Submitted:
09 October 2023
Posted:
09 October 2023
Read the latest preprint version here
Abstract
Background
Candida auris is an emerging multidrug-resistant fungal pathogen that represents a serious threat to healthcare settings currently.
Objective: Its objective was to determine the prevalence of C. auris in the hospital since its initial detection in late 2019.
Methods: Using an adapted risk assessment tool, we reviewed the charts. and medical files of all suspected? and confirmed cases of C. auris cases reported at King Khalid University Hospital, Riyadh between November 2019 and December 2022. Anonymized data were retrieved in a pre-established datasheet and analyzed to determine the epidemiological characteristics of C. auris infection in our facility. We established our initial prevalence by age, gender, risk factors, and according to sampling source.
Results: Of the 53 confirmed cases positive for C. auris during the study period, 33 (62%) were males. Their ages ranged between 15 and 98; most positive cases occurred in 50 and above. Only one of the confirmed cases was hospital-acquired. All patients had at least one risk factor, and Urine samples yielded the greatest number of positive cases while admission to healthcare facilities constituted the highest risk in our study.
Conclusion: Establishing a local prevalence could serve as our baseline/benchmark to compare with regional and international benchmarks.
Keywords:
1. Candida auris
; 2. C. auris
; 3. Candida
; 4. Candidemia
; 5. Multi drug resistant organism
; 6. MDRO
; 7. Emerging pathogens
; 8 Resistant pathogens.
1. Introduction
This study investigated the incidence of Candida auris in a tertiary care teaching hospital located in Riyadh, Saudi Arabia. The C. auris, first emerged in 2009,[1] and has continued to cause hospital-acquired infections in individuals with compromised immune systems and has also been associated with persistent candidemia and high mortality rates globally.
Candida auris was first identified in 2009 when it was found in the outer ear of a patient in Japan [2]. Since then, clinical cases of C. auris infections have been reported in in other countries including South Korea [3], India [4], Pakistan [5], South Africa [6,7], Canada[8] with a phenomenal surge between 2018 and 2021 in the United States [9].The first Saudi case was reported in 2018 [10] and later followed by several reports from other parts of the country [11,12].
This fungal specie is rapidly spreading worldwide, with several outbreaks [13] reported from five continents in recent years. [4] Between the years 2019 and 2020, C. auris has been reported in over 40 countries across the world. The Asian continent has the highest number (14) of countries where C. auris is reported, followed by Europe (13), and then trailed far behind by South America (4), Africa (4), North America (3), and Oceania (1) [14].
The surge in the incidence rates of candidemia has been an immense burden on public health, particularly among patients in intensive care units. [5,7]. The mortality rate is higher among infected patients compared with those who were colonized. [15] C. auris is an opportunistic pathogen that can cause candidemia [16] with risk factors including immunocompromised patients, patients with organ transplants, diabetic patients, or patients on recent antifungal use, catheter use, and prolonged ICU stay. [9] Other risk factors include chronic kidney diseases, recent vascular surgery, or surgery within the previous three months.[17,18]
C. auris started attracting considerable global attention due to its growing reports, transmission through health professionals, high rate of treatment failure, and multidrug resistance.[19] C. auris is increasingly becoming a threat to human health because of its intrinsic resistance to 1 or more classes of antifungal drugs [14,20] However, other studies have noted that C. auris is less resistant to 5-fluorocytosine and caspofungin.[21]
Whole genome sequencing has identified geographically distinct C. auris genotypes thus suggesting the region-specific resistance and transmission patterns. [22] Therefore, the multidrug resistance of C. auris are geographically expressed as thus: Clade 1: South Asian; Clade II: East Asian; Clade III: African; Clade IV: South American and recently, Clade V: Iranian.[23] Although the clades are attributed to specific geographical locations, a mixed isolates may be found in a single location[22,24] Accordingly, a study has documented trans-border importation of C. auris by patients with recent exposure to healthcare in another country where C. auris has been reported. [8]
It is difficult to identify C. auris using the traditional fungal identification methods, [25] and can lead to wrongful identification. [9,25] Owing to their close genetic relatedness, as a haploid fungal specie, C. auris is often reported as C. haemulonii [26,27] while using conventional identification systems like APIC20C, Vitek2YST and BD Phoenix, [28] and, as C. parapsilosis using the RapiID[29] thus, necessitating additional testing methods with higher specificity to elicit species identification.[30,31] A mis-identification of C. auris can potentially result in incorrect treatment or delay of proper treatment with increasing chances of fatalities. [32]
Similarly, there are currently no established C. auris-specific susceptibility breakpoints, but clinicians often rely on their expert opinion and previously established breakpoints for other related Candida species. Currently, there is no evidence of relationship between microbiologic breakpoints and clinical outcomes. [33]
Furthermore, some of the epidemiological distinctiveness of C. auris include its swift transmission,[34] and its resistance to conventional disinfectants. [35,36]. Unfortunately, Candida auris is considered among the most virulent environmental pathogens that are associated with hospital transmission.[13] It can survive on surfaces for a prolonged period.[1]Also, a recent isolation of C. auris from a natural aquatic habitat in India indicates that this fungus may also exist without a human host.[37]
As C. auris is fast spreading within healthcare settings, it has become imperative to monitor its virulence and devise appropriate treatment approaches [9] in view of the several hospital-associated transmissions reported globally.[38,39,40] Therefore, an early detection and implementation of infection control practices can potentially reduce the risks. [18,35] Consequently, understanding its epidemiology can significantly help in planning specific infection control measures for healthcare settings.[41,42] Accordingly, this study aims to provide a descriptive overview on the occurrence of C. auris in the hospital since its initial detection in late 2019.
