Submitted:
16 October 2023
Posted:
18 October 2023
You are already at the latest version
Abstract
Background: As the impacts of diabetes-induced reproductive damage are now evident in young people, we are now in an urgent need to devise new ways to protect and enhance the reproductive health of diabetic people. The purpose of this study was to assess the protective impact of enalapril (an ACE inhibitor) and paricalcitol (a vitamin D analogue) alone and in combination, on streptozotocin (STZ) diabetes-induced testicular dysfunction in rats.
Material and methods: This study was carried on 50 male Sprague-Dawley rats; 10 normal rats were allocated as non-diabetic control group. 40 rats developed diabetes after receiving a single dose of STZ, then the diabetic rats were divided into four groups of equivalent number assigned as diabetic control, enalapril treated, paricalcitol treated, in addition to combined enalapril and paricalcitol treated groups. The effects of mono and combined therapy with paricalcitol and enalapril on testicular functions, sperm activity, glycemic state oxidative stress and inflammatory parameters as well as histopathological examination were assessed when compared to the normal and diabetic control rats.
Results: As a result of diabetes induction, epididymal sperm count, sperm motility, serum levels of testosterone, follicle stimulating hormone (FSH) as well as luteinizing hormone (LH) and the antioxidant enzyme activities were significantly decreased, while abnormal sperm (%), insulin resistance, nitric oxide (NO), malondialdehyde (MDA), interleukin-6 (IL-6) as well as tumor necrosis factor-α (TNF-α) were significantly increased, along with sever distortion of testicular structure. Interestingly, treatment with paricalcitol and enalapril either alone or in combination significantly improved the sperm parameters, increased antioxidant enzyme activities in addition to serum levels of testosterone, FSH and LH, reduced insulin resistance, IL-6 and TNF-α levels and finally ameliorated the diabetes-induced testicular oxidative stress and histopathological damage with somewhat superior effect for paricalcitol monotherapy and combined therapy with both drugs than monotherapy with enalapril alone.
Conclusion: Monotherapy with paricalcitol and its combination therapy with enalapril has a somewhat superior effect in improving the diabetes-induced testicular dysfunction (most probably as a result of their hypoglycemic, antioxidant, anti-inflammatory and anti-apoptotic properties), than monotherapy with enalapril alone in male rats, recommending a synergistic impact of both drugs.
Keywords:
diabetes
; oxidative stress
; enalapril
; paricalcitol
; testicular dysfunction
Introduction
Among the most common chronic diseases globally is diabetes mellitus (DM), which is defined by hyperglycemia caused by inadequate insulin production and/or reduced insulin action [1]. Hyperglycaemia, substantially disturb the balance among the production of reactive oxygen species (ROS) and the power of anti-oxidant defenses to eliminate or decompose them (oxidant/antioxidant imbalance), triggering oxidative stress, which in turn affects the normal physiological functions of most body organs including the brain, testis, heart, kidneys, and retina [2]. Compared to healthy individuals, diabetic men generally suffers many sexual problems including impotence, erectile dysfunction (ED), ejaculation disorders, and inhibited sexual desire [3], in addition to reduced testicular functions represented by decreased testosterone levels, seminal fluid volume, sperm count and motility [4].
Antioxidants either endogenous such as reduced glutathione (GSH), catalase, superoxide dismutase (SOD), glutathione peroxidase (GPx), as well as reductase or exogenous like antioxidant vitamins (A, C, and E), can scavenge free radicals or promote their decomposition, thus reducing oxidative stress [5]. Recently, vitamin D and the ACE inhibitors have been reported to be efficient ROS scavengers, and powerful antioxidant agents [6,7]. As the angiotensin II (Ang II) has been shown to induce endothelial dysfunction resulting in increased production of potent oxidants such as peroxynitrite (PN) [8], therefore, ACE inhibitors, (one of the most widely used antihypertensive medications), not only prevent the formation of Ang II, but also effectively scavenge this potent oxidants, thus protecting against cellular damage [9]. However, vitamin D is essential not just for calcium metabolism but additionally for a wide variety of other non-calcemic impacts, one of which is its antioxidant effect [10]. Deficiencies in vitamin D have been linked to multiple chronic diseases, such as cardiovascular problems [11], chronic kidney diseases [12], type 1 [13] and type 2 diabetes [14], suggesting its crucial role in preventing their progression by modulating oxidative stress [10].
Numerous studies have demonstrated the protective and ameliorative impacts of both vitamin D analogues and ACE inhibitors against the diabetes-induced oxidative stress in many tissues like the heart [6], kidney [7], and lung [15]. It would be interesting to study their effects on reducing oxidative stress in other tissues.
As the impacts of diabetes-induced reproductive damage are now evident in young people [16], we are now in an urgent need to devise new ways to protect and improve the reproductive health of diabetic people. Hence, the purpose of the study was to compare the impact of monotherapy with an ACE inhibitor (enalapril) in addition to a vitamin D analogue (paricalcitol), to the combined therapy with both drugs on STZ diabetes-induced testicular damage, in male albino rats.
Material and methods
Animals and experimental design:
50 local-strain male albino adult rats with a weight between 140 and 160 g were utilized. The rats were housed in cages measuring 20×30×50 cm (5 rats each cage), kept on a regular light/dark cycle, at room temperature, and allowed access to commercial rat pellets and water at all times. They were given two weeks to acclimate before any experiments were performed.
Induction of diabetes:
Twelve hours after fasting freshly prepared STZ (Sigma Aldrich Co., USA) was injected intraperitoneally (i.p) was administered at 60 mg/kg [17]. Before being injected, the STZ was dissolved within a 0.1 M citrate buffer (pH 4.5). 3 days afterwards the initial tail vein blood sample was taken, a commercial glucometer (ACCU CHEK, Rhoche Diagnostics, Germany) was used to measure fasting blood glucose levels. Diabetic rats were defined as those with a blood glucose level more than 300 mg/dl. The participants’ blood glucose levels were measured on a weekly basis throughout the study. The National Institutes of Health’s recommendations for the treatment of experimental animals were strictly adhered to in all cases (NIH Publication No. 85023, revised, 1996)
Grouping and drug intervention:
3 weeks following induction of diabetes, rats were randomly divided into five groups (n=10), and were treated as follows:
Group 1 (Non-diabetic control group): rats received a vehicle (100 µL of propylene glycerol [PPG], i.p.) three times per week for 12 wk.
Group 2 (Diabetic vehicle-treated group): rats were given vehicle only (100 µL of PPG, i.p.), three times per week for 12 wk.
Group 3 (Diabetic enalapril-treated group): rats received enalapril in their drinking water (25 mg enalapril/L), for 12 wk. [18].
Group 4 (Diabetic paricalcitol-treated group): rats received paricalcitol (0.8 µg/Kg dissolved in the equivalent volume of the vehicle, i.p.), three times per week for 12 wk. [18].
Group 5 (Diabetic enalapril as well as paricalcitol-treated group): rats received paricalcitol and enalapril in the same doses described earlier [18].
Blood collection and biochemical assessment:
Following 24 hours, the rats were weighed, received anesthesia using thiopental sodium (30 mg/Kg i.p. ), and had blood samples from the retro-orbital plexus of veins and then centrifuged at 3000 rpm for 20 minutes to separate serum, that was then stored at 20oC until utilized for measuring serum glucose [19] as well as serum insulin [20]. Insulin resistance was evaluated according to homeostasis model assessment-insulin resistance (HOMA-IR) = [FBG (mmol/L) × insulin (U/mL)]/22.5[21].
Moreover, serum levels of testosterone were measured utilizing ELIZA kits (Microlisa AMGENIX Int, Inc. USA) based on recommendation of the manufacturer [22], serum FSH as well as LH utilizing ELIZA kits obtained from DGR Diagnostic, Marburg, Germany based on manufacturer’s protocol.
Preparation of testicular tissue and samples
After sterilizing and weighing the testicles, they were surgically removed. The left testis was homogenized after being washed with cold saline. The testicular activity was determined by centrifuging the homogenate at 3000 rpm over 20 minutes.
Assessment of testicular oxidative stress and inflammatory parameters
Testicular reduced glutathione (GSH) [23], super oxide dismutase (SOD) [24], glutathione peroxidase (GPx) [25], catalase (CAT) [26] activities, and lipid peroxidation represented by nitric oxide (NO) (determined as the stable NO product nitrite and nitrate) and malondialdehyde (MDA) levels [27] were determined. Tissue interleukin-6 (IL-6) and tumor necrosis factor-α (TNF-α) were measured utilizing ultrasensitive rat ELIZA kits (Sigma Aldrich Co. USA) based on manufacturer’s recommendations [28].
Assessment of sperm characteristics
After killing the animals the cauda epididymis was removed and placed in a petri dish containing 3 ml of Hank’s balanced salt solution (HBSS) at room temperature. To release the sperm, the epididymis was cut into small pieces. After collecting the sperm suspension, it was centrifuged at 1000 rpm for 5 minutes. The sperm count in the epididymis was determined by collecting 1 ml of the supernatant as well as counting the sperm utilizing a Neubaur’s hemocytometer (Lauda-Ko nigshof, Germany) [29]. Motility was determined by placing a single drop of sperm suspension onto a glass slide and covering it with a cover slip. Following 2–4 minutes of removing sperm from the epididymis, 10 microscopic fields were examined at 400 magnification to estimate the proportion of motile sperm [30].
For determination of the morphological sperm abnormalities, at night, smears were made on clean, degreased slides. The slides were then evaluated for morphological anomalies such as bicephlic, coild, or aberrant tails at 400 magnifications after being stained with Eosin -Y/ 5% nigrosine [31].
Histopathological examination
Right testes were collected from all experimental groups at the final stage of the study, washed, and fixed in Bouin’s solution so that they could be processed into paraffin sections (5 m in thickness). The following was used as the staining paper for the sections:
Immunohistochemical studies
Activated caspase-3 (check for cellular apoptosis) was identified using a rabbit polyclonal antibody (1:1000 dilution, BD Biosciences, Le Pont-de-Claix, France) that recognizes the big fragment (17kDa) of the active protein. A standard avidin-biotin peroxidase complex system was used for detection of caspase-3. Sections were counterstained with hematoxylin [33]
Statistical analysis:
The data were represented as a mean SD. SPSS (SPSS Inc., Chicago, IL, USA) version 18 for Windows was used for all statistical analyses. Tukey’s multiple comparison test was utilized after a one-way analysis of variance (ANOVA) was performed to determine statistical significance among the groups. The level of statistical significance was set at P<0.05.
Results
Effect of different treatments on body weight and testicular weight in studied groups:
The result of the current study showed significant decline in the final body weight and testicular weight in the diabetic vehicle treated group when compared to the normal control group (P < 0.05). However, treatment with enalapril or paricalcitol induced significant improvement in both parameters in comparison with diabetic vehicle treated group. The most prominent improvement in body weight as well as testicular weight was recorded in the rats treated with both drugs compared to the monotherapy groups (Table 1).
