Submitted:
15 August 2023
Posted:
22 August 2023
You are already at the latest version
Abstract
Introduction: Frostbite is a condition that mostly affects skin, but also the underlying tissues, resulting from prolonged exposure to temperatures below freezing point (-0.55°C). Although frostbite has been a known phenomenon for several millennia, the exact incidence of frostbite is not known. This is partly due to variable internal and external etiological factors. One of the many consequences of climate change are extreme cold events, which increase the risk of frostbite in the general population, particularly among individuals who are involuntarily exposed to cold for prolonged periods of time. Severe cold injury can lead to deep frostbite with irreversible sequalae such as amputations.
Objectives: The reviews objective is to compare data collection and incidence rates of frostbite in different studies and populations.
Methods: Out of a total of 61 studies using the keywords "frostbite" and "incidence", 7 were selected that dealt with frostbite causes and incidence over 20 years. The studies results were briefly summarized and their conditions were compared.
Results: Frostbite can damage tissue superficially or deeply, depending on its degree. The results of the seven studies show a great variation of frostbite incidence depending on population, its size, and method of data collection. Studies that include the entirety of the civilian population show significantly lower frostbite incidence rates than studies focusing individuals who are exposed to temperatures below -0.55°C for long periods of time, such as mountaineers, military personnel, or homeless people. Although cold injuries are rare, they are becoming increasingly problematic for individuals who are exposed to a cold environment for prolonged periods of time due to climate change. This includes homeless individuals, outdoor workers in cold regions, alpinists and persons with inadequate equipment. The results underline different incidence rates for different populations and show that retrospectively collected data are insufficiently comparable. Enhanced frostbite susceptibility in some individuals should also be considered in the future in order to estimate the frostbite incidence more accurately. Moreover, defining frostbite susceptibility in advance could prevent frostbite incidence in the future to some degree, especially in military operations in the cold and certain leisure activities (e.g. mountaineering).
Conclusions: Frostbite poses a significant risk in cold regions and can lead to severe complications without adequate protection. To enhance our ability to predict frostbite occurrences within the general population, it is crucial to understand its incidence in relation to climatic factors. Establishing an international or national frostbite registry in high-risk countries could effectively guide preventive measures and safeguard individuals. This registry should encompass frostbite occurrences alongside contextual elements, such as freezing temperatures and cold exposure duration. Moreover, comprehensive weather conditions like wind chill, precipitation, humidity, and cloud cover must also be considered. When similar external conditions result in frostbite, investigating protective measures becomes pivotal. Furthermore, researching individual susceptibility to cold is essential to discern variations in frostbite vulnerability, especially for activities in cold environments.
Keywords:
frostbite
; incidence
1. Introduction
Frostbite is a condition that mostly affects skin, but also the underlying tissues, resulting from prolonged exposure to temperatures below freezing point (-0.55°C). It can range in severity from superficial (mild frostbite affecting only the superficial layers of the skin), to deep (severe frostbite that also affects muscles, tendons, and bones. In cases of severe frostbite, damaged tissue has to be removed and digit amputations may be necessary)1.
Frostbite has been known for many centuries. The first occurrence of cold-induced injury was identified in a pre-Columbian mummy dating back approximately 5000 years. Hannibals soldiers also experienced frostbite during their crossing of the Pyrenean Alps, loosing about half of the 46,000-strong army. Nearly all of the 250,000 soldiers who participated in Napoleon's invasion of Russia in the winter of 1812-1813 suffered from frostbite, resulting in only 350 able-bodied soldiers returning six months later2. Today, there are numerous studies examining frostbite among military personnel3 4. However, interest in frostbite and its causes, as well as possible preventive measures, has increased among the civilian population in recent years. This could be due to increased extreme weather events with very cold temperatures as a result of current climate change, leading to more frequent occurrences of frostbite5 6. Individuals who are involuntarily exposed to cold, such as homeless persons or those who must work outside during extreme cold, are particularly at risk for frostbite7 8 9 10. Severe frostbite can lead to complications such as cold sensitivity, persistent numbness, amputations, or death11. The biggest issue with the studies concerning frostbite incidence so far is the variable methodology, which is due to the fact that the published articles are mostly retrospective in nature, dealing with a specific population in a particular environment. Comprehensive studies, describing the incidence of frostbite precisely or predicting it, are currently lacking. Preventive measures such as education on proper behavior during extreme cold and the selection of appropriate clothing can lead to fewer cases of frostbite12 13. Prevention would not only result in fewer cases of frostbite but could also reduce healthcare costs incurred by both acute treatment and post-treatment of frostbite. To work preventively, a database is needed that comprehensively records frostbite, its causes, and severity. Furthermore, being aware of the existence of frostbite susceptibility (individuals, diagnostic tests to assess the predisposition to frostbite before cold exposure occurs could enable a preventive pre-selection of individuals, especially prone to cold injury. Based on the results of the Ski-Everest study and others, additional preventive measures can be adjusted in such alpinists accordingly 13, 14. The purpose of this review is to provide an overview of some of the data collected thus far regarding frostbite to illustrate the extent of frostbite within a larger population and to demonstrate data variability. One of the goals of analyzing frostbite incidence is better understanding its occurrence in general population and prevent it in the future as far as possible.
2. Methods
To conduct a review on the incidence of frostbite, articles using the keywords "frostbite" and "incidence" were searched on PubMed for the period between 2002 and 2022 (a duration of 20 years). Out of a total of 61 studies, 7 were selected, which reported on the occurrence, incidence in a specific population, and exploration of causes. Studies focusing on data collection rather than methods of treating cold-induced injuries were chosen.
Studies that focused more on the treatment methods of frostbite rather than its occurrence were excluded from this review. The studies can be broadly categorized based on their data collection methods. Five studies gathered data from patients records, while two studies utilized questionnaires (Figure 1).
In addition to reporting frostbite incidences, this review also presented pertinent cofactors derived from the study findings, which are considers contributory risk factors for frostbite. These identified cofactors encompassed a range of demographic, environmental and individual variables that may influence the susceptibility and occurrence of frostbite. The comprehensive exploration of their cofactors adds valuable insights into the multifaceted nature of frostbite etiology and aids in enhancing our understanding of preventive measures. The following provides a brief overview of the results of the studies.
3. Results
This review is based on a collection of articles aimed at determining the incidence of frostbite. Additionally, the studies pursued various objectives related to frostbite. The following goals were pursued: The aim of the Juopperi et al. study was to determine the incidence of frostbite and its association with sex, age, and ambient temperature in a nationwide sample14. The aim of the Ervasti et al. study was to analyze the life-time occurrence of frostbite in young men and its association with the cold-provoked white finger syndrome (CPWF), smoking, and hand vibration15. Harirchi et al. investigated the incidence of frostbite and associated factors in mountaineering, with a focus on identifying modifiable factors that could reduce its frequency and severity16. Némethy et al. recorded all visits to the Everest Base Camp Medical Clinic (Everest ER) to characterize the medical problems that occur in these patients including dermal trauma such as frostbite17. Ströhle et al. investigated the incidence of frostbite injuries in the Austrian Alps, identify frostbite risk factors, and optimize prevention and treatment strategies18. The aims of the Endorf and Nygaard studies from 2021 were to investigate the incidence of amputation as a result of frostbite injury in the United States using a national sample of hospitalization, and to describe the social determinants of amputation from frostbite injury in a nationally representative sample and to examine social and comorbid factors associated with frostbite injury in comparison to isolated hand or foot burns19 20.
