Submitted:
30 October 2023
Posted:
31 October 2023
You are already at the latest version
Abstract
Background. ADHD is a neurodevelopmental disorder that is accompanied by executive deficits. Objectives. To obtain evidence of the usefulness of the BRIEF-P and to analyse the possible ceiling and floor effect of its scores in the assessment of executive function in preschoolers with signs compatible with a possible diagnosis of ADHD. Methods. Seven articles were selected from 2538 potentially eligible articles from different databases. We included studies assessing samples of individuals with symptoms compatible with ADHD, with age range 2-6 years, published in English or Spanish, during the period 2012-2022. References published in: Science Direct, NCBI (PubMed), ProQuest Education Journals in the last decade. Risk of bias was assessed using the QUADAS-2 questionnaire. The main variables were: age and executive functioning. Conclusions. Executive deficits in early-life individuals with ADHD-compatible symptoms are more extensive than deficits in working memory. BRIEF-P is an instrument that facilitates obtaining a sensitive and discriminative executive profile. It should be used in combination with other neuropsychological performance tests, finding a floor effect in tests associated with warm executive functions and a ceiling effect in cold executive functions. This requires using a variety of tests to assess executive performance in preschoolers with symptoms compatible with ADHD and designing intervention proposals in line with them...
Keywords:
BRIEF-P
; floor effect
; ceiling effect
; executive functions
; Attention-Deficit and Hyperactivity Disorders
; ADHD
; test
; diagnostic validation
1. Introduction
Attention Deficit Hyperactivity Disorder (ADHD) is one of the most common neurodevelopmental disorders, its prevalence in children is estimated at 2-7% [1]. Although there are very old precedents for its description in the literature {see [2]], its current concept dates back to the publication of the DSM-IV-TR [3] The most characteristic symptoms are inattention (daydreaming), forgetting or losing things, motor restlessness, excessive talking (without control or respecting the turn of the conversation), making careless mistakes or committing recklessness, problems in relationships with others, etc. The DSM 5 [4] establishes as a criterion the presence of a persistent behavioral pattern of inattention and/or hyperactivity-impulsivity that interferes with functioning or development. In DSM 5 TR [5]establishes up to five diagnostic subcategories depending on the combined presence of inattention and hyperactivity. As it is a disorder with a multifactorial etiology and heterogeneous symptoms [6, 7] there is no specific diagnostic test for its detection and diagnosis, usually acting by steps, eliminating possible alternatives and by behavioral observation.
Many of the symptoms of ADHD are linked to different impairments of executive functions (EFs): inhibition, self-regulation, working memory, flexibility, among others [8, 9, 10]. However, given the symptomatologic heterogeneity of ADHD, its high co-morbidity with other disorders and difficulties [11, 12, 13] and the different conceptions of the FE there is no consensus on the existence of a characteristic profile [14, 15, 16]. Thus, the assessment of EFs is taken as complementary information aimed both at excluding another disorder and at planning intervention.
Most studies on EFs consider the Miyake et al. [17] model as a reference, emphasizing cold EFs: inhibitory control [18], cognitive flexibility (or set shifting) [19] and working memory [20], among others. There is also a more or less general consensus that the development of EFs starts during the first years of life and accelerates with schooling [21, 22]. Evidence suggests that it is during the school period (6 to 12) that the development of hot and cold EFs is most evident [23]. Some studies reveal the possibility of slower development of warm EFs compared to cold EFs [24, 25]. Rastikerdar et al. [26] compare the development of cold and warm executive functions in people with and without ADHD, pointing out differences in their development throughout the life cycle. Thus, cold EFs reach adult levels by the age of twelve, while warm EFs progress more slowly at school age and improve throughout adolescence. Shakehnia et al [27], after controlling for age, parental education and number of children, report significant differences between group means (hyperactivity disorder versus ADHD) in EF assessed with BRIEF (Behavior Rating Inventory of Executive Function): warm (Behavioral Regulation Index), cold executive function (Metacognitive Index), total executive function and other subscales. These researchers consider that warm executive functions and cold executive functions are related and interact, but that in people with ADHD, they are dissociated. Several studies have found a delay in the development of EF in people with ADHD [28, 29]. This delay is not homogeneous or equal in all dimensions. Delays have been found in: (i) inhibitory control [28] working memory (Yáñez-Téllez, y otros, 2012); (iii) cognitive flexibility [30]; (iv) delayed gratification and risky decision-making [31]. In conclusion [32], people who develop ADHD present a wide range of cognitive deficits, but they are only manifested in some EFs [fundamentally cold, see model by Zelazo & Carlson [33]].
In general terms, it is accepted that the main impairment in people who develop ADHD is a deficit in inhibitory control (cold executive function) [34, 28, 35, 36, 37]. To such an extent that Barkley [38] proposes the self-regulation model, understanding that the basic problem of people with ADHD is a deficit in behavioral inhibition which, in turn, has repercussions on other parallel processes of executive function: non-verbal working memory, verbal working memory, planning and reconstruction, self-regulation of emotions, motivation and arousal. Barkley's model has been studied and compared with others that also consider the deficit in self-regulation as the core deficit of ADHD [39], however, the variability of symptoms poses unsolvable problems for a single or predominant factor model of EFs. Evidence suggests that working memory deficits are also present in people who develop ADHD [40, 41, 23, 42, 43]. In the same way that impaired cognitive flexibility (cold executive function) is critical in ADHD. Lack of adaptive capacity (cognitive flexibility), which allows individuals to adapt their cognitive processing strategies to cope with unforeseen conditions [44], its deficit correlates with mental health problems [45]. From a more organismic point of view, the results of studies based on brain imaging using functional magnetic resonance imaging (fMRI) show that the anterior cingulate, as well as the superior and inferior frontal gyri, which are involved in cognitive flexibility, are less active in people with ADHD [46].
Although the scientific literature shows a high level of interest in EF, its assessment remains complex and there is no consensus on the type of measure to use. The complexity of measuring EF lies in the different conceptual models [47] and in the need to perform a task where EF performance is evidenced. Some of the measures used, such as the Stroop Test, the Tower of Hanoi or the Wisconsin Card Sorting Test, have low ecological validity and are not representative of the individual's functioning in real-life contexts [48, 49, 50, 51, 52, 53, 54]. Based on these measures and sometimes benefiting from technological resources, digitised test batteries such as CANTAB [Cambridge Neuropsychological Test Automated Battery, [55]] have been developed. The NIH EXAMINER [Executive Abilities: Measures and Instruments for Neurobehavioral Evaluation and Research [56]]; The CAS [Cognitive Assessment System [57] and CAS2 [58]]; The D-KEFS [Delis - Kaplan Executive Function System [59]]; The CEFI [Comprehensive Executive Function Inventory [60], are examples of complex EF assessment systems.
An alternative are questionnaires based on rating scales such as the BRIEF [Behavior Rating Inventory of Executive Function; [61]]. The BRIEF is undoubtedly one of the most widely used in ADHD diagnosis and intervention. It is a family of questionnaires that attempt to capture the behavioural manifestations of executive dysfunction across the lifespan (2 to 90 years). The original BRIEF [61] has a range of application from age 5 to 18 years, with separate forms for parents and teachers. There are self-report versions for adolescents (11-18 years) [BRIEF-SR [62]] and for adults (BRIEF-A [63]) from 18 to 90 years with separate self-report or third-person forms.
As mentioned above, ADHD presents the first symptoms at early ages and the need for valid and reliable tools at early stages in order to plan early intervention [64], so it is worth highlighting the preschool version of the BRIEF [BRIEF-P [65]], applicable from 2 to 5 years of age.
