
Submitted:
02 December 2023
Posted:
04 December 2023
You are already at the latest version
Abstract
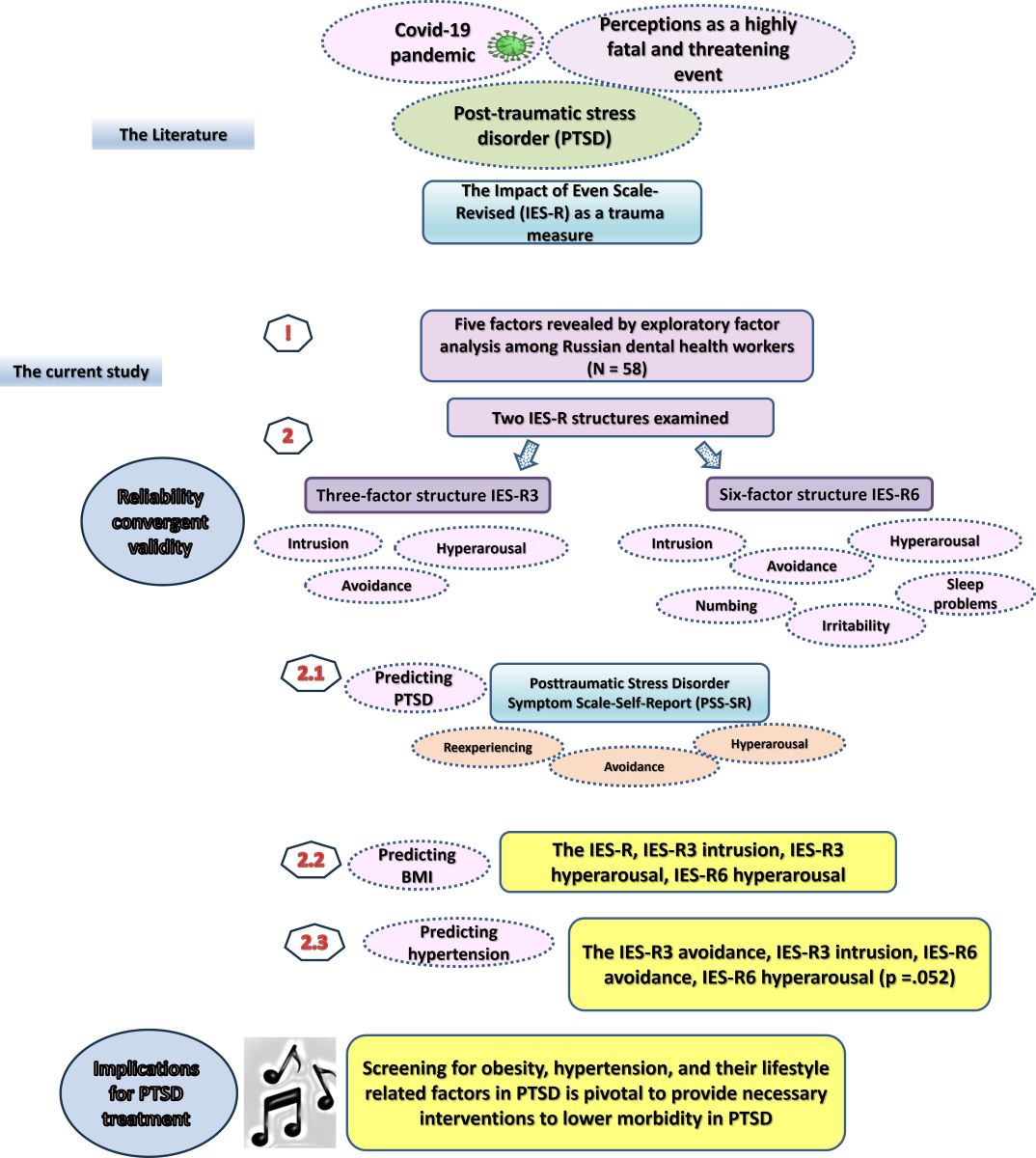
Posttraumatic stress disorder (PTSD) and/or specific PTSD symptoms may evoke disordered eating and unhealthy lifestyles, resulting in adverse cardiometabolic events (e.g., hypertension and obesity) in certain groups, which may implicate the treatment of this complex condition. The diagnostic criteria of PTSD have lately expanded beyond the three common symptoms (intrusion, avoidance, and hyperarousal). Simultaneously, four-, five-, and six-dimensional structures of the Impact of Event Scale-Revised (IES-R), a popular PTSD measure, seem to be more robust than the original three-dimension structure. Within the context of COVID-19, this instrumental study used a convenience sample of 58 dental healthcare workers (HCWs) from Russia (mean age = 44.1±12.2 years, 82.8% females) to examine the criterion and predictive validity of two IES-R structures: the IES-R3 and the IES-R6 (with the added symptoms of numbing, sleep disturbance, and irritability). The subscales of the two IES-R structures expressed good internal consistency, strong correlations with the PTSD Symptom Scale (PSS), hypertension diagnosis, and high body mass index (BMI). In receiver-operating characteristic (ROC) curve analysis, all IES-R models perfectly predicted the PSS (all area under the curve (AUC) >0.9, p values <0.001). The IES-R, both hyperarousal subscales, and the IES-R3 intrusion subscale significantly predicted high BMI. Both avoidance subscales and the IES-R3 intrusion subscale, not the IES-R, significantly predicted hypertension. In conclusion, both IES-R structures can reliably measure PTSD symptoms. The IES-R, hyperarousal, and intrusion may be credible criterion variables for predicting high BMI within PTSD while the intrusion and avoidance subscales may reflect the cardiovascular consequences associated with PTSD more reliably than the IES-R itself. The IES-R subscales may predict cardiometabolic adversities in PTSD, signifying a need for proper assessment of lifestyle and the application of dietary and exercise interventions in order to lower physical morbidity in PTSD. Replicating the study in larger samples, which comprise different physical and mental conditions from heterogenous cultural contexts is pivotal to validate the results (e.g., in specific groups such as those with confirmed traumatic exposure and comorbid mood dysfunction).
Keywords:
Impact of Event Scale-Revised/IES-R
; cutoff score/cutoff point
; three factors/six factors/dimensions
; receiver operator curve (ROC)
; cardiometabolic* /hypertension
; obesity/ high body mass index
; dental healthcare workers
1. Introduction
Posttraumatic stress disorder (PTSD) may develop in individuals witnessing direct or threatened exposure to traumatic events such as terrorist attacks, war/combat, rape, etc. [1,2]. PTSD main symptoms include intrusion or rumination, avoidance, and hyperarousal. These symptoms frequently recover in the first month following trauma exposure. However, emotion regulation strategies that involve suppressing rather than modifying trauma-related emotional responses may account for the persistence of PTSD symptoms in certain groups due to persistent activation of the hypothalamic-pituitary-adrenal (HPA) axis [3-5]. Stress-susceptibility in PTSD is noted by increased activity of the anterior pituitary glucocorticoid receptor [6]. Parenthetically, cumulative research shows that PTSD is a systemic stress-related mental disorder, which evokes physiological, behavioral, and psychological responses that are conducive to the development of cardiovascular disorders (CVD) [7,8].
