Submitted:
28 November 2023
Posted:
29 November 2023
You are already at the latest version
Abstract
Background: Hospital accreditation has become ubiquitous in developing countries. Although studies recognize that accreditation can improve healthcare quality, efficiency, and safety, there are doubts about how hospitals deal with conflicts caused by the different institutional logics that inhabit this process. Therefore, this study aimed to investigate how professional and market logics, as well as the conflict between institutional demands, affect compliance with hospital accreditation. Methods: To this end, we developed a multiple case study in four Brazilian hospitals through in-depth interviews with sixteen participants (managers, physicians, nurses, physiotherapist) and on-site observation by the triangulation between the analysis of the narratives and the results of the multiple correspondence analysis. The interpretation and subsequent categorization of the interviews were guided by the study's analytical categories: institutional logics (professional and market); adoption objectives (legitimacy and efficiency); strategic responses to adoption (conformity, non-conformity, and customization); nature of demands (origin in the means and in goal). Results. The data showed that when professional logic is prominent, there is a greater tendency to customize activities, as there are conflicts in the means by which activities can be developed. When market logic stands out, there is a risk of non-conformity, mainly because the focus falls exclusively on goals. Finally, the data point to the absence of conflicts between justifications related to efficiency and legitimacy. Conclusion. We conclude the study by highlighting the theoretical and practical implications of recognizing the conflict between logics, contributing to a deeper understanding of how logic influences the attention given to specific demands and, more significantly, how they affect compliance with hospital accreditation standards, expanding the body of knowledge in the area.
Keywords:
hospital accreditation
; institutional logics
; organizational practices
; strategic responses
; institutional theory
1. Introduction
Hospital organizations around the world, including emerging countries, have been pressured to adopt health care standards that are certified by hospital accreditation programs [1,2,3,4,5]. Such programs consist of an evaluation process by a certifying authority, which verifies whether the hospital meets rigorous quality and safety standards in healthcare, attesting to its effectiveness [6,7]. However, despite the recognition that such programs lead to relevant structural changes in hospitals, there are doubts as to whether the results are effective [2,5,8,9].
Although studies indicate that the effectiveness of hospital accreditation refers to the commitment of management, access to resources, team leadership, and integration between professionals [5,10], few studies seek to understand which conflicts and contradictions culminate in difficulties in such processes [2]. Seeking to fill this gap, this article focuses on the complex dynamics surrounding hospital accreditation, exploring the conflicting influences of market and professional logic that manifest themselves in the daily lives of hospitals. To this end, we look at the literature on institutional logics in organizational theories [11,12], which points out that the process of change caused by the adoption of accreditation practices involves, on the one hand, a logic market, whose concern refers to economic and business issues, with a greater focus on objectives and efficiency measures [13,14,15]. On the other hand, from a professional perspective, which highlights aspects related to the exercise and identity of health professionals [2,16], who are immensely concerned with the work processes of medical care of patients [1,17].
Knowing that market and professional logics present contradictory aspects [13], we analyzed the consequences in four hospitals, interviewing evaluators from certification agencies, managers, physicians, nurses, and other professionals involved. First, we checked whether there was any relationship between the logic and objectives established for adoption, which refers to the search for efficiency and legitimacy before the audience [18,19]. Second, we checked hospitals' responses in terms of conformity, customization, and non-conformity with hospital accreditation norms and standards [19,20,21,22]. Third, we identified the conflicts that emerged regarding the demands on the middle activities, emphasizing certified practices and the objectives, whose focus was on the reasons or interests of senior management with the results [14,23]. Finally, given the duality between the material and symbolic aspects of hospital accreditation, we analyzed the overlap between the different analytical categories - logic, adoption objectives, responses, and nature of demands - through triangulation between the analysis of narratives [24] and multiple correspondence analysis (MCA), as such aspects are mutually constituted in the practical exercise of accreditation [25].
We argue that managers and professionals identified with market and professional logics tend to emphasize specific demands in the means or the goals [23]. As such, logics can be incompatible. To avoid extensive conflict, they are segmented into different parts of hospitals [26,27]. In the prominence of professional logic, conflicts are expected to be in the middle of activities, leading to customization. In the dominance of market logic, conflicts tend to be with the goals, leading to non-conformity. Indeed, this study aimed to investigate how professional and market logics and the conflict between institutional demands affect compliance with hospital accreditation.
This study offers significant contributions to the existing literature on hospital accreditation and institutional logics by analyzing the aspects raised in this argument. First, while previous research has primarily focused on assessing compliance in general terms [18], our study advances by exploring the complex interactions between market and professional logics in the specific context of hospital accreditation [23,27]. Second, in contrast to studies that have treated compliance as an end [19], our findings highlight how the salience of a specific logic can drive demands and conflicts in different directions [26]. Thus, we offer a deeper understanding of how hospital organizations face compliance and practice customization challenges in an environment where multiple logics often overlap [2,14]. Third, by emphasizing the distinction between demands on means and goals, our study also fills a gap in the literature, helping to clarify how specific demands affect accreditation [23].
We have organized this article into five parts in addition to the introduction. In the first part, we present the foundations of institutional logics, pointing out that hospital accreditation practices are constituted by two competing logics, market and professional, whose nature of demands, strategic responses, and adoption objectives may vary according to the emergency of such logics. Afterward, we detail the methodological aspects, highlighting the analytical categories and the triangulation between methods. Next, we present the results of narrative analysis and multiple correspondence analysis to, in the discussion section, derive a set of empirically verifiable propositions. Finally, we point out the theoretical and practical implications, highlighting the limitations and suggestions for future studies and drawing a conclusion.
2. Theoretical Framework
2.1. Institutional Logics
Institutional logics are "an order of production, composed of distinct individuals and objects mediated by a regime of material practice. Institutional logics point to […] orders of practice that depend on the particular identities of individuals and ontologies of objects, which, in turn, depend on these same orders of practice (p. 336)" [25]. This definition highlights the material and symbolic aspects of the adoption of organizational practices, which include hospital accreditation [13,14], which, in turn, is influenced by the identity and interests of members who work in the accreditation process [2,16].
According to Thornton et al. [12], the idea of institutional logic is introduced into organizational studies by Alford and Friedland [28] and Friedland and Alford [11] to understand the different practices and beliefs that shape institutions in Western society. Friedland et al. [25] argued that institutional logics are founded by institutional substances (or objects). These substances are not represented by something tangible or material but rather by unobservable reasons that can only be phenomenized through practice. Therefore, practice becomes the explicit part of these institutional substances.
In addition to positioning everyday practice as composed of symbolic issues such as values and interests, the institutional logics approach highlights both the contradictions between the ways of thinking of different groups that make up organizations [29] and the multiplicity of demands that organizations need to adapt [30]. Consequently, multiple logics increase institutional complexity [27], especially in organizational change processes, such as hospital accreditation [17].
This study highlights the contradictions between different logics that manifest themselves when they present competing aspects. This is because resistance to institutional change occurs both as a result of competition between logics, as well as the combination of environmental pressures [31], the institutional power of relevant actors [10,13] and the organization's strategic objectives [16,23].
In the hospital context, studies indicate that competing institutional logics explain how hospital organizations reacted to the regulation process [1] and can influence the strategies and practices adopted [30]. Furthermore, when looking at hospital accreditation, previous studies indicate that the contradiction between institutional logics can increase resistance to adoption, as physicians and nurses seek to emphasize their identity while avoiding acquiescing to market pressures [2,13,15].
Despite the existence of distinct institutional logics, this fact does not necessarily imply competition between them, as the convergence of these logics can also occur, or even the formation of a hybrid form, especially when there is pressure to adopt practices certified by external agencies, such as hospital accreditation [2,14].
2.2. Hospital Accreditation as an Institutional Standard
There is an extensive research agenda in using organizational institutionalism to analyze adopting organizational practices [18,21], mainly when such practices refer to certification processes [19]. Many studies have focused on adopting quality certifications, such as ISO9000 and other variants of total quality management [32,33], as well as environmental and sustainability certifications [34].
This literature maintains that the certification process, in addition to seeking to improve quality and productivity, which refers to reasons related to efficiency, also seeks to signal that the organization meets the criteria socially required by the audience [35]. Hospital accreditation processes would be no different [2,22].
In the health literature, there is widespread discussion about the institutional aspects of accreditation, often looking at the search for quality in hospital care [3,36,37] since its origins, in the United States, at the beginning of the 20th century, to the present day, around the world [4,38]. In Brazil, the first work focused on quality in hospital organization was in 1935, when Odair Pedroso prepared a form to evaluate hospital quality for the extinct Hospital Assistance Commission of the Ministry of Health [39].