Although there is evidence on the psychometric goodness of the BRIEF [66] and in particular of the BRIEF-P [67], at the clinical level the differentiation between typically developing children and ADHD is made dependent on the combination of the cut-off points of the test [68]. The aim of this paper is to determine, through an analysis of the scientific literature, the floor and ceiling scores of the EF components measured by the BRIEF-P.
2. Materials and Methods
The research question was formulated following PICOS (Population, Intervention, Comparison, Outcome, Study Design) in an attempt to delve into the floor effect and ceiling effect of the BRIEF-P as an instrument to be considered in the early identification of symptoms compatible with ADHD:
Regarding the floor effect (minimum score), are there statistically significant differences in the executive profile of preschool children with ADHD versus typically developing children?
In terms of the ceiling effect (maximum score), are there significant differences in the executive profile of preschool children with ADHD versus typically developing children?
This systematic search and meta-analysis was registered in the Prospero platform under the registration number CRD42023465855. Articles in Spanish and English published in the databases Science Direct, NCBI (PubMed), ProQuest Education Journals were reviewed. The articles had to be between 2013 and 2023. In the databases, the search was restricted to "all article" and "journal article", in psychology, health and education journals. The keywords used were: Attention Deficit Hyperactivity Disorder or ADHD or ADHD; Behavior Rating Instrument of Executive Function - School or BRIEF-P.
2.1. Search strategy
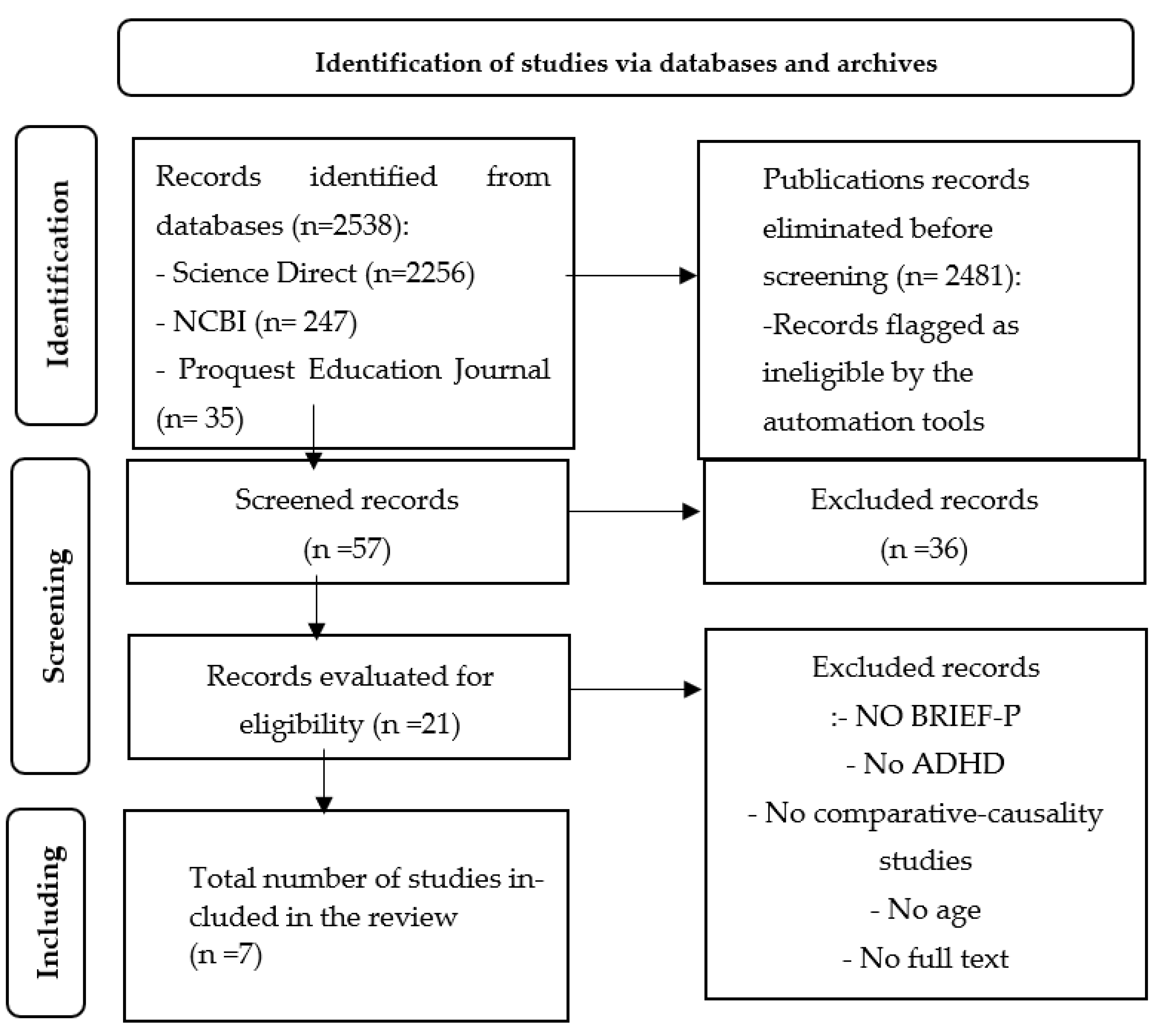
In order for studies to be included in the review, they had to meet the inclusion-exclusion criteria set out in table 1. The methodological structure of the search and screening methods followed the guidelines of the PRISMA guide [Preferred Reporting Items for Systematic Reviews and Meta-Analyses, [69]]. After analysing the 2538 papers, those that met the inclusion-exclusion criteria were selected; only 7 papers were selected. The resulting flow can be visualised in figure 1.

Table 1.
Inclusion-exclusion criteria.
| Inclusion criteria | Exclusion criteria |
|---|---|
| (a) Participants: persons with symptoms compatible with ADHD obtained from the application of standardized tests | (a) Participants: not diagnosed with ADHD |
| (b) Cognitive age that allows the application of BRIEF-P | (b) Cognitive age: does not allow application of BRIEF-P |
| (c) Cognitive competence: obtained through the application of standardized tests | (c) Cognitive competence: not available |
| (d) Executive dimensions: single construct or basic dimensions (flexibility, inhibition and working memory). | |
| (e) Assessment instruments: standardized for assessing executive functions: hetero- and/or self-report | (d) Assessment instruments: non-standardized |
| (f) Type of studies: empirical | (e) Type of studies: case study and review |
| (g) type of design: non-experimental, comparative-causal (group with ADHD-compatible symptoms versus group with typical development) | (f) type of design: non-comparative-causal |
| (h) Language: English and Spanish | (g) Language: other |
| (i) Other characteristics: full text | (h) Other characteristics: abstract, full text not available |
Figure 1.
PRISMA flow diagram (based on the work of [69]).
3. Results
Table 2 (see suplementary materials) summarizes the characteristics of the seven studies included in the review with participants under 6 years of age with ADHD-compatible symptoms compared to typically developing participants, with executive functioning being assessed using BRIEF-P and with data on mean scores obtained by both the ADHD group versus the typically developing control group.
3.1. Risk of bias
Using QUADAS-2 [QUality Assessment of Diagnostic Accuracy Studies [72]; available at https://www.bristol.ac.uk/population-health-sciences/projects/quadas/quadas-2/], this instrument assesses the methodological quality and risk of bias of primary studies included in a systematic review of diagnostic tests [73]. The questionnaire is organised into four domains: (i) patient selection; (ii) test under evaluation; (iii) baseline test; and (iv) patient flow and time between tests.