2. Methodology
This is a retrospective study of patients had been reported with C. auris at a tertiary healthcare institution during the period from Nov 2020 to the end of 2022. It was during this period that the hospital started recording additional C. auris cases (after our first case in November 2019), and specific infection prevention and control measures were adapted and implemented to minimize hospital associated transmissions within the hospital.
2.1. Data Collection
Although no patient identifiable data is used for the reporting, an Institutional Review Board Approval No. No. 22/0701/IRB was obtained before proceeding with the research. The ethical approval required us to abide by the rules and regulations of the Kingdom of Saudi Arabia and the research policies and procedures of the KSU IRB related to data privacy.
Accordingly, all data are mined from the hospital’s electronic health information system (eSIHI) after properly anonymizing, i.e., after removing the patient’s medical record number, national identification number, nationality, names and any other patient identifiers. Data on patients' demographic information, baseline features, comorbidity, laboratory results, and clinical outcome were then compiled in an Excel worksheet and analysed after reviewing the electronic patient records.
2.2. Specimen Sampling
All C. auris strains identified in the lab throughout the research period from both clinical and surveillance screening samples were included. For the purpose of inclusion, all active surveillance samples, all contact tracing samples and all clinical samples are considered. Surveillance samples include those taken when it is determined that the risk factors for colonization or infection exists, or if an inpatient is included as a contact of a positive case (as part of contact tracing). See Table 1 for the list of risk factors included. Active surveillance samples taken include nasal, axilla, groin, wounds, indwelling device sites etc. Additionally, based on clinical assessment other sites were potentially included like the anus, chronic wounds, blood, urine, wound, tissue, drains etc. For the purpose of the study, only the first positive isolate per patient was included.
2.3. Testing and Identification
Surveillance swabs were cultured on Sabouraud dextrose agar with chloramphenicol and incubated at 37 C° for 48 hours. Any growth of yeast from surveillance samples underwent identification. Additionally, significant growth of yeast from clinical samples (e.g., blood, urine, wound etc.) was identified. Yeast identification from surveillance and clinical samples was done using the matrix assisted laser desorption ionization time of flight mass spectrometry (biomerieux, Marcy-l'Étoile, France).
2.4. Determining Hospital Associated Transmission
And, for the purpose of determining if a C. auris isolate is to be considered hospital or community acquired, the study adopted the epidemiological definition of hospital acquired infections coined by the National Health Safety Network of the USA.[43] The Network considers as hospital acquired, any infection that is determined not to be “present on admission (POA)”.
An infection is considered as POA if an element of the specific infection criterion manifests during the POA window period i.e., 2 days prior to an inpatient admission, on admission date, and the calendar day after admission. In other words, if an element (sign, or symptom) occur after the second calendar date, it is considered as hospital acquired infection.
And therefore, if a sample is taken after the second calendar date of admission and the patient did not exhibit any symptom before the third calendar date, the isolate is considered as being hospital acquired.
2.5. Statistical Analysis
Statistical analysis was done by SPSS version 28 (IBM Co., Armonk, NY, USA). The inclusion criteria for the multivariable analysis is based an epidemiological criterion derived from the risk factors identified and selected, the patient’s demographic information, and the outcome of the disease. The study then expresses categorical data in a form of frequency and percentage (%), with statistical significance is noted where a two-tailed P value is < 0.05.
3. Results
A total of 53 patients (33 males and 20 females) with C. auris were included in this study. Urine specimens were the most frequently obtained sample in 30.2% of patients followed by axilla from 11.3% then thigh and anal specimens, each from 9.4%. Samples labeled as buttocks and hip are lumped with that of the thigh, the proportion of sample source for the thigh would be 18.8% (n/10) second highest to the urine samples.
3.1. Prevalence: Age
The median age of screened patients was 64 years (inter-quartile range (IQR) 15 – 98). A further analysis of C. auris incidence by age (Table 2) showed a drastic increase in the incidence of C. auris among patients aged 51 years and above with a stair-case raise with every new decade of age above 51.
3.2. Prevalence: Patient Characteristics
Additionally, most patients (83%) had comorbidities, while half (50.9%) of them having been previously admitted to other hospitals. Other risk factors include admission to high-risk units (35.8%), wounds, and indwelling devices respectively in 34% and 32.1% as summarized in Table 3.
3.3. Prevalence: Hospital versus Community-Acquired C. auris
Out of the 53 isolates identified in the study, only one meets the epidemiological definition of hospital-acquired C. auris infection/colonization. In other words, as per the NHSN surveillance definition of hospital-acquired infections alluded to in the methodology section, all but one was identified as being POA during active surveillance screening.[43] One case, considered as hospital acquired, was on admission for longer than one week when his condition worsened and a clinical sample tested positive.
3.4. Prevalence: Infection versus Colonization
Out of the 53 isolates included in this study, seven (7) cases as their clinical specimens were taken when the patient’s condition worsened and required ICU admission. Four (4), out of the seven that required ICU admissions, developed C. auris candidemia. Therefore, out of the total of 53 cases, 4 are considered as C. auris infections and the remaining 49 are considered as colonization.
3.5. Prevalence: Clinical versus Surveillance samples
Our sample size includes 7 clinical samples and 46 active surveillance samples. This explains the vigor with which we have endeavored to identify all possible patients that are a risk of C. auris infection/colonization for the purpose of proactively identifying and isolating all positive cases. The proportions of clinical versus surveillance samples could, respectively, identify already sick (potentially infected) patients who are not necessarily sick, but maybe colonized and picked during the surveillance sampling. This could be useful in distinguishing our prevalence from other comparable hospitals. For instance, in a recent Saudi Arabian study[11] where 27 patients with invasive candidemia were studied for their risk factors and mortality, their prevalence cannot be compared with ours as we had a greater number of colonized patients and only one infected patient.
