
Submitted:
03 November 2023
Posted:
06 November 2023
You are already at the latest version
Abstract
This comprehensive review delves into the intricate relationship between Sodium-GlucoseCo-Transporter 2 (SGLT2) inhibitors and AF, highlighting the multifaceted actions of thesedrugs and their significant cardiovascular benefits. Mechanisms: SGLT2 inhibitors inducesubstantial hemodynamic changes, impacting blood pressure, adipose tissue function, andinflammation. They enhance glycemic control while potentially reducing oxidative stress andinflammation, and they modulate atrial electrophysiology, collectively contributing to the reductionof AF risk. Clinical Evidence: This review synthesizes a wealth of clinical evidence,drawing from observational studies and randomized controlled trials, consistently demonstratinga correlation between SGLT2 inhibitors, particularly dapagliflozin and empagliflozin, anda decreased risk of AF. This protective effect is most pronounced in patients with type 2 diabetesand heart failure, underscoring their potential as therapeutic agents for high-risk populations.Potential Benefits: SGLT2 inhibitors offer a spectrum of potential benefits, includingsubstantial reductions in AF risk, particularly in patients with type 2 diabetes and heart failure.These drugs have consistently demonstrated benefits in reducing heart failure hospitalizations,cardiovascular mortality, and stroke risk, which indirectly contribute to better AF management.Furthermore, SGLT2 inhibitors exhibit renoprotective properties by slowing theprogression of chronic kidney disease and reducing albuminuria, offering substantial benefitsfor AF patients with comorbid kidney disease. Metabolic improvements involving weight loss,blood pressure reduction, and favorable changes in lipid profiles contribute to enhanced cardiovascular health and reduced AF risk. Originally designed for diabetes management, thesemedications offer a holistic approach to AF risk reduction, particularly in patients with type 2diabetes and heart failure.
Keywords:
Atrial fibrillation
; SGLT2 inhibitors
; cardiovascular outcomes
; hemodynamic effects
; AF risk reduction
Introduction
- Overview of Atrial Fibrillation (AF):
Atrial fibrillation (AF) is a common cardiac arrhythmia associated with adverse outcomes such as stroke, heart failure, and mortality [1]. It can occur in various clinical contexts, including as an isolated condition or in conjunction with other cardiovascular diseases [2]. Understanding the epidemiology, pathophysiology, and clinical implications of AF is crucial for effective cardiovascular care [3]. AF is characterized by irregular and often rapid heart rate, leading to ineffective atrial contractions [4]. Catheter ablation has emerged as an important treatment strategy for symptomatic AF, with increasing use in more complex cases [5]. Idiopathic ventricular fibrillation is a rare condition characterized by abrupt onset ventricular fibrillation in the absence of known cardiac, respiratory, or metabolic causes. AF after coronary artery bypass grafting is associated with long-term cardiovascular complications, including increased incidence of AF, ischemic stroke, heart failure, and mortality [6].
- Role of SGLT2 Inhibitors in Cardiovascular Disease Management
Sodium-glucose co-transporter 2 (SGLT2) inhibitors have demonstrated remarkable cardiovascular benefits in individuals with type 2 diabetes mellitus (T2DM), with or without a history of cardiovascular disease. These medications have shown efficacy in reducing major adverse cardiovascular events and improving heart failure outcomes. Studies have shown that SGLT2 inhibitors can reduce blood pressure, weight, and body mass index in individuals without diabetes, heart failure, and/or chronic kidney disease [7].
SGLT2 inhibitors have multiple mechanisms of action beyond glycemic control. These drugs not only reduce glucose reabsorption in the kidneys, but also improve glycemic control, blood pressure, and body weight [8,9]. They have been shown to have potential cardiac and renal protection [10]. SGLT2 inhibitors improve cardiovascular outcomes by increasing the bioavailability of nitric oxide, restoring endothelium-dependent vasodilation, and regulating the proliferation, migration, and survival of endothelial cells [11]. They also exert antioxidant and anti-inflammatory effects in endothelial cells and inhibit the contraction, proliferation, and migration of vascular smooth muscle cells [12]. Additionally, SGLT2 inhibitors have been shown to reduce cortical hypoxia, decrease intraglomerular hypertension, and increase glomerular filtration rate, leading to a decrease in nephropathy incidence and severity [13]. These drugs also have an effect on lipid metabolism, decreasing lipid accumulation and shifting substrate utilization from carbohydrates to lipids and ketone bodies [11].
As we delve deeper into the complex interplay between AF and SGLT2 inhibitors, it becomes evident that this relationship is multifaceted and extends beyond traditional antidiabetic properties. This comprehensive review seeks to explore and elucidate this intricate association, focusing on various aspects such as mechanisms, clinical implications, potential therapeutic applications, and areas that warrant further research.
The purpose of this review is to provide clinicians, researchers, and healthcare practitioners with a thorough understanding of the interrelationship between SGLT2 inhibitors and AF. By examining the mechanisms that underlie this relationship, summarizing the available clinical evidence, and discussing potential benefits and risks, this review aims to contribute to a more nuanced approach to managing AF in patients receiving SGLT2 inhibitors. Furthermore, we address important considerations for patient care and highlight areas that require further investigation to enhance the overall cardiovascular health of individuals with AF.
- Mechanisms Underlying the Relationship:
Understanding the intricate relationship between Sodium-Glucose Co-Transporter 2 (SGLT2) inhibitors and atrial fibrillation (AF) requires an exploration of the underlying mechanisms that connect these two phenomena. This section is divided into three subsections for clarity, each delving into specific aspects of the mechanistic pathways involved.
- Hemodynamic Effects:
SGLT2 inhibitors have been shown to induce significant hemodynamic changes that can impact the development and progression of AF. The mechanisms contributing to these effects include reductions in blood pressure and improvements in adipose tissue function and inflammation [14]. In addition, SGLT2 inhibitors have been found to reduce body weight and adipose tissue mass while maintaining stable lean tissue parameters [15]. These drugs may also have an anti-inflammatory effect, as evidenced by reductions in cytokine and chemokine concentrations [16]. Furthermore, SGLT2 inhibitors have been shown to improve the circadian rhythm of blood pressure, potentially contributing to their cardioprotective effects [17]. While the direct impact of SGLT2 inhibitors on the cardiovascular system and their specific mechanisms of action are still being investigated, these drugs have demonstrated significant cardiovascular benefits in patients with type 2 diabetes [18].
- 1.Blood Pressure Modulation:
GLT2 inhibitors have consistently shown reductions in systolic and diastolic blood pressure, which may have potential benefits in reducing the likelihood of atrial fibrillation (AF) initiation and maintenance [19,20]. These inhibitors have been found to improve cardiovascular outcomes and prevent progression of renal dysfunction in patients with type 2 diabetes mellitus (T2DM) [21,22]. Additionally, SGLT2 inhibitors have demonstrated beneficial effects on morning, evening, and nocturnal home blood pressure, as well as reductions in arterial stiffness. [23] These agents have also been associated with a decrease in the apnea-hypopnea index in patients with obstructive sleep apnea [24]. The use of SGLT2 inhibitors has shown favorable effects in patients with heart failure (HF), including reduced HF with reduced or preserved ejection fraction, and chronic kidney disease. These findings suggest that SGLT2 inhibitors may have a role in blood pressure modulation and potentially reducing the risk of AF [25,26,27].
