
Submitted:
30 May 2023
Posted:
01 June 2023
You are already at the latest version
Abstract
(1) Background: Proximal humerus fractures can be a debilitating condition if not properly treated. These fracture patterns are varied and differ in every patient. Functional outcomes may be determined by the integrity of the shoulder girdle involving the rotator cuff insertion. The post-operative resorption or malreduction of the greater tuberosity is an important factor contributing to the poor functional outcome of a patient. (2) Methods: A single-center retrospective comparative study was performed to evaluate the functional outcomes of patients undergoing operative fixation for this injury. A total of 387 consecutive cases treated operatively from 2019-2021 were included for analysis. (3) Results: 94 cases fulfilled our criteria for analysis. A matched-group comparison of 19 patients each was performed to compare demographics, post-operative fracture characteristics and functional outcomes. (4) Conclusions: The resorption or malreduction of the greater tuberosity contributes greatly to the prognostic outcome in patients treated with ORIF surgery. In our demographic study, obesity is another contributing factor affecting the parameters of post-operative reduction in proximal humerus fractures. Appropriate surgical planning and post-operative multidisciplinary care must be taken into consideration to attain a satisfactory prognostic outcome.
Keywords:
Fractures
; Greater tuberosity
; Humerus
; Malreduction
; Resorption
1. Introduction
Proximal humeral fractures, defined as fractures occurring at or proximal to the surgical neck of the humerus, is one of the most frequent injury affecting the shoulder girdle in adults [1]. An estimated 706,000 proximal humeral fractures happened worldwide in 2000 [2]. In 2008, proximal humeral fractures lead to 185,000 emergency department visits in the United States alone [3]. It is an osteoporosis-related fracture and its incidence is rising as the population ages, from 4% 50 years ago to 7% of all fractures nowadays [4,5]. In the United States, the numbers of patients presenting with proximal humeral fractures are expected to reach 275,000 by 2030 [3].
The vast majority of proximal humeral fractures are treated nonoperatively [3,6]. Although most studies support good clinical outcomes of conservative treatment, a recent prospective study has shown that significant functional impairment may occur even in non-displaced proximal humeral fractures with over two-thirds of patients having chronic pain and significant reductions in functional capacity [7]. After the introduction of locking plates around 2000, surgical intervention is becoming more frequent owing to the angular stability between the screws and plate, forming a more stable construct even in an osteoporotic bone [6,8]. Several studies have shown high rates of healing and excellent functional recovery with proximal humeral locking plates [9,10]. On the other hand, complications such as screw back out, screw cut out, varus collapse, subacromial impingement, avascular necrosis, nonunion, malunion and deep infection were also reported [11,12]. Poor results may be related to a lack of experience of the treating surgeon, inexact technique, and/or specific failure of the material [13,14]. In the clinical practice, despite incorporated suture fixation through the entheses of the rotator cuff into the plate construct to neutralize the deforming force, resorption and malreduction of the greater tuberosity are sometimes observed but have not yet been well understood in the current literatures. Miyamura et al. (2021) have studied the fragment characteristics and intraoperative risk factors of greater tuberosity resorption in complex proximal humeral fracture treated with ORIF [15]. However, few literatures report the functional outcomes in such condition. Therefore, this study aims to study the functional outcome in proximal humeral fractures with postoperative resorption or malreduction of greater tuberosity and the results show that it is associated with poor functional outcomes.
2. Materials and Methods
2.1. Study setting
This is a single center study. In this retrospective comparative study, the requirement for written informed consent by the patients was waived.
2.2. Patient enrollment
We retrospectively collected data of patients diagnosed with proximal humeral fractures treated operatively from 2019 to 2021. All of the radiographs and CT images were reviewed. We included fractures involving the greater tuberosity defined as 11B1.1, 11C3 in AO/OTA classification system and determined whether the greater tuberosity was resorbed or in malreduction in the follow-up period. The greater tuberosity involvement was defined on plain film with obvious greater tuberosity displacement (>5 mm), or definite fracture line around the greater tuberosity on computed tomography (CT). We excluded patients diagnosed with AO/OTA 11A fractures (2-part fractures and isolated greater tuberosity fractures) and AO/OTA 11B1.2 fractures (unifocal fractures with lesser tuberosity involvement), periprosthetic fractures, open fractures, pathological fractures, proximal humeral bone tumor and patients presented with neurovascular injury of the affected limb. We included the patients treated operatively with locking compression plate (LCP) and excluded those treated with arthroplasty. Patients with follow-up period less than 24 weeks and incomplete data were excluded.
Three hundred and eighty-seven consecutive cases with proximal humeral fractures treated operatively with locking plates were initially reviewed, and 293 cases were subsequently excluded. A total of 94 patients were included in the analysis. AO Philos, Zimmer ALPS, and Aplus proximal humeral locking compression plates were used among these patients according to surgeons’ preference. All of the locking plates have side holes for incorporation of the suture fixation. The average length of follow-up was 45.55 weeks. We identified 19 patients (20.2%) in whom bone resorption or malreduction of the greater tuberosity developed after ORIF and 75 patients (79.8%) who did not show any resorption or malreduction of the greater tuberosity. (Figure 1 and Figure 2) The average time to determine the development of greater tuberosity resorption was 14.72 weeks after surgery. The average time to determine the development of greater tuberosity malreduction was 4.2 weeks after surgery.
2.3. Surgical technique
Most surgeries were performed within the first week of the injury (from 1 to 29 days, on an average of 2 days). The surgeries were performed in beach-chair position by several senior surgeons or under the direct supervision of a senior surgeon. An extended deltopectoral approach with limited detachment of anterior deltoid or an anterolateral approach through a deltoid-splitting was used according to the surgeons’ preference. The periosteal attachment of the greater tuberosities and the medial hinge was preserved. The reduction was performed under intraoperative fluoroscopy and kept temporarily by use of Kirschner wires. The rotator cuff was secured through the enthesis with several heavy nonabsorbable sutures (No.5 Ethibond), which would later on be threaded through the plate to reinforce the construct. A new proximal humeral locking compression plate was positioned at least 5 to 8 mm distal to the upper end of the greater tuberosity and 2 mm lateral to the bicipital groove to prevent plate impingement. The tendon of the long head of biceps was checked to ensure that sufficient gap was maintained from the plate. The plate was then fixed definitively with several angular stable screws into the humeral head. The humeral shaft holes were fixed with either locking screws or standard cortical screws according to the surgeons’ decision. A final check was done to ensure good reduction quality of the greater tuberosity, optimal plate position and no screw penetration from the humeral head under an image intensifier before the wound closure.
