Submitted:
12 January 2024
Posted:
15 January 2024
You are already at the latest version
Abstract
To obtain long-term data on the use of everolimus in patients who underwent liver transplantation for hepatocellular carcinoma, we conducted a retrospective, single-center analysis of adult recipients transplanted between 2013 and 2021. Patients on everolimus-incorporating immunosuppression were matched with those on tacrolimus using an inverse probability of treatment weighting methodology. Two propensity-matched groups of patients were thus compared: 233 (45.6%) receiving everolimus versus 278 (54.4%) on tacrolimus. At a median (interquartile range) follow-up of 4.4 (3.8) years after transplantation, everolimus patients showed a reduced risk of recurrence versus tacrolimus (7.7% versus 16.9%; RR=0.45; P=0.002). At multivariable analysis, microvascular infiltration (HR=1.22; P<0.04) and a higher tumor grading (HR=1.27; P<0.04) were associated with higher recurrence rate while being within Milan criteria at transplant (HR=0.56; P<0.001), a successful pre-transplant downstaging (HR=0.63; P=0.01) and use of everolimus (HR=0.46; P<0.001) had a positive impact on the risk of post-transplant recurrence. EVR patients with earlier drug introduction (30 days; P<0.001), longer treatment duration (P<0.001), and higher drug exposure (5.9ng/mL; P<0.001) showed lower recurrence rates versus TAC. Based on our experience, everolimus provides a reduction of the relative risk of hepatocellular carcinoma recurrence, especially for advanced-stage patients and those with earlier drug administration, higher drug exposure, and longer time on treatment. These data advocate for early everolimus introduction after liver transplantation to reduce the attrition rate consequent to chronic immunosuppression.
Keywords:
liver transplantation
; immunosuppression
; everolimus
; hepatocellular carcinoma
; recurrence
Introduction
Survival after liver transplantation (LT) in the long term is impacted by the complications of chronic immunosuppression (1). Nearly all long-term survivors show diverse co-morbidities, the most frequent being hypertension, chronic kidney dysfunction (CKD), de novo malignancies, diabetes mellitus (DM) and metabolic disease (2). Most of these complications are consequent to the use of calcineurin inhibitors (CNI) (cyclosporine (CyA) and tacrolimus (TAC)), although the impact of surgery, non-immunosuppressive co-medication, recipients’ aging, and native liver disease cannot be underestimated (1,2).
Introduced in clinical practice a decade ago (3-5), everolimus (EVR) is a member of the mammalian target of rapamycin (mTOR) inhibitors (mTORi) together with sirolimus (SRL) and has extensively been studied in pre-clinical studies (6), registration trials (3-5), and real-life clinical practice (7). Although approved for use in combination with tacrolimus (TAC) (3), numerous reports have investigated its administration as a single immunosuppressant. This is especially true for the treatment of CNI-associated nephrotoxicity or the prevention/treatment of post-transplant de novo or recurrent malignancies (8). Several pooled analyses and meta-analyses have shown that incorporating EVR into immunosuppression therapy can lead to an improvement in renal function (9-11). Additionally, it can reduce the risk of post-transplant malignancies and recurrence of hepatocellular carcinoma (HCC) (12). However, there is a large variability in reported outcomes across studies due to differences in patient selection, indications for EVR use, mode of administration and exposure, and study designs.
The antiproliferative profile of EVR makes it an ideal immunosuppressive agent for patients with HCC, especially for recipients with an advanced tumor stage or a higher risk of post-transplant recurrence (8). However, the impact of any immunosuppressive strategy on the risk of post-transplant tumor recurrence is dependent on a complex interplay of tumor-related (i.e., stage at transplantation, response to pre-transplant downstaging, biologic markers), condition-related (i.e., indication to transplantation, native liver disease, severity of liver dysfunction) and treatment-related correlates (i.e., time, mode, and duration of drug administration) (1). To elucidate these interactions in large populations and the long term, we carried out a retrospective analysis at our center on the post-transplant recurrence of HCC in adult LT recipients.
Materials and Methods
Study Design
This was a retrospective, single-center study at an Italian National Health System (NHS)-based liver transplant center.
Population
We conducted a retrospective comparison of two groups of adult HCC patients who underwent primary, whole-size transplantation from deceased brain-dead donors (DCD) at our institution using a 2-tiered approach. Initially, we selected transplant recipients with HCC on explant histology, excluding those with macrovascular tumor portal infiltration and mixed cellular lineage (i.e. hepato-cholangio-hepatocellular carcinoma (CHC-HCC)). We then compared patients who received immunosuppression with EVR to those who received tacrolimus (TAC) with or without mycophenolate derivatives (MPA) between 2013 and 2021.
Primary Exposure
Our primary exposure was the use of EVR alone or in combination with TAC versus TAC (±MPA) in the post-transplant immunosuppressive schedule.
Data Source
For the current study, we used data from the regional transplant authority (CRT, Centro Regionale Trapianti) and the prospectively maintained recipient database of our institution. The CRT data system includes data on all donors, waitlisted candidates, and transplant recipients and provides regular oversight to the integrity, validity, and transparency of the database. The local ethics committee of the University of Pisa (Prot. 0036349/2020) approved all procedures.
Measure Outcomes
Our primary outcome was the cumulative incidence of post-transplant HCC recurrence in patients who received EVR versus TAC. The secondary outcome was overall survival (OS). All these measures were treated as time-to-event occurrences. Data were censored at the time of the event, the last follow-up visit, or December 31st, 2022, whichever came first.
Immunosuppression
In the study period, de novo immunosuppression consisted of a triple/quadruple regimen of anti-CD25 (basiliximab, Simulect®, Novartis, Origgio (VA), Italy), calcineurin inhibitors (CNI), CyA or TAC, steroids (S), and antimetabolites (azathioprine (AZA) or mycophenolic acid (MPA) derivatives) according to era, pre-transplant, intra-operative and post-transplant patient characteristics.
When used for prophylaxis of HCC recurrence or prevention of TAC-related adverse events, EVR (Certican®, Novartis, Origgio (VA), Italy) was introduced ≥1 month after transplant at a dosage of 1.0 mg bid with antimetabolites elimination and stepwise TAC dose reduction, unless otherwise clinically indicated. Prior to EVR introduction, patients were tested for liver function tests (LFT), hematocrit, lipid profile and creatinine/protein ratio. When used in combination schedules, EVR was adjusted to a trough level between 3 and 8 ng/mL and TAC between 3 and 5 ng/mL. When used alone, EVR trough level was between 6 and 10 ng/mL as clinically appropriate. When introduced for TAC-related complications, the time, mode, and dose of EVR were dependent on clinical indications.
Rejection episodes were histologically proved and graded according to the BANFF classification system (13). Treatment of rejection was with steroid boluses for non-HCV patients, while CNI and MMF dose increase/reintroduction were preferred for HCV-RNA positive recipients. In case of refractory rejection episodes, we tested patients for donor-specific and anti-HLA antibodies and used plasmapheresis, intravenous immunoglobulin, or rabbit anti-thymocyte immunoglobulin (rATG) as clinically appropriate. Anti-CMV prophylaxis was administered to recipients without acquired immunity (i.e., D+/R- and D-/R- combinations).
Drug Exposure Assay
EVR exposure was tested in whole blood with the QMS™ Everolimus Immunoassay, a homogeneous particle-enhanced turbidimetric immunoassay based on Quantitative Microparticle System (QMS®) technology. Mean EVR exposure was calculated based on samples obtained at our institution at follow-up visits.
Special Considerations
The transplant procedure, perioperative management, and immunosuppressive schedules changed during the study period according to technological advancements and scientific evidence. Celsior® (IGL, Lissieu, France) was utilized for graft perfusion until 2017 and replaced by Servator C® (SALF, Cenate Sotto (BG), Italy) thereafter. Bypass or the classical technique was standard until 2017.
Pre-Transplant Management of HCC
The diagnosis of HCC was according to the European Association for the Study of Liver Disease (EASL) guidelines (14). Patients within the Barcelona Clinic Liver Cancer (BCLC) stage B (intermediate) were considered for transplantation (15). Pre-transplant downstaging/bridging was indicated for patients with >3 cm tumor mass, those with AFP levels >400 ng/mL, or with segmental portal infiltration. The down-staging technique was agreed upon during tumor board case evaluation and based on tumor size, location, and number of nodules. It consisted of trans-arterial chemoembolization (TACE), radiofrequency/microwave ablation, trans-arterial radioembolization (TARE), or surgery as appropriate. A successful downstaging procedure was associated with regression from beyond to within Milan criteria as per pre-transplant imaging or explant histology.
