
Submitted:
17 November 2023
Posted:
17 November 2023
You are already at the latest version
Abstract
Background: Poisoning is a growing public problem that has shown increased prevalence in many countries worldwide, contributing to increased costs and mortalities. A lack of or insufficient information regarding the circumstances, chemicals, drugs and people at risk due to imperfect reporting system is regarded as a barrier to successful poisoning prevention and intervention efforts. In Saudi Arabia, poisoning cases are monitored at the central level in the Ministry of Health, with meticulous follow-up of cases across country areas through public health departments. The current study's objective was to describe the poisoning notification and reporting system in Makkah.Subjects and methods: All reports of chemical and drug overdose poisoning delivered to the environmental health and occupational safety department in Makkah Almukarramah over two years (2018-2019) were reviewed, together with verification of all systems, rules and guidelines organizing the performance of the department.Results: The total number of cases reported in 2018 was 209 cases, while it reached 42 cases in 2019. The overwhelming majority of the cases were Saudi (91.6%), with a slight predominance of males (57.4%) over females (42.6%). Generally, almost two-thirds of the cases occurred in children below 13 years (61.4%), most of the poisoning cases resulted from drug overdose (63.3%), while 34.7% were chemical poisoning. The most common drug poisoning was attributed to analgesics followed by antiepileptics, antihypertensive drugs, antipsychotics and antimicrobials, while cleaning and detergent agents were the most commonly poisoned chemicals. The majority of these agents were taken by the oral route. Children's chemical poisoning was significantly higher than that in older age groups (p<0.05). All intentional poisoning occurred in adults; the great majority of them (88.9%) used drug overdosing rather than chemical substances.Conclusion and recommendations: The current study results are consistent with most of the previous studies carried out in different regions in Saudi Arabia. Reviewing the performance and adherence of the “Environmental Health and Occupational Safety Department” to the guidelines and instruction regulating monitoring, notification and reporting of poison cases are satisfactory and the poisoning surveillance system is effective. Further in-depth studies are needed to elaborate other socioeconomic and demographic factors associated with chemical and drug overdose poisoning. Public health plans, policies and legislations should be implemented to reduce these factors, including prohibition over-the-counter pharmaceutical sales, selling the possibly harmful substances in kid-proof bottles and additional stringent rules governing chemical sale and storage. Intensive supervision of children is needed. Suicidal poisoning patients should seek psychiatric help to limit the possibility of attempting suicide again in the future. Furthermore, efforts are needed to plan and implement health education programs and campaigns about the factors proven in the current study to be significantly related to chemical and drug overdose poisoning to raise public knowledge about exposure to chemicals and its consequences. Popular communication media, commercial malls, road ads, learning institutions and workplaces can be used to deliver health education campaigns and programs. Advice on how to store chemicals safely and how to keep kids safe should be focused on during such programs.
Keywords:
reporting
; system
; chemical
; drug overdose
; poisoning
; surveillance
; Makkah Almukarramah
; Saudi Arabia
1. Introduction:
The World Health Organization (WHO) states that “poisoning occurs when people eat, drink, inject, breathe or touch enough of a substance (poison) to cause illness or death”; some can cause harm immediately, while others might develop over a long time. Additionally, some poisons could induce harm in minimal doses, while other types become harmful only in large enough doses. [1]
Poisoning is still a major public health issue; it is estimated that more than 340,000 people die from accidental poisoning worldwide,[1] and it is the second leading cause of morbidity after traffic accidents.[2] Moreover, poisoning is responsible for a global loss of approximately 7.4 million of the time lived with disability and the time lost due to premature mortality (healthy life years or DALYs), and approximately one million suicides happen each year, most of which are related to chemical poisoning.[1]
The Economic Co-operation and Development Organization (ECDO), in 2014, addressed the growing use of chemical products in daily life over the past few decades, for example, insecticides and fertilizers, with increased exposure of human beings and an increased likelihood of poisoning. Therefore, limiting availability and access to highly toxic chemicals are essential for reducing the risk of poisoning. [3]
In Saudi Arabia, the poison center at King Fahd healthcare city was one of the earliest toxic control units in the Saudi Arabian Kingdom. In 2012, an improved project proposal was submitted to create the unit, which would handle all poison patients and toxicological consults at KFHC. An organizational order was issued in 2014 to set up a new unit to become one of the units within the emergency care department. For toxicological and poisoned patients, the unit's medical facilities can provide quick and professional medical guidance and support through the telephone. They additionally support emergency doctors in the care and diagnosis of toxicological and poisoned patients over 24 hours a day throughout the year.[4]
1.1. Background:
Formally, the reporting system for drug and chemical poisoning cases started in 1996, where cases were reported using a report form for each individual case and sent from the directorate of health affairs to the General Administration of Occupational and Environmental Health in the Ministry of Health, where a vertical program for chemical safety was committed to manipulating all the reports received from various regions in Saudi Arabia.
In 2005, with the increased number of received reports, two major modifications were made for the reporting system. The first was the updating of the reporting forms, which became more informative by adding important and critical variables to provide a more comprehensive view of the cases and enable epidemiologists to obtain better analysis and interpretation of the epidemiological situation of chemical and drug hazards. The second modification was made on the timeliness of the reports, which also incorporated the hierarchy for the flow of the reports, from discovery of the case until its final destination at the MOH.
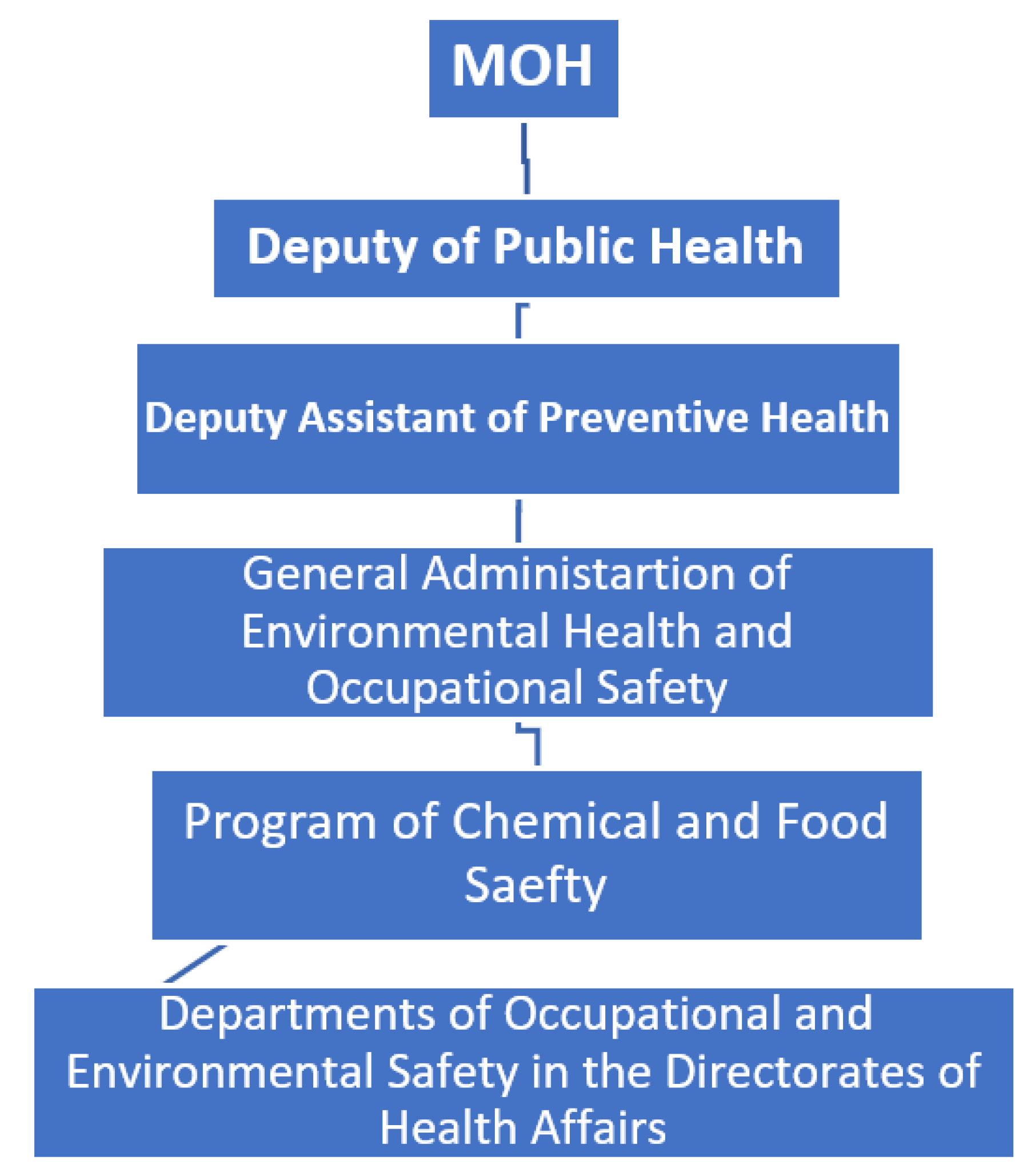
Accordingly, over time, the hierarchy of notification of poisoning cases was clearly established, together with detailed guidelines for the responsibilities of sharing partners in the process of reporting, as displayed in the following scheme:
Scheme.
