Submitted:
29 January 2024
Posted:
29 January 2024
You are already at the latest version
Abstract
Background: Mechanical ventilation in preterm neonates aims for synchrony, preventing complications such as lung injury. Neurally Adjusted Ventilatory Assist (NAVA) stands out as a unique mode relying on diaphragmatic electrical signals for synchronization. We attempted to review studies that have explored the long-term consequence of using invasive NAVA in neonates with a specific focus on respiratory outcomes, namely bronchopulmonary dysplasia (BPD).
Methods: A systematic review following PRISMA explored invasive NAVA in preterm neonates. Primary objectives compared NAVA to conventional ventilation, assessing BPD incidence, ventilation duration, length of stay, and adverse events. Secondary objectives analyzed ventilator parameters.
Results: After screening 282 records, nine studies were included. NAVA showed reduced oxygen requirement at 28 days but no significant differences in oxygen need at 36 weeks postmenstrual age, total length of stay, or ventilator days. Adverse events such as air leak, mortality, patent ductus arteriosus, and intraventricular hemorrhage revealed no substantial variations. Ventilator variables favored NAVA, indicating decreased peak inspiratory pressure, tidal volume, work of breathing, and respiratory severity score.
Conclusion: Despite short-term benefits, our study found no significant reduction in BPD with NAVA. Future large-scale trials are essential to comprehensively assess NAVA's impact on preterm infants' long-term outcomes.
Keywords:
neurally adjusted ventilatory assist
; bronchopulmonary dysplasia
; preterm
; patient-ventilator synchrony
1. Introduction
Ensuring patient-ventilator synchrony is one of the main objectives of mechanical ventilation in preterm neonates, particularly those with Extremely Low Birth Weight (ELBW < 1000 grams). In critically ill pediatric and adults as well as animal studies, patient-ventilator asynchrony has been linked to increased work of breathing, lung injury, diaphragmatic dysfunction, and mortality [1,2,3,4,5,6,7,8,9,10,11,12,13]. Although studies have shown that noninvasive respiratory support is superior [14,15], invasive mechanical ventilation is unavoidable, particularly in preterm neonates born at less than 28 weeks of gestation [16,17]. Various ventilatory modes are currently used in neonatal mechanical ventilation, with Neurally Adjusted Ventilatory Assist (NAVA) standing out due to its unique and exceptionally appealing characteristics.
NAVA is a form of respiratory support that relies on detecting an electrical signal from the diaphragm. NAVA ensures synchronization not only during breath initiation but also during breath termination. The magnitude of the patient’s respiratory demand on NAVA is synchronized between the patient and the ventilator [18,19,20]. Several clinical studies in neonates have demonstrated a significant improvement in synchrony between the patient and the ventilator when utilizing NAVA, whether invasive or noninvasive [21,22,23,24,25,26]. Moreover, up to the present moment, the Electrical Activity of the Diaphragm (EAdi) represents the earliest signal in the neural respiratory pathway, beginning from the central respiratory system, traversing the phrenic nerve, and concluding with diaphragmatic contraction [19].
NAVA delivers pressure assistance proportional to and synchronized with the EAdi. A specially designed single-use feeding tube with measuring electrodes is positioned in the esophagus, enabling the isolation of diaphragmatic electrical signals from other signals in the body, especially those originating from the heart [19,20,27,28]. NAVA level is the factor by which the Edi signal is multiplied to adjust the amount of ventilator assist delivered. Utilizing the Edi waveform, NAVA can monitor neural respiratory drive and breathing patterns, providing valuable insights even without the routine techniques, such as measuring airflow, airway pressure, or volume commonly employed in conventional mechanical ventilation (CMV) [29,30].
Several studies have compared NAVA to other conventional mechanical ventilator modes and have mainly been centered on the short-term outcomes, including respiratory support parameters, lung mechanics, work of breathing, duration of mechanical ventilation, sedation requirements, as well as EAdi [31,32,33,34,35,36,37,38,39,40,41,42]. However, only a few studies have investigated the long-term outcomes of applying this novel technique in the preterm population. We attempted to review studies that have explored the long-term consequence of using NAVA in neonates with a specific focus on respiratory outcomes, namely bronchopulmonary dysplasia (BPD) [19,24].
2. Materials and Methods
2.1. Study Design
A systematic review was conducted following the guidelines outlined by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [43] to explore the application of invasive NAVA in preterm newborn infants. The primary objectives included investigating whether NAVA leads to lower incidences of BPD compared to conventional triggered ventilation methods, as well as assessing the risk for mortality, intraventricular hemorrhage (IVH), air leak, patent ductus arteriosus (PDA), duration of mechanical ventilation, and total length of stay in NAVA and conventional ventilation groups. In addition to primary objectives, secondary objectives involved examining differences in various ventilator parameters, including peak inspiratory pressure (PIP), mean airway pressure (MAP), Tidal Volume (TV), Work of Breathing (WOB), and Respiratory Severity Score (RSS) between NAVA and conventional ventilation from crossover trials in newborns.
2.2. Search Strategy
A comprehensive literature search strategy encompassed diverse databases, including PubMed, Embase, Google Scholar, clinicaltrials.gov, and the Cochrane Library. The search strategy incorporated Medical Subject Headings (MeSH) terms like ’infant,’ ’newborn,’ and ’Interactive Ventilatory Support’ alongside title keywords such as ’neurally adjusted’ and ’NAVA’ without constraints on date, language, or publication status. The strategic application of Boolean operators ’AND’ and ’OR’ enhanced the search to refine and broaden the relevant literature in the field.
2.3. Data Extraction and Data Analysis
Two reviewers independently extracted data from the studies, encompassing study characteristics and outcomes, including publication year and author information. For outcomes, the difference between the means of the data after the intervention period was extracted. In cases where the average was unavailable, the difference between the average of the changed values and their standard deviation was extracted. Effect measures were chosen based on the nature of the variables. Relative risk ratios (RRs) with 95% confidence intervals (CI) served as the effect measure for binary variables such as O2 requirement at 28 days, O2 requirement at 36 weeks, and adverse events (mortality rate, PDA, IVH, air leak). Mean difference (MD), standardized MD (SMD), and 95% CI were used as the effect measure for continuous variables, including duration of invasive ventilation, length of stay in the Neonatal Intensive Care Unit (NICU), and ventilator variables (PIP, MAP, TV, RSS, WOB). Using the NCSS 2023 Statistical Software (NCSS, LLC, Kaysville, Utah, USA), we generated comprehensive summary statistics and forest plots for these variables, contributing to a robust understanding of outcomes associated with these distinctions.
3. Results
This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
In December 2023, we conducted a thorough search for pertinent articles. A total of 282 records were initially identified through database searching. After excluding duplicates (n = 196), 86 records underwent screening. Subsequently, 26 reports were considered for full-text articles, but two were not retrieved. Following the eligibility assessment of 24 reports, 15 were excluded, resulting in the final inclusion of 9 studies in the review. Figure 1 provides an overview of our search methods and the study selection process.