- 2.Reduction in Extracellular Volume:
SGLT2 inhibitors, such as ipragliflozin, empagliflozin, and dapagliflozin, have been shown to reduce extracellular volume in patients with type 2 diabetes mellitus (T2DM) [28,29,30]. These drugs promote natriuresis and diuresis, leading to a decrease in fluid volume [31]. The reduction in extracellular volume can have beneficial effects on atrial dilation and structural remodeling, potentially reducing the substrate for atrial fibrillation (AF) [32]. SGLT2 inhibitors, such as ipragliflozin and empagliflozin, have shown potential cardiovascular benefits in patients with type 2 diabetes mellitus (T2DM). Ipragliflozin treatment over 24 months significantly reduced estimated plasma volume and estimated extracellular volume [33]. Empagliflozin treatment resulted in a decrease in cardiac adipose tissue volume and improvements in myocardial structure and function [34]. These findings suggest that SGLT2 inhibitors may have clinical cardiovascular benefits by reducing extracellular volume and improving atrial remodeling, potentially reducing the risk of atrial fibrillation (AF).
- Electrophysiological Changes:
Alterations in cardiac electrophysiology play a crucial role in the development of AF. SGLT2 inhibitors may influence these changes through various mechanisms:
- 1. Atrial Repolarization:
Interestingly, SGLT-2 inhibitors have been shown to have a shortening effect on the QT interval, indicating a potential reduction in ventricular repolarization time [35].
SGLT-2 inhibitors have beneficial effects on ventricular repolarization through various mechanisms. These include the reduction of QT interval and Tp-e interval, as well as the decrease in Tp-e/QT and Tp-e/QTc ratios [35]. The favorable effects on ventricular repolarization indices are observed in patients with type 2 diabetes mellitus who are using SGLT2 inhibitors as an add-on therapy to metformin [36] The mechanisms underlying these effects involve the optimization of ventricular loading conditions through diuresis and natriuresis, reduction of afterload, and improvement of vascular structure and function [37]. Additionally, SGLT2 inhibitors may regulate Na+/H+ exchange at the level of the heart and kidney and modulate adipokine production [38]. These drugs also have direct cardiac effects, including anti-inflammatory and antioxidative stress actions, modulation of ion transport mechanisms, and improvement of metabolic and mitochondrial pathways [39].
a recent meta-analysis has found that prolonging the corrected QT interval (QTc) by 10-ms leads to a 17% increase in the associated risk for atrial fibrillation (AF) [40]. This suggests that electrocardiographic indices of ventricular repolarization show strong predictive capabilities for the future occurrence of AF in the general population [41].
- 2. Intracellular Calcium Handling:
GLT2 inhibitors may affect intracellular calcium handling in atrial myocytes, which is implicated in both triggered and re-entry mechanisms of AF [42,43]. Studies have shown that abnormalities in intracellular calcium handling, such as altered calcium release from the sarcoplasmic reticulum (SR) and enhanced spontaneous calcium release events, can contribute to proarrhythmic cellular ectopic activity in AF [44,45]. Additionally, rapid activations in the pulmonary veins, which are important for the initiation and maintenance of AF, can also result from abnormal intracellular calcium handling and calcium overload [46]. These findings suggest that GLT2 inhibitors, by affecting intracellular calcium handling, may have an impact on the development and perpetuation of AF.
- Metabolic and Renal Factors:
Metabolic factors, particularly glucose and lipid metabolism, as well as renal function, are closely intertwined with the development of AF. SGLT2 inhibitors exert influence on these factors, potentially impacting AF in the following ways:
- 1. Glucose Control:
Improved glycemic control with SGLT2 inhibitors may indirectly reduce the risk of AF in individuals with diabetes, as hyperglycemia can promote atrial electrical and structural remodeling [47].The sodium-glucose co-transporter 2 (SGLT2) inhibitors have been shown to improve glycemic control and reduce cardiovascular events in patients with type 2 diabetes [48]. These inhibitors have also been found to improve both cardiovascular and renal outcomes when added to guideline-recommended treatment [49]. SGLT2 inhibitors have multiple effects beyond glucose control, including reducing blood pressure, weight, and arterial stiffness, as well as improving myocardial energetics and reducing oxidative stress [50]. However, it is important to note that SGLT2 inhibitors can also have unintended consequences, such as increasing the risk of diabetic ketoacidosis in some patients [51].
- 2. Lipid Profile Modification:
SGLT2 inhibitors have shown favorable effects on lipid profiles, including reductions in triglycerides and low-density lipoprotein cholesterol. These lipid modifications may contribute to reduced inflammation and oxidative stress in atrial tissue, mitigating AF risk [52,53,54].
- 3. Renal Hemodynamics:
SGLT2 inhibitors have renal effects that can impact cardiac function and atrial fibrillation (AF) risk. These inhibitors reduce glomerular filtration rate (GFR) [55] and cause natriuresis [56]. The reduction in GFR leads to a decrease in tubular transport work and metabolic demand, improving renal cortical oxygenation [57]. Additionally, SGLT2 inhibitors have been shown to lower glomerular capillary hypertension and hyperfiltration, reducing the physical stress on the filtration barrier and albuminuria [58]. These effects on the kidney may contribute to the preservation of tubular function and GFR in the long term [59]. Overall, the renal effects of SGLT2 inhibitors can have downstream consequences on cardiac function and AF risk.
- Clinical Evidence:
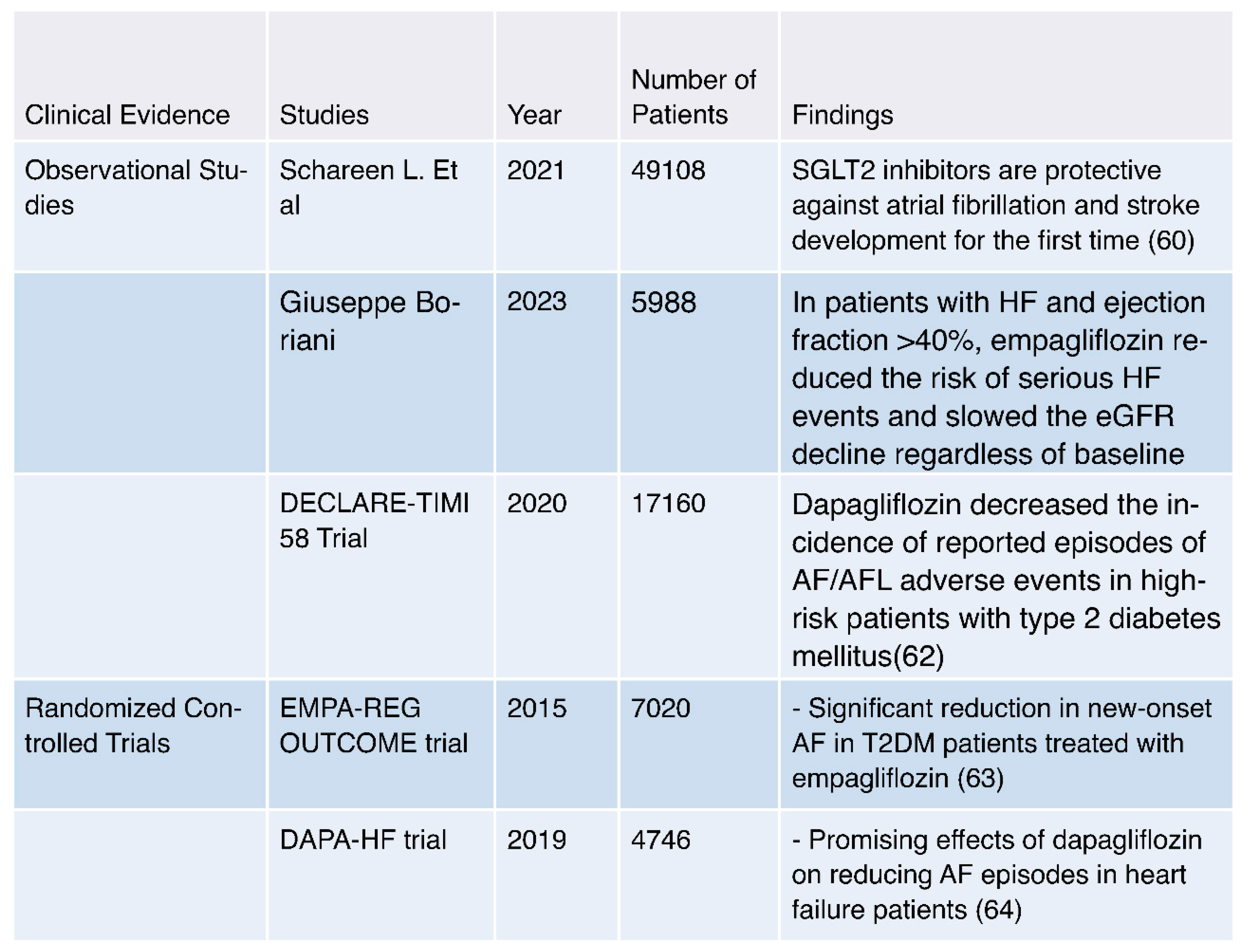
The collective body of research on the relationship between SGLT2 inhibitors and atrial fibrillation (AF) has unveiled intriguing findings with significant implications for clinical practice. Starting with Schareen L. et al.'s groundbreaking study in 2021, it was observed for the first time that SGLT2 inhibitors may possess a protective role against AF and stroke development. This pivotal discovery hints at the potential cardioprotective effects of these agents, particularly in individuals with type 2 diabetes mellitus (T2DM) [60].