Since then, several initiatives have taken place, but progress has been slow. Only in 1989, when the World Health Organization (WHO) gave significant importance to accreditation for the development of quality in healthcare in Latin America, this process gained strength in the country. Only almost ten years later, in 1998, the Brazilian Accreditation Commission (CBA) was created, the Brazilian representative of the Joint Commission International. A year later, it was the turn of the National Accreditation Organization (ONA), a typically national organization created after the launch of the Brazilian Accreditation Manual. Other accrediting organizations have since emerged. However, ONA and CBA stand out in the country for being the pioneers and having more customers.
The ONA defines hospital accreditation as a system of evaluation and certification of the quality of health services, whose character is eminently educational, voluntary, and without supervisory or regulatory purposes. It is worth mentioning that both Organizations, ONA, and CBA, are private organizations whose adherence to the process is done voluntarily and at a high financial cost. This definition of hospital accreditation is consistent with the frequently used literature, which sees it as an assessment of structures and processes conducted by an independent accreditation agent who verifies whether a hospital meets the ideal quality and safety requirements [5].
The accreditation process involves the entire hospital team: physicians, nurses, technicians, directors, managers, etc. Therefore, accreditation agencies follow a strict manual that contains a series of protocols that must be followed for the hospital to be accredited. This process differs from other certifications as it is exclusive to the health sector, involving more robust standards of ethics and morality [5] and more technical and effective aspects.
The quality search is explicit as being one of the objectives of this accreditation process [37]. However, hospital organizations certainly have other objectives that can influence the results. In this line of thought, how institutional logics condition the reach and even the formulation of these objectives is one of the questions this work seeks to answer. But what is the relationship between institutional logics and the results achieved and expected by the hospital accreditation process?
2.3. Institutional Logics Constituting the Hospital Accreditation Process
Previous studies that used organizational institutionalism to analyze the adoption of quality management practices emphasized the search for efficiency and legitimation [33,40]. In the last decade, in addition to this emphasis, studies have sought to understand how various social orders in society – capitalist market, the bureaucratic State, families, democracy, and religion, each with a central logic – can legitimize hospital activity [16,17].
Such studies on institutional logics in the health area, as well as seminal studies, found that two logics are very present in such organizations: market logic, interested in the commercial exploitation of hospital activity, and professional logic, which refers to aspects related to the exercise of medical care in hospitals [32,41,42]. The essence of such logics is presented in Table 1.
The technical specificity of healthcare professionals strengthens professional logic; however, the need for a market-oriented organization of hospital management is increasingly present in healthcare organizations [1]. However, there are doubts about how these logics operate, converging or diverging in hospital practices. In the search for quality certifications, a prevalent action in the hospital field, how do these logics help to understand organizational decisions?
Mintzberg [43] highlighted the importance of the operational core in Hospitals, where technicians in the sector have significant autonomy to dictate their work processes and highly influence the organizations' decision-making. This scenario allows us to identify the existence of a very present logic in the health field: professional logic. Based on the concepts of Friedland et al. [25], professional logic can be considered an institution jointly composed of a substance (profession), forms of subjectivity (emotions such as protection, dedication, zeal, and competition), and a set of practices (actions such as carrying out work in a prudent manner, search for quality, defense of the profession's rights). Aspects such as the relational network, professional associations, status, and quality search [12] are common and evident characteristics in healthcare organizations. Therefore, holders of technical knowledge strongly influence the organization's decision-making.
Under market logic, the private hospital organization aims for profit and, to this end, seeks to reduce costs, increase efficiency competitiveness, and reach more customers. In effect, market logic manifests itself as an institution with a substance (market), forms of subjectivity (characteristics that emerge, such as competitiveness, opportunism, and selfishness), and a set of practices (cost reduction, investments, increased production, mimicry).
It turns out that such logics coexist in the hospital context, which can coexist without significant difficulties. However, there are contradictions, so the answers regarding hospital accreditation can differ.
2.4. How do Hospitals Respond to the Hospital Accreditation Process?
The reason why organizations adopt practices is a question that persists in organizational studies. In addition to issues related to technical nature and efficiency issues, organizations adopt practices to legitimize themselves [35,44]. Thus, organizations, when implementing new practices such as hospital accreditation, seek to achieve legitimacy before the audience: "a generalized perception or assumption that an entity's actions are desirable or appropriate within a structure of norms, values, beliefs, and socially constructed beliefs (p. 574)" [45].
Despite the importance of legitimacy for organizations, many practices considered legitimate are adopted without effectiveness regarding actual organizational demands, which leads them to be exercised ceremonially. For example, a certificate hanging on the wall, where managers cannot even assess whether that document brings any practical benefit to the organization's activities, in addition to prestige and acceptability. It is important to emphasize that we are not discrediting the need for legitimacy here, as something legitimate does not necessarily need to be ceremonial [46].
From a possible ceremonial response, Oliver [21] developed a typology of strategic responses to institutional pressures, which even influenced investigations in the hospital area [18,19,20]. Such responses vary in degree of conformity and resistance and are classified as acquiescence, compromise, avoidance, defiance, and manipulation.
Although useful, Oliver's [21] theoretical model has limitations, as the Brazilian hospital accreditation process has a characteristic that must be taken into consideration: it is voluntary. That means that the hospital suffers little external regulatory pressure, whether from the State or other control organizations, making the existence of normative and cognitive pressures from professionals and clients more evident. Even so, given the non-obligation and little knowledge of customers about this process, internal pressures are more prominent and robust.
Voluntarily, the hospital organization must follow the protocols and practices pre-established by the certifying organization until it is accredited. After this period, there is no guarantee that it will follow these protocols, which may lead it to camouflage practices or act ceremonially before external actors, except when it needs to renew certification. Accreditation also does not accredit hospitals to have benefits for joining credit programs and participating in associations, among other facilitating aspects. According to ONA [47], hospital accreditation "has an eminently educational character, aimed at continuous improvement, without the purpose of inspection or official/governmental control, and should not be confused with licensing procedures and typical actions of State (p. 12)."
Such characteristics of accreditation diverge, in part, from the elements that conceptualize the responses established by Oliver's study [21], which does not mean that the only response to such certifications is mere acceptance. That's why we simplified organizational responses, seeking to make the analysis more objective and coherent with the research object: Conformity when the hospital fully complies with the accreditation process; Non-conformity, when the hospital does not meet the minimum requirements of the process; and Customization when the hospital partially meets the needs of the accreditation process, but customizes some actions, according to its convenience.
In addition to analyzing strategic responses, knowing what demands accreditation requires in its adoption is necessary. Thus, we consider where the nature of the demands is located: whether the demands are in the mean activities or whether they occur about the desired goals [23].
The nature of the demands allows us to identify where conflicts are present, either in the practice of the means to reach the goals set by the organization or in which goals the organization should pursue [23]. Conflict in the means is focused on how acting, such as implementation actions. In contrast, Conflict in goals indicates a disagreement in the reasons for adopting a particular practice.
Both the model proposed by Oliver [21] and the model developed by Pache and Santos [23] contribute significantly to identifying possible responses or behaviors of the organization in the face of existing logic that compete with each other. However, such models do not assess the importance or influence of specific logic in organizations' responses, making it impossible to identify whether different logic can provoke different responses.
For this reason, we analytically consider that organizational responses to the practice of hospital accreditation (conformity, customization, and non-conformity) refer both to the organization's objectives (efficiency and legitimacy) and the predominant competing logics (professional and market), as well as as the nature of the demands (in the means or the goals). To this end, it is essential to consider a possible competition of institutional logics within hospital organizations in the face of the accreditation process, as different institutional logics coexist [12].
Therefore, this study highlighted the logics most present in the hospital environment [13,41] so that the analytical representation of logics provides a more effective way of analyzing the results obtained. Furthermore, we modeled the study considering that logics must be investigated as practical achievements, in which demands of a material nature present a relationship of duality with issues of a symbolic nature [48,49], which led us to adopt triangulation of qualitative data with formal relational methods of analysis [25].
3. Materials and Methods
As the focus of the research was to understand the mechanisms through which institutional logics and the nature of demands affect hospital accreditation in terms of adequacy to objectives and types of strategic responses, we opted for the multiple case study strategy [50,51]. This choice was made due to the need to understand the complexity of such processes through an inductive process of categorization and analysis of interviews and observations at the research site [52].
Furthermore, as the literature already pointed out, what were the dominant logics regarding the hospital accreditation process [1,2,13,14], as well as which were the other analytical categories relevant for analysis, we followed the methodological recommendations for capturing institutional logics by Reay and Jones [53]. The authors point out that qualitative material must be analyzed, in such circumstances, based on previously defined analytical categories (Table 3). Even starting from a priori categories, we use inductive logic to generate propositions based on the analysis of qualitative material present in interviews and observations [54].
