Submitted:
07 November 2023
Posted:
07 November 2023
You are already at the latest version
Abstract
Background: Patients with infectious complications related to the presence of cardiac implantable electronic devices (CIED) constitute a heterogeneous group, including local pocket infection (PI) and lead related infectious endocarditis (LRIE). The diagnosis of CIED-related infection is often difficult and requires complex imaging and microbiological tests. The aim of the current study was to evaluate the usefulness of new simple hematological parameters in detecting infectious complications in patients with CIED and assessing their extent.
Methods: The retrospective analysis of clinical data of 2909 patients (36.37% with CIED-related infections), undergoing transvenous lead extraction (TLE) procedures in three high-volume centres in the years 2006-2020, was conducted. The sensitivity and specificity of new hematological markers were evaluated: the neutrophil to lymphocyte ratio (NLR), neutrophil to platelet ratio (NPR), and lymphocyte to platelet ratio (LPR) in the diagnosis of infectious complications, assessment of the spread of the infectious process and differentiation of additional structures related to the presence of leads.
Results: In patients with CIED infections, compared to the non-infectious group, high inflammatory parameters were confirmed, and the highest specificity of the new markers in detecting the infectious process was demonstrated. (79.47% for NPR and 72.82% for NLR). Analysis of laboratory parameters in infectious and non-infectious patients with the presence of additional lead-related masses showed the highest specificity of NPR (82,78%) in predicting the diagnosis of vegetation. Comparison of laboratory parameters in patients with LRIE and PI showed higher NLR % (4.24 vs 2.56; p<0.001, area under curve (AUC) in a receiver operating characteristic (ROC) curve: 0.67 and 0.78 respectively) and higher NPR (0.03 vs 0.02; p<0.001; AUC: 0,51 and 0,55) in patients with LRIE. The highest sensitivity in the detection of coexistence LRIE with PI has been demonstrated for NLR (87.33%).
Conclusions: Novel hematological markers may be helpful in the recognition of the inflammatory process in patients with CIED, differentiation of vegetation and vegetation-like masses, and the extent of infection in patients with PI.
Keywords:
Hematological parameters
; cardiac implantable electronic device-related infections
; extension of CIED-related infections
; vegetations
Introduction
Cardiac implantable electronic device (CIED) related infections constitute a heterogeneous group of diseases with a poor prognosis. The spectrum of infectious complications in patients with CIED includes pocket infection (PI) and lead related infectious endocarditis (LRIE). LRIE may coexist with pocket infection or occur in an isolated form [1,2]. There are two pathophysiological mechanisms of LRIE, which include contamination of the leads and/or generator during implantation or subsequent CIED-related procedures, and bloodstream infection, which may occur in the setting of bacteremia due to a distant infection [3]. The diagnosis and the assessment of the extent of infection in patients with CIED is often difficult.
LRIE is a severe condition with a very dangerous course. The symptoms might develop slowly with short episodes of fever which is often ignored by both the patient and the doctor [4]. If local signs of pocket infection are present, a proper diagnosis seems to be easier; however, the assessment of the spread of inflammatory process is still challenging. Similar to other infectious diseases, a gradual increase in the number of neutrophils and a simultaneous decrease in the number of lymphocytes is a typical change in leukocytes in response to acute bacterial infections, while a new hematological parameter – the neutrophil-to-lymphocyte ratio (NLR) – may reflect the severity of the disease [5]. During an infection, we also observe an increase in thrombotic processes associated with increased platelet count. A new lymphocyte-to platelet ratio (LPR) and neutrophil-to-platelet ratio (NPR) parameterr may be also helpful in the assessment of the intensity of this phenomenon in patients with LRIE [6].
The aim of the current study was to evaluate the sensitivity and the specificity of new simple hematological parameters in the detection of CIED-related infection, confirming/excluding the presence of vegetation, and the assessment of the extent of the infectious process.
Methods
Study group
The retrospective analysis of data of 2909 patients undergoing transvenous lead extraction (TLE) in three high volume centers in Poland (Zamość, Radom and Lublin) by one main operator in the years 2006-2020 was conducted. All information relating to patients and procedures was entered into the computer on an ongoing basis. The procedures were performed because of both infectious and non-infectious indicators. Infectious indicators included: isolated pocket infection and lead related infective endocarditis (with or without PI). Additionally, a comparative analysis was performed between a group of patients with the presence of vegetation (connected with the lead or valve) and a non-infectious group with additional structures on the lead (vegetation-like masses). The diagram of the study population is presented in Figure 1.
Definitions
According to the current guidelines [7], certain LRIE diagnosis was confirmed if two major criteria or one major and three minor criteria were fulfilled. Isolated pocket infection was characterized by the local signs of infection including swelling, warmth, erythema, and a significant skin erosion around the device pocket [7]. All patients underwent preoperative transthoracic echocardiography (TTE) and in all patients with suspected LRIE, transesophageal echocardiography (TEE) was performed. Patients with additional structures associated with the lead or surrounding heart structures, without infection, were qualified to vegetation-like masses group.
Laboratory markers
We analyzed laboratory tests of patients qualified for transvenous lead extraction, performed in referral centers and at TLE centers. The hematological results included: lowest values of hemoglobin level, hematocrit level and platelet count, highest value of white blood cell (WBC) count, neutrophil count and ratio, highest value of erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and procalcitonin. Furthermore, we analyzed neutrophil-to-lymphocyte ratio (NLR), lymphocyte-to-platelet ratio (LPR) and neutrophil-to-platelet ratio (NPR). Laboratory test results were compared in patients with infectious and non-infectious indications for TLE, as well as between individual groups of infectious patients and between patients with vegetation and vegetation-like masses.
Echocardiographic findings
Vegetation was defined based on echocardiography (TTE and TEE) as multi shaped, mobile masses of inhomogeneous echogenicity (hypoechoic in the initial phase of infection) attached to the lead or to the neighboring anatomic structures, most frequently tricuspid valve leaflets. Vegetation was accompanied by clinical signs of an infection [8]
Vegetation-like masses were characterized by heterogeneous echogenicity and irregular contour. They were attached to the lead or surrounding structures, varied in size and mobility, and were found only in patients without symptoms of an active infection [8]
Statistical Analysis
Statistical analyses were conducted using Statistica v. 13.3 (TIBCO Software Inc.). Categorical variables were expressed in numbers and percentages, whereas continuous variables as either the mean and standard deviation (SD) or median depending on variable distribution. The variables were compared using the nonparametric Chi2 test with Yates correction (dichotomous data) or the unpaired Mann-Whitney U test (continuous data), as appropriate. Receiver operating characteristic (ROC) curve analysis was used to assess the value of laboratory markers in predicting the development of LRIE and the presence of vegetation. Optimal cut-off levels were determined, and their sensitivities and specificities were calculated. A p-value less than 0.05 was considered statistically significant.
Approval of the Bioethics Committee
The study was conducted according to the ethical guidelines of the Declaration of Helsinki and approved by the Bioethics Committee at the Regional Chamber of Physicians in Lublin no. 288/2018/KB/VII.
