
Submitted:
27 October 2023
Posted:
27 October 2023
You are already at the latest version
Abstract
Background. Type 2 diabetes mellitus (T2DM) is becoming a major global health concern, especially in poorer nations. The high prevalence of obesity and the ensuing diabetes is attributed to rapid economic progress, physical inactivity, consumption of high-calorie foods, and changing lifestyles.
Objectives. We investigated the role of pro-inflammatory chemokines; CCL1, 2, 4 and 5 with varying levels of obesity in T2DM in the Asir region of Saudi Arabia.
Materials and methods. 170 confirmed T2DM patients and a normal control group were enrolled. The demographic data, serum levels CCL-1, 2, 4 and 5 and the biochemical indices were assessed in patients and control groups by standard procedures.
Results. T2DM patients were divided into four groups: A (normal body weight), B (Overweight), C (obese), and D (highly obese). n controls. We observed that male and female control patients had similar mean serum concentrations of pro-inflammatory chemokines CCL 1, 2, 4, and 5. Chemokines CCL1, CCL2, and CCL4 in the serum of Type 2 Diabetes Mellitus patients with normal or overweight body weights were significantly higher than the control group, regardless of gender. In T2DM individuals with obesity and severe obesity, the rise was most significant. There was a progressive rise in the concentrations of CCL1, 2, and 4 in T2DM) patients with increasing BMI. Serum CCL5 levels increased significantly in all T2DM patient groups. The increase in CCL5 was more predominant in normal-weight people as compared to overweight and obese T2DM patients.
Conclusions.
Male and female control patients had similar serum levels of pro-inflammatory chemokines CCL 1, 2, 4, and 5. The progressive rise in blood concentrations of three Pro-inflammatory chemokines; CCL1, 2, and 4 in T2DM patients with increasing BMI supports the idea that dyslipidemia and obesity contribute to chronic inflammation and insulin resistance. Serum CCL5 levels increased significantly in all T2DM patient groups. The selective and more pronounced increase of CCL5 in the T2DM group with normal BMI as compared to patients with varying degrees of obesity, was rather surprising. Further research is needed to determine if CCL5 under-expression in overweight and obese T2DM patients is due to some unexplained counterbalancing processes.
Keywords:
type-2 diabetes mellitus
; pro-inflammatory chemokines
; obesity
; CCL1
; CCL2
; CCL4
; CCL5
1. Introduction:
Type 2 diabetes mellitus, also known as T2DM, is a complex disease that has rapidly become a major public health concern around the globe, particularly in less developed nations [1,2,3,4]. The rapid advancement of the economy, the rise in the number of people who are inactive physically, the consumption of foods high in calories, and the evolution of lifestyles are all factors that have contributed to the increased prevalence of obesity and diabetes [4,5]. According to the International Diabetes Federation (IDF), the prevalence of type 2 diabetes mellitus among adults around the world was anticipated to be 536.6 million individuals in 2021, which would account for 10.5% of the global population. In addition, IDF forecasts that by the year 2045, the number of people worldwide who have diabetes will have increased to 783.2 million, making up 12.2% of the total population [6]. China, the world's second most populous developing nation with a population that accounts for roughly one-fifth of the total global population, has seen a significant rise in the number of people who are diagnosed with diabetes in recent years [7]. As per the recent estimates in Saudi Arabia, which has a total population of 24,194,300 people, the prevalence of diabetes is 17.7%, and there are around 4274100 adult diabetic patients (https://idf.org/our-network/regions-members/middle-east-and-north-africa/members/46-saudi-arabia.html, accessed on Oct.16, 2023). Diabetes, which is consistently ranked among the top 10 causes of death around the world, can more than double or even triple a person's likelihood of passing away from any cause [1,2]. Type 2 diabetes is responsible for nearly 95% of all cases of diabetes. The hallmark symptom is hyperglycemia which lasts for an extended period of time, and can be caused by either inadequate insulin synthesis or impaired insulin action [3,8]
It has been established that the frequency and occurrence of T2DM varies greatly around the world based on ethnicity and geographic location, with the largest risks being faced by Japanese, Hispanic, and Native American individuals [9,10,11]. The incidence rates of T2DM among Asians have been observed to be higher compared to white American and UK populations. Noteworthy is the fact that the black population is the category with the highest risk level in both demographics [1].
Although the precise etiology has not yet been determined, there are a number of factors that have been proposed as possible contributors [14,15]. These include social and economic variables, innate genetic predispositions, interactions between genes and the environment, and current lifestyle elements that contribute to obesity. A person's genetic susceptibility has a profound bearing on the likelihood that they may develop T2DM. The complex polygenic aspects of T2DM have been revealed thanks to the numerous genome-wide association studies that have been carried out over the course of the past decade [4,14,15] By primarily influencing the body's ability to produce insulin, the great majority of these genetic loci raise the chance of developing T2DM.
Long-term risks of T2DM include kidney failure, blindness, and cardiovascular disease in addition to diabetic neuropathy. Acute problems include diabetic ketoacidosis and hyperosmolar hyperglycemic syndrome [16]. Insulin resistance (IR), metabolic syndrome (MS), and decreased insulin production are hallmarks of T2DM, both of which contribute to the pathophysiology of the disease and make it practically impossible to effectively manage glycemic levels. It is estimated that 90 percent of persons who have diabetes are either overweight or obese, and obesity has emerged as one of the most significant risk factors for T2DM [17,18].
Recent observations suggest that inflammation, immunological dysregulation, alterations in gut microbiota, and cytokine dysregulation are the key pathophysiological contributors to T2DM [3,4,814]. The focus of many recent investigations has been on unraveling the molecular bases, of metabolic inflammation and its association with cardiometabolic disease and T2DM [19,20]. This inflammatory nexus has been a hallmark of obesity and MS [21,22]. Obesity-induced inflammation is mainly mediated by immune cells especially the macrophages and T lymphocytes [22,23]. In particular, adipose tissue macrophages (ATMs) are the major sources of pro-inflammatory cytokines that participate in diverse molecular signals leading to IR [23].
Chemokines, a well-known family of cytokines, play a significant role in inflammation and autoimmune disorders. [23,24]. More than fifty chemokines and a set of around 20 chemokine receptors expressed in adipocytes have been implicated in the acute and chronic inflammatory processes [25,26,27]. Chemokines can be broken down into four groups, each based on a different motif sequence containing two N-terminal cysteine residues (where X is any amino acid residue) [27]. Most CC chemokines act on monocytes, T cells, eosinophils, and basophils, which mediate chronic inflammation and allergies, while CXC chemokines are mostly chemotactic for neutrophils and are known to be involved in acute inflammation. Complex metabolic signals involving obesity and inflammation involve chemokines since most chemokines bind to multiple chemokine receptors and chemokine receptors have overlapping ligand specificities [22,25,27].
Chemo and cytokines are expressed in response to diverse stimulations that include excess nutrients and lead to an inflammatory cascade which creates a favorable ambiance for obesity, dysfunction of beta cells, and /or reduced insulin production [25,28]. Many Pro-inflammatory chemokines have been implicated in the pathogenesis of T2DM which is supposed to be multifaceted [22,24].
CCL1: Chemokine (C-C motif) ligand 1 is a small inducible glycoprotein cytokine and is also known as I-309 or TCA-3. It is encoded by the gene, Scya 1 and binds CCR8 as its receptor [22,24]. Increased levels of CCL1 have been reported in patients with T2DM who had comorbidities and diabetic complications [22,29]. The reports are inconsistent with some investigators suggesting a role for CCL1 in the pathogenesis of T2DM while others are of a contrary opinion [24,29]. Low sample sizes have also been a common feature of these studies, thus justifying further investigation of CCL1 in T2DM patients with a reasonable sample size.
CCL2: CCL2 is commonly known as monocyte chemoattractant protein-1(MCP-1). MCP-1 is widely known as a pro-inflammatory cytokine due to its chemotactic activity. It has been implicated in the pathogenesis of many diseases including atherosclerosis, obesity, and type-1 diabetes mellitus (T1DM) [30,31]. High levels of CCL2 were reported to be protective against T1DM and intriguingly associated with its complications [30,31]. While as many studies have shown higher CCL2 levels in T2DM [22], CCL2 is involved in the recruitment and differentiation of macrophages to a Pro-inflammatory state [30,32]. Several studies have shown positive outcomes in diabetic complications in association with decreased levels of CCL2 [32].
CCL4: It is a Pro-inflammatory chemokine and is also known as macrophage Inflammatory Protein-beta MIP-1β. It is encoded by the gene Scya4 and signals via the receptors CCR1 and CCR5. CCL4 has been reported to be upregulated in both type 1 and 2 diabetes and the circulatory levels of CCL4 were inversely associated with proinsulin. [22,33,34]. Inhibition of CCL4 has been reported to improve IR and decrease the chances of a hyperglycemic state leading to the progression of T2DM. [33].
CCL5: Aa a pro-inflammatory chemokine, CCK5 helps in the recruitment of leukocytes to the site of inflammation. Also known as RANTES (regulated on activation, normal T cell expressed and secreted), it is an 8 kDa protein made up of 68 amino acids and encoded by the Scya5 gene [35]. CCL5 is associated with many diseases including cardiovascular disorders, cancer, and different types of diabetes including T2DM [35,36,37]. CCL 5 is thought to be associated with IR in relation to age, HbA1c, obesity, and other factors, although the number of studies is limited [38]. With this background, we intended to study, the relationship of Pro-inflammatory chemokines, CCL1, CCL2, CCL4, and CCL5 with the etiopathogenesis of T2DM in patients with varying levels of obesity, BMI, and HbA1c in a patient cohort from Asir region of Saudia Arabia.
