
Submitted:
17 January 2024
Posted:
17 January 2024
You are already at the latest version
Abstract
Urinary tract infections (UTIs) are a prevalent bacterial infection in both community and healthcare settings. They account for approximately 40% of all bacterial infections and require around 15% of all antibiotic prescriptions. Although antibiotics have traditionally been used to treat UTIs for several decades, the significant increase in antibiotic resistance in recent years has made many previously effective treatments ineffective. Biofilm on medical equipment in healthcare settings creates a reservoir of pathogens that can be easily transmitted to patients. Urinary catheter infections are frequently observed in hospitals and are caused by microbes that form a biofilm after the catheter is inserted into the bladder. Managing infections caused by biofilms is challenging due to the emergence of antibiotic resistance. Biofilms enable pathogens to evade the host's innate immune defences, resulting in long-term persistence. The incidence of sepsis caused by urinary tract infections that have spread to the bloodstream is increasing, and drug-resistant infections may be even more prevalent. While the availability of upcoming tests to identify the bacterial cause of infection and its resistance spectrum is critical, it alone will not solve the problem; innovative treatment approaches are also needed. This review analyses the main characteristics of biofilm formation and drug resistance in recurrent uropathogen-induced UTI. The importance of innovative and alternative therapies to combat biofilm-caused UTI is emphasised.
Keywords:
urinary tract infection
; nanoparticles
; multidrug resistance
; alternative strategies
1. Introduction
Approximately 15% of antibiotics are prescribed for the treatment of urinary tract infections (UTIs), which are one of the most common bacterial infections. UTIs affect over 400 million people annually and result in 150 million deaths worldwide [1,2]. It is estimated that around 50% of women and 5% of men will experience a UTI during their lifetime [3]. The incidence of UTIs increases with age, affecting between 30% and 50% of women over the age of 60 [4]. UTI pathogenesis is the result of several complex interactions between uropathogen and host [5,6]. However, it is widely recognised that outpatient antibiotic use is often excessive and unnecessary [7]. While antibiotics have been used to treat common infections for many years, antibiotic resistance has made several antibiotics commonly used for urinary tract infections ineffective, leading to more serious illness, hospital admissions and deaths, as well as increased healthcare costs [6,8]. Antimicrobial resistance is a major concern, with antibiotic-resistant UTIs being a critical aspect [9]. Antimicrobial resistance has been identified by the World Health Organization as one of the top ten global public health threats in 2021 [10]. A urinary tract infection that spreads to the bloodstream and causes sepsis can be fatal, and drug-resistant infections can make this more likely [6,11]. In 2019, drug-resistant infections directly caused 1.27 million of the approximately 4.95 million deaths attributed to antimicrobial resistance. This exceeds the number of deaths caused by HIV/AIDS. [12,13]. Antibiotic resistance is a natural phenomenon, but its acceleration due to the misuse of antibiotics in humans and animals is a serious problem [14]. This is especially concerning for urinary tract infections, which are among the most prevalent infectious diseases [15]. Biofilms are widely recognised as a major contributing factor to the high rates of recurrence and antimicrobial resistance commonly associated with urinary tract infections [16,17]. Biofilms can be formed by different types of bacteria, including both gram-positive and gram-negative species, and are known to play an important role in several disease processes [18,19]. This review analyses the significance of biofilm formation in recurrent urinary tract infections and summarises recent developments in understanding how drug resistance evolves in major uropathogens. The importance of rational antibiotic use in UTI treatment and the factors contributing to increasing bacterial resistance are also highlighted. It also assesses the advantages and disadvantages of alternative treatments for UTI.
2. Classification and pathogenesis of UTIs
2.1. Types of UTI
There are several classification systems for urinary tract infections [20]. However, the most widely used systems are those developed by the CDC, which distinguish between uncomplicated and complicated UTIs on the basis of the presence of risk factors such as anatomical or functional abnormalities in the urinary tract [5,6,21]. UTI are also classified according to the location of the infection and the clinical presentation of the UTI [6]. The urinary tract consists of the kidneys, ureters, bladder, and urethra. The kidneys filter waste products from the blood and produce urine, which then passes through the ureters to the bladder. UTIs are typically categorized as upper or lower depending on their location within the urinary tract. Urethritis is an inflammation of the urethra, and ureteritis is an inflammation of the ureter [22]. Lower urinary tract infections, including cystitis which refers to a bladder infection, and upper urinary tract infections such as pyelonephritis involving the kidney, are classified based on the affected area [23]. In healthy, pre-menopausal, non-pregnant women with no history of abnormal urinary tract, acute cystitis and pyelonephritis are the classifications for uncomplicated urinary tract infections, with women being more commonly affected than men [24]. Complicated UTIs involve functional or metabolic abnormalities, such as obstruction, urolithiasis, pregnancy, diabetes, neurogenic bladder, renal or other immunocompromising conditions [25]. Recurrent, catheter-associated, and urosepsis are also included in the classification of urinary tract infections [26]. UTIs are classified as recurrent if two or more episodes occur within six months or three or more episodes occur within 12 months [27,28]. Catheter-associated urinary tract infections (CAUTI) account for around 75% of all hospital-acquired urinary tract infections [29]. The risk of contracting these infections increases with prolonged use of a urinary catheter, which is a tube inserted into the bladder through the urethra to drain urine. Urosepsis is a systemic inflammatory response to urinary tract infections such as cystitis, bladder infection and pyelonephritis that can lead to multiple organ dysfunction, failure and even death [30].
2.2. Clinical syndromes
Diagnosing urinary tract infections can be challenging, especially in patients with non-specific symptoms [31]. However, it is crucial to differentiate between UTIs and asymptomatic bacteriuria to determine the necessity of antibiotic treatment [6]. Asymptomatic bacteriuria is the presence of one or more bacterial species in urine, as indicated by a positive urine culture, in a patient who does not exhibit any signs or symptoms of UTI (see below) [32]. n contrast, UTIs are infections that can affect the urethra, bladder, ureters, and/or kidneys. The symptoms experienced depend on which part of the urinary tract is affected [4,32]. Table 1 shows the signs and symptoms of urinary tract infections depending on the location of the bacterial infection.
UTIs are more common in women and typically affect the bladder and urethra [18]. Uropathogens commonly infect the urinary tract through an ascending route that starts in the genital area, passes through the urethra to the bladder, and then ascends the ureters to reach the kidneys (Figure 1). Cystitis is a prevalent UTI among women, especially pregnant women, due to pregnancy's interference with bladder emptying [33]. Women are more susceptible to cystitis due to the shorter length of their urethra and its proximity to the anus. Recurrent episodes of cystitis are common among women, especially during their reproductive years, as bacteria can travel from the urethra to the bladder during sexual intercourse [34]. Bladder infections in women can also be caused by the use of a diaphragm for contraception or the decrease in estrogen production after menopause [35]. The spermicide used in conjunction with the diaphragm suppresses the natural vaginal flora, allowing the bacteria responsible for cystitis to thrive [21]. Bladder prolapse can occur as a result of decreased estrogen production during menopause, which can make it difficult to empty the bladder and increase the risk of bladder infections [36]. In men, cystitis and urethritis are frequently caused by bacterial prostatitis resulting from ascending urethral infection or intraprostatic reflux [37]. If antibiotics fail to eliminate all bacteria, such as when they do not penetrate the prostate adequately or when treatment is discontinued prematurely, prostatitis may recur and become chronic [38]. Bacteria that persist in the prostate gland have a tendency to re-infect the bladder. Cystitis can also result from a urethral stone obstructing urine flow, preventing the removal of residual bacteria that can rapidly multiply in the bladder, or from a catheter that introduces bacteria into the bladder [4]. Urethritis is an infection of the urethra, which is the tube that carries urine from the bladder to the outside of the body. Symptoms of urethritis typically include pain during urination, a strong urge to urinate, and sometimes discharge (which is more common in men than women) [39]. The most common causes of urethritis are sexually transmitted microorganisms, such as Neisseria, Chlamydia, Herpes simplex virus and Trichomonas [40]. Pyelonephritis is a type of urinary tract infection (UTI) that typically originates in another part of the urinary tract, such as the urethra or bladder, and then spreads to one or both kidneys [41]. In rare cases (about 5%), infections can also spread to the kidneys from other parts of the body through the bloodstream [4]. Pyelonephritis is more common in women than in men and may be milder and more difficult to recognize in children and the elderly [41]. Pyelonephritis risk factors include kidney stones, catheterization, urinary anatomical abnormalities, reflux, diabetes mellitus, enlarged prostate, and pregnancy [6].
2.3. Urinary Tract Infections Caused by Bacteria
Urinary tract infections (UTIs) are caused by both Gram-negative and Gram-positive bacteria [42]. Uropathogenic Escherichia coli is the most common pathogen found in both uncomplicated and complicated urinary tract infections. This bacterium is responsible for at least 80% and 65% of community and hospital-acquired UTIs, respectively [6]. For several decades, it was believed that the bladder and urethra of healthy individuals were sterile or contained too few bacteria to cause infection [43]. However, recent studies have shown evidence of numerous microorganisms in the bladder of adult humans without clinical infection. The relevance and contribution of these microorganisms to health and disease are still under investigation [43,44]. Common pathogens causing UTIs include Enterococcus faecalis, Proteus mirabilis, Klebsiella pneumoniae, Staphylococcus saprophyticus, Group B Streptococcus, Pseudomonas aeruginosa and Staphylococcus aureus [6]. Uropathogens express fimbrial adhesins that bind to glycolipids and glycoproteins on the mucosal-epithelial surface of the host [45]. Adhesins are used by uropathogens to create biofilms on both biotic and abiotic surfaces, enabling them to colonise the mucosa of the urinary tract and indwelling devices such as urinary catheters.[46]. Furthermore, some pathogens secrete substances, such as haemolysin, capsule, proteases, and phospholipases, which aid bacterial invasion by disrupting epithelial integrity [47]. Additionally, certain uropathogens, like UPEC, can invade the host's epithelial cells and replicate within them, creating a reservoir for recurrent infections [48]. This enables the bacteria to colonise and cause UTI. Bacterial virulence factors such as fimbriae, adhesins, P and type 1 pili and others that facilitate bacterial invasion have been described in detail in previous comprehensive reviews (Figure 2) [4,6,45,49].
