Submitted:
29 December 2023
Posted:
29 December 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background
Although COVID-19 outcomes vary between and within countries, there is little published data on how aspects of social determinants of health (SDoH) affect COVID-19 outcomes in the African context.
Objective
The current study set to examine COVID-19 case and death rates and their correlates among African countries using data from different sources.
Methods
An ecological cross-sectional study comprising 28 African countries with a recent Demographic and Health Survey, DHS (2010-2018). Response variables were COVID-19 case and death rates (as of August 15, 2020). Covariates comprised three healthcare systems measures; rates of hospital beds (2005-2017), ventilators (2020) and doctors (2010-2018) per 10,000 population, and 9 broad topics common to multiple SDoH frameworks aggregated to the country level; geography (urban residence), wealth index, education, employment, crowding, and access to information. Rates per 10,000 population were calculated for healthcare measures and mapped for visualization. A Negative Binomial regression was used to assess whether aspects of SDoH are correlated with COVID-19.
Results
Our analysis indicated that 1 in 4 (25.1%) households in study countries are without clean water and handwashing access. Country-level health system capacity (hospital beds, ventilators, and medical doctors) varied considerably between the countries. Negative Binomial regression showed that the odds of COVID-19 morbidity and death was higher in countries with a high proportion of households without access to quality water and doctors per 10,000 people. Having a high proportional of educated women (1.003: 95% CI, 1.001 – 1.005), hospital beds per population and less people per room (0.959: 95% CI, 0.920 – 1.000) was negatively correlated with COVID-19 deaths while being insured and owning a mobile phone was correlated with illness.
Conclusion
Both aspects of SDoH and healthcare system contribute either negatively or positively to COVID-19 outcomes. Addressing healthcare system capacity and economic and environmental SDoH will be critical for mitigating the spread of COVID-19 and re-emerging diseases on the African continent.
Keywords:
Social determiants of health
; Africa
; vaccines
; prevention
1. Introduction
The 2019 coronavirus disease (COVID-19) pandemic continues to wreak havoc globally, with more than 600 million cases, and 6.6 million deaths recorded as of December 27, 2022 (1). Consequently, healthcare systems have been severely impacted worldwide, and African countries are no exception (2). In Africa, where the pandemic is expanding (3, 4), COVID-19 has exposed gaps in already overstressed health services that require urgent attention, with most countries woefully unprepared for addressing the crisis(5, 6). Of concern is the limited or lack of beds in public facilities intensive care units (ICUs). For example, compared to the United States that has 34.5 ICU beds per 100,000 people(7), a recent report by the World Health Organization (WHO) found only five ICU beds per one million people in most African countries (8). Although there is no consensus on the ideal number of ICU beds to serve a population (9), having more beds can facilitate patient transfer directly from the emergency room rather than having to initially receive care on a general ward (10). Other challenges include high caseloads of COVID-19 patients compared to the healthcare systems’ treatment capacity, inadequate staffing levels, and limited access to care partly due to poor roads or lack of reliable transportation (5, 11).
Although the risk for COVID-19 varies both between and within countries (e.g., urban versus rural)(12), the progression of disease and potential impact of COVID-19 in the context of Africa and actual estimates have been mixed(13), with some studies finding low COVID-19 burden(14), fast disease spread(15). There are also concerns that the reported cases and/or deaths rates are an underestimation, with Bradshaw et al. calling “for surveillance of hospitalizations, comorbidities, emergence of new variants of concern, and scale-up of representative seroprevalence studies as core response strategies”(16). To note, as of November 22, 2022, the Africa CDC Dashboard showed that over 200,000 people have died from COVID 19 in the region (54 of 55 African Union Member States (except Western Sahara); the southern region accounts for over half (55%, n=652,707) of all reported cases and half of the case-fatalities (50%, n=14,061) on the continent. South Africa (n=611,450 cases), Egypt (n=97,478), Morocco (n=53,252 cases), Algeria (n= 42,302) and Ethiopia (n= 42,143) drive the overall cases.
A set of other complex factors, both internal and external exacerbate disease and the healthcare burden of disease outbreaks in Africa. In the case of COVID-19, factors include a lack of COVID-19 testing(17), personal protective equipment (PPE), and vaccines (17), overcrowding (e.g., for people living in slums and often in close quarters), living with a chronic illness, poverty, poor infrastructure (e.g., sanitation), low per capita health expenditure(18) and belonging to lower socio-economic class (19). These factors are considered social determinants of health (SDoH)(20, 21) and have contributed significantly to African countries’ vulnerabilities and resulting in poor health outcomes across the continent. Challenges in surveillance, and capacity building including the provision of and access to health care are immense. As the WHO (8), and El-Sadr (5) note, containment is still possible if African countries can use their experience in managing infectious diseases such as HIV, malaria, tuberculosis, and Ebola (22). Moreover, African countries can further tap into aspects of their strengthened healthcare systems in diagnostic testing, ICU, surveillance, and systems for reporting emergencies resulting from global initiatives established during the Ebola Virus Disease outbreak (23). However, others question whether Africa is ready for the next disease “X”, and call for accurate predictions, a better understanding of the role of SDoH, and increased training, resources, and adequate healthcare staffing levels (24, 25). Moreover, in the wake of international de-regulation and financing initiatives such as COVAX, better understanding of the dynamics, access, and distribution of vaccine supply in rapidly unfolding epidemic situations is needed (26, 27). Further, although individual risk behaviors that contribute to COVID-19 have been established (e.g., close personal contact such as shaking hands) (20, 28), there is little published data on how aspects of economic, social, and environmental conditions, also referred to as SDoH affect COVID-19 risk in the African context. This lack of research presents a significant gap in health- plausible pathways and biological mechanisms and effects.
Given the role of social factors (e.g., wealthy, income, and education) on influencing health behaviors and outcomes of individuals or communities, we argue that there is a dearth of comparable sub-national data that accurately reflect country residents’ living conditions and socio-economic development, making it difficult to timely address challenges and inequalities that augment negative disease outcomes among residents in the African context. However, the availability of the DHS dataset allows us to complement country-level datasets on SDoH with additional external information about the healthcare system in the countries. Such datasets and data triangulation are vital for understanding the potential strength, direction, and timing of these causal relationships and is critical for pandemic response preparedness and prediction of disease frequencies in the context of disease emergencies (re-emerging). Therefore, we conducted an ecological study to examine the associations between indicators of the social determinants of health (SDoH) and health care systems across 29 African countries with SDoH data and COVID-19 rates. The goals of the study are to characterize the potential relationships between SDoH and COVID-19 measures at the country level, to determine the gaps in knowledge, and to offer opportunities for policy-relevant research on living conditions or inequality, inclusive development, and demographic trends at the sub-national level.
