
Submitted:
04 September 2023
Posted:
06 September 2023
You are already at the latest version
Abstract
The functional capacity of the cervical spine plays a central role in healthy living. This study evaluated and created a comprehensive strength, range of motion (ROM), and musculoskeletal pain profile of the cervical spine in young adults. 60 physically active individuals (30 males/30 females; 19-24 year-old) participated in the study. Cervical ROM (forward flexion, extension, lateral flexion, and rotation), maximal isometric strength (forward flexion, extension, lateral flexion), and musculoskeletal pains were assessed using an electronic goniometer, a handheld dynamometer, and the Nordic questionnaire, respectively. Data analysis revealed that: a) fe-males had higher ROM values, during extension and lateral flexion, than males (p<0.05), b) males had higher absolute strength values than females in all movement directions, higher rela-tive strength values/body mass (at forward flexion) and flexion/extension ratio values (p<0.05), c) ROM and strength values were not significantly different between right-left sides (p>0.05), d) a great proportion (43.3%) of the participants had cervical pains (no sex-related differences) and e) cervical strength showed significant small negative correlation with pains (p<0.05; r=-0.225 to -0.345). The reference values created may be used by health and fitness professionals to exten-sively evaluate the cervical spine and to design specific exercise programs for injury prevention and rehabilitation.
Keywords:
neck
; isometric assessment
; hand‐held dynamometer
; functional capacity
; cervical flexion/extension ratio
; injury prevention
; strength asymmetries
; rehabilitation
; sex effect
1. Introduction
The cervical spine consists of the seven first vertebrae of the spine and plays an important role in daily life because it supports the head, surrounds and protects the spinal cord, and is responsible for a wide range of head and neck motions [1]. Different factors such as the adoption of sedentary life (reduced physical activity), the poor ergonomic conditions (inadequate posture using electronic devices, repetitive and hurried movements, long static and sitting positions, poor sleep quality, etc.), in conjunction with different individual (age, sex, musculoskeletal pain history, etc.) and psychosocial factors (stress, anxiety, depression, etc.), may affect the prevalence of cervical pain in the adult population [2,3,4,5,6,7,8,9,10,11]; although, future studies are needed to strengthen these findings. Nowadays, cervical pain is one of the most common musculoskeletal disorders (prevalence ranged: from 17% to 75%) [4,6,12,13,14,15] with detrimental effects not only for the individual itself but also for the society and economy in general. There is evidence that cervical pain is associated with reduced quality of life, increased morbidity and disability, increased sick leaves and health care costs, and reduced work productivity [4,14,16,17].
For this reason, the protection of the cervical spine and the maintenance of satisfactory functional capacity levels (range of motion and strength) in the specific body area is of crucial importance [18] for healthy and independent living. The timely and systematic evaluation of cervical range of motion and isometric strength, using specialized tests, can decisively contribute to injury prevention and rehabilitation process of the cervical joint; since a good level of them seems to have beneficial effects on pain elimination [19,20]. The above findings are strengthened by previous investigations, which report that individuals with neck pain, loss of cervical lordosis, migraines, or whiplash show lower levels of cervical strength and/or range of motion compared to healthy individuals [19,20,21,22,23].
In the scientific literature, several studies evaluated and created indicative values or norms for cervical isometric strength using a great variety of devices (fixed frame dynamometers, computerized dynamometers, or hand-held dynamometers), testing positions (standing or sitting or supine or prone or quadruped) and protocols in different populations such as workers, athletes and non-athletes, younger and older individuals, males and females [14,18,19,24,25,26,27,28,29,30,31,32,33,34,35]. It should be mentioned that most of the aforementioned studies have mainly focused on absolute cervical isometric strength values reporting conflicting results concerning age- and sex-related effects [25,30,34,35]; while there is limited information regarding a) the relative cervical isometric strength values, b) the cervical strength asymmetries between left and right side as well as c) the cervical flexion to extension ratios. However, the evaluation and calculation of all the above strength parameters may provide a more complete picture of the proper function, stability, and balance of the cervical spine. There is a notion that the muscular imbalance between the strength of cervical extensors and flexors muscles can be negatively correlated with the stabilization of the cervical spine [21,28]. It has, also, been reported that low levels of cervical strength as well as cervical flexor-to-extensor ratio values less than 60% are associated with an increased prevalence and incidence of sport-related concussion in adolescents and adults [28,36,37,38]; while other studies reported no significant relationship between cervical strength and concussion [39].
The measurement and evaluation of the range of motion constitute a basic component of the physical examination of the cervical joint. Numerous studies evaluated and created indicative values or norms for cervical range of motion using multiple radiological (functional x-rays) or non-radiological devices (goniometers, inclinometers, electromagnetic, ultrasonic, and optoelectronic systems), testing positions and protocols in different populations showing wide variations in the measured values [40,41,42]. Age and sex are two of the most important factors that could affect the cervical range of motion; however, previous studies that examined the age- and sex-related effects on cervical range of motion demonstrated controversial results [40,43,44]. Several studies stated that a) females have greater cervical ROM than males and b) cervical ROM is reduced with increasing age; whereas other studies reported no significant differences between males and females as well as between different ages [40,43,44]. Therefore, the influence of sex or age on cervical ROM still merits discussion to draw safer conclusions [40].
Taking all the above into consideration, the main objective of this study was to evaluate and create a comprehensive strength, range of motion (ROM), and musculoskeletal pain profile of the cervical spine, using simple, handy, and portable equipment, in young adults (19 - 24 years old). In more detail, the specific objectives of this study were:
- a)
- to evaluate maximal cervical isometric strength (forward flexion, extension, lateral flexion) in absolute values using a handheld dynamometer, and to calculate cervical isometric strength in relative values (in relation to body mass and body height), flexion/extension ratios and strength asymmetries between left and right side,
- b)
- to evaluate the range of motion in all directions of movements (forward flexion, extension, lateral flexion, and rotation) using a digital goniometer, and to examine possible differences between left and right sides,
- c)
- to examine the relationship among cervical strength, range of motion, and musculoskeletal pain at the cervical joint,
- d)
- to examine the sex-related effect on cervical strength, range of motion (ROM), and musculoskeletal pain profile in young adults.
2. Materials and Methods
2.1. Participants
Sixty (30 women and 30 men) healthy young adults (19-24 years old), volunteered to participate in the present study (Table 1). All the participants were physically active and participated 3 times per week (1 h/day) in non-organized physical activities, without doing specialized training for the cervical spine. The participants were healthy and free of any illness, disease, or injury at the cervical spine in the last 6 months and did not report the use of any medication. Before the initiation of the study, the participants were informed about the experimental procedures and signed an informed consent form. The study was approved by the Ethics Committee of the University of Thessaly.