The characteristics of these included studies are detailed in Table 1.
3.1. Impact on BPD outcome
The National Institute of Child Health and Human Development (NICHD) revised BPD criteria, defining it as the need for oxygen support (>21%) at 36 weeks postmenstrual age (PMA) for infants <32 weeks and for >28 days for those >32 weeks [51]. The Vermont Oxford Network (VON) defines BPD based solely on FiO2 requirement at 36 weeks PMA [52]. Two studies, Fang et al. and Kallio et al., reported data on O2 requirement at 36 weeks PMA, with Fang et al. also including information on O2 requirement at 28 days of life.
The collective analysis, encompassing studies by Fang et al. and Kallio et al., comparing proportions regarding oxygen requirements at 36 weeks PMA for NAVA vs. CMV, reveals a combined risk ratio of 0.8143 (95% CI: 0.4055 to 1.6351). However, non-directional and directional zero-effect tests did not achieve statistical significance, and the heterogeneity test indicated homogeneous effects across studies. (Figure 2a)
The analysis comparing oxygen requirement at 28 days for NAVA versus CMV, based on the study by Fang et al., reveals a risk ratio of 0.6029 (95% CI: 0.3827 to 0.9498). The random effects model suggests a significant directional effect (p = 0.0291), indicating that patients on NAVA have a reduced risk of needing oxygen at 28 days compared to CMV. (Figure 2b)
3.2. Impact on Length of Stay and Ventilator Days
When comparing the total length of NICU stay between NAVA and conventional models, the combined analysis showed a fixed mean difference of -1.395 (95% CI: -3.308 to 0.517), suggesting a potential decrease in total NICU stay length with NAVA compared to conventional models, as implied by the negative fixed mean difference of -1.395. However, it is crucial to approach this finding with caution due to the lack of statistical significance and notable heterogeneity among the included studies (τ² = 48.036). Similarly, in comparing ventilator days between NAVA and conventional models, the combined analysis suggested a potential decrease with NAVA, but the observed average difference of -4.54 (95% CI: -14.25 to 5.17) wasn’t statistically significant. Caution is warranted due to the observed significant heterogeneity among the included studies (τ² = 48.741). (Figure 3) Further research and consideration of individual study characteristics are necessary to draw more definitive conclusions on the impact of NAVA on NICU stay length and ventilator days.
3.3. Impact on Adverse Events
The combined analysis comparing NAVA and Conventional ventilation suggests a non-significant decrease in the risk of air leaks with NAVA (risk ratio: 0.7301, 95% CI: 0.2186 to 2.4387, p = 0.6092). There is a non-significant increase in the risk of IVH with NAVA (risk ratio: 2.0024, 95% CI: 0.7390 to 5.4254, p = 0.6135). No significant difference is observed in death rates (risk ratio: 1.5681, 95% CI: 0.2736 to 8.9871, p = 0.1884) and PDA incidence (risk ratio: 0.6198, 95% CI: 0.3039 to 1.2642, p = 0.2551). Heterogeneity tests indicate no significant variation in effects among studies for all comparisons. (Figure 4)
3.4. Impact on ventilator variables
The combined analysis indicates a significant decrease in peak inspiratory pressure (PIP) in NAVA versus CMV, with a mean difference of -3.367 (95% CI: -4.327 to -2.407), across studies including Hunt et al., Jung et al., Lee et al., Rosterman et al., and Stein et al. For tidal volume (TV) in NAVA versus CMV, a significant mean difference of -0.738 (95% CI: -1.139 to -0.338) is observed, with both fixed and random-effect models showing significance and an inconsistency index (I²) of 72.065%. In the comparison of mean airway pressures (MAP), a non-significant mean difference of -0.264 (95% CI: -0.631 to 0.104) is found between NAVA and CMV, but there is significant overall heterogeneity (I² = 83.677%). NAVA demonstrates a significantly lower Work of Breathing (WOB) compared to CMV, with a mean difference of -0.331 (95% CI: [-0.410, -0.251]). Despite statistical significance, notable heterogeneity exists among the studies (Cochran’s Q test, Q = 9.300, p = 0.0023). The combined analysis comparing NAVA and CMV for Respiratory Severity Score (RSS) shows a significant reduction with NAVA (mean difference -1.179, 95% CI: [-1.772, -0.587]). However, heterogeneity exists among studies (Cochran’s Q = 5.993, p = 0.0144). (Figure 5)
4. Discussion
Based on the limited number of studies exploring the long-term effects of invasive NAVA in neonates, this meta-analysis is the first to address this knowledge gap in the literature. BPD is a multifactorial disease of preterm neonates and stands as one of the leading causes of morbidity and mortality in these populations. The etiology of BPD is influenced by various antenatal and postnatal factors, among which ventilator-induced lung injury emerges as a significant contributor to the pathogenesis of this condition. The prevalence of BPD continues to be substantial despite significant advancements in neonatal care and contemporary ventilatory management [14,53,54,55,56].
NAVA relies on an electromyographic potential of the diaphragm to trigger the ventilator rather than a pneumatic pressure or flow signal located at the airway opening or the ventilator end [18,19,20]. This unique property of NAVA minimizes patient-ventilatory asynchrony [21,22,23,24,25,26]. Several studies examining short-term outcomes in neonates ventilated with invasive NAVA have shown improved patient-ventilator synchrony, enhanced oxygenation, favorable blood gas data, reduced respiratory severity scores, and decreased work of breathing [31,32,33,34,35,36,37,38,40,41]. Additionally, studies have reported reduced sedation requirements among neonates ventilated with invasive NAVA [31,39,40]. Our combined analysis from crossover studies has also revealed a lower PIP, TV, WOB, and RSS in neonates ventilated with invasive NAVA. From the study on short-term outcomes, one could expect and hypothesize that the recognized beneficial effects of NAVA use may reduce the incidence of BPD.
In this systematic review and meta-analysis, the comparative assessment of invasive NAVA and CMV did not reveal a superiority of NAVA concerning clinically relevant outcomes for premature infants. Despite observing a decreased risk of oxygen requirement at 28 days with NAVA compared to CMV, the combined analysis of RCTs did not reveal a statistically significant reduction in oxygen requirements at 36 weeks PMA. Additionally, the combined meta-analysis could not establish a statistically significant difference between the two ventilator modalities concerning length of stay, ventilator days, IVH, air leak, PDA, or mortality. With the limited number of available RCTs and the observed bias among the analyzed studies, generating a definitive recommendation regarding the use of invasive NAVA versus other CMV modes may be constrained by the current body of evidence.
The analysis of ventilator variables demonstrated a significant decrease in PIP, TV, WOB, and RSS with NAVA compared to conventional ventilation, while no significant difference was observed in MAP. However, it is important to interpret these findings cautiously, as significant overall heterogeneity suggests variability among the studies.