3.1. Selection of Hospitals, Participants, and Field Research
Firstly, a preliminary immersion was carried out in different accredited hospitals that completed the accreditation process recently to negotiate access to the target organizations of the investigation [55], which allowed us to observe the differences in the accreditation processes of the hospital. When listing the hospitals with the most remarkable capacity to reveal information, access to the field was negotiated with the leading managers. That was facilitated because one of the researchers has worked in health management for over a decade.
Thus, four hospitals in Rio de Janeiro, Brazil, were selected: two accredited by the National Accreditation Organization (ONA) and two by the Brazilian Accreditation Consortium (CBA). The choice of these two accrediting organizations is justified because both certifiers are already consolidated in the field and have a more significant number of accredited hospitals in Brazil.
Before the field research, information about the accreditation process from the ONA and CBA manuals regarding the evaluation forms and minimum requirements for obtaining the certificate was extracted. Next, in-depth interviews were carried out with an evaluator from each accrediting organization, aiming to enrich knowledge of the accreditation process and clarify doubts that existed when reading the manuals.
Table 2
presents the subjects involved in the field research, composed of managers directly involved with the accreditation process, based on 16 guiding questions, as well as physicians, nurses, and physiotherapists involved in the routine implementation of accreditation in the hospitals where they work, who openly answered 11 questions (see
Table 3
). The questionnaire used in the interviews was developed specifically for this study. It is available in the supplementary material, together with the consent letter.
In addition to the interviews, it was possible to observe the work routine of the hospitals during the field research and the functioning of some evaluation processes conducted by the accrediting organizations.
3.2. Ethical Aspects
The study did not need to be approved by the research ethics committee of the University of Grande Rio, as the rules of that university do not require that studies that do not involve risks for participants go through the committee, as long as the researchers comply with the aspects of the CNS/MS Resolution No. 466/2012.
It should be noted that both hospitals and respondents signed a research consent form, which declared the objective of the research, its strictly academic nature, and the preservation of participants' rights to confidentiality and withdrawal. The anonymity of the participants was maintained by replacing their names with their profession, adding an identifying number, and categorizing the hospital in which they were assigned using a letter (e.g., Physician 1 at Hospital B).
Finally, it should be noted that the researchers do not present any conflict of interest, being not directly involved with the accredited hospitals or the accreditation agents. Furthermore, the authors do not benefit directly or indirectly from the results of this study.
3.3. Measures
The interpretation and subsequent categorization of the interviews were guided by the study's analytical categories, described in Table 3, which presents the definition of each of the dimensions and which driving questions were used. Concerning Institutional Logics (professional and market), both managers and employees of accredited hospitals were interviewed to identify which institutional logic is most present in hospital accreditation, assuming they can compete in the adoption process [27]. Regarding the Adoption Objectives (legitimacy and efficiency), as it involves strategic choices made on behalf of hospitals, the focus was on hospital managers. However, we also looked for such elements in the speech of the other interviewees. Strategic Responses to Adoption (Conformity, Non-Conformity, and Customization), we sought to identify how hospitals responded to the accreditation process in practice. Although everyone has achieved the accreditation certificate, the level of adoption and internalization may vary. Finally, regarding the Nature of Demands (Origins in Means or Goals), we sought to assess where conflicts or actions contrary to the adoption of accreditation arose within organizations and which aspects were most emphasized by the different interviewees.

Table 3.
Analytical categories, dimensions, and questions used in the questionnaires.
| Categories | Definitions of dimensions for each category | Questions |
|---|---|---|
| Institutional Logics [2,12,23,34] | Professional Logic: Practices based on the performance of the health professional, advocating the quality of services, patient and professional safety, and ensuring reputation and protection. The decline in the quality of care and possible errors in hospital care serve as threatening mechanisms for this logic. | a) Are you in favor of implementing accreditation in the hospital? What improvements can accreditation bring to the hospital? b) Can you name the most significant difficulties you encountered during the accreditation process? c) When choosing to join the Hospital Accreditation program, were there differences of opinions or any conflict between the members of the management? d) What are the main obstacles/problems that the hospital faced in achieving this adoption during the process? |
| Market Logic: Focus on the organization's financial performance and status in the market in which it operates. Profit and organizational advancement are the main objectives. The main threatening mechanisms are poor financial results, decreased performance, operational efficiency, and increased costs. | ||
| Goals of Adoption [19,46] | Legitimacy: Focus on obtaining greater acceptance, respect, and status by stakeholders, involving customers, suppliers, and competitors. | a) When did the institution decide to adopt Hospital Accreditation in the Hospital? b) What do you understand as Hospital Accreditation? How would you define it? c) For what reasons was it decided to adopt Hospital Accreditation? Were there other options? d) Why do you consider Hospital Accreditation Important for the Hospital? e) What did the institution hope to achieve by adopting Hospital Accreditation? |
| Efficiency: The organization's primary focus is to improve the technical aspect of the activity it carries out, such as reducing costs, improving procedures, and increasing productivity, among others. | ||
| Strategic Responses [19,20,21,22] | Conformity: The hospital fully adopts the practices established by the Hospital Accreditation Program, remaining faithful to the precepts and protocols required even after certification. | a) Were all requirements strictly met, or could they be met with alternative methods? b) After obtaining certification, were all processes maintained? c) When the hospital is reassessed, what difficulties are encountered? d) Do you believe that everyone in your sector meets all the standards required by accreditation daily? e) If you were visited by an evaluator today, do you think the hospital would be accredited again? |
| Non-conformity: The hospital mostly rejects the practices established by the Hospital Accreditation program, maintaining only those already practiced or having less impact than competing logics. | ||
| Customization: The hospital organization mainly adopts the practices established by the Hospital Accreditation program but with modifications aimed at adapting them to the real needs of the hospital. | ||
| Nature of Demands [14,23,30] | Origin in the Means: When the nature of the demands originates in the means, these conflicts occurred during the accreditation process, that is, in their implementation and reproduction within the organization. | a) What are the main obstacles/problems that the hospital faced in achieving this adoption during the process? b) For what reasons was it decided to adopt Hospital Accreditation? Were there other options? c) Who was the decision made by? |
| Origin in Goals: When the source is located in the goals, these are actions contrary to the decision to adopt accreditation; the obstacles are located in the decision-making phase before implementation. |
Note: Five questions related to management were not asked of professionals.
3.4. Categorization of Interview Excerpts
The in-depth interviews and observations were organized into segments, which were interpreted by both researchers, assigning them categories through analysis of the content of the excerpts [56], in which similarity was sought between the narratives and the range of the categories [24,50]. Following previous studies [57], we sought greater reliability in interpreting the segments by evaluating the similarity of judgments between researchers using the Krippendorff alpha index, which was 0.92, pointing to high similarity in the evaluation. Disagreements were resolved by mutual agreement between the researchers [58]. Notably, the classification of excerpts occurred throughout the text of the interviews, not just in the answers that would refer to each of the categories.
Using the definitions in
Table 3
, each text segment was analyzed considering the analytical categories and their respective dimensions. With the help of a data spreadsheet, the segments were highlighted, organized into lines in the same column, and categorized into four variables that refer to the categories and dimensions of the study. Exemplifying excerpts were identified and extracted from the interviews to illustrate the authors' statements. When, for example, the interviewee says that "not all accreditation determinations were made", we categorize the excerpt as a customization to the accreditation process. In the case, for example, of physicians who resisted the implementation of accreditation protocols, this category of conflict in media becomes evident.
3.5. Analytical Strategy
Seeking greater study validity through triangulation between methods [59,60], we compared researchers' interpretations regarding each text segment with the interweaving of categories identified through multiple correspondence analysis (MCA). MCA consists of a formal method of analyzing the proximity and distance of analytical categories, considering how much they recur among themselves [61]. Its interpretation is facilitated because the method provides a graphical visualization of the relationships between nominal categories.
To this end, we generated multiple correspondence analysis in the SPSS statistical package, in which the visual representation was improved through the Power BI application to make the visualization more readable. In operational terms, we included all analytical categories as variables, whose category map was generated from the scores on a two-dimensional map (see Appendix: Analytical Category Scores). The MCA presented adequate adjustment, as dimension 1 had a Cronbach's alpha of 0.739 (Inertia of 0.560) and the second of 0.645 (Inertia of 0.484), in which all included categories presented significant discrimination (p < 0.05).
It should be emphasized that the choice of MCA as a formal method is due to the need to analyze the relationship between individuals and categories as if they were mutually constituted in fields of action [62] or institutional orders [25]. This suggests that the understanding of what organizational and professional agents do, understand, and justify in their context is expanded when we go beyond what they say, as what is also not said can help to reveal how the hospital accreditation process is organized.