2.2. Study design
One week before the start of the study, the participants were familiarized with the experimental testing protocols. Then, the measurements were performed on one day, with the evaluation of cervical range of motion to precede the evaluation of cervical strength. Before the evaluation of the cervical range of motion and cervical strength, the participants were warming up. The warm-up protocol was performed from a sitting position in a chair (with the back straight, the hands on the thighs of the legs, and the feet flat on the floor) and included cervical dynamic movements (forward flexion, extension, lateral flexion and rotation) of 10 repetitions, stretching exercises (forward flexion, extension, lateral flexion and rotation) of 10 second and submaximal isometric contractions at the cervical spine (flexion, extension, lateral flexion) with the participant's hand as resistance. The measurements took place at the Training Laboratory of the Department of Physical Education and Sports Science of the University of Thessaly and were performed by the same investigator and under the same conditions.
2.3. Testing Procedures
Anthropometric characteristics, musculoskeletal pains, cervical range of motion (forward flexion, extension, lateral flexion, and rotation), and cervical strength (forward flexion, extension, lateral flexion) were measured.
2.3.1. Anthropometric characteristics
Body mass and body height were measured using a calibrated physician’s scale (Seca model 755, Seca, Hamburg, Germany) and a telescopic height rod respectively, according to the recommendations of the American College of Sports Medicine - ACSM [45].
2.3.2. Musculoskeletal pains
Duration and intensity (using a 10-point scale) of pain in the cervical spine, days off from everyday activities, and difficulties in daily activities due to pain, were evaluated, using the Nordic questionnaire [46].
2.3.3. Cervical Range of Motion - Cervical strength
2.3.3.1. Testing position
Both cervical range of motion and cervical strength were measured in a standardized sitting position to minimize errors and movement compensation. It should be mentioned that special emphasis was placed on the selection of the appropriate chair used for the ROM and strength measurements. In more detail, the criteria for choosing the appropriate chair were as follows: (a) a stable chair without wheels and armrests, (b) a chair with a back for better lumbar spine support (not a softback), and (c) a height adjusted chair depending on the height of the participants, so that the feet could be flat on the floor with a knee angle approximately at 90°. During the measurements, the participants were positioned in a sitting position with their backs straight and stabilized with Velcro straps in the back of the chair, their hands on the thighs of their legs, and their feet flat on the floor (Photo 1). At the beginning of every trial, the participant started from a fixed point with his/her head in the neutral position.

Photo 1. Set-up of the participant during the cervical range of motion and strength measurements. .
2.3.3.2. Range of motion measurement
Cervical range of motion was assessed in 4 directions: a) extension b) forward flexion, c) lateral flexion (right & left), and d) rotation (right & left) using an electronic goniometer (KINVENT K-FORCE) and the values demonstrated on degrees (Photo 2). The examiner placed and stabilized with velcro strap the electronic goniometer within the center of the participant's forehead. For each direction of movement, the participant performed 3 maximal trials with 20 s rest between each trial and 1 min rest between each direction of movement, and the best score (at each direction) was considered for analysis.

Photo 2. Cervical range of motion measurements (a. extension, b. forward flexion, c. lateral flexion, and d. rotation).
2.3.3.3. Maximal isometric strength measurement
Maximal isometric cervical strength was assessed in three directions: a) forward flexion, b) extension, and c) lateral flexion (right & left) using a handheld dynamometer (K-Force Dynamometer Muscle Controller) (Photo 3). During the measurements, the investigator placed the hand-held dynamometer in the appropriate position, and then he held resistance with both hands (to the participant's strength) so that the head and neck remained in the neutral position. In more detail, the hand-held dynamometer was placed: a) in the center of the forehead just superior to the eyebrows for the forward flexion test, b) slightly superior to the external occipital protuberance for the extension test, and c) on the lateral aspect of the head just superior to the ear for lateral (right and left) flexion tests [18,35] (Photo 3).
In each direction of movement, the participants performed 3 maximal trials (duration of isometric contraction: 5 s) with 1 min rest between each trial and 1 min rest between each direction, and the best score was considered for analysis. The absolute cervical strength values (kg) were assessed in each direction of movement, and the relative cervical strength values per unit of body mass (kg of cervical strength/kg of body mass) and body height (kg of cervical strength/cm of body height) were calculated. The cervical flexion (CF) to cervical extension (CE) strength ratio was, also, calculated using the following equation: CervicalF/E ratio = (Cervical flexion strength/ Cervical extension strength) * 100.
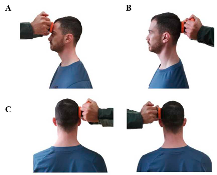
Photo 3. Cervical maximal isometric strength measurements (a. forward flexion, b. extension, and c. lateral flexion).
2.4. Statistics
In our study, all the statistical analyses were performed using IBM SPSS Statistics v.26 software (IBM Corporation, Armonk, NY, USA), and the results are presented as means ± standard deviations. A statistical power analysis (software package GPower 3.0) before the initiation of the study indicated that a total number of 60 participants (30 participants in each sex group) would yield adequate power (>0.85) and a level of significance (<0.05). The normality of data was examined using the Kolmogorov-Smirnov test (all variables followed the normal distribution). Independent samples t-tests were used to investigate possible differences in cervical range of motion, maximal strength, and musculoskeletal pains between males and females; while paired t-tests were used to examine possible differences in range of motion and strength values between right and left sides. Furthermore, Bivariate correlation analyses were used to examine the association among neck pain, cervical strength, and range of motion as well as among cervical strength, range of motion, and anthropometric characteristics (body mass and body height). Cohen's effect sizes were also calculated using the equation: d=difference between means/pooled SD. The level of significance for all statistical analyses was set at p<0.05.
3. Results
3.1. Cervical range of motion
Independent samples t-test showed that females had higher range of motion values at extension (t58 = - 4.03, p < 0.01; Cohen d: 1.04; mean % difference: 14.7), as well as at right (t58 = -2.30, p < 0.05; Cohen d: 0.60; mean % difference: 10.5) and left lateral flexion (t58 = -2.70, p < 0.05; Cohen d: 0.70; mean % difference: 11.1) (Table 2). On the other hand, no significant differences were observed between males and females on the range of motion values at forward flexion (t58 = 0.52, p > 0.05) as well as at right (t58 = -0.97, p > 0.05) and left rotation (t58 = -1.48, p > 0.05).
Moreover, paired samples t-test analyses showed that there are no statistically significant differences between right and left lateral flexion (t59 = - 0.51; p > 0.05; mean % difference: 0.27-0.89) and right and left rotation (t59 = -1.87; p > 0.05; mean % difference: 1.8-2.8) both in males and females.
3.2. Cervical isometric strength
3.2.1. Absolute values
Independent samples t-test showed that males have statistically greater values at cervical strength in forward flexion (t58 = 7.82; p = 0.000; Cohen d: 2.12; mean % difference: 37.7), extension (t58 = 4.04; p = 0.000; Cohen d: 1.06; mean % difference: 20.4), right lateral flexion (t58 = 4.07 p = 0.000; Cohen d: 1.08; mean % difference: 23.7) and left lateral flexion (t58 = 4.03; p = 0.000; Cohen d: 1.05; mean % difference: 23.3) as well as greater cervical flexion/extension ratio (t58 = 4.99; p = 0.000; Cohen d: 1.31; mean % difference: 21.8) than females (Table 3). Furthermore, paired samples t-test analyses showed that there are no statistically significant differences between right and left lateral flexion (t59 = - 1.42; p > 0.05) both in males (mean % difference: 1.3) and females (mean % difference: 1.8).