Results
The study group consisted of 2909 patients (mean age 69 years; 46.06% female). Infectious indications for TLE occurred in 1029 (36.37%) patients, while TLE for non-infectious reasons was performed in 1880 (64.63%) patients. There were 296 patients (10.18%) with isolated PI and 733 patients (25.20%) with LRIE (with and without PI) in the infectious group. The group of patients with vegetation consisted of 507 patients (17.43%) and the group with vegetation-like masses consisted of 117 patients (4.02%) (Table 1).
Patients undergoing TLE for infectious reasons were older, more often male, had a lower left ventricular ejection fraction (LVEF), and had a higher incidence of comorbidities. Comparison of laboratory parameters showed a significantly higher level of leukocytes and neutrophils with lower lymphocyte values (along with higher NLR and LPR) in patients with CIED-related infections compared with the non-infectious group. The level of platelets was comparable in both study groups. Significantly higher levels of ESR and CRP were found in infectious patients with comparable procalcitonin values (Table2).
The receiver operating characteristic (ROC) curve analysis for infectious process in patients with CIED showed the highest area under curve (AUC) for CRP (0.77; p<0,001) followed by WBC (0.61; p < 0.001), NLR (0.59; p < 0.001) and NPR (0.56; p < 0.001). The sensitivity and specificity for CRP was 72.66% and 70.62%; for WBC: 42.73% and 74.86%; for NLR: 40.54% and 72.82%; for NPR: 31.98% and 79.47% respectively (Figure 2).
Comparison of hematological parameters in patients referred to TLE for non-infectious and infectious reasons in whom the presence of additional intracardiac structures was demonstrated showed significantly higher NLR (3.37 vs 2.61), NLR% (3.39 vs 2.61), NPR (0.03 vs 0.02), ESR (30.00 vs 10.50 mm/h), and CRP (32.58 vs 3.00 mg/l) parameters in patients with vegetation compared with the group with vegetation-like masses (Table 3).
The areas under the curve of the CRP, WBC, NLR and NPR for prediction of vegetation was: 0.80 (p<0.01), 0.65 (p<0.01), 0,65 (p<0.01) and 0.60 (p<0.01) respectively. The highest sensitivity was shown for CRP (79.71%), and the highest specificity was found for NPR (82.78%) (Figure 3).
Comparison of the hematological markers in patients with LRIE and isolated pocket infection showed significantly higher NLR (4.11 vs 2.55) and NLR% (4,24 vs 2.56), higher NPR (0.03 vs 0.02), lower LPR% (0.08 vs 0.12), and higher standard inflammatory markers – maximal CRP (65.00 vs 7.30 mg/l), ESR (45.50 vs 15.00 mm/h), and procalcitonin (0.23 vs 0.08) in the LRIE group (Table 4).
The results of the ROC curve analysis for isolated pocket infection showed the highest AUC for CRP (0.67; p<0.001) and lower AUC for WBC, NLR and NPR (respectively: 0.53; p=0.08, 0.51; p=0.78 and 0.51; p=0.68). The sensitivity and specificity of CRP was 64,45% and 63,13% (Figure 4A).
The ROC curve analysis for coexistence LRIE with PI showed higher AUC for all analyzed parameters compared with isolated PI: CRP-0.78; p<.,001, WBC-0.62; p<0,001, NLR-0.57; p<0,001 and NPR-0.55; p=0.008. The CRP value was characterized by the highest sensitivity in the detection of coexistence LRIE with PI- 77.49%; the highest specificity has been demonstrated for NLR-87.33%. (Figure 4B).
Discussion
Hematological parameters, including novel markers such as neutrophil-to-lymphocyte ratio or platelet-to-lymphocyte ratio, appear to have a growing significance in diagnosis and prognosis of diseases in many branches of medicine [9,10,11,12]. Currently, more and more studies suggest that NLR and NPR are inexpensive and easily accessible markers of inflammation in various infectious processes [13,14,15] and cardiovascular diseases [16,17]. The present study assessed the usefulness of the new laboratory parameters in the initial diagnosis of infection in patients with cardiac implantable electronic devices. In addition to an increase of typical inflammatory parameters, comparative analysis of clinical data of patients referred for transvenous lead extraction procedures showed significantly higher NLR and NPR markers in patients with infectious indications for TLE. The study demonstrated higher specificity of new markers in the diagnosis of CIED-related infections compared with typical inflammatory parameters (79.47% for NPR and 72.82% for NLR).
Assessment of simple hematological parameters may also be helpful in the initial differentiation of additional structures associated with lead or surrounding tissues. In our study population, the presence of vegetation-like masses was observed in 4.02% of non-infectious patients, while according to the literature, additional lead-related structures were found in up to 5-28% of asymptomatic patients with CIED [18,19,20,21]. Histopathological analysis of the removed lead confirmed the frequent occurrence of connective tissue growths and thrombi in patients without symptoms of infection as a reaction to the presence of a foreign body [22,23,24]. Due to the possibility of bacterial colonization, it is very important to exclude an active inflammatory process in patients with lead-related structures. Of course, advanced imaging techniques: l8-Fluorodeoxyglucose PET/computed tomography (FDG-PET/CT) and 99mTc-hexamethypropylene-amine oxime labelled autologous white blood cell scintigraphy (WBC SPECT) can be very helpful in detecting inflammation, but this is associated with high costs [25,26]. Meanwhile, the comparative analysis of new hematological markers in infectious patients with vegetation and non-infectious patients with the presence of vegetation-like masses, conducted in the current study, showed a high predictive value of NPR in detecting true vegetation (specificity 82.78%).
The most dangerous form of CIED-related infection is lead-related infective endocarditis. LRIE may develop in patients with pocket infection or occur in an isolated form. In patients with PI, there are often problems with assessing the extent of the infection, which may spread along the lead to the endocardium. As mentioned above, FDG-PET/CT and WBC SPECT imaging techniques can be very helpful in LRIE diagnosis; however, the use of this technique is still limited, and the need for cheap, non-invasive inflammatory parameters is increasing. Previous literature has not analyzed the usefulness of hematological parameters in the diagnosis of LRIE. One of the few studies documented that NLR could be considered a novel marker of bacteremia and/or sepsis. That study demonstrated high sensitivity (57.8%) and specificity (83.9%) of this parameter in patients with bacteremia compared to the local infectious process [27]. Another study showed the highest predictive value of NLR in the detection of infective endocarditis: AUC under the ROC curve of NLR was 0.817 (95% CI 0:794 − 0:839); the standard deviation was 0.012, and p < 0.001. Moreover, high sensitivity and specificity of the parameter was demonstrated: 69% and 88% [28]. High NLR may also predict the outcome of infective endocarditis, especially with identified bacterial pathogen [6,28,29]. However, the above-mentioned studies do not focus on LRIE. In the present study, NLR, and NPR together with standard markers (CRP, procalcitonin), were significantly higher in patients with LRIE compared with isolated PI group, which is an essential information in a diagnostic process. Among the tested parameters, the highest specificity of NLR (87.33%) in predicting the spread of the infectious process from the pocket to the endocardium was demonstrated. These results may be important in the diagnosis of lead-related infective endocarditis and contribute to further insightful diagnostics and therapy.