4. Discussion
Our study's strength, however, comes from the fact that it is the first in Saudi Arabia to give verifiable proof of the prevalence of this infamous yeast in hospital settings. It seems evident our findings echo conclusions from several other studies that C. auris is already prevalent across the globe, although in different proportions. For instance, a systematic review by [44] has shown that, from January 2019 to January 2021, several countries, including those in the Middle East have reported a significant number of C. auris. From data collected from nine studies, they reported a number of cases from several countries; Kuwait: 71[45], Oman: 29 (from two separate studies) [46] and [47] Saudi Arabia: 35, Spain: 47 [48], Mexico: 12 [49] Kenya [50], and the USA: 47 (from two studies) [51] and [52] The totals shown here included both C. auris candidemia and colonisations.
Most of the patients (clinical and active surveillance) from which C. auris confirmed samples were retrieved were males (33;62%) (Table 2). This is consistent with the findings of a retrospective analysis of the clinical characteristics of C. auris infection worldwide from 2009 to 2020.[42] and another study where 62% of the patients were male.[53]
The first three cases of C. auris were reported in Saudi Arabia in the year 2018 [54] and subsequently reported in other parts of the Kingdom [55,56,57] The United Arab Emirates, too, reported its first case of C. auris candidemia in the same year as with the Kingdom of Saudi Arabia.[58] Six other Middle Eastern countries also followed suit. All of those patients, all adults, were also initially misdiagnosed as c. haemulonii were. [28]
It is noteworthy that the first case of C. auris was reported in our health facility in late November of 2019, and our prevention and control measures were overshadowed by the declaration of COVID-19 as a global pandemic in March, 2020.[59] A number of factors have complicated the treatment of COVID-19 co-infecting with C. auris during the COVID-19 pandemic. Such factors include the multi-drug resistant nature of C. auris, their shared risk factors including co-morbidities, immunosuppressive states, and mechanical ventilator dependent states. [60] Therefore superimposed C. auris infection in a COVID-19 patient could exacerbate the severity of secondary comorbidities, including severe lung injury, acute respiratory distress syndrome (ARDS) and heighten mortality rates among critically ill patients.[61,62] Another similarity between the two pathogens is that they are both found on patient care environmental surfaces e.g., floors and air ducts making transmission among ventilated patients easy.[63]
During the first 6 months of the study period (November 2019 to April 2021), 4 (active infections and/or active surveillance) cases were reported. However, through the remaining three-quarters of the year 2021, there were between 1-3 cases reported monthly. This could be associated with the optimization of the C. auris identification and control measures during the period. March 2022 marked the peak of the graph with 9 cases being reported. This period marked a massive active surveillance screening of many patients that had unprotected contact with an index C. auris-positive patient. There was then a steady stair-case increase in cases? from June to September 2022 until it final declined to zero in December 2022. See Figure 1
As shown inTable 2, the incidence of C. auris according to age which has shown that there was a sharp rise in the incidence from the age of 51 and above. There was also a staircase-fashioned increase by each decade from the attainment of the golden jubilee and beyond. This is consistent with the findings in other reports where nearly half of the cases were around the age of 70 years.[64,65]. A similar Omani study has shown that out of 108 patients, 40 (37%) were >65 years of age.[66] However, a South African study that compared, among others, the age distribution of patients with candidemia caused by C. auris with other candida species, has shown the incidence is highest among neonates, followed by those in the 40-70 years age bracket, but lowest in the 10 – 20 years age range.[67] However, as opposed to our findings, there was a steady decline in the rates with the advance in each decade of age from 50 years. The bottom line would seem to be that extremes of age are a significant risk factor for C. auris.
Among the samples taken with positive results for C. auris, our study showed that urine samples yielded the highest number of cases (30.2%), followed by samples taken from the thigh, buttock, and hip, clumped together (18.8%), axilla (11.3%) and others taking the remaining balance. There was only one case of candidemia reported. Most samples (n=?) were taken during enhanced active surveillance rather than as diagnostic samples in suspected clinical infections (Table 2).
Although the first case of C. auris was found in Japan from the ear, thus the name, auris.[2] it has since been found in different parts of the body. In a study of 108 clinical samples with C. auris isolates, the most common sample was blood (38.9%), urine (36.3%), respiratory (8%), central line tip (8%), wound (6.2%), and other samples (2.6%).[66] It has also been found in bronchoalveolar lavage, [68] diabetic foot tissue culture, etc., [69] that is consistent with findings in several other studies of clinical samples. [70] It is noteworthy that their study involved a majority of clinical samples taken from sick patients while our study includes a majority of surveillance samples with quite a few clinical samples. Although they are distinctively different classes of microbes, C. auris cases are similar to MDROs in their risk factors, environmental source, and mode of transmission and, patients infected with C. auris are often co-infected with other MDROs. [8,71]
As shown in Table 3, a review of the patient’s characteristics revealed that all of the reported cases (100%) had at least one risk factor, similar to findings in other studies where 98.1% had at least a risk factor.[66] Also, 83% of our studied patients had some co-morbidities that include chronic kidney diseases, septicemia, diabetes mellitus, or chronic lung disease. As reported in the results, 50.9% had been admitted to other hospitals, while admission to a high-risk unit followed with 35.8%. Patients with wounds constituted 34% and those with devices were 32.1%. Devices implicated include urinary catheters, central venous catheters, and mechanical ventilator. Our findings seem to reiterate the findings of other studies. In an Omani study, 68.5% had comorbidities[66] while a New York study showed that extensive healthcare exposure and underlying comorbidities constituted significant risk factors in the reported cases.[65]
It is noteworthy that an alternative approach: multiparametric approach may have been successfully used in some research, e.g., to identify high-risk prostate cancer (with a Gleason score of at least 7) with better sensitivity and specificity than that provided by PSA screening alone.[72] However, our approach is to identify and isolate potentially infected or colonized patients based on epidemiological criteria for the purpose of early recognition and isolation, and not on clinical criteria for treatment purposes.