2. Methods
2.1. Study population
This collaborative and case-control study was conducted on 200 T2DM patients and 100 healthy controls from Asir region of Saudi Arabia (Figure 1).
All the study participants were Saudi citizens. The blood samples were collected at the Diabetic Centre, King Abdullah Hospital (KAH) in Bisha, and Asir General Hospital (AGH) in Abha. The recruitment period of the patients and controls was from March 2020 to May 2022. Informed consent was obtained from all patients and control subjects before the collection of blood samples.
2.2. Inclusion criteria
Only Saudi citizens living Asir region (Bisha and Abha cities and surrounding areas) were enrolled in this study. 200 confirmed T2DM patients who were on oral hypoglycemic agents and/or insulin were included in this study which comprised 110 males and 90 females.
2.3. Exclusion Criteria
The T2DM patients with other significant chronic diseases or malignancies were excluded from the study. Type 1 diabetes patients were also excluded from the study.
2.4. Inclusion criteria for controls
100 control subjects included healthy volunteers with no history of diabetes or any major clinical disorders and had normal fasting and random plasma glucose levels.
2.5. Exclusion criteria for controls
Those control subjects who had abnormal laboratory indices were excluded from the study, as a result, 85 control subjects (44 males and 41 females) were included in the study. The other criterion for selecting this limited number of control subjects was the availability of ELISA kits as each 96-well kit was sufficient for less than 88 samples after including the calibrators and QC samples.
2.6. Data collection
Finally, 170 Saudi citizens with confirmed T2DM (96 males and 74 females) who visited KAH and AGH for regular follow-up and met the inclusion criteria were made a part of the study. T2DM was diagnosed according to the parameters of WHO criteria. The case history, age, gender, body mass index (BMI), glycated hemoglobin (HbA1c), fasting and random blood glucose levels, total cholesterol, triacylglycerol (TG), high-density lipoprotein-cholesterol (HDL-C), and low-density lipoprotein-cholesterol (LDL-C) concentrations were among the various variables analyzed from the T2DM patients and controls. The established techniques were used to measure the anthropometric and biochemical parameters.
2.7. Blood specimen collection from T2DM patients
For each T2DM patient, 4 ml of peripheral blood was drawn into a red top tube without the use of any anticoagulants. One serum aliquot was immediately stored at -20oC till the estimation of interleukins. The second serum sample was sent right away for biochemical evaluation.
2.8. Blood specimen collection from healthy controls
Sample collections from all healthy age-matched control subjects were timed around routine blood draws that were part of the standard health exam. This eliminated the need for additional phlebotomy. For all controls, a sample of peripheral blood measuring about 4 ml was taken and placed in a red top tube without any anticoagulant. One serum aliquot was immediately stored at -20oC till the estimation of interleukins. The second serum part was immediately used for biochemical evaluation.
2.9. Estimation of Biochemical parameters
All the serum chemistry investigations were performed on a random access, multi-channel analyzer (Roche Diagnostics) in the medical laboratory department KAH, Bisha. The commercially available test kits including the calibrators and internal quality control samples from the manufacturer were used for these analyses.
Estimation of Chemokines: The serum concentrations of the four Pro-inflammatory chemokines viz. CCL1, CCL2, CCl4, and CCL5 were determined by enzyme-linked immunosorbent assays (ELISA) assays using commercially available kits from abcam, UK. The intra and inter-assay variations were less than 5%.
CCL1: The serum level of CCL1 was determined using a commercially available, high-sensitivity CCL1 Human ELISA Kit (abcam, UK, Cat No. ab314600, 96 wells) with a sensitivity of 1.4 picograms per milliliter (pg/mL) and a measuring range of 4.7 -300 pg/mL. The assay was performed as per the instructions of the manufacturer and the results were reported as pg/mL.
CCL2 (MCP-1): The serum level of CCL2 was determined using a commercially available Human MCP-1 ELISA kit (abcam UK. ab179886) with a sensitivity of 1.26 pg/mL and a measuring range of 4.7 -300 pg/mL. The assay was performed as per the instructions of the manufacturer and the results were reported as pg/mL.
CCL4 (MIP-β): The serum level of CCL4 was determined using a commercially available Human MIP- β ELISA kit (abcam UK. Ab100597) with a sensitivity of 2.5 pg/mL and a measuring range of 4.1 -1000 pg/mL. The assay was performed as per the instructions of the manufacturer and the results were reported as pg/mL.
CCL5 (RANTES): The serum level of CCL5 was determined using a commercially available Human RANTES ELISA kit (abcam UK. ab174446) with a sensitivity of 0.091 pg/mL and a measuring range of 0.94-60 pg/mL. The assay was performed as per the instructions of the manufacturer and the results were reported as pg/mL.
Statistical analysis: SPSS, version 20, was used to conduct the statistical analysis. Data that had a normally distributed distribution were presented as means with standard deviations (SD), while data that had a skewed distribution were displayed as medians (Q1–Q3). One-way analysis of variance (ANOVA) with the Tukey HSD test was used to determine the significance of differences for variables with normal distribution and homogenous variances; otherwise, Kruskal-Wallis one-way analysis of variance by ranks and the multiple comparison post hoc test were used. Values equal to or less than 0.05 (p<0.05) were deemed significant.
3. Results
3.1. Anthropometric indices and biochemical parameters of male T2DM patients
Table 1 lists the anthropometric and biochemical indices for male T2DM patients. The 96 male T2DM patients were divided into 4 groups on the basis of their BMI values. Group A comprised 25 T2DM patients with a normal BMI of 21.80 ± 2.14 kg/m2); Group B included 23 overweight patients with BMI of 27.44 ± 2.29 kg/m2; Group C had 24 patients with obesity and a BMI of 34.94 ± 3.18 kg/m2; and group D included 24 T2DM patients with severe obesity and a BMI of 47.22 ± 5.70 kg/m2. The 44 male control subjects had a normal BMI of 21.74 ± 1.78 (mean7±SD) kg/m2 as is presented in Table 1. The age for male T2DM patients ranged from 28 to 67 years and for controls from 28 to 62 years. There was no significant difference in WHR in groups A and B as compared to the controls while the group C and group D patients showed highly significant changes in WHR as compared to controls. Group D showed a very significant increase in WHR p<0.001 as compared to groups A and B whereas group C patients showed a significant increase p< 0.01 in WHR versus groups A and B. T2DM patients in groups A and B did not exhibit any significant increase in BMI as compared to controls whereas BMI increased significantly in group C and D as compared to controls.
T2DM patients in Group C had significantly higher BMI as compared to groups A and B with p<0.001 whereas Group D patients had very significantly increased BMI versus Group A and B with p< 0.001 and also significantly increased BMI versus Group C with p<0.01. T2DM patients in groups A, B, and C didn’t show any significant differences in fasting glucose levels compared to controls while group D patients had significantly higher fasting glucose values(p<0.001). HbA1c did not exhibit any significant differences between the various patient groups (groups A, B, and D), although it was considerably higher in all four groups of T2DM patients when compared to the control group with a p< 0.001. T2DM patients in group C patients showed significantly higher HbA1c as compared to groups A, B, and D (p<0.001). Groups A to C depicted significant differences in total cholesterol in comparison with the control group (p<0.01) but group D showed a very significantly increased total cholesterol level as compared to the controls(p<0.001). Group A-C did not show any significant differences in the total cholesterol levels mutually. HDL-cholesterol levels were unremarkable in all the patients as compared to the control group, although there was an apparent and comparable decrease in HDL values in the patient groups. LDL cholesterol was similar in control subjects and T2DM patients in group A but was significantly higher in patient groups B and C as compared to controls(p<0.001). Group D patients also had very significantly higher LDL levels as compared to group A T2DM patients and controls (p< 0.001). The triglyceride levels in T2DM patients of groups A-C were significantly higher as compared to the controls (p<0.01). The Group D patients showed a very significant increase in the TG levels with p<0.001 in comparison to controls. Group D also reported significantly higher TG levels as compared to T2DM patients in groups A-C with p<0.01.
3.2. Anthropometric indices and biochemical parameters of female T2DM patients
Table 2 summarizes the anthropometric and biochemical indices for 74 female T2DM patients. As can be seen in Table 2, the age for 74 female T2DM patients ranged from 27 to 69 years, and for controls from 27 to 64 years. WHR was significantly higher in group C and group D patients as compared to control subjects. Group D showed a very significant increase in WHR p<0.001 as compared to controls and groups A and B whereas group C patients showed a significant increase in WHR versus groups A and B and control group with p< 0.01.