Impact of different treatments on sperm parameters in studied groups:
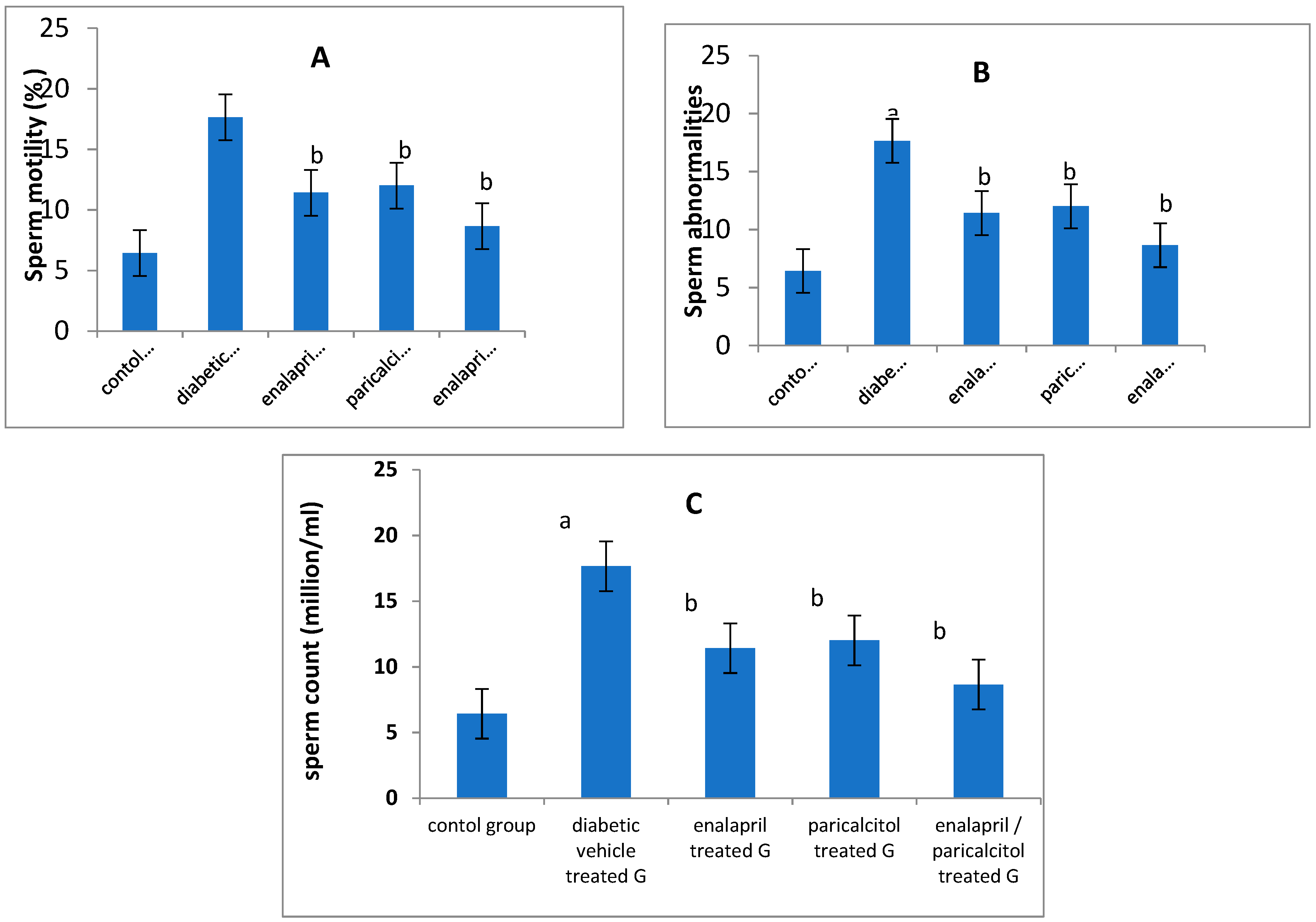
When Compared to the non-diabetic control group, epididymal sperm count as well as sperm motility were significantly reduced whereas abnormal sperms were significantly elevated in diabetic vehicle treated group (P < 0.05). treating diabetic rats with enalapril and/or paricalcitol resulted in significant improvement in the sperm motility as well as sperm count with significant declinein the abnormal forms in comparison with diabetic vehicle treated rats. Paricalcitol/enalapril combination made significant enhancement in these parameters when compared administration of either drug alone (Table 1 and Figure 2).

Table 1.
Impact of different treatment on body & testicular weight and sperm parameters in STZ-induced diabetic rats.
Table 1.
Impact of different treatment on body & testicular weight and sperm parameters in STZ-induced diabetic rats.
| Groups Parameters |
Non diabetic Controls | Diabetic groups | p-value | |||
|---|---|---|---|---|---|---|
| Vehicle treated | Enalapril treated | Paricalcitol treated | Enalapril + Paricalcitol treated | |||
| Body weight (gm) | 230.2 ± 17.4 | 120.5 ± 15.4a | 170.3 ± 12.2b | 173.4 ± 14.4b | 205.7 ± 14.3b | < 0.05 |
| Testicular weight (gm) | 1.54 ± 0.02 | 0.78 ± 0.04 a | 1.15 ± 0.01b | 1.12 ± 0.05b | 1.43 ± 0.04b | < 0.05 |
| Sperm count (mill/ml) | 52.23 ± 6.5 | 25.2 ± 5.85a | 35.33 ± 3.21b | 36.11 ± 4.96b | 45.75 ± 5.22b | < 0.05 |
| Sperm motility (%) | 65.3 ± 5.32 | 35.4 ± 4.76a | 47.45 ± 5.11b | 48.32 ± 4.89b | 58.45 ± 6.39b | < 0.05 |
| Abnormal sperms (%) | 6.43 ± 0.97 | 17.6 ± 1.85a | 11.42 ± 0.89b | 12.01 ± 0.76b | 8.65 ± 0.56b | < 0.05 |
Data are expressed as mean ± SD, n = 10 rats; P < 0.05 was considered significant. a Significantly different from non-diabetic control group; bSignificantly different from diabetic vehicle treated group.
Figure 1.
Impact of treatment with enalapril and paricalcitol on body weight (A), and testicular weight (B). aSignificantly different from non-diabetic control group; bSignificantly different from diabetic vehicle treated group.
Figure 1.
Impact of treatment with enalapril and paricalcitol on body weight (A), and testicular weight (B). aSignificantly different from non-diabetic control group; bSignificantly different from diabetic vehicle treated group.
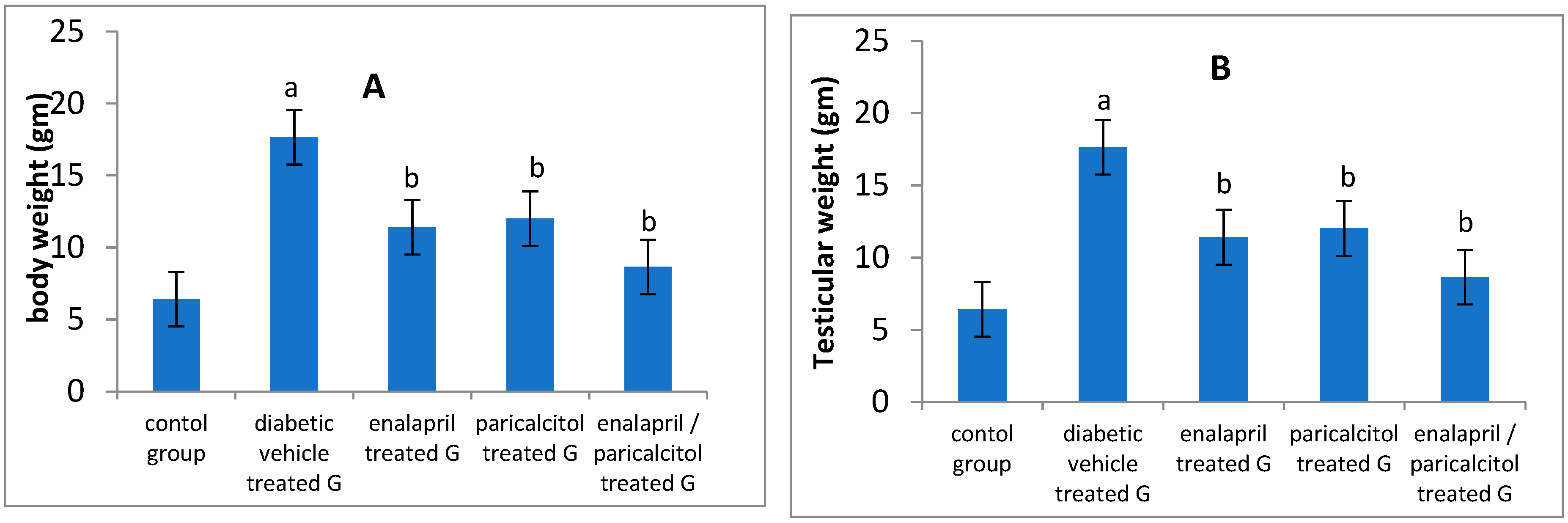
Figure 2.
Impact of treatment with enalapril and paricalcitol on sperm motility (A), sperm abnormalities (B), and sperm count (C). aSignificantly different from non-diabetic control group; bSignificantly different from diabetic vehicle treated group.
Figure 2.
Impact of treatment with enalapril and paricalcitol on sperm motility (A), sperm abnormalities (B), and sperm count (C). aSignificantly different from non-diabetic control group; bSignificantly different from diabetic vehicle treated group.
Impact of different treatments on testosterone, FSH and LH in studied groups:
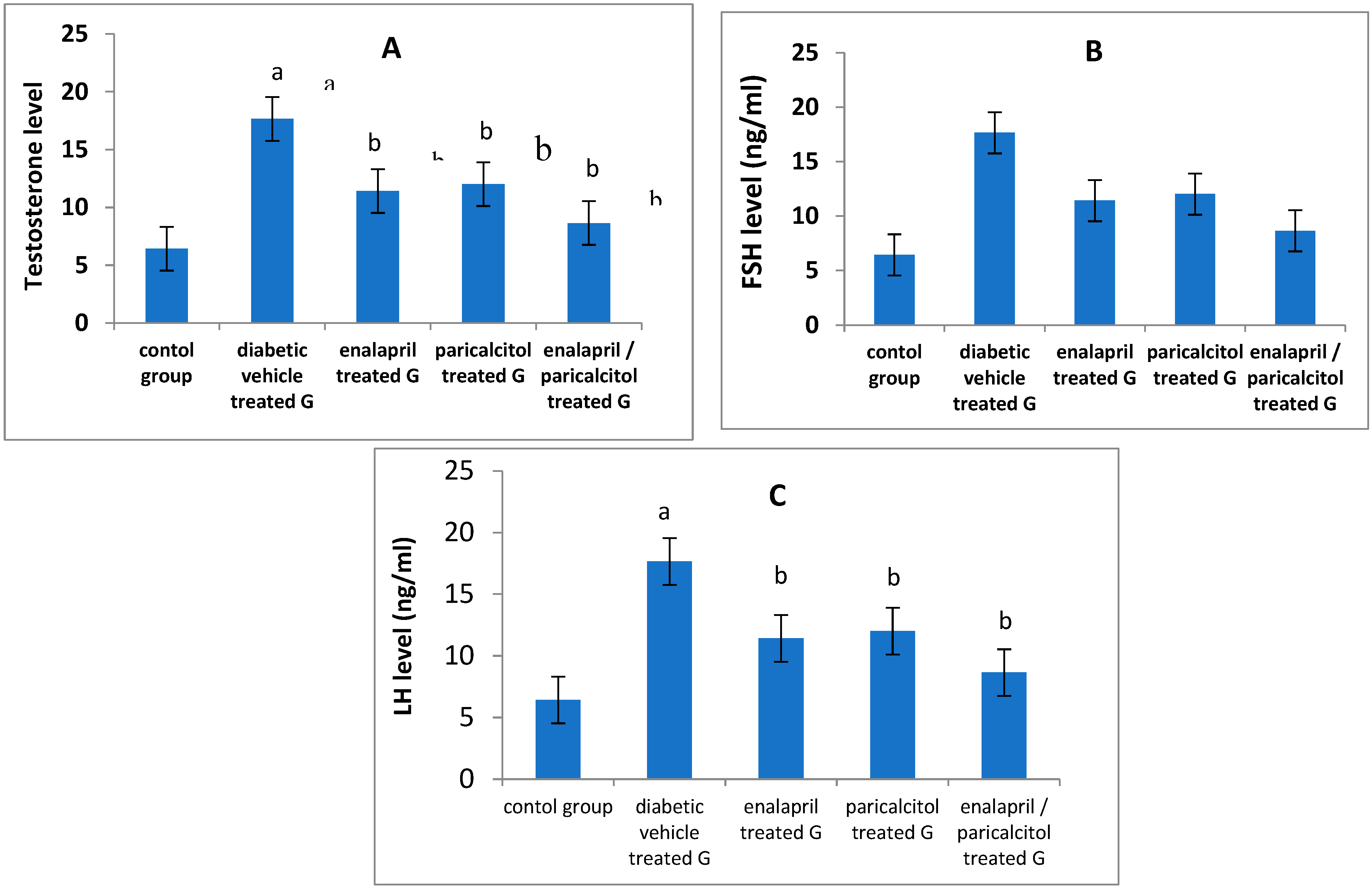
Serum levels of testosterone, FSH as well as LH were significantly reduced in vehicle treated diabetic group when compared to the normal control group (P < 0.05). Administration of paricalcitol and /or enalapril to the diabetic rats led to significant improvement (P < 0.05) in the levels of these hormones as compared to the diabetic untreated rats. The increase in the aforementioned hormones was significantly more prominent (P < 0.05) with the combined therapy compared to the individual therapy with either drug (Table 2, Figure 3).