However, this study is not without limitations. Being the first study of its type within the Kingdom, and the lack of regional benchmark to compare our rates with, it is difficult to posit our prevalence rates in relative terms. Also, the use of risk factors for active surveillance screening might not be so specific as compared, for example, with a multiparametric approach. We might have overlooked a few situations.
The inherent risk of misdiagnosis or wrong identification could result in missing out on some potential cases of C. auris colonisations/infections. Although c. auris are properly identified, our hospital laboratory relied on the susceptibility of other candida species, or rely on expert opinion in deciding on appropriate antifungal treatment. This explains why we did not include the susceptibility results in our study.
C. auris is globally endemic and continues to spread within healthcare settings. Following our index case in November 2019, our enhanced active surveillance suggests that C. auris may be under-reported and its endemicity in the Kingdom more than what meets the eye. Enhanced active surveillance for C. auris and infection control measures could avert future nosocomial? outbreaks.
Author Contributions
Conceptualization, Sara Alsubaie; Methodology, Abba Amsami Elgujja and Lulwa Alabdan; Validation, Fatimah S. Alshahrani and Salah Ahmed Ezreqat; Investigation, Abba Amsami Elgujja; Resources, Sara Alsubaie; Writing – original draft, Abba Amsami Elgujja; Writing – review & editing, Abba Amsami Elgujja, Salah Ahmed Ezreqat, Ahmed M. Albarrag, Mazin Barry and Khalifa Bin Khamis; Supervision, Fatimah S. Alshahrani; Project administration, Fatimah S. Alshahrani.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of King Saud University College of Medicine (Ref. No. 22/0701/IRB of 20.09.2022).
Informed Consent Statement
Not applicable.
Data Availability Statement
Raw study data are not readily available online, but can be made available on request, following local regulations and policies.
Acknowledgments
The study team acknowledges the support it received from the College of Medicine, King Saud University, Professor Ahmed Hersi (CEO, KS-Medical City), Professor Jasser Alfauzi (CMO, KSU-Medical City) for their support and encouragement, and all staff of Infection Prevention and Control Staff of King Saud University Medical City for their invaluable contribution towards the success of the study.,.
Conflicts of Interest
The authors declare no conflict of interest.
References
- S. Vallabhaneni et al., “Investigation of the First Seven Reported Cases of Candida auris, a Globally Emerging Invasive, Multidrug-Resistant Fungus—United States, May 2013–August 2016,” American Journal of Transplantation, vol. 17, no. 1. Blackwell Publishing Ltd, pp. 296–299, Jan. 01, 2017. [CrossRef]
- K. Satoh, K. Makimura, Y. Hasumi, Y. Nishiyama, K. Uchida, and H. Yamaguchi, “Candida auris sp. nov., a novel ascomycetous yeast isolated from the external ear canal of an inpatient in a Japanese hospital,” Microbiol Immunol, vol. 53, no. 1, pp. 41–44, Jan. 2009. [CrossRef]
- S. R. Lockhart et al., “Simultaneous emergence of multidrug-resistant candida auris on 3 continents confirmed by whole-genome sequencing and epidemiological analyses,” Clinical Infectious Diseases, vol. 64, no. 2, pp. 134–140, 2017. [CrossRef]
- M. Biswal et al., “Controlling a possible outbreak of Candida auris infection: lessons learnt from multiple interventions,” Journal of Hospital Infection, vol. 97, no. 4, pp. 363–370, Dec. 2017. [CrossRef]
- M. A. Sayeed, J. Farooqi, K. Jabeen, S. Awan, and S. F. Mahmood, “Clinical spectrum and factors impacting outcome of Candida auris: A single center study from Pakistan,” BMC Infect Dis, vol. 19, no. 1, p. 384, Dec. 2019. [CrossRef]
- R. E. Magobo, C. Corcoran, S. Seetharam, and N. P. Govender, “Candida auris –Associated Candidemia, South Africa,” Emerg Infect Dis, vol. 20, no. 7, pp. 1250–1251, Jul. 2014. [CrossRef]
- D. A. Solomon, A. K. Nyerere, A. Kanyua, and C. W. Ngugi, “Prevalence, Species Distribution and Antifungal Susceptibility Profile of <i>Candida</i> Species Isolated from Bloodstream of Critical Care Unit Patients in a Tertiary Care Hospital in Kenya,” Open J Med Microbiol, vol. 11, no. 01, 2021. [CrossRef]
- H. F. Garcia-Jeldes et al., “Prevalence of Candida auris in Canadian acute care hospitals among at-risk patients, 2018,” Antimicrob Resist Infect Control, vol. 9, no. 1, 2020. [CrossRef]
- A. Sanyaolu et al., “Candida auris : An Overview of the Emerging Drug-Resistant Fungal Infection,” Infect Chemother, vol. 54, no. 2, p. 236, 2022. [CrossRef]
- Abdalhamid, R. Almaghrabi, S. Althawadi, and A. Omrani, “First report of Candida auris infections from Saudi Arabia,” Journal of Infection and Public Health, vol. 11, no. 4. Elsevier Ltd, pp. 598–599, Jul. 01, 2018. [CrossRef]
- R. Kaki, “Risk factors and mortality of the newly emerging Candida auris in a university hospital in Saudi Arabia,” Mycology, pp. 1–8, Jun. 2023. [CrossRef]
- M. B. Alashqar, L. Alabdan, M. Khan, A. H. Almakadma, and S. Almustanyir, “A Case Report of a Candida auris Infection in Saudi Arabia,” Cureus, May 2021,. [CrossRef]
- R. Sabino, C. Veríssimo, Á. A. Pereira, and F. Antunes, “Candida auris, an agent of hospital-associated outbreaks: Which challenging issues do we need to have in mind?,” Microorganisms, vol. 8, no. 2. 2020. [CrossRef]
- H. Du, J. Bing, T. Hu, C. L. Ennis, C. J. Nobile, and G. Huang, “Candida auris: Epidemiology, biology, antifungal resistance, and virulence,” PLoS Pathog, vol. 16, no. 10, 2020. [CrossRef]
- R. S. Almaghrabi et al., “Molecular characterisation and clinical outcomes of Candida auris infection: Singlecentre experience in Saudi Arabia,” Mycoses, vol. 63, no. 5, pp. 452–460, May 2020. [CrossRef]
- S. S. Ilan and Tanis C. Dingle, “Candida auris,” CMAJ, vol. 191, no. E865, Aug. 2019, Accessed: Jul. 02, 2023. [Online]. Available: https://www.cmaj.ca/content/cmaj/191/31/E865.full.pdf.