3. Biofilm formation
Bacterial biofilms are a significant cause of UTIs, accounting for around 65% of nosocomial infections and 80% of all microbial infections [50,51]. Biofilms are communities of microorganisms that permanently attach to biotic or abiotic surfaces and are embedded in their own extracellular matrix [52]. This matrix, known as exopolysaccharides (EPS), consists of several compounds, including polysaccharides, lipids, extracellular DNA, and proteins [53]. The formation of a matrix causes changes in growth rate and gene transcription, resulting in an altered phenotype compared to planktonic counterparts [54]. EPS plays a crucial role in biofilm formation, although its composition varies depending on the bacteria forming the biofilm [55]. It maintains the functional and structural integrity of biofilms, prevents the diffusion of antibiotics to the cell surface of microbes, and protects bacteria in the biofilm from various environmental stresses [56]. Biofilm formation is a multistep process involving reversible and irreversible attachment, production of EPS, biofilm maturation and detachment [57]. The first step in bacterial adhesion is determined by attractive or repulsive forces, such as hydrophobicity, electrostatic interactions, and van der Waals forces [58]. At this stage, planktonic bacteria attach to the surface in a reversible manner, with adhesion being mainly influenced by the surface properties of the substrate [57]. Reversible attachment is typically followed by irreversible attachment, which is mediated by physical appendages of the bacteria, such as fimbriae and pili [59]. This attachment marks the beginning of the evolution of microbes as a biofilm. At this stage, the adhesion process is strengthened by producing EPS, which facilitate aggregation and adhesion, enabling better surface colonisation. EPS composition varies among organisms [60]. For example, E. coli's matrix is primarily composed of colanic acid, while P. aeruginosa's matrix produces alginate as its main capsular polysaccharide [61]. Once bacteria have irreversibly attached to a surface, the biofilm begins to grow and mature [18,57]. The ability of a bacterial biofilm to grow is primarily determined by quorum sensing and is limited by factors such as waste removal and nutrient availability in the surrounding environment [62]. The biofilm grows and matures until it reaches a critical mass, which is characterized by a defined three-dimensional structure, water channels, and considerable thickness [18]. Once mature, microbes detach from the biofilm and return to a planktonic state, enabling them to colonise other surfaces and initiate a new biofilm cycle [63]. Different bacteria use various mechanisms to disperse biofilms, which is a crucial step in their transmission both between and within hosts, facilitating the spread of infection [18,46]. Biofilms are also present inside host cells, where they play a vital role in the development of recurrent urinary infections by creating intracellular bacterial communities (IBCs) that shield bacteria from neutrophils and antibiotics [64]. These structures, which are responsible for chronic cystitis, have been extensively described in uropathogenic E. coli (UPEC) [64]. Biofilms significantly impact human healthcare, as their formation on medical devices is often linked to persistent infections and tolerance to antimicrobial agents [46]. Additionally, medical device-associated infections are among the leading causes of nosocomial infections [65]. Bacterial biofilms have a significant impact on the development of urinary tract infections (UTIs), especially in cases of catheter-associated UTIs (CAUTIs), which account for 40% of all hospital-acquired infections [66]. Biofilms can be developed on urothelium, prostate stones, and implanted biomedical devices by both gram-positive and gram-negative bacteria [46]. The most commonly reported bacteria causing UTIs include E. coli, P. mirabilis, K. pneumoniae, S. epidermidis, S. saprophyticus, S. aureus, and E. faecalis [18]. Proteus mirabilis is a bacterial pathogen that frequently causes both uncomplicated and complicated UTIs, including catheter-associated UTIs (CAUTIs). The pathogen can form biofilms because of virulence factors such as fimbriae, capsules, and ureases (Figure 3) [67]. Urea hydrolysis leads to the formation of ammonium ions, which cause precipitation of magnesium and calcium phosphate crystals [67]. The formation of bacterial biofilms protects bacteria from antimicrobial compounds which are used to coat catheters. The presence of bacterial biofilm on the urothelium can facilitate bacterial invasion of renal tissue, leading to pyelonephritis [6]. Biofilm formation also increases the ability of strains to persist in the prostatic secretory system, leading to recurrent UTIs [68]. Previous studies have shown a clear link between recurrent UTIs and biofilm-producing isolates [68]. In healthy women, biofilm formation by uropathogenic E. coli (UPEC) in the vaginal reservoir has been linked to the majority of recurrent UTIs [69]. Biofilms are known to be more resistant to antimicrobial treatment than planktonic bacterial cells which poses a challenge for removing biofilm from devices [16].
4. The Role of Biofilm in the persistence and recurrence of UTI
Biofilm cells have distinct characteristics compared to planktonic cells, including increased antibiotic resistance and evasion of the innate and adaptive immune response [46]. These characteristics arise from the unique structure of biofilms and the activation of various processes. The high viscosity of the biofilm obstructs the host immune defence system and antimicrobial treatments, contributing to its resistance and persistence [70]. Furthermore, the release of extracellular toxins results in significant tissue damage, leading to an increase in nutrient availability and further consolidation of the biofilm [71]. Asynchronous microbial growth within the biofilm gives rise to variant bacterial phenotypes, such as persister cells, which are inherently resistant to antibiotics [57]. Biofilm-forming bacteria exhibit phenotypic variation, which increases the rate of horizontal gene transfer (HGT). HGT can occur through several mechanisms, including conjugation, transformation, and transduction [72]. It is important to note that while these mechanisms are well-known, they are not the only ones. Recently, a fourth mechanism has been identified, which involves membrane vesicles that transfer antibiotic resistance genes between members of the biofilm community [73]. CAUTIs, caused by bacterial biofilms, are a common type of hospital-acquired infection [66]. Urinary catheters are drainage tubes made of silicone or latex that are inserted into the bladder to collect urine. They are commonly used during or after surgery, to reduce overflow incontinence or to relieve urinary retention [66]. E. coli, Klebsiella pneumoniae and Proteus mirabilis are the most common causes of CAUTIs [74]. Bacteria attach to the surface of the catheter and produce urease, which hydrolyses urea into ammonium ions [75]. This process raises the pH of the urine, resulting in the formation of crystals of magnesium and calcium phosphate. These crystals become part of the growing biofilm, which protects the bacteria from antimicrobial compounds used to coat catheters [76]. Previous studies have shown that patients may develop UTIs within a few days of catheterisation due to the presence of biofilm on urinary catheters [26,66]. Additionally, it has been found that patients who undergo catheterisation for more than 28 days are at a high risk of developing catheter-associated urinary tract infections [17]. Biofilms formed in the initial stages of CAUTI are often colonized by a single species, and subsequently, mixed communities develop, resulting in a thick biofilm that makes antibiotic therapy ineffective [46]. CAUTIs are often caused by gram-negative bacteria, such as E. coli and K. pneumoniae, originating from the patient's perineal microbiota or from the hands of medical professionals [77]. These bacteria can contaminate the urethra and migrate to the bladder, where they create biofilms that act as a reservoir of infection and promote antimicrobial resistance. Catheters increase the risk of UTI because they promote bacterial adherence by damaging the protective mucopolysaccharide layer of the uroepithelium, making it more vulnerable to bacterial invasion [26]. Recent research has shown that enhancing care practices can reduce the incidence of CAUTI and their associated negative outcomes, including higher costs, longer hospital stays, and increased mortality rates, particularly in critical care units [78,79].
5. Resistance of bacteria in biofilm
Antimicrobial resistance may be significantly higher in uropathogens that reside in biofilms, up to 1000 times higher than in planktonic bacteria [80]. Biofilms produced by uropathogens play a crucial role in antimicrobial resistance through several mechanisms. Firstly, antibiotics diffuse inadequately within the biofilm due to the extracellular matrix, causing delayed penetration and reduced effectiveness; (2) bacteria within biofilms exhibit increased expression of efflux pumps compared to planktonic cells, which contributes to their resilient resistance to antibiotics; (3) the close cell-to-cell contact within biofilms facilitates the transmission of antibiotic resistance genes through HGT [16,80]. HGT facilitates the transfer of transposons and other mobile genetic elements between biofilm-forming cells, leading to the dissemination of resistance markers [72]. These markers encode secretion of antibiotic-inactivating enzymes and other virulence factors; 4) The presence of slow-growing intrinsically resistant to antibiotics persister cells that represent a reservoir of surviving cells capable of rebuilding the biofilm population [81]. The effectiveness of antibiotics is often limited by various mechanisms within a biofilm, which in turn drives antimicrobial resistance, a topic that has been extensively investigated in many previous studies [6,16,46].
6. Strategies to Combat Biofilm-Forming Pathogenic Microorganisms in UTI
Given the high levels of antibiotic resistance and the significant contribution to pathogenicity made by microbial biofilms, particularly those formed on catheters in hospitalised patients, there is an urgent need to develop strategies to inhibit uropathogenic biofilms in UTI [66]. Although antibacterial drugs can often stop early biofilm formation, once established, biofilms are difficult to eradicate with traditional antibiotic treatments [63,82]. In recent years, a variety of natural and synthetic agents, as well as nanotechnology-based approaches, have been used in clinical settings to disrupt mature biofilms [83]. The following section discusses the most promising strategies for eradicating biofilms.
