
Submitted:
18 September 2023
Posted:
22 September 2023
You are already at the latest version
Abstract
Alcohol use disorder (AUD) is a chronic and relapsing biopsychosocial condition that leads to a wide range of medical, psychological, social, economic, and personal issues. The study investigated the predictors of quality of life (QoL) among male patients seeking treatment for AUD based on attention, cognitive instability, motor impulsiveness, perseverance, and self-control dimensions of trait impulsivity. The study also investigated the potential mediating effect of anxiety and alcohol use severity in this relationship. After an initial assessment, participants underwent comprehensive evaluations, including sociodemographic data, clinical history, and QoL domains. Evaluations also covered AUD severity, impulsivity dimensions, cognitive functions, craving intensity, depression, anxiety and self-efficacy. Multiple linear regressions were employed to identify associations between independent variables and QoL. Attention dimension of impulsivity and anxiety symptoms significantly predicted physical health QoL. Self-control dimension and severity of alcohol use disorder predicted psychological QoL. Indirect effect of attention dimension on physical health was significant [effect =-1.082,95% CI (-2.008, -0.3598)].The significance of impulsivity in influencing QoL for individuals with AUD has profound clinical implications. These findings underscore the importance of addressing anxiety and impulsivity in managing AUD, given their considerable impact, particularly on QoL, ultimately shaping treatment outcomes.
Keywords:
quality of life
; impulsivity
; attention and self-control dimensions of impulsivity
; alcohol use disorder
; anxiety symptoms
; WHOQOL-BREF
1. Introduction
Alcohol use disorder (AUD) is a chronic and relapsing biopsychosocial condition that leads to a wide range of medical, psychological, social, economic, and personal issues. This complex challenge not only affects physical health but also psychological well-being and overall quality of life. Problematic alcohol use is associated with various health problems such as liver cirrhosis, cardiovascular diseases, mental disorders, and increased risks of accidents and injuries [1]. In the year 2020, 1.03 billion males and 312 million females worldwide consumed harmful amounts of alcohol in excess of the non-drinker equivalence (NDE) and contributing to a total of 1.78 million deaths in the same year. Notably, alcohol consumption emerged as the primary risk factor for mortality among males aged 15–49 years [2].
In 2016, approximately 43% of the global population aged 15 years and above were identified as current drinkers. This also contributed to the loss of 132.6 million disability-adjusted life years (DALYs), equivalent to 5.1% of the total DALYs for that year. Globally, harmful alcohol use ranks as the seventh leading cause of premature death and disability [3]. It’s worth noting that the mortality caused by problematic alcohol use surpasses that of diseases like tuberculosis, HIV/AIDS, and diabetes [1].
The goal of AUD recovery is not only to stop heavy drinking or to achieve abstinence but to improve biopsychosocial functioning and quality of life as well. A sustained recovery process requires progress in these areas that are indicators of progress in recovery [4,5,6]. Therefore researchers have expanded their studies to explore the impacts of AUD treatment on quality of life and nondrinking outcomes beyond mere reductions in drinking [7]. The integration of behavioral and medical services, along with resilience and well-being, is increasingly being recognized as important to addressing chronic relapses in substance use disorders [8]. Consequently, improving quality of life (QoL) is now gaining attention in AUD treatment [7].
QoL is defined by the World Health Organization as “an individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns”[9]. Studies have found significant impairment of QOL in individuals with alcohol use disorder, particularly with respect to their physical health and psychological domains compared to general population [10,11]. It has also been studied the predictors of QOL among patients with alcohol use disorder under treatment. There are several factors that predict baseline QOL in such studies, such as severity of alcohol use disorder, marital status, employment status, age, and personality disorder [12,13,14]. Recent studies have highlighted impulsivity, positive affect, anxiety, and craving as predictors of quality of life during treatment for AUD [15,16,17,18]. There is also evidence that various dimensions of impulsivity, including non-planning, attentional impulsivity, and motor impulsivity, are associated with well-being and health-related quality of life (HRQoL) in in individuals recently detoxified from AUD [19].
Researchers have also found a relationship between the outcome of AUD treatment and quality of life, and they report that poorer drinking outcomes are often associated with lower quality of life and more alcohol-related problems [20]. While improved drinking outcomes during treatment are associated with improved QoL scores [21,22]. Studies indicate that behavioral interventions combined with anti-craving medication maintenance can improve drinking outcomes by improving QoL [14,23]. It appears that the outcome of treatment and QoL may be bidirectional, both during and after the treatment process.
Numerous behavioral models of impulsivity have been put forth in research. A comprehensive definition that encompasses these various viewpoints characterizes impulsivity as a tendency for quick, unplanned behaviors, disregarding the possible adverse outcomes [24]. The concept of impulsivity aligns with a couple of indicators of alcohol dependence and use disorder outlined in both the ICD-10 and DSM-V criteria. These indicators involve consuming more alcohol than initially intended and continuing to drink despite awareness of potential adverse outcomes.
Recent research suggests that impulsivity is a complex concept that can be viewed from different angles. It can be seen as a consistent personality trait or as a behavioral indicator of decision-making and actions. “Trait impulsivity” refers to a relatively stable form of impulsivity that is part of a person’s character. This aspect is usually evaluated using self-report questionnaires. On the other hand, “behavioral impulsivity” refers to patterns of impulsive behavior, assessed through objective measurements in various situations, often involving tasks [25,26]. The Barratt Impulsiveness Scale (BIS) developed by Patton et al. (1995) [27], and the UPPS-P Impulsive Behavior Scale by Whiteside and Lynam (2001) [28], are self-report questionnaires used to assess impulsivity as a personality trait. These scales also identify various subcategories of impulsive traits through specific subsections. People with alcohol use disorder score higher on BIS compared to those without the disorder [29,30]. Earlier research has demonstrated a positive link between trait impulsivity and alcohol consumption [31,32,33]. Studies have also indicated bidirectional relationship between impulsivity and alcohol use [34]. Individuals diagnosed with alcohol use disorder (AUD) who also exhibit comorbid gambling symptoms were found to have elevated levels of trait impulsivity and a propensity for non-planning behaviors. Interestingly, this association remains significant irrespective of factors such as intelligence, age, and psychopathological symptoms [35].
Impulsivity appears to play a significant role in the onset and progression of substance use disorder, either as an underlying susceptibility or as a result of prolonged substance abuse [36]. Moreover, there is evidence indicating that alcohol can potentially influence impulsivity patterns as time goes on [37]. Moreover, it has been observed that all three facets of impulsivity, encompassing ‘trait impulsivity,’ ‘motor impulsivity,’ and ‘impulsive choice impulsivity,’ are associated with AUD relapse [38]. Cognitive-behavioral therapies focused on addressing impulsivity have the potential to augment individuals’ ability to manage their alcohol consumption, thereby resulting in enhanced treatment outcomes. However, the absence of premeditation and the presence of high negative urgency have been associated with less favorable results in psychotherapy for Substance Use Disorder (SUD) [39].
In AUD recovery, the emphasis on successful outcomes has primarily revolved around traditional measures like decreased alcohol and drug consumption during treatment. However, there’s a growing realization that the overall QoL is a crucial aspect of recovery. Current AUD treatment and medication trials have centered on endpoints like abstinence and reduced heavy drinking days. Hence, there is a requirement to investigate clinical, impulsivity, and cognitive indicators linked to the quality of life in individuals with AUD. This investigation should particularly focus on fundamental aspects of trait impulsivity such as attention, cognitive instability, motor impulsiveness, perseverance, and self-control. By examining factors that can predict quality of life throughout and after AUD treatment, it becomes possible to pinpoint areas for intervention and improvement in the treatment process.
In AUD recovery, the emphasis on successful outcomes has primarily revolved around traditional measures like decreased alcohol and drug consumption during treatment. However, there’s a growing realization that the overall QoL is a crucial aspect of recovery. Current AUD treatment and medication trials have centered on endpoints like abstinence and reduced heavy drinking days. Hence, there is a requirement to investigate clinical, impulsivity, and cognitive indicators linked to the quality of life in individuals with AUD. This investigation should particularly focus on fundamental aspects of trait impulsivity such as attention, cognitive instability, motor impulsiveness, perseverance, and self-control. By examining factors that can predict quality of life throughout and after AUD treatment, it becomes possible to pinpoint areas for intervention and improvement in the treatment process.
This study examined the association between attention, cognitive instability, motor impulsiveness, perseverance, and self-control dimensions of trait impulsivity and QoL among male patients seeking treatment for AUD. Furthermore, the study investigated the predictors of QoL among male patients seeking treatment for AUD based on attention, cognitive instability, motor impulsiveness, perseverance, and self-control dimensions of trait impulsivity. The study also investigated the potential mediating effect of anxiety and alcohol use severity in this relationship. This study hypothesized that attention, cognitive instability, motor impulsiveness, perseverance, and self-control dimensions of trait impulsivity would be predictive of all four domains of QoL. A second hypothesis was that anxiety and severity of alcohol use would mediate the effects of impulsivity dimensions on QoL.
2. Materials and Methods
2.1. Study setting & participants
This study was carried out at a leading substance use disorder treatment centre in India. The 50-bed centre is staffed by well-qualified multidisciplinary faculty and staff to provide a variety of treatments. Recruitment for this study took place between December 2018 and June 2020. At the time of recruitment, all patients were undergoing detoxification and remained in treatment as inpatients. Ethical approval was received from the Institute Ethics Committee of the All India Institute of Medical Sciences, New Delhi. Written informed consent was obtained from all study participants.
2.2. Inclusion and Exclusion
Inclusion criteria were: (1) age between 18 and 60 years, (2) able to read and write, (3) diagnosis of alcohol use disorder (AUD) as per DSM 5 using the Mini-International Neuropsychiatric Interview (MINI) - Plus, (4) inpatient with score <7 on Clinical Institute Withdrawal Assessment of Alcohol Revised Scale (CIWA-Ar), (5) Willing to participate in the study. Exclusion criteria were as follows: (1) comorbid chronic physical illness, (2) comorbid psychotic or bipolar disorder, (3) DSM 5 substance use disorders other than nicotine and alcohol.