In 2023, Giuseppe Boriani initiated a comprehensive study, demonstrating that empagliflozin yielded a significant reduction in the risk of severe heart failure events and a deceleration in the decline of estimated glomerular filtration rate (eGFR), irrespective of the presence of atrial fibrillation, in patients with heart failure and an ejection fraction greater than 40% [61].
Moving on to the DECLARE-TIMI 58 Trial of 2020, which engaged 17,160 participants, dapagliflozin emerged as a significant player. This trial demonstrated that dapagliflozin could reduce the incidence of reported episodes of AF/AFL adverse events, especially in high-risk patients with T2DM. This finding underscores the potential role of dapagliflozin in reducing AF in populations at heightened cardiovascular risk [62].
Observational studies and clinical trials have collectively painted a promising picture. SGLT2 inhibitors, with a notable nod to dapagliflozin, appear to offer a shield against atrial fibrillation and stroke development in individuals grappling with T2DM. This revelation opens doors to the possibility of utilizing these medications in the pursuit of cardiovascular risk reduction within this patient cohort.
The journey into randomized controlled trials reinforces the notion of SGLT2 inhibitors as formidable allies against AF. In the EMPA-REG OUTCOME trial of 2015, featuring 7,020 participants, empagliflozin showcased its ability to significantly reduce new-onset AF among T2DM patients. The trial's results provide concrete evidence of the advantageous effects of empagliflozin in the realm of AF prevention [63].
The DAPA-HF trial of 2019, with 4,746 participants, further bolstered the case for dapagliflozin. Promising effects emerged, demonstrating dapagliflozin's potential in reducing AF episodes, particularly in patients grappling with heart failure. This finding hints at a broader role for dapagliflozin in enhancing cardiovascular outcomes in heart failure patients [64].
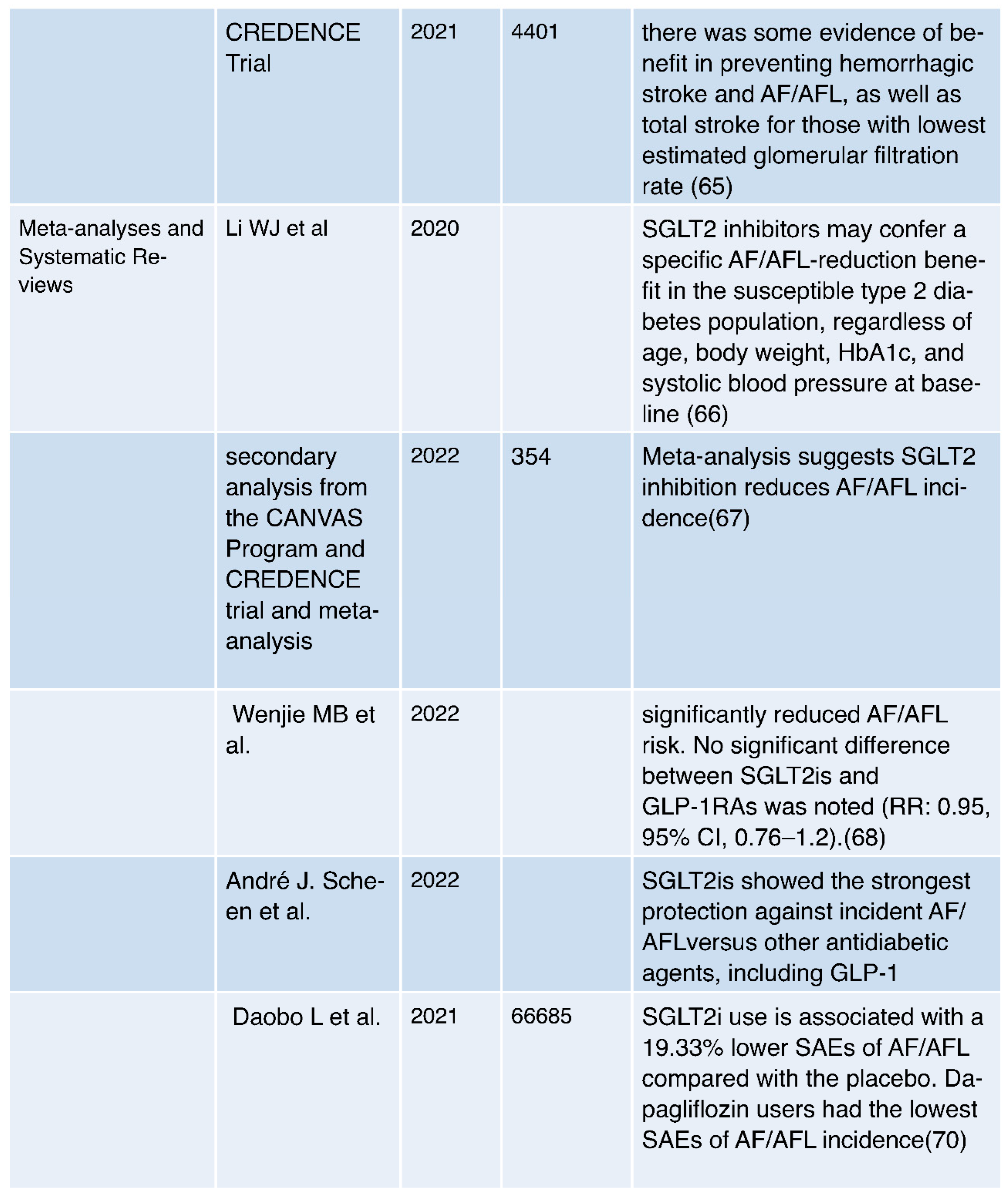
In 2021, the CREDENCE Trial, engaging 4,401 participants, introduced intriguing insights. It offered evidence of potential benefits in averting hemorrhagic stroke, AF/AFL, and total stroke. This benefit seemed particularly pronounced in patients with the lowest estimated glomerular filtration rate, pointing to a potential avenue for stroke risk reduction [65].
The randomized controlled trials collectively suggest that SGLT2 inhibitors, including empagliflozin and dapagliflozin, hold significant promise in the reduction of AF episodes and the improvement of cardiovascular outcomes for individuals living with T2DM and heart failure.
Shifting our gaze toward meta-analyses and systematic reviews, the evidence begins to coalesce. In 2020, Li WJ et al. emphasized that SGLT2 inhibitors may confer a unique benefit in reducing AF/AFL incidence among susceptible type 2 diabetes populations. This benefit appears to transcend baseline characteristics such as age, body weight, HbA1c, and systolic blood pressure [66].