6.1. Effectiveness of Anti-Microbial Peptides (AMPs) Against Biofilm Formation
Antimicrobial peptides (AMPs) are small peptides that exhibit anti-biofilm activity against both Gram-positive and Gram-negative bacteria that cause UTIs [84]. Several peptides have been shown to prevent bacterial biofilm formation through various mechanisms, including depolarisation and subsequent disruption of cell membranes, which allows better penetration of biofilm-inhibiting agents [82]. AMPs not only disrupt membranes but also inhibit biofilm formation and adhesion by degrading extracellular polymeric substances, disrupting cell communication, and down-regulating genes responsible for biofilm formation [85]. The antimicrobial properties of AMPs have been extensively studied against various bacteria. Table 2 presents the most well-defined antimicrobial properties of AMPs against different gram-positive and negative bacteria.
6.2. QS-inhibitors
Quorum sensing (QS) is a cell-to-cell signalling mechanism that enables bacteria to release small signalling molecules called autoinducers that regulate gene expression involved in virulence and biofilm formation [95]. Several QS-Inhibitors of both natural and synthetic origins have been identified. Blocking QS receptors by downregulation of the autoinducer synthetase encoding gene is one mechanism by which a large group of inhibitors, such as glyptins, exert their activity [96,97]. Phytochemicals from traditional medicinal plants, such as terpenoids, phenols, essential oils, alkaloids, polyacetylene and lectins, are among the anti-biofilm agents that act by blocking the quorum-sensing inducers of bacteria [98,99]. However, bacteria can develop resistance to phytochemicals through various mechanisms. Therefore, these products are effectively used in combination with traditional antibiotics to eradicate microbial biofilms [99].
6.3. Biofilm Inhibition by Nanoparticles
Nanoparticles, which are less than 100 nm in size, exhibit unique biological activities and have been reported to be effective in treating biofilm-resistant urinary tract infections [100]. Due to their small size, nanoparticles can penetrate cells and deposit ultra-thin coatings on various materials. Previous studies have shown that silver (Ag), nickel (Ni), zinc oxide (ZnO), gold (Au) and copper (Cu) nanoparticles possess significant antibiofilm properties [101]. In addition, modifying the surface of nanoparticles with appropriate capping agents can enhance their interaction with biofilms [83]. When nanoparticles (NPs) are introduced into physiological fluids, they become coated by proteins, forming a protein corona (PC) that modifies their physicochemical properties, including size, charge, and functionality. Recent studies have shown that modifying NPs with an organic corona can improve their interaction with biofilms [102]. Nanotechnology provides significant benefits in treating urinary tract infections by enabling controlled and sustained drug release. When combined with magnetic nanoparticles, macrolides - the primary drugs used to treat biofilm-related infections - exhibit significantly enhanced antimicrobial activity [103]. Table 3 displays the nanoparticles that have demonstrated effectiveness against biofilm-forming bacteria that cause urinary tract infections.
Metal nanoparticles have been shown to inhibit biofilm formation by bacteria that cause UTIs through various mechanisms, such as damaging bacterial DNA or cell membranes, causing component leakage, and oxidizing constituents by generating reactive oxygen species (ROS) [109]. In addition to drug delivery, many NPs can be used to impregnate medical devices due to their biocompatibility and innate antimicrobial activity that prevents the formation of biofilms [110].
6.4. Bacteriophages therapy for treating UTIs
In recent years, there has been renewed interest in bacteriophages as potential agents to combat antibiotic-resistant and chronic urinary tract infections [111]. Bacteriophages are highly specific in targeting bacteria, safe (as they do not infect eukaryotic cells), lack bacterial resistance mechanisms, and have potential for easy incorporation into hydrogel-coated catheters [112]. The use of bacteriophages as agents to destroy bacterial biofilm is therefore a promising resource. However, the broader use of phage therapy in humans has been limited by the requirement for specific authorizations [113].
7. Discussion and Conclusions
Among the infectious diseases associated with the presence of biofilm, those of the urinary tract are especially important. Although the urinary tract has natural antimicrobial host defenses, such as urine flow, urinary pH, polymorphonucleate mediated inflammatory response, and the presence of bacterial adhesion inhibitors, most uropathogens are able to attach to, colonize, and form biofilms in the urinary tract due to the presence of several virulence factors, including adhesins. Over the last two decades, the frequent use of antibiotics for the treatment of infections associated with biofilms has led to a steady and progressive increase in virulent and antibiotic-resistant bacteria that cannot be eradicated by traditional antibiotic treatment. In biofilms, resistance to conventional antimicrobials is mainly due to the inability of these molecules to reach the persister cells within the biofilm. These cells are also resistant to antimicrobials due to their low metabolic activity. They are not mutants, but rather phenotypic variants of the wild type that become active and rebuild the biofilm when antibiotic treatment is stopped. Previous research has demonstrated that biofilm can impede the effectiveness of antimicrobial agents, either by obstructing or delaying their spread or by chemically interacting with the antibiotics. The high levels of antibiotic resistance that characterises biofilms are largely due to the exopolysaccharide matrix that represents one of the key elements in the establishment and maintenance of the biofilm integrity. For example, lysing alginate, the main component of the extracellular matrix of the biofilm formed by P. aeruginosa, facilitates the diffusion of antimicrobial substances, suggesting that the matrix polysaccharide of the biofilm is responsible for the resistance of microorganisms to antimicrobial agents. In addition, the level of resistance is also dependent on the stage of development of the biofilm. Studies on P. aeruginosa biofilms at different stages have shown that older, slow-growing biofilms are considerably more resistant to antimicrobial agents than younger, fast-growing ones. Due to the resistance of the biofilm to destruction by a single agent, combination therapy has been proposed in several studies to improve the penetration of existing antimicrobial agents into the rigid structure of the biofilm. For example, the combination of clarithromycin, a macrolide antibiotic, and vancomycin was found to completely eradicate the biofilm formed by Pseudomonas aeruginosa and Staphylococcus sp. and thereby resolve the infection. Bacterial biofilms are the leading cause of healthcare-associated infections in humans, particularly catheter-associated urinary tractitis. While many antibacterial coatings have been developed to prevent biofilm formation on catheter surfaces, including metal ions, nanoparticles, bacteriophages, quorum sensing inhibitors, and bioactive molecules, only a few antifouling coatings have been approved for marketing. Therefore, there is an urgent need for new approaches and strategies to inhibit biofilm formation.
8. Future Directions
Biofilms pose a significant concern in medical device-associated infections. Currently, many efforts are underway to discover new potential candidates to treat or prevent bacteria that form biofilms and cause UTIs. However, it is important to note that the gap between in vitro and in vivo testing has not yet been overcome. Despite considerable interest in various agents that inhibit biofilms in vitro, the current models used to test these agents are unable to recapitulate the conditions of the human bladder, where bacterial biofilm formation occurs. This is because in vitro studies cannot perfectly replicate in vivo conditions. As we gain a better understanding of the antibiotic tolerance mechanisms of the biofilm, our ability to develop drugs that can overcome the bacterial biofilm will improve. It is important to study CAUTI and its different treatment modalities, bearing in mind that there are differences that cannot be ignored.