We recruited healthy controls who were matched with the study subjects in terms of age, sex, and socioeconomic status. Exclusion criteria were as follows: current or past psychiatric disorders, any substance use disorders other than nicotine, co-morbid chronic physical illnesses, and AUDIT scores of 8 or higher. These control subjects were selected from the same neighborhoods or from within the close circle of friends of our study cases, ensuring a suitable comparison group for the study.
2.3. Procedure
Prior to obtaining their informed consent, all participants were provided with a comprehensive overview of the entire research protocol. Following this, a thorough screening process was conducted to determine adherence to the specified inclusion and exclusion criteria. Once all criteria were met, patients were officially enrolled in the study. After that, we conducted detailed assessments to collect the following information:
Sociodemographic and clinical characteristics: All participants were assessed for sociodemographic data, including their name, age, gender, educational qualifications, occupation, family type, and residence type, age of onset of alcohol use, duration and quantity of alcohol use.
Quality of Life Assessment: The World Health Organization Quality of Life-BREF (WHOQOL-BREF) questionnaire was employed to evaluate participants’ quality of life.
Alcohol Use Disorder Severity Evaluation: The Alcohol Use Disorders Identification Test (AUDIT) was utilized to gauge the severity of alcohol use disorder among participants.
Impulsivity Measurement: The Barratt Impulsiveness Scale-11 (BIS-11) was administered to assess the levels of impulsivity exhibited by participants.
Cognitive Function Assessment: Cognitive functions were evaluated using the NIMHANS Battery, a comprehensive battery of cognitive tests.
Craving Evaluation: At the baseline, the Obsessive Compulsive Drinking Scale (OCDS) was employed to measure the intensity of craving in relation to alcohol consumption.
Depressive Symptom Assessment: The Hamilton Depression Rating Scale (HAM-D) was utilized to quantify the presence and severity of depressive symptoms.
Anxiety Symptom Evaluation: The Hamilton Anxiety Rating Scale (HAM-A) was employed to measure the extent and intensity of anxiety symptoms.
Self-Efficacy Examination: The Alcohol Abstinence Self-Efficacy (AASE) questionnaire was administered to assess participants’ beliefs in their ability to abstain from alcohol consumption.
- Instruments
- World Health Organization Quality of Life Brief Version (WHOQOL) Group, 1998). [9]
The QoL was assessed using the World Health Organization Quality of Life Brief Version. This self-report tool comprises 25 items measuring QoL across four domains: physical health, psychological, social relationships, and environment quality of life. Responses are rated on a 5-point Likert scale, with higher scores indicating improved QoL. The WHOQOL-BREF has shown strong reliability and validity in previous studies.
- Barratt Impulsiveness Scale (BIS) [27]
The BIS is widely used to measure impulsivity in psychiatric studies. The BIS-11 version assesses three impulsivity domains: motor, cognitive, and non-planning. The study identified six first-order factors through principal component analysis (PCA): attention, motor, self-control, cognitive complexity, perseverance, and cognitive instability. A subsequent analysis revealed three higher-order factors: “motor impulsiveness,” “non-planning impulsiveness,” and “attentional impulsiveness.” While the BIS-11(α = 0.83), and some factors demonstrated good reliability, such as non-planning impulsiveness (α = 0.72) and attentional impulsiveness (α = 0.74), motor impulsiveness had lower reliability (α = 0.59). Among the first-order factors, only attention (α = 0.72) and self-control (α = 0.72) showed good reliability.
- Alcohol Use Disorders Identification Test (AUDIT) [40]
It is a comprehensive assessment tool, comprised of 10 items, meticulously crafted by the World Health Organization (WHO). This instrument is designed to thoroughly evaluate patterns of alcohol consumption, behaviors related to drinking, and the presence of alcohol-associated issues. Each of the 10 questions within the AUDIT framework is accompanied by a scale of responses, ranging from 0 to 4. Notably, questions 9 and 10 deviate slightly, offering responses on a scale of 0, 2, and 4.The scoring spectrum spans from 0 to 40, encompassing the gamut of potential responses. According to the discerning guidelines set forth by the World Health Organization (WHO), a score of 1 to 7 indicates consumption patterns associated with minimal risk. In contrast, scores between 8 and 14 signify a potential for hazardous or detrimental alcohol use, while a score of 15 or higher raises concerns about the prospect of alcohol dependence, indicating a moderate to severe alcohol use disorder. Notably, individuals with the most profound severity, as classified by the DSM-5, consistently manifest notably elevated mean scores on the AUDIT, distinguishing them from those exhibiting less severe manifestations.
- Obsessive Compulsive Drinking Scale (OCDS) [41]
The OCDS is a 14-item questionnaire. It is a widely used tool to measure cravings for alcohol. It’s a quick and reliable test that gives you a total score and two scores: one for the obsessive cravings (based on questions 1-6) and another for the compulsive cravings (based on questions 7-14). The OCDS has been tested with adults who have issues with alcohol use. The test-retest correlation for the OCDS total score is 0.96, and the obsessive and compulsive subscales test-retest correlations are 0.94 and 0.86, respectively. The internal consistency of the items in the OCDS is high (0.86).
- Alcohol Abstinence Self-Efficacy Scale (AASE) [42]
It is a 20 item questionnaire that measures an individual’s self-confidence to abstain from drinking in a range of situations. AASE demonstrated a solid subscale structure and strong indices of reliability and validity. The four 5-item subscales measured types of relapse precipitants labeled negative affect, social positive, physical and other concerns, and withdrawal and urges. Both in structure and mean scores the AASE demonstrated no substantive gender differences. The AASE appears to represent a brief, easily usable and psychometrically sound measure of an individual’s self-efficacy to abstain from drinking.
- NIMHANS neuro-psychological Battery for Cognitive Functions [43]
Cognitive functions were assessed using the NIMHANS Battery, including the Auditory Verbal Learning Test, Complex Figure Test, Verbal N Back Test, Digit Symbol Substitution Test, Animal Names Test, Stroop Test and Wisconsin Card Sorting Test.
- Hamilton Anxiety Rating Scale (HAM-A) [44]
The HAM-A was one of the first tools created to measure how serious anxiety symptoms are. It’s still used a lot today in both medical and research settings. The tool has 14 questions, each describing a set of symptoms. It measures two kinds of anxiety: mental anxiety (feeling restless or distressed) and physical anxiety (having physical problems because of anxiety). The HAM-A doesn’t have set questions for the person being tested. Even so, the results show that different testers get similar scores, which is good. Each question gets a score from 0 (no problem) to 4 (very serious). The total score can range from 0 to 56. Scores under 17 mean mild anxiety, scores between 18 and 24 mean mild to medium anxiety, and scores between 25 and 30 mean medium to serious anxiety.
- The Hamilton Depression Rating Scale (HAM-D) [45]
It stands as the preeminent tool for evaluating depression under the guidance of clinicians. Comprising a set of 17 items, this assessment scale delves into the spectrum of depressive symptoms experienced over the course of the previous week. The methodology for scoring varies across different iterations of the scale. In the context of the HAM-D, a score ranging from 0 to 7 is conventionally interpreted as indicative of a state within the normal range or clinical remission. Conversely, a score of 20 or higher, denoting at least a moderate level of severity, is typically the threshold for eligibility in clinical trial enrollment.
2.5. Statistical analysis
The data were analyzed using Statistical Package for Social Sciences (SPSS) version 25.0. P values <0.05 were considered significant. Continuous variables were presented as mean and standard deviation (SD), while categorical variables were expressed as percentages. Within the WHOQoL BREF scores (ranging from 0 to 100), an assessment was conducted for each domain, encompassing physical, psychological, social relationships, and environmental domains. To compare QoL scores between individuals with alcohol use disorder and non-user controls, an independent t-test was utilized, with significance set at a p-value below 0.05. Categorical variables pertaining to sociodemographic and clinical characteristics were evaluated between the two groups using a chi-squared (X2) test, where significance was considered at a p-value less than 0.05. Multiple linear regression analysis was performed to examine the relationship between independent variables and QoL. Variables that exhibited a p-value of less than 0.2 during the initial unadjusted analysis were simultaneously entered into the model using the “Enter” method, and unstandardized beta coefficients were estimated. Significance in this analysis was recognized at a p-value of less than 0.05.Mediation analysis was conducted using the PROCESS Macro -Model 4. The focus of this analysis was the Physical Health domain of QoL, with attention factor scores on the BIS-11 serving as the predictor variable and anxiety scores on the HAM-A serving as the mediator variable. The outcome of the analysis was assessed in terms of statistical significance.
2.6. Sample size
(a) Assuming a pooled standard deviation of 3.95 units (raw score on WHOQOL- BREF scale for physical health domain) and a design effect (DEFF) of 1.4, the study would require a sample size of: 83 for the test group (Individuals with alcohol use disorder) and 42 for the control group (i.e., a total sample size of 125; to ensure that the control group is 0.5 times larger than the test group) to achieve a power of 80% and a level of significance of 5% (two sided), for detecting a true difference in means between the test and the control group of -2.5 (i.e., 21.45–23.95) units(raw score on WHOQOL- BREF scale for physical health domain) [46].
(b) Assuming a pooled standard deviation of 3.27 units (raw score on WHOQOL- BREF scale for Psychological domain) and a design effect (DEFF) of 1.4, the study would require a sample size of: 84 for the test group and 42 for the reference group (i.e., a total sample size of 126; to ensure that the Reference group is 0.5 times larger than the test group) to achieve a power of 80% and a level of significance of 5% (two sided), for detecting a true difference in means between the test and the reference group of -2.05 (i.e., 18.39–20.44) units(raw score on WHOQOL- BREF scale for psychological domain) [46].