- J. de Cássia Orlandi Sardi, D. R. Silva, M. J. Soares Mendes-Giannini, and P. L. Rosalen, “Candida auris: Epidemiology, risk factors, virulence, resistance, and therapeutic options,” Microbial Pathogenesis, vol. 125. Academic Press, pp. 116–121, Dec. 01, 2018. [CrossRef]
- K. Vinayagamoorthy, K. C. Pentapati, and H. Prakash, “Prevalence, risk factors, treatment and outcome of multidrug resistance Candida auris infections in Coronavirus disease (COVID-19) patients: A systematic review,” Mycoses, vol. 65, no. 6. 2022. [CrossRef]
- S. Mahmoudi, K. Ahmadikia, M. Kord, A. Ahmadi, and S. Khodavaisy, “Candida auris, an emerging fungal pathogen,” Journal of Mazandaran University of Medical Sciences, vol. 29, no. 172, 2019. [CrossRef]
- M. Kordalewska and D. S. Perlin, “Identification of drug resistant candida auris,” Frontiers in Microbiology, vol. 10, no. AUG. Frontiers Media S.A., 2019. [CrossRef]
- M. G. Frías-De-león et al., “Antifungal resistance in Candida auris: Molecular determinants,” Antibiotics, vol. 9, no. 9. 2020. [CrossRef]
- Narayanan, P. Selvakumar, R. Siddharthan, and K. Sanyal, “ClaID: a Rapid Method of Clade-Level Identification of the Multidrug Resistant Human Fungal Pathogen Candida auris,” Microbiol Spectr, vol. 10, no. 2, Apr. 2022. [Google Scholar] [CrossRef]
- N. A. Chow, T. de Groot, H. Badali, M. Abastabar, T. M. Chiller, and J. F. Meis, “Potential Fifth Clade of Candida auris, Iran, 2018,” Emerg Infect Dis, vol. 25, no. 9, pp. 1780–1781, Sep. 2019. [CrossRef]
- D. G. De Luca et al., “Four genomic clades of Candida auris identified in Canada, 2012–2019,” Med Mycol, vol. 60, no. 1, Jan. 2022. [CrossRef]
- S. Tsay, A. Kallen, B. R. Jackson, T. M. Chiller, and S. Vallabhaneni, “Approach to the Investigation and Management of Patients with Candida auris, an Emerging Multidrug-Resistant Yeast,” Clinical Infectious Diseases, vol. 66, no. 2, pp. 306–311, Jan. 2018. [CrossRef]
- A. Cortegiani, G. Misseri, T. Fasciana, A. Giammanco, A. Giarratano, and A. Chowdhary, “Epidemiology, clinical characteristics, resistance, and treatment of infections by Candida auris,” Journal of Intensive Care, vol. 6, no. 1. BioMed Central Ltd., p. 69, Oct. 29, 2018. [CrossRef]
- H. Du, J. Bing, T. Hu, C. L. Ennis, C. J. Nobile, and G. Huang, “Candida auris: Epidemiology, biology, antifungal resistance, and virulence,” PLoS Pathog, vol. 16, no. 10, p. e1008921, Oct. 2020. [CrossRef]
- W. Alfouzan, R. Dhar, A. Albarrag, and H. Al-Abdely, “The emerging pathogen Candida auris: A focus on the Middle-Eastern countries,” Journal of Infection and Public Health, vol. 12, no. 4. Elsevier Ltd, pp. 451–459, Jul. 01, 2019. [CrossRef]
- M. Snayd, F. Dias, R. W. Ryan, D. Clout, and D. B. Banach, “Misidentification of Candida auris by RapID yeast plus, a commercial, biochemical enzyme-based manual rapid identification system,” Journal of Clinical Microbiology, vol. 56, no. 5. 2018. [CrossRef]
- R. M. Welsh et al., “Survival, Persistence, and Isolation of the Emerging Multidrug-Resistant Pathogenic Yeast Candida auris on a Plastic Health Care Surface,” J Clin Microbiol, vol. 55, no. 10, p. 2996, Oct. 2017. [CrossRef]
- W. Alfouzan, R. Dhar, A. Albarrag, and H. Al-Abdely, “The emerging pathogen Candida auris: A focus on the Middle-Eastern countries,” Journal of Infection and Public Health, vol. 12, no. 4. Elsevier Ltd, pp. 451–459, Jul. 01, 2019. [CrossRef]
- S. Chatterjee, S. V. Alampalli, R. K. Nageshan, S. T. Chettiar, S. Joshi, and U. S. Tatu, “Draft genome of a commonly misdiagnosed multidrug resistant pathogen Candida auris,” BMC Genomics, vol. 16, no. 1, 2015. [CrossRef]
- “Antifungal Susceptibility Testing and Interpretation | Candida auris | Fungal Diseases | CDC.” Accessed: May 31, 2023. [Online]. Available: https://www.cdc.gov/fungal/candida-auris/c-auris-antifungal.html.
