and PS conducted data analysis, and writing of the paper. PI, WU participated in the performance of the
research and data collection. PI, FH, provided advice and support. All authors have read and approved the manuscript.
Acknowledgments
Support from relevant University and clinic administration.
Competing Interests (Disclosures/Sources of Funding)
None.
References
- Anderson, L., & Taylor, R. S. (2014). Cardiac rehabilitation for people with heart disease: an overview of Cochrane systematic reviews. The Cochrane database of systematic reviews, 2014(12), CD011273-CD011273. [CrossRef]
- Bachmann, J. M., Huang, S., Gupta, D. K., Lipworth, L., Mumma, M. T., Blot, W. J., . . . Freiberg, M. S. (2017). Association of Neighborhood Socioeconomic Context With Participation in Cardiac Rehabilitation. Journal of the American Heart Association, 6(10), e006260. [CrossRef]
- Beckie, T. M., & Beckstead, J. W. (2010). Predicting cardiac rehabilitation attendance in a gender-tailored randomized clinical trial. Journal of Cardiopulmonary Rehabilitation and Prevention, 30(3), 147-156. [CrossRef]
- Bethell, H. J. N., Lewin, R. J. P., & Dalal, H. M. (2008). Cardiac rehabilitation: it works so why isn't it done? The British journal of general practice : the journal of the Royal College of General Practitioners, 58(555), 677-679. [CrossRef]
- Bloom, D. E., Chisholm, D., Jané-Llopis, E., Prettner, K., Stein, A., & Feigl, A. (2011). From Burden to “Best Buys”: Reducing the Economic Impact of Non-Communicable Diseases. World Health Org., Geneva, Switzerland.
- Borg, S., Öberg, B., Leosdottir, M., Lindolm, D., Nilsson, L., & Bäck, M. (2019). Factors associated with non-attendance at exercise-based cardiac rehabilitation. BMC sports science, medicine & rehabilitation, 11, 13-13. [CrossRef]
- Chamosa, S., Alarcón, J. A., Dorronsoro, M., Madruga, F. J., Barrera, J., Arrazola, X., . . . San Vicente, J. M. (2015). Predictors of Enrollment in Cardiac Rehabilitation Programs in Spain. Journal of Cardiopulmonary Rehabilitation and Prevention.
- , 35(4), 255-262. [CrossRef]
- Cieza, A., Causey, K., Kamenov, K., Hanson, S. W., Chatterji, S., & Vos, T. (2020). Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet, 396(10267), 2006-2017. [CrossRef]
- Darin-Mattsson, A., Fors, S., & Kåreholt, I. (2017). Different indicators of socioeconomic status and their relative importance as determinants of health in old age. International Journal for Equity in Health, 16(1), 173. [CrossRef]
- Davidson, P., Digiacomo, M., Zecchin, R., Clarke, M., Paul, G., Lamb, K., . . . Daly, J. (2008). A cardiac rehabilitation program to improve psychosocial outcomes of women with heart disease. J Womens Health (Larchmt), 17(1), 123-134. [CrossRef]
- Demmler, J. C., Hill, R. A., Rahman, M. A., Bandyopadhyay, A., Healy, M. A., Paranjothy, S., . . . Brophy, S. T. (2017). Educational Attainment at Age 10-11 Years Predicts Health Risk Behaviors and Injury Risk During Adolescence. The Journal of adolescent health : official publication of the Society for Adolescent Medicine, 61(2), 212-218. [CrossRef]
- Gaalema, D. E., Cutler, A. Y., Higgins, S. T., & Ades, P. A. (2015). Smoking and cardiac rehabilitation participation: Associations with referral, attendance and adherence. Preventive medicine, 80, 67-74. [CrossRef]
