Submitted:
18 August 2023
Posted:
22 August 2023
You are already at the latest version
Abstract
According to cancer death rates for women worldwide, this form of cancer ranks fourth after breast, bronchopulmonary, and colorectal cancer, affecting around 570,000 women annually. About 270,000 women each year pass away from this illness, 85% of them are from underdeveloped nations where cervical cancer claims more lives than any other kind of cancer. In Romania, cervical cancer ranks fourth in terms of death, behind breast, bronchopulmonary, and colorectal cancers, and second in terms of incidence, behind breast cancer. Endometriosis in the cervical region is quite uncommon. Only a tiny fraction of women had the condition upon diagnosis. It might be challenging to detect cervical endometriosis since it rarely manifests any symptoms or markers. Women who are asymptomatic can manage the condition expectantly; however, if the symptoms return often, surgery may be required. As many patients have concurrent diseases such fibroids, adenomyosis, ovarian cysts, and pelvic endometriosis, cervical endometriosis therapy appears to be straightforward. There ought to be surgical intervention. Symptomatic cervical endometriosis, such as irregular or post-coital bleeding, may be treated surgically using the LLETZ surgery or another cervical ablation approach. Background and Objectives: (1) To assess one's degree of knowledge on the signs, causes, and methods of preventing cervical cancer or cervical endometriosis, as well as screening for these conditions. (2) To ascertain how the responder behaves about cervical cancer screening and prevention, as well as endometriosis in the cervical region. Materials and Methods: A case report about cervical cancer or cervical endometriosis was conducted among a patient from Romania, Timisoara. Results: In this study, we report the patient with cervical endometriosis, although he was initially diagnosed with cervical cancer. Conclusions: Cervical cancer, a condition that can have serious repercussions on the patient's health, even if there is no clear picture of paraclinical investigations, to raise the suspicion of cervical endometriosis and not cervical cancer.
Keywords:
cervical cancer
; cervical endometriosis
; conization
; adenomyosis
; cervical malignancy
; infertility
; HPV
1. Introduction
Cervical endometriosis does not usually generate signs and symptoms, it can be difficult to diagnose [1,2]. Cervical endometriosis appears to be a diverse pathology. Asymptomatic cervical endometriosis may not necessitate therapy until it is identified by an abnormal screening. Patients should be recommended to take four weeks of progesterone or oral contraceptive pill treatment to postpone monthly flow for four weeks prior to any endometrial implantation of the cervix [3].
Endometriosis is described as the presence of endometrial glands and stroma out the uterine cavity. Although endometriosis is a prevalent condition, particularly among women of reproductive [4] age, cervical endometriosis is uncommon. A few case reports have been published since the 1950s, as it is an uncommon pathology with a small incidence rate varying between 0.11 and 2.4% [5]. Cervical endometriosis may be mistaken as a cervical cancer and discovered accidentally during a regular workup to screen out cervical malignant tumors [6]. The reported incidence is rising due to the increased use of cervical invasive procedures for the identification of cervical diseases, such as cervical biopsy and loop excision [7].
Around 10% (190 million) of women and adolescents in reproductive age suffer with endometriosis worldwide. It is an ongoing disease that causes excruciating, life-altering agony during periods, sexual activity, bowel and/or bladder movements, chronic pelvic discomfort, stomach bloating, nausea, exhaustion, and occasionally depression, anxiety, and infertility.
Endometriosis therapy often focuses on managing symptoms because there is presently no recognized cure for the disease. Although it is crucial, not everyone has access to early detection and efficient endometriosis treatment, especially in countries with middle and low incomes. Endometriosis is a disorder where tissue that resembles uterine lining develops outside of the uterus. It can make getting pregnant more difficult and result in severe pelvic discomfort. Endometriosis can develop during a person's first menstruation and persist beyond menopause. Endometriosis has no recognized cause. Endometriosis cannot be prevented in any known method. There is no cure, although medications or, in certain situations, surgery can be used to address the symptoms [8].
Deep penetrating cervical endometriosis involving the ureter mimicking cervical cancer, the need of include cervical endometriosis as a differential diagnosis in cases of period abnormalities, and its potential to produce severe problems [9]. Several hypotheses have been offered to explain the etiology of cervical endometriosis; however, no one explanation can explain all cases; hence, the interaction of coupled elements indicated by each postulated theory plays a part in the formation of cervical endometriosis [1].
Cervical endometriosis is classified as superficial, profound, or polypoid [9,10,11]. The presence of endometrial tissue on the anterior lip of the cervix, restricted to the cervix surface and not spreading beyond the squamous epithelium, is defined as primary cervical endometriosis. Secondary cervical endometriosis is more frequent than primary endometriosis and refers to disease extensions from the pelvis, most often the rectovaginal septum. After a standard cervical screening, superficial endometriosis is generally identified by fne-needle aspiration, colposcopy, and cervical biopsy, because endometrial cells discovered during a Pap smear may be incorrectly eliminated as atypical glandular cells. Pelvic discomfort, vaginal bleeding, are all symptoms of deep endometriosis [12,13].
It is a benign disease that is often asymptomatic but can occasionally show signs like intermenstrual spotting and post-coital bleeding. For superficial endometriosis, colposcopy, cervical biopsies, and Fine Needle Aspiration Cytology (FNAC) are crucial investigations since only a histopathological report can definitively diagnose the disease and guide future care. For profound endometriosis, surgical therapy is the best option to ease the patient's discomfort and lower the fatality. [9] It is quite uncommon for endometriosis in the cervical region to cause bleeding during pregnancy. It is highly uncommon for bleeding to occur during pregnancy due to cervical endometriosis. This case emphasizes the significance of a comprehensive pelvic examination in women who arrive with bleeding in the early stages of pregnancy and the need for a biopsy of any lesions, if possible and safe to do so. Cervical endometriosis with ongoing symptoms may make vaginal delivery impossible [14].
Height, shorter menstrual cycles, and early menarche are all linked to an increased risk of endometriosis, whereas parity, a higher body mass index (BMI), and smoking are linked to a lower risk. Endometriosis frequently manifests as infertility or persistent pelvic discomfort despite analgesic and cyclic oral contraceptive pill therapy. Endometriosis symptoms are treated with hormone therapy and analgesics for pain. However, because endometriosis frequently returns, the effectiveness of these therapies is limited [15].
The implantation and persistence of lesions deposited in the pelvic cavity may be influenced by other variables such as the hormonal, inflammatory, or immunologic context or as a result of Müllerian remnants that failed to correctly migrate or differentiate when a fetus was developing or as a result of circulating blood cells that differentiate into endometriosis. In addition, this tissue, in its invasion of the myometrium, frequently extends in the spaces occupied by the vessels and sinuses of the uterine wall but is separated from the lumen of the latter by the layer of endothelial tissue in a direct or primary endometriosis (so-called adenomyoma of mucosal origin).
Robert Meyer's discoveries on the extra-endothelial course of endometrial tissue around the uterine wall vessels in a direct endometriosis were verified, however it is thought that these are often venous veins rather than lymph vessels. Although it hasn't been able to conclusively establish it, it was thought that the endometrial tissue next to a vessel's endothelial lining may rupture during menstruation, allowing fragments of endometrial tissue to escape into the lumen of a blood vessel. Jacobson has demonstrated via his experimental work with rabbits and monkeys that small fragments of the uterine mucosa of these species become implanted on the peritoneum and result in peritoneal endometriosis that is identical to that occurring in humans [16,17,18,19,20,21,22,23].