for the organizational skeleton of the program of chemical and food safety in the Saudi Arabian Kingdom.
Scheme.
for the organizational skeleton of the program of chemical and food safety in the Saudi Arabian Kingdom.
- Collaboration with the relevant sectors.
- Risk assessment for chemical substances.
- Review for the laws and guidelines legislating safe dealing with the chemical substances.
- Continuous monitoring for the reporting system.
- Representing the Ministry of Health in meetings with pertinent sectors in all matters related to chemical and drug poisoning.
- Ensure the compliance of different sectors with the regulations of the drug and chemical safety program.
- Dissemination of the decrees governing adherence to the regulations of the program.
- Reviewing, monitoring and follow up for all the cases of chemical and drug poisoning occurring all over the Kingdom.
- Receiving all reports and notifications from all directorates in the Kingdom.
- Confirm uploading all relevant data received from the regions on the Health Electronic Surveillance Network (HESN) designated for this purpose.
- Immediate to the Deputy of Public Health about mortality cases together with the laboratory and the forensic reports.
- Preparing the annual statistics about all chemical and drug poisoning occur all over the Kingdom.
- Collaboration with other sectors in conducting field inspection on the shops dealing with chemical substances and insecticides and companies specialized in insect and rodent control.
- Training and continuous education.
- Training of all employees serving in the program about Health Electronic Surveillance Network (HESN).
- Training workers in the regions about surveillance of the chemical and drug poisoning and documentation of the data either on paper or electronic programs.
- Preparing health education materials disseminated for the regions to increase awareness of the workers as well as the community about risks of chemical and drug poisoning and how to prevent it.
- Prepare and disseminate updated scientific materials to the workers in the regions.
- Regular meetings with coordinators of the regions.
- Regular field visits to health institutes in different regions encourage notification of poison cases.
1.3. Tasks and responsibilities of the regional Departments of Environmental Health and Occupational Safety regarding chemical and drug poisoning:
- Act as a liaison for disseminating the regulations set at the ministerial level to all governmental and private sectors and ensuring adherence to these regulations.
- Monitoring timeliness and accuracy of the reporting system and perform regular supervisory visits to the reporting health institutes in the region.
- Receiving, organizing and saving all reports sent from the hospitals.
- Immediate for any mortalities, cases of group poisoning and cases of methanol or aluminum phosphide poisoning to the central Program of Chemical and Drug safety at the MOH.
- Preparing and submitting a monthly report for all drug and chemical poisoning cases occur in the region to the central program at the MOH.
- Preparing and submitting an annual report for all drug and chemical poisoning cases occur in the region to the central program at the MOH.
- Active participation of the primary health care centers should be ensured in providing health education about protective measures against chemical and drug poisoning accidents.
- Organizing and sharing in training activities regarding awareness about the notification system for chemical and drug poisoning incidents.
1.4. Responsibilities of the notifying health institute:
- On arrival of the case and suspicion of chemical or drug poisoning, the relevant form should be completed by the treating physician and the health inspector.
- The physician is responsible for collecting the appropriate sample from the case (blood, urine, gastric lavage, etc.) depending on the type of poisoning.
- The samples were sent to the laboratory of chemical and forensic poisoning in the region.
-
Notifying the coordinator of the program of chemical and drug safety in the region according to the following time ranges:
- ○
- If the incident occurs in only one case, which is stable, the form should be sent within one week together with the laboratory results.
- ○
- If the incident occurs in a group of cases, notification should be instant to the regional coordinator.
- ○
- Mortalities should be notified at once to the regional coordinator.
- ○
- Additionally, cases of methanol and aluminum phosphide poisoning should be notified immediately to the regional coordinator.
- The notifying health institute should keep forms and reports about the poisoning cases and send copies for the coordinator in the region as well as the primary health care center in the catchment area of the case.
- The health inspector in the institute is responsible for follow-up of the laboratory investigation results conducted in the hospital or any other laboratories.
- A full report about the case and forensic report (in case of mortality) should be sent to the regional coordinator after completing the case.
1.5. Rationale of the study:
The lack of or inadequate information about the circumstances, substances and populations at risk due to imperfect reporting system are considered barriers to the actual prevention of poisoning and effective intervention strategies. As a result, the purpose of this study was to describe the reporting system and the acute poisoning in terms of the demographic features of the patients (i.e., age, gender, education level, etc.) and more frequent toxic substances utilized. The study uses data retrieved from the environmental health department in Makkah Almukarramah representing the period from 2018 until the end of 2019.
1.6. Aim of the study:
This study aims to provide documented background about chemical and drug overdose poisoning in Makkah Almukarramah covering the period 2018 - 2019.
1.7. Objective(s) of the study:
- To describe the notification and reporting system in the environmental health and occupational safety department in the public health directorate in Makkah Almukarramah.
2. Review of Literature:
Chemical poisoning is a growing public problem that has shown increased prevalence in many countries worldwide, contributing both to increased costs and mortalities.[5] Chemical poisoning incidence occurs at varying rates around the world and may vary even within the same country due to disparities in socioeconomic level and other variables.[6]
According to the World Health Organization report about changes in mortality rates attributed to unintentional poisoning from 2000-2016 [Table 1], the overall mortality rate due to unintentional poisoning in Saudi Arabia decreased from 1.3/100,000 in 2000 to 1 in 2005, 0.9 in 2010 and 0.7 in 2016. The same trend of decline is applicable to rates among males, which decreased from 1.5 in 2000 to 0.8 in 2016, and females, which decreased from 1 in 2000 to 0.5/100,000 in 2016.