Thus, we follow the example of Friedland et al. [25] in using MCA to find out how professional and market logics manifested themselves when conflicts in accreditation were in processes or goals, as well as how such aspects were related to adoption objectives and the response in terms of conformity or not. So, the greater the proximity between the dimensions of the analytical categories, the more significant the overlap between them. So, the greater the distance, the more these categories differ.
Finally, after interpreting the results, we seek greater transferability [63], as well as more significant potential for analytical generalization [64] through the statement of empirically verifiable propositions [65] to support new studies on hospital accreditation from the perspective of institutional logics.
4. Results
From the analysis of interviews with the 16 survey respondents, including managers and employees from 4 different hospitals, 187 segments of texts were identified that present the categories that make up this research, of which we highlight some excerpts.
4.1. Institutional Logics
When evaluating the institutional logic category, reports from employees and evaluators initially point to the bureaucratic nature of the accreditation process, that is, a standardization process following precise protocols.
"It is a methodology in which it evaluates healthcare institutions to determine whether they comply with the requirements of the chapters of the accreditation manual aimed at patient safety and improvement of the organization." (CBA Assessor)
"He has a spreadsheet that has to give the grades. But the spreadsheet is exactly the manual. So that's his instrument. The grade is zero, five or ten. So, there are things that they point out." (Hospital manager C)
Managers and employees were asked about the main obstacles to the accreditation process and actions or facts that delayed or interrupted the process. Of the 56 highlighted excerpts that explain the logic that most compete with the accreditation process, 91% are causes linked to professional logic, while only 9% are related to market logic. Generally, this competition causes resistance from physicians, nurses, and other employees, difficulties in integration between teams, etc.
The research indicates that the professional category within hospitals, especially the more technical part, nurses, and physicians, exerts considerable influence on organizational practices and actions. The managers also emphasized that all processes must be well negotiated with the medical and nursing staff. Otherwise, the accreditation process would not progress as the executive body desired.
"The biggest difficulty is the engagement of the medical staff. First place because they think it already has quality. It is challenging for the physician to recognize and assume it needs improvement. So, scientific evidence shows that physicians are the last to incorporate these procedures. Still, when he arrives, the entire institution has already moved towards this." (Hospital manager B)
"The biggest difficulty was aligning the activities I had to do with those of other professionals. Sometimes we depended on others to complete our part, and that got in the way a little." (Nurse 1 from hospital C)
It is also worth highlighting that, when referring to the professional ethics of people who deal directly with patients, the logic of health care, which underlies professional logic, also manifests itself in the discourse of managers. This demonstrates that professional logic is prominent in the accreditation process, even among managers.
"The most important person here is the patient. I work for the patient. Everything I do is for the patient. So we had to translate this not following the manual." (Hospital manager A)
The research also showed that conflicts related to market logic are more linked to financial investment, such as spending on renovations, structural adjustments, and hiring. Conflicts in board decisions for more significant investments were also reported as major obstacles to achieving accreditation.
"In 2001, there was an absurd administrative mess here. Several people were sent away [...] the process stalled for months." (Hospital manager C)
"[...] there was a period when they needed to make changes in my sector, and this required a lot of expense, which was not authorized immediately, and the process was stopped for a while until the hospital fulfilled the requirements [...]" (Nurse 2 at Hospital C)
4.2. Adoption Objectives
The narratives pointed to a search for efficiency by hospitals when deciding to adopt hospital accreditation. Of the 35 excerpts collected in the category, around 65% point only to efficiency as the main objective of adoption. In the words of respondents, especially managers, the efficiency pursued by hospitals is related to the search for quality patient care, increased safety, and improved organization management.
"The Organization sought to improve the performance of its professional processes and adopt a certification model recognized as efficient in its purpose of offering quality and safety in healthcare provision." (Hospital manager B)
However, it was possible to identify that the objective of adoption refers to a desire to legitimize oneself before the hospital audience. In particular, the research indicated that the legitimacy sought to be achieved is more associated with the search for acceptance in the hospital organizational field. In line with previous studies [18,32,41], the interviews showed that accredited hospitals are concerned about signaling the quality of their procedures, including for physicians and nurses, as they are a source of legitimization of hospital activity [66,67].
"The hospital where I work has always valued providing quality medical care that exceeds patients' expectations." (Hospital manager B)
"It is a voluntary evaluation method, where a health institution, for example, a hospital, agrees to submit its administrative processes and assistance to the standards of a manual if, once the required conformity is achieved, it is given a seal that determines it as having a quality and safety program for patients that positively differentiates it from its peers." (Hospital manager B)
Furthermore, the managers' narrative also highlighted the concern about obtaining hospital accreditation even when patients have difficulty judging its direct effect on quality [6]. According to managers, the vast majority of customers do not associate the quality of the hospital with whether it is accredited or not. Even so, managers defend the accreditation process.
"He [the patient] sees it but doesn't understand. So, I think the system lacks information [...] many find it strange to wear bracelets, and even complain. Still, they don't know that an accreditation protocol increases safety and quality of care." (Hospital manager A)
4.3. Strategic Responses
We also sought to analyze how hospitals responded to accreditation requirements, especially concerning the inclusion of new methodologies, practices, and work routines. Interview reports indicate that 75% of the segments primarily emphasized that accreditation underwent a customization process. In other words, hospitals did not strictly follow all the protocols required by the accreditor, something already pointed out in the literature [33], especially when there is a shortage of resources [4] and when the professional body does not renounce autonomy in carrying out procedures [10]. However, most of them were maintained, while others were readjusted.
"[...] in my routine, I had no difficulty in [making] many changes, especially because, when I was admitted, it was at the same time that accreditation was being implemented." (Physiotherapist at hospital B)
Customization points to more incredible difficulty, including revalidating hospital accreditation certification every three years. The following excerpts show how hospitals had trouble following all the regulations and that there is a certain relaxation over time, causing people to stop following the protocol customizing adoption.
"[…] there's no way you can make up everything. You have to have an organized process. Now... it's logical that, after the visits pass, you give it a little time, right? Well... you can't be with everyone all the time, so it's challenging to maintain it. People are confined and tend to form small relationships, so you always have to keep working." (Hospital manager A)
"Believing is very difficult. But it is ten times more difficult to sustain. We lose processes and recover them all the time. We have to be sensitive and aware of understanding when we lose the process. Losing, everyone loses, happens. You must see if you are missing a vital process impacting some outcome. It isn't easy to sustain. Conquering is difficult, but it is not the most difficult." (Hospital manager D).
In cases with some evidence of non-conformity, although rare (only three segments appeared), most referred much more to a postponement of accreditation activities than to refusing to adopt what the accreditor determined. In any case, the statements point out that there is a risk of non-conformity when there are financial interests.
"[...] there was a period when they needed to make changes in my sector, which required greater investment, which was not authorized immediately, and the process was stopped until the hospital fulfilled the requirements." (Nurse 1 of the hospital A)
4.4. Nature of Demands
There was mention in 8% of the text segments that highlight conflicts involving the purposes and goals of adoption, generally linked to the decision to continue or not with the accreditation process, as well as the conflict between hospital management and executives who would lead the accreditation goals.
"So, halfway through, the manager changed. Then until that [new] manager understood, bought into the process... there were several elections along the way... changing care leadership, changing nursing management... then there is a discontinuity, a break in the process..." Hospital manager C)
The narratives also pointed out that the managers' concern was primarily with aspects linked to meeting the demands of stakeholders, with the intention of not threatening the functioning of the hospital, especially when they involved government entities that had the power of influence, even if indirect.
"Then, shortly afterward, José Serra came to the Ministry of Health [who had guidance for certification by ONA], and they forced us to do ONA. They made a pact with the ONA. So, we were evaluated. The CBA itself did ONA. So, they made visits through ONA and were there. For several reasons, we think the CBA is much better than the ONA. Then, when the government changed, and it no longer needed to be ONA, we went back to JCI, and soon after, we scheduled the visit and ended up getting accreditation later through CBA." (Hospital manager C)
As a result, what was seen in all hospitals was a process of segmenting activities related to the adoption process [27], which was concerned with demands and goals, many of them involving issues linked to financial efficiency and operational, was not shared with the professional body. Thus, while it was up to professionals to carry out the middle activities, regardless of whether they agreed or not, managers compartmentalized their concerns only in terms of goals, both efficiency and legitimacy [17]. This is evident in the speech of a hospital manager when approached by the researcher with the pressure for accreditation.
"So, the ONA case was more external pressure? (Researcher 1) Yes. Because otherwise, we wouldn't have changed. So, in this item, change of direction, and so, there were days when there were 29 auditors, we were unable to work. So, it was a very troubled period." (Hospital manager D).