Endometriosis manifests differently clinically in different female patients. Intermenstrual bleeding, painful periods (dysmenorrhea), painful sexual activity (dyspareunia), painful defecation, and painful urination (dysuria) are among the symptoms that patients frequently complain of [24]. Before menstruation even starts, there may be pelvic discomfort. Endometriosis frequently has no symptoms and is only discovered by a doctor while doing an infertility examination [15]. Endometriosis has been compared to a malignant tumor even though its histology normally shows it to be benign because the lesions enlarge, infiltrate, and connect to nearby tissues, interfering with physiologic functions. Similar to ectopic endometrium, ectopic endometriotic growths multiply and shed cells in response to cyclical fluctuations in estrogen. This recurrent ectopic activity causes internal bleeding, the development of scar tissue, inflammation, and even life-altering chronic pain [25,26]. The real incidence of endometriosis is unclear since laparoscopy is the only procedure that provides confirmation of the diagnosis, and an unidentified proportion of women are either asymptomatic or choose not to get treatment for their symptoms [27,28]. About 20% (within a range of 2% to 78%) of women receiving laparoscopic infertility investigations and 24% (within a range of 4% to 82%) of women undergoing laparoscopic investigations for pelvic discomfort have also been discovered to have endometriosis [29]. Women of reproductive age are affected by endometriosis; the average age of initial diagnosis is 28. There is no ethnic or socioeconomic tendency to the disorder, although among women with severe disease, there does seem to be a familial association [30,31].
Endometriosis is assumed to be the gynecologic outward sign of a systemic illness that encompasses a variety of medical conditions with underlying immunological or hormonal issues. Asthma, eczema, allergies, fibromyalgia, asthma, autoimmune inflammatory disease, chronic fatigue syndrome, and hypothyroidism are among the other symptoms that endometriosis patients frequently experience. Women who have endometriosis may develop autoimmune disorders such Hashimoto's thyroiditis, systemic lupus erythematosus (SLE), Sjogren's syndrome (SS), rheumatoid arthritis (RA), and multiple sclerosis (MS) if their immune surveillance is compromised. The endometriosis has an immunological component is supported by the early start of thyroid illness and rheumatoid arthritis, as well as the greater risk of autoimmune inflammatory disorders [32,33].
Due to their greater exposure to enhanced endogenous estrogen, women with endometriosis who are diagnosed after age 40 also have a higher chance of developing breast cancer [34,35]. Studies indicate that women with endometriosis may be more susceptible to some cancers, including breast cancer. A significant indicator of breast cancer risk is mammographic breast density (MBD). MBD and endometriosis had an opposite correlation. Additionally independent influencing variables for MBD were age and past progesterone [36] usage. This result demonstrates that the favorable link between endometriosis and breast cancer is not mediated by MBD [37].
The coelomic metaplasia theory asserts that endometriosis originates from the metaplasia of the multipotent coelomic epithelium since peritoneal and endometrial cells both stem from the same embryonic progenitor [38].
The "retrograde menstruation" idea is currently the most widely recognized explanation for most endometriosis types [39]. The anatomical distribution of endometriosis in the pelvis, where it is more common on the left side than the right, which is consistent with the anatomical differences between the right and left hemipelvis, and the distribution of peritoneal fluid in the abdomen, where it is more common on the right diaphragm than the left, further support the "retrograde menstruation" theory (Figure 1) [40,41,42]. Studies show that hormones play an important role into endometriosis detection [43].
The economic cost of endometriosis to society is significant. The chronic nature of endometriosis, the length of time between development of symptoms and diagnosis, expensive medical and surgical therapies, and indirect expenses related to diminished capacity to work are the causes of this burden. The morbidity, healthcare costs [44], and lost productivity related to endometriosis can be significantly decreased by raising awareness of the condition, speeding up diagnosis, and offering centralized, evidence-based specialized care [45].
2. Materials and Methods
A case report about cervical cancer or cervical endometriosis was conducted among a patient from Romania, Timisoara. The 45-year-old patient is diagnosed in June 2021 according to the Pap test with high-grade squamous intraepithelial lesion HSIL (Figure 2). According to the protocol, the investigation of colposcopy (Figure 3) with biopsy from the tumor formation, the result being the cervical neoplasm.
Conization is then performed. The result of the histopathological examination reveals cervical fragment, conization – cone with height of 12 mm – excision with the flange, seriated sections, fully processed material. Resection margins marked with green tusk.
Diagnosis: Chronic ulcer granulomatous cervicitis, condyspilomatous squamous epithelium that shows at the level of the squamous-cylindrical junction area the aspects of severe dysplasia CIN gr. III and carcinoma in situ with damage and package of endocervical glands (high grade intraepithelial squamous lesion), limited area of microinvasion- 1 mm in surface, 1 mm in depth. Microinvasive carcinoma diagnosed only microscopically, with no lymphovascular damage. Tangential resection edges to endocervical dysplastic epithelium.
Laboratory analyzes were performed and their values are within normal limits.
3. Results
This section provides the visualization, description of the experimental results and their interpretation.
Complementary is performed, in July, mammography examination – the result reveals: skin, subcutaneous tissue of normal appearance, radiopaque neomogenous structure, relatively dense. Multiple round-oval radiopaque masses with diameters up to about 8 mm, on the right and 11 mm on the left, with net or blurred contours. Normal appearance, and in conclusion: dense breasts, suckling appearance for firbrochistic mastosis ACR-BIRADS C/2. Posttherapeutic ultrasound control is recommended after 3 months.
In august 2021, the patient is doing computer Tomography (CT) abdomen and pelvis. It is observed: uterus with homogeneous structure and iodifixation. There is a spatial demarcation from the neighboring structures. No peri-aorto-cave celiomesenteric adenopathies in renal or inguinal-pelvic hiles. The rest of normal CT organs.
The IRM pelvis is performed.
Diagnosis of referral: uterine tumor with unpredictable evolution; cervical neoplasm biopsied; Positive CIII Pap test result.
Uterus in antero-flexion, with dimensions up to 73.5/46.4mm. Linear endometrium. Hypertrophied junctional area diffuse up to 15.2mm. Uterine endocol mildly native and postcontrast; Small uterine fibroids. Moderate angorging of parauterine venous plexuses. Fluid blade at the bottom of the Douglas bag. Right Bartholin gland cyst (max. 26/16.2mm). The bladder is free of volume, without parietal or endocavitary lesions. Rect, sigma is normal. No obvious intrapelvic lymphadenopathy. No secondary pathological changes in the pelvic belt bones.
Discharge diagnostics: Carcinoma in situ cervix, without specification.
Secondary diagnosis: The leiomyoma of the uterus, without specification. Functional disorders of neutrophil polynucleate. Spondylosis, unspecified, lumbo-sacral region. Other specified conditions of an intervertebral disc
The person advised to explain the results or examinations. Uterus tumor with unpredictable and unknown evolution.
An oncological consultation is performed that establishes the diagnosis of cervical neoplasm biopsied by conization.
Recommendations:
- Total hysterectomy with bilateral LSK adnexectomy
- Post-operative oncological reassessment
The patient is discharged with good general condition, afebrile, appetite, present intestinal transit, physiological myctions, soft mobile abdomen, painless, without vaginal bleeding.
Recommendations: Return for admission and surgery.
In September 2021, the surgery is performed, total hysterectomy with bilateral LSK adnexectomy, having favorable postoperative evolution. The result from the histopathological examination to paraffin is highlighted:
Macroscopy:
Total hysterectomy with bilateral LSK adnexectomy piece with total dimensions 7/6.5/4.5 cm, with partially smooth outer surface, tan, partially irregular appearance. The piece consists of:
- Cervical size 4.5/3.5/2 cm, with white brown exocervical mucosa, smooth, linear OCE.
At sectioning, endocervical canal lined by mucosa endocervical slightly falliduration, whitish-yellowish, with maximum thickness of 0.3 cm, without macroscopic obvious tumor formation.
- uterine body 5/6.5/4.5 cm. At sectioning, endometrial cavity lined with brown mucosa with brown areas, with a maximum thickness of 0.2 cm; the presence of intracavitary polypoid formation with dimensions of 1.3/0.5/0.1 cm, white-brown, with the implantation base in the isthmic area; white-brown myometer with a beam drawing.
- the right uterine appendix consists of the ovary with dimensions of 2.5/2.2/1.5 cm, with the external surface of the cuneal with a bosselated and the uterine tube with length of 5 cm. At sectioning, non-homogeneous, brown-black appearance, with a cystic with gelatinous, brown-hemorrhagic content; there are present yellow bodies. Paratubar identifies small cystic areas (1.8 cm in diameter).