Author Contributions
Conceptualization, C.B., G.M.; figure and preparation of the original draft, M.T., A.M., G.M., G.V. and S.Z.; proofreading and editing, C.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Maddali, N.; Cantin, A.; Koshy, S.; Eiting, E.; Fedorenko, M. Antibiotic prescribing patterns for adult urinary tract infections within emergency department and urgent care settings. The American journal of emergency medicine 2021, 45, 464–471. [Google Scholar] [CrossRef] [PubMed]
- Brodie, A.; El-Taji, O.; Jour, I.; Foley, C.; Hanbury, D. A Retrospective Study of Immunotherapy Treatment with Uro-Vaxom (OM-89(R)) for Prophylaxis of Recurrent Urinary Tract Infections. Current urology 2020, 14, 130–134. [Google Scholar] [CrossRef]
- Medina, M.; Castillo-Pino, E. An introduction to the epidemiology and burden of urinary tract infections. Therapeutic advances in urology 2019, 11, 1756287219832172. [Google Scholar] [CrossRef] [PubMed]
- Flores-Mireles, A.L.; Walker, J.N.; Caparon, M.; Hultgren, S.J. Urinary tract infections: epidemiology, mechanisms of infection and treatment options. Nature reviews. Microbiology 2015, 13, 269–284. [Google Scholar] [CrossRef] [PubMed]
- Biondo, C. New Insights into the Pathogenesis and Treatment of Urinary Tract Infections. Pathogens 2023, 12. [Google Scholar] [CrossRef]
- Mancuso, G.; Midiri, A.; Gerace, E.; Marra, M.; Zummo, S.; Biondo, C. Urinary Tract Infections: The Current Scenario and Future Prospects. Pathogens 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Goebel, M.C.; Trautner, B.W.; Grigoryan, L. The Five Ds of Outpatient Antibiotic Stewardship for Urinary Tract Infections. Clinical microbiology reviews 2021, 34, e0000320. [Google Scholar] [CrossRef]
- Dadgostar, P. Antimicrobial Resistance: Implications and Costs. Infection and drug resistance 2019, 12, 3903–3910. [Google Scholar] [CrossRef] [PubMed]
- Paul, R. State of the Globe: Rising Antimicrobial Resistance of Pathogens in Urinary Tract Infection. Journal of global infectious diseases 2018, 10, 117–118. [Google Scholar] [CrossRef] [PubMed]
- Walsh, T.R.; Gales, A.C.; Laxminarayan, R.; Dodd, P.C. Antimicrobial Resistance: Addressing a Global Threat to Humanity. PLoS medicine 2023, 20, e1004264. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, G.; Midiri, A.; Zummo, S.; Gerace, E.; Scappatura, G.; Biondo, C. Extended-spectrum beta-lactamase & carbapenemase-producing fermentative Gram-negative bacilli in clinical isolates from a University Hospital in Southern Italy. The new microbiologica 2021, 44, 227–233. [Google Scholar] [PubMed]
- Li, X.; Fan, H.; Zi, H.; Hu, H.; Li, B.; Huang, J.; Luo, P.; Zeng, X. Global and Regional Burden of Bacterial Antimicrobial Resistance in Urinary Tract Infections in 2019. Journal of clinical medicine 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Antimicrobial Resistance, C. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, G.; Midiri, A.; Gerace, E.; Biondo, C. Bacterial Antibiotic Resistance: The Most Critical Pathogens. Pathogens 2021, 10. [Google Scholar] [CrossRef] [PubMed]
- Mlugu, E.M.; Mohamedi, J.A.; Sangeda, R.Z.; Mwambete, K.D. Prevalence of urinary tract infection and antimicrobial resistance patterns of uropathogens with biofilm forming capacity among outpatients in morogoro, Tanzania: a cross-sectional study. BMC infectious diseases 2023, 23, 660. [Google Scholar] [CrossRef] [PubMed]
- Uruen, C.; Chopo-Escuin, G.; Tommassen, J.; Mainar-Jaime, R.C.; Arenas, J. Biofilms as Promoters of Bacterial Antibiotic Resistance and Tolerance. Antibiotics 2020, 10. [Google Scholar] [CrossRef] [PubMed]
- Vestby, L.K.; Gronseth, T.; Simm, R.; Nesse, L.L. Bacterial Biofilm and its Role in the Pathogenesis of Disease. Antibiotics 2020, 9. [Google Scholar] [CrossRef]
- Lila, A.S.A.; Rajab, A.A.H.; Abdallah, M.H.; Rizvi, S.M.D.; Moin, A.; Khafagy, E.S.; Tabrez, S.; Hegazy, W.A.H. Biofilm Lifestyle in Recurrent Urinary Tract Infections. Life 2023, 13. [Google Scholar] [CrossRef] [PubMed]
- Hola, V.; Opazo-Capurro, A.; Scavone, P. Editorial: The Biofilm Lifestyle of Uropathogens. Frontiers in cellular and infection microbiology 2021, 11, 763415. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.W.; Chlebicki, M.P. Urinary tract infections in adults. Singapore medical journal 2016, 57, 485–490. [Google Scholar] [CrossRef]
- Sihra, N.; Goodman, A.; Zakri, R.; Sahai, A.; Malde, S. Nonantibiotic prevention and management of recurrent urinary tract infection. Nature reviews. Urology 2018, 15, 750–776. [Google Scholar] [CrossRef]
- Li, J.; Yu, Y.F.; Qi, X.W.; Du, Y.; Li, C.Q. Immune-related ureteritis and cystitis induced by immune checkpoint inhibitors: Case report and literature review. Frontiers in immunology 2022, 13, 1051577. [Google Scholar] [CrossRef] [PubMed]
- Mahyar, A.; Ayazi, P.; Farzadmanesh, S.; Sahmani, M.; Oveisi, S.; Chegini, V.; Esmaeily, S. The role of zinc in acute pyelonephritis. Le infezioni in medicina 2015, 23, 238–242. [Google Scholar] [PubMed]
- Van Eyssen, S.R.; Samarkina, A.; Isbilen, O.; Zeden, M.S.; Volkan, E. FimH and Type 1 Pili Mediated Tumor Cell Cytotoxicity by Uropathogenic Escherichia coli In Vitro. Pathogens 2023, 12. [Google Scholar] [CrossRef]
- Alelign, T.; Petros, B. Kidney Stone Disease: An Update on Current Concepts. Advances in urology 2018, 2018, 3068365. [Google Scholar] [CrossRef]
- Werneburg, G.T. Catheter-Associated Urinary Tract Infections: Current Challenges and Future Prospects. Research and reports in urology 2022, 14, 109–133. [Google Scholar] [CrossRef] [PubMed]
- Ingram, A.; Posid, T.; Pandit, A.; Rose, J.; Amin, S.; Bellows, F. Risk factors, demographic profiles, and management of uncomplicated recurrent urinary tract infections: a single institution study. Menopause 2021, 28, 943–948. [Google Scholar] [CrossRef] [PubMed]
- Zare, M.; Vehreschild, M.; Wagenlehner, F. Management of uncomplicated recurrent urinary tract infections. BJU international 2022, 129, 668–678. [Google Scholar] [CrossRef] [PubMed]
- Mekonnen, S.A.; El Husseini, N.; Turdiev, A.; Carter, J.A.; Belew, A.T.; El-Sayed, N.M.; Lee, V.T. Catheter-associated urinary tract infection by Pseudomonas aeruginosa progresses through acute and chronic phases of infection. Proceedings of the National Academy of Sciences of the United States of America 2022, 119, e2209383119. [Google Scholar] [CrossRef] [PubMed]
- Guliciuc, M.; Porav-Hodade, D.; Mihailov, R.; Rebegea, L.F.; Voidazan, S.T.; Ghirca, V.M.; Maier, A.C.; Marinescu, M.; Firescu, D. Exploring the Dynamic Role of Bacterial Etiology in Complicated Urinary Tract Infections. Medicina 2023, 59. [Google Scholar] [CrossRef]
- Woodford, H.J.; George, J. Diagnosis and management of urinary infections in older people. Clinical medicine 2011, 11, 80–83. [Google Scholar] [CrossRef] [PubMed]
- Geerlings, S.E. Clinical Presentations and Epidemiology of Urinary Tract Infections. Microbiology spectrum 2016, 4. [Google Scholar] [CrossRef] [PubMed]
- Ebell, M.H.; Gagyor, I. Diagnosis of Urinary Tract Infection in Women. American family physician 2022, 106, 335–336. [Google Scholar] [PubMed]
- Kwok, M.; McGeorge, S.; Mayer-Coverdale, J.; Graves, B.; Paterson, D.L.; Harris, P.N.A.; Esler, R.; Dowling, C.; Britton, S.; Roberts, M.J. Guideline of guidelines: management of recurrent urinary tract infections in women. BJU international 2022, 130 Suppl 3, 11–22. [Google Scholar] [CrossRef]
- Caretto, M.; Giannini, A.; Russo, E.; Simoncini, T. Preventing urinary tract infections after menopause without antibiotics. Maturitas 2017, 99, 43–46. [Google Scholar] [CrossRef] [PubMed]
- Alperin, M.; Burnett, L.; Lukacz, E.; Brubaker, L. The mysteries of menopause and urogynecologic health: clinical and scientific gaps. Menopause 2019, 26, 103–111. [Google Scholar] [CrossRef]
- Lipsky, B.A.; Byren, I.; Hoey, C.T. Treatment of bacterial prostatitis. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America 2010, 50, 1641–1652. [Google Scholar] [CrossRef] [PubMed]
- Le, B.; Schaeffer, A.J. Chronic prostatitis. BMJ clinical evidence 2011, 2011. [Google Scholar]
- Sell, J.; Nasir, M.; Courchesne, C. Urethritis: Rapid Evidence Review. American family physician 2021, 103, 553–558. [Google Scholar]
- Sadoghi, B.; Kranke, B.; Komericki, P.; Hutterer, G. Sexually transmitted pathogens causing urethritis: A mini-review and proposal of a clinically based diagnostic and therapeutic algorithm. Frontiers in medicine 2022, 9, 931765. [Google Scholar] [CrossRef]
- Herness, J.; Buttolph, A.; Hammer, N.C. Acute Pyelonephritis in Adults: Rapid Evidence Review. American family physician 2020, 102, 173–180. [Google Scholar]
- Kline, K.A.; Lewis, A.L. Gram-Positive Uropathogens, Polymicrobial Urinary Tract Infection, and the Emerging Microbiota of the Urinary Tract. Microbiology spectrum 2016, 4. [Google Scholar] [CrossRef] [PubMed]
- Roth, R.S.; Liden, M.; Huttner, A. The urobiome in men and women: a clinical review. Clinical microbiology and infection : the official publication of the European Society of Clinical Microbiology and Infectious Diseases 2023, 29, 1242–1248. [Google Scholar] [CrossRef] [PubMed]