2.4. Data collection
Demographic information including gender, height, weight, body mass index (BMI), smoking status and alcohol use was collected through chart review. We assessed the bone quality using the deltoid tuberosity index in the preoperative humeral AP radiograph. The location for calculating the deltoid tuberosity index is defined as directly proximal to the deltoid tuberosity where the outer cortical borders become parallel. It is calculated by dividing the outer cortical by the inner endosteal diameter at this level [16].
For fracture characteristics, the preoperative plain films or CT image were reviewed to determine the AO/OTA classification, the presence of a varus or valgus fracture type and a fracture-dislocation. Surgery-related characteristics were also collected: interval from injury to surgery and artificial bone graft use. We assessed the immediate postoperative radiographic parameters including inadequate medial support, lateral humeral offset, head diameter, head height, perpendicular height, neck-shaft angle, superior displacement of greater tuberosity above articular surface, medial gap (whether the gap was more than 4 mm or not), use of calcar specific screw. Malreduction of the greater tuberosity is defined as out of 5 to 10 mm under the tangent line of the humeral head, perpendicular to the humeral shaft axis according to previous studies [17,18]. Greater tuberosity resorption was defined as more than one half decrease in the diameter of greater tuberosity in the follow-up period compared with initial postoperative plain film. Inadequate medial support is defined as either no intact or anatomically reduced calcar, no stable head-on-shaft impaction or no superiorly directed oblique locking screw that was appropriately placed into the infero-medial quadrant of the proximal humeral head fragment on the immediate postoperative radiograph. For postoperative functional outcomes, the Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire was used for evaluation.
Those with greater tuberosity resorption or malreduction were independently matched on age and sex by use of propensity score to those without resorption or malreduction (n = 19) in a 1:1 ratio for further analysis.
2.5. Statistical analysis
Continuous variables were described with use of means, standard deviation, and ranges. Categorical variables were tabulated with absolute and relative frequencies. Numerical data were studied with the Student t test. Categorical variables were studied with Chi-Square test of independence. The significant difference is defined as P < 0.05.
3. Results
In all 94 patients included, the mean age is 63.32 years old, with 31 males (33%) and 63 females (67%). The average height is 159.16 cm and weight is 63.94 kg with average BMI 25.09 kg/m2. 9 persons (9.57%) with habit of alcohol consumption and 8 persons (8.51%) with habit of smoking were found. The average deltoid tuberosity index measured on plain radiograph is 1.41. 82 patients were classified as AO/OTA 11B1.1 (87%) and 12 as AO/OTA 11C3 (13%). The average interval from injury to surgery was 2.93 days and average follow up period was 45.55 weeks. Postoperative greater tuberosity resorption was found in 13 patients (13.82%) and malreduction was noted in 11 patients (11.7%). We pooled them together for analysis and there were 19 patients noted with the event of postoperative greater tuberosity resorption or malreduction. The average period from surgery to first notice of the event is 8.77 weeks. (Table 1)
The demographic and fracture characteristics between the 19 patients with greater tuberosity resorption or malreduction and the matched groups are similar except for BMI. The average BMI is 27.35 kg/m2 in the resorption or malreduction group and 23.85 kg/m2 in the matched group, with significance difference (p value < 0.05). (Table 2)
In the comparison of the immediate postoperative radiographic parameters between the greater tuberosity resorption or malreduction group and the matched group, the results are similar in lateral humeral offset, head diameter, head height, perpendicular height and neck shaft angle. There are significant difference in the results of superior displacement of the greater tuberosity above articular surface, medial gap more than 4mm and the use of calcar specific screw. (Table 3)
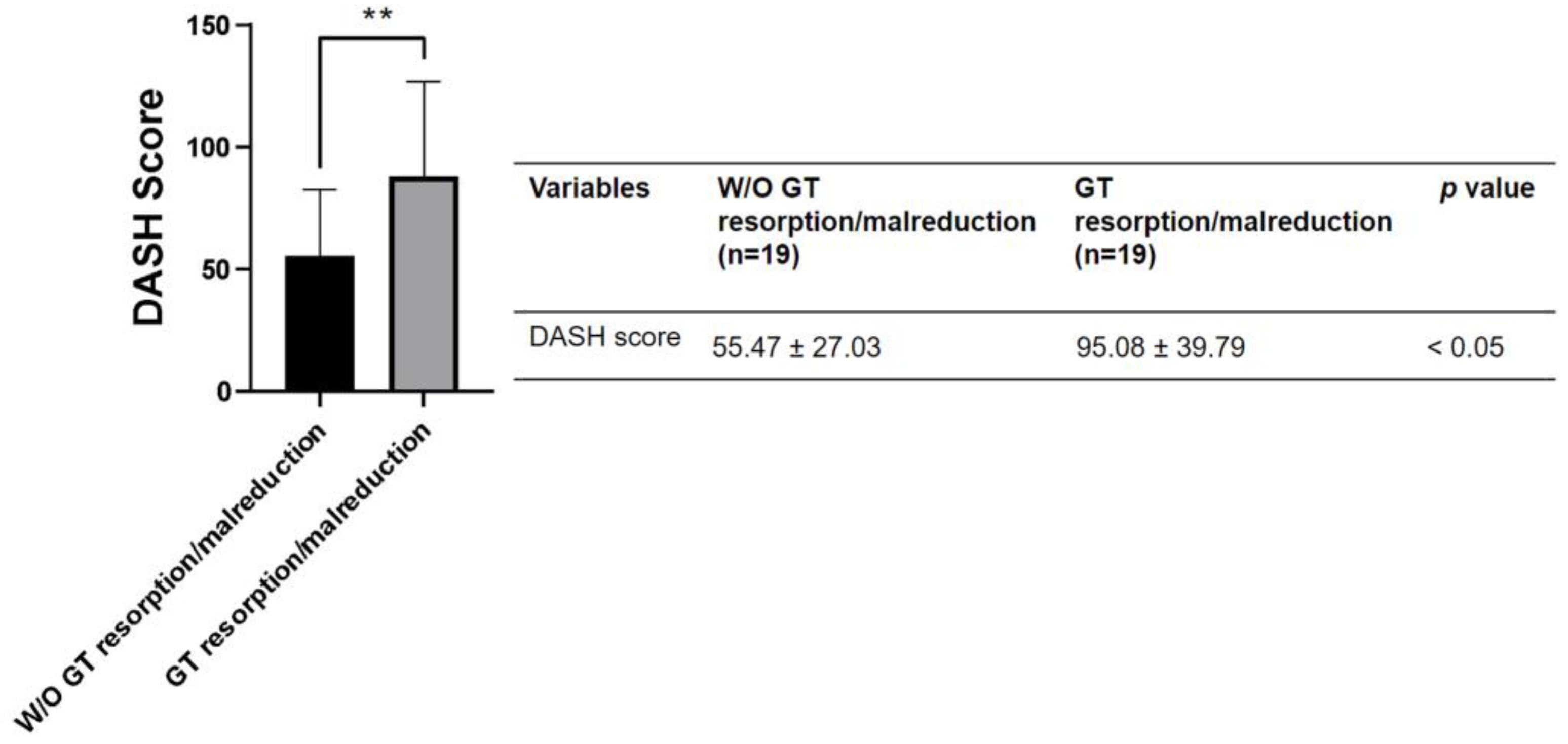
There are significant differences in the clinical outcomes between the resorption or malreduction groups and the matched group, with the average DASH score 95.08 and 55.47 respectively and p value < 0.05.
