
Submitted:
05 September 2023
Posted:
08 September 2023
You are already at the latest version
Abstract
The inaugural AIDS Program in Brazil was established in São Paulo in 1983, with the Instituto Adolfo Lutz appointed for laboratory assistance. Subsequently, research on HIV infections and HIV/HTLV (HIV/HTLV-1 and HIV/HTLV-2) co-infections were conducted. This narrative review focuses on studies from the Immunology Department (1983–2017) that significantly influenced AIDS diagnosis or provided epidemiological data such as prevalence rates, sex, age, and risk factors. Ten studies, encompassing over 8,000 individuals, are discussed. During 1983–1985, nearly all AIDS cases were attributed to homosexual/bisexual men aged 31 years old. Subsequently, heterosexual men and women emerged as risk groups owing to intravenous drug use (IDU) and/or unprotected sexual intercourse with AIDS patients or multiple partners per year. From 1985 onwards, vertical transmission led to child infections. HIV/HTLV co-infection rates decreased over time, initially associated with male IDU, and in the 2010s, with females, IDU, and individuals aged >40 years. Trends in HIV and HIV/HTLV co-infections among younger men and women (<30 years of age) were observed from 2015–2017. The changing characteristics and risk groups for HIV and HIV/HTLV co-infections over the years underscore the necessity for ongoing public policies to prevent retrovirus transmission, particularly among adolescents and young adults.
Keywords:
HIV
; HTLV-1
; HTLV-2
; sex
; risk factors
; prevalence
; co-infection
; public policies
1. Introduction
In June 1983, a group of homosexual intellectual men visited the Secretary of Health of the State of São Paulo, to request containment measures against a disease that had been reported in the United States of America (USA) and was beginning to emerge in Brazil [1] (p. 18). This disease was characterized by a profound immunosuppression due to a decrease in the number of lymphocytes, mainly the CD4+ T helper lymphocytes (former T4). The initial cases were reported in homosexual men in 1981, followed by reports in heterosexual men who were intravenous drug abusers (heroin), hemophiliacs, and Haitians [2,3,4,5,6]. Considering the epidemiological bulletins from the Centre for Disease Control and Prevention (CDC) in Atlanta, USA, which showed the widespread nature of the disease, it was termed Acquired Immunodeficiency Syndrome [6]. The acronym was officially adopted in the second half of 1982.
In São Paulo, Brazil, the Secretary of Health approved the first AIDS Program on 25 July 1983 [1] (p. 54) and designated the Instituto de Saúde as coordinator and the Public Health Laboratory - Instituto Adolfo Lutz (IAL) as the reference for laboratory support [1] (p. 55). The implementation of the AIDS Program took place in August 1983 [1] (p. 57), and the Immunology Department of IAL was tasked with analysing the cellular immune profile of suspected AIDS cases. [1] (p. 58). Notably, during this time, the etiological agent of AIDS had not yet been identified. The serology for the human immunodeficiency virus became available in Brazil by the end of 1985 and was made mandatory in São Paulo's blood banks in 1986 (Law No. 5,190, of 20 June 1986).
Interestingly, in 1980, a team led by Professor Robert Gallo in the USA discovered the first human T-lymphotropic retrovirus in patients suffering from leukemia/lymphoma. They named this virus human T-cell leukemia virus I (HTLV-I) [7]. Two years later, in 1982, the same team identified the second human retrovirus, HTLV-II, from a single case of hairy cell lymphoma [8].
In 1983, Françoise Barré-Sinoussi, a member of a research team led by Professor Luc Montagnier in France, isolated the first T-lymphotropic retrovirus from an AIDS-risk patient. The techniques used for this isolation were similar to those utilized for the detection of HTLV-I and HTLV-II. The patient, a homosexual man, presented with multiple lymphadenopathies, and the virus was isolated from his lymph node. This virus was subsequently named the lymphadenopathy associated virus (LAV) [9].
In 1984, Gallos’ team documented the identification, isolation, and ongoing propagation of cytopathic retroviruses (HTLV family) derived from the peripheral blood lymphocytes of numerous AIDS and pre-AIDS patients. These retroviruses were designated as HTLV-III, marking them as the third identified human retrovirus [10,11]. It was later established that LAV and HTLV-III were indeed the same retrovirus linked to AIDS. Consequently, in 1986, it was renamed as the human immunodeficiency virus (HIV).
Significantly, a consensus on the nomenclature of the HTLV family remains elusive. However, the prevalent and recommended terminology is ‘human T-lymphotropic virus’ followed by an Arabic numeral, such as HTLV-1 and HTLV-2 [12].
HIV, HTLV-1, and HTLV-2 share transmission routes, leading to co-infections that could influence the progression of associated diseases [13,14,15,16]. Distinct differences in endemic regions, risk factors and risk groups, and pathogenicity between HTLV-1 and HTLV-2 have been documented [17,18,19,20,21,22]. For example, HTLV-1 is endemic in Southwestern Japan, sub-Saharan Africa, South America (primarily Brazil), the Caribbean, and specific areas in the Middle East and Australo-Melanesia. It is linked to high morbidity and mortality owing to adult T-cell leukemia/lymphoma, HTLV-1-associated myelopathy (HAM), and other inflammatory disorders [17,18,21]. Conversely, HTLV-2 is hyperendemic among Amazonian Indians in Brazil, certain African pygmy tribes, and intravenous drug users (IDUs) in urban areas of the USA, Europe, and Latin America, including Brazil [19,20,21,22]. Unlike HTLV-1, HTLV-2 has not been associated with a specific disease, although sporadic cases of neurological disorders similar to HAM have been reported [21,22].
The Immunology Department at IAL began its research on HIV/AIDS in 1983, focusing on cellular immunity, diagnosis, and monitoring in both adults and children. In 1991, IAL launched studies on HIV/HTLV-1 and HIV/HTLV-2 co-infections, aiming to determine prevalence rates, affected sex, age, and risk groups susceptible to these retroviruses. This paper presented the most significant studies conducted from 1983 to 2017, discussed potential factors contributing to epidemiological changes, and suggested public policies necessary for controlling and preventing the transmission of these retroviruses.
2. Materials and Methods
2.1. Study design
This narrative review displays significant studies conducted by the Immunology Department of IAL from 1983–2017, which have left a mark on the history of HIV/AIDS in São Paulo, Brazil. The review included studies that provide epidemiological data on the overall prevalence rates of HIV/HTLV co-infections, segmented by sex, age, and risk groups associated with acquiring these retroviruses at specific points in time. Furthermore, it offers a comparative analysis of these epidemiological data over the years and discusses potential reasons for observed changes in the characteristics of infected individuals.
2.2. Data presentation and Statistical Analysis
Data was collected from the articles incorporated in this study and the author’s personal experience and archives. Tables were constructed and figures were displayed to aid in data visualization and analysis. In terms of cellular immunity assessment, all leucocyte, lymphocyte, lymphocyte subpopulation counts and lymphoproliferative responses to mitogens and antigens were presented as mean values. These were compared among groups using the Kruskal–Wallis variance analysis, supplemented with the Dunn multiple comparison test. Prevalence rates were determined by the total number of individuals with HIV/HTLV and separately with HIV/HTLV-1 and HIV/HTLV-2 co-infections at a specific point in time, divided by the total number of individuals examined. The Chi-square test was utilized for prevalence rate comparisons. A 5% level (p value ≤ 0.05) was considered significant for all statistical analyses.
2.3. Ethics approval
The IAL’s Research Ethics Committee, and when required, the Ethics Committee of collaborating institutions, granted approval for all primary studies discussed herein. The study adhered to the Declaration of Helsinki, with data presented in a blinded manner.
3. Results and Commentaries
3.1. Cellular immune profile in AIDS (1983–1985)
The Immunology Department at IAL conducted its inaugural study on AIDS, focusing on the cellular immune response in suspected cases. Briefly, between September 1983 and June 1985, 111 individuals who were part of the first AIDS Program in São Paulo, Brazil were referred to IAL for in vitro analyses of their cellular immune responses.
The counts of leucocytes, lymphocytes, T and B lymphocytes, as well as T4 (helper/inducer) and T8 (suppressor/cytotoxic) lymphocytes were ascertained. Subsequently, the T4/T8 ratio was computed. The lymphoproliferative response was also evaluated using T-cell mitogens (phytohaemagglutinin [PHA] and concanavalin A [Con-A]), T-dependent B-cell mitogen (pokeweed mitogen [PWM]), and the tuberculin purified protein derivative (PPD) antigen. All laboratory tests were conducted in accordance with the standardization of the Laboratory of Cellular Immunology and were performed blind, without knowledge of the demographic and clinical attributes of the study population.
At the end of 1985, we undertook a comparative analysis of our results with a CONTROL group. Collaborating with physicians from the Instituto de Saúde, we accessed epidemiological and clinical data. Patients were categorized into three groups: RISK (n=17), lymphadenopathy associated syndrome/AIDS related complex (LAS/ARC, n=37), and AIDS (n=47), based on the definitions provided by the CDC [6].
The RISK group comprised 23 homosexual/bisexual men and four heterosexual women, all of whom had contact with AIDS partners. The LAS/ARC group consisted of 36 homosexual/bisexual men and one heterosexual woman, all exhibiting persistent unexplained lymphadenopathy and other nonspecific clinical symptoms such as fever, malaise, diarrhoea, and weight loss. The AIDS group included patients suffering from opportunistic infections and/or Kaposi’s sarcoma, all of whom were homosexual/bisexual men. The CONTROL group included 11 lab staff members, consisting of five men and six women, all of whom were heterosexual.
No significant variation was found among the age groups, with a mean age of approximately 31 years. A comparison of the mean values for each laboratory test among the groups is presented in Table 1. The demographic and laboratory analyses led to the following conclusions: (i) Homosexual men constituted the population most affected by AIDS. (ii) The age group most impacted by the syndrome had a mean age of 31 years. (iii) The AIDS group exhibited leukopenia, lymphopenia, and a reduced count of T and B lymphocytes, a finding that was statistically significant when compared to other groups. (iv) A notable decrease in T4 lymphocytes was observed in the AIDS group, a difference that was statistically significant when compared to other groups. (v) The count of suppressor/cytotoxic T lymphocytes (T8) was significantly higher in the AIDS and ARC groups, a difference that was statistically significant when compared to other groups. (vi) A significant inversion of the T4/T8 ratio was detected in the AIDS and ARC groups, a difference that was significant when compared to other groups. (vii) The AIDS group showed decreased lymphoproliferative responses to PHA, Con-A, and PWM mitogens compared to other groups and diminished lymphoproliferative responses to PPD antigen in the AIDS and ARC groups when compared to the CONTROL group. (viii) A characteristic cellular immunological profile was established for AIDS cases. These findings were first presented in the author’s master's thesis on the cellular immune response in AIDS in Brazil and have since been published [23].