- Ge, C., Ma, J., Xu, Y., Shi, Y.-J., Zhao, C.-H., Gao, L., . . . Chen, Y.-D. (2019). Predictors of adherence to home-based cardiac rehabilitation program among coronary artery disease outpatients in China. Journal of geriatric cardiology : JGC, 16(10), 749-755. [CrossRef]
- Gheorghe, A., Griffiths, U., Murphy, A., Legido-Quigley, H., Lamptey, P., & Perel, P. (2018). The economic burden of cardiovascular disease and hypertension in low- and middle-income countries: a systematic review. BMC Public Health, 18(1), 975. [CrossRef]
- Grace, S. L., Russell, K. L., Reid, R. D., Oh, P., Anand, S., Rush, J., . . . Stewart, D. E. (2011). Effect of cardiac rehabilitation referral strategies on utilization rates: a prospective, controlled study. Arch Intern Med, 171(3), 235-241. [CrossRef]
- Grace, S. L., Russell, K. L., Reid, R. D., Oh, P., Anand, S., Rush, J., . . . Cardiac Rehabilitation Care Continuity Through Automatic Referral Evaluation, I. (2011). Effect of Cardiac Rehabilitation Referral Strategies on Utilization Rates: A Prospective, Controlled Study. Archives of Internal Medicine, 171(3), 235-241. [CrossRef]
- Gravely, S., Leung, Y., Nariani, R., Tamim, H., Oh, P., Chan, V., & Grace, S. (2009). Effects of cardiac rehabilitation referral strategies on referral and enrollment r. Nature reviews. Cardiology, 7, 87-96. [CrossRef]
- Fraser, M. J., Leslie, S. J., Gorely, T., Foster, E., & Walters, R. (2022). Barriers and facilitators to participating in cardiac rehabilitation and physical activity: A cross-sectional survey. World journal of cardiology, 14(2), 83–95. [CrossRef]
- Krishnamurthi, N., Schopfer, D. W., Shen, H., & Whooley, M. A. (2019). Association of Mental Health Conditions With Participation in Cardiac Rehabilitation. J Am Heart Assoc, 8(11), e011639. [CrossRef]
- Lavie, C. J., & Milani, R. V. (2001). Benefits of cardiac rehabilitation and exercise training programs in elderly coronary patients. Am J Geriatr Cardiol, 10(6), 323-327. [CrossRef]
- Liu, C., Wang, D., Liu, C., Jiang, J., Wang, X., Chen, H., . . . Zhang, X. (2020). What is the meaning of health literacy? A systematic review and qualitative synthesis. Family Medicine and Community Health, 8(2), e000351. [CrossRef]
- Moradi, B., Maleki, M., Esmaeilzadeh, M., & Abkenar, H. B. (2011). Physician-related factors affecting cardiac rehabilitation referral. The journal of Tehran Heart Center, 6(4), 187-192. Retrieved from https://pubmed.ncbi.nlm.nih.gov/23074367.
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3467958/.
- Parashar, S., Spertus, J. A., Tang, F., Bishop, K. L., Vaccarino, V., Jackson, C. F., . . . Sperling, L. (2012). Predictors of Early and Late Enrollment in Cardiac Rehabilitation, Among Those Referred, After Acute Myocardial Infarction. Circulation, 126(13), 1587-1595. [CrossRef]
- Pesah, E., Turk-Adawi, K., Supervia, M., Lopez-Jimenez, F., Britto, R., Ding, R., . . . Grace, S. L. (2019). Cardiac rehabilitation delivery in low/middle-income countries. Heart (British Cardiac Society), 105(23), 1806-1812. [CrossRef]