Cut-Offs and Definitions
Cold ischemia time (CIT) was defined as the time from cross-clamping until removal of the organ from the ice for implantation, and warm ischemia time (WIT) as a time of ischemia during graft implantation. EAD was defined according to Olthoff et al. (16) MELD scores at transplant were recalculated retrospectively based on available laboratory data. HCV recurrence was diagnosed by liver biopsy in the presence of HCV-RNA positivity. HBV infection recurrence was defined as HBsAg (± HBV DNA) reappearance in previously seroconverted patients irrespective of liver function. Renal function was evaluated as an estimated glomerular filtration rate (eGFR) by the Modification of Diet in Renal Disease (MDRD)-4 formula. Chronic kidney dysfunction (CKD) was defined as: a) estimated glomerular filtration rate (eGFR) <60 ml/min/1.73m2 for a post-LT period greater than three months according to Kidney Disease: Improving Global Outcomes (KDIGO) criteria in patients with previous eGFR ≥60ml/min/1.73m2 (17); b) evidence of intrinsic renal disease (proteinuria or kidney disease at ultrasound) (17); or c) presence of end-stage renal disease requiring renal replacement therapy (17). Acute kidney injury (AKI) was defined as doubling of baseline serum creatine (sCr) and/or a ≥50% reduction in eGFR within 14 days (17). Deteriorating renal function was defined as ≥one-grade downward shift in the kidney function category according to the KDIGO classification system (18). A post-transplant diabetes mellitus (PTDM) was defined using the comprehensive American Diabetes Association (ADA) 2018 criteria (19).
Arterial hypertension was defined as the need for medication or blood pressure 140/90 mmHg at two following visits. Dyslipidemia was defined as hypercholesterolemia >220 mg/dL and/or hypertriglyceridemia >200 mg/dL at two following visits. Biliary complications included symptomatic and treated biliary fistula, biliary stones, anastomotic biliary strictures, and posttransplant ischemic-type biliary lesion (ITBL). ITBL was defined as any non-anastomotic stenosis associated with symptoms or signs requiring an endoscopic or surgical procedure without vascular complications.
Statistical Analyses
Initially, 2 groups of patients were extracted from the original population of HCC recipients transplanted at our center between 1996 and 2021 based on the mentioned inclusion criteria. The EVR group included patients who received the drug in their de novo immunosuppressive regimen for prophylaxis of post-transplant tumor recurrence or CNI -related complications other than HCC recurrence (i.e., renal function deterioration). The TAC group included patients who received TAC until complication (i.e., HCC recurrence, renal function deterioration) or the latest follow-up.
To address the non-randomized design of the study, the two groups were balanced using an inverse probability of treatment weighting (IPTW) approach. A propensity score for each patient in the original population was generated. The score was created using a multivariate logistic regression model considering post-transplant HCC recurrence (no/yes) as the dependent variable. Eighteen confounding factors that have clinical significance were chosen to serve as covariates for both DFS and OS: patient sex (20); age (21); HCV (22); diabetes mellitus at transplant (23); CKD at transplant (24); MELD score (25); donor sex (26); donor age (27); cerebrovascular accident (CVA) as donor cause of death (28); use of machine perfusion (MP) (29); CIT (30); pre-transplant tumor stage according to Milan criteria (31); pre-transplant alpha-fetoprotein (AFP) (32); efficacy of pre-transplant downstaging and defined as downstaging from beyond to within Milan criteria (33); tumor stage at histology according to Milan criteria (31-33); G3-G4 tumor grading (34); presence of microvascular infiltration (34), and mean TAC trough level within the first post-transplant month (≤10 ng/mL) (35).
With the intent to reduce the artificial modification of the sample size in the pseudo data, we used stabilized weights (SW) according to the formula:
SW = p/PS for the study group, and SW = (1-p)/(1-PS) for the control group
where p is the probability of etiology without considering covariates and PS is the propensity score. A stabilized approach was preferred not to inflate the sample populations versus the original ones.
Because p-values can be biased from population size, results from the comparisons between covariates subgroups were reported as effect size (Cohen's D value): values lower than |0.1| indicated very small differences between means, values between |0.1| and |0.3| indicated small differences, values between |0.3| and |0.5| indicated moderate differences, and values greater than |0.5| indicated considerable differences.
Multivariable Cox regression analyses were run after the stabilized IPTW to identify the risk factors for HCC recurrence and after LT. Hazard ratios (HR) and 95.0% confidence intervals (CI) were reported for significant variables. Survival analyses were performed using the Kaplan-Meier method, and the log-rank test was adopted to compare the obtained survivals. Variables with a p<0.05 were considered statistically significant.
Finally, after propensity matching, 3 further co-variates were used to explore the impact of EVR administration on the risk of HCC recurrence: (1) timing of EVR introduction; (2) duration of EVR treatment, and (3) EVR whole-blood concentration throughout the study period. Patients were dichotomized according to median values, and sensitivity analyses were performed between recurring and non-recurring patients.
According to their measure and level of distribution, variables were expressed by frequencies and percentages, medians, and interquartile ranges (IQR) or means and standard deviations (SD) as appropriate. Data errors and missingness were identified across the database and solved with specific queries. Missing data were handled with a single imputation method. In detail, a median of nearby points imputation was adopted. The median instead of the mean was adopted due to the skewed distribution of the managed variables. Recurrence-free survival (RFS) was defined as the time (months) from transplant to diagnosis of HCC recurrence. OS was defined as the time from transplantation to either death or last observation.
All statistical analyses and plots were run using the SPSS statistical package version 27.0 (SPSS Inc., Chicago, IL, USA). This study conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution's human research committee and was conducted according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Results
Demographics and Clinical Characteristics of the Original Cohort
A total of 1,019 adult patients transplanted for HCC at our center between 1996 and 2021 were initially considered (Table 1). Among them, 463 (45.4%) received EVR for HCC recurrence prophylaxis or complications other than HCC recurrence, while 556 (54.6%) received CNI (either TAC or CyA) as the primary de novo immunosuppressant until CNI-related adverse events. At a median (IQR) follow-up of 8.7 (8.1) years, 384 (37.6%) patients died, 41 (4.0%) were retransplanted, and 635 (62.3%) were alive. The 1, 5, and 10-year Kaplan-Meier probability (95% CI) of survival was 91% (89-93%) and 90.2% (88-93%), 77% (74-80%), and 75.8% (72-79%), 67% (63-71%) and 65% (61%-70.2%) for patient and graft, respectively.
Table 1 shows the clinical features of the recipients and donors from 1996 to 2021 and before matching. CNI patients were more frequently transplanted before 2013 (66.0% versus 31.7%; P<0.0001), while EVR patients were more frequently beyond Milan criteria (32.8% versus 18.1%; P<0.0001), underwent more frequent pre-transplant downstaging procedures (59.6% versus 62.4%; P=0.01), and showed higher median (IQR) AFP levels before surgery (46.3 (28) versus 4.7 (19) ng/mL; P=0.002). Similarly, the proportion of G3-G4 grading (31.9% versus 25.1%; P=0.01) and microvascular infiltration (39.5% versus 32.7%; P=0.02) were higher in the EVR group.
Stabilized IPTW Effect
To minimize the effect of selection biases caused by the non-randomized design of this retrospective study, the EVR and TAC pseudo-groups were balanced using a stabilized IPTW method. Table 2 illustrates the results of the balancing procedure for the 18 potential confounders. Namely, 7 variables showed very small differences before balancing, 6 small, 4 moderate, and 1 considerable. After IPTW, 14 variables showed very small differences; 3 were small, and one was moderate. The IPTW yielded 2 pseudo-groups, i.e., 233 EVR patients versus 278 on TAC.
Results in the Balanced Groups
After conducting IPTW balancing, Table 3 presents the clinical characteristics of both groups. At a median follow-up of 4.4 (3.8) years after transplantation, the number of deaths, re-transplants, and HCC recurrences were 167 (32.7%), 20 (4.0%), and 65 (12.7%), respectively (Table 4). TAC patients showed higher death (37.8% versus 26.6%; RR=1.41; P=0.007) and HCC recurrence rates (16.9% versus 7.7%; RR=2.2; P=0.002). The main reasons for death in the TAC and EVR groups included HCC recurrence (15.1% versus 6.8%; RR=2.51; p=0.003), HCV recurrence (5.4% versus 6.9%; RR=0.8; P=0.48), infections/sepsis (5.7% versus 5.1%; RR=1.11; P=0.84), and de novo malignancies (3.9% versus 2.1%; RR=1.85; P=0.31) (Table 4).