Table 2.
Effect of different treatment on testosterone, LH and FSH in STZ-induced diabetic rats.
| Groups Parameters |
Non-diabetic Controls | Diabetic groups | p-value | |||
|---|---|---|---|---|---|---|
| Vehicle treated | Enalapril treated | Paricalcitol treated | Enalapril + Paricalcitol treated | |||
| Testosterone (ng/ml) | 4.71 ± 0.24 | 1.9 4 ± 0.13a | 3.55 ± 0.34b | 3.71 ± 0.11b | 4.4 ± 0.23b | < 0.05 |
| FSH (ng/ml) | 5.61 ± 0.98 | 2.75 ± 0.37a | 3.97 ± 0.57 b | 4. 02 ± 0.45b | 4.99 ± 0.31b | < 0.05 |
| LH (ng / ml) | 4.32 ± 0.45 | 1.97 ± 0.36a | 3.41 ± 0.54b | 3.56 ± 0.34b | 4.1 ± 0.65b | < 0.05 |
Data are expressed as mean ± SD, n = 10 rats; P < 0.05 was considered significant. FSH, Follicle-Stimulating Hormone; LH, Luteinizing Hormone; aSignificantly different from non-diabetic control group; bSignificantly different from diabetic vehicle treated group.
Figure 3.
Effect of treatment with enalapril and paricalcitol on testosterone (A), FSH (B), and LH (C) levels. aSignificantly different from non-diabetic control group; bSignificantly different from diabetic vehicle treated group.
Figure 3.
Effect of treatment with enalapril and paricalcitol on testosterone (A), FSH (B), and LH (C) levels. aSignificantly different from non-diabetic control group; bSignificantly different from diabetic vehicle treated group.
Effect of different treatments on glycemic status and inflammatory parameters:
Table 3 and Figure 4 reveal that when compared to normal rats, FBG and PPG levels were significantly (P<0.01) higher in the diabetic control (vehicle treated) rats. In addition, both enalapril as well as paricalcitol treatment alone and the combination treatment significantly (P<0.01) decreased FBG and PPG levels in comparison with that in diabetic vehicle treated rats. The hypoglycemic impact of paricalcitol monotherapy as well as the combined therapy with both medicines was superior to that of enalapril monotherapy, as measured by fasting blood glucose (FBG) and postprandial plasma glucose (PPG), respectively (P > 0.05).
On the other hand, the diabetic control rats had significantly (P < 0.05) lower insulin levels in comparison with the normal rats. while, treatment with enalapril and/or paricalcitol significantly (P < 0.05) elevated the insulin level compared to that of diabetic control rats, with no significant (P > 0.05) difference among the individual or the combined treatment with both drugs (Table 3). Regarding the HOMA-IR, rats in the diabetic control, enalapril treated and paricalcitol treated groups revealed significant (P < 0.01) higher levels of HOMA-IR compared to normal rats. while, combined treatment with enalapril and paricalcitol showed significant (P < 0.05) decline in HOMA-IR compared to the diabetic control and the monotherapy groups, suggesting the superior effect of the combined treatment in reducing the insulin resistance than the monotherapy with either drug (Table 3 & Figure 4).
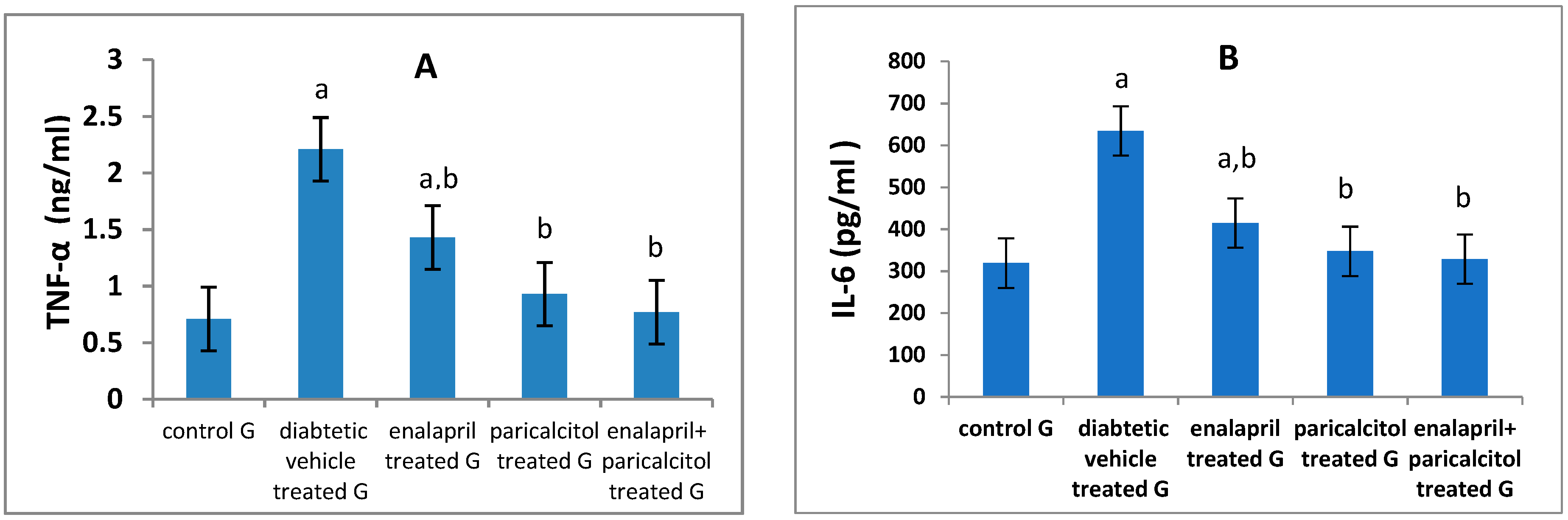
Regarding the inflammatory parameters, Table 3 & Figure 5 showed a significant (p < 0.01) increase in the levels of IL-6 and TNF-α in diabetic control rats when compared to the normal rats. Interestingly, Paricalcitol therapy, either alone or in conjunction with enalapril, nearly normalized their levels, reflecting a stronger anti-inflammatory effect for treatment with both drugs together or the individual therapy with paricalcitol alone than enalapril.
Table 3.
Effect of treatment on glycemic state and inflammatory parameters in STZ-induced diabetic rats.
Table 3.
Effect of treatment on glycemic state and inflammatory parameters in STZ-induced diabetic rats.
| Groups Parameters |
Non-diabetic Controls | Diabetic groups | p-value | |||
|---|---|---|---|---|---|---|
| Vehicle treated | Enalapril treated | Paricalcitol treated | Enalapril + Paricalcitol treated |
|||
| FBG (mg/dl) | 67.5 ± 11.3 | 188.02 ± 9.3a | 169.22 ± 4.71a | 136.19 ± 5.37a,b | 121.15 ± 3.54a,b | P < 0.01 |
| PPG (mg/dl) | 97.11 ± 14.3 | 241.26 ± 7.6a | 221.32 ± 4.51a | 201.31 ± 0.65a,b | 179.69 ± 4.14a,b,c | P < 0.01 |
| Insulin (ng/ml) | 2.96 ± 0.25 | 0.92 ± 0.58a | 1.86 ± 2.42b | 1.97 ± 3.04b | 2.148 ± 3.34b | P < 0.05 |
| HOMA-IR | 1.85 ± 0.16 | 4.93 ± 1.58a | 4.11 ± 1.45a | 3.76 ± 4.33a | 2.11 ± 1.51b,c,d | P < 0.05 |
| IL-6 (pg/ml) | 319.1 ± 9.07 | 634.7 ± 24.5a | 414.9 ± 10.9a.b | 347.35 ± 31.2b | 328.5 ± 13.8b | P < 0.01 |
| TNF-α (ng/ml) | 0.71 ± 0.16 | 2.21 ± 0.03a | 1.43 ± 0.19a.b | 0.93 ± 0.19b | 0.77 ± 0. 9b | P < 0.01 |
Data are expressed as mean ± SD, n = 10 rats; P < 0.05 was considered significant. FBG, fasting blood glucose; PPG, postprandial glucose; HOMA-IR: homeostasis model assessment of insulin resistance; IL-6, interleukin-6; TNF-α, tumor necrosis factor-α; aSignificantly different from non-diabetic control group; bSignificantly different from diabetic vehicle treated group; cSignificantly different from diabetic enalapril treated group; dSignificantly different from diabetic paricalcitol treated group.
Figure 4.
Effect of treatment with enalapril and paricalcitol on FBG, fasting blood glucose (A); PPG, postprandial glucose (B); insulin level (C), and HOMA-IR, homeostasis model assessment of insulin resistance (D). aSignificantly different from non-diabetic control group; bSignificantly different from diabetic vehicle treated group; cSignificantly different from diabetic enalapril treated group; dSignificantly different from diabetic paricalcitol treated group.
Figure 4.
Effect of treatment with enalapril and paricalcitol on FBG, fasting blood glucose (A); PPG, postprandial glucose (B); insulin level (C), and HOMA-IR, homeostasis model assessment of insulin resistance (D). aSignificantly different from non-diabetic control group; bSignificantly different from diabetic vehicle treated group; cSignificantly different from diabetic enalapril treated group; dSignificantly different from diabetic paricalcitol treated group.