Limitations
The current analysis was performed retrospectively, but entry of patients' clinical data was performed prospectively, and it is not possible to redesign the study. Additionally, in the current study, a specific population of patients qualified for TLE was analyzed. To confirm the value of new hematological parameters, a comparative analysis of laboratory tests in patients before and after CIED implantation would also be advisable.
Conclusion
Neutrophil-to-lymphocyte ratio and neutrophil-to-platelet ratio are novel, cheap markers of the inflammation process in patients with cardiac implantable electronic devices. They are highly useful in a preliminary assessment of the spread of infection in patients with CIED and confirmation of diagnosis of lead-related infective endocarditis. In clinical practice, NLR and NPR should be helpful in the early stage of LRIE diagnosis in patients with pocket infection, as well as in those with suspected isolated LRIE and in patients with the presence of additional structures on the lead.
Author Contributions
MP – writing-original draft preparation; WJ – methodology, statistical study, DSS – Investigation, data curation; AP – investigation, data curation, AT – investigation, data curation, WB – investigation, DN – data curation, AK – supervision, writing-review, and editing.
Funding
No funding.
Data availability
All data underlying this study are included in the current manuscript.
Conflicts of interest
The authors declare no conflict of interest.
References
- Sandoe JA, Barlow G, Chambers JB, Gammage M, Guleri A, Howard P, Olson E, Perry JD, Prendergast BD, Spry MJ, Steeds RP, Tayebjee MH, Watkin R British Society for Antimicrobial Chemotherapy; British Heart Rhythm Society; British Cardiovascular Society; British Heart Valve Society; British Society for Echocardiography. Guidelines for the diagnosis, prevention and management of implantable cardiac electronic device infection. Rep\ort of a joint Working Party project on behalf of the BritishSociety for Antimicrobial Chemotherapy (BSAC, host organization), BritishHeart Rhythm Society (BHRS), British Cardiovascular Society (BCS), BritishHeart Valve Society (BHVS) and British Society for Echocardiography (BSE).J AntimicrobChemother. 2015; 70: 325-359.
- Polewczyk A, Jacheć W, Polewczyk AM, Tomasik A, Janion M, Kutarski A. Infectious complications in patients with cardiac implantable electronic devices: risk factors, prevention, and prognosis.Pol Arch Intern Med. 2017; 29;127:597-607.
- Uslan DZ, Sohail MR, St Sauver JL, Friedman PA, Hayes DL, Stoner SM, Wilson WR, Steckelberg JM, Baddour LM. Permanent pacemaker and implantable cardioverter defibrillator infection: a population-based study. Arch Intern Med 2007; 167:669–675.
- Polewczyk A, Janion M, Podlaski R, Kutarski A. Clinical manifestations of lead-dependent infective endocarditis: analysis of 414 cases Eur J Clin Microbiol Infect Dis 2014; 33:1601–1608.
- Wyllie D. H., Bowler I. C., Peto T. E. Relation between lymphopenia and bacteraemia in UK adults with medical emergencies. Journal of Clinical Pathology. 2004;57:950–955.
- Meshaal MS, Nagi A, Eldamaty A, Elnaggar W, Gaber M, Rizk H. Neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) as independent predictors of outcome in infective endocarditis (IE). Egypt Heart J. 2019; 18;71:13.
- Blomström-Lundqvist C, Traykov V, Erba PA, Burri H, Nielsen JC, Bongiorni MG, Poole J, Boriani G, Costa R, Deharo JC, Epstein LM, Sághy L, Snygg-Martin U, Starck C, Tascini C, Strathmore N. European Heart Rhythm Association (EHRA) international consensus document on how to prevent, diagnose, and treat cardiac implantable electronic device infections—endorsed by the Heart Rhythm Society (HRS), the Asia Pacific Heart Rhythm Society (APHRS), the Latin American Heart Rhythm Society (LAHRS), International Society for Cardiovascular Infectious Diseases (ISCVID), and the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS) European Heart Journal (2020) 41, 2012–2032.
- Nowosielecka D, Jacheć W, Polewczyk A, Tułecki Ł, Kleinrok A, Kutarski A. The role of transesophageal echocardiography in predicting technical problems and complications of transvenous lead extractions procedures. Clin Cardiol. 2021; 44:1233-1242.
- Neul-Bom Y, Choonhee S, Soo-Jung U. Role of the Neutrophil-Lymphocyte Count Ratio in the Differential Diagnosis between Pulmonary Tuberculosis and Bacterial Community-Acquired Pneumonia. Ann Lab Med 2013;33:105-110.
- Ishizuka M, Shimizu T, Kubota K. Neutrophil-to-Lymphocyte Ratio Has a Close Association With Gangrenous Appendicitis in Patients Undergoing Appendectomy. Int Surg 2012;97:299–304.
- Kahramanca S, Ozgehan G, Seker D, Gökce EI, Seker G, Tunç G, Küçükpınar T, Kargıcı H. Neutrophil-to-lymphocyte ratio as a predictor of acute appendicitis. Ulus Travma Acil CerrahiDerg 2014;20:19-22.
- Kekilli M, Tanoglu A, Sakin YS, Kurt M, Ocal S, Bagci S. Is the neutrophil to lymphocyte ratio associated with liver fibrosis in patients with chronic hepatitis B? World J Gastroenterol 2015; 14; 21: 5575-558.
- de Jager CP, van Wijk PT, Mathoera RB, de Jongh-Leuvenink J, van der Poll T, Wever PC.Lymphocytopenia and neutrophil-lymphocyte count ratio predict bacteremia better than conventional infection markers in an emergency care unit. Crit Care. 2010;14:R192.
- Gharebaghi N, ValizadeHasanloei MA, MedizadehKhalifani A, Pakzad S, Lahooti D. Neutrophil-to-lymphocyte ratio in patients with gram-negative sepsis admitted to intensive care unit. AnaesthesiolIntensiveTher. 2019;51:11-16.
- Naess A, Nilssen SS, Mo R, Eide GE, Sjursen H. Role of neutrophil to lymphocyte and monocyte to lymphocyte ratios in the diagnosis of bacterial infection in patients with fever. Infection. 2017 ;45:299-307.
- Afari ME, Bhat T. Neutrophil to lymphocyte ratio (NLR) and cardiovascular diseases: an update. ExpertRevCardiovascTher. 2016;14:573-7.
- Hong D, Choi KH, Song YB, Lee JM, Park TK, Yang JH, Hahn JY, Choi JH, Choi SH, Kim SM, Choe Y, Kim EK, Chang SA, Lee SC, Oh JK, Gwon HC. Prognostic implications of post-percutaneous coronary intervention neutrophil-to-lymphocyte ratio on infarct size and clinical outcomes in patients with acute myocardial infarction. Sci Rep. 2019; 4;9:9646.