Altered arousal and reactivity—a core component of the current DSM-5-TR diagnostic criteria of PTSD— is an acute sympathetic arousal in the trauma response, which has been described during the Civil War as “soldiers’ heart” [9]. A possible causative effect of PTSD on CVD has been reported in a longitudinal study following 320 normotensive individuals. Developing hypertension significantly correlated with six variables (age, educational level, body mass index (BMI), smoking, diabetes, and PTSD diagnosis). However, in regression analysis, only PTSD diagnosis was significantly associated with incident hypertension (multivariate HR = 1.94; 95% CI 1.11-3.40) [10]. In a case-control study recruiting hypertensive and normotensive individuals from a city enduring war for 25 years—Bukavu in the Democratic Republic of Congo—hypertension was associated with greater exposure to man-made traumas, PTSD, major depressive disorder (MDD), and alcohol use disorder (61 vs. 13%, 36 vs. 7%, 37 vs. 13%, and 23 vs. 4%, respectively, all p values <0.001) [11]. Similarly, PTSD diagnosis and symptom severity in veterans were linked to a 29% increase in hypertension risk independent of MDD or depressive symptom severity, relative to veterans without lifetime diagnoses of either disease. However, MDD comorbidity in PTSD is associated with considerably increased risk to hypertension (66%) [12]. In support of clinical results, a study involving biobank data (N = 36,412) and genome-wide association study (GWAS) summary statistics from publicly available large-scale samples of PTSD and CVD reported significant genetic correlations between PTSD and CVD, which were stronger when summary statistics from CVD and MDD were incorporated. Mendelian randomization analysis revealed a causal link from PTSD to hypertension but not the opposite. The shared PTSD-CVD risk incorporates genetic variants, which are involved in postsynaptic structure, synapse organization, and interleukin-7-mediated signaling pathways [13]. Moreover, PTSD has been associated with several independent loci and single nucleotide polymorphisms in the PARK2 gene. Genetic variants associated with PTSD polygenic risk scores are suggestively associated with PTSD incidence and severity as well as the incidence of metabolic syndrome (obesity, dyslipidemia, and insulin resistance) [14]. A robust positive genetic correlation between PTSD and metabolic syndrome, especially its obesity-related component, is also reported [15].
PTSD patients display increased likelihood for behavioral risk factors for CVD compared with PTSD free individuals. A meta-analysis of 29 studies records 5%, 9%, 31%, and 22% increased risk for the intake of unhealthy diet, physical inactivity, obesity, and smoking among PTSD patients [16]. Such risk factors evoke environmentally activated disease-promoting pathways, which affect all vital systems e.g., gastrointestinal system, central nervous system, and cardiovascular system [7,17,18,19]. Proinflammatory cytokines such as interleukin-1 beta, interleukin-1 receptor, and toll-like receptor are highly expressed in veterans with PTSD as well as integrin-linked kinase. The latter is highly produced in the brain as a compensatory attempt to combat dysregulated hippocampal neurogenesis and memory deficits [20]. The expression of cytokines is commonly high in MDD, which frequently co-occurs with PTSD due to shared biological pathways. Two out of four gene modules associated with PTSD are also associated with MDD: the UBA7, HLA-F, HSPA1B, and RERE genes demonstrate a high probability of a shared causal quantitative trait loci variant with PTSD and MDD GWAS variants [20]. Therefore, comorbid people with PTSD-MDD express increased symptom severity in addition to greater occurrence of hypertension and high BMI [11,12].
Obesity is an inflammatory condition, which is associated with a surge of inflammatory mediators [21,22], which may justify its high occurrence in PTSD. A meta-analysis of 54 studies, 30 of which include 191,948 PTSD patients and 418,690 trauma-exposed or healthy individuals documents a pooled standard mean difference in obesity of 0.41 (95% CI: 0.28-0.54; z = 6.26; p < .001) [23]. Another meta-analysis of 30 studies comprising 589,781 participants reported odds ratio for obesity of 1.55 (95% CI: 1.32-1.82) [24]. Longitudinal studies tentatively note that PTSD may increase BMI, especially in women [23]. This is possibly because of the effect of stress hormones as well as limbic system and prefrontal cortex dysregulations in PTSD, which trigger craving for carbohydrates and ultra-processed food [25,26]. The development of obesity and other aspects of metabolic syndrome in people exposed to severe, life-threatening or traumatic stress is mediated by the physiological response to stress and related behavioral adaptations (under the conditions of high caloric/fat intake). They act through the neuropeptide Y (NPY) and glucocorticoid systems through a mechanism, which involves exaggerated inflammatory response [27]. On the other hand, fatty tissue contributes to the release of cytokines and free radicals, resulting in extensive diffuse cellular damage and greater physical and mental pathogenicity [22,28]. Veterans with PTSD and comorbid obesity display increased likelihood for mental and physical health problems such as MDD, suicidality, nicotine dependence, diabetes, hypertension, insomnia, and migraine relative to veterans with solo PTSD or obesity [29]. PTSD is also a significant predictor of poor attention and processing speed in older adult male veterans with cognitive deficits [30]. This is probably because of its cardiovascular and metabolic consequences. Indeed, obesity and hypertension are reported as key factors in premature mortality as well as devastating and irreversible mental conditions such as dementia [17]. Therefore, it is pivotal to carefully identify PTSD and associated cardiovascular and metabolic effects in people exposed to traumatic events.
Being in close contact with infected COVID-19 patients, frontline healthcare workers (HCWs) have been reported to exhibit a higher prevalence of PTSD than infected patients themselves [31]. This is possibly due to their perceived susceptibility to contracting infection along with vicarious trauma, which may stem from witnessing patients die unexpectedly or endure severe suffering [32]. Those who are females, less experienced, or working in closed units with difficult to manage conditions express the highest levels of trauma and burnout, especially when they lack social support [33,34]. The risk for COVID-19 and related fear of infection are high in dentistry because of its special nature—operating in the mouth entails a risk of exposure to droplets from asymptomatic patients [35]. HCWs hospitalized because of contracting COVID-19 infection are those with advanced age and comorbidities (e.g., diabetes, obesity, hypertension) [36]. Therefore, HCWs with such comorbidities may have higher perceived susceptibility to COVID-19 and consequently be more prone to PTSD, rendering them worthy of an evaluation for PTSD symptomatology.
The Impact of Event Scale-Revised (IES-R) is a famous measure of PTSD, which corresponds to PTSD main criteria (intrusion, avoidance, and arousal) that were plotted in the earlier versions of the Diagnostic and Statistical Manual of Mental Disorders (DSM). In different studies, the IES-R demonstrated various structures ranging from a single dimension to six dimensions (reviewed in [37]). PTSD criteria have been further expanded in the most recent version of the DSM according to the latest research findings [1,2], which may support the credibility of multi-dimensional structures of the IES-R. The six-dimension structure of the IES-R has been reported recently in two Arab samples of healthy adults and psychiatric patients, and it expressed superior construct validity relevant to previously reported structures. Its subscales demonstrated good internal consistency, discriminant validity, convergent validity, and criterion validity, which denotes their usefulness for revealing people with higher levels of distress [37,38]. The concurrent validity of this structure has not been tested yet, with a possibility that its psychometric qualities may considerably vary in a different cultural context. This study expands existing knowledge on the characteristics of the six-dimensional structure of the IES-R in a sample of Russian dental HCWs during the COVID-19 pandemic. As per the existing literature, we hypothesized that the six-dimension structure of the IES-R would strongly correlate with another measure of PTSD same as the three-dimension structure. Both structures would efficiently predict hypertension and high BMI in the sample.
2. Methods
2.1. Design and participants
This instrumental study employed a cross-sectional design recruiting a convenience sample of dental HCWs (N = 58) from two emergency hospitals in Ekaterinburg in the Russian Federation during the period between the 1st and 20th of September 2020. The study included dental frontline HCWs who consented to participate in the study and who were working before January 2020 and continued to work after that. They were excluded if they refused to take part or were on a sick leave or maternity/parental leave [39,40].
Females were a majority (n = 49, 82.8%) with an average age of 44.1±12.2, range = 22-71 years. They had a median work experience (Q1-Q3) of 16.0 (5.0-30.0) years. HCWs in this sample are categorized according to their position into three classes: 1) dental auxiliaries such as dental laboratory technicians, front desk receptionists, and nurse aides (n = 31, 53.5%); 2) dentists with an MD degree (n = 17, 29.3%); and 3) dental assistants, HCWs without an MD degree (n = 10, 17.2%). Data describing the frequency of hypertension, smoking, and BMI are reported in the Results section, (Table 2). We conducted the analysis using data from a public dataset shared under the terms of Creative Common License CC By 4.0 [39]. Ethical approval for the procedure of data collection has been previously granted during meeting # 6 of the Ethics Commission of the Academic Council of the Chelyabinsk State University (Russia) [40], exempting us from attaining an ethical agreement for the current analysis.
2.2. Measures
Posttraumatic Stress Disorder Symptom Scale-Self-Report (PSS-SR) is a valid tool for evaluating PTSD diagnosis and its severity. It comprises 17 items in three subscales, which identify three key PTSD symptoms: reexperiencing (items 1 to 5), avoidance (items 6 to 12), and hyperarousal (items 13 to 17). The respondents rate the items of the PSS-SR on 4-point equal response intervals ranging from 0 (not at all) to 3 (almost always). An optimal cutoff score of 23 of the PSS-SR has been reported for identifying the possibility of a PTSD diagnosis [41]. The reliability of the PSS-SR and its three subscales in the current sample is excellent or good (alpha = 0.92, 0.88, 0.86, and 0.76, respectively).