3.2. Floor effect and ceiling effect
A comparison was made between the group with symptoms compatible with ADHD and the typically developing group, considering the lower and upper scores to find out the floor effect and the ceiling effect. Effect size estimates were calculated, taking Cohen's d, the random effects model, as the effect size measure.
The results are presented in a forest plot or effects graph, in which the results obtained in each study, as well as the overall effect and its 95% confidence interval, are presented in vertical order according to a certain criterion (the study number). The studies with lower precision are those that have greater visual impact (longer horizontal lines due to the greater confidence interval), the mean value of each study is usually represented by a symbol (square or diamond) whose area is proportional to the weight with which the study intervenes in the overall calculation (inversely proportional to the variance), highlighting the most precise studies.
3.2.1. Floor effect
The studies with the lowest mean score obtained after application of the BRIEF-P were selected. As a clinical instrument, higher scores indicate greater executive dysfunction.
The 10th percentile was chosen, placing the mean score between the following values: ADHD group [15-26] and typically developing group [13-20]. Five studies obtained mean scores on the Flexibility clinical scale and on the Emotional Control index. The studies included in the meta-analysis are presented in Table 4 with the mean score: ADHD-compatible symptoms group [14.26] and the mean score of the typically developing group [12.32]. Significant differences were observed between the ADHD group and the typically developing control group [d=.615; Z=4.335; p=<.001; 95% CI .337- .893] (Table 5).
The studies included in the meta-analysis are represented in a forest plot (Figure 4). The study with the highest impact is study 4 [71] and the study with the lowest impact is study 2 [70].
3.2.2. Ceiling effect
The studies with the lowest scores were selected. Thus, studies with scores above the 90th percentile were selected, placing the mean score between the following values: ADHD group [100-108] and typically developing group [54-84]. Four studies obtained mean scores on the Flexibility clinical scale and on the Emotional Control index. The studies included in the meta-analysis are presented in Table 4 with the mean score of the ADHD group [103.84] and the score of the typically developing group [67.89].
| Study | Author | BRIEF_P | ADH | Typical Development | |||||
| N | M | STD | N | M | STD | ||||
| 7 | Çak et al. (2017). | Emergent Metacognition (Working Memory + Planning/Organization) | 21 | 100.46 | 11.61 | 52 | 54.09 | 9.54 | |
| 7 | Çak et al. (2017). | Global Executive Functioning | 21 | 103.05 | 10.07 | 52 | 54.39 | 10.79 | |
| 3 | Zhang, et al. (2018). | Global Executive Functioning | 163 | 104.59 | 16.26 | 63 | 79.54 | 12.75 | |
| 2 | Ezpeleta, L., & Granero, R. (2015) | Global Executive Functioning | 23 | 107.27 | 21.81 | 538 | 83.54 | 19.19 | |
| N: Sample size; M: Mean; STD: Standard Desviation; | |||||||||
Significant differences were observed between the group with symptoms compatible with ADHD and the typically developing control group [d=2.962; Z=3.249; p=<.001; C.I.95% 1.175- 4.749] (Table 6).
| Effect size | Standard error | Z | Sig. (bilateral) | Confidence interval 95% | Prediction interval 95%a | ||||
| Lower | Upper | Lower | Upper | ||||||
| Global | 2.962 | .9117 | 3.249 | .001 | 1.175 | 4.749 | -5.679 | 11.603 | |
| a. Based on t-distribution. | |||||||||
The study with the highest impact is study 3 [18] and the study with the lowest impact is study 7 [64]. The studies included in the meta-analysis are represented in a forest plot (Figure 5).
4. Discussion and Conclusions
The executive deficits presented by individuals in the early stages of the life cycle with symptoms compatible with ADHD are broader than deficits in working memory. There is a need for comprehensive assessment protocols for all dimensions that make up EF in line with the model of Miyake et al. [17] and adapted for children by Wiebe et al. [74] and the model developed by Zelazo and Carlson [33]. The results of the assessment will be the key to developing a personalised intervention [75]. With this review we aimed to obtain evidence of the usefulness of the BRIEF-P by analysing its floor and ceiling effects in the assessment of executive function in preschoolers with signs compatible with a possible diagnosis of ADHD.
The floor effect was associated with the Flexibility clinical scale and the Emotional Control index, both warm executive functions according to the model proposed by Zelazo & Carlson [33]. The study with the highest impact was the study by Skogan et al. [71] and the one with the lowest impact was the study by Ezpeleta & Granero [70]. Like other researchers [76], it is suggested that emotional dysregulation contributes to ADHD symptomatology and is prevalent in ADHD across the lifespan.
The ceiling effect was associated with two of the BRIEF-P indices: Global Executive Functioning and the Emergent Metacognition index, configured by the clinical scales: Working Memory and Planning/Organisation. These indices are associated with the cold dimensions of executive functioning proposed in the model of [33]. The study with the highest impact is the study by Zhang et al. [18] and the one with the lowest impact is the study by Çak et al. [64]. Preschoolers with early symptoms consistent with ADHD presented significant difficulties in BRIEF-P. These results are in line with previous studies in which the core domains of EF (response inhibition, working memory and flexibility) were closely associated with ADHD symptoms.
These results provide us with information on the executive dimensions to be strengthened in preschoolers with early symptoms compatible with ADHD and the tests to be included to complement the information obtained after the application of BRIEF-P. This review supports the clinical utility of the BRIEF-P as a measure of EF in preschoolers with ADHD-compatible symptoms in combination with performance-based neuropsychological tests, integrating two models: (i) the three domains proposed by Miyake et al [17] and (ii) the warm versus cold executive functions model developed by Zelazo and Carlson [33].
Studies suggest that children with ADHD exhibit statistically significant and large working memory deficits relative to their typically developing peers, however, executive deficits, which are broader, affecting several executive dimensions, including, for example, emotional dysregulation, need to be further explored. This requires a comprehensive assessment and subsequent intervention accordingly.
The results obtained point to the need to work on cold executive functions in preschoolers with symptoms compatible with ADHD. This includes: working memory, attentional control, problem solving, cognitive flexibility, phonological fluency, semantic fluency, error detection and inhibition of automatic responses [77].
The review has some limitations as it is based on studies with small sample sizes. The average age of the participants (before ADHD diagnosis) precludes considering the influence of factors related to developmental stage and maturity in the study of people with ADHD.
The study of EF in preschoolers involves greater difficulties. The structure of EF in preschoolers requires further study. Some studies suggest a single general factor of executive functioning, with these functions being more differentiated with age, and others propose two (inhibition, working memory), three (inhibitory self-control, flexibility, emergent metacognition) or four (hyperactive behaviours, attention problems, disinhibition behaviours, emotional regulation behaviours).
Subtypes of ADHD also need to be considered in future studies. Follow-up with children assessed for the first time at preschool age, in additional diagnostic groups and in larger samples, together with multiple performance-based EF tests, would be necessary. For future studies we plan to analyse the concordance between standardised and performance measures in the identification of executive difficulties in preschoolers with early symptoms compatible with ADHD.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table 2: Characteristics of the studies included in the review.
