
Submitted:
02 December 2023
Posted:
04 December 2023
You are already at the latest version
Abstract
Spironucleosis is considered one of the most significant enteric infectious diseases in young and growing game birds. Despite its importance diagnosing spironucleosis in game birds remains a continuing problem as no 'gold standard' test exists and there is no consensus for the use of the available methods for the diagnosis of spironucleosis in game birds. In this study we describe veterinarians’ perceptions of the adoption of existing methods for the diagnosis of spironucleosis in game birds and identify implications for the development of diagnostic guidelines. A questionnaire was used to evaluate participants’ familiarity with and use of existing diagnostic methods for spironucleosis, and to assess their perceptions of the adoption of these methods in their geographic regions. We surveyed veterinarians in practices in East Anglia (EA) and Northern Ireland (NI), UK with expertise or involvement in the treatment and/or diagnosis of spironucleosis in game birds. Of the 261 participants surveyed, 15 EA and 13 NI veterinarians (10.7%) responded to the questions on existing diagnostic methods. The study results indicate an overall insufficient knowledge and skills in the diagnosis and treatment of spironucleosis among veterinarians surveyed. These findings highlight the need for improved training of veterinarians in the diagnosis of spironucleosis.
Keywords:
spironucleosis
; spironucleus
; hexamitosis
; protozoan parasites
; game birds
; diagnosis
; questionnaires
1. Introduction
Spironucleosis is an enteric disease caused by the flagellated diplomonad protozoan Spironucleus (Family Hexamitidae). The disease is characterized by severe loss of condition [1] and various signs of enteritis [2]. Significant mortality has been reported in game bird flocks [3-6], which is evident in pheasants from three weeks of age [7] up to four months of age [6]. Young birds which survive Spironucleus infection become potential carriers for the disease [3,5,8], and could be potential sources of infection for reared birds of a younger age. The incidence of Spironucleus meleagridis in game birds is rapidly growing and spironucleosis is unquestionably one of the major enteric diseases that the industry needs to take notice of [5,9]. It has been reported worldwide in game birds, with cases from Europe to the USA [4,5,8,9,10] and yet S. meleagridis is a vastly understudied organism considering the impact it has on the game bird industry [9]. In 1999, it was estimated that there were over 40 million pheasants and partridges reared every year in the UK with the suggestion that this figure may increase substantially each year  . These birds therefore demand a great deal of costs, such as feed, labour and importantly, treatment of disease.
. These birds therefore demand a great deal of costs, such as feed, labour and importantly, treatment of disease.
. These birds therefore demand a great deal of costs, such as feed, labour and importantly, treatment of disease.Various methods exist for the diagnosis of spironucleosis. However, controversy remains as to the optimal methodology used to effectively establish aetiological diagnosis of spironucleosis in game birds, thus contributing to differences in clinical management [1,2,3,5,11,12]. The majority of these methods requires the examination of freshly killed birds [2,12] or at least dead birds that are still “warm” [11]. Diagnostic tests are based around the demonstration of the motile Spironucleus organisms under a light microscope. One such method utilizes wet smears of intestinal contents using a microscope slide [7,11,12]. Caecal contents have also been used [4,7]. These methods could potentially be misleading as it has recently been found that the protozoa are able to exist in the crypts of Lieberkuhn [13] and even between epithelial cells [5]. Therefore, using intestinal or caecal contents alone may fail to detect protozoa harboured within the gut wall. Instead scrapes from the intestinal or caecal mucosa [1] are more likely to detect any protozoa that may be within the crypts or epithelium. There is some variability in sites sampled for spironucleosis diagnosis. In one study the crypts of the jejunum and ileum were found to have protozoa present [13] whereas a contradicting study states that the parasites are found in the duodenum and jejunum [5]. This latter study is backed up by another which suggests the upper small intestine is where the parasites reside [12].
Despite its economic importance, there is a considerable lack of knowledge about the epidemiology of S. meleagridis. In addition, reliable data are lacking on the best diagnostic approach. How game birds are diagnosed with spironucleosis disease, and how the treatment protocols are put in place are important questions yet to be thoroughly answered. Reported inconsistencies in the methods used to diagnose spironucleosis suggest that there is a general lack of veterinarians’ awareness, recognition, and understanding of spironucleosis, which contribute to deficits in the diagnosis and management of spironucleosis in game birds. Therefore, the study described herein was undertaken to assess the veterinarian’s’ perception of the current testing methods and testing criteria for spironucleosis, as well as to determine the regional differences, including veterinarians from East Anglia (EA) and Northern Ireland (NI) in the diagnostic standards and management of spironucleosis, in hope of identifying specific factors which contribute to the difficulty in diagnosing and managing spironucleosis. Steps could then be taken to improve knowledge and understanding of these specific factors to improve game bird care.
2. Results
2.1. Questionnaire returns
A total of 28 participants completed the questionnaires, including 15 from EA and 13 from NI. Only 7 of 15 (47%) respondents from EA and 4 of 13 (31%) from NI were able to complete the entire questionnaire. The other 21 respondents completed the questionnaire as far as their knowledge would allow and any remaining uncompleted questions were excluded from analysis. Of the list of practices provided by the RCVS this translates to a response rate of 8% of practices in EA (15 of 200) and 21% in NI (13 of 61).
2.2. Participants’ charactaeristics
Here, the participants were asked 5 questions to determine the nature of the veterinary practice and how many, if any, veterinarians practice there is established, and proportion of the caseload involving game birds, which game bird they see most often and at what age.
2.2.1. Practice type
Eighteen of the 28 (64%) participating practices were mixed animal practices, 53% in EA and 77% in NI. In NI neither purely small animal nor large animal practices participated, however in EA three (20%) small animal practices and one (7%) large animal practice were interviewed. Specialist poultry practices constituted 13% (2 of 15) of EA responses and 8% (1 out of 13) of NI. One laboratory from EA (7%) and two from NI (15%) also participated (Table 1; Figure A1).
2.2.2. Associated veterinarians
Grouping the data into groups of < 7 veterinarians to represent small practices and groups of > 7 veterinarians to represent large practices allowed the one EA respondent not associated with any veterinarians to be disregarded. No statistically significant difference was found between the numbers of associated veterinarians in both regions. The largest participating practice in each region had 13 and 14 practicing veterinarians from EA and NI, respectively (Table 1; Figure A2).
2.2.3. Game bird caseload
Twenty-six of the total 28 (93%) respondents stated that game bird work represents < 5% of their caseload; 14 (93%) of which were from EA and 12 (92%) from NI. One practice from each region (8% of NI respondents and 7% of EA respondents) had a higher exposure to game birds with 5-25% of their caseload consisting of game bird work (Table 1; Figure A3).
2.2.4. Most common breed of game birds
Pheasants were the most common game bird seen by participating practices in EA and NI. Partridges were encountered by significantly more respondents from EA than NI. In NI 100% of the respondents seen mostly pheasants compared to 10 of 15 (67%) respondents in EA. In EA partridges were seen by 13% of the practices and partridges and pheasants in equal measure by 20% (Table 1; Figure A4).
2.2.5. Most common age of game birds
Poults were the most common age of birds seen in both the regions; seen by 80% of respondents in EA and 54% in NI. Each region had 1 respondent who most frequently seen adult birds (7% of respondents in EA and 8% in NI). Chicks were most frequently seen by one respondent in EA (7%), but none in NI. Chicks and poults in equal measure were seen most frequently by 7% of EA respondents and by 38% of NI respondents (Table 1; Figure A5).
2.3. Preliminary questions
Here, we investigated which bodily system was most often affected in the presented game birds and determined how the cases are handled and the participant’s position on prescribing drugs.
2.3.1. Bodily system most often treated/diagnosed
In both regions game birds with gastrointestinal disorders were the most frequently seen case; treated or diagnosed by 12 of 15 (80%) practices in EA and 9 of 13 (69%) in NI. Respiratory diseases were seen by two (13%) practices in EA and by two (15%) practices in NI. No practices in either NI or EA stated that musculoskeletal, reproductive or any other bodily systems were the most frequently treated or diagnosed. However, gastrointestinal, and respiratory diseases in equal measure were experienced by 7% of EA practices and 15% of practices in NI (Table 2; Figure A6).
2.3.2. Location of diagnosis
The most common location for veterinarians to make diagnoses of disorders in game birds in both regions was on site at the practice, as stated by 11 out of 15 (73%) respondents in EA and 7 out of 13 (54%) in NI. Twenty percent of respondents from EA diagnose on location, at the game farm, compared to only 8% of NI respondents. Five (38%) respondents in NI stated that they made their diagnoses elsewhere, neither on site nor on location, as did one (7%) respondent in EA (Table 2; Figure A7). There is no statistically significant difference between regions when comparing whether diagnoses are made at the practice or at the game farm.
2.3.3. Drug prescription
2.3.4. Treatment protocol
When asked whether respondents insist on seeing the affected game birds before constructing a treatment plan, four of 13 (31%) practices in NI stated that they insist on seeing the birds initially compared to eight of 15 (53%) practices in EA. Instead, most practices in NI (54%) do not insist on seeing the birds at all before commencing treatment whereas in EA only four of 15 (27%) do not insist on seeing the birds initially. Two practices (13%) in NI and three (20%) in EA answered with ‘Other’ (Table 2; Figure A9). No statistically significant difference exists between regions for this question. However, it may suggest a trend that respondents from EA are more likely to see birds before prescribing treatment than those from NI.
2.4. Importance and perception of enteric disease
Here, we investigated the respondent’s opinion on how willing members of the game industry are to approach veterinarians for advice and treatment option. Additionally, we asked the respondents to assign importance to both enteric disease and to hexamitosis /spironucleosis on a scale of one to 10, where a score of one indicated the lowest importance and 10 the highest importance. The questions enabled the interviewer to establish the respondent’s knowledge on this Hexamita/Spironucleus and whether they can proceed to further sections of the questionnaire or not.
2.4.1. Eagerness of game farmers to consult veterinarians
When asked their opinion on how willing game farmers are to consult veterinarians for treatment and diagnosis of birds most respondents in EA, seven of 15 (47%), stated that they are very willing. However, in NI most respondents, six of 13 (46%), stated that game farmers are unwilling to consult veterinarians. One respondent answered ‘Unknown’ to this question. The data was grouped into either willing (comprising of ‘very willing’ and ‘somewhat willing’ responses) or unwilling (comprising of ‘unwilling’ and ‘never will consult a vet’ responses) groups with the ‘unknown’ response being disregarded. This allowed for analysis using the Fisher’s Exact Test and although no statistically significant difference exists for this question (P = 0.057), it does suggest a trend that game farmers in EA are more willing to consult veterinarians for treatment, advice, and diagnosis than in NI (Table 3; Figure A10).
2.4.2. Enteric disease investigation
In total, 47% of practices in EA sent birds suspected to have an enteric disorder elsewhere to be diagnosed and an equal number (47%) carried out investigation into enteric disease themselves on site. In NI most practices, eight of 13 (62%), sent cases of suspected enteric disease elsewhere to be diagnosed and 38% carried out the diagnosis themselves. The difference between regions was not significant. One practice (7%) in EA and none in NI answered ‘Other’ (Table 3; Figure A11).
2.4.3. Importance assigned to enteric disease
Each participant was asked to assign a number from 1 – 10 to express the importance of enteric disease in game birds, one carrying the least importance and 10 the most. Answers were grouped; 0-5 meaning it is of little importance and 6-10 meaning it is of high importance. There was no statistically significant difference between regions. In EA two of 15 (13%) respondents considered enteric disease of game birds to be of little importance compared to zero respondents from NI. 100% of NI respondents and 87% of EA respondents considered enteric disease of game birds to be of high importance (Table 3; Figure A12).
2.4.4. Most common causative agent of enteric disease
Coccidian species were the most common causative agent of enteric disease of game birds by both regions; described by 11 of 14 (79%) respondents from EA and six out of 13 (46%) respondents from NI. 29% of EA respondents stated Spironucleus as did 15% of NI respondents. EA respondents also indicated histomoniasis (7%) and Rotavirus infections (7%); however, in NI these were not indicated at all. Bacterial infections were described by two (15%) respondents in NI and one (7%) in EA. One (8%) NI respondent also suggested gapeworms; however, this was not specified by any respondents from EA. 23% of NI respondents and 7% of EA respondents answered ‘Unknown’ to this question (Table 3; Figure A13).
2.4.5. Importance assigned to spironucleosis
Each participant was asked to assign a number from 1 – 10 to express the importance of spironucleosis in game birds, 1 carrying the least importance and 10 the most. Answers were grouped; 0-5 meaning it is of little importance and 6-10 meaning it is of high importance. Sixty percent of NI respondents and 50% of EA respondents considered spironucleosis of game birds to be of high importance. No statistically significant difference exists between regions for this question (Table 3; Figure A14).
2.4.6. Rearing stage(s) most closely associated with Spironucleus infection
Zero respondents from either region suggested the laying pens, hatchery, or release pens alone to be most closely associated with Spironucleus infections. Instead, each region experienced cases of spironucleosis in the rearing field and in the rearing field & release pen in equal measure. Five of 12 (42%) respondents from EA stated that the rearing field was most closely associated with Spironucleus as did two of five (40%) respondents from NI. The remaining 60% of NI respondents stated that they experience spironucleosis in the rearing field & release pen in equal measure. 17 % of EA respondents also stated this. Forty-two per cent of EA respondents answered this question with ‘Unknown’ (Table 3; Figure A15).
2.5. Sample collection and adoption of existing methods
In this part of the survey the veterinarians were asked questions regarding their approach of sample collection and perception of the adoption of existing methods for the diagnosis of spironucleosis in game birds.
2.5.1. Selection of sample birds
12 out of 13 respondents (92%) from both regions stated that the client (game keeper) collects the birds to be used as samples for diagnosis. This was stated by 100% of EA respondents and 75% of NI respondents. In 1 practice from NI (25%) the veterinarian collects the samples (Table 4; Figure A16).
2.5.2. Sample birds removed from flocks
Neither region selected dead birds alone nor living non-clinically infected birds alone for diagnosis of spironucleosis. Most birds taken for samples by respondents from EA, 5 out of 9 respondents (56%), were a combination of dead and alive birds whereas this was the case for only 25% of NI respondents. Instead, most birds taken by NI respondents were living clinically infected birds (75%), which were also practiced by 33% of EA respondents. One EA practice (11%) also selected a combination of living clinically infected and non-clinically infected birds; this was not practised by any NI participants (Table 4; Figure A17).
2.5.3. Clinically infected flock
Most practices in both regions, 3 out of 4 in NI (75%) and 5 out of 8 in EA (63%), didn’t isolate and/or euthanise any remaining clinically infected birds after the sample birds had been removed for diagnosis. One practice in NI (25%) and 3 in EA (38%) did isolate and/or euthanise remaining clinically infected birds (Table 4; Figure A18).
2.5.4. Method of euthanasia
Throughout participants in EA the main method of euthanasia of collected birds was via cervical dislocation, carried out by 5 out of 8 practices (63%). The remaining practices (38%) used IV barbiturates and zero EA respondents used gas. In contrast the major method of euthanasia used by participants from NI was via gas, implemented by 2 out of 4 practices (50%). One NI respondent (25%) used cervical dislocation and a further one NI respondent (25%) used IV barbiturates (Table 4; Figure A19).
2.5.5. Time between death and examination
Nine out of 12 respondents (75%) from both regions examined the sample bird for diagnosis of spironucleosis less than 5 minutes after death. 100% of all NI respondents examined the bird in less than 5 minutes whereas only 5 out 8 (63%) EA respondents did so. 25% of EA respondents examined the sample bird 5-10 minutes after death and one EA respondent (13%) answered ‘Other’ (Table 4; Figure A20).
2.5.6. Time limit for diagnosis of spironucleosis
Most respondents from both regions (71% of EA respondents and 75% of NI respondents) stated that they have in place a time limit between death of the sample bird and examination for Spironucleus. Two respondents from EA (29%) and one from NI (25%) stated they do not implement a time limit and will attempt to diagnose Spironucleus in the sample bird regardless of time since death (Table 4; Figure A21).
2.6. Spironucleosis diagnosis questions
In this part of the survey veterinarians from EA and NI were asked 18 questions regarding the adoption of existing methods for the diagnosis of spironucleosis in game birds.
2.6.1. Clinical signs associated with spironucleosis
The most described clinical sign associated with spironucleosis in EA was abnormal faeces/diarrhoea described by 6 out of the 7 respondents (86%). This was closely followed by thin, ill thrifty birds described by 71% of EA respondents. Only 2 practices from NI (50%) described thinness/ill thrift as a common clinical sign. In NI the two most described clinical signs were mortality (100%) and abnormal faeces/diarrhoea (75%). Only 1 practice from EA described mortality (14%). Respondents from EA also described depression (57%), dehydrated birds (14%), lethargic birds (14%), birds with altered gait and/or hunched over (14%), birds with ruffled feathers (14%) and general malaise (14%). General malaise was also noted by 50% of NI respondents as was depression (50%) (Table 5; Figure A22).
2.6.2. Post-mortem protocol for cases of enteric disease
One hundred per cent of all respondents stated that a full post-mortem was always carried out for cases of suspected enteric disease (Table 5; Figure A23).
2.6.3. Pathological changes visible on external examination
Four out of 7 respondents from EA (57%) considered no visible changes to be seen on external examination of birds infected with Spironucleus whereas only 1 respondent from NI considered this (25%). The most common changes among NI respondents were dehydrated birds (75%) and excrement visible around the bird’s rear vent (75%). Only 14% of EA respondents described dehydrated carcasses and only 7% of EA respondents described a dirty vent. Both regions described thinness/razor keel (50% of NI respondents and 29% of EA respondents). NI responses also included ruffled feathers (25%) and poor growth (50%) neither of which was described by any respondents from EA. One respondent from EA (14%) answered this question with ‘Unknown’ (Table 5; Figure A24).
2.6.4. Pathological changes visible on internal examination
The most frequently described internal changes visible on gross examination of a bird infected with Spironucleus by both regions were frothy gut content as described by 5 out of 7 EA respondents (71%) and 3 out of 4 NI respondents (75%). Frothy caecal contents were described by 43% of EA and by 25% of NI respondents. A distended caecum was also described by 3 EA (43%) and 1 NI (25%) respondent however a distended gut was described by only 1 EA (14%) and zero NI respondents. Yellow caecal contents were a common description by both regions (25% of NI and 14% of EA respondents). The final common internal change described by both regions was enteritis, stated by 2 NI (50%) and 1 EA (14%) respondent. Yellow gut contents (14%), dehydration (14%), poor crop fill (14%) and visible urates (14%) all were described by EA respondents but not by NI respondents. Liver lesions were stated by 1 NI respondent (25%) (Table 5; Figure A25).
2.6.5. Sites used for spironucleosis diagnosis
In both regions the caecum proved to be the most used area for spironucleosis diagnosis, 7 respondents utilising it in EA (100%) and 3 in NI (75%). Five respondents from EA (71%) used the duodenum as did 2 respondents from NI (50%). Fifty per cent of NI respondents utilised the distal small intestine for diagnosis; however, this was not described in EA. The same occurs for the use of the rectum, which was used by 25% of NI respondents but none in EA. On the other hand, practices in EA utilised both the mid small intestine (14%) and the large intestine (14%) neither of which were described by any respondents from NI. It must also be noted that 1 practice from each region (14% of EA respondents and 25% of NI respondents) described the whole of the small intestine as a site for spironucleosis diagnosis (Table 5; Figure A26).
2.6.6. Spironucleosis diagnosis
Contents vs. scrapes: Most respondents from EA, 5 out of 7 (71%), used lumen contents alone for diagnosis of spironucleosis. Instead, the preferred method by respondents in NI was to use mucosal scrapes (75%). Between regions no statistically significant difference exists for the use of either lumen contents or mucosal scrapes. Twenty-nine per cent of EA respondents utilised both lumen contents and mucosal scrapes simultaneously for diagnosis however this was not described by any NI respondents.
Magnification: 40x magnification was the most frequently used magnification in both regions; described by 3 respondents from EA (43%) and 2 from NI (50%); 25 x magnification was used by 1 respondent from NI (25%) and 1 respondent from EA (14%). Other magnifications described include x50 by 1 NI respondent (25%) and a range of x20-40 by 1 EA respondent (14%). In addition to this, a high magnification was described by 1 EA respondent (14%), a medium by 1 NI respondent (25%) and a low magnification by 1 EA respondent (14%).
Dilution: The collected sample was diluted by 3 NI (75%) and 1 EA (14%) respondents. In addition to this 1 EA respondent (14%) diluted their sample with iodine, which was the only description of this throughout both regions. Although a trend may be observed these differences are not statistically significant.
Slide preparation: Four EA (57%) and 2 NI (50%) respondents described the use of a coverslip on the slide, 1 NI respondent (25%) also described the suspension of the coverslip using a ring of Vaseline. Significantly more NI respondents (75%) pre-heated the slide than in EA. The slide was inverted by 1 NI respondent (25%) and 1 respondent from EA (14%) rinsed off the lumen contents before making a scrape. Twenty-five per cent of NI and 14% of EA respondents used a scalpel blade to make the mucosal scrape (Table 5; Figure A27).
2.6.7. Positive result confirmation
All respondents across both regions considered motile protozoa to be most crucial. Other factors considered crucial in confirming a positive result by EA respondents were large numbers of protozoa (43%), a suitable/specific history (14%) and specific lesions on gross examination (14%) (Table 5; Figure A28). Regarding the negative result description, all the respondents responded with a lack of motile protozoa to be the defining factor of a negative result.
2.6.8. Utilisation of faeces for spironucleosis diagnosis
Most respondents from both regions considered the utilisation of faeces in the diagnosis of spironucleosis to be impossible (55% of all respondents). Three respondents from NI (75%) stated this as did 3 respondents from EA (43%). Twenty-nine per cent of EA and 25% of NI respondents believed that faeces could be used for diagnosis. Two respondents from EA (29%) answered this question with ‘Unknown’ (Table 5; Figure A29).
2.6.9. Morphological appearance of Spironucleus
Spironucleus was described as motile by most EA respondents, 5 out of 7 (71%), along with 3 out of 4 NI respondents (75%). One hundred per cent of NI respondents described the protozoan as being flagellated contrasted to 29% of EA respondents. Another common description was being described as small by 57% of EA and 50% of NI respondents. Respondents in EA compared Spironucleus to Trichomonas and described it as being relatively smaller (29%) and faster (14%). Fourteen per cent of EA respondents also described Spironucleus as transparent; however, this was not described by any NI respondents. In terms of its’ shape, both regions commonly described Spironucleus as oval shaped (25% of NI and 14% of EA respondents) and spindle shaped (25% of NI and 14% of EA respondents). In addition to this, 1 respondent (14%) from EA described it as being drop shaped and another 1 (14%) as being “maggot” shaped. One NI respondent (25%) termed Spironucleus as circular (Table 5; Figure A30).
2.6.10. Spironucleus differentiation
A majority of both NI (100%) and EA respondents (5 out of 7, 71%) stated it was difficult to differentiate Spironucleus from other protozoa without a history being provided. However, 29% of EA respondents considered it relatively easy to differentiate from other protozoa. No statistically significant differences exist between regions for this question (Table 5; Figure A31).
2.6.11. Confirmation of infection in a bird
One hundred percent of NI respondents and 6 out of 7 EA respondents (86%) stated that only one sample needs to test positive to confirm spironucleosis in a bird. One EA respondent (14%) considered two positive samples to be needed (Table 5; Figure A32).
2.6.12. Confirmation of infection in a flock
One hundred percent of NI respondents and 3 out of 7 EA respondents (43%) believe that only one infected bird is needed to confirm spironucleosis in a flock of birds. 14% of EA respondents believe two birds are needed, and a further 14% of EA respondents believe three birds are needed while 2 EA respondents (29%) answered this question with ‘Other’. No statistically significant differences exist for this question (Table 5; Figure A33).
2.6.13. Quantifying spironucleosis
Significantly more NI respondents (4 out of 4) than EA respondents (0 out of 7) believed it was possible to quantify Spironucleus infection levels. Most EA respondents (6 out of 7) believed it to be impossible and 14% of EA respondents answered this question with ‘Unknown’ (Table 5; Figure A34).
2.6.14. Reliance on stated method
100% of all respondents across both regions stated that they always rely on their stated method of diagnosis for spironucleosis and never rely on gross post-mortem findings alone (Table 5; Figure A35).
2.6.15. Knowledge of other methods
100% of EA respondents and 3 out of 4 NI respondents (75%) did not know of any other methods used to diagnose spironucleosis. One participant from NI (25%) knew of other available methods (Table 5; Figure A36).
2.6.16. Reproducibility in general practice
One hundred percent of all respondents believe their method of diagnosis to be reproducible in general practice (Table 5; Figure A37).
2.6.17. Spironucleosis diagnosis in general practice
Most respondents across both regions believed that the diagnosis of spironucleosis is not carried out in general practice (58%). This was stated by 80% of NI and 43% of EA respondents. Two respondents from EA (29%) believed it is carried out in general practice while 29% of EA and 20% of NI respondents answered this question ‘Unknown’ (Table 5; Figure A38).