Re-transplantation
A total of 20 (3.9%) patients were retransplanted (Table 4). The main indication was primary non-function (PNF) of the liver graft, which accounted for 40% of such cases and was followed by ischemic cholangiopathy (30%) and hepatic artery thrombosis (HAT) (15.0%). No significant difference was found in the causes of re-transplantation between the two groups.
HCC Recurrence
HCC recurred at a median (IQR) of 26.1 (48.7) months after transplantation and accounted for 15.1% of deaths in TAC versus 6.8% in EVR patients (RR=2.51; P=0.003). One-third of recurrences were in the liver only, while TAC patients showed more frequent multi-organ involvement (P=0.002) (Table 4).
immunosuppression
Table 5 and Table 6 illustrate the immunosuppressive regimen in the EVR group regarding indication, timing of introduction, duration of treatment, and median exposure. EVR was introduced at a median (IQR) interval post-transplantation of 30 (16) days for a median (IQR) of 46.6 (36.1) months. Median (IQR) EVR whole-blood exposure was 5.8 (1.7) ng/mL.
In the EVR group, patients with HCC recurrence showed later EVR introduction (median (IQR) = 52 (26.4) versus 30 (12) days; P<0.001), shorter duration of treatment (median (IQR) = 47.6 (57.0) versus 69.9 (24.8) months; P<0.001), and lower drug exposure (median (IQR) = 3.65 (0.55) versus 5.9 (1.4) ng/mL; P<0.001) (Table 6).
Risk Factors for Recurrence-Free and Overall Survival
Table 7 illustrates the results of the multivariable analysis of risk factors for OS and RFS in the entire post-IPTW population. A successful pre-transplant downstaging (HR=0.79; P=0.006), being within Milan criteria at transplant (HR=0.67; P<0.001) and at histology (HR=0.78; P=0.02) and use of EVR (HR=0.69; P=0.009) had a positive impact on survival.
As for HCC recurrence, the presence of vascular micro-infiltration (HR=1.22; P=0.04) and higher tumor grading (HR=1.27; P=0.044) had a negative impact on RFS, while a successful pre-transplant downstaging (HR=0.65; P=0.01), being within Milan criteria at transplant (HR=0.56; P=0.01) and at histology (HR=0.68; P=0.012) and use of EVR (HR=0.46; P<0.001) had a positive impact on the probability of tumor-free survival.
Figure 1 illustrates the OS according to Milan criteria at transplant and type of immunosuppressant (EVR versus TAC). All strata comparisons were statistically significant except for EVR Milan-in versus TAC Milan-in patients (log-rank P =0.560). The 1-, 3- and 5-year actuarial OS (95% CI) for EVR patients within the Milan criteria were 98% (93-99%), 89% (82-90%), and 84% (79-88%) versus 98% (94-99%), 89% (83-90%), and 85% (80-87%) for EVR and TAC, respectively (log-rank p=0.506). For patients exceeding the Milan criteria, the OS (95% CI) was 94% (91-96%), 84% (81-86%), and 76% (72-79%) versus 92% (89-94%), 79% (73-80%), and 69% (66-70%) for EVR and TAC, respectively (log-rank p<0.001).
Figure 2 illustrates the RFS according to Milan criteria at transplant and type of immunosuppressant (EVR versus TAC). All strata comparisons were statistically significant (log-rank P <0.001) except for EVR Milan-in versus TAC Milan-in patients (log-rank P=0.205). The actuarial (95% CI) RFS for patients within the Milan criteria was 96% (94-100%), 87% (84-89%) and 82% (77-89%) at 1, 3, and 5 years in the EVR group versus 96% (CI 88-99%), 87% (74-91%) and 80% (72-84%) in the TAC group, respectively (log-rank P=0.205). On the other hand, it was 90% (82-94%), 78% (64-81%), and 68% (57-71%) at 1, 2, and 3 years for EVR patients exceeding the Milan criteria versus 86% (72-90%), 75% (66-84%), and 65% (52-69%) for TAC patients beyond the Milan criteria. (log-rank p<0.001).
Discussion
To the best of our knowledge, this is one of the largest single-center series on the use of EVR in recipients of a liver graft for HCC, and with long-term follow-up data available in the international literature. Despite the expansion of the practice of LT for advanced HCC, information on the impact of EVR or SRL is derived mainly from systematic reviews and meta-analyses incorporating both drugs (11,36-40), with only a few multi-institutional research studies (9,41-43) and real-life clinical series (44-46). Although some authors dispute the advantage of mTORi for the reduction of post-transplant HCC recurrence (43), the overall evidence originating from these studies supports the use of mTORi for patients with HCC, suggesting earlier drug introduction and higher exposure levels to achieve greater antiproliferative activity (46).
Dysregulation of the mTOR pathway is frequently observed in HCC (47). However, transferring this evidence from the in vitro experimental setting to clinical practice is challenging because the overall impact of EVR on post-transplant HCC appears to be dependent on a complex interplay of molecular signaling, tumor cell viability, total tumor volume, plasma, and tumor drug concentration (48). In addition, pre-transplant tumor characteristics, response to adjuvant treatment, type of native liver disease, quality of liver graft, surgery, and immunosuppressive regimens all account for the variable outcomes reported in the literature. One strategy to overcome these limitations is to analyze real-life clinical practice and large data sets with the use of propensity-matching methodologies for the reduction of selection biases. For this reason, we opted for a retrospective comparison of 2 propensity-matched samples of HCC patients with the IPTW methodology.
The analysis revealed that the use of EVR could reduce the risk of HCC recurrence and increase RFS and OS in LT recipients. This was especially true for tumors beyond the Milan criteria and for patients with earlier drug introduction (≤30 days), longer time on treatment (about 5 years), and higher median EVR exposure level (≥5.9ng/mL). In such cases, a twofold reduction of the relative risk of HCC recurrence was observed alongside improved OS. In patients within Milan criteria, the oncological impact of EVR-based immunosuppression is weaker, but the overarching benefits of EVR on renal function deterioration and de novo malignancies suggest its use also in this category of patients.
Transferring these considerations to current clinical practice, however, is not simple.
Earlier EVR administration requires proper patient management due to a reported higher incidence of leukopenia, thrombocytopenia, dyslipidemia, and infections with the use of mTORi versus CNIs, as well as a higher discontinuation rate for patients on higher drug exposure (3,10). This is why the originally recommended exposure levels for EVR monotherapy (i.e., 6-10ng/mL) (3-5) are seldom implemented in clinical practice to avoid concentration-related adverse events. Furthermore, the current focus on immunosuppression minimization has expanded from CNI to include antimetabolites and mTORi alongside increased concerns about transplant recipients’ quality of life (49).
Despite its large number of patients and robust statistical methodology, our study has several limitations. First, its retrospective design does not always allow the granular information that real-practice clinical studies need to produce clinically transferable data. This is especially true for pre-transplant information on tumor clinical course and biology, and limited availability of drug exposure levels for patients with longer follow-ups. Additionally, it included the initial experience with EVR at our center and might inevitably be biased by a learning curve effect in terms of patient selection, drug discontinuation rates, and post-transplant therapeutic strategies for HCC recurrence.
Secondly, we excluded patients with unfavorable tumor characteristics from the current analysis, i.e., neoplastic portal thrombosis, due to its negative impact on RFS and OS and the limited number of cases at our center. Given the clinical expansion of Milan criteria and the introduction of novel neoadjuvant pre-transplant treatments (i.e., immunotherapy), it would be interesting to analyze the relative benefit of EVR-incorporating immunosuppression for this category of high-risk patients.
In conclusion, based on our results, EVR allows us to mitigate the risk of post-transplant HCC recurrence, especially for tumors beyond the Milan criteria and patients with earlier drug introduction, higher drug exposure, and longer time on treatment. These data advocate considering the use of mTORi for patients with HCC to reduce the attrition rate of chronic immunosuppression after LT.
Funding
None.
