
Submitted:
05 February 2024
Posted:
06 February 2024
You are already at the latest version
Abstract
Inflammation plays a key role in the induction of choroidal neovascularization (CNV). Inflammatory choroidal neovascularization (iCNV) is a severe but uncommon complication of both infectious and non-infectious uveitides. It is hypothesized that its pathogenesis is similar to that of wet age-related macular degeneration (AMD), and involves hypoxia as well as the release of vascular endothelial growth factor, stromal cell-derived factor 1-alpha, and other mediators. Inflammatory CNV develops when inflammation or infection directly involves the retinal pigment epithelium (RPE)–Bruch’s membrane complex. Inflammation itself can compromise perfusion, generating a gradient of retinal-choroidal hypoxia that additionally promotes the formation of choroidal neovascularization in the course of uveitis. The development of choroidal neovascularization is extremely common in conditions such as punctate inner choroidopathy, multifocal choroiditis, serpiginous choroiditis, and presumed ocular histoplasmosis syndrome. Although the majority of iCNV cases are well defined and appear as the “classic” type on fluorescein angiography, the diagnosis of iCNV is challenging due to difficulties in differentiating between inflammatory choroiditis lesions and choroidal neovascularization. Modern multimodal imaging, particularly the recently introduced technology of optical coherence tomography (OCT) and OCT angiography (noninvasive and rapid imaging modalities) can reveal additional features that aid the diagnosis of iCNV. However, more studies are needed to establish their role in the diagnosis and evaluation of iCNV activity. Keywords: uveitis; inflammatory choroidal neovascularization; multimodal imaging; fluorescein angiography; indocyanine green angiography; optical coherence tomography; optical coherence tomography angiography; near-infrared autofluorescence
Keywords:
inflammatory choroidal neovascularization
; multimodal imaging
; fluorescein angiography
; indocyanine green angiography
; optical coherence tomography
; optical coherence tomography angiography
; fundus autofluorescence
1. Introduction
Uveitis-related choroidal neovascularization (CNV), known as inflammatory CNV (iCNV), is an uncommon complication of uveitis. At the same time, it is one of the most severe causes of visual impairment in patients with uveitis [1,2,3]. Inflammatory CNV is the third cause of CNV following wet age-related macular degeneration (AMD) and pathological myopia [2,3]. Inflammatory CNV develops more frequently in patients with posterior uveitis (2.7%) and panuveitis (0.8%) as compared with those with anterior and intermediate uveitis (0.1%) [4]. CNV is a clinically important complication of both infectious and non-infectious uveitis and is found to be more frequent in some specific clinical entities. Its incidence in non-infectious posterior uveitis has been reported to reach 2% [5]. A higher incidence of CNV was reported in multifocal choroiditis, punctate inner choroidopathy, serpiginous choroidopathy, birdshot retinochoroidopathy, and Vogt–Koyanagi–Harada disease [6,7,8,9,10,11,12,13,14,15,16,17,18]. On the other hand, data on the incidence of iCNV secondary to infectious uveitis are scarce and are derived mainly from case series and case reports. The prevalence of iCNV depending on the etiology of uveitis is presented in Table 1.
According to Baxter et al. [4], the presence of epiretinal neovascularization is associated with an over three-fold higher risk of iCNV. Moreover, the risk of CNV was significantly greater in eyes with active inflammation vs those with inactive inflammation. The presence of anterior chamber cells grade 2+ as defined by the Standardization of Uveitis Nomenclature Working Group was shown to be associated with iCNV. However, increased vitreous cells and vitreous haze were not significantly associated with an altered risk of incident CNV in patients with uveitis [4]. Previous diagnosis of CNV in the contralateral eye was associated with a several-fold higher risk of CNV in the second eye. However, the eyes of patients with bilateral uveitis were less likely to develop CNV than affected eyes of patients with unilateral uveitis [4].
The underlying pathophysiology of iCNV is likely similar to the pathophysiology of CNV in other conditions associated with CNV, such as age-related macular degeneration (AMD) or pathologic myopia. Inflammatory CNV may thus be considered not as a distinct form of CNV, but rather as associated with a set of circumstances that permit their development [1,8].
It was demonstrated that vascular endothelial growth factor (VEGF) plays a key role in CNV development [2,3]. Moreover, CNV has an extravascular component consisting of fibroblasts and leukocytes that express C-X-C motif chemokine receptor 4 (CXCR4). Retinal pigment epithelial (RPE) cells showed an increased production of tumor necrosis factor as well as interleukins IL-1, IL-2, IL-6, and IL-10, accounting for the inflammatory component of CNV [47,48]. Also other mediators are involved in CNV development, such as nitric oxide, angiostatin, endostatin, C-C chemokine receptor type 3 (CCR3), and pigment epithelium-derived growth factor (PEDF) contrasting the neovascularization [49].
D’Ambrosio et al. [8] assessed the immunohistochemical staining grading of three structures of CNV, namely, the RPE, vascular network, and fibroblasts for SDF1, CXCR4, and VEGF receptor 2. The authors revealed differences in the CXCR4 staining of the vascular meshwork of iCNV as compared with AMD-related CNV, suggesting that capillaries have a different role in membrane development [8].
There are two pathophysiological mechanisms by which uveitis can promote the development of iCNV [2,47]. The first one is associated with inflammation-mediated damage of the RPE-Bruch’s membrane complex, which disrupts the outer blood-retinal barrier and permits neovascular upgrowth from the choroid. The damage can be induced by an angiogenic stimulus mediated by local inflammation, or it can result from the combination of both [2]. Activated inflammatory cells secrete enzymes that damage cells and cause degradation in the Bruch’s membrane. Proangiogenic cytokines released by these inflammatory cells may promote CNV growth through breaks in the membrane and into the sub-RPE space, potentially leading to edema, exudation, hemorrhages, and fibrosis, resulting in profound central vision loss [1,2]. Thus, a higher risk of damage of the RPE–Bruch’s membrane complex related with adjacent chorioretinal inflammation may explain the higher incidence of iCNV in patients with panuveitis and posterior uveitis [50]. It is noteworthy that the RPE is often intact in individuals with iCNV [2]. The proposed mechanism of iCNV development is thus the focal breach of the RPE due to infection or inflammation leading to the growth and entry of new vessels into the outer retinal space [50]. The second theory explains that retinal and choroidal inflammation directly compromises perfusion, generating a gradient of retinal-choroidal hypoxia that promotes the formation of choroidal neovascularization [2]. It should also be noted that in some cases “idiopathic” choroidal neovascularization may herald the subsequent development posterior uveitis [51].
Inflammatory CNV is typically diagnosed when a patient with uveitis reports a sudden deterioration of vision and/or metamorphopsias [2,3,4,52]. In advanced cases of iCNV, central scotoma may be present. Some of active extrafoveal lesions can be asymptomatic and may be detected only during an ophthalmological examination or on imaging studies alone [1,6,52,53].
In patients with posterior uveitis, the identification of iCNV is challenging due to related abnormalities including choroiditis as well as chorioretinal scarring and inflammatory lesions [52,53]. Difficulties in a differential diagnosis of iCNV and active inflammatory lesions arise from the characteristic presence of intraretinal or subretinal fluid as well as serous retinal detachment in both [1,8,52]. An accurate characterization of inflammatory lesions is important for the diagnosis of an underlying pathology and implementation of adequate treatment.
The aim of this paper was to discuss current multimodal imaging tools for the diagnosis of iCNV, with an emphasis on technological advances and future perspectives.
2. Imaging tools for the detection of iCNV
2.1. Fluorescein angiography
Fluorescein angiography (FA) has been widely employed in the diagnosis of CNV secondary to various ocular pathologies. Since iCNV is often a classic type of neovascular membrane (type 2), it can be visualized by FA. CNV lesions present on FA as early iso- or hyperfluorescence with late leakage [54].(Figure 1) Similarly, active inflammatory lesions show features of early isofluorescence (although mostly hypofluorescence) and late leakage, while inactive atrophic lesions are characterized by early hypo- or isofluorescence with late staining (suggesting RPE window defect) without leakage [4,55,56] (Figure 2) These highly similar FA features of iCNV and inflammatory lesions pose a diagnostic challenge. In conditions such as multifocal choroiditis, serpiginous choroiditis, or Vogt–Koyanagi–Harada disease, which present with scarring and pigmentation due to extensive retinal involvement, the detection of hyperfluorescence associated with CNV may be particularly difficult [52,53,57]. Thus, FA alone may be insufficient to identify inflammatory CNV lesions and initiate an appropriate therapy. Therefore, a multimodal approach with additional tests is recommended.
2.2. Indocyanine green angiography
One of the imaging techniques for the visualization of the choroid is indocyanine green angiography (ICGA), which allows a better visualization of the choroid compared with FA [58]. ICGA plays an important role in assessing pathologies involving the choroidal vasculature and choriocapillaris in chorioretinal inflammatory diseases. It is helpful in differentation between iCNV and inflammatory lesions [59,60]. ICGA allows to tell the difference between a recurrent inflammatory focus and CNV: the former appears as an early hypofluorescent lesion, whereas the latter as a hyperfluorescent lesion since early angiographic frames [58,59]. ICGA is also mandatory in the case of CNV associated with choriocapillaritis such as multifocal choroiditis, where it shows the extent of occult choriocapillaris nonperfusion and hence the risk for CNV development [60,61]. Importantly, ICGA was shown to outperform FA in detecting occult CNV lesions [54]. While iCNV is typically a classic lesion that can be easily visualized by FA, ICGA has been recently reported to be more accurate in assessing the size of neovascular lesions, especially in patients with idiopathic CNV, which shares several clinical features with iCNV [62]. Thus, ICG helps identify both iCNV and inflammatory choroidal alterations in patients with uveitis, allowing a clinical differentiation between these lesions and a more comprehensive evaluation of the disease [60] (Figure 3 and Figure 4).