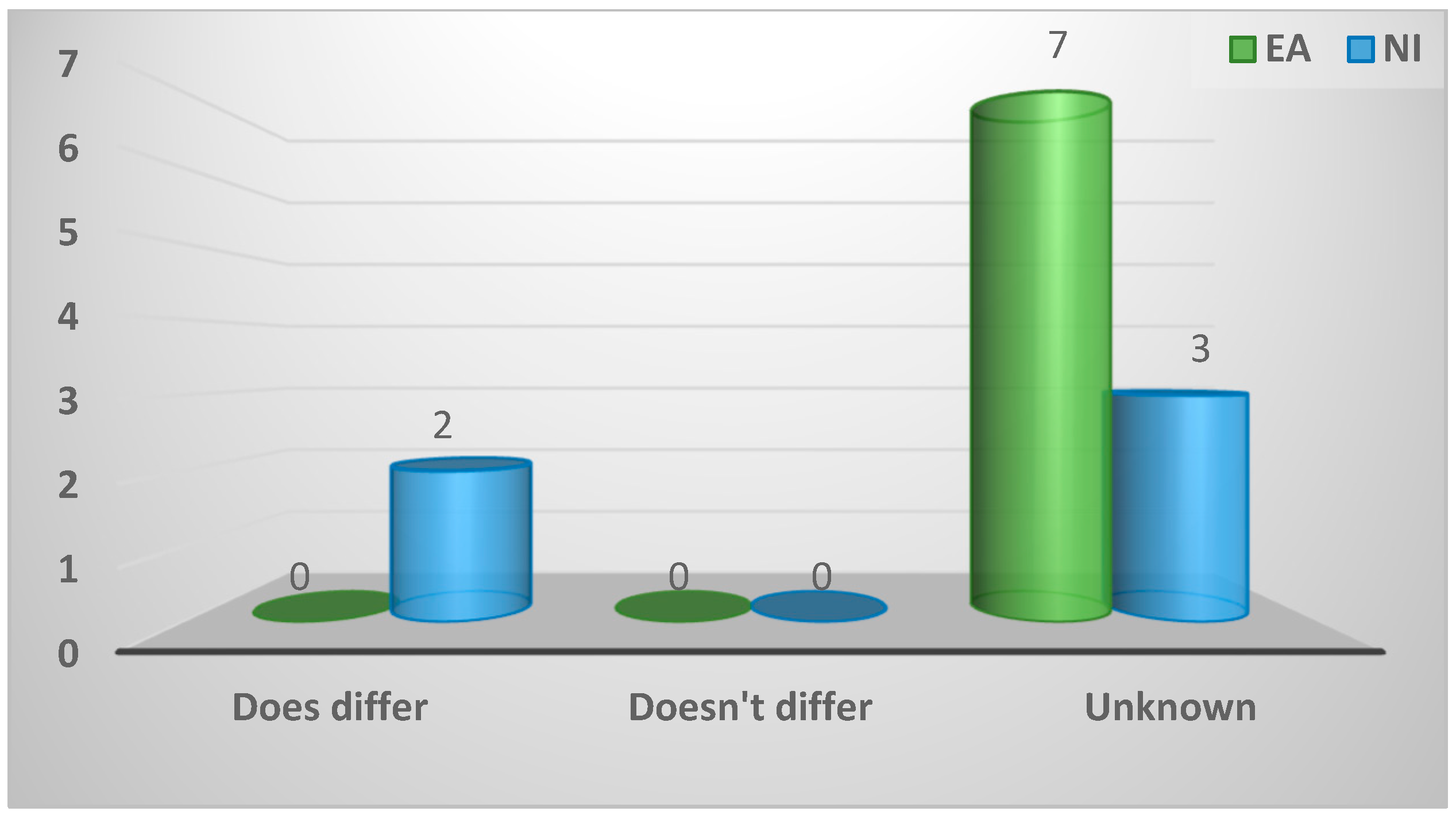
2.6.18. Differences between regions
When asked if the methods for diagnosis of spironucleosis differ between their region and elsewhere 100% of EA respondents and 3 out of 5 (60%) NI respondents answered with ‘Unknown’. Two respondents from NI (40%) believed that it does differ between regions (Table 5; Figure A39).
3. Discussion
The importance of spironucleosis in game birds is well established [9,14]. However, controversy remains as to the optimal methodology to effectively diagnose spironucleosis in game birds [1-3,5,11,12]. In this study, we examined and compared the perception of practising veterinarians with respect to enteric disease in game birds and the diagnosis of spironucleosis in EA and NI. Telephone surveys of veterinary establishments in both EA and NI were conducted to investigate how veterinarians from both regions manage enteric disease and diagnose spironucleosis in game birds. Although many methods of spironucleosis diagnosis are recorded in the literature [1-3,5,11,12,15], this is the first study to determine the diagnostic practices of veterinarians in two geographically distinct regions of the UK.
Most respondents from both regions believe enteric disease of game birds to be of high importance. Importantly, we found most respondents believe spironucleosis is a highly important disease of game birds, emphasising the need for establishing which diagnostic methodologies are routinely used within the UK. More practices from EA (15 out of 200) than from NI (13 out of 61) participated in the survey, however a much higher response rate was recorded from NI (21%) than from EA (8%). The initial lists provided by the RCVS include all practices that classify themselves as dealing with any type of birds, not specifically game birds. The relatively larger number of these practices in EA than in NI may be attributed to the larger geographical size of the region. However, the higher response rate in NI indicates that a larger percentage of veterinarians from NI experience game birds of some sort. This may be due to the differences in practice type between regions. It is possible that most game bird work goes directly to the comparatively higher percentage of specialist poultry practices in EA explaining the relatively lower response rate. However, in NI most mixed practices with their broad and general caseload are more likely to experience game birds explaining the higher response rate.
Interestingly, a much higher percentage of EA respondents were able to fully complete the questionnaire (47%) and a comparatively higher percentage of practices from EA diagnose cases of enteric disease themselves. This suggests a comparatively better understanding of enteric disease of game birds in EA than in NI. This may be due to the greater knowledge of the subject among the higher percentage of specialist poultry practices in EA and/or to the fact that more respondents from EA have experience of Spironucleus associated cases compared to those from NI. Significantly, more partridges were seen by respondents in EA than NI. Partridges are more suited to the flat, roaming arable land of EA whereas the pheasant is more suited to the rougher, wetter lands of NI. Partridges are much more susceptible to coccidiosis than pheasants [7], however despite this, a higher percentage of respondents in EA experience Spironucleus. This suggests a higher prevalence of spironucleosis in EA than in NI, however the fact that most NI respondents prescribe drugs to treat enteric disease of birds without an examination of the infected bird could account for the fewer cases of spironucleosis seen in NI. Further regional differences identified in this study suggest a trend towards respondents believing that game keepers in EA are more willing to consult veterinarians than in NI. This may be due to the higher number of commercial shoots in EA having more finances available for veterinary consult fees and treatment. In contrast to the “hobby shoots” of NI which operate on a tighter budget and cannot afford the veterinarian to examine the birds before commencing treatment.
The most common clinical signs of spironucleosis in living birds described across both regions were anorexia, depression, and abnormal faeces, which is consistent with previous studies [1,5,13,14]. Interestingly, an altered gait and ruffled feathers were described by EA respondents but could not be found in any literature. An altered gait is likely to be due to the severe weight loss along with depression and the ruffled feathers may be due to the huddling of birds [7]. Spironucleus-infected birds are described as thin and dehydrated on gross external examination during post-mortem [3,13]. Interestingly, most EA respondents (57%) believe there to be no visible changes on external examination of the birds. Second to this however, EA respondents described the carcasses as thin and dehydrated with a faeces-stained vent. NI respondents agree with these descriptions with the addition of comparatively poor growth of the infected birds.
On gross internal examination of infected carcasses, frothy gut contents were the most frequently described visible change by both regions (71% of EA and 75% of NI), which were also described as distended by EA respondents. The small intestine of infected birds has been described to be distended with fluid contents [1,7,12]. The small intestine contents has been described as yellow in colour [13], which was also depicted by respondents from EA (14%) alone. The caecum can be filled with frothy mustard coloured contents [7], as reflected by descriptions from both regions. Additional internal changes observed by respondents included enteritis and liver lesions (reported by NI respondents alone), poor crop fill and dehydration along with visible urates (reported by EA respondents alone). Apart from enteritis these additional changes were only observed by one respondent each, and so the weighting given to these must be minimal.
Despite the inclusion of an investigation into respondent’s description of clinical signs in the questionnaire, all respondents from both regions stated that they never rely on gross findings alone for diagnosis of spironucleosis and always carry out a laboratory-based diagnostic test. This suggests that diagnosis of spironucleosis in both regions is performed regardless of clinical signs. Freshly killed birds are needed for the diagnosis of spironucleosis [2,12]. This was reflected in the results, as 75% of all respondents examined the birds less than five minutes after death. However, both regions had a portion of respondents who believe that there is no limit to the time between death of the bird and examination for Spironucleus putting into doubt the reliability of their diagnostic method. A similar percentage of respondents from both regions stated this; 29% in EA and 25% in NI.
The caecum was the most harvested individual site for spironucleosis diagnosis across both regions (100% of EA and 75% of NI respondents). However, the total number of respondents that use sites within the small intestine equals the number of responses for the caecum in EA (7) and outnumbers the number of responses for the caecum in NI (5). Spironucleus can be found in the duodenum and jejunum [5], which are utilised by EA respondents. In a contradicting study [13], Spironucleus was found to be present in the jejunum and ileum. NI respondents use the duodenum and distal small intestine/ileum, but not the jejunum/mid small intestine. These studies along with our results suggest that Spironucleus is present throughout the entire small intestine. Interestingly, one respondent from NI believes that the rectum can be utilised for spironucleosis diagnosis and one respondent from EA utilises the large intestine, however neither method is reported by any previous studies.
Most respondents from EA (71%) use lumen contents for the identification of Spironucleus whereas most NI respondents (75%) use mucosal scrapes. A portion of EA respondents (29%) also use a combination of both scrapes and contents. As the protozoa can exist in the crypts of Lieberkuhn [13] and between epithelial cells [5], it is likely that simply using lumen contents alone is insufficient to confirm a diagnosis in lightly infected birds especially when combined with the frothy contents described by respondents from both regions. Small intestine contents and scrapes have been reported in previous studies [1,12] as have caecal contents and scrapes [1,4]. Further study should include work into which areas are more likely to yield Spironucleus.
Trees, [12] suggests that the collected sample can be diluted to help with visualization, which was done by 43% of EA and 25% of NI respondents. However, one EA respondent diluted the sample with iodine which had not previously been described in the literature. A range of magnifications ranging from x100 [4] to x200 [1] have been used to identify Spironucleus, however the most common magnification used across both regions was x400 with a x500 being used by one NI respondent. Another novel method of spironucleosis diagnosis reported here by a NI respondent described the slide coverslip as being suspended in vaseline and then the slide inverted to allow the protozoa more room to move freely. It should be noted that significantly more NI respondents heat the slide prior to use to keep Spironucleus viable.
Respondents from both regions most frequently describe Spironucleus to be small, motile, and flagellated, agreeing with others [13,16]. Respondents also believe Spironucleus to be smaller and faster than Trichomonas, in agreement with others [2,7]. The differentiation between Trichomonas and Spironucleus is best achieved by an experienced examiner and hence the potential exists for inexperienced examiners to fail to distinguish between Trichomonas and Spironucleus [2]. Consistent with this, most respondents from both regions (100% of NI and 71% of EA) had difficulty differentiating these protozoa without a history, emphasizing the possible error that can creep into the accurate diagnosis of spironucleosis at this stage.
Most respondents across both regions (55%) believe that faeces cannot be utilised for the diagnosis of spironucleosis. Despite the use of faeces in the identification of Spironucleosis meleagridis, having never been reported before in game birds, faeces have been used to identify Hexamita columbae in pigeons [17]. Further study should investigate the possibility of using faeces for spironucleosis diagnosis in game birds. Veterinarians from both regions agree that motile protozoa are the most crucial factor needed for diagnosis of spironucleosis, however significantly more NI respondents believe it is possible to quantify infection levels compared to EA respondents. Previous studies were able to quantify infection levels using simple groups [1,15], therefore more investigations are needed to address the reasons why EA respondents believe it is impossible.
It was proposed that a carrier state of spironucleosis can be identified by showing that Spironucleus can be found on the post-mortem of asymptomatic birds [5]. This however was not reflected by our results as the bulk of respondents form both regions (100% of NI and 86% of EA) believe that only one positive sample taken from a bird is needed to confirm disease in that individual and 100% of NI and 43% of EA respondents believe only one infected individual is needed to diagnose the flock with spironucleosis. However, this is not very representative of the respondent’s knowledge of carrier birds, as these cases obviously present with symptoms of enteric disease.
4. Materials and Methods
4.1. Sampling and recruitment
This survey was conducted in two regions in the UK: East Anglia (EA) and Northern Ireland (NI). For the purposes of this study EA is defined as Cambridgeshire, Essex, Norfolk, and Suffolk. Veterinary practices categorized as dealing with birds and/or poultry were selected from the list provided by The Royal College of Veterinary Surgeons (RCVS). Also, selection was based on government-based laboratory locations; Agri-Food and Biosciences Institute (AFBI) in NI and the Animal Health and Veterinary Laboratories Agency (AHVLA) in EA.
4.2. Approach
A questionnaire survey was designed to collect data on awareness, general knowledge, perceptions, and experience with the diagnosis of spironucleosis among veterinarians of different specialties. Questions were designed to be closed (where specific information was sought) or open (where opinion and personal views were sought).
4.3. Strategy of data collection
An initial pilot study was carried out on both AFBI laboratories in NI via face-to-face interviews with the relevant persons. Then, the original question set was adjusted and finalized in preparation for contacting the remaining practices. To qualify for participation in the study, veterinarians must be active in any practices that treated or diagnosed game birds and reside in one of the regions included in the study. Practices that regularly see game birds but rely upon commercial diagnostic services for cases of putative enteric disease were excluded from the analysis related to questions 12-41. The survey was a 15-min interview conducted via telephone using a fully structured questionnaire to speak to the most relevant person, explaining the purpose of the survey and why they were chosen, and assured their responses would be maintained confidential. If the most relevant person was unreachable, the questionnaire was sent via email and returned to the authors completed. Throughout the interviews the organism was referred to using the more common terminology, Hexamita. However, during each interview the nomenclature of Hexamita/Spironucleus was clarified for each participant.
3.4. Data recording and coding
During the interviews data was recorded via hand with all additional information being noted. A database was then created in Microsoft Excel to save answers. Each establishment was assigned a unique ID to ensure confidentiality of the master Excel sheet. The key linking all unique ID’s to their corresponding practice names was held under an encrypted document. On the master Excel sheet every answer to each question was assigned a separate code and recorded. This allowed tallies of each answer to be made, graphs to be drawn and comparisons made between geographic regions.
3.5. Data analysis
Statistical analysis was performed using Stata 16.1 statistical software (StataCorp LP, College Station, TX, USA). Fisher’s exact test was used to assess the statistical significance and a P value of <0.05 was considered significant. Descriptive statistics were used to suggest trends and interpret the data. Percentages in the tables may not total 100 due to rounding.
5. Conclusions
The results indicates that veterinarians practising in both EA and NI believe enteric disease of game birds, specifically spironucleosis, to be of high importance. However, there was a comparative lack of knowledge or experience of Spironucleus among NI respondents. This may be attributable to either fewer cases of spironucleosis in NI or due to the apparent better knowledge of EA respondents. The results confirm veterinarians in both regions have (i) difficulty differentiating Spironucleus from Trichomonas and (ii) spironucleosis diagnosis is based on laboratory tests alone regardless of presenting clinical signs and gross pathological changes. Our findings support the hypothesis that no single method is used consistently for the diagnosis of spironucleosis, rather that many techniques are utilised in both regions. However, there were differences between the regions in the techniques and sites used. Further investigation into the effectiveness of the methods used for spironucleosis diagnosis is needed. Additionally, further research is required to establish the prevalence of spironucleosis in NI and EA.
Author Contributions
Conceptualization, M.H., M.C. and H.E.; methodology, M.H. and H.E.; formal analysis, M.H. and N.H.; investigation, M.H. and M.C.; resources, M.C.; writing—original draft preparation, M.H.; writing—review and editing, H.E.; visualization, H.E. and N.H.; supervision, H.E. and M.C.; project administration, M.C. and H.E. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical approval for this study was obtained from the Committee for Animal Research Ethics, School of Veterinary Medicine and Science, University of Nottingham.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available in the article and supplementary material.
Acknowledgments
The author would like to acknowledge the cooperation and enthusiasm of all veterinarians who participated in the study.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Figure A1.
Nature of participating establishments from each region.
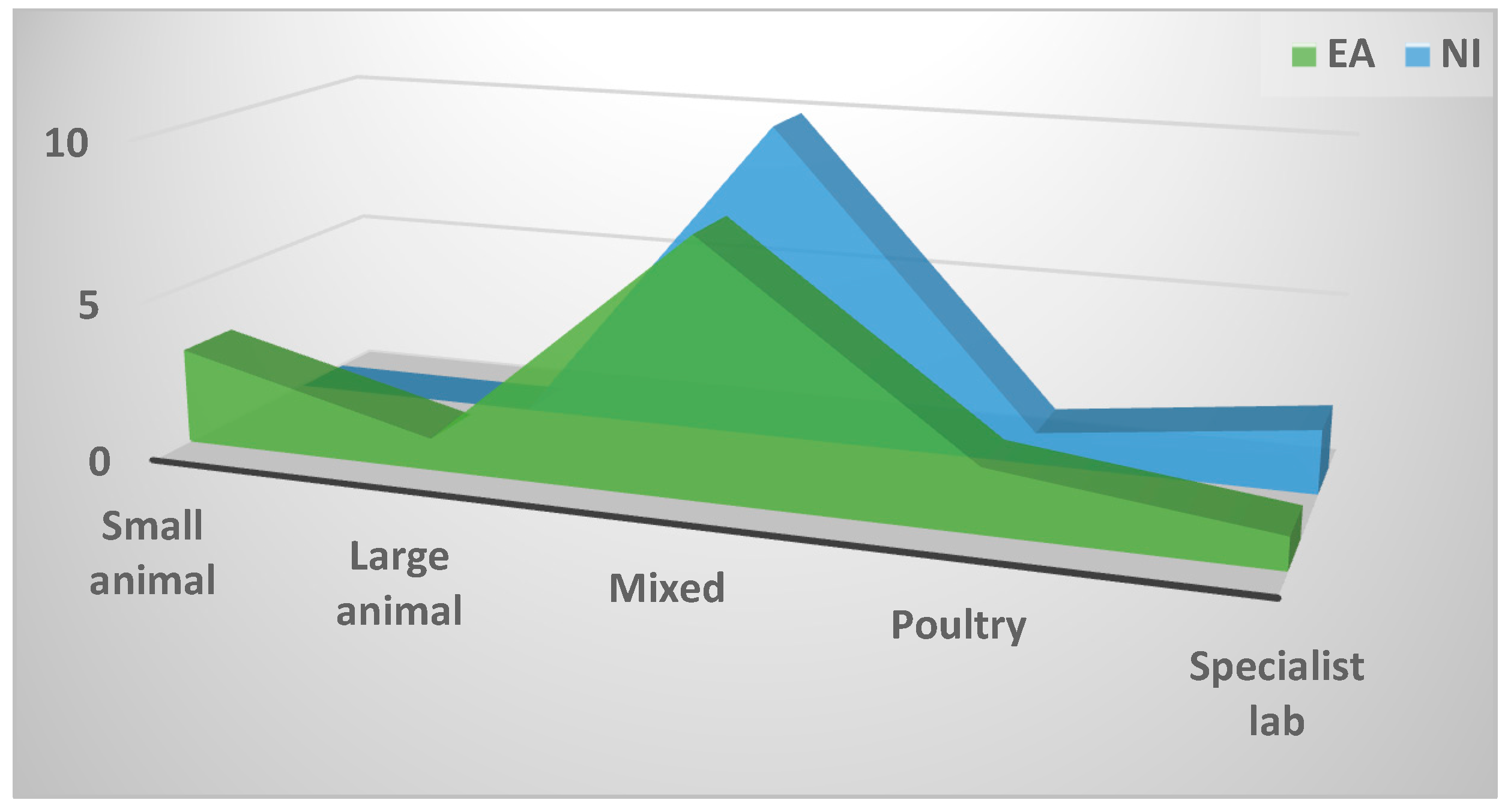
Figure A2.
Number of veterinarians associated with the establishment.
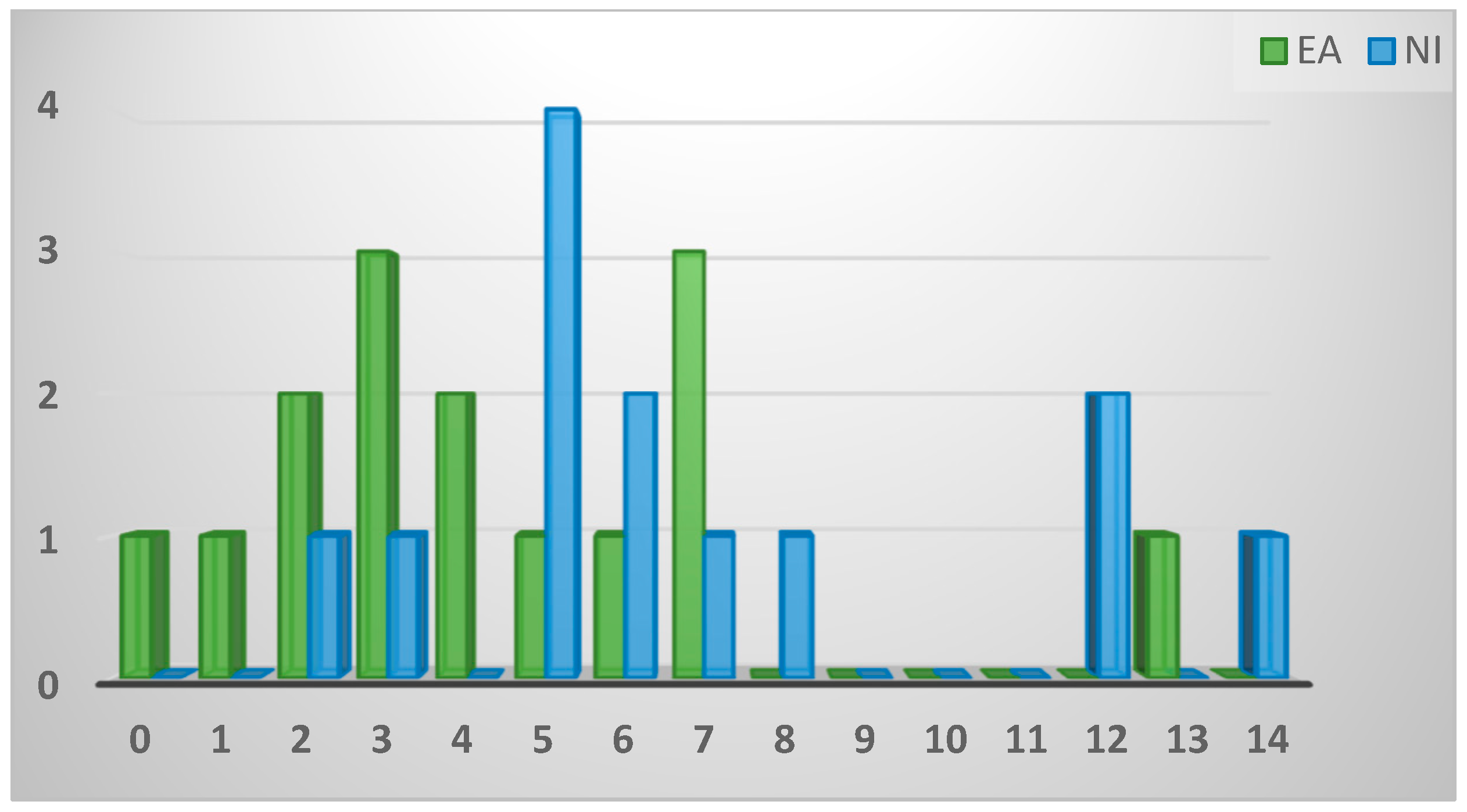
Figure A3.
Exposure to game birds expressed as percentage of overall caseload.
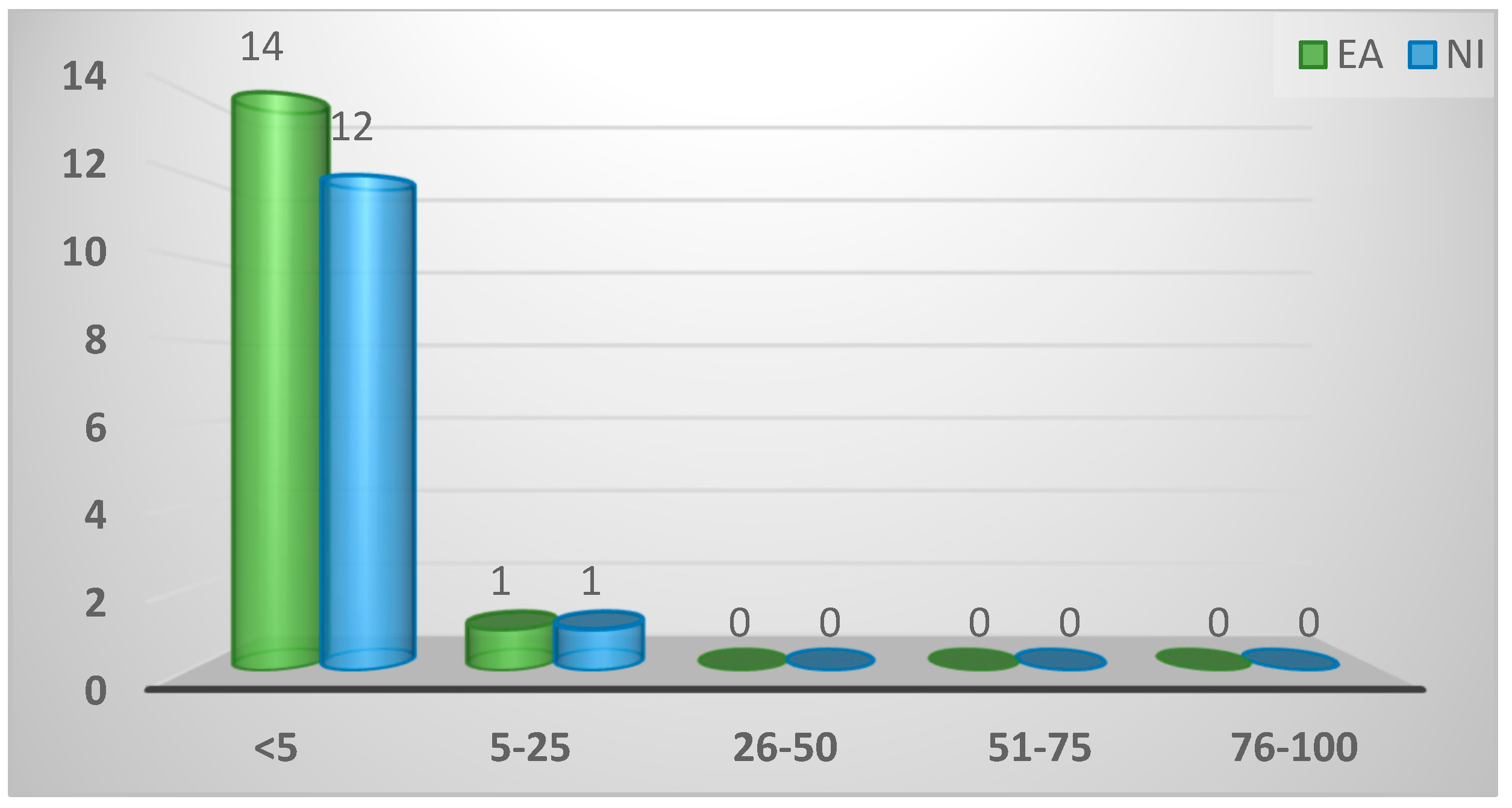
Figure A4.