But there are some differences in studies population, which, among other things, lead to varying results in frostbite incidence.
The study population in Juopperi et al. included all patients admitted to hospitals in Finland between October and May from 1986 to 1995, who had frostbite as their primary or secondary diagnosis. The data were collected from the nationwide hospital discharge register maintained by the National Research and Development Centre for Welfare and Health since 1967. A total of 1212 patients who met the study criteria were included21. Ervasti et al. had a study population consisted of Finnish men aged 17-30 years entering military service. Data were collected using questionnaires. A total of 5839 men were asked about cold-related disturbances in the peripheral circulation, exposure to vibration, and smoking habits22. In Harirchi et al. participants included mountaineers selected by simple non-randomized sampling from active members of the Tehran Province Mountaineering Council, registered mountaineering clubs in the city, and collegiate mountaineering groups at their scheduled gatherings and ascents. The study defined mountaineers as those with at least two years of mountaineering experience involving at least two ascents per month to summits higher than 3000 m. Data were collected using questionnaires. A total of 637 participants met the study criteria23. The clinic documentation of patients attended at Everest ER during the initial 10 consecutive seasons (2003 to 2012) was examined in the Némethy et al. study. The medical staff at Everest ER attended to a total of 2941 patients, resulting in 3569 diagnoses including dermal diagnosis which also means frostbite24. The data from Ströhle et al. included out-of-hospital data from the National Registry of Alpine Accidents from January 1, 2005, to December 31, 2015, with frostbite injuries. The collected data were obtained from the National Registry of Alpine Accidents maintained by the Austrian Board for Alpine Safety and a clinical information system used by the Innsbruck Medical University Hospital, the referral center for critical medical cases in western Austria. A total of 31 patients' data were collected25. Endorf and Nygaard had a population consisted of patients who were identified using International Classification of Diseases Version 10 diagnosis codes associated with the initial encounter of frostbite injury (T33-T34). The data were obtained from the National Inpatient Sample from 2016 to 2018. A total of 8085 patients were included in the study26 In their next study from 2021 the population was a bit different: Eligible patients were those aged 15 years and older who were identified using International Classification of Diseases Version 10 diagnosis codes associated with the initial encounter of frostbite injury (T33-T34) or isolated burns to the hands or feet (T23-T24). Data were obtained from the National Inpatient Sample from 2016 to 2018. A total of 42,810 patients were included, of which 7,560 had frostbite injury27.
Certain studies exhibited a substantial variability in the scope of data analyzed from frostbite patients, while others provided only limited supplementary information.
Juopperi et al., Ströhle et al., Endorf and Nygaard all incorporated variable related to sex, age, length of hospitalization and location of frostbite occurrence in their studies. Additionally, Ströhle at al provided supplementary data penitent to frostbite occurrence, notably including environmental factors across the year in the Austrian Alps such as ambient temperature, wind speed, weather forecast, altitude of the event and duration of cold exposure (Figure 2).
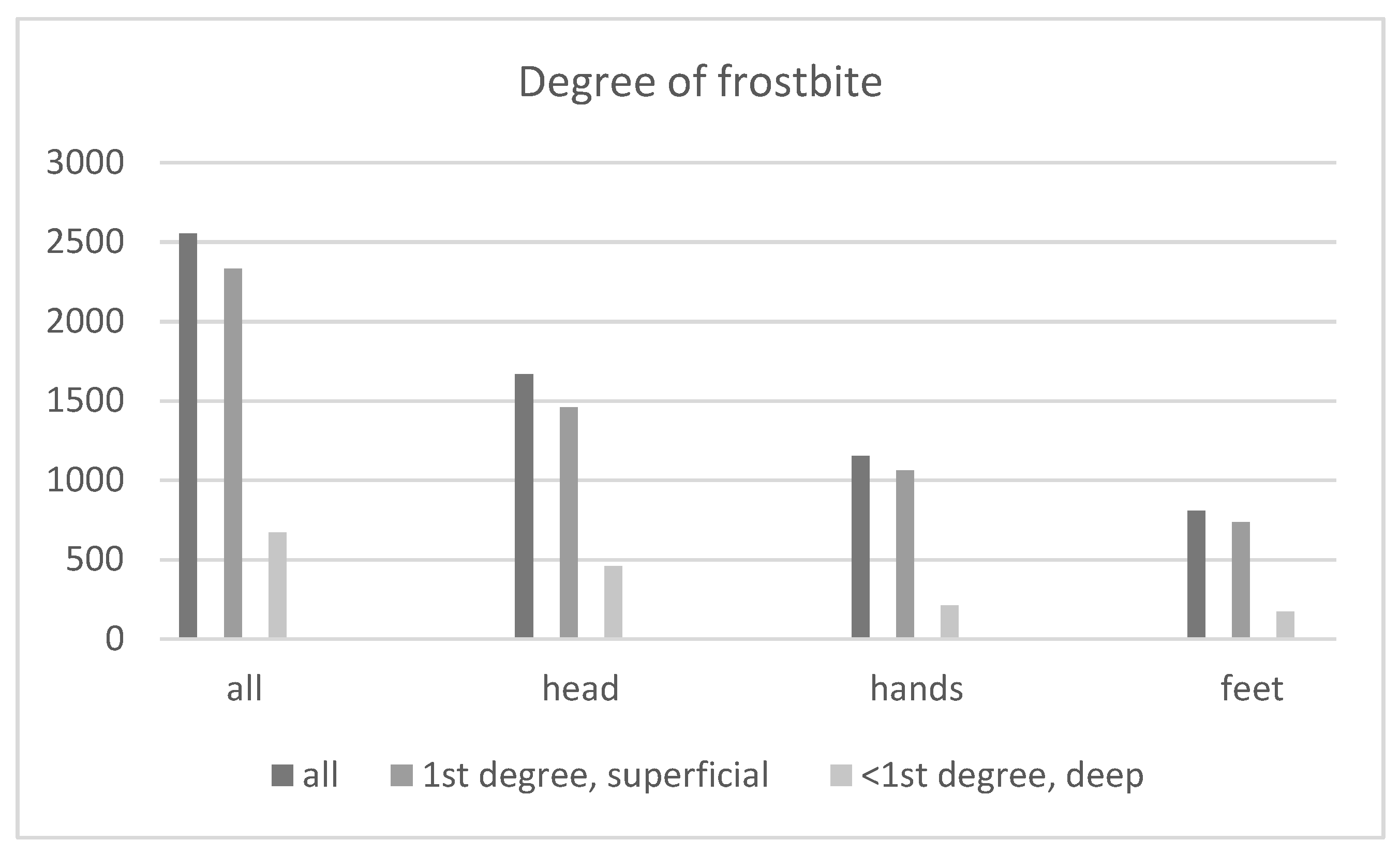
Ervasti et al. focused on the affected body parts as data: The sites most prone to frostbite were the head, 1668 cases (31%), followed by the hands, 1154 (20%), and the feet, 810 (15%). The risk for frostbite in different body parts was increased among the subjects with CPWF (95% CI: 1.66 to 3.87), regular smokers (95% CI: 1.02 to 3.15), and those exposed to vibration (95% CI: 1.07 to 4.03).