Significantly, the majority of this data was collected during a period when the aetiology of AIDS was yet to be determined and Brazil lacked access to HIV serological tests.

Table 1.
Number of peripheral blood lymphocytes and values of lymphoproliferative response using PHA, Con-A, PWM mitogens, and PPD antigen in CONTROL, RISK, LAS/ARC, and AIDS groups.
Table 1.
Number of peripheral blood lymphocytes and values of lymphoproliferative response using PHA, Con-A, PWM mitogens, and PPD antigen in CONTROL, RISK, LAS/ARC, and AIDS groups.
| GROUPS | ||||
|---|---|---|---|---|
| CONTROL (n=11) |
RISK (n=27) |
LAS/ARC (n=37) |
AIDS (n=47) |
|
| Age (years) | 30.4 | 30.7 | 31.9 | 30.8 |
| Leucocytes/mm3 | 5263.6 | 5955.6 | 5689.2 | 4763.8* |
| Lymphocytes/mm3 | 1967.6 | 2316.7 | 2264.2 | 1218.2* |
| T lymphocyte (%) | 64.0 | 64.8 | 62.2 | 52.1* |
| T lymphocytes/mm3 | 1247 | 1509.8 | 1403.9 | 662.3* |
| B lymphocytes (%) | 18.2 | 16.6 | 15.0 | 18.6 |
| B lymphocytes/mm3 | 397.3 | 362.7 | 307.6 | 214.4* |
| T4 (%) | 44.4 | 37.8 | 26.3 | 13.5* |
| T4/mm3 | 863 | 833.9 | 591.4 | 191.2* |
| T8 (%) | 21.6 | 26.6 | 37.3* | 39.0* |
| T8/mm3 | 451.9 | 620.2 | 797.6* | 550.7 |
| T4/T8 | 2.3 | 1.6 | 0.74* | 0.53* |
| PHA 20 µg/mL | 255979.7 | 233381.8 | 175852.9 | 118450.1* |
| Con-A 20 µg/mL | 172269.5 | 136493.3 | 111128.2 | 54795.5* |
| PWM 20 µg/mL | 75942.8 | 71469.8 | 27760.5 | 17930.1* |
| PPD 10 µg/mL | 59989.1 | 16696.0 | 15505.3* | 7098.8* |
The results for peripheral blood cells are presented as mean values of both percentage and absolute number. The lymphoproliferative response is expressed as mean counts per minute (cpm) following a 3-day culture with mitogens and a 7-day culture with PPD. Statistical significance was determined using the Kruskal-Wallis analysis of variance, supplemented by the Dunn multiple comparison test, with a significance level set at *p ≤ 0.05.
Following the publication, the Laboratory of Cellular Immunology sustained its support for the AIDS Program by quantifying CD4+ and CD8+ T cells until 1993. This 10-year period concluded when the immunofluorescence assay used for these analyses was outdated by flow cytometry, and the routine was transferred to another IAL laboratory. Significantly, in 1995, the CD4+/CD8+ network was established across the state of São Paulo, with numerous laboratories participating under the coordination of IAL.
3.2. HIV diagnosis in children (1989–1993)
Following the emergence of AIDS in São Paulo, Brazil, the demographics of HIV-infected individuals moved. An increasing number of women contracted the virus through IDU and unprotected sexual encounters with multiple partners or those with AIDS, particularly during their peak years of sexual and reproductive activity. This trend raised concerns owing to the potential for vertical transmission of AIDS to children, a fear that was subsequently realized.
Maternal antibodies against HIV cross the placenta during pregnancy and can be identified in the offspring from birth until 18 months of age. Consequently, HIV serology is not applicable for diagnosing HIV in children within this age range. Furthermore, in 1989, the polymerase chain reaction (PCR) for detecting HIV-RNA was unavailable in Brazil. Therefore, an alternative method for perinatal HIV diagnosis in children was necessary.
Considering the literature that highlights the polyclonal activation of B lymphocytes in HIV infection [24], along with the spontaneous secretion of HIV antibodies in the supernatant of prolonged lymphocyte cultures [25], we have developed an alternative method for use with children. This technique is referred to as in vitro induced antibody production (IVIAP) (Figure 1).
Figure 1.
In vitro induced antibody production (IVIAP) steps for detecting specific antibodies production by B lymphocytes in HIV-1 infected individuals.
Figure 1.
In vitro induced antibody production (IVIAP) steps for detecting specific antibodies production by B lymphocytes in HIV-1 infected individuals.
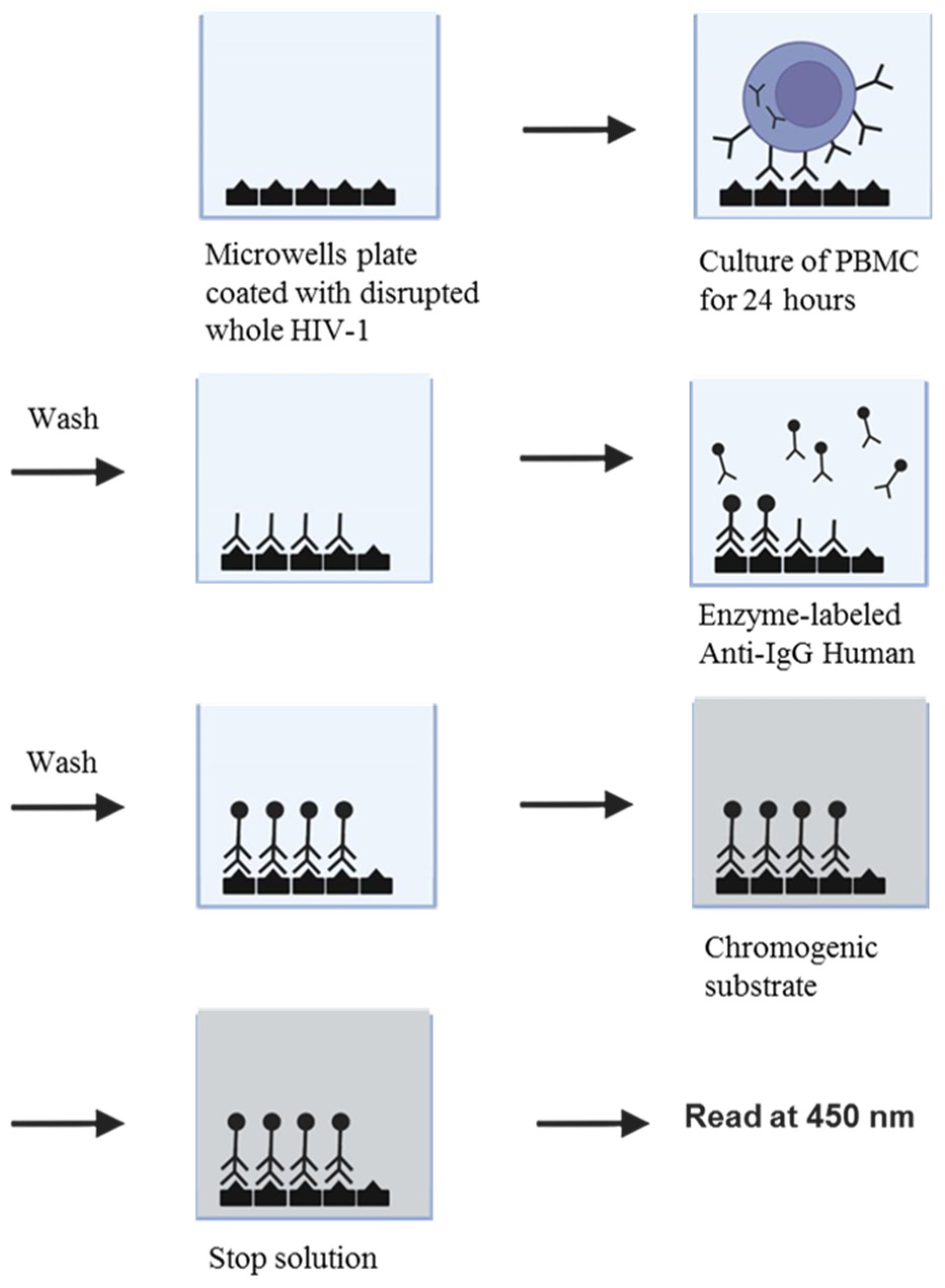
Briefly, we developed and standardized an assay for detecting HIV-specific antibodies with high sensitivity and specificity using a 24-h culture of peripheral blood mononuclear cells (PBMC) and a commercial enzyme immune assay (EIA) kit (EIA-LAV Genetic Systems, Seattle, USA). This kit contains disrupted inactivated whole virus adsorbed onto microwell plates as antigens. The assay can discriminate between antibodies present in plasma and those produced by B lymphocytes in both adults and children [26,27].
The IVIAP was subsequently utilized in a 2-year follow-up study of 57 children born to HIV-infected mothers. The results confirmed its applicability in diagnosing children older than 2 months. A comparative analysis of the IVIAP and PCR results, the latter conducted at the Istituto di Oncologia, Università degli Studi di Padova, Padova, Italy, showed concordance (PhD Thesis from the author, 1993). Most importantly, the IVIAP facilitated the adoption of three children who tested negative (one female and two male twins).
