Submitted:
17 December 2023
Posted:
18 December 2023
You are already at the latest version
Abstract
The overhead squat movement engages various bodily structures, and its interaction with three-dimensional elastic resistance along the kinetic chain approach remains insufficiently comprehended. This study aimed to describe the scapular kinematics during an overhead squat with the forearm in a supination exercise against an ER and clarify the therapeutic potential of this exercise on scapular rehabilitation. Using an electromagnetic tracking system, we recorded the three-dimensional shoulder kinematics of 19 male participants across seven humeral elevation positions. These positions were captured at 15-degree intervals, spanning from 30 to 120 degrees. The results indicated notable distinctions in scapular upward rotation [F(1,17)=6.09, p=0.024] and scapular posterior tilt [F(1,17)=6.04, p=0.025] between the phases. Furthermore, the interactions revealed significant differences in resistance and phases during humeral elevation for scapular upward/downward rotation [F(3.77,62.48)=7.99, p<0.001], scapular internal/external rotation [F(2.98, 50.64, p<0.001)], and scapular tilt [F(2.58, 43.81)=4.76, p=0.008]. The findings demonstrated that increasing resistance through elastic resistance played a pivotal role in enhancing scapular stability throughout the humerus elevation motion. This underscores the potential of the overhead squat movement as a valuable tool for both shoulder assessment and treatment.
Keywords:
shoulder rehabilitation
; overhead squat
; elastic resistance
; kinetic chain approach
; VETOR 3D
; scapular kinematics
1. Introduction
Human movement is a complex process marked by a seamlessly coordinated sequence of actions, mobilization, and stabilization across various body segments. The interconnection between these segments is known as the kinetic chain [1,2] which consists of the sequential activation of body segments during daily movement patterns and sports gestures, resulting in the transfer of mechanical energy throughout a neuromusculoskeletal chain [3,4]. Such energy transfer initiates in the lower part of the body and progresses upward, passing through the hip and trunk, ultimately aiding in the coordination of upper limb movements [1,5].
In this context, the squat exercise offers several advantages, including lower limb strength training [6], and it replicates components of everyday functional movements like walking, ascending and descending stairs, sitting and standing up [7]. The overhead squat (OHS) stands out among the various types of squats. During the OHS, individuals maintain their hands positioned above their head, gripping the bar with their palms, fully extending their elbows, and pronating their radioulnar joint [8]. Furthermore, executing the OHS demands that the scapula maintains alignment with the thoracic spine while the glenohumeral joint performs arm flexion or abduction movements [8]. Additionally, the OHS serves as a valuable tool for assessing mobility and stability tests for multiple joints.
Within this kinetic chain, when performing squats, limitations can arise that affect the movement. For instance, restrictions in hip and knee mobility in the sagittal plane [9], along with limited ankle dorsiflexion, may lead to medial displacement of the knee [10] and an increased valgus angle [7]. These limitations are important to consider as they can be regarded as potential risk factors for injuries in the lower extremities. Among the advantages of the squat movement, it can serve as a tool for assessing and preventing lower extremity injuries, including patellofemoral syndrome, anterior cruciate ligament injury, and meniscal degeneration [6,11,12,13,14]. Furthermore, it’s worth noting that the positioning of the trunk during the squat movement has been demonstrated to impact the knee extensor muscle action [14,15]. Straub, Barrack, Cannon, and Powers [14] found that during the squat at 60° and 90° of knee flexion, there was an average trunk inclination of 19.6° and 27.6°, respectively. They also observed that for every degree of trunk inclination, there was a decrease of 1.3% to 2.3% in the knee extensor moment. Furthermore, the trunk serves the dual purpose of providing support for the lower body and establishing a stable base for upper quadrant movements. This interconnection between the quadrants is facilitated by myofascial structures, which play a crucial role in forming the kinetic chain. For instance, the thoracolumbar fascia, as part of the crossed muscular chain, links the lower quadrant, represented by the gluteus maximus muscle, to the upper quadrant on the opposite side, connecting through the latissimus dorsi muscle [16]. However, despite the extensive use of the OHS for evaluating the lower quadrant, there remains a limited understanding of its potential for assessing the upper quadrant, particularly the relationship between the trunk and the scapula associated with the context of the kinetic chain.
Shoulder injuries can originate from perturbations within the kinetic chain, either due to its overall deficiency or the presence of "weak links" in specific components such as the core, spine, hip, glenohumeral range of motion, and scapular kinetics [4]. In this regard, the scapula plays a crucial role in bridging the trunk with the upper limb, providing a stable base for the head of the humerus [3,4,17,18], facilitating the transmission of force and energy throughout the kinetic chain, especially during overhead activities when forces need to be efficiently channeled. Therefore, during OHS, it's expected that the scapula will maintain alignment with the thorax, ensuring dynamic stability while allowing controlled mobility. This alignment optimizes the orientation of the humeral head [8]. In addition, the scapula exhibits symmetrical behavior in a closed kinetic chain, particularly above 90˚ of shoulder flexion, where the humerus moves along the thorax during body movement [19]. Furthermore, research suggests that trunk positioning, in conjunction with the lower quadrant, influences scapular kinematics [20,21,22]. However, it remains unclear how the three-dimensional position of the scapula and the humerus change when elastic resistance is incorporated into OHS activity.
Research, including systematic reviews of randomized clinical trials, underscores the importance of therapeutic exercises as the primary treatment approach for alleviating pain, enhancing range of motion [23], and reinstating functionality in individuals with shoulder problems. Current shoulder rehabilitation programs encompass various therapeutic modalities, encompassing pain mitigation techniques, mobility-enhancing exercises, manual therapies, strength conditioning, laser therapy, taping, and acupuncture [23,24]. It's worth noting that therapeutic exercises with resistance hold a prominent position in this spectrum of interventions and have demonstrated their superiority over no intervention at all [23,25]. Within this context, elastic bands emerge as a versatile tool. Their unique properties enable them to be employed in various directions, regardless of the gravitational pull, making them adaptable to a wide range of exercises. These elastic bands can be stretched in any direction, providing consistent and linear resistance [26], which renders them invaluable within the kinetic chain. Furthermore, elastic resistance isn't limited to strength and endurance training [25,27]. It contributes significantly to enhancing the range of motion [28,29], joint stability [30], and improving overall performance [25,27]. Its applicability spans across diverse populations, from the youth to the elderly, as well as athletes. However, many existing approaches primarily emphasize unidirectional resistance, whether in association with the kinetic chain [31,32,33,34] or not [28,35]. What's missing is the full integration of elastic resistance into a kinetic chain approach that permeates the entirety of the activity.
The kinetic chain approach to shoulder rehabilitation is a comprehensive method that promotes coordinated patterns of movement, often referred to as “kinetic chain exercises”. These exercises recognize the integral role of the shoulder within a kinetic link system that encompasses multiple joints, operating in a proximal-to-distal manner. This approach leads to the development of intricately coordinated motor patterns within the shoulder, marking a significant advancement in the field of shoulder rehabilitation.
Indeed, comprehending how the shoulder behaves in various activities, such as the OHS, is crucial in making informed decisions during the rehabilitation process. Integrating exercises that encompass the kinetic chain approach, along with the innovative concept of variation elastic tensional optimized resistive three-dimensional (VETOR 3D), can provide substantial value in the rehabilitation journey. The VETOR 3D concept draws inspiration from principles rooted in the neuromuscular chain, incorporating concepts like proprioceptive neuromuscular facilitation (PNF), dynamic neuromuscular stabilization (DNS), anatomical trains, and Stecco's fascial manipulation into exercise development. Moreover, it holds the potential to significantly enhance muscle endurance in the thoracolumbar and hip regions, refine neuromuscular control in both upper and lower quadrants, and increase joint mobility.
Preserving normal kinematics is crucial for the movement of the upper extremities, and this pursuit of balance lies at the core of the rehabilitation process. It is important to highlight the importance of implementing shoulder rehabilitation strategies that integrate elastic resistance, especially when accompanied by progressive loading. It's essential to recognize that this facet of rehabilitation research remains relatively unexplored. Although some studies explore the use of therapeutic kinetic chain exercises for shoulder rehabilitation, there remains a significant gap in the literature concerning their impact on the shoulder when these exercises are performed with three-dimensional elastic resistance.
Thus, the purpose of this study was to provide a comprehensive description of scapular kinematics during an overhead shoulder exercise (OHS) against an external resistance. Additionally, the study aimed to shed light on how the OHS could be beneficial for shoulder rehabilitation, especially in addressing issues related to scapular dysfunction. In simpler terms, the study sought to explain how a particular exercise impacts the way scapular kinematics and how it could be useful for treating shoulder problems, particularly those involving scapular dysfunction.