Figure 3.
Life-time cumulative occurrence of frostbite in different areas of the body. The total number of respondents was 5839. Values denote absolute (percentage) numbers of subjects. Data items designated as missing represent subjects whose answers on frostbite were not complete. (Based on the data from: Ervasti, et al., 2004).
Figure 3.
Life-time cumulative occurrence of frostbite in different areas of the body. The total number of respondents was 5839. Values denote absolute (percentage) numbers of subjects. Data items designated as missing represent subjects whose answers on frostbite were not complete. (Based on the data from: Ervasti, et al., 2004).
The same did Harirchi et al. as they also investigated the different body parts that were affected: Participants were asked to indicate the body part affected, the degree of injury, approximate altitude, season, equipment used, whether they were accompanied by a guide, and perceived causes of the injury (Figure 4).
Lack of proper equipment and lack of a guide (p<0.001) were significantly associated with frostbite. Inappropriate clothing, lack or incorrect use of equipment, and lack of knowledge about how to deal with cold and severe weather were identified as the main reasons for frostbite (Figure 5).
Due to variations in population characteristics, environmental factors and research methodologies employed in these studies, a wide range of frostbite injury incidences was observed (Figure 6).
The results from Juopperi et al. showed that the overall incidence of frostbite in Finland was 2.5 per 100,000 inhabitants. In northern Finland the incidence was higher than in Southern and central Finland and the Helsinki area (3.9/100,000 per year to 2.8/100,000 per year). There was a higher incidence in males than females and a linear increase with age. The annual incidence of frostbite began to rise at temperatures below -15°C and was significant at under -20°C, particularly in northern Finland. However, the daily incidence increased most in the urban area of Helsinki (Figure 7). The results from Ervasti et al. showed that the life-time and annual occurrences of frostbite were 44% and 2.2%, respectively (n=2555). 2333 subjects (41%) had suffered first-degree freezing injury, and 671 (12%) suffered severe injury at some time in their lives. The mean incidence of frostbite in Hariarchi et al. was 366/1000 population per year, with grade 1 injuries (83.0%), and hands (26.4%) and feet (24.1%) involvement being most common.
Némethy et al. identified a total of 280 dermatology cases, out of which 27% were attributed to frostbite injuries. This corresponds to 43 frostbite cases, resulting in an annual frostbite incidence of 0.8/100,000. Ströhle et al. found an incidence of 0.07/100,000 per year. The results showed that thirty-one frostbite cases were documented nationwide, 18 (58%) of which occurred in the western states of Austria and were potentially referred to the Innsbruck Medical University Hospital. Six (19.6%) patients were female. Frostbite was almost exclusively related to fingers and toes (90% of cases).
The incidence rate in Endorf and Nygaard was 0.83/100,000 per year when patients aged 15 and younger were excluded. Including these patients as in the second study of Endorf and Nygaard the incidence was 0.95. The results of both studies showed, among other things, that the social factors associated with frostbite injury, homelessness and black race were independently associated with a higher likelihood of amputation at the primary admission.
Although the Gorjanc et al. articles and the work of the author´s research group do not explicitly analyse the occurrence of frostbite in a population, the idea behind might be of importance for better understanding the frostbite incidence in the future. The fact, that some alpinists seem to be more prone to frostbite injury and also that this susceptibility can be measured or at least estimated with a simple cold water immersion test could prevent and/or reduce many frostbite injuries in predicted outdoor activities in the cold28 29.
The results presented here are characterized by the utilization of diverse methodologies and the collection of different data sets. The retrospectively gathered incidences, in this regard, exhibit significant variations among them.
4. Discussion
Frostbite injuries, a form of cold injury, are relatively rare but their incidence is expected to increase with the progression of climate change.
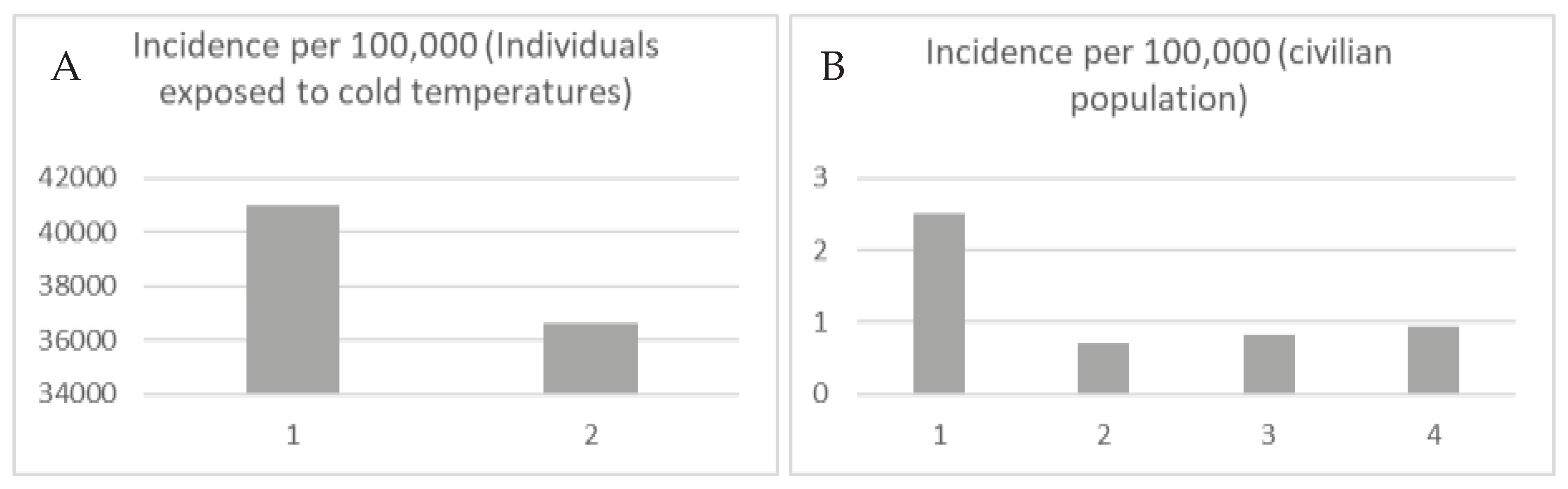
The previously presented studies demonstrate that there are varying incidences and degrees of frostbite depending on the studied population and their environment (Figure 8). This indicated that data comparability is compromised unless the external and internal circumstanced surrounding the occurrence of cold injury are documented.