A meta-analysis in 2022, drawing data from the CANVAS Program and CREDENCE trial, provided further support. It suggested that SGLT2 inhibition is linked to a reduction in AF/AFL incidence, further cementing the idea of cardioprotective effects stemming from these inhibitors [67].
In the same year, Wenjie MB et al. delivered encouraging news. Their findings showcased a significant reduction in AF/AFL risk when utilizing SGLT2 inhibitors compared to a placebo. Interestingly, no significant differences were noted between SGLT2 inhibitors and GLP-1 receptor agonists, opening doors to comparative effectiveness [68].
André J. Scheen et al. reinforced this sentiment in 2022 by reporting that SGLT2 inhibitors provided the most robust protection against incident AF/AFL when compared to other antidiabetic agents, including GLP-1 receptor agonists [69].
Daobo L et al. in 2021 brought safety into the spotlight. Their research demonstrated that SGLT2 inhibitor use was associated with a significant 19.33% lower incidence of serious adverse events (SAEs) related to AF/AFL compared to a placebo. Within this realm, dapagliflozin emerged as the standout option with the lowest SAEs of AF/AFL incidence [70].
In summary, the comprehensive body of evidence from observational studies, randomized controlled trials, meta-analyses, and systematic reviews paints a compelling narrative. SGLT2 inhibitors, notably dapagliflozin and empagliflozin, appear to possess a protective mantle against atrial fibrillation, offering hope for improved cardiovascular outcomes in individuals with type 2 diabetes mellitus and heart failure.
- Potential Benefits:
- 1. AF Risk Reduction:
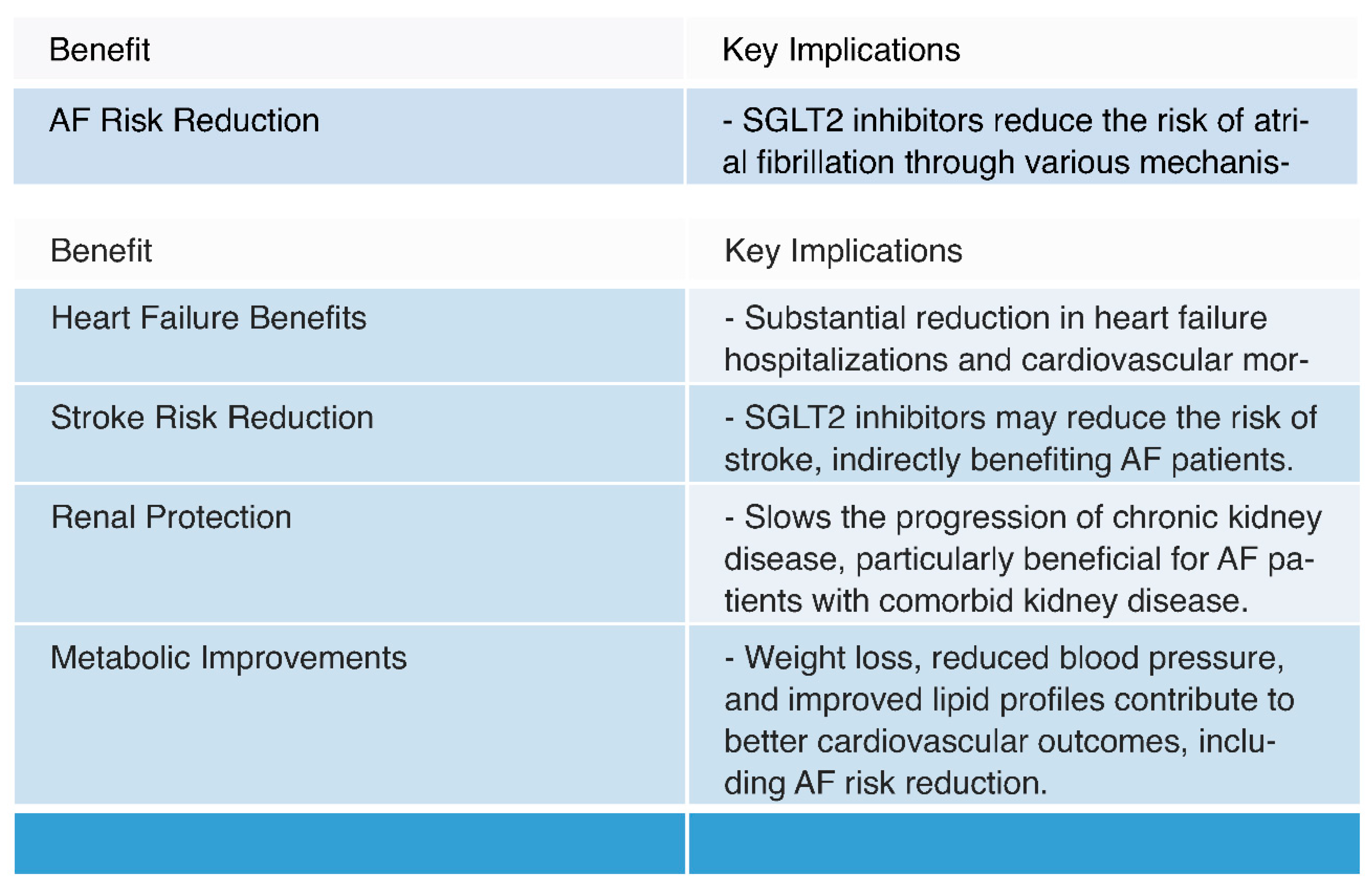
- Mechanisms: SGLT2 inhibitors have been shown to reduce the risk of atrial fibrillation (AF) through various mechanisms. These include improved glycemic control, diuresis leading to reduced plasma volume and blood pressure, reduction in oxidative stress and inflammation, and potential modulation of atrial electrophysiology [23,71,72].
- Observational Evidence: Multiple observational studies have reported a consistent association between SGLT2 inhibitor use and a reduced risk of AF in individuals with type 2 diabetes mellitus (T2DM) and heart failure. This suggests a potential protective effect of these medications against AF [60,61,62].
- Clinical Trials: Randomized controlled trials, such as the EMPA-REG OUTCOME trial and the DECLARE-TIMI 58 Trial, have provided clinical evidence supporting the reduction of AF risk in patients treated with specific SGLT2 inhibitors, such as empagliflozin and dapagliflozin. These trials demonstrate the real-world applicability of AF risk reduction [62,63].
- 2. Cardiovascular Outcomes:
- Heart Failure Benefits: SGLT2 inhibitors have consistently demonstrated substantial benefits in reducing heart failure hospitalizations and cardiovascular mortality. Given the frequent coexistence of AF and heart failure, improved heart failure outcomes indirectly contribute to better AF management [7,25,73,74].
- Renal Protection: SGLT2 inhibitors have shown renal benefits, including a reduction in albuminuria and slowing the progression of chronic kidney disease [26,76,77]. Improved renal function can have a positive impact on overall cardiovascular health, potentially benefiting AF patients, especially those with comorbid kidney disease [26].
Conclusions
Gaining an understanding of the mechanisms underlying this association and the clinical evidence surrounding it yields valuable insights into potential therapeutic applications and areas for further research. SGLT2 induce significant alterations in hemodynamics, including reductions in blood pressure and improvements in the function and inflammation of adipose tissue. These changes may impact the development and progression of AF, thus providing a potential avenue for risk reduction. The observation that SGLT2 inhibitors enhance circadian blood pressure rhythms further underscores their potential cardioprotective effects. This effect is particularly noteworthy as prolonged QT intervals are associated with an increased risk of AF. The optimized loading conditions of the ventricles, reduced afterload, and improved structure and function of the vasculature resulting from the use of SGLT2 inhibitors contribute to these favorable changes in ventricular repolarization. Improved glycemic control indirectly reduces the risk of AF, as hyperglycemia can promote remodeling of the atrial tissue in terms of electrical and structural aspects. The favorable effects on lipid profiles, including reductions in triglycerides and low-density lipoprotein cholesterol, contribute to reduced inflammation and oxidative stress in the atrial tissue, thereby mitigating the risk of AF.