2.3. Optical coherence tomography
Optical coherence tomography (OCT) is a noninvasive and highly repeatable imaging technique that has revolutionized the management of retinal and choroidal diseases. By providing the quasi-histological sections of the ocular structure , it allows clinicians to identify ocular pathologies and assess response to treatment [63]. Moreover, the enhanced depth imaging modality of OCT can be used to evaluate choroidal thickness and structural modifications, which is particularly valuable in the treatment of uveitis [63].
Inflammatory CNV usually develops between the RPE and neurosensory retina, demonstrating similar features on OCT imaging as classic (type 2) CNV [58]. In both cases, the lesions appear as hyperreflective structures located in front of a disrupted RPE, with solid tissue in the subretinal space [1,64,65,66]. However, there is a single OCT feature that can help distinguish between iCNV and other classic CNVs. This is the so called “pitchfork sign”, characterized by finger-like hyperreflective lesions extending from the CNV into the outer retinal layers, and it allows to differentiate iCNV from other causes of CNV [1,53,67]. It was reported that the OCT features of CNV activity such as retinal thickening, subretinal and intraretinal fluid, intraretinal hyperreflective flecks, and undefined boundaries of subretinal material (Figure 5a) predicted the presence of FA leakage [1,66]. Thus, it was concluded that OCT can be used for monitoring disease progression and response to treatment [68,69].
Moreover, central retinal thickness evaluated by OCT is often used as an objective measure of iCNV activity [70,71,72]. Recently, Giuffrè et al. [73] demonstarted increased choroidal thickness under iCNV that decreases after therapy: the so called “sponge sign”. Thus OCT-based choroidal thickness evaluation may represent an additional useful tool to monitor inflammatory choroidal neovascularization activity. Moreover, choroidal thickness under CNV could be used to discriminate the origin of choroidal neovascular membrane in doubtful cases (either inflammatory or myopic) and to guide therapeutic management [73].
OCT images can also help differentiate between iCNV lesions and nonneovascular alterations at the RPE level that are characteristic for several types of uveitis. For example, acute inflammatory foci in multifocal choroiditis show a deeper penetration of the OCT signal, a feature that is usually not seen in iCNV [56,65]. However, when distinguishing CNV lesions from iCNV, the use of OCT alone may be limited as these lesions display similar features of outer retinal or RPE hyperreflectivity, intraretinal edema, sub-RPE fluid, and exudation in conditions with the involvment of the RPE or choriocapillaris (e.g., multifocal choroiditis and punctate inner choroidopathy) [1,71,72,74,75]. In such cases, the characteristics of the lesions can be determined by a combination of FA, ICGA, and OCT angiography (OCTA).
2.4. Optical coherence tomography angiography
The usefulness of OCTA as a noninvasive technique for the detection of iCNV has been reported by several investigators. Cheng et al [76] assessed the ability of OCTA to detect iCNV and differentiate it from inflammatory lesions as compared with conventional FA in 26 patients with multifocal choroiditis. The authors concluded that OCTA outperformed FA in differentiating CNV from inflammatory lesions as the latter do not show any blood flow signals. It also permitted the visualization of detailed vascular structure of CNV. Therefore, it could be used as an alternative option for CNV identification and to guide therapeutic decision making [74]. Similarly, in a recent retrospective study of 14 patients, Zahid et al. [77] used OCTA to evaluate neovascular flow signals in macular chorioretinal lesions occurring in idiopathic multifocal choroiditis. They concluded that OCTA may be a useful tool for understanding the pathophysiology of the disease and monitoring disease course. The utility of OCTA for the noninvasive diagnosis of iCNV and its subsequent follow-up was also confirmed by Yee et al. [78]. Finally, in a recent study, Aggarwal et al. [79] investigated OCTA features of tuberculosis-associated choroiditis in comparison with conventional imaging modalities including FA, ICGA, and OCTA. This was the first study to demonstrate that OCTA can identify type 1 neovascular networks. The research led to a conclusion that OCTA is indispensable to exclude neovascular networks when FA, ICGA, and OCT results are inconclusive [78] (Figure 5c, Figure 6b and Figure 7c).
In patients with posterior uveitis, the identification of iCNV is challenging due to related abnormalities including associated pathologies such as choroiditis, chorioretinal lesions, and choroidal scarring [1,79,80]. In such cases, OCTA provides objective evidence of CNV lesions because it has an advantage of differentiating iCNV lesions from inflammatory lesions as these do not show any neovascular flow signals [80]. Thus, OCTA allows noninvasive diagnostic imaging of iCNV and differantation from inflammatory pathologies [1,79,80].
While the above studies prove the role for OCTA in the diagnosis and follow-up of patients with iCNV, larger prospective studies are needed to determine its advantages over conventional imaging.
2.5. Near-infrared autofluorescence imaging
Fundus autofluorescence (FAF) is a valuable imaging tool for multiple anatomical and physiological alterations in the ocular tissue [81]. Essentially, FAF is a map of lipofuscin distribution, which is the autofluorescent pigment of the eye naturally found in the RPE–photoreceptor complex [81]. It was reported that iCNV lesions may show a different pattern on FAF imaging than active inflammatory foci [1,81,82]. In FAF, normal autofluorescence may occur in active iCNV with preserved neurosensory retina [1,80,81,82,83]. Prolonged active CNV tends to present hyperautofluorescence, while hypoautofluorescent areas correlate with photoreceptor and RPE loss [1,80,83] (Figure 1a and Figure 7b). Active inflammatory foci may show increased autofluorescence signal [81,82] (Figure 3a). Therefore, the technique may be used for differentiating between inflammatory and CNV lesions.
3. Conclusions
The detection of inflammatory CNV remains a challenge due to the presence of choroiditis lesions, scarring, and pigmentation that make it difficult to visualize CNV lesions. Available case reports and case series point to the benefits of using OCTA in combination with conventional imaging modalities such as FA, OCT, and ICGA. This multimodal approach may improve the detection and follow-up of iCNV lesions. OCTA is also an important addition to FA and ICGA in terms of providing important information on retinochoroidal abnormalities associated with uveitis: the severity of inflammation or the presence of any vascular changes and focal lesions. It may offer advantages over traditional modalities in the detection of neovascular flow in uveitis, but it should be used as an additional tool rather than a replacement of the existing ones. Also FAF requires further research to reveal whether this imaging modality can be used to differentiate between iCNV and inflammatory lesions and between AMD-related CNV and CNV related to inflammatory disease.
Author Contributions
Conceptualization, A.K.-T.; investigation, A.K.-T., I.K.-B. and W.P.-M.; data curation, K.Ż-Ł, A.M., M.C. and W.P.-M, writing—original draft preparation, A.K.-T, I.K.-B., and A.M.; writing—review and editing, A.K.-T., I.K.-B. and B.R.-D.; visualization, W.P.-M., M.C. and K.Ż.-Ł; supervision, A.K.-T and B.R.-D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
All procedures were carried out in accordance with guidelines set forth by the Declaration of Helsinki.
Informed Consent Statement
The patients signed an institutional informed consent for the use of medical records and the publication of this information for research purposes.