Conflicts of interest
PDS has served as advisory board member for Novartis, Astellas, and Chiesi. The other authors have no interest to declare.
Abbreviations:
AFP, alpha-fetoprotein.
Anti-HBc, antibody to the hepatitis virus B core antigen.
Anti-HBs, antibody to the hepatitis B surface antigen.
BCLC, Barcelona Clinic Liver Cancer.
BMI, body mass index
CHC, cholangiocarcinoma;
CNI, calcineurin inhibitors.
CyA, cyclosporine.
EASL, European Association for the Study of Liver Disease
eGFR, estimated glomerular filtration rate.
EVR, everolimus.
HBc, hepatitis B core antigen.
HBs, hepatitis B surface antigen.
HBV, hepatitis B virus.
HCC, hepatocellular carcinoma.
HCV, hepatitis C virus.
HR, hazard ratio.
IQR, interquartile range.
LFT, liver function tests.
LT, liver transplantation.
MACE, major adverse cardiovascular events.
MDRD, modified diet and renal disease.
MELD, model for end-stage liver function.
MPA, mycophenolic acid derivatives.
mTOR, mammalian target of rapamycin.
mTORi, mammalian target of rapamycin inhibitors.
OS, overall survival.
PNF, primary non-function.
RFS, recurrence-free survival.
RR, relative risk.
S, steroids.
SD, standard deviation.
SRL, sirolimus.
TAC, tacrolimus.
References
- Di Maira, T.; Little, E.C.; Berenguer, M. Immunosuppression in liver transplant. Best Pract Res Clin Gastroenterol 2020, 46-47, 101681. [Google Scholar] [CrossRef] [PubMed]
- Noble, J.; Terrec, F.; Malvezzi, P.; Rostaing, L. Adverse effects of immunosuppression after liver transplantation. Best Pract Res Clin Gastroenterol, 2021; 54-55, 101762. [Google Scholar]
- De Simone, P.; Nevens, F.; De Carlis, L.; Metselaar, H.J.; Beckebaum, S.; Saliba, F.; et al. Everolimus with Reduced Tacrolimus Improves Renal Function in De Novo Liver Transplant Recipients: A Randomized Controlled Trial. Am J Transplant 2012, 12, 3008–3020. [Google Scholar] [CrossRef] [PubMed]
- Saliba, F.; De Simone, P.; Nevens, F.; De Carlis, L.; Metselaar, H.J.; Beckebaum, S.; et al. Renal function at two years in liver transplant patients receiving everolimus: Results of a randomized, multicenter study. Am J Transplant 2013, 13, 1734–1745. [Google Scholar] [CrossRef] [PubMed]
- Fischer, L.; Saliba, F.; Kaiser, G.M.; De Carlis, L.; Metselaar, H.J.; De Simone, P.; et al. Three-year outcomes in de novo liver transplant patients receiving everolimus with reduced tacrolimus: Follow-up results from a randomized, multicenter study. . Transplantation. 2015, 99, 1455–1462. [Google Scholar] [CrossRef] [PubMed]
- Levy, G.; Schmidili, H.; Punch, J.; Tuttle-Newhall, E.; Mayer, D.; Neuhaus, P.; et al. Safety, tolerability, and efficacy of everolimus in de novo liver transplant recipients: 12- and 36-month results. Liver Transpl 2006, 12, 1640–1648. [Google Scholar] [CrossRef]
- Saliba, F.; Dharancy, S.; Salamé, E.; Conti, F.; Eyraud, D.; Radenne, S.; et al. Time to conversion to an everolimus-based regimen: Renal outcomes in liver transplant recipients from the EVEROLIVER registry. Liver Transpl 2020, 26, 1465–1476. [Google Scholar] [CrossRef] [PubMed]
- De Simone, P.; Fagiuoli, S.; Cescon, M.; De Carlis, L.; Tisone, G.; Volpes, R.; Cillo, U. Use of everolimus in liver transplantation: Recommendations from a working group. Transplantation 2017, 101, 239–251. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.G.; Jeng, L.B.; Saliba, F.; Singh Soin, A.; Lee, W.C.; De Simone, P.; et al. Efficacy and safety of everolimus with reduced tacrolimus in liver transplant recipients: 24-month results from the pooled analysis of 2 randomized controlled trials. Transplantation 2021, 105, 1564–1575. [Google Scholar] [CrossRef]
- Lin, M.; Mittal, S.; Sahebjam, F.; Rana, A.; Sood, G.K. Everolimus with early withdrawal or reduced dose calcineurin inhibitors improves renal function in liver transplant recipients: A systematic review and meta-analysis. Clin Transplant 2017, 31. [Google Scholar] [CrossRef]
- Guan, T.W.; Lin, Y.J.; Ou, M.Y.; Chen, K.B. Efficacy and safety of everolimus treatment on liver transplant recipients: A meta-analysis. Eur J Clin Invest 2019, 49, e13179. [Google Scholar] [CrossRef]
- Yan, X.; Huang, S.; Yang, Y.; Lu, Z.; Li, F.; Jiang, L.; et al. Sirolimus or everolimus improves survival after liver transplantation for hepatocellular carcinoma: A systematic review and meta-analysis. Liver Transpl 2022, 28, 1063–1077. [Google Scholar] [CrossRef]
- [No authors listed] Banff schema for grading liver allograft rejection: An international consensus document. Hepatology 1997, 25, 658–663. [CrossRef]
- EASL-EORTC clinical practice guidelines: Management of hepatocellular carcinoma. J Hepatol 2012, 56, 908–943. [CrossRef] [PubMed]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, A.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J Hepatol 2022, 76, 681–693. [Google Scholar] [CrossRef]
- Olthoff, K.M.; Kulik, L.; Samstein, B.; Kaminski, M.; Abecassis, M.; Emond, J.; Shaked, A.; Christie, J.D. Validation of a current definition of early allograft dysfunction in liver transplant recipients and analysis of risk factors. Liver Transpl 2010, 16, 943–949. [Google Scholar] [CrossRef] [PubMed]
- KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney International Supplements 2012, 2, 1–141.
- Tonon, M.; Rosi, S.; Gambino, C.G.; Piano, S.; Calvino, V.; Romano, A.; Martini, A.; Pontisso, P.; Angeli, P. Natural history of acute kidney disease in patients with cirrhosis. J Hepatol 2021, 74, 578–583. [Google Scholar] [CrossRef]
- Diabetes Standards of Care: ADA guidelines (2018). Available at: http://diabetesed.net/wp-content/uploads/2017/12/2018-ADA-Standards-of-Care.pdf. Accessed 1st September 2023.