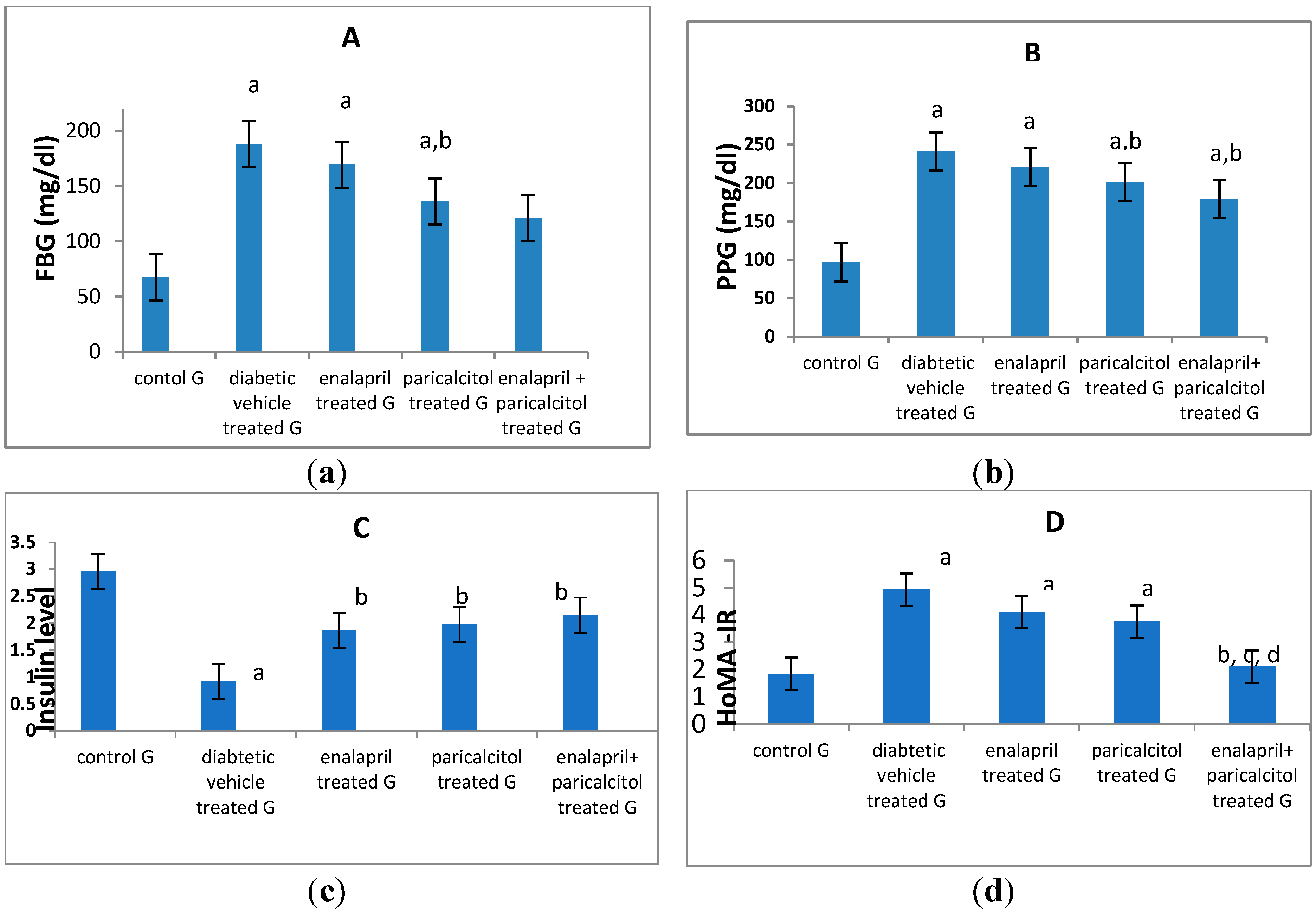
Figure 5.
Effect of treatment with paricalcitol and enalapril on TNF-α, tumor necrosis factor-α (A); and IL-6, interleukin-6 (B). aSignificantly different from non-diabetic control group; bSignificantly different from diabetic vehicle treated group.
Figure 5.
Effect of treatment with paricalcitol and enalapril on TNF-α, tumor necrosis factor-α (A); and IL-6, interleukin-6 (B). aSignificantly different from non-diabetic control group; bSignificantly different from diabetic vehicle treated group.
Impact of different treatments on testicular oxidative stress parameters:
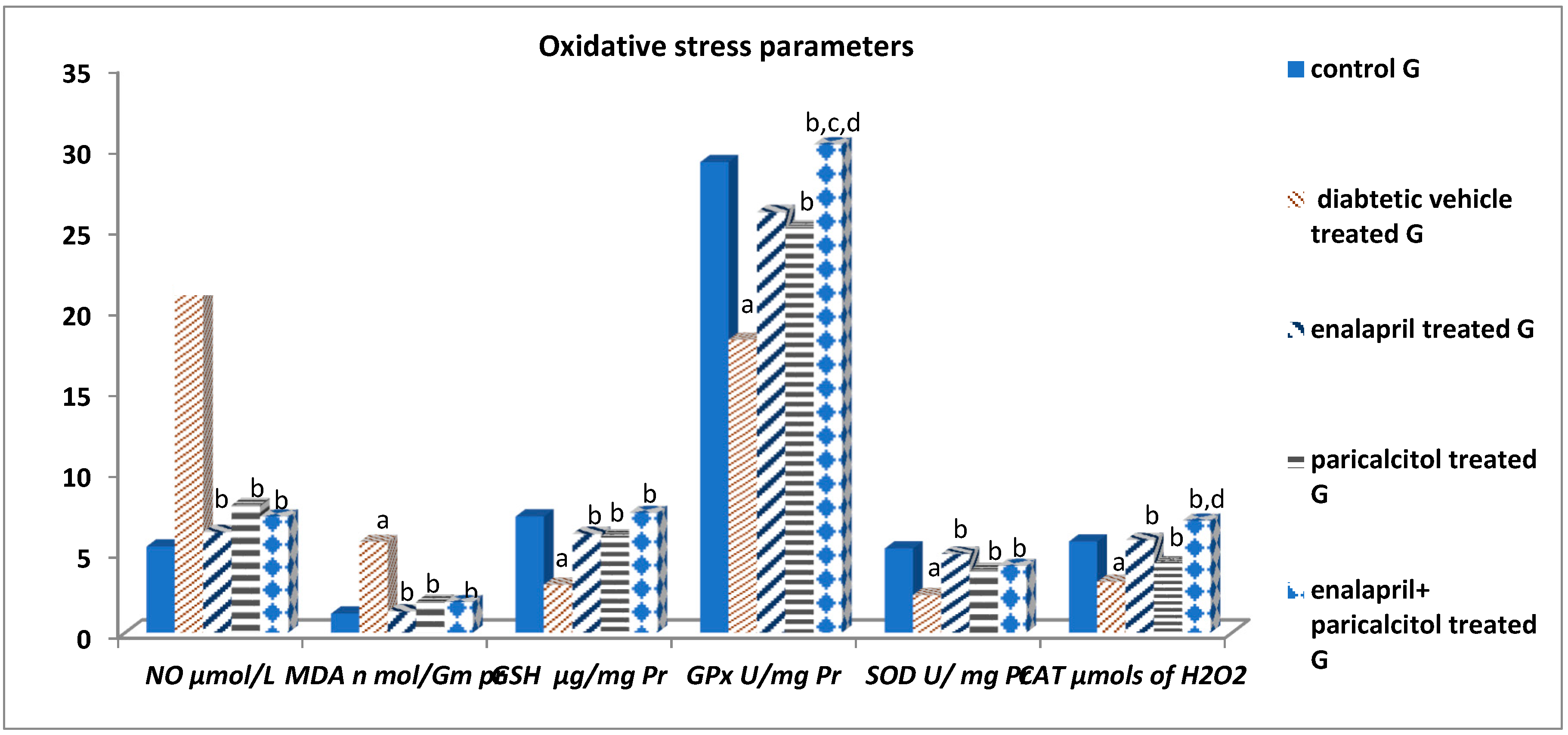
Table 4 and Figure 6 reveal that the NO and MDA levels in the diabetic control rats were statistically significant (p<0.01) higher than in the normal control rats. When compared to diabetic control rats, nevertheless, treatment using enalapril as well as paricalcitol significantly (p<0.01) decreased their levels. Regarding the antioxidant parameters, Table 4 also shows that, the diabetic control rats had significantly (p ˂ 0.01) lower GSH, GPx, SOD and CAT activities in comparison with the non-diabetic control rats, while such impacts were significantly (p ˂ 0.01) ameliorated by treatment with either enalapril and/or paricalcitol, with no significant (P > 0.05) difference between the monotherapy and the combined therapy with both drugs, except for the activity of GPx, which was significantly increased (p ˂ 0.05) as a result of the combined treatment compared to the monotherapy.
Table 4.
Effect of treatment on testicular oxidative stress parameters in STZ-induced diabetic rats.
Table 4.
Effect of treatment on testicular oxidative stress parameters in STZ-induced diabetic rats.
| Groups Parameters |
Non-diabetic Controls | Diabetic groups | p-value | |||
|---|---|---|---|---|---|---|
| Vehicle treated | Enalapril treated | Paricalcitol treated | Enalapril + Paricalcitol treated |
|||
| NO (μmols/L) | 5.33 ± 1.13 | 21.24 ± 4.6a | 6.23 ± 1.11b | 7.89 ± 2.32b | 7.19 ± 1.44b | P < 0.001 |
| MDA (nmol/mg pr) | 1.18 ± 0.13 | 5.61 ± .34a | 1.32 ± 0.41b | 1.91 ± 0.15b | 1.89 ± 0.11b | P < 0.001 |
| GSH (μg/mg pr) | 7.19 ± 1.05 | 2.97 ± 0.88a | 6.11 ± 0.72b | 5.93 ± 1.08b | 7.41 ± 1.54b | P < 0.01 |
| GPx (U/mg pr) | 29.12 ± 2.82 | 18.12 ± 2.02a | 26.03 ± 3.08b | 25.06 ± 2.03b | 30.22 ± 2.08b,c,d | P < 0.01 |
| SOD (units/mg pr) | 5.21 ± 0.43 | 2.33 ± 1.55a | 4.88 ± 1.39b | 3.85 ± 1.13b | 4.13 ± 1.48b | P < 0.01 |
| CAT (μmols of H2O2) | 5.64 ± 1.56 | 3.15 ± 0.96a | 5.73 ± 1.07b | 4.31 ± 1.16b | 6.93 ± 1.35b,d | P < 0.01 |
Data are expressed as mean ± SD, n = 10 rats; P < 0.05 was considered significant. NO, nitric oxide; MDA, malondialdehyde; GSH, reduced glutathione; GPx, glutathione peroxidase; SOD, superoxide dismutase; CAT, catalase; aSignificantly different from non-diabetic control group; bSignificantly different from diabetic vehicle treated group; cSignificantly different from diabetic enalapril treated group; dSignificantly different from diabetic paricalcitol treated group.
Figure 6.
Effect of treatment with enalapril and paricalcitol on testicular oxidative stress parameters. NO, nitric oxide; MDA, malondialdehyde; GSH, reduced glutathione; GPx, glutathione peroxidase; SOD, superoxide dismutase; CAT, catalase; aSignificantly different from non-diabetic control group; bSignificantly different from diabetic vehicle treated group; cSignificantly different from diabetic enalapril treated group; dSignificantly different from diabetic paricalcitol treated group.
Figure 6.