Figure 3.
Postoperative function outcome (DASH score) in patient with or without greater tuberosity resorption or malreduction.
Figure 3.
Postoperative function outcome (DASH score) in patient with or without greater tuberosity resorption or malreduction.
4. Discussion
The shoulder girdle is the link between the trunk and the upper extremities and is the most dynamic and mobile joint in the body. It consists of many articulations and the glenohumeral joint is no doubt the main contributor of its motion [19]. The proximal humerus, from both an anatomical and a fracture perspective, is conceptualized as consisting the humeral head, the greater and the lesser tuberosities and the humeral shaft, as first proposed by Neer in 1970 [20,21]. The greater tuberosity is located laterally on the proximal humerus. It serves as the insertion site of three tendons: the supraspinatus tendon superiorly, the infraspinatus tendon posterosuperiorly, and the teres minor tendon posteroinferiorly [22]. The greater tuberosity is positioned on average of 9 mm (range from 6 to 10 mm) below the most proximal aspect of the humeral head. This head-to-tuberosity distance is extremely important to allow adequate rotator cuff function. Insufficient rotator cuff tension and subacromial impingement may occur if the greater tuberosity heals excessively proximal. On the contrary, cuff strain and failure may occur if it is placed too low. It has been shown that inability to reconstitute the normal head-tuberosity distance leads to suboptimal results in both anatomical fracture reconstruction and arthroplasty [17,18]. Clavert et al. (2010) also indicated that the clinical outcomes were influenced by the quality of the greater tuberosity, with inferior Constant score noted in the patients with a malunion of the greater tuberosity [23]. In this retrospective comparative study assessing 94 complex proximal humeral fractures that underwent ORIF, the presence of postoperative greater tuberosity resorption or malreduction is associated with a higher DASH score, which indicates poor clinical outcomes.
Based on the fact that the average time to determine the development of greater tuberosity resorption was 14.72 weeks after surgery and the average time to determine the development of greater tuberosity malreduction was 4.2 weeks after surgery, we inferred that the cause of malreduction is early construct failure (e.g., knot loosening of the suture through the rotator cuff or tissue cut through by the suture) and the cause of resorption is avascular necrosis or atrophic nonunion despite a strong suture fixation. According to Ministry of Health and Welfare in Taiwan, obesity is defined as BMI ≧ 27.0 and in the demographic analysis, we found that obesity is related to postoperative greater tuberosity resorption or malreduction. A number of factors have been identified to affect bone healing, and obesity is one of them [24]. There is a complex relationship between obesity and bone. Obesity affects bone metabolism in many ways, both potentially positive and negative, and its net influence is controversial [25,26,27,28,29]. Obesity is traditionally believed to be beneficial to bone health owing to a well-established positive effect of mechanical loading conferred by body weight to stimulate bone formation by decreasing apoptosis and increasing proliferation and differentiation of osteoblasts and osteocytes [30]. Also, greater amount of estrogens, a protecting factor against osteoporosis by reducing bone resorption and stimulating bone formation, present in the adipose tissue [31]. Nevertheless, obesity may decrease bone formation while increasing adipogenesis because adipocyte and osteoblasts are derived from a common multi-potential mesenchymal stromal cell [32]. Moreover, obesity may increase osteoclastogenesis and bone resorption through upregulating proinflammatory cytokines such as IL-6 and TNF-α, which are capable of stimulating osteoclast activity through the RANKL/RANK/OPG pathway [33,34,35]. Aside from its impact on bone, obesity also increases the risk of tendinopathy, enthesopathy, tendon tear and rupture, and postoperative complications [36,37]. Several studies have shown that, in obese subjects, tendons frequently undergo degeneration. Higher BMI was associated with macroscopic tendon changes such as greater thickness but lower stiffness [38,39]. The main histopathological findings are a relative paucity of small collagen fibrils, impaired remodeling process, deposition of lipid droplets which can lead to tendolipomatosis, and a disorganized architecture in the tension site [40,41]. Preclinical studies also demonstrated that the tendons of rats with obesity induced by high-fat-diet had compromised biomechanical and healing properties [42,43]. The cause might be the increased mechanical stress and low-grade, chronic inflammatory microenvironment [44]. The inflammatory status seems to be caused by adipocytes because they suffer from hypoxic, mechanical, and oxidative stress secondary to cell hypertrophy, ultimately leading to cellular apoptosis, release of the intracellular pro-inflammatory molecules and continues recalling of macrophages [45,46,47,48]. The relatively poor quality of the rotator cuff tendon in an obese patient might lead to tissue cut through by the suture, leading to early malreduction of the greater tuberosity. Excessive instability, caused by poor quality of the tendon accompanied with compromised vascularisation owing to fracture and surgical intervention, might merely permit the formation of fibrous tissue and the development of an atrophic non-union [41], eventually seen on X ray as greater tuberosity resorption.