- Colella, M.; Topi, S.; Palmirotta, R.; D'Agostino, D.; Charitos, I.A.; Lovero, R.; Santacroce, L. An Overview of the Microbiota of the Human Urinary Tract in Health and Disease: Current Issues and Perspectives. Life 2023, 13. [Google Scholar] [CrossRef]
- Govindarajan, D.K.; Kandaswamy, K. Virulence factors of uropathogens and their role in host pathogen interactions. Cell surface 2022, 8, 100075. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Mohler, J.; Mahajan, S.D.; Schwartz, S.A.; Bruggemann, L.; Aalinkeel, R. Microbial Biofilm: A Review on Formation, Infection, Antibiotic Resistance, Control Measures, and Innovative Treatment. Microorganisms 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- Qin, S.; Xiao, W.; Zhou, C.; Pu, Q.; Deng, X.; Lan, L.; Liang, H.; Song, X.; Wu, M. Pseudomonas aeruginosa: pathogenesis, virulence factors, antibiotic resistance, interaction with host, technology advances and emerging therapeutics. Signal transduction and targeted therapy 2022, 7, 199. [Google Scholar] [CrossRef]
- Whelan, S.; Lucey, B.; Finn, K. Uropathogenic Escherichia coli (UPEC)-Associated Urinary Tract Infections: The Molecular Basis for Challenges to Effective Treatment. Microorganisms 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- Sarshar, M.; Behzadi, P.; Ambrosi, C.; Zagaglia, C.; Palamara, A.T.; Scribano, D. FimH and Anti-Adhesive Therapeutics: A Disarming Strategy Against Uropathogens. Antibiotics 2020, 9. [Google Scholar] [CrossRef] [PubMed]
- Assefa, M.; Amare, A. Biofilm-Associated Multi-Drug Resistance in Hospital-Acquired Infections: A Review. Infection and drug resistance 2022, 15, 5061–5068. [Google Scholar] [CrossRef]
- Soto, S.M. Importance of Biofilms in Urinary Tract Infections: New Therapeutic Approaches. Advances in Biology 2014, 2014, 13. [Google Scholar] [CrossRef]
- Zhang, K.; Li, X.; Yu, C.; Wang, Y. Promising Therapeutic Strategies Against Microbial Biofilm Challenges. Frontiers in cellular and infection microbiology 2020, 10, 359. [Google Scholar] [CrossRef] [PubMed]
- Di Martino, P. Extracellular polymeric substances, a key element in understanding biofilm phenotype. AIMS microbiology 2018, 4, 274–288. [Google Scholar] [CrossRef]
- Guzman-Soto, I.; McTiernan, C.; Gonzalez-Gomez, M.; Ross, A.; Gupta, K.; Suuronen, E.J.; Mah, T.F.; Griffith, M.; Alarcon, E.I. Mimicking biofilm formation and development: Recent progress in in vitro and in vivo biofilm models. iScience 2021, 24, 102443. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Datta, S.; Narayanan, K.B.; Rajnish, K.N. Bacterial exo-polysaccharides in biofilms: role in antimicrobial resistance and treatments. Journal, genetic engineering & biotechnology 2021, 19, 140. [Google Scholar] [CrossRef]
- Abdalla, A.K.; Ayyash, M.M.; Olaimat, A.N.; Osaili, T.M.; Al-Nabulsi, A.A.; Shah, N.P.; Holley, R. Exopolysaccharides as Antimicrobial Agents: Mechanism and Spectrum of Activity. Frontiers in microbiology 2021, 12, 664395. [Google Scholar] [CrossRef]
- Rather, M.A.; Gupta, K.; Mandal, M. Microbial biofilm: formation, architecture, antibiotic resistance, and control strategies. Brazilian journal of microbiology : [publication of the Brazilian Society for Microbiology] 2021, 52, 1701–1718. [Google Scholar] [CrossRef]
- Li, Y.; Li, X.; Hao, Y.; Liu, Y.; Dong, Z.; Li, K. Biological and Physiochemical Methods of Biofilm Adhesion Resistance Control of Medical-Context Surface. International journal of biological sciences 2021, 17, 1769–1781. [Google Scholar] [CrossRef] [PubMed]
- Oluwole, O.M. Biofilm: Formation and Natural Products' Approach to Control - a Review. African journal of infectious diseases 2022, 16, 59–71. [Google Scholar] [CrossRef]
- Costa, O.Y.A.; Raaijmakers, J.M.; Kuramae, E.E. Microbial Extracellular Polymeric Substances: Ecological Function and Impact on Soil Aggregation. Frontiers in microbiology 2018, 9, 1636. [Google Scholar] [CrossRef] [PubMed]
- Balducci, E.; Papi, F.; Capialbi, D.E.; Del Bino, L. Polysaccharides' Structures and Functions in Biofilm Architecture of Antimicrobial-Resistant (AMR) Pathogens. International journal of molecular sciences 2023, 24. [Google Scholar] [CrossRef] [PubMed]
- Preda, V.G.; Sandulescu, O. Communication is the key: biofilms, quorum sensing, formation and prevention. Discoveries 2019, 7, e100. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.; Zhang, Y.; Lin, S.; Zhang, W.; Shu, G.; Lin, J.; Li, H.; Xu, F.; Tang, H.; Peng, G.; et al. Strategies for Interfering With Bacterial Early Stage Biofilms. Frontiers in microbiology 2021, 12, 675843. [Google Scholar] [CrossRef] [PubMed]
- Sharma, K.; Dhar, N.; Thacker, V.V.; Simonet, T.M.; Signorino-Gelo, F.; Knott, G.W.; McKinney, J.D. Dynamic persistence of UPEC intracellular bacterial communities in a human bladder-chip model of urinary tract infection. eLife 2021, 10. [Google Scholar] [CrossRef]
- Szabo, S.; Feier, B.; Capatina, D.; Tertis, M.; Cristea, C.; Popa, A. An Overview of Healthcare Associated Infections and Their Detection Methods Caused by Pathogen Bacteria in Romania and Europe. Journal of clinical medicine 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Rubi, H.; Mudey, G.; Kunjalwar, R. Catheter-Associated Urinary Tract Infection (CAUTI). Cureus 2022, 14, e30385. [Google Scholar] [CrossRef] [PubMed]
- Yuan, F.; Huang, Z.; Yang, T.; Wang, G.; Li, P.; Yang, B.; Li, J. Pathogenesis of Proteus mirabilis in Catheter-Associated Urinary Tract Infections. Urologia internationalis 2021, 105, 354–361. [Google Scholar] [CrossRef] [PubMed]
- Murray, B.O.; Flores, C.; Williams, C.; Flusberg, D.A.; Marr, E.E.; Kwiatkowska, K.M.; Charest, J.L.; Isenberg, B.C.; Rohn, J.L. Recurrent Urinary Tract Infection: A Mystery in Search of Better Model Systems. Frontiers in cellular and infection microbiology 2021, 11, 691210. [Google Scholar] [CrossRef]
- Terlizzi, M.E.; Gribaudo, G.; Maffei, M.E. UroPathogenic Escherichia coli (UPEC) Infections: Virulence Factors, Bladder Responses, Antibiotic, and Non-antibiotic Antimicrobial Strategies. Frontiers in microbiology 2017, 8, 1566. [Google Scholar] [CrossRef] [PubMed]
- Khan, J.; Tarar, S.M.; Gul, I.; Nawaz, U.; Arshad, M. Challenges of antibiotic resistance biofilms and potential combating strategies: a review. 3 Biotech 2021, 11, 169. [Google Scholar] [CrossRef] [PubMed]
- Abdelhamid, A.G.; Yousef, A.E. Combating Bacterial Biofilms: Current and Emerging Antibiofilm Strategies for Treating Persistent Infections. Antibiotics 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Michaelis, C.; Grohmann, E. Horizontal Gene Transfer of Antibiotic Resistance Genes in Biofilms. Antibiotics 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Tao, S.; Chen, H.; Li, N.; Wang, T.; Liang, W. The Spread of Antibiotic Resistance Genes In Vivo Model. The Canadian journal of infectious diseases & medical microbiology = Journal canadien des maladies infectieuses et de la microbiologie medicale 2022, 2022, 3348695. [Google Scholar] [CrossRef] [PubMed]
- Palusiak, A. Proteus mirabilis and Klebsiella pneumoniae as pathogens capable of causing co-infections and exhibiting similarities in their virulence factors. Frontiers in cellular and infection microbiology 2022, 12, 991657. [Google Scholar] [CrossRef]
- Cortese, Y.J.; Wagner, V.E.; Tierney, M.; Devine, D.; Fogarty, A. Review of Catheter-Associated Urinary Tract Infections and In Vitro Urinary Tract Models. Journal of healthcare engineering 2018, 2018, 2986742. [Google Scholar] [CrossRef] [PubMed]
- Kanti, S.P.Y.; Csoka, I.; Jojart-Laczkovich, O.; Adalbert, L. Recent Advances in Antimicrobial Coatings and Material Modification Strategies for Preventing Urinary Catheter-Associated Complications. Biomedicines 2022, 10. [Google Scholar] [CrossRef] [PubMed]
- Stahlhut, S.G.; Struve, C.; Krogfelt, K.A.; Reisner, A. Biofilm formation of Klebsiella pneumoniae on urethral catheters requires either type 1 or type 3 fimbriae. FEMS immunology and medical microbiology 2012, 65, 350–359. [Google Scholar] [CrossRef] [PubMed]
- Taha, H.; Raji, S.J.; Khallaf, A.; Abu Hija, S.; Mathew, R.; Rashed, H.; Du Plessis, C.; Allie, Z.; Ellahham, S. Improving Catheter Associated Urinary Tract Infection Rates in the Medical Units. BMJ quality improvement reports 2017, 6. [Google Scholar] [CrossRef] [PubMed]
- Van Decker, S.G.; Bosch, N.; Murphy, J. Catheter-associated urinary tract infection reduction in critical care units: a bundled care model. BMJ open quality 2021, 10. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, L.B.; Baral, R.; Khanal, B. Comparative study of antimicrobial resistance and biofilm formation among Gram-positive uropathogens isolated from community-acquired urinary tract infections and catheter-associated urinary tract infections. Infection and drug resistance 2019, 12, 957–963. [Google Scholar] [CrossRef] [PubMed]
- Verderosa, A.D.; Totsika, M.; Fairfull-Smith, K.E. Bacterial Biofilm Eradication Agents: A Current Review. Frontiers in chemistry 2019, 7, 824. [Google Scholar] [CrossRef] [PubMed]