Individuals who are frequently exposed to cold environments are more likely to suffer from frostbite. For example, the incidence among mountain climbers is several times higher than in a population of all residents of an area30. Comparability of the incidences is not given when comparing experienced mountain climbers with suitable equipment31 on the one hand and disadvantaged individuals, such as homeless people, drug or alcohol addicts, or those suffering from psychiatric diagnosis on the other hand32. Also, groups of people who are involuntarily exposed to the outdoors, such as workers in a cold environment, are more likely to suffer from frostbite)33 34 35 36. Different groups of people with frostbite also occur in different regions of a country. The urban population seems to differ from a more rural population, as it has been shown that when comparing urban incidence with incidence in the northern, more rural Finland, different incidences occur37.
It has been shown that frostbite occurs regardless of age and gender, although some results showed a lower risk of frostbite in women38 39. No study has addressed the causes of the different incidences of frostbite in men and women. It is possible that frostbite injuries are due to different risk-taking behaviors between men and women. However, it could also be that there are physiological factors that account for the different incidences.
The retrospective nature of the studies poses a problem, as not all patient data may have been documented correctly. Early discharge from the hospital may result in incomplete patient records40 41. In addition, it is possible that not all patients with frostbite are documented if they are treated in hospitals that are not part of the dataset42. With mild frostbite, it is also conceivable that no treatment was performed or that treatment was performed so late that cofactors such as alcohol or drug abuse were no longer detectable if they had caused the frostbite43. Accurate incidences are difficult to determine without a complete dataset and are therefore unreliable.
Further inaccuracies in data collection and thus in the correct representation of incidences can arise from the use of questionnaires, as these are filled out by participants themselves based on their memories44. Even though painful experiences are better remembered than others, errors can occur, which make it more difficult to predict incidences with certainty.
Thus, reliable data is lacking to enable predictability of frostbite worldwide. According to recent studies dealing with frostbite susceptibility, frostbite incidence could further be reduced by positive selection of participants in predicted outdoor activities in the cold.
More accurate predictability, based also on individuals’ cold susceptibility, could contribute to more accurate prevention measures, such as cold-resistant clothing, better protective measures, or in a higher concentration of homeless shelters in cold environments)45 46. A comprehensive database is needed that provides exact information about frostbite patients. It must be known under what conditions the frostbite was contracted (e.g. temperature, wind speed, and humidity), what degree the frostbite had, and what initial treatment steps were taken.
5. Conclusion
In cold regions, frostbite can occur with insufficient cold protection and can sometimes result in severe complications. To obtain better predictability of frostbite occurrence in a general population, it is necessary to know the exact incidence of frostbite depending on climatic environmental factors. An international registry of frostbite or at least national registries in the countries with high frostbite incidence could be helpful in targeting prevention measures and protecting people from frostbite in the future.
Such a registry should document both the occurrence of frostbite and consider the external circumstances, such as the temperature at which the freezing injury occurred, as well as the duration of cold exposure experienced by the patient. Additionally, weather conditions, including wind chill, precipitation, humidity and cloud cover, should also be taken in account. In cases where frostbite occurs in individuals under the same external conditions, it is crucial to ascertain whether and with what protective equipment the patients were safeguarded against the cold. If external circumstances are consistent, it becomes necessary to investigate individual differences in susceptibility to cold and determine whether some individuals are more prone to experiencing frostbite than others.
For planned outdoor activities in the cold (alpinists, military personal, etc.), individual cold susceptibility assessment can be helpful in order to prevent frostbite.
References
- Endorf, F. W., & Nygaard, R. M. (2021). Social Determinants of Poor Outcomes Following Frostbite Injury: A Study of the National Inpatient Sample. Journal of Burn Care & Research 1261-5. [CrossRef]
- Endorf, F. W., & Nygaard, R. M. (2021). Socioeconomic and Comorbid Factors Associated With Frostbite Injury in the United States. Journal of Burn Care & Research 646-51. [CrossRef]
- Endorf, F. W., Alapati, D., Xiong, Y., DiGiandomenico, C., Rasimas, C. S., Rasimas, J. J., & Nygaard, R. M. (2022, 101:34). Biopsychosocial factors associated with complications in patients with frostbite. Medicine 1-5. [CrossRef]
- Ervasti, O., Juopperi, K., Kettunen, P., Remes, J., Rintamäki, H., Latvala, J.,... Hassi, J. (2004). The occurrence of frostbite and its risk factors in young men. International Journal of Circumpolar Health 71-80. [CrossRef]
- Freer, L., Handford, C., & Imray, C. H. (2016). Frostbite. In P. S. Auerbach, T. A. Cushing, & N. S. Harris, Auerbach's Wilderness Medicine. Elsevier.
- Gorjanc, J., Morrison, S., Blagus, R., & Mekjavic, I. (2018, Jun). Cold Susceptibility of Digit Stumps Resulting from Amputation After Freezing Cold Injury in Elite Alpinists. High Alt Med Biol. 19(2), 185–192. [CrossRef]
- Gorjanc, J., Morrison, S., McDonnell, A., Mekjavic, P., Blagus, R., & Mekjavic, I. (2019). Ski-Everest (8848 m) Expedition: Digit Skin Temperature Responses to Cold Immersion May Reflect Susceptibility to Cold Injury. Wilderness Environ Med. 141–149. [CrossRef]
- Gross, E. A., & Moore, J. C. (2012;5). Using thrombolytics in frostbite injury. Journal of Emergencies, Trauma, and Shock 267–271. [CrossRef]
- Harirchi, I., Arvin, A., Vash, J. H., & Zafarmand, V. (2005;39). Frostbite: incidence and predisposing factors in mountaineers. Br J Sports Med 898–901. [CrossRef]
- Hickey, S., Whitson, A., Jones, L., Wibbenmeyer, L., Ryan, C., Fey, R.,... Bailey, J. K. (2020;41). Guidelines for thrombolytic therapy for frostbite. Journal of Burn Care & Research 176-83. [CrossRef]
- Juopperi, K., Hassi, J., Ervasti, O., Drebs, A., & Näyhä, S. (2002;61). Incidence of frostbite and ambient temperature in Finland, 1986–1995. A national study based on hospital admissions. International Journal of Circumpolar Health 352-62. [CrossRef]
- MSMR. (2019). Update: cold weather injuries, active and reserve components, U.S. Armed Forced, July 2014-June 2019. MSMR, 17-26.
- Némethy, M., Pressman, Andrew B, Freer, Luanne, & McIntosh, Scott E. (2015). Mt Everest Base Camp Medical Clinic "Everest ER": Epidemiology of Medical Events During the First 10 Years of Operation. Wilderness & Environmental Medicine(26) 4-10. [CrossRef]
- Nygaard, R. M., & Endorf, F. W. (2018;39). Frostbite in the United States: An examination of the National Burn Repository and National Trauma Data Bank. Journal of Burn Care & Research 780-5. [CrossRef]
- tröhle, M., Rauch, S., Lastei, P., Brodmann Maeder, M., Brugger, H., & Paal, P. (2018). Frostbite Injuries in the Austrian Alps: A Retrospective 11-Year National Registry Study. High Altitude Medicine & Biology 1-5. [CrossRef]
Figure 1.
Research methods for reviewed studies.