Effect of treatment with enalapril and paricalcitol on testicular oxidative stress parameters. NO, nitric oxide; MDA, malondialdehyde; GSH, reduced glutathione; GPx, glutathione peroxidase; SOD, superoxide dismutase; CAT, catalase; aSignificantly different from non-diabetic control group; bSignificantly different from diabetic vehicle treated group; cSignificantly different from diabetic enalapril treated group; dSignificantly different from diabetic paricalcitol treated group.
Histological and Immunohistochemical results
Hematoxylin and eosin-stained sections results
Testicular tissue from non-diabetic controls showed firmly packed seminiferous tubules bordered by stratified germinal epithelium when examined histologically with H&E staining. The tubules’ lumina contained spermatozoa. There are spermatogonia, primary spermatocytes, spermatids, as well as sperm in the spermatogenic epithelium. Tubules are isolated from one another by Leydig cells-rich interstitial connective tissue (Fig7, 1A). Additionally, there was an identified widening of the interstitial tissue including the Leydig cells and congestion of blood vessels in the interstitium (Fig. 7; 1B) within the diabetic control group, causing severe distortion of the testicular structure. This was caused by a complete dearth of spermatogenic epithelium as well as small remnants of the epithelial cells. While, testicular sections in other treated groups with either enalapril or paricalcitol or both, showed restoration of the previous changes with noticed marked improvement in rats treated with both drugs (Fig7, 1C, 1D and 1E).
Accumulation of collagen fibers surrounding seminiferous tubules was absent or minimal in the control group, as shown by histological inspection of Masson trichrome stained portions of the testes (Fig 8, 2A). In diabetic control group there was marked deposition of collagen fibers around seminiferous tubules (Fig 8, 2B). In diabetic treated groups with either enalapril (fig 8, 2C) or paricalcitol (Fig 8, 2D) or both (Fig 8, 2E) there was weak deposition of collagen fibers with noticed minimal expression in animals treated with both drugs.
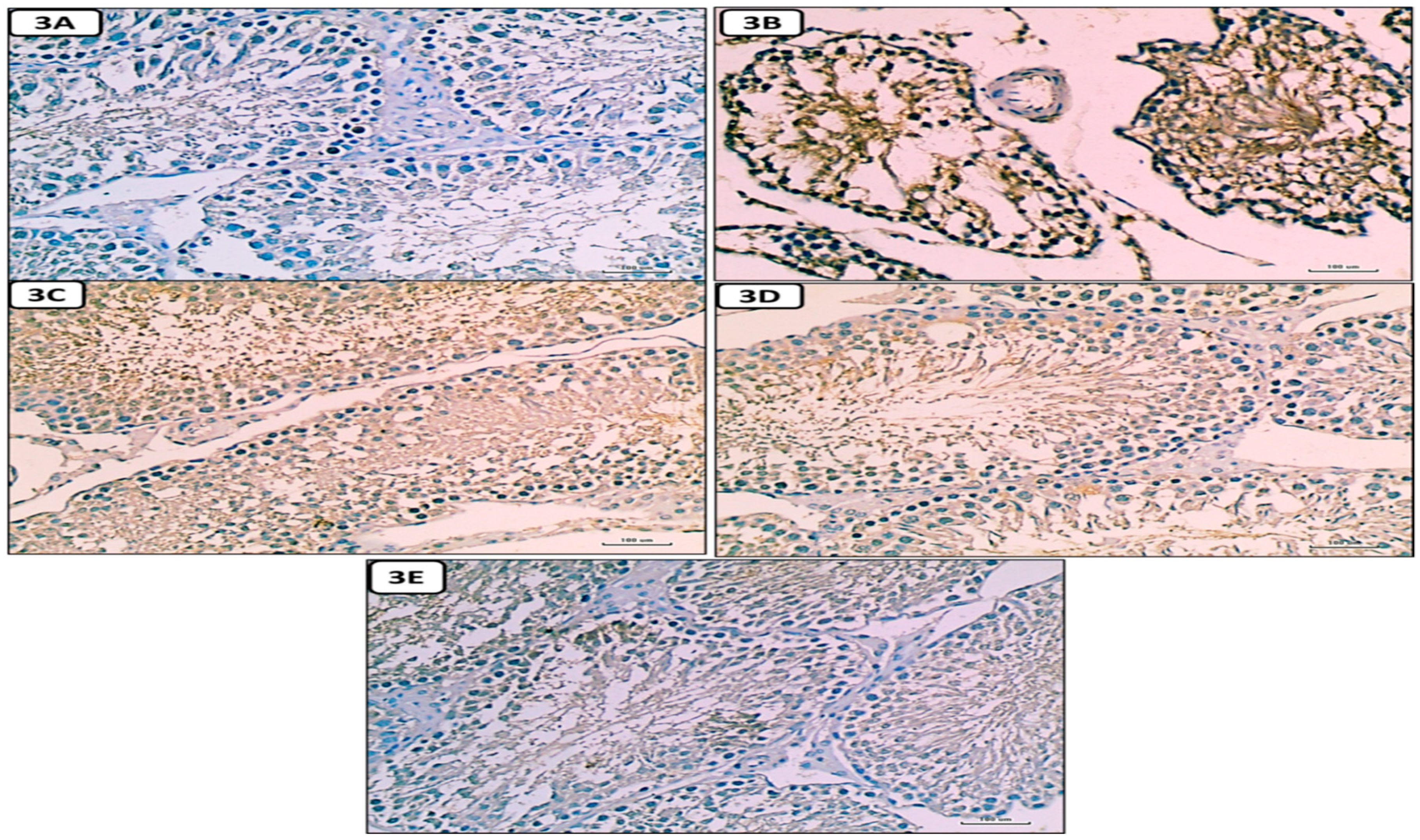
Immunostained testicular sections for caspase-3 showed: negative expression of caspase-3 in spermatogenic and Leydig cells in control group. (Fig 9, 3A); marked expression of caspase-3 in diabetic group.(Fig 9, 3B); mild expression of caspase-3 in diabetic treated groups with either enalapril (fig 9, 3C) or paricalcitol (fig 9, 3D) or both (9, 3E), with noticed minimal expression in rats treated with both drugs.
Figure 7.
Photomicrographs of testicular sections from non-diabetic control (1A), diabetic control rats (1B), diabetic enalapril-treated group (1C), diabetic paricalcitol-treated animals (1D), and diabetic enalapril + paricalcitol treated group (1E). Regarding the control group, the seminiferous tubules were densely packed, along with the lumen was filled with spermatogonia (curved arrow), primary spermatocytes (Sp), spermatids (St), as well as sperms (S). Leydig cells (thick arrow) are located in the interstitial space that separates tubules and is bordered by a basement membrane (arrow head). Diabetic animals’ testes exhibited pronounced vacuolations (V) caused by germinal epithelium detachment from tubular basement membrane (V) in numerous seminiferous tubules characterized by an irregularly thick basement membrane (arrow head) as well as an enlargement of the interstitial tissue including the Leydig cells and dilated blood vessels (thin arrow). While testicular sections in other treated groups with either enalapril or paricalcitol or both, showed restoration of the previous changes, with noticed marked improvement in rats treated with both drugs (Hx. & E. X400) Scale bars, 100 µm.
Figure 7.
Photomicrographs of testicular sections from non-diabetic control (1A), diabetic control rats (1B), diabetic enalapril-treated group (1C), diabetic paricalcitol-treated animals (1D), and diabetic enalapril + paricalcitol treated group (1E). Regarding the control group, the seminiferous tubules were densely packed, along with the lumen was filled with spermatogonia (curved arrow), primary spermatocytes (Sp), spermatids (St), as well as sperms (S). Leydig cells (thick arrow) are located in the interstitial space that separates tubules and is bordered by a basement membrane (arrow head). Diabetic animals’ testes exhibited pronounced vacuolations (V) caused by germinal epithelium detachment from tubular basement membrane (V) in numerous seminiferous tubules characterized by an irregularly thick basement membrane (arrow head) as well as an enlargement of the interstitial tissue including the Leydig cells and dilated blood vessels (thin arrow). While testicular sections in other treated groups with either enalapril or paricalcitol or both, showed restoration of the previous changes, with noticed marked improvement in rats treated with both drugs (Hx. & E. X400) Scale bars, 100 µm.
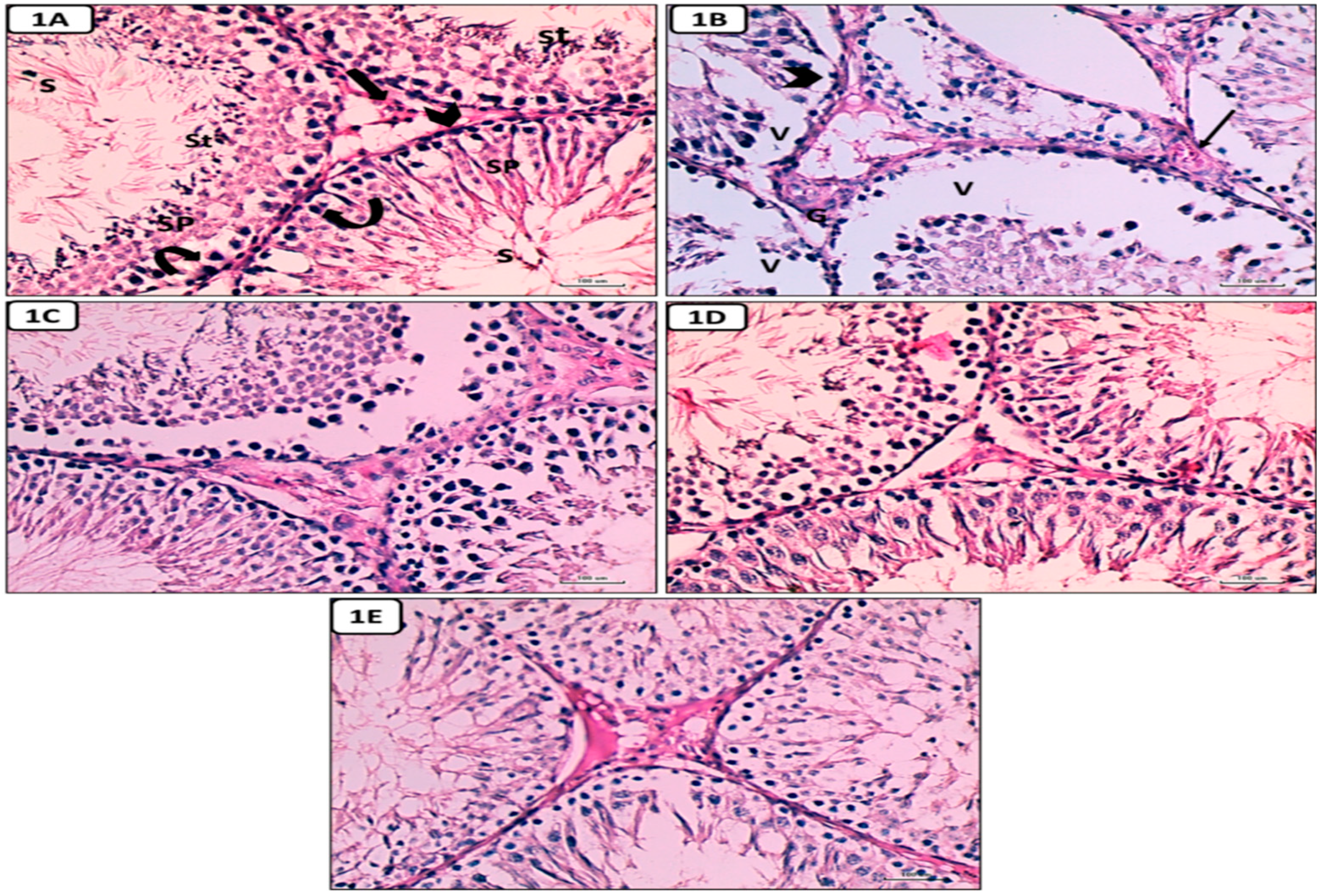
Figure 8.