- Mirghani, R.; Saba, T.; Khaliq, H.; Mitchell, J.; Do, L.; Chambi, L.; Diaz, K.; Kennedy, T.; Alkassab, K.; Huynh, T.; et al. Biofilms: Formation, drug resistance and alternatives to conventional approaches. AIMS microbiology 2022, 8, 239–277. [Google Scholar] [CrossRef] [PubMed]
- Sahli, C.; Moya, S.E.; Lomas, J.S.; Gravier-Pelletier, C.; Briandet, R.; Hemadi, M. Recent advances in nanotechnology for eradicating bacterial biofilm. Theranostics 2022, 12, 2383–2405. [Google Scholar] [CrossRef] [PubMed]
- Lopes, B.S.; Hanafiah, A.; Nachimuthu, R.; Muthupandian, S.; Md Nesran, Z.N.; Patil, S. The Role of Antimicrobial Peptides as Antimicrobial and Antibiofilm Agents in Tackling the Silent Pandemic of Antimicrobial Resistance. Molecules 2022, 27. [Google Scholar] [CrossRef] [PubMed]
- Pontes, J.T.C.; Toledo Borges, A.B.; Roque-Borda, C.A.; Pavan, F.R. Antimicrobial Peptides as an Alternative for the Eradication of Bacterial Biofilms of Multi-Drug Resistant Bacteria. Pharmaceutics 2022, 14. [Google Scholar] [CrossRef]
- Okuda, K.; Zendo, T.; Sugimoto, S.; Iwase, T.; Tajima, A.; Yamada, S.; Sonomoto, K.; Mizunoe, Y. Effects of bacteriocins on methicillin-resistant Staphylococcus aureus biofilm. Antimicrobial agents and chemotherapy 2013, 57, 5572–5579. [Google Scholar] [CrossRef] [PubMed]
- Almaaytah, A.; Farajallah, A.; Abualhaijaa, A.; Al-Balas, Q. A3, a Scorpion Venom Derived Peptide Analogue with Potent Antimicrobial and Potential Antibiofilm Activity against Clinical Isolates of Multi-Drug Resistant Gram Positive Bacteria. Molecules 2018, 23. [Google Scholar] [CrossRef] [PubMed]
- Hwang, I.S.; Hwang, J.S.; Hwang, J.H.; Choi, H.; Lee, E.; Kim, Y.; Lee, D.G. Synergistic effect and antibiofilm activity between the antimicrobial peptide coprisin and conventional antibiotics against opportunistic bacteria. Current microbiology 2013, 66, 56–60. [Google Scholar] [CrossRef]
- Xie, Z.; Wei, H.; Meng, J.; Cheng, T.; Song, Y.; Wang, M.; Zhang, Y. The Analogs of Temporin-GHa Exhibit a Broader Spectrum of Antimicrobial Activity and a Stronger Antibiofilm Potential against Staphylococcus aureus. Molecules 2019, 24. [Google Scholar] [CrossRef] [PubMed]
- Park, S.C.; Lee, M.Y.; Kim, J.Y.; Kim, H.; Jung, M.; Shin, M.K.; Lee, W.K.; Cheong, G.W.; Lee, J.R.; Jang, M.K. Anti-Biofilm Effects of Synthetic Antimicrobial Peptides Against Drug-Resistant Pseudomonas aeruginosa and Staphylococcus aureus Planktonic Cells and Biofilm. Molecules 2019, 24. [Google Scholar] [CrossRef]
- de la Fuente-Nunez, C.; Cardoso, M.H.; de Souza Candido, E.; Franco, O.L.; Hancock, R.E. Synthetic antibiofilm peptides. Biochimica et biophysica acta 2016, 1858, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Dosler, S.; Karaaslan, E.; Alev Gerceker, A. Antibacterial and anti-biofilm activities of melittin and colistin, alone and in combination with antibiotics against Gram-negative bacteria. Journal of chemotherapy 2016, 28, 95–103. [Google Scholar] [CrossRef] [PubMed]
- de la Fuente-Nunez, C.; Korolik, V.; Bains, M.; Nguyen, U.; Breidenstein, E.B.; Horsman, S.; Lewenza, S.; Burrows, L.; Hancock, R.E. Inhibition of bacterial biofilm formation and swarming motility by a small synthetic cationic peptide. Antimicrobial agents and chemotherapy 2012, 56, 2696–2704. [Google Scholar] [CrossRef] [PubMed]
- Batoni, G.; Maisetta, G.; Esin, S. Antimicrobial peptides and their interaction with biofilms of medically relevant bacteria. Biochimica et biophysica acta 2016, 1858, 1044–1060. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Gamez, S.; Hochberg, M.E.; van Doorn, G.S. Quorum sensing as a mechanism to harness the wisdom of the crowds. Nature communications 2023, 14, 3415. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Bhatia, S. Quorum Sensing Inhibitors: Curbing Pathogenic Infections through Inhibition of Bacterial Communication. Iranian journal of pharmaceutical research : IJPR 2021, 20, 486–514. [Google Scholar] [CrossRef] [PubMed]
- Duplantier, M.; Lohou, E.; Sonnet, P. Quorum Sensing Inhibitors to Quench P. aeruginosa Pathogenicity. Pharmaceuticals 2021, 14. [Google Scholar] [CrossRef] [PubMed]
- Mishra, R.; Panda, A.K.; De Mandal, S.; Shakeel, M.; Bisht, S.S.; Khan, J. Natural Anti-biofilm Agents: Strategies to Control Biofilm-Forming Pathogens. Frontiers in microbiology 2020, 11, 566325. [Google Scholar] [CrossRef] [PubMed]
- Khameneh, B.; Eskin, N.A.M.; Iranshahy, M.; Fazly Bazzaz, B.S. Phytochemicals: A Promising Weapon in the Arsenal against Antibiotic-Resistant Bacteria. Antibiotics 2021, 10. [Google Scholar] [CrossRef] [PubMed]
- Crintea, A.; Carpa, R.; Mitre, A.O.; Petho, R.I.; Chelaru, V.F.; Nadasan, S.M.; Neamti, L.; Dutu, A.G. Nanotechnology Involved in Treating Urinary Tract Infections: An Overview. Nanomaterials 2023, 13. [Google Scholar] [CrossRef]
- Moradi, F.; Ghaedi, A.; Fooladfar, Z.; Bazrgar, A. Recent advance on nanoparticles or nanomaterials with anti-multidrug resistant bacteria and anti-bacterial biofilm properties: A systematic review. Heliyon 2023, 9, e22105. [Google Scholar] [CrossRef] [PubMed]
- Garcia Vence, M.; Chantada-Vazquez, M.D.P.; Vazquez-Estevez, S.; Manuel Cameselle-Teijeiro, J.; Bravo, S.B.; Nunez, C. Potential clinical applications of the personalized, disease-specific protein corona on nanoparticles. Clinica chimica acta; international journal of clinical chemistry 2020, 501, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Siraj, E.A.; Yayehrad, A.T.; Belete, A. How Combined Macrolide Nanomaterials are Effective Against Resistant Pathogens? A Comprehensive Review of the Literature. International journal of nanomedicine 2023, 18, 5289–5307. [Google Scholar] [CrossRef]
- Bharadwaj, K.K.; Rabha, B.; Pati, S.; Choudhury, B.K.; Sarkar, T.; Gogoi, S.K.; Kakati, N.; Baishya, D.; Kari, Z.A.; Edinur, H.A. Green Synthesis of Silver Nanoparticles Using Diospyros malabarica Fruit Extract and Assessments of Their Antimicrobial, Anticancer and Catalytic Reduction of 4-Nitrophenol (4-NP). Nanomaterials 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Shunmugaperumal, T.; Ramamurthy, S. Assessment of antibiofilm activity of magnesium fluoride nanoparticles-stabilized oil-in-water nanosized emulsion. Drug development and industrial pharmacy 2012. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos Ramos, M.A.; Da Silva, P.B.; Sposito, L.; De Toledo, L.G.; Bonifacio, B.V.; Rodero, C.F.; Dos Santos, K.C.; Chorilli, M.; Bauab, T.M. Nanotechnology-based drug delivery systems for control of microbial biofilms: a review. International journal of nanomedicine 2018, 13, 1179–1213. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Pandit, S.; Beshay, M.; Mokkapati, V.; Garnaes, J.; Olsson, M.E.; Sultan, A.; Mackevica, A.; Mateiu, R.V.; Lutken, H.; et al. Anti-biofilm effects of gold and silver nanoparticles synthesized by the Rhodiola rosea rhizome extracts. Artificial cells, nanomedicine, and biotechnology 2018, 46, S886–S899. [Google Scholar] [CrossRef] [PubMed]
- Alomary, M.N.; Ansari, M.A. Proanthocyanin-Capped Biogenic TiO(2) Nanoparticles with Enhanced Penetration, Antibacterial and ROS Mediated Inhibition of Bacteria Proliferation and Biofilm Formation: A Comparative Approach. Chemistry 2021, 27, 5817–5829. [Google Scholar] [CrossRef] [PubMed]
- Qindeel, M.; Barani, M.; Rahdar, A.; Arshad, R.; Cucchiarini, M. Nanomaterials for the Diagnosis and Treatment of Urinary Tract Infections. Nanomaterials 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Polivkova, M.; Hubacek, T.; Staszek, M.; Svorcik, V.; Siegel, J. Antimicrobial Treatment of Polymeric Medical Devices by Silver Nanomaterials and Related Technology. International journal of molecular sciences 2017, 18. [Google Scholar] [CrossRef]
- Zalewska-Piatek, B.; Piatek, R. Bacteriophages as Potential Tools for Use in Antimicrobial Therapy and Vaccine Development. Pharmaceuticals 2021, 14. [Google Scholar] [CrossRef] [PubMed]
- Amankwah, S.; Abdella, K.; Kassa, T. Bacterial Biofilm Destruction: A Focused Review On The Recent Use of Phage-Based Strategies With Other Antibiofilm Agents. Nanotechnology, science and applications 2021, 14, 161–177. [Google Scholar] [CrossRef] [PubMed]
- Suh, G.A.; Lodise, T.P.; Tamma, P.D.; Knisely, J.M.; Alexander, J.; Aslam, S.; Barton, K.D.; Bizzell, E.; Totten, K.M.C.; Campbell, J.L.; et al. Considerations for the Use of Phage Therapy in Clinical Practice. Antimicrobial agents and chemotherapy 2022, 66, e0207121. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Urinary tract infections (UTIs). UTIs are classified as upper or lower based on their anatomical location. Lower UTIs are further categorised by the specific anatomical part affected, such as urethritis for the urethra, ureteritis for the ureter, and cystitis for the bladder. If microorganisms evade the host's defences and are not promptly eradicated, they can travel from the lower urinary tract to the kidneys and, if left untreated, can lead to pyelonephritis.