At section of the ovary and section of the fallopian tube:
- the left uterine annex consists of the ovary with dimensions of 3/2.5/1 cm, with the external surface of the cuneal and 4.5 cm long fallopian tube. In the sectioning, a non-homogeneous appearance, brown-tan with multiple cystic areas with gelatinous-green content, the largest with a diameter of 0.9 cm.
At the section of the ovary and section of the fallopian tube:
Histopathological examination complete Hematoxylin-Eosin (HE) procedure:
The usual color is Hematoxylin-Eosin.
Cervical: Subacute non-specific cervical cervix with areas of endocervical mucosa ulceration, showing lesions of mature squamous metaplasia of the surface endocervical epithelium and sometimes glandular, cystic dilated glands and foci of tubo-endometriosis metaplasia of the epithelium of some glands; interstitial fibrosis, hyperemised vessels and hematic welding in the thickness of the endocervical wall; large caliber vessels at parameters with fibrous thickened walls and dystrophic calcifications.
Additional: Multifocal lesions of cervical endometriosis (glands + hemorrhagic cytogenic chorion) dislocated predominantly in the exocervical superficial chorion; slightly thickened and discreetly inflamed zonal squamous epithelium, with aspects of exocytosis and discrete epithelial atypia in the lower layers - more likely reactive, associating aspects of diffuse parakeratosis. No tumor aspects obviously on the sections examined.
Uterine body captured by the benign histological endometrium, in the proliferative phase; associated, hyperplastic endometrial polyp consisting of numerically enhanced glands arranged in a fibrous chorion, with proliferated blood vessels and interstitial hematic suffusions.
Diffuse leiomyoma thickened myometer with discreet nodular sketches, associating lesions of florid adenomyosis at the isthmic level.
Serous uterine without significant histological changes.
Conclusions:
- Cervical endometriosis associating non-specific subacute cervicitis lesions.
- Hyperplastic endometrial polyp; uterine adenomyosis.
- Bilateral functional ovarian cysts.
Postoperatively received treatment with Dipheriline 3.75 mg, one dose per month for 6 months (2021-2022).
In 2023 pelvic and abdominal MRI, total post-hysterectomy with bilateral LSK adnexectomy, without detectable adenopathies.
4. Discussion
Anatomically, the cervix is located in the lower part of the uterine cavity and is lined with two types of cells: glandular and squamous. The junction area of the two cell types is called the transformation area. This area is very important because most cervical cancers occur here. From the total case of neoplasms, histologically two major histological types of an epithelial tumor of the cervix are identified: squamous cell carcinoma (95%) and adenocarcinoma (5%). Rarely, the tumor can also derive from an unquamous variant: adenosine carcinoma, neuroendocrine carcinoma, carcinoma glass cells [58].
Anatomically, endometriosis is spread in several places in the pelvis: on the ovaries, uterus, fallopian tubes, uterosacral ligaments, wide ligaments, round ligaments, cul-de-sac or ovarian fossa, as well as on the appendix, large intestine, ureters, bladder or rectovaginal septum. In the reported case, our focus is on the endometriosis of the cervix [59].
Literatures published in English from 1980 to the present have been searched in the PubMed database using the keywords “cervical endometriosis”, or “cervical cancer”.
A total of 110,295 works related to cervical endometriosis or cervical cancer have been returned in search of the database.
Cervical cancer is the abnormal growth of cells in the lining of the cervix. Squamous cell carcinoma is the most frequent type of cervical cancer. [60] Cervical cancer incidence in the Romania is estimated to affect 3,380 (7.5%) women (Figure 4) in 2020, with 1,805deaths [61].
The pregnancy of cervical cancer remains high in many parts of the world, and in most countries the incidence and mortality of the disease remain much higher than the threshold set by the World Health Organization (WHO) initiative at elimination of cervical cancer [61].
In the early stages of cervical cancer, patients are largely asymptomatic, but few of those who are symptomatic, accuse lower abdominal pain, postcoital vaginal bleeding, abnormal menstrual bleeding, postmenopausal bleeding, vaginal discharge and disappearance [62].
One of the 13 genotypes of human papillomavirus (HPV) that are known to cause cancer, namely 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59 and 68, is the leading cause of almost all cervical malignant tumors in the world. Vaccination against HPV between the ages of 9 and 12 is likely to prevent more than 90% of cervical cancer and precancers. Cervical precancer, also known as high-grade squamous intraepithelial lesions of the cervix (HSIL), is detected and treated in women aged 21 to 65 years who have a cervix to avoid cervical cancer. In the absence of treatment, high-grade lesions can turn into cervical cancer [63].
The literature also shows an association of clear cervical cell carcinoma (CCC) and cervical endometriosis [64]. According to an epidemiological study to analyze the association between the two diseases, it was observed that the low risk of cervical cancer decreased in women with cervical endometriosis [65].
Cervical endometriosis is one of the rare types of endometrioses. In the literature, the prevalence is 0.7–2.4%, but no precise data are available for Romania [5,56,66,67].
In situations of cervical endometriosis, the results of cervical smear may be misleading. Cervical smears can be misinterpreted as high-grade squamous intraepithelial lesions, atypical glandular cells of undetermined meaning or adenocarcinoma in situ, especially in patients who have cervical endometriosis and have previously received cone for pre-invasive cervical lesions [11,68,69,70].
On pelvic examination, computed tomography and even macroscopic inspection at laparotomy, endometriosis can be misinterpreted for easy tumor extension, leading to inaccurate staging and wrong therapeutic choices. Frozen sections are advised to help intraoperative management whenever the diagnosis of endometriosis could be accepted, because clinical staging is often erroneous in patients with cervical cancer with a history of endometriosis. Pre-treatment surgical evaluation should also be considered [71,72].
Extending screening and vaccination programs can lead to reductions in the incidence and mortality of cervical cancer [61,73,74,75].
Cervical cancer ranks 4th in the most common types of cancer found in women globally. It was noted that the incidence is higher in low- and middle-income countries than high-income countries [75,76].
It is important to be aware that cervical endometriosis should be considered as a differential diagnosis in cases of menstrual abnormalities since it can have catastrophic consequences and is a rare instance of deep infiltrating cervical endometriosis affecting the ureter that mimics cervical cancer [9].
5. Conclusions
Our analysis study shows that the elimination of cervical cancer as a major health problem, and the HPV vaccine is a very feasible solution in low-income and lower-middle-income countries, proof being given by the registration of a low death rate in developed countries where this vaccine was made.
Furthermore, due to technological development, cervical cancer screening algorithms based on artificial intelligence (AI) could be developed that have the potential to become a key tool due to their ability to learn from data to identify patterns in new patients enrolled in rapid, efficient detection and high performance of cervical cancer.
Moreover, AI to support cervical cancer screening would be an extremely desirable solution, especially in the absence of medical infrastructure and staff trained to quickly identify potential risks and recommend personalized treatment depending on the pathology detected.
In this case report we could observe how easily it can be wrong to make a diagnosis, a condition that can have serious repercussions on the patient's health. But with the appearance of clinical symptoms, correlated with blood markers, even if there is no clear picture of paraclinical investigations, to raise the suspicion of cervical endometriosis.
In this way a clinical picture can be outlined for both cervical cancer and cervical endometriosis in order to reduce the likelihood of confusion of the two pathologies, and the rapid identification of the neoplasm in order to initiate an adequate treatment as soon as possible in order to diminish its effects and the degree of evolution.
Without any additional intervention, in order to combat cervical cancer, the death rate due to cervical cancer is expected to increase, similarly by the inability to put the correct diagonal of cervical endometriosis to lead to a decrease in the patient's quality of life.