Micrographs of testicular tissue stained with masson trichrome reveal that collagen fiber deposition is absent or minimal in the non-diabetic control group, but extensive in the diabetes control group. (B): weak deposition of collagen fibers in diabetic treated groups with either enalapril (C) or paricalcitol (D) or both (E) with noticed minimal expression in rats treated with both drugs (Masson trichrome stain X400) Scale bars, 100 µm.
Figure 8.
Micrographs of testicular tissue stained with masson trichrome reveal that collagen fiber deposition is absent or minimal in the non-diabetic control group, but extensive in the diabetes control group. (B): weak deposition of collagen fibers in diabetic treated groups with either enalapril (C) or paricalcitol (D) or both (E) with noticed minimal expression in rats treated with both drugs (Masson trichrome stain X400) Scale bars, 100 µm.
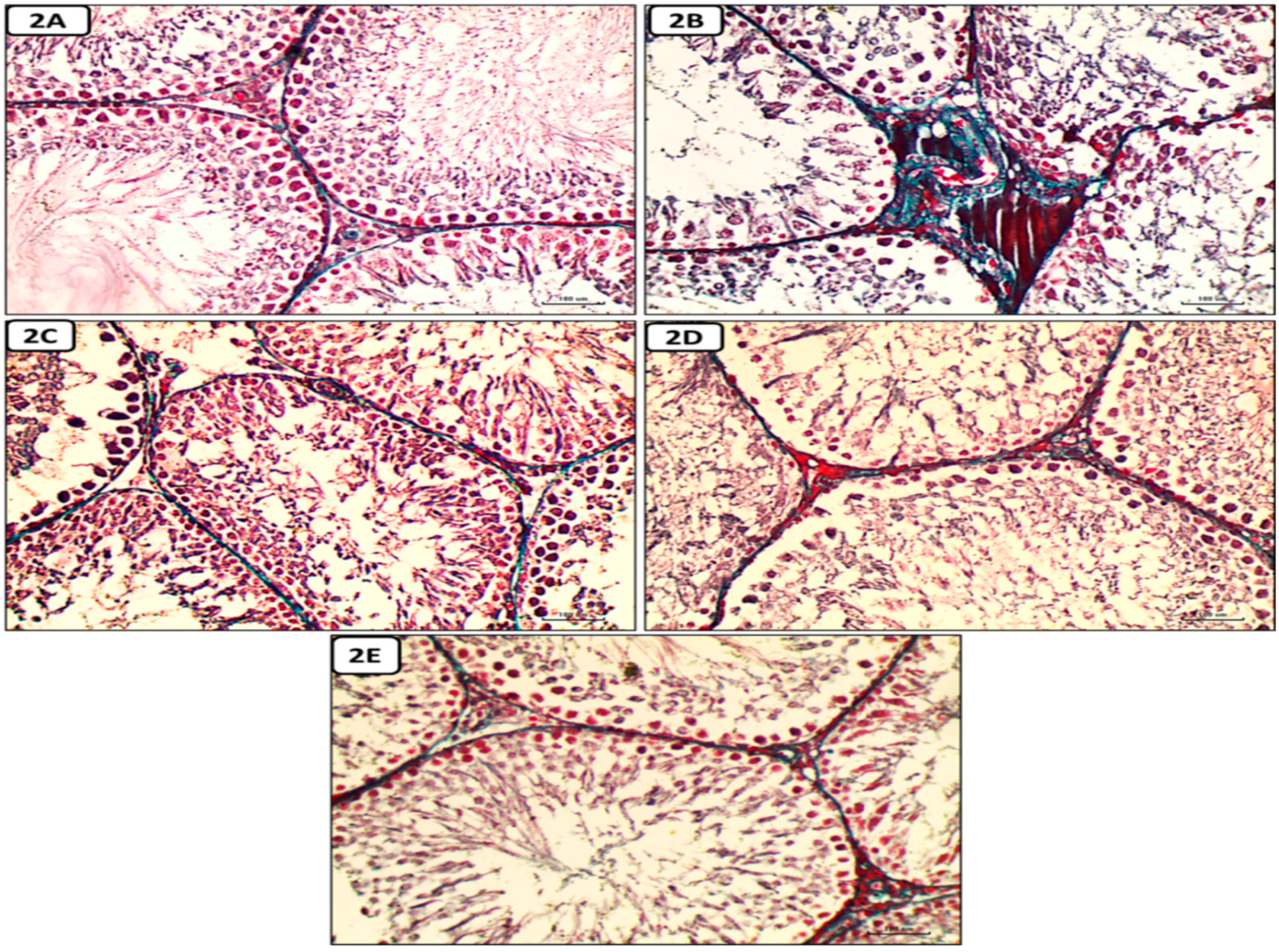
Figure 9.
Photomicrographs of Immunostained testicular sections for caspase-3 showing: no or weakest expression of caspase-3 in control group (A); marked expression of caspase-3 in diabetic control group (B); weak expression of caspase-3 in diabetic treated groups with either enalapril (C) or paricalcitol (D) or both (E) with noticed minimal expression in the treated group with combination of both. (anti caspase 3 immunostaining X400) Scale bars, 100 µm.
Figure 9.
Photomicrographs of Immunostained testicular sections for caspase-3 showing: no or weakest expression of caspase-3 in control group (A); marked expression of caspase-3 in diabetic control group (B); weak expression of caspase-3 in diabetic treated groups with either enalapril (C) or paricalcitol (D) or both (E) with noticed minimal expression in the treated group with combination of both. (anti caspase 3 immunostaining X400) Scale bars, 100 µm.
Discussion
Diabetes mellitus (DM) is a chronic metabolic disease that causes multiple complications including retinopathy, nephropathy, neuropathy as well as reproductive dysfunction [34,35]. DM is known to impair microcirculation and hemodynamics in various organs and systems, and increase their oxidative stress leading to their damage and dysfunction [36]. In this study, we investigated the antioxidant and anti-inflammatory activities of enalapril (an ACEI) and/or paricalcitol (a vitamin D analogue), and their protective effects on STZ diabetes-induced testicular damage, in male rats.
In accordance with Schoeller et al. [37] and Ozdemir et al. [38] the findings of this study revealed that, the STZ-induced diabetic rats exhibited decreased body weight as the hyperglycemia induce calorie loss, and protein exhaustion in muscles and adipose tissue. The diabetes-induced weight loss was reversed by mono and combined therapy with enalapril and paricalcitol with somewhat superior effect for the combined therapy.
The current study also showed significant increase in the fasting and postprandial glucose levels and HOMA-IR value with a concomitant decrease in the serum insulin level in diabetic control rats as compared to the non-diabetic controls. These effects were improved when the diabetic rats were treated by paricalcitol alone or when combined with enalapril than when treated with enalapril alone. These results go parallel with Ali et al. [6] who suggested that the combined therapy with both drugs is more effective in improving the tissue sensitivity to insulin, and attributed the glucose-lowering effect of paricalcitol to its antioxidant activity which protect the β-cells of pancreatic islets from the superfluous free radicals, as well as its ability to induce them to release insulin, as evidenced by its rising effect on C-peptide level in addition to its lowering effect on MDA level [39]
Also in our study, the testicular oxidative stress was significantly increased and the antioxidant defense systems were attenuated due to induction of diabetes in rats, as evidenced by a significant increase in the testicular NO and MDA with a concomitant suppression of GPx, SOD, and CAT activities as well as a decrease in the testicular content of GSH in diabetic control rats in comparison with the normal rats.
These findings are consistent with Shrilatha and Muralidhara, [3] who found that diabetes disturbs the balance among the rate of ROS production and the power of deoxidation, increasing oxidative stress in male reproductive system that can impair the normal protein and DNA structure in reproductive cells and thus their survival, in addition to its detrimental effect on spermatogenesis, leading to male infertility [17]. Our results showed that the testicular oxidant/antioxidant balance was restored when diabetic rats were treated with enalapril or paricalcitol, with a greater increase in GPx and CAT activities by their combination. In line with these results, Ali et al. [40] demonstrated the ability of both drugs, either separately or together, to suppress the generation of free radicals and to restore the actions of antioxidant enzymes in diabetic rats to levels close to those of control rats, suggesting their antioxidant activities. Moreover, the ameliorating effect of both drugs on diabetes-induced oxidant/antioxidant imbalance has been investigated and confirmed in different organs including the heart [6] and kidneys [7]. Also their role in improving the uremic-induced renal [41] and cardiac [41,42] oxidative stress was confirmed.
Our results also demonstrated the anti-inflammatory effect of both drugs, especially paricalcitol and the combined treatment, as the inflammatory markers (IL-6 and TNF-α) were significantly increased as a result of induction of diabetes, then improved in treated groups in the order of enalapril + paricalcitol > paricalcitol > enalapril. These findings came in agreement with Izquierdo et al. [43] who demonstrated the efficacy of paricalcitol therapy in reducing the levels of inflammatory markers including TNF-α, IL-6, CRP and IL-18 in patients with kidney disease. In another study conducted by Navarro et al. [44] enalapril was also shown to have similar anti-inflammatory activities.
In addition, diabetic rats involved in this study were also exhibited impaired testicular functions that were manifested by decreased serum levels of testosterone, FSH and LH, testicular weight, sperm count and motility with increased percentage of abnormal sperms with distortion of testicular histological structure. These findings are in accordance with Long et al. [16] who demonstrated a significant reduction in testicular expression of vascular endothelial growth factor (VEGF) in animals with type 2 diabetes, which induces impairment of testicular microcirculation, via reduction of vascular area and blood velocity in the testis, leading to testicular histological and functional disorders. In addition to the low level of VEGF which is also necessary for maintaining normal male reproductive function and germ cell homeostasis [45]. Schoeller et al. [37] also attributed the STZ-induced testicular damage to the diminution of serum levels of insulin, as the normal insulin level is essential for prevention of testicular apoptosis and diabetes-induced sexual disorders, it is also needed for physiological secretory activity of pituitary gland, normal LH release and proper function of Leydig cell [46]. Furthermore, the hypothalamic Gonadotropin Releasing Hormone (GnRH) neurons are extremely sensitive to insulin, and they express insulin receptors [47]. Therefore these hormonal abnormalities in diabetic rats were attributed to dysfunction of hypothalamic-pituitary-testicular axis as due to direct impact of insulin shortage and decline of activities of Leydig cellular enzymes [30,48]. Moreover, previous studies showed that hyperglycemia causes testicular damage, impair spermatogenesis and decrease sperm count by increasing ROS and decreasing capacity of antioxidant mechanisms in testis, epididymis and sperms causing oxidative stress which leads to apoptosis of somatic and germ cells [49,50,51]. Also ROS generated in the sperms can induce lipid peroxidation, nuclear DNA damage and protein oxidation leading to reduction of sperm count, motility and viability as well as an increase in sperm abnormalities [52,53]. Many other publications also reported significant decline in testicular hormones and sperm parameters with significant rise in abnormal forms of sperm in STZ-induced diabetic animals [54,55].