3.2.2. Relative values
When the cervical strength values were adjusted to body height, independent samples t-test showed that males have statistically greater strength values at forward flexion (t58 = 7.05; p = 0.000; Cohen d: 2; mean % difference: 30), extension (t58 = 2.82; p = 0.007; Cohen d: 0.5; mean % difference: 9), right lateral flexion (t58 = 3.03; p = 0.004; Cohen d: 0.67; mean % difference: 12.5) and left lateral flexion (t58 = 2.98; p = 0.004; Cohen d: 0.5; mean % difference: 12.4) than females (Figure 1).
On the other hand, when the values were adjusted to body mass, independent samples t-test showed no statistically significant differences between males and females in cervical extension (t58 = 0.66; p = 0.513), right lateral flexion (t58 = 1.39; p = 0.170) and left lateral flexion (t58 = 1.33; p = 0.188) (Figure 2). The only significant difference between males and females was found in forward flexion; where males showed greater relative cervical strength values than females (t58 = 5.86; p = 0.000; Cohen d: 1.43; mean % difference: 21.7).
3.3. Relationship of anthropometric characteristics with cervical strength and ROM
Bivariate correlation analysis showed a significant positive correlation of body mass with cervical forward flexion (r = 0.716, p = 0.000), extension (r = 0.619, p = 0.000), right lateral flexion (r = 0.657, p = 0.000) and left lateral flexion (r = 0.647, p = 0.000) in the total sample (males and females). Furthermore, Bivariate correlation analysis showed a significant positive correlation of body height with cervical forward flexion (r = 0.665, p = 0.000), extension (r = 0.480, p = 0.000), right lateral flexion (r = 0.465, p = 0.000) and left lateral flexion (r = 0.464, p = 0.000) in the total sample (males and females).
However, no significant relationship was observed between anthropometric characteristics (body mass and body height) and range of motion measurements both in males and females (p > .05).
3.4. Neck pain
According to data analysis, 43.3% of the total sample presented cervical pain in the last 2 months (no significant difference in the prevalence of pain was observed between males and females); while 56.7% of the sample had no cervical pain.
In those who experienced cervical pain, the mean duration of pain (total days of pain in 2 months) was 2.54 ± 0.99 days and the mean intensity of pain (from 1 to 10) was 3.65 ± 1.41; while the days off from daily activities due to cervical pain were 0.46 ± 1.96 days and the days with difficulties in daily activities due to cervical pain were 3.81 ± 7.14 days. It should be mentioned that independent samples t-tests showed that there were no significant differences between males and females at duration and intensity of cervical pain as well as at days off from daily activities due to cervical pain (p>0.05).
Bivariate correlation analysis showed a statistically significant small negative correlation of the duration of cervical pain (total days of pain) with cervical forward flexion strength (r = - 0.288, p< 0.05), extension strength (r = - 0.255, p < 0.05), right lateral flexion strength (r = - 0.287, p < 0.05) and left lateral flexion strength (r = - 0.345, p < 0.05). On the contrary, Bivariate correlation analysis showed that cervical range of motion did not significantly associate with cervical pain (p>0.05).
4. Discussion
An adequate level of the functional capacity (range of motion and strength) of the cervical joint is very important for everyday life as well as for injury prevention and rehabilitation processes [18,19]. During the last decades, several investigators have tried to find the most effective exercise approach to improve or maintain the functional capacity of the cervical joint, eliminating at the same time the detrimental effect and the global burden of cervical pain in different populations [47]. A key factor that plays one of the most central roles in the successful designing, implementation, and guidance of a specific exercise program for the cervical joint is the comprehensive assessment of the existing situation (weaknesses, asymmetries, imbalances, musculoskeletal pain history, mobility level, etc.) of the specific body area. Thus, the most important aspect of this study is that it evaluated and created an extensive strength (absolute and relative values, strength asymmetries, reciprocal ratios), range of motion (ROM), and musculoskeletal pain profile of the cervical spine, using simple, accessible and portable equipment (hand-held dynamometer for strength measurements and digital goniometer for range of motion measurements), in young physically active males and females.
In the present study, we documented a sex-related effect in absolute cervical strength values, with males presenting greater values (20-38%, depending on the movement direction) than females in all the tested movement directions. The results of this study are in line with previous investigations in the scientific literature in which males have greater absolute cervical strength values in comparison with females [24,25,26,29,35]. The sex-related differences in cervical strength values may be attributed to different factors, such as the head and neck anthropometric parameters and geometry/morphology (i.e., females have smaller external neck and vertebral dimensions as well as more slender necks and less neck cross-sectional area) [29], the basic anthropometric characteristics (body mass and/or body height) [26], the higher concentrations of anabolic hormones observed in males individuals and probably the higher voluntary neural activity of the muscle actions [48,49] as well as the different lifestyle behaviors (i.e., higher levels of physical activity observed in males compared to females).
As mentioned earlier, the basic anthropometric characteristics (body mass and body height) could affect absolute cervical strength values. This notion has been strengthened by the results of this and previous studies which reported a significant relationship between body mass, body height, or body mass index with cervical strength measurements [24,33], although there are studies which did not found a significant relationship between basic anthropometric characteristics and cervical strength values [25]. It seems that the correlation of basic anthropometric characteristics (especially of body mass) with cervical strength is higher in physically active and trained individuals; whereas, this correlation in a normal population is much lower [26,27]. Furthermore, some researchers find sex-related differences in the correlation of basic anthropometric characteristics with cervical strength [26,30]. Specifically, Garces et al. [26] showed a high positive correlation between weight and height with isometric cervical strength in men, while women showed a significant correlation only between height and cervical isometric strength. In the same context, Jordan and colleagues [30] found a highly positive correlation between height and cervical isometric strength only in men; while they did not find any correlation in females. It should be, also, mentioned that in the present study, when the absolute cervical strength values were adjusted to body height significant sex-related differences (males reported greater values than females) remained after height adjustment, however, the differences between males and females were significantly lower (forward flexion: 30%, extension: 9%, lateral flexion: 12.4-12.5%) compared to that observed in absolute values (forward flexion: 37.7%, extension: 20.4%, lateral flexion: 23.3-23.7%). On the other hand, when the absolute values were adjusted to body weight the only sex-related difference between males and females was observed in forward flexion (21.7%); while, in other movement directions (extension, right and left lateral flexion) no significant differences were observed between males and females. The results of this study are in line with that of Peolsson et al. [32] who reported greater sex-related differences in absolute cervical strength values (mean difference 55%) compared to relative values per body mass (mean difference 30%) or body mass index (mean difference 41%). Taking into account the above findings of the studies, further investigations are needed to draw safer conclusions regarding the possible correlation between anthropometric characteristics and cervical isometric strength in males and females.