Author Contributions
Conceptualization, X.X. and Y.Y.; methodology, X.X.; software, X.X.; validation, EBH, AEY and FAM; formal analysis, EBH; investigation, EBH; resources, EBH.; data curation, EBH.; writing—original draft preparation, EBH.; writing—review and editing, AEY and FAM.; supervision, FAM. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sayal, K., Prasad, V., Daley, D., Ford, T., & Coghill, D., "ADHD in children and young people: prevalence, care pathways, and service provision," The Lancet Psychiatry, 2018, Volume 5(2), pp. 175-186. [CrossRef]
- Lange, K., Reichl, S., Lange, K., Tucha, L., & Tucha, O., "The history of attention deficit hyperactivity disorder," ASHD Attention Deficit and Hyperactivity Disorders, 2010, Volume 2, pp. 241-255. [CrossRef]
- [3] American Psychiatric Association (APA), Diagnóstic and Statistical Manual of Mental Disorders.Text Revision (DSM-IV-TR), Washington: American Psychiatric Association, 2000.
- American Psychiatric Association (APA), Diagnostic and Statistical Manual of Mental Disorders 5th ed., Arlington: American Psychiatric Publishing, 2013.
- American Psychiatric Association (APA), Diagnóstic and Statistical Manual of Mental Disorders. 5th T R Edition, Arlington: American Psychiatric Association, 2022.
- Faraone, S., Perlis, R. H., Doyle, A. E., Smoller, J. W., Goralnick, J., Holmgren, M. A., & Sklar, P., "Molecular Genetics of Attention-Deficit/Hyperactivity Disorder," Biological Psychiatry, 2005, Volume 57(11), pp. 1313-1323. [CrossRef]
- Millichap, J., "Etiologic Classification of Attention-Deficit/Hyperactivity Disorder," Pediatrics, 2008, Volume 121(2), pp. e358-e365. [CrossRef]
- Antshel, K., Hier, B. O., & Barkley, R., "Executive Functioning Theory and ADHD," in Handbook of Executive Funtioning, New York, Springer, 2014, pp. 107-120. [CrossRef]
- Barkley, R. A., Attention-deficit hyperactivity disorder: A handbook for diagnosis and treatment, The Guilford Press, 2006.
- Doyle, A. E., "Executive functions in attention-deficit/hyperactivity disorde," Journal od Clinical Psychiatry, 2006, Volume 67, Suppl 8, pp. 21-26, Retrieved from https://www.psychiatrist.com/pcc/neurodevelopmental/adhd/executive-functions-attention-deficit-hyperactivity/.
- Bauermeister, J., Shrout, P., Ramírez, R., Bravo, M., Alegría, M., Martínez-Taboas, A., Chávez, L., Rubio-Stipec, M. and García P. R. J., "ADHD correlates, comorbidity, and impairment in community and treated samples of children and adolescents.," Journal of Abnormal Child Psychology, 2007, Volume 35(6), pp.883-898. [CrossRef]
- Gnanavel, S., Sharma, P., Kaushal, P., & Hussain, S., "Attention deficit hyperactivity disorder and comorbidity: A review of literature," World Journal of Clinical Cases, 2019, Volume 7(17), pp. 2420-2426. [CrossRef]
- Marqués-Cabezas, P., Segura-Rodríguez, A., García-Barriuso, P., Gallardo-Borge, L., Mateos-Sexmero, M., Blanco, J., Queipo de LLano De la Viuda, M., Perez-Carranza, M., Aparicio-Parras, A., Espina-Barrio, J. and Rodriguez-Campos, A., "Comorbility symptoms in AHDH adult patients," European Psychiatry, 2022, Volume 65(S1), pp. S466-S466. [CrossRef]
- Brown, T. E., "Executive Functions and Attention Deficit Hyperactivity Disorder: Implications of two conflicting views," International Journal of Disability, Development and Education, 2006, Volume53(1), pp. 35-46. [CrossRef]
- Castellanos, X.F., Sonuga-Barke,E. J.S., Milham, M. P., & Tannock, R., "Characterizing cognition in ADHD: beyond executive dysfunction," Trends in Cognitive Sciences, 2006, Volume 10(3), pp. 117-123. [CrossRef]
- Lambek, R., Tannock, R., Dalsgaard, S., Trillingsgaard, A., Damm, D., & Thomsen, P., "Validating neuropsychological subtypes of ADHD: how do children with and without an executive function deficit differ?," The Journal of Child Psychological and Psychiatry, 2010, Volume 51(8), pp. 895-904. [CrossRef]
- Miyake, A., Friedman, N. P., Emerson, M. J., Witzki, A. H., Howerter, A., & Wager, T. D., "The Unity and Diversity of Executive Functions and Their Contributions to Complex “Frontal Lobe” Tasks: A Latent Variable Analysis," Cognitive Psychology, 2000, Volume 41(1), pp. 49-100. [CrossRef]
- Zhang, H., Shuai, L., Zhang, J., Wang, Y., Lu, T., Tan, X., Pan, J. and Shen, L., "Neuropsychological Profile Related with Executive Function of Chinese Preschoolers with Attention-Deficit/Hyperactivity Disorder: Neuropsychological Measures and Behavior Rating Scale of Executive Function-Preschool Version.," Chinese Medical Journal, 2018, Volume 131(6), pp. 648-656. [CrossRef]
- Babb, K. A., Levine, L. J., & Arseneault, J. M., "Shifting gears: Coping flexibility in children with and without ADHD.," International Journal of Behavioral Development, 2010, Volume 34(1), pp. 10-23. [CrossRef]
- Petersen, I., Hoyniak, C., McQuillan, M., Bates, J., & Staples, A., "Measuring the development of inhibitory control: The challenge of heterotypic continuity.," Developmental Review, 2016, Volume 40, pp. 25-71. [CrossRef]
- Bausela-Herreras, E., "Development of Executive Function at the Preschool Age," in Handbook of Research on Neurocognitive Development of Excecutive Funtions and Implications for Intervention, IGI Glogal, 2022, pp. 1-22.
- Zelazo, P., Müller, U., Frye, D., Marcovitch, S., Argitis, G., Boseovski, J., Chiang, J., Hongwanishkul, D., Schuster B. and Sutherland, A., "The development of executive function in early childhood.," Monographs of the Society for Research in Child Development, 2003, Volume 68(3), pp. vii-137. [CrossRef]
- Lensing, N., & Elsner, B., "Development of hot and cool executive functions in middle childhood: Three-year growth curves of decision making and working memory updating," Journal of Experimental Child Psychology, 2018, Volume 173, pp. 187-204. [CrossRef]
- Homer, B. D., Plass, J. L., Rose, M. C., MacNamara, A. P., Pawar, S., & Ober, T. M., "Activating adolescents’ “hot” executive functions in a digital game to train cognitive skills: The effects of age and prior abilities," Cognitive Development, 2019, Volume 49, pp. 20-32. [CrossRef]
- Prencipe, A., Kesek, A., Cohen, J., L. C., Lewis, M., & Zelazo, P., "Development of hot and cool executive function during the transition to adolescence," Jorunal of Experimental Child Psychology, 2011, Volume 108(3), pp. 621-631. [CrossRef]
- Rastikerdar, N., N. V., Sammaknejad, N., & Fathabadi, J., "Developmental trajectory of hot and cold executive functions in children with and without attention deficit-hyperactivity disorder (ADHD)," Research in Developmental Disabilities, 2023, Volume 137, Art. 104514. [CrossRef]
- Shakehnia, F., Amiri, S., & Ghamarani, A., "he comparison of cool and hot executive functions profiles in children with ADHD symptoms and normal children," Asian Journal of Psychiatry, 2021, Volume 55, pp.102483. [CrossRef]
- Berger, I., Slobodin, O., Aboud, M., Melamed, J., & Cassuto, H., "Maturational delay in ADHD: evidence from CPT," Frontiers in Human Neuroscience, 2013, Volume 7, pp.1-11. [CrossRef]
- Schoemaker, K., Bunte, T., Wiebe, S., Espy, K., Deković, M., & Matthys, W., "Executive function deficits in preschool children with ADHD and DBD," Journal of Child Psychology and Psychiatry, 2012, Volume 53, pp.111-119. [CrossRef]
- Roshani, F., Piri, R., & Malek A, M. T., "Comparison of cognitive flexibility, appropriate risk-taking and reaction time in individuals with and without adult ADHD.," Psychiatry Research, 2020 Volume 284, Art. 112494. [CrossRef]
- Karalunas, S. L., & Huang-Pollock, C. L., "Examining relationships between executive functioning and delay aversion in attention deficit hyperactivity disorder.," Journal of Clinical Child and Adolescent Psychology, 2011, Volume 40(6), pp. 837–847. [CrossRef]
- Yáñez-Téllez, G., Romero-Romero, H., Rivera-García, L., Prieto-Corona, B., Bernal-Hernández, J., Marosi-Holczberger, Guerrero-Juárez, E. V., Rodríguez-Camacho, M. and Silva-Pereyra, J. F., "Cognitive and executive functions in ADHD.," Actas Españolas de Psiquiatria, 2012, Volume 40(6), pp. 293-298.