2.1. International studies:
In India, Ramesha and his colleague in 2009 reviewed the nonchronic poisoning medical records and attended a tertiary hospital's urgent care department, where 136 cases were included; they found that incidence was higher in males (75.4%) than females (24.3), and the age groups 20 to 29 years had the highest prevalence (31.2%), followed by 12 to 19 years (30.2%). Organophosphorus compounds were responsible for a large proportion of cases (36.0%). The overall mortality rate reported was 15.4%. When compared to OPC poisoning, the mortality rate from corrosives was significantly higher. (χ2 = 4.12, P = 0.04.[2]
In Ethiopia, in 2016, Teklimariam and his colleague analyzed the data of poisoning cases presented in a university hospital over two years from 2012 to 2013 and found that out of cases (n=103), females represented 54 (52.4%). “The highest prevalence of poisoning was observed in persons aged 12–20 years (70, 67.96%). The majority of the cases were intentional poisoning (52, 50.5%), and 28, 27.2% of the cases were accidental. The common causes of poisoning were house hold cleansing agents (43, 41.7%), organophosphates (28, 27.2%) and drugs (13, 12.6%). Diarrhea and vomiting (49.5%), altered consciousness (16.5%) and epigastric pain (13.6%) were the common presenting symptoms”.[7]
In South Africa, in 2009, Malangu and Ogunbanjo revised the data of all cases with nonchronic poisoning treated in 8 hospitals; they found that out of a total of 424 cases, females constituted 57.8%, and 17.6 years was their median age. More than half of the poisoning cases (59%) were intentional, and the hazardous substances implicated were “household chemicals (45.7%), modern medicines (17.5%), animal/insect bites (15.8%), agrochemical chemicals (9.7%), food poisoning (5.4%), drugs of abuse (3.3%), traditional medicines (2.4%), and plants (0.2%)”.[8]
2.2. Studies in Saudi Arabia:
In 2010, Al-Barraq and Farahat reviewed the data available at the University Hospital's poisoning center in King Saud University in Riyadh city, Saudi Arabian kingdom, where the study covered 1161 patients. They found that 7.9% of the cases were newborns, 7.2% were between the ages of six and twelve, 32.0% were above the age of twelve, and 52.9% were under the age of five. "The proportion of males exposed to harmful substances was nearly equivalent to that of females.". Oral route poisoning occurred in more than 92% of cases. Drugs were the leading cause of poisoning in 76.7% of patients, followed by domestic chemicals (6.8%). In 25.6% of patients, suicidal ideation was noted. Individuals who arrived at the hospital between 1–3 hours after poisoning, were more than 12 years old and were exposed to more than one poison substance were all significant predictors of attempted suicide, according to multivariate regression analysis.[9]
In Saudi Arabia's western area, Bakhaidar and his colleagues in 2015 reviewed the medical records of cases with drug overdose and chemical poisoning who attended the urgent care unit at King Khalid Hospital in the Ministry of National Guard between 2008 and 2012; there were 129 patients in this study, and they found that the majority of the cases were Saudis (97.7%), and “almost half of them were females (54.3%). Children under 12 years were the most affected age group (44.2%). Drug overdose was the most common cause of poisoning (92.2%). Analgesics and nonsteroidal anti-inflammatory drugs represented the highest percentage of medications used (20.4%)”. Thirty-four incidences of intentional poisoning were documented (26.4%). Patients who attempted suicide were significantly more likely to be female (OR = 7.22, 95% CI = 1.70, 30.62).[6]
In another study conducted in Jeddah in 2017, Alzahrani et al revised the medical records of chemical poisoning cases from 2011 to 2015. They found that there were 994 cases of poisoning by chemicals, with an upward pattern from 2011 to 2013 and a slight decrease in 2014 and 2015. “More than half of the cases involved were males (55%) and children aged less than 5 years (56.6%). Approximately three-fourths of the cases occurred accidentally and through ingestion. The most common poisonous agents were detergents (36.0%). Poisoning with addictive drugs occurred in 13 cases (1.3%). Only 1.1% of cases received a poisoning-specific antidote, and the same percentage died because of poisoning. Sex, age, nationality, the route and the circumstances of the exposure were significantly associated with the type of poisoning (P <.001)”.[10]
In the Al-Qassim region, Moazzam and his colleagues evaluated all documented events of exposure to chemicals reported to the public health department in Al-Qasim province between 1999 and 2003. During the research, they discovered that the patients number grew from 66 to 114.“Mean age of patients was 17.7 years, and over 39% were children aged < or = 5 years. Pesticides were the most common chemical involved; paracetamol and other analgesics were also frequently reported. The oral route was the most frequent route, and the solid medicine form was the most common physical form reported (43.6%), while vomiting was the most common symptom. Nine deaths were recorded, of which 4 were due to pesticide poisoning”.[11]
In the Saudi Arabian area of Al-Mejmah, Abdolhaleem and Almeqhem in 2014, through retrospective analysis of the medical records of poisoning cases that occurred in the period from 2009 to 2012, 591 acute poisoned cases presented to emergency departments were included. They found that there was a marked preponderance of males over females (73.6% vs 26.4%). Children aged <12 years accounted for 20.6% of the cases. In children below the age of 12, pharmacological medications and home items were the most common sources of toxicity (84.4%), while wildlife envenomation, particularly scorpion bites, was responsible for the majority of patients above the age of 12. (62 %).[12]
In Makkah, Hegazy and Almalki (2012), through a cross-sectional design, the cases of poison registered in all Holy Makkah hospitals were studied to identify and evaluate different variables affecting the poisoning patterns from January 2009 to January 2011. A total of 330 patients were treated in health care facilities; of them, 200 (60.6%) were adults, and 130 (39.4%) were pediatric cases. Adults poisoned were mostly intentional (51%), whereas all children poisoned episodes were 100% unintentional. Pharmaceutical medicines, particularly paracetamol, were utilized in the majority of intentionally poisoned events (45%). The ratio of males to females was 3:5. The majority of adulthood poisoned cases (40%) were reported among those aged 21 to 35 years. [13]
3. Material and methods:
3.1. Study setting:
This study was conducted in Holy Makkah, which is located in Saudi Arabia's western area. and is considered the main place for residence of those who are coming to perform Hajj or Umra rituals; the resident population in Makkah city was estimated to be approximately three million in 2018. Medical services are provided through governmental and private hospitals and health centers under the jurisdiction of the Directorate of Health Affairs in Makkah, under which preventive services are managed by the Public Health Administration, which covers several departments, including the “Environmental Health and Occupational Safety” department.
The “Environmental Health and Occupational Safety” department is responsible for managing many activities related to monitoring the environment and occupational health; among these activities is the control and monitoring of cases of poisoning. The current study was conducted in this department, where all cases of poisoning reported over two years from 2018 to 2019 were reviewed, in addition to auditing the extent of compliance of the department to the rules and regulations governing surveillance, control and management of poison cases. All health care practitioners must use the reporting system for every case of poisoning. A case definition for chemical and drug overdose poisoning was achieved as any individual of any age who developed symptoms following exposure to medications that exceeded their prescribed limits or chemical materials; addicted cases were not included.[11]
3.2. Study population:
This study covers all chemical and drug overdose poisoning reported to the “Environmental Health and Occupational Safety” department in Makkah Almukarramah over two years from 2018 to 2019. The overall number of reported cases was 251.