3.3. HIV/HTLV co-infections in patients attended by one Hospital of São Paulo (1991–1994)
In the 1990s, our research focused on identifying other human retroviruses (HTLV-1 and HTLV-2) in HIV patients referred to the Instituto de Infectologia Emílio Ribas (IIER) in São Paulo, a hospital recognized as a reference centre for HIV/AIDS. Concurrently, studies in the USA and Europe reported cases of HIV/HTLV-2 co-infection linked to IDU [20,28,29]. In São Paulo, we identified both HIV/HTLV-1 and HIV/HTLV-2 co-infections, predominantly in white and mixed-race individuals associated with IDUs [30,31]. This observation is likely attributable to Brazil being an endemic country for HTLV-1 and HTLV-2 [17,18,21,22] and São Paulo’s status as a cosmopolitan city attracting migrants and immigrants globally. In summary, the prevalence rate of HIV/HTLV co-infection in samples collected between 1991 and 1992 was 13.2% (7.9% for HIV/HTLV-1 and 5.3% for HIV/HTLV-2) (Table 2) [30], corroborating the prevalence rates detected at this point in time among IDUs from others parts of the world [29].
Table 2.
Prevalence rates and demographic characteristics among HIV-1 and HIV-1/HTLV-1 and HIV-1/HTLV-2 co-infected individuals sampled from 1991 to 2016.
Table 2.
Prevalence rates and demographic characteristics among HIV-1 and HIV-1/HTLV-1 and HIV-1/HTLV-2 co-infected individuals sampled from 1991 to 2016.
| Year of collection | Local/ Group |
Number of cases | Mean age (years) |
Sex (number) | HTLV-1/-2 (%) |
HTLV-1 (%) | HTLV-2 (%) | Ref |
|---|---|---|---|---|---|---|---|---|
| 1991–1992 | IIER, SP | 471 | M (406) F (65) | 62 (13.2) | 37 (7.9) | 25 (5.3) | [30] | |
| IDU | 216 | 29 | M (155) F (61) | 57 (26.4) | 33 (15.3) | 24 (11.1) | ||
| Homo/Bis | 229 | 34 | M (229) | 3 (1.3) | 2 (0.9) | 1 (0.4) | ||
| Othersa | 26 | 30 | M (22) F (4) | 2 (7.7) | 2 (7.7) | |||
| 1994 | IIER, SP | 553 | 32 | M (358) F (195) | 56 (10.1) | 22 (4.0) | 34 (6.1) | [31] |
| IDU | 89 | 29 | M (65) F (24) | 25 (28.0) | 10 (11.2) | 15 (16.8) | ||
| Hetero | 236 | 33 | M (96) F (140) | 21 (8.9) | 8 (3.4) | 13 (5.5) | ||
| Homo/Bis | 139 | 33 | M (139) | 5 (3.6) | 2 (1.4) | 3 (2.2) | ||
| Others/Unkb | 89 | 32 | M (58) F (31) | 5 (5.6) | 2 (2.2) | 3 (3.4) | ||
| 2001–2002 | CRTA-PR | 758 | 36 | M (424) F (334) | 43 (5.7) | 6 (0.8) | 37 (4.9) | [32,33] |
| Sexual | 633 | 16 (2.5) | 2 (0.3) | 14 (2.2) | ||||
| IDU | 57 | 17 (29.8) | 2 (3.5) | 15 (26.3) | ||||
| Sexual+IDU | 33 | 7 (21.2) | 1 (3.0) | 6 (18.2) | ||||
| Otherc | 35 | 3 (8.6) | 1 (2.9) | 2 (5.7) | ||||
| 1999–2006 | CRTAs, SP | 1,393 | M (982) F (411) | 81 (5.8) | 46 (3.3) | 35 (2.5) | [35] | |
| Clinics, SP | 919 | M (538) F (381) | 121 (13.2) | 88 (9.6) | 33 (3.6) | |||
| 2014–2015 | CRTA-SP | 1,608 | 44 | M (1237) F (371) | 50 (3.1) | 26 (1.6) | 22 (1.4) | [36] |
| 2012–2015 | CRTAs, SP | 1,383 | 36 | M (930) F (453) | 58 (4.2) | 29 (2.1) | 24 (1.7) | [43,45] |
M, male; F, Female; a multiple transfusion (n=7) and multiple partners (n=19); b unknown risk (n=83), blood transfusion (n=6); c combined risk factors of blood transfusion and sexual contact (n=28), tattooing (n=5), work accidents (n=1), and haemophilia (n=1).
Interestingly, samples collected from the same hospital two years later revealed a relatively low overall prevalence rate of 10.1%, with a higher frequency of HTLV-2 cases (Table 2) [31]. This outcome may be partially attributed to modifications in diagnostic techniques that have increased sensitivity for HTLV-2 detection [28,31]. This was later corroborated by subsequent studies conducted in the laboratory.
Significant findings from these studies revealed high HIV/HTLV prevalence rates among IDUs. In 1992, the prevalence rate was 26.4% (15.3% for HIV/HTLV-1 and 11.1% for HIV/HTLV-2), and in 1994, it increased to 28.0% (11.2% for HIV/HTLV-1 and 16.8% for HIV/HTLV-2) (Table 2) [30,31]. These data underscore the high risk of HTLV-1/-2 infections among this population in São Paulo.
In late 1999, we initiated a search for these co-infections among patients attended by different AIDS Reference Centres (acronym in Portuguese CRTA) in São Paulo city and its surrounding areas (state of São Paulo, Southeast region of Brazil), as well as in Londrina and its vicinities (state of Paraná, South region of Brazil). Despite the continued detection of HIV/HTLV-1 and HIV/HTLV-2 co-infections, there was a significant decrease in prevalence rates.
3.4. HIV/HTLV co-infections in Londrina, Paraná (2001–2002)
During 2001-2002 in Londrina and surrounding areas of Paraná, CRTAs primarily attended white, HIV-infected individuals of both sexes. A preliminary study identified a 6.5% co-infection rate of HIV/HTLV. This co-infection was associated with IDU, hepatitis C virus (HCV) infection, low socioeconomic status, and low educational attainment [32].
Using the Western Blot (WB, HTLV Blot 2.4, Abbott Murex, Singapore) as a confirmatory serological assay, a large number of HTLV WB-indeterminate results were identified [32].
To address this problem, patients were asked to return for an additional blood sample collection. This was used for in-house PCR confirmatory assays, which amplified the LTR, env, and tax segments of the HTLV-1 and HTLV-2 genomes. The majority of WB-indeterminate cases were confirmed as HTLV-2 infections by these PCR assays [33]. Consequently, we determined the overall prevalence of HIV/HTLV to be 5.7% (0.8% for HIV/HTLV-1 and 4.9% for HIV/HTLV-2) (Table 2). Notably, and in line with the present data, problems with diagnostic tests for HTLV infections, mostly for HTLV-2, had been previously described in IDUs with AIDS [28,30,31,34].
Significantly, this study highlighted that female IDUs, as well as those with an IDU partner, constitute a critical risk group for acquiring HIV and HTLVs (data not showed).
3.5. HIV/HTLV co-infections in patients of several CRTAs and out-patient clinics of São Paulo (1999–2006)
Between December 1998 and March 2006, IAL received 2,312 serum samples from São Paulo city and its surrounding areas for HTLV-1/-2 serology. Of these, 1,393 were from various CRTAs (Group I, HIV-1 infected) and 919 were from HTLV out-patient clinics (Group II, patients treated in Specialized Health Units of Haematology, Neurology, Infectious Diseases, and others). These samples were from individuals aged 21–50 years, with the majority falling within the 31- to 40-year age group.
Seven distinct EIA kits were employed for screening during the study period, with the WB (HTLV Blot 2.4) serving as the confirmatory assay. An analysis of samples tested by two EIA kits revealed that no single EIA kit was 100% effective in detecting all true HTLV-1 and HTLV-2 infections (WB positive), corroborating previous description by other groups of researchers from São Paulo and Italy [28,34]. This underscores the necessity of using two EIA kits with different antigen compositions and formats in HTLV at-risk populations in São Paulo. Furthermore, a significant number of WB-indeterminate results were confirmed. Overall, HTLV-1/-2 positivity was detected in 5.8% of Group I and 13.2% of Group II (Table 2). In addition, we conducted an analysis of the results, taking into account factors such as sex, age, and the public health units that provided the patients’ samples to IAL. A brief overview reveals that both HTLV-1 and HTLV-2 were detected in both groups (Table 2). In the case of seropositive females, HTLV-2 was slightly more prevalent in Group I (HIV-infected, 54.5%), whereas HTLV-1 was more common in patients from Group II (HTLV out-patient clinics, 73.9%). This could be attributed to the fact that Group II were more likely to present with HTLV-1 associated diseases. Male patients in Group II exhibited a higher percentage of WB-indeterminate results. We found no correlation between HTLV serological results and age. Our temporal analyses revealed a significant number of HTLV WB-indeterminate samples, along with a wide range of WB-indeterminate profiles, many of which were associated with seroconversion to HTLV-1 or HTLV-2 [35].
Considering these findings and the substantial expense associated with the WB test, we emphasized the importance of enhancing serological screening and confirmatory tests for use in Brazil. We suggested PCR as an appropriate confirmatory and discriminatory assay for this geographical region.
3.6. HIV/HTLV co-infections in patients of the pioneer CRTA-SP (2014–2015)
We conducted a study between 2014 and 2015 to ascertain the prevalence rates and risk factors associated with HIV/HTLV co-infections in São Paulo.
We conducted a study using blood samples from 1,608 patients at the pioneering CRTA in São Paulo, with the majority undergoing highly antiretroviral therapy (HAART). Our objective was to detect HTLV-1/2-specific antibodies. To achieve this, we used two EIA kits, namely EIA Murex HTLV-I + II (Diasorin) and Gold ELISA HTLV-I + II (REM). We also employed two immunoblotting methods, HTLV Blot 2.4 (MP Biomedicals) and INNO-LIA HTLV-I/II (Innogenetics). Owing to a high number of HTLV WB-indeterminate results, we incorporated an in-house real-time PCR assay to confirm the presence of HTLV-1 and HTLV-2 proviral DNA in blood cells.
The analysis of confirmatory assay results revealed a 3.1% prevalence rate of HTLV-1/-2; with 1.6% being HTLV-1 and 1.4% HTLV-2 (Table 2). The median age for HIV/HTLV co-infected individuals was found to be 50 years, compared to 44 years in the general population (p=0.000). Factors associated with an increased risk of HIV/HTLV co-infection included being female, of black/pardum ethnicity, having concurrent HBV or HCV infections and IDU [36]; the same associated factors described elsewhere [29,37].