The influence of local bone mineral density (BMD) on proximal humeral fractures is controversial [49,50,51,52,53]. For example, Fankhauser et al. [49] in their cadaver study found that low local BMD negatively affects the stability of ORIF of proximal humerus. Krappinger et al. [51] in their clinical study found that low local BMD to be a predictor for later failure of ORIF. However, Franz Kralinger et al. [50] in their clinical study did not find evidence of an association between BMD and the rate of mechanical failures. Anil Taskesen et al. [52] found that osteoporosis is not the main factor affecting the surgical outcomes in proximal humeral fractures. Mats Bue et al. [53] also showed that osteoporosis does not affect the functional outcome after ORIF of displaced 3- or 4-part proximal humeral fractures in a prospective multicenter study. In concern of nonunion, a cohort nested case-control study also showed that osteoporosis is not a risk factor for the development of nonunion [54]. Merely focusing on the greater tuberosity of the humerus, the data is scarce. Satoshi Miyamura et al. [15] in their clinical study showed that greater tuberosities with a larger number of fragments, smaller fragments, and fragments with a lower bone density have higher rates of resorption. In current literature, local bone mineral density could be measured with methods ranging from measuring the cortical thickness on AP radiographs, dual-emission X-ray absorptiometry, to calculating BMD on peripheral quantitative CT scans [55,56,57,58]. On AP radiographs of the shoulder, the combined cortical thickness (Tingart measurement) is a frequent reported method used to measure bone quality [58]. Deltoid tuberosity index is another simple and effective method reported for measuring the bone quality with good correlation with peripheral quantitative CT scans and Tingart measurement [16]. In our study, we use deltoid tuberosity index to measure the local BMD and check whether there is an association between postoperative greater tuberosity resorption or malreduction and local bone mineral density. However, in our study, there is no significant difference between the matched two groups.
In our comparison of the immediate postoperative radiographic parameters between groups with and without greater tuberosity resorption or malreduction, significant differences were found in superior displacement of greater tuberosity above articular surface, medial gap > 4mm, and the use of calcar specific screws. These radiographic parameters are related to the quality of reduction and stability of fixation that influence functional outcomes [59]. Medial gap > 4 mm means a comminuted medial cortex or a non-anatomical reduced medial hinge. In such condition, if there is no calcar screw providing medial support, a higher rate of varus collapse was reported by Dheenadhayalan et al. [59] In our study, 16 of 19 patients with greater tuberosity resorption or malreduction were found to have superior displacement of greater tuberosity above articular surface in the immediate postoperative radiograph. Among which, 13 patients were noted with greater tuberosity resorption and 11 patients had further greater tuberosity displacement that meet the definition of malreduction. In our opinion, superior displacement of the greater tuberosity above the articular surface could be viewed as a risk factor of late malposition or resorption. Other radiographic parameters such as lateral humeral offset, head diameter, head height, perpendicular height, neck shaft angle are reported to be related to functional outcome [60]. In our study, there is no significant difference between the two groups.
5. Conclusion
Post-operative greater tuberosity resorption or malreduction is associated with poor prognostic outcomes in patients with proximal humeral fractures treated with ORIF. Surgeons should be committed to obtain an adequate reduction and secure fixation of the greater tuberosity on a stable locking plate construct. Obesity, a patient specific risk factor which is modifiable, should be dealt with in a multidisciplinary approach.
6. Limitation
First, this is a retrospective study. In this study, DASH score was used to assess functional outcomes. It is a questionnaire assessing patient’s function subjectively. Range of motion of the shoulders were not assessed. Second, due to the vast majority of the subjects are old patients, some comorbidities such as cancer, senile dementia, Parkinsonism and geriatric frailty might bias the results. Further studies are needed to investigate this problem.
Funding
This study was financially supported by Taipei Medical University Shuang Ho Hospital Grant (112HHR-08).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Taipei Medical University.
Informed Consent Statement
nil.