3.3. Data collection and statistical analysis:
Three experts evaluated the face and content validity of the data collection sheet for the standardized reporting form, and its internal consistency reliability measured by Cronbach's alpha test was 80%. The data were collected by well-trained health care practitioners in each health institute and then reviewed and checked for completeness by a specialized poisoning unit in the regional environmental health and occupational safety department. Software for the he Package of Statistical analysis for Social Science (SPSS) 21 was used for statistical analysis. All received cases were registered and saved in Microsoft Excel. Initially, all data available in Excel files were exported to the SPSS program. The frequency distribution and simple descriptive statistical analysis and percentages for qualitative variables were performed for the study sample. The chi-square test was used to compare qualitative variables. Throughout the statistical findings, the statistical significance limit was set at P < 0.05.
3.4. Ethical consideration:
Data were obtained after applying for ethical approval from the Directorate of Health Affairs institution (the institution responsible for approval of the research) with IRB committee ethical approval code (H-02-K076-0222-672) at 08-03-2022. As there was no direct contact with persons in the study and the study works on already available data in the Environmental Health and Occupational Safety” department in Makkah Almukarramah, informed consent was obtained from the Directorate of Health Affairs institution after reviewing the study. The collected data were strictly confidential, were not disclosed for any reason and were used only for the study purposes.
4. Results:
All cases in Makkah Al-Mukarramah that have been reported to the public health administration as substance poisoning, either chemical or drug poisoning, in 2018-2019 were included in the current study.
4.1. Characteristics of the cases:
The total number of cases reported in 2018 accounted for 209 cases, whereas in 2019, there were just 42 cases. Table 2 illustrates that the overwhelming majority of the cases were Saudis (91.6%), and the rest were non-Saudi 21 (8.4%) who were mainly Indonesian (5 cases), Pakistani (5 cases) and Egyptians (3 cases), with a slight predominance of males (57.4%) over females (42.6%). Generally, almost two-thirds of the cases occurred in children younger than 13 years (61.4%); among them, children aged 1 to 5 years accounted for 51.0% of all cases, while children aged 6 to 12 years accounted for 6.4% of all cases. In addition, 4% of the cases were in infants under the age of one year.
4.2. Epidemiological and clinical characteristics of the cases:
Figure 1 demonstrates that most of the poisoning cases resulted from drug overdose (63.3%), while 34.7% were chemical poisoning and five cases (2%) were unknown.
Table 3 shows that although almost two-thirds of poisoning cases that occurred in Saudi Arabia were due to drug overdose (66.1%) compared to 47.4% in non-Saudi Arabia, and a slightly higher percentage of drug overdose poisoning was observed in females than males (68.9% vs 61.4%), these differences, however, were not statistically significant (p>0.05). On the other hand, it was found that there were significantly higher percentages of chemical poisoning in children than in older age groups, ranging between 50% in children aged 6-12 years and 47.2% in those aged 1-5 years to as low as 17.6% in those aged 40 years or older (p<0.05).
Table 3 shows that although drug overuse poisoning was more frequent in Saudi cases (66.1%) than in non-Saudi cases (47.4%) and more frequent in females (68.9%) than in males (61.4%), these differences were not statistically significant (p>0.05). On the other hand, chemical poisoning was significantly more frequent in children aged 1-5 years (47.2%) and those aged 6-12 years (50%), especially when compared to older age groups; those aged 13-19 years (3.8%) p<0.05.
Figure 2 demonstrates that both the drug overdose and chemical poisoning follow almost the same seasonal trend, with a rise in the number of cases reported in January, February, and March, followed by a decline in April, May and June, then an increase in July, reaching another peak in September, followed by a decline towards the end of the year.
Table 4 shows the list of medicines reported in the cases of drug overdose poisoning, where analgesics came on top of the list (n=48 cases), followed by antiepileptics (n=17 cases), antihypertensives (n=13 cases), antipsychotics (n=12 cases) and antimicrobials (n=9 cases).
In the same context, Table 5 shows that cleansing substances are the most common causes of chemical poisoning (n=30 cases), followed by disinfectants (n=17 cases), insecticides (n=8 cases) and antiseptics (n=2 cases).
Circumstances for using the substances that caused poisoning are displayed in Table 6; it demonstrates that while the overwhelming majority of the cases of chemical poisoning resulted from accidental intake of the substance (92%) and only 3.4% were taken intentionally, a significantly higher percentage was observed in the intentional intake of medicines that caused drug overdose poisoning (p<0.05). Most of the medicines were in a solid form (92.1%), while chemical substances were in liquid (64.4%), solid (16.1%), gas (11.5%) and powder forms (8%) p<0.05. The great majority of the medicines (98.1%) and chemical substances (90.7%) were taken by the oral route; however, more cases of the chemical substances than medicines were taken by inhalation (9.3%). These differences were statistically significant at p<0.05.
Table 7 displays a comparison between accidental and intentional poisoning according to the characteristics of the cases and type of poisoning; it shows that the percentage of females formed approximately three quarters of cases (70.4%) who took the poisonous substances intentionally, and almost all cases of intentional poisoning were in the age groups 13-19 years (48.1%) and 20-39 years (48.1%). Furthermore, the overwhelming majority of intentional poisoning cases identified (88.9%) used drug overdosing rather than chemical substances (11.1%). These differences were statistically significant at p<0.05.
Regarding the clinical presentation and management of the cases, Table 8 demonstrates that the most common presenting symptoms for the cases were vomiting (26.7%), nausea (22.9%), abdominal pain (12.2%), headache (11.5%) and difficulty breathing (9.2%). Only 6 cases (2.4%) were in deteriorating condition, and almost half of the cases (44.2%) necessitated admission to the hospital, in addition to 25.6% who were discharged against medical advice. Blood samples for toxicological testing were withdrawn from more than one-third of the cases (37.1%), urine samples were taken from 6.8% of the cases, and gastric lavage was performed for 6% of the cases for toxicological investigations.
5. Discussion:
Acute poisoning is a common emergency situation worldwide; it requires high medical attention, as it usually results in serious outcomes in terms of morbidities and mortalities. In Saudi Arabia, specialized units are present in public health administrations in all regions; these units are responsible for managing and monitoring poison cases. The current study was carried out in the poison unit in Makkah Almukarramah, where all cases reported to the unit in the period from 2018 until the end of 2019 were reviewed.
Out of all reported cases (n=251), males constituted 57.4%, which is in accordance with what had been reported by Alzhrani et al. (2017), who reported that males formed 55% of poison cases in Jeddah,[10] and Abd-elhaleem (2014), who noted that there was a marked dominance of males over females in poisonous cases that occurred in the AlMajmah region in the period from 2009 to 2012 (73.6% vs 26.4%).[12] However, these findings were in contrast to those revealed by Bakhaidar (2015), who found that there was a slight preponderance of females (54.3%) over males (45.7%) in poison cases in the western region of Saudi Arabia.[6] These differences could be attributed to the variation in demographic and cultural traits between communities in different regions. Such a tendency could be linked to the exposure of particular people to various chemical substances, changes in lifestyle patterns, the frequency or location of recorded events, social class, economic status, aggressiveness and societal structure. Furthermore, in Saudi culture, males usually stay outside their homes for work, collect money, and are more active in terms of physical, intellectual, psychological and social activity than females, and they are predisposed to higher levels of stress, as the great majority of them are under pressure to maintain themselves and their family members, have a variety of obligations (both monetary and emotional), and are victims of poverty or any domestic or societal conflict; these factors may make people more prone to engaging in risky activities. Moreover, the male population in some regions of Saudi Arabia is greater than the female population.