The relatively low prevalence of HIV/HTLV co-infections observed in São Paulo at this point can be partially attributed to initiatives that supply IDUs with sterile needles and syringes, such as the Harm Reduction Program. Additionally, shifts in drug consumption habits, specifically the transition from injecting cocaine to smoking crack cocaine, have also contributed to this reduced prevalence [38,39].
3.7. HIV and HIV/HTLV co-infection in patients of several CRTAs of São Paulo (2010–2016)
A study carried out in São Paulo examined the characteristics (sex and age) and prevalence rates of HTLV-1/-2 among 1,715 HIV-1-infected individuals (1,192 men and 523 women). These individuals received care at three AIDS service centres between 2010 and 2016, and their samples were forwarded to IAL for HTLV-1/-2 serology.
We first categorized the study population based on the year of sample collection, from 2010 to 2016, and further divided them by sex into five age groups: G1 (16–25 years), G2 (26–30 years), G3 (31–40 years), G4 (41–50 years), and G5 (>50 years). We observed an increase in HIV infections among men aged 16–25 years (10% in 2010 vs. 43% in 2015/2016), and similarly in the 26–30 years age group (10% in 2010 vs. 25% in 2015/2016). In the female population, although the percentages were lower, there was also an increase in HIV infections among those aged 16–25 years and 26–30 years (Figure 2).
Figure 2.
Distribution of the percentages of individuals infected with HIV-1 whose blood samples were sent to Instituto Adolfo Lutz, São Paulo, Brazil for HTLV-1/-2 infection determination during 2010–2016, according to sex- and age-groups.
Figure 2.
Distribution of the percentages of individuals infected with HIV-1 whose blood samples were sent to Instituto Adolfo Lutz, São Paulo, Brazil for HTLV-1/-2 infection determination during 2010–2016, according to sex- and age-groups.
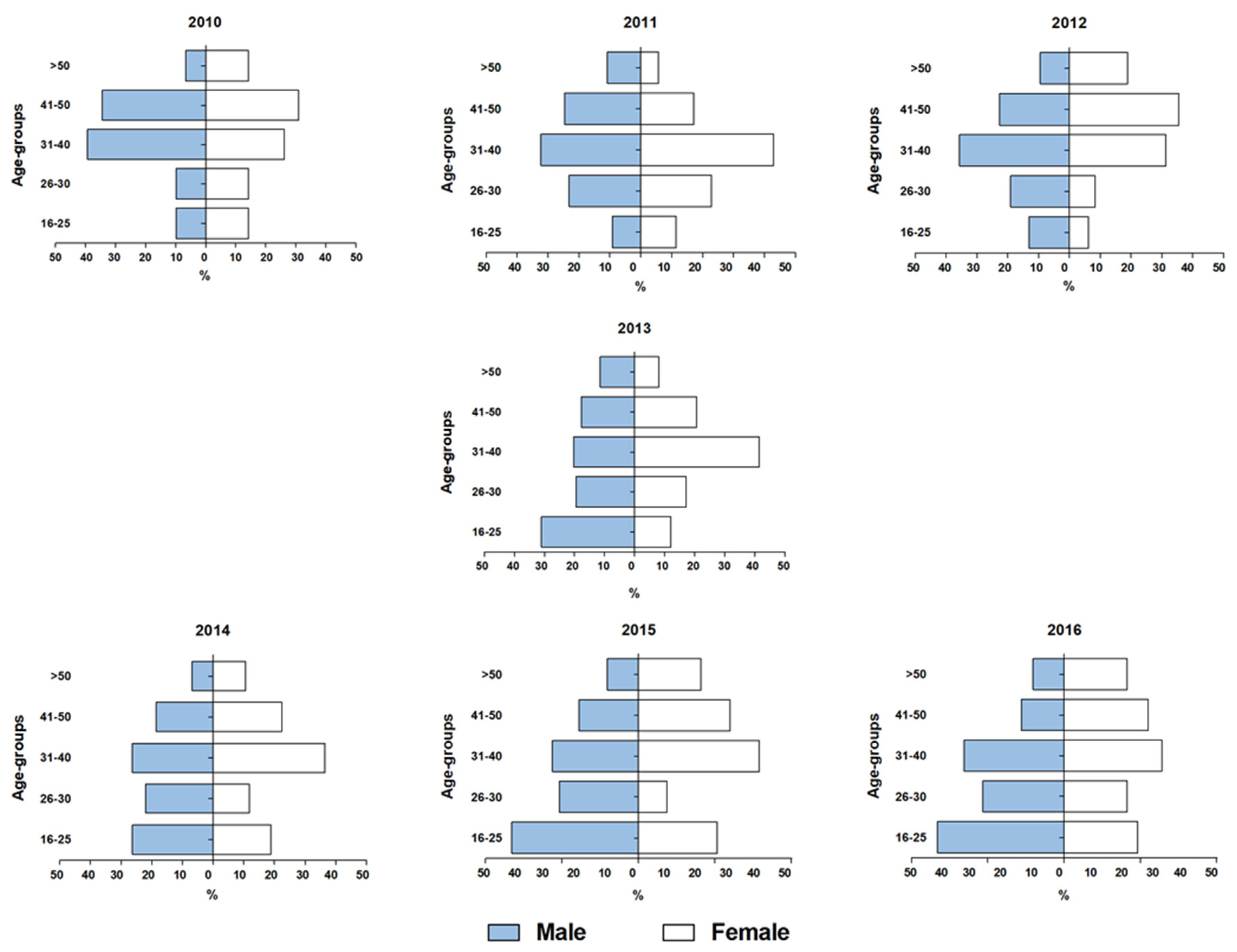
In the context of HIV/HTLV co-infection, all cases identified between 2010 and 2014 were found in patients aged over 30 years (G3, G4, G5). However, between 2015 and 2016, three cases of HTLV infection were discovered in patients under 30 years of age (one in G1 and two in G2). As for HTLV-1/-2 infections, the overall prevalence rate was 3.6% (2.0% among men, and 1.6% among women). There was also a noted increase in HIV/HTLV co-infections in patients aged <30 years. Despite a higher number of HTLV positive cases in men, a correlation with the female sex was observed [40]. Interestingly, HTLV sexual transmission was identified as the main route of transmission from male to female [41].
The rise in young individuals utilizing AIDS care services in São Paulo corroborated data from the 2016 Epidemiological Bulletin of the Brazilian Ministry of Health. This data indicated an increase in AIDS notifications among individuals aged 15 to 34 years, with a male to female ratio of 2.4:1.0. Sexual exposure was identified as the primary risk factor. Furthermore, 50.4% of men reported homosexual practices; 36.8%, heterosexual; and 9.0%, bisexual. In contrast, 96.4% of women reported heterosexual contact [42].
3.8. HIV/HTLV co-infections in recent CRTAs setting in São Paulo (2012–2015)
To corroborate and expand upon prior findings, we investigated the presence of HIV/HTLV co-infections in the latest HIV/AIDS service setting in São Paulo. We selected blood samples from 1,382 HIV-1 infected individuals (930 men and 453 women; median age 35.6 years) for analysis. These individuals, who had recently contracted HIV through sexual contact and had not yet started HAART, provided the samples between 2012 and 2015.
Following HTLV screening with two EIAs, four confirmatory assays were performed: HTLV Blot 2.4, INNO-LIA, and in-house qPCR and PCR-RFLP. The performance of these assays was then comparatively analysed. The overall HIV/HTLV prevalence was 4.2% (2.1% for HTLV-1, 1.7% for HTLV-2, 0.1% for HTLV-1 + HTLV-2, and 0.3% for HTLV) (Table 2). An association between HTLV and women, as well as individuals aged >40 years, was identified [43], supporting the notion that repeated exposure is necessary for HTLV sexual transmission, which is more efficient from male to female [41]. The molecular assays demonstrated low sensitivity, while the LIA showed the best performance in detecting HTLV-1/-2 in these patients. We hypothesized that the negative PCR results might be attributable to the presence of defective provirus and/or low HTLV proviral load in these patients, and the inconclusive WB results could be associated with the seroconversion period [43]; noteworthy, these hypotheses were later confirmed by further studies performed in Japan [44] and in our laboratory.
In a following study, the performance of four HTLV-1/-2 confirmatory tests between two patient groups was compared: those with long-term HIV infection on HAART [36] and those recently infected (HAART naïve) [43]. Our findings confirmed that LIA showed the best performance in detecting HTLV-1 and HTLV-2 in these patients [45]. Interestingly, a collaborative study for performance evaluation of HTLV-1 diagnostic assays in Japan established a novel test algorithm that LIA replaces the WB as the first confirmatory assay [46].
3.9. Variations of HIV/HTLV co-infections prevalence rates regarding the years of sample collection (1991–2015)
Statistical analyses revealed differences in the overall prevalence rates of HIV/HTLV co-infections, as well as separate HIV/HTLV-1 and HIV/HTLV-2 co-infections, based on the years of blood sample collection (Table 3). These differences were statistically significant (all p<0.0000001).
Table 3.
Summary of the prevalence rates of HIV/HTLV and HIV-1/HTLV-1 and HIV-1/HTLV-2 co-infected individuals sampled from 1991 to 2015
Table 3.
Summary of the prevalence rates of HIV/HTLV and HIV-1/HTLV-1 and HIV-1/HTLV-2 co-infected individuals sampled from 1991 to 2015
| Years of samples collection | |||||||
|---|---|---|---|---|---|---|---|
| 1991–1992a (n=471) |
1994b (n=553) |
2001–2002c (n=758) |
1999–2006d (n=1,393) |
2014–2015e (n=1,608) |
2012–2015f (n=1,383) |
p-value | |
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | ||
| HIV/HTLV | 62 (13.2) | 56 (10.1) | 43 (5.7) | 81 (5.8) | 50 (3.1) | 58 (4.2) | <0.0000001 |
| HIV/HTLV-1 | 37 (7.9) | 22 (4.0) | 6 (0.8) | 46 (3.3) | 26 (1.6) | 29 (2.1) | <0.0000001 |
| HIV/HTLV-2 | 25 (5.3) | 34 (6.1) | 37 (4.9) | 35 (2.5) | 22 (1.4) | 24 (1.1) | <0.0000001 |
n, number of samples analysed; p values were calculated using the Chi-square test. A p-value ≤ 0.05 was considered significant.