Data Availability Statement
Data supporting the findings of this study are available upon request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Agarwal, A.; Invernizzi, A.; Singh, R.B.; Foulsham, W.; Aggarwal, K.; Handa, S; Agrawal, R.; Pavesio., C.; Gupta, V. An update on inflammatory choroidal neovascularization: epidemiology, multimodal imaging, and management. J. Ophthalmic Inflamm. Infect. 2018, 8, 13. [Google Scholar] [CrossRef]
- Dhingra, N.; Kelly, S.; Majid, M.A.; Bailey, C.B.; Dick, A.D. Inflammatory choroidal neovascular membrane in posterior uveitis-pathogenesis and treatment. Indian J. Ophthalmol. 2010, 58, 3–10. [Google Scholar] [CrossRef]
- Neri, P.; Lettieri, M.; Fortuna, C.; Manoni, M.; Giovannini, A. Inflammatory choroidal neovascularization. Middle East Afr J Ophthalmol. 2009, 16, 245–251. [Google Scholar] [CrossRef]
- Baxter, S.L.; Pistilli, M.; Pujari, S.S.; Liesegang, T.L.; Suhler, E.B.; Thorne, J.E.; Foster, C.S.; Jabs, D.A.; Levy-Clarke, G.A.; Nussenblatt, R.B.; Rosenbaum, J.T.; Kempen, J.H. Risk of choroidal neovascularization among the uveitides. Am. J. Ophthalmol. 2013, 156, 468–477. [Google Scholar] [CrossRef] [PubMed]
- Dreyer, R.F.; Gass, D.J. Multifocal choroiditis and panuveitis. A syndrome that mimics ocular histoplasmosis. Arch. Ophthalmol. 1984, 102, 1776–1784. [Google Scholar] [CrossRef]
- Morgan, C.M.; Schatz, H. Recurrent Multifocal Choroiditis. Ophthalmology. 1986, 93, 1138–1147. [Google Scholar] [CrossRef]
- Brown, J., Jr.; Folk, J.C.; Reddy, C.V.; Kimura, A.E. Visual prognosis of multifocal choroiditis, punctate inner choroidopathy, and the diffuse subretinal fibrosis syndrome. Ophthalmology. 1996, 103, 1100–1105. [Google Scholar] [CrossRef]
- Ahnood, D.; Madhusudhan, S.; Tsaloumas, M.D.; Waheed, N.K.; Keane, P.A.; Denniston, A.K. Punctate inner choroidopathy: A review. Surv Ophthalmol. 2017, 62, 113–126. [Google Scholar] [CrossRef]
- Kuo, I.C.; Cunningham, E.T., Jr. Ocular neovascularization in patients with uveitis. Int. Ophthalmol. Clin. 2000, 40, 111–126. [Google Scholar] [CrossRef]
- Saatci, A.O.; Ayhan, Z.; Engin Durmaz, C.; Takes, O. Simultaneous Single Dexamethasone Implant and Ranibizumab Injection in a Case with Active Serpiginous Choroiditis and Choroidal Neovascular Membrane. Case Rep. Ophthalmol. 2015, 6, 408–414. [Google Scholar] [CrossRef]
- Kępka, M.; Brydak-Godowska, J.; Ciszewska, J.; Turczyńska, M.; Ciszek, M.; Kęcik, D. Clinical features, diagnosis and management of serpiginuos choroiditis. Ophthalmol. J. 2022, 7, 127–135. [Google Scholar] [CrossRef]
- Rao, N.A.; Gupta, A.; Dustin, L.; Chee, S.P.; Okada, A.A.; Khairallah, M.; Bodaghi, B.; Lehoang, P.; Accorinti, M.; Mochizuki, M.; Prabriputaloong, T.; Read, R.W. Frequency of distinguishing clinical features in Vogt Koyanagi-Harada disease. Ophthalmology. 2010, 117, 591–599. [Google Scholar] [CrossRef] [PubMed]
- Brucker, A.J.; Deglin, E.A.; Bene, C.; Hoffman, M.E. Subretinal Choroidal Neovascularization in Birdshot Retinochoroidopathy. Am. J. Ophthalmol. 1985, 99, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Mehta, S.; Hariharan, L.; Ho, A.C.; Kempen, J.H. Peripapillary choroidal neovascularization in pars planitis. J. Ophthalmic Inflamm. Infect. 2013, 3, 13. [Google Scholar] [CrossRef] [PubMed]
- Nageeb, M.R. Intermediate Uveitis Complicated by Peripapillary Choroidal Neovascularization. Cureus. 2022, 14, e31040. [Google Scholar] [CrossRef] [PubMed]
- Inagaki, M.; Harada, T.; Kiribuchi, T.; Ohashi, T.; Majima, J. Subfoveal choroidal neovascularization in uveitis. Ophthalmologica. 1996, 210, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Pagliarini, S.; Piguet, B.; Ffytche, T.J.; Bird, A.C. Foveal involvement and lack of visual recovery in APMPPE associated with uncommon features. Eye (Lond). 1995, 9, 42–47. [Google Scholar] [CrossRef]
- Bowie, E.M.; Sletten, K.R.; Kayser, D.L.; Folk, J.C.; James, C. Acute Posterior Multifocal Placoid Pigment Epitheliopathy And Choroidal Neovascularization. Retina 2005, 25, 362–364. [Google Scholar] [CrossRef]
- Saatci, A.O.; Ayhan, Z.; Ipek, S.C.; Soylev Bajin, M. Intravitreal Aflibercept as an Adjunct to Systemic Therapy in a Case of Choroidal Neovascular Membrane Associated with Sympathetic Ophthalmia. Turk. J. Ophthalmol. 2018, 48, 209–211. [Google Scholar] [CrossRef]
- Rouvas, A.A.; Ladas, I.D.; Papakostas, T.D.; Moschos, M.M.; Vergados, I. Intravitreal ranibizumab in a patient with choroidal neovascularization secondary to multiple evanescent white dot syndrome. Eur. J. Ophthalmol. 2007, 17, 996–999. [Google Scholar] [CrossRef]
- Burova, M.; Stepanov, A.; Almesmary, B.; Jiraskova, N. Choroidal neovascularization in a patient after resolution of multiple evanescent white dot syndrome: A case report. Clin Case Rep 2022, 10, e05802. [Google Scholar] [CrossRef]
- Liu, T.Y.A.; Zhang, A.Y.; Wenick, A. Evolution of Choroidal Neovascularization due to Presumed Ocular Histoplasmosis Syndrome on Multimodal Imaging including Optical Coherence Tomography Angiography. Case Rep. Ophthalmol. Med. 2018, 13, 2018:4098419. [Google Scholar] [CrossRef]
- Hu, J.; Hoang, Q.V.; Chau, F.Y.; Blair, M.P.; Lim, J.I. Intravitreal anti-vascular endothelial growth factor for choroidal neovascularization in ocular histoplasmosis. Retin. Cases Brief Rep. 2014, 8, 24–29. [Google Scholar] [CrossRef]
- Nielsen, J.S.; Fick, T.A.; Saggau, D.D.; Barnes, C.H. Intravitreal anti-vascular endothelial growth factor therapy for choroidal neovascularization secondary to ocular histoplasmosis syndrome. Retina 2012, 32, 468–472. [Google Scholar] [CrossRef]
- Walia, H.S.; Shah, G.K.; Blinder, K.J. Treatment of CNV secondary to presumed ocular histoplasmosis with intravitreal aflibercept 2.0 mg injection. Can. J. Ophthalmol. 2016, 51, 91–96. [Google Scholar] [CrossRef]
- Zonnevylle, K.E.; Stanescu-Segall, D. Intravitreal Bevacizumab for Treatment of Bilateral Candida Chorioretinitis Complicated with Choroidal Neovascularization. Ocul. Immunol. Inflamm. 2020, 28, 39–42. [Google Scholar] [CrossRef]
- Jampol, L.M.; Sung, J.; Walker, J.D.; Folk, J.C.; Townsend-Pico, W.A.; Lowder, C.Y.; Dodds, E.M.; Westrich, D.; Terry, J. Choroidal neovascularization secondary to Candida albicans chorioretinitis. Am. J. Ophthalmol. 1996, 121, 643–649. [Google Scholar] [CrossRef]
- Makragiannis, G.; Vahdani, K.; Carreño, E.; Lee, R.W.J.; Dick, A.D.; Ross, A.H. Bevacizumab for treatment of choroidal neovascularization secondary to candida chorioretinitis. Int. Ophthalmol. 2018, 38, 781–785. [Google Scholar] [CrossRef]
- Fine, S.L.; Owens, S.L.; Haller, J.A.; Knox, D.L.; Patz, A. Choroidal neovascularization as a late complication of ocular toxoplasmosis. Am. J. Ophthalmol. 1981, 91, 318–322. [Google Scholar] [CrossRef]
- Willerson, D.; Aaberg, T.M.; Reeser, F.; Meredith, T.A. Unusual ocular presentation of acute toxoplasmosis. Br. J. Ophthalmol. 1977, 61, 693–698. [Google Scholar] [CrossRef]
- Benevento, J.D.; Jager, R.D.; Noble, A.G.; Latkany, P.; Mieler, W.F.; Sautter, M.; Meyers, S.; Mets, M.; Grassi, M.A.; Rabiah, P.; Boyer, K.; Swisher, C.; McLeod, R. Toxoplasmosis Study Group. Toxoplasmosis-associated neovascular lesions treated successfully with ranibizumab and antiparasitic therapy. Arch. Ophthalmol. 2008, 126, 1152–1156. [Google Scholar] [CrossRef]