The current study discovered that the majority of cases of poisoning occurred among Saudis (91.6%), which is most likely representative of Saudi Arabia's demographic distribution; such a result aligns with the findings of previously mentioned Saudi Arabian studies.[6]
Almost two-thirds of the cases (61.4%) were children aged less than 13 years; among them, children aged 1 to 5 years accounted for 51.0% of all cases, and 4% of the cases occurred in infants <1 year, which supports the explanation assumed by Kaale and his colleagues (2014), who said that “Many cases are likely to occur in young people under the age of six, as they have a desire to investigate their environment by placing anything within their mouths and lack the ability to distinguish between hazardous and harmless substances; furthermore, the higher proportion of males in the poisoning pediatric population might be due to males kid's greater movement and adventurous activities than females.[14] These differences in our data could be attributed to the inherent curiosity, mobility and restlessness of children compared to adults. Furthermore, there was more poisoning in boys than in girls, which could be related to males’ greater mobility and exploration activity than females. Additionally, increased levels of testosterone may be responsible for the hyperactivity behavior of boys, which supports the explanation assumed by Wang LJ and his colleagues (2017), who said that "the high level of testosterone contributes to the development of hyperactivity in children".[15]
Most of the poisoning cases investigated in our study resulted from drug overdose (63.3%), while 34.7% were due to chemical poisoning. In this respect, the Annual.
According to an American Association of Poison Control Center report, "poisonous agents demonstrate regional variances driven by economic level." Poisoning is most commonly caused by cosmetics, drugs and household cleaning products, alcohol, and beauty products in developed countries, whereas pesticides, hydrocarbons, mushrooms, and traditional medicines are common causes of poisoning in underdeveloped nations where agricultural production is the primary source of income. [16]
The present study's types of poisoning support the rising likelihood of suicidal behaviors, with medications being the most frequent reason.
The majority of medication overdose cases of poisoning (96.2%) were seen in the age group 13-19 years in the current study, which may attract attention that adolescents are at more risk. Bakar et al., 1999 and Sharma et al., 2010 found the same results; they state that failing in the exams, failing in their issues, and inability to live up to the expectations of others were the most common reasons for poisoning in this age group. In general, such individuals are emotionally unbalanced in addition to their immaturity to withstand intense physical or mental stress. [17,18]
Similarly, analgesics, antipyretics or anti-inflammatory agents came on top of the list of drugs incriminated in drug overdose poisoning in our study, which accords with the findings of Bakhaidar (2015), where analgesics accounted for the greatest proportion of utilized drugs;[6] this could be attributed to the wide distribution and usages of these drugs by Saudis compared to other drugs. Because basic analgesics (street drugs) are so easily accessible, they are one of the leading causes of drug poisoning. The second drug group incriminated in drug overdose poisoning in our study was antiepileptic drugs, which could be attributed to the wide distribution and usages of these drugs by knowledgeable, affluent and wealthy Saudis, which is most likely related to the fact that this group of individuals is aware of the medications' capacity to do painless death (sleep death); such medications were utilized frequently as a result of emotional problems or to attract people focus to anything else, which was demonstrated by ingesting just a small quantity (few pills) and retaining the medication strip. Further research is required to supplement our work on why patients choose analgesics, antipyretics or anti-inflammatory and antiepileptic drugs as a self-poison and to identify the best way of reducing the mortality and morbidity associated with these drugs in overdose.
According to the present study, all pediatric cases were attributed to unintentional poisoning (100%). Such findings are consistent with [13], [19], who discovered zero events of intentional poisoning in this pediatric group in their investigations in Hafr Al Baten and Makkah, Saudi Arabian Kingdom, possibly due to the scarcity of this attitude and practice within that part of the globe. The researchers linked such pediatric group behavior to their firm and higher level of attachment to their households, which offers considerable prevention from unintentional poisoning. The preponderance of unintentional poisoning in this age group can be explained by a combination of the drive for discovery, mouth exploration, and poor risk assessment.
In the current study, most poisoning incidents that occurred in young children were due to drug overdose. In the Saudi Arabian Kingdom, comparable studies found the same thing.[16], where the authors explained that children toddler age are inquisitive and mostly exploratory in their attitudes and actions, almost putting every substance, e.g., thrown tablets, inside their mouths and lacking the ability to differentiate between hazardous and harmless substances, while hyperactivity is associated with poisoning at home in some older children, and it is not associated with poisoning in toddlers. Furthermore, because medications may be sold directly to consumers without the need for prescriptions from a treating physician and Saudis continually change physicians for almost the same disease, an excess of medications can be discovered in Saudi households.[20]
Similarly, Asiri and his colleagues (2007) added that some of the reasons for the increased likelihood of drug overdose poisoning include drug delivery in envelopes rather than kid-resistant bottles, free medical care, growing wealth and easily accessible medications without even prescriptions, Saudis family members' natural propensity to save unused medicine for future usage, and the irresponsible storing of pharmaceuticals in the majority of houses.[21]
Additionally, the current study showed that males outnumbered females in accidental poisoning, while the reverse was noticed in suicidal poisoning. This does not come in accordance with AL Nsour, 2002, who found that in Jordan, males outnumbered females in suicide.[22]This may be attributed to the Islamic particular religious disapproval and severe prohibition of purposeful of self-killing, which affects Saudi boys and men more than girls and woman.
Intentional poisoning, which is viewed typically as a suicidal attempt, was significantly more frequent in females than males in the current study, which is in accordance with previous studies that pointed to the notion that females are more likely than males to commit suicide.[6,7,8,13] This might be related to the fact that Saudi females, unlike males, spend the majority of their time at home. This may be attributed to the high rate of depression among Saudi females as a result of long stays home compared to males. High levels of burnout in social, educational, and economic aspects, along with difficulty in achieving educational, professional, and socioeconomic goals, resulting in fewer options, were all variables that contributed to suicidal behavior. Furthermore, the existence of some sort of cultural social repression among Saudi females, including domestic violence and psychologically and physically abusive behavior, usually by the partner, as well as their late seeking medical assistance, may explain our finding.
Additionally, in our study, the great majority of intentional poisoning cases used drugs rather than chemical substances, which supports other studies that showed that drugs are the most commonly used for suicide attempts followed by household chemicals; [9] This might be linked to the ease with which pharmacological drugs are available without prescription, over the counter in the pharmacies, more suitable taste of drugs than chemical substances.
The majority of poisoning cases in our study occurred as a consequence of oral consumption, which is consistent with the observations of the aforementioned Saudi Arabian studies. [9,10,11]
In our drug poisoning cases, the most common route was oral (98.1%), and the most frequent physical form reported was solid medication (92.1%). This is consistent with the findings of the aforementioned Saudi Arabian studies. [10,11]
Signs and symptoms of poisoning vary greatly according to the type and dose of poisoning, age of the victim and route of administration; [23] our data showed that the most reported symptoms for the cases were vomiting, nausea and abdominal pain, which supports our findings that most of the poisonous substances were taken through the oral route. This could be related to the simplicity with which poisoning substances can be administered orally as opposed to other methods. and it may decrease the likelihood of environmental and occupational poisoning and increase the risk of suicidal ideation and behavior or exposure in the home, particularly among babies and children.
Only 6 cases (2.4%) were in deteriorating condition, and almost half of the cases (44.2%) necessitated admission to the hospital, which indicates a rapid response of the victims or their relatives to seek medical intervention. Additionally, the results showed that blood samples for toxicological testing were withdrawn from more than one-third of the cases, while urine samples were taken from 6.8% of the cases, and gastric lavage was performed for 6% of the cases for toxicological investigations, which could reflect the degree of adherence of the treating health personnel to the guidelines regulating management of poison cases in Saudi Arabia.