2. Materials and Methods
2.1. Participants
Nineteen healthy male subjects voluntarily participated in this study. The subjects were included if were free of shoulder or neck problems in the past 6 months and had no fracture or surgery of the shoulder in the past. The shoulder clinical evaluation comprised five tests to ensure the participants did not suffer from a shoulder disorder: Jobe, Neer, Hawkins, painful arc, or external rotation against resistance [36]. None of the subjects reported any painful item during this examination. For the lower limb, two tests were performed with the aim of identifying any change in the kinetic chain of the lower limb and trunk, the lunge test [37,38] and step-down test [39]. The assessment of the shoulder and lower limb was performed by three physiotherapists (M.A., D.S., and A.P.).
2.1.1. Demographics
Table 1 presents the demographic data of the participants. The study found a significant difference in height between the TheraBand groups (mean difference = 6.20, p = 0.024), while the other demographic variables did not show a significant difference. Additionally, there was no significant difference in intensity between the TheraBand group (mean difference = 3.78, p = 0.264).
2.2. Sample Size Estimation and Ethics
An “a priori” sample size calculation was conducted in G*Power (version 3.1.9.2) with an effect size of 0.25, a significance level of 0.05, a power (1-β error probability) of 0.80, nonsphericity correction ε of 1.0 (ANOVA - Repeated measures test), and partial Ƞ2 of 0.06. The calculation revealed that a total sample size of at least 08 participants in each group was required.
2.3. Instrumentation and data collection
A six-degrees-of-freedom electromagnetic tracking device (Hardware: “FASTRACK” by Polhemus. Inc., Colchester, VT, USA; Software: Motion Monitor v7.0), was used to record shoulder and thorax kinematics. The hardware configuration included a direct current transmitter and four sensors, operating at a frequency of 30 Hz. According to the manufacturer (3SPACE FASTRAK User’s Manual, Revision C. Colchester, VT; Polhemus Inc.; 2002), each sensor provided position information and angular orientation of body segments with 0.3–0.8 mm root mean square (RMS) accuracy for position and 0.15° RMS accuracy for orientation when the sensor receivers are within 76 cm range of the transmitter. To capture scapular motion during arm elevation/depression, test-retest reliability and agreement parameters of the FASTRACK system are, good to excellent when measurements are taken at close intervals (standard error of the measurement [SEM] ranges = [0.9°–2.2°]; intraclass correlation coefficients [ICC] ranges = [0.76–0.99]), and fair to excellent when data is acquired one week apart (SEM ranges = [1.4°–4.9°]; ICC ranges = [0.22–0.92]) [40].
Four sensors were employed in the arrangement: the thorax sensor was positioned above the spinous process of T1, the scapula sensor was situated on the broad flat surface of the posterolateral acromion of the dominant scapula, and the humeral sensor was located on the posterior aspect of the dominant humerus, distal to the triceps muscle belly. To adhere the sensors to the skin, double-sided adhesive disks were used [41]. Thorax and scapula sensors were wrapped using athletic tape to minimize any skin–receiver movement, while the humeral sensor was secured using a customized cuff. A fourth sensor mounted on a handheld stylus (±6.5 cm) was used to digitize bony landmarks and link the sensors to local anatomical coordinate systems (LCS). This enabled us to compute segments and joint rotations by integrating the Local Coordinate Systems (LCSs) with the motions recorded by the sensors, in accordance with the shoulder International Society of Biomechanics (ISB) standardization protocol [41] (Figure 1).
Shoulder bony landmarks were identified through palpation and subsequently digitized using a stylus. Past research indicates that the error related to palpation is approximately 2° [42], and the resulting orientation error of the shoulder bones, resulting from measurement inaccuracy, is less than 2° [43]. During the digitalization process of the bony landmarks, participants assumed a seated position with their eyes fixed forward and their arms positioned alongside their bodies with their palms facing medially.
The anatomical landmarks that were digitized comprised: the eighth thoracic vertebra, the xiphoid process, the seventh cervical vertebrae, the jugular notch, the trigonum spinae scapulae, i.e., the medial scapular border at which the scapular spine intersects, the inferior scapular angle, the glenohumeral joint center, the medial epicondyle, and the lateral epicondyle [41]. The glenohumeral joint center was estimated using a least-squares algorithm [44], as the point that moves the least with respect to the scapula when the humerus is moved passively through several short arcs.
2.4. Data processing
To establish the scapular and humeral position and orientation with respect to the thorax, local coordinate systems were constructed in the thorax, scapula, and humerus, based on the digitization of the anatomical landmarks on each segment. This was achieved by embedding a local coordinate system in each segment, and subsequently by calculating the scapular and humeral position and orientation with respect to the thorax. Scapular rotations were defined with respect to the thorax using a Y, X’, Z’’ Euler sequence, as described in [41]. The first rotation around the y-axis describes the scapular internal (positive) and external (negative) rotation. The second rotation around the rotated x-axis describes upward (positive) and downward rotation (negative). The third rotation around the scapular z-axis describes anterior (negative) and posterior (positive) scapular tilts. Precisely, anterior scapular tilting occurs when the inferior angle of the scapula moves away from the thorax.
The humerus angles were defined both as thoracohumeral angles with respect to the thorax, and as scapulohumeral or glenohumeral angles with respect to the scapula using a Y,X’,Y’’ Euler sequence. The first rotation around the humeral y-axis describes the “plane of arm elevation” (when approaching 0˚ equals the frontal plan and when approaching 90˚ equals the sagittal plan) defined the anterior (positive) and posterior (negative). The second rotation around the x-axis describes the “arm elevation angle” depression (positive) and elevation (negative). The third rotation around the moved y-axis (axial arm rotation) defines the humeral external (negative) and internal (positive) rotation. In this study, only arm elevation angles were considered with negative values.
The thorax kinematics were calculated relative to the global reference coordinate system using a Y, X’, Z Euler sequence, where the first rotation around the world the thorax y-axis describes the left (positive) and right (negative) rotation. The second rotation around the world the thorax x-axis describes the left (negative) and right (positive) flexion. The third rotation around the world the thorax z-axis defines the thorax flexion (negative) and extension (positive).
2.5. Experimental procedures
After digitalization, participants were divided into two groups according to the characteristics of the elastic TheraBand used: LT-B (Low Tension - Blue TheraBand) and HT-B (High Tension - Black TheraBand).
2.5.1. Overhead squat exercise (Description)
Participants were instructed to perform a bilateral arm elevation-depression action while standing, with their upper limbs positioned alongside the body (0º of shoulder flexion). During the elevation phase, they were asked to raise their arms (flexion) synchronously with the flexion movements of their thighs and knees, resembling an overhead squatting action. In the depression phase, participants returned to the initial position by extending their arms, thighs, and knees (Figure 1).
Each subject completed five repetitions of the exercise. This exercise was analyzed in both the absence and inclusion of progressive elastic resistance. The distribution was randomly assigned as follows: R00 – exercises performed without elastic resistance, R01 – exercises performed with elastic resistance from the foot to the upper limbs, and R02 – exercises performed with elastic resistance between the upper and lower limbs.
Two phases of the exercise were considered: the lifting phase, referred to as the "LOAD Phase," where the arm movement occurs against external resistance; and the UNLOAD phase, where both arms return to the initial position with the assistance of gravity and/or the action of the elastic bands. In the R00 condition, the external force was the action of the force of gravity, while in the R01 and R02 conditions, the resistance resulted from the sum of the force of gravity with the tension of the elastic band (TheraBand®, Performance Health, Akron, OH, USA)
2.5.2. Verbal Instructions
All participants were instructed to use the same verbal and visual demonstration of the overhead squat. Participants were asked to stand with feet shoulder-width apart and complete the squat to maximum depth with good trunk control [45]. Participants squatted down as low as they could and return to starting position for five repetitions. For all conditions, standardized instructions were provided (Figure 2). All participants were familiarized with the movement prior to data collection under the supervision of a physiotherapist (F.S. and P.B.).
2.6. Statistic
Dependent variable: On each resistance condition and exercise phase, the scapular motion was described at seven selected humeral elevation positions, ranging from 30° to 120° humerothoracic angles, in 15° increments. On each of these humeral positions, the scapular position was obtained from five repetitions of continuous motion of arm elevation/depression (arm motion).