Author Contributions
Conceptualization, Carolina Gobjila; methodology, Doru Anastasiu; software, Ion Petre; validation and formal analysis, Marina-Adriana Mercioni; investigation and resources, Zoran Popa; data curation, Marina-Adriana Mercioni; writing—original draft preparation and writing—review and editing, Izabella Petre.; visualization, Anca Bordianu; supervision, Simona Ioana Sipos. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sung, H., J. Ferlay, R.L. Siegel, M. Laversanne, I. Soerjomataram, A. Jemal, and F. Bray. 2021. "Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries." CA Cancer J. Clin. 71: 209–249. [CrossRef]
- Horne, A. W., & Missmer, S. A. 2022. "Pathophysiology, diagnosis, and management of endometriosis." BMJ (Clinical research ed.) 379, e070750. [CrossRef]
- Naqvi, A., MacKintosh, M. L., Derbyshire, A. E., Tsakiroglou, A. M., Walker, T. D. J., McVey, R. J., Bolton, J., Fergie, M., Bagley, S., Ashton, G., Pemberton, P. W., Syed, A. A., Ammori, B. J., Byers, R., & Crosbie, E. J. 2022. "The impact of obesity and bariatric surgery on the immune microenvironment of the endometrium." International journal of obesity (2005) 46(3): 605–612. [CrossRef]
- Wang S, Li XC, Lang JH. 2011. "Cervical endometriosis: clinical character and management experience in a 27-year span." Am J Obstet Gynecol. 205(5):452.e1-5. [CrossRef] [PubMed]
- Seval MM, Cavkaytar S, Atak Z, Guresci S. 2013. "Postcoital bleeding due to cervical endometriosis." BMJ Case Rep. [CrossRef]
- Felix Wu Shun Wong, Chi Eung Danforn Lim, Sonal Karia, Leonardo Santos. 2010. "Cervical endometriosis: Case series and review of literature." The Journal of Obstretics and Gynaecology Research Volume 36, Issue 4, https://doi.org/10.1111/j.1447-0756.2010.01209.x: 916-919. [CrossRef]
- Ata, B.; Ates, U.; Usta, T.; Attar, E. Cervical endometriosis, a case presenting with ıntractable spotting. " MedGenMed. 2005, 7, 64. [Google Scholar] [PubMed]
- Veiga-Ferreira MM, Leiman G, Dunbar F, Margolius KA. 1987. "Cervical endometriosis: facilitated diagnosis by fne needle aspiration cytologic testing." Am J Obstet Gynecol. 157: 849–856. [CrossRef]
- SM., Ismail. 1991 . "Cone biopsy causes cervical endometriosis and tuboendometrioid metaplasia. ." Histopathology. 18: 107–114. [CrossRef]
- Atalay Mert, S., Dilbaz, B., Ercan, E.E. et al. 2023. "A Rare Case of the Cervical Endometriosis and Overview of the Literature." Reprod. Sci. [CrossRef]
- Siddal RS, Mack HC. 1949. "Primary endometriosis of the vaginal portion of the cervix uteri." Am J Obstet Gynecol. 58: 765–769. [CrossRef]
- Swetha P, Nagashree U, Kondammal R. 2020. "A rare presentation of deep infiltrating cervical endometriosis mimicking cervical cancer." Int J Reprod Contracept Obstet Gynecol. 9: 3903–3905. [CrossRef]
- Félix A, Nogales FF, Arias-Stella J. 2010. "Polypoid endometriosis of the uterine cervix with Arias-Stella reaction in a patient taking phytoestrogens." Int J Gynecol Pathol. 29: 185–188. [CrossRef]
- Lundeen SJ, Horwitz CA, Larson CJ, Stanley MW. 2002. "Abnormal cervicovaginal smears due to endometriosis: a continuing problem." Diagn Cytopathol. 26: 35–40. [CrossRef]
- Nawras Zayat, Ariane M Chabanne, Ishola Adeyemo. Cervical endometriosis in pregnancy: A rare cause of bleeding in pregnancy. J Case Rep Images Obstet Gynecol 2023, 9, 75–78. [Google Scholar] [CrossRef]
- Organization, World Health. n.d. "Endometriosis." 2023. Available online: https://www.who.int/news-room/fact-sheets/detail/endometriosis (accessed on 2 August 2023).
- Parasar P, Ozcan P, Terry KL. 2017. "Endometriosis: Epidemiology, Diagnosis and Clinical Management." Curr Obstet Gynecol Rep. 6(1): 34-41. [CrossRef]
- Farland LV, Shah DK, Kvaskoff M, Zondervan K, Missmer SA. 2015. "Epidemiological and Clinical Risk Factors for Endometriosis." In: D’Hooghe T, editor. Biomarkers for Endometriosis. Springer Science.
- Anaf, V.; Simon, P.; El Nakadi, I.; Fayt, I.; Simonart, T.; Buxant, F.; et al. Hyperalgesia, nerve infiltration and nerve growth factor expression in deep adenomyotic nodules, peritoneal and ovarian endometriosis. Hum Reprod. 2002, 17, 1895–1900. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Tokushige, N.; Markham, R.; Fraser, I.S. Rich innervation of deep infiltrating endometriosis. Hum Reprod. 2009, 24, 827–834. [Google Scholar] [CrossRef]
- Berkley, K.J.; Rapkin, A.J.; Papka, R.E. The pains of endometriosis. Science 2005, 308, 1587–1589. [Google Scholar] [CrossRef]
- SE, Bulun. Endometriosis. N Engl J Med 2009, 360, 268–79. [Google Scholar] [CrossRef]
- JA, Sampson. Metastatic or embolic endometriosis due to menstrual dissemination of endometrial tissue into the venous circulation. Am J Pathol. 1927, 3, 93–109. [Google Scholar]
- Ferguson BR, Bennington JL, Haber SL. Histochemistry of mucosubstances and histology of mixed mullerian pelvic lymph node glandular inclusions: evidence for histogenesis by mullerian metaplasia of coelomic epithelium. Obstet Gynecol. 1969, 33, 617–625. [Google Scholar]
- Joi, A. SAMPSON, MD. 1927. "METASTATIC OR EMBOLIC ENDOMETRIOSIS, DUE TO THE MENSTRUAL DISSEMINATION OF ENDOMETRIAL TISSUE INTO THE VENOUS CIRCULATION." THE AMERICAN JOURNAL OF PATHOLOGY III, 2.
- Sinaii, N.; Plumb, K.; Cotton, L.; Lambert, A.; Kennedy, S.; Zondervan, K.; Stratton, P. Differences in characteristics among 1,000 women with endometriosis based on extent of disease. Fertil Steril. 2008, 89, 538–545. [Google Scholar] [CrossRef]
- Bloski T, Pierson R. 2008. "Endometriosis and Chronic Pelvic Pain: Unraveling the Mystery Behind this Complex Condition." Nurs Womens Health 12(5): 382-395. Nurs Womens Health. [CrossRef]
- Kitawaki, J.; Kado, N.; Ishihara, H.; Koshiba, H.; Kitaoka, Y.; Honjo, H. Endometriosis: The pathophysiology as an estrogen-dependent disease. Journal of Steroid Biochemistry and Molecular Biology 2002, 83, 149–155. [Google Scholar] [CrossRef]
- Signorello, L.B.; Harlow, B.L.; Cramer, D.W.; Spiegelman, D.; Hill, J.A. Epidemiologic determinants of endometriosis: A hospital-based case-control study. Annals of Epidemiology 1997, 7, 267–741. [Google Scholar] [CrossRef] [PubMed]
- C. , Wellbery. Diagnosis and treatment of endometriosis. American Family Physician. 1999, 60, 1753–1762. [Google Scholar]
- Schenken, R.S. Treatment of human infertility: The special case of endometriosis. Reproductive endocrinology, surgery, and technology 1996, 2, 2121–2140. [Google Scholar]
- Dos Reis, R.M.; Silva De Sa, M.F.; De Moura, M.D.; Nogueira, A.A.; Ribeiro, J.U.; Ramos, E.S.; et al. Familial risk among patients with endometriosis. Journal of Assisted Reproduction and Genetics 1999, 16, 500–503. [Google Scholar] [CrossRef] [PubMed]
- Moen, M.H.; Magnus, P. The familial risk of endometriosis. Acta Obstetricia et Gynecologica Scandinavica 1993, 72, 560–564. [Google Scholar] [CrossRef]
- Sinaii, N.; Cleary, S.D.; Ballweg, M.L.; Nieman, L.K.; Stratton, P. High rates of autoimmune and endocrine disorders, fibromyalgia, chronic fatigue syndrome and atopic diseases among women with endometriosis: A survey analysis. Human Reproduction 2002, 17, 2715–2724. [Google Scholar] [CrossRef]
- Bertelsen, L.; Mellemkjaer, L.; Frederiksen, K.; Kjaer, S.K.; Brinton, L.A.; Sakoda, L.C.; et al. Risk for breast cancer among women with endometriosis. International Journal of Cancer 2007, 22, 2693–2697. [Google Scholar] [CrossRef]
- Moini, A.; Salari, E.; Rashidi, H.; et al. Evaluation of the association of endometriosis and mammographic breast density, a cross-sectional study. BMC Women's Health 2022, 22, 81. [Google Scholar] [CrossRef]
- Mounsey, A.L.; Wilgus, A.; Slawson, D.C. Diagnosis and management of endometriosis. American Family Physician 2006, 74, 594–600. [Google Scholar]
- Laganà, A.S.; Garzon, S.; Götte, M.; Viganò, P.; Franchi, M.; Ghezzi, F.; Martin, D.C. The Pathogenesis of Endometriosis: Molecular and Cell Biology Insights. Int J Mol Sci. 2019, 20, 5615. [Google Scholar] [CrossRef]
- Vercellini P., Aimi G., De Giorgi O., Maddalena S., Carinelli S., Crosignani P.G. 1998. "Is cystic ovarian endometriosis an asymmetric disease?" Br. J. Obstet. Gynaecol. 105: 1018–1021. [CrossRef]
- ercellini P., Abbiati A., Vigano P., Somigliana E.D., Daguati R., Meroni F., Crosignani P.G. 2007. "Asymmetry in distribution of diaphragmatic endometriotic lesions: Evidence in favour of the menstrual reflux theory." Hum. Reprod. 22: 2359–2367. [CrossRef]
- Jenkins, S.; Olive, D.L.; Haney, A.F. Endometriosis: Pathogenetic implications of the anatomic distribution. Obstet. Gynecol. 1986, 67, 335–338. [Google Scholar] [PubMed]
- Winterhager, E. 2012. "Endometriosis: Science and Practice." Role of Steroid Hormones: Estrogen and Endometriosis; 140–144.