- Pesah, E., Turk-Adawi, K., Supervia Pola, M., Lopez-Jimenez, F., Britto, R., Ding, R., . . . Grace, S. (2019). Cardiac rehabilitation delivery in low/middle-income countries. Heart, 105, heartjnl-2018. [CrossRef]
- Prabhu, N. V., Maiya, A. G., & Prabhu, N. S. (2020). Impact of Cardiac Rehabilitation on Functional Capacity and Physical Activity after Coronary Revascularization: A Scientific Review. Cardiology research and practice, 2020, 1236968-1236968. [CrossRef]
- Rodrigo, S. F., Van Exel, H. J., Van Keulen, N., Van Winden, L., Beeres, S. L. M. A., & Schalij, M. J. (2021). Referral and participation in cardiac rehabilitation of patients following acute coronary syndrome; lessons learned. IJC Heart & Vasculature, 36, 100858. [CrossRef]
- Roth, G. A., Mensah, G. A., Johnson, C. O., Addolorato, G., Ammirati, E., Baddour, L. M., . . . Fuster, V. (2020). Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update From the GBD 2019 Study. Journal of the American College of Cardiology, 76(25), 2982-3021. [CrossRef]
- Schopfer, D. W., Priano, S., Allsup, K., Helfrich, C. D., Ho, P. M., Rumsfeld, J. S., . . . Whooley, M. A. (2016). Factors Associated With Utilization of Cardiac Rehabilitation Among Patients With Ischemic Heart Disease in the Veterans Health Administration: A QUALITATIVE STUDY. J Cardiopulm Rehabil Prev, 36(3), 167-173. [CrossRef]
- Shields, G. E., Wells, A., Doherty, P., Heagerty, A., Buck, D., & Davies, L. M. (2018). Cost-effectiveness of cardiac rehabilitation: a systematic review. Heart (British Cardiac Society), 104(17), 1403-1410. [CrossRef]
- Soroush, A., Heydarpour, B., Komasi, S., Saeidi, M., & Ezzati, P. (2018). Barriers for the referral to outpatient cardiac rehabilitation: A predictive model including actual and perceived risk factors and perceived control. Annals of Cardiac Anaesthesia, 21(3), 249-254. [CrossRef]
- Starbird, L. E., DiMaina, C., Sun, C.-A., & Han, H.-R. (2019). A Systematic Review of Interventions to Minimize Transportation Barriers Among People with Chronic Diseases. Journal of Community Health, 44(2), 400-411. [CrossRef]
- Syed, S. T., Gerber, B. S., & Sharp, L. K. (2013). Traveling towards disease: transportation barriers to health care access. Journal of Community Health, 38(5), 976-993. [CrossRef]
- Tessler, J., & Bordoni, B. (2021). Cardiac Rehabilitation. Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK537196/.
- Turk-Adawi, K., Supervia, M., Lopez-Jimenez, F., Pesah, E., Ding, R., Britto, R. R., . . . Grace, S. L. (2019). Cardiac Rehabilitation Availability and Density around the Globe. EClinicalMedicine, 13, 31-45. [CrossRef]
- Turk-Adawi, K. I., Terzic, C., Bjarnason-Wehrens, B., & Grace, S. L. (2015). Cardiac rehabilitation in Canada and Arab countries: comparing availability and program characteristics. BMC Health Services Research, 15, 1-10. [CrossRef]
- World Health Organisation. (2021). Cardiovascular Diseases (CVD). Retrieved from https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds).
- Yohannes, A., Doherty, P., Bundy, C., & Yalfani, A. (2010). The long-term benefits of cardiac rehabilitation on depression, anxiety, physical activity and quality of life. Journal of Clinical Nursing, 19, 2806-2813. [CrossRef]