In our comparative analysis, Fang et al. and Kallio et al. emerged as crucial contributors, each shedding a unique light on the use of invasive NAVA in neonatal ventilation. Fang et al. focused on infants with a GA< 32 weeks who were intubated during delivery room resuscitation and were enrolled within 24 hours of birth. On the other hand, Kallio et al. encompassed a broader GA range (28 to 36 6/7 weeks) and concentrated on infants with RDS who were intubated for at least 4 hours, with a median enrollment age of 9 days. These distinctions in enrollment criteria highlight the diverse neonatal populations studied in this review.
A limited number of studies and the observed heterogeneity among the included studies highlight the need for cautious interpretation. In addition to significant heterogeneity in the baseline patient characteristics among the RCTs included in our review, particularly concerning gestational age and birth weight, these studies employed varied terminology for BPD. Moreover, BPD was treated as a secondary outcome or necessitated multiple linear regression analysis to account for several independent variables. Consequently, when analyzed individually, these outcomes might lack sufficient statistical power, enabling only the generation of hypotheses that should be confirmed in future trials, with BPD being the primary outcome. In light of this, our review aggregated data from these individual trials to enhance the statistical power and the precision of effect size estimates.
5. Conclusions
Despite the observed short-term advantages, including lower PIP and MAP, as well as reduced oxygen requirements at 28 days, our study did not find a significant reduction in BPD incidence at 36 weeks PMA with invasive NAVA. Therefore, determining the clinical benefit of NAVA on late neonatal outcomes remains inconclusive based on current literature. In summary, our analysis, limited by the number of studies, underscores the need for future trials to thoroughly investigate the effects of NAVA on long-term outcomes in premature infants. As a suggestion for future research, it would be beneficial to conduct large-scale studies with a focus on the impact on BPD. Large sample sizes in future research endeavors would provide more power to determine the impact of NAVA on BPD outcomes conclusively.
Author Contributions
Conceptualization: P.B., M.S.; methodology: P.B.; software: P.B.; validation: P.B., M.S.; formal analysis: P.B., M.S.; investigation, resources, and data curation: P.B., M.S.; writing - original draft preparation: P.B., writing—review, and editing, M.S.; visualization, supervision, and project administration: P.B.; funding acquisition: Not applicable. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Not applicable
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Blanch, L.; Villagra, A.; Sales, B.; Montanya, J.; Lucangelo, U.; Luján, M.; et al. Asynchronies during mechanical ventilation are associated with mortality. Intensive Care Med. 2015, 41, 633–41. [Google Scholar] [CrossRef]
- Bosma, K.; Ferreyra, G.; Ambrogio, C.; Pasero, D.; Mirabella, L.; Braghiroli, A.; et al. Patient-ventilator interaction and sleep in mechanically ventilated patients: pressure support versus proportional assist ventilation. Crit Care Med. 2007, 35, 1048–54. [Google Scholar] [CrossRef]
- Colombo, D.; Cammarota, G.; Alemani, M.; Carenzo, L.; Barra, F.L.; Vaschetto, R.; et al. Efficacy of ventilator waveforms observation in detecting patient-ventilator asynchrony. Crit Care Med. 2011, 39, 2452–7. [Google Scholar] [CrossRef]
- de Wit, M.; Miller, K.B.; Green, D.A.; Ostman, H.E.; Gennings, C.; Epstein, S.K. Ineffective triggering predicts increased duration of mechanical ventilation. Crit Care Med. 2009, 37, 2740–5. [Google Scholar] [CrossRef] [PubMed]
- Epstein, S.K. How often does patient-ventilator asynchrony occur and what are the consequences? Respir Care. 2011, 56, 25–38. [Google Scholar] [CrossRef]
- Kyo, M.; Shimatani, T.; Hosokawa, K.; Taito, S.; Kataoka, Y.; Ohshimo, S.; et al. Patient-ventilator asynchrony, impact on clinical outcomes and effectiveness of interventions: a systematic review and meta-analysis. J. Intensive Care 2021, 9, 50. [Google Scholar] [CrossRef] [PubMed]
- Levine, S.; Nguyen, T.; Taylor, N.; Friscia, M.E.; Budak, M.T.; Rothenberg, P.; et al. Rapid disuse atrophy of diaphragm fibers in mechanically ventilated humans. N Engl J Med. 2008, 358, 1327–35. [Google Scholar] [CrossRef] [PubMed]
- Neumann, P.; Wrigge, H.; Zinserling, J.; Hinz, J.; Maripuu, E.; Andersson, L.G.; et al. Spontaneous breathing affects the spatial ventilation and perfusion distribution during mechanical ventilatory support. Crit Care Med. 2005, 33, 1090–5. [Google Scholar] [CrossRef] [PubMed]
- Petrof, B.J.; Hussain, S.N. Ventilator-induced diaphragmatic dysfunction: what have we learned? Curr Opin Crit Care. 2016, 22, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Putensen, C.; Zech, S.; Wrigge, H.; Zinserling, J.; Stüber, F.; Von Spiegel, T.; et al. Long-term effects of spontaneous breathing during ventilatory support in patients with acute lung injury. Am J Respir Crit Care Med. 2001, 164, 43–9. [Google Scholar] [CrossRef]