Our data showed that both drug overdose and chemical poisoning follow almost the same seasonal trend, with an increase in the reported case number during January, February and March, followed by a decline in April, May and June; this decline may be attributed to the period of vacation during this time of the year, where most people are outside the home and away from sources of poisoning. Another explanation might be that the father and mother are frequently in vacation and away from their jobs. Therefore, they may be close to their young children in social gathering (which normally rises throughout vacation seasons) and supervise them with their elder siblings and servants.
The current study revealed that the most common chemical poisonings are cleaning substances and disinfectants, which are often accessible in most Saudi houses in nonsolid forms and are frequently improperly preserved, and their multicolored appearance is appealing to children. Furthermore, these products are routinely offered in containers that lack an identifying label that informs the consumer of their origin and provides safety precautions; these may explain our finding. However, in 2008, worldwide health organizations and the United Nations Children's Fund published a study on child injury prevention that advised that as a strategy to avoid child poisoning and minimize accompanying lesions, the replacement of possibly harmful household items by identical items with more benign characteristics, as well as giving immediate medical care and professional knowledge, are highly recommended. [24]
6. Conclusion and recommendations:
The current study results are consistent with most of the previous studies carried out in different regions in the Saudi Arabian Kingdom, where there was a slight predominance of males over females, and most of the poisoning cases resulted from overdose of drug. The most frequent drug poisoning was attributed to analgesics, followed by antiepileptics, antihypertensive drugs, antipsychotics and antihistamines, while cleaning and detergent agents were the most common poisonous chemicals. Poisoning by chemicals was significantly higher in children than in older age groups, and all intentional poisoning occurred in adults.
Reviewing the performance and adherence of the “Environmental Health and Occupational Safety Department” to the guidelines and instruction regulating monitoring, notification and reporting of poison cases are satisfactory and the poisoning surveillance system is effective.
Further in-depth studies are needed to elaborate other socioeconomic and demographic factors associated with chemical and drug overdose poisoning. Public health plans, policies and legislations should be implemented to reduce these factors, including prohibition over-the-counter pharmaceutical sales, selling the possibly harmful substances in kid-proof bottles and additional stringent rules governing chemical sale and storage. Intensive supervision of children is needed. Suicidal poisoning patients should seek psychiatric help to limit the possibility of attempting suicide again in the future. Furthermore, efforts are needed to plan and implement health education programs and campaigns about the factors proven in the current study to be significantly related to chemical and drug overdose poisoning to raise public knowledge about exposure to chemicals and its consequences. Popular communication media, commercial malls, road ads, learning institutions and workplaces can be used to deliver health education campaigns and programs. Advice on how to store chemicals safely and how to keep kids safe should be focused on during such programs.
References
- WHO, “WHO | Poisoning Prevention and Management,” 2016.
- Ramesha, K.B. Rao, and G.S. Kumar, Pattern and outcome of acute poisoning cases in a tertiary care hospital in Karnataka, India. Indian journal of critical care medicine: peer-reviewed, official publication of Indian Society of Critical Care Medicine, 2009. 13(3): p. 152. [CrossRef]
- “OED Environmental Outlook for the Chemical Industry.”. Available online: https://www.oecd.org/env/ehs/2375538.pdf (accessed on 21 October 2019).
- “King Fahad medical city Poison control department,” 2016. Available online: https://www.kfmc.med.sa/EN/Patient/Poison-Control/Pages/default.aspx (accessed on 21 October 2019).
- Martins, S.S., et al., Worldwide prevalence and trends in unintentional drug overdose: a systematic review of the literature. American journal of public health, 2015. 105(11): p. e29-e49. [CrossRef]
- Bakhaidar, M., et al., Pattern of drug overdose and chemical poisoning among patients attending an emergency department, western Saudi Arabia. Journal of community health, 2015. 40(1): p. 57-61. [CrossRef]
- Teklemariam, E., S. Tesema, and A. Jemal, Pattern of acute poisoning in Jimma University specialized hospital, south West Ethiopia. World journal of emergency medicine, 2016. 7(4): p. 290. [CrossRef]
- Malangu, N. and G. Ogunbanjo, A profile of acute poisoning at selected hospitals in South Africa. Southern African Journal of Epidemiology and Infection, 2009. 24(2): p. 14-16.
- Al-Barraq, A. and F. Farahat, Pattern and determinants of poisoning in a teaching hospital in Riyadh, Saudi Arabia. Saudi Pharmaceutical Journal, 2011. 19(1): p. 57-63. [CrossRef]
- Alzahrani, S.H., et al., Five-year epidemiological trends for chemical poisoning in Jeddah, Saudi Arabia. Annals of Saudi medicine, 2017. 37(4): p. 282-289. [CrossRef]
- Moazzam, M., et al., Pattern of acute poisoning in Al-Qassim region: a surveillance report from Saudi Arabia, 1999-2003. EMHJ-Eastern Mediterranean Health Journal, 15 (4), 1005-1010, 2009.
- Abd-Elhaleem, Z.A.E. and B. Al Muqhem, Pattern of acute poisoning in Al Majmaah region, Saudi Arabia. Am. J. Clin. Exp. Med, 2014. 4(2): p. 79-85. [CrossRef]
- Hegazy, R. and W. Almalki, Pattern of acute poisoning in makkah region saudi arabia, 2009-2011. In presentations from the 22nd Congress of the ilam (July 5-8, 2012, Istanbul, Turkey). 2012.
- Kaale, E., et al., A retrospective study of poisoning at Muhimbili National Hospital in Dar-Es Salaam, Tanzania. J Public Health Front, 2013. 2(1): p. 21-26.
- Wang, L.-J., et al., The trend in morning levels of salivary cortisol in children with ADHD during 6 months of methylphenidate treatment. Journal of attention disorders, 2017. 21(3): p. 254-261. [CrossRef]
- Gummin, D.D., et al., 2017 Annual report of the American Association of Poison control centers’ National Poison Data System (NPDS): 35th annual report. Clinical toxicology, 2018. 56(12): p. 1213-1415.
- Sharma, B., et al., Toxicological emergencies and their management at different health care levels in Northern India-An overview. Journal of Pharmacology & Toxicology, 2010. 5(7): p. 418-430.
- Bakar, M., S. Ahsan, and P. Chowdhury, Acute poisoning-nature and outcome of treatment in a teaching hospital. Bangladesh Med J (Khulna), 1999. 32(1): p. 19-21.
- Izuora, G.I. and A. Adeoye, A seven-year review of accidental poisoning in children at a military hospital in Hafr Al Batin, Saudi Arabia. Annals of Saudi medicine, 2001. 21(1-2): p. 13-15. [CrossRef]
- El-Mouzan, M., A. Elaged, and N. Ali, Accidental poisoning of children in the Eastern Province. Saudi medical journal, 1986. 7(3): p. 231-236.
- Asiri, Y.A., et al., Evaluation of drug and poison information center in Saudi Arabia during the period 2000-2002. Saudi medical journal, 2007. 28(4): p. 617-619.
- AL-Nsour, T.S. and K.A. Hadidi, Investigating the presence of a common drug of abuse (benzhexol) in hair; the Jordanian experience. Journal of clinical forensic medicine, 2002. 9(3): p. 119-125. [CrossRef]
- Gossel, T.A., Principles of clinical toxicology. 2018: CRC Press. [CrossRef]
- Branche, C., et al., World report on child injury prevention. 2008.