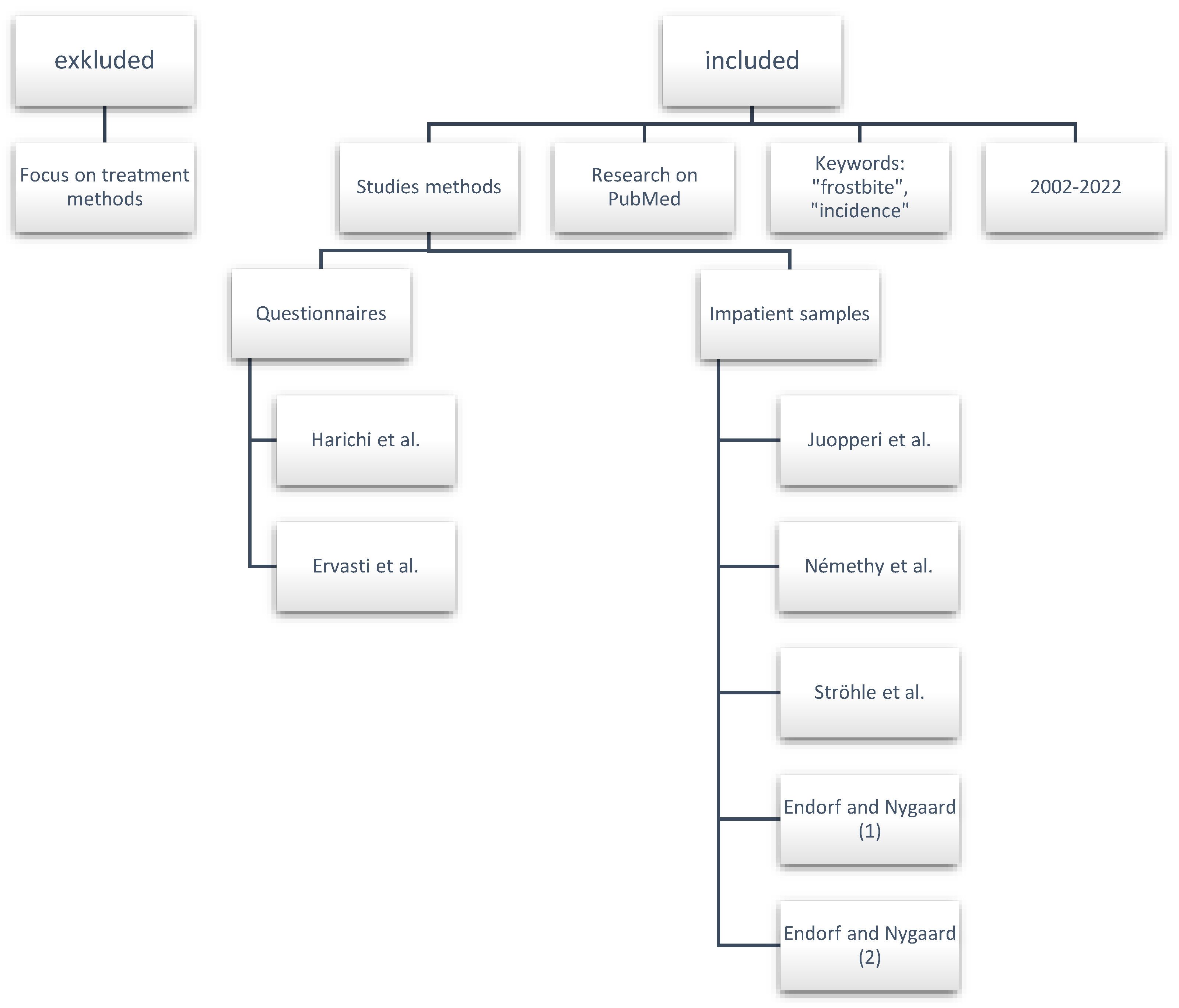
Figure 2.
Incidence of frostbite injuries across the year in the Austrian Alps (N=31, 2005-2015) (Ströhle, et al., 2018).
Figure 2.
Incidence of frostbite injuries across the year in the Austrian Alps (N=31, 2005-2015) (Ströhle, et al., 2018).
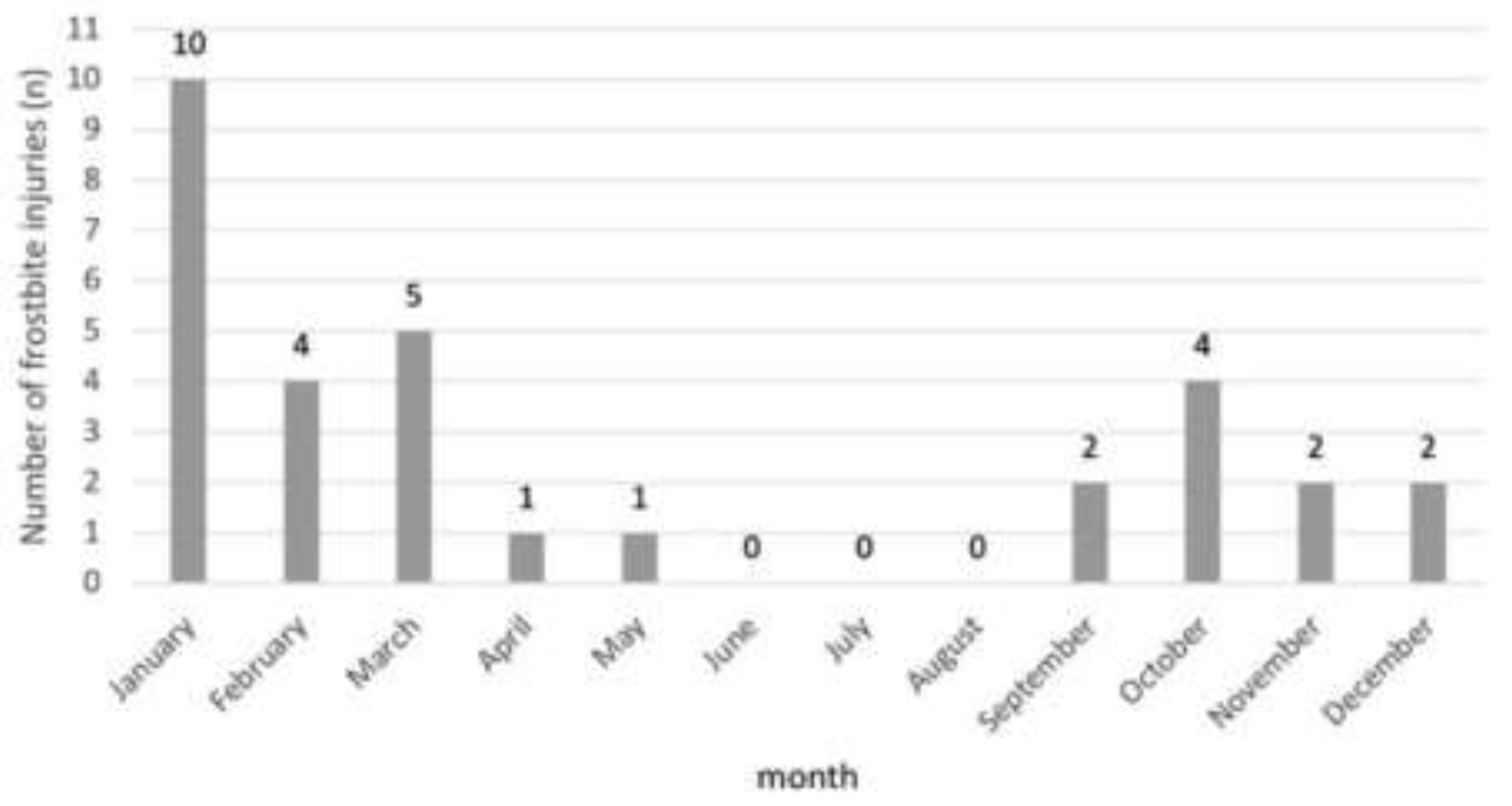
Figure 4.