Figure 1.
Urinary tract infections (UTIs). UTIs are classified as upper or lower based on their anatomical location. Lower UTIs are further categorised by the specific anatomical part affected, such as urethritis for the urethra, ureteritis for the ureter, and cystitis for the bladder. If microorganisms evade the host's defences and are not promptly eradicated, they can travel from the lower urinary tract to the kidneys and, if left untreated, can lead to pyelonephritis.
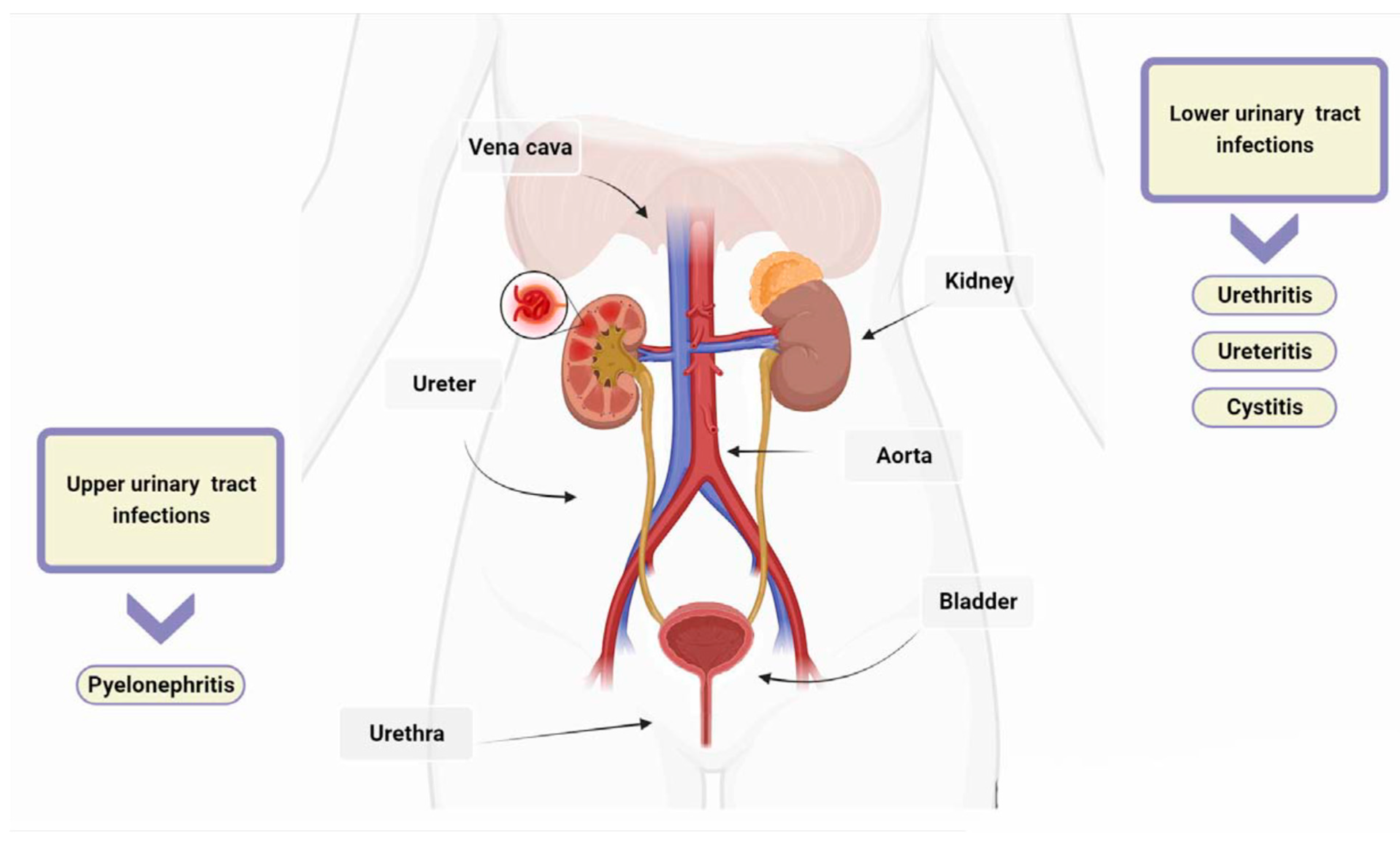
Figure 2.
Biofilms are bacterial formations that occur on urothelial surfaces. The spread and colonisation of uropathogens is facilitated by several virulence factors, including adhesion proteins. The figure displays bacterial adhesins that bind to specific host cell membrane structures, such as glycosphingolipids, sialic acid-containing receptors, glycolipid and mannose receptors, expressed in different tracts of the uroepithelium. Type 1 fimbriae facilitate bacterial adhesion at the proximal and distal tubules, as well as at the level of the collecting duct. Bacteria expressing type 2 and S fimbriae can adhere to various parts of the urinary tract, including the glomeruli, Bowman's capsule, collector duct, proximal and distal tubules. Adhesion is also possible at the level of the bladder, collecting ducts, and distal and proximal tubules through Dr adhesins. Furthermore, bacteria that are able to colonise the bladder, distal tubule, and collector duct express the adhesion protein F1C, which can result in the formation of biofilms.
Figure 2.
Biofilms are bacterial formations that occur on urothelial surfaces. The spread and colonisation of uropathogens is facilitated by several virulence factors, including adhesion proteins. The figure displays bacterial adhesins that bind to specific host cell membrane structures, such as glycosphingolipids, sialic acid-containing receptors, glycolipid and mannose receptors, expressed in different tracts of the uroepithelium. Type 1 fimbriae facilitate bacterial adhesion at the proximal and distal tubules, as well as at the level of the collecting duct. Bacteria expressing type 2 and S fimbriae can adhere to various parts of the urinary tract, including the glomeruli, Bowman's capsule, collector duct, proximal and distal tubules. Adhesion is also possible at the level of the bladder, collecting ducts, and distal and proximal tubules through Dr adhesins. Furthermore, bacteria that are able to colonise the bladder, distal tubule, and collector duct express the adhesion protein F1C, which can result in the formation of biofilms.
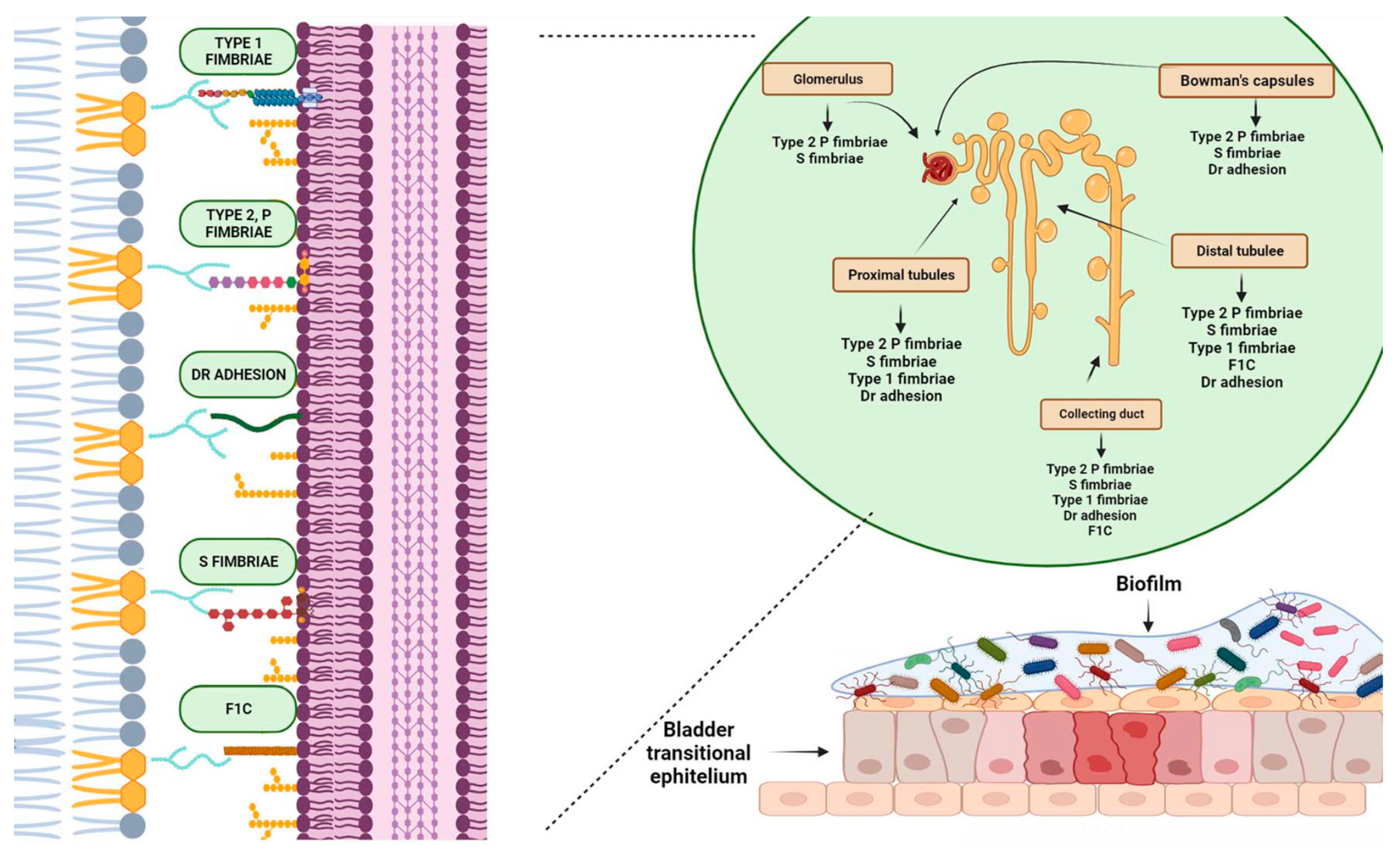
Figure 3.