- S. Tsay, A. Kallen, B. R. Jackson, T. M. Chiller, and S. Vallabhaneni, “Approach to the Investigation and Management of Patients with Candida auris, an Emerging Multidrug-Resistant Yeast,” Clinical Infectious Diseases, vol. 66, no. 2, pp. 306–311, Jan. 2018. [CrossRef]
- D. H. Caceres et al., “Candida auris: A review of recommendations for detection and control in healthcare settings,” Journal of Fungi, vol. 5, no. 4. MDPI AG, Dec. 01, 2019. [CrossRef]
- T. S. N. Ku, C. J. Walraven, and S. A. Lee, “Candida auris: Disinfectants and Implications for Infection Control,” Front Microbiol, vol. 9, Apr. 2018. [CrossRef]
- P. Arora et al., “Environmental Isolation of Candida auris from the Coastal Wetlands of Andaman Islands, India,” mBio, vol. 12, no. 2, Apr. 2021. [CrossRef]
- F. Visan et al., “ First Candida auris Outbreak Experience in a Tertiary-Care General Hospital in Qatar, 2019,” Infect Control Hosp Epidemiol, vol. 41, no. S1, 2020. [CrossRef]
- M. Theut et al., “The first two cases of Candida auris in Denmark,” Ugeskr Laeger, vol. 184, no. 16, 2022.
- S. Schelenz et al., “First hospital outbreak of the globally emerging Candida auris in a European hospital.,” Antimicrob Resist Infect Control, vol. 5, no. 1, p. 35, Oct. 2016. [CrossRef]
- J. O. KIM, K. H. ST. JOHN, and S. E. COFFIN, “Epidemiology and Infection Prevention and Control,” in Pediatric Infectious Diseases, 2008. [CrossRef]
- S. Hu et al., “Retrospective Analysis of the Clinical Characteristics of Candida auris Infection Worldwide From 2009 to 2020,” Front Microbiol, vol. 12, 2021. [CrossRef]
- CDC, Ncezid, and DHQP, “Identifying Healthcare-associated Infections (HAI) for NHSN Surveillance,” 2023, Accessed: Jun. 01, 2023. [Online]. Available: https://www.cdc.gov/nhsn/pdfs/pscmanual/2psc_identifyinghais_nhsncurrent.pdf.
- S. Ahmad and W. Alfouzan, “Candida auris: Epidemiology, diagnosis, pathogenesis, antifungal susceptibility, and infection control measures to combat the spread of infections in healthcare facilities,” Microorganisms, vol. 9, no. 4. 2021. [CrossRef]
- W. Alfouzan et al., “Molecular epidemiology of candida auris outbreak in a major secondary-care hospital in Kuwait,” Journal of Fungi, vol. 6, no. 4. 2020. [CrossRef]
- A. Al Maani et al., “Ongoing challenges with healthcare-associated candida auris outbreaks in Oman,” Journal of Fungi, vol. 5, no. 4, 2019. [CrossRef]
- J. Mohsin et al., “A Cluster of Candida auris Blood Stream Infections in a Tertiary Care Hospital in Oman from 2016 to 2019.,” Antibiotics (Basel), vol. 9, no. 10, pp. 1–11, Sep. 2020. [CrossRef]
- J. V. Mulet Bayona et al., “Characteristics and management of candidaemia episodes in an established candida auris outbreak,” Antibiotics, vol. 9, no. 9. 2020. [CrossRef]
- H. Villanueva-Lozano et al., “Outbreak of Candida auris infection in a COVID-19 hospital in Mexico,” Clinical Microbiology and Infection, vol. 27, no. 5. 2021. [CrossRef]
- P. S. Shastri, S. A. Shankarnarayan, J. Oberoi, S. M. Rudramurthy, C. Wattal, and A. Chakrabarti, “Candida auris candidaemia in an intensive care unit – Prospective observational study to evaluate epidemiology, risk factors, and outcome,” J Crit Care, vol. 57, 2020,. [CrossRef]
- K. Arensman et al., “Clinical Outcomes of Patients Treated for Candida auris Infections in a Multisite Health System, Illinois, USA,” Emerg Infect Dis, vol. 26, no. 5. 2020. [CrossRef]
- C. Prestel et al., “ Candida auris Outbreak in a COVID-19 Specialty Care Unit — Florida, July–August 2020 ,” MMWR Morb Mortal Wkly Rep, vol. 70, no. 2, 2021,. [CrossRef]
- K. Etienne et al., “Epidemiology and Whole Genome Sequence Typing of Globally Emerging, Multidrug-Resistant Candida auris,” Open Forum Infect Dis, vol. 3, no. suppl_1, Dec. 2016. [CrossRef]
- B. Abdalhamid, R. Almaghrabi, S. Althawadi, and A. Omrani, “First report of Candida auris infections from Saudi Arabia,” Journal of Infection and Public Health, vol. 11, no. 4. Elsevier Ltd, pp. 598–599, Jul. 01, 2018. [CrossRef]
- A. Elsawy, K. Alquthami, N. Alkhutani, D. Marwan, and A. Abbas, “The second confirmed case of Candida auris from Saudi Arabia,” Journal of Infection and Public Health, vol. 12, no. 6. Elsevier Ltd, pp. 907–908, Nov. 01, 2019. [CrossRef]
- R. AlJindan, D. M. AlEraky, N. Mahmoud, S. AbdulAzeez, and J. F. Borgio, “Emergence of multi-drug resistance Candida auris in Saudi Arabia,” Jun. 2020. [CrossRef]
- M. M. Alshamrani et al., “Management of Candida auris outbreak in a tertiary-care setting in Saudi Arabia,” Infect Control Hosp Epidemiol, 2020. [CrossRef]
- A. Alatoom et al., “Persistent candidemia despite appropriate fungal therapy: First case of Candida auris from the United Arab Emirates,” International Journal of Infectious Diseases, vol. 70, pp. 36–37, May 2018. [CrossRef]
- “WHO Director-General’s opening remarks at the media briefing on COVID-19 - 11 March 2020.” Accessed: Jul. 03, 2023. [Online]. Available: https://www.who.int/director-general/speeches/detail/who-directorgeneral- s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020.