- Sienicka, P. Eye toxoplasmosis complicated by choroidal neovascularization effectively treated with the anti-vascular endothelial growth factor aflibercept. Klin. Oczna 2022, 124, 114–119. [Google Scholar] [CrossRef]
- Lampariello, D.A.; Primo, S.A. Ocular toxocariasis: a rare presentation of a posterior pole granuloma with an associated choroidal neovascular membrane. J. Am. Optom. Assoc. 1999, 70, 245–252. [Google Scholar]
- Lyall, D.; Hutchison, B.; Gaskell, A.; Varikkara, M. Intravitreal Ranibizumab in the treatment of choroidal neovascularisation secondary to ocular toxocariasis in a 13-year-old boy. Eye 2010, 24, 1730–1731. [Google Scholar] [CrossRef]
- Yoon, D.Y.; Woo, S.J. Intravitreal Administration of Ranibizumab and Bevacizumab for Choroidal Neovascularization Secondary to Ocular Toxocariasis: A Case Report, Ocular Immunol. Inflamm. 2018, 26, 639–641. [Google Scholar] [CrossRef] [PubMed]
- Chung, Y.M.; Yeh, T.S.; Sheu, S.J.; Liu, J.H. Macular subretinal neovascularization in choroidal tuberculosis. Ann. Ophthalmol. 1989, 21, 225–229. [Google Scholar] [PubMed]
- Lee Kim, E.; Rodger, D.C.; Rao, N.A. Choroidal neovascularization secondary to tuberculosis: Presentation and management. Am. J. Ophthalmol. Case Rep. 2017, 6, 124–129. [Google Scholar] [CrossRef]
- Zhang, Y.K.; Fu, H.Y.; Guan, Y.; Li, Y.J.; Bai, H.Z. Concurrent tuberculous chorioretinitis with choroidal neovascularization and tuberculous meningitis: a case report. BMC Ophthalmol 2020, 20, 227. [Google Scholar] [CrossRef]
- Interlandi, E.; Pellegrini, F.; Pavesio, C.; De Luca, M.; De Marco, R.; Papayannis, A.; Mandarà, E.; Cuna, A.; Cirone, D.; Ciabattoni, C.; Liberali, T.; Zappacosta, A.; Latanza, L. Intraocular Tuberculosis: A Challenging Case Mimicking Wet Age-Related Macular Degeneration. Case Rep. Ophthalmol. 2021, 12, 519–524. [Google Scholar] [CrossRef]
- Deutman, A.F.; Grizzard, W.S. Rubella retinopathy and subretinal neovascularization. Am J Ophthalmol. 1978, 85, 82–87. [Google Scholar] [CrossRef]
- Parodi, M.B.; Romano, F.; Montagna, M.; Bandello, F. Large choroidal excavation in a patient with rubella retinopathy. Eur. J. Ophthalmol. 2018, 28, 251–252. [Google Scholar] [CrossRef]
- Dewan, L.; Hasan, N.; Aron, N.; Chawla, R.; Sundar, D. Rubella retinopathy with choroidal neovascular membrane in a 7-year-old. Indian J. Ophthalmol. 2020, 68, 1176–1177. [Google Scholar] [CrossRef]
- Hirano, K.; Tanikawa, A.; Miyake, Y. Neovascular maculopathy associated with rubella retinopathy. Jpn. J. Ophthalmol. 2000, 44, 697. [Google Scholar] [CrossRef]
- Khairallah, M.; Ben Yahia, S.; Attia, S.; Jelliti, B.; Zaouali, S.; Ladjimi, A. Severe ischemic maculopathy in a patient with West Nile virus infection. Ophthalmic Surg Lasers Imaging 2006, 37, 240–242. [Google Scholar] [CrossRef] [PubMed]
- Seth, R.K.; Stoessel, K.M.; Adelman, R.A. Choroidal neovascularization associated with West Nile virus chorioretinitis. Semin. Ophthalmol. 2007, 22, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Zito, R.; Micelli Ferrari, T.; Di Pilato, L.; Lorusso, M.; Ferretta, A.; Ferrari, L.M.; Accorinti, M. Clinical course of choroidal neovascular membrane in West Nile virus chorioretinitis: a case report. J. Med. Case Reports 2021, 15, 206. [Google Scholar] [CrossRef] [PubMed]
- Campa, C.; Costagliola, C.; Incorvaia, C.; Sheridan, C.; Semeraro, F.; De Nadai, K.; Sebastiani, A.; Parmeggiani, F. Inflammatory mediators and angiogenic factors in choroidal neovascularization: pathogenetic interactions and therapeutic implications. Mediators Inflamm. 2010, 2010, 546826. [Google Scholar] [CrossRef]
- D'Ambrosio, E.; Tortorella, P.; Iannetti, L. Management of uveitis-related choroidal neovascularization: from the pathogenesis to the therapy. J. Ophthalmol. 2014, 2014, 450428. [Google Scholar] [CrossRef] [PubMed]
- Cerquaglia, A.; Fardeau, C.; Cagini, C.; Fiore, T.; LeHoang, P. Inflammatory Choroidal Neovascularization: Beyond the Intravitreal Approach. Ocul. Immunol. Inflamm. 2018, 26, 1047–1052. [Google Scholar] [CrossRef]
- Sato, K.; Takeda, A.; Hasegawa, E.; Jo, Y.; Arima, M.; Oshima, Y.; Ryoji, Y.; Nakazawa, T.; Yuzawa, M.; Nakashizuka, H.; Shimada, H.; Kimura, K.; Ishibashi, T.; Sonoda, K.H. Interleukin-6 plays a crucial role in the development of subretinal fibrosis in a mouse model. Immunol. Medicine 2018, 41, 23–29. [Google Scholar] [CrossRef]
- Tatar, O.; Adam, A.; Shinoda, K.; Stalmans, P.; Eckardt, C.; Lüke, M.; Bartz-Schmidt, K.U.; Grisanti, S. Expression of VEGF and PEDF in Choroidal Neovascular Membranes Following Verteporfin Photodynamic Therapy. Am. J. Ophthalmol. 2006, 142, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, E.T. Jr; Pichi, F.; Dolz-Marco, R.; Freund, K.B.; Zierhut, M. Inflammatory Choroidal Neovascularization. Ocular Immunol. Inflamm. 2020, 28, 2–6. [Google Scholar] [CrossRef]
- Bou Ghanem, G.; Neri, P.; Dolz-Marco, R.; Albini, T.; Fawzi, A. Review for Diagnostics of the Year: Inflammatory Choroidal Neovascularization - Imaging Update. Ocul. Immunol. Inflamm. 2023, 31, 819–825. [Google Scholar] [CrossRef] [PubMed]
- Machida, S.; Fujiwara, T.; Murai, K.; Kubo, M.; Kurosaka, D. Idiopathic choroidal neovascularization as an early manifestation of inflammatory chorioretinal diseases. Retina 2008, 28, 703–710. [Google Scholar] [CrossRef]
- Bansal, R.; Bansal, P.; Gupta, A.; Gupta, V.; Dogra, M.R.; Singh, R.; Katoch, D. Diagnostic challenges in inflammatory choroidal neovascular membranes. Ocul. Immunol. Inflamm. 2017, 25, 554–562. [Google Scholar] [CrossRef]
- Atmaca, L.S.; Batioğlu, F.; Atmaca, P. Evaluation of choroidal neovascularization in age-related macular degeneration with fluorescein and indocyanine green videoangiography. Ophthalmologica 1996, 210, 148–151. [Google Scholar] [CrossRef]
- Kotsolis, A.I.; Killian, F.A.; Ladas, I.D.; Yannuzzi, L.A. Fluorescein angiography and optical coherence tomography concordance for choroidal neovascularisation in multifocal choroidtis. Br. J. Ophthalmol. 2010, 94, 1506–1508. [Google Scholar] [CrossRef] [PubMed]
- Spaide, R.F.; Goldberg, N.; Freund, K.B. Redefining multifocal choroiditis and panuveitis and punctate inner choroidopathy through multimodal imaging. Retina (Philadelphia, Pa) 2013, 33, 1315–1324. [Google Scholar] [CrossRef]
- Perentes, Y.; Van Tran, T.; Sickenberg, M.; Herbort, C.P. Subretinal neovascular membranes complicating uveitis: frequency, treatments, and visual outcome. Ocul. Immunol. Inflamm. 2005, 13, 219–224. [Google Scholar] [CrossRef]
- Bischoff, P.M.; Flower, R.W. Ten years’ experience with choroidal angiography using indocyanine green dye: a new routine examination or an epilogue? Doc. Ophthalmol. 1985, 60, 235–291. [Google Scholar] [CrossRef]
- Agrawal, R.V.; Biswas, J.; Gunasekaran, D. Indocyanine green angiography in posterior uveitis. Indian J. Ophthalmol. 2013, 61, 148–159. [Google Scholar] [CrossRef] [PubMed]
- Herbort, C.P. Fluorescein and indocyanine green angiography for uveitis. Middle East Afr. J. Ophthalmol. 2009, 16, 168–187. [Google Scholar] [CrossRef] [PubMed]