- Zelazo, P., & Carlson, S., "Hot and Cool Executive Function in Childhood and Adolescence: Development and Plasticity," Child Development Perspectives, 2012, Volume 6(4), pp. 354-360. [CrossRef]
- Barkley, R. "Behavioral inhibition, sustained attention, and executive functions: constructing a unifying theory of ADHD," Psychological Bulletin, 1997, Volume 121(1), pp. 65-94. [CrossRef]
- Hobson, C., Scott, S., & Rubia, K., "Investigation of cool and hot executive function in ODD/CD independently of ADHD," The Journal of Child Psychology and Psychiatry, 2011, Volume 52(10), pp.1035-1043. [CrossRef]
- Nejati, V., "Reading mind from the eyes in individuals with attention deficit-hyperactivity disorder (ADHD): A meta-analysis," Expert Review of Neurotherapeutics, 2022, Volume 22(10), pp. 889-896. [CrossRef]
- Nigg, J., "Is ADHD a disinhibitory disorder?," Psychological Bulletin, 2001, Volume 127(5), pp. 571-598. [CrossRef]
- Barkley, R. "Advances in the diagnosis and subtyping of attention deficit hyperactivity disorder: what may lie ahead for DSM-V," Revista de Neurologia, 2009, Volume 48, suppl 2, pp. S101-106. [CrossRef]
- Servera, M., "Modelo de autorregulación de Barkley aplicado al trastorno por déficit de atención con hiperactividad: una revisión," Revista de Neurologia, 2005, Volume 40(6), pp. 358-368. [CrossRef]
- Kofler, M., Singh, L., Soto, E., Chan, E., Miller, C., Harmon, S., & Spiegel, J., "Working memory and short-term memory deficits in ADHD: A bifactor modeling approach.," Neuropsychology, 2020, Volume 34(6), pp. 686-698. [CrossRef]
- Kasper, L., Alderson, R., & Hudec, K., "Moderators of working memory deficits in children with attention-deficit/hyperactivity disorder (ADHD): a meta-analytic review.," Clinical Psychology Review, 2012, Volume 32(7), pp. 605-617. [CrossRef]
- Nejati, V., Derakhshan, Z., & Mohtasham, A., "The effect of comprehensive working memory training on executive functions and behavioral symptoms in children with attention deficit-hyperactivity disorder (ADHD)," Asian Journal of Psychiatry, 2023, Volume 81, Art.103469. [CrossRef]
- Yang, B., Chan, R., Gracia, N., Cao, X., Zou, X., Jing, J., Mai, J., Li, J. and Shum, D., "Cool and hot executive functions in medication-naive attention deficit hyperactivity disorder children," Psychological Medicine, 2011, Volume 41(12), pp. 2593-2602. [CrossRef]
- Cañas, J., Quesada, J., Antolí, A., & Fajardo, I., "Cognitive flexibility and adaptability to environmental changes in dynamic complex problem-solving tasks.," Ergonomics, 2003, Volume 46(5), pp. 482-501. [CrossRef]
- Schoemaker, M., Hijlkema, M., & Kalverboer, A., "Physiotherapy for clumsy children: an evaluation study," Developmental Medicine and Child Neurology, 1994, Volume 36(2), pp. 143-155. [CrossRef]
- Wixted, E., Sue, I., Dube, S., & Potter, A., Cognitive Flexibility and Academic Performance in College Students with ADHD: An fMRI Study., UVM Honors College Senior Theses. 126, 2016.Reetreived from https://scholarworks.uvm.edu/cgi/viewcontent.cgi?article=1144&context=hcoltheses.
- Chan, R. C., Shum, D., Toulopoulou, T., & Chen, E. Y., "Assessment of executive functions: Review of instruments and identification of critical issues," Archives of Clinical Neuropsychology, 2008, Volume 23, pp. 201-216. [CrossRef]
- Donders, J., "The Behavior Rating Inventory of Executive Function: Introduction," Child Neuropsychology, 2002 Volume 8(4), pp. 229-230. [CrossRef]
- Gioia, G., Kenworthy, L., & Isquith, P., "Executive Function in the Real World: BRIEF lessons from Mark Ylvisaker," Journal of Head Trauma Rehabilitation, 2010, Volume 25(6), pp. 433-439. [CrossRef]
- Henry, L. A., & Bettenay, C., "The assessment of executive functioning in children," Child and Adolescent Mental Health, 2010, Volume 15(2), pp. 110-119. [CrossRef]
- Lezak, M., Howieson, D., Bigler, E., & Tranel, D., Neuropsychological assessment, New York : Oxford University Press, 2012.
- Miyake, A., Emerson, M. J., & Friedman, N. P., "Assessment of executive functions in clinical settings: Problemas and recomendations," Seminars in speech and language, 2000, Volume 21(2), pp. 169-183. [CrossRef]
- Toplak, M., Bucciarelli, S., Jain, U., & Tannock, R., "Executive functions: performance-based measures and the behavior rating inventory of executive function (BRIEF) in adolescents with attention deficit/hyperactivity disorder (ADHD).," Child Neuropsychology, 2009, Volume 15(1), pp. 53-72. [CrossRef]
- Verdejo-García, A., & Bechara, A., "Neuropsychology of the executive Funtions," Psicothema, 2010, Volume 22(2), pp. 227-235. Retreived from https://www.psicothema.com/pdf/3720.pdf.
- Wild, K., & Musser, E. D., "The Cambridge Neuropsychological Test Automated Battery in the Assessment of Executive Functioning," in Handbook of Executive Funtioning, New York, Springer, 2014, pp. 171-190. [CrossRef]
- Kramer, J., Mungas, D., Possin, K., Rankin, K., Boxer, A., Rosen, H., Bostrom, A., Sinha, L., Berhel, A. and Widmeyer, M., "NIH EXAMINER: conceptualization and development of an executive function battery," Journal of International Neuropsychological Society, 2014, Volume 20, pp. 11-19. [CrossRef]
- Naglieri, J., & Das, J., Cognitive Assessment System, Itasca:: Riverside Publishing Company, 1997.
- Naglieri, J., Das, J., & Goldstein, S., Cognitive Assessment System2, Austin: ProEd, 2013.
- Delis, D., Kaplan, E., & Kramer, J., Delis Kaplan (D-KEFS) technical manual, San Antonio, TX: NCS Pearson Inc., 2001.