- Radell, P.; Edström, L.; Stibler, H.; Eriksson, L.I.; Ansved, T. Changes in diaphragm structure following prolonged mechanical ventilation in piglets. Acta Anaesthesiol Scand. 2004, 48, 430–7. [Google Scholar] [CrossRef] [PubMed]
- Thille, A.W.; Rodriguez, P.; Cabello, B.; Lellouche, F.; Brochard, L. Patient-ventilator asynchrony during assisted mechanical ventilation. Intensive Care Med. 2006, 32, 1515–22. [Google Scholar] [CrossRef] [PubMed]
- Wrigge, H.; Zinserling, J.; Neumann, P.; Defosse, J.; Magnusson, A.; Putensen, C.; et al. Spontaneous breathing improves lung aeration in oleic acid-induced lung injury. Anesthesiology 2003, 99, 376–84. [Google Scholar] [CrossRef]
- Jobe, A.H.; Bancalari, E. Bronchopulmonary dysplasia. Am J Respir Crit Care Med. 2001, 163, 1723–9. [Google Scholar] [CrossRef]
- Govindaswami, B.; Nudelman, M.; Narasimhan, S.R.; Huang, A.; Misra, S.; Urquidez, G.; et al. Eliminating Risk of Intubation in Very Preterm Infants with Noninvasive Cardiorespiratory Support in the Delivery Room and Neonatal Intensive Care Unit. Biomed Res Int. 2019, 2019, 5984305. [Google Scholar] [CrossRef] [PubMed]
- Goldsmith, J.P.; Karotkin, E.; Suresh, G.; Keszler, M. Assisted ventilation of the neonate; Elsevier Health Sciences, 2016. [Google Scholar]
- Finer, N.N.; Carlo, W.A.; Walsh, M.C.; Rich, W.; Gantz, M.G.; Laptook, A.R.; et al. Early CPAP versus surfactant in extremely preterm infants. N Engl J Med. 2010, 362, 1970–9. [Google Scholar] [CrossRef] [PubMed]
- Sinderby, C.; Navalesi, P.; Beck, J.; Skrobik, Y.; Comtois, N.; Friberg, S.; et al. Neural control of mechanical ventilation in respiratory failure. Nat Med. 1999, 5, 1433–6. [Google Scholar] [CrossRef] [PubMed]
- Sinderby, C.; Beck, J.C. Chapter 13. Neurally Adjusted Ventilatory Assist. In Tobin MJ, editor. Principles and Practice of Mechanical Ventilation, 3rd ed.; The McGraw-Hill Companies: New York, NY, USA, 2013. [Google Scholar]
- ATS/ERS Statement on respiratory muscle testing. Am J Respir Crit Care Med. 2002, 166, 518–624. [CrossRef]
- Mally, P.V.; Beck, J.; Sinderby, C.; Caprio, M.; Bailey, S.M. Neural Breathing Pattern and Patient-Ventilator Interaction During Neurally Adjusted Ventilatory Assist and Conventional Ventilation in Newborns. Pediatr Crit Care Med. 2018, 19, 48–55. [Google Scholar] [CrossRef]
- Longhini, F.; Ferrero, F.; De Luca, D.; Cosi, G.; Alemani, M.; Colombo, D.; et al. Neurally adjusted ventilatory assist in preterm neonates with acute respiratory failure. Neonatology. 2015, 107, 60–7. [Google Scholar] [CrossRef]
- Matlock, D.N.; Bai, S.; Weisner, M.D.; Comtois, N.; Beck, J.; Sinderby, C.; et al. Work of Breathing in Premature Neonates: Noninvasive Neurally-Adjusted Ventilatory Assist versus Noninvasive Ventilation. Respir Care. 2020, 65, 946–53. [Google Scholar] [CrossRef] [PubMed]
- Beck, J.; Reilly, M.; Grasselli, G.; Mirabella, L.; Slutsky, A.S.; Dunn, M.S.; et al. Patient-ventilator interaction during neurally adjusted ventilatory assist in low birth weight infants. Pediatr Res. 2009, 65, 663–8. [Google Scholar] [CrossRef] [PubMed]
- Breatnach, C.; Conlon, N.P.; Stack, M.; Healy, M.; O’Hare, B.P. A prospective crossover comparison of neurally adjusted ventilatory assist and pressure-support ventilation in a pediatric and neonatal intensive care unit population. Pediatr Crit Care Med. 2010, 11, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Alander, M.; Peltoniemi, O.; Pokka, T.; Kontiokari, T. Comparison of pressure-, flow-, and NAVA-triggering in pediatric and neonatal ventilatory care. Pediatr Pulmonol. 2012, 47, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Sinderby, C.A.; Beck, J.C.; Lindström, L.H.; Grassino, A.E. Enhancement of signal quality in esophageal recordings of diaphragm EMG. J Appl Physiol. 1997, 82, 1370–7. [Google Scholar] [CrossRef] [PubMed]
- Beck, J.; Sinderby, C.; Weinberg, J.; Grassino, A. Effects of muscle-to-electrode distance on the human diaphragm electromyogram. J Appl Physiol. 1995, 79, 975–85. [Google Scholar] [CrossRef] [PubMed]
- Stein, H.; Firestone, K.; Beck, J. Neurally Adjusted Ventilatory Assist (NAVA) Ventilation. In Manual of Neonatal Respiratory Care; Donn, S.M., Mammel, M.C., van Kaam, A.H.L.C., Eds.; Springer International Publishing: Cham, Switzerland, 2022; pp. 443–454. [Google Scholar]
- Shi, Y.; Muniraman, H.; Biniwale, M.; Ramanathan, R. A Review on Non-invasive Respiratory Support for Management of Respiratory Distress in Extremely Preterm Infants. Front Pediatr. 2020, 8, 270. [Google Scholar] [CrossRef]
- Baez Hernandez, N.; Milad, A.; Li, Y.; Van Bergen, A.H. Utilization of Neurally Adjusted Ventilatory Assist (NAVA) Mode in Infants and Children Undergoing Congenital Heart Surgery: A Retrospective Review. Pediatr Cardiol. 2019, 40, 563–9. [Google Scholar] [CrossRef]
- Baudin, F.; Emeriaud, G.; Essouri, S.; Beck, J.; Javouhey, E.; Guerin, C. Neurally adjusted ventilatory assist decreases work of breathing during non-invasive ventilation in infants with severe bronchiolitis. Crit Care 2019, 23, 120. [Google Scholar] [CrossRef]
- Crulli, B.; Khebir, M.; Toledano, B.; Vobecky, S.; Poirier, N.; Emeriaud, G. Neurally Adjusted Ventilatory Assist After Pediatric Cardiac Surgery: Clinical Experience and Impact on Ventilation Pressures. Respir Care 2018, 63, 208–14. [Google Scholar] [CrossRef]