The normality of the dependent variables was assessed using the Shapiro-Wilk test, in combination with a protocol proposed by Mishra et al. (2019). This protocol calculated Z-scores by dividing the skewness and kurtosis values by their standard errors. A Z-score greater than 1.96 was considered to indicate that the data met the assumptions of normality. A repeated measures analysis of variance (ANOVA) was conducted to assess the impact on scapular and humerus kinematics.
The analysis involved one between-subjects factor, TheraBand (LT-B vs. HT-B), and three within-subject factors: resistance (R00 vs. R01 vs. R02), phase (LOAD vs. UNLOAD), and arm elevation moments. The statistical analysis was conducted with a significance level set at P < 0.05. Mauchly's test was utilized to examine sphericity, and in case of violation, the Greenhouse-Geisser correction was applied. When significant ANOVA effects were observed, post hoc t-tests with the Bonferroni correction were employed to determine significant differences. IBM SPSS version 28 (IBM Corp., Armonk, NY, USA) was utilized for the statistical analysis.
3. Results
3.1. Scapular Upward/downward rotation
During humerothoracic elevation, there was increased upward rotation on load phase for R00 (an average increase of 33.3˚, from an initial position of 5.7˚ to an end position of 39.0˚), R01 (an average increase of 35.1˚, from 5.0˚ to 40.0˚) e R02 (an average increase of 34.3˚, from 5.9˚ to 40.2˚). During the lowering of the arm and shoulder, there was a decrease in upward rotation during the unloading phase. Specifically, R00 showed an average decrease of 35.2˚, going from an initial position of 40.5˚ to an end position of 5.4˚. R01 showed an average decrease of 31.3˚, going from 39.0˚ to 7.6˚, while R02 showed an average decrease of 33.7˚, going from 39.6˚ to 5.9˚.
The study found that there was a significant main effect of phases [F(1,17)=6.09, p=0.024], a post hoc pairwise comparison showed that upward rotation was higher during the unload phase compared to the load phase [df=0.56, p=0.024]. There was a significant interaction between resistance, phase, and moment also showed differences [F(3.77,62.48)=7.99, p<0.001], a post hoc pairwise comparison showed during the load phase, R00 had higher upward rotation than R01 at 45˚ [df=1.92, p<0.001] and at 60˚ [df=1.10, p=0.031]. During the unload phase R01 had higher upward rotation compared to R00 at 30˚ [df=2.25, p=0.021], 45˚ [df=3.01, p=0.005], and 60˚ [df=2.67, p=0.008]. R01 also had higher upward rotation compared to R02 at 45˚ [df=2.18, p=0.012] (Figure 3).
3.2. Scapular Internal/external rotation
During humerothoracic elevation, there was increased internal rotation on load phase for R00 (an average increase of 21.1˚, from an initial position of 23.3˚ to an end position of 44.4˚), R01 (an average increase of 13.1˚, from 31.7˚ to 44.8˚) e R02 (an average increase of 12.6˚, from 30.0˚ to 41.3˚). During the lowering of the arm and chest, there was a reduction in the amount of internal rotation in the unload phase. Specifically, R00 showed an average decrease of 14.8 degrees, starting from an initial position of 44.4 degrees and ending at 29.7 degrees. R01 had an average decrease of 18.3 degrees, starting from 44 degrees and ending at 25.7 degrees. Finally, R02 showed an average decrease of 12.6 degrees, starting from 43.9 degrees and ending at 31.4 degrees.
The study found significant interactions between resistance and moment [F(2.64,44.83)=7.90, p<0.001], a post hoc pairwise comparison showed a greater internal rotation at 30˚ for R02 compared to R00 [df=4.24, p=0.003]. There were significant differences between resistance, phase, and moment [F(2.98, 50.64, p<0.001)], a post hoc pairwise comparison showed during the load phase at 30˚ a greater internal rotation for R01 [df=8.50, p<0.001] and R02 [df=6.81, p=0.031] compared to R00, and at 45˚ for R01 compared to R00 [df=3.00, p=0.028]. During the unload phase R02 showed greater internal rotation compared to R01 at 30˚ [df=5.78, p=0.001], at 45˚ [df=3.39, p=0.011], and at 60˚ [df=2.57, p=0.042].
3.3. Scapular Anterior/posterior tilt
During humerothoracic elevation, there was increased posterior tilt on load phase para R00 (an average increase of 0.5˚, from an initial position of -17.3˚ to an end position of -16.8˚), R01 (an average decrease of 2.0˚, from -15.5˚ to -17.4˚) e R02 (an average increase of 2.0˚, from -17.9˚ to -16.0˚). Along the humeral elevation, R00 and R01 showed an increase in anterior tilt from 45˚ to 105˚, followed by a posterior tilt at 120˚. Similarly, R02 also exhibited an increase in anterior tilt from 45˚ to 90˚ and then a posterior tilt starting from 105˚. During the humerothoracic lowering phase, a reduction in upward rotation was noted across all resistances. Specifically, for R00, there was an average decrease of 1.3˚, transitioning from an initial position of -17.7˚ to a concluding position of -16.4˚. In the case of R01, a slight average increase of 0.6˚ occurred, shifting from -17.5˚ to -18.1˚. Similarly, for R02, an average increase of 0.9˚ was observed, transitioning from -15.9˚ to -16.7˚. As the humerus lowered, a distinctive pattern emerged regarding anterior and posterior tilt. In R00, an increase in anterior tilt was observed between 120˚ and 105˚, followed by a subsequent transition to posterior tilt. This same pattern was mirrored in R01 and R02 between 120˚ and 90˚, with the tilt maintained until 75˚. A posterior tilt was then observed at the 60˚ mark for both R01 and R02, consistently demonstrating a recurrent trend during humerus lowering across the resistances.
The study found that there was a significant main effect during the of phase [F(1,17)=6.04, p=0.025] and a greater difference in posterior tilt during a phase load [df=0.55, p=0.025]. There were also significant differences between resistance and phase [F(2,34)=6.29, p=0.005], a post hoc pairwise comparison showed a greater posterior tilt for R02 during unload phase compared to R01 [df=2.26, p=0.002] (Figure 4). There were significant differences between resistance, and moment [F(2.18, 36.99)=6.61, p=0.003], a post hoc pairwise comparison showed a greater posterior tilt for R00 than R01 at 45˚ [df=1.00, p=0.005], 60˚ [df=1.30, p=0.002], and 75˚ [df=1.15, p=0.010]. There were significant differences between resistance, phase and moment [F(2.58, 43.81)=4.76, p=0.008], a post hoc pairwise comparison showed a greater posterior inclination at 30˚ for R01 compared to R00 [df=1.81, p=0.038] and R02 [df=2.36, p=0.002], while at 45˚ R00 [df=1.82, p=0.040] and R01 [df=2.60, p=0.007] had greater posterior tilt compared to R02. During the unload phase, a greater posterior tilt was observed at 45˚for R00 [df=2.76, p=0.001] and R02 [df=2.13, p=0.010] about R01, at 60˚ for R00 [df=2.92, p= 0.002 ] and R02 [df=2.75, p=0.002] compared to R01, at 75˚ for R00 [df=2.22, p=0.037] and R02 [df=2.79, p=0.001] compared to R01, at 90˚ for R02 compared to R01 [df=2.78, p=0.001], and at 105˚ for R02 compared to R01 [df=2.42, p=0.005] (Figure 5).
4. Discussion
Our study aimed to explore the behavior of the shoulder during an overhead squat with the forearm in supination while gradually increasing the elastic resistance. The findings revealed that using various resistance levels caused disruptions throughout the body's kinetic chain as the resistance interacted with the phase and arm moment. Specifically, we observed differences in scapular upward and internal rotation at 30-60˚, and posterior tilt at 30-105˚.
The results of this study indicate that scapular upward rotation was affected between 30-60˚, which is linked to controlling and stabilizing the scapula so that the humerus can move in a coordinated manner [46,47,48]. Inman, Saunder and Abbot [46] suggest that between 0-60˚ of humerus elevation, there is a higher involvement of the glenohumeral joint and less involvement of the scapulothoracic joint, which aligns with our findings. Our study detected a scapulohumeral rhythm of 4.72 between 30-60˚ and 2.46 between 60-120˚, indicating increased scapular involvement after 60˚ of humerus elevation. McQuade and Smidt [49] found that the scapulohumeral rhythm varied greatly between the start and end of the lifting movement, where the unloaded group had a range of 2.9–7.9:1, the light load group had 3.1–4.3:1, and the maximum effort loading group had 1.9–4.5:1. Our study yielded comparable values for the resistances, with R00 ranging from 2.11 to 3.82:1, R01 ranging from 1.99 to 5.78:1, and R02 ranging from 2.02 to 4.40:1 during the load phase.