The Impact of Event Scale-Revised (IES-R) is a 22-item measure of subjective distress level associated with specific traumatic exposure, herein direct exposure to possible COVID-19 infection. It consists of three subscales, herein referred to as IES-R3, which measure intrusion (e.g., intrusive thoughts/feelings/imagery and nightmares: items 1, 2, 3, 6, 9, 14, 16, and 20), avoidance (e.g., avoidance of feelings/situations/ideas: items 5, 7, 8, 11, 12, 13, 17, and 22), and hyperarousal (e.g., anger/irritability and hypervigilance/heightened startle: items 4, 10, 15, 18, 19, and 21) [40]. The six dimension structure of the IES-R, herein referred to as IES-R6, are avoidance (items 5, 8, 11, 17, 22), intrusion (items 1, 3, 6, 9, 20), numbing (e.g., numbing of responsiveness: items 7, 12, 13, 14), hyperarousal (e.g., physical reactions and being on guard: items 16, 18, 19, 21), sleep problems/disturbance (e.g., trouble falling staying asleep, items 2, 15), and irritability/dysphoria (e.g., anger and irritability: items 4, 10) [38]. The respondents rate the items of the IES-R on 5-point equal response intervals ranging from 0 (not at all) to 4 (extremely) [40]. The reliability of the IES-R and its three and six subscales in the current sample is reported in the next section.
2.3. Statistical analysis
Categorical variables were reported as frequency and percentage. Quantitative variables with normal and non-normal distribution were reported as mean ± standard deviation and median (interquartile range: Q1-Q3), respectively. A preliminary investigation of the structure of the IES-R was conducted by exploratory factor analysis (maximum likelihood, direct Oblimin rotation, Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy, and Bartlett’s test of sphericity). The reliability of the IES-R and its subscales were described using coefficient alpha. Item total correlations and subscale correlations with the IES-R were used to describe convergent validity. Concurrent validity was reported by correlating the IES-R and its subscales with the PSS-SR and its subscales. Criterion validity was tested by correlating the IES-R and its subscales with hypertension diagnosis and BMI.
We also ran receiver-operating characteristic (ROC) curve analysis using the two IES-R structures to predict the PSS-SR, hypertension diagnosis, and high BMI. For this test, the IES-R and its subscales were used as continuous variables. In the meantime, the participants were categorized according to reported cutoff of the PSS-SR into two categories (23 or below: no PTSD and above 23: possible PTSD) [41] as well as BMI (below 25: normal weight and 25 or above: overweight/obesity). This test was intended to examine the cutoff scores of the IES-R and its three/six subscales, which might distinguish those with PTSD, hypertension, and high BMI. The diagnostic accuracy of the ROC model corresponds to the values of the Area Under Curve (AUC), the sensitivity and specificity for all possible cut points, and the Youden index—the sum of sensitivity and specificity of the optimal point minus one [5]. The analyses were performed in SPSS version 28, with significance considered at a level below 0.05 in two-tailed tests.
3. Results
EFA analysis revealed that the structure of the IES-R covers five factors with eigenvalues greater than one, which explained 76.0% of the variance (Supplementary materials). Despite the small size of the present sample, the values of the KMO (0.79) and Bartlett’s test (χ2(231) = 1154.61, p < .001), and Bartlett’s test were high sample suggesting sample suitability for EFA. The reliability of the IES-R was excellent (alpha = 0.95) with total item correlations ranging from 0.48 to 0.83 and alpha if item deleted ranging from 0.946 to 0.951. The reliability of the subscales of the IES-R3 and the IES-R6 was very good for the former and ranged from acceptable to very good for the six dimensions (Table 1). The values of item total correlations were evidently high, especially for the six subscales, which suggests adequate convergent validity.
As shown in Table 2, the three and six subscales of the IES-R strongly correlated with the parent scale as well as with each other, denoting good convergent validity. They also strongly correlated with the PSS-SR, and its three subscales, suggesting good concurrent validity as hypothesized. Only the correlation between the irritability dimension and the reexperiencing subscale of the PSS-SR was not significant.