2. Methods
2.1. Design and setting
We conducted an ecological cross-sectional study comprising 28 African countries (Figure 1), with a recent Standard Demographic and Health Survey completed within the past ten years(29). To be included, countries also had to have COVID-19 data publicly available. Initiated in 1984, the DHS was used because it captures comparable population-based data on indicators of household-level living conditions as well as the broader socioeconomic, demographic, and environmental conditions in in low and middle-income countries (LMICs)(30) allowing a comprehensive assessment of a country’s health situation including comparison between and within countries (urban, rural). Moreover, the DHS questionnaires are consistent to enhance the comparability of indicators across populations and time. The DHS survey participants are selected from clusters and households within a fully covered geographic sampling frame using multistage design, providing opportunities for examining both ecological and individual-level factors that relate to the distribution of health outcomes(31). We excluded countries if they did not have a survey conducted in 2010 or later or if they did not include likely significant measures that contribute to differential COVID-19 outcomes as part of the information collected.
2.2. Country-level COVID-19 data source
We obtained reported COVID-19 case and death rates as of August 15, 2020, for African countries with DHS data from the Africa Centers for Disease Control and Prevention (CDC) Dashboard (accessible at: https://africacdc.org/covid-19/). The Africa CDC Dashboard compiles COVID-19 testing data from official regional collaborating centers and member state reports. Therefore, these data may not be indicative of the actual tests as of the date of the dashboard update. To determine the country level case and death rates, we calculated the number of COVID-19 deaths and/or cases per country in each period and divided it by the population exposed to risk of infection and death in that period multiplied by 10,000.
2.3. Country-level health system data source, measures
We obtained data for hospitals (e.g., hospital beds, ventilators) and physicians from the World Health Organization’s Global Health Observatory for years 2005-2018 (accessible at: https://apps.who.int/gho/data/node.main) for all African countries (n=54 countries). Definitions of systems of care have been described elsewhere(32). Because there are no centralized databases for ventilators on the African continent, we obtained the number of ventilators from various sources. The first source was a recent Reuter’s survey of African health ministries and public health officials. We also reviewed the New York Times, and World Bank were for ventilator information(33). Of the 54 African countries, 43 reported having ventilators except for Benin, Comoros, Congo, Lesotho, Malawi, Mauritius, Sao Tome and Principe, Seychelles, South Sudan, and Tanzania. The second source of ventilators was the New York Times, which provided ventilator data for Malawi and South Sudan (34).
2.4. Country-level social determinants of health data source, measures
To determine the association between SDoH and COVID-19 outcomes, we abstracted from the most recent DHS in each country (n=28 countries) 9 variables commonly reported as shaping health outcomes. The measures comprised nine broad topics common to multiple SDoH frameworks and aggregated them to the country level(20). Because there are gender differences in educational attainment while COVID-19 has affected girls/women differently than boys/men, a few independent indicators focus on women. These measures of interested represented geography (urban residence), wealth (Human Development Index or HDI, and indicator reported to be better than “GDP per capita” in measuring the progress of nations, particularly LMICs; and a wealth index – poor or average living)(35, 36), education (women with no education, primary, secondary or higher, percentage, %), sanitation (women living in households with high quality water access, have a place to wash hands, soap or detergent present, %), employment (currently working, %), insurance coverage (%), crowding (average number of household members based on more than three people per sleeping room), distance to safe clean water (average time to get to drinking water), access to information (women owning a mobile phone (%)) and women listening to the radio at least once a week (%). The DHS SDOH measures of interest were selected based on the literature and conceptual SDOH frameworks (21, 37, 38). These measures are associated with differentiating COVID-19 screening and testing outcomes (30, 39).
The DHS dataset was used because it represents the primary source of data in many low-middle income countries on the demographic, socioeconomic and environmental conditions and trends in a country(29) and datasets are available to the public upon request to the DHS Program(40). The DHS Program uses a two-stage cluster sampling design to capture representativeness of the data at the national and sub-national level. Variables collected via the DHS are often the same across countries and period, enabling comparison over space and time.
2.5. Data Processing
Country-level DHS SDoH measures: To abstract the SDoH measures of interest from the DHS, we first put together a full continent database, drawn from the DHS program(40). We included only countries with the most recent DHS survey (conducted in the past 10 years) and had COVID-19 as well as health measures data. The DHS household survey data was converted to country level, and for that we used the data processing and aggregation methods documented in detail elsewhere by LivWell;(41) briefly, household-level data was first aggregated to the sub-national level; a corresponding R function was used to transform the raw data into the final measures at the country level. Data was then validated using data obtained from other sources (e.g., the DHS complier, Livwell data repository the subnational human development database(41, 42, 43). Sampling weights were used in calculations as provided by the DHS Program (44), and to account for sampling weight, the weight in the pooled data was divided by the number of surveys available for the respective countries as used in previous studies(30).
Country-level health system measures: We calculated rates of medical doctors, ventilators and hospital beds per 10,000 population for all countries using population data obtained from the World Bank as of 2019 (45) (28). These newly developed measured were then combined with the calculated COVID-19 hospitalization and death rates and SDOH measures.
This study uses publicly available secondary data, as such, ethical approvals are not necessary.
2.6. Statistical Analysis
We used ArcGIS Software version 10.5 (46) to visualize health system measures (hospital bed, ventilator, and physician rates per 10,000 population). Negative Binomial regression was used to assess the association between COVID-19 risks, health care system measures and SDoH. Negative Binomial regression was chosen over Poisson regression because the COVID-19 death and case rates (dependent variable) were over-dispersed. The approach was adopted only after performing the Likelihood ratio test for over dispersion for both Negative Binomial regression and Poisson regression. The denominator included all surveyed households in the DHS study countries with measures aggregated to the country-level (n=28 countries). Predictors were added sequentially to the model, in which the fixed effects can be interpreted as conditional on countries, with all random effects fixed at zero (e.g., unit-specific models). Model goodness of fit and assessment of outliers were evaluated by the Akaike information criterion (AIC), the Bayesian information criterion (BIC) and McFadden's pseudo-R-squared statistic. All analyses were conducted using IBM SPSS statistics version 26.0 (47).
3. Results
3.1. Characteristics of study countries
Table 1 presents the characteristics of the DHS SDOH measures, count, and percentages for the study countries. The study sample (n =416,459 surveyed households in 28 study countries). Of the 63.9% surveyed countries, inhabitants live in rural areas and 36.1% are urban dwellers. One in four (25.1%) respondents are without a designated place for household members to wash their hands, and a staggering 41% of residents reported not having soap or detergent for handwashing. The share of countries reporting households with more than three people per sleeping room is 21.4%, while about 36.0% of countries report that inhabitants do not have any education while 42.6% of the surveyed countries have inhabitant living in poverty.
Country-level health system capacity (hospital beds, ventilators, and medical doctors) varied considerably between the countries. On average there were 12.58 hospital beds per 100,000 population and 3.79 doctors per 100, 000 population in the study countries. Most countries (75.9%, 41 of 54) had less than one ventilator per 100,000 population (Figure 2, Appendix A).
Of the study countries, Libya (20.30), Seychelles (20.79) and Mauritius had the highest number of medical doctors per 10,000 inhabitants followed by Algeria (16.86). The number of doctors per 100,000 inhabitants was less than 10 in 89% of the surveyed countries. Likewise, Seychelles (36.0), Mauritius (34.0) and Libya (32.0) had the highest rates of hospital beds per 10,000 population.