Furthermore, we have conscientiously considered the recommendations regarding sample size, as put forth by Green (1991). Green’s guidance suggests that for testing the multiple correlation, a sample size of N > 50 + 8m is advisable, with ‘m’ denoting the number of independent variables in question. This recommendation takes into account the expectation of a medium-sized relationship
We chose to focus on the Physical Health and Psychological domains of the WHOQOL - BREF scale as our variables of interest, based on a comprehensive review of existing literature. Consequently, following these calculations, we arrived at a total of 88 participants for the test group and 44 for the control group.
In our study analysis. We converted WHOQOL-BREF raw scores into transformed scores on a 0-100 scale.
2.6. Ethical approval
All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the study was approved by the Ethics Committee, All India Institute of Medical Sciences, New Delhi. Committee Reference number: IEC-278/01.06.2018, RP-31/2018 dated 19th June 2018.
3. Results
Table 1 and Table 2 consists of information from 88 participants, and various variables have been examined in relation to different domains of QoL. The average age of the participants was 37.55 years, with a standard deviation of 8.31. Among the participants, 43.2% (38) had received a school education, while 56.8% (50) had a college education. In terms of employment status, 36.4% (32) were unemployed, while 63.6% (56) were employed. Additionally, 45.5% (40) lived in joint family setups, while 54.5% (48) lived in nuclear family setups. Marital status indicated that 31.8% (28) were unmarried, and 63.6% (60 individuals) were married.
The differences in QoL between individuals with alcohol use disorder and healthy controls was found to be statistically significant across domains of physical health, psychological, and social relationships. However, there was no statistically significant difference observed in the domain of environment. Significant associations were observed between marital status and the social relationship domain of QoL. The mean QoL score for the social relationship domain was 47.29 (SD = 27.15) for unmarried individuals and 77.27 (SD = 15.98) for married individuals. This association was found to be statistically significant (p = 0.004).
Table 3 presents the descriptive statistics and correlation matrix of various study variables based on a sample size of 88 individuals. The table provides means, standard deviations (SD), and the correlation coefficients between different variables. Correlations are denoted by coefficients ranging from -1 to 1, with positive values indicating a positive relationship and negative values indicating a negative relationship. Correlation coefficients marked with ** are significant at the 0.01 level (two-tailed), while those marked with * are significant at the 0.05 level (two-tailed). The table helps to understand the relationships between different variables and provides insights into potential associations between factors such as quality of life, impulsiveness, psychological measures, cognitive function, and alcohol-related assessments. The BIS-11 1st Order factor of Attention exhibited significant correlations with the Physical Health (r=-0.655) and Environment (r=-0.547) domains of QoL. Similarly, the BIS-11 1st Order factor of Self-Control demonstrated significant correlations with the domains of Physical Health (r=-0.343) and Psychological Health (r=-0.406) in the context of QoL. Scores on the HAM-D (Hamilton Depression Rating Scale) and HAM-A (Hamilton Anxiety Rating Scale) exhibited significant correlations with all four domains of QoL. Furthermore, the total scores from the Alcohol Use Disorders Identification Test were significantly correlated with the Psychological Health domain (r=-0.325) of QoL. The scores from the Obsessive Compulsive Drinking Scale displayed significant correlations with the Environment (r=-0.388) and Physical Health (r=-0.388) domains of QoL. There was no significant correlation between any cognitive test assessment and the four domains of quality of life. The mean age of onset of alcohol use was found to be 20.11 years with a standard deviation of 5.33.However, it is important to note that our study did not find a significant correlation between the age of onset of alcohol use and impulsivity. Furthermore, the scores derived from the Alcohol Abstinence Self-Efficacy Scale (Confident) demonstrated significant associations with both the Psychological Health domain (r = 0.345) and the Relationships domain (r = 0.436) of QoL.
Table 4 presents the univariate and multivariate Linear Regression Analyses to identify predictors of quality of life (WHOQOL-BREF) among individuals undergoing detoxification for alcohol use disorder.
A multiple linear regression analysis was conducted to predict the physical health domain of quality of life based on the attention dimension scores of the BIS-11, the self-control dimension scores of the BIS-11, as well as scores from the HAM-A and HAM-D scales were utilized. The results revealed a statistically significant regression equation (F(4, 83) = 13.87, p < .000), with an R-squared value of .587. Both attention factor scores on BIS and anxiety score on HAM –A were significant predictors of physical health domain of quality of life. These predictors demonstrated that higher scores on attention factor of the BIS-11 and elevated anxiety scores on the HAM-A were associated with lower scores in the physical health domain of quality of life. The mediation analysis was performed using PROCESS Macro. The outcome variable for analysis was Physical health domain of QoL. The Predictor variable for the analysis was attention factor scores on BIS-11. The mediator variable for the analysis was anxiety scores on HAM-A. The indirect effect of attention factor scores on BIS -11on Physical health domain of QoL was found to be statistically significant [effect = -1.082, 95% CI (-2.008, -0.3598)], and the results are comprehensively presented in Table 5. Importantly, these effects were found to be partially mediated by anxiety scores, as depicted in Figure 1.
A multiple linear regression analysis was conducted to predict the psychological health domain of quality of life. The predictor variables included the attentional factor scores of BIS-11, the self-control factor scores of BIS-11, scores from the HAM-A scale, scores from the HAM-D scale, and total scores from the AUDIT. The analysis revealed a statistically significant regression equation (F(5,82) = 5.258, p < .001), with an R-squared value of .409. Both self-control factor scores on BIS and AUDIT scores were significant predictors of psychological health domain of quality of life. This indicated that higher self-control factor scores on the BIS-11 and greater severity of alcohol use, as indicated by higher AUDIT scores, were linked to lower scores on the psychological health domain of quality of life. The mediation analysis was performed using PROCESS Macro. The outcome variable for analysis was psychological domain of QoL. The Predictor variable for the analysis was self-control factor scores on BIS-11. The mediator variable for the analysis was alcohol use severity measured by AUDIT. The indirect effect of self-control factor scores on BIS -11on psychological domain of QoL was not found to be statistically significant [effect = .303 95% (-.273,.900)] as demonstrated in Figure 2. The results are comprehensively presented in Table 5.
A multiple linear regression analysis was conducted to predict the quality of life within the social relationships domain. The predictive factors included scores from the attention factor of BIS-11, HAM-A scores, HAM-D scores, and marital status. The results revealed a statistically significant regression equation (F(4, 83) = 3.655, p < .013) with an R-squared value of .273.The predicted quality of life score in the relationship domain for participants was estimated using the formula: 51.526 − 1.332 (BIS Attention) − 1.903 (HAM-D) − 0.123 (HAM-A) + 18.1 (Marital status). It’s important to note that all independent variables were measured on a continuous scale, except for marital status, which was coded as 1 for unmarried and 2 for married participants. Remarkably; the marital status emerged as the sole significant predictor of quality of life in the relationship domain. Married participants exhibited a notable increase of 18.1 points in their quality of life in relationship domain scores compared to unmarried participants.
A multiple linear regression analysis was conducted to assess the relationship between the quality of life in the environmental domain and several variables, including the attentional factor scores from BIS-11, self-control factor scores from BIS-11, HAM-A (Hamilton Anxiety Rating Scale) scores, HAM-D (Hamilton Depression Rating Scale) scores, OCDS (Obsessive-Compulsive Drinking Scale) scores, and AASE (Adolescent Alcohol Sensation Seeking) scores. The results revealed a statistically significant regression equation (F(6, 81) = 7.235, p < .000), with an R-squared value of .540.The predicted environmental quality of life score for participants can be calculated using the following equation: 104.098 − 0.887(BIS Attention) − 1.041(BIS Self-control) − 0.475(HAM-D) − 1.360(HAM-A) − 0.090(OCDS score) + 0.140(AASE), where all the independent variables were measured on a continuous scale. No independent variables were found to be significant predictors of quality of life in the environmental domain.
4. Discussion
Our study aimed to assess the association between attention, cognitive instability, motor impulsiveness, perseverance, and self-control dimensions of trait impulsivity and QoL among male patients seeking treatment for AUD. Furthermore, the study investigated the predictors of QoL among male patients seeking treatment for AUD based on attention, cognitive instability, motor impulsiveness, perseverance, and self-control dimensions of trait impulsivity. The study also investigated the potential mediating effect of anxiety and alcohol use severity in this relationship. These scores were then compared to those of demographically matched, healthy individuals who did not consume alcohol. We also explored the correlations between domains of QoL and socio-demographic, cognitive, and clinical factors in order to pinpoint the most significant predictors of QoL.
The differences in QoL between individuals with alcohol use disorder and healthy controls who do not consume alcohol was found to be statistically significant across domains of physical health, psychological, and social relationships. However, there was no statistically significant difference observed in the domain of environment. The psychological domain exhibited the lowest mean score, followed by the mean score in the physical health domain among individuals with alcohol use disorder. These findings are consistent with previous studies that have also documented diminished scores in the psychological and physical health domains [12,18,47]. However, a deviation from these findings is observed in a separate study, Olickal et al.(2021) which reported the highest mean (SD) score in the physical domain when compared to other QoL domains [18]. This discrepancy in our findings could potentially be attributed to variations in the study setting and the characteristics of the study subjects, including the inclusion of patients experiencing severe addiction and undergoing inpatient detoxification. Patients with AUD demonstrated higher mean scores on impulsivity factors assessed by the BIS 11 compared to the control group, aligning with findings from prior research [29,30].
Marital status exhibited a significant association with the social relationships domain of QoL among individuals with alcohol use disorder. Those who were married showed a notable positive effect on the social relationships domain of QoL. This observation aligns with prior research that highlights the beneficial effects of cohabitation with a partner on the social functioning aspect of QoL [48,49]. Conversely, factors such as age and education did not demonstrate any correlation with the various domains of QoL within this study, which is consistent with findings from earlier investigations [49]. It’s worth noting, however, that contrary to these results, other studies have presented evidence indicating that advancing age [50] and lower educational attainment [14] do indeed exert a negative impact on QoL.