- Gibu, C.K.; Cheng, P.Y.; Ward, R.J.; Castro, B.; Heldt, G.P. Feasibility and physiological effects of noninvasive neurally adjusted ventilatory assist in preterm infants. Pediatr Res. 2017, 82, 650–7. [Google Scholar] [CrossRef]
- Hunt, K.A.; Dassios, T.; Greenough, A. Proportional assist ventilation (PAV) versus neurally adjusted ventilator assist (NAVA): effect on oxygenation in infants with evolving or established bronchopulmonary dysplasia. Eur J Pediatr. 2020, 179, 901–8. [Google Scholar] [CrossRef]
- Kallio, M.; Mahlman, M.; Koskela, U.; Aikio, O.; Suo-Palosaari, M.; Pokka, T.; et al. NIV NAVA versus Nasal CPAP in Premature Infants: A Randomized Clinical Trial. Neonatology 2019, 116, 380–4. [Google Scholar] [CrossRef] [PubMed]
- McKinney, R.L.; Keszler, M.; Truog, W.E.; Norberg, M.; Sindelar, R.; Wallström, L.; et al. Multicenter Experience with Neurally Adjusted Ventilatory Assist in Infants with Severe Bronchopulmonary Dysplasia. Am J Perinatol. 2021, 38, e162–e6. [Google Scholar] [CrossRef]
- Meinen, R.D.; Alali, Y.I.; Al-Subu, A.; Wilhelm, M.; Wraight, C.L.; McAdams, R.M.; et al. Neurally-Adjusted Ventilatory Assist Can Facilitate Extubation in Neonates With Congenital Diaphragmatic Hernia. Respir Care. 2021, 66, 41–9. [Google Scholar] [CrossRef] [PubMed]
- Nam, S.K.; Lee, J.; Jun, Y.H. Neural feedback is insufficient in preterm infants during neurally adjusted ventilatory assist. Pediatr Pulmonol. 2019, 54, 1277–83. [Google Scholar] [CrossRef]
- Oda, A.; Kamei, Y.; Hiroma, T.; Nakamura, T. Neurally adjusted ventilatory assist in extremely low-birthweight infants. Pediatr Int. 2018, 60, 844–8. [Google Scholar] [CrossRef]
- Protain, A.P.; Firestone, K.S.; McNinch, N.L.; Stein, H.M. Evaluating peak inspiratory pressures and tidal volume in premature neonates on NAVA ventilation. Eur J Pediatr. 2021, 180, 167–75. [Google Scholar] [CrossRef]
- Rosterman, J.L.; Pallotto, E.K.; Truog, W.E.; Escobar, H.; Meinert, K.A.; Holmes, A.; et al. The impact of neurally adjusted ventilatory assist mode on respiratory severity score and energy expenditure in infants: a randomized crossover trial. J. Perinatol. 2018, 38, 59–63. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Fang, S.J.; Su, C.H.; Liao, D.L.; Chen, C.C.; Chung, M.Y.; Chen, F.S.; et al. Neurally adjusted ventilatory assist for rapid weaning in preterm infants. Pediatr Int. 2023, 65, e15360. [Google Scholar] [CrossRef]
- Kallio, M.; Koskela, U.; Peltoniemi, O.; Kontiokari, T.; Pokka, T.; Suo-Palosaari, M.; et al. Neurally adjusted ventilatory assist (NAVA) in preterm newborn infants with respiratory distress syndrome-a randomized controlled trial. Eur J Pediatr. 2016, 175, 1175–83. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Kim, H.S.; Sohn, J.A.; Lee, J.A.; Choi, C.W.; Kim, E.K.; et al. Randomized crossover study of neurally adjusted ventilatory assist in preterm infants. J Pediatr. 2012, 161, 808–13. [Google Scholar] [CrossRef]
- Oda, A.; Parikka, V.; Lehtonen, L.; Azimi, S.; Porres, I.; Soukka, H. Neurally adjusted ventilatory assist in ventilated very preterm infants: A crossover study. Pediatr Pulmonol. 2021, 56, 3857–62. [Google Scholar] [CrossRef] [PubMed]
- Stein, H.; Alosh, H.; Ethington, P.; White, D.B. Prospective crossover comparison between NAVA and pressure control ventilation in premature neonates less than 1500 grams. J Perinatol. 2013, 33, 452–6. [Google Scholar] [CrossRef]
- Shetty, S.; Hunt, K.; Peacock, J.; Ali, K.; Greenough, A. Crossover study of assist control ventilation and neurally adjusted ventilatory assist. Eur J Pediatr. 2017, 176, 509–13. [Google Scholar] [CrossRef]
- Jung, Y.H.; Kim, H.S.; Lee, J.; Shin, S.H.; Kim, E.K.; Choi, J.H. Neurally Adjusted Ventilatory Assist in Preterm Infants With Established or Evolving Bronchopulmonary Dysplasia on High-Intensity Mechanical Ventilatory Support: A Single-Center Experience. Pediatr Crit Care Med. 2016, 17, 1142–6. [Google Scholar] [CrossRef]
- Higgins, R.D.; Jobe, A.H.; Koso-Thomas, M.; Bancalari, E.; Viscardi, R.M.; Hartert, T.V.; et al. Bronchopulmonary Dysplasia: Executive Summary of a Workshop. J Pediatr. 2018, 197, 300–8. [Google Scholar] [CrossRef] [PubMed]
- Nuthakki, S.; Ahmad, K.; Johnson, G.; Cuevas Guaman, M. Bronchopulmonary Dysplasia: Ongoing Challenges from Definitions to Clinical Care. J Clin Med. 2023, 12. [Google Scholar] [CrossRef]
- Jensen, E.A.; Schmidt, B. Epidemiology of bronchopulmonary dysplasia. Birth Defects Res A Clin Mol Teratol. 2014, 100, 145–57. [Google Scholar] [CrossRef]
- Onland, W.; Debray, T.P.; Laughon, M.M.; Miedema, M.; Cools, F.; Askie, L.M.; et al. Clinical prediction models for bronchopulmonary dysplasia: a systematic review and external validation study. BMC Pediatr. 2013, 13, 207. [Google Scholar] [CrossRef] [PubMed]
- Romijn, M.; Dhiman, P.; Finken, M.J.J.; van Kaam, A.H.; Katz, T.A.; Rotteveel, J.; et al. Prediction Models for Bronchopulmonary Dysplasia in Preterm Infants: A Systematic Review and Meta-Analysis. J Pediatr. 2023, 258, 113370. [Google Scholar] [CrossRef] [PubMed]
- Kwok, T.C.; Batey, N.; Luu, K.L.; Prayle, A.; Sharkey, D. Bronchopulmonary dysplasia prediction models: a systematic review and meta-analysis with validation. Pediatr Res. 2023, 94, 43–54. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Search Methods.
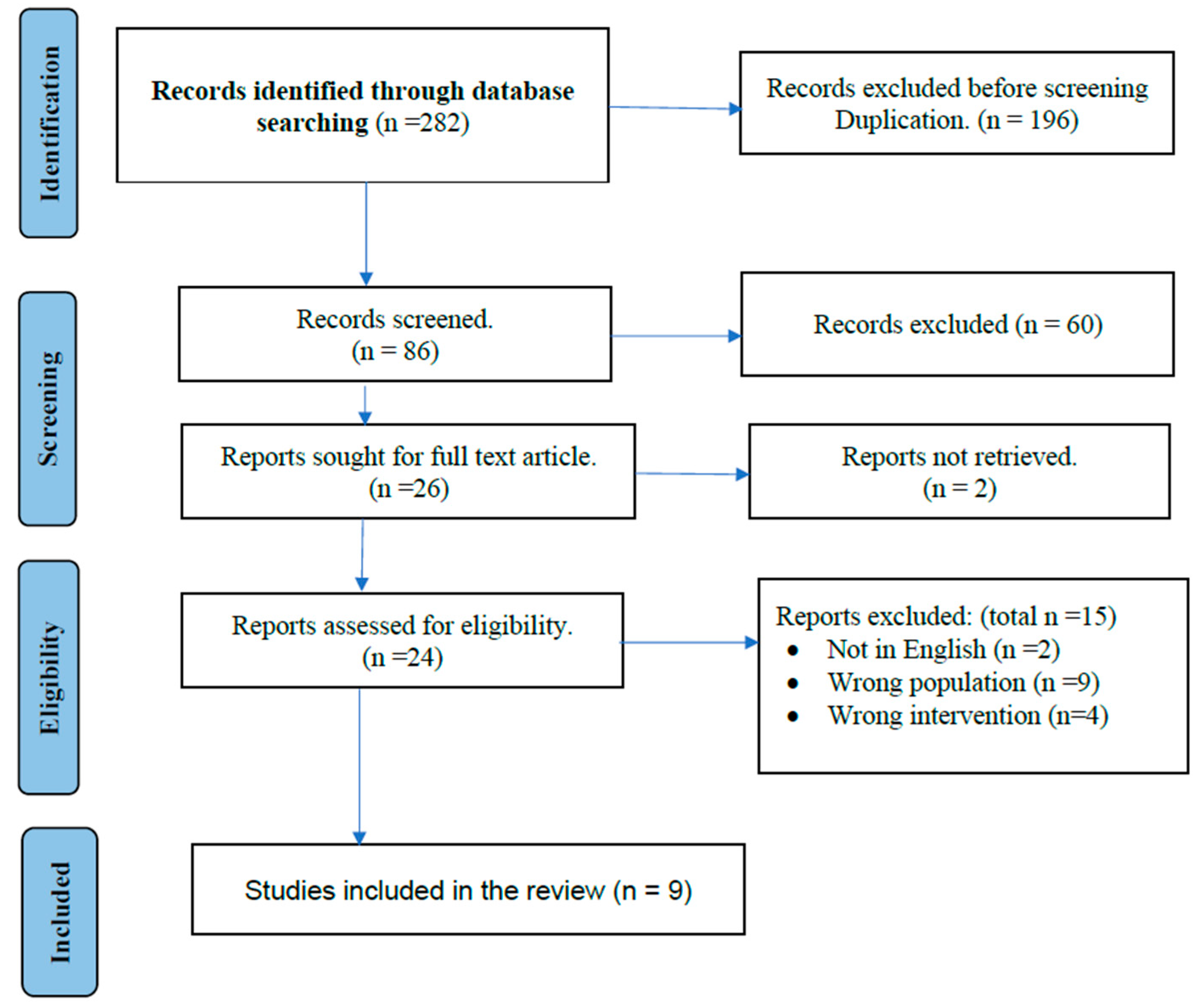
Figure 2.