- Lo R, D’AncaM, Cohen T, Kerwin T. Incidence and prognosis of pacemaker lead-associated masses: a study of 1,569 transesophageal echocardiograms. J Invasive Cardiol 2006; 18:599–601.
- Downey BC, Juselius WE, Pandian NG, et al. Incidence and significance of pacemaker and implantable cardioverter-defibrillator lead masses discovered during transesophageal echocardiography. Pacing Clin Electrophysiol 2011; 34:679–683.
- Dundar C, Tigen K, Tanalp C, et al. The prevalence of echocardiographic accretions on the leads of patients with permanent pacemakers. J Am Soc Echocardiogr 2011; 24:803–807.
- Golzio PG, Errigo D, Peyracchia M, Gallo E, Frea S, Castagno D, Budano C, Giustetto C, Rinaldi M. Prevalence and prognosis of lead masses in patients with cardiac implantable electronic devices without infection. J Cardiovasc Med (Hagerstown). 2019;20:372-378.
- Kołodzińska A, Kutarski A, Koperski Ł, Grabowski M, Małecka B, Opolski G. Differences in encapsulating lead tissue in patients who underwent transvenous lead removal. Europace 2012;14 :994-1001.
- Kolodzińska K, Kutarski A, Grabowski M, Jarzyna I, Małecka B, Opolski G. Abrasions of the outer silicone insulation of endocardial leads in their intracardiac part: a new mechanism of lead-dependent endocarditis. Europace.2012;14:903-10.
- Novak M, Dvorak P, Kamaryt P, Slana B, Lipoldova J.Autopsy and clinical context in deceased patients with implanted pacemakers and defibrillators: intracardiac findings near their leads and electrodes. Europace. 2009;11:1510-6.
- Rodríguez-Alfonso B, Mitjavila Casanovas M, Castro Urda V, Cobo Marcos M, Sánchez Romero I, Ramos-Martínez A. PET/CT with 18 F-FDG in suspected intracardiac device-related infections: analysis of performance and diagnostic usefulness. Rev Esp Cardiol 2021;74:238-246.
- Erba PA, Sollini M, Conti U, Bandera F, Tascini C, De Tommasi SM, Zucchelli G, Doria R, Menichetti F, Bongiorni MG, Lazzeri E, Mariani G. Radiolabeled WBC scintigraphy in the diagnostic workup of patients with suspected device-related infections. JACC Cardiovasc Imaging 2013; 6:1075–1086.
- Gürol G, Çiftci İH, Terizi HA, Atasoy AR, Ozbek A, Köroğlu M. Are There Standardized Cutoff Values for Neutrophil-Lymphocyte Ratios in Bacteremia or Sepsis? J. Microbiol. Biotechnol. 2015, 25, 521–525.
- Chen Y, Ye LJ, Wu Y, Shen BZ, Zhang F, Qu Q, Qu J. Neutrophil-Lymphocyte Ratio in Predicting Infective Endocarditis: A Case-Control Retrospective Study Mediators Inflamm 2020; 27;2020:8586418.
- Bozbay M, Ugur M, Uyarel H, Cicek G, Koroglu B, Tusun E, Sunbul M, Murat A, Sari I, Eren M. Neutrophil-to-lymphocyte ratio as a prognostic marker in infective endocarditis: in-hospital and long-term clinical results. J Heart Valve Dis 2014 ;23:617-623.
Figure 1.
Flowchart of the study population.
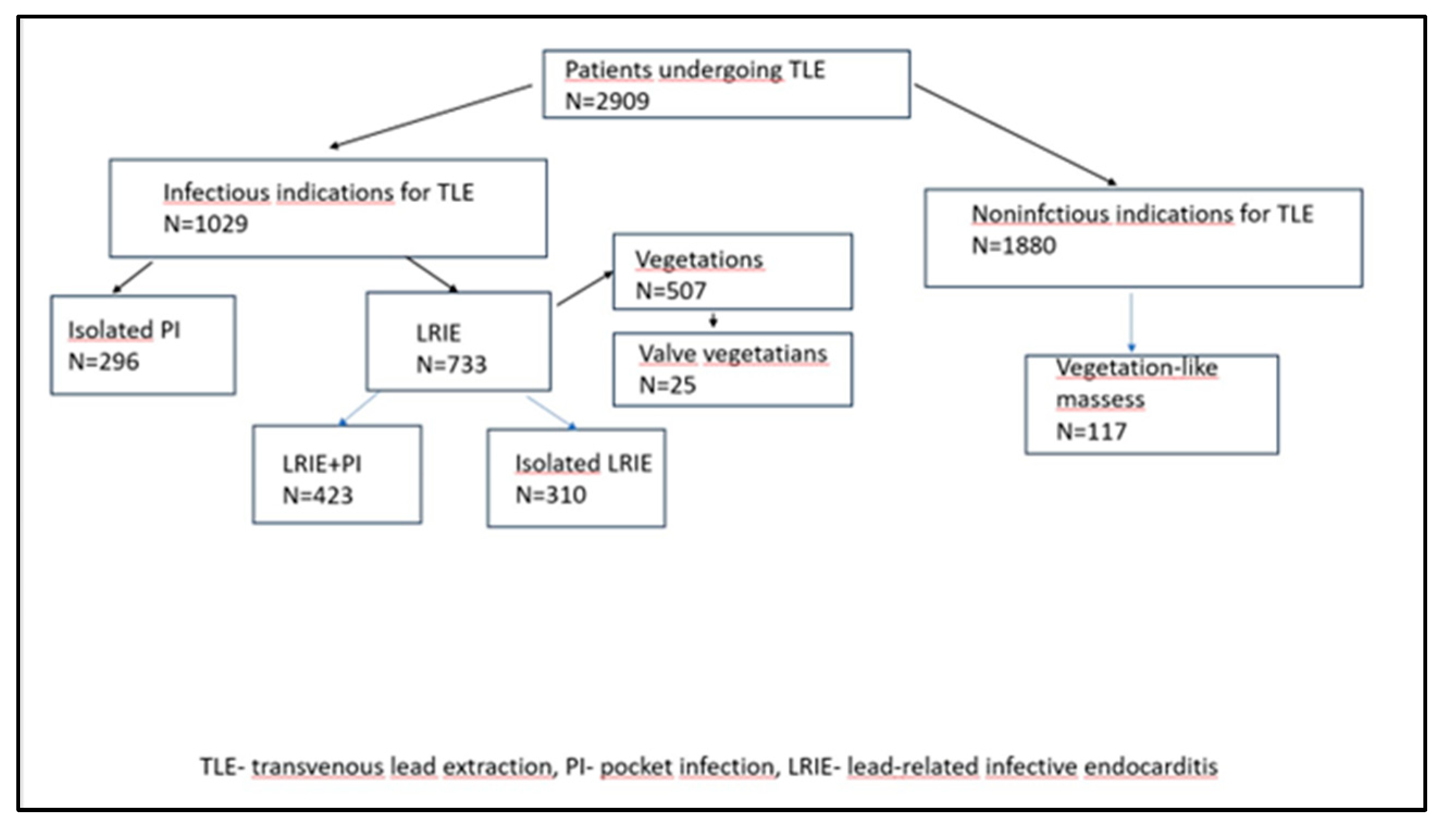
Figure 2.