Our findings did not show any significant correlation between cognitive abilities and QoL. In prior studies, the relationship between anxiety/depressive symptoms and QoL in individuals with AUD was examined. These studies indicated that both depression and anxiety could contribute to diminished QoL among AUD patients [17,51,52]. Consistent with these findings, we observed a significant correlation between anxiety/depressive symptoms and various domains of QoL. Thus, the individuals with AUD who experience more pronounced symptoms of depression and anxiety are likely to have a lower QoL. Consistent with prior research carried out in the context of AUD and binge drinking, our study revealed a significant correlation between psychological domain of QoL and the AUDIT score. However, in contrast to earlier studies, we did not identify any significant correlation between the age of onset of AUD and QoL [53,54]. This observed relationship indicates that the extent of AUD severity is negatively correlated with the psychological domain of QoL.
A multivariable linear regression was conducted using the four domains of QoL as the dependent variables to identify the predictors of QoL. Notably, the dimensions of impulsivity that showed significant predictive power were attention dimension and self-control dimension of impulsivity.
The predictive equation for participants’ physical health domain of quality of life was determined as follows: Y = 92.111 − 2.272(BIS Attention) − 0.101(BIS Self-control) − 0.393(HAM-D) − 1.642(HAM-A), where all independent variables were measured as continuous on a scale. Notably, a one-unit increase in attention factor scores on the BIS 11 led to a significant decrease of 2.272 units in participants’ predicted physical health domain of quality of life. Similarly, a one-unit increase in HAM-A scores resulted in a substantial decrease of 1.642 units in the predicted score for the physical health domain of quality of life. Both attention factor scores on BIS and anxiety score on HAM –A were significant predictors of physical health domain of quality of life. The equation representing the prediction of participants’ psychological health domain of quality of life was determined as follows: Predicted Psychological Health = 116.30 − 0.083 (BIS Attention) − 1.941 (BIS Self-control) − 0.188 (HAM-D) − 1.112 (HAM-A) − 1.053 (AUDIT score).All independent variables were measured as continuous values on a scale. Notably, a one-unit increase in self-control factor scores on the BIS 11 led to a significant decrease of 1.941 units in participants’ predicted physical health domain of quality of life. Similarly, a one-unit increase in AUDIT scores resulted in a decrease of 1.053 units in the predicted score for the psychological health domain of quality of life.
Specifically, attention dimension was found to be a predictor of physical QoL, while self-control was associated with psychological QoL. This finding aligns with a prior study [17,19]. It’s worth mentioning that the study’s results diverged from those of Reichl et al. (2022) [19], as the motor dimension of impulsivity did not emerge as a significant predictor across QoL domains. This discrepancy could potentially be attributed to methodological differences in measurement tools—our study employed the BIS-11, whereas Reichl et al. (2022) [19] utilized alternative tasks for assessment. A plausible explanation for how the attention and self-control dimensions of impulsivity are linked to a diminished quality of life is as follows: The inability to plan ahead and involve oneself in intricate tasks (self-control impulsivity) can pose challenges in making purposeful choices and restoring a stable overall functioning, encompassing aspects like employment and financial stability. Concurrently, a deficiency in focus (attentional impulsivity) may hinder an individual’s ability to stay present and prevent persistent rumination. Nevertheless, it is essential for forthcoming research endeavors to validate this conjecture.
Anxiety symptoms, as measured by the HAM-A scale, were found to predict the physical domain of QoL. This finding aligns with previous research indicating that both impulsivity and anxiety were predictors of QoL among individuals with AUD [17]. Moreover, using PROCESS Model 4 analysis, a significant indirect correlation was established. This link correlated the attention dimension of impulsivity to the physical QoL domain through anxiety symptoms. It’s important to note that the partial mediation effect was notable specifically for the physical domain QoL. This means that higher scores on the attention dimension of impulsivity could result in heightened anxiety symptoms, subsequently increasing the likelihood of a lower level of physical QoL. Studies have shown that anxiety significantly affects the quality of life in individuals with Alcohol Use Disorder (AUD) [55]. Anxiety and AUD can influence each other in a two-way manner. Some people with anxiety disorders may turn to alcohol as a way to self-medicate and manage their symptoms. This can, in turn, increase the risk of developing AUD [56]. On the other hand, research has also demonstrated that AUD can lead to the emergence of anxiety symptoms [57,58]. As a result, addressing anxiety becomes a crucial consideration when treating individuals with AUD. Moreover, it has been noted that several proximal factors are associated with regular alcohol consumption. These factors include emotional regulation and early tobacco use. Addressing these determinants could significantly aid in the management of individuals with AUD [59].
The severity of AUD as measured by the AUDIT was found to predict psychological domain QoL. On the other hand, being married was found to have a positive impact, acting as a protective factor for social relationship QoL. There was an observed negative correlation between QoL scores and AUDIT scores, with the AUDIT score standing out as a predictor of psychological domain QoL. However, we didn’t identify a significant indirect correlation between the self-control dimension of impulsivity and psychological domain QoL through the severity of AUD.
There are a few notable limitations associated with this research. Firstly, the use of a small sample size poses a significant constraint. Such small sample sizes can substantially diminish the statistical power of the study findings, necessitating a cautious interpretation of the results. Furthermore, the fact that this study was conducted at a single-center raises concerns about its representativeness for a broader population and more diverse settings. This limitation hampers the external validity and generalizability of the findings and requires a careful interpretation of the results. To mitigate these limitations, it is imperative that future research endeavors consider employing a larger sample size and adopting a multicentric approach. By doing so, researchers can bolster the statistical power of their studies, thereby enhancing the reliability and generalizability of the results. In conclusion, the path forward for future investigations in this area should involve a commitment to larger and more diverse samples, ultimately enabling a more comprehensive understanding of the subject matter.
4.1. Clinical Implications
Furthermore, the role of impulsivity in determining QoL for those with AUD is highly significant from a clinical standpoint. Notably, various studies have indicated that impulsivity is not only linked to the initial development of AUD [60], but it also contributes to the likelihood of relapse [61], even following periods of abstinence [62]. Given these findings, when dealing with AUD, it is essential to take into accounts both anxiety and impulsivity due to their impact, particularly through their influence on QoL, on the outcome of treatment. Along with medications, various approaches like engaging in physical activity [63] or practicing meditation [64] could be suggested to help control anxiety and impulsivity in people with AUD.
5. Conclusion
AUD is chronic biopsychosocial condition leading to various health and life challenges. The study, conducted at a prominent Indian treatment center from Dec 2019 to Jun 2020, gathered data on demographics, AUD severity, impulsivity, cognitive function, craving, emotional well-being, and self-efficacy. Analysis showed attention dimension of impulsivity and anxiety predicted physical health QoL, while self-control dimension and severity of alcohol use disorder anxiety predicted psychological QoL health. Attention dimension of impulsivity indirectly affected physical health. The significance of impulsivity in influencing the QoL for individuals with AUD holds substantial clinical importance. Remarkably, impulsivity plays a dual role—it is not only intertwined with the initial onset of AUD but also exerts a notable influence on the probability of relapse, even subsequent to phases of abstinence. These research findings underscore the imperative of considering both anxiety and impulsivity in the context of AUD management. This consideration becomes pivotal due to their profound effects, notably through their sway over QoL, ultimately shaping the treatment outcomes.
Author Contributions
Prabhoo Dayal: Fund acquisition, Conceptualization, Methodology, Project administration, Formal analysis, Resources, Validation, Writing—original draft, Writing—review & editing. Gauri s Kaloiya: Methodology (supporting) Writing—review & editing. Rohit Verma: Conceptualization (supporting), Writing—review & editing. Nand Kumar: Writing—review & editing.
Funding
This study was funded by a research grant (DST/CSRI/2017/149) from the Department of Science & Technology, Government of India under the Cognitive Science Research Initiative (CSRI).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee the Institute Ethics Committee of the All India Institute of Medical Sciences, New Delhi. Committee Reference number: IEC-278/01.06.2018, RP-31/2018 dated 19th June 2018.
Informed Consent Statement
All subjects gave their informed consent for inclusion before they participated in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
We want to thank all patients who agreed to participate in this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Global status report on alcohol and health 2018. Geneva: World Health Organization; 2018.
- Bryazka, D.; Reitsma, M.B.; Griswold, M.G.; Abate, K.H.; Abbafati, C.; Abbasi-Kangevari, M.; Abbasi-Kangevari, Z.; Abdoli, A.; Abdollahi, M.; Abdullah, A.Y.M.; et al. Population-level risks of alcohol consumption by amount, geography, age, sex, and year: a systematic analysis for the Global Burden of Disease Study 2020. Lancet 2022, 400, 185–235. [Google Scholar] [CrossRef] [PubMed]
- BD 2016 Alcohol Collaborators: Alcohol use and burden for195 countries and territories, 1990–2016: a systematic analysis forthe Global Burden of Disease Study 2016. Lancet 2016, 392, 1015–1035.
- Hagman, B.T.; Falk, D.; Litten, R.; Koob, G.F. Defining Recovery From Alcohol Use Disorder: Development of an NIAAA Research Definition. Am. J. Psychiatry 2022, 179, 807–813. [Google Scholar] [CrossRef]
- Kelly, J.F.; Greene, M.C.; Bergman, B.G. Beyond abstinence: changes inindices of quality of life with time in recovery in a nationally rep-resentative sample of US adults. Alcohol Clin Exp Res 2018, 42, 770–780. [Google Scholar] [CrossRef] [PubMed]
- Laudet, A.B. The case for considering quality of life in addiction research and clinical practice. Addict Sci Clin Pract 2011, 6, 44–55. [Google Scholar] [PubMed]
- Kirouac, M.; Stein, E.R.; Pearson, M.R.; Witkiewitz, K. Viability of the World Health Organization quality of life measure to assess changes in quality of life following treatment for alcohol use disorder. Qual. Life Res. 2017, 26, 2987–2997. [Google Scholar] [CrossRef]
- Dennis, M.; Scott, C. Managing Addiction as a Chronic Condition. Addict. Sci. Clin. Pr. 2007, 4, 45–55. [Google Scholar] [CrossRef]
- Group WHOQOL. (1997). Measuring quality of life. Geneva: The World Health Organization, 1–13.