The renal effects of SGLT2 inhibitors, such as reduced glomerular filtration rate and increased excretion of sodium in the urine, have downstream consequences on cardiac function and the risk of AF. Improved renal function can be particularly beneficial for individuals with comorbid kidney disease. The clinical evidence presented in this review solidifies the association between SGLT2 inhibitors and the reduction of AF risk. Observational studies and clinical trials consistently report a decreased risk of AF in individuals with type 2 diabetes mellitus (T2DM) and heart failure. These findings suggest that SGLT2 inhibitors, particularly dapagliflozin and empagliflozin, offer protection against the development of atrial fibrillation and stroke. In randomized controlled trials, empagliflozin and dapagliflozin have demonstrated their potential to significantly reduce the incidence of new-onset AF in patients with T2DM. The EMPA-REG OUTCOME trial and the DAPA-HF trial provide robust clinical evidence supporting the reduction of AF risk in specific patient populations. The CREDENCE Trial adds a layer of complexity, suggesting a potential reduction in the risk of stroke associated with the use of SGLT2 inhibitors.
This benefit appears to be particularly pronounced in patients with the lowest estimated glomerular filtration rate, emphasizing the broader implications of these medications for the reduction of stroke risk. They highlight the potential advantages of these medications in reducing the incidence of AFL, surpassing fundamental characteristics such as age, body weight, HbA1c, and systolic blood pressure. SGLT2 inhibitors not only emerge as protective agents against AF but also exhibit a favorable safety profile in this context, with dapagliflozin being particularly noteworthy. They offer distinct benefits for specific patient populations, particularly those with T2DM and heart failure. These medications provide control over glycemia, weight reduction, and cardiovascular advantages, all of which have a direct impact on the risk of AF. Patients with established cardiovascular diseases also experience cardiovascular protection provided by these medications, resulting in reduced AF risk. The reductions in hospitalizations due to heart failure, cardiovascular mortality, stroke risk, improved renal function, metabolic changes, and overall cardiovascular protection offered by SGLT2 inhibitors contribute to a positive impact on AF risk across various patient groups. By addressing not only glycemic control but also cardiovascular and renal health, these medications become invaluable instruments in the management of AF risk.
- Future Research and Clinical Practice:
As is the case with any developing field of medicine, further research is imperative. A deeper comprehension of the mechanisms that underlie the relationship between SGLT2 inhibitors and AF is required, including electrophysiological alterations and metabolic modifications. Clinical trials exploring the utilization of SGLT2 inhibitors in diverse patient populations will shed light on their efficacy in reducing AF risk. Additionally, understanding the long-term outcomes and potential adverse effects associated with the use of these medications is crucial.
Author Contributions
Behzad Fahimi MD1 contributed to the conceptualization, data analysis, and manuscript writing. Somayeh Beikmohammadi MD2 provided expertise in cardiology, contributed to data collection, and assisted in revising the manuscript.
Acknowledgments
We do not have any acknowledgment.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Song, S., Ko, J. S., Lee, H. A., et al. (2022). Clinical Implications of Heart Rate Control in Heart Failure With Atrial Fibrillation: Multi-Center Prospective Observation Registry (CODE-AF Registry). Frontiers in Cardiovascular Medicine, 9. [CrossRef]
- Thorén, E., Wernroth, ML., Christersson, C. et al. Compared with matched controls, patients with postoperative atrial fibrillation (POAF) have increased long-term AF after CABG, and POAF is further associated with increased ischemic stroke, heart failure and mortality even after adjustment for AF. Clin Res Cardiol 109, 1232–1242 (2020). [CrossRef]
- Gumprecht, J., Domek, M., Lip, G.Y.H. et al. Invited review: hypertension and atrial fibrillation: epidemiology, pathophysiology, and implications for management. J Hum Hypertens 33, 824–836 (2019). [CrossRef]
- Guo, Xue-Yuan; Ma, Chang-Sheng. Atrial Fibrillation Ablation: Indications, Outcomes, Complications, and Future Directions. Chinese Medical Journal 130(16):p 1891-1893, August 20, 2017. |. [CrossRef]
- Kochhar, S. (2016). Atrial fibrillation: An update. Independent Nurse, 2016(2), 30. Published Online:2 Feb 2016. [CrossRef]
- Stroo, J. F., van Steenbergen, G. J., van Straten, A. H. M., Houterman, S., & Soliman-Hamad, M. A. (2023). Long-term Outcome of Reexploration for Bleeding After Coronary Artery Bypass Grafting. Journal of Cardiothoracic and Vascular Anesthesia, Published online June 09, 2023. [CrossRef]
- Khiali, S., Taban-Sadeghi, M., Sarbakhsh, P., et al. (2023). SGLT2 Inhibitors’ Cardiovascular Benefits in Individuals Without Diabetes, Heart Failure, and/or Chronic Kidney Disease: A Systematic Review. Journal of Clinical Pharmacy and Therapeutics, Published online July 16, 2023. [CrossRef]
- Pawlos, Agnieszka, Marlena Broncel, Ewelina Woźniak, and Paulina Gorzelak-Pabiś. 2021. "Neuroprotective Effect of SGLT2 Inhibitors" Molecules 26, no. 23: 7213. [CrossRef]
- Kaneto, Hideaki, Atsushi Obata, Tomohiko Kimura, Masashi Shimoda, Tome Kinoshita, Taka-aki Matsuoka, and Kohei Kaku. 2021. "Unexpected Pleiotropic Effects of SGLT2 Inhibitors: Pearls and Pitfalls of This Novel Antidiabetic Class" International Journal of Molecular Sciences 22, no. 6: 3062. [CrossRef]
- Vallon V, Verma S. Effects of SGLT2 Inhibitors on Kidney and Cardiovascular Function. Annu Rev Physiol. 2021 Feb 10;83:503-528.
- Szekeres, Zsolt, Kalman Toth, and Eszter Szabados. 2021. "The Effects of SGLT2 Inhibitors on Lipid Metabolism" Metabolites 11, no. 2: 87.