- Xin Gao, Jackie Outley, Marc Botteman, James Spalding, James A. Simon, Chris L. Pashos. 2006. "Economic burden of endometriosis." Fertility and Sterility 86 (6): 1561-1572. [CrossRef]
- Toniyan, K.A., E.Y. Gorbacheva, V.V. Boyarintsev, and I.V. Ogneva. 2023. "Endometriosis of the Cervix: A Rare Clinical Case with the Possibility of Comparing the Eutopic and Ectopic Endometrium at the Cellular Level." Int. J. Mol. Sci. 24. [CrossRef]
- Raluca Gabriela SUBA, Ion IONUT, Octavian ENCIU, Bogdan MARINESCU. 2019. "Cervical Endometriosis – Case Report and Review of Literature." Modern Medicine 26, No. 1.
- Junsik Park, Tae-Hee Kim, Hae-Hyeog Lee, Woo Seok Lee, Soo-Ho Chung, Sang-Mo Park. 2011. "Cervical Endometriosis in a Post-menopausal Woman: A Case Report." J Korean Soc Menopause 17, No. 3.
- Phadnis, S.V., Doshi, J.S., Ogunnaike, O. et al. 2005. "Cervical endometriosis: a diagnostic and management dilemma." Arch Gynecol Obstet 272: 289–293. [CrossRef]
- Naho Yokota, MD, MD Hiroshi Yoshida, MD Hideya Sakakibara, MD Yoshiaki Inayama, and MD Fumiki Hirahara. 2008. "A severe vaginal hemorrhage caused by cervical endometriosis." American Journal of Obstetrics & Gynecology. [CrossRef]
- Melin A, Sparen P, Bergqvist A. The risk of cancer and the role of parity among women with endometriosis. Hum Reprod 2007, 22, 3021–3026. [Google Scholar] [CrossRef]
- Brinton LA, Gridley G, Persson I, Baron J, Bergqvist A. Cancer risk after a hospital discharge diagnosis of endometriosis. Am J Obstet Gynecol 1997, 176, 572–579. [Google Scholar] [CrossRef] [PubMed]
- Mingdan Wang, Tongtong Xu, Yue Li, Chen Shi, Lili Jiang, Kuiran Liu. 2022. "Cervical Endometriosis Cyst Complicated with HPV Infection and CIN I:A Case and Review of Literature.
- Priyanka Bagdi*, and Nithya R. 2021. "Cervical Endometriosis: A Case Report." Research Journal of Pharmaceutical, Biological and Chemical Sciences 12 (2).
- J. W. KWEK, M. W. C. H’NG*, S. H. CHEW and E. H. TAY. 2010. "Florid polypoid endometriosis of the cervix with left uretericobstruction: a mimic of cervical malignancy." Ultrasound Obstet Gynecol 36: 252 – 254. [CrossRef]
- Aleksandra Pečovnik, Simona Šramek Zatler, Uršula Salobir Gajšek, Alenka Repše Fokter. 2021. "Cervical endometriosis – a case report and review of literature ." Slovenian Slovenian Medical Medical JournaJourna l l 91(1–2) : 57–60. [CrossRef]
- Bava SV, Thulasidasan AK, Sreekanth CN, Anto RJ. 2016. "Cervical cancer: a comprehensive approach towards extermination. ." Ann Med. 48: 149-161. [CrossRef]
- Cirstoiu, M.; Munteanu, O. Strategies of preventing ureteral iatrogenic injuries in Obstetrics-Gynecology. " Journal of Medicine and Life 2012, 5, 277–279. [Google Scholar] [PubMed]
- Canfell K, Kim JJ, Brisson M, Keane A, Simms KT, Caruana M, Burger EA, Martin D, Nguyen DTN, Bénard É, Sy S, Regan C, Drolet M, Gingras G, Laprise JF, Torode J, Smith MA, Fidarova E, Trapani D, Bray F, Ilbawi A, Broutet N, Hutubessy R. 2020. "Mortality impact of achieving WHO cervical cancer elimination targets: a comparative modelling analysis in 78 low-income and lower-middle-income countries." Lancet 395(10224): 591-603. [CrossRef]
- Deependra Singh, Jerome Vignat, Valentina Lorenzoni, Marzieh Eslahi, Ophira Ginsburg, Beatrice Lauby-Secretan, Marc Arbyn, Partha Basu, Freddie Bray, Salvatore Vaccarella. 2023. "Global estimates of incidence and mortality of cervical cancer in 2020: a baseline analysis of the WHO Global Cervical Cancer Elimination Initiative." The Lancent Global Health 11.