Receiver operating characteristic (ROC) curve for the blood parameters according to the presence of infectious complications in patients with cardiac implantable electronic devices (CIED).
Figure 2.
Receiver operating characteristic (ROC) curve for the blood parameters according to the presence of infectious complications in patients with cardiac implantable electronic devices (CIED).
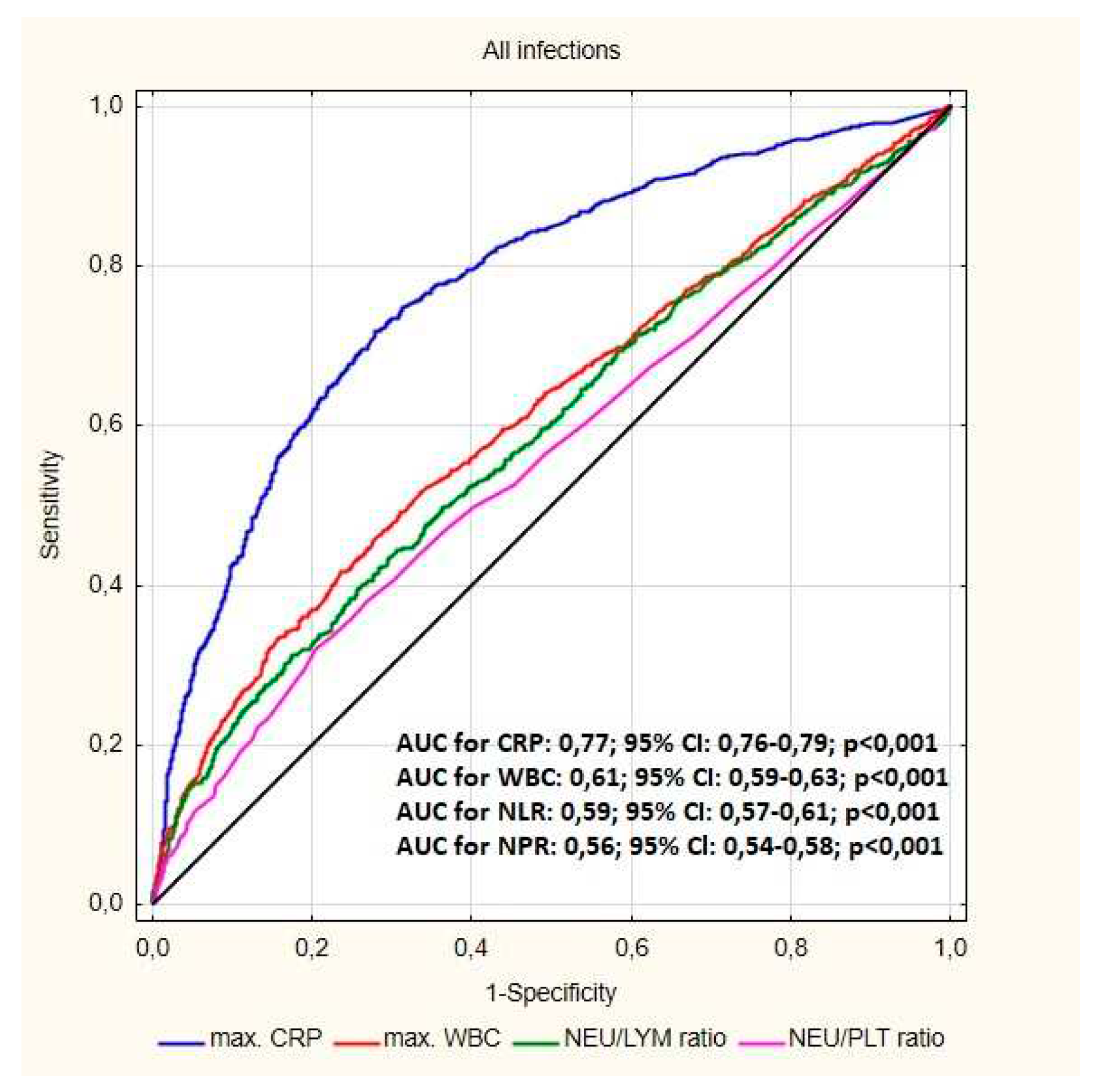
Figure 3.
Receiver operating characteristic (ROC) curve for the blood parameters according to the presence of vegetation.
Figure 3.
Receiver operating characteristic (ROC) curve for the blood parameters according to the presence of vegetation.
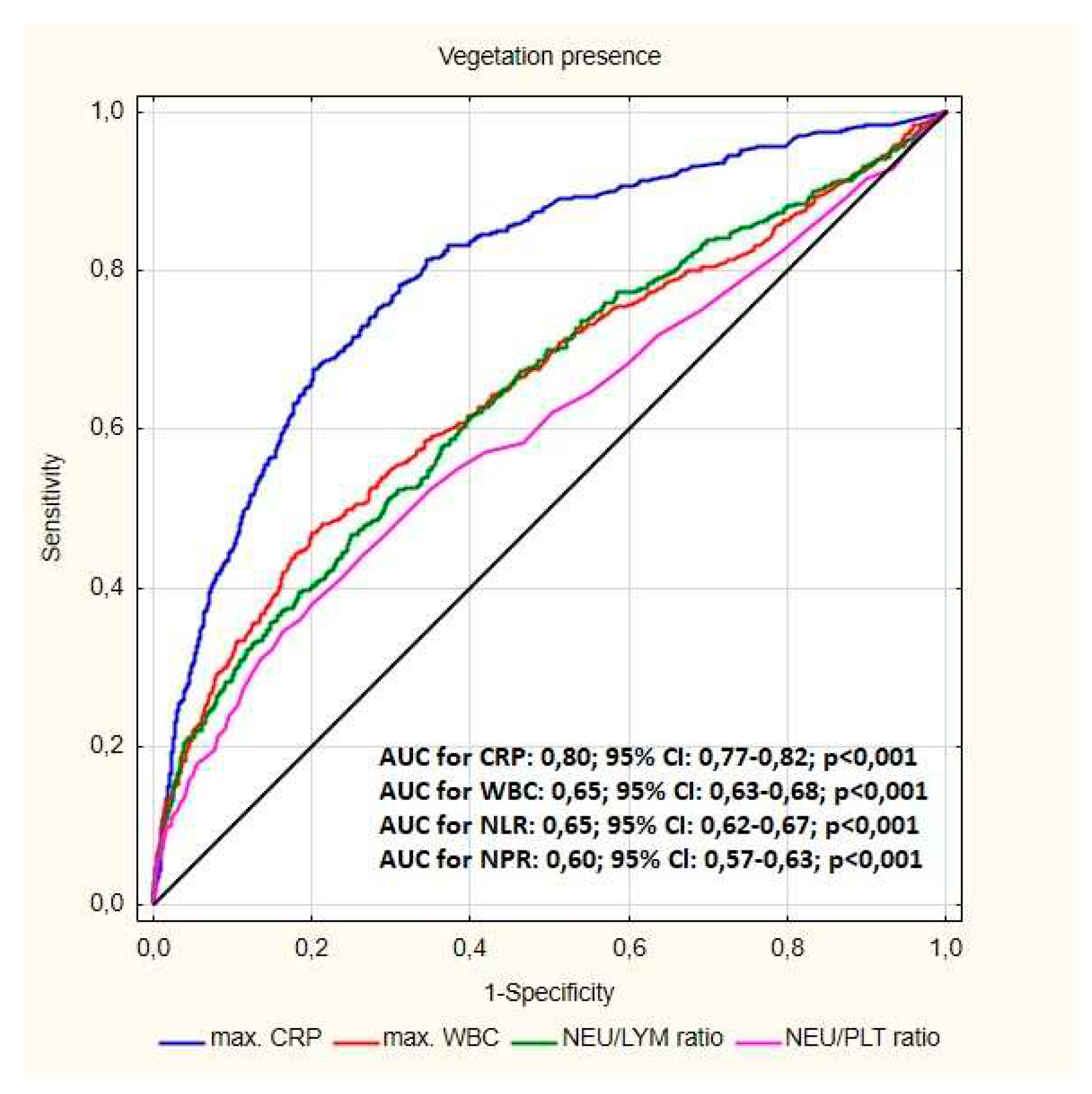
Figure 4.