Data Availability Statement
Data is unavailable due to privacy or ethical restrictions.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Nordqvist, A.; Petersson, C.J. Incidence and causes of shoulder girdle injuries in an urban population. J Shoulder Elbow Surg 1995, 4, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Johnell, O.; Kanis, J.A. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int 2006, 17, 1726–1733. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Szabo, R.M.; Marder, R.A. Epidemiology of humerus fractures in the United States: nationwide emergency department sample, 2008. Arthritis Care Res (Hoboken) 2012, 64, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Horak, J.; Nilsson, B.E. Epidemiology of fracture of the upper end of the humerus. Clin Orthop Relat Res 1975, 250–253. [Google Scholar] [CrossRef]
- Tornetta, P., III. Rockwood and Green’s fractures in adults, 9th ed.; Wolters Kluwer: Philadelphia, 2020; Volume 1. [Google Scholar]
- Bell, J.E.; et al. Trends and variation in incidence, surgical treatment, and repeat surgery of proximal humeral fractures in the elderly. J Bone Joint Surg Am 2011, 93, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Calvo, E.; et al. Nondisplaced proximal humeral fractures: high incidence among outpatient-treated osteoporotic fractures and severe impact on upper extremity function and patient subjective health perception. J Shoulder Elbow Surg 2011, 20, 795–801. [Google Scholar] [CrossRef]
- Siffri, P.C.; et al. Biomechanical analysis of blade plate versus locking plate fixation for a proximal humerus fracture: comparison using cadaveric and synthetic humeri. J Orthop Trauma 2006, 20, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Papadopoulos, P.; et al. Mid-term results of internal fixation of proximal humeral fractures with the Philos plate. Injury 2009, 40, 1292–1296. [Google Scholar] [CrossRef]
- Björkenheim, J.M.; Pajarinen, J.; Savolainen, V. Internal fixation of proximal humeral fractures with a locking compression plate: a retrospective evaluation of 72 patients followed for a minimum of 1 year. Acta Orthop Scand 2004, 75, 741–745. [Google Scholar] [CrossRef]
- Kavuri, V.; et al. Complications Associated with Locking Plate of Proximal Humerus Fractures. Indian J Orthop 2018, 52, 108–116. [Google Scholar] [CrossRef]
- Aksu, N.; et al. Complications encountered in proximal humerus fractures treated with locking plate fixation. Acta Orthop Traumatol Turc 2010, 44, 89–96. [Google Scholar] [CrossRef]
- Südkamp, N.; et al. Open reduction and internal fixation of proximal humeral fractures with use of the locking proximal humerus plate. Results of a prospective, multicenter, observational study. J Bone Joint Surg Am 2009, 91, 1320–1328. [Google Scholar] [CrossRef] [PubMed]
- Egol, K.A.; et al. Early complications in proximal humerus fractures (OTA Types 11) treated with locked plates. J Orthop Trauma 2008, 22, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Miyamura, S.; et al. Bone resorption of the greater tuberosity after open reduction and internal fixation of complex proximal humeral fractures: fragment characteristics and intraoperative risk factors. J Shoulder Elbow Surg 2021, 30, 1626–1635. [Google Scholar] [CrossRef] [PubMed]
- Spross, C.; et al. Deltoid Tuberosity Index: A Simple Radiographic Tool to Assess Local Bone Quality in Proximal Humerus Fractures. Clin Orthop Relat Res 2015, 473, 3038–3045. [Google Scholar] [CrossRef] [PubMed]
- Boileau, P.; et al. Tuberosity malposition and migration: reasons for poor outcomes after hemiarthroplasty for displaced fractures of the proximal humerus. J Shoulder Elbow Surg 2002, 11, 401–412. [Google Scholar] [CrossRef] [PubMed]
- Iannotti, J.P.; et al. The normal glenohumeral relationships. An anatomical study of one hundred and forty shoulders. J Bone Joint Surg Am 1992, 74, 491–500. [Google Scholar] [CrossRef] [PubMed]
- Nordin, M. Basic Biomechanics of the Musculoskeletal System, 5th ed.; Lippincott Williams & Wilkins: Philadelphia, 2022. [Google Scholar]
- CHARLES S NEER, II. Displaced Proximal Humeral Fractures: Part I. Classification and Evaluation. JBJS 1970, 52, 1077–1089. [Google Scholar] [CrossRef]
- Neer, C.S., 2nd. Four-segment classification of proximal humeral fractures: purpose and reliable use. J Shoulder Elbow Surg 2002, 11, 389–400. [Google Scholar] [CrossRef]
- Mochizuki, T.; et al. Humeral insertion of the supraspinatus and infraspinatus. New anatomical findings regarding the footprint of the rotator cuff. J Bone Joint Surg Am 2008, 90, 962–969. [Google Scholar] [CrossRef]
- Clavert, P.; et al. Pitfalls and complications with locking plate for proximal humerus fracture. J Shoulder Elbow Surg 2010, 19, 489–494. [Google Scholar] [CrossRef]
- Zura, R.; et al. Epidemiology of Fracture Nonunion in 18 Human Bones. JAMA Surg 2016, 151, e162775. [Google Scholar] [CrossRef]
- Rinonapoli, G.; et al. Obesity and Bone: A Complex Relationship. International Journal of Molecular Sciences 2021, 22, 13662. [Google Scholar] [CrossRef] [PubMed]
- Hou, J.; et al. Obesity and Bone Health: A Complex Link. Frontiers in Cell and Developmental Biology 2020, 8. [Google Scholar] [CrossRef] [PubMed]
- Savvidis, C.; Tournis, S.; Dede, A.D. Obesity and bone metabolism. Hormones 2018, 17, 205–217. [Google Scholar] [CrossRef] [PubMed]
- Greco, E.A.; Lenzi, A.; Migliaccio, S. The obesity of bone. Ther Adv Endocrinol Metab 2015, 6, 273–286. [Google Scholar] [CrossRef]
- Cao, J.J. Effects of obesity on bone metabolism. J Orthop Surg Res 2011, 6, 30. [Google Scholar] [CrossRef] [PubMed]
- Ehrlich, P.J.; Lanyon, L.E. Mechanical strain and bone cell function: a review. Osteoporos Int 2002, 13, 688–700. [Google Scholar] [CrossRef] [PubMed]
