Submitted:
30 October 2023
Posted:
01 November 2023
You are already at the latest version
Abstract
Introduction: Bone fractures may be the result of high force impact or stress, or a minimal trauma injury as a result of certain medical conditions that weaken the bones, such as osteoporosis, osteopenia, bone cancer, or osteogenesis imperfecta, where the fracture is then properly termed a pathologic fracture. Bone cancer can be primarily or secondary to metastasis. Case presentation: We report a rare case of left humerus fracture in a 59-year-old male patient due to metastatic renal cell carcinoma. Our patient had no important past medical history. He suffered from two months of left arm pain, moderate disability and fever at night. Analgesics consumption resulted in minimal relieve. Trauma history was negative. X-ray of the left arm showed an osteolytic lesion with humerus fracture. Abdominal computed tomography with contrast showed right renal mass.Radical right nephrectomy was performed in addition to alignment nailing of the left humerus fracture with biopsy. Pathology report documented clear cell carcinoma with metastatic bone. The treatment was completed by chemotherapyDiscussion: Secondary bone tumors are metastatic lesions which have spread from other organs, most commonly carcinomas of the breast, lung, and prostate, and rarely from kidney. In some cases, bone metastasis could be the first symptoms of renal cell carcinoma. Conclusion: suspected pathological bone fractures should be investigated completely. It may hide a tumor as a cause.
Keywords:
metastatic renal cell carcinoma
; humerus fracture
; osteolytic
Introduction:
During last decade diagnosis of Renal cell carcinoma has increased becoming the seventh most common site for tumors [1].
Common among patients with RCC, bone metastasis accounts for one-third of patients with metastatic disease [2].
Skeletal metastasis is very destructive in patients with renal cell carcinoma leading to mainly osteolytic lesions that compromise bone integrity and negatively impact patient’s outcome. Skeletal involvement in RCC is associated with skeletal related events [SRE] including pains, impending fractures, nerve compressions, hypercalcemia and even pathological fractures which may require surgical interventions and other therapy [3,4].
The humerus is the second most commonly affected long bone after femur. Lesion in this site usually occurs late and induces a wide bone loss resulting in severe pain and disability [5].
Here, we present a rare case of left arm pain diagnosed later in pathological fracture due to metastatic renal cell carcinoma.
Case presentation:
A 59 years old male presented to out-patient orthopedic clinic after two months of left arm pain. His past medical and surgical history was unremarkable. His pain was more severe at night with elevate body temperature. He took ibu-brufen 400 mg twice daily with 500 mg citamol resulted in minimal relieve. In the past week, he suffered from strong pain even his arm at rest. This pain stooped him doing his job as a bank accountant. The patient does not remember any trauma to his arm. His family history was positive for ischemic heart disease in his mother. On examination, he was moderately in painful state. Examination of his left arm was not completed due to severe pain that was induced by examination. His vital signs were as follow: blood pressure was 135/75 mmHg, pulse rate was 88/min, his temperature was 38.1.
Laboratory tests are shown in Table 1.
Radiograph of the left arm revealed a pathological humerus fracture (Figure 1).
Chest x-ray was normal. Abdominal and pelvis ultrasound showed a 45 × 32 × 29 mm mass at the right kidney site with vascularization on Doppler.
Computed tomography with contrast confirmed the diagnosis of right renal mass (Figure 2).
After taking patient consent, radical nephrectomy was performed.
Kuntscher-type centromedullary alignment nailing of the left humerus fracture site was done for the patient. In addition, the bone was filled with acrylic cement.
The specimen was sent to the pathology department.
Pathology report showed a clear cell renal cell carcinoma. We referred our patient to another center for chemotherapy.
Our patient underwent 6 courses of chemotherapy (protocol: Cisplat-SFU).
Follow-up for 12 months later, the patient was doing well.
Discussion:
Renal cell carcinoma accounts for 90% of all malignant renal tumours. It comprises four main histological types: clear cell carcinoma (75%), tubulo-papillary carcinoma (10% - 15%), chromophore carcinoma (<5%), Bellini or collecting-tube carcinoma (1%) (6).