The heightened involvement of the scapula becomes more present starting at 60˚ of humeral elevation, contributing to a reduced impact risk. However, it's worth noting that between 50˚ and 70˚, there is an elevated risk of impact due to the narrower distances between the humeral head and acromion [50]. Another study found that individuals with shoulder problems have less upper rotation between 30-60˚ [51], our study included only healthy individuals. During the activity, the resistance R01 showed a higher rotation than R00 and R02 in both phases, particularly during the unloading phase. This difference may be due to a larger moment arm for R01 during the activity compared to R02, which presented a smaller moment arm. At the end of the load phase and the beginning of the unloading phase, a change in behavior between the scapula and the humerus was observed, where the scapula presents a behavior change when moving on the humerus. These results are in line with the study by Turgut, Pedersen, Duzgun and Baltaci [19] who evaluated the kinetic chain and its repercussions on the shoulder using fixation of the distal segment (hand) and observed that during body movement there was an elevation of the humerus about the thorax, a behavior similar to our study. These authors suggest that such behavior may increase proprioceptive information due to the change in behavior provoked by resistance. The scapula is expected to provide a stable base for the humeral head from 90˚ of humeral flexion [17], also contributing to promoting a connection between the shoulder complex and the spine [3,4,17,18], functioning as a bridge for the transmission of force and energy through the kinetic chain. R02 showed a more uniform behavior and a smaller ROM variation between phases compared to R01 and R00. During the unloading phase, a significant angular displacement was noticed between R00 and the other resistors. The results showed that the upper rotation presented behavior like another study [52].
During the load phase, differences were observed in internal rotation ranging from 30 to 60 degrees. Resistance R01 showed a difference to R00 during this phase, while R02 showed a difference to R01 during the unloading phase. At 30 degrees of elevation, internal rotation showed differences greater than 5 degrees for both phases, indicating that using resistance can improve control during the setting phase [53,54]. Posterior tilt, on the other hand, showed a greater number of interactions. During the unload phase for R02, there was a greater posterior displacement about R01 along most of the range of motion. This suggests an increase in resistance due to the activation of the kinetic chain, mainly during the eccentric phase. During the load phase, R01 showed a greater contribution at 30 degrees, while R00 and R01 showed a greater contribution at 45 degrees. No differences were observed between resistances throughout the movement after 45 degrees. Our results showed a smaller angular displacement for the three resistance interactions, which differed from other studies involving humerus elevation movement [51,52]. This difference is because the trunk moves simultaneously with the arm, changing the positioning of the scapula from a vertical posture to an almost horizontal one during the squatting movement. Although muscle activation was not measured, biomechanical data suggest an initial increased activation of the serratus anterior at the beginning of the movement for posterior tilt, followed by increased activation of the lower trapezius as upper rotation "normalizes". This theory should be further investigated, and if supported, could guide an exercise intervention.
According to a study by Camci, Duzgun, Hayran, Baltaci and Karaduman [54], scapular kinematics were compared between active and resisted shoulder elevation in various planes (sagittal, frontal, and scapular). The load group showed greater internal rotation at 30˚ and 60˚ flexion, while the no-load group demonstrated higher upper rotation between 30˚-90˚ flexion and greater posterior tilt. These findings are like our study, which also showed higher values for groups with resistance. Another study by Borms, Maenhout, Berckmans, Spanhove, Vanderstukken and Cools [31] evaluated muscle activity of the scapula in different variations of the kinetic chain in the prone position on the ball. The results showed greater facilitation of lower and middle trapezius activity, inhibition of upper trapezius activity with external rotation, and facilitation of upper trapezius activity with trunk extension. Although our study did not assess muscle activation, kinematic behavior suggests similar results. De Mey, Danneels, Cagnie, Van den Bosch, Flier and Cools [33] evaluated the influence of the kinetic chain on the activation of the upper and lower trapezius muscle, in addition to studying the influence of the position or movement of the trunk and lower extremity on the scapula in overhead athletes. The study found that exercises can be useful in the early stages of scapular rehabilitation training due to trapezius muscle balance. Our study also used the squat, however different from this study which used scapula retraction to activate the kinetic chain. Our study used the ground reaction force associated with resistance to activate the kinetic chain. In this way, incorporates resistance to the subject within the task.
There are some limitations to consider regarding this study. Firstly, the research only involved healthy college men without any recent shoulder or arm pain. This means that the findings may not apply to older or pathological populations. Therefore, future studies should focus on investigating the effects of this exercise on those groups to better understand its role in shoulder rehabilitation. Secondly, this study only collected data at one point in time, so we cannot determine the long-term effects on learning and neuromuscular control. Further studies with follow-up evaluations would be beneficial to understand this behavior over time. Lastly, this study introduces a new concept of using elastic bands with progressive loads, which restricts the comparison of current results to previous findings. Therefore, more studies are necessary to confirm the results of this study. We recommend that future studies incorporate evaluations of ground reaction force to determine how the force generated by the kinetic chain's proximal component affects the shoulder.
5. Conclusions
In summary, this study reveals that augmented load resulted in enhanced scapular stability, facilitating glenohumeral joint mobility. Additionally, the scapulothoracic joint demonstrated heightened stability across the entire range of motion. The VETOR 3D concept combined with overhead squat movement showcases promise as both a valuable tool for shoulder assessment and a potential therapeutic approach for addressing shoulder-related disorders.
Author Contributions
Conceptualization, F.S. and A.P.; methodology, F.S. and A.P.; software, F.S. and A.P.; formal analysis, F.S. and A.P.; investigation, F.S. and A.P.; resources, X.X.; data curation, A.P.; writing—original draft preparation, F.S.; writing—review and editing, F.S. and A.P.; figure preparation, F.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by Ethics Committee of Faculdade de Motricidade Humana, Universidade de Lisboa (CEIFMH n˚: 45/2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Acknowledgments
The authors would like to thank all participants of this study. We would also like to express our gratitude to Pedro Sales Rosário de Castro Botelho, Marta Gonçalves de Sousa Anastácio, Duarte da Graça Santana for their invaluable assistance in the data collection process.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sciascia, A.; Thigpen, C.; Namdari, S.; Baldwin, K. Kinetic chain abnormalities in the athletic shoulder. Sports Med. Arthrosc. Rev. 2012, 20, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Chu, S.K.; Jayabalan, P.; Kibler, W.B.; Press, J. The Kinetic Chain Revisited: New Concepts on Throwing Mechanics and Injury. Pm r 2016, 8, S69–S77. [Google Scholar] [CrossRef] [PubMed]
- Richardson, E.; Lewis, J.S.; Gibson, J.; Morgan, C.; Halaki, M.; Ginn, K.; Yeowell, G. Role of the kinetic chain in shoulder rehabilitation: Does incorporating the trunk and lower limb into shoulder exercise regimes influence shoulder muscle recruitment patterns? Systematic review of electromyography studies. BMJ Open Sport. Exerc. Med. 2020, 6, e000683. [Google Scholar] [CrossRef] [PubMed]
- Zaremski, J.L.; Wasser, J.G.; Vincent, H.K. Mechanisms and Treatments for Shoulder Injuries in Overhead Throwing Athletes. Curr. Sports Med. Rep. 2017, 16, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Oliver, G.D.; Washington, J.K.; Barfield, J.W.; Gascon, S.S.; Gilmer, G. Quantitative Analysis of Proximal and Distal Kinetic Chain Musculature During Dynamic Exercises. J. Strength. Cond. Res. 2018, 32, 1545–1553. [Google Scholar] [CrossRef] [PubMed]
- Forman, D.A.; Forman, G.N.; Button, D.C.; Holmes, M.W.R. THERABAND(R) CLX gold reduces knee-width index and range of motion during overhead, barbell squatting. Sports Biomech. 2021, 20, 198–212. [Google Scholar] [CrossRef] [PubMed]
- Lorenzetti, S.; Ostermann, M.; Zeidler, F.; Zimmer, P.; Jentsch, L.; List, R.; Taylor, W.R.; Schellenberg, F. How to squat? Effects of various stance widths, foot placement angles and level of experience on knee, hip and trunk motion and loading. BMC Sports Sci. Med. Rehabil. 2018, 10, 14. [Google Scholar] [CrossRef]
- Bautista, D.; Durke, D.; Cotter, J.A.; Escobar, K.A.; Schick, E.E. A Comparison of Muscle Activation Among the Front Squat, Overhead Squat, Back Extension and Plank. Int. J. Exerc. Sci. 2020, 13, 714–722. [Google Scholar] [PubMed]
- Heredia, C.; Lockie, R.G.; Lynn, S.K.; Pamukoff, D.N. Comparison of Lower Extremity Kinematics during the Overhead Deep Squat by Functional Movement Screen Score. J. Sports Sci. Med. 2021, 20, 759–765. [Google Scholar] [CrossRef]
- Mauntel, T.C.; Post, E.G.; Padua, D.A.; Bell, D.R. Sex Differences During an Overhead Squat Assessment. J. Appl. Biomech. 2015, 31, 244–249. [Google Scholar] [CrossRef]
- Graber, K.A.; Halverstadt, A.L.; Gill, S.V.; Kulkarni, V.S.; Lewis, C.L. The effect of trunk and shank position on the hip-to-knee moment ratio in a bilateral squat. Phys. Ther. Sport. 2023, 61, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, S.; Tsuda, E.; Yamamoto, Y.; Maeda, S.; Kimura, Y.; Fujita, Y.; Ishibashi, Y. Core-Muscle Training and Neuromuscular Control of the Lower Limb and Trunk. J. Athl. Train. 2019, 54, 959–969. [Google Scholar] [CrossRef] [PubMed]
- Bell, D.R.; Vesci, B.J.; DiStefano, L.J.; Guskiewicz, K.M.; Hirth, C.J.; Padua, D.A. Muscle activity and flexibility in individuals with medial knee displacement during the overhead squat. Athletic Training & Sports Health Care 2012, 4, 117–125. [Google Scholar]
- Straub, R.K.; Barrack, A.J.; Cannon, J.; Powers, C.M. Trunk Inclination During Squatting is a Better Predictor of the Knee-Extensor Moment Than Shank Inclination. J. Sport. Rehabil. 2021, 30, 899–904. [Google Scholar] [CrossRef] [PubMed]
- Powers, C.M. The influence of abnormal hip mechanics on knee injury: A biomechanical perspective. J. Orthop. Sports Phys. Ther. 2010, 40, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Myers, T.W. Trilhos anatômicos Elsevier Brasil: 2010; Volume 2a edição.