Breed of game bird most frequently seen.
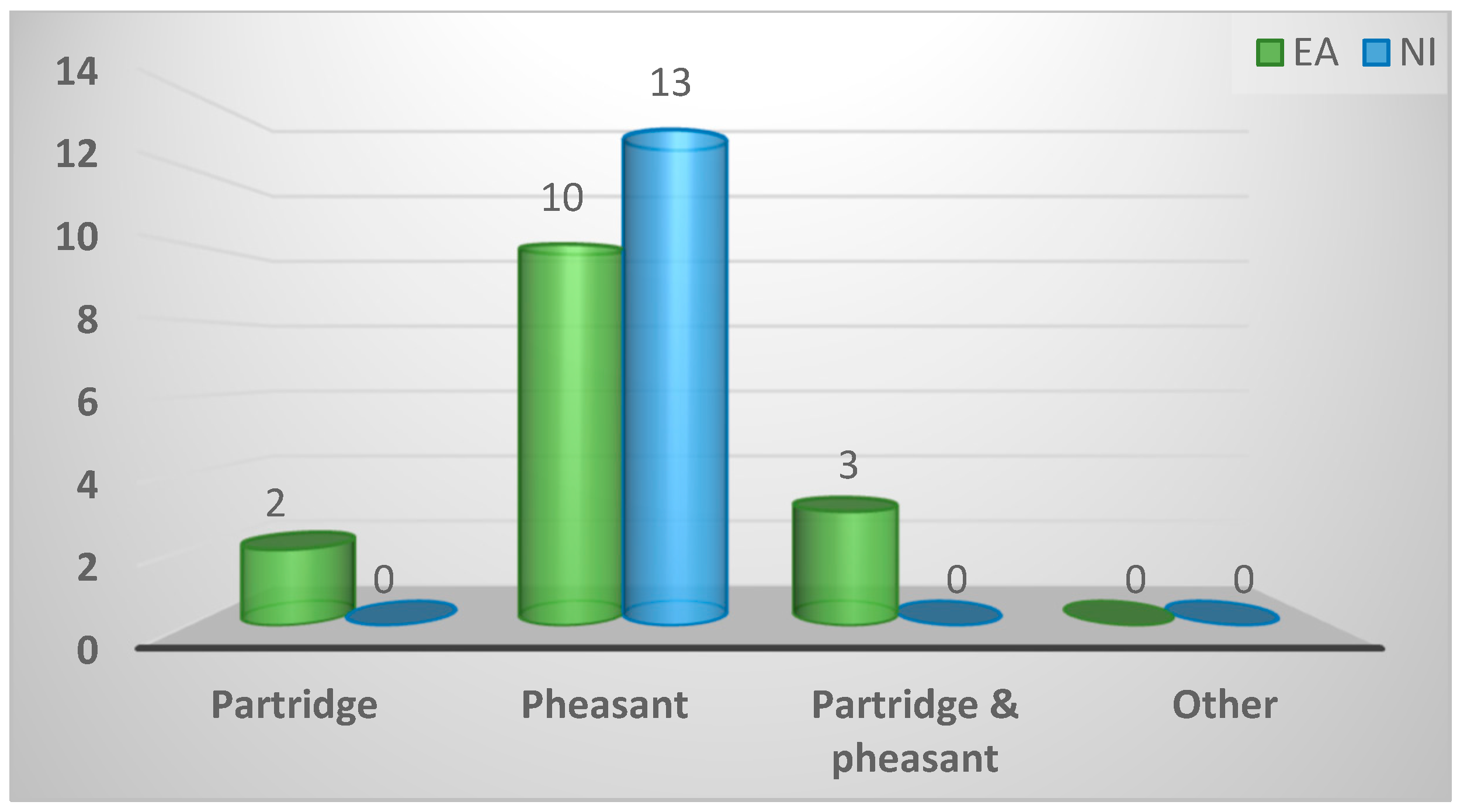
Figure A5.
Age of game bird most frequently seen.
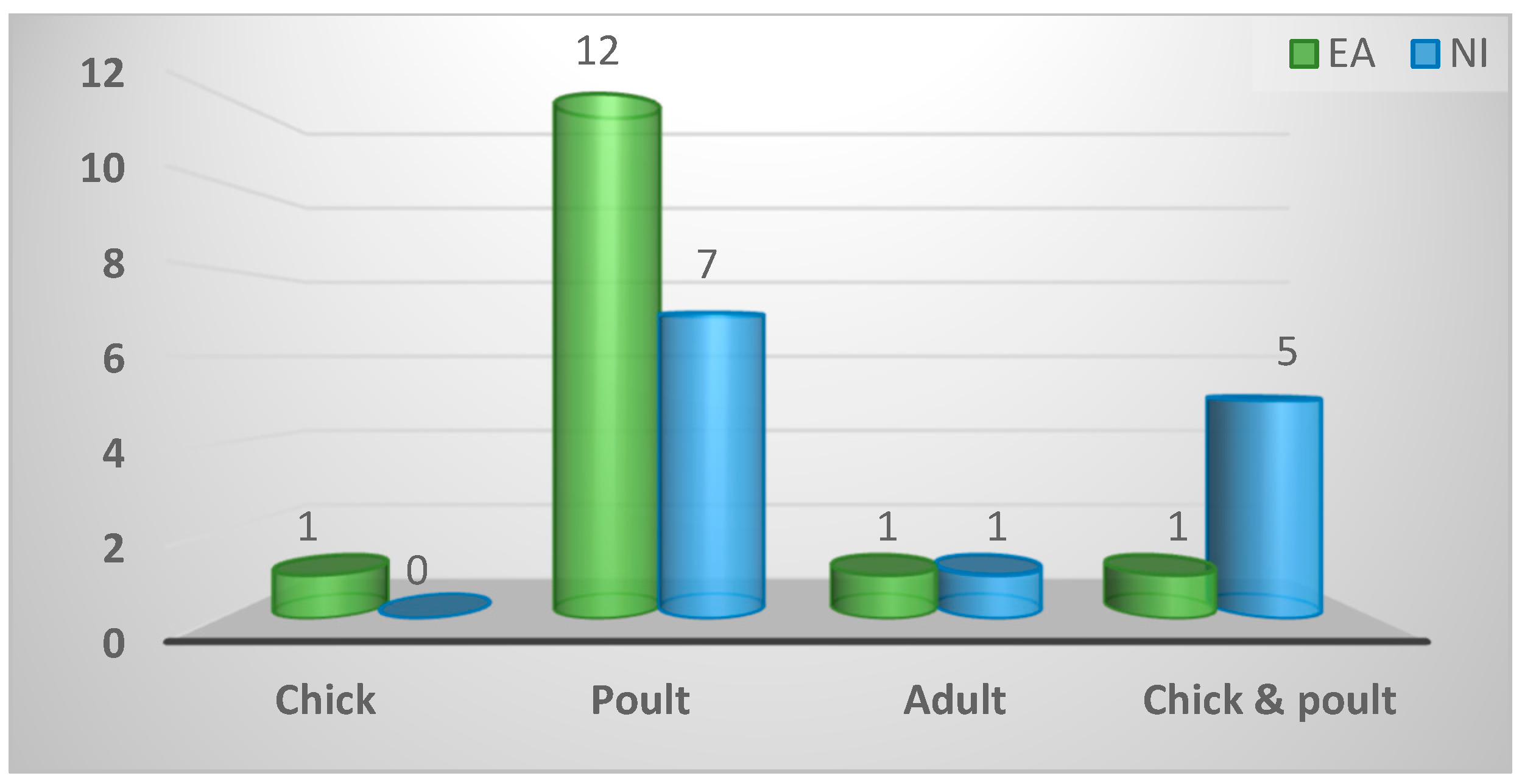
Figure A6.
Bodily system of game birds most frequently diagnosed with spironucleosis. GI (gastrointestinal); Resp (respiratory; MK (musculoskeletal); Repr (reproductive).
Figure A6.
Bodily system of game birds most frequently diagnosed with spironucleosis. GI (gastrointestinal); Resp (respiratory; MK (musculoskeletal); Repr (reproductive).
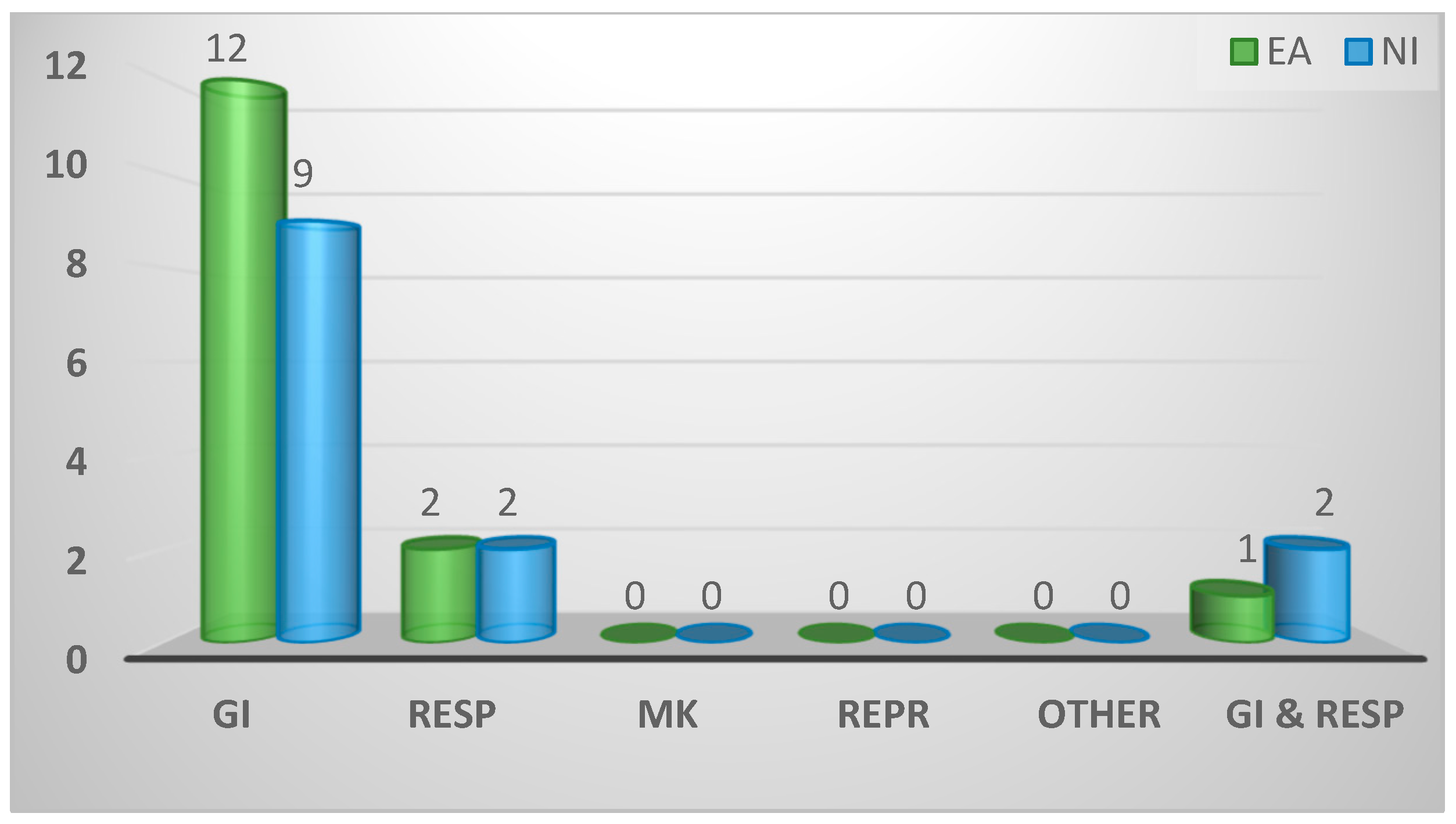
Figure A7.
Location of diagnosis of disorders in game birds; on site (at the practice), on location (at the game farm) or other.
Figure A7.
Location of diagnosis of disorders in game birds; on site (at the practice), on location (at the game farm) or other.
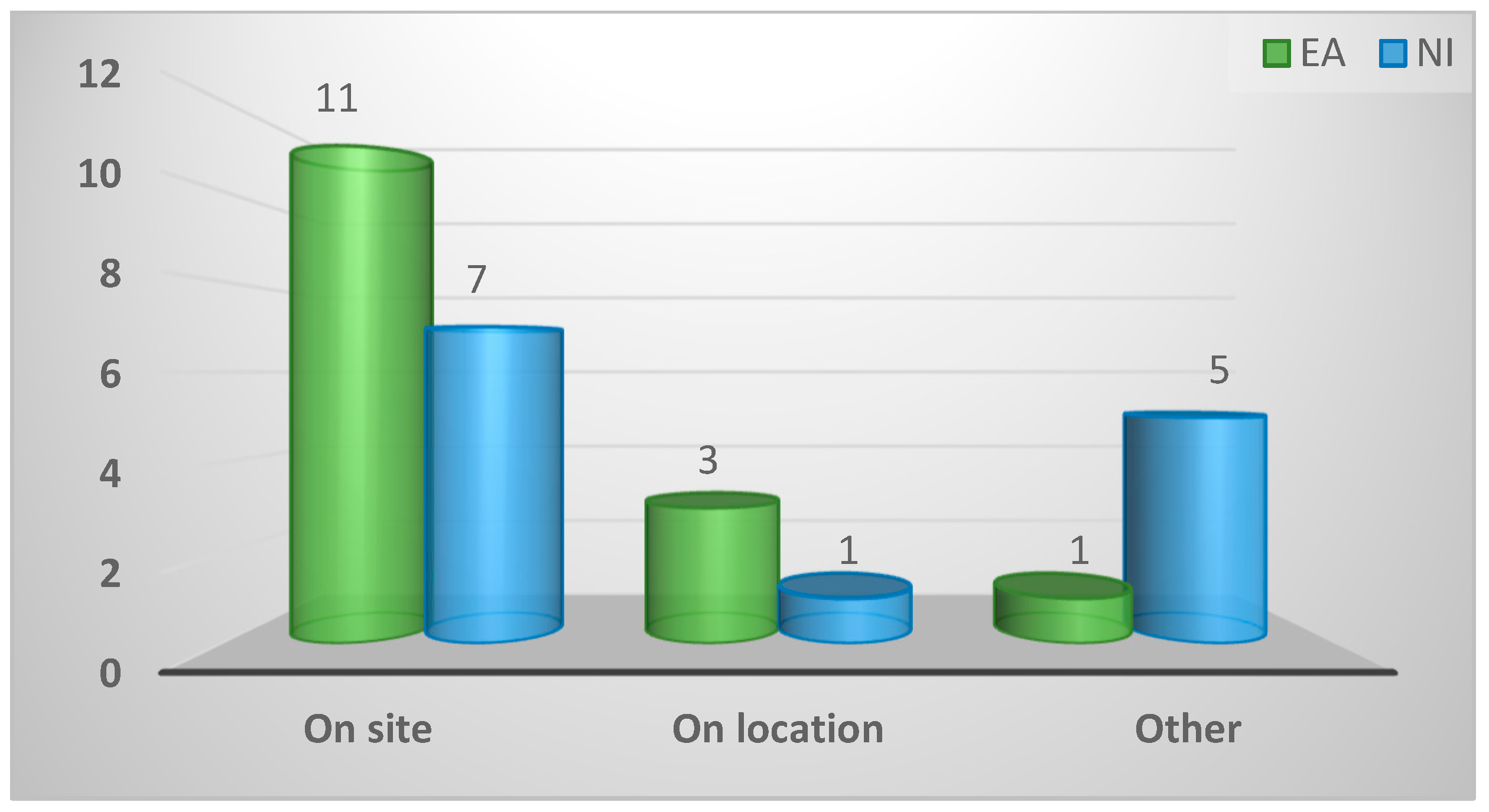
Figure A8.
Practice position on prescribing drugs to game birds.
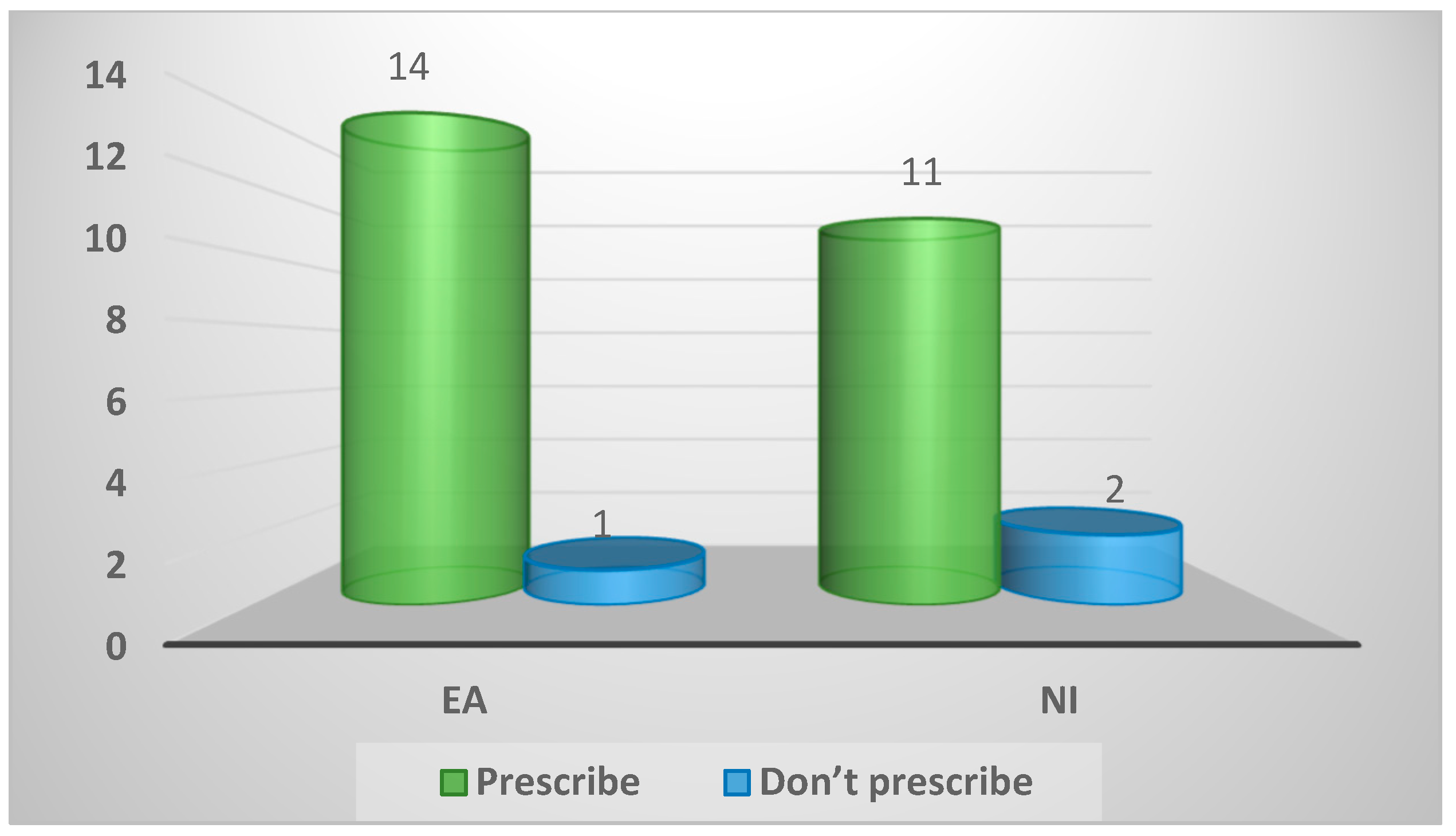
Figure A9.
Practice protocol on seeing affected birds before treatment.
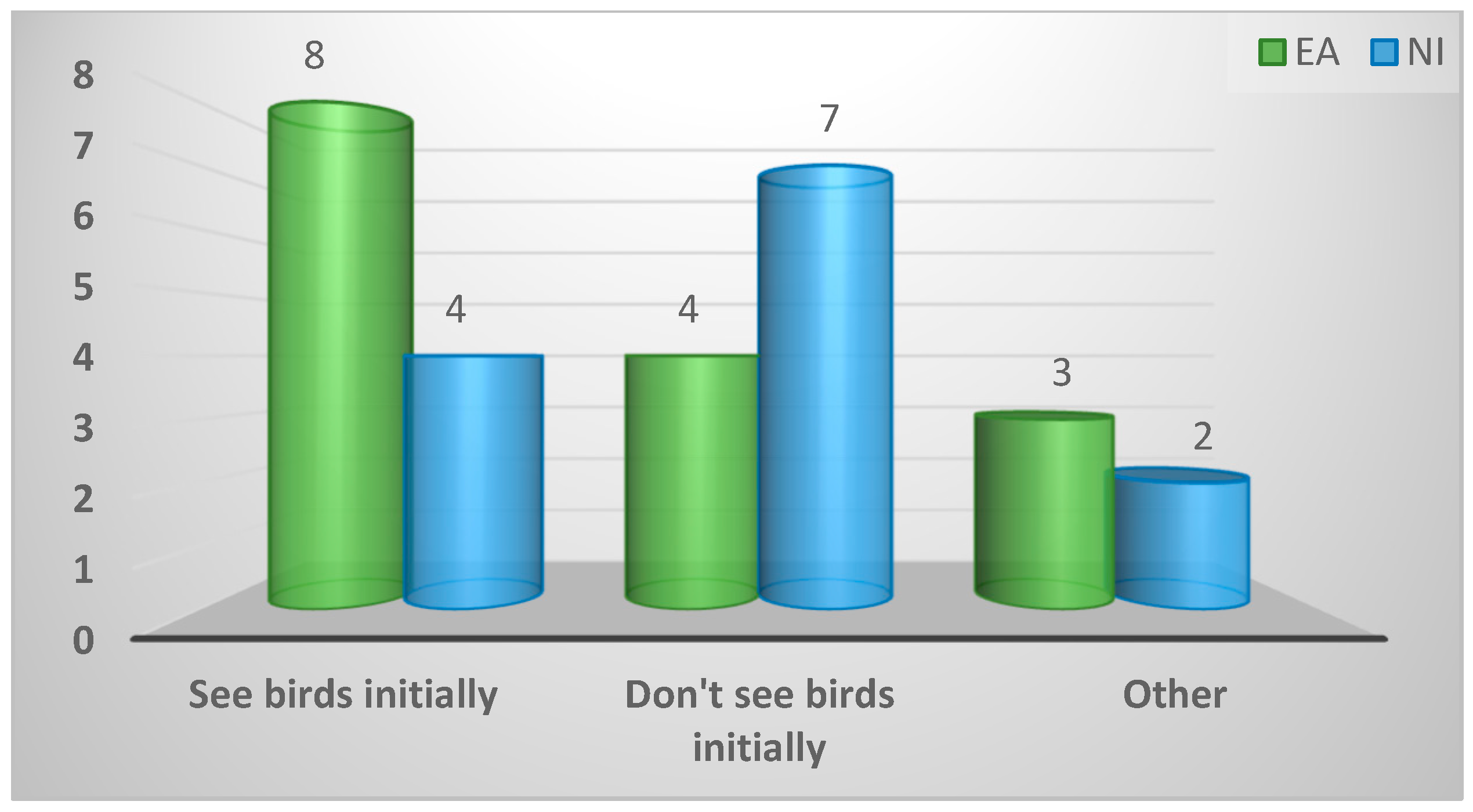
Figure A10.
Eagerness of game farmers to consult veterinarians for advice, treatment, and diagnosis of birds.
Figure A10.
Eagerness of game farmers to consult veterinarians for advice, treatment, and diagnosis of birds.