The reciprocal ratios as well as the strength asymmetries between the right and left sides should not be neglected, as they can cause muscle imbalances and affect the overall stability of the cervical spine [21,25]. In the present study, we found no significant difference in lateral flexion cervical strength between the right and left side (mean % difference: 1.3 - 1.8) both in males and females. The results of the present study are in agreement with previous studies that also reported no significant differences between right and left lateral flexion in adults and adolescents [18,24,50], due to the bilateral arrangement of the involved musculature in different activities of daily life as well as in different sport activities. On the other hand, Chiu et al. [25] demonstrated that lateral flexion of the right side is 11% stronger than that of the left side in men, but no difference was found in women. The authors of the above study [25] hypothesized that the sex-related difference in strength asymmetry between the right and left sides may be because men were more involved in heavy manual work and most people are right-handed, leading to higher demand on the neck muscles over the right side in male individuals. Moreover, Vernon et al. [23] also reported a 6-8% difference in cervical lateral flexion strength between the right and left sides in young male adults. However, it seems that further investigations are needed to document if there are cervical strength asymmetries between the right and left sides in males and females.
Regarding the cervical flexion to extension ratio, in the present study, we reported a significant difference between males and females, with males (mean ratio value: 89.17%) presenting greater ratio values than females (mean ratio value: 69.75%). Most previous studies that evaluated cervical flexion to extension ratio in healthy males and females, using different dynamometers, reported values ranging approximately from 60-75% [18,21,23,26]. In the present study, the cervical flexion to extension ratio value for females agrees with the normal values reported in the international literature; while the mean cervical flexion to extension ratio value in males is much higher. In the present study, the greater flexion-to-extension ratio value in males compared to females may be attributed to the greater difference observed in cervical forward flexion strength. Indeed, we reported almost double sex-related differences in cervical flexion compared to extension strength values. The finding of this study agrees with a previous study which found greater sex-related differences in cervical flexion compared to extension (females have 32% weaker neck strength during flexion and 20% during extension than males) [29]. From the results of the present study, it seems that males should emphasize specific exercise programs for the improvement, especially of cervical extensor muscles to change the flexion-to-extension ratio values to more normal levels according to the scientific literature. This is of crucial importance since there is a notion that high cervical flexion to extension ratio values, as observed in males of the present study, may be associated with the loss of cervical lordosis [21] and the dropped head syndrome [51].
Concerning cervical ROM, many studies evaluated and created indicative values or norms in different age groups but it seems that exist quite large differences between them [40], making the comparisons of ROM values difficult among studies. The reported measurements vary considerably, due to differences in measurement instruments (radiological or non-radiological), testing positions and setups (constrained or unconstrained), testing protocols, and subjects' differences [40,41,42]. In our study females showed significantly higher values in extension (mean % difference: 14.7) and both right (mean % difference: 10.5, with medium effect size) and left (mean % difference: 11, with medium effect size) lateral flexion in comparison with males; while no differences were observed on forward flexion and rotation (no differences in ROM values were observed between right and left side at lateral flexion and rotation both in males and females). The sex-related difference in cervical ROM has been made "a subject of debate" in an attempt to draw safer conclusions on this topic. Several studies showed that females overcome the males at cervical ROM and others showed no significant differences between males and females [40,41,42,43,44]. Differences in subjects' characteristics as well as in testing protocols may account for these equivocal findings among studies regarding the sex-related effect on cervical ROM.
Previous studies reported that age is an important factor that could affect sex-related differences in cervical ROM [40,43]. According to the systematic review and meta-analysis of Pan et al. [40] in the younger age group (20s), no sex-related differences in the cervical ROM were observed, probably because in most cases the youngest age group exhibited the greatest ROM level. On the other hand, males in their 30s and 40s demonstrated lower ROM values than females both in sagittal and axial motions. It is interesting to note, that males in their 50s displayed greater ROM values (although not significant) than females [40]. The authors hypothesized that the females during this age experienced menopause, which could decrease spine mobility [52,53]. After this period, females in their 60s again showed greater cervical ROM values than males.
An additional important finding of this study is that 43.3% of the total sample presented cervical pain in the last 2 months. Previous studies reported a similar prevalence of neck pain in young adults as well as in middle-aged individuals [13,14,15]. In the present study, no significant differences were observed between males and females in the musculoskeletal pain parameters (prevalence of pain, duration, and intensity of pain, negative impact of musculoskeletal pains in daily activities). Other studies in the scientific literature reported conflicting results regarding the sex-related effect on musculoskeletal pain of the cervical joint. Several studies reported that cervical pain is more common in females than males greater; while other studies which are in line with the results of the present study reported no differences in cervical pain between males and females [54]. Previous investigators, who demonstrated sex-related differences in musculoskeletal pain of the cervical joint, mentioned that the lower cervical strength level is an important factor that may be liable for this situation [33,55]. It is not clear whether weak cervical muscles promote cervical pain or if cervical pain results in weaker musculature, but it seems that there is a connection between cervical pain and weakness [33]. In the present study, we also found a significant negative association between cervical pain and cervical strength; while no significant association was observed between range of motion values and cervical pain. The association between cervical range of motion and musculoskeletal pain shows conflicting results in the international literature, strengthening the importance of future studies on this topic. Some studies found significant associations between cervical range of motion and pain and others did not found significant associations [20,42].
Finally, the results of this study and previous studies reinforce the importance of designing and implementing specific interventions for the improvement of the functional capacity (especially of strength) of the cervical joint as well as for the prevention and rehabilitation of cervical musculoskeletal pains in young adults. This is of crucial importance since low back and neck pain are the second leading causes of years lived with disability (YLD) for young adults aged 20-24 years, according to the Global Burden of Disease (GBD) study [56]. Young adulthood (often referred to as the age span between 18 and 29 years) is the transitional stage between adolescence and adulthood, which is characterized by wide changes, handling choices and opportunities [57]. Previous studies have shown that choices made during young adulthood influence overall health and well-being [58] later in life. Therefore, previous investigators reported that this period (young adulthood) is vulnerable to future musculoskeletal health [59], reducing the incidence of cervical pain and its’ consequences (reduced productivity, impaired quality of life, disability, etc.) in late adulthood.
This study has some limitations that could affect its outcomes, and, as a result, their generalization. Firstly, the findings of this study are clearly limited to young (19-24 years old) physically active males and females, without any chronic health problem. Future studies could evaluate and create indicative values for cervical strength, ROM and musculoskeletal pain in other age-groups (children and adolescents, middle-aged and older individuals) as well as in individuals with different health and physical activity / training status. Furthermore, the results of this study are limited to the testing position (sitting position in a chair), the testing protocols and the equipment (hand-held dynamometer for cervical strength measurements and digital goniometer for cervical ROM measurements) used for the evaluation of cervical strength and ROM. Another limitation of this study is the fact that, except of the basic anthropometric characteristics (body mass and body height), we did not measure any head or neck anthropometric characteristics (absolute and relative neck length, neck circumference, head circumference etc.) in order to examine their association with cervical strength and ROM values in males and females. Finally, the sample size (although yielded adequate power as mentioned in the methods section) may be an additional limitation of this study. A larger sample could further strengthen the findings of the present study.