- Tejada, S.; Martinez-Revejo, R.; Nogueira, T.A.; Gòmez, A.; Pont, T.; Liao, X.; et al. The effect of sex inequality on solid organ transplantation: A systematic review and meta-analysis. Eur J Int Med 2023, 109, 58–67. [Google Scholar] [CrossRef]
- Gil, E.; Kim, J.M.; Jeon, K.; Park, H.; Kang, D.; Cho, J.; Suh, G.Y.; Park, H. Recipient age and mortality after liver transplantation: A population-based cohort study. Transplantation 2018, 102, 2025–2032. [Google Scholar] [CrossRef]
- Bhamidimarri, K.R.; Satapathy, S.K.; Martin, P. Hepatitis C virus and liver transplantation. Gastroenterol Hepatol (N Y) 2017, 13, 214–220. [Google Scholar]
- Brodosi, L.; Petta, S.; Petroni, M.L.; Marchesini, G.; Morelli, M.C. Management of diabetes in candidates for liver transplantation and in transplant recipients. Transplantation 2022, 106, 462–478. [Google Scholar] [CrossRef]
- Cullaro, G.; Verna, E.C.; Lee, B.P.; Lai, J.C. Chronic Kidney Disease in Liver Transplant Candidates: A rising burden impacting post-liver transplant outcomes. Liver Transpl 2020, 26, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Avolio, A.W.; Franco, A.; Schlegel, A.; Lai, Q.; Meli, S.; Burra, P.; et al. Development and validation of a comprehensive model to estimate early allograft failure among patients requiring early liver retransplant. JAMA Surg 2020, 155, e204095. [Google Scholar] [CrossRef]
- Sarkar, M.; Watt, K.D.; Terrault, N.; Berenguer, M. Outcomes in liver transplantation: Does sex matter? J Hepatol 2015, 62, 946–955. [Google Scholar] [CrossRef]
- Kanneganti, M.; Olthoff, K.M.; Bittermann, T. Impact of older donor age on recipient and graft survival after LDLT: The US Experience. Transplantation 2023, 107, 162–171. [Google Scholar] [CrossRef]
- Singhal, A.K.; Sheng, X.; Drakos, S.G.; Stehlik, J. Impact of donor cause of death on transplant outcomes: UNOS registry analysis. Transplant Proc 2009, 41, 3539–3544. [Google Scholar] [CrossRef]
- Tingle, S.J.; Dobbins, J.J.; Thompson, E.R.; Figueiredo, R.S.; Mahendran, B.; Pandanaboyana, S.; Wilson, C. Machine perfusion in liver transplantation. Cochrane Database of Systematic Reviews 2023, Issue 9. Art. No.: CD014685. [CrossRef]
- Figiel, W.; Smoter, P.; Krasnodębski, M.; Rykowski, P.; Morawski, M.; Grąt, M.; Patkowski, W.; Zieniewicz, K. Predictors of long-term outcomes after liver transplantation depending on the length of cold ischemia time. Transpl Proc 2022, 54, 1025–1028. [Google Scholar] [CrossRef]
- Lingiah, V.A.; Niazi, M.; Olivo, R.; Paterno, F.; Guarrera, J.V.; Pyrsopoulos, N.T. Liver transplantation beyond Milan criteria. J Clin Transl Hepatol 2020, 8, 69–75. [Google Scholar] [CrossRef]
- Duvoux, C.; Roudot-Thoraval, F.; Decaens, T.; Pessione, F.; Badran, H.; Piardi, P.; et al. Liver transplantation for hepatocellular carcinoma: A model including α-fetoprotein improves the performance of Milan criteria. Gastroenterology 2012, 143, 986–994. [Google Scholar] [CrossRef] [PubMed]
- Mehta, N.; Guy, J.; Frenette, C.T.; Dodge, J.L.; Osorio, R.W.; Minteer, W.B.; Roberts, J.P.; Yao, F.Y. Excellent outcomes of liver transplantation following down-staging of hepatocellular carcinoma to within Milan criteria: A multicenter study. Clin Gastroenterol Hepatol 2018, 16, 955–964. [Google Scholar] [CrossRef]
- Jonas, S.; Bechstein, W.O.; Steinmueller, T.; Hermann, M.; Radke, C.; Berg, T.; Settmacher, U.; Neuhaus, P. Vascular invasion and histopathologic grading determine outcome after liver transplantation for hepatocellular carcinoma in cirrhosis. Hepatology 2001, 33, 1080–1086. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Perálvarez, M.; Tsochatzis, E.; Naveas, M.C.; Pieri, G.; García-Caparrós, C.; O'Beirne, J.; et al. Reduced exposure to calcineurin inhibitors early after liver transplantation prevents recurrence of hepatocellular carcinoma. J Hepatol 2013, 59, 1193–1199. [Google Scholar] [CrossRef] [PubMed]
- Aloun, A.; Abu-Zeid, E.E.D.; Garzali, I.U. Does mTORi based immunosuppression offer survival advantage after liver transplantation for hepatocellular carcinoma? Systematic review and meta-analysis of randomized controlled trials. Hepatol Forum 2023, 4, 82–88. [Google Scholar] [PubMed]
- Zhang, G.; Duan, B.; Li, G. mTORi-based immunosuppression reduces HCC recurrence at the expenses of increased adverse side effects: A systematic review and meta-analysis. Clin Transplant 2022, 36, e14823. [Google Scholar] [CrossRef] [PubMed]
- Grigg SE, Sarri GL, Gow PJ; Yeomans ND. Systematic review with meta-analysis: Sirolimus- or everolimus-based immunosuppression following liver transplantation for hepatocellular carcinoma. Aliment Pharmacol Ther 2019, 49, 1260–1273.
- Tarantino, G.; Magistri, P.; Ballarin, R.; Di Francia, R.; Berretta, M.; Di Benedetto, F. Oncological impact of mTOR inhibitor immunosuppressive therapy after liver transplantation for hepatocellular carcinoma: Review of the literature. Front Pharmacol 2016, 7, 387. [Google Scholar] [CrossRef] [PubMed]
- Holdaas, H.; De Simone, P.; Zuckermann, A. Everolimus and malignancy after solid organ transplantation: A clinical update. J Transplant 2016, 2016, 4369574. [Google Scholar] [CrossRef] [PubMed]
- Geissler, E.K.; Schnitzbauer, A.A.; Zülke, C.; Lamby, P.E.; Proneth, A.; Duvoux, C.; et al. Sirolimus use in liver transplant recipients with hepatocellular carcinoma: A randomized, multicenter, open-label Phase 3 trial. Transplantation 2016, 100, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Sapisochin, G.; Lee, W.C.; Joo Dj Joh, J.W.; Hata, K.; Soin, A.S.; et al. Long-term effects of everolimus-facilitated tacrolimus reduction in living donor liver transplant recipients with hepatocellular carcinoma. Ann Transplant 2022, 27, e937988. [Google Scholar] [CrossRef]
- Rodriguez-Peralvarez, M.; Guerrero, M.; Barrera, L.; Ferrin, G.; Alamo, J.M.; et al. Impact of early initiated everolimus on the recurrence of hepatocellular carcinoma after liver transplantation. Transplantation 2018, 102, 2056–2064. [Google Scholar] [CrossRef]
- Kang, I.; Lee, J.G.; Choi, S.H.; Kim, H.J.; Han, D.H.; Choi, G.H.; et al. Impact of everolimus on survival after liver transplantation for hepatocellular carcinoma. Clin Mol Hepatol 2021, 27, 589–602. [Google Scholar] [CrossRef] [PubMed]
- Wasilewicz, M.P.; Moczydlowska, D.; Janik, M.; Grat, M.; Zienewicz, K.; Raszeja-Wyszomirska, J. Immunosuppressive treatment with everolimus in patients after liver transplant: 4 years of single-center experience. Pol Arch Intern Med 2019, 129, 686–691. [Google Scholar] [PubMed]
- Cholongitas, E.; Antoniadis, N.; Goulis, I.; Theocharidou, E.; Imvrios, G.; Giouleme, O.; et al. Trough levels of everolimus are associated with recurrence rates of hepatocellular carcinoma after liver transplantation. Transplant Proc 2019, 51, 450–453. [Google Scholar] [CrossRef] [PubMed]
- Engl, T.; Rutz, J.; Maxeiner, S.; Juengel, E.; Roos, F.; Khoder, W.; et al. mTOR inhibition reduces growth and adhesion of hepatocellular carcinoma in vitro. Mol Med Rep 2017, 16, 7064–7071. [Google Scholar] [CrossRef] [PubMed]
- Ande, A.; Chaar, M.; Ait-Oudhia, S. Multiscale systems pharmacological analysis of everolimus action in hepatocellular carcinoma. J Pharmacokinet Pharmacodyn 2018, 45, 607–620. [Google Scholar] [CrossRef]
- Cillo, U.; De Carlis, L.; Del Gaudio, M.; De Simone, P.; Fagiuoli, S.; Lupo, F.; Tisone, G.; Volpes, R. Immunosuppressive regimens for adult liver transplant recipients in real-life practice: Consensus recommendations from an Italian working group. Liver Int 2020, 146, 930–943. [Google Scholar] [CrossRef]
Figure 1.
Kaplan-Meier probability of post-transplant overall patient survival according to everolimus (EVR) versus tacrolimus (TAC) and Milan stage at transplantation. All strata comparisons were statistically significant (log-rank p <0.001) except Milan-in on EVR versus Milan-in on TAC (log-rank P=0.506).
Figure 1.
Kaplan-Meier probability of post-transplant overall patient survival according to everolimus (EVR) versus tacrolimus (TAC) and Milan stage at transplantation. All strata comparisons were statistically significant (log-rank p <0.001) except Milan-in on EVR versus Milan-in on TAC (log-rank P=0.506).