- Durante, William, Ghazaleh Behnammanesh, and Kelly J. Peyton. 2021. "Effects of Sodium-Glucose Co-Transporter 2 Inhibitors on Vascular Cell Function and Arterial Remodeling" International Journal of Molecular Sciences 22, no. 16: 8786. [CrossRef]
- Lymperopoulos, Anastasios, Jordana I. Borges, Natalie Cora, and Anastasiya Sizova. 2021. "Sympatholytic Mechanisms for the Beneficial Cardiovascular Effects of SGLT2 Inhibitors: A Research Hypothesis for Dapagliflozin’s Effects in the Adrenal Gland" International Journal of Molecular Sciences 22, no. 14: 7684. [CrossRef]
- Gailin, Ye., Shuai, Wang., Daoquan, Peng. (2021). Effects of SGLT2 Inhibitor on Ischemic Events Stemming From Atherosclerotic Coronary Diseases: A Systematic Review and Meta-analysis With Trial Sequential Analysis of Randomized Controlled Trials.. Journal of Cardiovascular Pharmacology. [CrossRef]
- Fernand, Bonnet., André, Scheen. (2018). Effects of SGLT2 inhibitors on systemic and tissue low-grade inflammation: The potential contribution to diabetes complications and cardiovascular disease.. Diabetes & Metabolism. [CrossRef]
- Anja, Schork., Janine, Saynisch., Andreas, Vosseler., Benjamin, Assad, Jaghutriz., Nils, Heyne., Andreas, Peter., Hans-Ulrich, Häring., Norbert, Stefan., Andreas, Fritsche., Ferruh, Artunc. (2019). Effect of SGLT2 inhibitors on body composition, fluid status and renin-angiotensin-aldosterone system in type 2 diabetes: a prospective study using bioimpedance spectroscopy.. Cardiovascular Diabetology. [CrossRef]
- Asadur, Rahman., Hirofumi, Hitomi., Akira, Nishiyama. (2017). Cardioprotective effects of SGLT2 inhibitors are possibly associated with normalization of the circadian rhythm of blood pressure.. Hypertension Research. [CrossRef]
- Abdullah, Kaplan., Emna, Abidi., Ahmed, F., El-Yazbi., Ahmed, F., El-Yazbi., Ali, H., Eid., Ali, H., Eid., George, W., Booz., Fouad, A., Zouein. (2018). Direct cardiovascular impact of SGLT2 inhibitors: mechanisms and effects.. Heart Failure Reviews. [CrossRef]
- Kazuomi, Kario., Keith, C., Ferdinand., James, H., O'Keefe. (2020). Control of 24-hour blood pressure with SGLT2 inhibitors to prevent cardiovascular disease. Progress in Cardiovascular Diseases. [CrossRef]
- Steven, G., Chrysant. (2017). Promising cardiovascular and blood pressure effects of the SGLT2 inhibitors: a new class of antidiabetic drugs.. Drugs of Today. [CrossRef]
- Samar, A., Nasser., Neha, Arora., Keith, C., Ferdinand. (2022). Addressing Cardiovascular Disparities in Racial/Ethnic Populations: The Blood Pressure-Lowering Effects of SGLT2 Inhibitors. Reviews in Cardiovascular Medicine. [CrossRef]
- Jamie, L., Benham., Jane, E., Booth., Ronald, J., Sigal., Stella, S., Daskalopoulou., Alexander, A., Leung., Doreen, M., Rabi. (2021). Systematic review and meta-analysis: SGLT2 inhibitors, blood pressure and cardiovascular outcomes. IJC Heart & Vasculature. [CrossRef]
- V., K., Kurashin., N., Yu., Borovkova., V., A., Kurashina., T., E., Bakka. (2021). Possibilities of cardio- and nephroprotective eff ects of drugs of the SGLT2 inhibitor group. [CrossRef]
- Monda, V.M., Gentile, S., Porcellati, F. et al. Heart Failure with Preserved Ejection Fraction and Obstructive Sleep Apnea: A Novel Paradigm for Additional Cardiovascular Benefit of SGLT2 Inhibitors in Subjects With or Without Type 2 Diabetes. Adv Ther 39, 4837–4846 (2022). [CrossRef]
- Vincenzo, De, Marzo., Gianluigi, Savarese., Italo, Porto., Marco, Metra., Pietro, Ameri. (2023). Efficacy of SGLT2-inhibitors across different definitions of heart failure with preserved ejection fraction. Journal of Cardiovascular Medicine. [CrossRef]
- Sajad, Khiali., Mohammad, Reza, Sadeghi., Parvin, Sarbakhsh., Naser, Khezerlouy, Aghdam., Afra, Rezagholizadeh., Hila, Asham., Taher, Entezari, Maleki. (2023). SGLT2 Inhibitors' Cardiovascular Benefits In Individuals Without Diabetes, Heart Failure, And/Or Chronic Kidney Disease: A Systematic Review. The Journal of Clinical Pharmacology. [CrossRef]
- Ping-Fan, Lu. (2023). Efficacy of sacubitril-valsartan and SGLT2 inhibitors in heart failure with reduced ejection fraction: A systematic review and meta-analysis. Clinical Cardiology. [CrossRef]
- Atsushi, Tanaka., Takumi, Imai., Shigeru, Toyoda., Kazuhiro, Sugimoto., Ruka, Yoshida., Machi, Furuta., Koichi, Node. (2023). Long-term observation of estimated fluid volume reduction after the initiation of ipragliflozin in patients with type 2 diabetes mellitus: a sub-analysis from a randomized controlled trial (PROTECT). Diabetology & Metabolic Syndrome. [CrossRef]
- Niels, H, Brandt-Jacobsen., Mikkel, Jürgens., Phillip, Hasbak., Peter, Gæde., Peter, Rossing., Jon, J, Rasmussen., Camillla, Fuchs, Andersen., Julie, Lyng, Forman., Jens, Faber., Silvio, E., Inzucchi., Finn, Gustafsson., Morten, Schou., Caroline, Kistorp. (2022). ODP154 Reduction of Cardiac Adipose Tissue Volume with Short-Term Empagliflozin in Patients with Type 2 Diabetes: Results from the SIMPLE Randomized Clinical Trial. Journal of the Endocrine Society. [CrossRef]
- Kristina, Johnsson., Eva, Johnsson., TA, Mansfield., Yshai, Yavin., Agata, Ptaszynska., Shamik, Parikh. (2016). Osmotic diuresis with SGLT2 inhibition: analysis of events related to volume reduction in dapagliflozin clinical trials. Postgraduate Medicine. [CrossRef]
- Marianna, Fontana., Ana, Martinez-Naharro., Liza, Chacko., Dorota, Rowczenio., Janet, A., Gilbertson., Carol, J., Whelan., Svetla, G., Strehina., Thirusha, Lane., James, C., Moon., David, F., Hutt., Peter, Kellman., Aviva, Petrie., Philip, N., Hawkins., Julian, D., Gillmore. (2021). Reduction in CMR Derived Extracellular Volume With Patisiran Indicates Cardiac Amyloid Regression.. Jacccardiovascular Imaging. [CrossRef]
- Giuseppe, Cannella., S., Ghielmi., Massimo, Sandrini., Claudio, Poiesi., Mario, Gaggiotti., A., Rodella., Rosario, Maiorca. (1988). Effect of reduction of blood volume on plasma immunoreactive atrial natriuretic factor concentrations in normal man.. Nephrology Dialysis Transplantation. [CrossRef]