- Yuan, G., Shi, J., Jia, Q., Shi, S., Zhu, X., Zhou, Y., . . . Hu, Y. (2021). Cardiac Rehabilitation: A Bibliometric Review From 2001 to 2020. Frontiers in Cardiovascular Medicine, 8(469). [CrossRef]
Figure 1.
PRISMA Flow Diagram.
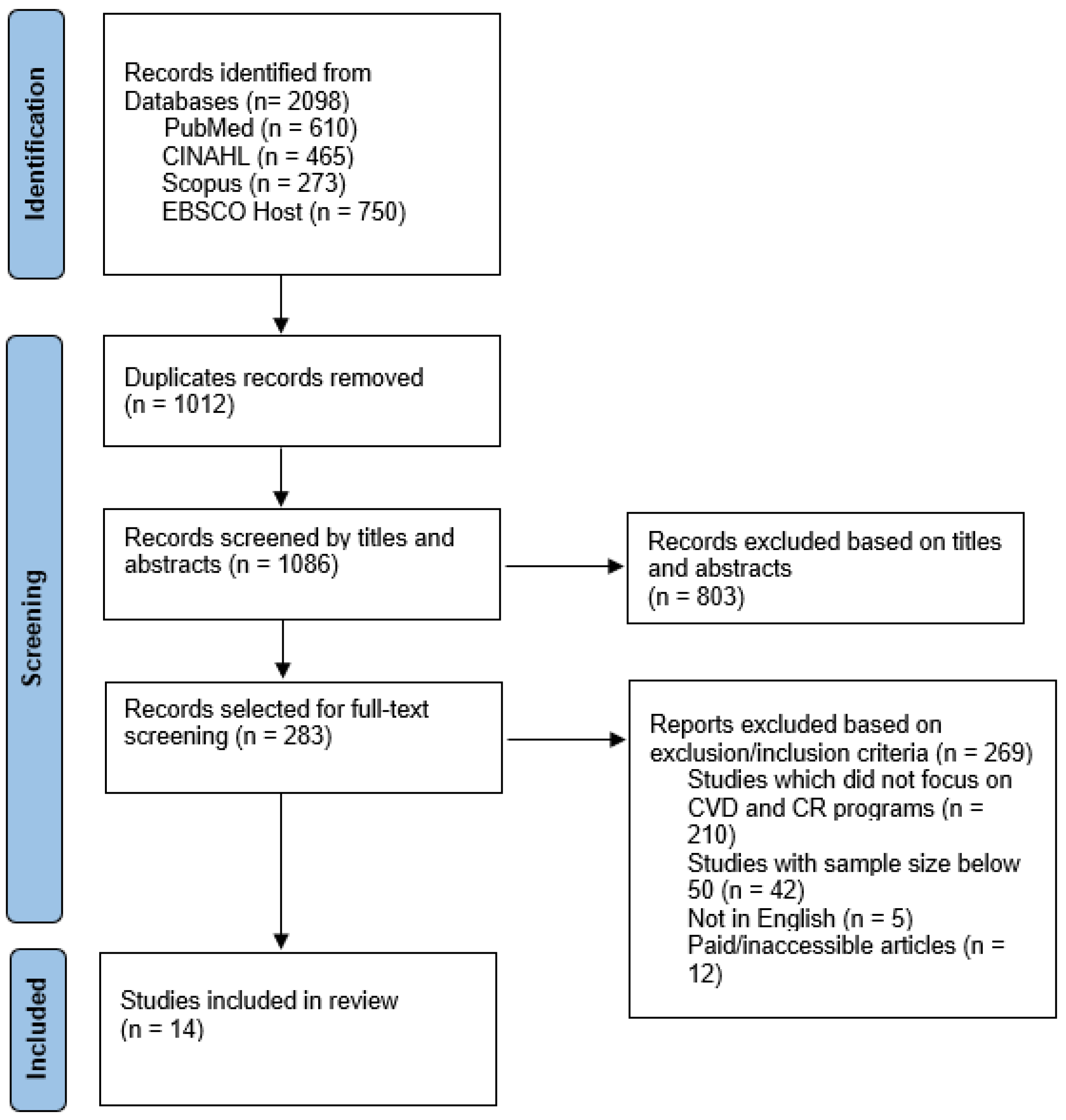

Table 1.
Characteristics of included studies.
| Study title | Author/year/ country | Design | Study subjects (n) | Barriers/Parameters |
|
Predictors of Early and Late Enrolment in Cardiac Rehabilitation, Among Those Referred, After Acute Myocardial Infarction |
(Parashar et al., 2012) USA |
Prospective cohort study | 1568 | demographic factors comorbidities Patient’s education level Cost of care |
|
Smoking and Cardiac Rehabilitation Participation: Associations with Referral, Attendance, and Adherence |
(Gaalema et al., 2015) USA |
Systematic review | 56 peer-reviewed articles | comorbidities |
|
Factors Associated with Utilization of Cardiac Rehabilitation Among Patients With Ischemic Heart Disease in the Veterans Health Administration |
(Schopfer et al., 2016) USA Qualitative study |
56 patients, providers, and CR program managers |
Lack of provider knowledge of the benefits and guidelines Inter-provider communication Cost-of care Travel/distance Lack of patient desire |
|
|
Association of Mental Health Conditions With Participation in Cardiac Rehabilitation |
(Krishnamurthi et al., 2019) USA Prospective cohort study |
86 537 patients | Comorbidities | |
|
Barriers for the Referral to Outpatient Cardiac Rehabilitation: A Predictive Model Including Actual and Perceived Risk Factors and Perceived Control |
(Soroush et al., 2018) Iran Cross-sectional study |
312 CABG patients | demographic factors employment status accessibility |
|
|
Factors associated with non-attendance at exercise-based cardiac rehabilitation Retrospective cohort study |
(Borg et al., 2019) Sweden |
31,297 | comorbidities employment status accessibility |
|
|
Association of Neighborhood Socioeconomic Context With Participation in Cardiac Rehabilitation Prospective cohort study |
(Bachmann et al., 2017) USA |
4096 | income educational status demographic factors comorbidities |
|
|
Effect of cardiac rehabilitation referral strategies on utilization rates Prospective cohort study |
( Grace et al., 2011) Canada |
1809 | Referral strategies | |
|
Cardiac Rehabilitation Availability and Density around the Globe Cross-sectional study |
(Turk-Adawi et al., 2019) Global |
98 countries | CR availability Referral strategy Mode of delivery |
|
|
Cardiac rehabilitation delivery in low/middle-income countries Cross-sectional study |
(Pesah et al., 2019) Global |
55 countries | Availability Core components of the program Cost of care |
|
|
Physician-Related Factors Affecting Cardiac Rehabilitation Referral Cross-sectional study |
(Moradi et al., 2011) Iran |
122 Cardiologists |
Physician’s knowledge about CR | |
|
Referral and participation in cardiac rehabilitation of patients following acute coronary syndrome; lessons learned Retrospective cohort study |
(Rodrigo et al., 2021) Netherland |
469 | Accessibility Comorbidities |
|
|
Predictors of Enrollment in Cardiac Rehabilitation Programs in Spain Retrospective cohort study |
( Chamosa et al., 2015) Spain |
756 | Demographic factors Comorbidities accessibility |
Table 2.