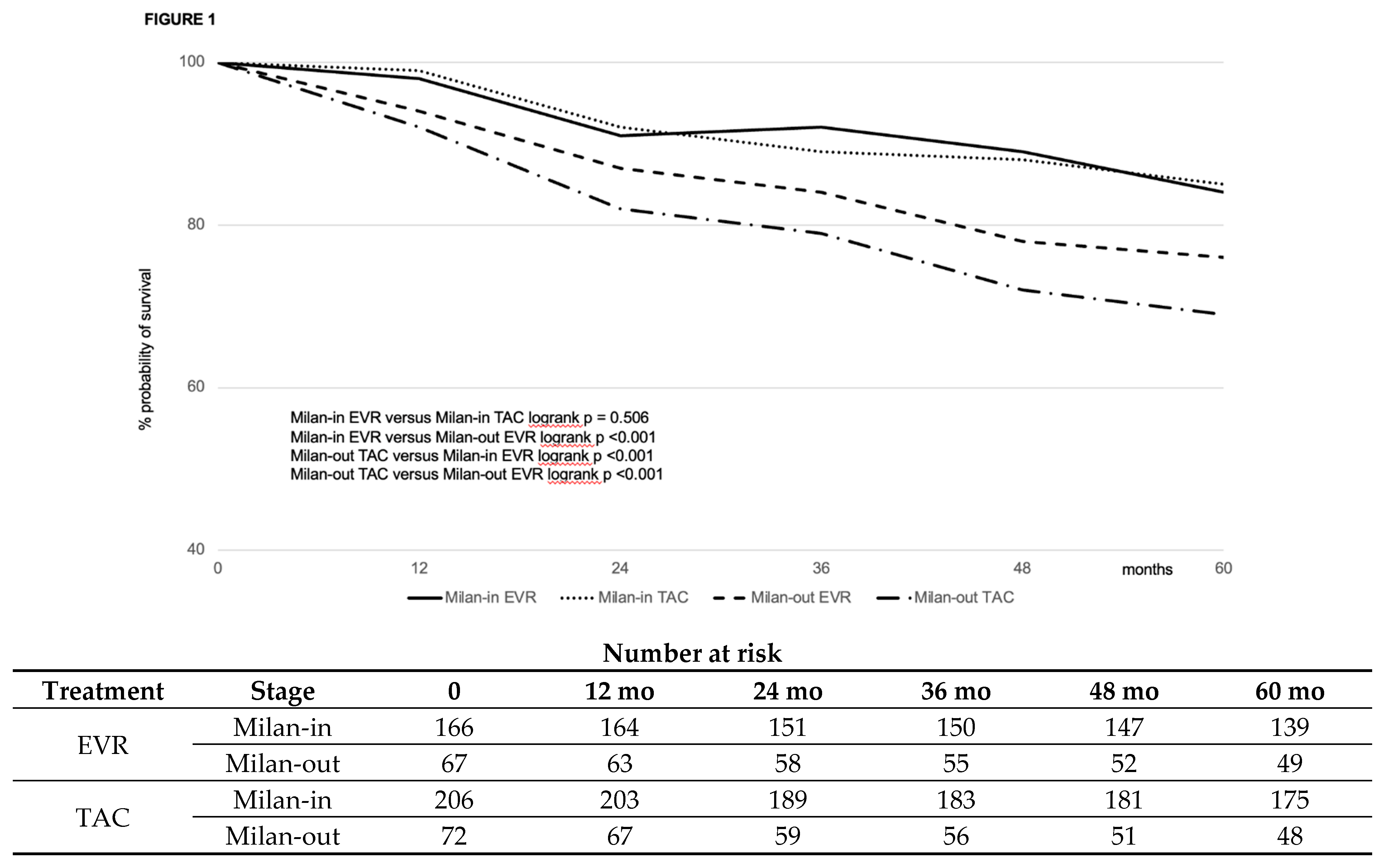
Figure 2.
Kaplan-Meier probability of post-transplant recurrence-free survival according to everolimus (EVR) versus tacrolimus (TAC) and Milan stage at transplantation. All strata comparisons were statistically significant (log-rank p <0.001) except Milan-in on EVR versus Milan-in on TAC (log-rank P=0.205).
Figure 2.
Kaplan-Meier probability of post-transplant recurrence-free survival according to everolimus (EVR) versus tacrolimus (TAC) and Milan stage at transplantation. All strata comparisons were statistically significant (log-rank p <0.001) except Milan-in on EVR versus Milan-in on TAC (log-rank P=0.205).
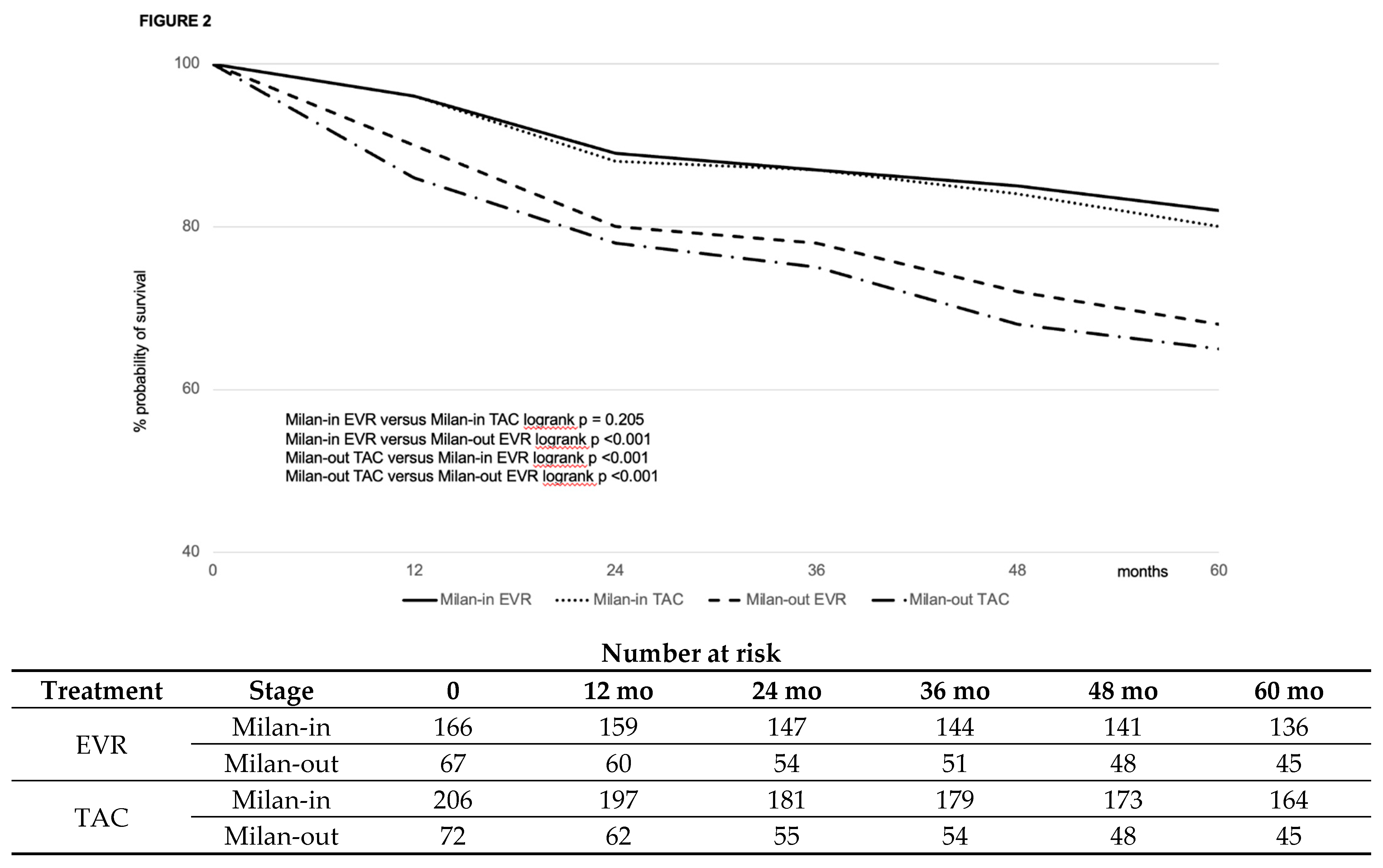

Table 1.
demographic and clinical characteristics of interest of the population of patients with HCC transplanted between 1996 and 2021 at our center.