- Donovan, D.; E Mattson, M.; A Cisler, R.; Longabaugh, R.; Zweben, A. Quality of life as an outcome measure in alcoholism treatment research. J. Stud. Alcohol, Suppl. 2005, 119–139. [Google Scholar] [CrossRef]
- Volk, R.J.; Cantor, S.B.; Steinbauer, J.R.; et al. Alcohol use disorders, consumption patterns, and health-related quality of life of primary care patients. Alcohol Clin Exp Res 1997, 21, 899–905. [Google Scholar] [CrossRef]
- Colpaert, K.; De Maeyer, J.; Broekaert, E.; et al. Impact of addiction severity and psychiatric comorbidity on the quality of life of alcohol-, drug-and dual-dependent persons in residential treatment. Eur Addict Res 2012, 19, 173–183. [Google Scholar] [CrossRef]
- Goldstein, R.B.; Dawson, D.A.; Smith, S.M.; Grant, B.F. Antisocial behavioral syndromes and 3-year quality-of-life outcomes in United States adults. Acta Psychiatr. Scand. 2012, 126, 137–150. [Google Scholar] [CrossRef] [PubMed]
- Morgan, M.Y.; Landron, F.; Lehert, P. for the New European AlcoholismTreatment Study Group. Improvement in quality of life after treatment for alcohol dependence with acamprosate and psychosocialsupport. Alcohol Clin Exp Res 2004, 28, 64–77. [Google Scholar] [CrossRef] [PubMed]
- Carlon, H.A.; Hurlocker, M.C.; Witkiewitz, K. Mechanisms of quality-of-life improvement in treatment for alcohol use disorder. J. Consult. Clin. Psychol. 2022, 90, 601–612. [Google Scholar] [CrossRef] [PubMed]
- Chamberlain, S.R.; Grant, J.E. Relationship between quality of life in young adults and impulsivity/compulsivity✰. Psychiatry Res. 2019, 271, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Lahbairi, N.; Laniepce, A.; Segobin, S.; Cabé, N.; Boudehent, C.; Vabret, F.; Rauchs, G.; Pitel, A.-L. Determinants of health-related quality of life in recently detoxified patients with severe alcohol use disorder. Heal. Qual. Life Outcomes 2022, 20, 149. [Google Scholar] [CrossRef] [PubMed]
- Olickal, J.J.; Saya, G.K.; Selvaraj, R.; Chinnakali, P. Association of alcohol use with quality of life (QoL): A community based study from Puducherry, India. Clin. Epidemiology Glob. Heal. 2021, 10, 100697. [Google Scholar] [CrossRef]
- Reichl, D.; Enewoldsen, N.; Weisel, K.K.; Fuhrmann, L.; Lang, C.; Saur, S.; Berking, M.; Zink, M.; Ahnert, A.; Falkai, P.; et al. Association of impulsivity with quality of life and well-being after alcohol withdrawal treatment. J. Clin. Psychol. 2022, 78, 1451–1462. [Google Scholar] [CrossRef]
- LoCastro, J.S.; Youngblood, M.; Cisler, R.A.; Mattson, M.E.; Zweben, A.; Anton, R.F.; Donovan, D.M. Alcohol Treatment Effects on Secondary Nondrinking Outcomes and Quality of Life: The COMBINE Study. J. Stud. Alcohol Drugs 2009, 70, 186–197. [Google Scholar] [CrossRef]
- Daeppen, J.-B.; Faouzi, M.; Sanchez, N.; Rahhali, N.; Bineau, S.; Bertholet, N. Quality of Life Depends on the Drinking Pattern in Alcohol-Dependent Patients. Alcohol Alcohol. 2014, 49, 457–465. [Google Scholar] [CrossRef]
- Witkiewitz, K.; Kranzler, H.R.; Hallgren, K.A.; O'Malley, S.S.; Falk, D.E.; Litten, R.Z.; Hasin, D.S.; Mann, K.F.; Anton, R.F. Drinking Risk Level Reductions Associated with Improvements in Physical Health and Quality of Life Among Individuals with Alcohol Use Disorder. Alcohol. Clin. Exp. Res. 2018, 42, 2453–2465. [Google Scholar] [CrossRef]
- Prisciandaro, J.J.; DeSantis, S.M.; Bandyopadhyay, D. Simultaneous Modeling of the Impact of Treatments on Alcohol Consumption and Quality of Life in the COMBINE Study: A Coupled Hidden Markov Analysis. Alcohol. Clin. Exp. Res. 2012, 36, 2141–2149. [Google Scholar] [CrossRef] [PubMed]
- Moeller, F.G.; Barratt, E.S.; Dougherty, D.M.; Schmitz, J.M.; Swann, A.C. Psychiatric Aspects of Impulsivity. Am. J. Psychiatry 2001, 158, 1783–1793. [Google Scholar] [CrossRef]
- Broos, N.; Schmaal, L.; Wiskerke, J.; Kostelijk, L.; Lam, T.; Stoop, N.; Weierink, L.; Ham, J.; de Geus, E.J.C.; Schoffelmeer, A.N.M.; et al. The Relationship between Impulsive Choice and Impulsive Action: A Cross-Species Translational Study. PLOS ONE 2012, 7, e36781. [Google Scholar] [CrossRef] [PubMed]
- Herman, A.M.; Critchley, H.D.; Duka, T. The role of emotions and physiological arousal in modulating impulsive behaviour. Biol Psychol 2018, 133, 30–43. [Google Scholar] [CrossRef] [PubMed]
- Patton, J.H.; Stanford, M.S.; Barratt, E.S. Factor structure of the Barratt Impulsiveness Scale. J Clin Psychol 1995, 51, 768–74. [Google Scholar] [CrossRef]
- Whiteside, S.P.; Lynam, D.R. The Five Factor Model and impulsivity: using a structural model of personality to understand impulsivity. Pers. Individ. Differ. 2001, 30, 669–689. [Google Scholar] [CrossRef]
- E Ketzenberger, K.; Forrest, L. Impulsiveness and compulsiveness in alcoholics and nonalcoholics. Addict. Behav. 2007, 25, 791–795. [Google Scholar] [CrossRef]
- von Diemen, L.; Bassani, D.G.; Fuchs, S.C.; Szobot, C.M.; Pechansky, F. Impulsivity, age of first alcohol use and substance use disorders among male adolescents: a population based case–control study. Addiction 2008, 103, 1198–1205. [Google Scholar] [CrossRef]
- Adams, Z.W.; Kaiser, A.J.; Lynam, D.R.; Charnigo, R.J.; Milich, R. Drinking motives as mediators of the impulsivity-substance use relation: Pathways for negative urgency, lack of premeditation, and sensation seeking. Addict. Behav. 2012, 37, 848–855. [Google Scholar] [CrossRef]
- Coskunpinar, A.; Dir, A.L.; Cyders, M.A. Multidimensionality in Impulsivity and Alcohol Use: A Meta-Analysis Using the UPPS Model of Impulsivity. Alcohol. Clin. Exp. Res. 2013, 37, 1441–1450. [Google Scholar] [CrossRef]
- Stephan, R.A.; Alhassoon, O.M.; Allen, K.E.; Wollman, S.C.; Hall, M.; Thomas, W.J.; Gamboa, J.M.; Kimmel, C.; Stern, M.; Sari, C.; et al. Meta-analyses of clinical neuropsychological tests of executive dysfunction and impulsivity in alcohol use disorder. Am. J. Drug Alcohol Abus. 2016, 43, 24–43. [Google Scholar] [CrossRef] [PubMed]
- De Wit, H. Impulsivity as a determinant and consequence of drug use: a review of underlying processes. Addict Biol 2009, 14, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Kovács, I.; Demeter, I.; Janka, Z.; Demetrovics, Z.; Maraz, A.; Andó, B. Different aspects of impulsivity in chronic alcohol use disorder with and without comorbid problem gambling. PLOS ONE 2020, 15, e0227645. [Google Scholar] [CrossRef]
- Jentsch, J.D.; Ashenhurst, J.R.; Cervantes, M.C.; Groman, S.M.; James, A.S.; Pennington, Z.T. Dissecting impulsivity and its relationships to drug addictions. Ann. New York Acad. Sci. 2015, 1327, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, A.; Bonsu, J.A.; Charnigo, R.J.; Milich, R.; Lynam, D.R. Impulsive Personality and Alcohol Use: Bidirectional Relations Over One Year. J. Stud. Alcohol Drugs 2016, 77, 473–482. [Google Scholar] [CrossRef] [PubMed]
- Sliedrecht, W.; Roozen, H.G.; Witkiewitz, K.; de Waart, R.; Dom, G. The Association Between Impulsivity and Relapse in Patients With Alcohol Use Disorder: A Literature Review. Alcohol Alcohol. 2021, 56, 637–650. [Google Scholar] [CrossRef] [PubMed]
- Hershberger, A.R.; Um, M.; Cyders, M.A. The relationship between the UPPS-P impulsive personality traits and substance use psychotherapy outcomes: A meta -analysis. Drug Alcohol Depend. 2017, 178, 408–416. [Google Scholar] [CrossRef]
- Saunders, J.B.; Aasland, O.G.; Babor, T.F.; De La Fuente, J.R.; Grant, M. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption-II. Addiction 1993, 88, 791–804. [Google Scholar] [CrossRef]
- Anton, R.F. Obsessive–compulsive aspects of craving: development of the Obsessive Compulsive Drinking Scale. Addiction. 2000, 95, 211–217. [Google Scholar]
- DiClemente, C.C.; Carbonari, J.P.; Montgomery, RP.; Hughes, S.O. The Alcohol Abstinence Self-Efficacy scale. Journal of studies on alcohol. 1994, 55, 141–148. [Google Scholar] [CrossRef]
- Gopukumar K., Rao Shobini L., Subbakrishna D. K.NIMHANS neuropsychology battery. National institute of mental Health and neuro sciences, Bangalore,2004.