As expected [18,68], most segments that deal with demands during the accreditation program implementation process focused on means and procedures (92% of mentions). We can exemplify such difficulties encountered in the following report.
"The manual changed last year, and I think next year will be calmer. But like this: many of the things so-and-so stopped doing. With indicator and stopped doing it!? When you think you're almost there... you have to recover. So it's an ant and systematic work. It demands a certain organization [...]" (Hospital manager A)
Even though there are several challenges on the part of professional and management teams, the research shows that organizations tend not to give up on the accreditation process, even though it takes longer than expected.
"For example, I saw a hospital that had been ISO-certified for eight years. When they entered the accreditation process, they already had structured documentation. But it still took them almost three years to achieve accreditation. Because there is much more detail about patient care and not necessarily with documentation, I saw an institution that took nine years. But with great difficulty." (ONA Appraiser)
"The ones I worked with achieved [accreditation]. I started Three particular ones from the first day working; one took two and a half years; the other 3 and a half; and the other 3 years; and the three did it. I started the process with this audience and stayed there for seven years. But then I left, and it took them another two years or so, and then they managed to do it. But it is a public institution." (CBA Appraiser)
The reports also point to the centrality of medical professionals and nurses, who, despite being subordinate to managers and executives, do not readily acquiesce to the demands of the governing body to facilitate the accreditation process, nor do they renounce their professional identity.
"Over time, you will say that there was no resistance... of course, there was one here and there, but as it was the Management's will, and we said it was something important, people understood. So, decoding that this will bring improvement to the quality of patient care is important. So, of course, today, when we visit, there is no longer any stress... there was already stress. My God, how is this? This no longer exists because it is already part of everyday life." (Hospital manager A)
"Accreditation is sometimes seen as a bargain. If I believe, then I want it. You don't have to want anything! So when we decoded it for them, that what the person comes to see is what we have to do." (Hospital manager A)
In the words of one of the professionals (Physiotherapist from hospital B), there was even more excellent resistance from physicians: "The main difficulty encountered was the more active participation of physicians who were always very critical". This occurred specifically because accreditation leads to greater use of control and bureaucratization systems. This not only challenges the autonomy of the medical professional but also requires skills that they are often unaware of. As one of the physicians (hospital B) said: "It was mainly due to increasing bureaucracy [...] Bureaucracy increased the number of reports and other similar actions." Furthermore, there was a consensus that the biggest challenge of accreditation was working as a team, not the division of work itself, but more fluid and collaborative coordination, which converges with other studies [2,18].
4.5. The Convergence of Logics, Demands, Objectives and Responses
To point out the aspects related to the manifestations of logic and other analytical categories that go beyond the analysis of narratives, we present the multiple correspondence analysis (MCA) results in Figure 1. The most revealing thing is that the MCA corroborates the overlap between the categories in the interviewees' statements, highlighting what differentiates them. As seen in the bottom left corner of the figure, there is a more remarkable recurrence of non-conformity and demands focused on goals when market logic manifested itself as a relevant aspect of the actions.
In effect, all these dimensions move away from competing dimensions, demonstrating a certain antagonism with the others. So much so that the professional logic, while aligning itself with the demands related to the activities and, consequently, responds strategically by customizing the adoption processes, distances itself from the market logic and other related dimensions.
Finally, the MCA demonstrates that the objectives of adoption do not differ, which shows that, in hospital accreditation processes, there are no conflicts between the intention of seeking efficiency and legitimacy. It should also be noted that compliance with accreditation rules is well related to concerns about adoption objectives, not presenting a significant contradiction with the customization of such processes, as these are relatively close.
5. Discussion
The analysis of the narratives and the analysis of correspondence between categories allowed us to develop propositions that can guide future studies that aim for a possible validation of the results [65]. Such prepositions also point to gaps in knowledge about how market and professional logics manifest themselves in hospital accreditation processes.
Firstly, the results indicate that when professional logic is dominant in the accreditation process, hospitals can customize the actions required by the accrediting organization. As some challenge from professionals was already expected [23], the interviews illustrated that the prominence of professional logic leads to resistance from the clinical staff, a lack of leadership, and non-harmonization between teams. Consistent with the literature, customization occurred because there is a need for professionals to reinterpret how work is done [13], requiring hospitals to work with the medical staff and nurses so that they believe new practices are authentic in a way that validates their professional identity [16].
"We don't put a lot of bosses in these groups, sometimes we have to, because it's not happening, because the boss isn't doing things." (Hospital manager C)
"The mobility of professionals (made it difficult)... so, not necessarily physicians. There is always in the administration: "Ah, the physicians... [referring to the resistance of these professionals]" (Hospital manager D)
There are reports that the hospital has adopted the standards and protocols required by the accrediting organization. However, some of these practices are lost throughout the process and its reproduction. Both managers and evaluators interviewed reported that, as a way of seeking the institutionalization of practices included by hospital accreditation, constant monitoring by team leaders and support from management stand out. Still, research has found that full conformity is complex and takes time. Expressions such as "most", "almost always" and "practically" were used by interviewees to demonstrate that the adoption of accreditation did not achieve full conformity.
Another relevant factor in customizing the accreditation process based on professional logic is the segmentation between groups of professionals in hospital organizations [27]. The high technical level among professionals with different specialties results in small "fiefdoms" within the organization, making the interaction between teams more complex, which aligns with previous studies [23,30]. Without integration between professionals, monitoring actions and compliance with the practice required by the hospital accreditation program becomes more difficult. Given such relationships, we propose that:
Proposition 1a:In hospital accreditation processes, the more prominent the professional logic, the greater the chance of customizing practices.
Proposition 1b: In the presence of distinct professional logics, the greater the likelihood of
segmenting practices and processes.
Secondly, when hospitals dealt with market demands involving investment decisions and resource mobilization, there was a tendency to pause adapting practices to accreditation standards, leading the organization to not conform to the accreditation protocol during this period.
"We only stopped the process when we had to postpone scheduling the visit for evaluation, as in the last one, we had many adjustments pending that required a huge expense. This took a while to be approved and put into practice." (Hospital manager D)
"Belief is not cheap. It's not cheap because it involves royalties that have to be paid for the methodology. It involves paying international evaluators who earn, which comes with everything paid for. Well... when we have a problem with the budget, this interrupts the process." (Hospital manager C)
The reports led us to conclude that the likelihood of non-conformity is more significant when there are conflicts related to market logic. This is because the aspects related to this logic proved to be more complicated to overcome throughout the organization. After all, it always refers to a management position of placing financial issues at the top of the hierarchy, such as investments in works, structural readjustments, and costs, to the detriment of other aspects of accreditation [69]. Therefore, we propose that:
Proposition 2: In hospital accreditation processes, the more prominent the market logic, the greater
the chance of non-conformity of practices.
Thirdly, when evaluating the nature of the demands [23] in the hospital accreditation process, the research indicated that the vast majority originate from the media. The conflicting aspects between the accreditation process's needs and professionals' identity led hospitals to customize their certified practices, not fully adopting the protocols. However, they adopted enough to be approved, creating a hybrid type of organizational practice that mixes [27] and bricolages [70] professional aspects with those of certification. This leads us to propose that:
Proposition 3a: In hospital accreditation processes, when the focus of demands is on means, there is
a greater chance of customization.
In such cases, professional logic tends to prevail, as the main conflict factors are linked to the practice of technical activities and work routines [23,30]. Furthermore, the customization caused by the strong presence of professional logic in the process shows that the hospital, when faced with obstacles during the implementation of certification, remains on the path set in the initial objectives, even if this decision takes more or less time to achieve accreditation. Therefore, we propose that:
Proposition 3b: The greater the centrality of professional logic, the greater the likelihood of conflicts
occurring in the demands of environmental activities.
However, when conflicts focus on goals generally related to market logic [2], the organization tends not to conform to the process, usually pausing it or postponing adoption. Thus, when the conflict focuses on the goals and the purpose of adoption, the process tends to stall or be interrupted until the issue is resolved. So we propose that:
Proposition 4a: In hospital accreditation processes, when the focus of demands is on goals, there is
a greater chance of non-conformity.
Proposition 4b: The greater the centrality of market logic, the greater the likelihood that conflicts
will focus on goals.
Finally, the analyses showed that the hospital accreditation process, even because it is voluntary, did not lead to conflicts related to the pursuit of legitimacy to the detriment of efficiency, even though such disputes are recurrent [18,19,34]. It turns out that when there is no pressure for mandatory certifications, there is no excellent reason for organizations, including hospitals, to adopt practices such as certification. This is primarily because they are also pursuing improvements in efficiency and quality. Thus, the voluntary nature of hospital accreditations in Brazil does not cause contradictions between the objectives of adoption [71], leading us to propose that:
Proposition 5a: When hospital accreditation processes are voluntary, there is less likelihood of
conflicts between efficiency and legitimacy objectives.