Table 1.
demographic and clinical characteristics of interest of the population of patients with HCC transplanted between 1996 and 2021 at our center.
| Variable | EVR (#463) | CNI (#556) | P |
|---|---|---|---|
| RECIPIENT | |||
| Male sex, n (%) | 386 (83.4) | 487 (87.6) | 0.55 |
| Age at transplant (median, IQR), years | 56 (10) | 56 (10) | 0.28 |
| Indication to transplant, n (%) HCV HBV (±HDV) HCV-HBV(±HDV) Alcohol NAFLD Autoimmune/PSC |
237 (55.5) 123 (26.5) 17 (3.7) 54 (11.6) 20 (4.3) 12 (5.2) |
294 (52.8) 153 (27.5) 20 (3.5) 59 (9.5) 24 (4.3) 6 (1.1) |
0.59 0.73 0.94 0.59 0.99 0.67 |
| Lab-MELD at transplant (median, IQR) | 7 (6) | 8 (7) | 0.45 |
| DM at transplant, n (%) | 113 (24.4) | 144 (25.8) | 0.58 |
| CKD at transplant, n (%) | 27 (5.8) | 39 (7.0) | 0.44 |
| Hypertension at transplant, n (%) | 69 (14.9) | 76 (13.6) | 0.57 |
| <2013, n (%) | 147 (31.7) | 387 (66.0) | <0.0001 |
| TAC, n (%) | 403 (86.8) | 313 (56.3) | <0.0001 |
| Mean TAC exposure >10 ng/mL within the first month post-transplantation | 127 (27.4) | 172 (31.0) | 0.22 |
| DONOR | |||
| Male sex, n (%) | 241 (52.0) | 281 (50.5) | 0.63 |
| Age, median (IQR) | 69 (25) | 67 (26) | 0.78 |
| ICU stay, median (IQR) days | 3 (4) | 3 (4) | 0.67 |
| CVA as cause of death, n (%) | 333 (71.9) | 411 (73.9) | 0.47 |
| Anti-HCV-positive, n (%) | 4 (0.86) | 0 (0) | 0.58 |
| Anti-HBc-positive, n (%) | 60 (12.9) | 77 (13.8) | 0.67 |
| Cardiac arrest episodes, n (%) | 43 (9.3) | 42 (7.5) | 0.31 |
| Use of inotropes, n (%) | 407 (87.9) | 483 (86.8) | 0.62 |
| HCC | |||
| Tumor nodules*, median (IQR) | 2 (1) | 2 (1) | 0.78 |
| Largest nodule size*, median (IQR) (mm) | 28 (18) |
25 (15) |
0.04 |
| Total tumor size*, median (IQR) (mm) | 39.5 (25) |
36.5 (36) |
0.003 |
| Exceeding Milan criteria at transplant *, n (%) | 152 (32.8) | 101 (18.1) | <0.0001 |
| Pre-transplant treatment, n (%) None, n (%) TACE, n (%) RFA/MW, n (%) PEI, n (%) Resection, n (%) TACE + RFA/MW, n (%) TARE, n (%) Successful downstage**, n (%) |
141 (30.4) 229 (49.4) 33 (7.1) 6 (1.3) 6 (1.3) 42 (9.1) 6 (1.3) 75 (16.2) |
209 (37.6) 307 (55.2) 22 (3.9) 12 (2.1) 4 (0.7) 2 (0.5) 0 (0) 45 (8.1) |
0.01 0.06 0.02 0.29 0.35 <0.0001 0.008 0.0006 |
| AFP at transplant, median (IQR) (ng/mL) | 46.3 (28) |
4.7 (19) |
0.002 |
| Milan-out at explant histology, n (%) | 120 (25.9) |
167 (30.0) | 0.98 |
| G3-4, n (%) | 148 (31.9) | 140 (25.1) | 0.01 |
| Microvascular infiltration, n (%) | 88 (39.5) | 182 (32.7) | 0.02 |
| TRANSPLANTATION | |||
| CIT, median (IQR) (min) | 424 (89) | 420 (101) | 0.09 |
| MP, n (%) | 9 (1.9) | 7 (1.2) | 0.89 |
| Re-transplantation, n (%) | 18 (3.8) | 23 (4.1) | 0.45 |
NOTE: AFP, alpha-fetoprotein; CKD, chronic kidney failure; CNI, calcineurin inhibitor; DM, diabetes mellitus; EVR, everolimus; HBV, hepatitis B virus; HCV, hepatitis C virus; HDV, hepatitis delta virus; IQR, interquartile range; MELD, model for end-stage liver disease; NAFLD, non-alcoholic fatty liver disease; MW, microwave ablation; MP, machine perfusion; PEI, percutaneous ethanol injection; PSC, primary sclerosing cholangitis; RFA, radiofrequency ablation; TAC, tacrolimus; TACE, trans-arterial chemoembolization; TARE, trans-arterial radioembolization. *Radiological; ** Radiological, as downstaged from outside to within Milan criteria.
Table 2.
Effect of stabilized IPTW in the population on the variables used for balancing the two groups.
Table 2.
Effect of stabilized IPTW in the population on the variables used for balancing the two groups.
| Variables | Pre-IPTW | Post-IPTW | ||||
|---|---|---|---|---|---|---|
| EVR (n=463) | CNI (n=556) | Cohen’s D-value | EVR (n=233) | TAC (n=278) | Cohen’s D-value | |
| Mean (±SD) | Mean (±SD) | |||||
| Patient male sex | 0.83±0.15 | 0.87±0.14 | 0.05 | 0.81±0.17 | 0.82±0.15 | 0.05 |
| Patient age, years | 55.9±3.92 | 56.4±3.46 | -0.20 | 55.1±0.55 | 55.3±0.53 | -0.03 |
| HCV | 55.5±0.70 | 55.8±0.58 | -0.42 | 24.3±0.56 | 24.1±0.52 | 0.01 |
| Patient diabetes | 0.24±0.50 | 0.26±0.45 | 0.12 | 0.23±0.50 | 0.24±0.50 | 0.00 |
| Patient CKD | 0.05±0.02 | 0.07±0.42 | 0.42 | 0.05±0.01 | 0.05±0.01 | 0.01 |
| MELD | 0.07±0.26 | 0.11±0.33 | -0.15 | 0.08±0.38 | 0.07±0.37 | 0.01 |
| Donor male sex | 0.52±0.38 | 0.50±0.41 | -0.08 | 0.51±0.28 | 0.50±0.28 | 0.01 |
| Donor age, years | 0.69±0.65 | 0.67±0.64 | 0.01 | 0.68±0.38 | 0.67±0.37 | 0.03 |
| Donor cause of death (CVA) | 0.71±0.50 | 0.73±0.40 | 0.13 | 0.71±0.46 | 0.72±0.45 | -0.02 |
| MP | 0.09±0.02 | 0.08±0.02 | 0.01 | 0.08±0.02 | 0.08±0.02 | 0.00 |
| CIT, minutes | 431.77±79.02 | 423.50±85.79 | 0.10 | 0.53±0.50 | 0.53±0.50 | 0.01 |
| Milan-out stage, radiologic | 32.8±2.33 | 19±1.65 | 0.42 | 29.2±1.2 | 26.3±0.9 | 0.02 |
| Tumor downstaging | 0.17±0.05 | 0.08±0.04 | 0.43 | 0.10±0.02 | 0.08±0.08 | 0.04 |
| AFP at transplant | 0.45±0.27 | 0.04±0.02 | 0.38 | 0.23±0.04 | 0.19±0.06 | 0.14 |
| Milan-out stage, histology | 26.1±1.5 | 29.1±2.3 | 0.16 | 24.0±2.3 | 22.0±2.8 | 0.12 |
| G3-G4 | 32.0±2.4 | 25±1.8 | 0.23 | 29.0±2.3 | 28.2±2.0 | 0.21 |
| Microinfiltration | 40.2±1.2 | 33.7±1.7 | 0.26 | 38.1±2.3 | 32.5±1.9 | 0.20 |
| Mean TAC exposure >10 ng/mL within the first month | 0.28±0.04 | 0.32±0.45 | 0.13 | 0.15±0.02 | 0.13±0.03 | 0.00 |
| NOTE: AFP, alpha-fetoprotein; CIT, cold ischemia time; CKD, chronic kidney disease; CVA, cerebro-vascular accident; G, grading; HCV, hepatitis C virus; IPTW, inverse probability therapy weighting; MP, machine perfusion; n, number; SD, standard deviation; TAC, tacrolimus. | ||||||
Table 3.