- H. Najeeb et al., “The Menace of Candida auris Epidemic Amidst the COVID-19 Pandemic: A Systematic Review,” Diseases, vol. 10, no. 3, p. 58, Aug. 2022. [CrossRef]
- D. Lin et al., “Co-infections of SARS-CoV-2 with multiple common respiratory pathogens in infected patients,” Sci China Life Sci, vol. 63, no. 4, pp. 606–609, Apr. 2020. [CrossRef]
- A. Chowdhary, B. Tarai, A. Singh, and A. Sharma, “Multidrug-resistant candida auris infections in critically Ill Coronavirus disease patients, India, April–July 2020,” Emerg Infect Dis, vol. 26, no. 11, pp. 2694–2696, Nov. 2020. [CrossRef]
- A. Chowdhary and A. Sharma, “The lurking scourge of multidrug resistant Candida auris in times of COVID-19 pandemic,” J Glob Antimicrob Resist, vol. 22, pp. 175–176, Sep. 2020. [CrossRef]
- N. Pandya et al., “International Multicentre Study of Candida auris Infections,” Journal of Fungi, vol. 7, no. 10, p. 878, Oct. 2021. [CrossRef]
- K. Southwick et al., “A description of the first Candida auris-colonized individuals in New York State, 2016-2017,” Am J Infect Control, vol. 50, no. 3, pp. 358–360, Mar. 2022. [CrossRef]
- A. Al-Rashdi, A. Al-Maani, A. Al-Wahaibi, A. Alqayoudhi, A. Al-Jardani, and S. Al-Abri, “Characteristics, risk factors, and survival analysis of candida auris cases: Results of one-year national surveillance data from oman,” Journal of Fungi, vol. 7, no. 1. 2021. [Google Scholar] [CrossRef]
- E. van Schalkwyk et al., “Epidemiologic Shift in Candidemia Driven by Candida auris, South Africa, 2016–20171,” Emerg Infect Dis, vol. 25, no. 9, pp. 1698–1707, Sep. 2019. [CrossRef]
- X. Wang et al., “The first isolate of Candida auris in China: Clinical and biological aspects article,” Emerg Microbes Infect, vol. 7, no. 1. 2018. [CrossRef]
- M. V. Moreno et al., “First isolation de Candida auris in Chile,” Revista Chilena de Infectologia, vol. 36, no. 6. 2019. [CrossRef]
- F. Allaw et al., “First candida auris outbreak during a covid-19 pandemic in a tertiary-care center in Lebanon,” Pathogens, vol. 10, no. 2021. [CrossRef]
- E. J. Zasowski et al., “ 289. International Validation of a Methicillin-Resistant Staphylococcus aureus (MRSA) Risk Assessment Tool for Acute Bacterial Skin and Skin Structure Infections (ABSSSI) ,” Open Forum Infect Dis, vol. 5, no. suppl_1, 2018. [CrossRef]
- B. T. Helfand, C. A. Conran, J. Xu, and W. J. Catalona, “A multiparametric approach to improve upon existing prostate cancer screening and biopsy recommendations,” Curr Opin Urol, vol. 27, no. 5, pp. 475– 480, Sep. 2017. [CrossRef]
Figure 1.
Histogram of C. auris rates 2020-2022.