The analysis conducted at different time points of sample collection, such as 1991–1992a vs. 1994b (a vs. b), 1991–1992a vs. 2011–2001c (a vs. c), 1991–1992a vs. 1991–2006d (a vs. d), yielded intriguing results. In the context of HIV/HTLV co-infections, no significant differences were observed between a vs. b (p=0.08332), c vs. d (p=0.8859), c vs. f (p=0.09996), and e vs. f (p=0.1025). However, all other comparative analyses revealed statistically significant differences (all p<0.05). These findings confirm the variations in prevalence rates between the 1990s (higher) and the 2000s (lower). They also supported the period of observed changes in the transmission routes of such retroviruses, as well as shifts in risk factors, sex, and age of infected individuals in São Paulo and Brazil [36,38,39,40,42].
In the context of HIV/HTLV-1 co-infection, no significant differences were observed between b vs. d (p=0.2754), c vs. e (p=0.1422), and e vs. f (p=0.3037). All other comparisons revealed significant differences (all p<0.05). Interestingly, the lowest prevalence of HIV/HTLV-1 was found in the cohort sampled in 2001–2002c. This observation could be partially attributed to the fact that Paraná is not an endemic region for HTLV-1 infection in Brazil [47] (p.51–54), joined with the high proportion of IDUs in the population who are more susceptible to HTLV-2 infection [21,32,33]. Indeed, the highest rate of HIV/HTLV-2 co-infection (4.9%) was identified in this patient cohort in the 2000s (Table 3). With respect to the prevalence rates of all HIV/HTLV-2 co-infections, no significant differences were found between groups a vs. b (p=0.8040), a vs. c (p= 0.3151), b vs. c (p=0.1685), d vs. f (p=0.1236), and e vs. f (p=0.3838). All other comparisons yielded p<0.05. The observed results could be attributed to changes in drug usage patterns and a decrease in the number of IDUs sharing infected needles and syringes [38,39].
For comparative analyses of HIV/HTLV prevalence rates presented herein and those detected in other regions/populations from Brazil, we have to consider differences in demographic, sociocultural and economic status of individuals, variability in HTLV-1 and HTLV-2 endemic regions, and the years of samples collection.
For example, in the North of Brazil (Amazon region), considered endemic for HTLV-2 infection in Amerindians populations, studies conducted in HIV-infected individuals attended at specialized HIV/AIDS centres in Belém and vicinities (state of Pará) showed a decrease in HIV/HTLV co-infections over time. In 1998, samples collected from 1994–1996, an overall prevalence rate of 7.4% (2.7% for HIV/HTLV-1 and 4.7% for HIV/HTLV-2) was detected, mostly in homosexual/bisexual men, IDU, median age of 31.7 years [48]. In 2005, in the same region, the overall HIV/HTLV prevalence dropped to 3.6% (1.2% for HIV/HTLV-1 and 2.4% for HIV/HTLV-2), confirming high endemicity for HTLV-2 in the Amazon region of Brazil [49]. Curiously, in the same region, samples collected from 2016–2017 showed a shift from HTLV-2 to HTLV-1 (all co-infected patients were infected by HTLV-1); the prevalence decreased to 1.4%, and the risks associated with this co-infection were being a woman and not using a condom during sexual intercourse [50].
In the Northeast region of Brazil, considered the highest endemic region for HTLV-1 in the country [47], the prevalence rates of HIV/HTLV also changed over time. In 2011, in Salvador, state of Bahia, patients seen during the years of 1994 and 1995 at the AIDS clinics of the Hospital Universitário Prof. Edgard Santos, showed an overall HIV/HTLV prevalence of 20.3% (17.1% for HIV/HTLV-1 and 3.2% for HIV/HTLV-2). The median age of the co-infected patients was approximately 34 years, and the most important associated risk factor was IDU [51]. In 2022, another study conducted by the Central Public Health Laboratory in Salvador, employing samples collected from 2004–2013 through the state of Bahia, showed an overall HIV/HTLV prevalence of 2.4% (2.1% for HIV/HTLV-1, 0.2% for HIV/HTLV-2, and 0.1% for HIV/HTLV-1/-2). Co-infections were more frequently detected among women of the median age of 47.2 years; 57% concentrated in the municipality of Salvador. Co-infections were associated with unprotected sexual activity due to tourism and/or economic activity. The authors explained the discrepancy between the median age of the total cohort (29.5 years) and that of the co-infected individuals (>45 years), considering that the prevalence of HTLV-1 among women increases with age [52].
Also in Northeast region of Brazil, one study conducted in 2012 with HIV-infected individuals from an urban area of the state of Piauí showed an overall HIV/HTLV prevalence of 2.24%. Using molecular assay for confirming HTLV infection, prevalence rates of 1.12% for HIV/HTLV-1 and 0.5% for HIV/HTLV-2 were detected. The risk factors associated with co-infections were age >40 years, having undergone minor surgeries and blood transfusion [53]. In another state of the Northeast region, Paraíba, a cross-sectional study carried out in 2021, using samples collected in 2015 from HIV/AIDS patients of both sexes attended the Hospital Clementino Fraga, João Pessoa city, disclosed an overall HIV/HTLV prevalence of 1.5%; all patients were HIV/HTLV-1 co-infected and no association with risk factors was detected [54].
In Southeast region of Brazil, one study using samples from the Santos AIDS Reference Centre (state of São Paulo) collected during 1997–1998, showed an overall HIV/HTLV prevalence of 13.4% (6.0% for HIV/HTLV-1 and 7.4% for HIV/HTLV-2) associated with males, nonwhite color/race, low income, IDU, never condom use, and HCV [55]. Another study conducted in the cities of São Paulo and Ribeirão Preto, using samples collected in 2001, disclosed an HIV/HTLV overall prevalence of 7.5% (4.7% in São Paulo and 10.7% in Ribeirão Preto); the majority due to HTLV-2 infection associated with IDU and HCV [56]. These results and risk factors corroborate the data detected in our studies using samples collection during the 1990s.
Finally, although the South region of Brazil is considered not endemic for HTLV-1/2 infections in Brazil [47], studies conducted in the state of Rio Grande do Sul showed these retroviruses circulating in patients with HIV/AIDS. One of them conducted at three HIV counseling centres in Porto Alegre, using samples collected in 1996, showed an overall HIV/HTLV prevalence of 2.4% (1.4% for HIV/HTLV-1 and 1.0% for HIV/HTLV-2), and association with injecting cocaine use and older age [57]. Another study conducted in Canoas, metropolitan region of Porto Alegre, using samples collected during 2008–2009 from a specialized HIV/AIDS diagnosis and treatment centre, disclosed an overall HIV/HTLV prevalence of 5.0%. But after molecular assay analysis, only 2.9% confirmed HTLV infection (1.9% for HIV/HTLV-1 and 1.0% for HIV/HTLV-2), both associated with blood transfusion and tattoo [58].
Taken together, studies carried out in Brazil confirm a decrease in HIV/HTLV prevalence over time and emphasize differences in the type of HTLV that circulates in different regions of this country.
4. Discussion
Brazil has earned global acclaim for its efforts against AIDS, offering universal, free access to antiretroviral treatment for all patients and implementing education programs to prevent virus transmission/acquisition [59,60]. The success of HAART, initially in reducing AIDS-related hospitalizations in Brazil and subsequently in controlling HIV disease progression and transmission (evidenced by a decrease in HIV viral load to undetectable levels and stable maintenance of CD4+ cell counts), has been instrumental in preventing HIV transmission/acquisition and the onset of AIDS in infected individuals. Additionally, the Harm Reduction Program, which provides sterile needles and syringes to IDUs, along with changes in drug use patterns in Brazil, has contributed to a decrease in HIV prevalence rates [38,39]. Several other significant measures have enhanced our understanding of the HIV/AIDS situation in Brazil. These include: (i) mandatory reporting of AIDS cases (Ministry of Health Ordinance No. 542, dated 22 December, 1986), (ii) compulsory notification of HIV infection in pregnant women and parturient or puerperal women and children at risk of vertical HIV transmission (Ministry of Health Ordinance No. 993, dated 4 September, 2000), and (iii) the inclusion of HIV in the List of Diseases of Compulsory Notification and in the Information System for Notifiable Diseases (Sistema de Informação de Agravos de Notificação, Sinan), as per Ordinances No. 1,271, dated 6 June, 2014 and No. 1,984, dated 12 September, 2014, and following through other information systems: Mortality Information System (Sistema de Informações sobre Mortalidade, SIM); CD4 and viral load Laboratory Tests Control System (Sistema de Controle de Exames Laboratoriais CD4 e CV, Siscel), and Drug Logistic Control System (Sistema de Controle Logístico de Medicamentos, Siclom). These systems provide real-time updates on the HIV/AIDS situation in Brazil, contribute to Epidemiological Bulletins, and aid in establishing measures to control virus dissemination.
The latest HIV-AIDS Epidemiological Bulletin from the Brazilian Ministry of Health, 2022, reveals that from 1980 to June 2022, a total of 1,088,536 AIDS cases were reported, with 310,099 cases originating from São Paulo [61]. The rate of AIDS cases has fluctuated over time. In 2011, the rate was 22.5 cases per 100,000 inhabitants, which decreased to 15.6 cases per 100,000 inhabitants in 2021. This reduction was more pronounced in women (43.6%) than in men (16.2%). A similar decline in AIDS cases was observed in São Paulo, with 21.4 cases per 100,000 inhabitants in 2011 compared to 13.4 cases per 100,000 inhabitants in 2022 [61]. However, despite the overall decrease in new AIDS cases in Brazil, there has been a concerning increase among adolescents and young adults. This is particularly evident among homosexual men aged 20 to 29 years, who accounted for 57.1% of AIDS cases in this age group in 2015, a figure that rose to 62.4% in 2021 [61]. The same situation was described in Puerto Rico Island (Caribbean region), where in the years 2010 to 2014 an increase of 53% in HIV new diagnosis was observed among men and women aged 13 to 24 years, more pronounced in men who have sex with men [62]. In addition, similar circumstances have recently been described in USA; in recent years, increased rates of sexually transmitted diseases such as chlamydia, gonorrhea, and primary and secondary syphilis have been observed among men and women aged 15 to 24 years, and approximately one in five new HIV diagnoses among males aged 13 to 24 years, of whom 93% were attributable to homosexual contact, emphasizing the need for a continuing education program for these age groups [63].