- Hamilton, M. Hamilton anxiety rating scale (HAM-A). J Med. 1959, 61, 81–2. [Google Scholar]
- Hamilton, M. Hamilton Rating Scale for Depression (HRSD)-17 items. Br J Soc Clin Psychol 1967, 6, 278–296. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, S.; Bhatia, M. Quality of life as an outcome measure in the treatment of alcohol dependence. Ind. Psychiatry J. 2013, 22, 41–46. [Google Scholar] [CrossRef]
- Chen, C.-Y.; Storr, C.L. Alcohol Use and Health-Related Quality of Life among Youth in Taiwan. J. Adolesc. Heal. 2006, 39, 752–e9. [Google Scholar] [CrossRef]
- Nogueira, J.M.; Rodríguez-Míguez, E. Using the SF-6D to measure the impact of alcohol dependence on health-related quality of life. Eur. J. Heal. Econ. 2015, 16, 347–356. [Google Scholar] [CrossRef] [PubMed]
- Manning, V.; Gomez, B.; Guo, S.; Low, Y.D.; Koh, P.K.; Wong, K.E. An Exploration of Quality of Life and its Predictors in Patients with Addictive Disorders: Gambling, Alcohol and Drugs. Int. J. Ment. Heal. Addict. 2012, 10, 551–562. [Google Scholar] [CrossRef]
- Lahmek, P.; Berlin, I.; Michel, L.; Berghout, C.; Meunier, N.; Aubin, H.-J. Determinants of improvement in quality of life of alcohol-dependent patients during an inpatient withdrawal programme. Int. J. Med Sci. 2009, 6, 160–167. [Google Scholar] [CrossRef]
- Anker, J.J.; Kushner, M.G. Co-Occurring Alcohol Use Disorder and Anxiety: Bridging Psychiatric, Psychological, and Neurobiological Perspectives. Alcohol Res. 2019, 40. [Google Scholar] [CrossRef]
- Saatcioglu, O.; Yapici, A.; Cakmak, D. Quality of life, depression and anxiety in alcohol dependence. Drug Alcohol Rev. 2008, 27, 83–90. [Google Scholar] [CrossRef]
- Fischer, J.A.; Najman, J.M.; Plotnikova, M.; Clavarino, A.M. Quality of life, age of onset of alcohol use and alcohol use disorders in adolescence and young adulthood: Findings from an Australian birth cohort. Drug Alcohol Rev. 2015, 34, 388–396. [Google Scholar] [CrossRef]
- Solomon MAT, Sabari SOT, Srinivasan B. Correlation between age of alcohol dependence and quality of life—A hospital based cross sectional study. 2018 [cité 14 déc 2020]; Disponible sur: https://imsear.searo.who.int/jspui/handle/123456789/187032.
- Choi, S.W.; Na, R.H.; Kim, H.O.; Choi, S.B.; Choi, Y.S. The relationship between quality of life and psycho-socio-spiritual characteristics in male patients with alcohol dependence. J Korean Neuropsychiatr Assoc. 2006, 45, 459–467. [Google Scholar]
- Smith, J.P.; Randall, C.L. Anxiety and alcohol use disorders: comorbidity and treatment considerations. Alcohol Res. 2012, 34, 414–431. [Google Scholar] [PubMed]
- Flensborg-Madsen, T.; Mortensen, E.L.; Knop, J.; Becker, U.; Sher, L.; Grønbæk, M. Comorbidity and temporal ordering of alcohol use disorders and other psychiatric disorders: results from a Danish register-based study. Compr. Psychiatry 2009, 50, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Schneier, F.R.; Foose, T.E.; Hasin, D.S.; Heimberg, R.G.; Liu, S.-M.; Grant, B.F.; Blanco, C. Social anxiety disorder and alcohol use disorder co-morbidity in the National Epidemiologic Survey on Alcohol and Related Conditions. Psychol. Med. 2010, 40, 977–988. [Google Scholar] [CrossRef]
- Suasnabar, J.M.H.; Nadkarni, A.; Palafox, B. Determinants of alcohol use among young males in two Indian states: A population-based study. Trop. Med. Int. Heal. 2023, 28, 660–676. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.H.; Hong, H.G.; Jeon, S.-M. Personality and alcohol use: The role of impulsivity. Addict. Behav. 2012, 37, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Campanella, S.; Cimochowska, A.; Kornreich, C.; Hanak, C.; Verbanck, P.; Petit, G. Neurophysiological correlates of response inhibition predict relapse in detoxified alcoholic patients: some preliminary evidence from event-related potentials. Neuropsychiatr. Dis. Treat. 2014, 10, 1025–37. [Google Scholar] [CrossRef]
- Salgado, J.V.; Malloy-Diniz, L.F.; Campos, V.R.; Abrantes, S.S.C.; Fuentes, D.; Bechara, A.; Correa, H. Neuropsychological assessment of impulsive behavior in abstinent alcohol-dependent subjects. Rev. Bras. de Psiquiatr. 2009, 31, 4–9. [Google Scholar] [CrossRef]
- Cabé, N.; Lanièpce, A.; Pitel, A.L. Physical activity: A promising adjunctive treatment for severe alcohol use disorder. Addict. Behav. 2021, 113, 106667. [Google Scholar] [CrossRef]
- Gallo, G.G.; Curado, D.F.; Opaleye, E.S.; Donate, A.P.G.; Scattone, V.V.; Noto, A.R. Impulsivity and Mindfulness among Inpatients with Alcohol Use Disorder. Subst. Use Misuse 2020, 24, 1–8. [Google Scholar] [CrossRef]
Figure 1.
Mediation analysis: BIS attention -> HAM-A score -> QOL Physical Health.
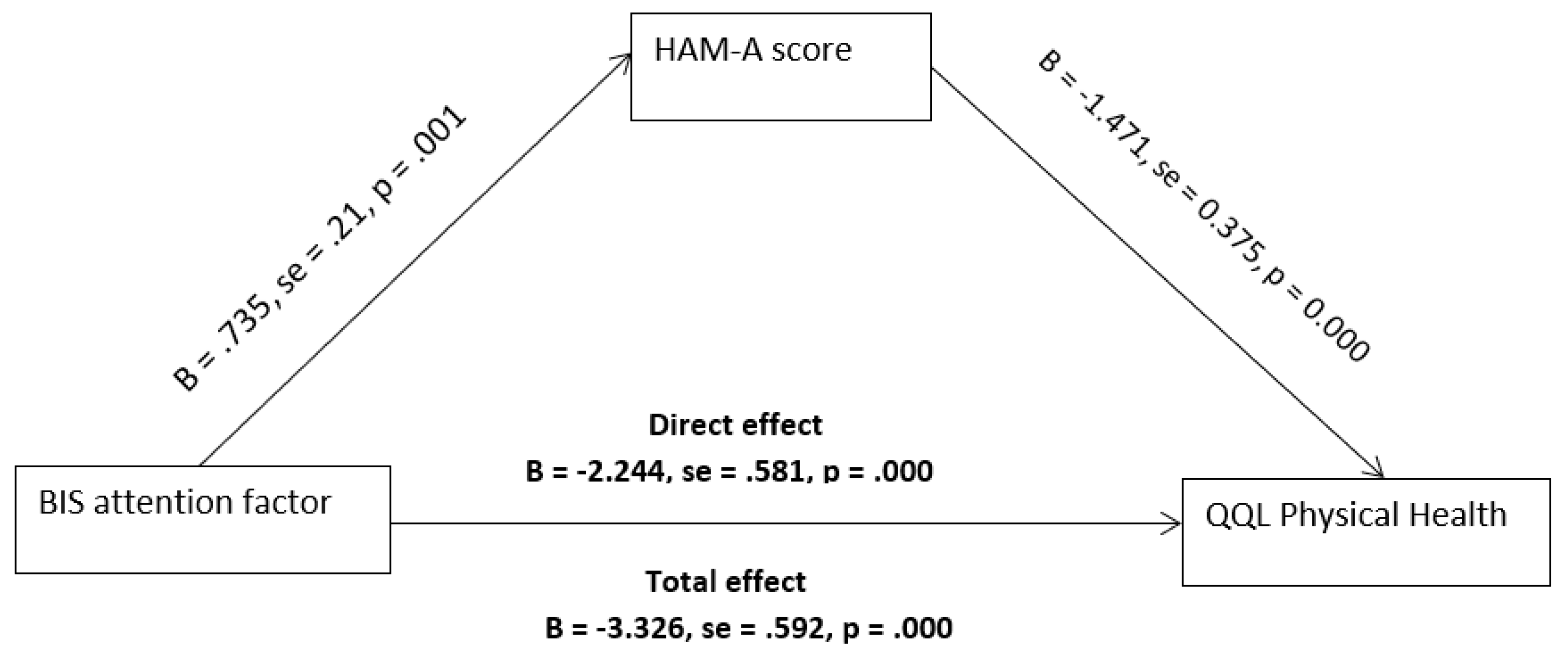
Figure 2.
Mediation analysis: BIS Self-control -> AUDIT score -> QOL Psychological Health.