We observed country differences in the rates of COVID-19 deaths and cases. Overall deaths from COVID-19 across the study African countries ranged from 0-1.99 per 10,000 population during the study period (Figure 2, Appendix A). As of August 15, 2020, South Africa had the highest COVID-19 case and death rates in Africa, and still has the highest COVID-19 related cases and deaths in Africa. For example, as of December 23, 2022, there were 4,046,603 confirmed cases of COVID-19 with 102,550 deaths, reported to WHO.
3.2. Multivariate analysis of correlates for COVID-19 case and death rates in the 28 study countries
The results of a Binomial Negative regression model on COVID-19 case rates across the 28 African study countries are shown in Table 2. Not having access to quality water (1.153; 95% CI, 1.036 - 1.284), health insurance (1.262: 95% CI, 1.124 - 1.417), women not owning a mobile phone and less doctor rates per 100,000 population COVID-19 case rates.
Regarding, COVID-19 death rates, we also observed that the odds of COVID-19 deaths was higher in countries with a high proportion of households without access to quality water (1.004: 95% CI, 1.002 – 1.006), uneducated women (1.003: 95% CI, 1.001 – 1.005), less doctor and hospital beds per 10,000 population (Table 3). Having less than three people sharing a room was negatively associated with COVID-19 deaths.
4. Discussion
We set out to examine the associations between indicators of the social determinants of health (SDoH) and health care systems across 28 African countries with COVID-19 outcomes (cases and death rates). We observed that countries in Africa have great variation in socioeconomic and COVID-19 health vulnerabilities. These results are likely related to a difference in the ability of countries to detect and test patients, limited PPE availability, the high prevalence of younger population, a lack of rapid and more effective national health policies, and the possibility of under reporting of cases and deaths(48). This finding was also reported in similar related studies(49, 50, 51).
As mentioned in the literature review, eight categories of the proximate social determinants of health (SDoH) and three healthcare system measures are responsible for COVID-19 case rates and subsequent death rates. Consistent with previous studies involving and COVID-19 outcomes and SDoH, we observed that not having the means to practice proper hygiene such as access to high quality water, being insured, access information (e.g., women not owning a mobile phone) considerably influenced the odds of COVID-19 case rates. Although it is difficult to explain the finding on the association between COVID-19 outcomes and women owning a mobile phone, access to mobile devices have been linked to health literacy(52), improved self-efficacy and communication between healthcare workers, clients, and better adherence outcomes(53, 54, 55). Notably, this is an important issue for future research. The SDoH measures of residence (urban vs. rural), Human Development Index, uneducated women, women in the workforce, having more than 3 people sharing a room in a household, and women listening to the radio at least once a week do not reach statistical significance (p < 05) in the Binomial Negative regression model.
Our results indicated that the single most important healthcare system measure in shaping COVID-19 case outcomes is the rate of available hospital beds in a country per population. A shortage in hospital beds in this study corroborates earlier findings and raises the possibility for delayed provision of health care to both COVID-19 and non-COVID-19 patients. This also accords with earlier observations that noted delayed COVID-19 response in China(56) and South Africa (57, 58, 59, 60).
Interestingly, the SDoH measures that are significantly related to the COVID-19 case rates are significantly associated with the COVID-19 death rates. As can be seen in Table 3, and in addition to high access to quality water, educated women, and crowding or having more than 3 people sharing a room in a household are significant. This result suggests the importance of educating women in developing countries as it can improve health outcomes. Notably, in the context of Africa, women’s educational level has been reported as shaping healthcare seeking behaviors, while among the most effective intervention strategies have been those to do with women education and health literacy(30, 61, 62, 63, 64). Moreover, COVID-19 has affected girls and women differently than boys and men, and women are more vulnerable to COVID-19–related economic impacts because of existing gender inequalities(20, 65). The other SDoH measures and rates of ventilators per population were not significant predictors of infant mortality.
The most unanticipated finding of this study was the apparent negative relationship between the Human Development Index (HDI) and COVID-19 outcomes. This outcome is contrary to that of recent studies that noted an association between the HDI and COVID-19 incidence by country(66, 67). Future studies on the current topic are therefore recommended.
5. Limitations
The current study adds to our knowledge regarding the influence of social determinants of health (SDoH)on the health outcomes in Africa. It is the first study to model the possible contribution of both SDoH and healthcare system measures on COVID-19 outcomes in Africa. However, this study is without limitations. First, a limitation of this study is the issue of omitted variable bias. For example, of all potential risk and protective factors (e.g., use of PPE) that can moderate an individual’s exposure to the COVID-19, we only include select SDoH and healthcare system measures. Further, the DHS data on healthcare services are limited to evaluating availability and utilization, and no indicators on quality of care are collected. Further research should be undertaken to assess the quality of care beyond the use of cross-sectional surveys. In addition, the available DHS vary by country, capturing only a brief snapshot of SDOH overtime and shedding little light on how SDOH change over time. This limitation is largely unavoidable due to a dearth of longitudinal data on COVID-19 and protective factors in Africa. A further study with more focus on protective factors that as the use of PPE that can be generated via focus groups and surveys is therefore suggested.
6. Conclusion
We observe both variation in COVID-19 disease risk and death outcome between countries, and these problems are largely correlated with aspects of social determinant of health and healthcare system measures. Addressing healthcare system capacity and economic and environmental determinants needs to become an integral part of the healthcare reform in African countries as countries prepare for next major re/emerging disease outbreak.