- Riggs, B.L. The mechanisms of estrogen regulation of bone resorption. The Journal of Clinical Investigation 2000, 106, 1203–1204. [Google Scholar] [CrossRef]
- Rosen, C.J.; Bouxsein, M.L. Mechanisms of disease: is osteoporosis the obesity of bone? Nat Clin Pract Rheumatol 2006, 2, 35–43. [Google Scholar] [CrossRef]
- Wei, S.; et al. IL-1 mediates TNF-induced osteoclastogenesis. The Journal of Clinical Investigation 2005, 115, 282–290. [Google Scholar] [CrossRef] [PubMed]
- Khosla, S. Minireview: the OPG/RANKL/RANK system. Endocrinology 2001, 142, 5050–5055. [Google Scholar] [CrossRef] [PubMed]
- Taguchi, Y.; et al. Interleukin-6-type cytokines stimulate mesenchymal progenitor differentiation toward the osteoblastic lineage. Proc Assoc Am Physicians 1998, 110, 559–574. [Google Scholar] [PubMed]
- Macchi, M.; et al. Obesity Increases the Risk of Tendinopathy, Tendon Tear and Rupture, and Postoperative Complications: A Systematic Review of Clinical Studies. Clin Orthop Relat Res 2020, 478, 1839–1847. [Google Scholar] [CrossRef] [PubMed]
- Abate, M.; et al. Metabolic syndrome associated to non-inflammatory Achilles enthesopathy. Clin Rheumatol 2014, 33, 1517–1522. [Google Scholar] [CrossRef] [PubMed]
- Taş, S.; et al. Patellar tendon mechanical properties change with gender, body mass index and quadriceps femoris muscle strength. Acta Orthop Traumatol Turc 2017, 51, 54–59. [Google Scholar] [CrossRef]
- Al-Qahtani, M.; et al. Body Mass Index and Segmental Mass Correlation With Elastographic Strain Ratios of the Quadriceps Tendon. J Ultrasound Med 2019, 38, 2005–2013. [Google Scholar] [CrossRef]
- Abate, M. How obesity modifies tendons (implications for athletic activities). Muscles Ligaments Tendons J 2014, 4, 298–302. [Google Scholar] [CrossRef]
- Biancalana, A.; Veloso, L.A.; Gomes, L. Obesity affects collagen fibril diameter and mechanical properties of tendons in Zucker rats. Connect Tissue Res 2010, 51, 171–178. [Google Scholar] [CrossRef]
- Ackerman, J.E.; et al. Obesity/Type II diabetes alters macrophage polarization resulting in a fibrotic tendon healing response. PLoS One 2017, 12, e0181127. [Google Scholar] [CrossRef]
- David, M.A.; et al. Tendon repair is compromised in a high fat diet-induced mouse model of obesity and type 2 diabetes. PLoS One 2014, 9, e91234. [Google Scholar] [CrossRef]
- Abate, M.; et al. Achilles tendinopathy in amateur runners: role of adiposity (Tendinopathies and obesity). Muscles Ligaments Tendons J 2012, 2, 44–48. [Google Scholar]
- Wasim, M.; et al. Role of Leptin Deficiency, Inefficiency, and Leptin Receptors in Obesity. Biochem Genet 2016, 54, 565–572. [Google Scholar] [CrossRef]
- Matarese, G.; et al. Regulatory T cells in obesity: the leptin connection. Trends Mol Med 2010, 16, 247–256. [Google Scholar] [CrossRef]
- Haanen, C.; Vermes, I. Apoptosis and inflammation. Mediators Inflamm 1995, 4, 5–15. [Google Scholar] [CrossRef]
- Kuroda, M.; Sakaue, H. Adipocyte Death and Chronic Inflammation in Obesity. J Med Invest 2017, 64, 193–196. [Google Scholar] [CrossRef] [PubMed]
- Fankhauser, F.; et al. Cadaveric-biomechanical evaluation of bone-implant construct of proximal humerus fractures (Neer type 3). J Trauma 2003, 55, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Kralinger, F.; et al. The Influence of Local Bone Density on the Outcome of One Hundred and Fifty Proximal Humeral Fractures Treated with a Locking Plate. J Bone Joint Surg Am 2014, 96, 1026–1032. [Google Scholar] [CrossRef] [PubMed]
- Krappinger, D.; et al. Predicting failure after surgical fixation of proximal humerus fractures. Injury 2011, 42, 1283–1288. [Google Scholar] [CrossRef]
- Taskesen, A.; et al. Effect of Osteoporosis on Proximal Humerus Fractures. Geriatr Orthop Surg Rehabil 2020, 11, 2151459320985399. [Google Scholar] [CrossRef] [PubMed]
- Bue, M.; et al. Osteoporosis does not affect bone mineral density change in the proximal humerus or the functional outcome after open reduction and internal fixation of unilateral displaced 3- or 4-part fractures at 12-month follow-up. Journal of Shoulder and Elbow Surgery 2023, 32, 292–301. [Google Scholar] [CrossRef]
- van Wunnik, B.P.; et al. Osteoporosis is not a risk factor for the development of nonunion: A cohort nested case-control study. Injury 2011, 42, 1491–1494. [Google Scholar] [CrossRef] [PubMed]
- Diederichs, G.; et al. Assessment of bone quality in the proximal humerus by measurement of the contralateral site: a cadaveric analyze. Arch Orthop Trauma Surg 2006, 126, 93–100. [Google Scholar] [CrossRef]
- Krappinger, D.; et al. Preoperative assessment of the cancellous bone mineral density of the proximal humerus using CT data. Skeletal Radiol 2012, 41, 299–304. [Google Scholar] [CrossRef]
- Mather, J.; et al. Proximal humerus cortical bone thickness correlates with bone mineral density and can clinically rule out osteoporosis. J Shoulder Elbow Surg 2013, 22, 732–738. [Google Scholar] [CrossRef] [PubMed]
- Tingart, M.J.; et al. The cortical thickness of the proximal humeral diaphysis predicts bone mineral density of the proximal humerus. J Bone Joint Surg Br 2003, 85, 611–617. [Google Scholar] [CrossRef] [PubMed]
- Dheenadhayalan, J.; et al. Correlation of radiological parameters to functional outcome in complex proximal humerus fracture fixation: A study of 127 cases. J Orthop Surg (Hong Kong) 2019, 27, 2309499019848166. [Google Scholar] [CrossRef]
- Ahrend, M.D.; et al. Radiographic parameter(s) influencing functional outcomes following angular stable plate fixation of proximal humeral fractures. Int Orthop 2021, 45, 1845–1852. [Google Scholar] [CrossRef]
Figure 1.
Flow chart of inclusion and exclusion criteria of the study cohort of patients with proximal humeral fractures.
Figure 1.
Flow chart of inclusion and exclusion criteria of the study cohort of patients with proximal humeral fractures.