Results of included studies.
| Author/ Year | Themes | Results | Interpretation of significant findings |
| Healthcare system-related factors | |||
|
(Turk-Adawi et al., 2019) ( Pesah et al., 2019) |
Availability of CR programs |
CR was available in 111/203 countries. Availability by region shows significant difference (p < .001) 5753 programs globally (χ2 =37.3, p<0.001) |
CR is available in 54.7% of countries worldwide 80.7% of countries in Europe, to 17.0% in Africa Could serve 1,655,083 patients/year, despite an estimated 20,279,651 incident IHD cases globally/year CR is only available in 16.7% of LICs, 47.1% of MICs, and 86.2% in HICs There was one CR spot for every 66 IHD patients in LMICs (vs 3.4 in HICs) |
|
(Grace et al., 2011) (Turk-Adawi et al., 2019) |
Referral strategies |
(OR,3.27; CI, 1.52-7.04) (OR,3.35; CI, 1.54-7.29) (OR,8.41; CI, 3.57-19.85) (OR,1.36; CI, 1.35-1.38) |
Automatic referral strategy resulted in 70.2% referral rate and 60% of enrollment in CR Liason referral strategy resulted in 59% referral rate & 50 % enrollment Combined use of automatic & Liason strategies resulted in 85.8% referral rate & 73.5% enrollment Traditional referral strategy resulted in a 32.2% referral rate & 29% enrollment Systematic referral strategies resulted in 36% higher referral rates compared to traditional referral strategies. |
|
(Schopfer et al., 2016) (Moradi et al., 2011) |
Providers’/ physicians’ knowledge | 73% - CR providers 79.5% - cardiologists |
73% of CR providers perceived lack of knowledge regarding the benefits and guidelines causes fewer referral rates to CR 79.5% of cardiologists perceived low general knowledge about CR programs as the standard of care impact on referral to CR |
|
(Schopfer et al., 2016) |
Inter-provider communication | 18% - CR providers 17% - CR managers |
18% of CR managers and 17% of providers perceived poor communication between clinicians regarding patients' eligibility to CR resulted in fewer referrals |
| (Turk-Adawi et al., 2019) | Mode/setting of delivery | (OR = 1.05, 95%CI = 1.04–1.06) | CR programs offered individualized consultation with physicians reported high participation rates and residential programs reported higher patient compliance |
| Socioeconomic factors | |||
|
(Parashar et al., 2012) (Bachmann et al., 2017) (Soroush et al., 2018) |
Level of education |
1st month(OR, 1.38; 95% CI, 1.04–1.84) After 6 month (OR, 1.81; 95% CI, 1.42–2.30 Complete high school-(OR 1.20; 95% CI,0.92-1.58) Complete college- (OR 1.61, 95% CI, 1.06–2.44) Illiterate -7% Less than diploma-9% Academic -16% |
People who have at least high school education have 38% higher participation at 1st month and 81% after 6 months of AMI People who have completed college has 61% higher participation in CR compared to people who completed high school Higher referral rate(16%) for CR among people who complete academic education |
|
(Parashar et al., 2012) (Pesah et al., 2019) (Schopfer et al., 2016) |
Cost of care |
Uninsured(first month) (OR, 0.39; 95% CI, 0.21–0.71) After 6months insured vs uninsured p<0.001 Economic burden(first vs 6th months) (OR, 1.48; 95% CI, 0.97-2.26). Vs (OR, 0.56; 95% CI, 0.38–0.81) LMICs vs HICs Out-of-pocket(n=212, 65.0%) vs(n=184, 24.9%) 27% of participants perceived cost of care as a barrier |
Uninsured patients were 40% less likely to participate in the first month and no significance in insured vs uninsured at 6 months Patients with economic burden showed 48% of higher participation in the first month but 44% of less participation at 6 months High out-of-pocket expenditure was significantly associated with less participation and high dropout rates in LMICs compared to HICs. 27% perceived higher cost of CR program reduce participation |