A ROC curve for the blood parameters according to the presence of isolated pocket infections (PI). B ROC curve for the blood parameters according to the coexistence PI with LRIE.
Figure 4.
A ROC curve for the blood parameters according to the presence of isolated pocket infections (PI). B ROC curve for the blood parameters according to the coexistence PI with LRIE.
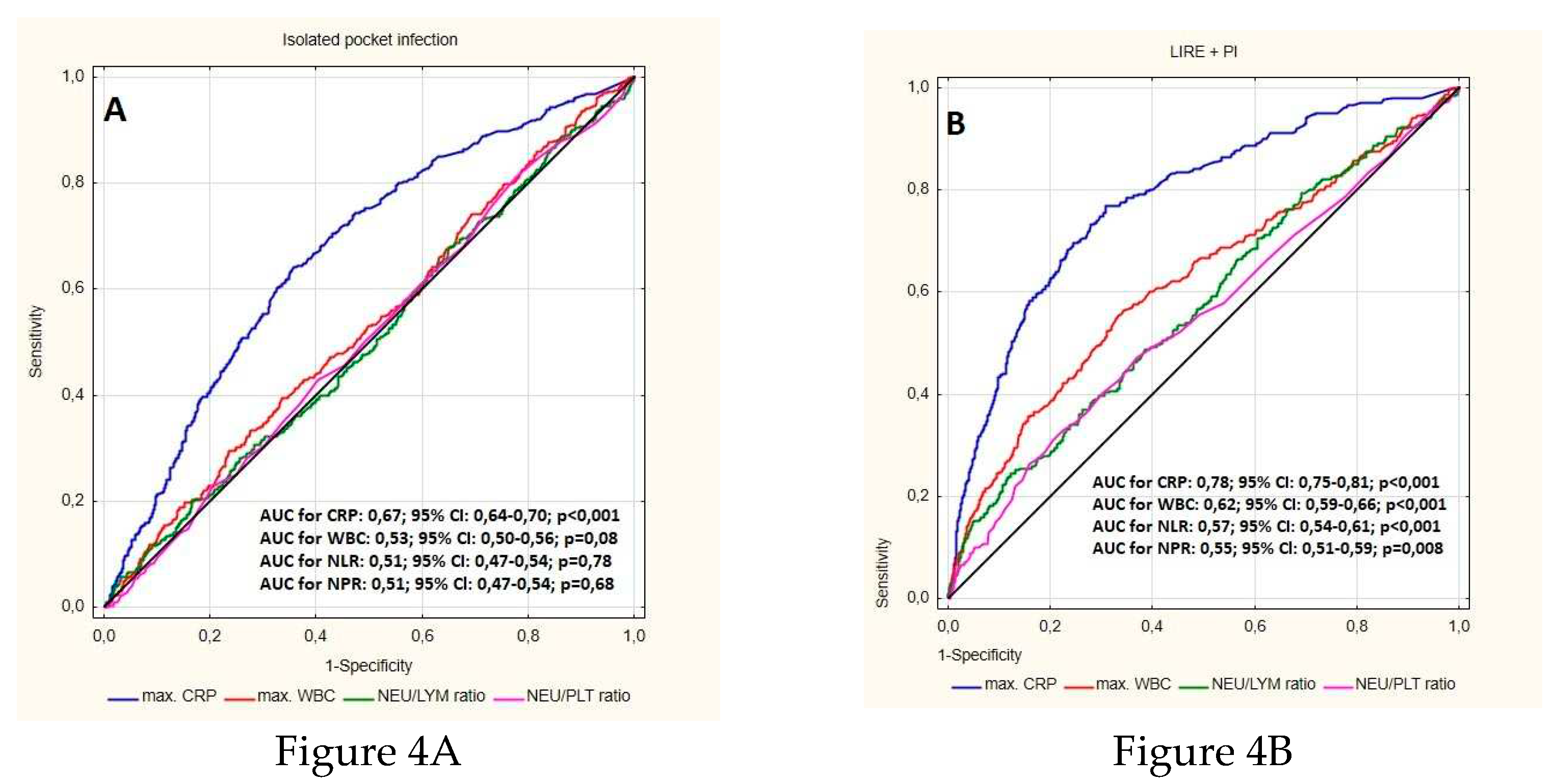
Figure 5.
Receiver operating characteristic (ROC) curve for the blood parameters according to the presence of vegetations.
Figure 5.
Receiver operating characteristic (ROC) curve for the blood parameters according to the presence of vegetations.