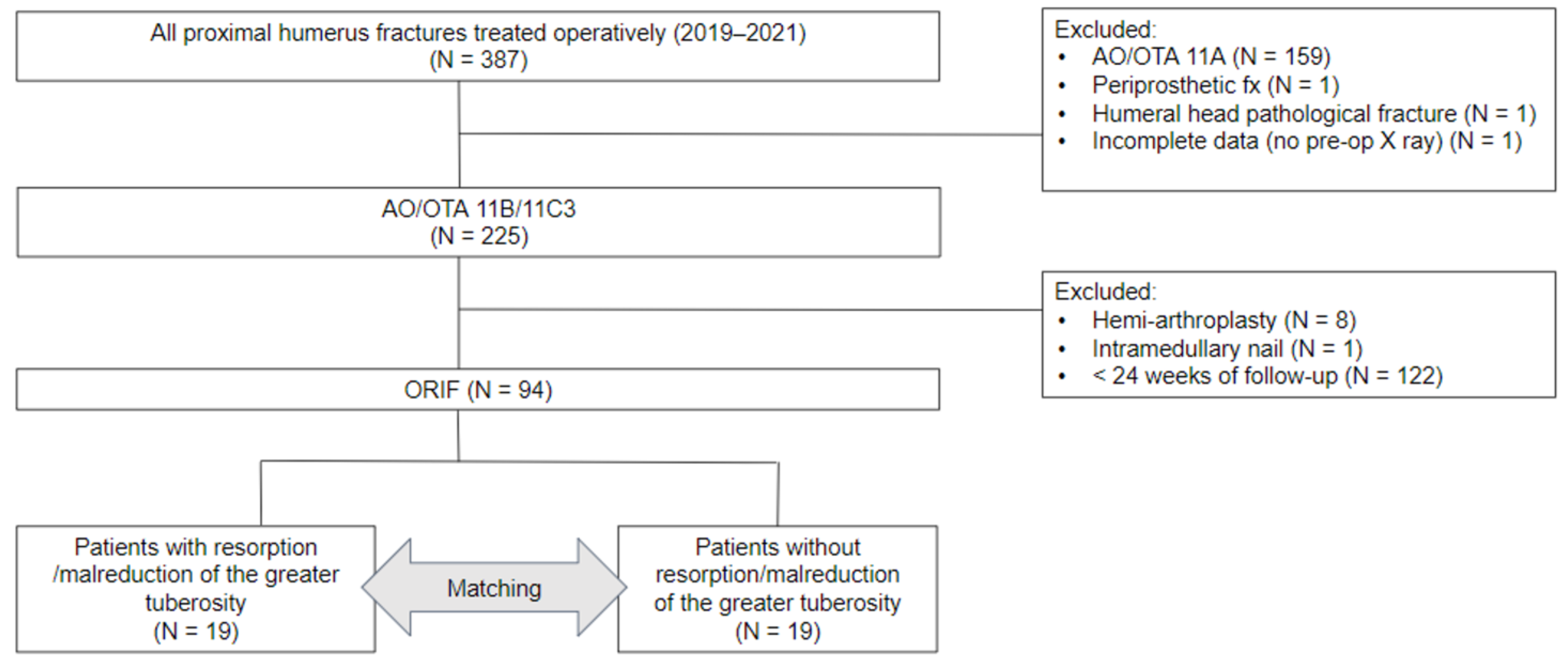
Figure 2.
Plan radiographic evaluation of patient’s injured shoulder joint with greater tuberosity (GT) absorption or malreduction during follow-up period. (A–C) GT absorption was noted at 3 months postoperatively. The red arrowheads point out the radiolucent zone indicating GT absorption. (D–F) Postoperative plain radiographs of patient presented with GT malreduction. The GT fragment was well-reduced to its anatomical position in the initial postoperative image. (2D). At 1-month after surgery, GT was found displaced superiorly and posteriorly (2E) and was remained at malreduction position (white arrowheads) throughout follow-up period (2F).
Figure 2.
Plan radiographic evaluation of patient’s injured shoulder joint with greater tuberosity (GT) absorption or malreduction during follow-up period. (A–C) GT absorption was noted at 3 months postoperatively. The red arrowheads point out the radiolucent zone indicating GT absorption. (D–F) Postoperative plain radiographs of patient presented with GT malreduction. The GT fragment was well-reduced to its anatomical position in the initial postoperative image. (2D). At 1-month after surgery, GT was found displaced superiorly and posteriorly (2E) and was remained at malreduction position (white arrowheads) throughout follow-up period (2F).
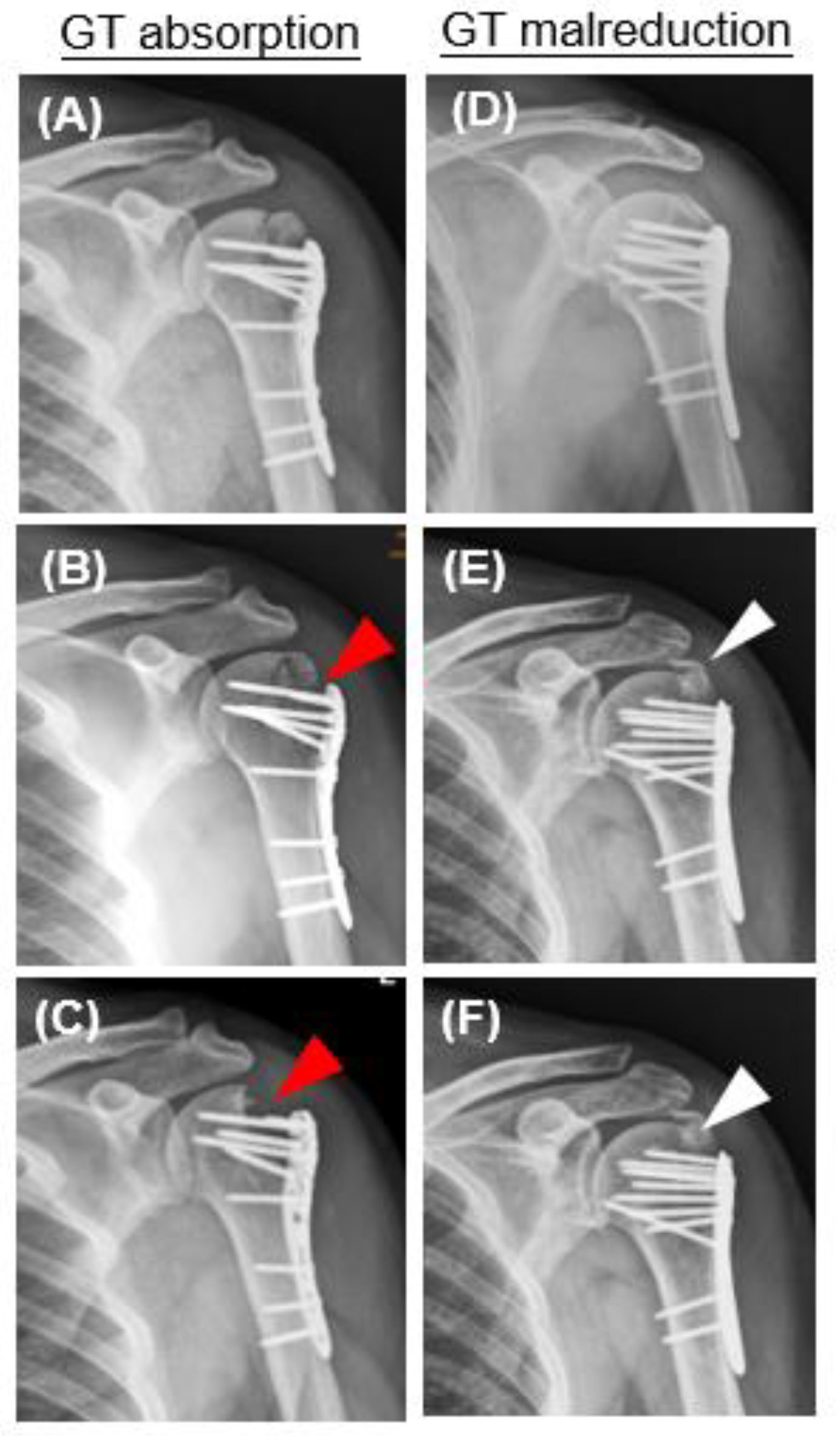

Table 1.