- Buskwofie A, David-West G, Clare CA. 2020. "A Review of Cervical Cancer: Incidence and Disparities." J Natl Med Assoc. 112(2): 229-232. [CrossRef] [PubMed]
- Vu M, Yu J, Awolude OA, Chuang L. 2018. "Cervical cancer worldwide." Curr Probl Cancer 42(5): 457-465. [CrossRef]
- Tsikouras, P.; Zervoudis, S.; Manav, B.; Tomara, E.; Iatrakis, G.; Romanidis, C.; Bothou, A.; Galazios, G. Cervical cancer: screening, diagnosis and staging. J BUON. 2016, 21, 320–325. [Google Scholar] [PubMed]
- Chiorean, DM, MI Mitranovici, MC Muresan, CF Buicu, R Moraru, L Moraru, TC Cotoi, et al. 2023. "The Approach of Artificial Intelligence in Neuroendocrine Carcinomas of the Breast: A Next Step towards Precision Pathology?-A Case Report and Review of the Literature." Medicina 59: 672. [CrossRef]
- Melinda-Ildiko Mitranovici, Diana Maria Chiorean, Sabin Gligore Turdean, Maria Cezara Muresan, Corneliu-Florin Buicu, Raluca Moraru, Liviu Moraru, Titiana Cornelia Cotoi, Havva Serap Toru, Adrian Apostol, Claudiu Marginean, Ion Petre, Ioan Emilian Oala, V. 2023. "A Rare Case of Malignant Ovarian Germ Cell Tumor: Dysgerminoma and Seminoma in the Same Patient." Reports 6, (14). [CrossRef]
- Ion Petre, Flavia Barna, Daniela Gurgus, Laurentiu Cezar Tomescu, Adrian Apostol, Izabella Petre, Cristian Furau, Miruna Lucia Năchescu, Anca Bordianu. 2023. "Analysis of the Healthcare System in Romania: A Brief Review." Healthcare 11(14), 2069. [CrossRef]
- MI, Mitranovici, Chiorean DM, Muresan MC, Buicu CF, Moraru R, Moraru L, Cotoi TC, et al. 2022. "Diagnosis and Management of Dysgerminomas with a Brief Summary of Primitive Germ Cell Tumors." Diagnostics 12, 3105. [CrossRef]
- MI Mitranovici, DM Chiorean, AH Sabău, IG Cocuz, AC Tinca, MC Mărginean, MC Popelea, T Irimia, R Moraru, C Mărginean, ML Craina, Izabella Petre, Elena Silvia Bernad, Ion Petre, Ovidiu Simion Cotoi. 2022. "An Interesting Image of Transmural Migration of a Levonorgestrel-Releasing Intrauterine Device (LNg-IUD)." Diagnostics 12(9), 2227. [CrossRef]
- odrin Dan Nicolae Ilea, Lucia Georgeta Daina, Simona Bungau, Delia Mirela Tit, Diana Uivarosan , Lavinia Moleriu, Ion Petre, Constantin Bungau, Izabella Petre. 2020. "Sustainable Management, Instable Legislation Regarding Wages, and Employee Satisfaction/Motivation in Two Romanian Hospitals." Sustainability 12(3), 909. [CrossRef]
- Perkins RB, Wentzensen N, Guido RS, Schiffman M. 2023. "Cervical Cancer Screening: A Review." JAMA 330(6): 547-558. [CrossRef]
- Marwah N, Garg M, Singh S, Sethi D, Sen RJIJOA. 2012. "Research BM Unusual form of squamous cell carcinoma of the cervix extending in situ into the endometrium: three case reports and review of literature." International Journal of Applied and Basic Medical Research 2: 139–141. [CrossRef]
- Hashiguchi M, Kai K, Nishiyama S, Nakao Y, Yokoyama M, Aishima S. 2018. "Clear cell carcinoma of the uterine cervix presented as a submucosal tumor arising in a background of cervical endometriosis." International Journal of Gynecological Pathology 37: 88–92. [CrossRef]
- Saavalainen L, Lassus H, But A, Tiitinen A, Härkki P, Gissler M, Pukkala E, Heikinheimo O. 2018. "Risk of gynecologic cancer according to the type of endometriosis." Obstetrics & Gynecology 131: 1095–1102. [CrossRef]
- Symonds, D.A.; Reed, T.P.; Didolkar, S.M.; Graham, R.R. AGUS in cervical endometriosis. J Reprod Med. 1997, 42, 39–43. [Google Scholar]
- Szyfelbein, W.M.; Baker, P.M.; Bell, D.A. Superficial endometriosis of the cervix: a source of abnormal glandular cells on cervicovaginal smears. Diagn Cytopathol. 2004, 30, 88–91. [Google Scholar] [CrossRef]
- Hanau, C.A.; Begley, N.; Bibbo, M. Cervical endometriosis: a potential pitfall in the evaluation of glandular cells in cervical smears. Diagn Cytopathol. 1997, 16, 274–280. [Google Scholar] [CrossRef]
- Walker, J.L.; Manetta, A.; Mannel, R.S.; Berman, M.L.; DiSaia, P.J. The influence of endometriosis on the staging of cervical cancer. Obstet Gynecol. 1990, 75, 543–545. [Google Scholar]
- Jörg B. Engel, Stefan Heuer, Sabine Segerer, Stephan Rauthe, Johannes Dietl, Arnd Hönig. 2011. "Cervical endometriosis associated with malignant pleural mesothelioma mimicking cervical cancer—Occam’s razor or the “third man”." Fertility and Sterility Volume 95. [CrossRef]
Figure 1.
Causes and impact of cervical endometriosis according to World Health Organization (WHO).
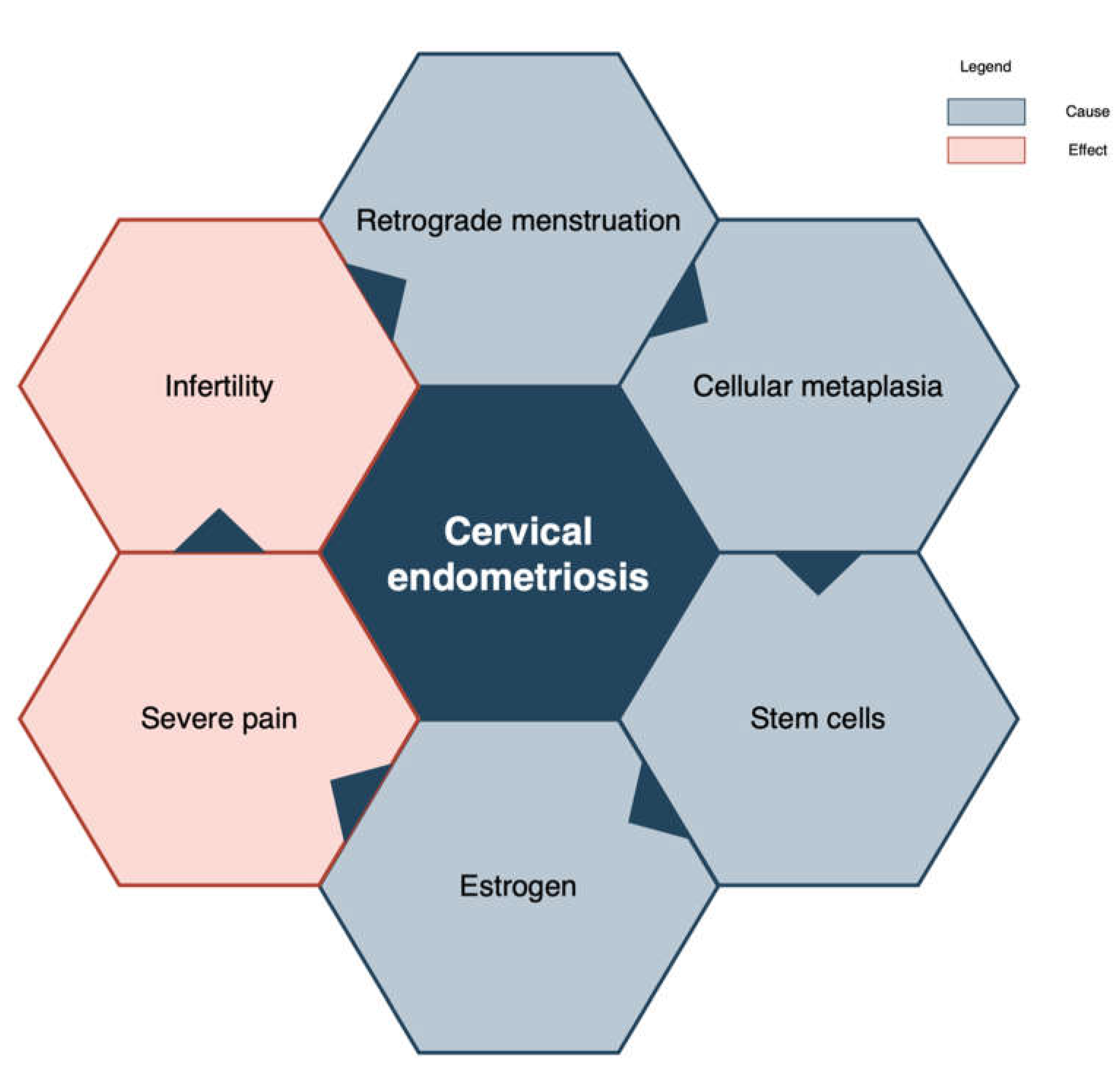
Figure 2.
Case report.