Frostbite injuries in different body parts (Harirchi, et al., 2005).
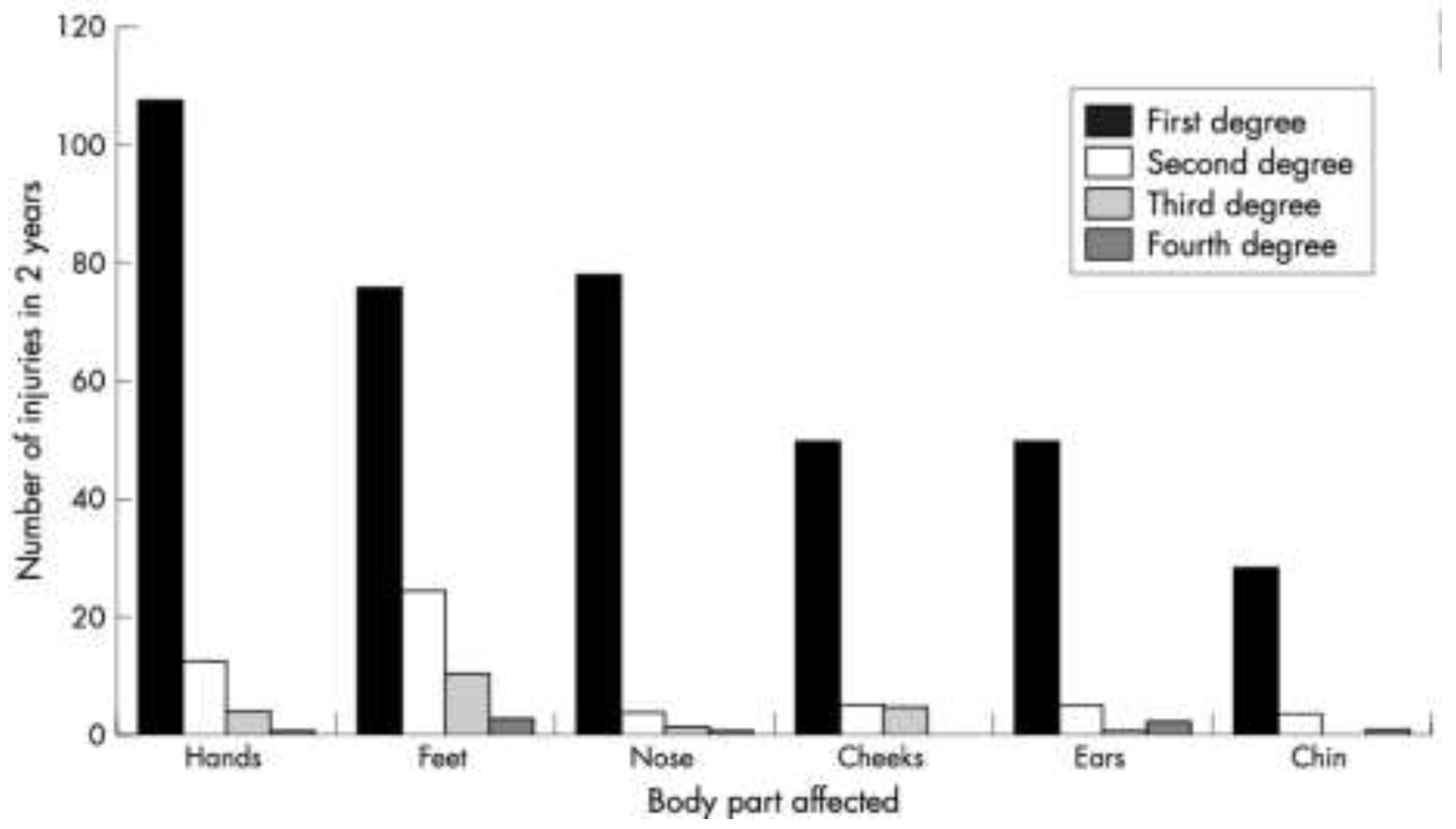
Figure 5.
Mountaineers’ view of the main cause of frostbite injury (Harirchi, et al., 2005).
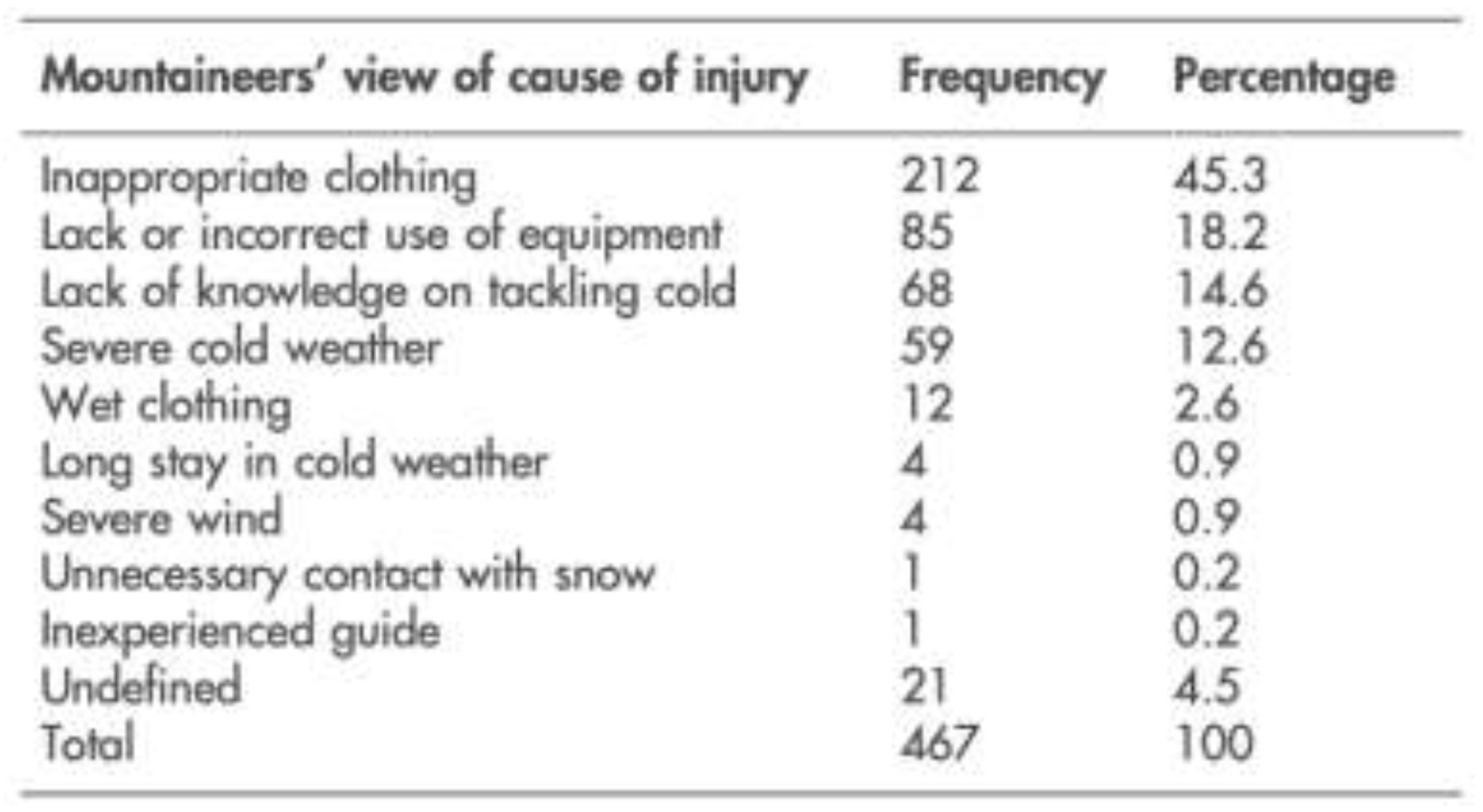
Figure 6.