- Naglieri, J. A., & Goldstein, S., Comprenhensive Executive Functioning Index, Toronto: Multi Health Systems, 2013.
- Gioia, G., Isquith, P., Guy, S., & Kenworthy, L., BRIEF: Behavior Rating Inventory of Executive Function professional manual, Lutz, Florida: Psychological Assessment Resources., 2000.
- Guy, S. C., Isquith, P. K., & Gioia, G. A., Behavior Rating Inventory of Executive Function—Self Report Version, Lutz, Florida: Psychological Assessment Resources, 2004.
- Roth, R. M., Isquith, P. K., & Gioia, G. A., Behavior Rating Inventory of Executive Function. Adult Version (BRIEF-A), Lutz, Florida: Psychological Assessment Resources, 2005.
- Çak, H. T., Çengel, S. E., Gökler, B., Öktem, F., & Taşkıran, C., "The Behavior Rating Inventory of Executive Function and Continuous Performance Test in Preschoolers with Attention Deficit Hyperactivity Disorder," Psychiatry Investigation, 2017, Volume14(3), pp. 260-270. [CrossRef]
- Gioia, G. A., Espy, K. A., & Isquith, P. K., Behavior Rating Inventory of Executive Function Preschool Version (BRIEF-P:), Lutz, florida: Psychological Assessment Resources, 2003.
- García-Fernández, T., González-Pienda, j. A., Rodríguez-Pérez, C., & Álvarez-García, D., "Psychometric characteristics of the BRIEF scale for the assessment of executive functions in Spanish clinical population," Psicothema, 2014, Volume 26(1), pp. 47-54. [CrossRef]
- Skogan, A. H., Egeland, J., Zeiner, P., Øvergaard, K. R., Oerbeck, B., Reichborn-Kjennerud, T., & Aase, H., "Factor structure of the Behavior Rating Inventory of Executive Functions (BRIEF-P) at age three years," Child Neuropsychology, 2016, Volume 22(4), pp. 472-492. [CrossRef]
- Mahone, E. M., & Hoffman, J., "Behavior Ratings of Executive Function among Preschoolers with ADHD," The Clinical Neuropsychologist, 2007, Volume 21(4), pp. 569-586. [CrossRef]
- Page, M., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetzlaff, J. M., Akl, E., Brennan, S. E., Chou, R., Glanville, J., Jeremy J. M., Grimshaw, M., Hróbjartsson, A., Lalu, M. Tianjina, L., Loder, E. W., Mayo-Wilson, E., McDonald, S., McGuinness, L. A. and Alonso-fernández, S., "The PRISMA 2020 statement: an updated guideline for reporting systematic reviews," Revista Española de Cardiologia, 2021, Volume74(9), pp. 790-799. [CrossRef]
- Ezpeleta, L. and Granero, R., "Executive functions in preschoolers with ADHD, ODD, and comorbid ADHD-ODD: Evidence from ecological and performance-based measures," Journal of Neuropsychology, 2015, Volume 9(2), pp. 258-270. [CrossRef]
- Skogan, A. H., Zeiner, P., Egeland, J., Urnes, A.-G., Reichborn-Kjennerud, T., & Aase, H., "Parent ratings of executive function in young preschool children with symptoms of attention-deficit/-hyperactivity disorder," Behavioral and Brain Functions, 2015, Volume 11, Article 16. [CrossRef]
- Whiting PF, R. A., Mallett, S., Deeks, J., Reitsma, J., Leeflang, M., Sterne, J., Bossuyt. P. and Q.-2. Group, "QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies.," Annals of Internal Medicine, 2011, Volume 155(8), pp. 529-536. [CrossRef]
- Mallen, C., Peat, G., & Croft, P., "Quality assessment of observational studies is not commonplace in systematic reviews.," Journal of Clinical Epidemiology, 2006, Volume 59(8), pp. 765-769. [CrossRef]
- Wiebe, S., Sheffield, T., Nelson, J., Clark, C., Chevalier, N., & Espy, K., "The structure of executive function in 3-year-olds," Journal of Experimental Child Psychology, 2011, Volume 108(3), pp. 436-452. [CrossRef]
- Takacs, Z. and Kassai, R., "The efficacy of different interventions to foster children's executive function skills: A series of meta-analyses.," Psychological Bulletin, 2019, Volume 145(7), pp. 653-697. [CrossRef]
- Shaw, P., Stringaris, A., Nigg, J., & Leibenluft, E., "Emotion dysregulation in attention deficit hyperactivity disorder.," The American Journal of Psychiatry , 2014, Volume 171(3) pp. 276-293. [CrossRef]
- Salehinejad, M., Ghanavati, E., Rashid, M., & Nitsche, M. A. , "Hot and cold executive functions in the brain: A prefrontal-cingular network," Brein and Neurocience Advances, 2021, Volume 23; Art. 5. [CrossRef]
Figure 2.
Portion of studies with low, high and unclear risk of bias.
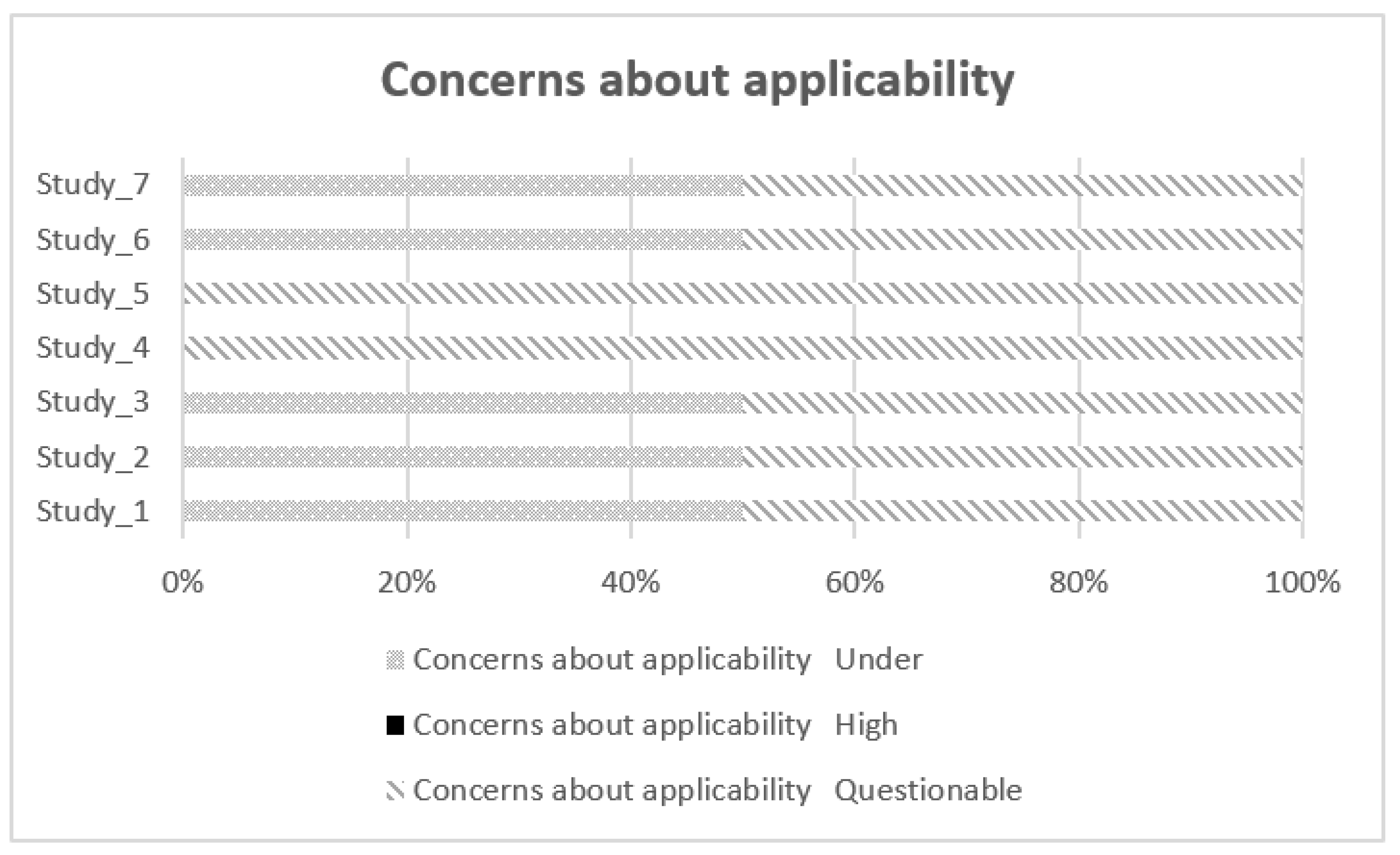
Figure 3.