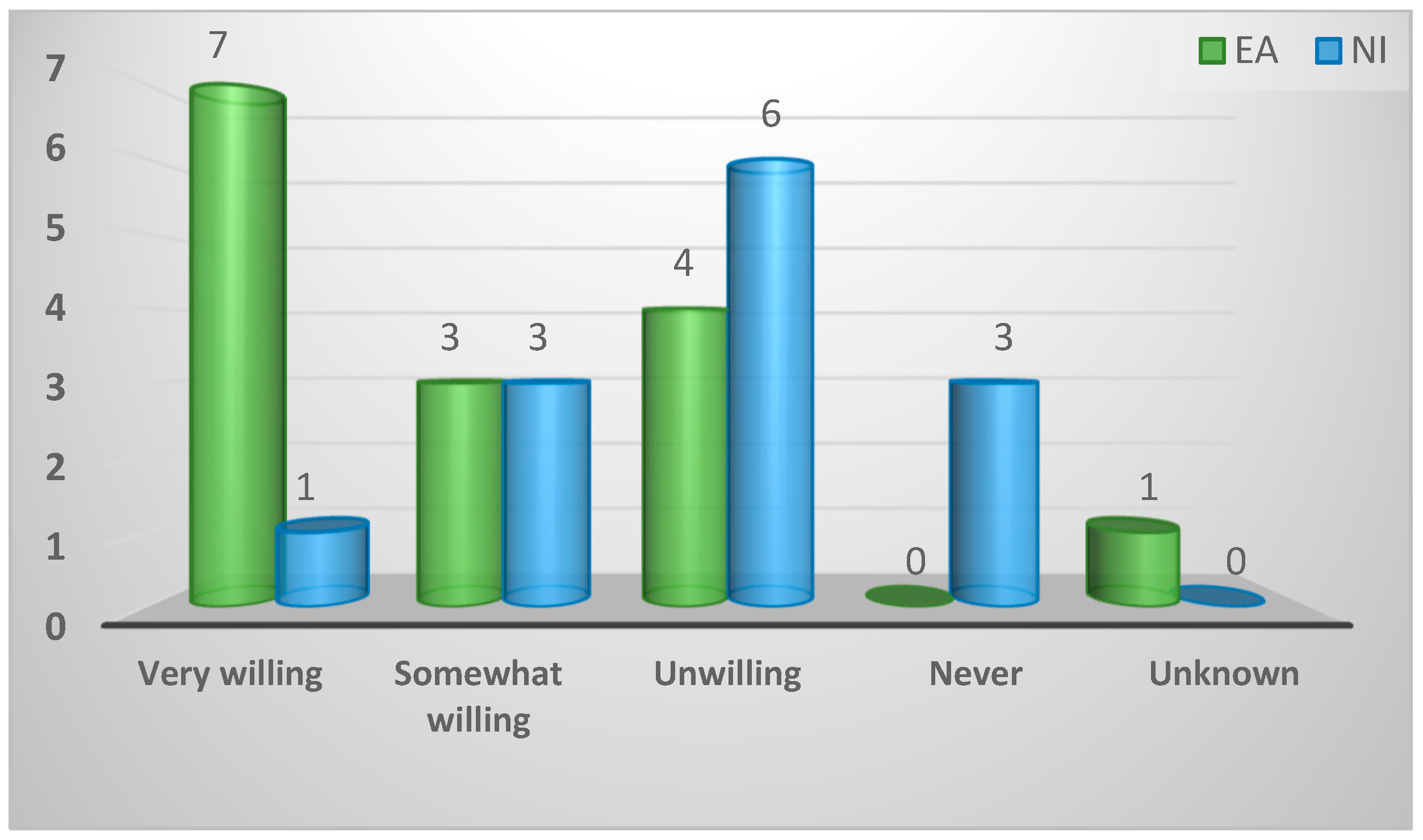
Figure A11.
Location of diagnosis of enteric disease.
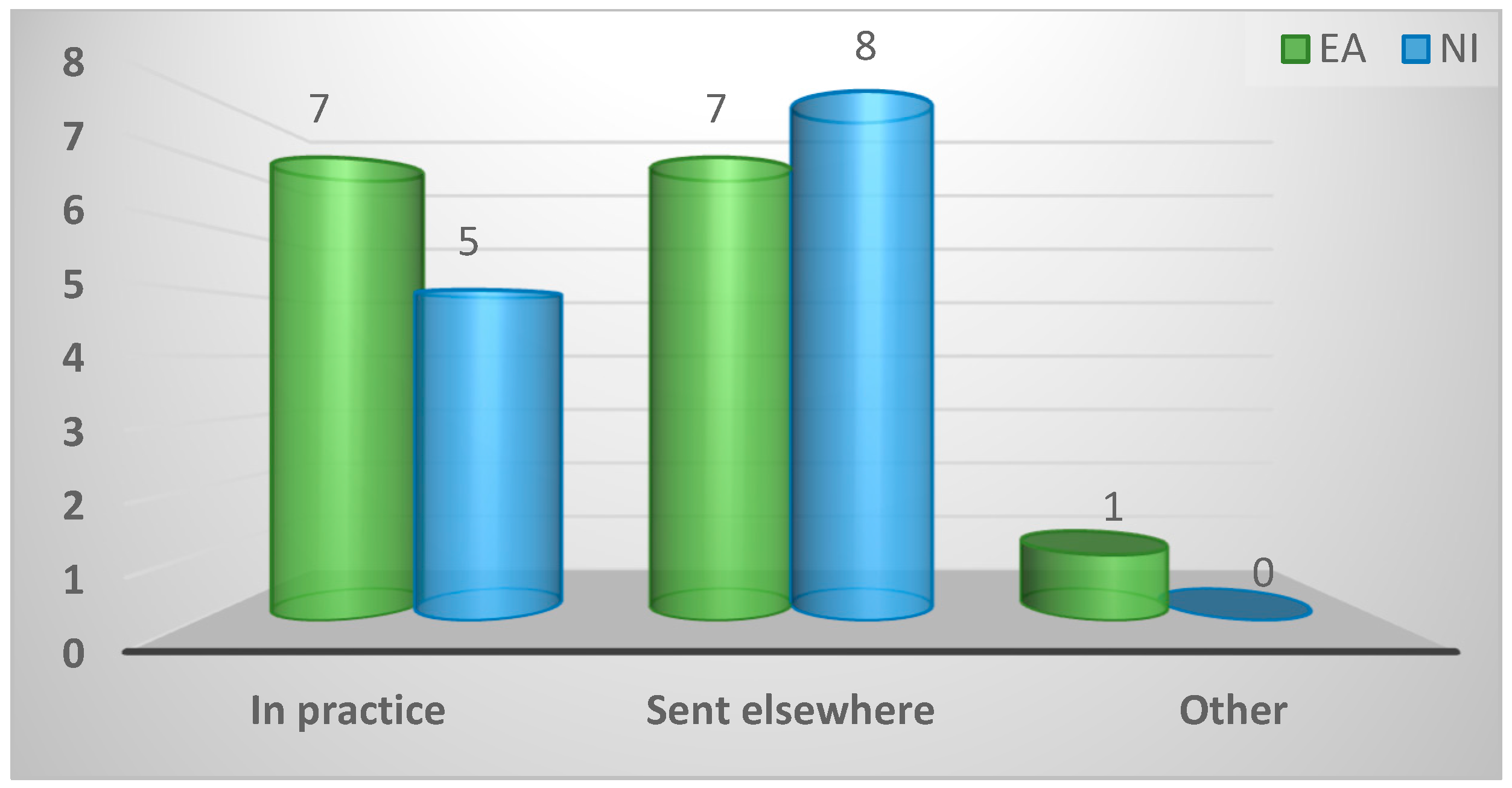
Figure A12.
Importance assigned to enteric disease of game birds by respondent.
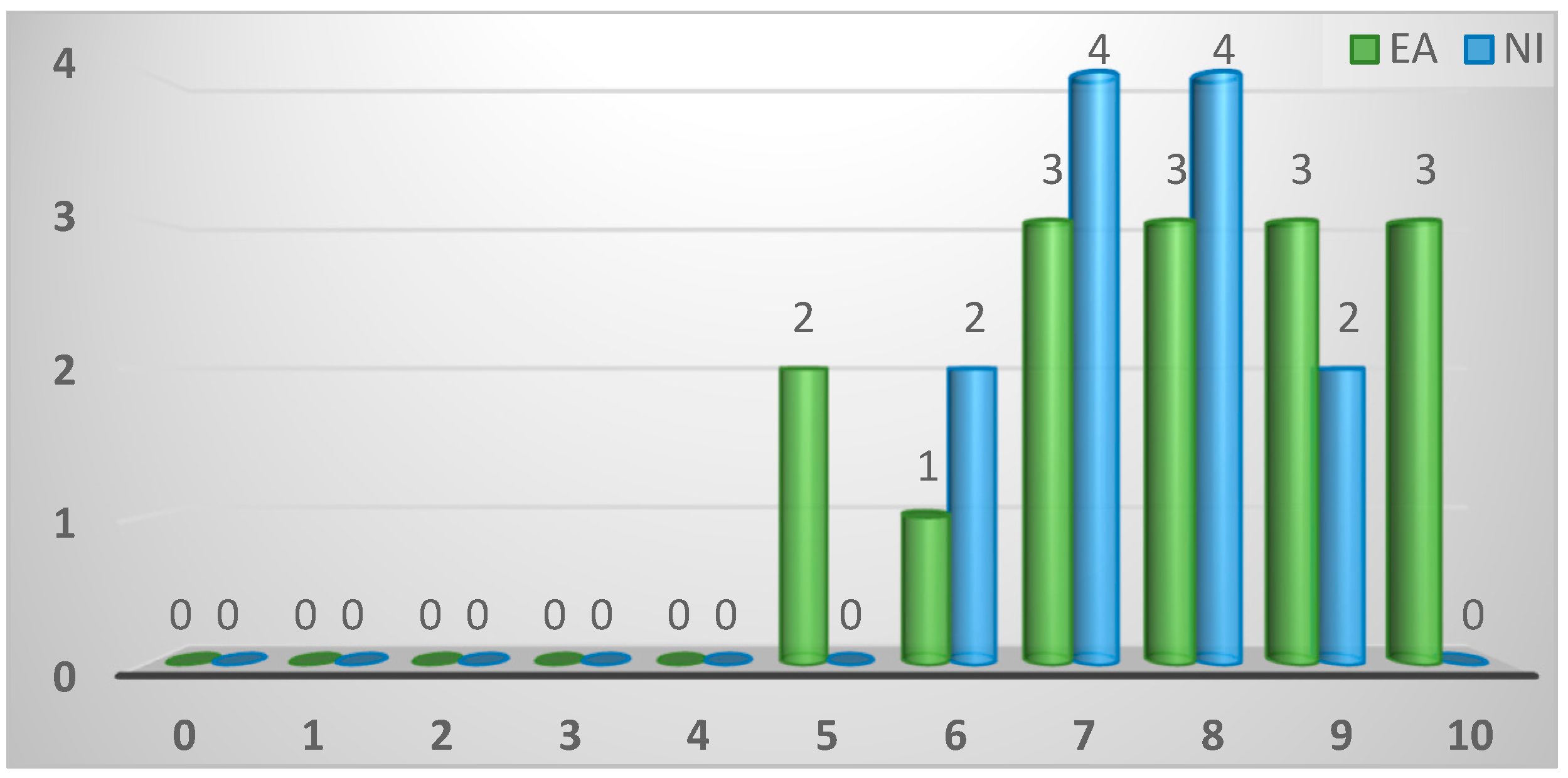
Figure A13.
Causative agent of enteric disease most frequently diagnosed.
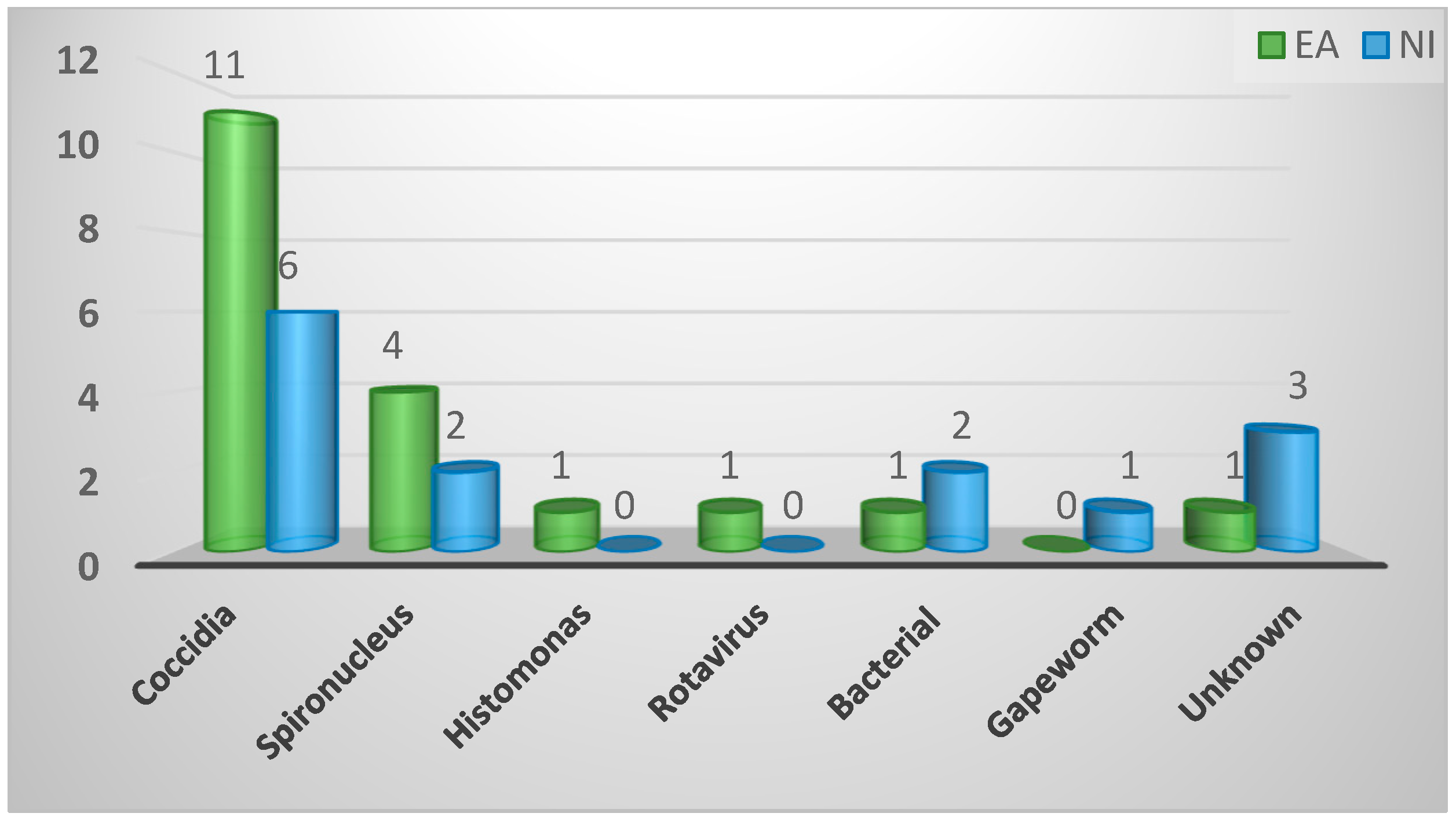
Figure A14.
Importance assigned to spironucleosis of game birds.
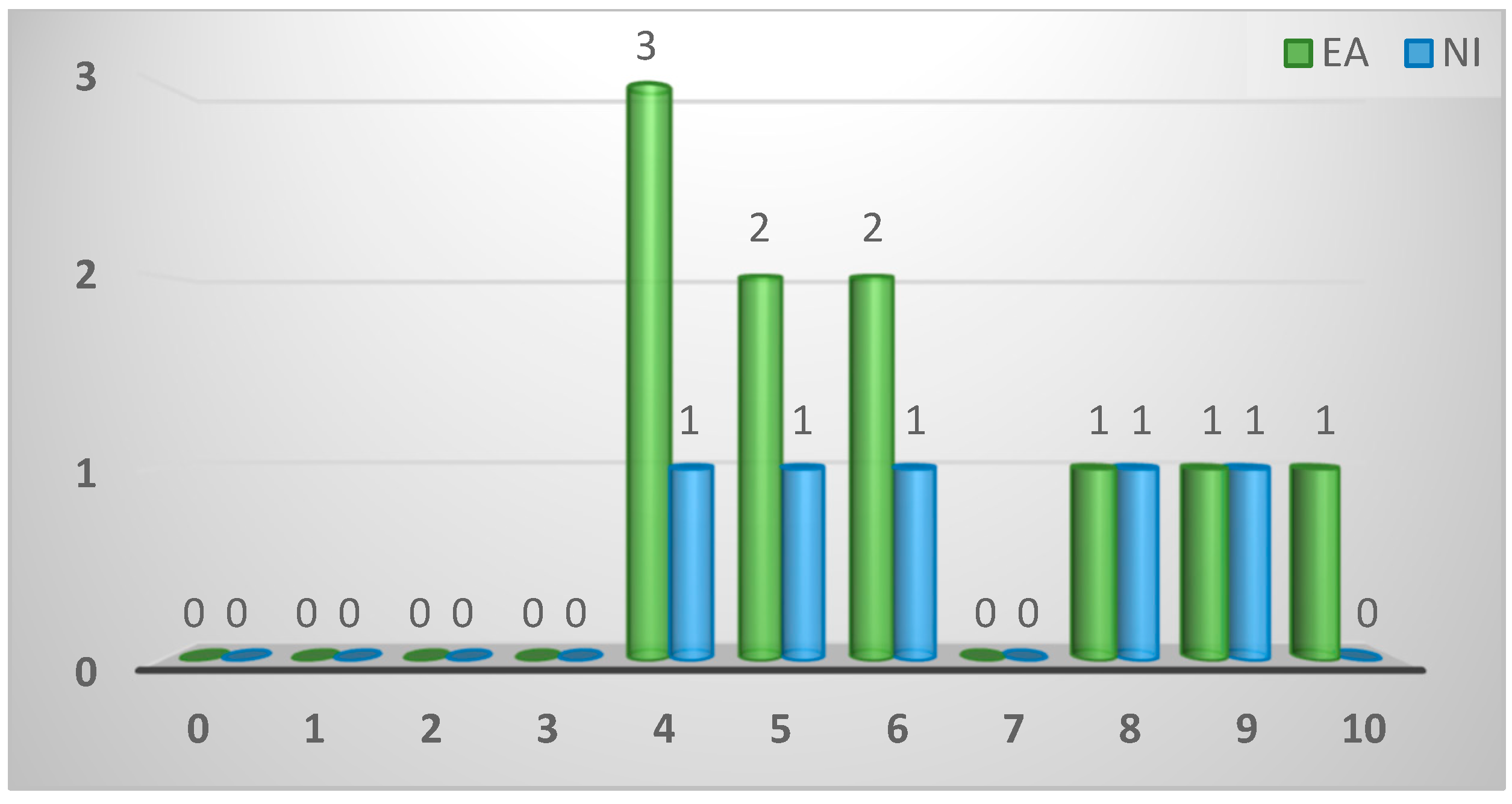
Figure A15.
Rearing stage/location where most cases of spironucleosis are experienced.
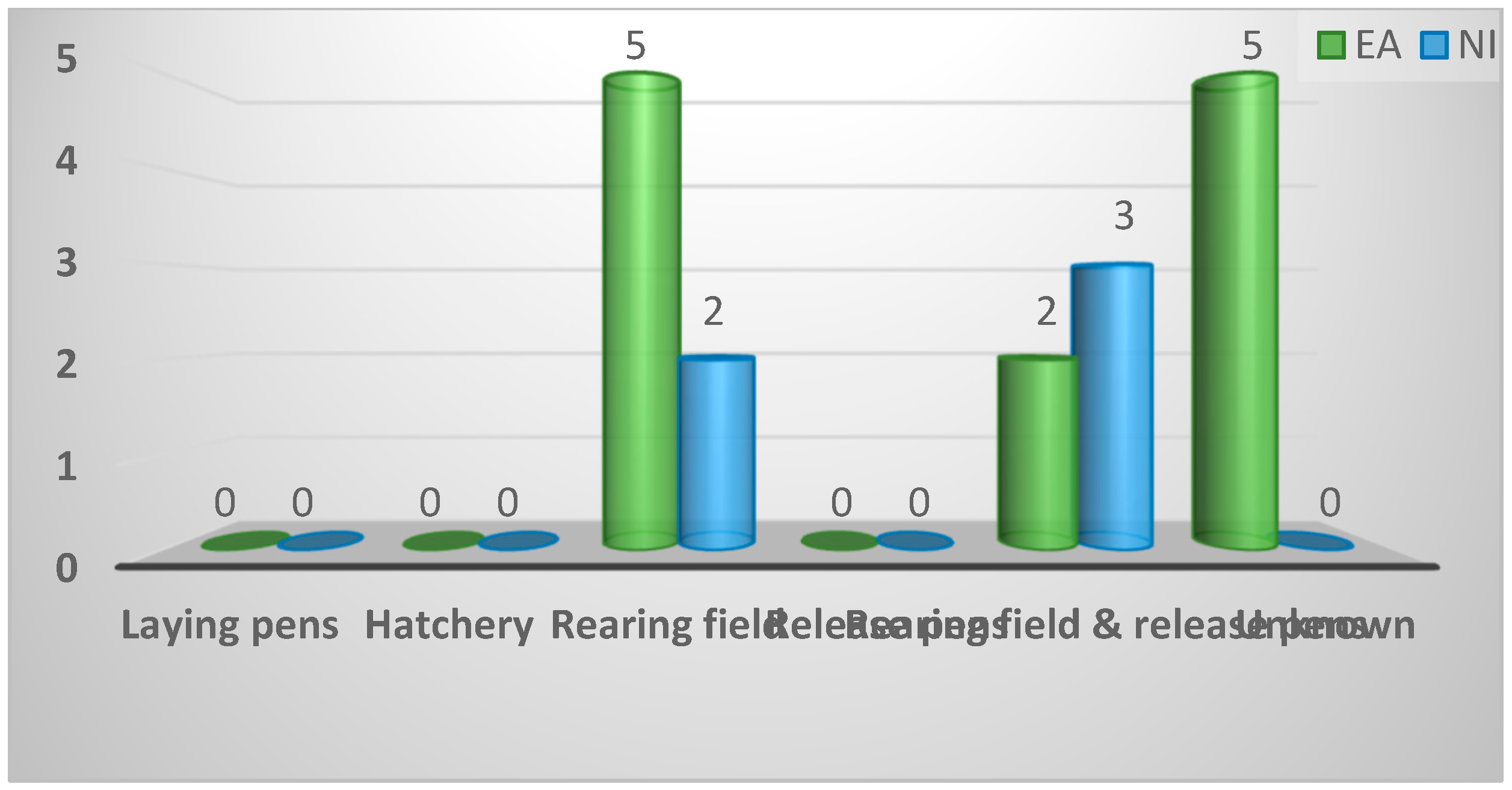
Figure A16.
Stakeholder responsible for selection of birds for diagnosis of spironucleosis.
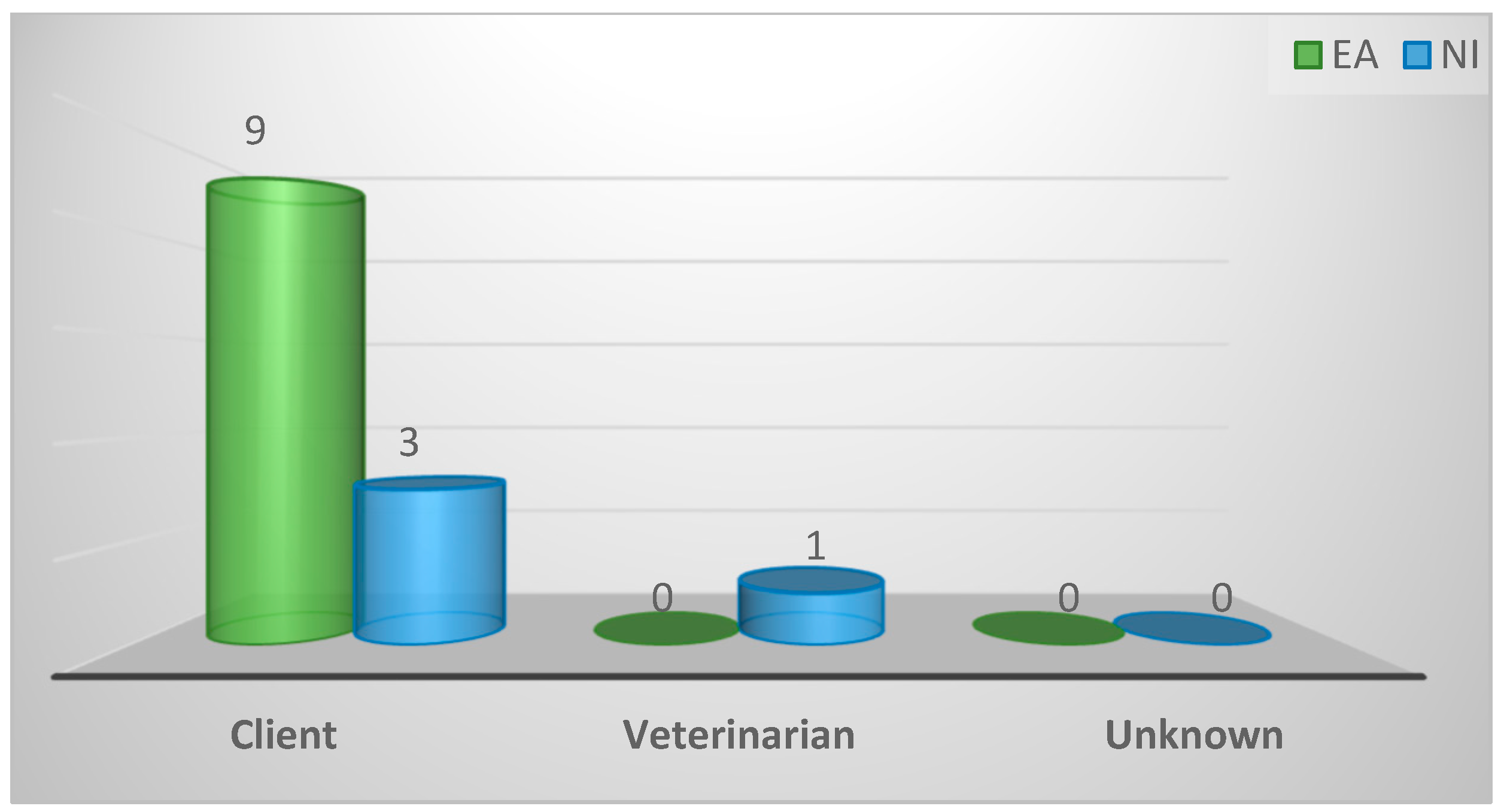
Figure A17.
Nature of birds removed from flock as samples for diagnosis of spironucleosis.