- Tamique, Mason., Otavio, R., Coelho-Filho., Subodh, Verma., Biswajit, Chowdhury., Fei, Zuo., Adrian, Quan., Kevin, E., Thorpe., Christopher, Bonneau., Hwee, Teoh., Richard, E., Gilbert., Lawrence, A., Leiter., Peter, Jüni., Bernard, Zinman., Michael, Jerosch-Herold., C., David, Mazer., Andrew, T., Yan., Kim, A., Connelly., Kim, A., Connelly. (2021). Empagliflozin Reduces Myocardial Extracellular Volume in Patients With Type 2 Diabetes and Coronary Artery Disease.. Jacc-cardiovascular Imaging. [CrossRef]
- Mads, Ersbøll., Mikkel, Jürgens., Philip, Hasbak., Andreas, Kjaer., Emil, Wolsk., Bo, Zerahn., Niels, H, Brandt-Jacobsen., Peter, Gæde., Peter, Rossing., Peter, Rossing., Jens, Faber., Silvio, E., Inzucchi., Finn, Gustafsson., Morten, Schou., Caroline, Kistorp., Caroline, Kistorp. (2021). Effect of empagliflozin on myocardial structure and function in patients with type 2 diabetes at high cardiovascular risk: the SIMPLE randomized clinical trial. International Journal of Cardiovascular Imaging. [CrossRef]
- Murat, Ziyrek., Mustafa, Duran. (2021). Effects of SGLT2 Inhibitors as an Addon Therapy to Metformin on Electrocardiographic Indices of Ventricular Repolarization. Acta Cardiologica Sinica. [CrossRef]
- Edoardo, Gronda., Gary, D., Lopaschuk., Arduino, Arduini., Antonio, Santoro., Giuditta, Benincasa., Alberto, Palazzuoli., Domenico, Gabrielli., Claudio, Napoli. (2022). Mechanisms of action of SGLT2 inhibitors and their beneficial effects on the cardiorenal axis.. Canadian Journal of Physiology and Pharmacology. [CrossRef]
- Subodh, Verma., John, J.V., McMurray. (2018). SGLT2 inhibitors and mechanisms of cardiovascular benefit: a state-of-the-art review. Diabetologia. [CrossRef]
- Jason, R.B., Samuel, Sossalla., Nazha, Hamdani., Ruben, Coronel., Nina, C., Weber., Peter, E., Light., Coert, J., Zuurbier. (2022). Cardiac mechanisms of the beneficial effects of SGLT2 inhibitors in heart failure: Evidence for potential off-target effects.. Journal of Molecular and Cellular Cardiology. [CrossRef]
- T, Sato., Takayuki, Miki., Hirofumi, Ohnishi., T., Yamashita., A., Takada., Toshiyuki, Yano., Masaya, Tanno., Akihito, Tsuchida., Tetsuji, Miura. (2017). Effect of sodium-glucose co-transporter-2 inhibitors on impaired ventricular repolarization in people with Type 2 diabetes. Diabetic Medicine. [CrossRef]
- Zhang, N., Gong, M., Tse, G., Zhang, Z., Meng, L., Yan, B. P.,... & Liu, T. (2018). Prolonged corrected QT interval in predicting atrial fibrillation: a systematic review and meta-analysis. Pacing and Clinical Electrophysiology, 41(3), 321-327. [CrossRef]
- Cho, M. S., Nam, G. B., Kim, Y. N., Kim, J., Choi, K. J., & Kim, Y. H. (2020). Clinical Implications of Ventricular Repolarization Parameters on Long-Term Risk of Atrial Fibrillation―Longitudinal Follow-up Data From a General Ambulatory Korean Population―. Circulation Journal, 84(7), 1067-1074. [CrossRef]
- Dobromir, Dobrev., Stanley, Nattel. (2008). Calcium Handling Abnormalities in Atrial Fibrillation as a Target for Innovative Therapeutics. Journal of Cardiovascular Pharmacology. [CrossRef]
- Chung-Chuan, Chou., Peng, Sheng, Chen., Delon, Wu., Delon, Wu. (2008). Intracellular Calcium Dynamics and Autonomic Stimulation in Atrial Fibrillation: Mechanisms and Implications. Journal of Arrhythmia. [CrossRef]
- Gary, L., Aistrup., Rishi, Arora., Søren, Grubb., Shin, Yoo., Benjamin, Toren., Manvinder, Kumar., Aaron, Kunamalla., William, Marszalec., Tej, Motiwala., Shannon, Tai., Sean, Yamakawa., Satya, Yerrabolu., Francisco, J., Alvarado., Héctor, H., Valdivia., Jonathan, M., Cordeiro., Yohannes, Shiferaw., J., A., Wasserstrom. (2017). Triggered intracellular calcium waves in dog and human left atrial myocytes from normal and failing hearts. Cardiovascular Research. [CrossRef]
- Funsho, E, Fakuade., Vanessa, Steckmeister., F., Seibertz., Judith, Gronwald., Stefanie, Kestel., Julia, Menzel., Julius, Ryan, D., Pronto., Karim, Taha., Fereshteh, Haghighi., George, Kensah., Charles, M., Pearman., Felix, Wiedmann., Arco, J., Teske., Constanze, Schmidt., Katharine, M., Dibb., Aschraf, El-Essawi., Bernhard, C., Danner., Hassina, Baraki., Blanche, Schwappach., Ingo, Kutschka., Fleur, E., Mason., Niels, Voigt. (2021). Altered atrial cytosolic calcium handling contributes to the development of postoperative atrial fibrillation. Cardiovascular Research. [CrossRef]
- Dobromir, Dobrev., Xander, H.T., Wehrens. (2017). Calcium-mediated cellular triggered activity in atrial fibrillation.. The Journal of Physiology. [CrossRef]
- Qing, Wang., Qing, Wang., Jing, Wang., Pei, Wang., Liaoyuan, Wang., Lanting, Jia., Xinyu, Ling., Wang, Xi., Jie, Min., Hua, Shen., Jian, Xiao., Jinxiang, Yuan., Zhinong, Wang. (2019). Glycemic control is associated with atrial structural remodeling in patients with type 2 diabetes. BMC Cardiovascular Disorders. [CrossRef]
- Shruti, S, Joshi., Trisha, Singh., David, E., Newby., Jagdeep, Singh. (2021). Sodium-glucose co-transporter 2 inhibitor therapy: mechanisms of action in heart failure. Heart. [CrossRef]
- David, Z.I., Cherney., Ayodele, Odutayo., Ronnie, Aronson., Justin, A., Ezekowitz., John, D., Parker. (2019). Sodium Glucose Cotransporter-2 Inhibition and Cardiorenal Protection: JACC Review Topic of the Week. Journal of the American College of Cardiology. [CrossRef]
- Silvio, E., Inzucchi., Bernard, Zinman., Christoph, Wanner., Roberto, Ferrari., David, Fitchett., Stefan, Hantel., Rosa-Maria, Espadero., Hans-Juergen, Woerle., Uli, C., Broedl., Odd, Erik, Johansen. (2015). SGLT-2 inhibitors and cardiovascular risk: Proposed pathways and review of ongoing outcome trials. Diabetes and Vascular Disease Research. [CrossRef]
- Christopher, Redford., Laura, Doherty., Jamie, Smith. (2015). SGLT2 inhibitors and the risk of diabetic ketoacidosis. Practical Diabetes. [CrossRef]
- Julieta, Lazarte., Tharsan, Kanagalingam., Robert, A., Hegele. (2021). Lipid effects of sodium-glucose cotransporter 2 inhibitors.. Current Opinion in Lipidology. [CrossRef]
- Zsolt, Szekeres., Kalman, Toth., Eszter, Szabados. (2021). The Effects of SGLT2 Inhibitors on Lipid Metabolism.. Metabolites. [CrossRef]
- Adriana, Sánchez-García., Mario, Simental-Mendía., Juan, Manuel, Millán-Alanís., Luis, E., Simental-Mendía. (2020). Effect of sodium-glucose co-transporter 2 inhibitors on lipid profile: A systematic review and meta-analysis of 48 randomized controlled trials. Pharmacological Research.