5. Conclusions
The data presented in this study serve to provide a comprehensive strength, ROM, and musculoskeletal pain profile of the cervical spine in young males and females to assist health and fitness professionals in extensively evaluating the functional capacity of the cervical spine, as well as to more efficiently design, implement and guide specialized exercise programs for injury prevention and rehabilitation. From the results of the present study, it seems that young physically active males have higher absolute cervical strength values than females (greater difference observed in cervical forward flexion strength). It should be mentioned that the differences in basic anthropometric characteristics (in body height, but especially in body mass) between males and females affect the absolute cervical strength values. In the present study, no cervical strength asymmetries between the right and left sides were observed in males and females; while the cervical flexion-to-extension ratio was greater in males compared to females. The cervical flexion-to-extension ratio value observed in females is in agreement with the proposed normal values; while the cervical flexion-to-extension ratio value in males is much higher than the proposed normal values. From the results of this study, it seems that males should emphasize the improvement of cervical extensor muscles to change the flexion-to-extension ratio values to more normal levels. Concerning the range of motion, females have higher ROM values, during extension and lateral flexion, than males; while ROM values during forward flexion and right and left rotation did not differ between males and females. It should be mentioned that no ROM differences between the right and left sides were observed in males and females. Finally, from the results of the present study, it seems that a significant proportion of the sample (both males and females) (43.3%) have cervical pains (no sex-related differences). This finding strengthens the importance of specific exercise programs for functional capacity improvement (especially of cervical strength that showed significant correlation with cervical pain) as well as for injury prevention and rehabilitation of the cervical joint.
Author Contributions
Conceptualization, C.B., K.K. and V.G.; methodology, C.B. and V.G.; investigation, C.B. and V.G.; data curation, C.B. and K.K; writing - original draft preparation, C.B.; writing - review and editing, K.K. and V.G.; supervision, V.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the University of Thessaly (protocol code: 1857 and date of approval: 8-12-2021).
Informed Consent Statement
Informed consent was obtained from all subjects and participant’s parents involved in the study.
Data Availability Statement
Data is unavailable due to privacy or ethical restrictions.
Acknowledgments
We wish to thank our subjects for their participation in the present study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kaiser JT, Reddy V, Lugo-Pico JG. Anatomy, Head and Neck: Cervical Vertebrae. [Updated 2022 Oct 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. Available from: https://www.ncbi.nlm.nih. 5397.
- Cimmino MA, Ferrone C, Cutolo M. Epidemiology of chronic musculoskeletal pain. Best Pract Res Clin Rheumatol. 2011;25:173-83. [CrossRef]
- Damasceno, G. M.; Ferreira, A. S.; Nogueira, L. A. C.; Reis, F. J. J.; Andrade, I.C.S.; Meziat-Filho, N. Text neck and neck pain in 18-21-year-old young adults. Eur Spine J. 2018, 27, 1249–1254. [Google Scholar] [CrossRef] [PubMed]
- Genebra CVDS, Maciel NM, Bento TPF, Simeão SFAP, Vitta A. Prevalence and factors associated with neck pain: a population-based study. Braz J Phys Ther. 2017 Jul-Aug;21(4):274-280. [CrossRef]
- Hansraj, K.K. Assessment of stresses in the cervical spine caused by posture and position of the head. Surg Technol Int. 2014, 25, 277–279. [Google Scholar] [PubMed]
- Kazeminasab S, Nejadghaderi SA, Amiri P, Pourfathi H, Araj-Khodaei M, Sullman MJM, Kolahi AA, Safiri S. Neck pain: global epidemiology, trends and risk factors. BMC Musculoskelet Disord. 2022 Jan 3;23(1):26. [CrossRef]
- Lee WH, Ko MS. Effect of sleep posture on neck muscle activity. J Phys Ther Sci. 2017 Jun;29(6):1021-1024. [CrossRef]
- Lei JX, Yang PF, Yang AL, Gong YF, Shang P, Yuan XC. Ergonomic Consideration in Pillow Height Determinants and Evaluation. Healthcare (Basel). 2021 Oct 7;9(10):1333. [CrossRef]
- Malchaire JB, Roquelaure Y, Cock N, Piette A, Vergracht S, Chiron H. Musculoskeletal complaints, functional capacity, personality and psychosocial factors. Int Arch Occup Environ Health. 2001 Oct;74(8):549-57. [CrossRef]
- Shahwan BS, D'emeh WM, Yacoub MI. Evaluation of computer workstations ergonomics and its relationship with reported musculoskeletal and visual symptoms among university employees in Jordan. Int J Occup Med Environ Health. 2022 Apr 11;35(2):141-156. [CrossRef]
- Walankar, P.P.; Kemkar, M.; Govekar, A.; Dhanwada, A. Musculoskeletal Pain and Risk Factors Associated with Smartphone Use in University Students. Indian J. Occup. Environ. Med. 2021, 25(4), 220–224. [Google Scholar] [PubMed]
- Algarni AD, Al-Saran Y, Al-Moawi A, Bin Dous A, Al-Ahaideb A, Kachanathu SJ. The Prevalence of and Factors Associated with Neck, Shoulder, and Low-Back Pains among Medical Students at University Hospitals in Central Saudi Arabia. Pain Res Treat. 2017;2017:1235706. [CrossRef]
- Fejer R, Kyvik KO, Hartvigsen J. The prevalence of neck pain in the world population: a systematic critical review of the literature. Eur Spine J. 2006 Jun;15(6):834-48. [CrossRef]
- Karatrantou K, Gerodimos V. A comprehensive wellness profile in sedentary office employees: Health, musculoskeletal pains, functional capacity, and physical fitness indices. Work. 2023;74(4):1481-1489. [CrossRef]
- Todd A, McNamara CL, Balaj M, Huijts T, Akhter N, Thomson K, Kasim A, Eikemo TA, Bambra C. The European epidemic: Pain prevalence and socioeconomic inequalities in pain across 19 European countries. Eur J Pain. 2019 Sep;23(8):1425-1436. [CrossRef]
- Daffner, S.D.; Hilibrand, A.S.; Hanscom, B.S.; Brislin, B.T. , Vaccaro, A.R., Albert, T.J. Impact of neck and arm pain on overall health status. J. Impact of neck and arm pain on overall health status. Spine. 2003, 28(17), 2030–5. [Google Scholar]
- IJzelenberg, W.; Burdorf, A. Risk factors for musculoskeletal symptoms and ensuing health care use and sick leave. Spine. 2005, 30(13), 1550–6. [Google Scholar] [CrossRef] [PubMed]
- Eagle, S. R. , Nagai, T., Morgan, P., Hendershot, R., & Sell, T. C. Naval Special Warfare (NSW) crewmen demonstrate diminished cervical strength and range of motion compared to NSW students. Work.