- Castelein, B.; Cagnie, B.; Cools, A. Scapular muscle dysfunction associated with subacromial pain syndrome. J. Hand Ther. 2017, 30, 136–146. [Google Scholar] [CrossRef] [PubMed]
- Cools, A.M.; Maenhout, A.G.; Vanderstukken, F.; Decleve, P.; Johansson, F.R.; Borms, D. The challenge of the sporting shoulder: From injury prevention through sport-specific rehabilitation toward return to play. Ann. Phys. Rehabil. Med. 2020, 101384. [Google Scholar] [CrossRef]
- Turgut, E.; Pedersen, O.; Duzgun, I.; Baltaci, G. Three-dimensional scapular kinematics during open and closed kinetic chain movements in asymptomatic and symptomatic subjects. J. Biomech. 2016. [Google Scholar] [CrossRef]
- Miyakoshi, K.; Umehara, J.; Komamura, T.; Ueda, Y.; Tamezawa, T.; Kitamura, G.; Ichihashi, N. Effect of different trunk postures on scapular muscle activities and kinematics during shoulder external rotation. J. Shoulder Elbow Surg. 2019, 28, 2438–2446. [Google Scholar] [CrossRef]
- Takahashi, K.; Yamaji, T.; Wada, N.; Shirakura, K.; Watanabe, H. Trunk kinematics and muscle activities during arm elevation. J. Orthop. Sci. 2015, 20, 624–632. [Google Scholar] [CrossRef]
- Yamauchi, T.; Hasegawa, S.; Matsumura, A.; Nakamura, M.; Ibuki, S.; Ichihashi, N. The effect of trunk rotation during shoulder exercises on the activity of the scapular muscle and scapular kinematics. J. Shoulder Elbow Surg. 2015, 24, 955–964. [Google Scholar] [CrossRef] [PubMed]
- Haik, M.N.; Alburquerque-Sendin, F.; Moreira, R.F.; Pires, E.D.; Camargo, P.R. Effectiveness of physical therapy treatment of clearly defined subacromial pain: A systematic review of randomised controlled trials. Br. J. Sports Med. 2016, 50, 1124–1134. [Google Scholar] [CrossRef] [PubMed]
- Brumitt, J.; Dale, R.B. Integrating shoulder and core exercises when rehabilitating athletes performing overhead activities. N. Am. J. Sports Phys. Ther. 2009, 4, 132–138. [Google Scholar] [PubMed]
- de Oliveira, P.A.; Blasczyk, J.C.; Souza Junior, G.; Lagoa, K.F.; Soares, M.; de Oliveira, R.J.; Filho, P.; Carregaro, R.L.; Martins, W.R. Effects of Elastic Resistance Exercise on Muscle Strength and Functional Performance in Healthy Adults: A Systematic Review and Meta-Analysis. J. Phys. Act. Health 2017, 14, 317–327. [Google Scholar] [CrossRef] [PubMed]
- Picha, K.J.; Almaddah, M.R.; Barker, J.; Ciochetty, T.; Black, W.S.; Uhl, T.L. Elastic Resistance Effectiveness on Increasing Strength of Shoulders and Hips. J. Strength. Cond. Res. 2019, 33, 931–943. [Google Scholar] [CrossRef] [PubMed]
- Seguin, R.C.; Cudlip, A.C.; Holmes, M.W.R. The Efficacy of Upper-Extremity Elastic Resistance Training on Shoulder Strength and Performance: A Systematic Review. Sports (Basel) 2022, 10. [Google Scholar] [CrossRef] [PubMed]
- Haberle, R.; Schellenberg, F.; List, R.; Pluss, M.; Taylor, W.R.; Lorenzetti, S. Comparison of the kinematics and kinetics of shoulder exercises performed with constant and elastic resistance. BMC Sports Sci. Med. Rehabil. 2018, 10, 22. [Google Scholar] [CrossRef]
- Aboodarda, S.J.; Page, P.A.; Behm, D.G. Muscle activation comparisons between elastic and isoinertial resistance: A meta-analysis. Clin Biomech (Bristol, Avon) 2016, 39, 52–61. [Google Scholar] [CrossRef] [PubMed]
- Iversen, V.M.; Mork, P.J.; Vasseljen, O.; Bergquist, R.; Fimland, M.S. Multiple-joint exercises using elastic resistance bands vs. conventional resistance-training equipment: A cross-over study. Eur. J. Sport. Sci. 2017, 17, 973–982. [Google Scholar] [CrossRef]
- Borms, D.; Maenhout, A.; Berckmans, K.; Spanhove, V.; Vanderstukken, F.; Cools, A. Scapulothoracic muscle activity during kinetic chain variations of a prone elevation exercise. Braz. J. Phys. Ther. 2022, 26, 100420. [Google Scholar] [CrossRef]
- Borms, D.; Maenhout, A.; Cools, A.M. Incorporation of the Kinetic Chain Into Shoulder-Elevation Exercises: Does It Affect Scapular Muscle Activity? J. Athl. Train. 2020, 55, 343–349. [Google Scholar] [CrossRef] [PubMed]
- De Mey, K.; Danneels, L.; Cagnie, B.; Van den Bosch, L.; Flier, J.; Cools, A.M. Kinetic chain influences on upper and lower trapezius muscle activation during eight variations of a scapular retraction exercise in overhead athletes. J. Sci. Med. Sport. 2013, 16, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Wasserberger, K.W.; Downs, J.L.; Barfield, J.W.; Williams, T.K.; Oliver, G.D. Lumbopelvic-Hip Complex and Scapular Stabilizing Muscle Activations During Full-Body Exercises With and Without Resistance Bands. J. Strength. Cond. Res. 2020, 34, 2840–2848. [Google Scholar] [CrossRef] [PubMed]
- Haraldsson, B.T.; Andersen, C.H.; Erhardsen, K.T.; Zebis, M.K.; Micheletti, J.K.; Pastre, C.M.; Andersen, L.L. Submaximal Elastic Resistance Band Tests to Estimate Upper and Lower Extremity Maximal Muscle Strength. Int. J. Environ. Res. Public. Health 2021, 18. [Google Scholar] [CrossRef] [PubMed]