|
(Soroush et al., 2018) (Borg et al., 2019) (Chamosa et al., 2015) (Bachmann et al., 2017) |
Employment status/income |
Employed 23% personal job 6.6% retired 12% unemployed 3.7% employed vs retired(OR 0.86;CI,0.80-0.93) self-employed(OR=1.56; 95% CI: 0.62-3.92) retired (OR = 1.33; 95% CI: 0.62-2.77). <$15,000 vs >$25,000 (OR 1.68, 95% CI, 1.17–2.42) |
unemployed, retired, or self-employed patients were less likely to be referred to CR than employed patients. Retired patients are 14% less likely to participate in CR Both self-employed(56%) and retired patients(33%) have higher enrollment Household income >$25,000/yr has 68% higher participation |
|
(Schopfer et al., 2016) (Soroush et al., 2018) (Rodrigo et al., 2021) (Borg et al., 2019) (Chamosa et al., 2015) (Bachmann et al., 2017) |
Accessibility to CR facilities |
68% respond to travel issues as a barrier Distance to CR e]center (p<0.042) <5km vs. > 20 km referral(OR 4.0; CI1.26–13.0) participation(OR 0.2, CI 0.07–0.79, (OR 1.75 [95% CI: 1.64–1.86] (OR = 2.87; 95% CI: 1.29-6.41) (OR 0.71, 95% CI, 0.59–0.84) |
The most perceived barrier to CR participation is long distance and transportation issues Larger distance was significantly associated with less referral Larger distance(>20km) to CR centers has 4 times higher referral rate but their participation in CR is significantly low Distance >16km increase the non-attendance by 75% Distance to CR unit >50km causes 3 folds more likely to CR non-enrollment Distance increase to CR centers from 3.8km to 25 km reduce the attendance by 29% |
| Individual characteristics | |||
|
(Parashar et al., 2012) (Chamosa et al., 2015) |
Age |
OR, 0.85 for each 10-year increment; 95% CI, 0.74–0.97 (OR = 1.05; 95% CI: 1.02-1.09). |
Older patients are 15% less likely to participate in CR Age was associated with no enrollment, with the chance of not enrolling increasing by 5% for every year of age |
|
(Parashar et al., 2012) (Borg et al., 2019) (Chamosa et al., 2015) |
Gender |
( OR, 0.61; 95% CI, 0.44, 0.86) (female vs male) OR, 0.85; 95% CI,0.80,0.90 Female vs male (20.8% vs 35.9%) Women with MI(OR, 6.35; CI, 2.53-11.81) |
Women 40% less likely to participate in CR Male were 15% less likely to participate Referral was less among women Women with MI has 35% higher non-participation |
|
(Parashar et al., 2012) (Borg et al., 2019) ( Krishnamurthi, Schopfer, Shen, & Whooley, 2019) ( Chamosa et al., 2015) (Gaalema et al., 2015) (Bachmann et al., 2017) |
Comorbidities |
hypertension (OR, 0.58; 95% CI, 0.43–0.78), PAD (OR, 0.43; 95% CI, 0.22–0.85), and previous PCI (OR, 0.55; 95% CI,0.36–0.83), Smokers (OR, 0.59; 95% CI,0.44–0.80) Diabetes (OR,1.20; 95% CI, 1.13-1.28) Hypertension (OR,0.94; 95%CI, 0.89-0.98) Smoking (OR, 1.63; 95% CI,1.54-1.74) (OR, 1.57; 95% CI, 1.43–1.74) (OR: 6.35; 95% CI: 2.53-11.81). (OR, 0.59; 95% CI, 0.44–0.80 (OR 0.65, 95% CI, 0.49–0.85,). |
Patients with a greater number of comorbidities were less likely to participate in CR non-attendance at CR was higher for individuals with a higher burden of comorbidities and for smokers Patients with both PTSD and depression had a 57% greater odds in participating in CR than those without depression or PTSD women with previous MI less likely to participate smokers were less likely to participate Smokers were 35% less likely to participate in CR programs |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