- De Loose, V.; Van den Oord, M.; Burnotte, F.; Van Tiggelen, D.; Stevens, V.; Cagnie, B.; Danneels, L.; Witvrouw, E. ; Functional assessment of the cervical spine in F-16 pilots with and without neck pain. Aviat Space Environ Med. 2009, 80(5), 477–81. [Google Scholar] [CrossRef] [PubMed]
- Stenneberg, M.S.; Rood, M.; de Bie, R.; Schmitt, M.A.; Cattrysse, E.; Scholten-Peeters, G. G. To What Degree Does Active Cervical Range of Motion Differ Between Patients With Neck Pain, Patients With Whiplash, and Those Without Neck Pain? A Systematic Review and Meta-Analysis. Arch Phys Med Rehabil. 2017, 98(7), 1407–1434. [Google Scholar] [CrossRef] [PubMed]
- Alpayci M, Şenköy E, Delen V, Şah V, Yazmalar L, Erden M, Toprak M, Kaplan Ş. Decreased neck muscle strength in patients with the loss of cervical lordosis. Clin Biomech (Bristol, Avon). 2016 Mar;33:98-102. [CrossRef]
- Shahidi B, Johnson CL, Curran-Everett D, Maluf KS. Reliability and group differences in quantitative cervicothoracic measures among individuals with and without chronic neck pain. BMC Musculoskelet Disord. 2012 Oct 31;13:215. [CrossRef]
- Vernon HT, Aker P, Aramenko M, Battershill D, Alepin A, Penner T. Evaluation of neck muscle strength with a modified sphygmomanometer dynamometer: reliability and validity. J Manipulative Physiol Ther. 1992 Jul-Aug;15(6):343-9. [PubMed]
- Catenaccio E, Mu W, Kaplan A, Fleysher R, Kim N, Bachrach T, Zughaft Sears M, Jaspan O, Caccese J, Kim M, Wagshul M, Stewart WF, Lipton RB, Lipton ML. Characterization of Neck Strength in Healthy Young Adults. PM R. 2017 Sep;9(9):884-891. [CrossRef]
- Chiu TT, Lam TH, Hedley AJ. Maximal isometric muscle strength of the cervical spine in healthy volunteers. Clin Rehabil. 2002 Nov;16(7):772-9. [CrossRef]
- Garcés GL, Medina D, Milutinovic L, Garavote P, Guerado E. Normative database of isometric cervical strength in a healthy population. Med Sci Sports Exerc. 2002 Mar;34(3):464-70. [CrossRef]
- Hamilton DF, Gatherer D, Jenkins PJ, Maclean JG, Hutchison JD, Nutton RW, Simpson AH. Age-related differences in the neck strength of adolescent rugby players: A cross-sectional cohort study of Scottish schoolchildren. Bone Joint Res. 2012 Jul 1;1(7):152-7. [CrossRef]
- Nutt S, McKay MJ, Gillies L, Peek K. Neck strength and concussion prevalence in football and rugby athletes. J Sci Med Sport. 2022 Aug;25(8):632-638. [CrossRef]
- Vasavada, A.N.; Danaraj, J.; Siegmund, G.P. ; Head and neck anthropometry, vertebral geometry and neck strength in height-matched men and women. J Biomech. 2008, 41(1), 114–121. [Google Scholar] [CrossRef]
- Jordan A, Mehlsen J, Bülow PM, Ostergaard K, Danneskiold-Samsøe B. Maximal isometric strength of the cervical musculature in 100 healthy volunteers. Spine (Phila Pa 1976). 1999 Jul 1;24(13):1343-8. [CrossRef]
- McBride L, James RS, Alsop S, Oxford SW. Intra and Inter-Rater Reliability of a Novel Isometric Test of Neck Strength. Sports (Basel). 2022 Dec 21;11(1):2. [CrossRef]
- Peolsson A, Oberg B, Hedlund R. Intra- and inter-tester reliability and reference values for isometric neck strength. Physiother Res Int. 2001;6(1):15-26. [CrossRef]
- Salo PK, Ylinen JJ, Mälkiä EA, Kautiainen H, Häkkinen AH. Isometric strength of the cervical flexor, extensor, and rotator muscles in 220 healthy females aged 20 to 59 years. J Orthop Sports Phys Ther. 2006 Jul;36(7):495-502. [CrossRef]
- Valkeinen H, Ylinen J, Mälkiä E, Alen M, Häkkinen K. Maximal force, force/time and activation/coactivation characteristics of the neck muscles in extension and flexion in healthy men and women at different ages. Eur J Appl Physiol. 2002 Dec;88(3):247-54. [CrossRef]
- Versteegh T, Beaudet D, Greenbaum M, Hellyer L, Tritton A, Walton D. Evaluating the reliability of a novel neck-strength assessment protocol for healthy adults using self-generated resistance with a hand-held dynamometer. Physiother Can. 2015 Winter;67(1):58-64. [CrossRef]
- Elliott J, Heron N, Versteegh T, Gilchrist IA, Webb M, Archbold P, Hart ND, Peek K. Injury Reduction Programs for Reducing the Incidence of Sport-Related Head and Neck Injuries Including Concussion: A Systematic Review. Sports Med. 2021 Nov;51(11):2373-2388. [CrossRef]
- Collins CL, Fletcher EN, Fields SK, Kluchurosky L, Rohrkemper MK, Comstock RD, Cantu RC. Neck strength: a protective factor reducing risk for concussion in high school sports. J Prim Prev. 2014 Oct;35(5):309-19. [CrossRef]
- Gillies L, McKay M, Kertanegara S, Huertas N, Nutt S, Peek K. The implementation of a neck strengthening exercise program in elite rugby union: A team case study over one season. Phys Ther Sport. 2022 May;55:248-255. [CrossRef]
- Garrett JM, Mastrorocco M, Peek K, van den Hoek DJ, McGuckian TB. The Relationship Between Neck Strength and Sports-Related Concussion in Team Sports: A Systematic Review With Meta-analysis. J Orthop Sports Phys Ther. 2023 Oct;0(10):1-9. [CrossRef]
- Pan F, Arshad R, Zander T, Reitmaier S, Schroll A, Schmidt H. The effect of age and sex on the cervical range of motion - A systematic review and meta-analysis. J Biomech. 2018 Jun 25;75:13-27. [CrossRef]
- Thoomes-de Graaf, M.; Thoomes, E.; Fernández-de-Las-Peñas, C.; Plaza-Manzano, G.; Cleland, J.A. Normative values of cervical range of motion for both children and adults: A systematic review. Musculoskelet Sci Pract. 2020, 49, 102–182. [Google Scholar] [CrossRef] [PubMed]
- Williams MA, McCarthy CJ, Chorti A, Cooke MW, Gates S. A systematic review of reliability and validity studies of methods for measuring active and passive cervical range of motion. J Manipulative Physiol Ther. 2010 Feb;33(2):138-55. [CrossRef]
- Dvorak J, Antinnes JA, Panjabi M, Loustalot D, Bonomo M. Age and gender related normal motion of the cervical spine. Spine (Phila Pa 1976). 1992 Oct;17(10 Suppl):S393-8. [CrossRef]
- Zárate-Tejero CA, Rodríguez-Rubio PR, Brandt L, Krauss J, Hernández-Secorún M, Lucha-López O, Hidalgo-García C. Association between Age, Sex and Cervical Spine Sagittal Plane Motion: A Descriptive and Correlational Study in Healthy Volunteers. Life (Basel). 2023 Feb 7;13(2):461. [CrossRef]
- Ferguson, B. ACSM’s Guidelines for Exercise Testing and Prescription, 9th ed. J Can Chiropr Assoc. 2014, 58(3), 328. [Google Scholar]
- Jannatbi, L.I.; Nigudgi, S.R.; Shrinivas, R. Assessment of musculoskeletal disorders by standardized Nordic questionnaire among computer engineering students and teaching staff of Gulbarga city. Int. J. Community Med. Public Health 2016, 3, 668–674. [Google Scholar]
- Bayattork M, Sköld MB, Sundstrup E, Andersen LL. Exercise interventions to improve postural malalignments in head, neck, and trunk among adolescents, adults, and older people: systematic review of randomized controlled trials. J Exerc Rehabil. 2020 Feb 26;16(1):36-48. [CrossRef]
- Häkkinen K, Pakarinen A. Muscle strength and serum testosterone, cortisol and SHBG concentrations in middle-aged and elderly men and women. Acta Physiol Scand. 1993 Jun;148(2):199-207. [CrossRef]
- Ryushi T, Hakkinen K, Kauhanen H, Komi PV. Muscle fiber characteristics, muscle cross-sectional area and force production in strength athletes, physically active males and females. Scand J Sports Sci. 1988; 10:7-15.