Antimicrobial resistance and new therapeutic strategies. Bacteria can develop resistance to antimicrobial drugs through various mechanisms, such as using hydrolytic enzymes to deactivate the drug, modifying the target through mutation, increasing the expression of ABC transporters to efflux the drug outside the cell, and forming biofilms on the surface of the uroepithelium and fixed devices, such as catheters, by uropathogens. Bacterial adhesion is facilitated by the inflammatory response of the immune system, which results in the formation of fibrinogen on their surface. The presence of biofilm increases the persistence of microorganisms and their antimicrobial resistance. Antibiotics alone may not always be sufficient to eradicate biofilm. Therefore, alternative treatments such as phagotherapy, enzymatic degradation, the use of antimicrobial peptides and nanoparticles, the development of new antibiotics, and vaccines are currently under investigation.
Figure 3.
Antimicrobial resistance and new therapeutic strategies. Bacteria can develop resistance to antimicrobial drugs through various mechanisms, such as using hydrolytic enzymes to deactivate the drug, modifying the target through mutation, increasing the expression of ABC transporters to efflux the drug outside the cell, and forming biofilms on the surface of the uroepithelium and fixed devices, such as catheters, by uropathogens. Bacterial adhesion is facilitated by the inflammatory response of the immune system, which results in the formation of fibrinogen on their surface. The presence of biofilm increases the persistence of microorganisms and their antimicrobial resistance. Antibiotics alone may not always be sufficient to eradicate biofilm. Therefore, alternative treatments such as phagotherapy, enzymatic degradation, the use of antimicrobial peptides and nanoparticles, the development of new antibiotics, and vaccines are currently under investigation.
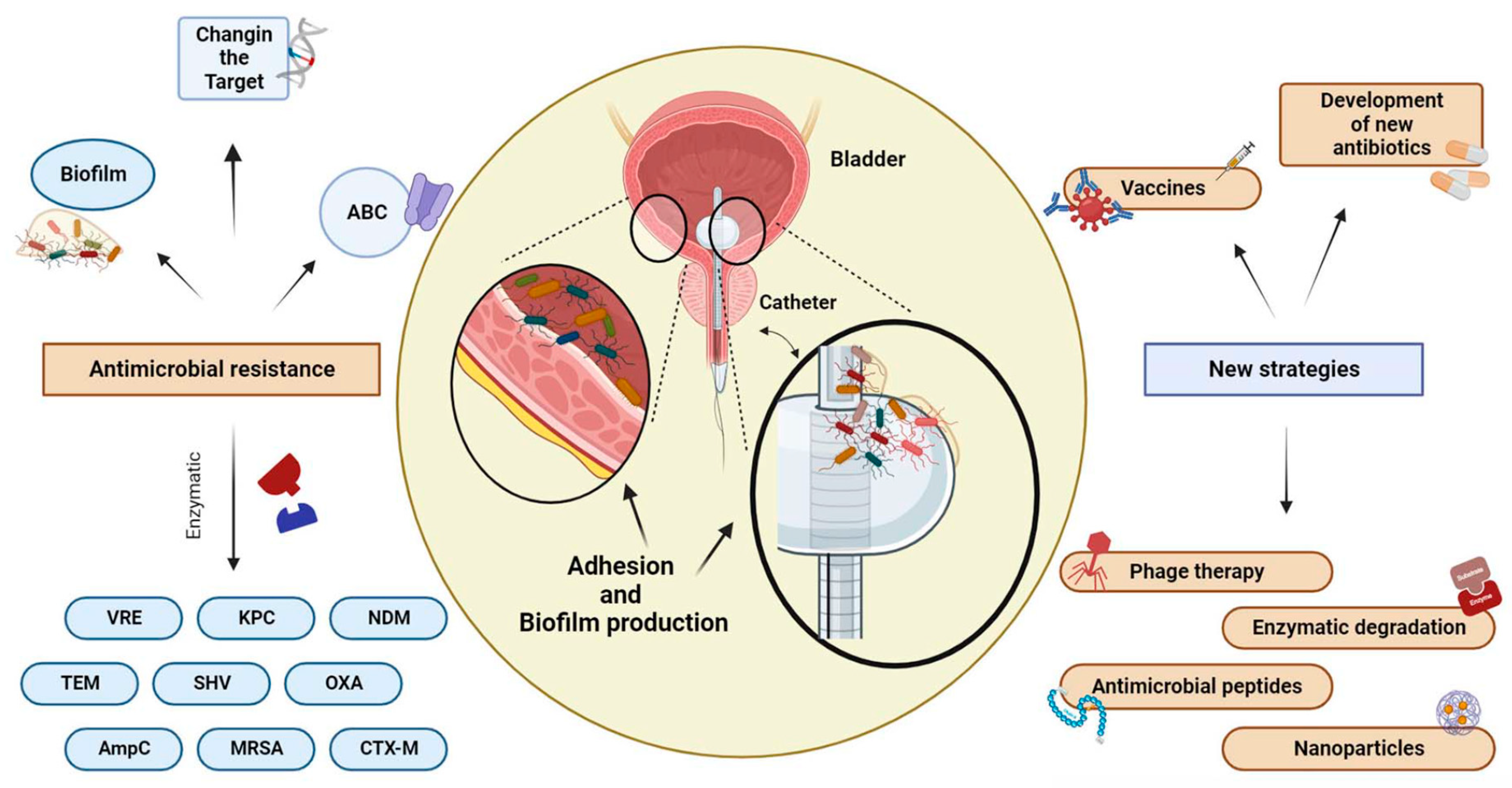

Table 1.
Signs and symptoms of UTIs in different parts of the urinary system.
| Organs of urinary tract | Signs and Symptoms |
|---|---|
| bladder | Dysuria*, blood in urine, frequency*, soprapubic pain |
| urethra | Burning with urination, disharge |
| kidneys | Nausea, vomoting, high fever, back or side pain |
| urethritis | Dysuria*, itching, frequency*, |
*, these symptoms may overlap the clinical presentation of STIs.
Table 2.
Anti-biofilm activity of antimicrobial peptides (AMPs) against bacteria responsible for UTIs.
Table 2.
Anti-biofilm activity of antimicrobial peptides (AMPs) against bacteria responsible for UTIs.
| AMPs | Anti-biofilm activity | Mechanism of action | Reference |
|---|---|---|---|
| Nisin A, Mastoparan | S. aureus | Membrane depolarization | [86] |
| A3 | E. faecalis, S. aureus | 214 | [87] |
| Coprisin | E.coli, S. aureus | 120 | [88] |
| GHaK | S. aureus | Membrane permeabilization | [89] |
| PS1 | P. aeruginossa, S. aureus | EPS production inhibition | [90] |
| DJK 5/6 | E. coli, P. aeruginosa, K. pneumoniae | Cell signal ineruption for biofilm formation | [91] |
| Melittin | E. coli, P. aeruginosa, K. pneumoniae | Membrane permeabilization | [92] |
| LL-37 | P. aeruginosa, S. epidermidis | Preventing the transcription of specific genes necessary for quorum sensing. | [93] |
| Hepcidin | S. epidermidis | Inhibition of EPS production | [94] |
Table 3.
Anti-microbial action of different NPs against biofilm-forming bacteria that cause UTIs.
| NPs | Anti-biofilm activity | Mechanism of action | Reference |
|---|---|---|---|
|
Silver nanoparticles (AgNPs) |
S. aureus, E. coli, P. aeruginosa, P. vulgaris | Nano-Based Drug Delivery | [104] |
| Fluorides based nanoparticles | E. faecalis, S. aureus | inhibit bacterial metabolism | [105] |
|
Polymeric nanoparticles (PNs) |
Gram-positive and Gram-negative bacteria | controlled drug delivery | [106] |
| Zinc-based nanoparticles | E. coli, S. aureus | disrupt membrane integrity | [105] |
| Gold nanoparticles (AuNPs) | P. aeruginossa, E. coli | Targeted drug delivery | [107] |
|
Iron, aluminium oxide, copper oxide, gallium-based NPs |
Gram-positive and Gram-negative bacteria | ROS generation | [108,109] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