- Thigpen, C.A.; Padua, D.A.; Michener, L.A.; Guskiewicz, K.; Giuliani, C.; Keener, J.D.; Stergiou, N. Head and shoulder posture affect scapular mechanics and muscle activity in overhead tasks. J. Electromyogr. Kinesiol. 2010, 20, 701–709. [Google Scholar] [CrossRef] [PubMed]
- Hoch, M.C.; Farwell, K.E.; Gaven, S.L.; Weinhandl, J.T. Weight-Bearing Dorsiflexion Range of Motion and Landing Biomechanics in Individuals With Chronic Ankle Instability. J. Athl. Train. 2015, 50, 833–839. [Google Scholar] [CrossRef] [PubMed]
- Hoch, M.C.; McKeon, P.O. Joint mobilization improves spatiotemporal postural control and range of motion in those with chronic ankle instability. J. Orthop. Res. 2011, 29, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Park, K.M.; Cynn, H.S.; Choung, S.D. Musculoskeletal predictors of movement quality for the forward step-down test in asymptomatic women. J. Orthop. Sports Phys. Ther. 2013, 43, 504–510. [Google Scholar] [CrossRef]
- Lopes, A.D.; Timmons, M.K.; Grover, M.; Ciconelli, R.M.; Michener, L.A. Visual scapular dyskinesis: Kinematics and muscle activity alterations in patients with subacromial impingement syndrome. Arch. Phys. Med. Rehabil. 2015, 96, 298–306. [Google Scholar] [CrossRef]
- Wu, G.; van der Helm, F.C.; Veeger, H.E.; Makhsous, M.; Van Roy, P.; Anglin, C.; Nagels, J.; Karduna, A.R.; McQuade, K.; Wang, X.; et al. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion-Part II: Shoulder, elbow, wrist and hand. Journal of Biomechanics 2005, 38, 981–992. [Google Scholar] [CrossRef]
- Groot, J.H. Kinematic and dynamic analysis of motion and loading. Dissertation, Delft University of Technology,, Delft, The Netherlands, 1998. [Google Scholar]
- Meskers, C.G.M.; Fraterman, H.; Van Der Helm, F.C.T.; Vermeulen, H.M.; Rozing, P.M. Calibration of the ""Flocks of Birds"" electromagnetic tracking device and its application in the shoulder motion studies. Notas para revisão 1997. [Google Scholar] [CrossRef] [PubMed]
- Veeger, H.E. The position of the rotation center of the glenohumeral joint. Journal of Biomechanics 2000, 33, 1711–1715. [Google Scholar] [CrossRef] [PubMed]
- Coyne, L.M.; Newell, M.; Hoozemans, M.J.M.; Morrison, A.; Brown, S.J. Marker location and knee joint constraint affect the reporting of overhead squat kinematics in elite youth football players. Sports Biomech. 2021, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Inman, V.T.; Saunder, M.; Abbot, L.C. Observations of the function of the shoulder joint. Journal Bone Joint Surgery 1944, 26-A, 1–30. [Google Scholar] [CrossRef] [PubMed]
- McClure, P.W.; Michener, L.A.; Sennett, B.J.; Karduna, A.R. Direct 3-dimensional measurement of scapular kinematics during dynamic movements in vivo. J. Shoulder Elbow Surg. 2001, 10, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Yano, Y.; Hamada, J.; Tamai, K.; Yoshizaki, K.; Sahara, R.; Fujiwara, T.; Nohara, Y. Different scapular kinematics in healthy subjects during arm elevation and lowering: Glenohumeral and scapulothoracic patterns. J. Shoulder Elbow Surg. 2010, 19, 209–215. [Google Scholar] [CrossRef] [PubMed]
- McQuade, K.J.; Smidt, G.L. Dynamic scapulohumeral rhythm: The effects of external resistance during elevation of the arm in the scapular plane. J. Orthop. Sports Phys. Ther. 1998, 27, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, R.L.; Braman, J.P.; Ludewig, P.M. The Impact of Decreased Scapulothoracic Upward Rotation on Subacromial Proximities. J. Orthop. Sports Phys. Ther. 2019, 49, 180–191. [Google Scholar] [CrossRef]
- Lawrence, R.L.; Braman, J.P.; Laprade, R.F.; Ludewig, P.M. Comparison of 3-dimensional shoulder complex kinematics in individuals with and without shoulder pain, part 1: Sternoclavicular, acromioclavicular, and scapulothoracic joints. J. Orthop. Sports Phys. Ther. 2014, 44, 636–A638. [Google Scholar] [CrossRef]
- Ludewig, P.M.; Phadke, V.; Braman, J.P.; Hassett, D.R.; Cieminski, C.J.; LaPrade, R.F. Motion of the shoulder complex during multiplanar humeral elevation. J. Bone Joint Surg. Am. 2009, 91, 378–389. [Google Scholar] [CrossRef]
- MacLean, K.F.; Chopp, J.N.; Grewal, T.J.; Picco, B.R.; Dickerson, C.R. Three-dimensional comparison of static and dynamic scapular motion tracking techniques. J. Electromyogr. Kinesiol. 2014, 24, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Camci, E.; Duzgun, I.; Hayran, M.; Baltaci, G.; Karaduman, A. Scapular kinematics during shoulder elevation performed with and without elastic resistance in men without shoulder pathologies. J. Orthop. Sports Phys. Ther. 2013, 43, 735–743. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Overhead Squat Exercise performed at various resistance levels: (A to B) without resistance, (C to D) with R001 level of elastic resistance, and (E to F) with R002 level of elastic resistance.
Figure 1.
Overhead Squat Exercise performed at various resistance levels: (A to B) without resistance, (C to D) with R001 level of elastic resistance, and (E to F) with R002 level of elastic resistance.
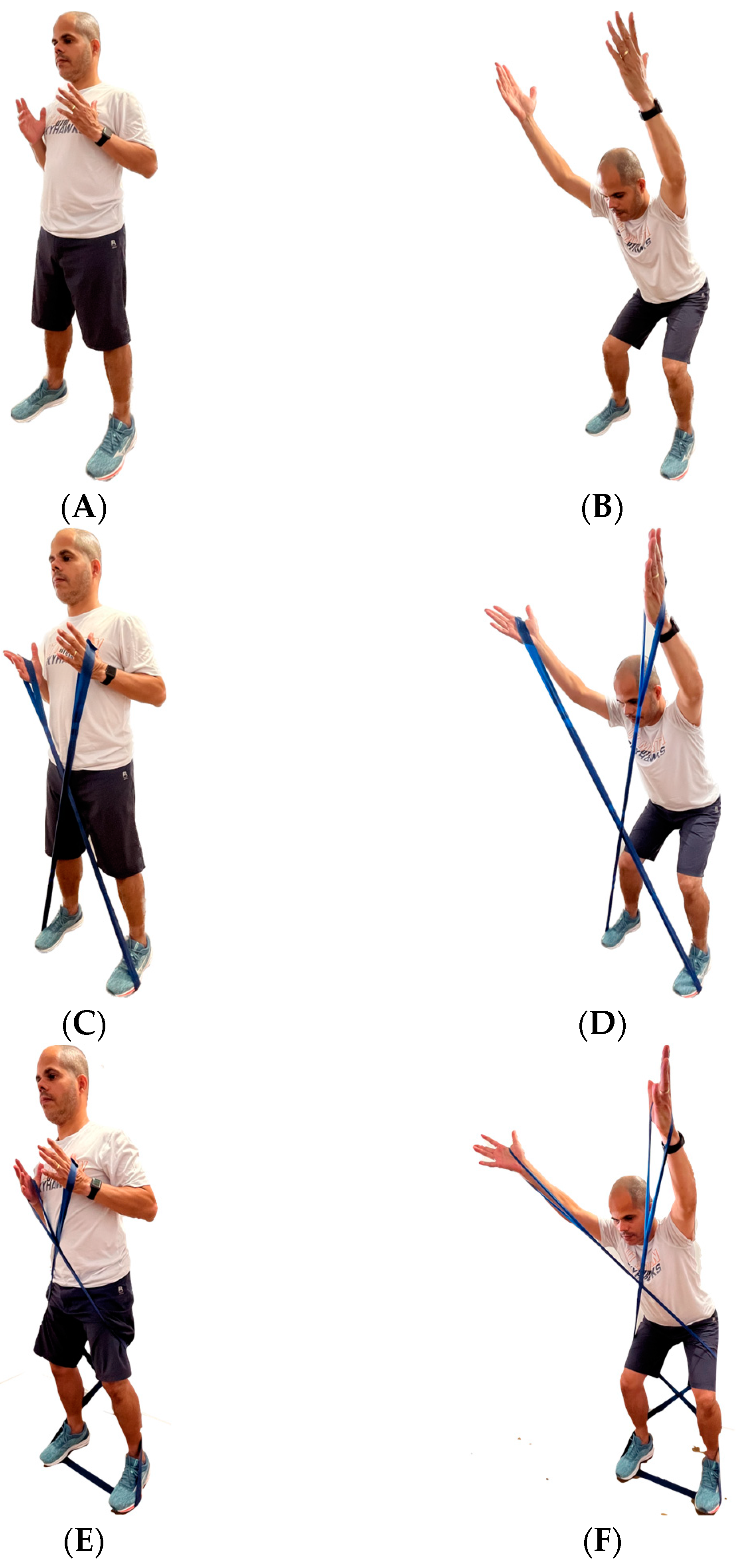
Figure 2.