Forest Plot for Impact on BPD Outcome (a) Forest Plot for Impact on O2 requirement at 36 weeks PMA; (b) Forest Plot for Impact on O2 requirement at 28 days.
Figure 2.
Forest Plot for Impact on BPD Outcome (a) Forest Plot for Impact on O2 requirement at 36 weeks PMA; (b) Forest Plot for Impact on O2 requirement at 28 days.
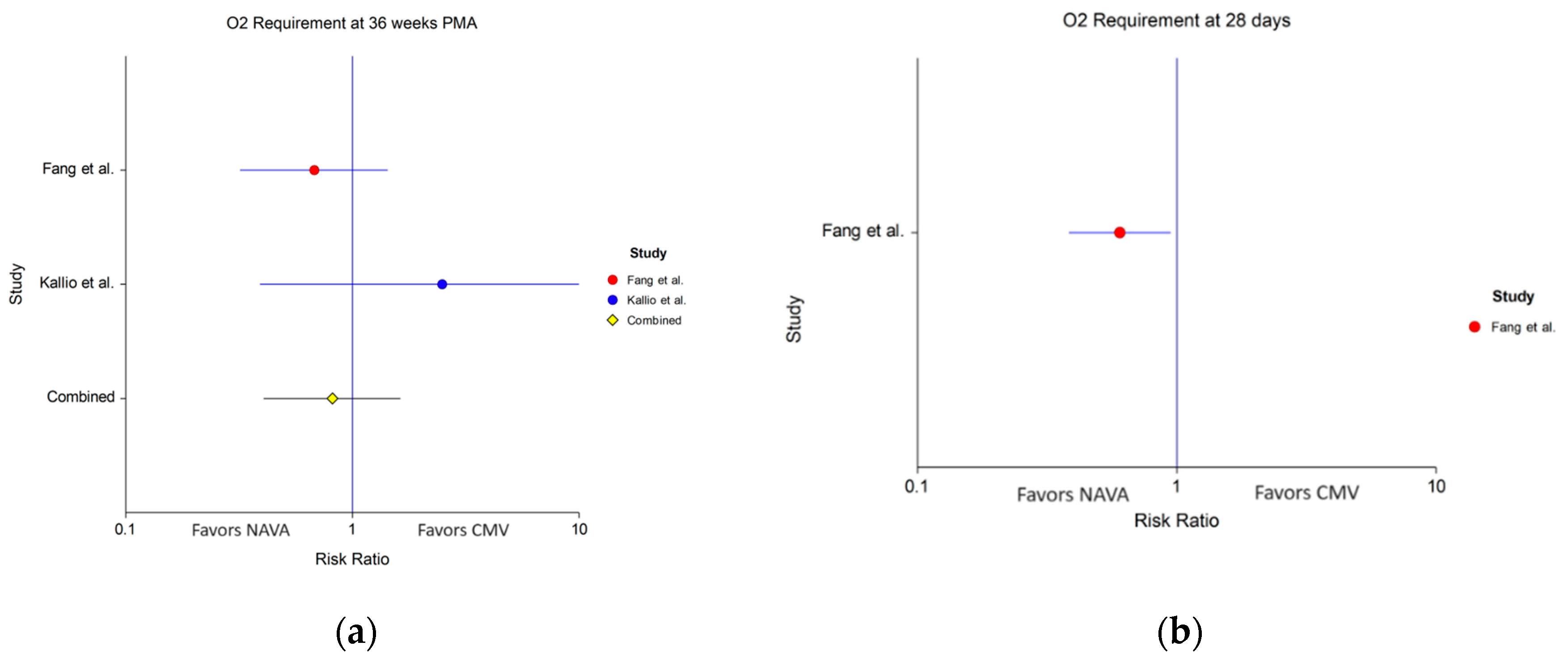
Figure 3.
(a) Forest Plot for NICU length of Stay; (b) Forest Plot for Ventilator Days.