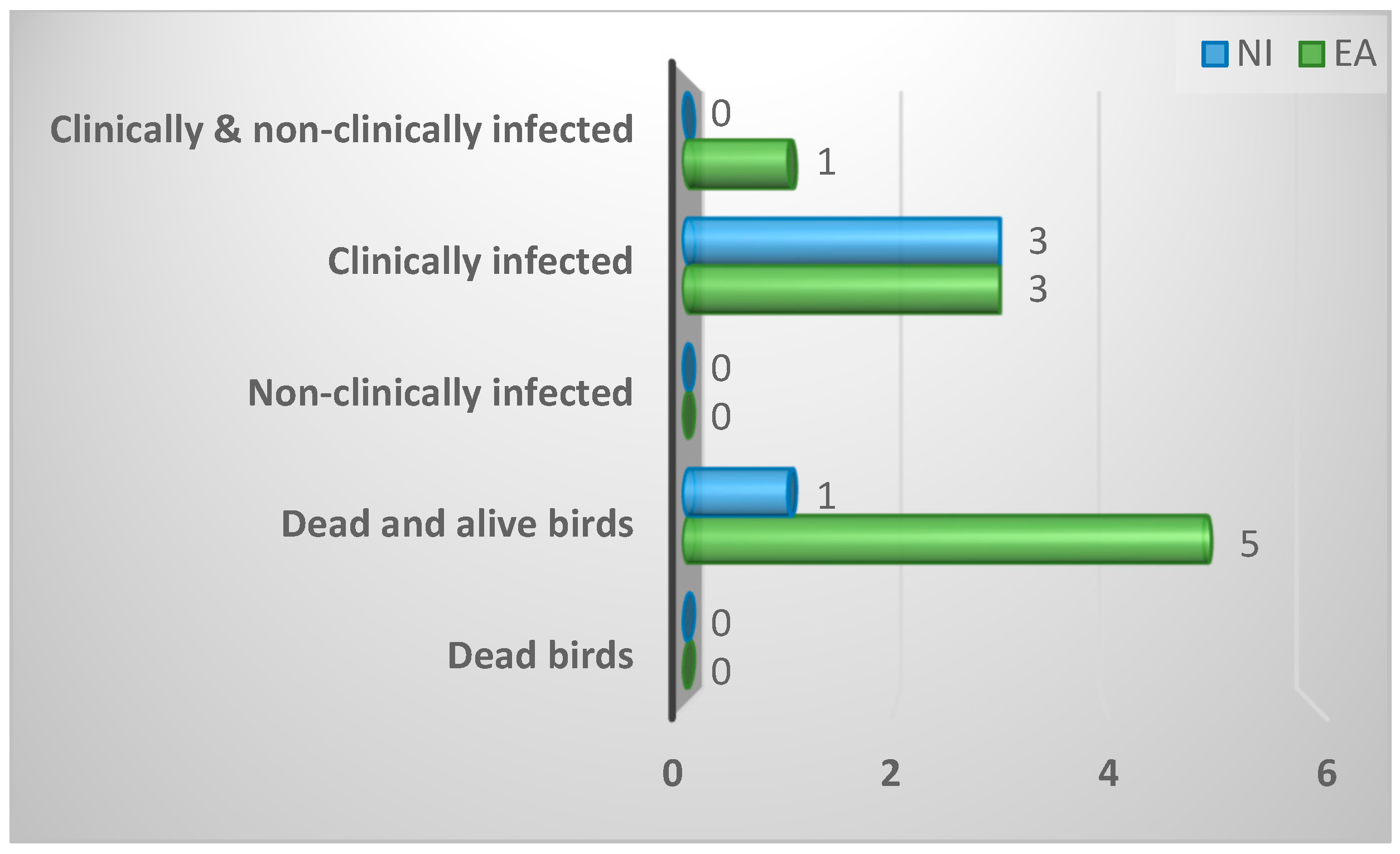
Figure A18.
Fate of remaining clinically infected birds in the flock after the sample birds have been removed.
Figure A18.
Fate of remaining clinically infected birds in the flock after the sample birds have been removed.
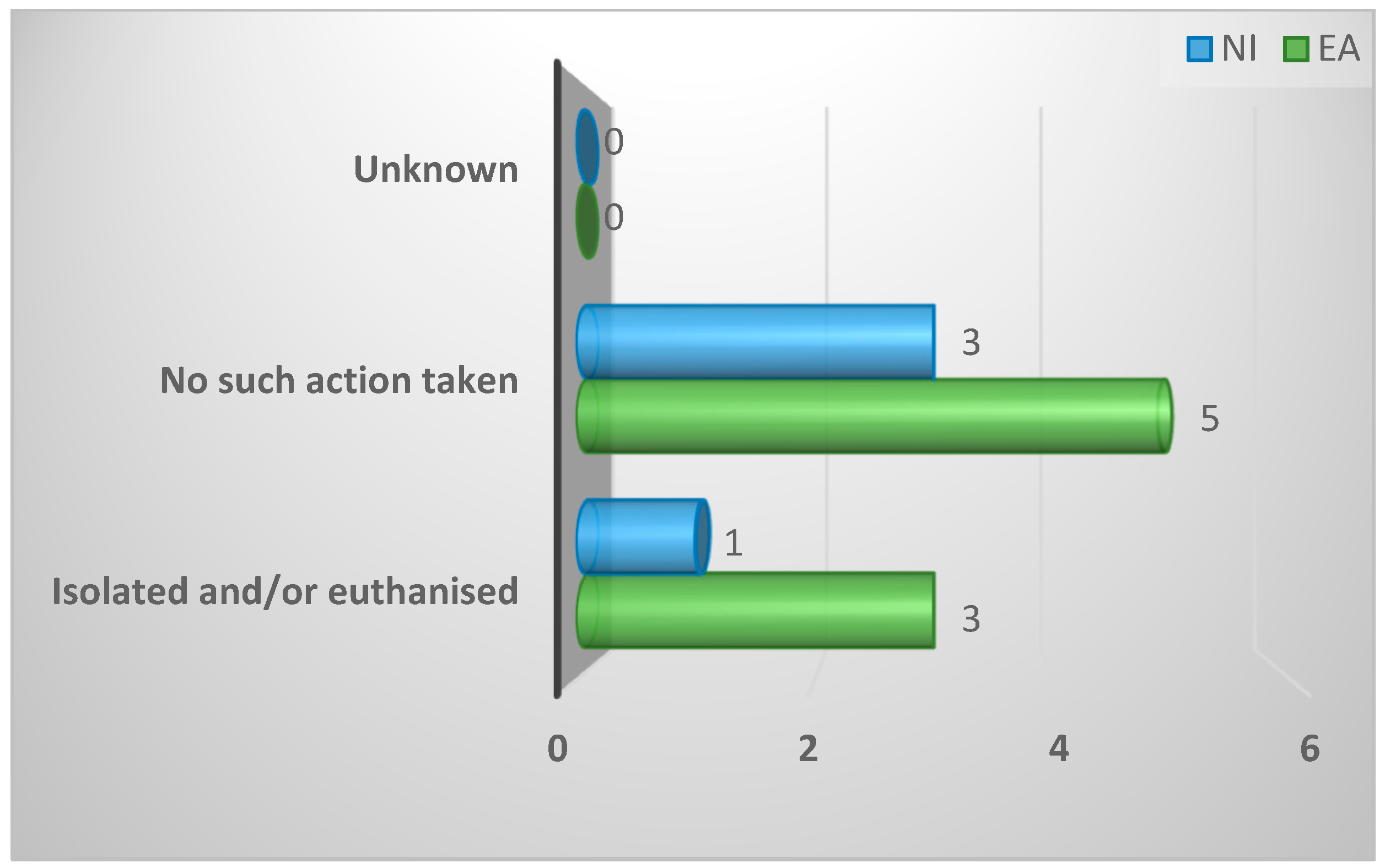
Figure A19.
Methods used for euthanasia of collected birds.
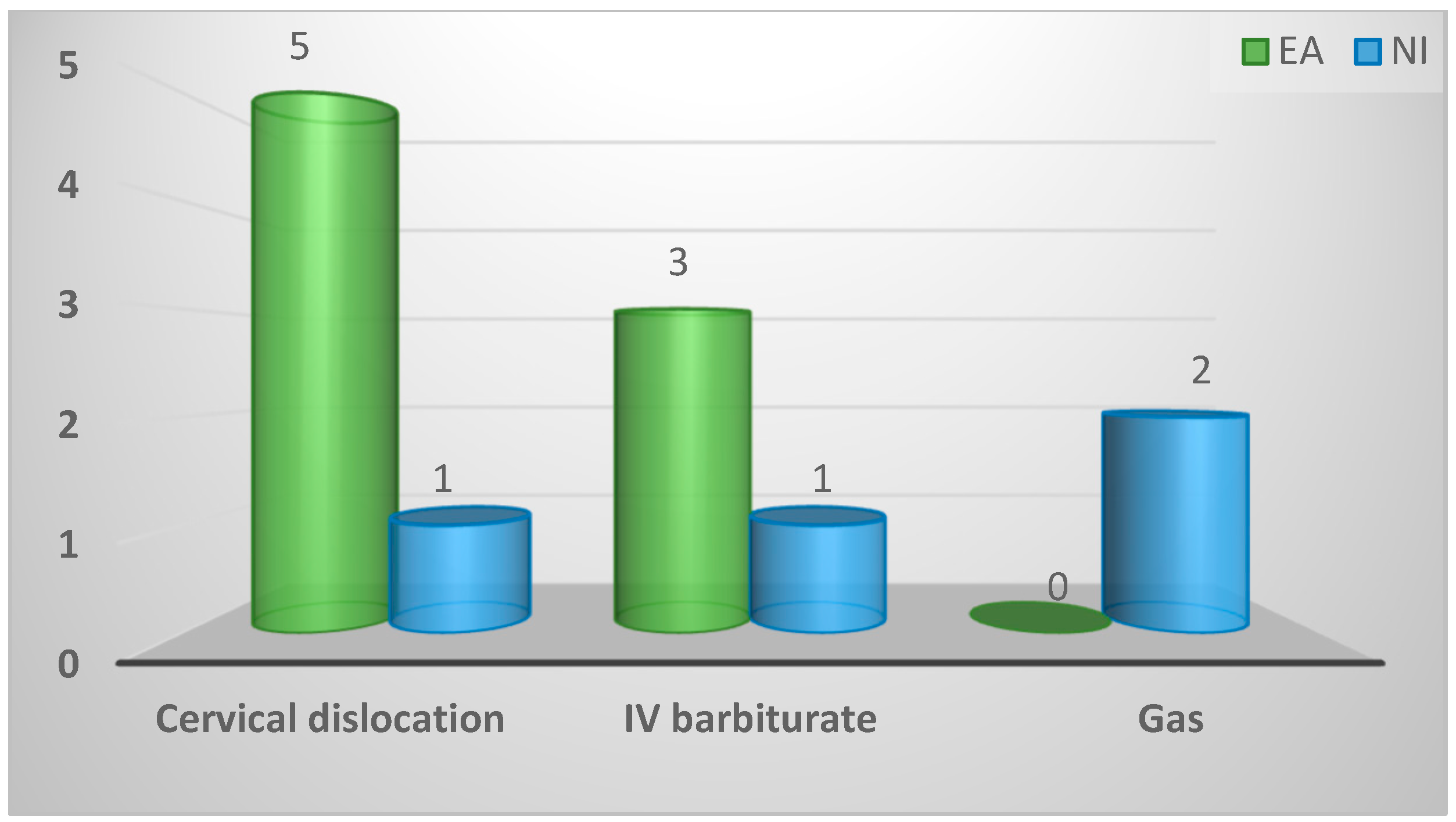
Figure A20.
Time lapse (minutes) between death and examination of sample birds for Spironucleus.
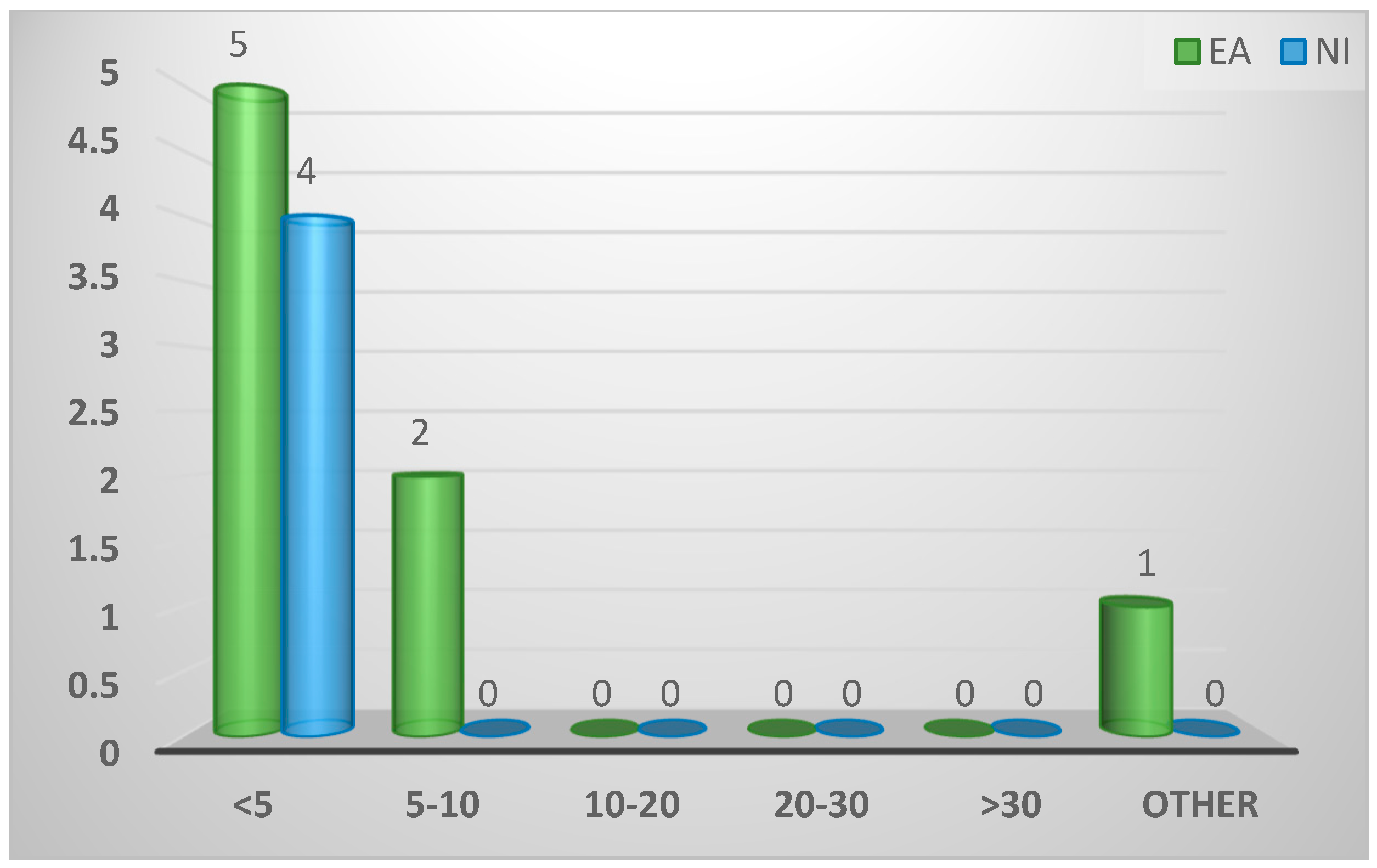
Figure A21.
Existence of time limit between death and examination of sample bird for Spironucleus.
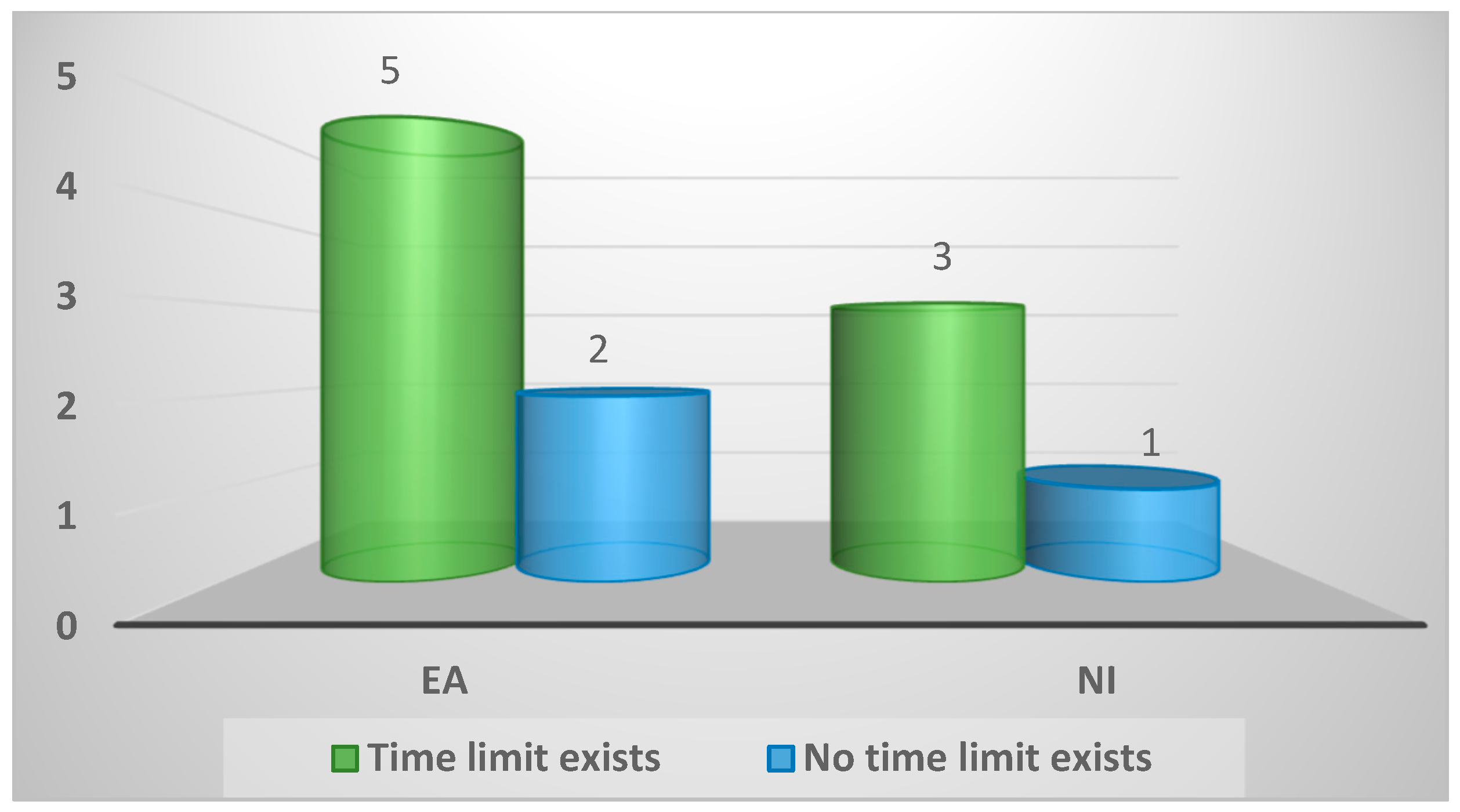
Figure A22.
Clinical signs of spironucleosis described by respondents.

Figure A23.
Practice protocol for post-mortem of suspected cases of enteric disease.
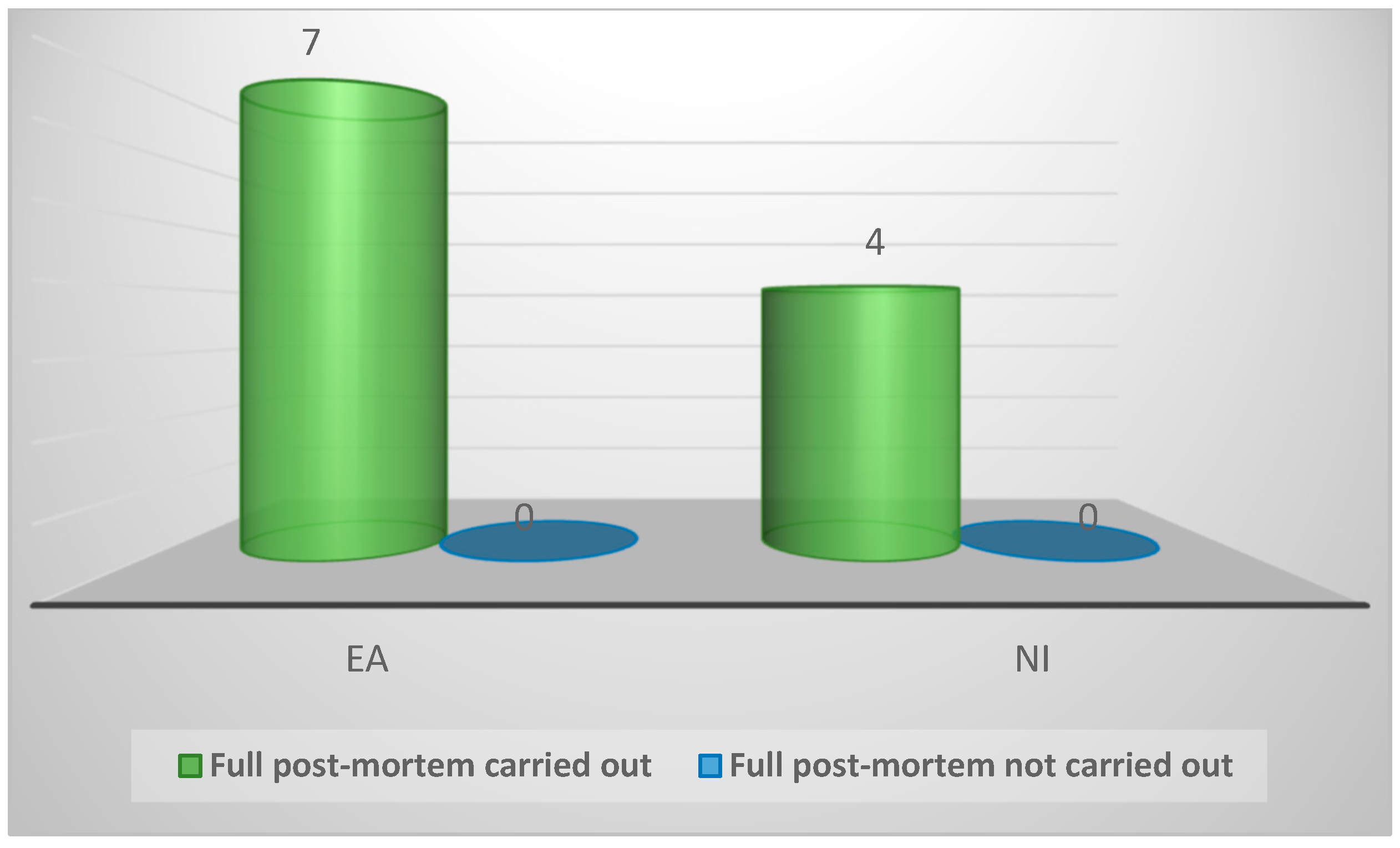
Figure A24.
Pathological changes visible on gross external examination.
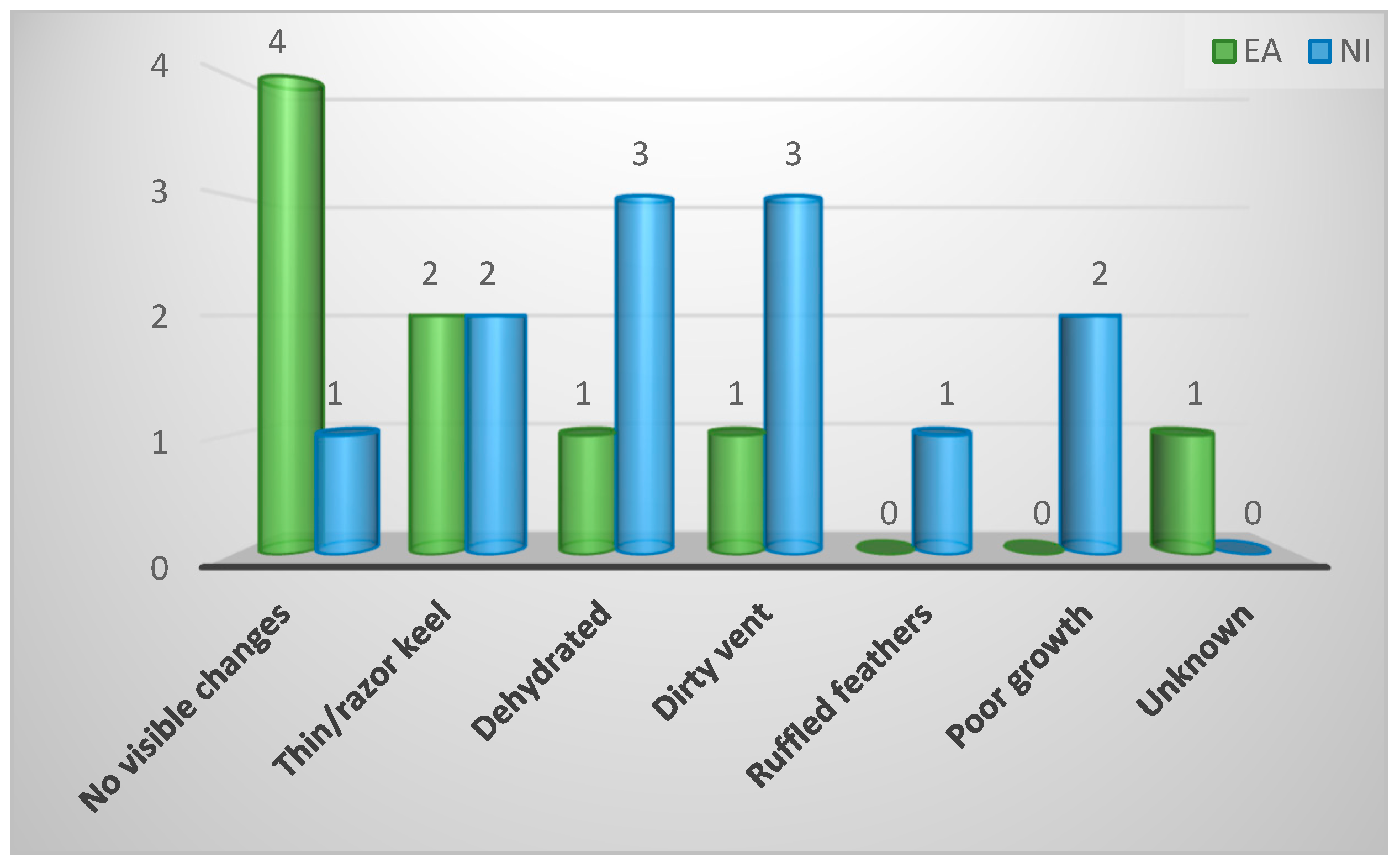
Figure A25.