Most renal tumors are growing locally with minimal symptoms. Distal metastases are sometimes considered the first symptom in those patients.
Among the 22% of RCC patients with bone metastasis, approximately one third presented with bone metastasis at the time of initial RCC diagnosis, whereas the remainder developed bone metastasis during disease progression (7).
In the study by Simon and et al, of surgical treatment of metastatic renal cell carcinoma in 65 cases operated on for metastatic renal cancer, 55 patients (41 men and 14 women) were included. The mean age was 60 years (41 to 84 years). In this series, eight patients underwent 2 operations and 1 underwent three operations for three metastatic locations. In 23% of cases, metastases were present at the time of diagnosis of the primary tumor; in 17% of cases, the metastasis was incidental. Pathological fractures were present in half the cases (33 cases) and the other half without pathological fractures. The most frequent site was the femur (40 cases). The second most common site was the humerus (15 cases), followed by other sites (10 cases). Surgery was centromedullary nailing for the femur and humerus. Functional outcome was good or fair in 78% of cases (8).
In our case, we had an old male patient who had left arm pain any night pyrexia. Investigations showed left humerus pathological fracture. The patient had no history of trauma. Full work up demonstrated right renal cell carcinoma.
The diagnosis was renal carcinoma (clear cell type) with isolated bone metastasis confirmed by the biopsy.
The tumor was resected successfully with no accidents during the operation.
The humeral fracture was treated surgically.
Conclusion:
In some cases, bone metastasis is the first symptom for primary tumors. Our case report demonstrates a humeral osteolytic lesion secondary to renal cell carcinoma.
References
- F. Levi, J. Ferlay, C. Galeone, F. Lucchini, E. Negri, P. Boyle, et al. The changing pattern of kidney cancer incidence and mortality in Europe BJU Int, 101 (2008), pp. 949-958. [CrossRef]
- Chen SC, Kuo PL. Bone Metastasis from Renal Cell Carcinoma. Int J Mol Sci. 2016 Jun 22;17(6):987. [CrossRef]
- Beuselinck B., Oudard S., Rixe O., Wolter P., Blesius A., Ayllon J. Negative impact of bone metastasis on outcome in clear-cell renal cell carcinoma treated with sunitinib. Ann. Oncol. 2010;22(4):794–800. [CrossRef]
- Patil S., Figlin R., Hutson T., Michaelson M., Négrier S., Kim S. Prognostic factors for progression-free and overall survival with sunitinib targeted therapy and with cytokine as first-line therapy in patients with metastatic renal cell carcinoma. Ann. Oncol. 2010;22(2):295–300. [CrossRef]
- W.-H. Park, T. Eisen Prognostic factors in renal cell cancer BJU Int, 99 (2007), pp. 1277-1281. [CrossRef]
- Patard, J.J., Baumert, H., Corréas, J.M., Escudier, B., Lang, H., Long, J.A., Neuzillet, Y., et al. (2010) Kidney Cancer, Oncology Committee of the French Association of Urology (CCAFU). Progrès en Urologie, 20, S319-S339. [CrossRef]
- Santini D, Procopio G, Porta C, Ibrahim T, Barni S, et al. (2013) Natural History of Malignant Bone Disease in Renal Cancer: Final Results of an Italian Bone Metastasis Survey. PLoS ONE 8(12): e83026. [CrossRef]
- Simon, P., Katzner, M., Montes, P., Gleyze, P. and Babin, S.R. (1996) Surgical Treatment of Metastases of Renal Carcinomas in 65. European Journal of Orthopaedic Surgery & Traumatology, 6, 57-62. [CrossRef]
Figure 1.
X-ray of left arm.

Figure 2.
CT with contrast showing right renal mass.