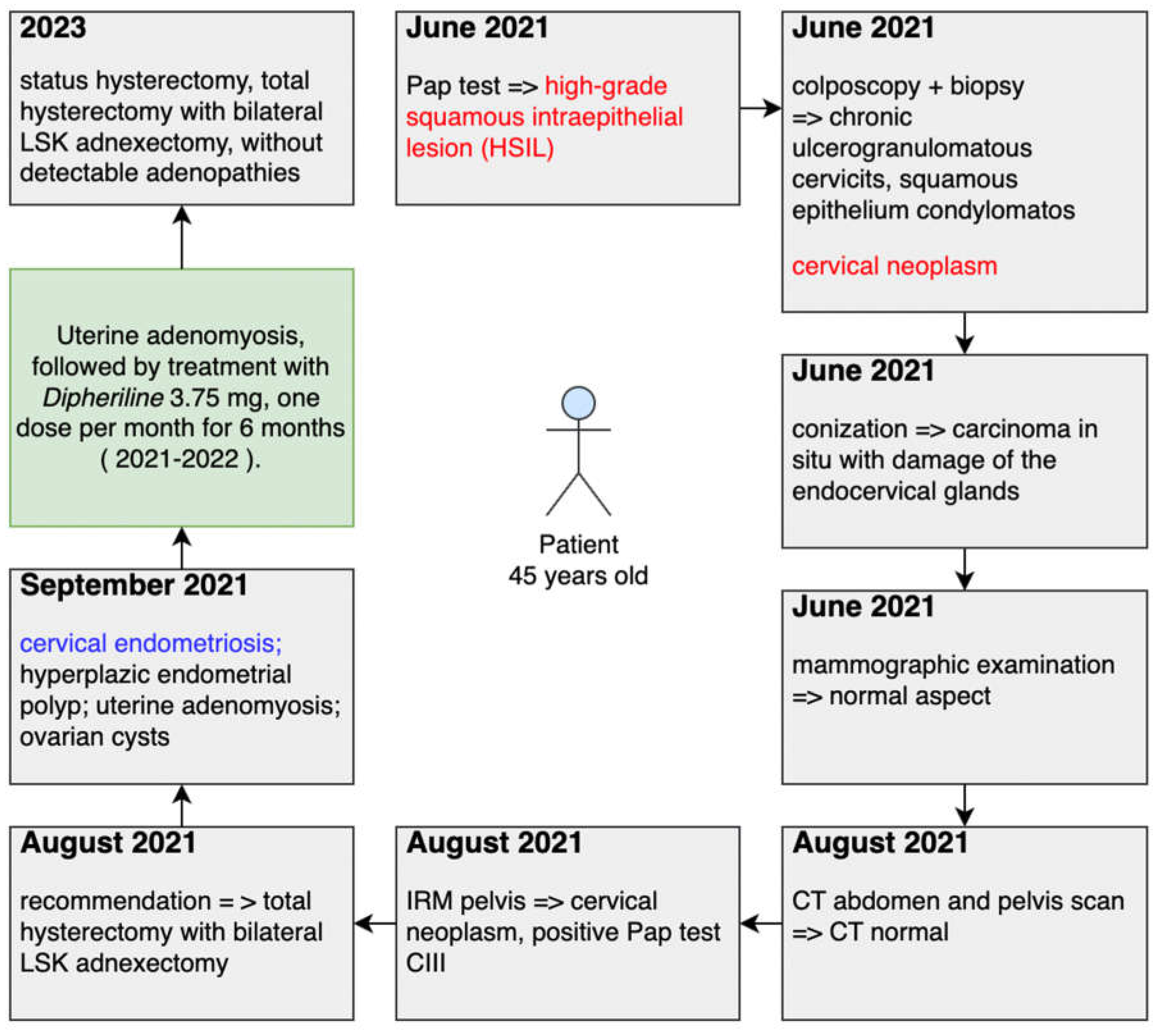
Figure 3.
Colposcopy aspects of the post cervix badijoning with solution (a) Lugol and (b) acid acetic.
Figure 3.
Colposcopy aspects of the post cervix badijoning with solution (a) Lugol and (b) acid acetic.
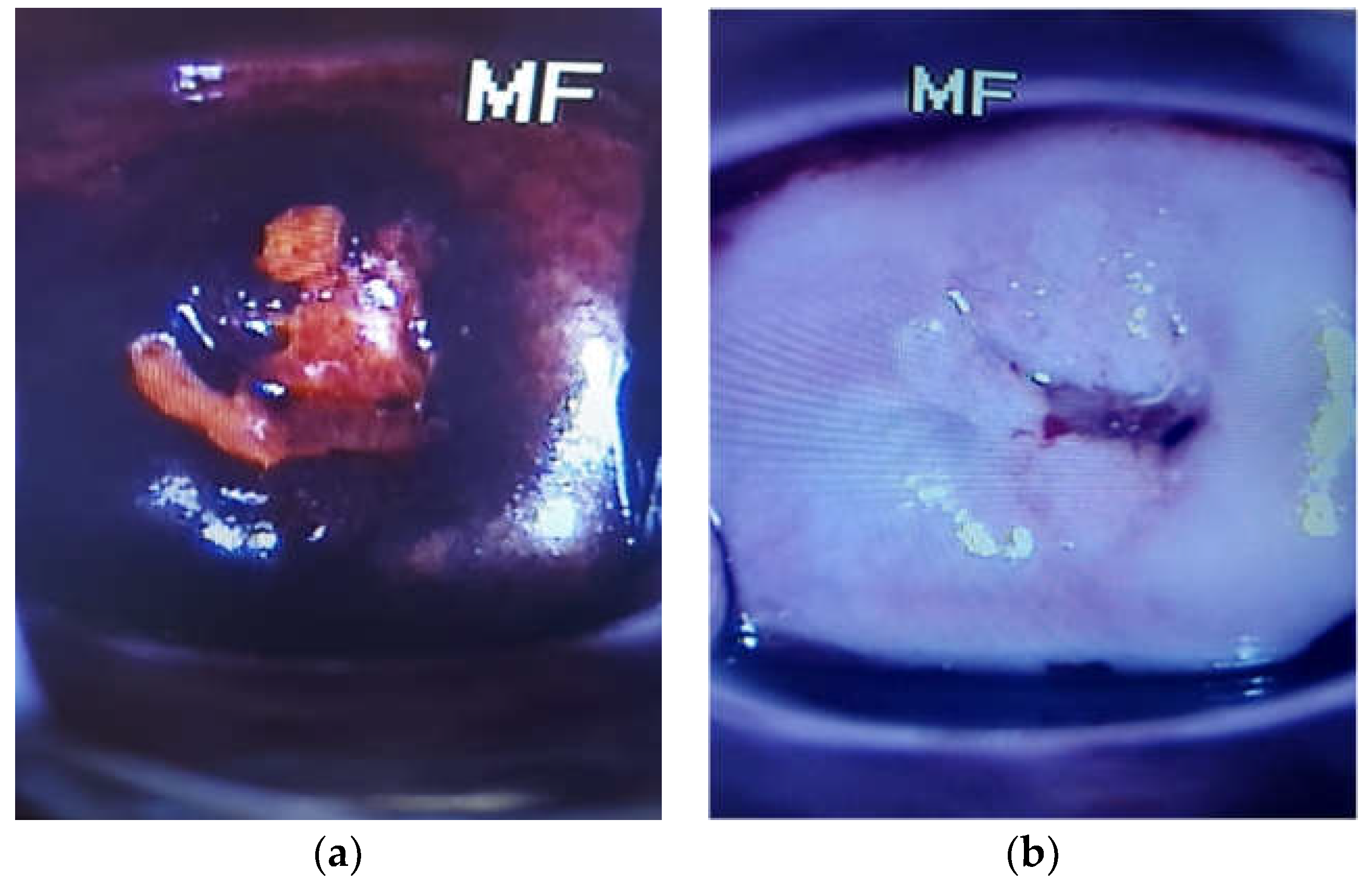
Figure 4.
Number of new cases in 2020, females, all ages in Romania, Globocan 2020 [61].