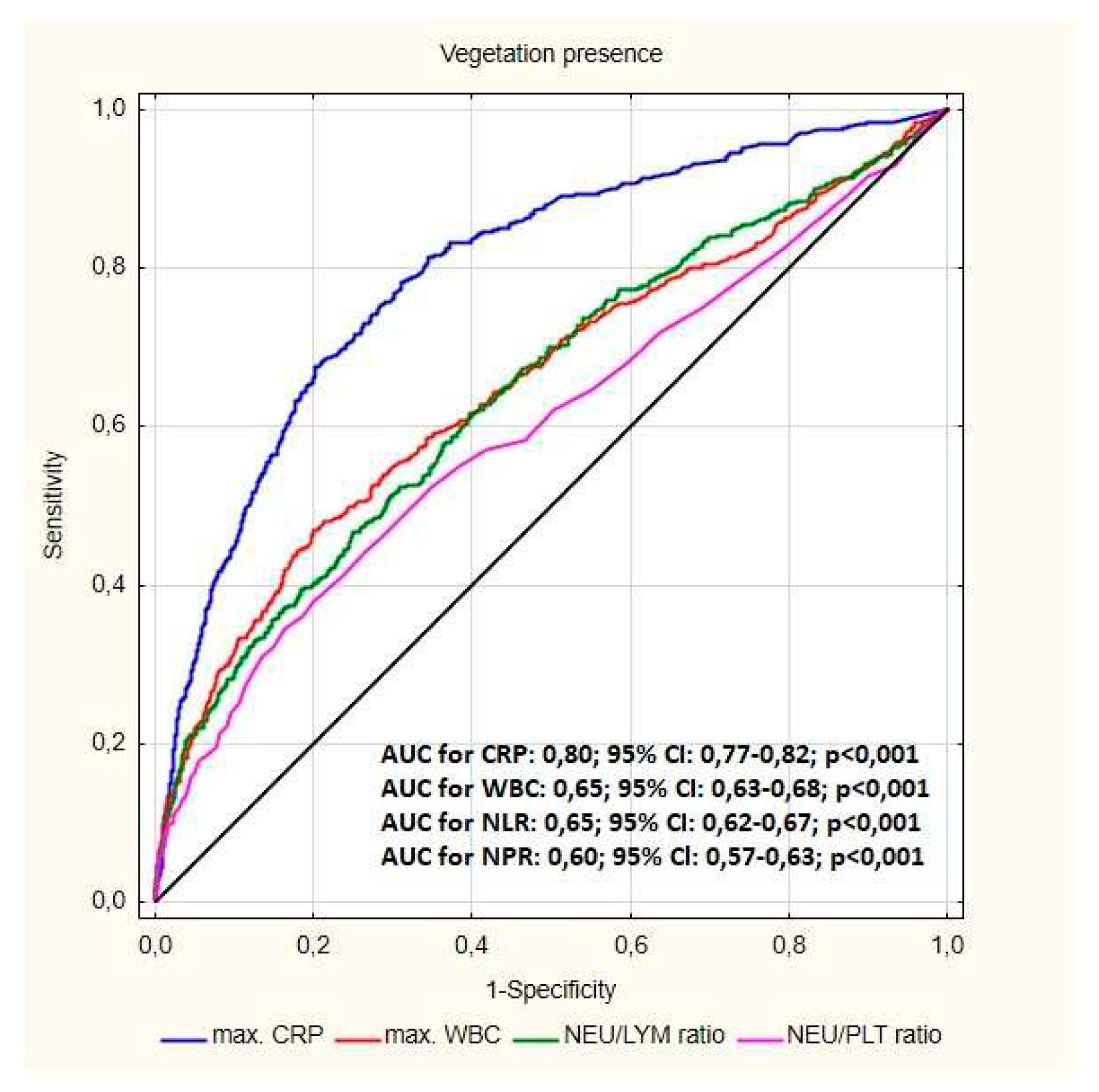

Table 1.
Characteristics of study group.
| All patients N=2909 |
|
|---|---|
| Patient’s age during TLE [years] median (Q1-Q3) | 69 (59-77) |
| Patient's age during first system implantation [years] median (Q1-Q3) | 61 (51-69) |
| Sex (% of female patients) (n, %) | 1340 (46.06) |
| LVEF [%] median (Q1-Q3) | 54 (36.00-60.00) |
| Renal failure (any) (n, %) | 885 (28.70) |
| Diabetes t.2 (n, %) | 775 (26.64) |
| Carlson's comorbidity index [number of points] median, (Q1 - Q3) | 4.00 (2.00-6.00) |
| Infectious indications for TLE (n, %) | 1029 (36.37) |
| LRIE (with and without pocket infection) (n, %) | 733(25.20) |
| Isolated pocket infections (n, %) | 296 (10.18) |
| Vegetations (n, %) | 507 (17.40) |
| Non-infectious indications for TLE (n, %) | 1880 (64.63) |
| Vegetations-like masses (n, %) | 117 (4.02) |
AF – atrial fibrillation, LRIE – lead related infective endocarditis, LVEF – left ventricle ejection fraction, MI – myocardial infarction, TLE – transvenous lead extraction.
Table 2.
Comparison of clinical and laboratory parameters in patients qualified for TLE for infectious and non-infectious causes.
Table 2.
Comparison of clinical and laboratory parameters in patients qualified for TLE for infectious and non-infectious causes.
| Infectious indications for TLE N=1029 |
Non-infectious indications for TLE N=1880 |
p | |
|---|---|---|---|
| Patient’s age during TLE [years] median (Q1-Q3) | 70(61-78) | 68(58-76) | <0.001 |
| Patient's age during first system implantation [years] median (Q1-Q3) | 63(54-71) | 60(48-68) | <0.001 |
| Sex (% of female patients) (n, %) | 306 (29.74) | 828(44.04) | 0.001 |
| LVEF [%] median (Q1-Q3) | 50 (36.00.00-60) | 55(35.00-60.00) | <0.001 |
| Renal failure (any) (n, %) | 271(26.34) | 352 (18.72) | <0.001 |
| Diabetes t.2 (n, %) | 232(22.55) | 332 (17.66) | <0.001 |
| Carlson's comorbidity index [number of points] median, (Q1 - Q3) | 4.00(3.00-7.00) | 4.00(2.00-5.50) | <0.001 |
| Hemoglobin (g/dl) (lowest) (mean, SD) | 12.5(11.0-13.30) | 13.30(12.10-14.40) | <0.001 |
| Hematocrit (%) (lowest) median (Q1-Q3) | 37.20(33.00-40.90) | 39.90(36.20-42.90) | <0.001 |
| Platelets/ul (lowest) median Q1-Q3) |
210.0(164.0-272.0) | 197.0(160.0-241.0) | 0.420 |
| Max WBC/ul (mean.SD) | 8185(6600-10360) | 7210(6070-8630) | 0.032 |
| Neutrophil count/ul (max) median (Q1-Q3) | 5.29(3.90-7.40) | 4.30(3.50-5.50) | 0.018 |
| Neutrophil % median (Q1-Q3) |
66.15(58.60-74.00) | 62.90(56.60-69.10) | 0.002 |
| Lymphocyte count/ul (max) median (Q1-Q3) | 1.60(1.30-2.30) | 1.70(1.30-2.19) | <0.001 |
| Lymphocyte% median (Q1-Q3) |
22.30(16.20-29.10) | 24.60(19.20-30.50) | <0.001 |
| Max ESR (mm/h) median (Q1-Q3) |
25.00(1.00-50.00) | 11.00(6.00-20.00) | <0.001 |
| Max CRP (mg/dl) median (Q1-Q3) |
17.57(5.07-60.40) | 2.00(0.60-7.17) | <0.001 |
| Max Procalcitonin (ug/L) median (Q1-Q3) |
0.10(0.06-0.30) | 0.07(0.04-0.125) | 0.154 |
| NLR median (Q1-Q3) | 3.07(2.12-4.91) | 2.59(1.86-3.57) | <0.001 |
| NLR % median (Q1-Q3) | 3.07(2.12-4.84) | 2.57(1.86-3.58) | <0.001 |
| NPR median (Q1-Q3) | 0.02(0.02-0.04) | 0.01(0.01-0.03) | 0.008 |
| LPR % median (Q1-Q3) | 0.10(0.07-0.15) | 0.13(0.10-0.17) | 0.001 |
| LPR (median IQR) | 0.01(0.01-0.01) | 0.01(0.01-0.01) | 0.003 |
Abbreviations: CRP – C-reactive protein, ESR – Erythrocyte Sedimentation Rate, LPR – lymphocyte-to-platelet ratio, LRIE – lead related infective endocarditis, NLR – neutrophil-to-lymphocyte ratio, NPR – neutrophil-to-platelet ratio, WBC – white blood cells.