Frostbite incidence in different studies per 100,000 per year and occurrence in %. Different studies had different numbers of frostbite cases in different study populations such as civil population (CP), Military personnel (MP) or mountaineers (M).
Figure 6.
Frostbite incidence in different studies per 100,000 per year and occurrence in %. Different studies had different numbers of frostbite cases in different study populations such as civil population (CP), Military personnel (MP) or mountaineers (M).
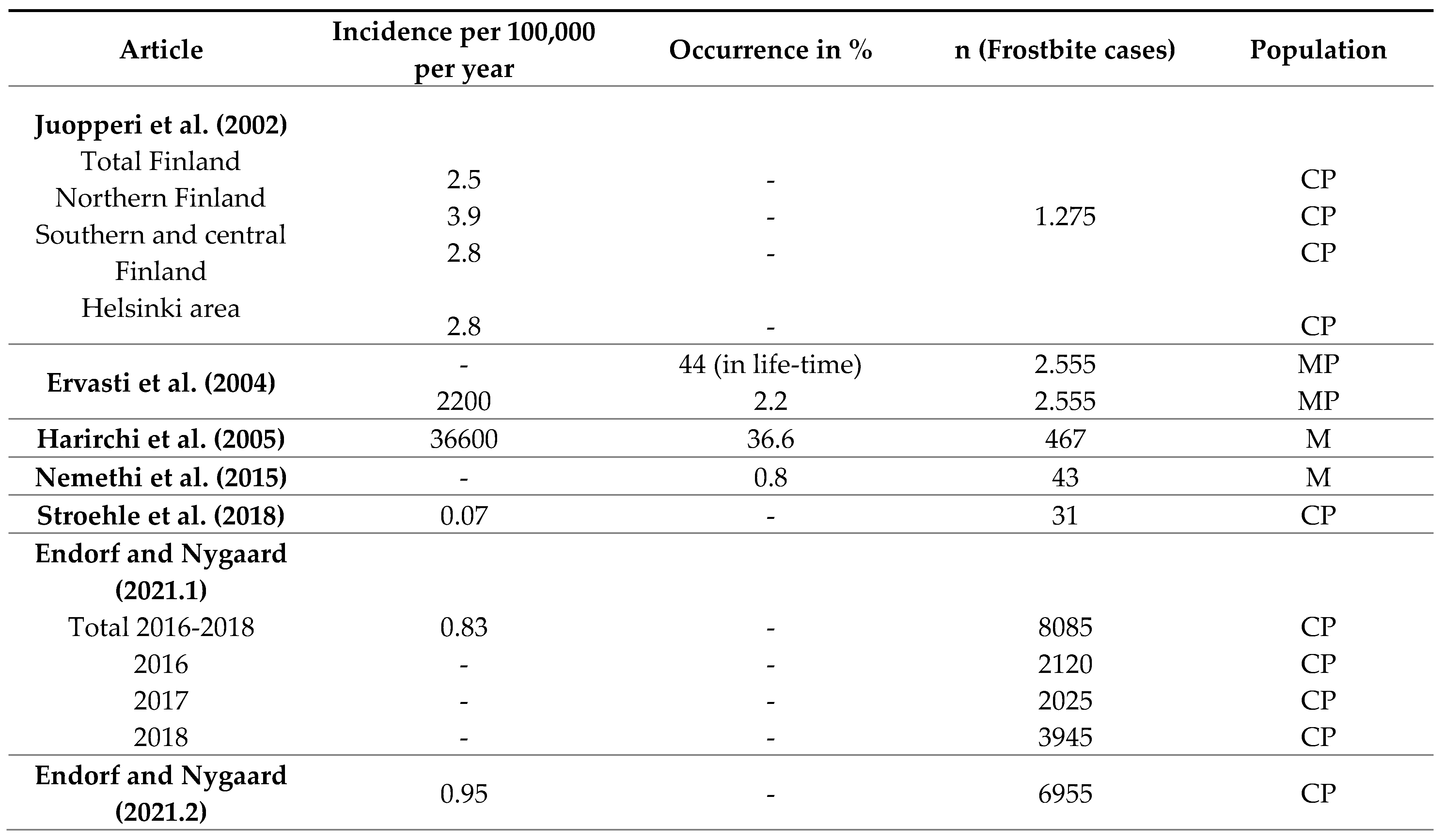
Figure 7.
Average annual incidence of frostbite per 100,000 inhabitants and monthly mean temperatures in southern Finland (Helsinki) and northern Finland (Oulu) in 1961-1990 (Juopperi, et al. 2002).
Figure 7.
Average annual incidence of frostbite per 100,000 inhabitants and monthly mean temperatures in southern Finland (Helsinki) and northern Finland (Oulu) in 1961-1990 (Juopperi, et al. 2002).