Demographic and surgical characteristics of patients with proximal humeral fractures treated operatively.
Table 1.
Demographic and surgical characteristics of patients with proximal humeral fractures treated operatively.
| Patients (n = 94) | Variables |
|---|---|
| Age (year) | 63.32 ± 14.6 |
| Gender | |
| Male | 31; 33% |
| Female | 63; 67% |
| Height (cm) | 159.16 ± 9.54 |
| Weight (Kg) | 63.94 ± 14.41 |
| BMI (Kg/m2) | 25.09 ± 4.53 |
| Alcohol consumption | 9/94 (9.57%) |
| Smoking | 8/94 (8.51%) |
| Deltoid tuberosity index | 1.41 ± 0.16 |
| Neer classification | |
| 2-part | 26/94 (27%) |
| 3-part | 60/94 (64%) |
| 4-part | 8/94 (9%) |
| AO/OTA classification | |
| 11B1.1 | 82/94 (87%) |
| 11C3 | 12/94 (13%) |
| Time to surgery (day) | 2.93 ± 5.40 |
| Time of follow up (weeks) | 45.55 ± 25.62 |
| Greater tuberosity resorption | 13/94 (13.82%) |
| Malreduction of greater tuberosity | 11/94 (11.7%) |
| Time from surgery to GT resorption or malreduction (week) | 8.77 ± 7.86 |
BMI: body mass index.
Table 2.
Demographic and surgical characteristics of matched patients with proximal humeral fractures with or without greater tuberosity resorption or malreduction. Values are presented as numbers or mean ± standard deviation.
Table 2.
Demographic and surgical characteristics of matched patients with proximal humeral fractures with or without greater tuberosity resorption or malreduction. Values are presented as numbers or mean ± standard deviation.
| Variables | W/O GT resorption/malreduction (n = 19) | GT resorption/malreduction (n = 19) | P value |
|---|---|---|---|
| Age (year) | 70.58 ± 10.62 | 70.68 ± 11.04 | n.s |
| Male | 4/19 (21%) | 4/19 (21%) | n.s |
| Female | 15/19 (79%) | 15/19 (79%) | n.s |
| Height (cm) | 157.42 ± 8.92 | 155.95 ± 7.71 | n.s |
| Weight (Kg) | 59.05 ± 9.16 | 67.16 ± 17.92 | n.s |
| BMI (Kg/m2) | 23.85 ± 3.37 | 27.35 ± 6.03 | 0.0337 |
| Smoking | 0/19 (0%) | 1/19 (5%) | n.s |
| Alcohol consumption | 1/19 (5%) | 1/19 (5%) | n.s |
| Deltoid tuberosity index | 1.36 ± 0.15 | 1.41 ± 0.13 | n.s |
| Neer classification | |||
| 2-part | 6/19 (32%) | 6/19 (32%) | n.s |
| 3-part | 13/19 (68%) | 11/19 (58%) | n.s |
| 4-part | 0/19 (0%) | 1/19 (10%) | n.s |
| AO/OTA classification | |||
| 11B1.1 | 18/19 (95%) | 17/19 (89%) | n.s |
| 11C3 | 1/19 (5%) | 2/19 (11%) | n.s |
| Time to surgery (day) | 4.11 ± 7.02 | 4.32 ± 8.45 | n.s |
| Time of follow up (week) | 40.48 ± 26.22 | 42.23 ± 29.01 | n.s |
| Artificial bone graft use | 11/19 (58%) | 12/19 (63%) | n.s |
| Inadequate medial support | 0/19 (0%) | 3/19 (16%) | n.s |
Table 3.
Comparison of postoperative radiographic parameters in patients with or without GT resorption or malreduction.
Table 3.
Comparison of postoperative radiographic parameters in patients with or without GT resorption or malreduction.
| Variables | W/O GT resorption/malreduction (n = 19) | GT resorption/malreduction (n = 19) | P value |
|---|---|---|---|
| Lateral humeral offset (cm) | 4.85 ± 0.44 | 4.56 ± 0.44 | n.s |
| Head diameter (cm) | 4.71 ± 0.45 | 4.5 ± 0.34 | n.s |
| Head height (cm) | 1.72 ± 0.2 | 1.68 ± 0.28 | n.s |
| Perpendicular height (cm) | 4.95 ± 0.6 | 4.69 ± 0.61 | n.s |
| Neck shaft angle (degree) | 138.27 ± 13.73 | 137.82 ± 9.6 | n.s |
| Superior displacement of GT above articular surface | 0/19 (0%) | 13/19 (68.42%) | 0.0463 |
| Medial gas > 4 mm | 0/19 (0%) | 5/19 (26.32%) | 0.0463 |
| Use of calcar specific screw | 19/19 (100%) | 16/19 (84.21%) | 0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