Standardized instructions for squat performance.
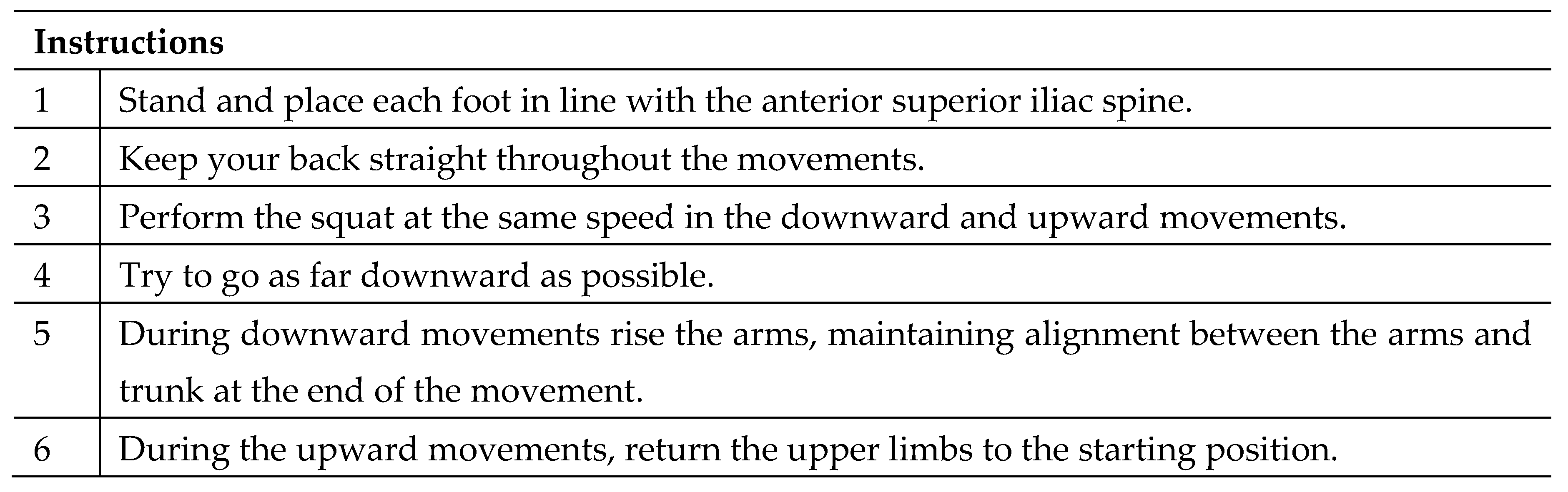
Figure 3.
Scapulothoracic external/internal rotation on interaction resistance vs. phase vs. arm elevation. Abbreviations: p < 0.05 determines significant statistical differences marked: *Load:Phase:R00 vs. R01, **Load:Phase:R00 vs. R02, and ***Load:Phase:R01 vs. R02.
Figure 3.
Scapulothoracic external/internal rotation on interaction resistance vs. phase vs. arm elevation. Abbreviations: p < 0.05 determines significant statistical differences marked: *Load:Phase:R00 vs. R01, **Load:Phase:R00 vs. R02, and ***Load:Phase:R01 vs. R02.
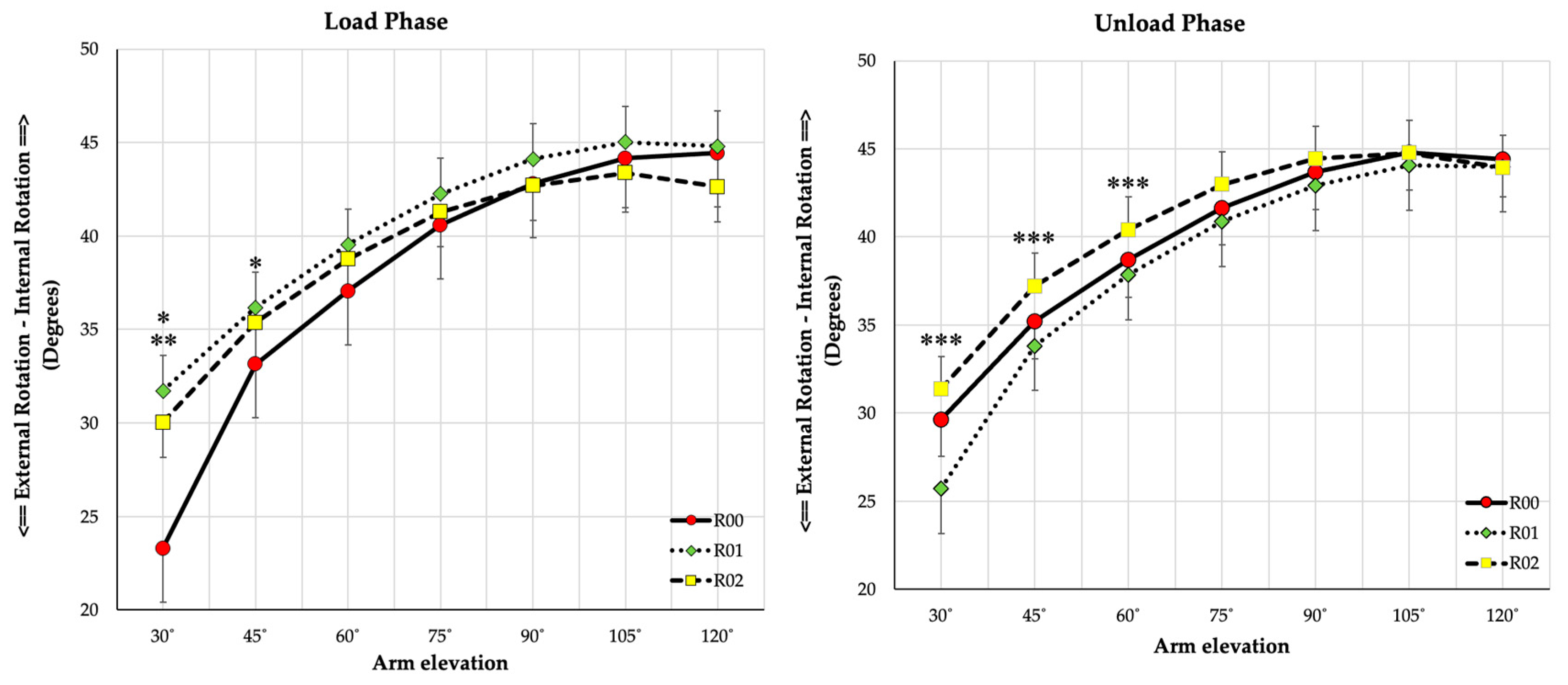
Figure 4.
Scapulothoracic anterior/posterior tilt on interaction resistance vs. phase. Statistical difference between *Load vs. Unload phase, and § Resistance for Unload phase.
Figure 4.
Scapulothoracic anterior/posterior tilt on interaction resistance vs. phase. Statistical difference between *Load vs. Unload phase, and § Resistance for Unload phase.