- Olivier PE, Du Toit DE. Isokinetic neck strength profile of senior elite rugby union players. J Sci Med Sport. 2008 Apr;11(2):96-105. [CrossRef]
- Gourie-Devi M, Nalini A, Sandhya S. Early or late appearance of "dropped head syndrome" in amyotrophic lateral sclerosis. J Neurol Neurosurg Psychiatry. 2003 May;74(5):683-6. [CrossRef]
- Kyllönen ES, Heikkinen JE, Väänänen HK, Kurttila-Matero E, Wilen-Rosenqvist G, Lankinen KS, Vanharanta JH. Influence of estrogen-progestin replacement therapy and exercise on lumbar spine mobility and low back symptoms in a healthy early postmenopausal female population: a 2-year randomized controlled trial. Eur Spine J. 1998;7(5):381-6. [CrossRef]
- Cunha-Henriques S, Costa-Paiva L, Pinto-Neto AM, Fonsechi-Carvesan G, Nanni L, Morais SS. Postmenopausal women with osteoporosis and musculoskeletal status: a comparative cross-sectional study. J Clin Med Res. 2011 Jul 26;3(4):168-76. [CrossRef]
- Jahre H, Grotle M, Smedbråten K, Dunn KM, Øiestad BE. Risk factors for non-specific neck pain in young adults. A systematic review. BMC Musculoskelet Disord. 2020 Jun 9;21(1):366. [CrossRef]
- Staudte HW, Duhr N. Age- and sex-dependent force related function of the cervical spine. Eur Spine J. 1994;3:155-161.
- Hurwitz EL, Randhawa K, Yu H, Côté P, Haldeman S. The Global Spine Care Initiative: a summary of the global burden of low back and neck pain studies. Eur Spine J. 2018;27:796-801. [CrossRef]
- Schulenberg J, Schoon I. The Transition to Adulthood across Time and Space: Overview of Special Section. Longit Life Course Stud. 2012;3:164-172. [CrossRef]
- Schoon I, Chen M, Kneale D, Jager J. Becoming adults in Britain: lifestyles and wellbeing in times of social change. J Longitudinal Life Course Stud. 2012;3:17.
- Dunn, KM. Extending conceptual frameworks: life course epidemiology for the study of back pain. BMC Musculoskelet Disord. 2010 Feb 2;11:23. [CrossRef]
Figure 1.
Differences in relative cervical strength values (per body height) between males and females. Where *p<0.05 significant difference between males and females.
Figure 1.
Differences in relative cervical strength values (per body height) between males and females. Where *p<0.05 significant difference between males and females.
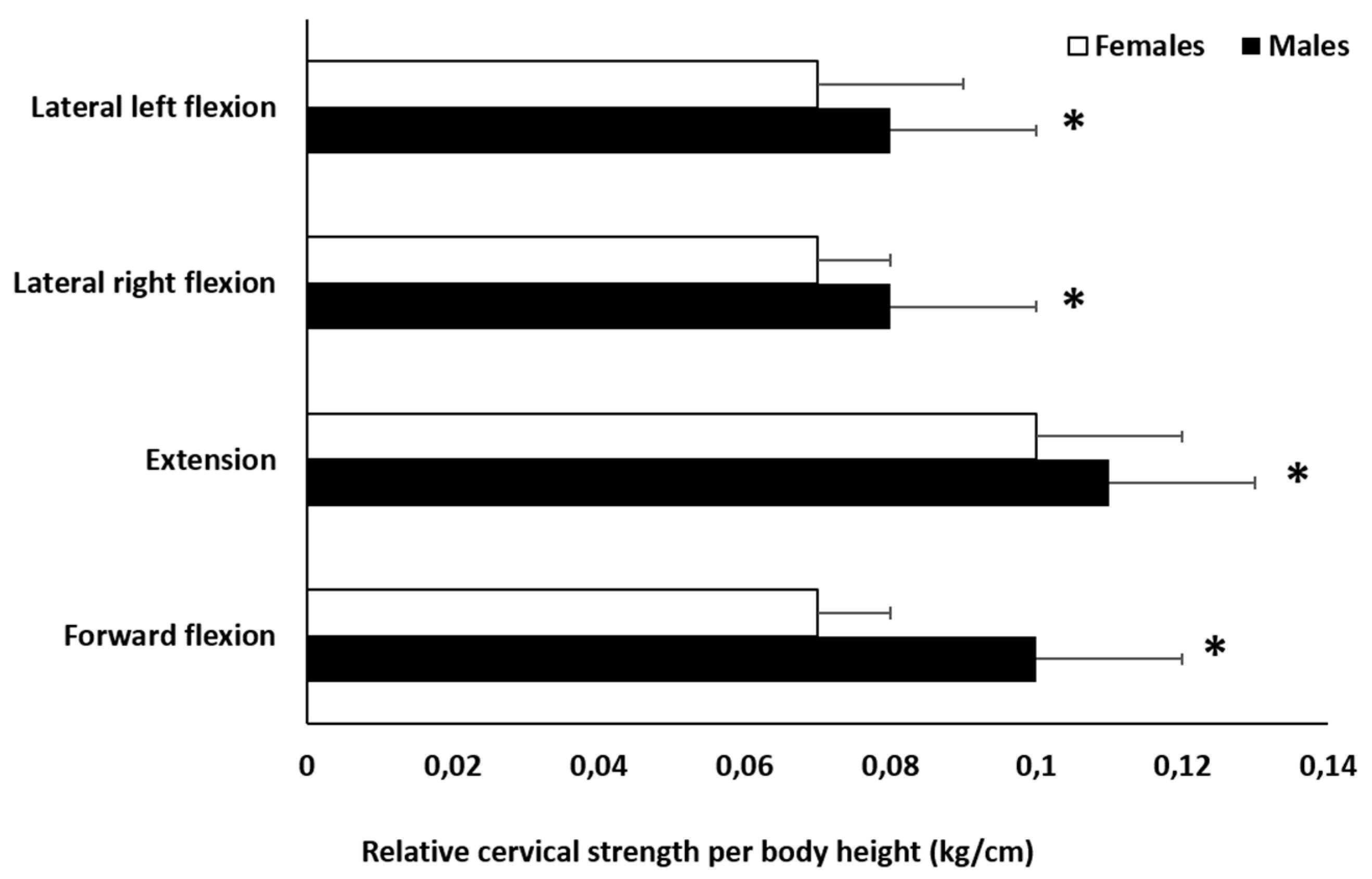
Figure 2.