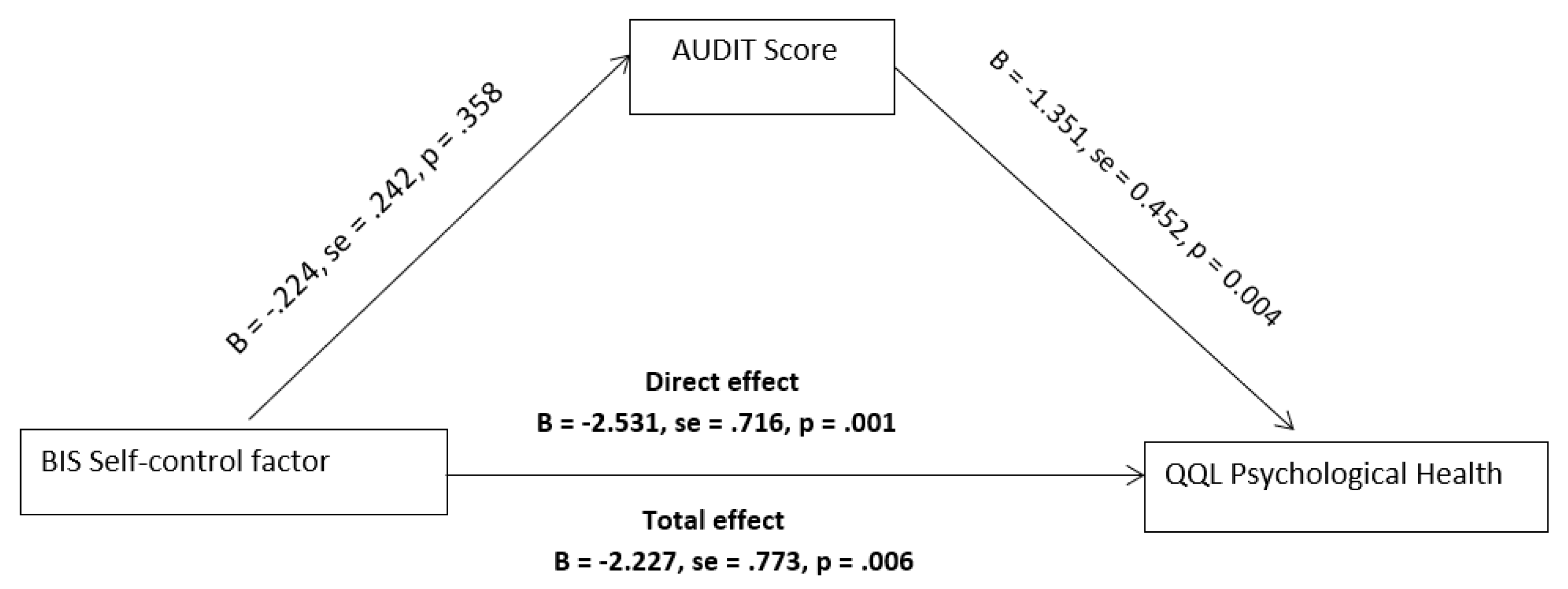

Table 1.
Comparison of socio-demographic characteristics, QOL domains, and BIS-11 dimensions between non-alcohol user healthy controls and individuals with alcohol use disorder.
Table 1.
Comparison of socio-demographic characteristics, QOL domains, and BIS-11 dimensions between non-alcohol user healthy controls and individuals with alcohol use disorder.
| Non-alcohol user healthy controls (n=44) | Alcohol Use Disorder (n=88) | |||
| Variable | N(%)/Mean (SD) | N(%)/Mean (SD) | P value | |
| Socio-demographic variables | ||||
| Education | School-educated | 14(31.82) | 38(43.2) | 0.207 |
| College-educated | 30 (68.18) | 50(56.8) | ||
| Type of family | Joint family | 30(68.18) | 48(54.4) | 0.133 |
| Nuclear Family | 14(31.3) | 40(45.5) | ||
| Employment status | Part-time Employed | 15(34.09) | 32(36.4) | 0.797 |
| Full-time Employed | 29(65.90) | 56(63.6) | ||
| Marital status | Unmarried | 11(25.0) | 28(31.8) | 0.338 |
| Married | 33(75.0) | 60(68.2) | ||
| Age at assessmnet | Age(yrs) | 36.06(9.80) | 37.55(8.31) | 0.387 |
| Quality of life domains | ||||
| QOL Physical health | 78.25(14.18) | 59.93(16.74) | <0.001 | |
| QOL Psychological | 75.56(13.45) | 50.75(18.93) | <0.001 | |
| QOL Social Relationships | 77.00(16.75) | 64.39(27.78) | 0.002 | |
| QOL Environment | 75.88(14.21) | 74.77(17.44) | 0.507 | |
| BIS -11 dimensions and total score | ||||
| BIS-11 Attention | 8.69(2.09) | 10.48 (3.29) | <0.001 | |
| BIS-11 Cognitive Instability | 6.23(2.31) | 6.70(2.03) | 0.225 | |
| BIS-11 Motor | 16.15(2.85) | 18.09(3.38) | <0.001 | |
| BIS-11 Perseverance | 6.38(1.44) | 7.95(2.47) | <0.001 | |
| BIS-11 Self-Control | 9.69(1.84) | 12.27(3.45) | <0.001 | |
| BIS-11 Cognitive Complexity | 12.69(2.42) | 14.07(2.43) | 0.003 | |
| BIS-11 Total | 59.84(6.90) | 68.43(8.79) | <0.001 | |
BIS-11=Barratt Impulsiveness Scale; QOL=Quality of life (Measured by WHOQOL-BREF).
Table 2.
Sociodemographic characteristics of the participants and their association with quality of life (QOL) (measured with the WHOQOL-Bref).
Table 2.
Sociodemographic characteristics of the participants and their association with quality of life (QOL) (measured with the WHOQOL-Bref).
| Total sample 88 |
QOL Physical Health |
QOL Psychological Health |
QOL Social Relationship |
QOL Environment |
||||||||||
| Variables | n(%) | Mean | (SD) | p | Mean | (SD) | p | Mean | (SD) | p | Mean | (SD) | p | |
| Age (mean) | 37.55(8.31) | 59.53 | 16.74 | 0.269* | 50.75 | 18.93 | 0.708* | 64.39 | 27.78 | 0.465* | 74.77 | 17.44 | 0.151* | |
| Education | School Educated | 38(43.2) | 60.79 | (19.49) | 0.771 | 53.42 | 21.08 | 0.421 | 66.79 | 30.02 | 0.623 | 75.84 | 17.75 | 0.727 |
| College Educated | 50(56.8) | 59.28 | (14.70) | 48.72 | 17.28 | 62.56 | 26.44 | 73.96 | 17.53 | |||||
| Employment Status | Unemployed | 32(36.4) | 56.81 | (17.93) | 0.356 | 49.82 | 19.58 | 0.672 | 63.38 | 35.213 | 0.858 | 74.81 | 16.794 | 0.991 |
| Employed | 56(63.6) | 61.71 | (16.09) | 52.38 | 18.24 | 64.96 | 23.232 | 74.75 | 18.112 | |||||
| Type of family | Joint Family | 40(45.5) | 61.65 | (16.46) | 0.541 | 50.80 | 17.79 | 0.987 | 65.35 | 18.79 | 0.837 | 77.05 | 19.86 | 0.436 |
| Nuclear Family | 48(54.5) | 58.50 | (17.11) | 50.71 | 20.14 | 63.58 | 33.91 | 72.88 | 15.32 | |||||
| Marital Status | Unmarried | 28(31.8) | 52.86 | 17.77 | 0.055 | 41.64 | 16.02 | 0.028 | 47.29 | 27.15 | 0.004 | 69.43 | 19.79 | 0.168 |
| Married | 60(63.6) | 63.23 | 15.45 | 55.00 | 18.91 | 72.37 | 24.64 | 77.27 | 15.98 | |||||
* Pearsons correlation with different domain of QOL.
Table 3.
Descriptive Statistics and Correlation Matrix of Study Variables (n = 88).