- Sulzbacher, F.; Kiss, C.; Munk, M.; Deak, G.; Sacu, S.; Schmidt-Erfurth, U. Diagnostic evaluation of type 2 (classic) choroidal neovascularization: optical coherence tomography, indocyanine green angiography, and fluorescein angiography. Am. J. Ophthalmol. 2011, 152, 799–806.e1. [Google Scholar] [CrossRef]
- Rush, R.B.; Rush, S.W. Evaluation of idiopathic choroidal neovascularization with indocyanine green angiography in patients undergoing bevacizumab therapy. J. Ophthalmol. 2015, 642624. [Google Scholar] [CrossRef]
- Mrejen, S.; Spaide, R.F. Optical coherence tomography: imaging of the choroid and beyond. Surv. Ophthalmol. 2013, 58, 387–429. [Google Scholar] [CrossRef]
- Amer, R.; Priel, E.; Kramer, M. Spectral-domain optical coherence tomographic features of choroidal neovascular membranes in multifocal choroiditis and punctate inner choroidopathy. Graefes Arch. Clin. Exp. Ophthalmol. 2015, 253, 949–957. [Google Scholar] [CrossRef]
- Giani, A.; Luiselli, C.; Esmaili, D.D.; Salvetti, P.; Cigada, M.; Miller, J.W.; Staurenghi, G. Spectral-domain optical coherence tomography as an indicator of fluorescein angiography leakage from choroidal neovascularization. Invest. Ophthalmol. Vis. Sci. 2011, 52, 5579–5586. [Google Scholar] [CrossRef]
- Gao, R.; Ma, J.; Zhang, Z.; Shang, Q.; Duan, J. Spectral domain-optical coherence tomography retinal biomarkers in choroidal neovascularization of multifocal choroiditis, myopic choroidal neovascularization, and idiopathic choroidal neovascularization. Ann. Med. 2021, 53, 1270–1278. [Google Scholar] [CrossRef]
- Roy, R.; Saurabh, K.; Bansal, A.; Kumar, A.; Majumdar, A.K.; Paul, S.S. Inflammatory choroidal neovascularization in Indian eyes: etiology, clinical features, and outcomes to anti-vascular endothelial growth factor. Indian J. Ophthalmol. 2017, 65, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Mansour, A.M.; Mackensen, F.; Arevalo, J.F.; Ziemssen, F.; Mahendradas, P.; Mehio-Sibai, A.; Hrisomalos, N.; Lai, T.Y.; Dodwell, D.; Chan, W.M.; Ness, T.; Banker, A.S.; Pai, S.A.; Berrocal, M.H.; Tohme, R.; Heiligenhaus, A.; Bashshur, Z.F.; Khairallah, M.; Salem, K.M.; Hrisomalos, F.N.; Wood, M.H.; Heriot, W.; Adan, A.; Kumar, A.; Lim, L.; Hall, A.; Becker, M. Intravitreal bevacizumab in inflammatory ocular neovascularization. Am. J. Ophthalmol. 2008, 146, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Karti, O.; Ipek, S.C.; Ates, Y.; Saatci, A.O. Inflammatory Choroidal Neovascular Membranes in Patients With Noninfectious Uveitis: The Place of Intravitreal Anti-VEGF Therapy. Med. Hypothesis Discov. Innov. Ophthalmol. 2020, 9, 118–126. [Google Scholar] [PubMed]
- Mansour, A.M.; Arevalo, J.F.; Ziemssen, F.; et al. Long-term visual outcomes of intravitreal bevacizumab in inflammatory ocular neovascularization. Am. J. Ophthalmol. 2009, 148, 310–316.e2. [Google Scholar] [CrossRef]
- Giuffrè, C.; Marchese, A.; Fogliato, G.; Miserocchi, E.; Modorati, G.M.; Sacconi, R.; Cicinelli, M.V.; Miere, A.; Amoroso, F.; Capuano, V.; Souied, E.; Bandello, F.; Querques, G. The "Sponge sign": A novel feature of inflammatory choroidal neovascularization. Eur. J. Ophthalmol. 2021, 31, 1240–1247. [Google Scholar] [CrossRef]
- Invernizzi, A.; Pichi, F.; Symes, R.; Zagora, S.; Agarwal, A.K.; Nguyen, P.; Erba, S.; Xhepa, A.; De Simone, L.; Cimino, L.; Gillies, M.C.; McCluskey, P.J. Twenty-four-month outcomes of inflammatory choroidal neovascularisation treated with intravitreal anti vascular endothelial growth factors: a comparison between two treatment regimens. Br. J. Ophthalmol. 2020, 104, 1052–1056. [Google Scholar] [CrossRef] [PubMed]
- Wu, K.; Zhang, X.; Su, Y.; Ji, Y.; Zuo, C.; et al. Clinical characteristics of inflammatory choroidal neovascularization in a Chinese population. Ocul. Immunol. Inflamm. 2016, 24, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.; Chen, X.; Weng, S.; Mao, L.; Gong, Y.; Yu, S.; Xu, X. Spectral-domain optical coherence tomography angiography findings in multifocal choroiditis with active lesions. Am. J. Ophthalmol. 2016, 169, 145–161. [Google Scholar] [CrossRef]
- Zahid, S.; Chen, K.C.; Jung, J.J.; Balaratnasingam, C.; Ghadiali, Q.; Sorenson, J.; Rofagha, S.; Freund, K.B.; Yannuzzi, L.A. Optical coherence tomography angiography of chorioretinal lesions due to idiopathic multifocal choroiditis. Retina (Philadelphia, Pa) 2017, 37, 1451–1463. [Google Scholar] [CrossRef]
- Yee, H.Y.; Keane, P.A.; Ho, S.L.; Agrawal, R. Optical coherence tomography angiography of choroidal neovascularization associated with tuberculous serpiginous-like choroiditis. Ocul. Immunol. Inflamm. 2016, 24, 699–701. [Google Scholar] [CrossRef]
- Aggarwal, K.; Agarwal, A.; Sharma, A.; Sharma, K.; Gupta, V. OCTA Study Group. Detection Of Type 1 Choroidal Neovascular Membranes Using Optical Coherence Tomography Angiography In Tubercular Posterior Uveitis. Retina 2019, 39, 1595–1606. [Google Scholar] [CrossRef]
- Astroz, P.; Miere, A.; Mrejen, S.; Sekfali, R.; Souied, E.H.; Jung, C.; Nghiem-Buffet, S.; Cohen, S.Y. Optical coherence tomography angiography to distinguish choroidal neovascularization from macular inflammatory lesionns in multifocal choroiditis. Retina (Philadelphia, Pa) 2018, 38, 299–309. [Google Scholar] [CrossRef]
- Theelen, T.; Berendschot, T.T.J.M.; Hoyng, C.B.; Boon, C.J.F.; Klevering, B.J. Near-infrared reflectance imaging of neovascular age-related macular degeneration. Graefes Arch. Clin. Exp. Ophthalmol. 2009, 247, 1625–1633. [Google Scholar] [CrossRef] [PubMed]
- Toju, R.; Iida, T.; Sekiryu, T.; Saito, M.; Maruko, I.; Kano, M. Near-infrared autofluorescence in patients with idiopathic submacular choroidal neovascularization. Am. J. Ophthalmol. 2012, 153, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Samy, A.; Lightman, S.; Ismetova, F.; Talat, L.; Tomkins-Netzer, O. Role of autofluorescence in inflammatory/infective diseases of the retina and choroid. J. Ophthalmol. 2024, 2024, 418193. [Google Scholar] [CrossRef]
Figure 1.
(a) Fundus autofluorescence image, showing hipoautoflurescence of inactive postinflammatory lesions (red arrows) and hiperautofluorescence of active inflammatory lesions (green asterix) (b-c) Fluoresceine angiography images, showing early isofluorescence with late staining of the lesions as a result of retinal pigmented epithelium window defect, without features f inflammatory choroidal neovascularization.
Figure 1.
(a) Fundus autofluorescence image, showing hipoautoflurescence of inactive postinflammatory lesions (red arrows) and hiperautofluorescence of active inflammatory lesions (green asterix) (b-c) Fluoresceine angiography images, showing early isofluorescence with late staining of the lesions as a result of retinal pigmented epithelium window defect, without features f inflammatory choroidal neovascularization.
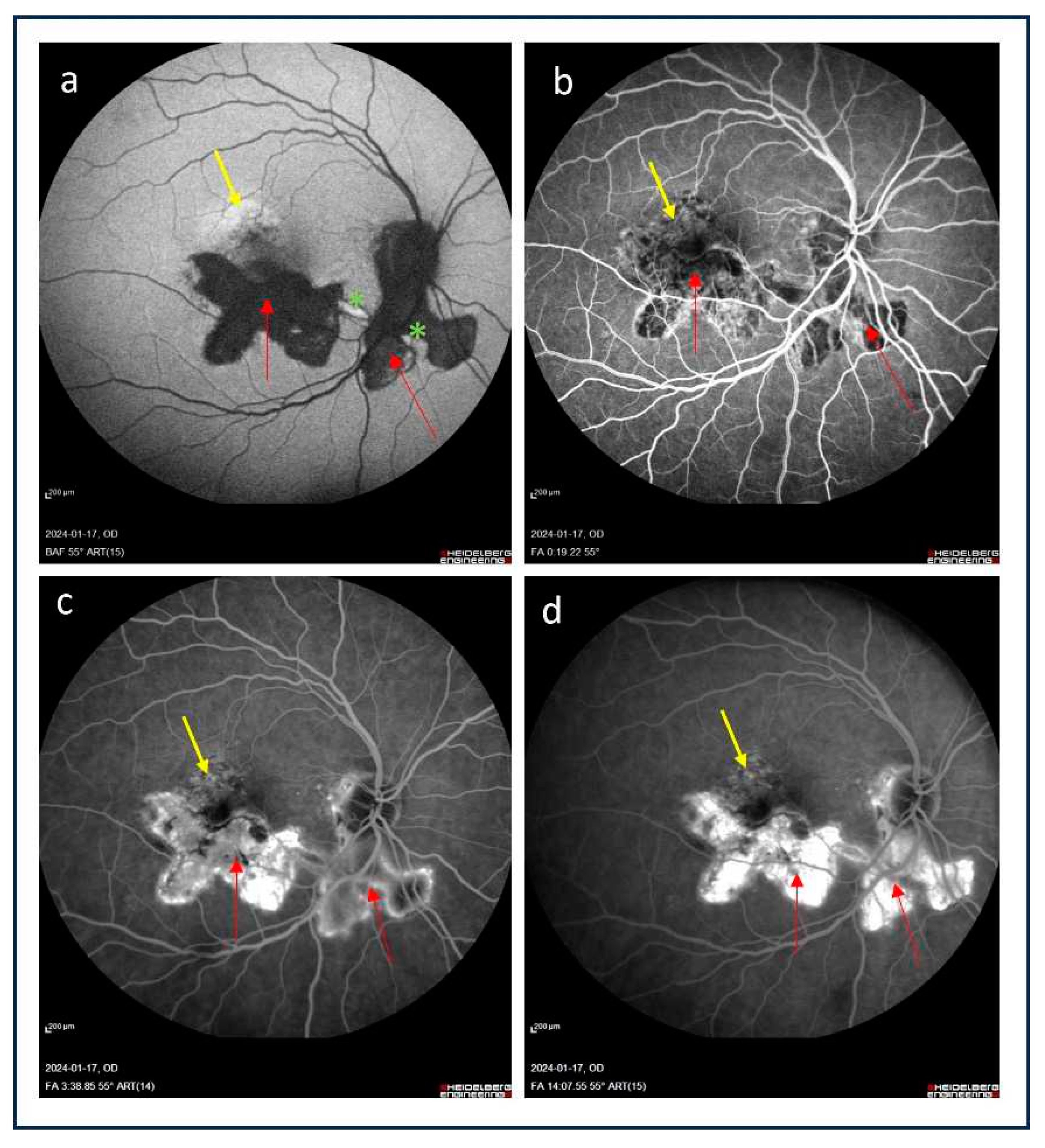
Figure 2.
(a) Color picture of the fundus showing inactive inflammatory foci in macula region with changes at retinal pigmented epithelium level; (b-c) Fluorescein angiography images demonstrated early isofluorescence with late staining of the lesions as a result of reinal pigmented epithelium window defect without features of inflammatory choroidal neovascularization.
Figure 2.