Author Contributions
Conceptualization, I.K.M, and L.R.O.; methodology, I.K.M,; software, I.K.M,; validation, L.R.O, Y.Y. and I.K.M.; formal analysis, X.X.; investigation, X.X.; resources, X.X.; data curation, L.R.O.; writing—original draft preparation, I.K.M.; writing—review and editing, H.H.; visualization, K.O.; supervision, I.K.M.; project administration, I.K.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable. This study used publicly available secondary data sources.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A. Health System Measures per 10,000 population and COVID-19 Outcomes
| Country | Health System Measures per 10,000 population | COVID-19 Outcomes per 10,000 population | ||||
| Doctors | Ventilators | Hospital Beds | Cases | Deaths | ||
| Algeria | 16.86 | 0.06 | 19.0 | 8.96 | 0.31 | |
| Angola | 2.01 | 0.07 | 8.0 | 0.59 | 0.03 | |
| Benin | 0.77 | ~ | 5.0 | 1.75 | 0.03 | |
| Botswana | 4.94 | 0.65 | 18.0 | 5.27 | 0.01 | |
| Burkina Faso | 0.80 | 0.01 | 4.0 | 0.61 | 0.03 | |
| Burundi | 0.94 | 0.02 | 7.9 | 0.36 | 0.00 | |
| Cabo Verde | 7.46 | 0.91 | 21.0 | 57.52 | 0.62 | |
| Cameroon | 0.71 | 0.02 | 15.0 | 7.00 | 0.15 | |
| CAR | 0.68 | 0.01 | 10.0 | 9.80 | 0.13 | |
| Chad | 0.41 | 0.01 | 4.0 | 0.60 | 0.05 | |
| Comoros | 2.54 | ~ | 21.6 | 4.69 | 0.08 | |
| Congo | 1.34 | ~ | 16.0 | 7.12 | 0.14 | |
| Côte d'Ivoire | 2.04 | 0.03 | 4.0 | 6.61 | 0.04 | |
| Djibouti | 2.06 | 0 | 14.0 | 55.13 | 0.61 | |
| DRC | 0.67 | 0.01 | 8.0 | 1.11 | 0.03 | |
| Egypt | 4.43 | 0.04 | 14.3 | 9.60 | 0.51 | |
| Equatorial Guinea | 3.74 | 0.15 | 21.0 | 35.55 | 0.61 | |
| Eritrea | 0.61 | 0 | 7.0 | 0.81 | 0.00 | |
| Eswatini | 3.19 | 0.14 | 21 | 32.62 | 0.60 | |
| Ethiopia | 0.75 | 0.05 | 3.3 | 2.58 | 0.05 | |
| Gabon | 6.48 | 0.46 | 13.0 | 37.86 | 0.23 | |
| Gambia | 0.91 | 0.02 | 11.0 | 7.19 | 0.23 | |
| Ghana | 1.30 | 0.07 | 9.0 | 13.88 | 0.08 | |
| Guinea | 0.76 | 0.02 | 3.0 | 6.47 | 0.04 | |
| Guinea-Bissau | 1.18 | 0.00 | 10.0 | 11.02 | 0.17 | |
| Kenya | 1.53 | 0.06 | 14.0 | 5.73 | 0.09 | |
| Lesotho | 0.65 | ~ | 13.0 | 4.45 | 0.14 | |
| Liberia | 0.34 | 0.01 | 8.0 | 2.55 | 0.17 | |
| Libya | 20.30 | 0.36 | 32.0 | 11.42 | 0.21 | |
| Madagascar | 1.59 | 0.01 | 2.0 | 5.13 | 0.06 | |
| Malawi | 0.35 | 0.01 | 13.0 | 2.70 | 0.08 | |
| Mali | 1.25 | 0.03 | 1.0 | 1.33 | 0.06 | |
| Mauritania | 1.81 | 0.00 | 4.0 | 14.70 | 0.35 | |
| Mauritius | 25.36 | ~ | 34.0 | 2.72 | 0.08 | |
| Morocco | 7.13 | 0.45 | 10.0 | 11.25 | 0.17 | |
| Mozambique | 0.81 | 0.01 | 7.0 | 0.94 | 0.01 | |
| Namibia | 4.10 | 1.25 | 27.0 | 15.66 | 0.14 | |
| Niger | 0.39 | 0.01 | 3.9 | 0.50 | 0.03 | |
| Nigeria | 3.71 | 0.02 | 5.0 | 2.43 | 0.05 | |
| Rwanda | 1.31 | 0.04 | 16.0 | 1.86 | 0.01 | |
| Sao Tome/ Principe | 0.51 | ~ | 29.0 | 41.15 | 0.70 | |
| Senegal | 0.65 | 0.02 | 3.0 | 7.38 | 0.15 | |
| Seychelles | 20.79 | ~ | 36.0 | 13.01 | 0.00 | |
| Sierra Leone | 0.21 | 0.02 | 4.0 | 2.50 | 0.09 | |
| Somalia | 0.2 | 0.01 | 8.7 | 2.10 | 0.06 | |
| South Africa | 8.81 | 0.55 | 23.0 | 99.67 | 1.99 | |
| South Sudan | ~ | 0 | ~ | 2.25 | 0.04 | |
| Sudan | 2.5 | 0.07 | 7.4 | 2.88 | 0.19 | |
| Tanzania | 0.13 | ~ | 7.0 | 0.09 | 0.00 | |
| Togo | 0.76 | 0.02 | 7.0 | 1.40 | 0.03 | |
| Tunisia | 12.73 | 0.21 | 21.8 | 1.73 | 0.05 | |
| Uganda | 1.56 | 0.02 | 5.0 | 0.32 | 0.00 | |
| Zambia | 11.53 | 0.06 | 20.0 | 5.23 | 0.15 | |
| Zimbabwe | 2.07 | 0.02 | 17.0 | 3.53 | 0.09 | |
| Africa Mean | 3.79 | 0.13 | 12.58 | 10.95 | 0.18 | |
| Note: ~ denotes countries without data. CAR= Central African Republic. DRC= Democratic Republic of Congo. The most recently completed Standard DHS was used for every country except for Senegal for which Continuous DHS was used. | ||||||
References
- Johns Hopkins University. COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) 2020 [Available from: https://coronavirus.jhu.edu/map.html.
- Sherrard-Smith E, Hogan AB, Hamlet A, Watson OJ, Whittaker C, Winskill P, et al. The potential public health consequences of COVID-19 on malaria in Africa. Nature Medicine 2020, 26, 1411–1416. [Google Scholar] [CrossRef] [PubMed]
- Haider N, Yavlinsky A, Simons D, Osman AY, Ntoumi F, Zumla A, et al. Passengers' destinations from China: low risk of Novel Coronavirus (2019-nCoV) transmission into Africa and South America. Epidemiol Infect. 2020, 148, e41. [Google Scholar] [CrossRef] [PubMed]
- Nkengasong JN, Mankoula W. Looming threat of COVID-19 infection in Africa: act collectively, and fast. Lancet (London, England). 2020, 395, 841–842. [Google Scholar] [CrossRef]
- El-Sadr WM, Justman J. Africa in the Path of Covid-19. New England Journal of Medicine. 2020, 383, e11. [Google Scholar]
- Gilbert M, Pullano G, Pinotti F, Valdano E, Poletto C, Boëlle PY, et al. Preparedness and vulnerability of African countries against importations of COVID-19: a modelling study. Lancet. 2020, 395, 871–877. [Google Scholar] [CrossRef] [PubMed]
- Wallace DJ, Angus DC, Seymour CW, Barnato AE, Kahn JM. Critical care bed growth in the United States. A comparison of regional and national trends. Am J Respir Crit Care Med. 2015, 191, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Preliminary Estimates of the Prevalence of Selected Underlying Health Conditions Among Patients with Coronavirus Disease 2019 - United States, February 12-March 28, 2020. MMWR Morb Mortal Wkly Rep. 2020, 69, 382–386. [CrossRef] [PubMed]
- Wunsch, H. Is there a Starling curve for intensive care? Chest. 2012, 141, 1393–1399. [Google Scholar] [CrossRef] [PubMed]
- Wunsch H, Angus DC, Harrison DA, Linde-Zwirble WT, Rowan KM. Comparison of medical admissions to intensive care units in the United States and United Kingdom. Am J Respir Crit Care Med. 2011, 183, 1666–1673. [Google Scholar] [CrossRef] [PubMed]
- Moise IK, Verity JF, Kangmennaang J. Identifying youth-friendly service practices associated with adolescents' use of reproductive healthcare services in post-conflict Burundi: a cross-sectional study. Int J Health Geogr. 2017, 16, 2. [Google Scholar] [CrossRef]
- Onovo AA, Kalaiwo A, Obanubi C, Odezugo G, Estill J, Keiser O. Estimates of the COVID-19 Infection Fatality Rate for 48 African Countries: A Model-Based Analysis. BioMed [Internet]. 2021, 1, 63–79. [Google Scholar]
- Cabore JW, Karamagi HC, Kipruto HK, Mungatu JK, Asamani JA, Droti B, et al. COVID-19 in the 47 countries of the WHO African region: a modelling analysis of past trends and future patterns. Lancet Glob Health. 2022, 10, e1099–e114. [Google Scholar] [CrossRef] [PubMed]
- Wamai RG, Hirsch JL, Van Damme W, Alnwick D, Bailey RC, Hodgins S, et al. What Could Explain the Lower COVID-19 Burden in Africa despite Considerable Circulation of the SARS-CoV-2 Virus? Int J Environ Res Public Health. 2021, 18, 8638. [Google Scholar] [CrossRef] [PubMed]
- 15. Pearson CA, Van Schalkwyk C, Foss AM, O'Reilly KM, Pulliam JR. Projected early spread of COVID-19 in Africa through 1 June 2020. Euro Surveill. 1 June.