The 41 control subjects in the female group had a normal BMI of 21.20 ± 1.66 kg/m2. Based on their BMI values, the female T2DM patients were divided into 4 groups. Group A comprised of 18 patients with normal body weight and BMI of 21.41 ± 2.14 kg/m2); group B included 19 overweight patients with BMI of 28.22 ± 2.26 kg/m2; group C had 20 patients with obesity and a BMI of 33.88± 3.20kg/m2 and group D included 17 T2DM patient with severe obesity and a BMI of 46.48 ± 5.20 kg/m2. BMI showed no significant increase in groups A and B whereas it was very significantly increased in group C and D as compared to controls (p< 0.001). Group C patients had significantly increased BMI as compared to groups A and B with a p<0.0.01 whereas group D patients had very significantly increased BMI versus group A and B (p< 0.001) and a significantly increased BMI versus group C with p<0.01.
The fasting glucose values in groups A to C were significantly higher as compared to controls with p< 0.01 while Group D had very significantly higher fasting glucose concentrations as compared to with controls p< 0.001. HbA1c was very significantly increased in all four female T2DM patient groups as compared to the control group with p< 0.001 but did not show any significant difference among the different patient groups (A-D) mutually.
The female T2DM patient groups A and B showed significantly higher total cholesterol values as compared to the control subjects with a p< 0.01. The Group C and D patients showed Very significantly higher levels of total cholesterol as compared to controls with p< 0.001. T2DM patients in groups C and D also depicted significantly higher total cholesterol results as compared to groups A and B with p< 0.01. HDL-cholesterol levels remained similar in groups A and B as compared to the control group but showed some insignificant decrease in groups C and D when compared to controls. LDL cholesterol was similar in controls and group A T2DM patients but was significantly higher in patient groups C and D as compared to controls(p<0.001). Group D patients depicted very significantly higher LDL levels as compared to group A T2DM patients (p< 0.001). The triglyceride levels in T2DM patients of groups A-C were significantly higher as compared to the controls (p<0.01). The Group D patients showed a very significant increase in the TG levels with p<0.001in comparison to controls. Group D also reported significantly higher TG levels as compared to Group A and Group B T2DM patients with p<0.01.
3.3. Chemokine Concentrations in male T2DM patients and controls
The serum levels of chemokines CCL1, CCL2, CCL4, and CCL5 in male T2DM patients and control subjects are depicted in n Table 3.
CCL1 (I-309 or TCA-3): The average serum level of CCL1 was 158± 21.02 pg/mL in normal male controls. CCL1 levels were significantly elevated in groups A and B as compared to controls with p<0.01. Groups C and D depicted elevated levels of CCL1 with very high significance (p<0.001 as compared to control subjects. Severely obese T2DM patients in Group D showed higher levels of CCL1 as compared to Group C with p<0.04. Group D T2DM patients also showed significantly high levels of CCL1 compared to groups A and B, with p<0.01. Obese T2DM patients in group C showed significantly elevated levels of CCL1 as compared to group A T2DM patients with normal body weight. The cluster charts of serum Chemokines CCL1, CLL2, and CCL4 in male controls and T2DM patient groups are displayed in Figure 2.
CCL2 (MCP-1): The mean serum level of CCL2 was 288 ± 33.12 pg/mL in normal male controls. CCL2 levels were significantly increased in groups A and B as compared to controls with p<0.05. Obese and highly obese patients in Groups C and D depicted elevated levels of CCL2 with very high significance (p<0.001 as compared to control subjects. Severely obese T2DM patients in Group D showed higher levels of CCL2 as compared to Group C with p<0.04. Group D T2DM patients also showed significantly high levels of CCL2 compared to groups A and B, with p<0.01. Obese T2DM patients in group C showed significantly elevated levels of CCL2 as compared to group A T2DM patients with normal body weight with p<0.01. The cluster charts of serum CLL2, and CCL4 in male controls and T2DM patient groups are displayed in Figure 2.
CCL4 (MIP-1β): The mean serum level of CCL4 was 186± 22.56 pg/mL in normal male controls. CCL4 levels were significantly increased in groups A and B as compared to controls with p<0.05. Obese and highly obese patients in Groups C and D depicted elevated levels of CCL4 with very high significance (p<0.001) as compared to control subjects. Severely obese T2DM patients in Group D showed higher levels of CCL4 as compared to Group C with p<0.04 and significantly high levels of CCL4 compared to groups A and B, with p<0.01. The cluster chart of serum CCL4 in male control and T2DM patient groups is displayed in Figure 2.
CCL5 (RANTES):The mean serum level of CCL5 was 4880± 348.98 pg/mL in normal male controls. The increase in CCL5 levels in group A was very highly significant as compared to controls with p< 0.001. Groups B and C showed significantly elevated levels of CCL5 as compared to controls with p< 0.01 Groups B, C, and D also showed significantly decreased levels of CCL5 as compared to group A with p< 0.01. Severely obese T2DM patients in Group D showed higher levels of CCL5 as compared to controls with p<0.05 and significantly lower levels of CCL5 as compared to T2DM patients with normal body weight with p<0.01. The error diagram of serum CCL5 levels in T2DM patients and male controls is displayed in Figure 3.
3.4. Chemokine Concentrations in female T2DM patients and controls
The serum levels of chemokines CCL1, CCL2, CCL4, and CCL5 in female T2DM patients and control subjects are summarized in Table 4.
CCL1 (I-309 or TCA-3): The mean serum level of CCL1 was 152± 20.88 pg/mL in normal female controls. CCL1 levels were significantly elevated in groups A and B (262± 27.52 and 311± 25.10 pg/mL respectively) as compared to controls with 152± 20.88 pg/mL (p<0.01). Obese and very obese female patients in Groups C and D depicted elevated levels of CCL1 with very high significance (p<0.001 as compared to control subjects. Severely obese female T2DM patients in Group D showed higher levels of CCL1 as compared to Group C with p<0.04. Group D T2DM patients also showed significantly high levels of CCL1 compared to groups A and B, with p<0.01. Obese female T2DM patients in group C also showed significantly elevated levels of CCL1 as compared to group A T2DM patients with normal body weight. The cluster charts of serum Chemokines CCL1, CCL2, and CCL4 in female controls and T2DM patients are displayed in Figure 4.
CCL2 (MCP-1): The mean serum level of CCL2 was 275 ± 32.14 pg/mL in normal female controls which is more or less similar to that of male control subjects. CCL2 levels were significantly increased in groups A and B as compared to controls with p<0.05. Obese and highly obese patients in Groups C and D depicted elevated levels of CCL2 with very high significance (p<0.001 as compared to control subjects. Severely obese female T2DM patients in Group D showed higher levels of CCL2 as compared to Group C with p<0.04. Group D T2DM patients also showed significantly high levels of CCL2 compared to groups A and B, with p<0.01. Obese T2DM female patients in group C showed significantly elevated levels of CCL2 as compared to group A T2DM patients with normal body weight with p<0.01. The cluster charts of serum CLL2 for male controls and T2DM patients are displayed in Figure 4.
CCL4 (MIP-1β): The mean serum level of CCL4 in female control subjects was 194± 22.54 mg/mL as compared to 186±22.56 pg/mL in male controls. CCL4 levels were significantly increased in groups A and B as compared to controls with p<0.05. Obese and highly obese patients in Groups C and D depicted elevated levels of CCL4 with very high significance (p<0.001) as compared to control subjects. Obese T2DM female patients in group C showed significantly elevated levels of CCL2 as compared to group A and B T2DM patients with p<0.04. Severely obese T2DM patients in Group D showed higher levels of CCL4 as compared to obese Group C T2DM patients with p<0.04 and significantly high levels of CCL4 compared to groups A and B, with p<0.01. A cluster chart of serum CCL4 in female control and T2DM patient groups is displayed in Figure 4.
CCL5 (RANTES): The mean serum level of CCL5 in female control subjects was 4756± 342.56 pg/mL as compared to 4880± 348.98 pg/mL in male controls. The mean CCL5 level in group A (9546± 522.44 pg/mL) was very highly elevated as compared to controls with p<0.001. Groups B and C showed significantly elevated levels of CCL5 as compared to controls with p< 0.01. Groups B, C, and D also showed significantly decreased levels of CCL5 as compared to group A with p<0.01. Severely obese T2DM patients in Group D showed higher levels of CCL5 as compared to controls with p<0.05 and significantly lower levels of CCL5 as compared to T2DM patients with normal body weight with p<0.01. The error diagram of serum CCL5 levels for female T2DM patients and controls is displayed in Figure 5.
4. Discussion
Insulin resistance and faulty insulin production are hallmarks of the pathogenesis of T2DM. One of the most prominent risk factors for type 2 diabetes is obesity [8,14,15]. Several studies have revealed key pathophysiological aspects of T2DM, including inflammation, chemokine dysregulation, gut microbiome alterations, and immunological dysregulation [3,4,8,14]. Many inflammatory cytokines and other variables contribute to the inflammatory nexus that is characteristic of obesity and MS [19,23,24]. Pro-inflammatory chemokines have been linked to the etiology of T2DM, although the results have been mixed and inconsistent [22,23,24]. Using a patient and a control cohort from the Asir region of Saudia Arabia, we looked into the association between the Pro-inflammatory chemokines CCL1, CCL2, CCL4, and CCL5 and the etiopathogenesis of T2DM in people with different degrees of obesity, BMI, and HbA1c.