Proposition 5b. The greater the imposition of hospital accreditation, the greater the likelihood that
adoption will be ceremonial and guided by legitimation interests.
5.1. Theoretical and Practical Implications
This study aimed to investigate how professional and market logics and the conflict between institutional demands affect compliance with hospital accreditation. To this end, we developed a qualitative multiple-case study in four Brazilian hospitals to understand this process's complexity. After data collection and analysis, it was possible to verify that institutional logics not only conditions the strategic responses of organizations in a significant way but also the type of strategic response adopted by the organization – conformity, non-conformity, or customization – will depend on what kind of logic is directly involved in the process.
The research also pointed out that despite the significant conflicts between institutional logics in the accreditation process, organizations tend to obtain effective rather than ceremonial results. At this point, it is possible to highlight a significant theoretical contribution of this work. Institutional logics and its variations must be considered when evaluating organizational strategic responses since it was found that when professional logic was prominent, the greater the chance of customization. When market logic prevailed, the organization tended not to conform to the practice of accreditation.
Several works have already had strategic responses as a study objective within the organizational field. Oliver [21] can be highlighted when evaluating institutional factors such as causes, constituents, control, context, and content; Pache and Santos [23] used variables such as internal representation and the nature of the demands. Although these, among other works, exist on strategic responses and institutional logics, the field of organizational studies still lacks research involving the direct correlation between these two categories of analysis. This work sought, in a way, to highlight that institutional logics and its variations significantly condition the strategic responses of organizations.
For the hospital field, the research contributed to a better understanding of the choice and practice of accreditation to achieve quality in Brazilian health organizations. Identifying concrete objectives linked to actions aimed at employees and patients was possible. Regarding the legitimacy of the program, although the client still knows little about hospital accreditation or other quality programs in the field, in addition to not being a mandatory process, it was possible to identify the normative nature of the practice, especially among hospital organizations. The search for efficiency was also a relevant factor evidenced in the research results, demonstrating that Hospital Accreditation goes beyond the ceremonial character, seeking to align the certification objectives with those of the hospital organization.
The propositions developed in this study provide a solid framework to guide future studies, allowing a deeper understanding of the complex interactions in hospital accreditation processes. As highlighted, the voluntary nature of hospital accreditations in Brazil does not seem to lead to significant conflicts between efficiency and legitimacy. This suggests that hospital organizations can pursue accreditation as an effective means of improving both efficiency and quality of services without substantial contradictions between these objectives.
From a practical point of view, the implications are equally relevant. Hospital managers can benefit from the propositions, understanding how market and professional logics affect the accreditation process. In line with studies such as Rey et al. [18] and Rossoni et al. [34], hospital accreditation often balances efficiency and legitimacy. Managers can use these propositions as guides for balancing these competing demands.
For example, when professional logic is prominent, managers may anticipate resistance from healthcare professionals and a lack of leadership. Resistance from professionals is a common challenge in hospital accreditation contexts, something already highlighted repeatedly in the literature [23]. To promote compliance, managers can adopt strategies that involve clinical staff in reviewing and adapting practices, emphasizing the importance of validating professional identity.
Likewise, when faced with demands related to market logic, managers may be aware of the tendency to pause the adaptation process due to financial challenges. Financial issues are often a significant obstacle in practice adoption processes, including hospital accreditation [19,69]. This can encourage the search for financing and investment strategies that allow the accreditation process to continue while balancing the organization's financial goals.
The practical implications also extend to understanding the nature of the demands of hospital accreditation. Managers can adopt more personalized approaches by recognizing that the nature of demands can affect the degree of customization and conflicts. Consistent with what is stated by Skelcher and Smith [27], multidisciplinary teams in hospitals often face integration challenges. When demands focus on means, teams can focus on adapting technical practices and work routines. On the other hand, when conflicts concentrate on goals, managers must resolve these issues before proceeding with the accreditation process, avoiding significant interruptions.
5.2. Limitations and Suggestions for Future Studies
Despite significant contributions to understanding the dynamics involved in organizational compliance and hospital accreditation, we recognize some limitations that must be considered when interpreting the results. First, our study focused on hospitals located in a specific context, which may limit the generalizability of findings to other regions or health systems with different characteristics [26]. It is recommended to conduct comparative studies in different contexts to evaluate the external validity of the propositions developed.
We also suggest exploring the influence of other key actors, such as patients and their families, on the dynamics of hospital accreditation [27]. Your perspectives and expectations can play a significant role in organizational compliance. Furthermore, additional investigations can focus on hospital managers' strategies to deal with the complex interactions between logics, demands, and objectives [26]. Understanding how managers can promote harmonization between different logics and minimize conflicts is crucial to improving the effectiveness of the hospital accreditation process. Finally, future studies can address the evolution of accreditation and compliance practices over time, considering how contextual factors and changes in legislation can affect the dynamics of hospital organizations [27]. This long-term perspective would provide a more comprehensive understanding of the complex relationships between logics, demands, and objectives in hospital accreditation.
6. Conclusion
The research reveals that identifying actors with specific logic influences the emphasis given to demands of a particular nature, corroborating previous findings [23]. Furthermore, given the multifaceted and sometimes incompatible context of various logics in hospital organizations, it is notable how these logics tend to segment to mitigate extensive conflicts [26,27]. When professional logic assumes prominence, conflicts arise in the media, resulting in customizing accreditation practices. In contrast, in scenarios dominated by market logic, conflicts focus on goals, leading to non-conformity. These findings contribute to a deeper understanding of how logic influences the attention given to specific demands and, more significantly, how they affect compliance with hospital accreditation standards, expanding the body of knowledge in the area.
Author Contributions
Conceptualization, TMRS and LR; methodology, TMRS and LR; validation, TMRS and LR; investigation, TMRS; formal analysis, TMRS and LR; writing—original draft preparation, TMRS and LR; writing—review and editing, LR; visualization, TMRS and LR; funding acquisition, LR. The authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by CNPq (Grant 313387/2021-4) and FAP-DF (Grant 00193-00001957/2023-11).
Institutional Review Board Statement
The requirement for ethical approval was waived by the Ethics Committee at the University of Gande Rio because of the retrospective nature of the study. All participants were informed verbally and in written form that their participation is voluntary and could be withdrawn at any time during the study without consequences. All participants gave their written and verbal informed consent to participate in this research, where parts of their interview transcripts are published in pseudonymised form. Data collection and analysis complies to the CNS/MS Resolution No. 466/2012. No files containing personal data were compiled within the remit of data protection laws. We confirm that all methods were carried out in accordance with relevant guidelines and regulations.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data used during this study are available from the corresponding author upon request by email.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Anthony DL, Appari A, Johnson ME. Institutionalizing HIPAA Compliance. J Health Soc Behav. 2014, 55, 108–124.
- Conceição A, Picoito C, Major M. Implementing an hospital accreditation programme in a context of NPM reforms: Pressures and conflicting logics. Public Money & Management. 2022, 1–8.
- Corrêa J, Turrioni J, Mello C, Santos A, da Silva C, de Almeida F. Development of a System Measurement Model of the Brazilian Hospital Accreditation System. Int J Environ Res Public Health. 2018, 15, 2520.
- Mansour W, Boyd A, Walshe K. The development of hospital accreditation in low- and middle-income countries: a literature review. Health Policy Plan. 2020, 35, 684–700.
- Mosadeghrad, AM. Hospital accreditation: The good, the bad, and the ugly. Int J Healthc Manag. 2021, 14, 1597–1601. [Google Scholar] [CrossRef]
- El-Jardali F, Jamal D, Dimassi H, Ammar W, Tchaghchaghian V. The impact of hospital accreditation on quality of care: perception of Lebanese nurses. International Journal for Quality in Health Care. 2007, 20, 363–371.
- de Oliveira JLC, Gabriel CS, Fertonani HP, Matsuda LM. Management changes resulting from hospital accreditation. Rev Lat Am Enfermagem. 2017, 25.
- Brubakk K, Vist GE, Bukholm G, Barach P, Tjomsland O. A systematic review of hospital accreditation: the challenges of measuring complex intervention effects. BMC Health Serv Res. 2015, 15, 280.
- Greenfield D, Braithwaite J. Health sector accreditation research: a systematic review. International Journal for Quality in Health Care. 2008, 20, 172–183.
- Cain, CL. Agency and Change in Healthcare Organizations: Workers’ Attempts to Navigate Multiple Logics in Hospice Care. J Health Soc Behav. 2019, 60, 3–17. [Google Scholar] [CrossRef]
- Friedland R, Alford R. Bringing society back in: Symbols, practices, and institutional contradictions. In: Powell WW, DiMaggio PJ, editors. The New Institutionalism in Organizational Analysis. Chicago: University of Chicago Press; 1991. p. 232–63.