As for tests of criterion validity, neither the PSS-SR nor its subscales correlated with BMI or having a diagnosis of hypertension. The correlations of the IES-R with BMI and hypertension were also non-significant unlike expectations (Table 2). However, having a diagnosis of hypertension significantly correlated with the avoidance and intrusion dimensions the IES-R3 as well as the avoidance, numbing, and hyperarousal dimensions of the IES-R6. BMI expressed significant positive correlations with the intrusion and hyperarousal dimensions of the IES-R3 and the IES-R6. Notably, only the irritability subscale of the IES-R correlated with current smoking while the PSS-SR and its avoidance subscale correlated with this variable.
According to the reported cutoff of the PSS-SR, only two participants can be considered probable cases of PTSD. ROC analysis using the IES-R (at a cutoff of ≥ 39.5) and its three and six subscales to predict the PSS-SR revealed excellent predictivity of the IES-R and its three and six dimensions (all AUC values and AUC 95% CI were above 0.9, see Table 3 for cutoff, Supplementary Figures 1 and 3). Supplementary Figures 2 and 4 show an excellent fit of both models. All the models were significant at the level of 0.001.
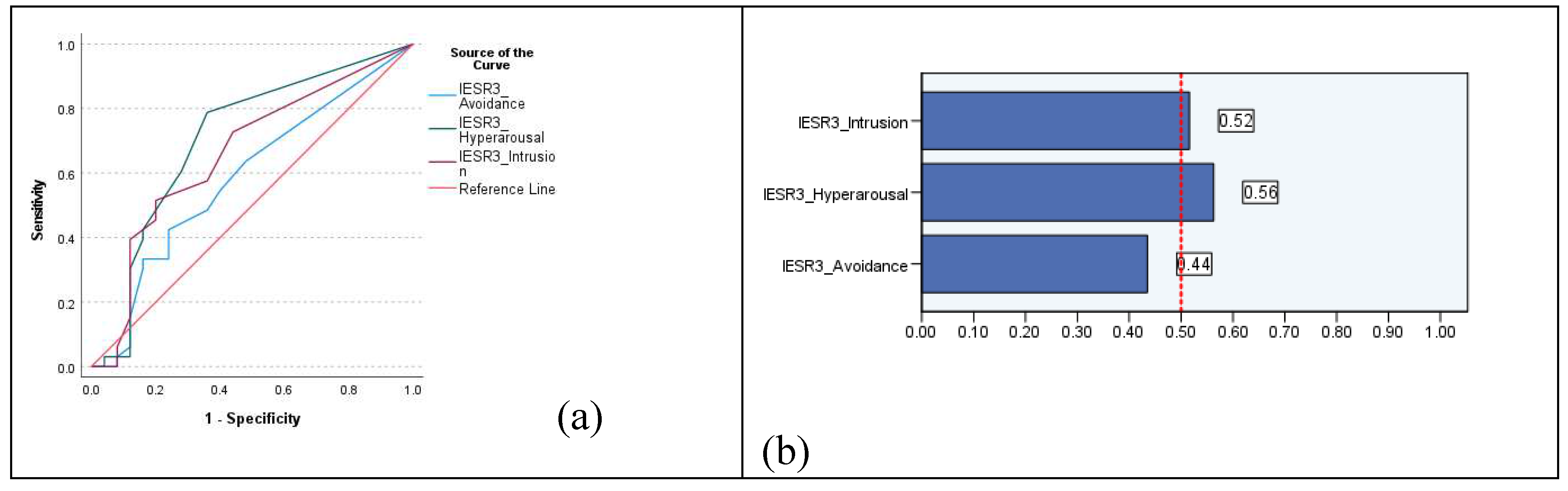
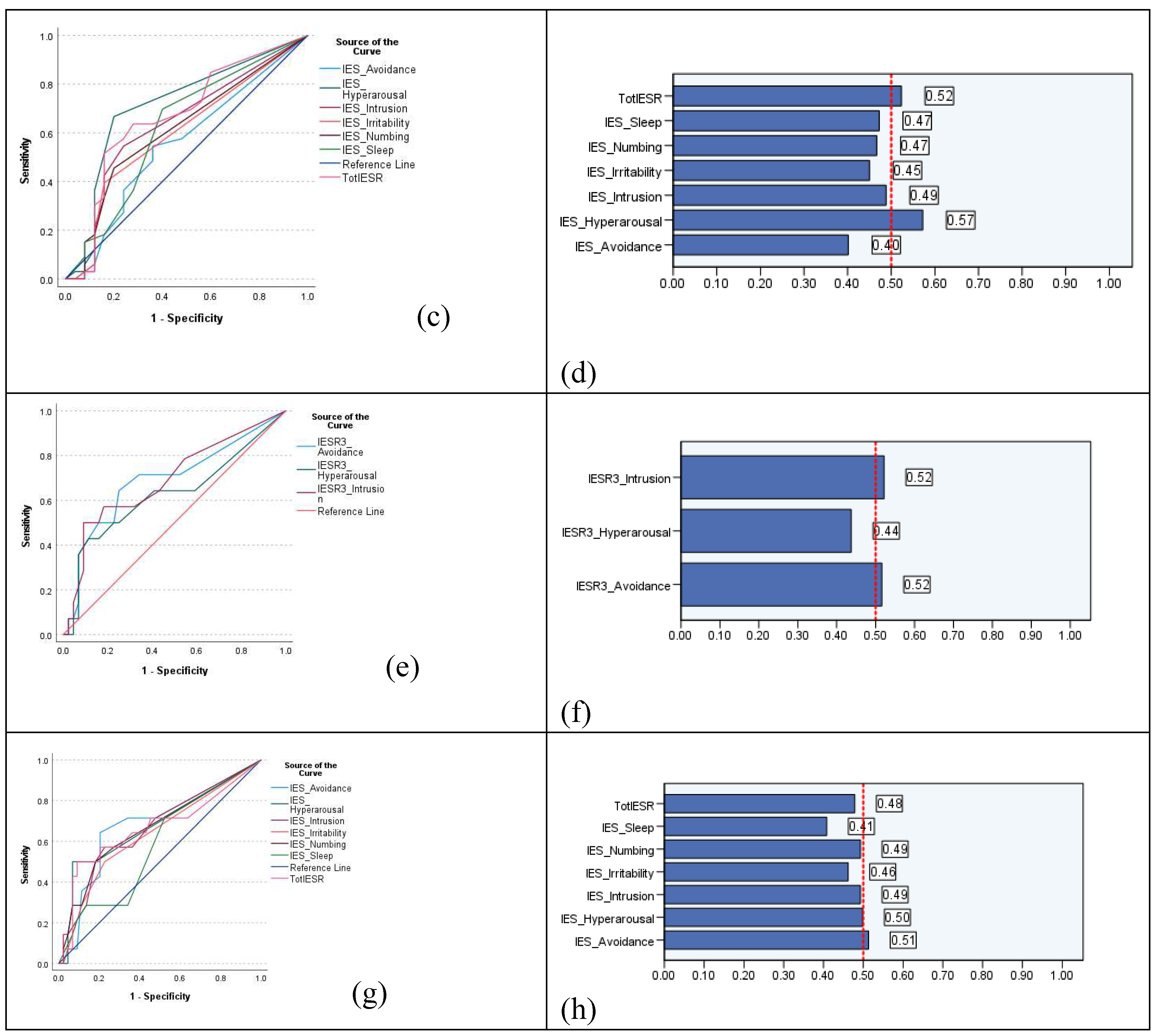
In ROC analysis, the IES-R significantly (p = 0.023) predicted high BMI. The same was true for the IES-R3 intrusion dimension (p = 0.030, Table 3). Both hyperarousal subscales expressed good predictivity for overweight/obesity, with slight variations in specificity and sensitivity between subscales from the three- and six-dimension IES-R structures. The IES-R did not predict hypertension (p = 0.083). However, models involving the avoidance and intrusion subscales of the of the IES-R3 were significant (p = 0.033 and 0.027). Only the model involving the avoidance subscale of the IES-R6 was significant (p = 0.035) while that of hyperarousal was marginally significant (p = 0.052). As shown in Table 3, the values of AUC and Youden index indicate fair predictivity of significant ROC models for BMI and hypertension. Figure 1 denotes marginally acceptable quality of significant models.

Table 2.
Convergent validity, concurrent validity, criterion validity, and descriptive statistics of the three and six subscales of the Impact of Event Scale-Revised (IES-R).
Table 2.
Convergent validity, concurrent validity, criterion validity, and descriptive statistics of the three and six subscales of the Impact of Event Scale-Revised (IES-R).
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. IES-R | -- | ||||||||||||||||
| 2. T-Avoidance | .916** | -- | |||||||||||||||
| 3. T-Intrusion | .903** | .792** | -- | ||||||||||||||
| 4. T-Hyperarousal | .893** | .721** | .768** | -- | |||||||||||||
| 5. S-Avoidance | .870** | .977** | .727** | .668** | -- | ||||||||||||
| 6. S-Intrusion | .861** | .786** | .960** | .706** | .733** | -- | |||||||||||
| 7. S-Numbing | .788** | .783** | .788** | .710** | .680** | .723** | -- | ||||||||||
| 8. S-Hyperarousal | .878** | .804** | .793** | .892** | .764** | .753** | .761** | -- | |||||||||
| 9. S-Sleep | .797** | .604** | .704** | .870** | .560** | .591** | .631** | .693** | -- | ||||||||
| 10. S-Irritability 11. PSS-SR 12. PSS_Avoidance 13. PSS_Arousal 14.PSS_Reexperiencing 15. BMI 16. Hypertension 17. Smoking |
.621** .642** .545** .630** .494** 0.250 0.245 0.034 |
.528** .516** .463** .469** .437** 0.185 .295* -0.074 |
.595** .692** .586** .646** .576** .303* .294* 0.038 |
.684** .573** .414** .644** .393** .276* 0.193 0.040 |
.485** .486** .453** .432** .404** 0.146 .286* -0.049 |
.558** .619** .576** .570** .501** .299* 0.257 0.019 |
.526** .542** .402** .510** .514** 0.240 .293* -0.201 |
.627** .579** .419** .568** .479** .390** .287* 0.037 |
.449** .589** .416** .658** .411** 0.106 0.123 -0.056 |
-- .416** .375** .471** 0.190 0.205 0.253 .279* |
-- .879** .904** .773** 0.009 0.177 .279* |
-- .719** .587** -0.008 0.166 .328* |
-- .564** -0.041 0.076 0.242 |
-- 0.200 0.251 0.125 |
-- .344** -0.116 |
-- -0.151 |
-- |
| Median | 5.0 | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | 0 | 0 | 1.0 | 0 | 6.0 | 1.0 | 1.0 | 1.0 | 26.8▪ | 14• | 10• |
| Q1 – Q3 | 0 – 13.0 | 0 – 6.0 | 0 – 5.3 | 0 – 4.0 | 0 – 5.0 | 0 – 4.0 | 0 – 2.0 | 0 – 2.0 | 0 – 2.0 | 0 – 1.0 | 1 – 11.0 | 0 – 6.3 | 0 – 5.3 | 0 – 4.0 | 5.2▪ | 24.1%• | 17.2%• |
T-: three-dimension structure of the of the IES-R, S-: six-dimension structure of the of the IES-R, PSS-SR: Posttraumatic Stress Disorder Symptom Scale-self reported, BMI: body mass index, ▪: results are reported as mean ± SD, •: results are reported as number and percentage.
Table 3.
Cutoff scores of the Impact of Event Scale-Revised (IES-R) and its subscales, along with goodness-of-fit indices associated with receiver-operating characteristic (ROC) curve analysis in dental healthcare workers.
Table 3.