CCL1 (I-309 or TCA-3): The mean levels of CCL1 were similar in male (N=44) and female (N=41) control subjects which is in agreement with previous studies [22,24,29]. CCL2 levels in T2DM patients with normal body weight (group A) and in overweight (group B) were significantly higher as compared to the controls in both males and females with p<0.01. Obese and highly obese T2DM patients of both genders in groups C and D depicted very highly significant elevations in CCL1 levels with p<0.001. The highest levels of CCL1 were observed in group D. These results are in conformity with other studies [22,24]. CCL 1 is believed to mediate the recruitment of monocytes, macrophages, Th2, and Treg cells by interacting with the CCR8 chemokine receptor [22,39]. This turn of events results in the release of many pro-inflammatory cytokines including IL-1 β [22,40]. The resultant inflammatory cascade results in impaired secretion of insulin in β islet cells [41]. IL-6 and IL-1 β are involved in IR mediated through the under-expression of insulin receptor substrate-1 (IRS-1) and also suppress the activity of lipoprotein lipase resulting in hypertriglyceridemia [42]. CCL1 is believed to act like a double-edged sword predisposing the patients to both obesity and insulin resistance, this assumption seems plausible in the light of significantly higher levels of CCL1 in T2DM patients in all the four groups A to D, ranging from normal body weight to severe obesity.
CCL2 (MCP-1): CCL-2 is a Pro-inflammatory chemokine that exerts its action by specifically binding to CCR2 receptors. The mean levels of CCL2 were similar in male (288 ± 33.12 pg/mL) and female (275 ± 32.14 pg/mL) controls, which agrees with previous studies [2,3,8]. CCL2 levels in T2DM patients with normal body weight (group A) and in overweight (group B) were significantly higher as compared to the controls in both males and females with p<0.05. Obese and highly obese T2DM patients of both genders in (groups C and D) showed very highly significant elevations in CCL2 levels with p<0.001 Group C (obese T2DM patients) showed significantly elevated levels of CCL2 as compared to controls with p<0.01. Although a few studies showed lower levels of CCL-2 in the prediabetic state, our results are partly consistent with earlier studies that reported higher levels of CCL2 in prediabetes, T1DM, and T2DM in general as there was no further subdivision on the basis of BMI and level of obesity in those studies [2,3,8,22]. A previous study from KSA showed higher levels of CCL2 in obese women and lower levels in obese men without any significance which is in contrast with our study outcomes and previous studies [43]. Overnutrition and resultant obesity is involved in the activation of adipose tissue especially the ATMs leading to higher levels of CCL2 [44,45]. CCL2 plays an active role in the recruitment of monocytes, NK cells, and other inflammatory cells and hence is a significant contributor to the inflammatory cascade which is a turning point in IR and MS[46,47]. The inhibition of CCL2 in animal models has been reported to modulate the inflammation cascade and ameliorate the symptoms of insulin resistance [48,49,50]. CCL2 has not been the subject of human studies like these, but it shows promise in both understanding the mechanisms behind the onset of IR and MS and in developing effective treatments for these conditions.
CCL4 (MIP-1β): Our results showed that mean levels of CCL4 were similar in male (186± 22.56 pg/mL) and female (194± 22.54 pg/mL) controls. CCL4 levels in T2DM patients with normal body weight (group A) and in overweight (group B) were significantly higher as compared to the controls in both the genders with p<0.05. T2DM patients in group C and D (obese and severely obese respectively in both genders showed very highly significant elevations in CCL4 levels with p<0.001. In both males and females, severely obese T2DM patients in Group D showed higher levels of CCL4 as compared to obese Group C T2DM patients with p<0.04 and significantly elevated levels of CCL4 compared to groups A and B, with p<0.01 as is displayed in Table 4 and Figure 4. Our results on CCL 4 are mostly consistent with previous studies which reported higher levels of CCL4 in all types of diabetes although there was no segregation of the patients on the basis of gender and BMI [22,50,51]. CCL4 is a Pro-inflammatory chemokine and is involved in the upregulation of the inflammatory pathways leading to IR and its inhibition has been seen to improve the IR and glycemic control in animal models [13,22]. The exact mechanism involving CCL4 in the IR and MS and its possible therapeutic roles (if any) are still elusive and need further studies.
CCL5 (RANTES): Also known as RANTES, CCL4 exerts its effects by binding to the chemokine receptor CCR5 and is a Pro-inflammatory chemokine [22]. Our study depicted almost similar serum levels of CCL5 in both male and female control groups as is true of other chemokines. In line with previous studies, our results showed a general trend of CCL5 elevation in T2DM patients as compared to controls (irrespective of gender) but an increase in serum CCL5 in the group A T2DM patients with normal body weight was highly pronounced with p < 0.001 in contrast to Groups B to D as can be seen in Figure 3 and Figure 5 [22,43,48]. CCL5 helps in the recruitment of leucocytes to the sites of inflammation and has been implicated in many diseases including T2DM [35,36,37]. Our observation that T2DM patients with varying levels of obesity (Groups B to D) showed significantly lower CCL5 levels irrespective of gender as compared to T2DM patients with normal body weight is a bit bewildering and we don’t have any concrete explanation for this phenomenon. It could be an observation that might have been overseen in previous studies as there was no subgrouping on the basis of BMI in T2DM patients in previous studies [22, 43). One possible explanation is that there might be some counterbalancing mechanism in overweight and obese T2DM patients which leads to the under-expression of CCL5.
5. Limitations
A Possible limitation of our study was the relatively small sample size. Future prospective studies are needed with a large sample size to explore the plausible role above and more chemokines in the etiopathogenesis of T2DM and therapeutic interventions (if any).
6. Conclusions
In this investigation, we observed that the mean serum concentrations of pro-inflammatory chemokines CCL 1, 2, 4, and 5 did not significantly differ between male and female control patients. The concentrations of chemokines CCL1, CCL2, and CCL4 in the serum of individuals with Type 2 Diabetes Mellitus who have a normal body weight and those who are overweight were shown to be considerably elevated compared to the control group, regardless of gender. The observed increase demonstrated the greatest level of statistical significance among those T2DM patients with both obesity and severe obesity. The observation of a progressive rise in blood concentrations of three Pro-inflammatory chemokines (CCL1, 2, and 4) among individuals with type 2 diabetes mellitus (T2DM), in relation to increasing body mass index (BMI), reinforces the notion that dyslipidemia and obesity play a substantial role in the pathogenesis of chronic inflammation, ultimately leading to insulin resistance. The levels of serum CCL5 exhibited a substantial and statistically significant increase across all groups of patients with T2DM. However, this elevation was particularly prominent in individuals with a normal body weight. Further work is warranted to explore potential counterbalancing mechanisms that may account for the observed under-expression of CCL5 in overweight and obese T2DM individuals.
Acknowledgments
The authors are thankful to the Deanship of Scientific Research at the University of Bisha for supporting this work through the Fast-Track Research Support Program.