- Bradshaw D, Dorrington R, Moultrie T, Groenewald P, Moultrie H. Underestimated COVID-19 mortality in WHO African region. Lancet Glob Health. 2022, 10, e1559. [Google Scholar] [CrossRef] [PubMed]
- Ihekweazu C, Agogo E. Africa’s response to COVID-19. BMC Medicine. 2020, 18, 151. [Google Scholar]
- Ghosh J, Moise IK, Kalipeni E. Regional integration and relationship with different forms of foreign direct investments in Southern Africa. In: Munoz JM, editor. Advances in Geoeconomics. London: Routledge; 2017. p. 151-9.
- Singu S, Acharya A, Challagundla K, Byrareddy SN. Impact of Social Determinants of Health on the Emerging COVID-19 Pandemic in the United States. Frontiers in Public Health. 2020, 8, 406. [Google Scholar] [CrossRef] [PubMed]
- Moise, I. Variation in Risk of COVID-19 Infection and Predictors of Social Determinants of Health in Miami–Dade County, Florida. Preventin Chronic Diseases. 2020, 17. [Google Scholar] [CrossRef]
- 21. Rojas D, Melo A, Moise IK, Saavedra J, Szapocznik J. The Association Between the Social Determinants of Health and HIV Control in Miami-Dade County ZIP Codes, 2017. J Racial Ethn Health Disparities. 2020.
- Mwisongo A, Nabyonga-Orem J. Global health initiatives in Africa – governance, priorities, harmonisation and alignment. BMC Health Services Research. 2016, 16, 212. [Google Scholar]
- 23. Dzinamarira T, Dzobo M, Chitungo I. COVID-19: A perspective on Africa's capacity and response. J Med Virol. 2020.
- Nuwagira E, Muzoora C. Is Sub-Saharan Africa prepared for COVID-19? Trop Med Health. 2020, 48, 18. [Google Scholar] [CrossRef] [PubMed]
- Braveman P, Gottlieb L. The social determinants of health: it's time to consider the causes of the causes. Public Health Rep. 2014, 129, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Leach M, MacGregor H, Akello G, Babawo L, Baluku M, Desclaux A, et al. Vaccine anxieties, vaccine preparedness: Perspectives from Africa in a Covid-19 era. Soc Sci Med. 2022, 298, 114826. [Google Scholar] [CrossRef] [PubMed]
- Msellati P, Sow K, Desclaux A, Cottrell G, Diallo M, Le Hesran JY, et al. Reconsidering the COVID-19 vaccine strategy in West and Central Africa. Lancet. 2022, 400, 1304. [Google Scholar] [CrossRef] [PubMed]
- Kavanagh MM, Erondu NA, Tomori O, Dzau VJ, Okiro EA, Maleche A, et al. Access to lifesaving medical resources for African countries: COVID-19 testing and response, ethics, and politics. Lancet. 2020, 395, 1735–1738. [Google Scholar] [CrossRef] [PubMed]
- MEASURE DHS. MEASURE DHS: Demographic and Health Surveys. DHS Survey Types. Calverton, MD: ICF Macro.
- Moise IK, Kangmennaang J, Halwiindi H, Grigsby-Toussaint DS, Fuller DO. Increase in Obesity Among Women of Reproductive Age in Zambia, 2002-2014. J Womens Health (Larchmt). 2019, 28, 1679–1687. [Google Scholar] [CrossRef]
- Ozodiegwu ID, Ambrose M, Battle KE, Bever C, Diallo O, Galatas B, et al. Beyond national indicators: adapting the Demographic and Health Surveys’ sampling strategies and questions to better inform subnational malaria intervention policy. Malaria Journal. 2021, 20, 122. [Google Scholar] [CrossRef] [PubMed]
- (US) NRC, (US) IoM. U.S. Health in International Perspective: Shorter Lives, Poorer Health. 2013.
- 33. Houreld K, Lewis D, McNeill R, Granados S. Virus exposes gaping holes in Africa’s health systems. Reuters Graphics, 2020.
- Maclean R, Marks S, et al. 10 African Countries Have No Ventilators. That’s Only Part of the Problem. New York Times. 2020 [Available from: https://www.nytimes.com/2020/04/18/world/africa/africa-coronavirus-ventilators.html.
- Islam, S. The human development index and per capita GDP. Applied Economics Letters. 1995, 2, 166–167. [Google Scholar] [CrossRef]
- Ghosh J, Moise IK, Kalipeni E. The role of regional integration in foreign direct investment in Southern Africa. Advances in Geoeconomics: Routledge; 2017. p. 151-9.
- Moise, IK. Geographic gender differences in traumatic unintentional injury hospitalization and youth drinking. Drug and Alcohol Dependence. 2019, 205, 107701. [Google Scholar] [CrossRef]
- Kolak M, Bhatt J, Park YH, Padrón NA, Molefe A. Quantification of Neighborhood-Level Social Determinants of Health in the Continental United States. JAMA Netw Open. 2020, 3, e1919928. [Google Scholar] [CrossRef] [PubMed]
- Tsai J, Wilson M. COVID-19: a potential public health problem for homeless populations. The Lancet Public health. 2020, 5, e186–e7.
- The DHS Program. Demographic and Health Surveys: The DHS Program,; 2017 [Available from: https://dhsprogram.com/.
- Belmin C, Hoffmann R, Elkasabi M, Pichler P-P. LivWell: a sub-national Dataset on the Living Conditions of Women and their Well-being for 52 Countries. Scientific Data. 2022, 9, 719. [Google Scholar] [CrossRef] [PubMed]
- Smits J, Permanyer I. The Subnational Human Development Database. Sci Data. 2019, 6, 190038.
- Kummu M, Taka M, Guillaume JHA. Gridded global datasets for Gross Domestic Product and Human Development Index over 1990–2015. Scientific Data. 2018, 5, 180004. [Google Scholar] [CrossRef] [PubMed]
- DHS Program. Description of the Demographic and Health Surveys Individual Recode Data File. DHS II; 2008.