Cutoff scores of the Impact of Event Scale-Revised (IES-R) and its subscales, along with goodness-of-fit indices associated with receiver-operating characteristic (ROC) curve analysis in dental healthcare workers.
| Sample | AUC | SE | AUC 95% CI | Cutoff | Sensitivity | Specificity | Youden index | |
|---|---|---|---|---|---|---|---|---|
| IES-R | PSS-SR | 1.00 | 0.00 | 0.98 to 1.01 | 39.5 | 1.00 | 1.00 | 1.00 |
| Obesity | 0.67 | 0.08 | 0.52 to 0.82 | 5.5 | 0.64 | 0.72 | 0.36 | |
| Hypertension | 0.66 | 0.10 | 0.48 to 0.85 | 17.5 | 0.50 | 0.91 | 0.41 | |
| IES-R3-Avoidance | PSS-SR | 1.00 | 0.00 | 1.00 to 1.00 | 12.5 | 1.00 | 1.00 | 1.00 |
| Obesity | 0.59 | 0.08 | 0.44 to 0.74 | 3.5 | 0.42 | 0.76 | 0.18 | |
| Hypertension | 0.69 | 0.09 | 0.52 to 0.87 | 3.5 | 0.57 | 0.73 | 0.30 | |
| IES-R3-Intrusion | PSS-SR | 1.00 | 0.00 | 1.00 to 1.00 | 14.5 | 1.00 | 1.00 | 1.00 |
| Obesity | 0.66 | 0.07 | 0.52 to 0.81 | 2.5 | 0.52 | 0.80 | 0.32 | |
| Hypertension | 0.69 | 0.09 | 0.52 to 0.86 | 6.5 | 0.50 | 0.91 | 0.41 | |
| IES-R3-Hyperarousal | PSS-SR | 0.99 | 0.01 | 0.97 to 1.01 | 10.5 | 1.00 | 0.98 | 0.98 |
| Obesity | 0.71 | 0.07 | 0.56 to 0.84 | 0.5 | 0.79 | 0.64 | 0.43 | |
| Hypertension | 0.63 | 0.10 | 0.44 to 0.81 | 6.5 | 0.43 | 0.87 | 0.32 | |
| IES-R6-Avoidance | PSS-SR | 1.00 | 0.008 | 0.98 to 1.01 | 7.5 | 1.00 | 0.98 | 0.98 |
| Obesity | 0.55 | 0.08 | 0.40 to 0.71 | 1.5 | 0.55 | 0.64 | 0.19 | |
| Hypertension | 0.68 | 0.09 | 0.51 to 0.85 | 3.5 | 0.64 | 0.80 | 0.44 | |
| IES-R6-Intrusion | PSS-SR | 1.00 | 0.00 | 1.00 to 1.00 | 8.5 | 1.00 | 1.00 | 1.00 |
| Obesity | 0.64 | 0.08 | 0.49 to 0.79 | 1.5 | 0.55 | 0.76 | 0.31 | |
| Hypertension | 0.66 | 0.09 | 0.49 to 0.84 | 2.5 | 0.57 | 0.77 | 0.34 | |
| IES-R6-Numbing | PSS-SR | 1.00 | 0.00 | 1.00 to 1.00 | 6.5 | 1.00 | 1.00 | 1.00 |
| Obesity | 0.62 | 0.08 | 0.47 to 0.76 | 0.5 | 0.46 | 0.80 | 0.26 | |
| Hypertension | 0.66 | 0.09 | 0.49 to 0.84 | 1.5 | 0.50 | 0.81 | 0.31 | |
| IES-R6-Hyperarousal | PSS-SR | 0.99 | 0.02 | 0.96 to 1.01 | 7.0 | 1.00 | 0.98 | 0.98 |
| Obesity | 0.71 | 0.07 | 0.57 to 0.85 | 0.5 | 0.67 | 0.80 | 0.47 | |
| Hypertension | 0.68 | 0.09 | 0.50 to 0.86 | 3.5 | 0.29 | 0.93 | 0.22 | |
| IES-R6-Sleep | PSS-SR | 0.98 | 0.02 | 0.93 to 1.01 | 5.5 | 1.00 | 0.95 | 0.95 |
| Obesity | 0.62 | 0.08 | 0.47 to 0.77 | 0.5 | 0.70 | 0.60 | 0.30 | |
| Hypertension | 0.58 | 0.09 | 0.41 to 0.75 | 0.5 | 0.71 | 0.48 | 0.19 | |
| IES-R6-Irritability | PSS-SR | 0.99 | 0.02 | 0.95 to 1.02 | 2.5 | 1.00 | 0.95 | 0.95 |
| Obesity | 0.60 | 0.08 | 0.45 to 0.75 | 0.5 | 0.39 | 0.84 | 0.23 | |
| Hypertension | 0.64 | 0.09 | 0.46 to 0.81 | 0.5 | 0.50 | 0.77 | 0.27 |
T-: three-dimension structure of the of the IES-R, S-: six-dimension structure of the of the IES-R, PSS-SR: Posttraumatic Stress Disorder Symptom Scale-self reported.
Figure 1.
Receiver operating characteristic (ROC) curve and quality of models using the scores of the three- and six-dimensions of the Impact of Event Scale-Revised (IES-R) and its subscales to classify dental healthcare workers according to their BMI (a-d) and history of hypertension (e-h).
Figure 1.
Receiver operating characteristic (ROC) curve and quality of models using the scores of the three- and six-dimensions of the Impact of Event Scale-Revised (IES-R) and its subscales to classify dental healthcare workers according to their BMI (a-d) and history of hypertension (e-h).
4. Discussion
Although they have been described more than three decades ago, DSM criteria of PTSD are still being refined based on evolving research findings. Consistent with studies reporting more than three factors of the IES-R in war and fire survivors [42,43], the six-dimension structure of the IES-R has been recently introduced in two Arab samples [37]. It significantly predicted psychological distress in psychiatric patients and healthy adults. The predictivity of the factors of this structure differed considerably, with the highest predictivity reported for hyperarousal and irritability [38]. Until this moment, this structure has not been tested in other groups or cultures. This study suggests the plausibility of this structure in a sample of Russian HCWs in relevance to the COVID-19 pandemic. EFA, which does not impose any constraints, revealed a five-factor structure of the IES-R. However, we refrained from further investigations of the structure of the scale because of the small sample relative to the number of items of the IES-R, which is also non-normally distributed. Nevertheless, further investigations were conducted, and they support the concurrent validity and predictive validity of three- and six-dimension structures of the IES-R
Both structures expressed adequate internal consistency (Table 1), and convergent validity as noted by high values of item total correlations as well as strong correlations of the subscales with the parent scale and the corresponding subscales. They demonstrated excellent concurrent validity through strong positive correlations with the PSS-SR and its subscales (all p values < 0.01)—the only non-significant correlation was that of the irritability subscale of the IES-R6 and the reexperiencing subscale of the PSS-SR. In ROC analysis, the IES-R and its two structures significantly predicted PTSD symptoms measured by the PSS-SR, with all AUC values above 0.9. These correlational and predictive patterns support the concurrent validity of the IES-R.
The correlations of the two IES-R structures with BMI and hypertension indicate that these measures may be considered criterion variables in stressed groups struck by obesity and CVD. In ROC analysis, the IES-R and some of its subscales significantly predicted BMI while only some of its subscales predicted hypertension, suggesting that they are fairly reliable criterion variables. In the meantime, the ROC models using the PSS-SR and its three subscales to predict BMI and hypertension were all non-significant and expressed poor fit, with AUC values ranging from 0.53 to 0.66 (Supplementary Tables 2 and 3, Supplementary Figures 5, 6, 7, and 8). These results suggest usefulness of both IES-R structures relative to the PSS-SR as criterion variables in research and clinical practice investigating PTSD in individuals with metabolic and cardiovascular alterations.