Pathological changes visible on gross internal examination.
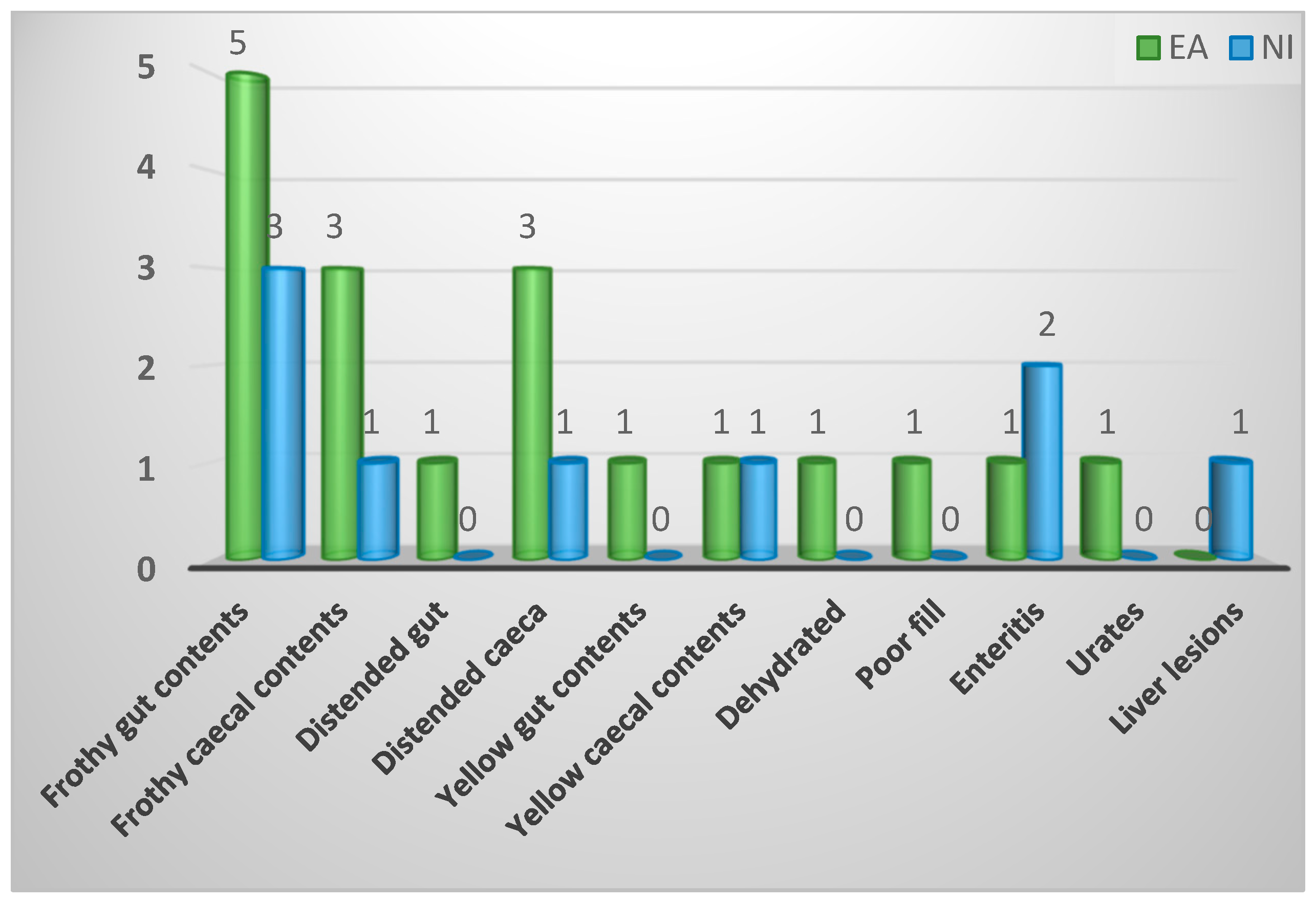
Figure A26.
Sites of sample bird utilised for spironucleosis diagnosis.
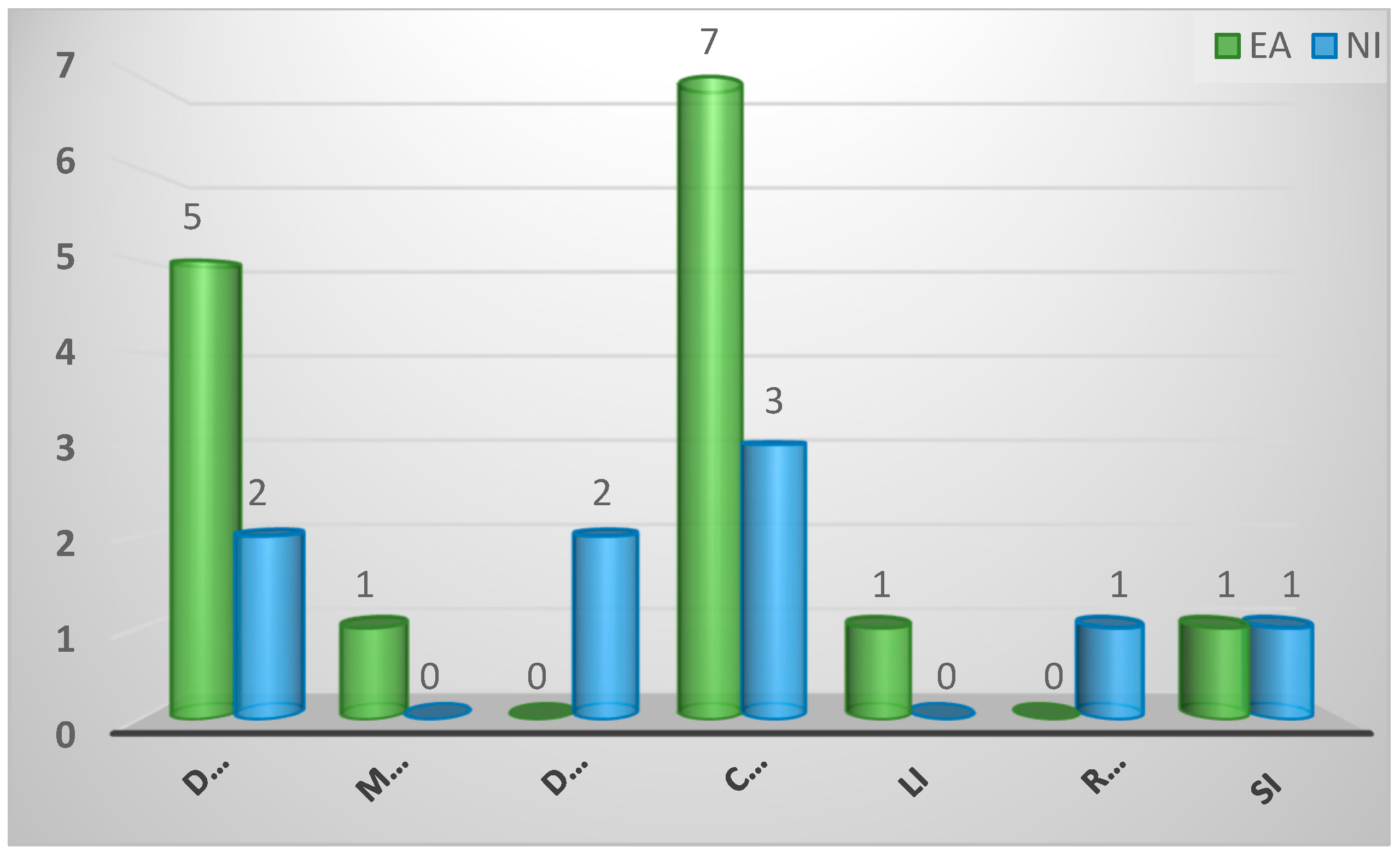
Figure A27.
Techniques described for spironucleosis diagnosis.
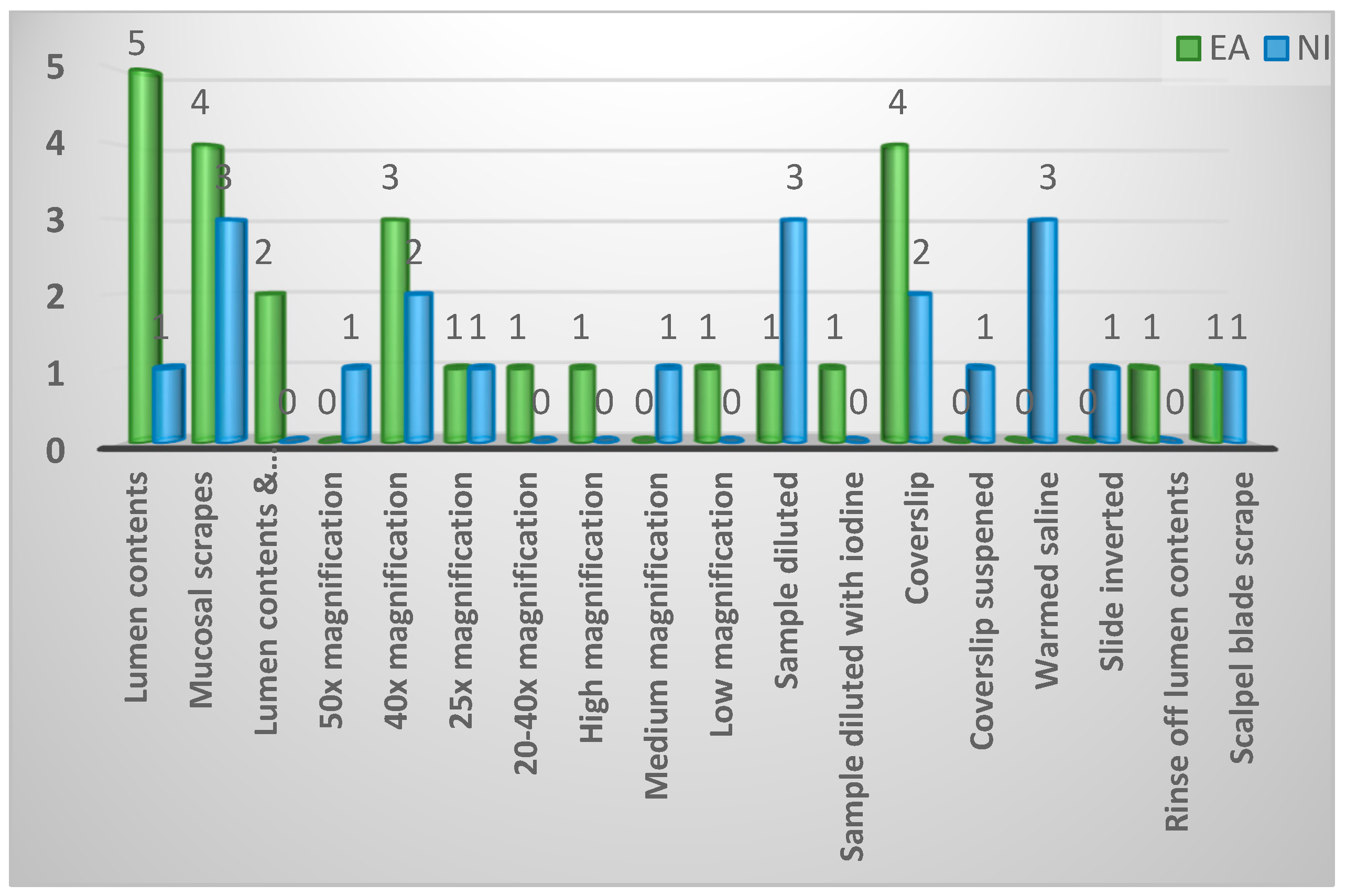
Figure A28.
Defining factors of a positive result.
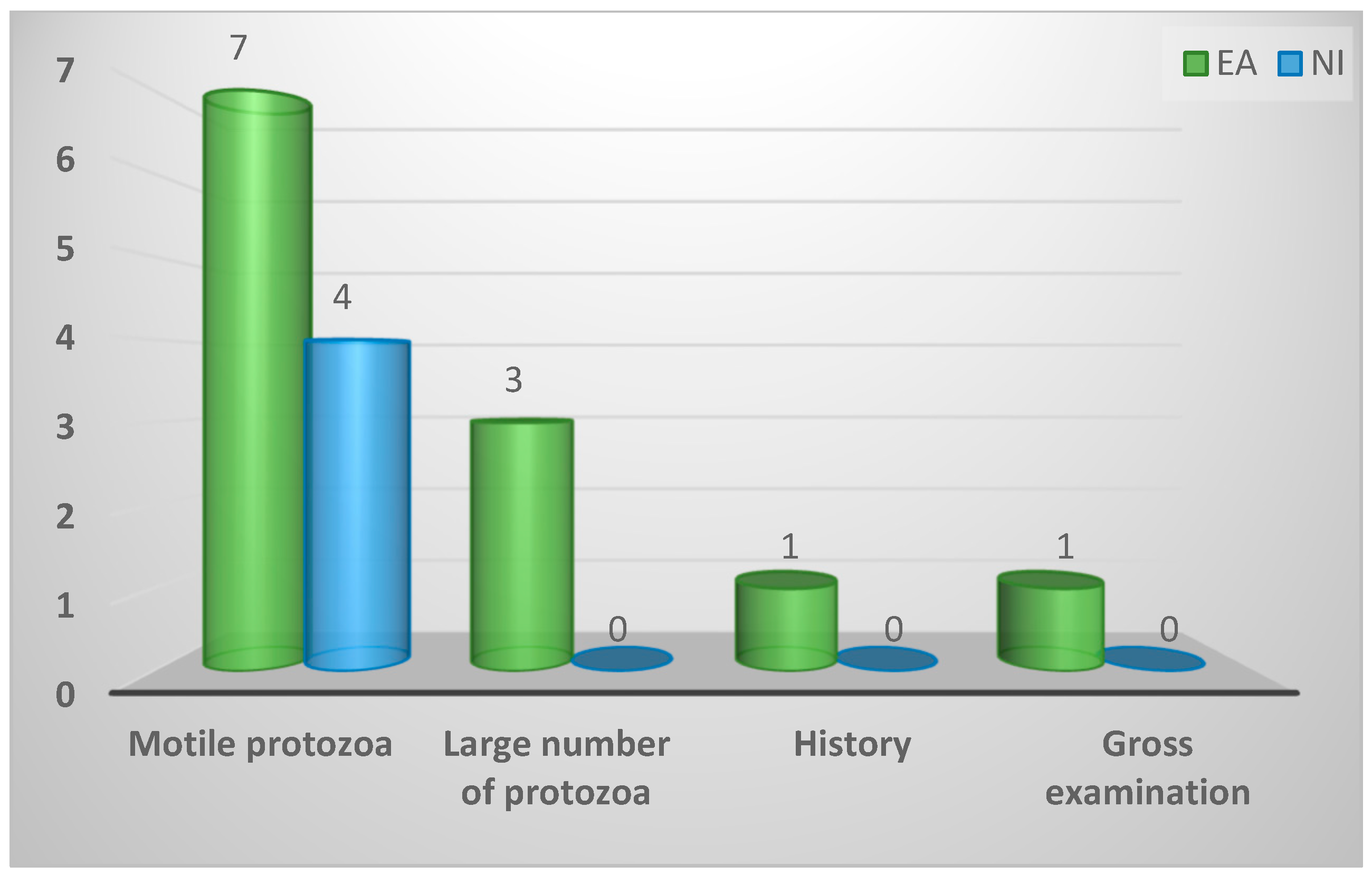
Figure A29.
Faeces utilisation in spironucleosis diagnosis.
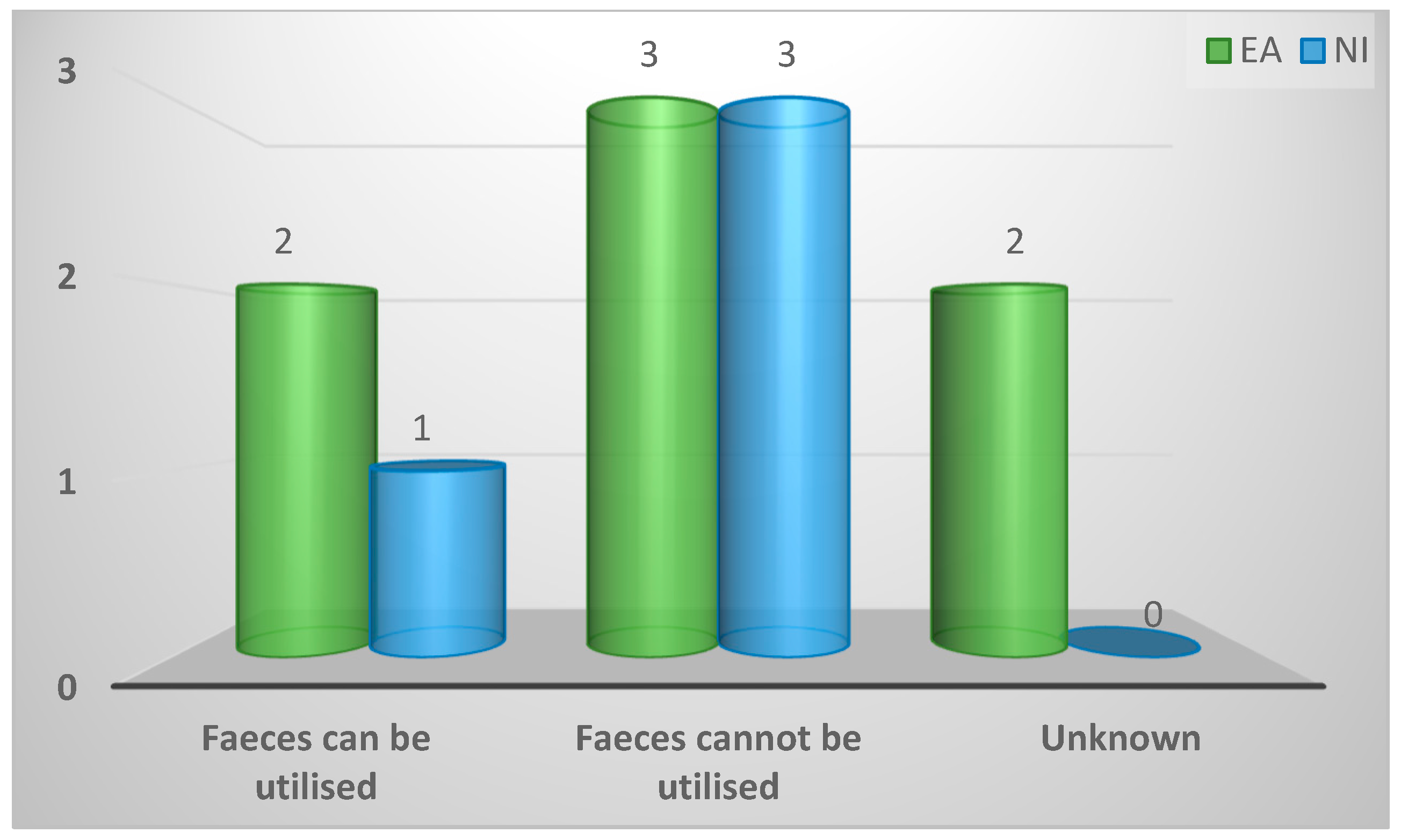
Figure A30.
Difficulty associated with Spironucleus differentiation.
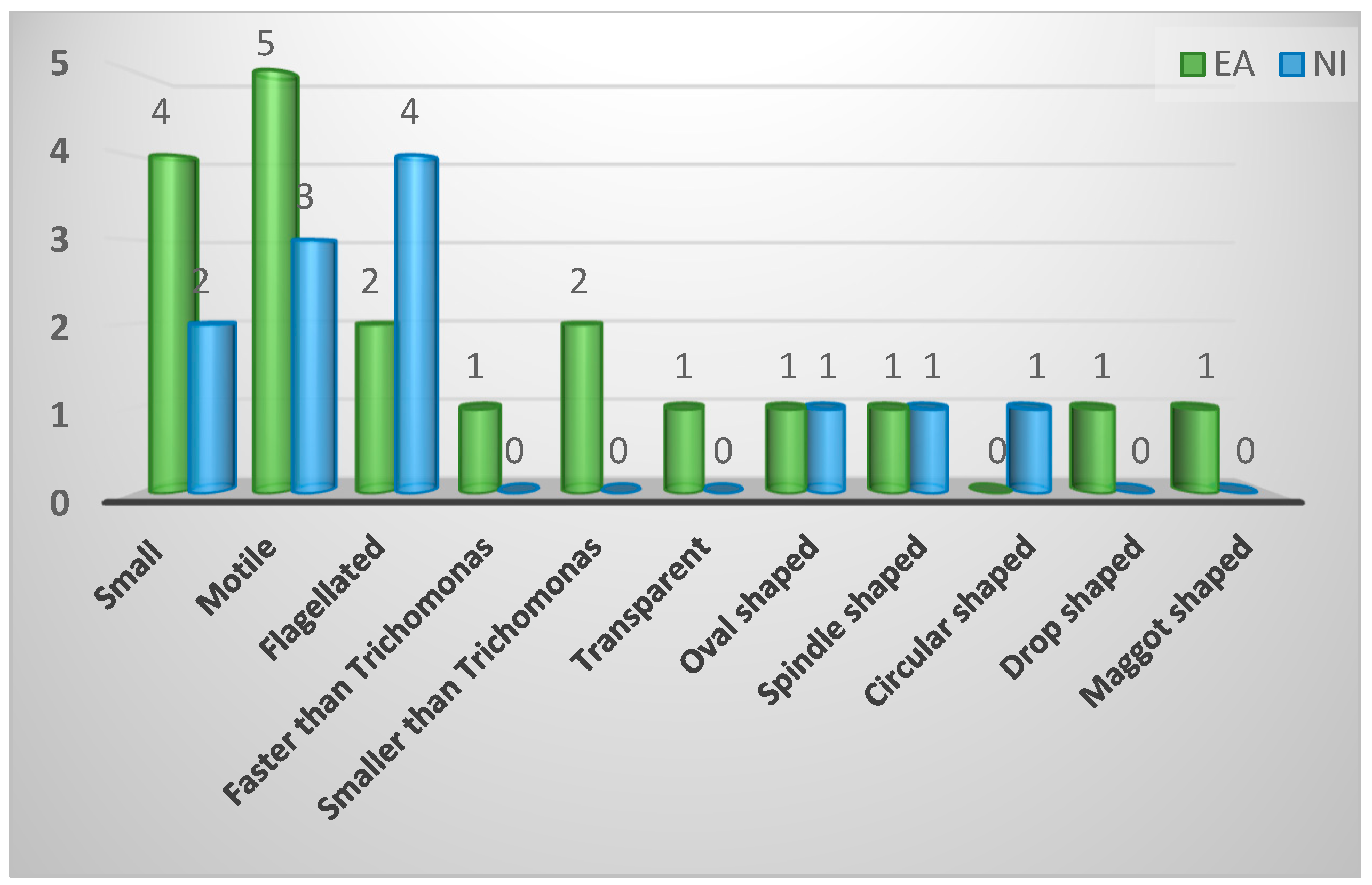
Figure A31.
Morphological descriptions of Spironucleus.
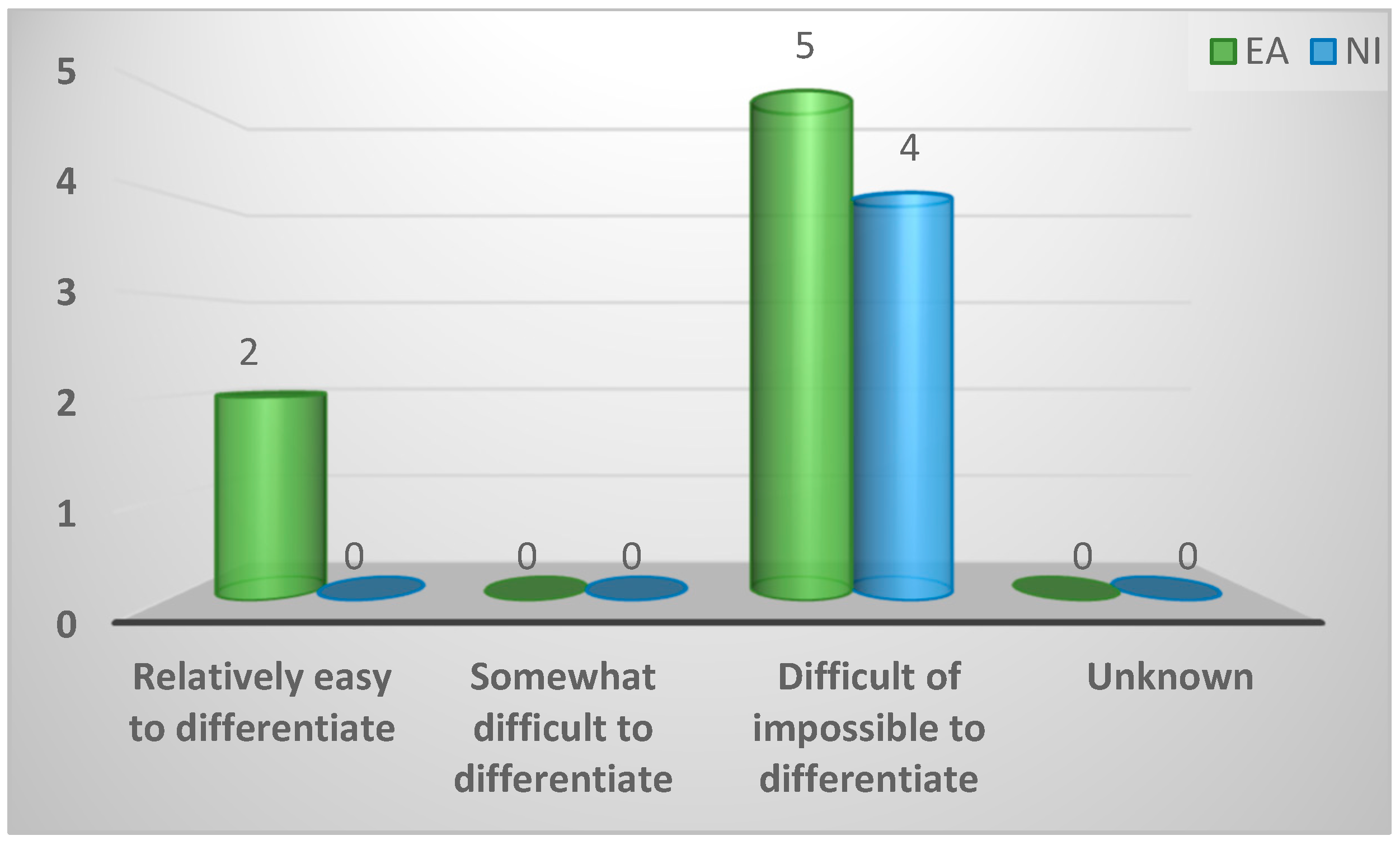
Figure A32.