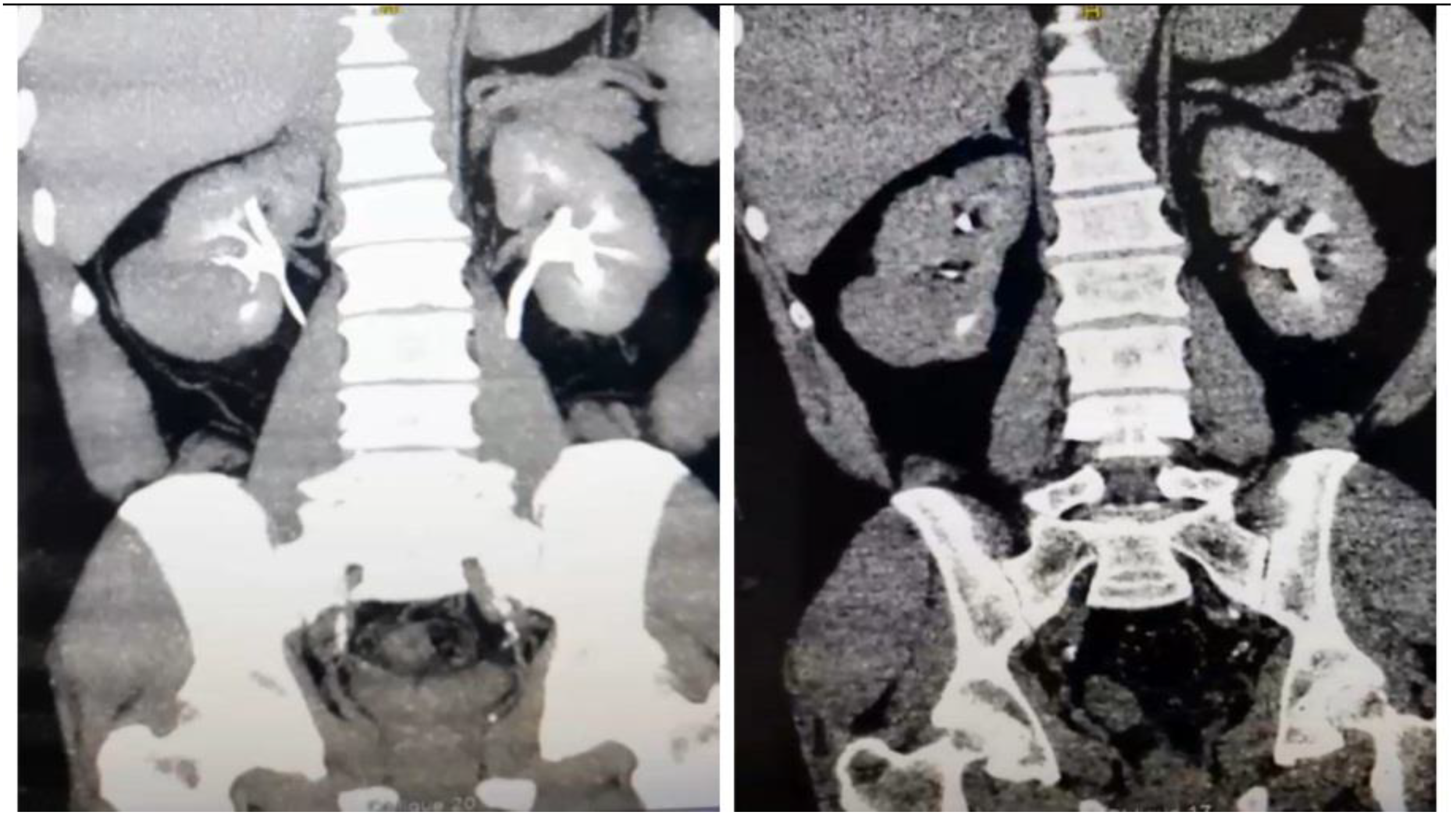

Table 1.
Laboratory tests at presentation.
| Wight blood cell count | Hemoglobine | Platelets | Creatinine | CRP | Urea | Glucose | Na+ | K+ |
| 11×105/ml | 13×105gr/dl | 310×105/mcl | 1 mg/dl | 14 | 28 mg/dl | 112 mg/dl | 139mEq/L | 3.8 mEq/L |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