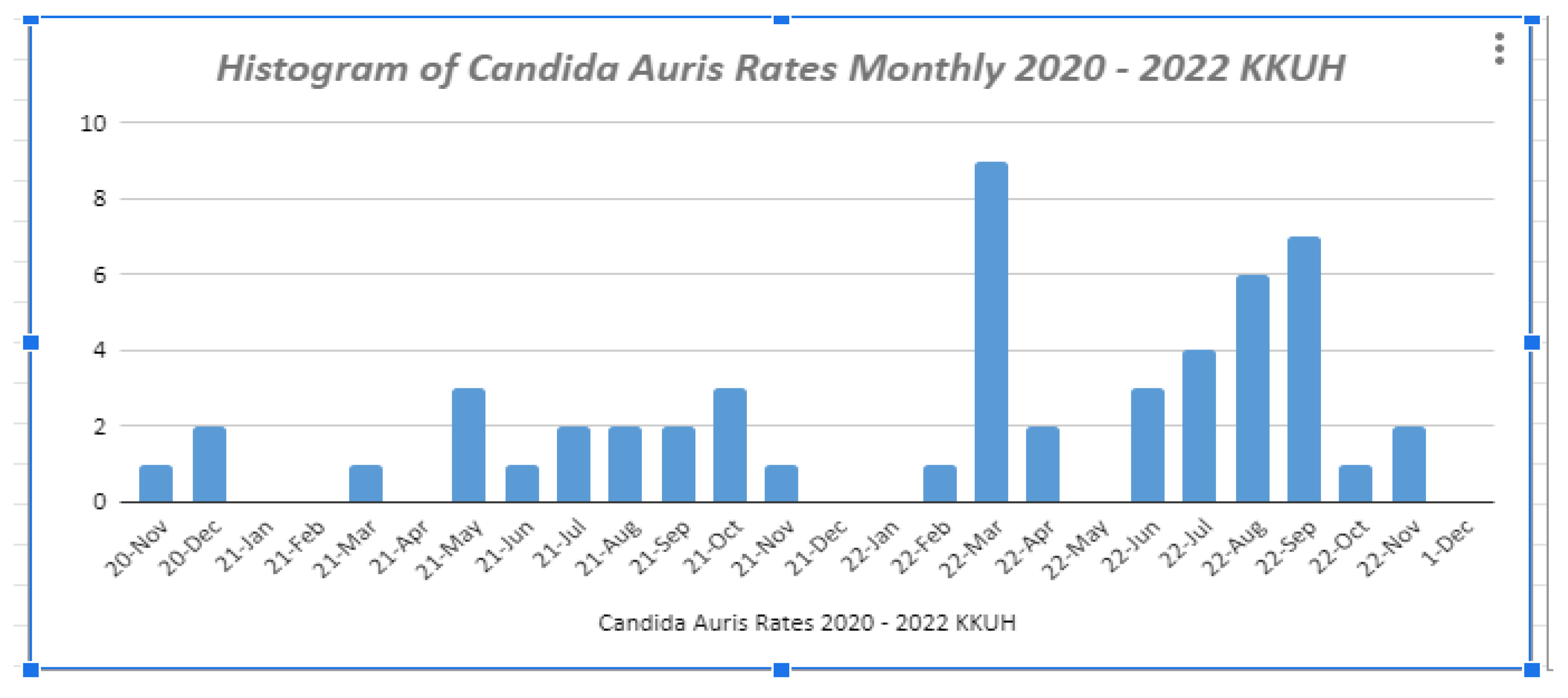

Table 1.
Risk Factors for C. auris.
| Bundle Element/Risk Factor | Score |
| History of Admission from other hospital, | 3 |
| Has any of these: Septicaemia + CKD, DM, or chronic lung disease | 1 |
| Previous history of MDRO infection or colonization | 1 |
| History of admission in hospital outside the KSA (within the past 12 months) | 1 |
| Presence of wounds or indwelling devices, | 1 |
| Admission to high risk units (ICU, HDU, Oncology etc) | 1 |
| Contact of MDRO / ASC | 1 |
| Previous surgery < 3 months | 1 |
HDU: High dependency unit; ICU: intensive care unit; ASC: active surveillance culture; KSA: Kingdom of Saudi Arabia.
Table 2.
Patients’ characteristics (n=53).
| N | % | |
| Age (years) | ||
| ≤20 | 2 | 3.8 |
| 21-30 | 4 | 7.5 |
| 31-40 | 3 | 5.7 |
| 41-50 | 2 | 3.8 |
| 51-60 | 13 | 24.5 |
| 61-70 | 14 | 26.4 |
| ≥71 | 15 | 28.3 |
| Gender | ||
| Male | 33 | 62.3 |
| Female | 20 | 37.7 |
| Specimen | ||
| Urine | 16 | 30.2 |
| Axilla | 6 | 11.3 |
| Thigh | 5 | 9.4 |
| Anus | 5 | 9.4 |
| Arm | 4 | 7.5 |
| Swab | 3 | 5.7 |
| Penis | 3 | 5.7 |
| Hip | 3 | 5.7 |
| Nose | 2 | 3.8 |
| Buttock | 2 | 3.8 |
| Leg | 2 | 3.8 |
| Neck | 2 | 3.8 |
| Nasal | 2 | 3.8 |
| Tissue | 1 | 1.9 |
| Wound | 1 | 1.9 |
| Nail | 1 | 1.9 |
| Rectal | 1 | 1.9 |
| Blood | 1 | 1.9 |
| Foot | 1 | 1.9 |
Table 3.
Patients’ Characteristics.
| N | % | 95% CI of rate | |
| Comorbidities | 44 | 83 | 60.3 to 111.5 |
| Admission to other hospital | 27 | 50.9 | 33.6 to 74.1 |
| High Risk Areas | 19 | 35.8 | 21.6 to 56 |
| Wounds | 18 | 34.0 | 20.1 to 53.7 |
| Devices | 17 | 32.1 | 18.7 to 51.4 |
| Antimicrobials | 12 | 22.6 | 11.7 to 39.6 |
| ASC | 11 | 20.8 | 10.4 to 37.1 |
| Surgeries | 7 | 13.2 | 5.3 to 27.2 |
| MDRO | 1 | 1.9 | 0.0 to 10.5 |
| Outside KSA | 0 | 0.0 | --- |
| Contact of MDRO | 0 | 0.0 | --- |
CI: Confidence interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