The characteristics of the 2 pseudo-groups after IPTW matching.
| Variable | EVR (#233) | TAC (#278) | P |
|---|---|---|---|
| RECIPIENT | |||
| Male sex, n (%) | 192 (82.4) | 228 (82.0) | 0.90 |
| Age at transplant (median, IQR), years | 55.5 (9) | 55.3 (10) | 0.89 |
| HCV, n (%) | 58 (24.3) | 69 (24.8) | 1 |
| Lab-MELD at transplant (median, IQR) * | 8 (6) | 7 (7) | 0.78 |
| DM at transplant, n (%) | 53 (22.7) | 66 (23.7) | 0.83 |
| CKD at transplant, n (%) | 12 (5.1) | 14 (5.0) | 1 |
| Mean TAC exposure >10 ng/mL within the first month post-transplantation | 35 (15.0) | 36 (12.9) | 0.52 |
| DONOR | |||
| Male sex, n (%) | 118 (50.6) | 140 (50.3) | 1 |
| Age, median (IQR) | 68.0 (23) | 67 (26) | 0.89 |
| CVA as cause of death, n (%) | 181 (77.7) | 200 (71.9) | 0.15 |
| HCC | |||
| Exceeding Milan criteria at transplant *, n (%) | 67 (28.7) | 72 (25.8) | 0.48 |
| Successful downstaging**, n (%) | 24 (10.3) | 23 (8.2) | 0.44 |
| AFP at transplant, median (IQR) (ng/mL) | 23.3 (18) | 19 (11) | 0.56 |
| Milan-out at explant histology, n (%) | 55 (23.6) |
62 (22.3) | 0.75 |
| G3-4, n (%) | 67 (28.7) | 78 (28.1) | 0.92 |
| Microvascular infiltration, n (%) | 88 (37.8) | 91 (32.7) | 0.26 |
| TRANSPLANTATION | |||
| CIT, median (IQR) (min) | 432 (89) | 489 (101) | 0.06 |
| MP, n (%) | 9 (1.9) | 7 (1.2) | 0.89 |
NOTE: AFP, alpha-fetoprotein; CIT, cold ischemia time; CKD, chronic kidney failure; CNI, calcineurin inhibitor; DM, diabetes mellitus; EVR, everolimus; HCV, hepatitis C virus; IPTW, inverse probability of treatment weighting; IQR, interquartile range; MELD, model for end-stage liver disease; MP, machine perfusion; TAC, tacrolimus. *Radiological; ** Radiological, as downstaged from outside to within Milan criteria.
Table 4.
Results in the study groups after stabilized IPTW matching.
| Variable | EVR (#233) | TAC (#278) | P |
|---|---|---|---|
| Death, n (%) HCC recurrence, n (%) HCV recurrence, n (%) Incomplete/delayed graft function, n (%) MACE, n (%) Intra/peri-operative, n (%) Ischemic cholangiopathy, n (%) Infection/sepsis, n (%) De novo malignancy, n (%) Stroke, n (%) |
62 (26.6) 16 (6.8) 16 (6.9) 1 (0.4) 2 (0.8) 2 (0.8) 4 (1.7) 12 (5.1) 5 (2.1) 4 (1.7) |
105 (37.8) 42 (15.1) 15 (5.4) 2 (0.7) 6 (2.1) 3 (1.1) 7 (2.5) 16 (5.7) 11 (3.9) 3 (1.1) |
0.007 0.003 0.48 0.22 0.30 1 0.76 0.84 0.31 0.70 |
| Re-transplantation, n (%) Ischemic cholangiopathy, n (%) PNF, n (%) HAT, n % Chronic rejection, n (%) HCV recurrence, n (%) |
9 (3.9) 3 (1.3) 3 (1.3) 2 (0.8) 1 (0.4) 0 (0) |
11 (3.9) 3 (1.1) 5 (1.8) 1 (0.3) 1 (0.3) 1 (0.3) |
1 1 0.73 0.59 1 0.99 |
| HCC recurrence, n (%) Liver only, n (%) Liver and lung, n (%) Liver and bone, n (%) Lung only, n (%) Bone only, n (%) Lung and bone, n (%) Nodes, n (%) >2 organs, n (%) |
18 (7.7) 7 (3.0) 1 (0.4) 0 (0) 4 (1.7) 4 (1.7) 1 (0.4) 1 (0.4) 2 (0.8) |
47 (16.9) 15 (5.4) 8 (2.8) 4 (1.4) 9 (1.8) 1 (0.2) 4 (1.4) 6 (2.1) 16 (5.7) |
0.002 0.19 0.04 0.12 0.39 0.18 0.38 0.13 0.002 |
NOTE: EVR, everolimus; HAT, hepatic artery thrombosis; HCC, hepatocellular carcinoma; HCV, hepatitis C virus; IPTW, inverse probability of treatment weighting; IQR, interquartile range; MACE, major cardiovascular events; PNF, primary non-function; TAC, tacrolimus. .
Table 5.
Immunosuppression in the EVR study groups after stabilized IPTW matching.
| Variable | EVR (#233) |
|---|---|
| Reason for EVR use, n (%) HCC recurrence prophylaxis, n (%) Deteriorating renal function *, n (%) Neurologic complication *, n (%) MACE *, n (%) |
212 (91.0) 14 (6.0) 4 (1.7) 3 (1.2) |
| Timing of EVR introduction, median (IQR) (days) * |
30 (16) |
| Duration of EVR treatment, median (IQR) (months) * |
46.6 (36.1) |
| EVR whole-blood exposure, median (IQR) (ng/mL) * |
5.8 (1.7) |
NOTE: EVR, everolimus; HC, hepatocellular carcinoma; IPTW, inverse probability of treatment weigthing; IQR, interquartile range; MACE, major cardiovascular events.
Table 6.
EVR mode of administration and exposure in recurring versus non-recurring patients of the EVR group.
Table 6.
EVR mode of administration and exposure in recurring versus non-recurring patients of the EVR group.
| Variable | Recurring HCC (#18) | Non-recurring HCC (#215) | P |
|---|---|---|---|
| Timing of EVR introduction, median (IQR) (days) * | 52 (26.4) | 30 (12) | <0.001 |
| Duration of EVR treatment, median (IQR) (months) * | 46.5 (57.0) | 69.9 (24.8) | <0.001 |
| EVR whole-blood exposure, median (IQR) (ng/mL) * | 3.65 (0.55) | 5.9 (1.4) | <0.001 |
NOTE: EVR, everolimus; HCC, hepatocellular carcinoma; IQR, interquartile range.
Table 7.
Results of the multivariable analysis of risk factors for both recurrence-free and overall survival.
Table 7.
Results of the multivariable analysis of risk factors for both recurrence-free and overall survival.
| Variable | Coefficients (95%CI) |
SE | z | HR | p |
|---|---|---|---|---|---|
| OS | |||||
| Successful pre-transplant downstaging | 0.6 (0.15; 1.06) | 0.23 | 2.6 | 0.79 | 0.006 |
| Within Milan criteria at transplant | -1.15 (-1.61;-0.7) | 0.23 | 5.02 | 0.67 | <0.01 |
| Within Milan criteria at histology | 0.01 (0; 0.01) | 0 | 2.41 | 0.78 | 0.02 |
| Micro-infiltration | 0.39 (-0.01; 0.78) | 0.2 | 1.91 | 1.13 | 0.056 |
| G3-G4 | 0.25 (0.01; 0.5) | 0.12 | 2.02 | 1.18 | 0.077 |
| EVR | -0.59 (-1.02; -0.16) | 0.22 | 2.7 | 0.69 | 0.009 |
| RFS | |||||
| Successful pre-transplant downstaging | 0.57 (0.12; 1.02) | 0.23 | 2.47 | 0.65 | 0.01 |
| Within Milan criteria at transplant | -1.18 (-1.63;-0.72) | 0.23 | 5.11 | 0.56 | 0.01 |
| Within Milan criteria at histology | 0.01 (0; 0.01) | 0 | 2.52 | 0.68 | 0.012 |
| Micro-infiltration | 0.42 (0.02; 0.81) | 0.2 | 2.06 | 1.22 | 0.04 |
| G3-G4 | 0.22 (-0.02; 0.47) | 0.13 | 1.77 | 1.27 | 0.04 |
| EVR | -0.78 (1.2; -0.36) | 0.21 | 3.66 | 0.46 | <0.001 |
NOTE: AFP, alpha-fetoprotein; EVR, everolimus; HCV, hepatitis C virus; OS, overall survival; RFS, recurrence-free survival.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