- The World Bank pcMsm-li, text-indent:-31.5pt, lfo1 m-lll, border:none, 31.0pt m-p-appp, mso-border-shadow:yes">. Population, total [Available from: https://data.worldbank.org/indicator/SP.POP.TOTL.
- ESRI Inc. ArcGIS Desktop: Release 10. Redlands, California: Environmental Systems Research Institute; 2010.
- IBM SPSS Statistics for Windows, Version 22.0. [Internet]. IBM Corp. 2013.
- Soko ND, Dlamini S, Ntsekhe M, Dandara C. The COVID-19 Pandemic and Explaining Outcomes in Africa: Could Genomic Variation Add to the Debate? OMICS: A Journal of Integrative Biology. 2022, 26, 594–607. [Google Scholar] [CrossRef] [PubMed]
- Rice BL, Annapragada A, Baker RE, Bruijning M, Dotse-Gborgbortsi W, Mensah K, et al. Variation in SARS-CoV-2 outbreaks across sub-Saharan Africa. Nature Medicine. 2021, 27, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Singini GC, Manda SOM. Inter-Country COVID-19 Contagiousness Variation in Eight African Countries. Front Public Health. 2022, 10, 796501. [Google Scholar] [CrossRef] [PubMed]
- Dalal J, Triulzi I, James A, Nguimbis B, Dri GG, Venkatasubramanian A, et al. COVID-19 mortality in women and men in sub-Saharan Africa: a cross-sectional study. BMJ Global Health. 2021, 6, e007225. [Google Scholar] [CrossRef] [PubMed]
- Moon Z, Zuchowski M, Moss-Morris R, Hunter MS, Norton S, Hughes LD. Disparities in access to mobile devices and e-health literacy among breast cancer survivors. Supportive Care in Cancer. 2022, 30, 117–126. [Google Scholar] [CrossRef]
- Ferrell KW, Woodard LM, Woodard TJ. Role of medication therapy management in preexposure prophylaxis therapy for HIV prevention. J Pharm Pract. 2015, 28, 10–12. [Google Scholar] [CrossRef] [PubMed]
- Friedman RH, Kazis LE, Jette A, Smith MB, Stollerman J, Torgerson J, et al. A telecommunications system for monitoring and counseling patients with hypertension. Impact on medication adherence and blood pressure control. Am J Hypertens. 1996, 9, 285–292. [Google Scholar] [CrossRef]
- Pintye J, Rogers Z, Kinuthia J, Mugwanya KK, Abuna F, Lagat H, et al. Two-Way Short Message Service (SMS) Communication May Increase Pre-Exposure Prophylaxis Continuation and Adherence Among Pregnant and Postpartum Women in Kenya. Global health, science and practice. 2020, 8, 55–67. [Google Scholar] [CrossRef] [PubMed]
- Zhuang Z, Cao P, Zhao S, Han L, He D, Yang L. The shortage of hospital beds for COVID-19 and non-COVID-19 patients during the lockdown of Wuhan, China. Ann Transl Med. 2021, 9, 200. [Google Scholar] [CrossRef] [PubMed]
- Alavinejad M, Mellado B, Asgary A, Mbada M, Mathaha T, Lieberman B, et al. Management of hospital beds and ventilators in the Gauteng province, South Africa, during the COVID-19 pandemic. PLOS Global Public Health. 2022, 2, e0001113.
- Naidoo R, Naidoo K. Prioritising ‘already-scarce’ intensive care unit resources in the midst of COVID-19: a call for regional triage committees in South Africa. BMC Medical Ethics. 2021, 22, 28. [Google Scholar]
- Rispel LC, Marshall C, Matiwane B, Tenza IS. Innovations, contestations and fragilities of the health system response to COVID-19 in the Gauteng Province of South Africa. PLoS One. 2021, 16, e0261339. [Google Scholar]
- McQuoid-Mason, DJ. COVID-19: May hospitals in one province of South Africa reserve empty beds for patients from their province and turn down emergency requests from other provinces? S Afr Med J. 2021, 111, 304–306. [Google Scholar] [CrossRef] [PubMed]
- Moise IK, Kalipeni E, Jusrut P, Iwelunmor JI. Assessing the reduction in infant mortality rates in Malawi over the 1990–2010 decades. Global Public Health. 2017, 12, 757–779. [Google Scholar] [CrossRef] [PubMed]
- Bicego GT, Boerma JT. Maternal education and child survival: a comparative study of survey data from 17 countries. Social science & medicine. 1993, 36, 1207–1227. [Google Scholar]
- Dallolio L, Di Gregori V, Lenzi J, Franchino G, Calugi S, Domenighetti G, et al. Socio-economic factors associated with infant mortality in Italy: an ecological study. Int J Equity Health. 2012, 11, 45. [Google Scholar] [CrossRef]
- Kalipeni, E. Determinants of infant mortality in Malawi: a spatial perspective. Soc Sci Med. 1993, 37, 183–198. [Google Scholar] [CrossRef] [PubMed]
- Flor LS, Friedman J, Spencer CN, Cagney J, Arrieta A, Herbert ME, et al. Quantifying the effects of the COVID-19 pandemic on gender equality on health, social, and economic indicators: a comprehensive review of data from March, 2020, to September, 2021. Lancet. 2022, 399, 2381–2397. [Google Scholar] [CrossRef] [PubMed]
- 66. Heo MH, Kwon YD, Cheon J, Kim KB, Noh JW. Association between the Human Development Index and Confirmed COVID-19 Cases by Country. Healthcare (Basel). 2020; 10.
- Faramarzi A, Javan-Noughabi J, Mousavi SA, Bahrami Asl F, Shabanikiya H. Socioeconomic status and COVID-19-related cases and fatalities in the world: A cross-sectional ecological study. Health Science Reports. 2022, 5, e628.
- Desmon, S. COVID-19 Prevention When There’s No Soap and Water 2020 [Available from: https://ccp.jhu.edu/2020/04/13/handwashing-covid-19-no-soap-water/.
- Amegah, AK. Improving handwashing habits and household air quality in Africa after COVID-19. Lancet Glob Health. 2020, 8, e1110–e1. [Google Scholar] [CrossRef] [PubMed]
- Hernán MA, Hernández-Díaz S, Robins JM. A structural approach to selection bias. Epidemiology. 2004, 15, 615–625. [Google Scholar] [CrossRef] [PubMed]
- Cole SR, Platt RW, Schisterman EF, Chu H, Westreich D, Richardson D, et al. Illustrating bias due to conditioning on a collider. International Journal of Epidemiology. 2009, 39, 417–420. [Google Scholar]
Figure 1.
Location of the 34 study countries and the Demographic and Health Survey year conducted, 2010-2018.
Figure 1.
Location of the 34 study countries and the Demographic and Health Survey year conducted, 2010-2018.