Interestingly, the UNAIDS Global AIDS update 2023 reported different figures of new HIV infections from 2010 to 2022 across the world. The rise in new HIV infections continued in Latin America (8% increase), Eastern Europe and central Asia (49% increase) and the Middle East and North Africa (61% increase). On the other hand, decreases in the numbers of new HIV infections were detected in Eastern and Southern Africa (57% reduction) and Western and Central Africa (49% reduction), but adolescent girls and young women in many parts of sub-Saharan Africa still have high risks of HIV infection. Decline of new HIV infections were also observed in western and central Europe and North America (23% decline), Caribbean (15% decline), and Asia and Pacific (14% decline, although in some countries in Asia and Pacific the number of new HIV infections is rising alarmingly). In summary, the HIV pandemic continues to affect key populations more than the general population worldwide. In 2022, comparative analyses among adults in the general population (aged 15–49 years) revealed HIV prevalence rate 11 times higher among homosexual men, four times higher among sex workers, seven times higher among IDUs and 14 times higher among transgender people [64]. In this regard, governments must provide treatment and prevention and prioritize inclusive approaches that respect people’s human rights and involve affected communities throughout the HIV response.
Unfortunately, concerns and the strategies, policies, information systems implemented for HIV/AIDS were not extended to HTLV-1 and HTLV-2 infections/diseases elsewhere, including Brazil, despite the high morbidity and mortality rate of HTLV-1associated diseases and the absence of curative treatment for HTLV-1/-2. Nevertheless, while specific interventions for IDUs have not been established for HTLVs, the measures taken for HIV have significantly decreased the incidence of HIV/HTLV co-infections among IDUs in urban regions [30,31,32,33,36]. In addition, some progress has been observed since the publication of a call for action to WHO [65], which in 2021 included a global consultation and the publication of a technical report and fact sheet [65,66].
Besides, a recent review article by an HTLV study group from Brazil and the United Kingdom examined the transmission routes of HTLV-1/2 and strategies to prevent its continued spread in Brazil. This review scrutinized public health policies implemented in Brazil since 1993, when HTLV serology became mandatory in blood banks (Ministry of Health Ordinance No. 1,376, dated 19 November, 1993). Additional policies included HTLV screening for organ and tissue donors and recipients (Ordinance No. 2600, dated 21 October, 2009) and gamete donors (Resolution - RDC No. 23, dated 27 May, 2011). The review also addressed recommendations for HTLV-seropositive mothers to avoid breastfeeding and the incorporation of HTLV into the national program for sexually transmitted infections [67]. Moreover, the review proposed several public health policies for HTLV, such as: (i) universal antenatal screening, (ii) confirmatory testing for those reactive in screening tests, (iii) mandatory reporting, (iv) establishment of multidisciplinary reference centres, (v) provision of HTLV testing for high-risk populations, and (vi) public education to enhance awareness of HTLV infection/diseases [67].
A subsequent review article examining the strengths, weaknesses, opportunities, and threats analysis for the implementation of HTLV-1 public health policies in Brazil identified several weaknesses: (i) inadequate HTLV knowledge, (ii) insufficient epidemiological data, (iii) a deficiency of patient care reference centres, (iv) limited availability of confirmatory tests, (v) absence of universal antenatal screening, and (vi) lack of cost-effectiveness studies [68]. Consequently, numerous studies have been initiated or are underway in Brazil to address these deficiencies.
In Japan, an HTLV-1 endemic country, horizontal transmission has emerged as the primary route of virus transmission, particularly among adolescents and young adults residing in urban areas. This trend is attributed to the migration of these age groups from rural to urban areas, influenced by superior education and employment prospects, coupled with more liberal social and sexual norms. Unprotected sexual encounters, especially with multiple partners, and transmission via contaminated needles, including drug injection or tattooing, have been identified as significant HTLV-1 transmission pathways in Japan [69]. This situation mirrors, to some extent, the circumstances in São Paulo and Brazil, where adolescents and young individuals, predominantly homosexual men, are exposed to retroviruses through unprotected sexual activity and promiscuity, often under the influence of substances such as alcohol, marijuana, crack, amphetamines, and hallucinogens.
In conclusion, the studies discussed herein, coupled with data from the Brazilian Ministry of Health and the author's expertise in HIV/AIDS and HTLV-1/-2 infections in Brazil, suggest a concerning lack of awareness among adolescents and young adults regarding the transmission methods and implications of these retroviral infections. Consequently, it is imperative to promptly initiate ongoing informational and awareness campaigns targeting these age and risk groups in Brazil, with the aim of curbing the spread of these retroviruses within the country.
Author Contributions
Not applicable.
Funding
This secondary review did not receive direct funding. The primary studies cited herein were supported by grants and fellowships from various agencies, as detailed in each respective work cited in this review.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are published and/or available on the given websites.
Acknowledgments
I would like to thank all co-authors and patients who participated in the primary studies reported here, and Editage (www.editage.com) for English language editing.
Conflict of Interest
The author declares no conflict of interest.
References
- Laurindo-Teodorescu, L.; Teixeira, P.R. Histórias da aids no Brasil: As respostas governamentais à epidemia de aids. Ministério da Saúde/Secretaria de Vigilância em Saúde/Departamento de DST, Aids e Hepatites Virais, Brasília, Brazil, 2015; Vol. 1, pp. 1–464. Available online: https://unesdoc.unesco.org/ark:/48223/pf0000235557?posInSet=2&queryId=f390b88f-74e1-450d-a274-cfb553262cc7 (accessed on 4 July 2023).
- CDC. Pneumocystis Pneumonia: Los Angeles. Morbidity and Mortality Weekly Report (MMWR). Centers for Disease Control, June 5, 1981; Volume 30(21), pp. 250–252. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/june_5.htm (accessed on 4 July 2023).
- CDC. Kaposi's Sarcoma and Pneumocystis Pneumonia Among Homosexual Men — New York City and California. Morbidity and Mortality Weekly Report (MMWR). Centers for Disease Control, July 3, 1981; Volume 30(25), pp. 305–308. Available online: https://www.jstor.org/stable/23300179 (accessed on 4 July 2023).
- CDC. Opportunistic Infections and Kaposi's Sarcoma among Haitians in the United States. Morbidity and Mortality Weekly Report (MMWR). Centers for Disease Control, July 9, 1982; Volume 31(26), pp. 353–354,360–361. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/00001123.htm (accessed on 4 July 2023).
- CDC. Pneumocystis carinii pneumonia among persons with hemophilia A. Morbidity and Mortality Weekly Report (MMWR). Centers for Disease Control, July 16, 1982; Volume 31(27), pp. 365–367. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/00001126.htm (accessed on 4 July 2023).
- CDC. Current Trends Update on Acquired Immune Deficiency Syndrome (AIDS) -United States. Morbidity and Mortality Weekly Report (MMWR). Centers for Disease Control, September 24, 1982; Volume 31(37), 507–508,513–514. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/00001163.htm (accessed on 4 July 2023).
- Poiesz, B.J.; Ruscetti, F.W.; Gazdar, A.F.; Bunn, P.A.; Minna, J.D.; Gallo, R.C. Detection and isolation of type C retrovirus particles from fresh and cultured lymphocytes of a patient with cutaneous T-cell lymphoma. Proc Natl Acad Sci USA. 1980; 77(12), 7415–7419. [CrossRef]
- Kalyanaraman, V.S.; Sarngadharan, M.G.; Robert-Guroff, M.; Miyoshi, I.; Golde, D.; Gallo, R.C. A new subtype of human T-cell leukemia virus (HTLV-II) associated with a T-cell variant of hairy cell leukemia. Science. 1982; 218, 571–573. [CrossRef]
- Barré-Sinoussi, F.; Chermann, J.C.; Rey, F.; Nugeyre M.T.; Chamaret, S.; Gruest, J.; Dauguet, C.; Axler-Blin,C.; Vézinet-Brun, F.; Rouzioux, C.; Rozenbaum, W.; Montagnier, L. Isolation of a T-lymphotropic retrovirus from a patient at risk for acquired immune deficiency syndrome (AIDS). Science. 1983 May 20; 220(4599), 868–871. [CrossRef]
- Popovic, M.; Sarngadharan, M.G.; Read, E.; Gallo, R.C. Detection, isolation, and continuous production of cytopathic retroviruses (HTLV-III) from patients with AIDS and pre-AIDS. Science. 1984 May 4; 224(4648), 497–500. [CrossRef]
- Gallo, R.C.; Salahuddin, S.Z.; Popovic, M.; Shearer, G.M.; Kaplan, M.; Haynes, B.F.; Palker. T.J.; Redfield, R.; Oleske, J.; Safai, B.; et al. Frequent detection and isolation of cytopathic retroviruses (HTLV-III) from patients with AIDS and at risk for AIDS. Science. 1984 May 4; 224(4648), 500–503. [CrossRef]
- Vallinoto, A.C.R.; Rosadas, C.; Machado, L.F.A.; Taylor, G.P.; Ishak, R. HTLV: It is time to reach a consensus on its nomenclature. Front Microbiol. 2022; 13, 896224. [CrossRef]
- Brites, C.; Sampaio, J.; Oliveira, A. HIV/Human T-cell lymphotropic virus coinfection revisited: Impact on AIDS progression. AIDS Rev. 2009; 11, 8–16 Available online: https://www.aidsreviews.com/resumen.php?id=1030&indice=2009111&u=unp.