Regarding the effect of treatment, our results reported a significant increase in sperm count as well as motility, plasma levels of testosterone, FSH and LH with a significant decline in the percentage of abnormal sperms owing to treatment of diabetic rats with enalapril or paricalcitol with marked improvement by their combination. These findings are consistent with those of Yang et al.[56], who found that giving vitamin D to diabetic rats significantly raised their plasma levels of testosterone hormone, sperm count, sperm motility and significantly decreased abnormal sperms by down regulation of TGF-β1and NF-kB and upregulation of PPAR-γ. Vitamin D supplementation protects testicular cells in diabetic rats, as described by Ding et al. [57], by inhibiting inflammatory factor expression, reducing apoptosis of cells, and increasing the expression of genes involved in testosterone production. Calcipotriol (a vitamin D derivative) alone or in combination with empagliflozin (an inhibitor of sodium-glucose co-transporter-2 [SGLT2]) have been shown to significantly increase the plasma levels of testosterone, FSH and LH, sperm count and motility, antioxidant defenses, and significantly decrease the abnormal sperms and the inflammatory markers (IL-6 and TGF-β1), and improves the histopathological pictures of the testis in cadmium induced testicular toxicity in rats [58]. Furthermore, Sood et al. [59] demonstrated that optimum vitamin D supplementation can reverse the delay of spermatogenesis caused by changes in Sertoli as well as Leydig cell function in vitamin D deficiency rats. Furthermore, Abozaid & Hany [60] revealed that Nano vitamin D3 has a potential protecting role in reducing the negative effects of high fat diet caused by obesity on testicular functioning as it produced significant elevation of testosterone level, sperm count, sperm motility and testicular antioxidant enzymes linked with significant reduction of lipid peroxidation, testicular TNF-α, and IL-6 with improvement of testicular histological picture. Our findings confirmed those of Kushawha and Jena, who [61] reported that enalapril treatment of diabetic rats significantly increases the testosterone level, sperm count and motility with significant reduction of sperm abnormalities associated with improvement of histopathological picture of testis by reversing sperm DNA damage, reducing oxidative stress and down-regulating NF-KB and COX-2 expression in STZ–induced diabetic rats. Furthermore, a previous study reported that enalapril intervention in nicotine treated diabetic rats decreased testicular damage as well as reestablished sperm count, nuclear DNA damage, testosterone level in addition to decreased expression of pro-inflammatory markers (NF-KB, TNF-α and COX-2) with improvement of histological picture of testis and epididymis [62]. Enalapril also in other studies protected the morphological changes of testis and restoring the spermatozoid production in hypertensive rats [63], and reduced the tubular damage and testicular cell apoptosis after unilateral testicular torsion [64].
Conclusions
Combination therapy with enalapril and paricalcitol ameliorates the diabetic induced reproductive damage (via their potencies in improving the glycemic state and tissue insulin sensitivity, restoring the oxidant/antioxidant balance, in addition to their anti-inflammatory and anti-apoptotic activities), than monotherapy in diabetic male rats, recommending a synergistic impact of both drugs. Additional studies would be required towards studying the underlying molecular mechanisms by which ACE inhibitors and vitamin D analogues can reduce oxidative stress in different tissues in diabetic rats.
Acknowledgments
We acknowledge Prof. Dr. Gaber Eldesoky, Department of Chemistry, College of Science, King Saud University, P. O. Box 2455, Riyadh 11451, Saudi Arabia, for the great help in performing the chemical laboratory findings. We also acknowledge Prof. Dr. Basem Hassan El-Essawy, Department of Pathology, Faculty of Medicine, Mansoura University, Mansoura, Egypt, for the great help in performing the histopathological findings.
Conflicts of Interest
The authors declared that there was no conflict of interest.
References
- Saeedi,P.; Petersohn, I.; Salpea, P.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract. 2019,157,107843. Doi:10.1016/j.diabres.2019.107843. [CrossRef]
- Aksu, I.; Baykara,B.; Kiray, M.; Gurpinar, T.; Sisman, A.R.; Ekerbicer, N., Tas, A.; Gokdemir-Yazar, O.; Uysal, N. Serum IGF-1 levels correlate negatively to liver damage in diabetic rats. Biotech Histochem. 2013, 88(3-4),194-201. doi: 10.3109/10520295.2012.758311. [CrossRef]
- Shrilatha, B.; Muralidhara. Occurrence of oxidative impairments, response of antioxidant defences and associated biochemical perturbations in male reproductive milieu in the Streptozotocin-diabetic rat. Int J Androl. 2007, 30(6), 508-518. doi:10.1111/j.1365-2605.2007. 00748.x. [CrossRef]
- Maresch, C.C.; Stute, D.C.; Ludlow, Hammes, H.P.; de Kretser, D.M.; Hedger, M.P.; Linn, T. Hyperglycemia is associated with reduced testicular function and Activin dysregulation in the Ins2 Akita+/− mouse model of type 1 diabetes. Mol Cell Endocrinol. 2017,446, 91–101.
- Tiwari, A. K. Imbalance in antioxidant defense and human diseases: multiple approach of natural antioxidants therapy. Current Science, 200, 81, 1179–1187.
- Ali, T.M.; Mehanna, O.M.; Elsaid, A.G.; Askary, A.E. Effect of Combination of Angiotensin-Converting Enzyme Inhibitors and Vitamin D Receptor Activators on Cardiac Oxidative Stress in Diabetic Rats. Am J Med Sci. 2016; 352(2), 208-214. doi: 10.1016/j.amjms.2016.04.016. [CrossRef]
- Ahmed, O.M.; Ali, T.M.; Abdel Gaid, M.; Elberry, A.A. Effects of enalapril and paricalcitol treatment on diabetic nephropathy and renal expressions of TNF-α, p53, caspase-3 and Bcl-2 in STZ-induced diabetic rats. PLoS One. 2019,14(9), e0214349. doi: 10.1371/journal.pone.0214349. [CrossRef]
- Rajagopalan, S.; Kurz, S.; Münzel, T.; et al. Angiotensin II-mediated hypertension in the rat increases vascular superoxide production via membrane NADH/NADPH oxidase activation. Contribution to alterations of vasomotor tone. J Clin Invest. 1996,97(8),1916-1923. doi:10.1172/JCI118623. [CrossRef]
- Bhuyan, B.J.; Mugesh, G. Synthesis, characterization and antioxidant activity of angiotensin converting enzyme inhibitors. Org Biomol Chem. 2011,9(5),1356-1365. doi:10.1039/c0ob00823k. [CrossRef]
- Mokhtari, Z.; Hekmatdoost, A.; & Nourian, M. Antioxidant efficacy of vitamin D. Journal of Parathyroid Disease, 2016; 5(1), 11-16.
- Wang, T.J.; Pencina, M.J.; Booth, S.L.; Jacques, P.F.; Ingelsson, E.; Lanier, K.; et al. Vitamin D deficiency and risk of cardiovascular disease. Circulation. 2008,117,503-11. [CrossRef]
- Ravani, P.; Malberti, F.; Tripepi, G.; Pecchini. P.; Cutrupi, S.; Pizzini, P.; et al. Vitamin D levels and patient outcome in chronic kidney disease. Kidney Int. 2009,75,88-95. [CrossRef]
- Mitri, J.; Muraru, M.; Pittas, A. Vitamin D and type 2 diabetes: a systematic review. Eur J Clin Nutr. 2011, 65,1005-15. [CrossRef]
- Hyppönen, E.; Läärä, E.; Reunanen, A.; Järvelin, M.R.; Virtanen, S.M. Intake of vitamin D and risk of type 1 diabetes: a birthcohort study. Lancet. 2001, 358,1500-3. [CrossRef]
- Yang, J.; XU, J.; & Zhang, H. Effect of Vitamin D on ACE2 and Vitamin D receptor expression in rats with LPS-induced acute lung injury. Chinese journal of emergency medicine, 2016,1284-1289.
- Long, L.; Qiu, H.; Cai, B.; Chen, N.; Lu, X.; Zheng, S.; Ye, X.; Li, Y. Hyperglycemia induced testicular damage in type 2 diabetes mellitus rats exhibiting microcirculation impairments associated with vascular endothelial growth factor decreased via PI3K/Akt pathway. Oncotarget, 2018,9 (4), 5321–5336. [CrossRef]
- Shrilatha, B.; Muralidhara. Early oxidative stress in testis and epididymal sperm in streptozotocin-induced diabetic mice: Its progression and genotoxic consequences. Reprod. Toxicol.2007, 23, 578-587. [CrossRef]
- Finch, J.L.; Suarez, E.B.; Husain, K.; et al. Effect of combining an ACE inhibitor and a VDR activator on glomerulosclerosis, proteinuria, and renal oxidative stress in uremic rats. Am J Physiol Renal Physiol 2012, 302(1), F141–9. [CrossRef]
- Tietz, N.W. Clinical Guide to Laboratory Tests, 3rd Ed., Pbl, W.B. Saunders Company, Philadelphia, 1995, Pp:509–580.
- Temple, R.C.; Clark, P.M, and Hales, C.N. Measurement of insulin secretion in type 2 diabetes: problems and pitfalls. Diabetic Medicine. 1992, 9, 503-512. [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; et al. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia1985, 28, 412–9.
- Huang, H.F.; Linsenmeyer, T.A.; Li M.T.; Giglio, W.; Anesetti, R.; von Hagen, J.; Ottenweller, J.E.; Pogach, L. Acute effects of spinal cord injury on the pituitary-testicular hormone axis and Sertoli cell functions: a time course study. J. Androl. 1995, 16, 148–157. [CrossRef]
- Ellman, M. A spectrophotometric method for determination of reduced glutathione in tissues. Anal Biochem.1959, 74(1), 214–226.
- Flohe, L.; Otting, F. Superoxide dismutase assays. Methods Enzymol. 1984,105, 93–104. [CrossRef]
- Husain, K.; Suarez, E.; Isidro, A.; Ferder, L. Effects of paricalcitol and enalapril on atherosclerotic injury in mouse aortas. Am J Nephrol. 2010, 32(4), 296-304. [CrossRef]
- Aebi H. (1984): Catalase in vitro. Methods Enzymology,105:121-6. [CrossRef]
- Ohkawa, H.; Ohishi, N.; Yagi, K. Assay for lipid peroxides in animal tissues by thiobarbaturic acid reaction. Anal.Biochem. 1982, 95, 351-358. [CrossRef]
- Hortelano, S.; Dewez, B.; Genaro, A.M.; Díaz-Guerra, M.J.; Boscá, L. Nitric oxide is released in regenerating liver after partial hepatectomy. Hepatology. 1995,21, 776-786. [CrossRef]
- Kushwaha, S.; Jena, GB. Effects of nicotine on the testicular toxicity of streptozotocin-induced diabetic rat: intervention of enalapril. Hum Exp Toxicol. 2014, 33, 609-622. doi:10.1177/0960327113491509. [CrossRef]
- Khaki, A.; Khaki, A.A.; Hajhosseini, L.; Golzar, F.S.; Ainehchi, N. The anti-oxidant effects of ginger and cinnamon on spermatogenesis dys-function of diabetes rats. Afr J Tradit Complement Altern Med. 2014,11,1-8. doi:10.4314/ajtcam. v11i4.1. [CrossRef]
- Shalizar, J.A.; Hasanzadeh, S.; Malekinejad, H. Chemoprotective effect of Crataegusmonogyna aqueous extract against cyclophosphamide-induced reproductive toxicity. Vet Res Forum. 2011, 2, 266–273.