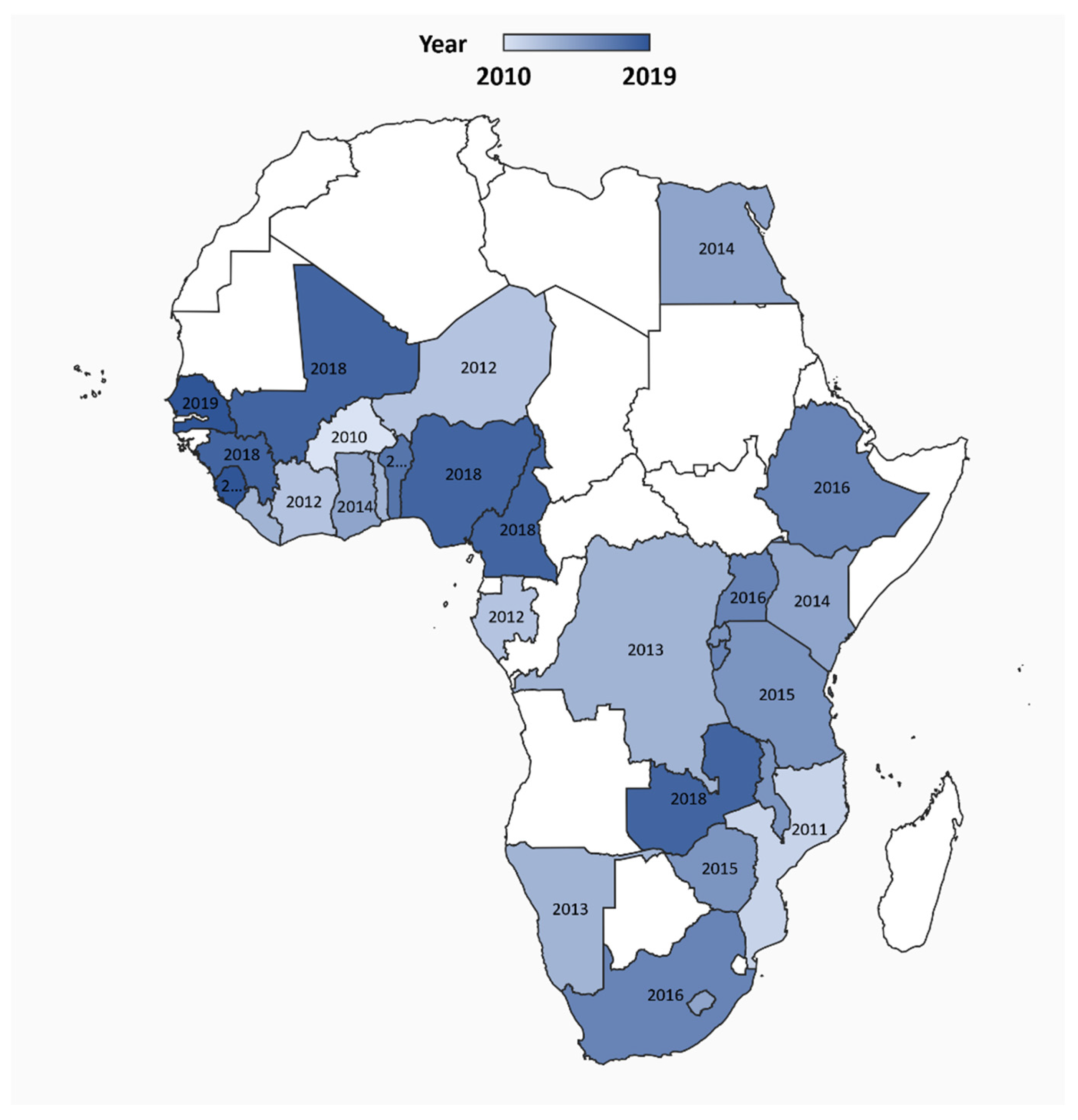
Figure 2.
Distribution of the three-health system measures: 1) medical doctors (2010-2018), 2) ventilators (2020), and 3) hospital beds (2005-2017) in 54 African countries, 2005-2020. Note: Not all countries had data for measures (e.g., for ventilators).
Figure 2.
Distribution of the three-health system measures: 1) medical doctors (2010-2018), 2) ventilators (2020), and 3) hospital beds (2005-2017) in 54 African countries, 2005-2020. Note: Not all countries had data for measures (e.g., for ventilators).


Table 1.
Summary Statistics of Social Determinants of Health Typologies for 28 Study Countries with recent Demographic and Health Surveys, 2010-2018 (n=486,173 surveyed households).
Table 1.
Summary Statistics of Social Determinants of Health Typologies for 28 Study Countries with recent Demographic and Health Surveys, 2010-2018 (n=486,173 surveyed households).
| Social Determinants of Health Measures | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Country | Residency (% households) | Wealth Index (% households) | Educational Status (% head of households) | Sanitation (% households) | Overcrowding (% households) | ||||||
| n | Rural | Urban | Poor | Average | No education | Primary | Secondary or higher | Place to wash hands | Soap or detergent present | >3 people per sleeping room | |
| Benin | 14423 | 55 | 45 | 36.9 | 18.9 | 51.8 | 22.2 | 24.5 | 55.5 | 20.4 | 22.5 |
| Burkina Faso | 14156 | 69.4 | 30.6 | 37.3 | 19.3 | 76.1 | 13 | 10.9 | 80.9 | 17.4 | 18.6 |
| Burundi | 15977 | 81.2 | 18.8 | 41.3 | 18.1 | 47.2 | 39.7 | 13.1 | 98.5 | 7.5 | 13.7 |
| Cameroon | 17223 | 44.8 | 55.2 | 33.2 | 22.5 | 19.4 | 32.9 | 46 | 95.2 | 46.4 | 15.7 |
| Côte d’Ivoire | 4466 | 58.6 | 41.4 | 42.6 | 21.8 | 57.4 | 20.3 | 22.1 | 84.8 | 28.7 | 24.1 |
| DR Congo | 18171 | 70.1 | 29.9 | 49.3 | 19.6 | 14.7 | 32.5 | 52.8 | 92.6 | 37.3 | 28.2 |
| Egypt | 28175 | 50.4 | 49.6 | 34.4 | 16.7 | 25.3 | 15.6 | 59.1 | 97 | 90.8 | 8.4 |
| Ethiopia | 16650 | 68.6 | 31.4 | 42.2 | 12.4 | 52.1 | 28 | 19.6 | 54.3 | 24.3 | 45.6 |
| Gambia | 11835 | 50.2 | 49.8 | 45.7 | 15.1 | 67.1 | 7.4 | 25.3 | 98.9 | 66.9 | 21.3 |
| Ghana | 6215 | 49.8 | 50.2 | 41.7 | 21.8 | 28.3 | 14.1 | 57.6 | 90.2 | 40.2 | 20.2 |
| Guinea | 7912 | 65.9 | 34.1 | 42.2 | 18.8 | 68.4 | 9.8 | 21.3 | 70.2 | 34 | 21.2 |
| Kenya | 36430 | 61.8 | 38.2 | 44.2 | 18.8 | 20.9 | 45.6 | 33.5 | 62.4 | 44.5 | 28.2 |
| Lesotho | 9333 | 70.2 | 29.8 | 42.6 | 19.9 | 17.3 | 53.1 | 27.8 | 7.5 | 47.2 | 15.5 |
| Liberia | 9402 | 63 | 37 | 58.4 | 19.7 | 38.3 | 21.3 | 40.4 | 26.3 | 38.3 | 25.6 |
| Malawi | 9510 | 81.1 | 18.9 | 39 | 19.1 | 15.8 | 56.1 | 27.5 | 84.2 | 14.7 | 19.4 |
| Mali | 26361 | 69 | 31 | 38.3 | 19.6 | 69.4 | 12.8 | 17 | 74 | 24.9 | 21.2 |
| Mozambique | 13919 | 63.4 | 36.6 | 33.7 | 20.2 | 29.6 | 50.9 | 17.5 | 98.6 | 39.1 | 18.9 |
| Namibia | 9840 | 51.6 | 48.4 | 37 | 20.4 | 17.6 | 28.3 | 53.7 | 94.6 | 60.1 | 13 |
| Nigeria | 40427 | 58.5 | 41.5 | 37.4 | 22.1 | 30.7 | 21.2 | 48 | 79.3 | 36.4 | 20.8 |
| Rwanda | 12699 | 77.2 | 22.8 | 42.5 | 18.4 | 25.5 | 60.9 | 13.6 | 76.6 | 54.1 | 11.4 |
| Senegal | 12598 | 62.1 | 37.9 | 52 | 20.1 | 70.6 | 14.2 | 13.4 | 39 | 56.4 | 20.2 |
| Sierra Leone | 4592 | 63.8 | 36.2 | 39.7 | 18.3 | 66 | 9.4 | 24.5 | 89 | 35.8 | 23.7 |
| South Africa | 9548 | 40.8 | 59.2 | 42.8 | 21.3 | 13.4 | 21.1 | 64 | 87.2 | 48.9 | 8.7 |
| Tanzania | 12561 | 71.1 | 28.9 | 34.1 | 20.4 | 20.8 | 60.4 | 18.7 | 77.2 | 59.5 | 17.6 |
| Togo | 19588 | 61.9 | 38.1 | 37.1 | 22.4 | 35.4 | 27.8 | 36.8 | 80.4 | 63.5 | 21.9 |
| Uganda | 11083 | 77.2 | 22.8 | 43.3 | 18.4 | 16.3 | 52 | 30.5 | 57.6 | 45.8 | 26.6 |