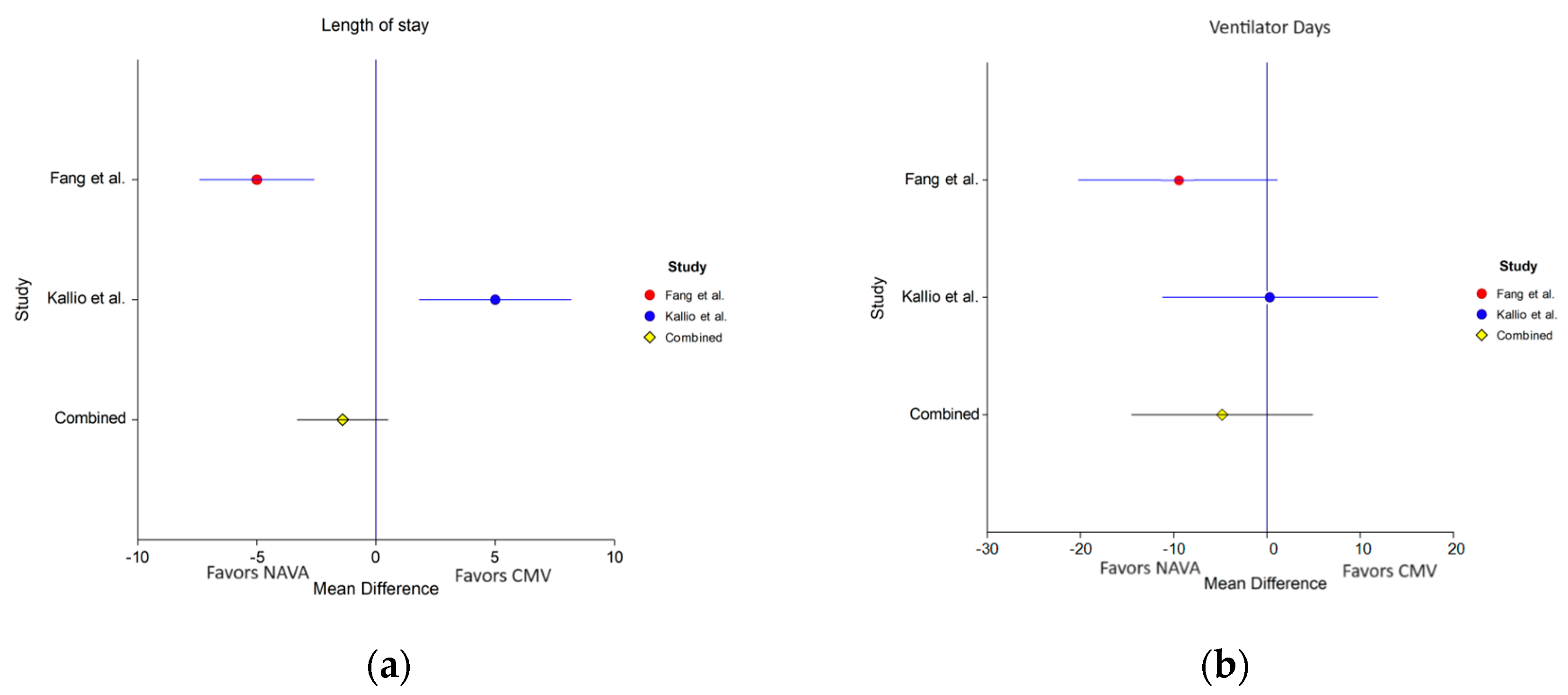
Figure 4.
Forest Plot for Adverse Events (NAVA vs CMV) (a) Forest Plot for Air leak; (b) Forest Plot for IVH (c) Forest Plot for PDA; (d) Forest Plot for Mortality.
Figure 4.
Forest Plot for Adverse Events (NAVA vs CMV) (a) Forest Plot for Air leak; (b) Forest Plot for IVH (c) Forest Plot for PDA; (d) Forest Plot for Mortality.
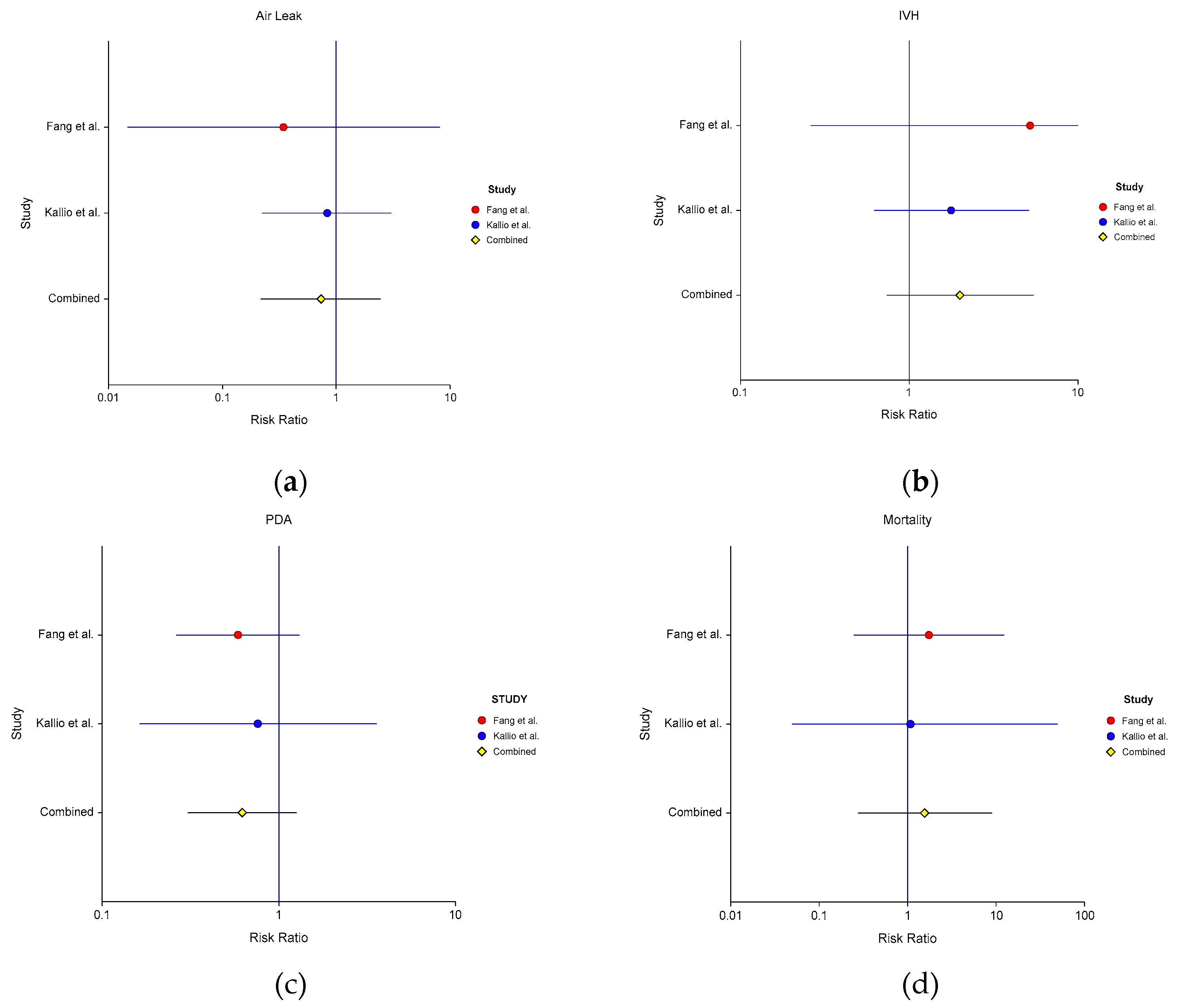
Figure 5.
Forest Plot for Ventilator Variables (NAVA vs CMV) (a) Forest Plot for PIP; (b) Forest Plot for TV (c) Forest Plot for MAP; (d) Forest Plot for WOB; (e) Forest Plot for RSS.
Figure 5.
Forest Plot for Ventilator Variables (NAVA vs CMV) (a) Forest Plot for PIP; (b) Forest Plot for TV (c) Forest Plot for MAP; (d) Forest Plot for WOB; (e) Forest Plot for RSS.