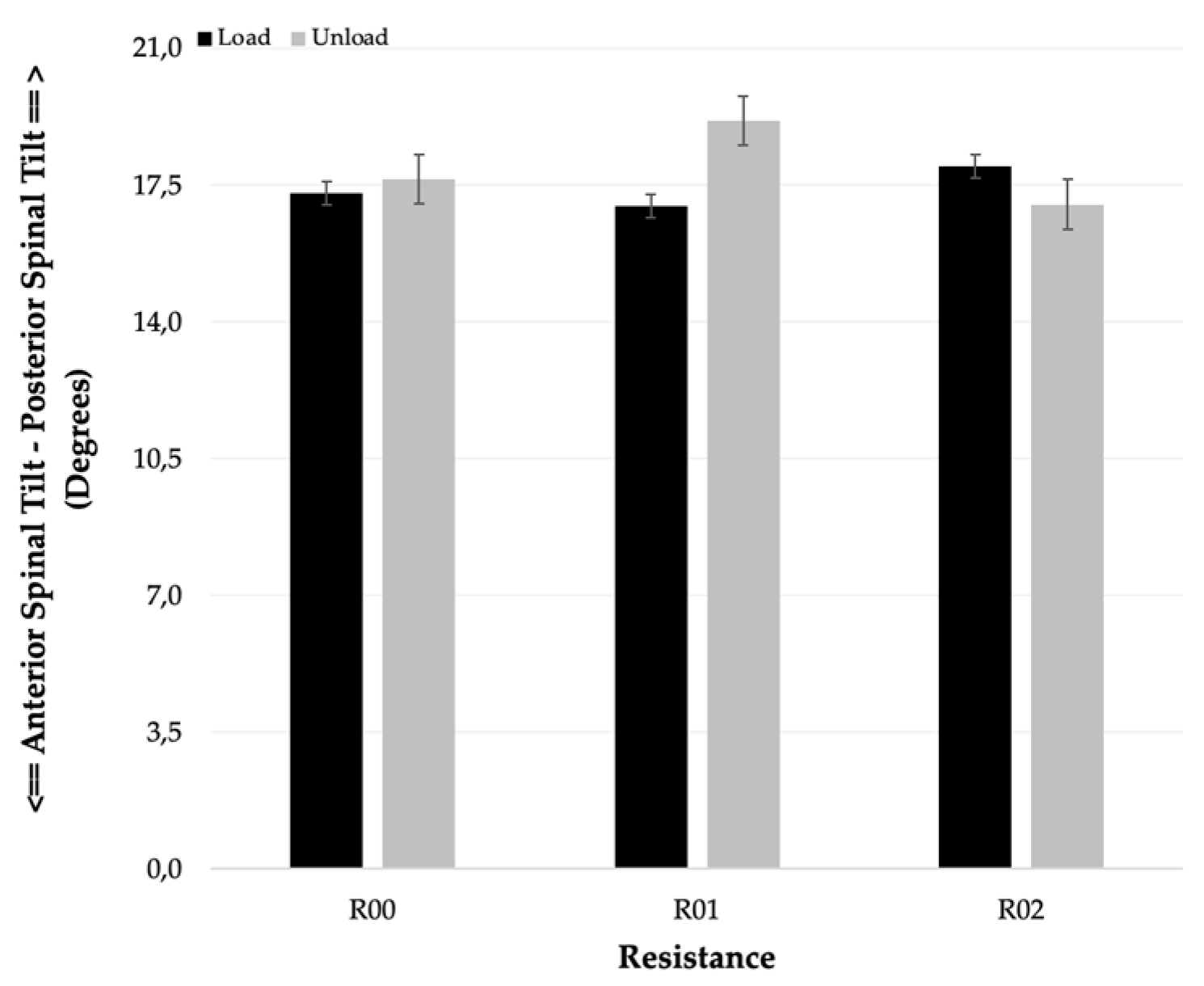
Figure 5.
Scapulothoracic anterior/posterior tilt on interaction resistance vs. phase vs. arm elevation. Abbreviations: p < 0.05 determines significant statistical differences marked: *Load:Phase:R00 vs. R01, **Load:Phase:R00 vs. R02, and ***Load:Phase:R01 vs. R02.
Figure 5.
Scapulothoracic anterior/posterior tilt on interaction resistance vs. phase vs. arm elevation. Abbreviations: p < 0.05 determines significant statistical differences marked: *Load:Phase:R00 vs. R01, **Load:Phase:R00 vs. R02, and ***Load:Phase:R01 vs. R02.
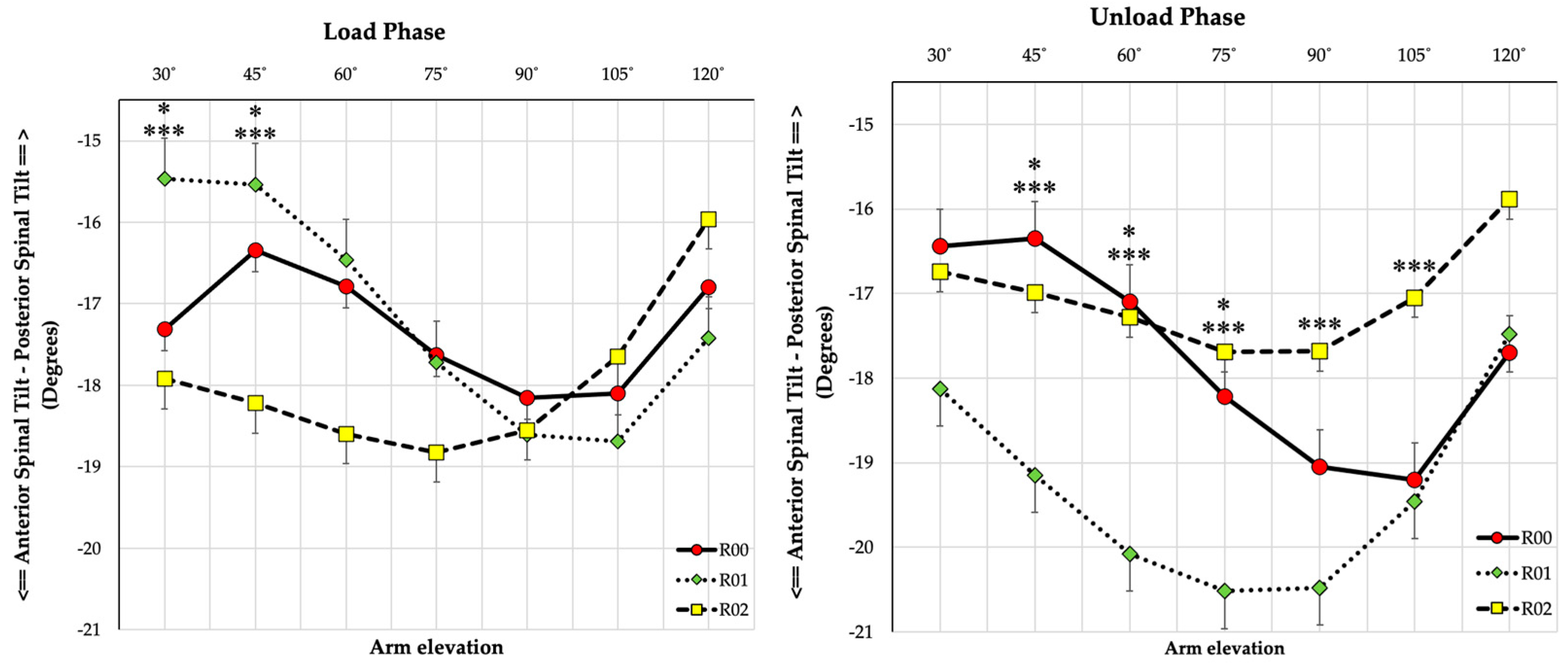

Table 1.
Participant demographics by TheraBand group. Data are presented as mean (SD) unless otherwise indicated.
Table 1.
Participant demographics by TheraBand group. Data are presented as mean (SD) unless otherwise indicated.
| TheraBand Group | Group difference | |||
|---|---|---|---|---|
| Variable | LT-B (n=9) | HT-B (n=10) | 95% CI | p-value |
| Age | 21 (4) | 23 (3) | –4.89, 2.34 | 0.466 |
| Weight (kg) | 76 (9) | 79 (17) | –16.70, 10.99 | 0.474 |
| Heigth (cm) | 179 (5) | 173 (6) | 0.92, 11.47 | 0.024 |
| BMI (Kg/m2) | 23.81 (2.36) | 26.46 (5.15) | –6.60, 1.31 | 0.177 |
| Step.Down.R | 3.33 (1.41) | 3.30 (0.82) | –1.13, 1.20 | 0.952 |
| Step.Down.L | 3.11 (1.05) | 3.4 (1.07) | –1.32, 0.74 | 0.563 |
| Lung.R | 32.89˚ (5.8˚) | 30.5˚ (7.18˚) | –3.97, 8.75 | 0.440 |
| Lung.L | 33.22˚ (4.49˚) | 31.10˚ (6.23˚) | –3.18, 7.43 | 0.411 |
| Exercise (min./week) | 373.33 (246.98) | 283 (181.17) | –117.76, 298.43 | 0.373 |
Groups: LT-B (Low Tension - TheraBand Blue) and HT-B (High Tension - TheraBand Black) according to a previous randomization. BMI - Body Mass Index. R – Right and L – Left. Significant difference observed between conditions (p < 0.05).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