Herein, we attempted to offer a mechanism through which certain IES-R components may relate to metabolic and cardiovascular co-morbidities in PTSD. In our study, hypertension significantly correlated with avoidance and intrusion (IES-R3) as well as with avoidance, numbing and hyperarousal (IES-R6). However, in ROC analysis, avoidance and intrusion predicted hypertension while hyperarousal was a marginal predictor. This result can be interpreted within the light of available literature. Consistent with our results, in an examination of the effect of different PTSD clusters in 1111 military personnel from the UK, avoidance significantly correlated with systolic blood pressure, intrusion correlated with visceral adiposity, and emotional numbing correlated with greater estimated glucose disposal rate while hyperarousal correlated with greater levels of triglycerides. In that study, PTSD clusters did not correlate with the inflammatory marker c-reactive protein, indicating robustness of the cardiometabolic aspect of PTSD [44]. Likewise, PTSD symptomatology and exposure to traumas in hypertensive patients who survive war conditions are associated with more use of expressive suppression and less cognitive reappraisal (p = 0.02), as emotional regulation strategies, than normotensive counterparts [11]. Expressive suppression in individuals exposed to trauma is associated with higher stress-related reactions than cognitive reappraisal [3]. Consistent with our results, expressive suppression significantly correlated with key psychopathologies involving stress-related reactions (PTSD, anxiety, and depression) among trauma-exposed community-dwelling individuals. Rumination partially mediated this association [3]. Examination of neural activity through functional magnetic resonance imaging among combat-related PTSD patients and combat-exposed controls who were asked to reappraise or suppress their emotional response prior to viewing combat-related images revealed reduced medial prefrontal neural activity during reappraisal and increased prefrontal neural activity during image viewing, with increased arousal ratings in all conditions [4]. PTSD re-experiencing is associated with low cerebrospinal fluid levels of the neuroactive steroids, allopregnanolone and its equipotent enantiomer, pregnanolone (collectively termed ALLO)—3-α-reduced biosynthetic derivatives of progesterone. Such alterations are conducive to fear conditioning in PTSD as well as HPA axis and sympathetic system reactivity and the release of cortisol and NPY into visceral fat tissues during severe stress [27]. Therefore, intrusive traumatic thoughts which are not assimilated through the defective use of avoidance/expressive suppression may subsequently give rise to arousal—an indicator of HPA axis dysregulation, which increases the risk for CVD.
In our participants, intrusion and hyperarousal correlated with and predicted high BMI, which is consistent with previous studies [23,24,44]. Obesity in PTSD is associated with disordered eating behaviors (e.g., binge eating) [7]. Experiential avoidance may play a role in this relation [45], which may operate through rumination—similar to that expressed in the stress reaction in PTSD-related CVD risk. In this respect, overweight and obese people exhibit impaired ability to inhibit intrusive thoughts of food and automatic or dominant eating behaviors [46,47], particularly because of their higher levels of poor impulse control (urgency, lack of perseverance, and sensitivity to reward) [46]. Indeed, obesity is also associated with food addiction, which takes the form of obsession with and uncontrolled intake of unhealthy diet (e.g., sugar-rich and ultra processed foods) despite the negative effects of these foods on physical health. The role of intrusive thoughts is pivotal as obesity increases people’s tendency to a range of addictive behaviors including the intake of illicit drugs [18,19]. Thus, avoidance in PTSD may activate rumination and subsequent hyperarousal, resulting in a chronic stress-related behavioral and neurophysiological adaptation through which disordered food intake and increased BMI are promoted [19,27]. The bidirectional roles of cytokines and adipokines in both obesity and PTSD should be also acknowledged [11,12,20].
This study shows that the IES-R functions properly as a free measure of PTSD. It may reflect cardiometabolic complications of PTSD. The findings emphasize the importance of screening for obesity and cardiovascular risk as well as high risk factors for these two conditions (e.g., unhealthy diet and physical inactivity) in people at risk for PTSD. However, this study has many limitations. Selection bias is key limitation as the sample is convenient, sample size was not calculated based on power analysis, and females were a majority. Reporting/recall bias is inherent in self-reported data like in the present study. PTSD as a diagnosis was based on self-reported measures only, with lack of confirmation of Criterion A in the DSM (COVID-19 was not confirmed by the respondents as a direct threat) [38], which casts doubt on the credibility of the results. The absence of some key measures (e.g., mood symptoms) deprived us of the chance of having an in-depth investigation of factors, which may influence the association of PTSD components with cardiometabolic problems in this sample. The cross-sectional design is another limitation. Longitudinal data provide more reliable evidence on the direction of the relationship between PTSD and obesity/hypertension [23]. The contribution of PTSD to unhealthy behaviors conducive to such conditions is reported [16]. However, in our study only smoking was assessed, and it was not predicted by the IES-R or any of its subscales. Therefore, future studies may consider whether the IES-R may reflect more directly related risk factors such as the intake of improper diet and lack of physical activity. Our study only reported overall obesity (BMI) while central/abdominal obesity may exist in people with normal BMI. A meta-analysis reports a prevalence of abdominal obesity in 49.3% (95% CI = 29.7%–69.0%) of PTSD victims [48]. A longitudinal study involving 7.33 year follow up of 33,569 US adults aged >20 years reports a significant association of abdominal obesity with increased risk of CVD-related (heart disease) and all-cause mortality, even among people with normal weight. In addition to weight control, guideline designer should provide recommendations for people to decrease abdominal fat accumulation, in their effort to reduce mortality risk in later life [49]. Therefore, future studies may address the predictivity of PTSD measures for both general and central obesity. Further investigations of the IES-R6 in larger samples of different conditions from various countries are still needed.
Conclusion
The concurrent validity of the two structures of the IES-R is supported by their significant correlations with and perfect predictive capacity for PTSD symptoms measured by the PSS-SR. The IES-R and/or some of its subscales (e.g., intrusion, avoidance, hyperarousal) expressed better predict capacity for high BMI and hypertension than the PSS-SR, which supports their usefulness as criterion variables for identifying PTSD related cardio-metabolic effects. Replication of the findings in different settings, samples, cultural contexts may be necessary.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, Amira Mohammed Ali, Abdulmajeed A. Alkhamees and Tariq Al-Dwaikat; Data curation, Saeed Al-Dossary and Haitham Khatatbeh; Formal analysis, Amira Mohammed Ali, Saeed Al-Dossary and Carlos Laranjeira; Funding acquisition, Abdulmajeed A. Alkhamees; Methodology, Amira Mohammed Al and Annamaria Pakai; Project administration, Amira Mohammed Ali; Resources, Haitham Khatatbeh; Software, Haitham Khatatbeh and Annamaria Pakai; Validation, Abeer Selim and Musheer A. Aljaberi; Visualization, Annamaria Pakai and Tariq Al-Dwaikat; Writing – original draft, Musheer A. Aljaberi, Maha Atout and Abdulmajeed A. Alkhamees; Writing – review & editing, Maha Atout, Carlos Laranjeira, Annamaria Pakai, Abeer Selim and Tariq Al-Dwaikat. All authors have critically revised and approved the final draft of the manuscript.
Funding
None.
Availability of data and materials
The dataset supporting the conclusions of this article is available in Mendeley repository [39], [https://data.mendeley.com/datasets/gdcmgkcf88], and also the datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgement
The authors would like to thank the Deanship of Scientific Research, Qassim University, for funding the publication of this paper.
Competing interests
The authors declare no conflict of interest.
Ethics approval and consent to participate
The data collection protocol was approved during meeting # 6 of the Ethics Commission of the Academic Council of the Chelyabinsk State University (Russia), and all the participants signed an informed consent before taking part in the study [35]. The present study was conducted according to the Declaration of Helsinki. The analysis was conducted using data from a public dataset shared under the terms of Creative Common License CC By 4.0 [39], exempting us from attaining an ethical agreement for the current analysis.
Consent for publication
Not applicable.
References
- Nagarajan, R.; Krishnamoorthy, Y.; Basavarachar, V.; Dakshinamoorthy, R. Prevalence of post-traumatic stress disorder among survivors of severe COVID-19 infections: A systematic review and meta-analysis. J Affect Disord 2022, 299, 52–59. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5-TR. 2022.