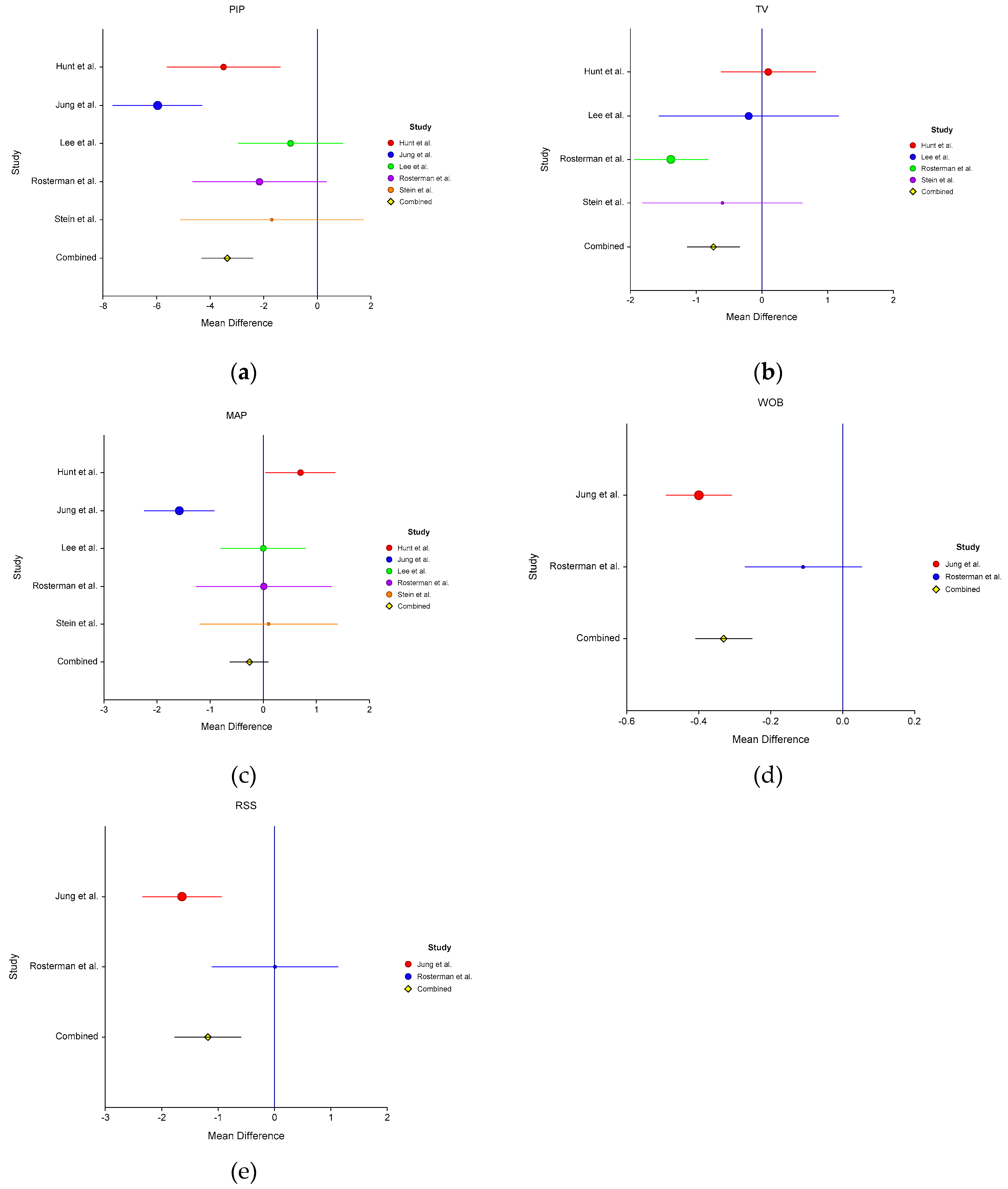

Table 1.
Characteristics of Included Studies in the Review.
| Study, Year | Study Type |
Inclusion, Exclusion, and Comparison Criteria | Sample Size | BW (g) Mean ± SD or Median (Range) | GA (weeks) Median |
Enrollment age Median (Range) |
|---|---|---|---|---|---|---|
| Fang, 2022 [44] | RCT | GA < 32 weeks, intubated for delivery room resuscitation. Exclusion: Lethal anomalies, BW < 500g. Comparison: SIMV or SIMV PS |
53 | 1207.9 ± 47.2 | 29.0 ± 0.3 | < 24 hrs |
| Kallio, 2016 [45] | RCT | GA 28 - 36 6/7 weeks, on invasive ventilation for RDS for at least 4 hrs. Exclusion: Diaphragm defects, inability to insert gastric tube, severe asphyxia, chromosomal abnormalities Comparison: Patient-triggered PC ventilation |
60 | 1735.9 ± 812 |
31.6 ± 2.6 | 9.3 (2.3 -49) days |
| Lee, 2012 [46] |
Randomized Crossover |
GA < 37 weeks, on invasive ventilation with spontaneous breathing Exclusion: Major anomalies, IVH (grade III+), phrenic nerve palsy. Comparison: SIMV with PS (4 hours crossover) |
19 | 1210 (670-2580) | 29.1 (25 - 36.4) | 7 (2-70) days |
| Oda, 2021 [47] |
Observational Crossover | GA < 30 weeks, on invasive ventilation with desaturation events. Exclusion: Major anomalies Comparison: SIMV + PS (3 hours crossover) |
20 | 610 (400–1160) | 26 4/7 (23 - 29 3/7) | 20 (1–82) days |
| Stein 2013 [48] |
Prospective Crossover | Low birth weight infants on invasive ventilation. Comparison: PCV (4 hours crossover) |
5 | 697 (370 –1140) | 26.2 (25–29) | 24 (6–34) days |
| Rosterman 2018 [42] | Randomized Crossover | GA >22 weeks, stable on MV. Exclusion: Phrenic nerve palsy, respiratory suppression due to sedation or neurologic compromise. Comparison: SIMV (PC)+PS (12h crossover) |
22 | 734 (432 to 3165) | 26 4/7 (23 to 39) | 40 (3 to 135) days |
| Hunt 2020 [35] |
Crossover | Born < 32 weeks, ventilated beyond 1 week. Comparison: A/C or SIMV (2 h crossover) |
18 | 750 [454–950] | 25.3 [23.6–30.3] | 20.5 (8–58) days |
| Shetty 2017 [49] | Retrospective | GA < 32 weeks, on invasive ventilation for > 2 weeks Comparison: A/C or SIMV |
9 | 750 (545–830) | 25 (22–27) | 20 (8–84) days |
| Jung 2020 [50] |
Retrospective | GA < 32 weeks on mechanical ventilation with RSS > 4 Comparison: SIMV-PC (PS) – (pre- and post-NAVA conversion) |
29 | 680 (370–1,230) | 25.4 (23.4–30.3) | 32.1 (26.4–43.3) days |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