Figure 1.
Types of poisoning reported in the cases in the period from 2018-2019.
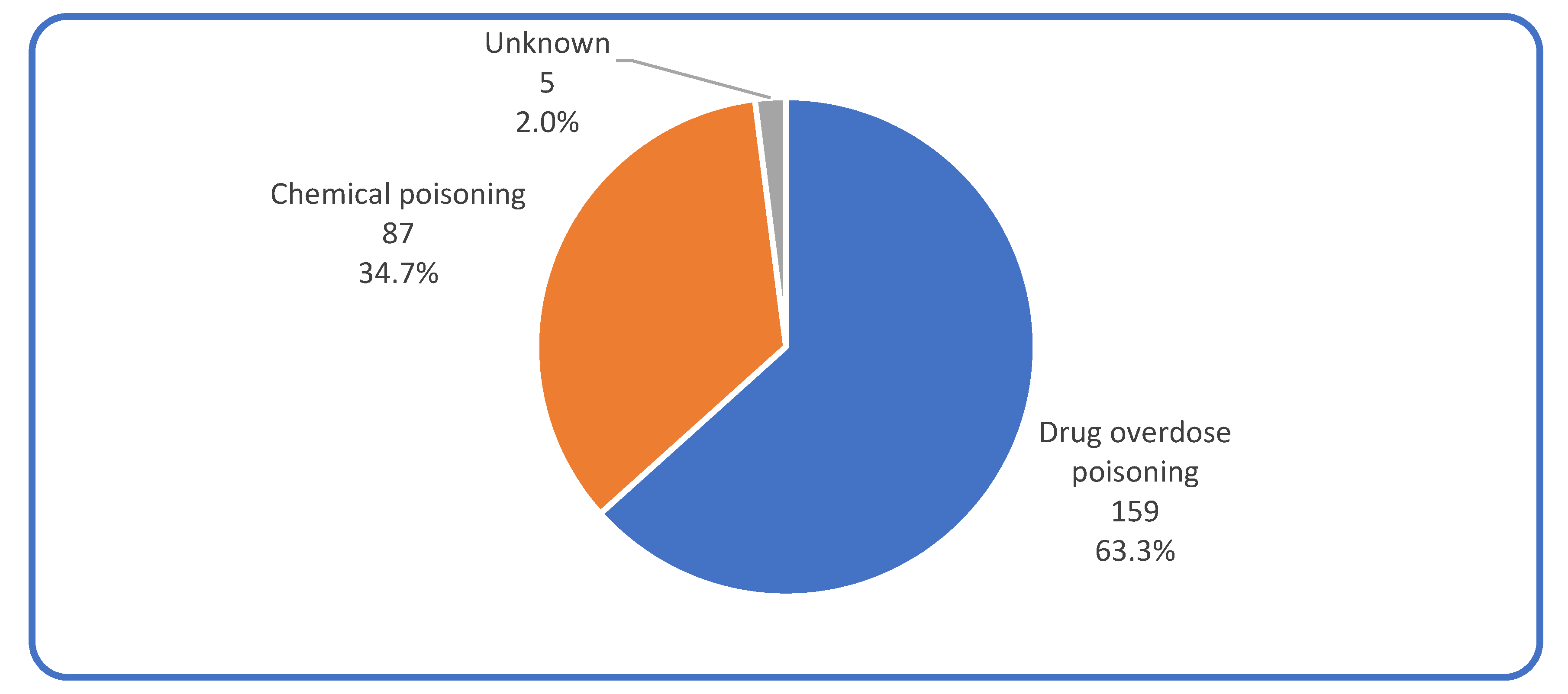
Figure 2.
Seasonal variations in the frequency of drug overdose and chemical poisoning.
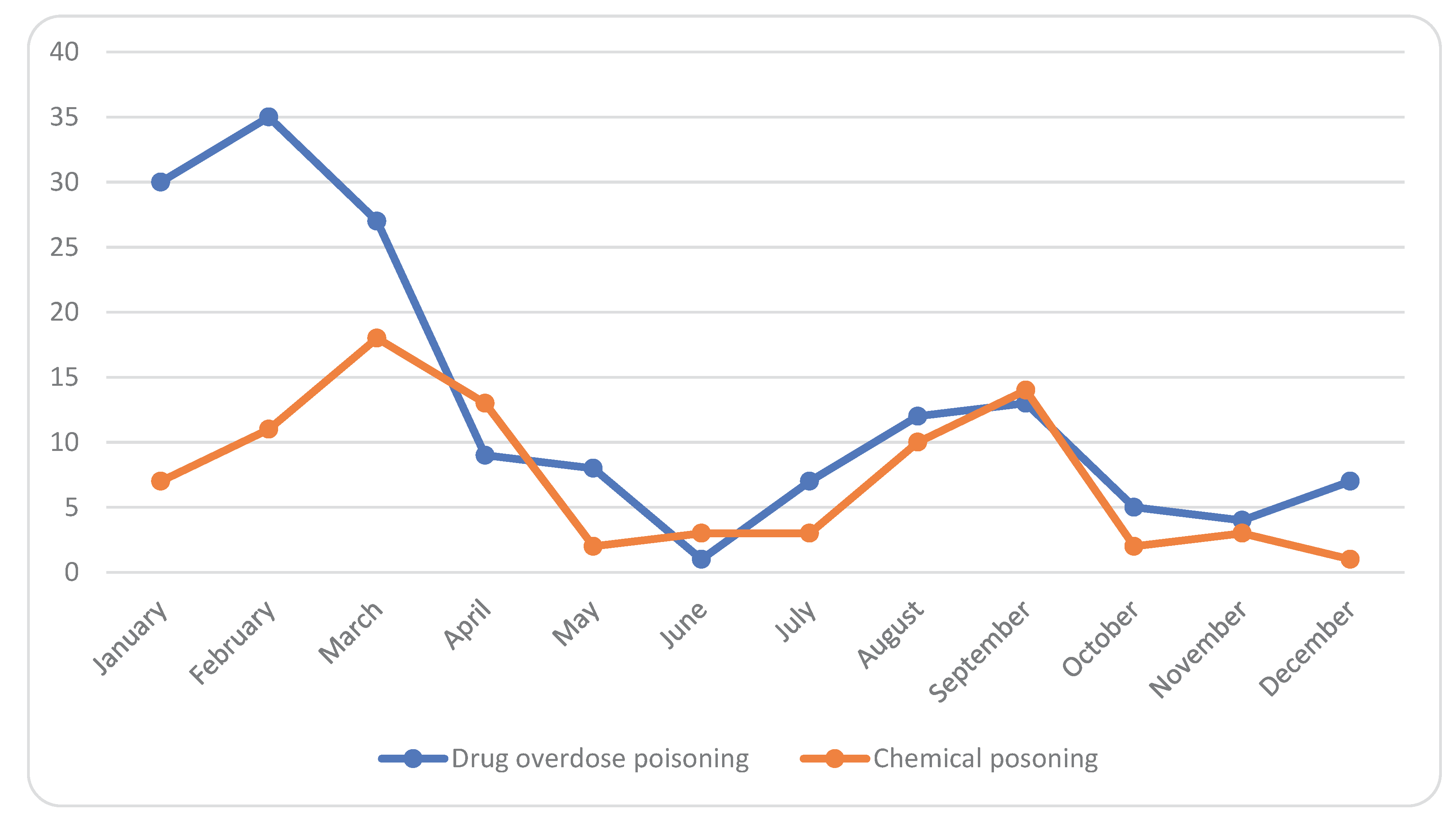

Table 1.