Portion of studies with low, high and uncertain applicability concerns.
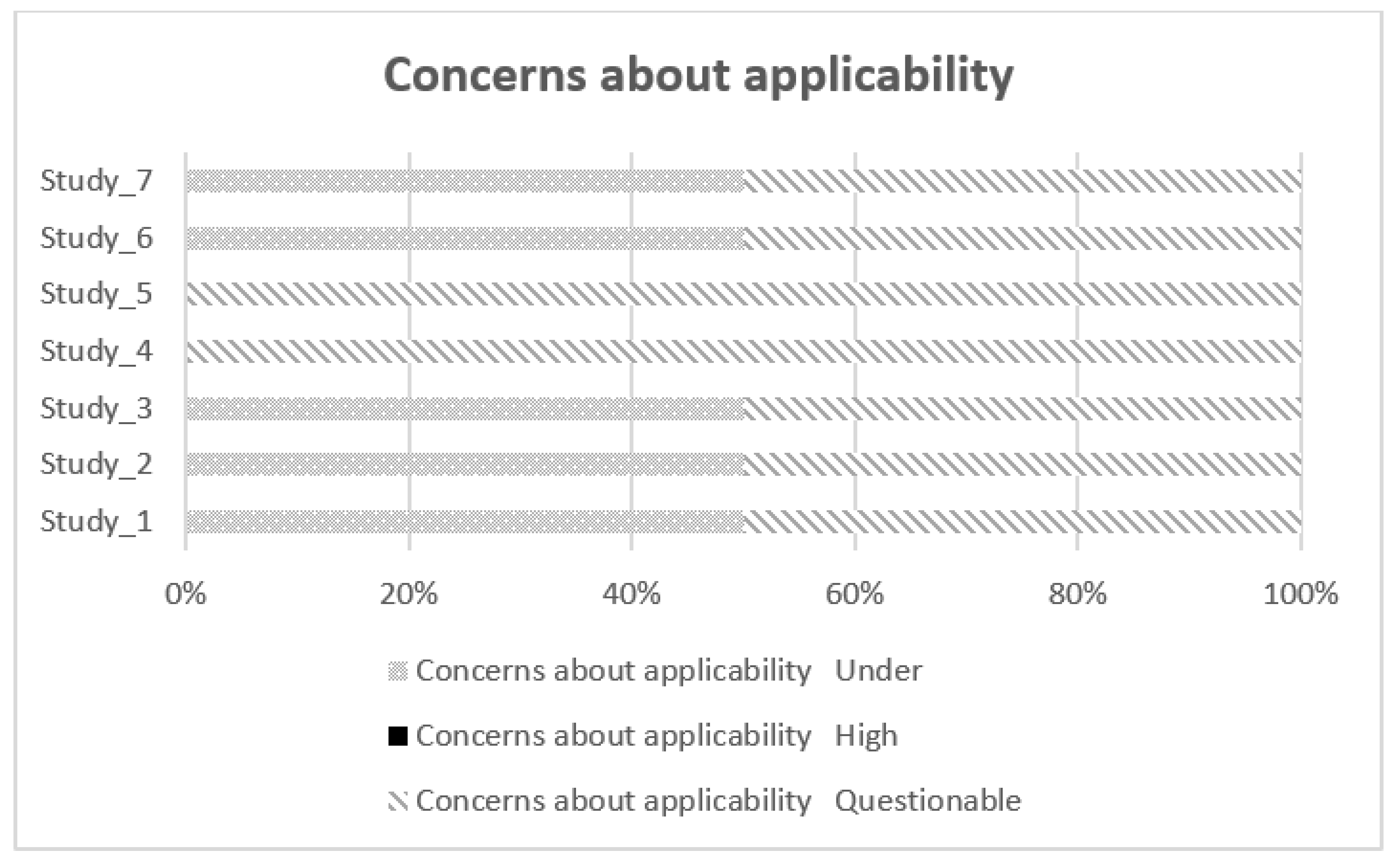
Figure 4.
Forest plot (soil effect).
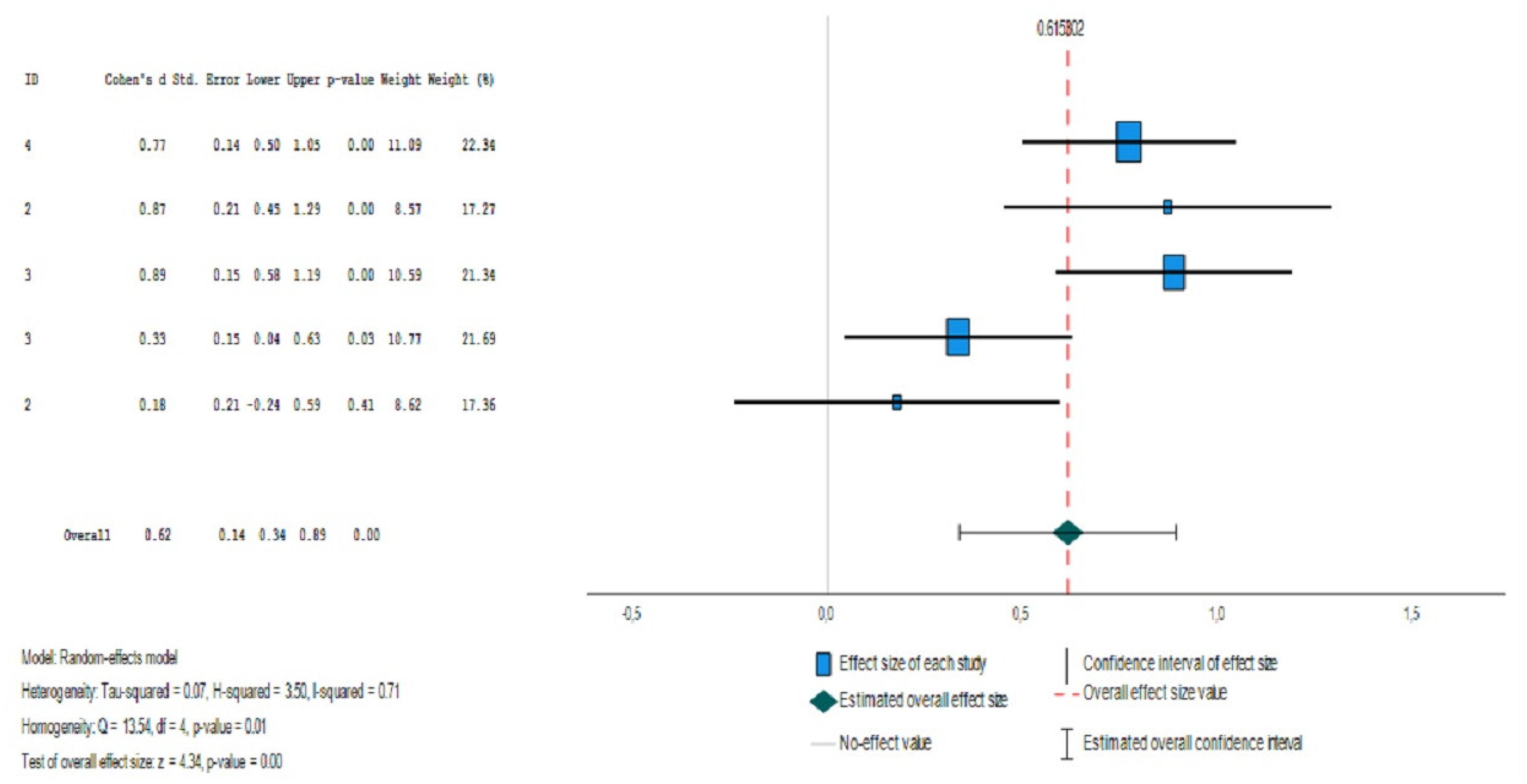
Figure 5.