(a) Color picture of the fundus showing inactive inflammatory foci in macula region with changes at retinal pigmented epithelium level; (b-c) Fluorescein angiography images demonstrated early isofluorescence with late staining of the lesions as a result of reinal pigmented epithelium window defect without features of inflammatory choroidal neovascularization.
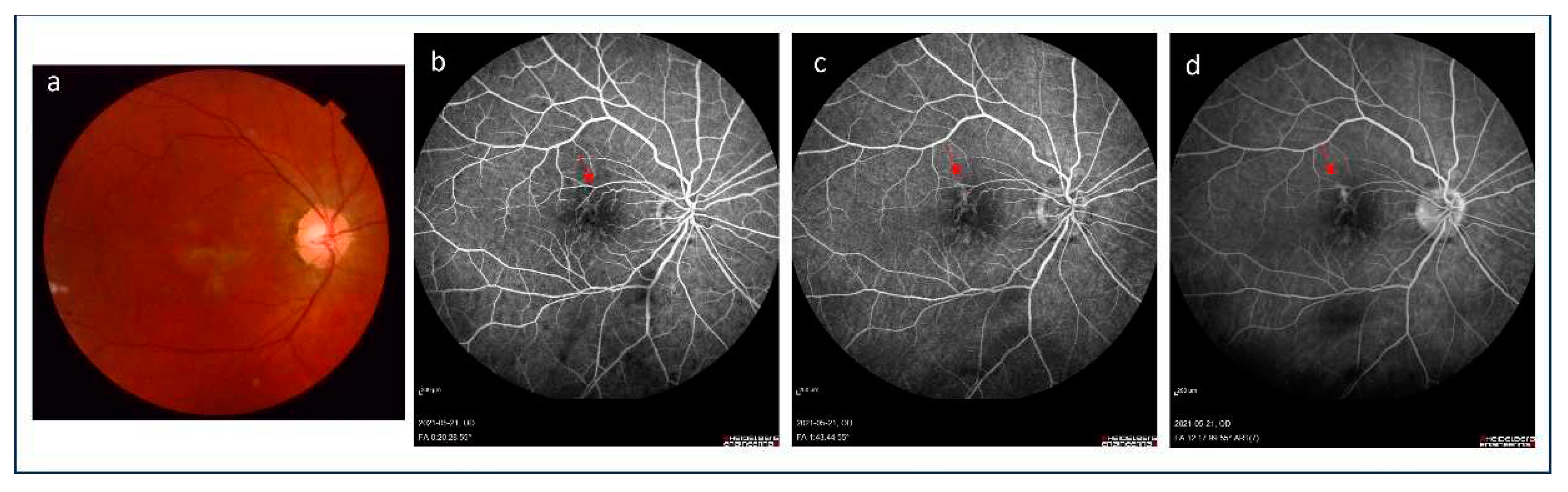
Figure 3.
(a) Fundus autofluorescence image shows hypoautoflurescence of inactive postinflammatory lesion in macula (red arrow) with hyperautofluorescent area representing the active inflammatory focus at its lower margin (green arrow), at the upper border of the hypofluorescent lesion the hyperfluorescent area is present (yellow arrow); (b-c) Early and middle frames of indocyanine green (ICG) angiograms reveal a visibility of the choroidal vessels in the area of the inactive postinflammatory focus and small hypocyanescent area at its lower border corresponding to active choroidal inflammation; (d) Late ICG angiogram demonstrates homogeneous hypocyanescence of the postinflammatory lesion with evidence of late hypercyanescence at its upper margin. The patient was diagnosed for inflammatory choridal neovascularization.
Figure 3.
(a) Fundus autofluorescence image shows hypoautoflurescence of inactive postinflammatory lesion in macula (red arrow) with hyperautofluorescent area representing the active inflammatory focus at its lower margin (green arrow), at the upper border of the hypofluorescent lesion the hyperfluorescent area is present (yellow arrow); (b-c) Early and middle frames of indocyanine green (ICG) angiograms reveal a visibility of the choroidal vessels in the area of the inactive postinflammatory focus and small hypocyanescent area at its lower border corresponding to active choroidal inflammation; (d) Late ICG angiogram demonstrates homogeneous hypocyanescence of the postinflammatory lesion with evidence of late hypercyanescence at its upper margin. The patient was diagnosed for inflammatory choridal neovascularization.
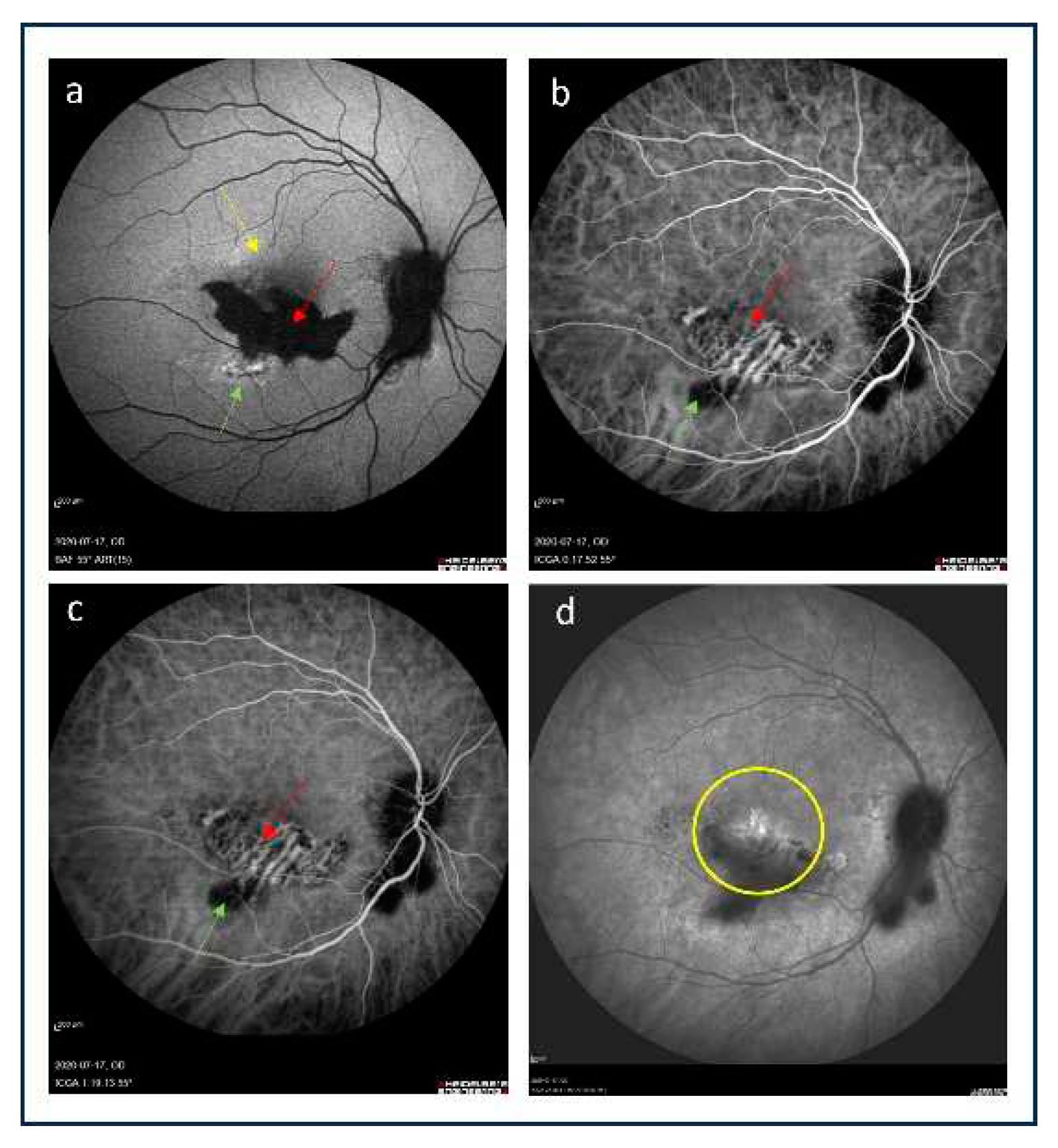
Figure 4.
(a and e) Color pictures of the fundus presenting well-defined and partially pigmented chorioretinal scars at the sites of previous inflammation in macula of both eyes; (b and f) Fundus autofluorescence demonstrated hypoautofluorescent foci which correlate with photoreceptor and retinal pigment epithelium damage; (c-d and g-h) Early and late frames of indo cyanine green angiograms revealed the presence of homogenous hypocyanescent foci related to retinal pigment epithelium damage due to postinflammatory scarring, no feature of inflammatory choroidal neovascularization is observed..
Figure 4.
(a and e) Color pictures of the fundus presenting well-defined and partially pigmented chorioretinal scars at the sites of previous inflammation in macula of both eyes; (b and f) Fundus autofluorescence demonstrated hypoautofluorescent foci which correlate with photoreceptor and retinal pigment epithelium damage; (c-d and g-h) Early and late frames of indo cyanine green angiograms revealed the presence of homogenous hypocyanescent foci related to retinal pigment epithelium damage due to postinflammatory scarring, no feature of inflammatory choroidal neovascularization is observed..