- Bancroft, J.D.; Layton C. The Hematoxylin and Eosin. In: SuVarna, S.K.; Layton, C.; Bancroft, J.D.; Eds., Theory & Practice of histological Technique, 7th Edition, Churchill Livingstone of ElSevier, Philadelphia, Ch.10 and 11, 2013,172-214.
- Jackson, P.; Blythe, D. Immunohistochemical Techniques. In: SuVarna, S.K.; Layton, C.; Bancroft, J.D.; Eds., Theory & Practice of histological techniques, 7th Edition, Churchill Livingstone of El Sevier, Philadelphia. Ch. 18, 2013, 381-434.
- Ricci, G.; Catizone, A.; Esposito, R.; Pisanti, F.A.; Vietri, M.T.; Galdieri, M. Diabetic rat testes: morphological and functional alterations. Andrologia. 2009, 41, 361-368. doi:10.1111/j.1439-0272.2009. 00937.x. [CrossRef]
- Take, G.; Ilgaz, C.; Erdogan, D.; Ozogul, C.; Elmas, C. A Comparative Study of the Ultrastructure of Submandibular, Parotid and Exocrine Pancreas in Diabetes and Fasting. Saudi Medical Journal. 2007, 28, 28-35.
- Long, L.; Wang, J.; Lu, X.; Xu, Y.; Zheng, S.; Luo, C.; Li, Y. Protective effects of scutellarin on type II diabetes mellitus-induced testicular damages related to reactive oxygen species/Bcl-2/Bax and reactive oxygen species/microcirculation/staving pathway in diabetic rat. J Diabetes Res. 2015, 2015, 252530. doi:10.1155/2015/252530. [CrossRef]
- Schoeller, E.L.; Albanna, G.; Frolova, A.I.; Moley, K.H. Insulin rescues impaired spermatogenesis via the hypothalamic-pituitary-gonadal axis in Akita diabetic mice and restores male fertility. Diabetes. 2011, 61(7):1869-1878. doi:10.2337/db11-1527. [CrossRef]
- Ozdemır, O.; Akalın, P.P.; Baspınar, N.; Hatıpoglu, F. Pathological changes in the acute phase of streptozotocin-induced diabetic rats.Bull Vet Inst Pulawy. 2009,53, 783-790.
- Husain, K.; Suarez, E.; Isidro, A.; Hernandez, W.; Ferder, L. Effect of paricalcitol and enalapril on renal inflammation/oxidative stress in atherosclerosis. World J Biol Chem. 2015, 6, 240-248. doi:10.4331/wjbc. v6.i3.240. [CrossRef]
- Ali, T.M.; Esawy, B.H.; Elmorsy, E.A. Effect of combining an angiotensin-converting enzyme inhibitor and a vitamin D receptor activator on renal oxidative and nitrosative stress in diabetic rats. Natl J Physiol Pharm Pharmacol 2015, 5(3), 222–31. [CrossRef]
- Husain, K.; Ferder, L.; Mizobuchi, M.; Finch, J.; Slatopolsky, E. Combination Therapy with Paricalcitol and Enalapril Ameliorates Cardiac Oxidative Injury in Uremic Rats. Am J Nephrol 2009,29:465-472. doi: 10.1159/000178251. [CrossRef]
- Ritter, C.; Zhang, S.; Finch, J. L.; Liapis.; Suarez, E.; Ferder, L.; Delmez, J.; Slatopolsky, E. Cardiac and Renal Effects of Atrasentan in Combination with Enalapril and Paricalcitol in Uremic Rats. Kidney Blood Press Res. 2014,39, 340-352. doi: 10.1159/000355811. [CrossRef]
- Izquierdo, M.J.; Cavia, M.; Muniz, P.; De Francisco, A.L.; Arias, M.; Santos, J.; et al. Paricalcitol reduced oxidative stress and inflammation in hemodialysis patients. BMC Nephrol 2012; 13: 159. https://doi.org/10.1186/1471-2369-13-159 PMID: 23186077. [CrossRef]
- Navarro, J.F.; Milena, F.J.; Mora, C. Leo, C.; Claverie, F.; Flores, C.; Garcia, J. Tumor necrosis factor-alpha gene expression in diabetic nephropathy: relationship with urinary albumin excretion and effect of angiotensin-converting enzyme inhibition. Kidney Int Suppl. 2005, (99, :S98-S102. doi:10.1111/j.1523-1755.2005. 09918.x. [CrossRef]
- Smith, G.A.; Fearnley, G.W.; Harrison, M.A.; Tomlinson, D.C.; Wheatcroft, S.B.; Ponnambalam, S. Vascular endothelial growth factors: multitasking functionality in metabolism, health and disease. J Inherit Metab Dis. 2015, 38(4), 753-763. doi:10.1007/s10545-015-9838-4. [CrossRef]
- Pérez Díaz, J.; Benitez, A.; Fernández Galaz, C. Effect of streptozotocin diabetes on the pituitary-testicular axis in the rat. Horm Metab Res. 1982, 14(9), 479-482. doi:10.1055/s-2007-1019052. [CrossRef]
- Salvi, R.; Castillo, E.; Voirol, M.J.; Glauser, M.; Rey, J.; Gaillard, R.C.; Vollenweider, P.; Pralong F.P. Gonadotropin-releasing hormone-expressing neurons immortalized conditionally are activated by insulin: implication of the mitogen-activated protein kinase pathway. Endocrinology. 2006, 147, 816-826. doi:10.1210/en.2005-0728. [CrossRef]
- Olivares, A.; Méndez, J.P.; Cárdenas, M.; Oviedo, N.; Palomino, M. Á.; Santos, I.; Ulloa-Aguirre, A.. Pituitary-testicular axis function, biological to immunological ratio and charge isoform distribution of pituitary LH in male rats with experimental diabetes. Gen Comp Endocrinol. 2009, 161(3), 304-312. doi: 10.1016/j.ygcen.2008.12.021. [CrossRef]
- Shoorei, H.; Khaki, A.; Khaki, A.A.; Hemmati, A.A.; Moghimian, M.; Shokoohi, M. The ameliorative effect of carvacrol on oxidative stress and germ cell apoptosis in testicular tissue of adult diabetic rats. Biomed Pharmacother. 2019, 111, 568-578. doi: 10.1016/j.biopha.2018.12.054. [CrossRef]
- Soltani, M.; Moghimian, M.; Abtahi-Eivari, S.H.; Shoorei, H.; Khaki, A.; Shokoohi, M. Protective Effects of Matricaria chamomilla Extract on Torsion/ Detorsion-Induced Tissue Damage and Oxidative Stress in Adult Rat Testis. Int J Fertil Steril. 2018, 12(3), 242-248. doi:10.22074/ijfs.2018.5324. [CrossRef]
- Nna, V.U.; Bakar, A.B.A.; Ahmad, A.; Mohamed, M. Down-regulation of steroidogenesis-related genes and its accompanying fertility decline in streptozotocin-induced diabetic male rats: ameliorative effect of metformin. Andrology. 2019, 7(1), 110-123. doi:10.1111/andr.12567. [CrossRef]
- Alahmar, A.T. Role of Oxidative Stress in Male Infertility: An Updated Review. J Hum Reprod Sci. 2019, 12, 4-18. doi:10.4103/jhrs.JHRS_150_18. [CrossRef]
- Laleethambika, N.; Anila, V.; Manojkumar, C.; Muruganandam, I.; Giridharan B.; Ravimanickam, T.; Balachandar, V. Diabetes and Sperm DNA Damage: Efficacy of Antioxidants. SN Compr. Clin. Med.2019, 1, 49–59.
- Alasmari, W. A.; Faruk, E. M.; Abourehab, M. A.; Elshazly, A. M. E.; & El Sawy, N. A. The effect of metformin versus vitamin E on the testis of adult diabetic albino rats: histological, biochemical and immunohistochemistry study. Advances in Reproductive Sciences, 2018, 6(4), 113-132.
- Samir, S.M.; Elalfy, M.; Nashar, E.M.E.; Alghamdi, M.A.; Hamza, E.; Serria, M.S.; Elhadidy, M.G. Cardamonin exerts a protective effect against autophagy and apoptosis in the testicles of diabetic male rats through the expression of Nrf2 via p62-mediated Keap-1 degradation. Korean J Physiol Pharmacol. 2021, 25(4), 341-354. doi:10.4196/kjpp.2021.25.4.341. [CrossRef]
- Liu, Y.; He, Y.; Wang, Q.; Guo, F.; Huang, F.; Ji, L.; An, T.; Qin, G. Vitamin D3 supplementation improves testicular function in diabetic rats through peroxisome proliferator-activated receptor-γ/transforming growth factor-beta 1/nuclear factor-kappa B. J Diabetes Investig. 2019, 10(2), 261-271. doi:10.1111/jdi.12886. [CrossRef]
- Ding, C.; Wang, Q.; Hao, Y.; Ma, X.; Wu, L., Li, W.; Du, M.; Li, W.; Wu, Y.; Guo, F.; Ma, S.; Huang, F.; Qin, G. Vitamin D supplement improved testicular functions in diabetic rats. Biochem Biophys Res Commun. 2016, 473, 161-167. doi:10.1016/j.bbrc.2016.03.072. [CrossRef]
- Borg, H. M.; Kabel, A.; Estfanous, R.; & Abd Elmaaboud, M. Effect of the combination between empagliflozin and calcipotriol on cadmium-induced testicular toxicity in rats. Bulletin of Egyptian Society for Physiological Sciences. 2020,40(1), 15-31. DOI:10.21608/BESPS.2019.14918.1029. [CrossRef]
- Sood, S.; Reghunandanan, R.; Reghunandanan, V.; Marya, R.K.; Singh, P.I. Effect of vitamin D repletion on testicular function in vitamin D-deficient rats. Ann Nutr Metab. 199, 39, 95-98. doi:10.1159/000177848. [CrossRef]
- ABOZAID, E. R.; & HANY, A. Vitamin D3 nanoemulsion ameliorates testicular dysfunction in high-fat diet-induced obese rat model. The Medical Journal of Cairo University, 2020, 88, 775-785. DOI: 10.21608/mjcu.2020.104886. [CrossRef]
- Kushwaha, S.; Jena, G.B. Enalapril reduces germ cell toxicity in streptozotocin-induced diabetic rat: investigation on possible mechanisms. Naunyn Schmiedebergs Arch Pharmacol. 2012, 385(2), 111-124. doi:10.1007/s00210-011-0707-x. [CrossRef]
- Kushwaha, S.; Jena, G.B. Effects of nicotine on the testicular toxicity of streptozotocin-induced diabetic rat: intervention of enalapril. Hum Exp Toxicol. 2014, 33(6), 609-622. doi:10.1177/0960327113491509. [CrossRef]
- Bechara G.R., deSouza D.B., Simeos M., Felix-Particio B., Medeiros Jr. J.L., Costa W.S., Sampaio F.J.B. Testicular Morphology and Spermatozoid Parameters in Spontaneously Hypertensive Rats Treated with Enalapril. J Urol. 2015, 194(5), 1498-1503. doi:10.1016/j.juro.2015.06.073. [CrossRef]
- Gokce, G.; Karboga, H.; Yildiz, E.; Ayan, S.; Gultekin, Y. Effect of angiotensin-converting enzyme inhibition and angiotensin II type 1 receptor blockade on apoptotic changes in contralateral testis following unilateral testicular torsion. Int Urol Nephrol. 2008, 40(4), 989-995. doi:10.1007/s11255-008-9348-5. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