- Thornton PH, Ocasio W, Lounsbury M. The Institutional Logics Perspective. Oxford University Press; 2012.
- Andersson T, Liff R. Co-optation as a response to competing institutional logics: Professionals and managers in healthcare. Journal of Professions and Organization. 2018, 5, 71–87.
- Cappellaro G, Tracey P, Greenwood R. From Logic Acceptance to Logic Rejection: The Process of Destabilization in Hybrid Organizations. Organization Science. 2020, 31, 415–438.
- Kodeih F, Greenwood R. Responding to Institutional Complexity: The Role of Identity. Organization Studies. 2014, 35, 7–39.
- Kyratsis Y, Atun R, Phillips N, Tracey P, George G. Health Systems in Transition: Professional Identity Work in the Context of Shifting Institutional Logics. Academy of Management Journal. 2017, 60, 610–641.
- Pouthier V, Steele CWJ, Ocasio W. From Agents to Principles: The Changing Relationship between Hospitalist Identity and Logics of Health care. p. 203–41.
- Reay T, Goodrick E, Casebeer A, Hinings CR (Bob). Legitimizing new practices in primary health care. Health Care Manage Rev. 2013, 38, 9–19.
- Yang C-W, Fang S-C, Huang W-M. Isomorphic pressures, institutional strategies, and knowledge creation in the health care sector. Health Care Manage Rev. 2007, 32, 263–270.
- Gray CS, Berta W, Deber R, Lum J. Organizational responses to accountability requirements. Health Care Manage Rev. 2017, 42, 65–75.
- Oliver, C. Strategic Responses to Institutional Processes. The Academy of Management Review. 1991;16:145.
- Silva BN Da, Abbas K, Crubellate JM. Lógicas Institucionais na Mensuração e Gestão de Custos em Hospitais Acreditados. Contabilidade Gestão e Governança. 2021, 24, 349–369.
- Pache A-C, Santos F. When Worlds Collide: The Internal Dynamics Of Organizational Responses To Conflicting Institutional Demands. Academy of Management Review. 2010, 35, 455–476.
- Riessman, CK. Strategic uses of narrative in the presentation of self and illness: A research note. Soc Sci Med. 1990, 30, 1195–1200. [Google Scholar] [CrossRef]
- Friedland R, Mohr JW, Roose H, Gardinali P. The institutional logics of love: measuring intimate life. Theory Soc. 2014, 43, 333–370.
- Besharov ML, Smith WK. Multiple Institutional Logics in Organizations: Explaining Their Varied Nature and Implications. Academy of Management Review. 2014, 39, 364–381.
- SKELCHER C, SMITH SR. Theorizing hybridity: institutional logics, complex organizations, and actor identities: the case of nonprofits. Public Adm. 2015, 93, 433–448.
- Alford R, Friedland R. Powers of theory: Capitalism, the State, and democracy. Cambridge University Press; 1985.
- Thornton PH, Ocasio W. Institutional Logics. In: The SAGE Handbook of Organizational Institutionalism. SAGE Publications Ltd; 2008. p. 99–128.
- Pache A-C, Santos F. Inside the Hybrid Organization: Selective Coupling as a Response to Competing Institutional Logics. Academy of Management Journal. 2013, 56, 972–1001.
- Shea CM, Turner K, Albritton J, Reiter KL. Contextual factors that influence quality improvement implementation in primary care: The role of organizations, teams, and individuals. Health Care Manage Rev. 2018, 43, 261–269.
- Ruef M, Scott WR. A Multidimensional Model of Organizational Legitimacy: Hospital Survival in Changing Institutional Environments. Adm Sci Q. 1998, 43, 877.
- Westphal JD, Gulati R, Shortell SM. Customization or Conformity? An Institutional and Network Perspective on the Content and Consequences of TQM Adoption. Adm Sci Q. 1997, 42, 366.
- Rossoni L, Poli IT, Fogliatti de Sinay MC, Aguiar de Araújo G. Materiality of sustainable practices and the institutional logics of adoption: A comparative study of chemical road transportation companies. J Clean Prod. 2020, 246.
- Scott, WR. Institutions and organizations: Ideas and interests. SAGE; 2008.
- Borowska M, Religioni U, Augustynowicz A. Patients’ Opinions on the Quality of Services in Hospital Wards in Poland. Int J Environ Res Public Health. 2022, 20, 412.
- Quartz-Topp J, Sanne JM, Pöstges H. Hybrid practices as a means to implement quality improvement: A comparative qualitative study in a Dutch and Swedish hospital. Health Care Manage Rev. 2018, 43, 148–156.
- Feldman LB, Gatto MAF, Cunha ICKO. História da evolução da qualidade hospitalar: dos padrões a acreditação. Acta Paulista de Enfermagem. 2005, 18, 213–219.
- Alonso LBN, Droval C, Ferneda E, Emidio L. Acreditação hospitalar e a gestão da qualidade dos processos assistenciais. Perspectivas em Gestão & Conhecimento. 2014, 34–49.
- Rossoni L, Teixeira RM. A interação dos relacionamentos com os recursos e a legitimidade no processo de criação de uma organização social. Cadernos EBAPEBR. 2008, 6, 1–19.
- Scott, WR. Health care organizations in the 1980s: The convergence of public and professional control systems. Organizational environments: Ritual and rationality. 1983.
- Scott, WR. Institutional change and healthcare organizations: From professional dominance to managed care. University of Chicago press; 2000.
- Mintzberg, H. Understanding Organizations... Finally!: Structuring in Sevens. Berrett-Koehler Publishers; 2023.
- Scott, WR. Lords of the Dance: Professionals as Institutional Agents. Organization Studies. 2008, 29, 219–238. [Google Scholar] [CrossRef]
- Suchman, MC. Managing Legitimacy: Strategic and Institutional Approaches. The Academy of Management Review. 1995, 20, 571. [Google Scholar] [CrossRef]
- Meyer JW, Rowan B. Institutionalized Organizations: Formal Structure as Myth and Ceremony. American Journal of Sociology. 1977, 83, 340.
- ONA. Manual brasileiro de acreditação hospitalar. ONA; 2014.
- Mohr JW, White HC. How to model an institution. Theory Soc. 2008, 37, 485–512.
- Breiger RL, Mohr JW. Institutional Logics from the Aggregation of Organizational Networks: Operational Procedures for the Analysis of Counted Data. Comput Math Organ Theory. 2004, 10, 17–43.
- Flick, U. An introduction to qualitative research. 2022.
- Yin, R. Case study research: Design and methods. Sage; 2013.
- Eisenhardt KM, Graebner ME. Theory Building From Cases: Opportunities And Challenges. Academy of Management Journal. 2007, 50, 25–32.
- Reay T, Jones C. Qualitatively capturing institutional logics. Strateg Organ. 2016, 14, 441–454.
- Eisenhardt KM, Graebner ME, Sonenshein S. Grand Challenges and Inductive Methods: Rigor without Rigor Mortis. Academy of Management Journal. 2016, 59, 1113–1123.
- Cunliffe AL, Alcadipani R. The Politics of Access in Fieldwork. Organ Res Methods. 2016, 19, 535–561.
- Krippendorff, K. Content Analysis: An Introduction to Its Methodology. SAGE Publications, Inc.; 2019.
- Weber K, Patel H, Heinze KL. From Cultural Repertoires to Institutional Logics: A Content-Analytic Method. 2013. p. 351–82.
- Krippendorff, K. The Reliability of Generating Data. Chapman and Hall/CRC; 2022.
- Oleinik, A. Mixing quantitative and qualitative content analysis: triangulation at work. Qual Quant. 2011, 45, 859–873. [Google Scholar] [CrossRef]
- Stamenkov, G. Recommendations for improving research quality: relationships among constructs, verbs in hypotheses, theoretical perspectives, and triangulation. Qual Quant. 2023, 57, 2923–2946. [Google Scholar] [CrossRef]
- Franco G, Di. Multiple correspondence analysis: one only or several techniques? Qual Quant. 2016, 50, 1299–1315. [Google Scholar] [CrossRef]
- Bourdieu, P. Distinction: A social critique of the judgment of taste. Cambridge: Harvard University Press; 2002.
- Weise A, Büchter RB, Pieper D, Mathes T. Assessing transferability in systematic reviews of health economic evaluations – a review of methodological guidance. BMC Med Res Methodol. 2022, 22, 52.
- Hays DG, McKibben WB. Promoting Rigorous Research: Generalizability and Qualitative Research. Journal of Counseling & Development. 2021, 99, 178–188.
- Tsang EWK. Generalizing from Research Findings: The Merits of Case Studies. International Journal of Management Reviews. 2014, 16, 369–383.