Forestry graph (soil effect).
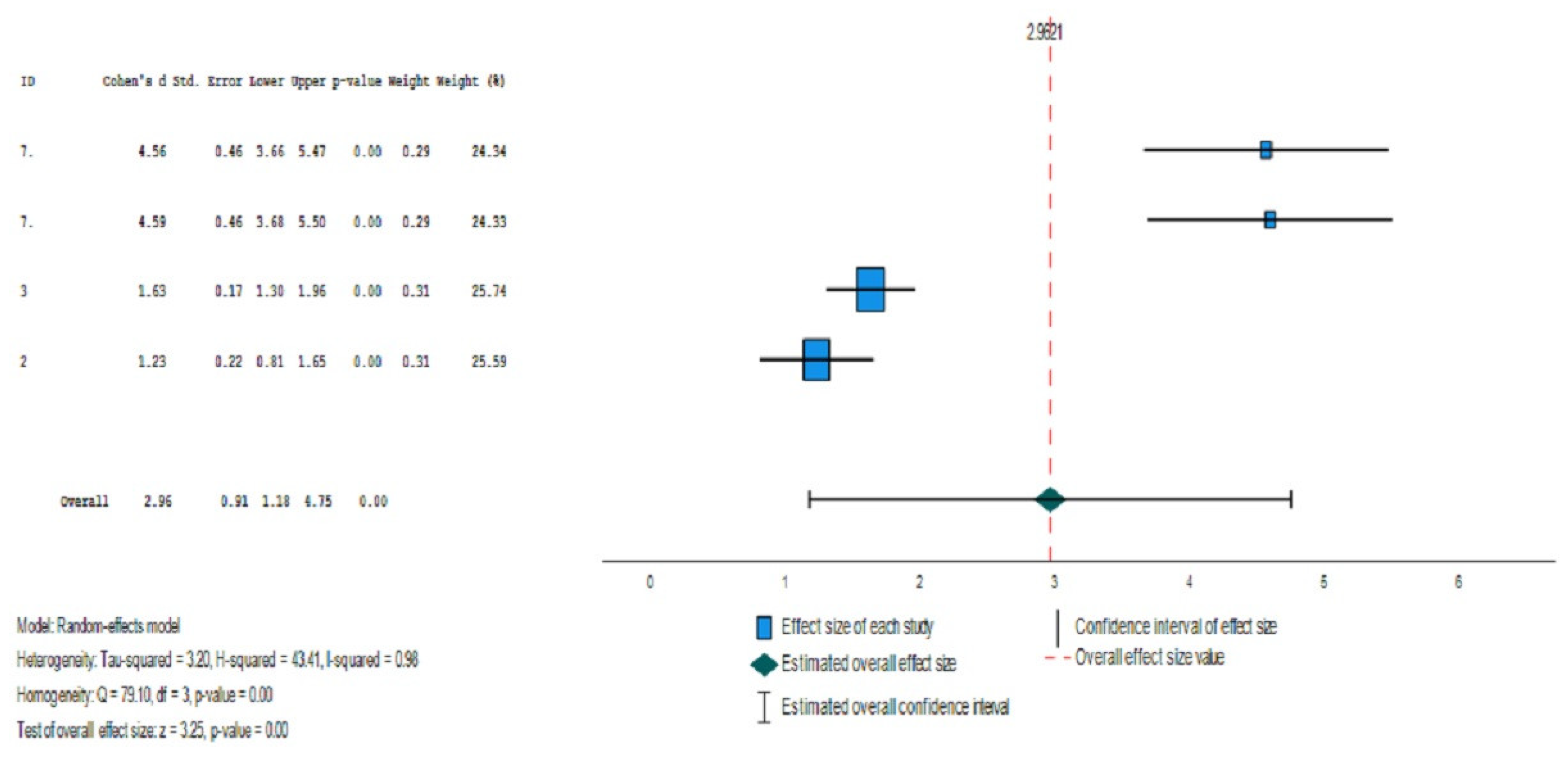
Table 3.
QUADAS-2 outcomes.
| Studies | Likelihood of bias | Concerns about applicability of results | |||||
| Selection of individuals | Index test | Reference test | Flow and schedule | Selection of patients | Index test | ||
| 1 | Low | Low | Low | Doubtful | Doubtful | Low | |
| 2 | High | Low | Low | Low | Low | Doubtful | |
| 3 | Low | Low | Low | Doubtful | Low | Doubtful | |
| 4 | Low | Low | Low | Doubtful | Doubtful | Doubtful | |
| 5 | Low | Low | Low | Doubtful | Doubtful | Doubtful | |
| 6 | Low | Low | Low | Low | Low | Doubtful | |
| 7 | Doubtful | Low | Low | Low | Low | Doubtful | |
Table 4.
Descriptive data of the studies included in the meta-analysis (floor effect).
| Study | Author | BRIEF_P | ADH | Typical Development | |||||
| N | M | STD | N | M | STD | ||||
| 4 | Skogan, et al. (2015) | Flexibility | 104 | 14.10 | 3,20 | 117 | 11.90 | 2.50 | |
| 2 | Ezpeleta, L., & Granero, R. (2015) | Emotional Control | 23 | 14.96 | 4,12 | 538 | 11.97 | 3.40 | |
| 3 | Zhang, H.-F., et al. (2018). | Emotional Control | 163 | 15.10 | 3,53 | 63 | 12.20 | 2.46 | |
| 3 | Zhang, H.-F., et al. (2018). | Flexibility | 163 | 13.40 | 3,03 | 63 | 12.41 | 2.79 | |
| 2 | Ezpeleta, L., & Granero, R. (2015) | Flexibility | 23 | 13.77 | 3,41 | 538 | 13.15 | 3.51 | |
| N: Sample size; M: Mean; STD: Standard Desviation; | |||||||||
Table 5.
Effect size estimates for the studies (floor effect).
| Effect size | Standard error | Z | Sig. (bilateral) | Confidence interval 95% | Prediction interval 95%a | ||||
| Lower | Upper | Lower | Upper | ||||||
| Global | .615 | .1419 | 4.335 | <.001 | .337 | .893 | -.343 | 1.574 | |
a. Based on t-distribution.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