- Beilke, M.A. Retroviral coinfections: HIV and HTLV: Taking stock of more than a quarter century of research. AIDS Res Hum Retroviruses. 2012; 28(2), 139–147. [CrossRef]
- Montaño-Castellón, I.; Marconi, C.S.C.; Saffe, C.; Brites, C. Clinical and laboratory outcomes in HIV-1 and HTLV-1/2 coinfection: A systematic review. Front Public Health. 2022; 10, 820727. [CrossRef]
- Rosadas, C.; Taylor, G.P. HTLV-1 and co-infections. Front Med. 2022; 9, 812016. [CrossRef]
- Gessain, A.; Cassar, O. Epidemiological aspects and world distribution of HTLV-1 infection. Front Microbiol. 2012; 3, 388. [CrossRef]
- Murphy, E.L.; Cassar, O.; Gessain, A. Estimating the number of HTLV-2 infected persons in the world. Retrovirology 2015, 12(Suppl 1):O5 Available online: http://www.retrovirology.com/content/12/S1/O5 (accessed on 22 August, 2023). [CrossRef]
- Carneiro-Proietti, A.B.F.; Catalan-Soares, B.C.; Castro-Costa, C.M.; Murphy, E.L.; Sabino, E.C.; Hisada, M.; Galvão-Castro, B.; Alcantara, L.C.J.; Remondegui, C.; Verdonck, K.; Proietti, F.A. HTLV in the Americas: Challenges and perspectives. Rev Panam Salud Publica. 2006; 19(1),44–53. [CrossRef]
- Briggs, N.C.; Battjes, R.J.; Cantor, K.P.; Blattner, W.A.; Yellin, F.M.; Wilson, S.; Ritz, A. L.; Weiss, S.H.; Goedert, J.J. Seroprevalence of human T cell lymphotropic virus type II infection, with or without human immunodeficiency virus type 1 coinfection, among US intravenous drug users. J Infect Dis. 1995; 172(1), 51-58. [CrossRef]
- Paiva, A.; Casseb, J. Origin and prevalence of human T-lymphotropic virus type 1 (HTLV-1) and type 2 (HTLV-2) among indigenous populations in the Americas. Rev Inst Med Trop Sao Paulo. 2015; 57(1), 1–13. [CrossRef]
- Ishak, R.; Ishak, M.O.G.; Azevedo V.N.; Machado, L.F.A.; Vallinoto, I.M.C.; Queiroz, M.A.F.; Costa, G.L.C.; Guerreiro, J.F.; Vallinoto, A.C.R. HTLV in South America: Origins of a silent ancient human infection. Virus Evol. 2020; 6(2), veaa053. [CrossRef]
- De-Araujo, A.C. Cell-mediated immunity in the Acquired Immunodeficiency Syndrome. Brazilian J Med Biol Res. 1987; 20, 579–582. PMID: 3452448. Available online: https://www.researchgate.net/profile/Adele-Caterino-De-Araujo/publications (accessed on 6 July 2023).
- Amadori, A.; Zamarchi, R.; Ciminale, V.; Del Mistro, A.; Siervo, A.; Alberti, A.; Colombatti, M.; Chieco-Bianchi, L. HIV-1-specific B cell activation. A major constituent of spontaneous B cell activation during HIV-1 infection. J Immunol. 1989; 143(7), 2146–2152. [CrossRef]
- Amadori, A.; De Rossi, A.; Faulkner-Valle, GP.; Chieco-Bianchi, L. Spontaneous in vitro production of virus-specific antibody by lymphocytes from HIV-infected subjects. Clin Immunol Immunopathol. 1988; 46(3), 342–351. [CrossRef]
- Caterino-de-Araujo, A.; de-los- Santos-Fortuna, E.; Grumach, A.S. An alternative method for in vitro production of HIV-1-specific antibodies. Brazilian J Med Biol Res. 1991; 24, 797–799. Available online: https://www.researchgate.net/profile/Adele-Caterino-De-Araujo/publications (accessed on 6 July 2023).
- Caterino-de-Araujo, A. Rapid in vitro detection of HIV-1-specific antibody secretion by cells-culture with virus antigens. Mem Inst Oswaldo Cruz. Rio de Janeiro. 1992; 87(2), 239–247. Available online: https://www.researchgate.net/profile/Adele-Caterino-De-Araujo/publications (accessed on 6 July 2023). [CrossRef]
- De Rossi, A.; Mammano, F.; Del Mistro, A.; Chieco-Bianchi, L. Serological and molecular evidence of infection by human T-cell lymphotropic virus type II in Italian drug addicts by use of synthetic peptides and polymerase chain reaction. Eur J Cancer Clin Oncol. 1991; 27(7), 835-838. [CrossRef]
- Koech, C.C.; Lwembe, R.M.; Odari, E.O.; Budambula, N.L.M. Prevalence and associated risk factors of HTLV/HIV co-infection among people who inject drugs (PWIDs): A review. J Hum Virol Retrovirol 6(1): 00188. [CrossRef]
- Caterino de Araujo, A.; do Rosario Casseb, J.S.; Neitzert, E.; Xavier de Souza, M.L.; Mammano, F.; Del Mistro, A.; De Rossi, A.; Chieco-Bianchi, L. HTLV-I and HTLV-II infections among HIV-1 seropositive patients in Sao Paulo, Brazil. Eur J Epidemiol. 1994; 10, 165–171. [CrossRef]
- Caterino-de-Araujo, A.; de los Santos-Fortuna, E.; Meleiro, M.C.Z.; Suleiman, J.; Calabrò, M.L.; Favero, A.; De Rossi, A.; Chieco-Bianchi, L. Sensitivity of two enzyme-linked Immunosorbent assay tests in relation to Western blot in detecting human T-cell lymphotropic virus types I and II infection among HIV-1 infected patients from São Paulo, Brazil. Diagn Microbiol Infect Dis. 1998; 30(3), 173–182. [CrossRef]
- Morimoto, H.K.; Caterino-De-Araujo, A.; Morimoto, A.A.; Reiche, E.M.V.; Ueda, L.T.; Matsuo, T.; Stegmann, J.W.; , Reiche, F.V. Seroprevalence and risk factors for Human T cell lymphotropic virus type 1 and 2 infection in human immunodeficiency virus-infected patients attending AIDS referral center health units in Londrina and other communities in Paraná, Brazil. AIDS Res Hum Retroviruses. 2005. 21(4), 256–262. [CrossRef]
- Morimoto, H.K.; Morimoto, A.A.; Reiche, E.M.V.; Ueda, L.T.; Matsuo, T.; Reiche, F.V.; Caterino-de-Araujo, A. Difficulties in the diagnosis of HTLV-2 infection in HIV/AIDS patients from Brazil: Comparative performances of serologic and molecular assays, and detection of HTLV-2b subtype. Rev Inst Med Trop. Sao Paulo. 2007; 49(4), 225–230. [CrossRef]
- Casseb, J.; Souza, T.; Pierre-Lima, M.T.; Yeh, E.; Hendry, M.; Gallo, D. Testing problems in diagnosing HTLV infection among intravenous drug users with AIDS in São Paulo city, Brazil. AIDS Res Hum Retroviruses. 1997; 13(18), 1639-1641. [CrossRef]
- Jacob, F.; Santos-Fortuna, E.; Azevedo, R.S.; Caterino-de-Araujo, A. Serological patterns for HTLV-I/II and its temporal trend in high-risk populations attended at Public Health Units of São Paulo, Brazil. J. Clin. Virol. 2008; 42(2), 149–155. [CrossRef]
- Caterino-de-Araujo, A.; Sacchi, C.T.; Gonçalves, M.G.; Campos, K.R.; Magri, M.C.; Alencar, W.K.; Group of Surveillance and Diagnosis of HTLV of São Paulo (GSuDiHTLV-SP). Current prevalence and risk factors associated with HTLV-1 and HTLV-2 infections among HIV/AIDS patients in São Paulo, Brazil. AIDS Res. Hum. Retroviruses. 2015; 31(5), 543–549. [CrossRef]
- Zunt, J.R.; Tapia, K.; Thiede, H.; Lee, R.; Hagan, H. HTLV-2 infection in injection drug users in King County, Washington. Scand J Infect Dis. 2006; 38(8), 654–663. [CrossRef]
- Mesquita, F.; Kral, A.; Reingold, A.; Bueno, R.; Trigueiros, D.; Araujo, P.J.; Santos Metropolitan Region Collaborative Study Group. Trends of HIV infection among injection drug users in Brazil in the 1990s: The impact of changes in patterns of drug use. J Acquir Immune Defic Syndr. 2001; 28(3), 298–302. [CrossRef]
- Mesquita, F.; Doneda, D.; Gandolfi, D.; Nemes M.I.B.; Andrade, T.; Bueno, R.; Trigueiros, D,P. Brazilian response to the human immunodeficiency virus/acquired immunodeficiency syndrome epidemic among injection drug users. Clin Infect Dis. 2003; 37(Suppl 5), S382–S385. [CrossRef]
- Caterino-de-Araujo, A.; Campos, K.R. Spread of human retrovirus infections in individuals at the second and third decades of life in São Paulo, Brazil. Austin J HIV/AIDS Res. 2017; 4(1), 1036. Available online: https://austinpublishinggroup.com/hiv-aids-research/fulltext/ajhr-v4-id1036.pdf (accessed on 11 July 2023).
- Paiva, A.; Casseb, J. Sexual transmission of human T-cell lymphotropic virus type 1. Rev Soc Bras Med Trop. 2014; 47(3), 265-274. [CrossRef]
- HIV–AIDS, Boletim Epidemiológico, Brasília, 2016. Ano V, Nº 1 da 27ª a 53ª semanas epidemiológicas - julho a dezembro de 2015 e da 01ª a 26ª semanas epidemiológicas - janeiro a junho de 2016. Available online: http://antigo.aids.gov.br/pt-br/pub/2016/boletim-epidemiologico-de-aids-2016 (accessed on 12 July 2023).