Number of individual samples that need to test positive to confirm infection with Spironucleus in a bird.
Figure A32.
Number of individual samples that need to test positive to confirm infection with Spironucleus in a bird.
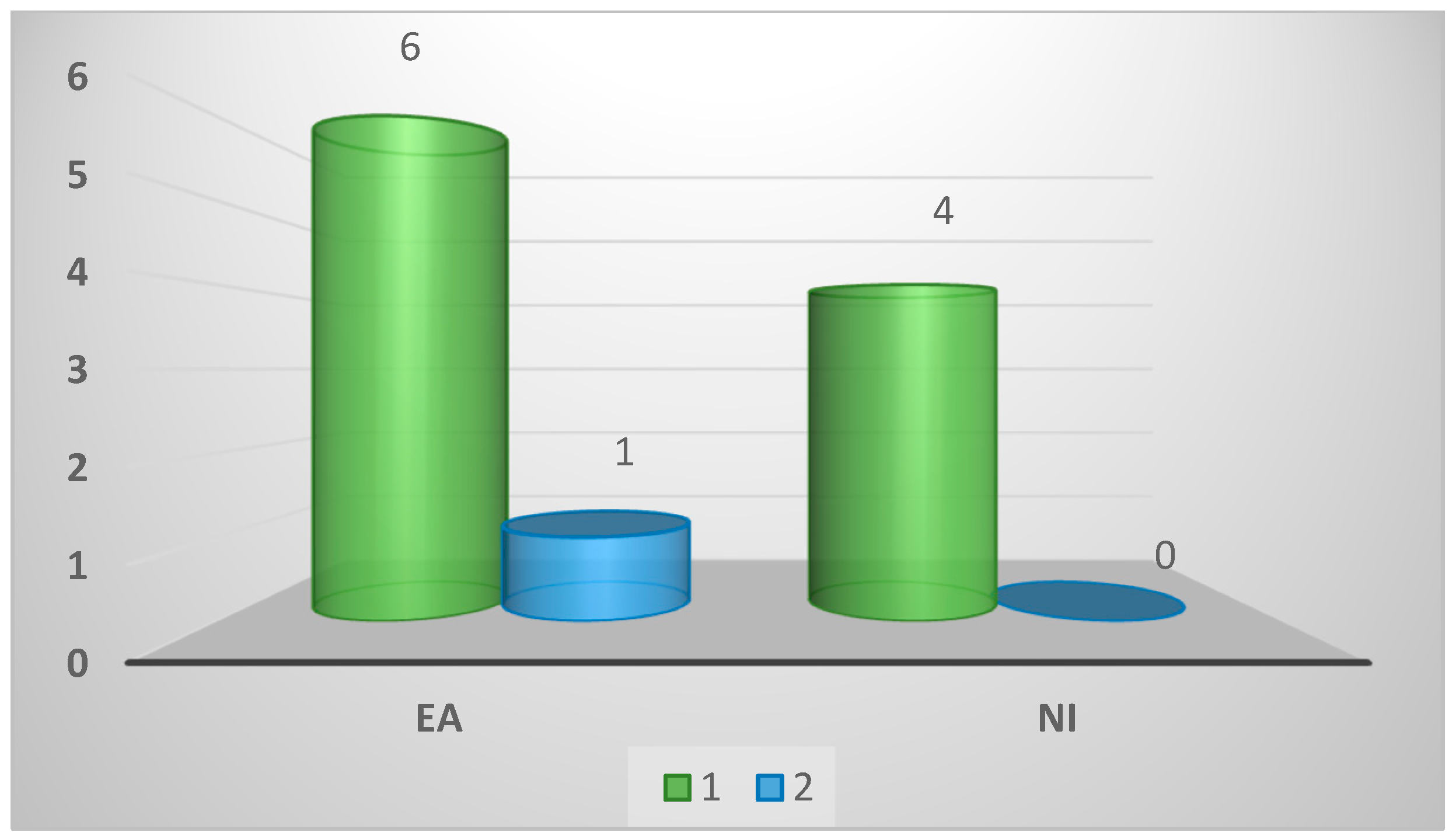
Figure A33.
Number of individual birds that need to test positive to confirm infection with Spironucleus in a flock.
Figure A33.
Number of individual birds that need to test positive to confirm infection with Spironucleus in a flock.
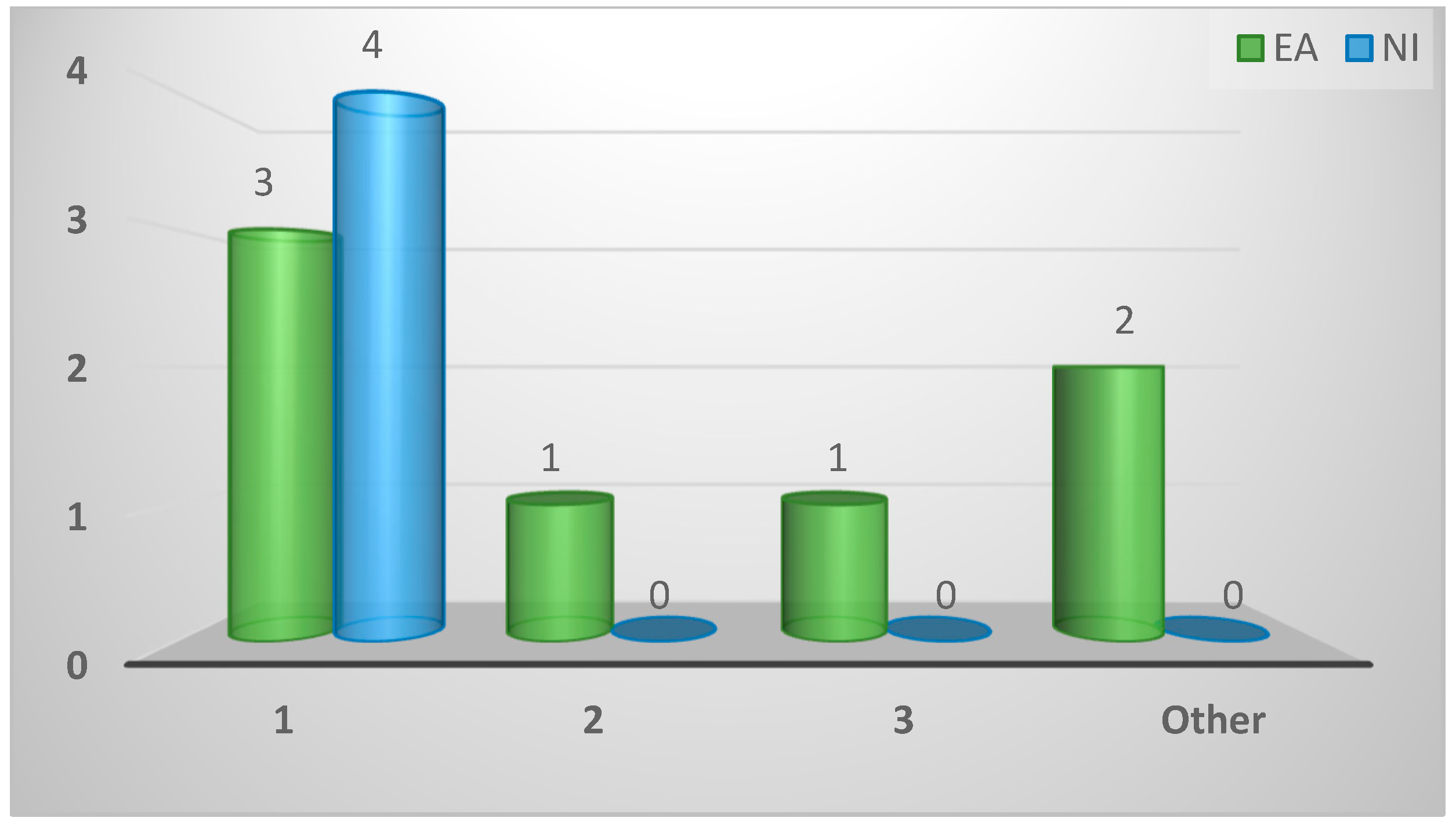
Figure A34.
Ability to quantify Spironucleus infection levels.
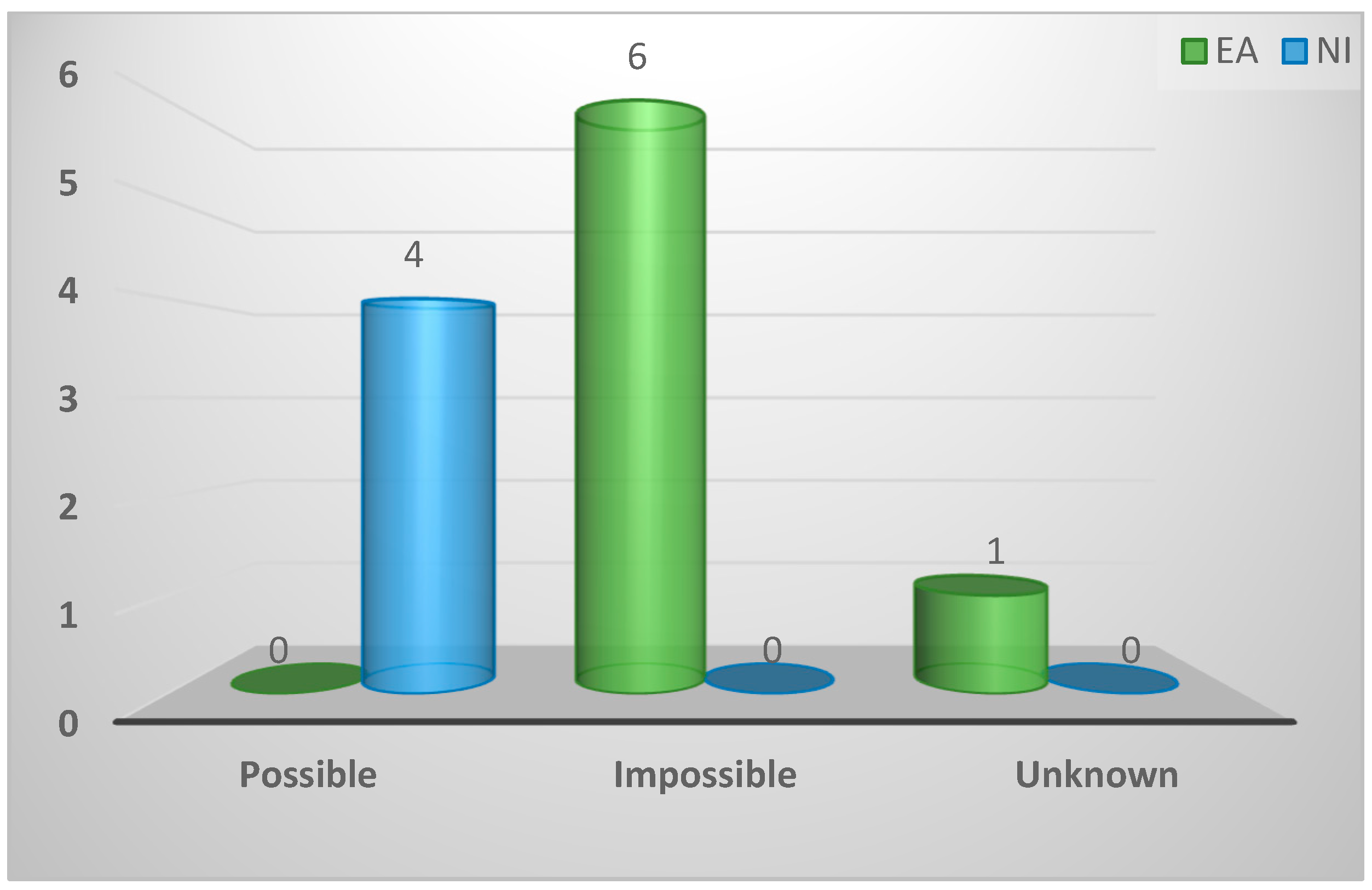
Figure A35.
Respondent’s reliance on stated method of diagnosis.
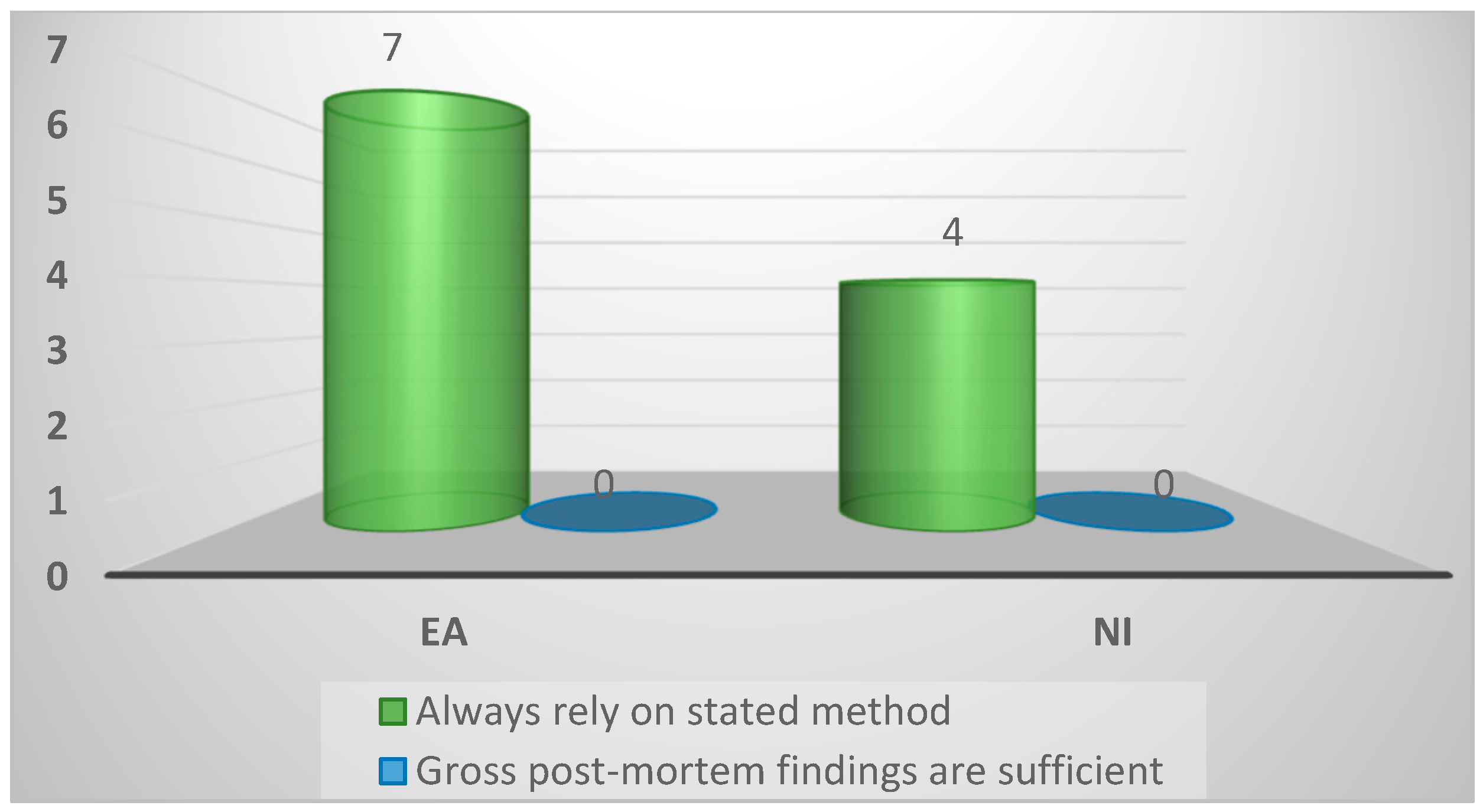
Figure A36.
Existence of other methods to diagnose spironucleosis.
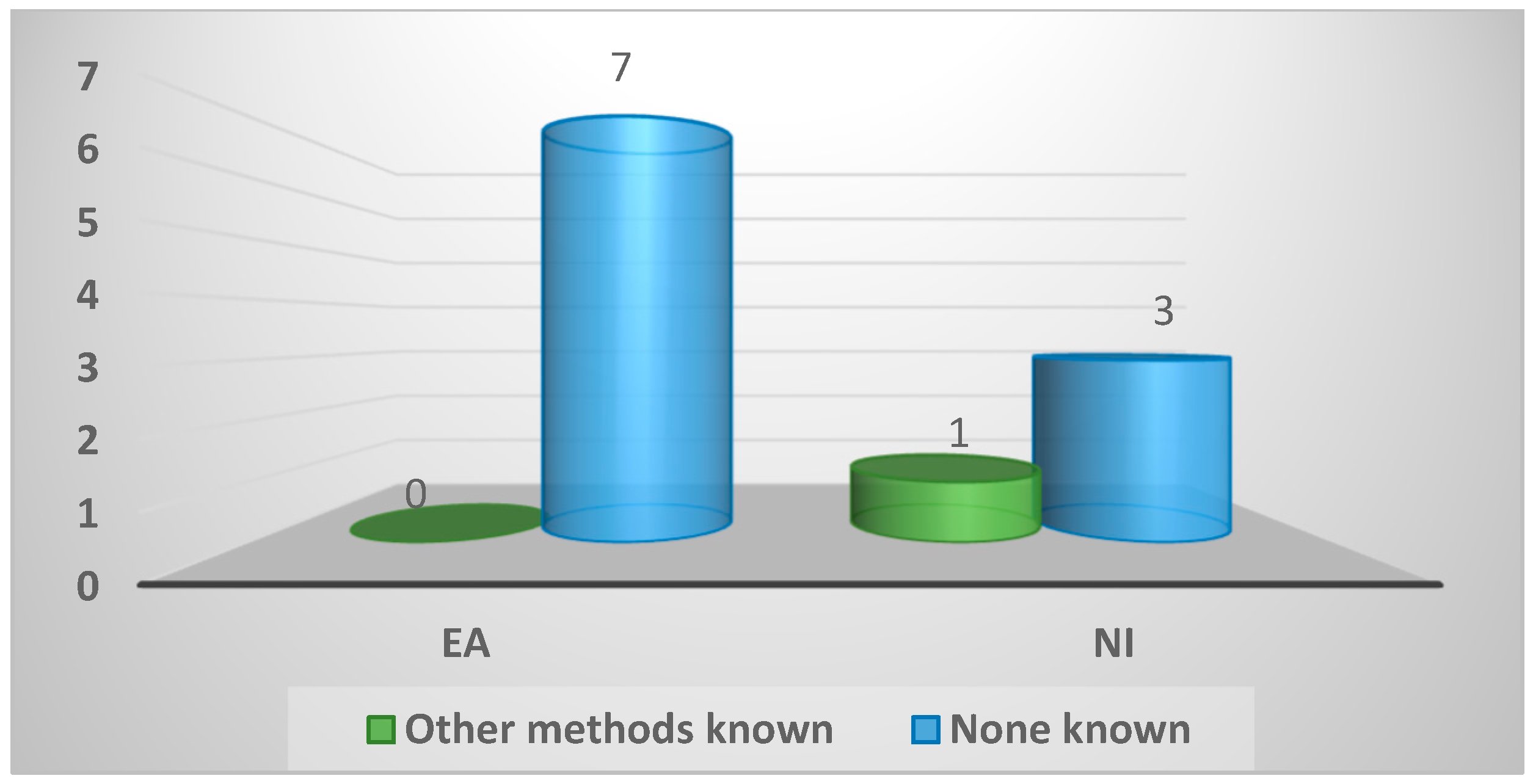
Figure A37.
Opinion on reproducibility of respondent’s method in general practice.
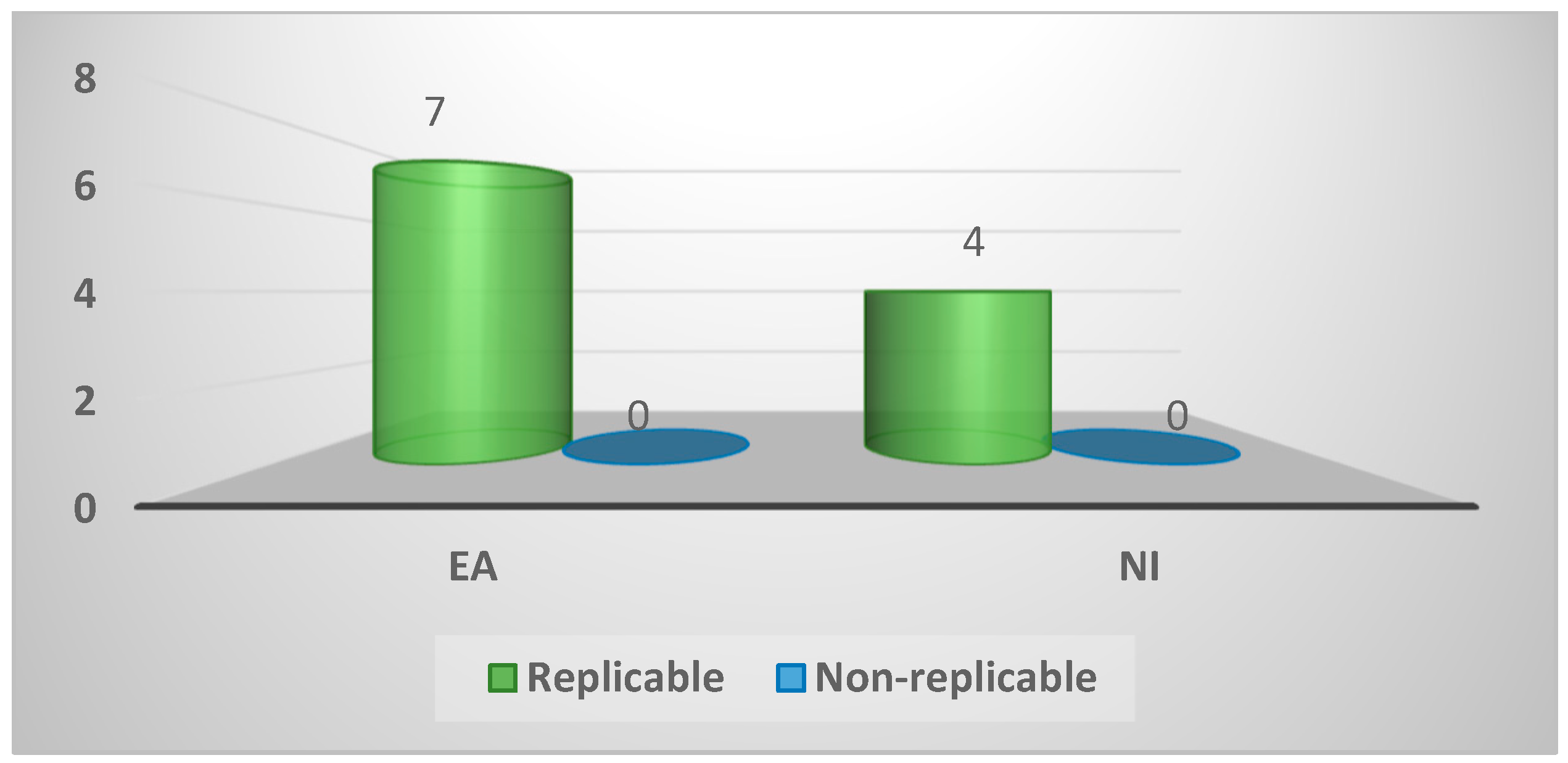
Figure A38.
Opinion on spironucleosis diagnosis in general practice.
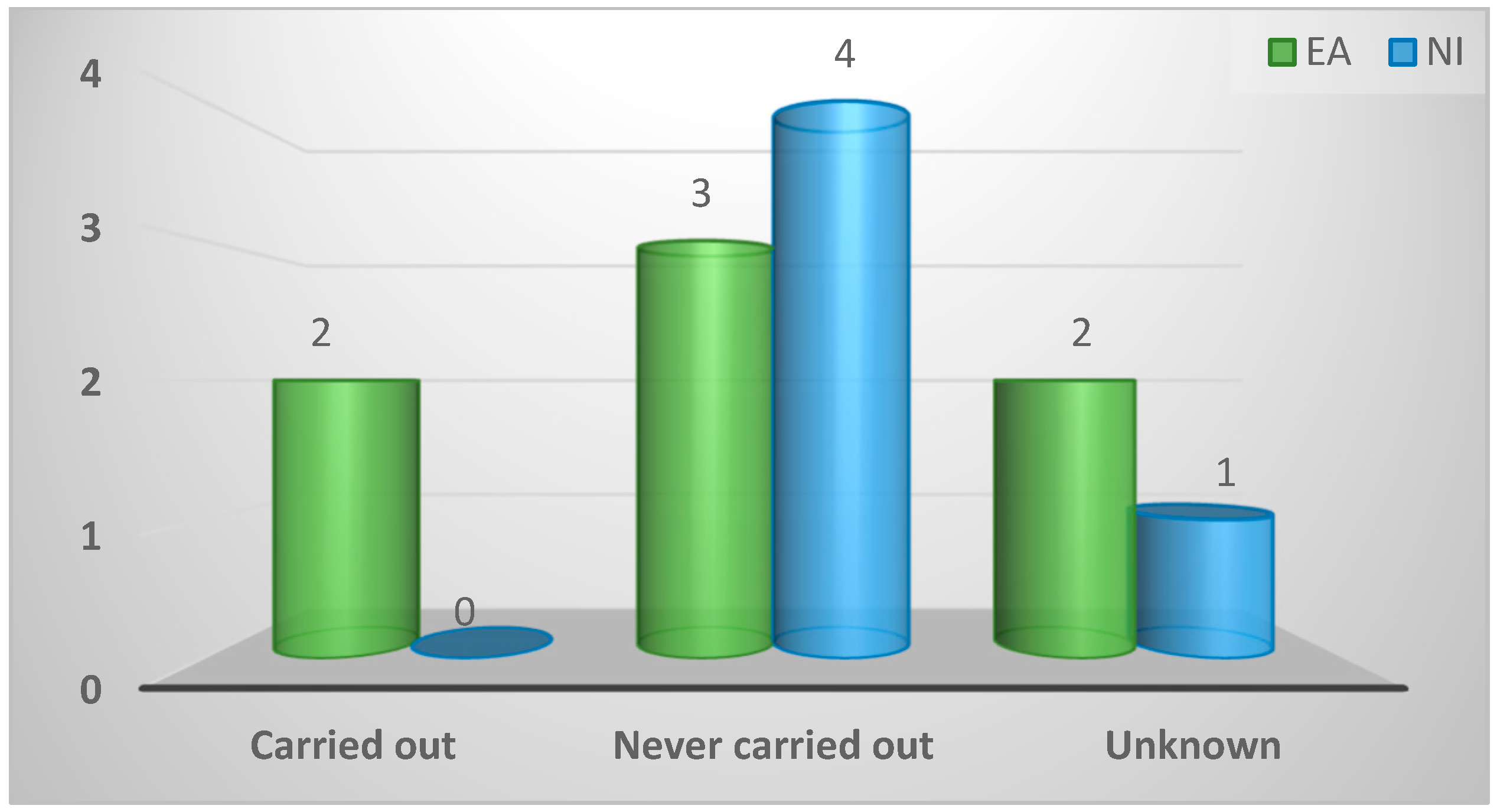
Figure A39.