- Hanny, Sawaf., Moarij, Qaz., Jeeda, Ismail., Ali, Mehdi. (2022). The Renal Effects of SGLT2 Inhibitors. [CrossRef]
- Volker, Vallon., Subodh, Verma. (2021). Effects of SGLT2 Inhibitors on Kidney and Cardiovascular Function.. Annual Review of Physiology. [CrossRef]
- Rosalie, A., Scholtes., Michaël, J.B., van, Baar., Megan, D., Kok., Petter, Bjornstad., David, Z.I., Cherney., Jaap, A., Joles., Daniël, H., van, Raalte., Daniël, H., van, Raalte. (2021). Renal haemodynamic and protective effects of renoactive drugs in type 2 diabetes: Interaction with SGLT2 inhibitors. Nephrology. [CrossRef]
- Shan-Jiang, Chen., Ruben, Coronel., Markus, W., Hollmann., Nina, C., Weber., Coert, J., Zuurbier. (2022). Direct cardiac effects of SGLT2 inhibitors. Cardiovascular Diabetology. [CrossRef]
- Josselin, Nespoux., Volker, Vallon. (2020). Renal effects of SGLT2 inhibitors: an update.. Current Opinion in Nephrology and Hypertension. [CrossRef]
- Lee, S., Zhou, J., Chang, C., Liu, T., Chang, D., Wong, W. T., Leung, K. S. K., Wai, A. K. C., Cheung, B. M. Y., Tse, G., & Zhang, Q. (2021). Comparative effects of sodium glucose cotransporter 2 (SGLT2) inhibitors and dipeptidyl peptidase-4 (DPP4) inhibitors on new-onset atrial fibrillation and stroke outcomes. medRxiv 2021.01.04.21249211. [CrossRef]
- Boriani G, Mei DA, Imberti JF. Therapeutic effects of sodium-glucose cotransporter 2 inhibitors in patients with heart failure with preserved ejection fraction: From outcome improvement to potentially favourable influences on atrial fibrillation burden, atrial fibrillation progression and atrial cardiomyopathy. Eur J Heart Fail. 2023 Jul;25(7):978-980. [CrossRef]
- Zelniker TA, Bonaca MP, Furtado RHM, Mosenzon O, Kuder JF, Murphy SA, Bhatt DL, Leiter LA, McGuire DK, Wilding JPH, Budaj A, Kiss RG, Padilla F, Gause-Nilsson I, Langkilde AM, Raz I, Sabatine MS, Wiviott SD. Effect of Dapagliflozin on Atrial Fibrillation in Patients With Type 2 Diabetes Mellitus: Insights From the DECLARE-TIMI 58 Trial. Circulation. 2020 Apr 14;141(15):1227-1234. [CrossRef]
- Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, Mattheus M, Devins T, Johansen OE, Woerle HJ, Broedl UC, Inzucchi SE; EMPA-REG OUTCOME Investigators. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N Engl J Med. 2015 Nov 26;373(22):2117-28. [CrossRef]
- McMurray JJV, DeMets DL, Inzucchi SE, Køber L, Kosiborod MN, Langkilde AM, Martinez FA, Bengtsson O, Ponikowski P, Sabatine MS, Sjöstrand M, Solomon SD; DAPA-HF Committees and Investigators. A trial to evaluate the effect of the sodium-glucose co-transporter 2 inhibitor dapagliflozin on morbidity and mortality in patients with heart failure and reduced left ventricular ejection fraction (DAPA-HF). Eur J Heart Fail. 2019 May;21(5):665-675. [CrossRef]
- Zhou Z, Jardine MJ, Li Q, Neuen BL, Cannon CP, de Zeeuw D, Edwards R, Levin A, Mahaffey KW, Perkovic V, Neal B, Lindley RI; CREDENCE Trial Investigators*. Effect of SGLT2 Inhibitors on Stroke and Atrial Fibrillation in Diabetic Kidney Disease: Results From the CREDENCE Trial and Meta-Analysis. Stroke. 2021 May;52(5):1545-1556. [CrossRef]
- Li WJ, Chen XQ, Xu LL, Li YQ, Luo BH. SGLT2 inhibitors and atrial fibrillation in type 2 diabetes: a systematic review with meta-analysis of 16 randomized controlled trials. Cardiovasc Diabetol. 2020 Aug 26;19(1):130. [CrossRef]
- Li C, Yu J, Hockham C, Perkovic V, Neuen BL, Badve SV, Houston L, Lee VYJ, Barraclough JY, Fletcher RA, Mahaffey KW, Heerspink HJL, Cannon CP, Neal B, Arnott C. Canagliflozin and atrial fibrillation in type 2 diabetes mellitus: A secondary analysis from the CANVAS Program and CREDENCE trial and meta-analysis. Diabetes Obes Metab. 2022 Oct;24(10):1927-1938. [CrossRef]
- Wenjie: Journal of Cardiovascular Pharmacology 79(3):p 281-288, March 2022. |. [CrossRef]
- Scheen: https://doi.org/10.1016/j.diabet.2022.101390, 2022 Nov;48(6):101390. [CrossRef]
- Li D, Liu Y, Hidru TH, Yang X, Wang Y, Chen C, Li KHC, Tang Y, Wei Y, Tse G, Xia Y. Protective Effects of Sodium-Glucose Transporter 2 Inhibitors on Atrial Fibrillation and Atrial Flutter: A Systematic Review and Meta- Analysis of Randomized Placebo-Controlled Trials. Front Endocrinol (Lausanne). 2021 Mar 19;12:619586. [CrossRef]
- Alex, Ali, Sayour., Mihály, Ruppert., Attila, Oláh., Kálmán, Benke., Bálint, András, Barta., Eszter, Zsáry., Béla, Merkely., Tamás, Radovits. (2021). Effects of SGLT2 Inhibitors beyond Glycemic Control—Focus on Myocardial SGLT1. International Journal of Molecular Sciences. [CrossRef]
- Ashish, Verma., Ankit, B., Patel., Sushrut, S., Waikar. (2020). SGLT2 Inhibitor: Not a Traditional Diuretic for Heart Failure.. Cell Metabolism. [CrossRef]
- Omar, Mourad., Shabana, Vohra., Sara, S., Tunes. (2023). SGLT2 transcriptomic expression atlas supports a kidney-centric role for empagliflozin’s benefits in heart failure. bioRxiv. [CrossRef]
- Sara, Albalushi. (2023). Meta-analysis on the effectiveness of SGLT2 inhibitors in heart failure. European heart journal. Acute cardiovascular care. [CrossRef]
- Fatima, Alzahra, Al, Hamed., Hazem, Elewa. (2020). Potential Therapeutic Effects of Sodium Glucose-linked Cotransporter 2 Inhibitors in Stroke.. Clinical Therapeutics. [CrossRef]
- Brendon, L., Neuen., Min, Jun., James, Wick., S., Kotwal., Sunil, Badve., Meg, Jardine., M., Gallagher., John, Chalmers., Kellie, Nallaiah., Vlado, Perkovic., D., Peiris., A., Rodgers., Mark, Woodward., Paul, E., Ronksley. (2023). Estimating the population-level kidney benefits of improved uptake of SGLT2 inhibitors in patients with chronic kidney disease in Australian primary care. med-Rxiv. [CrossRef]
- Pasquale, Paolisso., Luca, Bergamaschi., Arturo, Cesaro., Emanuele, Gallinoro., Felice, Gragnano., Celestino, Sardu., Niya, Mileva., Alberto, Foà., Matteo, Armillotta., Angelo, Sansonetti., S., Amicone., A., Impellizzeri., Marta, Belmonte., Giuseppe, Esposito., Nuccia, Morici., Gianni, Casella., Ciro, Mauro., Dobrin, Vassilev., Nazzareno, Galiè., Gaetano, Santulli., Paolo, Calabrò., Emanuele, Barbato., Raffaele, Marfella., Carmine, Pizzi. (2023). Impact of SGLT2-inhibitors on contrast-induced acute kidney injury in Diabetic patients with Acute Myocardial Infarction with and without chronic kidney disease: Insight from SGLT2-I AMI PROTECT Registry.. Diabetes Research and Clinical Practice. [CrossRef]
- Francisco, García-Carrizo., Sebastià, Galmés., Catalina, Picó., Andreu, Palou., Ana, M., Rodríguez. (2022). Supplementation with the Prebiotic High-Esterified Pectin Improves Blood Pressure and Cardiovascular Risk Biomarker Profile, Counteracting Metabolic Malprogramming. Journal of Agricultural and Food Chemistry. [CrossRef]
- J., Blose., P., Stickles., A., Battaglino., A., Trumbetti., J., James., K., Cooper., A., Schade., Melissa, A., Reed., Selen, Razon., Melissa, A., Whidden. (2020). The Effects of a Six-Week Weight Loss Program on Blood Lipid Profiles and Cardiovascular Health.
- Yukiko, Hasegawa., Tomoko, Nakagami., Junko, Oya., Kanako, Takahashi., Chisato, Isago., Moritoshi, Kurita., Yuki, Tanaka., Arata, Ito., Tadasu, Kasahara., Yasuko, Uchigata. (2019). Body Weight Reduction of 5% Improved Blood Pressure and Lipid Profiles in Obese Men and Blood Glucose in Obese Women: A Four-Year Follow-up Observational Study. Metabolic Syndrome and Related Disorders. [CrossRef]

Table 1.
Mechanisms Underlying the Relationship.

Table 3.
Cardiovascular Benefits and Potential Therapeutic Implications of SGLT2 Inhibitors.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