Differences in relative cervical strength values (per body mass) between males and females. Where *p<0.05 significant difference between males and females.
Figure 2.
Differences in relative cervical strength values (per body mass) between males and females. Where *p<0.05 significant difference between males and females.
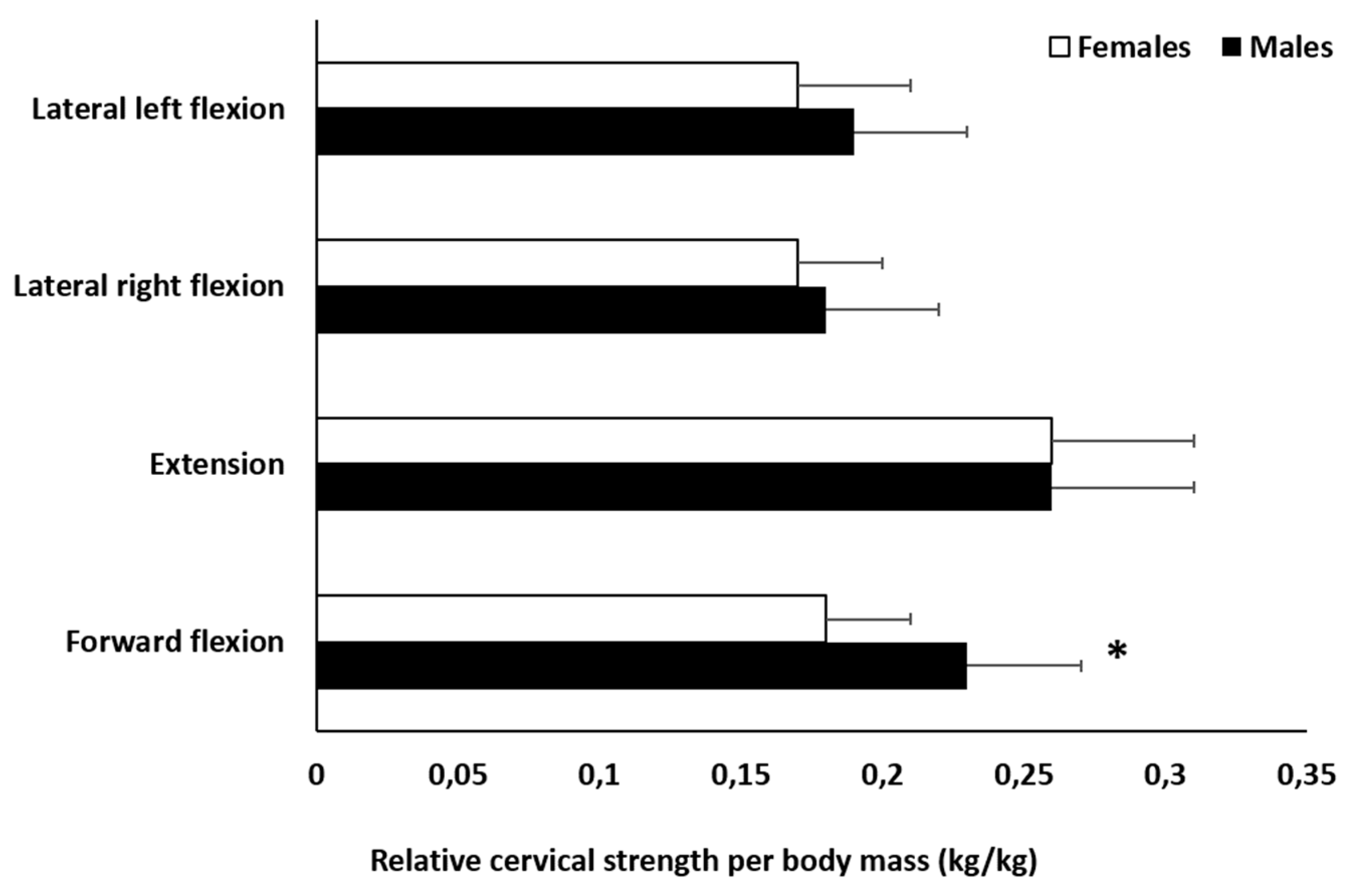

Table 1.
Age and anthropometric characteristics of the sample (mean ± standard deviation).
| Variables | Males (n=30) | Females (n=30) |
|---|---|---|
| Age (years old) | 21.95 ± 1.1 | 21.1 ± 1.2 |
| Body height (cm) | 178.5 ± 7.4 | 166.3 ± 6.3* |
| Body mass (kg) | 78.25 ± 14.4 | 64.6 ± 10.98* |
| BMI (kg/m2) | 24.4 ± 3.1 | 23.4 ± 3.99 |
BMI: body mass index = body mass/body height2. Where *p<0.05 significant differences between males and females.
Table 2.
Cervical range of motion values (mean ± standard deviation) in males and females.
| Movement | Males (n = 30) | Females (n = 30) |
|---|---|---|
| Forward flexion (ο) | 71.42 ± 10.34 | 69.81 ± 13.45 |
| Extension (ο) | 80.38 ± 12.48 | 94.28 ± 14.16* |
| Right lateral flexion (ο) | 47.76 ± 8.05 | 53.39 ± 10.71* |
| Left lateral flexion (ο) | 47.89 ± 8.69 | 53.87 ± 8.5* |
| Right lateral rotation (ο) | 80.83 ± 9.26 | 83.16 ± 9.34 |
| Left lateral rotation (ο) | 82.34 ± 8.44 | 85.56 ± 8.36 |
Where *p<0.05 = statistically significant difference between males and females.
Table 3.
Cervical absolute strength values (mean ± standard deviation) in males and females.
| Movement | Males (n = 30) | Females (n = 30) |
|---|---|---|
| Forward flexion (kg) | 17.92 ± 4.25* | 11.17 ± 2.10 |
| Extension (kg) | 20.45 ± 4.70* | 16.27 ± 3.17 |
| Right lateral flexion (kg) | 14.33 ± 3.89* | 10.93 ± 2.42 |
| Left lateral flexion (kg) | 14.52 ± 3.62* | 11.13 ± 2.85 |
| Flexion / Extension ratio (%) | 89.17 ± 17.51* | 69.75 ± 12.18 |
Where * p<0.01= statistically significant difference between males and females.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