- Moore, S.A.; Zoellner, L.A.; Mollenholt, N. Are expressive suppression and cognitive reappraisal associated with stress-related symptoms? Behav Res Ther 2008, 46, 993–1000. [Google Scholar] [CrossRef] [PubMed]
- Butler, O.; Willmund, G.; Gleich, T.; Zimmermann, P.; Lindenberger, U.; Gallinat, J.; Kühn, S. Cognitive Reappraisal and Expressive Suppression of Negative Emotion in Combat-Related Posttraumatic Stress Disorder: A Functional MRI Study. Cognit Ther Res 2019, 43, 236–246. [Google Scholar] [CrossRef]
- Ali, A.M.; Alameri, R.A.; Brooks, T.; Ali, T.S.; Ibrahim, N.; Khatatbeh, H.; Pakai, A.; Alkhamees, A.A.; Al-Dossary, S.A. Cut-off scores of the Depression Anxiety Stress Scale-8: Implications for improving the management of chronic pain. Journal of Clinical Nursing 2023, n/a. [Google Scholar] [CrossRef] [PubMed]
- Hadad, N.A.; Schwendt, M.; Knackstedt, L.A. Hypothalamic-pituitary-adrenal axis activity in post-traumatic stress disorder and cocaine use disorder. Stress 2020, 23, 638–650. [Google Scholar] [CrossRef] [PubMed]
- Rossi, L.; Isnard, P. Obesity and PTSD: A review on this association from childhood to adulthood. Neuropsychiatr Enfance Adolesc 2023. [Google Scholar] [CrossRef]
- Krantz, D.S.; Shank, L.M.; Goodie, J.L. Post-traumatic stress disorder (PTSD) as a systemic disorder: Pathways to cardiovascular disease. Health Psychol 2022, 41, 651–662. [Google Scholar] [CrossRef] [PubMed]
- Ursano, R.J.; Stein, M.B. From Soldier's Heart to Shared Genetic Risk: PTSD and Cardiovascular Disease. Am J Psychiatry 2022, 179, 785–787. [Google Scholar] [CrossRef] [PubMed]
- Mendlowicz, V.; Garcia-Rosa, M.L.; Gekker, M.; Wermelinger, L.; Berger, W.; Luz, M.P.; Pires-Dias, P.R.T.; Marques-Portela, C.; Figueira, I.; Mendlowicz, M.V. Post-traumatic stress disorder as a predictor for incident hypertension: a 3-year retrospective cohort study. Psychol Med 2021, 1–8. [Google Scholar] [CrossRef]
- Bapolisi, A.; Maurage, P.; Pappaccogli, M.; Georges, C.M.G.; Petit, G.; Balola, M.; Cikomola, C.; Bisimwa, G.; Burnier, M.; Persu, A.; et al. Association between post-traumatic stress disorder and hypertension in Congolese exposed to violence: a case-control study. J Hypertens 2022, 40, 685–691. [Google Scholar] [CrossRef]
- Reis, D.J.; Kaizer, A.M.; Kinney, A.R.; Bahraini, N.H.; Forster, J.E.; Brenner, L.A. The unique association of posttraumatic stress disorder with hypertension among veterans: A replication of Kibler et al. (2009) using Bayesian estimation and data from the United States-Veteran Microbiome Project. Psychol Trauma 2023, 15, 131–139. [Google Scholar] [CrossRef]
- Seligowski, A.V.; Misganaw, B.; Duffy, L.A.; Ressler, K.J.; Guffanti, G. Leveraging Large-Scale Genetics of PTSD and Cardiovascular Disease to Demonstrate Robust Shared Risk and Improve Risk Prediction Accuracy. Am J Psychiatry 2022, 179, 814–823. [Google Scholar] [CrossRef] [PubMed]
- Swart, P.C.; van den Heuvel, L.L.; Lewis, C.M.; Seedat, S.; Hemmings, S.M.J. A Genome-Wide Association Study and Polygenic Risk Score Analysis of Posttraumatic Stress Disorder and Metabolic Syndrome in a South African Population. Front Neurosci 2021, 15, 677800. [Google Scholar] [CrossRef] [PubMed]
- Misganaw, B.; Yang, R.; Gautam, A.; Muhie, S.; Mellon, S.H.; Wolkowitz, O.M.; Ressler, K.J.; Doyle, F.J., 3rd; Marmar, C.R.; Jett, M.; et al. The Genetic Basis for the Increased Prevalence of Metabolic Syndrome among Post-Traumatic Stress Disorder Patients. Int J Mol Sci 2022, 23. [Google Scholar] [CrossRef] [PubMed]
- van den Berk-Clark, C.; Secrest, S.; Walls, J.; Hallberg, E.; Lustman, P.J.; Schneider, F.D.; Scherrer, J.F. Association between posttraumatic stress disorder and lack of exercise, poor diet, obesity, and co-occuring smoking: A systematic review and meta-analysis. Health Psychol 2018, 37, 407–416. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Kunugi, H. Royal jelly as an intelligent anti-aging—a focus on cognitive aging and Alzheimer's disease: a review. Antioxidants 2020, 9, E937. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Hendawy, A.O.; Elhay, E.S.A.; Ali, E.M.; Alkhamees, A.A.; Kunugi, H.; Hassan, N.I. The Bergen Facebook Addiction Scale: Its psychometric properties and invariance among women with eating disorders. BMC Women’s Health 2022, 22, 99. [Google Scholar] [CrossRef]
- Ali, A.M.; Hori, H.; Kim, Y.; Kunugi, H. Predictors of nutritional status, depression, internet addiction, Facebook addiction, and tobacco smoking among women with eating disorders in Spain. Frontiers in Psychiatry 2021, 12, 2001. [Google Scholar] [CrossRef]
- Garrett, M.E.; Qin, X.J.; Mehta, D.; Dennis, M.F.; Marx, C.E.; Grant, G.A.; Stein, M.B.; Kimbrel, N.A.; Beckham, J.C.; Hauser, M.A.; et al. Gene Expression Analysis in Three Posttraumatic Stress Disorder Cohorts Implicates Inflammation and Innate Immunity Pathways and Uncovers Shared Genetic Risk With Major Depressive Disorder. Front Neurosci 2021, 15, 678548. [Google Scholar] [CrossRef]
- Ali, A.M.; Kunugi, H. Apitherapy for age-related skeletal muscle dysfunction (sarcopenia): A review on the effects of royal jelly, propolis, and bee pollen. Foods 2020, 9, E1362. [Google Scholar] [CrossRef]
- Ali, A.M.; Kunugi, H. Screening for sarcopenia (physical frailty) in the COVID-19 era. Int J Endocrinol 2021, 2021, 5563960. [Google Scholar] [CrossRef] [PubMed]
- Suliman, S.; Anthonissen, L.; Carr, J.; du Plessis, S.; Emsley, R.; Hemmings, S.M.; Lochner, C.; McGregor, N.; van den Heuvel, L.; Seedat, S. Posttraumatic Stress Disorder, Overweight, and Obesity: A Systematic Review and Meta-analysis. Harv Rev Psychiatry 2016, 24, 271–293. [Google Scholar] [CrossRef] [PubMed]
- Bartoli, F.; Crocamo, C.; Alamia, A.; Amidani, F.; Paggi, E.; Pini, E.; Clerici, M.; Carrà, G. Posttraumatic stress disorder and risk of obesity: systematic review and meta-analysis. J Clin Psychiatry 2015, 76, e1253–1261. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Nepal, B.; Moon, C.S.; Chabenne, A.; Khogali, A.; Ojo, C.; Hong, E.; Gaudet, R.; Sayed-Ahmad, A.; Jacob, A. Psychology of craving. Open Journal of Medical Psychology 2014, 3, 42106. [Google Scholar] [CrossRef]
- Carmassi, C.; Antonio Bertelloni, C.; Massimetti, G.; Miniati, M.; Stratta, P.; Rossi, A.; Dell׳Osso, L. Impact of DSM-5 PTSD and gender on impaired eating behaviors in 512 Italian earthquake survivors. Psychiatry Res 2015, 225, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Rasmusson, A.M.; Schnurr, P.P.; Zukowska, Z.; Scioli, E.; Forman, D.E. Adaptation to extreme stress: post-traumatic stress disorder, neuropeptide Y and metabolic syndrome. Exp Biol Med (Maywood) 2010, 235, 1150–1162. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Kunugi, H. Physical frailty/sarcopenia as a key predisposing factor to coronavirus disease 2019 (COVID-19) and its complications in older adults. BioMed 2021, 1, 11–40. [Google Scholar] [CrossRef]