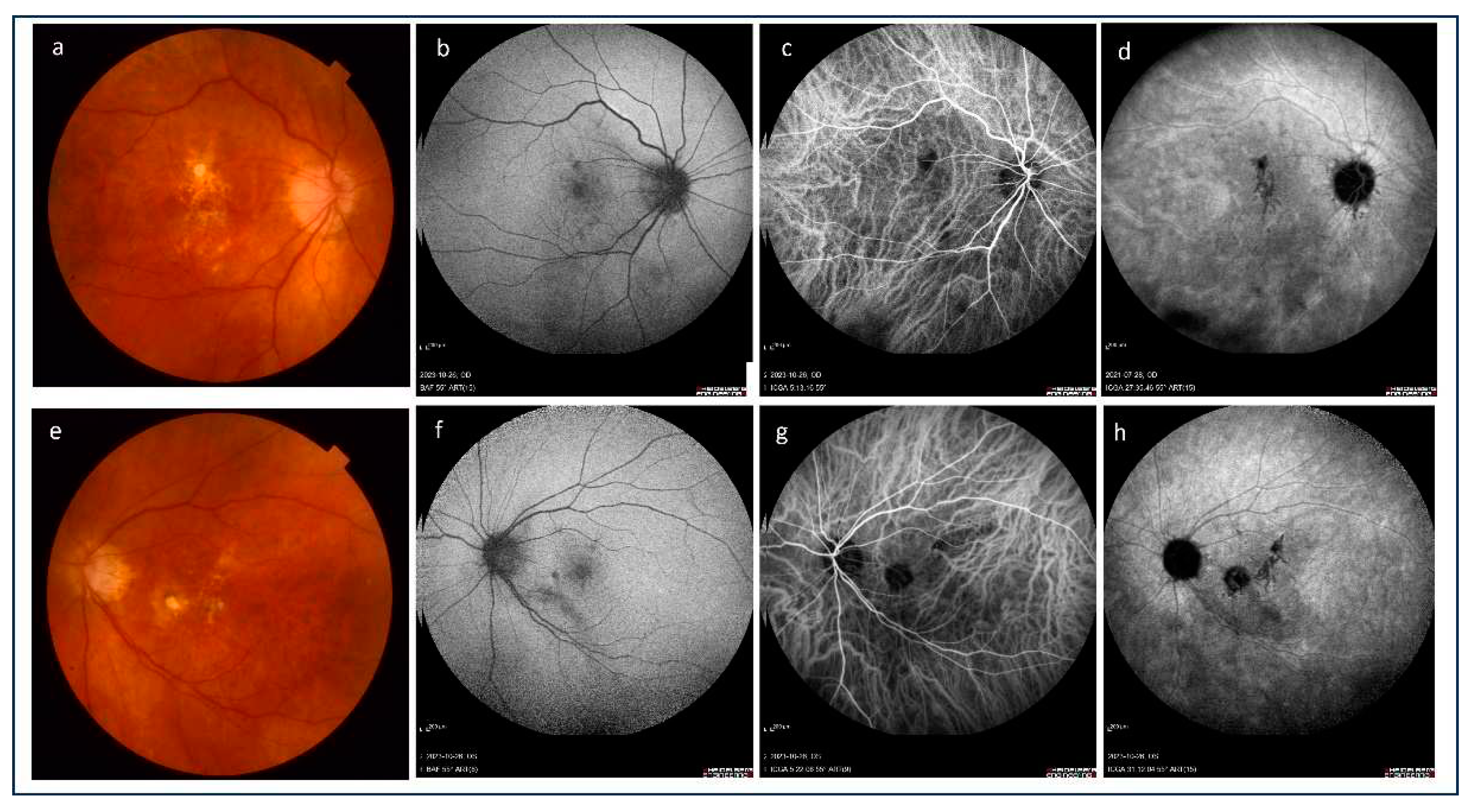
Figure 5.
(a) Color picture of the fundus shows macular subretinal fibrosis; (b) Optical coherence tomography revealed hyperreflective material under the retinal pigment epithelium (yellow arrows), subretinal fluid is present (red asterix), (c) Optical coherence tomography-angiography demonstrated pathological vessels in outer retinal layer presenting inflammatory choroidal neovascularization. .
Figure 5.
(a) Color picture of the fundus shows macular subretinal fibrosis; (b) Optical coherence tomography revealed hyperreflective material under the retinal pigment epithelium (yellow arrows), subretinal fluid is present (red asterix), (c) Optical coherence tomography-angiography demonstrated pathological vessels in outer retinal layer presenting inflammatory choroidal neovascularization. .
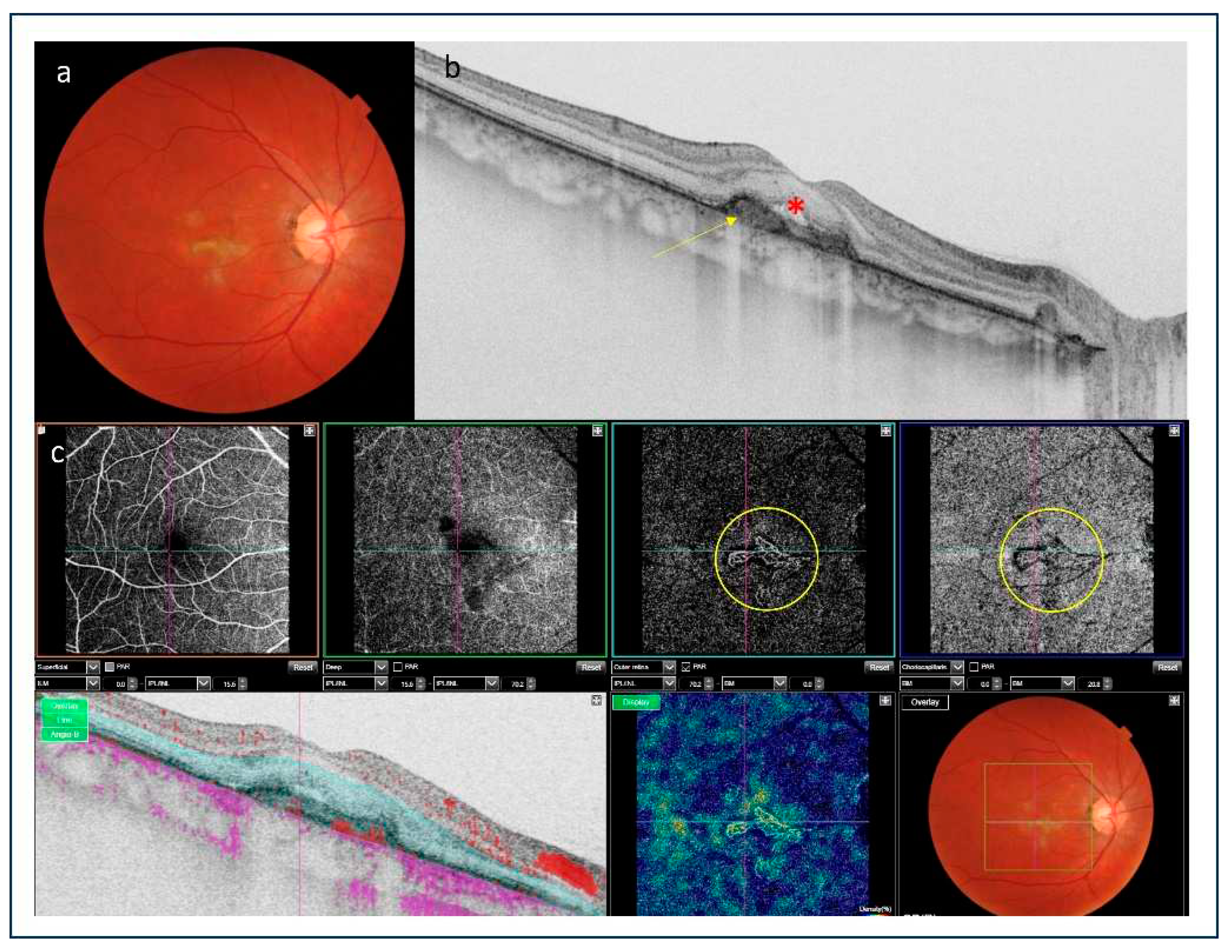
Figure 6.
(a) Early and middle stages of indocyanine green angiography presented hypocya nescence spots indicating active inflammatory lesions, late stage showed hypercyanescent. plaque (green circle); (b) Optical coherence tomography angiography revealed the presence of small inflammatory choroidal neovascularization in outer retina layer (green circle); (c). Optical coherence tomography showed the presence of a trace of subretinal fluid (yellow arrow), blood flow in outer retinal layers (green arrow) and intraretinal fluid (pink arrow) indicating the presence of inflammatory choroidal neovascularization.
Figure 6.
(a) Early and middle stages of indocyanine green angiography presented hypocya nescence spots indicating active inflammatory lesions, late stage showed hypercyanescent. plaque (green circle); (b) Optical coherence tomography angiography revealed the presence of small inflammatory choroidal neovascularization in outer retina layer (green circle); (c). Optical coherence tomography showed the presence of a trace of subretinal fluid (yellow arrow), blood flow in outer retinal layers (green arrow) and intraretinal fluid (pink arrow) indicating the presence of inflammatory choroidal neovascularization.