Conflicts of Interest
None
References
- Sun H, Saeedi P, Karuranga S, et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022;183:109119. [CrossRef]
- Yan Y, Wu T, Zhang M, Li C, Liu Q, Li F. Prevalence, awareness and control of type 2 diabetes mellitus and risk factors in Chinese elderly population. BMC Public Health. 2022;22(1):1382. Published 2022 Jul 19. [CrossRef]
- Mir MM, Mir R, Alghamdi MAA, et al. Differential Association of Selected Adipocytokines, Adiponectin, Leptin, Resistin, Visfatin and Chemerin, with the Pathogenesis and Progression of Type 2 Diabetes Mellitus (T2DM) in the Asir Region of Saudi Arabia: A Case Control Study. J Pers Med. 2022;12(5):735. Published 2022 May 1. [CrossRef]
- Mir MM, Mir R, Alghamdi MAA, et al. Potential impact of GCK, MIR-196A-2 and MIR-423 gene abnormalities on the development and progression of type 2 diabetes mellitus in Asir and Tabuk regions of Saudi Arabia. Mol Med Rep. 2022;25(5):162. [CrossRef]
- Qadir MI, Ahmed Z. lep Expression and Its Role in Obesity and Type-2 Diabetes. Crit Rev Eukaryot Gene Expr. 2017;27(1):47-51. [CrossRef]
- Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract. 2019;157:107843. [CrossRef]
- Zhou X, Guan H, Zheng L, et al. Prevalence and awareness of diabetes mellitus among a rural population in China: results from Liaoning Province. Diabet Med. 2015;32(3):332-342. [CrossRef]
- Moin ASM, Butler AE. Alterations in Beta Cell Identity in Type 1 and Type 2 Diabetes. Curr Diab Rep. 2019;19(9):83. Published 2019 Aug 10. [CrossRef]
- Yin J, Yeung R, Luk A, et al. Gender, diabetes education, and psychosocial factors are associated with persistent poor glycemic control in patients with type 2 diabetes in the Joint Asia Diabetes Evaluation (JADE) program. J Diabetes. 2016;8(1):109-119. [CrossRef]
- Liu M, Lv X, Li Y, Li J, He Y. Prevalence and Control Status of Diabetes and Related Risk Factors Among 4196 Chinese Male Older Elderly Aged ≥80 Years. Int J Gerontol. 2018;12(2):122–126. [CrossRef]
- Wang H, Yao J, Yin X, et al. Organisational and individual characteristics associated with glycaemic control among patients with type 2 diabetes: cross-sectional study in China. BMJ Open. 2020;10(4):e036331. Published 2020 Apr 6. [CrossRef]
- Irazola V, Rubinstein A, Bazzano L, et al. Prevalence, awareness, treatment and control of diabetes and impaired fasting glucose in the Southern Cone of Latin America. PLoS One. 2017;12(9):e0183953. Published 2017 Sep 6. [CrossRef]
- Hu D, Fu P, Xie J, et al. Increasing prevalence and low awareness, treatment and control of diabetes mellitus among Chinese adults: the InterASIA study. Diabetes Res Clin Pract. 2008;81(2):250-257. [CrossRef]
- Galicia-Garcia U, Benito-Vicente A, Jebari S, et al. Pathophysiology of Type 2 Diabetes Mellitus. Int J Mol Sci. 2020;21(17):6275. Published 2020 Aug 30. [CrossRef]
- Abdul-Ghani MA, Jayyousi A, DeFronzo RA, Asaad N, Al-Suwaidi J. Insulin Resistance the Link between T2DM and CVD: Basic Mechanisms and Clinical Implications. Curr Vasc Pharmacol. 2019;17(2):153-163. [CrossRef]
- Forbes JM, Cooper ME. Mechanisms of diabetic complications. Physiol Rev. 2013;93(1):137-188. [CrossRef]
- Niu G, Li J, Wang H, Ren Y, Bai J. Associations of A-FABP with Anthropometric and Metabolic Indices and Inflammatory Cytokines in Obese Patients with Newly Diagnosed Type 2 Diabetes. Biomed Res Int. 2016;2016:9382092. [CrossRef]
- Urbanavičius V, Abalikšta T, Brimas G, Abraitienė A, Gogelienė L, Strupas K. Comparison of changes in blood glucose, insulin resistance indices, and adipokine levels in diabetic and nondiabetic subjects with morbid obesity after laparoscopic adjustable gastric banding. Medicina (Kaunas). 2013;49(1):9-14. [CrossRef]
- Shoelson SE, Lee J, Goldfine AB. Inflammation and insulin resistance. J Clin Invest 2006;116:1793-801. [CrossRef]
- Hotamisligil GS, Shargill NS, Spiegelman BM. Adipose expression of tumor necrosis factor-alpha: direct role in obesity linked insulin resistance. Science 1993;259:87-91. [CrossRef]
- Xu H, Barnes GT, Yang Q, Tan G, Yang D, Chou CJ, Sole J, Nichols A, Ross JS, Tartaglia LA, Chen H. Chronic inflammation in fat plays a crucial role in the development of obesity-related insulin resistance. J Clin Invest 2003;112:1821-30. [CrossRef]
- Pan X, Kaminga AC, Wen SW, Liu A. Chemokines in Prediabetes and Type 2 Diabetes: A Meta-Analysis. Front Immunol. 2021;12:622438. Published 2021 May 13. [CrossRef]
- Liang W, Qi Y, Yi H, et al. The Roles of Adipose Tissue Macrophages in Human Disease. Front Immunol. 2022;13:908749. Published 2022 Jun 9. [CrossRef]
- Xu L, Kitade H, Ni Y, Ota T. Roles of Chemokines and Chemokine Receptors in Obesity-Associated Insulin Resistance and Nonalcoholic Fatty Liver Disease. Biomolecules. 2015;5(3):1563-1579. Published 2015 Jul 21. [CrossRef]
- Gerard C, Rollins BJ. Chemokines and disease. Nat Immunol 2001;2:108-15. [CrossRef]
- Zlotnik A, Yoshie O. Chemokines: a new classification system and their role in immunity. Immunity 2000;12:121-7. [CrossRef]
- Hughes CE, Nibbs RJB. A guide to chemokines and their receptors. FEBS J. 2018;285(16):2944-2971. [CrossRef]
- Chait A, den Hartigh LJ. Adipose Tissue Distribution, Inflammation and Its Metabolic Consequences, Including Diabetes and Cardiovascular Disease. Front Cardiovasc Med. 2020;7:22. Published 2020 Feb 25. [CrossRef]
- CHEN, Hai-jun, et al. "Association between serum levels of interleukin-12, Chemokine cytokines ligand 1 and occurrence of Type 2 diabetes mellitus complicated with pulmonary tuberculosis." Chinese Journal of Antituberculosis 39.12 (2017): 1278. [CrossRef]
- Ooms, Mark, et al. "Increased spontaneous CCL2 (MCP-1) and CCL5 (RANTES) secretion in vitro in LADA compared to type 1 diabetes and type 2 diabetes: Action LADA 14." Diabetes/metabolism research and reviews 37.7 (2021): e3431. [CrossRef]
- Guan, Ruili, et al. "Chemokine (CC motif) ligand 2 (CCL2) in sera of patients with type 1 diabetes and diabetic complications." PloS one 6.4 (2011): e17822. [CrossRef]
- Chang TT, Chen JW. The Role of Chemokines and Chemokine Receptors in Diabetic Nephropathy. Int J Mol Sci. 2020;21(9):3172. Published 2020 Apr 30. [CrossRef]
- Chang TT, Lin LY, Chen JW. A Novel Resolution of Diabetes: C-C Chemokine Motif Ligand 4 Is a Common Target in Different Types of Diabetes by Protecting Pancreatic Islet Cell and Modulating Inflammation. Front Immunol. 2021;12:650626. Published 2021 Apr 23. [CrossRef]
- Meagher C, Arreaza G, Peters A, et al. CCL4 protects from type 1 diabetes by altering islet beta-cell-targeted inflammatory responses. Diabetes. 2007;56(3):809-817. [CrossRef]
- Zeng Z, Lan T, Wei Y, Wei X. CCL5/CCR5 axis in human diseases and related treatments. Genes Dis. 2022;9(1):12-27. [CrossRef]
- Bogdanski P, Pupek-Musialik D, Dytfeld J, et al. Influence of insulin therapy on expression of chemokine receptor CCR5 and selected inflammatory markers in patients with type 2 diabetes mellitus. Int J Clin Pharmacol Ther. 2007;45(10):563-567. [CrossRef]
- Ooms M, Strom A, Strassburger K, Menart B, Leslie RD, Schloot NC. Increased spontaneous CCL2 (MCP-1) and CCL5 (RANTES) secretion in vitro in LADA compared to type 1 diabetes and type 2 diabetes: Action LADA 14. Diabetes Metab Res Rev. 2021;37(7):e3431. [CrossRef]
- Chen J, Guo W, Yin H, Ma L, Li S, Li H. Investigation of the Correlation Between the Polymorphism/Expression Level of RANTES and Its Receptor CCR5 Gene Promoter and Type 2 Diabetes Mellitus. Diabetes Metab Syndr Obes. 2023;16:213-223. Published 2023 Jan 24. [CrossRef]
- Mira E, León B, Barber DF, et al. Statins induce regulatory T cell recruitment via a CCL1 dependent pathway. J Immunol. 2008;181(5):3524-3534. [CrossRef]
- Hotamisligil GS, Erbay E. Nutrient sensing and inflammation in metabolic diseases. Nat Rev Immunol. 2008;8(12):923-934. [CrossRef]
- Jager J, Grémeaux T, Cormont M, Le Marchand-Brustel Y, Tanti JF. Interleukin-1beta-induced insulin resistance in adipocytes through down-regulation of insulin receptor substrate-1 expression. Endocrinology. 2007;148(1):241-251. [CrossRef]
- Kern PA, Ranganathan S, Li C, Wood L, Ranganathan G. Adipose tissue tumor necrosis factor and interleukin-6 expression in human obesity and insulin resistance. Am J Physiol Endocrinol Metab. 2001;280(5):E745-E751. [CrossRef]
- Harakeh S, Kalamegam G, Pushparaj PN, et al. Chemokines and their association with body mass index among healthy Saudis. Saudi J Biol Sci. 2020;27(1):6-11. [CrossRef]
- Hotamisligil GS. Inflammation and metabolic disorders. Nature. 2006;444(7121):860-867. [CrossRef]
- Xu L, Kitade H, Ni Y, Ota T. Roles of Chemokines and Chemokine Receptors in Obesity-Associated Insulin Resistance and Nonalcoholic Fatty Liver Disease. Biomolecules. 2015;5(3):1563-1579. Published 2015 Jul 21. [CrossRef]
- Feghali CA, Wright TM. Cytokines in acute and chronic inflammation. Front Biosci. 1997;2:d12-d26. Published 1997 Jan 1. [CrossRef]
- Purohit S, Sharma A, Hopkins D, et al. Large-Scale Discovery and Validation Studies Demonstrate Significant Reductions in Circulating Levels of IL8, IL-1Ra, MCP-1, and MIP-1β in Patients With Type 1 Diabetes. J Clin Endocrinol Metab. 2015;100(9):E1179-E1187. [CrossRef]
- Harakeh S, Kalamegam G, Pushparaj PN, et al. Chemokines and their association with body mass index among healthy Saudis. Saudi J Biol Sci. 2020;27(1):6-11. [CrossRef]
- Weisberg SP, Hunter D, Huber R, et al. CCR2 modulates inflammatory and metabolic effects of high-fat feeding [published correction appears in J Clin Invest. 2006 May;116(5):1457]. J Clin Invest. 2006;116(1):115-124. [CrossRef]
- Tamura Y, Sugimoto M, Murayama T, et al. Inhibition of CCR2 ameliorates insulin resistance and hepatic steatosis in db/db mice. Arterioscler Thromb Vasc Biol. 2008;28(12):2195-2201. [CrossRef]
- Pham MN, Hawa MI, Roden M, et al. Increased serum concentrations of adhesion molecules but not of chemokines in patients with Type 2 diabetes compared with patients with Type 1 diabetes and latent autoimmune diabetes in adult age: action LADA 5. Diabet Med. 2012;29(4):470-478. [CrossRef]
Figure 1.