- Stefanovics, E.A.; Potenza, M.N.; Pietrzak, R.H. PTSD and obesity in U.S. military veterans: Prevalence, health burden, and suicidality. Psychiatry Res 2020, 291, 113242. [Google Scholar] [CrossRef] [PubMed]
- Noland, M.D.W.; Paolillo, E.W.; Noda, A.; Lazzeroni, L.C.; Holty, J.C.; Kuschner, W.G.; Yesavage, J.; Kinoshita, L.M. Impact of PTSD and Obstructive Sleep Apnea on Cognition in Older Adult Veterans. J Geriatr Psychiatry Neurol 2023, 8919887221149132. [Google Scholar] [CrossRef]
- Yuan, K.; Gong, Y.-M.; Liu, L.; Sun, Y.-K.; Tian, S.-S.; Wang, Y.-J.; Zhong, Y.; Zhang, A.-Y.; Su, S.-Z.; Liu, X.-X.; et al. Prevalence of posttraumatic stress disorder after infectious disease pandemics in the twenty-first century, including COVID-19: a meta-analysis and systematic review. Mol Psychiatry 2021, 26, 4982–4998. [Google Scholar] [CrossRef]
- Ali, A.M.; Alkhamees, A.A.; Elhay, E.S.A.; Taha, S.M.; Hendawy, A.O. COVID-19-related psychological trauma and psychological distress among community-dwelling psychiatric patients: people struck by depression and sleep disorders endure the greatest burden. Frontiers in Public Health 2022. [Google Scholar] [CrossRef]
- d’Ettorre, G.; Ceccarelli, G.; Santinelli, L.; Vassalini, P.; Innocenti, G.P.; Alessandri, F.; Koukopoulos, A.E.; Russo, A.; d’Ettorre, G.; Tarsitani, L. Post-Traumatic Stress Symptoms in Healthcare Workers Dealing with the COVID-19 Pandemic: A Systematic Review. International Journal of Environmental Research and Public Health 2021, 18, 601. [Google Scholar] [CrossRef] [PubMed]
- Khatatbeh, H.; Al-Dwaikat, T.; Alfatafta, H.; Ali, A.M.; Pakai, A. Burnout, quality of life and perceived patient adverse events among paediatric nurses during the COVID-19 pandemic. J Clin Nurs 2022. [Google Scholar] [CrossRef] [PubMed]
- Lin, G.S.S.; Lee, H.Y.; Leong, J.Z.; Sulaiman, M.M.; Loo, W.F.; Tan, W.W. COVID-19 vaccination acceptance among dental students and dental practitioners: A systematic review and meta-analysis. PLoS One 2022, 17, e0267354. [Google Scholar] [CrossRef] [PubMed]
- Robles-Pérez, E.; González-Díaz, B.; Miranda-García, M.; Borja-Aburto, V.H. Infection and death by COVID-19 in a cohort of healthcare workers in Mexico. Scand J Work Environ Health 2021, 47, 349–355. [Google Scholar] [CrossRef]
- Ali, A.M.; Al-Amer, R.; Kunugi, H.; Stănculescu, E.; Taha, S.M.; Saleh, M.Y.; Alkhamees, A.A.; Hendawy, A.O. The Arabic version of the Impact of Event Scale – Revised: Psychometric evaluation in psychiatric patients and the general public within the context of COVID-19 outbreak and quarantine as collective traumatic events. Journal of Personalized Medicine 2022, 12, 681. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.M.; Al-Dossary, S.A.; Almarwani, A.M.; Atout, M.; Al-Amer, R.; Alkhamees, A.A. The Impact of Event Scale – Revised: Examining its cutoff scores among Arab psychiatric patients and healthy adults within the context of COVID-19 as a collective traumatic event. Healthcare 2023, 11, 892. [Google Scholar] [CrossRef] [PubMed]
- Sarapultsev, A.; Zolotareva, A.; Berdugina, O. BMI and PTSD among HCWs. Mendeley Data 2021, V1. [Google Scholar] [CrossRef]
- Sarapultseva, M.; Zolotareva, A.; Kritsky, I.; Nasretdinova, N.y.; Sarapultsev, A. Psychological Distress and Post-Traumatic Symptomatology among Dental Healthcare Workers in Russia: Results of a Pilot Study. International Journal of Environmental Research and Public Health 2021, 18, 708. [Google Scholar] [CrossRef]
- Foa, E.B.; McLean, C.P.; Zang, Y.; Zhong, J.; Rauch, S.; Porter, K.; Knowles, K.; Powers, M.B.; Kauffman, B.Y. Psychometric properties of the Posttraumatic Stress Disorder Symptom Scale Interview for DSM-5 (PSSI-5). Psychol Assess 2016, 28, 1159–1165. [Google Scholar] [CrossRef]
- Gargurevich, R.; Luyten, P.; Fils, J.F.; Corveleyn, J. Factor structure of the Impact of Event Scale-Revised in two different Peruvian samples. Depress Anxiety 2009, 26, E91–98. [Google Scholar] [CrossRef]
- Morina, N.; Böhme, H.F.; Ajdukovic, D.; Bogic, M.; Franciskovic, T.; Galeazzi, G.M.; Kucukalic, A.; Lecic-Tosevski, D.; Popovski, M.; Schützwohl, M.; et al. The structure of post-traumatic stress symptoms in survivors of war: confirmatory factor analyses of the Impact of Event Scale--revised. J Anxiety Disord 2010, 24, 606–611. [Google Scholar] [CrossRef] [PubMed]
- Dyball, D.; Bennett, A.N.; Schofield, S.; Cullinan, P.; Boos, C.J.; Bull, A.M.J.; Stevelink, S.A.M.; Fear, N.T. The underlying mechanisms by which PTSD symptoms are associated with cardiovascular health in male UK military personnel: The ADVANCE cohort study. Journal of Psychiatric Research 2023, 159, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Wooldridge, J.S.; Herbert, M.S.; Dochat, C.; Afari, N. Understanding relationships between posttraumatic stress disorder symptoms, binge-eating symptoms, and obesity-related quality of life: the role of experiential avoidance. Eating Disorders 2021, 29, 260–275. [Google Scholar] [CrossRef] [PubMed]
- Mobbs, O.; Crépin, C.; Thiéry, C.; Golay, A.; Van der Linden, M. Obesity and the four facets of impulsivity. Patient Educ Couns 2010, 79, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Davidson, T.L.; Ramirez, E.; Kwarteng, E.A.; Djan, K.G.; Faulkner, L.M.; Parker, M.N.; Yang, S.B.; Zenno, A.; Kelly, N.R.; Shank, L.M.; et al. Retrieval-induced forgetting in children and adolescents with and without obesity. Int J Obes (Lond) 2022, 46, 851–858. [Google Scholar] [CrossRef]
- Rosenbaum, S.; Stubbs, B.; Ward, P.B.; Steel, Z.; Lederman, O.; Vancampfort, D. The prevalence and risk of metabolic syndrome and its components among people with posttraumatic stress disorder: a systematic review and meta-analysis. Metabolism 2015, 64, 926–933. [Google Scholar] [CrossRef]
- Huai, P.; Liu, J.; Ye, X.; Li, W.Q. Association of Central Obesity With All Cause and Cause-Specific Mortality in US Adults: A Prospective Cohort Study. Front Cardiovasc Med 2022, 9, 816144. [Google Scholar] [CrossRef]
Table 1.
Internal consistency of the Impact of Event Scale-Revised (IES-R) and its three and six subscales.
Table 1.
Internal consistency of the Impact of Event Scale-Revised (IES-R) and its three and six subscales.
| Alpha | Alpha if item deleted | Item total correlations | |
|---|---|---|---|
| IES-R | 0.95 | 0.946 to 0.951 | 0.48 to 0.83 |
| T-Avoidance | 0.84 | 0.81 to 0.84 | 0.46 to 0.64 |
| T-Intrusion | 0.88 | 0.85 to 0.88 | 0.46 to 0.85 |
| T-Hyperarousal | 0.86 | 0.82 to 0.88 | 0.39 to 0.81 |
| S-Avoidance | 0.75 | 0.67 to 0.72 | 0.46 to 0.59 |
| S-Intrusion | 0.81 | 0.72 to 0.80 | 0.47 to 0.77 |
| S-Numbing | 0.83 | 0.72 to 0.87 | 0.48 to 0.80 |
| S-Hyperarousal | 0.88 | 0.67 to 0.72 | 0.81 to 0.87 |
| S-Sleep | 0.84 | - | 0.72 |
| S-Irritability | 0.69 | - | 0.52 |
T-: three-dimension structure of the of the IES-R, S-: six-dimension structure of the of the IES-R.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