| Zambia | 12831 | 63.3 | 36.7 | 44.6 | 20.4 | 9.7 | 42.7 | 45.7 | 52.4 | 40.5 | 25.1 |
| Zimbabwe | 10534 | 58.8 | 41.2 | 32.9 | 16.8 | 6.6 | 31.4 | 61.1 | 97.4 | 45.6 | 15.4 |
Table 2.
Negative Binomial regression of 28 African countries social determinants of health factors on COVID-19 case rates.
Table 2.
Negative Binomial regression of 28 African countries social determinants of health factors on COVID-19 case rates.
| Coefficient | Std. Error | P-value | Odds Ratio 95% Wald CI |
|
|---|---|---|---|---|
| Social Determinants of Health (SDoH) measures | ||||
| Geography | ||||
| Population living in urban areas (%) | -0.042 | 0.048 | 0.384 | 0.959 (0.874 - 1.053) |
| Wealth | ||||
| Human Development Index | -2.387 | 6.525 | 0.715 | 0.092 (0.000 - 32,925.611) |
| Education | ||||
| Women education (%) | 0.089 | 0.054 | 0.102 | 1.093 (0.982 - 1.215) |
| Sanitation | ||||
| Households, quality water access, %) | 0.143 | 0.055 | 0.009 | 1.153 (1.036 - 1.284) |
| Employment | ||||
| Women currently working (%) | -0.041 | 0.046 | 0.379 | 0.96 (0.877 - 1.051) |
| Healthcare access | ||||
| Not having health insurance (%), | 0.232 | 0.059 | 0.001 | 1.262 (1.124 - 1.417) |
| Crowding | ||||
| Average number of householders (> than 3) | -1.735 | 1.069 | 0.105 | 0.176 (0.022 - 1.433) |
| Access to Information | ||||
| Women, mobile phone (%) | 0.089 | 0.046 | 0.053 | 1.093 (0.999 - 1.195) |
| Women listening to the radio at least once a week (%) | 0.061 | 0.057 | 0.284 | 1.063 (0.951 - 1.188) |
| Healthcare System Measures | 0.462 | |||
| Doctor rates per 10,000 population | 1.792 | 4.732 | 0.000 | 5.999 (2.427 - 14.832) |
| Ventilator rates per 10,000 population | 9.086 | 0.314 | 0.055 | 8,826.966 (0.827 - 941,768) |
| Hospital bed rates per 10,000 population | 0.072 | 0.048 | 0.820 | 1.074 (0.58 - 1.988) |
Bold = p < 0.05. CI = Confidence Interval.
Table 3.
Negative Binomial regression of 28 African countries and social determinants of health factors on COVID-19 death rates.
Table 3.
Negative Binomial regression of 28 African countries and social determinants of health factors on COVID-19 death rates.
| Coefficient | Std. Error | P-value | Odds Ratio 95% Wald CI |
|
|---|---|---|---|---|
| Social Determinants of Health (SDoH) measures | ||||
| Geography | ||||
| Population living in urban areas (%) | -0.001 | 0.0010 | 0.166 | 0.999 (0.997 – 1.001 |
| Wealth | ||||
| Human Development Index | -0.182 | 0.1309 | 0.165 | 0.834 (0.645 – 1.078) |
| Education | ||||
| Women education (%) | 0.003 | 0.0011 | 0.014 | 1.003 (1.001 – 1.005) |
| Sanitation | ||||
| Households with high quality water access, %) | 0.004 | 0.0011 | 0.001 | 1.004 (1.002 – 1.006) |
| Employment | ||||
| Women currently working (%) | -0.001 | 0.0009 | 0.247 | 0.999 (0.997 – 1.001) |
| Healthcare Access | ||||
| Insurance coverage (%), | 0.001 | 0.0012 | 0.370 | 1.001 (0.999 – 1.003) |
| Crowding | ||||
| Average number of householders (> than 3) | -0.042 | 0.0214 | 0.051 | 0.959 (0.920 – 1.000) |
| Access to Information | ||||
| Women owning a mobile phone (%) | 0.001 | 0.0009 | 0.181 | 1.001 (0.999 – 1.003) |
| Women listening to the radio at least once a week (%) | 0.002 | 0.0011 | 0.058 | 1.002 (1.000 – 1.004) |
| Healthcare System Measures | ||||
| Doctor rates per 10,000 population | 0.025 | 0.0093 | 0.007 | 1.025 (1.007 – 1.004) |
| Ventilator rates per 10,000 population | -0.107 | 0.0949 | 0.258 | 0.898 (0.746 – 1.082) |
| Hospital bed rates per 10,000 population | 0.013 | 0.0063 | 0.044 | 1.013 (1.000 – 1.025) |
Bold = p < 0.05. CI = Confidence Interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