Map showing different provinces of Saudi Arabia. The study areas (Bisha and Abha) are encircled in red.
Figure 1.
Map showing different provinces of Saudi Arabia. The study areas (Bisha and Abha) are encircled in red.
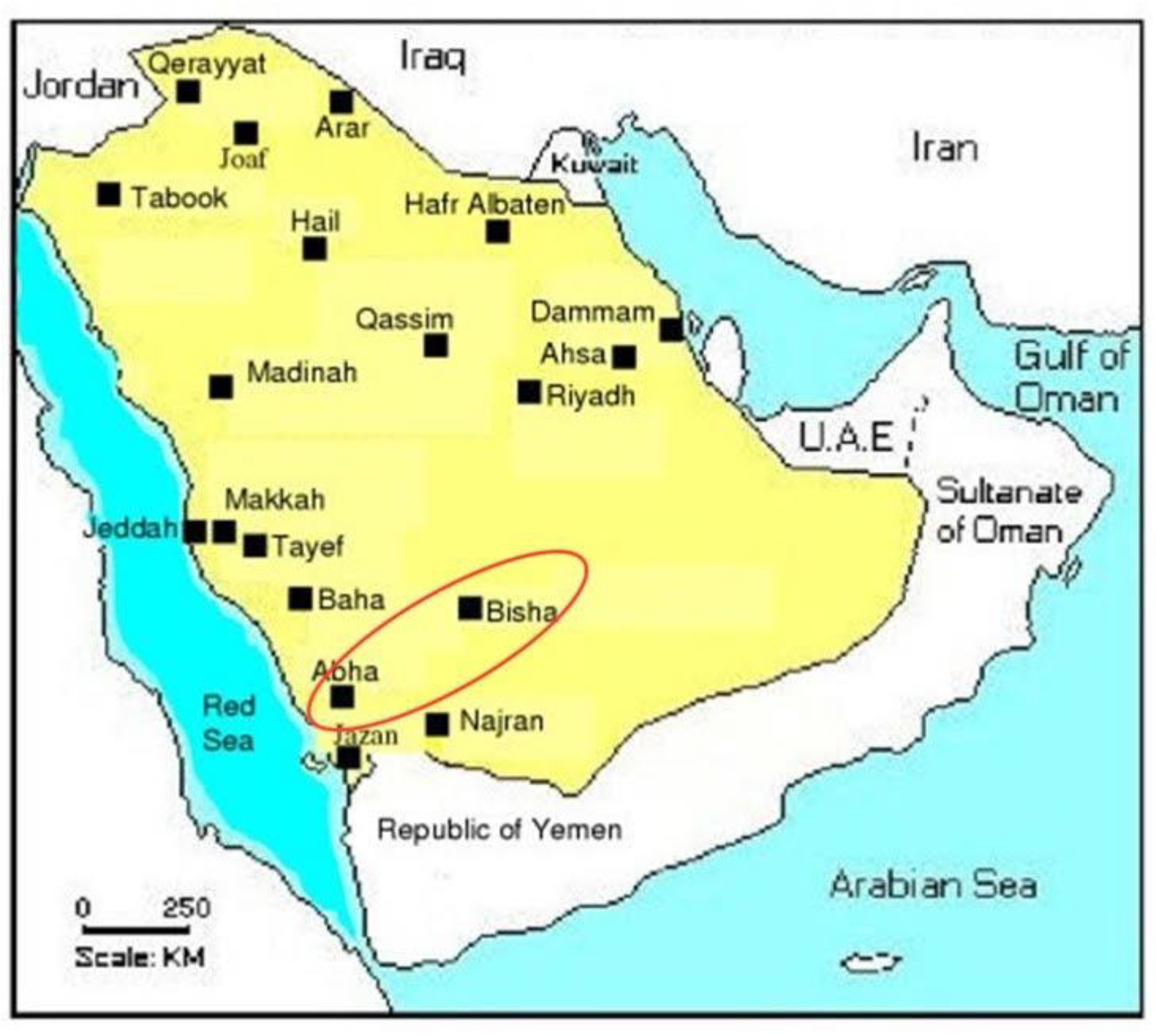
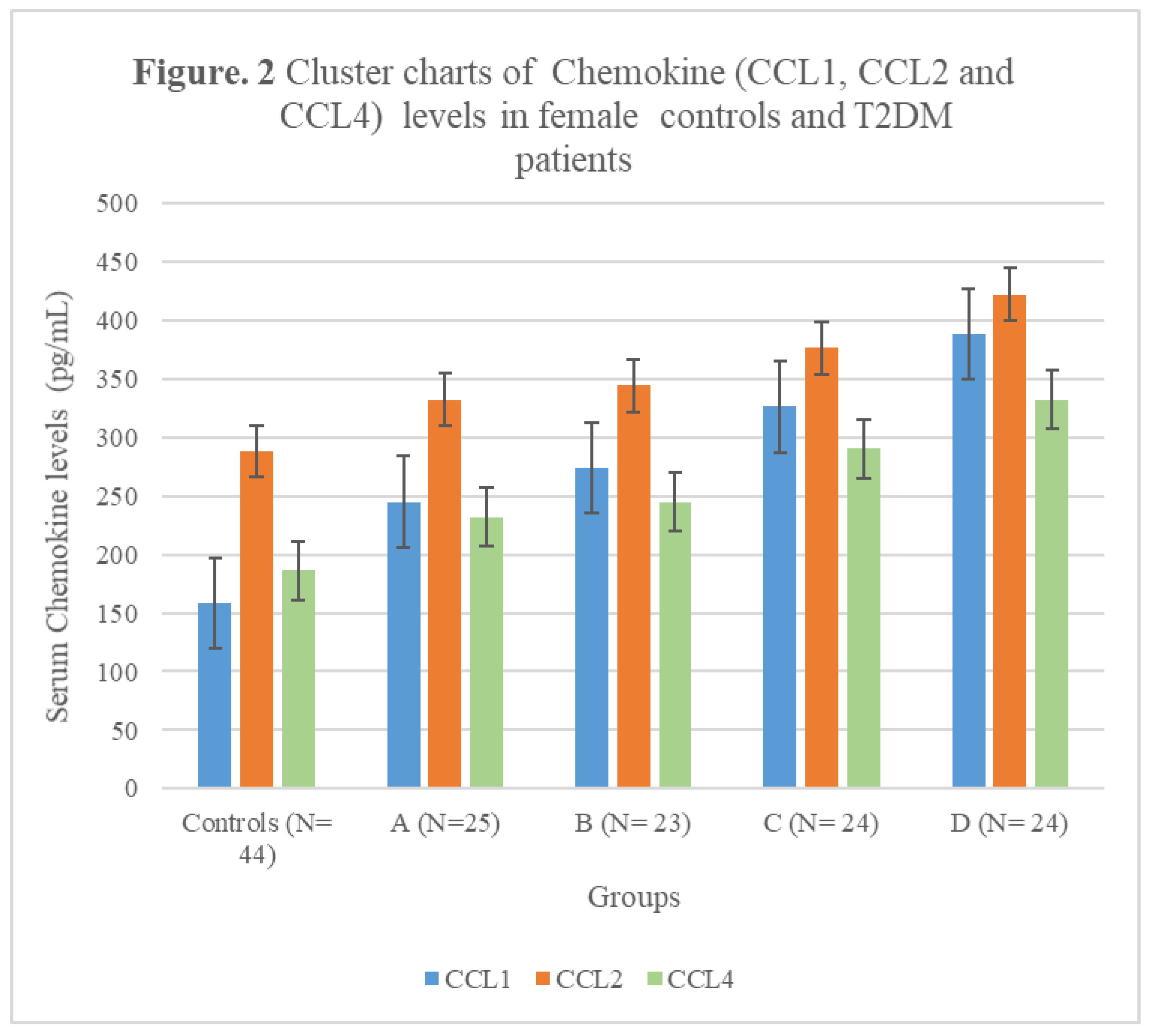
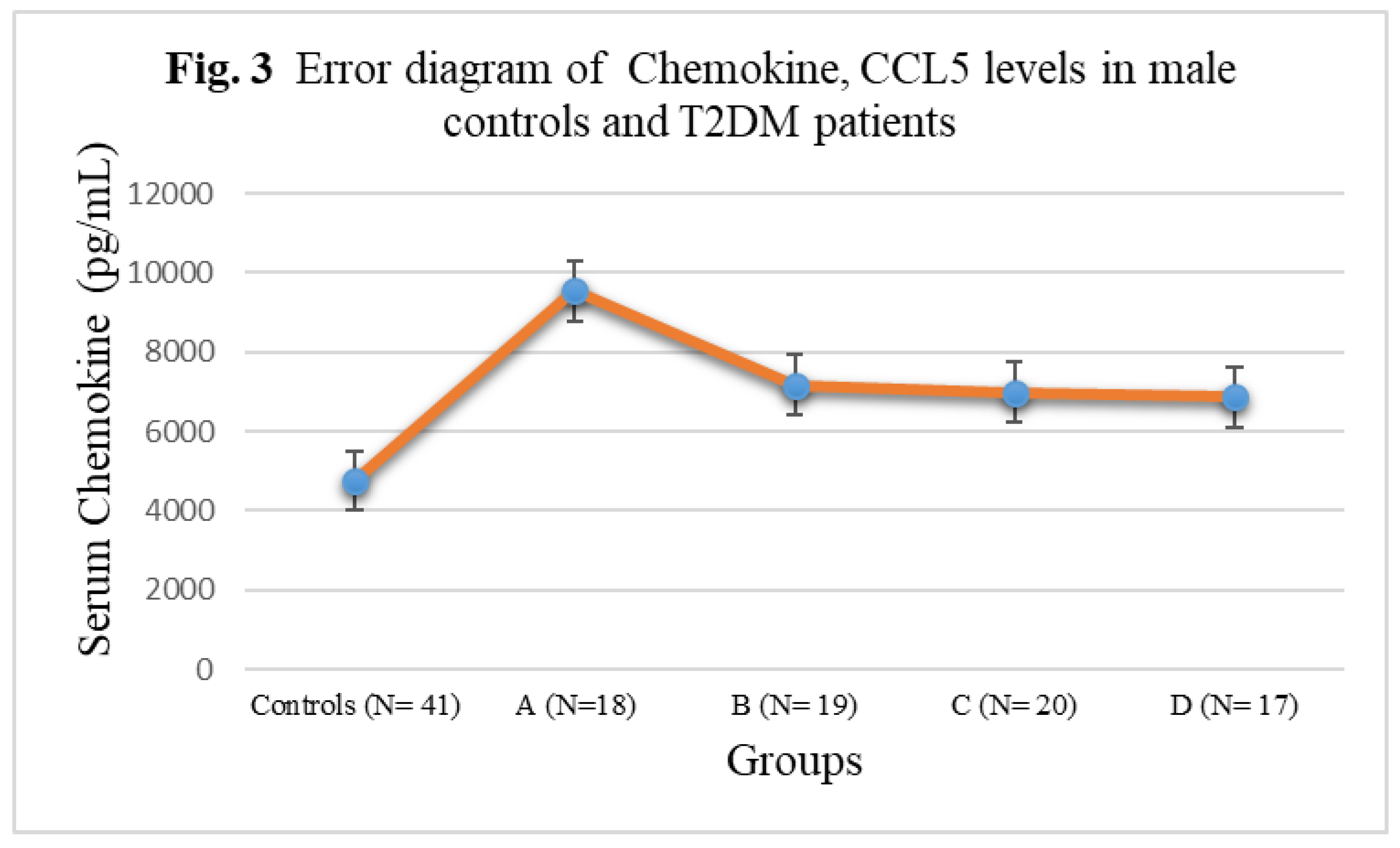
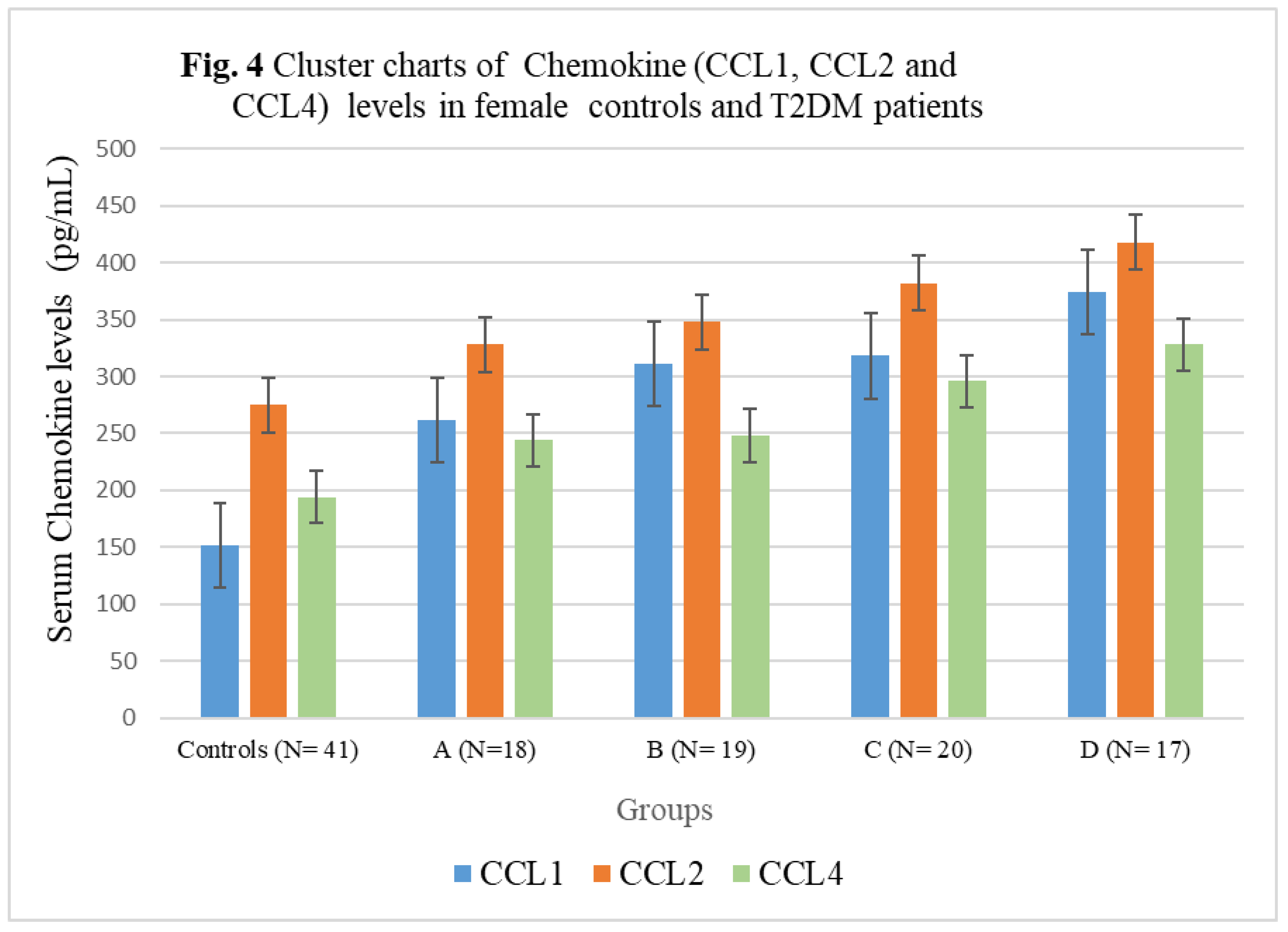
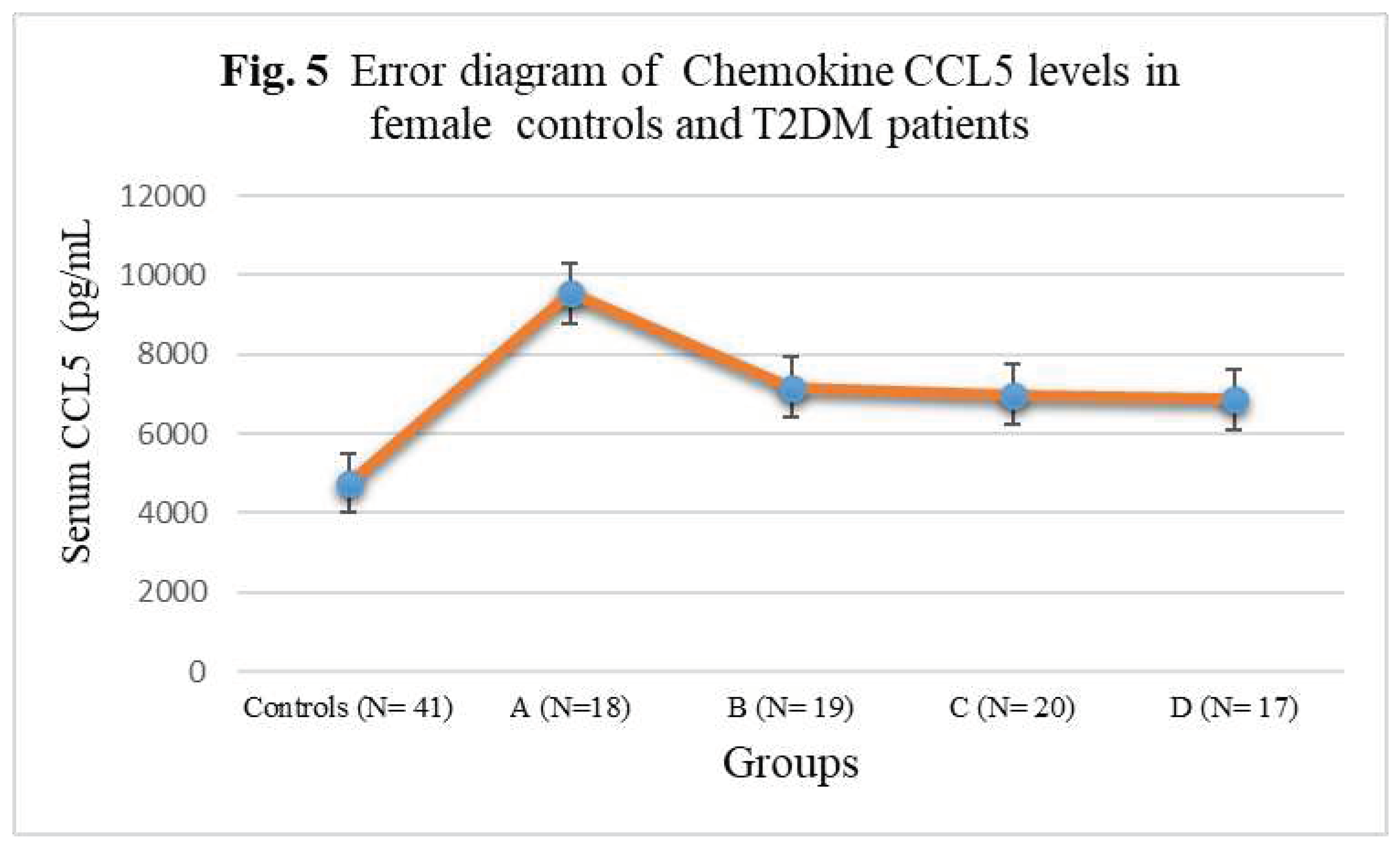

Table 1.