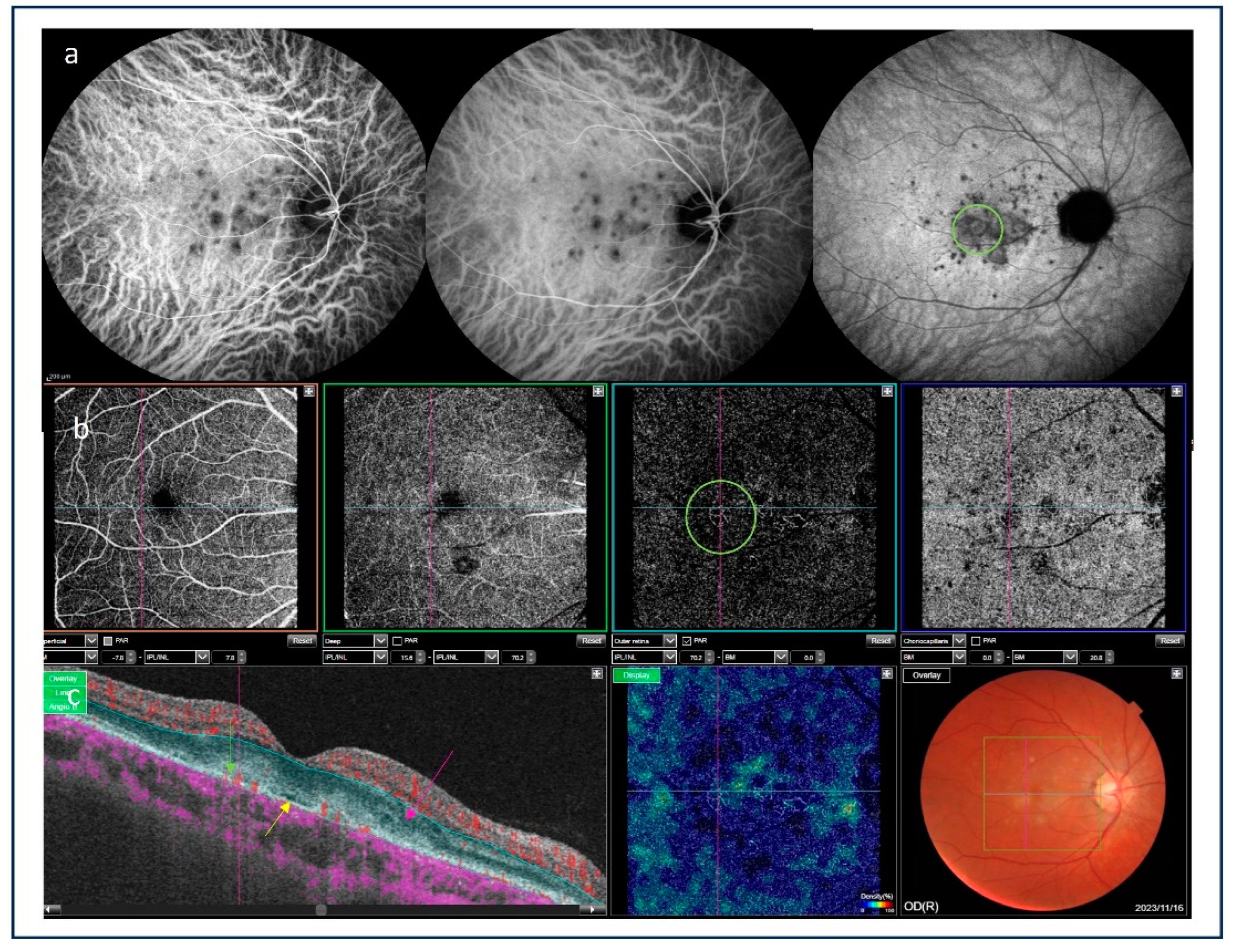
Figure 7.
Figure 7. (a) Color picture of the fundus shows the presence of partially pigmented inactive inflammatory lesion related to serpiginous choroidopathy suspected for inflammatory choroidal neovascularization; (b) Fundus autofluorescence image shows hypoautoflurescence of inactive postinflammatory lesion in macula with hyperautofluorescent lesion above it; (c) Optical coherence tomography angiography demonstrated the net of pathological vessels in outer retina layer; (d) optical coherence tomography revealed the presence of subretinal mass (yellow arrow) with subretinal (red asterix) and intraretinal fluid (blue arrow) showing the evidence of inflammatory choroidal neovasularization.
Figure 7.
Figure 7. (a) Color picture of the fundus shows the presence of partially pigmented inactive inflammatory lesion related to serpiginous choroidopathy suspected for inflammatory choroidal neovascularization; (b) Fundus autofluorescence image shows hypoautoflurescence of inactive postinflammatory lesion in macula with hyperautofluorescent lesion above it; (c) Optical coherence tomography angiography demonstrated the net of pathological vessels in outer retina layer; (d) optical coherence tomography revealed the presence of subretinal mass (yellow arrow) with subretinal (red asterix) and intraretinal fluid (blue arrow) showing the evidence of inflammatory choroidal neovasularization.
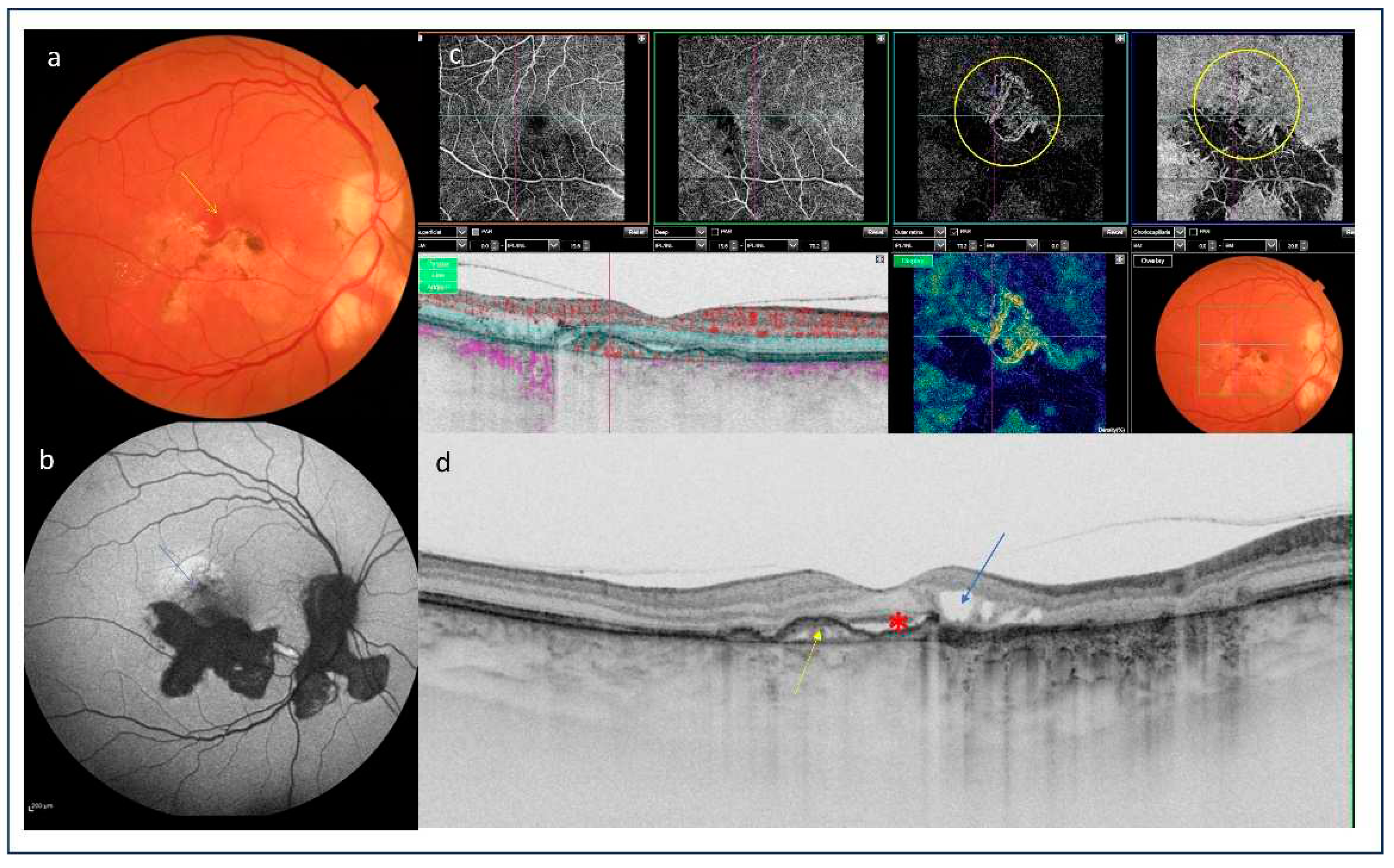

Table 1.
Prevalence of inflammatory choroidal neovascularization (iCNV) depending on the etiology of uveitis.
Table 1.
Prevalence of inflammatory choroidal neovascularization (iCNV) depending on the etiology of uveitis.
| Type of uveitis | Prevalence of iCNV, [references] |
|---|---|
| Non-infectious | |
| Multifocal choroiditis | 32–50% [4,5,6,7] |
| Punctate inner choroidopathy | 17-40% [1,4,8,9] |
| Serpiginous choroidopathy | 10-25% [4,10,11] |
| Vogt–Koyanagi–Harada disease | 9-15% [4,7,9,12] |
| Birdshot chorioretinitis | 5% [4,13] |
| Intermediate uveitis | single cases reported [14,15] |
| Behçet disease | very rare [4,16] |
| Acute posterior multifocal placoid pigment epitheliopathy | single cases reported [4,16,17,18] |
| Sympathetic ophthalmia | single cases reported [16,19] |
| Sarcoidosis | single cases reported [4,9,16] |
| Multiple evanescent white dot syndrome | single cases reported [4,20,21] |
| Infectious | |
| Histoplasmosis | 5-17.4% [4,9,16,22,23,24,25] |
| Candidiasis | rare; prevalence unknown [26,27,28] |
| Toxoplasmosis | 0.3-19% [29,30,31,32] |
| Toxocariasis | single cases reported [33,34,35] |
| Tuberculosis | single cases reported [36,37,38,39] |
| Rubella retinopathy | single cases reported [40,41,42,43] |
| West Nile virus | single cases reported [44,45,46] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