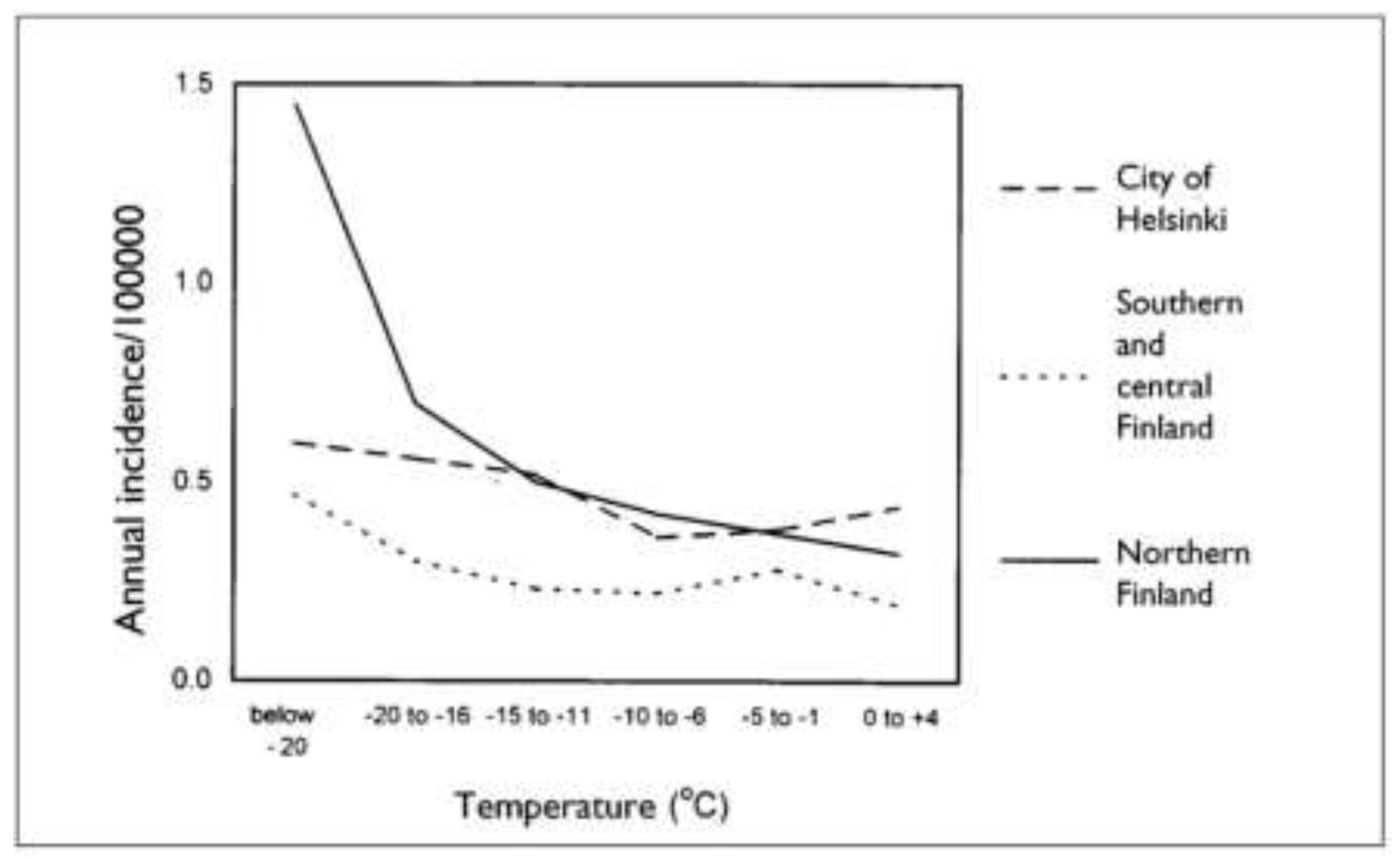
Figure 8.
A Frostbite incidence per 100,000 Individuals exposed to cold temperatures. A1 shows the incidence based on Ervasti, et al. (2004), A2 shows the incidence based on Harirchi, et al. (2005) B Frostbite incidence per 100,000 civilian population. B1 shows the incidence based on Juopperi, et al. (2002), B2 shows the incidence based on Stroehle, et al. (2018), B3 shows the incidence based on Endorf and Nygaard (2021) and B4 shows the incidence based on Endorf and Nygaard (2021).
Figure 8.
A Frostbite incidence per 100,000 Individuals exposed to cold temperatures. A1 shows the incidence based on Ervasti, et al. (2004), A2 shows the incidence based on Harirchi, et al. (2005) B Frostbite incidence per 100,000 civilian population. B1 shows the incidence based on Juopperi, et al. (2002), B2 shows the incidence based on Stroehle, et al. (2018), B3 shows the incidence based on Endorf and Nygaard (2021) and B4 shows the incidence based on Endorf and Nygaard (2021).
| 1 | Gross & Moore, 2012 |
| 2 | Freer, Handford & Imray, 2016 |
| 3 | MSMR, 2019 |
| 4 | Ervasti, et al., 2004 |
| 5 | Nygaard & Endorf, 2018 |
| 6 | Hickey, et. al., 2020 |
| 7 | Ervasti, et al., 2004 |
| 8 | Endorf & Nygaard, 2021 |
| 9 | Endorf & Nygaard, 2022 |
| 10 | Endorf, et al., 2022 |
| 11 | Ervasti, et al., 2004 |
| 12 | Harirchi, et al., 2005 |
| 13 | Ströhle, et al., 2018 |
| 14 | (Juopperi, Hassi, Ervasti, Drebs, & Näyhä, 2002;61) |
| 15 | (Ervasti, et al., 2004) |
| 16 | (Harirchi, Arvin, Vash, & Zafarmand, 2005;39) |
| 17 | (Némethy, Pressman, Andrew B, Freer, Luanne, & McIntosh, Scott E, 2015) |
| 18 | (Ströhle, et al., 2018) |
| 19 | (Endorf & Nygaard, Social Determinants of Poor Outcomes Following Frostbite Injury: A Study of the National Inpatient Sample, 2021) |
| 20 | (Endorf & Nygaard, Socioeconomic and Comorbid Factors Associated With Frostbite Injury in the United States, 2021) |
| 21 | (Juopperi, Hassi, Ervasti, Drebs, & Näyhä, 2002;61) |
| 22 | (Ervasti, et al., 2004) |
| 23 | (Harirchi, Arvin, Vash, & Zafarmand, 2005;39) |
| 24 | (Némethy, Pressman, Andrew B, Freer, Luanne, & McIntosh, Scott E, 2015) |
| 25 | (Ströhle, et al., 2018) |
| 26 | (Endorf & Nygaard, Social Determinants of Poor Outcomes Following Frostbite Injury: A Study of the National Inpatient Sample, 2021) |
| 27 | (Endorf & Nygaard, Socioeconomic and Comorbid Factors Associated With Frostbite Injury in the United States, 2021) |
| 28 | (Gorjanc J. , et al., 2019) |
| 29 | (Gorjanc J. , Morrison, Blagus, & Mekjavic, 2018) |
| 30 | Harirchi, et al., 2005 |
| 31 | Ströhle, et al., 2018 |
| 32 | Endorf & Nygaard, 2021 |
| 33 | Ervasti, et al., 2004 |
| 34 | Endorf & Nygaard, 2021 |
| 35 | Endorf & Nygaard, 2022 |
| 36 | Endorf, et al, 2022 |
| 37 | Juopperi, et al., 2002 |
| 38 | Endorf & Nygaard, 2021 |
| 39 | Endorf, et al., 2022 |
| 40 | Edorf & Nygaard, 2021 |
| 41 | Endorf & Nygaard, 2022 |
| 42 | Ströhle, et al., 2018 |
| 43 | Endorf & Nygaard, 2022 |
| 44 | Harirchi, et al., 2005 |
| 45 | Harirchi, et al., 2005 |
| 46 | Endorf, et al., 2022 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