Anthropometric indices and biochemical parameters of T2DM patients and controls (Male group).
Table 1.
Anthropometric indices and biochemical parameters of T2DM patients and controls (Male group).
| Anthropometric and biochemical indices | Controls | Group A | Group B | Group C | Group D |
| N= 44 | N=96 | ||||
| 25 | 23 | 24 | 24 | ||
| Age | 46(28-62) | 43(27-51) | 47(29-55) | 49(30-66) | 47(32-67) |
| WHR | 0.86 (0.84-0.95) |
0.92 (0.84-0.1.05) |
0.94 (0.83-1.06) |
1.07**T (0.97-1.11) |
1.14*S (1.02-1.19) |
| BMI (kg/m2) | 21.78 ± 1.78 | 21.80 ± 2.14 | 27.44 ± 2.29 | 34.94 ± 3.18*T | 47.22± 5.70*WX |
| Fasting Glucose (mg/dL) | 92(78-116) | 115(88-130) | 114(92-138) | 116(92-144) | 124(103-152) |
| HbA1c (g/dL) | 4.9±0.88 | 7.4 ±1.02* | 8.1±1.2* | 8.7±1.48*S | 7.6±0.78* |
| Cholesterol-T (mg/dL) | 186 (135-224) | 204**(154-230) | 214*(148-232) | 215*(142-240) | 226*(158-258) |
| HDL-C (mg/dL) | 53(38- 63) | 46(36—60) | 48(38-56) | 45(33-58) | 44(28-54) |
| LDL-C (mg/dL) | 94±32.20 | 98 (62-131) | 118** (80-136) | 120** (80-152) | 136*w (95-162) |
| TG (mg/dL) | 116(86-132) | 122(96-136) | 146(98-178) | 232*(162-256) | 242*w(162-286) |
Age is presented in years with the range in parentheses. WHR-waist to hip ratio; BMI-body mass index. HbA1c- Glycated hemoglobin; Cholesterol-T-Total cholesterol; HDL–High density lipoprotein; LDL-Low density lipoprotein; TG-Triglycerides. Group A -T2DM patients with normal body weight; Group B–overweight T2DM patients; Group C-T2DM patients with obesity and Group D -T2DM patients with severe obesity. *p<0.001 vs control group; **p< 0.01 vs control group; S p< 0.001 vs group A and B: T p< 0.01 vs group A and B; W p< 0.001 vs controls and group A ; X p< 0.01 vs group C
Table 2.
Anthropometric indices and biochemical parameters of T2DM patients and controls (Female group).
Table 2.
Anthropometric indices and biochemical parameters of T2DM patients and controls (Female group).
| Anthropometric and biochemical indices | Controls | Group A | Group B | Group C | Group D |
| N= 41 | N=74 | ||||
| 18 | 19 | 20 | 17 | ||
| Age | 48(27-64) | 44(26-55) | 47(27-57) | 46(28-62) | 48(30-69) |
| WHR | 0.85 (0.78-0.96) |
0.91 (0.82-0.1.04) |
0.92 (0.84-1.05) |
1.06**T (0.97-1.13) |
1.10*S (1.02-1.22) |
| BMI (kg/m2) | 21.2 ± 1.66 | 21.41 ± 2.14 | 28.22 ± 2.26 | 33.88± 3.20*T | 46.48± 5.20*WX |
| Fasting Glucose(mg/dL) | 96(82-114 | 118**(90-141) | 114**(92-138) | 116**(92-144) | 124*(103-152) |
| HbA1c (g/dL) | 4.5±0.43 | 7.8±1.02* | 8.1±1.2* | 8.5±1.48*S | 8.4±0.98* |
| Cholesterol-T(mg/dL) | 168 (132-224) | 196**(145-227) | 204**(144-238) | 215**(155-235) | 228**(162-262) |
| HDL-C (mg/dL) | 56(41- 66) | 54 (39—62) | 52(40-63) | 46(35-64) | 44(35-62) |
| LDL-C (mg/dL) | 96±28.22 | 92±28.28 | 111**±33.08 | 108**±30.30 | 132*±32.12 |
| TG (mg/dL) | 96(88-124) | 126**(94-168) | 142**(88-222) | 152**(99- 223) | 195*wx(98-245) |
Age is presented in years with the range in parentheses. WHR-waist to hip ratio; BMI-body mass index. HbA1c- Glycated hemoglobin; Cholesterol-T-Total cholesterol; HDL –High density lipoprotein; LDL-Low density lipoprotein; TG-Triglycerides Group A -T2DM patients with normal body weight; Group B–overweight T2DM patients; Group C-T2DM patients with obesity and Group D -T2DM patients with severe obesity. *p<0.001 vs control group; **p< 0.01 vs control group; S p< 0.001 vs group A and B; T p< 0.01 vs group A and B; W p< 0.001 vs controls and group A ; X p< 0.01 vs group C
Table 3.
The serum levels of chemokines CCL1, CCL2, CCL4, and CCL5 in male T2DM patients and control subjects.
Table 3.
The serum levels of chemokines CCL1, CCL2, CCL4, and CCL5 in male T2DM patients and control subjects.
| Subject Groups | CCL1 (pg/mL) | CCL2 (pg/mL) | CCL4 (pg/mL) | CCL5 (pg/mL) |
|---|---|---|---|---|
| Controls (N= 44) | 158± 21.02 | 288 ± 33.12 | 186± 22.56 | 4880± 348.98 |
| A (N=25) | 245± 27.46** | 332 ± 35.76*** | 232± 25.44*** | 9620± 523.22* |
| B (N= 23) | 274± 23.12** | 344 ± 35.87*** | 245± 25.72*** | 7266± 387.55**N |
| C (N= 24) | 326± 35.44*N | 376 ± 36.92*N | 290± 24.14*O | 7056± 382.34**N |
| D (N= 24) | 388± 37.12*LM | 422 ± 44.25*LM | 332± 29.90*LM | 6892± 377.16***NQ |
Group A -T2DM patients with normal body weight; Group B–overweight T2DM patients; Group C-T2DM patients with obesity and Group D -T2DM patients with severe obesity. *p<0.001 vs control group; ** p<0.01 vs control group; *** p<0.05 vs control group; L p< 0.04 vs Group C; p<0.01 compared to groups A and B; N p< 0.01 vs groups A, O p< 0.04 compared to groups A and B; Q p<0.01 compared to group A.
Table 4.
The serum levels of chemokines CCL1, CCL2, CCL4, and CCL5 in female T2DM patients and control subjects.
Table 4.
The serum levels of chemokines CCL1, CCL2, CCL4, and CCL5 in female T2DM patients and control subjects.
| Subject Groups | CCL1 (pg/mL) | CCL2 (pg/mL) | CCL4 (pg/mL) | CCL5 (pg/mL) |
|---|---|---|---|---|
| Controls (N= 41) | 152± 20.88 | 275 ± 32.14 | 194± 22.54 | 4756± 342.56 |
| A (N=18) | 262± 27.52** | 328± 35.66*** | 244± 25.38*** | 9546± 522.44* |
| B (N= 19) | 311± 25.10** | 348 ± 35.58*** | 248± 25.24*** | 7168± 388.24**N |
| C (N= 20) | 318± 35.08*N | 382± 36.82*N | 296± 26.08*O | 6978± 384.74**N |
| D (N= 17) | 374± 37.04*LM | 418 ± 44.16*LM | 328± 29.88*LM | 6866± 376.12***NQ |
Group A-T2DM patients with normal body weight; Group B–overweight T2DM patients; Group C-T2DM patients with obesity and Group D - 2DM patients with severe obesity. *p<0.001 vs control group; ** p<0.01 vs control group; *** p<0.05 vs control group; L p< 0.04 vs Group C; M p<0.01 compared to groups A and B, N p< 0.01 vs groups A, O p< 0.04 compared to groups A and B; Q p<0.01 compared to group A.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