- de Oliveira JLC, Matsuda LM. Disqualification Of Certification By Hospital Accreditation: Perceptions Of Professional Staff. Texto & Contexto - Enfermagem. 2016, 25.
- de Sousa Vilela G, Ferraz CMLC, de Araújo Moreira D, Brito MJM. Expressões da ética e do di stresse moral na prática do enfermeiro intensivista. Acta Paulista de Enfermagem. 2021, 34.
- Lewis K, Hinchcliff R. Hospital accreditation: an umbrella review. International Journal for Quality in Health Care. 2023, 35.
- Arman R, Liff R, Wikström E. The hierarchization of competing logics in psychiatric care in Sweden. Scandinavian Journal of Management. 2014, 30, 282–291.
- Xing Y, Liu Y, Lattemann C. Institutional logics and social enterprises: Entry mode choices of foreign hospitals in China. Journal of World Business. 2020, 55, 100974.
- Tolbert PS, Zucker LG. Institutional Sources of Change in the Formal Structure of Organizations: The Diffusion of Civil Service Reform, 1880-1935. Adm Sci Q. 1983, 28, 22.
Figure 1.
Multiple Correspondence Analysis of the researched categories. Note: Each geometric shape refers to an analytical category, which is also in different colors. The dimensions of the categories are represented by other figures in the two-dimensional graph, whose size indicates the frequency of mentions. Dimension 1 is more strongly affected by adoption objectives, while dimension 2 is more strongly affected by strategic responses. The institutional logic and the nature of the demands are intensely manifested in both dimensions.
Figure 1.
Multiple Correspondence Analysis of the researched categories. Note: Each geometric shape refers to an analytical category, which is also in different colors. The dimensions of the categories are represented by other figures in the two-dimensional graph, whose size indicates the frequency of mentions. Dimension 1 is more strongly affected by adoption objectives, while dimension 2 is more strongly affected by strategic responses. The institutional logic and the nature of the demands are intensely manifested in both dimensions.
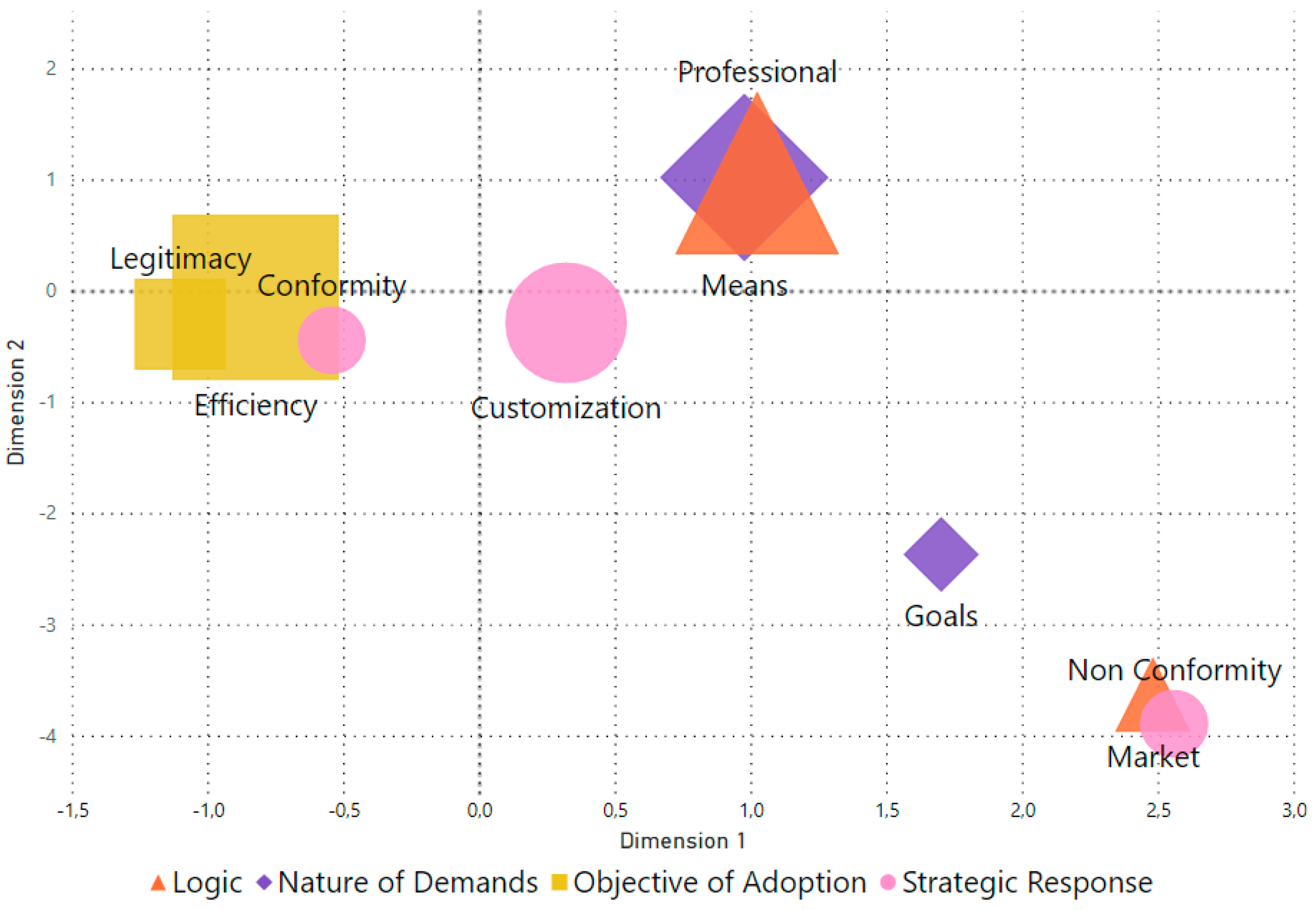
Table 1.
Ideal types of institutional logics relevant to the hospital accreditation process.
| Logic | Market | Professional |
|---|---|---|
| Guidance | Focuses on business strategies, market competition, and return on investment. | Based on norms and standards established by professional health associations and bodies. |
| Main Emphasis | Maximizing operational efficiency and financial profitability. | Providing high-quality healthcare based on best practices and professional standards. |
| Motivation | Obtaining profit, optimizing resources, and growing the market. | Commitment to professional ethics, continuous improvement in the quality of care, and patient well-being. |
| Threats | Increased costs and loss of customers. | Reduction in the quality of services and professional malpractice. |
| Basis of authority | Owners, investors and managers. | Professionals with the most outstanding technical and scientific reputations, especially physicians and nurses. |
| Source of Legitimacy | Position of the hospital in the market compared to other competitors. | Status of the hospital in the professional community, available resources, and structure quality. |
| Performance Measurement | Based on financial indicators such as profit margins, revenue, and market share. | Based on quality indicators, patient satisfaction, and adherence to professional standards. |
| Decision Making | Considerations of efficiency, competition and financial return often guide strategic decisions. | Physicians and healthcare professionals frequently make clinical and operational decisions to meet patient needs best. |
| Organizational structure | Organizational structure is often oriented toward management, finance, and operations functions. | Organizations are often structured around medical specialties and multidisciplinary teams. |
| Relationship with Patients | Attention to customer satisfaction, attracting and retaining patients, and maximizing the customer life cycle. | Focus on providing high-quality care and building trusting relationships with patients. |
| Regulation | Subject to government regulations, including compliance with health laws and healthcare regulations. | Subject to professional regulations, standards of practice, and healthcare licensing bodies. |
| Underlying Logic | Managerial | Healthcare |
Table 2.
Research participants.
| Hospital, Nature, Time of Foundation and Accreditor | Interviewed | Number of Interviews | Total Recording Time |
|---|---|---|---|
| A (Private), 18 years old, ONA | Manager | 4 | 236 minutes |
| Physician | 2 | 54 minutes | |
| Nurse | 2 | 55 minutes | |
| Nurse | 3 | 41 minutes | |
| B (Private), 86 years old, CBA | Manager | 4 | 190 minutes |
| Physician | 1 | 25 minutes | |
| Physiotherapist | 2 | 74 minutes | |
| Nurse | 1 | 22 minutes | |
| C (Public), 43 years old, ONA | Manager | 5 | 274 minutes |
| Physician | 2 | 49 minutes | |
| Nurse | 1 | 81 minutes | |
| Nurse | 3 | 171 minutes | |
| D (Public), 116 years old, CBA | Manager | 4 | 212 minutes |
| Physician | 1 | 12 minutes | |
| Physician | 2 | 44 minutes | |
| Nurse | 2 | 87 minutes |
Note: All interviews were recorded and transcribed, maintaining the anonymity of the respondents.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