Mortality rates in Saudi Arabia attributed to unintentional poisoning (per 100 000 population).
Table 1.
Mortality rates in Saudi Arabia attributed to unintentional poisoning (per 100 000 population).
| Year | Gender | Mortality rate/100,000 |
| 2000 | Both (males and females) | 1.300 |
| Males | 1.500 | |
| Females | 1.00 | |
| 2005 | Both (males and females) | 1.00 |
| Males | 1.20 | |
| Females | 0.80 | |
| 2010 | Both (males and females) | 0.90 |
| Males | 1.0 | |
| Females | 0.70 | |
| 2015 | Both (males and females) | 0.70 |
| Males | 0.80 | |
| Females | 0.50 | |
| 2016 | Both (males and females) | 0.70 |
| Males | 0.80 | |
| Females | 0.50 |
After courtesy of worldwide health organization, 2019 (http://apps.who.int/gho/data/node.sdg.3-9-data?lang=en).
Table 2.
Demographic characteristics of the cases (n=251).
| Characteristics | No. | % |
| Nationality: | ||
| Saudi | 230 | 91.6 |
| Non Saudi | 21 | 8.4 |
| Gender: | ||
| Male | 144 | 57.4 |
| Female | 107 | 42.6 |
| Age: | ||
| <1 year | 10 | 4.0 |
| 1-5 years | 128 | 51.0 |
| 6-12 years | 16 | 6.4 |
| 13-19 years | 27 | 10.8 |
| 20-39 years | 53 | 21.1 |
| 40+ years | 17 | 6.8 |
Table 3.
Differences in types of poisoning based on the demographic characteristics of the cases.
| Characteristics | Types of poisoning | |||||
| Drug overuse poisoning | Chemical poisoning | X2 | p | |||
| No | % | No | % | |||
| Nationality: | 2.685 | 0.101 | ||||
| Saudi | 150 | 66.1% | 77 | 33.9% | ||
| Non Saudi | 9 | 47.4% | 10 | 52.6% | ||
| Gender: |
1.461 |
0.227 |
||||
| Male | 86 | 61.4% | 54 | 38.6% | ||
| Female | 73 | 68.9% | 33 | 31.1% | ||
| Age: |
25.925 |
<0.001* |
||||
| < 1 year | 7 | 70.0% | 3 | 30.0% | ||
| 1-5 years | 67 | 52.8% | 60 | 47.2% | ||
| 6-12 years | 8 | 50.0% | 8 | 50.0% | ||
| 13-19 years | 25 | 96.2% | 1 | 3.8% | ||
| 20-39 years | 38 | 76.0% | 12 | 24.0% | ||
| 40+ years | 14 | 82.4% | 3 | 17.6% | ||
Table 4.
List of medicine categories reported in the drug overdose poisoning cases.
| Medicines’ categories | Frequency |
| Analgesic Antipyretic or Anti-inflammatory | 48 |
| Antiepileptic | 17 |
| Anti-Hypertensive | 13 |
| Antipsychotic | 12 |
| Anti-Histaminic | 9 |
| Antibiotic | 7 |
| Vitamins | 6 |
| Anti-emetic | 6 |
| Anti-diabetic | 5 |
| Contraceptive | 4 |
| Anti-Asthmatic | 2 |
| Iron Preparations | 1 |
| Unknown | 7 |
| Others | 16 |
Table 5.
List of chemical substances reported in the chemical poisoning cases.
| Chemical substances | Frequency |
| Cleansing Substance | 30 |
| Disinfectant | 17 |
| Insecticide | 8 |
| Antiseptic | 2 |
| Carbon Monoxide | 1 |
| Fuel | 1 |
| Unknown | 5 |
| Other | 19 |
Table 6.
Form, route and circumstances of taking the substances that caused poisoning.
| Types of poisoning | ||||||
| Drug overuse poisoning | Chemical poisoning | X2 | P | |||
| No | % | No | % | |||
| Circumstances: | 39.512 | <0.001* | ||||
| Accidental | 81 | 52.3% | 80 | 92.0% | ||
| Intentional | 25 | 16.1% | 3 | 3.4% | ||
| Unknown | 49 | 31.6% | 4 | 4.6% | ||
| Physical form: |
141.338 |
<0.001* |
||||
| Solid | 140 | 92.1% | 14 | 16.1% | ||
| Liquid | 12 | 7.9% | 56 | 64.4% | ||
| Gas | 0 | 0.0% | 10 | 11.5% | ||
| Powder | 0 | 0.0% | 7 | 8.0% | ||
| Route of administration: |
16.314 |
<0.001* |
||||
| Oral | 151 | 98.1% | 78 | 90.7% | ||
| Injection | 3 | 1.9% | 0 | 0.0% | ||
| Inhalation | 0 | 0.0% | 8 | 9.3% | ||
Table 7.
Comparing accidental and intentional poisoning among cases according to their characteristics and type of poisoning.
Table 7.
Comparing accidental and intentional poisoning among cases according to their characteristics and type of poisoning.
| Circumstances of poisoning | ||||||
| Accidental | Intentional | X2 | p | |||
| No | % | No | % | |||
| Gender: | 6.852 | 0.009* | ||||
| Males | 92 | 56.8% | 8 | 29.6% | ||
| Females | 70 | 43.2% | 19 | 70.4% | ||
| Age: |
NA |
NA |
||||
| <13 years | 146 | 90.1% | 0 | 0.0% | ||
| 13-19 years | 2 | 1.2% | 13 | 48.1% | ||
| 20-39 years | 12 | 7.4% | 13 | 48.1% | ||
| 40+ years | 2 | 1.2% | 1 | 3.7% | ||
| Type of poisoning: |
13.956 |
<0.001* |
||||
| Drug overdose poisoning | 81 | 50.3% | 24 | 88.9% | ||
| Chemical poisoning | 80 | 49.7% | 3 | 11.1% | ||
Table 8.
Clinical condition and management of the cases.
| Clinical condition | Frequency | % |
| Symptoms | ||
| Vomiting | 35 | 26.7 |
| Nausea | 30 | 22.9 |
| Abdominal pain | 16 | 12.2 |
| Headache | 15 | 11.5 |
| Difficulty in breathing | 12 | 9.2 |
| Dizziness | 7 | 5.3 |
| Loss of consciousness | 4 | 3.1 |
| Disorientation | 3 | 2.3 |
| Weakness | 2 | 1.5 |
| Blurred vision | 2 | 1.5 |
| Seizures | 2 | 1.5 |
| Fever | 1 | 0.8 |
| Skin rashes | 1 | 0.8 |
| Coma | 1 | 0.8 |
| Condition | ||
| Stable | 245 | 97.6 |
| Deteriorated | 6 | 2.4 |
| Management | ||
| Admitted to the hospital | 107 | 44.2 |
| Discharge against medical advice | 62 | 25.6 |
| Not admitted | 73 | 30.2 |
| Laboratory Investigations | ||
| Blood sample hospital lab | 164 | 65.3 |
| Blood sample toxicological | 93 | 37.1 |
| Urine sample hospital lab | 28 | 11.2 |
| Urine sample toxicological | 17 | 6.8 |
| Gastric lavage hospital lab | 33 | 13.1 |
| Gastric lavage toxicological | 15 | 6.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