Table 3.
Comparison of hematological parameters of patients with vegetation-like masses and patients with vegetation.
Table 3.
Comparison of hematological parameters of patients with vegetation-like masses and patients with vegetation.
| Parameters | Presence of vegetation-like masses | Presence of vegetations | p |
|---|---|---|---|
| Hemoglobin (mg/dl) (lowest) median (Q1-Q3) | 13.70 (11.90-14.70) | 11.90 (10.30-13.20) | <0.001 |
| Hematocrit (%) (lowest) median (Q1-Q3) | 40.20 (36.00-43.90) | 35.90 (31.20-39.70) | <0.001 |
| Platelets/ul (lowest) median (Q1-Q3) | 200.0 (163.0-252.0) | 215.0 (157.0-278.0) | 0.063 |
| MaxWBC/ul median (Q1-Q3) | 7440 (6060-8640) | 8880 (7000-11400) | <0.001 |
| Neutrophil count /ul(max) median (Q1-Q3) | 4.50 (3.56-5.54) | 5.70 (4.10-8,30) | <0.001 |
| Neutrophil % median (Q1-Q3) | 63.40 (54.80-69.80) | 67.70 (60.40-76.20) | <0.001 |
| Lymphocyte count/ul(max) median (Q1-Q3) | 1.65 (1.38-2.10) | 1.60 (1.20-2.20) | 0.927 |
| Lymphocyte% median (Q1-Q3) | 24.30 (18.70-31.90) | 19.80 (13.60-26.10) | <0.001 |
| Max ESR (mm/h)median (Q1-Q3) | 10.50 (5.00-19.50) | 30.00 (13.00-54.00) | <0.001 |
| MaxCRP (mg/dl) median (Q1-Q3) | 3.00 (0.67-10.75) | 32.58 (9.30-90.00) | <0.001 |
| Max Procalcitonin (ug/L)median (Q1-Q3) | 0.05 (0.04-1,52) | 0.12(0,07-0.50) | 0.581 |
| NLR median (Q1-Q3) | 2.61 (1.72-3.67) | 3.37 (2.35-5.55) | <0.001 |
| NLR % median (Q1-Q3) | 2.61 (1.70-3,81) | 3.39 (2,37-5.56) | <0.001 |
| NPR median (Q1-Q3) | 0.02 (0.02-0.03) | 0.03 (0.02-0,04) | 0..008 |
| LPR % median (Q1-Q3) | 0.13 (0.09-0.18) | 0.09 (0.06-0,14) | 0.025 |
| LPR median (Q1-Q3) | 0.01(0.01-0.01) | 0.01 (0.01-0.01) | 0.937 |
Abbreviations: CRP – C-reactive protein, ESR – Erythrocyte Sedimentation Rate, LPR – lymphocyte-to-platelet ratio; LRIE – lead related infective endocarditis NLR – neutrophil-to-lymphocyte ratio, NPR – neutrophil-to-platelet ratio, WBC – white blood cells.
Table 4.
Hematological parameters of patients undergoing TLE due to LRIE and isolated PI.
| Parameters | LRIE | Isolated pocket infection | p |
|---|---|---|---|
| Hemoglobin (g/dl) (lowest) median (Q1-Q3) | 11.90 (10.50-13.30) | 13.20 (12.00-14.30) | <0.001 |
| Hematocrit (%) (lowest) median (Q1-Q3) | 33.95 (29.15-37.80) | 39.30 (35.90-42.10) | <0.001 |
| Platelets /ul(lowest) median (Q1-Q3) | 222.0 (159.0-293.0) | 202.00 (166.0 -250.5) | 0.001 |
| MaxWBC/ul (mean.SD) | 10100 (7550-13300) | 7370(6280-8900) | <0.001 |
| Neutrophil count/ul (max) median (Q1-Q3) | 6.80 (4.65-9.50) | 4.40 (3.60-5.80) | <0.001 |
| Neutrophil % median (Q1-Q3) | 71.10 (63.75-78.45) | 62.75 (56.25-70.50) | <0.001 |
| Lymphocyte count/ul (max) median (Q1-Q3) | 1.60 (1.02-2.2.0) | 1.70 (1.30-2.29) | 0.93 |
| Lymphocyte% median (Q1-Q3) | 17.00(11.45-23.30) | 24.70 (18.80-30.30) | <0.001 |
|
Max ESR (mm/h) median (Q1-Q3) |
44.50 (22.00-68.00) | 15.00 (8.00-30.00) | <0.001 |
| MaxCRP (mg/dl ) median (Q1-Q3) | 65.00 (24,70-120.7) | 7.30 (2.20-19.20) | <0.001 |
| Max Procalcitonin (ug/L)median (Q1-Q3) | 0.23 (0.10-1.53) | 0.08 (0.05-0.10) | 0.03 |
| NLR median (Q1-Q3) | 4.11 (2.72-6.98) | 2.55 (1.85-3.70) | <0.001 |
| NLR % median (Q1-Q3) | 4.24 (2.75-6.93) | 2.56 (1.87-3.73) | <0.001 |
| NPR median (Q1-Q3) | 0.03 (0.02-0.05) | 0.02 (0.02-0.03) | <0.001 |
| LPR % median (Q1-Q3) | 0.08 (0.05-0.11) | 0.12 (0.08-0.16) | 0.001 |
| LPR median (Q1-Q3) | 0.01 (0.00-0.01) | 0.01 (0.01-0.01) | 0.41 |
Abbreviations: CRP – C-reactive protein, ESR – Erythrocyte Sedimentation Rate, LPR – lymphocyte-to-platelet ratio; LRIE – lead related infective endocarditis, NLR – neutrophil-to-lymphocyte ratio, NPR – neutrophil-to-platelet ratio, WBC – white blood cells.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