| N | Mean | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | ||
| 1 | QOL Physical Health | 88 | 59.93 | 16.74 | - | ||||||||||
| 2 | QOL Psychological | 88 | 50.75 | 18.93 | .551** | - | |||||||||
| 3 | QOL Social Relationships | 88 | 64.39 | 27.78 | .314* | .346* | - | ||||||||
| 4 | QOL Environment | 88 | 74.77 | 17.44 | .651** | .438** | 0.264 | - | |||||||
| 5 | BIS Attention | 88 | 10.48 | 3.29 | -.655** | -.441* | -.372* | -.547** | - | ||||||
| 6 | BIS Cognitive Instability | 88 | 6.70 | 2.03 | -0.239 | -0.113 | -0.204 | -0.075 | 0.213 | - | |||||
| 7 | BIS Motor | 88 | 18.09 | 3.38 | -0.145 | -0.148 | -0.025 | -0.062 | 0.325* | 0.237 | - | ||||
| 8 | BIS Perseverance | 88 | 7.95 | 2.47 | 0.161 | 0.201 | -0.255 | 0.047 | -0.029 | 0.275 | 0.039 | - | |||
| 9 | BIS Self-control | 88 | 12.27 | 3.45 | -.343* | -.406* | -0.144 | -.462** | .497** | 0.042 | .310* | -0.083 | - | ||
| 10 | BIS Cognitive Complexity | 88 | 14.07 | 2.43 | 0.106 | -0.109 | 0.219 | 0.165 | -0.140 | 0.018 | 0.104 | 0.074 | 0.081 | - | |
| 11 | BIS Total Score | 88 | 68.43 | 8.79 | -.402** | -360* | -0.245 | -.369* | .661** | ..459** | .682** | .305* | .685** | .295 | - |
| 12 | HAM D score | 88 | 3.02 | 3.40 | -.527** | -.433** | -.388** | -.595** | .504** | 0.045 | 0.088 | -0.074 | .347* | -0.124 | 0.310* |
| 13 | HAM A score | 88 | 6.45 | 5.10 | -.658** | -.485** | -.317* | -.637** | .475* | .054 | 0.089 | -0.226 | .255 | -.062 | .239 |
| 14 | AUDIT Total scores | 88 | 31.52 | 5.47 | -0.269 | -.325* | -0.270 | 0.025 | .299* | 0.266 | 0.252 | 0.093 | -0.142 | -0.073 | 0.202 |
| 15 | OCDS Total scores | 88 | 7.80 | 11.40 | -0.229 | -0.171 | -0.142 | -.388** | 0.318* | -0.296 | 0.170 | -0.079 | 0.284 | -0.096 | 0.180 |
| 16 | Age of onset of alcohol use | 88 | 20.11 | 5.33 | 0.083 | 0.029 | 0.083 | 0.129 | -0.126 | -0.042 | -0.007 | -0.198 | -0.123 | -0.201 | -0.191 |
| 17 | Age | 88 | 37.55 | 8.31 | 0.170 | 0.058 | -0.113 | 0.220 | -0.113 | 0.070 | 0.274 | -0.042 | -0.169 | -0.179 | -0.066 |
| 18 | Duration of alcohol use | 88 | 12.77 | 8.04 | -0.001 | -0.114 | -0.173 | -0.087 | .114 | 0.184 | 0.182 | 0.011 | 0.128 | -0.113 | 0.147 |
| 19 | AASE (C)Total | 88 | 58.75 | 19.74 | 0.281 | .345* | 0.285 | .436** | -.476* | -0.023 | -0.218 | -0.075 | -.444** | 0.127 | -.390* |
| 20 | RAVLT Total | 88 | 45.59 | 7.23 | -0.135 | 0.066 | -0.015 | -0.191 | 0.321* | -0.005 | 0.014 | 0.193 | 0.242 | -0.022 | 0.245 |
| 21 | RAVLT IR | 88 | 9.73 | 2.35 | -0.189 | -0.206 | 0.051 | -0.223 | 0.239 | -0.149 | -0.227 | 0.085 | 0.129 | -0.013 | 0.031 |
| 22 | RAVLT DR | 88 | 10.00 | 2.27 | -0.055 | -0.010 | -0.037 | -0.022 | 0.177 | -0.066 | -0.175 | 0.194 | 0.003 | 0.021 | 0.038 |
| 23 | N 2 BACK Hits | 88 | 6.25 | 1.33 | -0.142 | -0.154 | 0.080 | -0.261 | 0.189 | 0.011 | 0.026 | -0.060 | -0.147 | 0.081 | .034 |
| 24 | N 2 BACK Error | 88 | 3.75 | 1.54 | 0.125 | 0.144 | -0.225 | 0.194 | 0.040 | -0.098 | -0.062 | -0.149 | 0.105 | -0.218 | -0.115 |
| 25 | CFT Copy | 88 | 34.15 | 2.87 | 0.016 | -0.227 | -0.072 | 0.000 | 0.102 | -0.193 | -0.112 | 0.039 | 0.037 | -0.022 | -0.040 |
| 26 | CFT IR | 88 | 19.64 | 6.31 | 0.046 | 0.117 | -0.074 | -0.021 | 0.024 | 0.026 | -0.248 | 0.000 | -0.022 | -0.175 | -0.149 |
| 27 | CFT DR | 88 | 18.78 | 6.38 | 0.118 | 0.189 | -0.073 | 0.030 | -.035 | -0.048 | -0.196 | 0.004 | -0.120 | -0.236 | -0.221 |
| 28 | DSST TT | 88 | 310.20 | 112.41 | 0.016 | 0.144 | 0.240 | -0.183 | -0.073 | -0.153 | 0.116 | 0.028 | -0.088 | 0.053 | -0.034 |
| 29 | ANT Total | 88 | 11.73 | 3.07 | 0.097 | 0.207 | .211 | 0.244 | -.026 | 0.035 | 0.005 | 0.069 | -0.050 | 0.180 | 0.048 |
| 30 | Stroop Effect | 88 | 153.63 | 78.80 | -0.147 | -.046 | 0.100 | -.105 | .202 | -0.292 | 0.145 | -0.144 | 0.057 | 0.142 | 0.093 |
QOL = Quality of life; BIS = The Barratt Impulsiveness Scale Version 11; HAM D = Hamilton Depression Rating Scale; HAM A = Hamilton Anxiety Rating Scale; AUDIT = Alcohol Use Disorders Identification Test; OCDS = Obsessive Compulsive Drinking Scale; AASE(C) = Alcohol Abstinence Self-Efficacy Scale (Confident); RAVLT Total = Rey Auditory Verbal Learning Test total score of 5 trials; RAVLT IR = Immediate recall; RAVLT DR = Delayed recall; N 2 BACK Hits = Verbal 2 N Back test Hist; N 2 BACK Error = Errors; CFT Copy = Complex Figure Test copy score; CFT IR = Immediate Recall; CFT DR = Delayed Recall; DSST TT = Digit Symbol Substitution Test Time Taken; ANT Total = Animal Names Test total score. ** Correlation significant at the 0.01 level (2 tailed). * Correlation significant at the 0.05 level (2 tailed).
Table 4.
Univariate and Multivariate Linear Regression Analyses to Identify Predictors of Quality of Life (WHOQOL-BREF) among Individuals Undergoing detoxification for Alcohol Use Disorder (n = 88).
Table 4.
Univariate and Multivariate Linear Regression Analyses to Identify Predictors of Quality of Life (WHOQOL-BREF) among Individuals Undergoing detoxification for Alcohol Use Disorder (n = 88).
| Variables | Unadjusted | Adjusted | ||||||||
| Estimate | SE | 95% CI | p | Estimate | SE | 95% CI | p | |||
| LL | UL | LL | UL | |||||||
| Linear regression results for physical health domain | ||||||||||
| (Constant) | 92.111 | 7.021 | 77.9 | 106.31 | <0.001 | |||||
| BIS Attention | -3.327 | 0.593 | -4.523 | -2.131 | <0.001 | -2.272 | 0.672 | -3.631 | -0.912 | 0.002 |
| BIS Self-control | -1.664 | 0.703 | -3.082 | -0.246 | 0.023 | -0.101 | 0.582 | -1.278 | 1.076 | 0.863 |
| HAM D Total Score | -2.589 | 0.645 | -3.890 | -1.288 | <0.00 | -0.393 | 0.796 | -1.217 | 2.003 | 0.624 |
| HAM-A Total Score | -2.160 | 0.381 | -2.928 | -1.391 | <0.001 | -1.642 | 0.517 | -2.687 | -0.597 | 0.003 |
| R2/Adjusted R2 | .587/.545 | |||||||||
| Liner regression results for Psychological domain | ||||||||||
| (Constant) | 116.30 | 17.95 | 79.94 | 152.65 | <0.001 | |||||
| BIS Attention | -2.533 | 0.796 | -4.139 | -0.927 | 0.003 | -0.083 | 0.991 | -2.165 | 3.058 | 0.731 |
| BIS Self-control | -2.227 | 0.773 | -3.788 | -0.667 | 0.006 | -1.941 | 0.851 | -3.663 | -0.219 | 0.028 |
| HAM D Total Scores | -2.404 | 0.773 | -3.965 | -0.844 | 0.003 | -0.188 | 1.091 | -2.397 | 2.021 | 0.864 |
| HAM A Total Score | -1.798 | 0.501 | -2.808 | -0.788 | 0.001 | -1.112 | 0.711 | -2.551 | 0.327 | 0.126 |
| AUDIT Total Scores | -1.125 | 0.505 | -2.144 | -0.105 | 0.031 | -1.053 | 0.485 | -2.551 | -0.071 | 0.036 |
| R2/Adjusted R2 | .409/.331 | |||||||||
| Linear regression results for social relationships domain | ||||||||||
| (Constant) | 51.526 | 22.038 | 6.95 | 96.101 | 0.025 | |||||
| BIS Attention | -3.137 | 1.208 | -5.574 | -0.700 | 0.013 | -1.332 | 1.389 | -4.142 | 1.478 | 0.344 |
| HAM D Total scores | -3.165 | 1.160 | -5.506 | -0.824 | 0.009 | -1.903 | 1.737 | -5.415 | 1.609 | 0.280 |
| HAM A Total scores | -1.728 | 0.796 | -3.335 | -0.121 | 0.036 | 0.123 | 1.138 | -2.178 | 2.424 | 0.914 |
| Marital Status | 25.081 | 8.236 | 8.460 | 41.702 | 0.004 | 18.1 | 8.772 | 0.457 | 35.742 | 0.045 |
| R2/adjusted R2 | 0.273/.198 | |||||||||
| Linear regression results for Environment domain | ||||||||||
| (Constant) | 104.098 | 14.901 | 73.906 | 14.291 | <0.001 | |||||
| BIS attention | -2.896 | 0.684 | -4.276 | -1.516 | <0.001 | -0.877 | 0.779 | -2.455 | 0.701 | 0.267 |
| BIS self-regulation | -2.333 | 0.691 | -3.729 | -0.938 | 0.002 | -1.041 | 0.678 | -2.414 | 0.332 | 0.133 |
| HAM D Total scores | -3.046 | 0.635 | -4.328 | -1.764 | <0.001 | -0.475 | 0.93 | -2.359 | 1.409 | 0.612 |
| HAM-A Total scores | -2.178 | 0.406 | -2.998 | -1.358 | <0.001 | -1.36 | 0.586 | -2.547 | 0.172 | 0.123 |
| OCDS Total scores | -0.594 | 0.218 | -1.033 | -0.155 | 0.009 | -0.09 | 0.225 | -0.545 | 0.336 | 0.692 |
| AASE Total scores | 0.385 | 0.123 | 0.137 | 0.633 | 0.003 | 0.046 | 0.14 | -0.239 | 0.33 | 0.748 |
| R2/adjusted R2 | 0.540/0.465 | |||||||||
QOL = Quality of life; BIS = The Barratt Impulsiveness Scale Version 11; HAM D = Hamilton Depression Rating Scale; HAM A = Hamilton Anxiety Rating Scale; AUDIT = Alcohol Use Disorders Identification Test ; OCDS = Obsessive Compulsive Drinking Scale; AASE(C) = Alcohol Abstinence Self-Efficacy Scale (Confident).
Table 5.
Results of mediation analysis performed using PROCESS Macro.
| Relationship | Total effect | Direct effect | Indirect effect | 95% CI | Conclusion | |
| LL | UL | |||||
| BIS attention -> HAM-A score -> QOL Physical Health domain | -3.326 | -2.244 | -1.082 | -2.008 | -0.3598 | Partial mediation |
| P value | <0.001 | <0.001 | ||||
| BIS Self-control -> AUDIT score -> QOL Psychological domain | -2.227 | -2.531 | .303 | -.273 | .900 | No Mediation |
| P value | .006 | .001 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