- Campos, K.R.; Gonçalves, M.G.; Caterino-de-Araujo, A. Failures in detecting HTLV-1 and HTLV-2 in patients infected with HIV-1. AIDS Res Hum Retroviruses. 2017; 33(4), 382–385. [CrossRef]
- Kuramitsu, M.; Sekizuka, T.; Yamochi, T.; Firouzi, S.; Sato, T.; Umeki, K.; Sasaki, D.; Hasegawa, H.; Kubota, R.; Sobata, R.; Matsumoto, C.; Kaneko, N.; Momose, H.; Araki, K.; Saito, M.; Nosaka, K.; Utsunomiya, A.; Koh, K-R.; Ogata, M.; Uchimaru, K.; Iwanaga, M.; Sagara, Y.; Yamano, Y.; Okayama, A.; Miura, K.; Satake, M.; Saito, S.; Itabashi, K.; Yamaguchi, K.; Kuroda, M.; Watanabe, T.; Okuma, K.; Hamaguchi, I. 2017. Proviral features of human T cell leukemia virus type 1 in carriers with indeterminate Western blot analysis results. J Clin Microbiol. 2017; 55(9), 2838–2849. [CrossRef]
- Campos, K.R.; Gonçalves, M.G.; Costa, N.A.; Caterino-de-Araujo, A. Comparative performances of serologic and molecular assays for detecting HTLV-1 and HTLV-2 in patients infected with HIV-1. Brazilian J Infect Dis. 2017; 21(3), 297–305. [CrossRef]
- Okuma, K.; Kuramitsu, M.; Niwa, T.; Taniguchi, T.; Masaki, Y.; Ueda G.; Matsumoto, C.; Sobata, R.; Sagara, Y.; Nakamura, H.; Satake, M.; Miura, K.; Fuchi, N.; Masuzaki, H.; Okayama, A.; Umeki, K.; Yamano, Y.; Sato, T.; Iwanaga, M.; Uchimaru, K.; Nakashima, M.; Utsunomiya, A.; Kubota, R.; Ishitsuka, K.; Hasegawa, H.; Sasaki, D.; Koh, K-R.; Taki, M.; Nosaka, K.; Ogata, M.; Naruse, I.; Kaneko, N.; Okajima, S.; Tezuka, K.; Ikebe, E.; Matsuoka, S.; Itabashi, K.; Saito, S.; Watanabe, T.; Hamaguchi, I. Establishment of a novel diagnostic test algorithm for human T-cell leukemia virus type 1 infection with line immunoassay replacement of western blotting: A collaborative study for performance evaluation of diagnostic assays in Japan. Retrovirology. 2020; 17(1), 26. [CrossRef]
- Brasil. Ministério da Saúde. Guia de Manejo Clínico da Infecção pelo HTLV / Ministério da Saúde, Secretaria de Vigilância em Saúde, Departamento de Doenças de Condições Crônicas e Infecções Sexualmente Transmissíveis. Brasília: Ministério da Saúde, 2021. 104p. : Il. ISBN 978-65-5993-116-3. Available online: http://antigo.aids.gov.br/pt-br/pub/2022/guia-de-manejo-clinico-da-infeccao-pelo-htlv (accessed on 14 July 2023).
- Vallinoto, A.C.R.; Azevedo, V.N.; Santos, D.E.M.; Caniceiro, S.; Mesquita, F.C.L.; Hall, W.W.; Ishak, M.O.G.; Ishak, R. Serological evidence of HTLV-I and HTLV-II coinfections in HIV-1 positive patients in Belém, state of Pará, Brazil. Mem Inst Oswaldo Cruz, Rio de Janeiro. 1998; 93(3), 407-409. [CrossRef]
- Laurentino, R.V.; Lopes, I.G.L.; Azevedo, V.N.; Machado, L.F.A.; Moreira, M.R.C.; Lobato, L.; Ishak, M.O.G.; Ishak, R.; Vallinoto, A.C.R. Molecular characterization of human T-cell lymphotropic virus coinfecting human immunodeficiency virus 1 infected patients in the Amazon region of Brazil. Mem Inst Oswaldo Cruz. 2005; 100(4), 371-376. [CrossRef]
- Alencar, S.P.; Souza, M.C.; Fonseca, R.R.S.; Menezes, C.R.; Azevedo, V.N.; Ribeiro, A.L.R.; Lima, S.S.; Laurentino, R.V.; Barbosa, M.A.A.P.; Freitas, F.B.; Oliveira-Filho, A.B.; Machado, L.F.A. Prevalence and molecular epidemiology of human T-lymphotropic virus (HTLV) infection in people living with HIV/AIDS in the Pará state, Amazon region of Brazil. Front Microbiol. 2020; 11, 572381. [CrossRef]
- Brites, C.; Goyanna, F.; França, L.G.; Pedroso C.; Netto, E.M.; Adriano, S.; Sampaio, J.; Harrington Jr, W. Coinfection by HTLV-I/II is associated with an increased risk of strongyloidiasis and delay in starting antiretroviral therapy for AIDS patients. Braz J Infect Dis. 2011; 15(1), 6-11. [CrossRef]
- Pereira, F.M.; Santos, F.L.N.; Silva, Â.A.O.; Nascimento, N.M.; Almeida, M.C.C.; Carreiro, R.P.; Galvão-Castro, B.; Grassi, M.F.R. Distribution of human immunodeficiency virus and human T-leukemia virus co-infection in Bahia, Brazil. Front Med. 2022; 8, 788176. [CrossRef]
- de Oliveira, E.H.; Oliveira-Filho, A.B.; Souza, L.A.; da Silva, L.V.; Ishak, M.O.G.; Ishak, R.; Vallinoto, A.C.R. Human T-cell lymphotropic virus in patients infected with HIV-1: Molecular epidemiology and risk factors for transmission in Piaui, Northeastern Brazil. Curr HIV Res. 2012; 10(8), 700-707. [CrossRef]
- Santos de Souza, M.; Prado Gonçales, J.; Santos de Morais, V.M.; Silva Júnior, J.V.J.; Lopes, T.R.R.; Costa, J.E.F.D.; Côelho, M.R.C.D. Prevalence and risk factor analysis for HIV/HTLV 1/2 coinfection in Paraíba state, Brazil. J Infect Dev Ctries. 2021; 15(10), 1551-1554. [CrossRef]
- Etzel, A.; Shibata, G.; Rozman, M.; Jorge, M.L.S.G.; Damas, C.D.; Segurado, A.A.C. HTLV-1 and HTLV-2 infections in HIV-infected individuals from Santos, Brazil: Seroprevalence and risk factors. JAIDS. 2001; 26(2), 185-190. Available online: https://journals.lww.com/jaids/abstract/2001/02010/htlv_1_and_htlv_2_infections_in_hiv_infected.13.aspx (accessed on 24 August 2023).
- Kleine-Neto, W.; SanabaniI, S.S.; Jamal, L.F.; Sabino, E.C. Prevalence, risk factors and genetic characterization of human T-cell lymphotropic virus types 1 and 2 in patients infected with human immunodeficiency virus type 1 in the cities of Ribeirão Preto and São Paulo. Rev Soc Bras Med Trop. 2009; 42 (3), 264-270. [CrossRef]
- Barcellos, N.T.; Fuchs, S.C.; Mondini, L.G.; Murphy, E.L. Human T lymphotropic virus type I/II infection: Prevalence and risk factors in individuals testing for HIV in counseling centers from Southern Brazil. Sex Transm Dis. 2006; 33(5), 302–306. [CrossRef]
- Galetto, L.R.; Lunge,V.R.; Béria, J.U.; Tietzmann, D.C.; Stein A.T.; Simon, D. Prevalence and risk factors for human T cell lymphotropic virus infection in Southern Brazilian HIV-positive patients. AIDS Res Hum Retroviruses. 2014; 30(9), 907-911. [CrossRef]
- Chequer, P.; Marins, J.R.P.; Possas, C.; Valero, J.D.A.; Bastos, F.I.; Castilho, E.; Hearst, N. AIDS research in Brazil. AIDS. 2005; 19 (suppl 4), S1–S3. [CrossRef]
- Okie, S. Fighting HIV – lessons from Brazil. N Engl J Med. 2006; 354: 1977–1981. [CrossRef]
- Boletim Epidemiológico. HIV – AIDS 2022. Secretaria de Vigilância em Saúde, Ministério da Saúde, Número Especial. Dez. 2022. Brasília. Available online: https://www.gov.br/aids/pt-br/centrais-de-conteudo/boletins-epidemiologicos/2022/hiv-aids/boletim_hiv_aids_-2022_internet_31-01-23.pdf/view (accessed on 17 July 2023).
- Colón-López, V.; Miranda-De León, S.; Machin-Rivera, M.; Soto-Abreu, R.; Marrero-Cajigas, E.L.; Rolón-Colón, Y.; Valencia-Torres, I.M.; Suárez-Pérez, E.L. New diagnoses among HIV+ men and women in Puerto Rico: Data from the HIV surveillance system 2003-2014. P R Health Sci J. 2019; 38(1), 33-39. PMID: 30924913. Available online: https://prhsj.rcm.upr.edu/index.php/prhsj/article/viewFile/1772/1171 (accessed on 22 August 2023).
- Agwu, A. Sexuality, sexual health, and sexually transmitted infections in adolescents and young adults. Top Antivir Med. 2020; 28(2), 459-462. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7482983/ (accessed on 22 August 2023).
- The path that ends AIDS: UNAIDS Global AIDS Update 2023. Geneva: Joint United Nations Programme on HIV/AIDS; 2023. Licence: CC BY-NC-SA 3.0 IGO. Available online: https://thepath.unaids.org/wp-content/themes/unaids2023/assets/files/2023_report.pdf (accessed on 22 August 2023).
- Martin, F.; Tagaya, Y.; Gallo, R. Time to eradicate HTLV-1: An open letter to WHO. Lancet. 2018; 391(10133), 1893-1894. [CrossRef]
- WHO. Human T-lymphotropic virus type 1: Technical report. 2021 Available online: https://www.who.int/publications/i/item/9789240020221 (accessed on 24 August 2023).
- Rosadas, C.; Menezes, M.L.B.; Galvão-Castro, B.; Assone, T.; Miranda, A.E.; Aragon, M.; Caterino-de-Araujo, A.; Taylor, G.P.; Ishak, R. Blocking HTLV-1/2 silent transmission in Brazil: Current public health policies and proposal of additional strategies. PLoS Negl Trop Dis. 2021; 15(9), e0009717. [CrossRef]
- Miranda, A.E.; Rosadas, C.; Assone, T.; Pereira, G.F.M.; Vallinoto, A.C.R.; Ishak, R. Strengths, Weaknesses, Opportunities and Threats (SWOT) analysis of the implementation of public health policies on HTLV-1 in Brazil. Front Med. 2022; 9:859115. [CrossRef]
- Sagara, Y.; Nakamura, H.; Satake, M.; Watanabe, T.; Hamaguchi, I. Increasing horizontal transmission of human T-cell leukemia virus type 1 in adolescents and young adults in Japan. J Clin Virol. 2022; 157, 105324. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