Differences in spironucleosis diagnosis between respondent’s region and elsewhere.
References
- Lloyd, S.; Irvine, K.L.; Eves, S.M.; Gibson, J.S. Fluid absorption in the small intestine of healthy game birds and those infected with Spironucleus spp. Avian Pathol 2005, 34, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Lister, S. Disease of Game Birds. In Practice 1989, 11, 170–174. [Google Scholar] [CrossRef]
- Swarbrick, O. Hexamitiasis and an emaciation syndrome in pheasant poults: clinical aspects and differential diagnosis. Vet Rec 1990, 126, 265–267. [Google Scholar]
- Pennycott, T.W. Carriage of trichomonads, Hexamita species and Blastocystis species by adult pheasants. Vet Rec 1998, 143, 142–143. [Google Scholar] [CrossRef] [PubMed]
- Cooper, G.L.; Charlton, B.R.; Bickford, A.A.; Nordhausen, R. Hexamita meleagridis (Spironucleus meleagridis) infection in chukar partridges associated with high mortality and intracellular trophozoites. Avian Dis 2004, 48, 706–710. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, S.; Gibson, J.S. Haematology and biochemistry in healthy young pheasants and red-legged partridges and effects of spironucleosis on these parameters. Avian Pathol 2006, 35, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Welchman, D. Avian Practice: Diseases in young pheasants. In Practice 2008, 30, 86–89. [Google Scholar] [CrossRef]
- Swarbrick, O. Pheasant rearing: associated husbandry and disease problems. Vet Rec 1985, 116, 610–617. [Google Scholar] [CrossRef]
- Wood, A.M.; Smith, H.V. Spironucleosis (Hexamitiasis, Hexamitosis) in the ring-necked pheasant (Phasianus colchicus): detection of cysts and description of Spironucleus meleagridis in stained smears. Avian Dis 2005, 49, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Harper, F.D. Hexamita species present in some avian species in South Wales. Vet Rec 1991, 128, 130. [Google Scholar] [CrossRef]
- Stoikov, D. Detection of Hexamita meleagridis in Bulgaria. Vet Med Nauki. 1985, 22, 44–50. [Google Scholar] [PubMed]
- Trees, A.J. Parasitic conditions in poultry 1: Protozoal diseases. In Practice 1987, 9, 86–89. [Google Scholar] [CrossRef]
- Dezfoulian, O.; Gharagozlou, M.J.; Rahbari, S. Hexamita infection associated with diarrhoea and stunting in native turkey poults. Trop Biomed 2010, 27, 504–508. [Google Scholar] [PubMed]
- Hussain, A.Z. Morphometric evaluation of the small intestines and caeca of pheasants infected with Hexamita and Trichomonas species. Vet Rec 2001, 148, 484–485. [Google Scholar] [CrossRef]
- Pennycott, T.W. Effect of four therapeutic agents on Trichomonas phasiani carriage in pheasants. Vet Rec 1996, 139, 214–215. [Google Scholar] [CrossRef] [PubMed]
- McNeil, E.H.; Hinshaw, W.R.; Kofoid, C.A. Hexamita meleagridis sp nov from the turkey. American Journal of Hygiene 1941, 34, 71–82. [Google Scholar]
- Zwart, P.; Hooimeijer, J. Hexamitiasis in carrier pigeons in the Netherlands. Tijdschr Diergeneeskd 1985, 110, 1074–1075. [Google Scholar] [PubMed]

Table 1.
Characteristics of participants’ veterinary practice and comparative relative frequencies between East Anglia and Northern Ireland.
Table 1.
Characteristics of participants’ veterinary practice and comparative relative frequencies between East Anglia and Northern Ireland.
| Variable | Total (n = 28) No. (%) |
EA (n = 15) No. (%) |
NI (n = 13) No. (%) |
P value |
|---|---|---|---|---|
| Type of practice | ||||
| Mixed practice | 18 (64%) | 8 (53%) | 10 (77%) | 0.43 |
| Small animal | 3 (11%) | 3 (20%) | 0 (0%) | |
| Large animal | 1 (4%) | 1 (7%) | 0 (0%) | |
| Poultry | 3 (11%) | 2 (13%) | 1 (8%) | |
| Laboratory | 3 (11%) | 1 (7%) | 2 (15%) | |
| No. of veterinarians per practice | ||||
| <7 | 19 (68%) | 11 (73%) | 8 (62%) | 0.7 |
| ≥7 | 9 (32%) | 4 (27%) | 5 (38%) | |
| Gamebird caseload | ||||
| <5 | 26 (93%) | 14 (93%) | 12 (92%) | 1.0 |
| 5-25 | 2 (7%) | 1 (7%) | 1 (8%) | |
| >25 | 0 (0%) | 0 (0%) | 0 (0%) | |
| Most common breed of game birds seen | ||||
| Pheasant | 23 (82%) | 10 (67%) | 13 (100%) | 0.07 |
| Partridge | 3 (11%) | 3 (20%) | 0 (0%) | |
| Partridge and pheasant | 2 (7%) | 2 (13%) | 0 (0%) | |
| Most common age of game birds seen | ||||
| Poult | 19 (68%) | 12 (80%) | 7 (54%) | 0.13 |
| Chick and poult | 6 (21%) | 1 (7%) | 5 (38%) | |
| Chick | 1 (4%) | 1 (7%) | 0 (0%) | |
| Adult | 2 (7%) | 1 (7%) | 1 (8%) | |
Table 2.
Relative frequencies of body systems affected in game birds, handling of cases and drug prescription between veterinarians in East Anglia and Northern Ireland.
Table 2.
Relative frequencies of body systems affected in game birds, handling of cases and drug prescription between veterinarians in East Anglia and Northern Ireland.
| Variables | Total (n = 28) N (%) |
EA (n = 15) N (%) |
NI (n = 13) N (%) |
P value |
|---|---|---|---|---|
| Bodily system of game birds most frequently diagnosed | ||||
| Gastrointestinal | 21 (75%) | 12 (80%) | 9 (69%) | 0.8 |
| Respiratory | 4 (14%) | 2 (13%) | 2 (15%) | |
| Gastrointestinal and respiratory | 3 (11%) | 1 (7%) | 2 (15%) | |
| Musculoskeletal | 0 (0%) | 0 (0%) | 0 (0%) | |
| Reproductive | 0 (0%) | 0 (0%) | 0 (0%) | |
| Location of diagnosis of disorders in game birds | ||||
| On site (Practice) | 18 (64%) | 11 (73%) | 7 (54%) | 0.16 |
| On location (Game farm) | 4 (14%) | 3 (20%) | 1 (8%) | |
| Other | 6 (21%) | 1 (7%) | 5 (38%) | |
| Practice position on prescribing drugs to game birds | ||||
| Prescribe | 25 (89%) | 14 (93%) | 11 (85%) | 0.58 |
| Do not prescribe | 3 (11%) | 1 (7%) | 2 (15%) | |
| Prescription protocol on seeing affected birds prior to treatment | ||||
| See birds initially | 12 (43%) | 8 (53%) | 4 (31%) | 0.37 |
| Do not see birds initially | 11 (39%) | 4 (27%) | 7 (54%) | |
| Other | 5 (18%) | 3 (20%) | 2 (16%) | |
Table 3.
The importance and perception of enteric disease in game birds amongst veterinarians in East Anglia and Northern Ireland.
Table 3.
The importance and perception of enteric disease in game birds amongst veterinarians in East Anglia and Northern Ireland.
| Variables | Total (n = 28) N (%) |
EA (n = 15) N (%) |
NI (n = 13) N (%) |
P value |
|---|---|---|---|---|
| Eagerness of gamekeepers to consult vet | ||||
| Very Willing | 8 (29%) | 7 (47%) | 1 (8%) | 0.04 |
| Somewhat Willing | 6 (21%) | 3 (20%) | 3 (23%) | |
| Unwilling | 10 (36%) | 4 (27%) | 6 (46%) | |
| Never | 3 (11%) | 0 (0%) | 3 (23%) | |
| Unknown | 1 (4%) | 1 (7%) | 0 (0%) | |
| Location of diagnosis of enteric disease | ||||
| In practice | 12 (43%) | 7 (47%) | 5 (38%) | 0.84 |
| Sent elsewhere | 15 (54%) | 7 (47%) | 8 (62%) | |
| Other | 1 (4%) | 1 (7%) | 0 (0%) | |
| Importance assigned to enteric disease of gamebirds (1-10) | ||||
| ≤4 | 0 (0%) | 0 (0%) | 0 (0%) | 0.45 |
| 5 | 2 (7%) | 2 (13%) | 0 (0%) | |
| 6 | 3 (11%) | 1 (7%) | 2 (15%) | |
| 7 | 7 (25%) | 3 (20%) | 4 (31%) | |
| 8 | 7 (25%) | 3 (20%) | 4 (31%) | |
| 9 | 5 (18%) | 3 (20%) | 2 (15%) | |
| 10 | 3 (11%) | 3 (20%) | 0 (0%) | |
| Missing | 1 (4%) | 0 (0%) | 1 (4%) | |
| Importance assigned to spironucleosis (1-10) | ||||
| ≤3 | 0 (0%) | 0 (0%) | 0 (0%) | 1.0 |
| 4 | 4 (27%) | 3 (30%) | 1 (20%) | |
| 5 | 3 (20%) | 2 (20%) | 1 (20%) | |
| 6 | 3 (20%) | 2 (20%) | 1 (20%) | |
| 7 | 0 (0%) | 0 (0%) | 0 (0%) | |
| 8 | 2 (13%) | 1 (10%) | 1 (20%) | |
| 9 | 2 (13%) | 1 (10%) | 1 (20%) | |
| 10 | 1 (7%) | 1 (10%) | 0 (0%) | |
| Variables |
Total (n = 28) n (%) |
EA (n = 15) n (%) |
NI (n = 13) n (%) |
P Value |
| Rearing stage(s) most closely associated with spironucleosis | ||||
| Rearing field | 7 (41%) | 5 (42%) | 2 (40%) | 0.18 |
| Rearing field and release pens | 5 (29%) | 2 (17%) | 3 (60%) | |
| Release pens | 0 (0%) | 0 (0%) | 0 (0%) | |
| Laying pens | 0 (0%) | 0 (0%) | 0 (0%) | |
| Hatchery | 0 (0%) | 0 (0%) | 0 (0%) | |
| Unknown | 5 (29%) | 5 (42%) | 0 (0%) | |
| Variables |
Total (n = 33) N (%) |
EA (n = 19) N (%) |
NI (n = 14) N (%) |
P value |
| Most commonly diagnosed causative agent of enteric disease | ||||
| Coccidia | 17 (52%) | 11 (58%) | 6 (43%) | 0.53 |
| Spironucleus | 6 (18%) | 4 (21%) | 2 (14%) | |
| Bacterial | 3 (9%) | 1 (5%) | 2 (14%) | |
| Gapeworm | 1 (3%) | 0 (0%) | 1 (7%) | |
| Histomonas | 1 (3%) | 1 (5%) | 0 (0%) | |
| Rotavirus | 1 (3%) | 1 (5%) | 0 (0%) | |
| Unknown | 4 (12%) | 1 (5%) | 3 (21%) | |
Table 4.
Approach of veterinarians in East Anglia and Northern Ireland on sample collection and diagnostic techniques for spironucleosis.
Table 4.
Approach of veterinarians in East Anglia and Northern Ireland on sample collection and diagnostic techniques for spironucleosis.
| Variables | Total (n = 13) No. (%) |
EA (n = 9) No. (%) |
NI (n = 4) No. (%) |
P value |
|---|---|---|---|---|
| Stakeholder responsible for selection of birds for diagnosis | ||||
| Client | 12 (92%) | 9 (100%) | 3 (75%) | 0.31 |
| Vet | 1 (8%) | 0 (0%) | 1 (25%) | |
| Nature of birds removed from flock for diagnosis | ||||
| Dead and alive birds | 6 (46%) | 5 (56%) | 1 (25%) | 0.69 |
| Dead Birds | 0 (0%) | 0 (0%) | 0 (0%) | |
| Clinically affected birds | 6 (46%) | 3 (33%) | 3 (75%) | |
| Clinically affected and non- clinically affected Birds | 1 (8%) | 1 (11%) | 0 (0%) | |
| Variables |
Total (n = 12) No. (%) |
EA (n = 8) No. (%) |
NI (n = 4) No. (%) |
P value |
| Fate of remaining clinically infected birds in flock | ||||
| Isolate and euthanise | 4 (33%) | 3 (38%) | 1 (25%) | 1.0 |
| No action taken | 8 (67%) | 5 (63%) | 3 (75%) | |
| Euthanasia method of collected birds | ||||
| Cervical dislocation | 6 (50%) | 5 (63%) | 1 (25%) | 0.19 |
| IV barbiturate | 4 (33%) | 3 (38%) | 1 (25%) | |
| Gas | 2 (17%) | 0 (0%) | 2 (50%) | |
| Time (minutes) between death of bird and examination for Spironucleus | ||||
| <5 | 9 (75%) | 5 (63%) | 4 (100%) | 0.66 |
| 5-10 | 2 (17%) | 2 (25%) | 0 (0%) | |
| >10 | 0 (0%) | 0 (0%) | 0 (0%) | |
| Other | 1 (8%) | 1 (13%) | 0 (0%) | |
| Variables |
Total (n = 11) No. (%) |
EA (n = 7) No. (%) |
NI (n = 4) No. (%) |
P value |
| Existence of a time limit between death and examination for Spironucleus | ||||
| Time limit exists | 8 (73%) | 5 (71%) | 3 (75%) | 1.0 |
| No time limit exists | 3 (27%) | 2 (29%) | 1 (25%) | |
Table 5.
Adoption of existing methods for diagnosis of spironucleosis in game birds amongst veterinarians in East Anglia and Northern Ireland.
Table 5.
Adoption of existing methods for diagnosis of spironucleosis in game birds amongst veterinarians in East Anglia and Northern Ireland.
| Variables | Total (n = 34) No. (%) |
EA (n = 21) No. (%) |
NI (n = 13) No. (%) |
P value |
|---|---|---|---|---|
| Clinical signs associated with spironucleosis | ||||
| Diarrhoea | 9 (27%) | 6 (29%) | 3 (23%) | 0.56 |
| Ill thrift | 7 (21%) | 5 (24%) | 2 (15%) | |
| Depression | 6 (18%) | 4 (19%) | 2 (15%) | |
| Mortality | 5 (15%) | 1 (5%) | 4 (31%) | |
| Malaise | 3 (9%) | 1 (5%) | 2 (15%) | |
| Altered gait | 1 (3%) | 1 (5%) | 0 (0%) | |
| Dehydration | 1 (3%) | 1 (5%) | 0 (0%) | |
| Lethargy | 1 (3%) | 1 (5%) | 0 (0%) | |
| Ruffled feathers | 1 (3%) | 1 (5%) | 0 (0%) | |
| Variables |
Total (n = 11) No. (%) |
EA (n = 7) No. (%) |
NI (n = 4) No. (%) |
P value |
| Practice protocol for post-mortem of suspected enteric disease | ||||
| Full post-mortem carried out | 11 (100%) | 7 (100%) | 4 (100%) | 1.0 |
| Full post-mortem not carried out | 0 (0%) | 0 (0%) | 0 (0%) | |
| Variables |
Total (n = 21) No. (%) |
EA (n = 9) No. (%) |
NI (n = 12) No. (%) |
P value |
| Pathological changes visible on gross external examination | ||||
| No visible changes | 5 (24%) | 4 (44%) | 1 (8%) | 0.35 |
| Dehydrated | 4 (19%) | 1 (11%) | 3 (25%) | |
| Dirty vent | 4 (19%) | 1 (11%) | 3 (25%) | |
| Thin keel | 4 (19%) | 2 (22%) | 2 (17%) | |
| Poor growth | 2 (10%) | 0 (0%) | 2 (17%) | |
| Ruffled feathers | 1 (5%) | 0 (0%) | 1 (8%) | |
| Unknown | 1 (5%) | 1 (11%) | 0 (0%) | |
| Variables |
Total (n = 27) No. (%) |
EA (n = 18) No. (%) |
NI (n = 9) No. (%) |
P value |
| Pathological changes visible on gross internal examination | ||||
| Frothy gut contents | 8 (30%) | 5 (28%) | 3 (33%) | 0.94 |
| Frothy caecal contents | 4 (15%) | 3 (17%) | 1 (11%) | |
| Distended gut | 1 (4%) | 1 (6%) | 0 (0%) | |
| Distended caeca | 4 (15%) | 3 (17%) | 1 (11%) | |
| Yellow gut contents | 1 (4%) | 1 (6%) | 0 (0%) | |
| Yellow caecal contents | 2 (7%) | 1 (6%) | 1 (11%) | |
| Enteritis | 3 (11%) | 1 (6%) | 2 (22%) | |
| Dehydrated | 1 (4%) | 1 (6%) | 0 (0%) | |
| Poor fill | 1 (4%) | 1 (6%) | 0 (0%) | |
| Urates | 1 (4%) | 1 (6%) | 0 (0%) | |
| Liver lesions | 1 (4%) | 0 (0%) | 1 (11%) | |
| Variables |
Total (n = 24) No. (%) |
EA (n = 15) No. (%) |
NI (n = 9) No. (%) |
P value |
| Sites of sample bird utilised for spironucleosis diagnosis | ||||
| Caecum | 10 (42%) | 7 (47%) | 3 (33%) | 0.36 |
| Duodenum | 7 (29%) | 5 (33%) | 2 (22%) | |
| Distal small intestine | 2 (8%) | 0 (0%) | 2 (22%) | |
| Small intestine | 2 (8%) | 1 (7%) | 1 (11%) | |
| Mid small intestine | 1 (4%) | 1 (7%) | 0 (0%) | |
| Large intestine | 1 (4%) | 1 (7%) | 0 (0%) | |
| Rectum | 1 (4%) | 0 (0%) | 1 (11%) | |
| Variables |
Total (n = 46) No. (%) |
EA (n = 26) No. (%) |
NI (n = 20) No. (%) |
P value |
| Diagnostic techniques described for spironucleosis diagnosis | ||||
| Mucosal scrapes | 7 (15%) | 4 (15%) | 3 (15%) | 0.38 |
| Lumen contents | 6 (13%) | 5 (19%) | 1 (5%) | |
| Lumen contents and mucosal scrapes | 2 (4%) | 2 (8%) | 0 (0%) | |
| 50x Magnification | 1 (2%) | 0 (0%) | 1 (5%) | |
| 40x Magnification | 5 (11%) | 3 (12%) | 2 (10%) | |
| 25x Magnification | 2 (4%) | 1 (4%) | 1 (5%) | |
| 20-40x Magnification | 1 (2%) | 1 (4%) | 0 (0%) | |
| High magnification | 1 (2%) | 1 (4%) | 0 (0%) | |
| Medium magnification | 1 (2%) | 0 (0%) | 1 (5%) | |
| Low magnification | 1 (2%) | 1 (4%) | 0 (0%) | |
| Sample diluted | 4 (9%) | 1 (4%) | 3 (15%) | |
| Sample diluted with iodine | 1 (2%) | 1 (4%) | 0 (0%) | |
| Coverslip | 6 (13%) | 4 (15%) | 2 (10%) | |
| Coverslip suspended | 1 (2%) | 0 (0%) | 1 (5%) | |
| Warmed saline | 3 (7%) | 0 (0%) | 3 (15%) | |
| Slide inverted | 1 (2%) | 0 (0%) | 1 (5%) | |
| Rinse off lumen contents | 1 (2%) | 1 (4%) | 0 (0%) | |
| Scalpel blade scrape | 2 (4%) | 1 (4%) | 1 (5%) | |
| Variables |
Total (n = 16) No. (%) |
EA (n = 12) No. (%) |
NI (n = 4) No. (%) |
P value |
| Most crucial factor of a positive result | ||||
| Motile protozoa | 11 (69%) | 7 (58%) | 4 (100%) | 0.73 |
| Large number of protozoa | 3 (19%) | 3 (25%) | 0 (0%) | |
| History | 1 (6%) | 1 (8%) | 0 (0%) | |
| Gross examination | 1 (6%) | 1 (8%) | 0 (0%) | |
| Variables |
Total (n = 31) No. (%) |
EA (n = 19) No. (%) |
NI (n = 12) No. (%) |
P value |
| Morphological appearance of Spironucleus | ||||
| Small | 6 (19%) | 4 (21%) | 2 (17%) | 0.86 |
| Motile | 8 (26%) | 5 (26%) | 3 (25%) | |
| Flagellated | 6 (19%) | 2 (11%) | 4 (33%) | |
| Faster than Trichomonas | 1 (3%) | 1 (5%) | 0 (0%) | |
| Smaller than Trichomonas | 2 (7%) | 2 (11%) | 0 (0%) | |
| Transparent | 1 (3%) | 1 (5%) | 0 (0%) | |
| Oval shaped | 2 (7%) | 1 (5%) | 1 (8%) | |
| Spindle shaped | 2 (7%) | 1 (5%) | 1 (8%) | |
| Circular shaped | 1 (3%) | 0 (0%) | 1 (8%) | |
| Drop shaped | 1 (3%) | 1 (5%) | 0 (0%) | |
| Maggot shaped | 1 (3%) | 1 (5%) | 0 (0%) | |
| Variables |
Total (n = 11) No. (%) |
EA (n = 7) No. (%) |
NI (n = 4) No. (%) |
P value |
| Utilisation of Faeces for Spironucleosis Diagnosis | ||||
| Faeces can be utilised | 3 (27%) | 2 (29%) | 1 (25%) | 0.73 |
| Faeces cannot be utilised | 6 (55%) | 3 (43%) | 3 (75%) | |
| Unknown | 2 (18%) | 2 (29%) | 0 (0%) | |
| Differentiation of Spironucleus from other protozoa | ||||
| Relatively easy to differentiate | 2 (18%) | 2 (29%) | 0 (0%) | 0.49 |
| Somewhat difficult to differentiate | 0 (0%) | 0 (0%) | 0 (0%) | |
| Difficult to differentiate | 9 (82%) | 5 (71%) | 4 (100%) | |
| No. of positive samples needed to confirm infection in an individual bird | ||||
| One | 10 (91%) | 6 (86%) | 4 (100%) | 1.0 |
| Two | 1 (9%) | 1 (14%) | 0 (0%) | |
| No. of infected birds needed to confirm Spironucleus in a flock | ||||
| One | 7 (64%) | 3 (43%) | 4 (100%) | 0.53 |
| Two | 1 (9%) | 1 (14%) | 0 (0%) | |
| Three | 1 (9%) | 1 (14%) | 0 (0%) | |
| Other | 2 (18%) | 2 (29%) | 0 (0%) | |
| Ability to quantify Spironucleus infection levels | ||||
| Possible | 4 (36%) | 0 (0%) | 4 (100%) | 0.003 |
| Impossible | 6 (55%) | 6 (86%) | 0 (0%) | |
| Unknown | 1 (9%) | 1 (14%) | 0 (0%) | |
| Reliance on stated method of Spironucleus diagnosis | ||||
| Always rely on stated method | 11 (100%) | 7 (100%) | 4 (100%) | 1.0 |
| Gross post-mortem findings sufficient | 0 (0%) | 0 (0%) | 0 (0%) | |
| Knowledge of other methods used for spironucleosis diagnosis | ||||
| Other methods known | 1 (9%) | 0 (0%) | 1 (25%) | 0.36 |
| None known | 10 (91%) | 7 (100%) | 3 (75%) | |
| Reproducibility of diagnostic method in general practice | ||||
| Replicable | 11 (100%) | 7 (100%) | 4 (100%) | 1.0 |
| Non-Replicable | 0 (0%) | 0 (0%) | 0 (0%) | |
| Variables |
Total (n = 12) No. (%) |
EA (n = 7) No. (%) |
NI (n = 5) No. (%) |
P value |
| Opinion on spironucleosis diagnosis in general practice | ||||
| Carried out | 2 (17%) | 2 (29%) | 0 (0%) | 0.72 |
| Never carried out | 8 (67%) | 4 (57%) | 4 (80%) | |
| Unknown | 2 (17%) | 1 (14%) | 1 (20%) | |
| Difference in spironucleosis diagnosis between regions | ||||
| Does differ | 2 (17%) | 0 (0%) | 2 (40%) | 0.15 |
| Does not differ | 0 (0%) | 0 (0%) | 0 (0%) | |
| Unknown | 10 (83%) | 7 (100%) | 3 (60%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