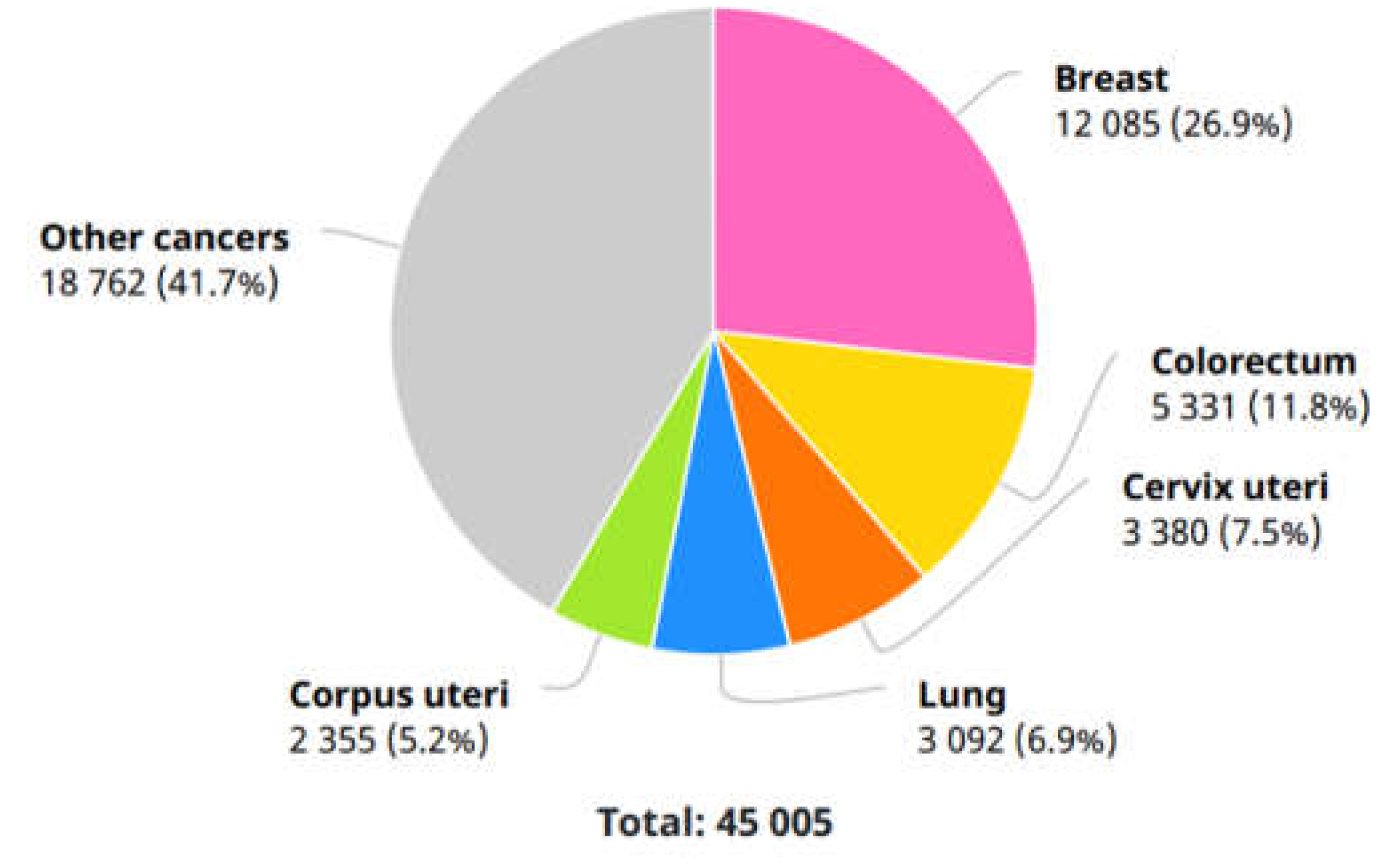

Table 1.
Descriptive characteristics of the participants with cervical endometriosis.
|
Study Ref. |
Total patients |
Age |
Additional information |
Gynecological anamnesis |
Total Pregnancy |
Pregnancy Delivery |
Diagnosis | Treatment |
| [13] 2023* | 1 | 38 | pelvic pain and menstrual irregularity, with endometrioma and adenomyosis, confirmed by histopathological evaluation of the specimen; a hearing impairment; divorce |
an enlarged and fixed cervix, and the gynecological examination was extremely painful for the patient. Pap smear normal Transvaginal ultrasonography |
NS | NS | anechoic cyst in the left adnexal area endocervical curettage the surgical specimens of endometrial sampling and endocervical curettage were found to be secretory endometrium. The presence of focal adenomyosis and 3 leiomyomas that were<2 cm using magnetic resonance imaging (MRI) A lobulated cyst in the left ovary hysteroscopy and cervical biopsy - Hysteroscopic biopsies as proliferative endometrium - cervical punch biopsy => cervical endometriosis pelvic infection endometriotic cyst and nonspecific salpingitis hypertensive very low chance of achieving pregnancy. Requested definitive surgery, including the removal of the right ovary and the uterus. a uterus with adenomyosis and cervical endometriosis |
2 mg/ day of dienogest (Visanne, Bayer Germany). antibiotics for pelvic infection treatment for hypertensive |
| [46], 2023 | 1 | 46 | stable clinical condition with no clinical, microbiological or laboratory evidence of infection, encephalopathy, renal failure, comorbidities including heart failure or pulmonary disease, malignancy, diabetes mellitus | the duration of the menstrual cycle—28 days, regularly, the duration of menstruation—4–5 days, average, painful | 1 | operative delivery (caesarean section) |
First: an endometrial polyp | |
| [50] 2022 | 1 | 27 | vaginal bleeding for 3 months | NS | NS | positive for HPV31, 53, and 56 and complicated with CIN I the rotten flesh-like tissue in the cervical posterior lip tumor was found during surgery |
GnRH | |
| [51] 2021 | 1 | 32 | extracyclic and contact bleeding and cervical erythroplakia regularly participated in the screening program for early detection of cervical cancer (ZORA) |
NS | NS | high-grade squamous intraepithelial lesion (HSIL; CIN3); endometriosis in the cervical transition zone |
||
| [53] 2019 | 1 | 24 | no history of cervical interventions; no family history of endometriosis |
nulliparous and suffered dysmenorrhea 7-VAS, chronic pelvic pain 3-VAS, without dyspareunia | First: cervical dysplasia primary infertility. Final: cervical endometriosis and vaginal endometriotic nodule |
laparoscopic surgery |
||
| [54] 2011 | 1 | 54 | post-menopause; menopause state three years ago without hormone therapy; Pap smear showed reactive cellular changes with inflammation and human papillomavirus (HPV) deoxyribonucleic acid (DNA) Chip test was negative; generally well, weighed 74.9 kg and not pale; underwent laparoscopy assisted vaginal hysterectomy on June 14, 2011 |
2 | full term vaginal deliveries | First: huge myoma uteri Final: Microscopically, both endometrial glands and stroma present at the cervical stroma. Pathologic findings indicate that there was endometriosis at cervix, atrophy at endometrium, and leiomyoma at myometrium |
||
| [55] 2010 | 1 | 48 | nulliparous Chinese woman subtotal hysterectomy and left salpingo-oophorectomy for uterine adenomyosis and left ovarian endometriotic cyst | heavy vaginal bleeding | 4.0-cm heterogeneous cervical mass with internal vascularity and irregular polypoid extension into the left parametrium and causing left hydroureter, suspicious for cervical tumor; an enlarged cervical stump was found with a polypoid mass in the cervical canal; polypoid lesion with histological features of polypoid endometriosis |
|||
| [56] 2008 | 1 | 37 | regular menstrual periods and heavy dysmenorrhea | 0 | regular menstrual periods and heavy dysmenorrhea regular menstrual periods and heavy dysmenorrhea | |||
|
[57] 2005 |
1 | 49 | Pelvic Pain, Intermenstrual bleeding | 2 | Laparoscopy: Endometriosis on the right utero-sacral ligament | Past: LLETZ(large loop excision of the transformation zone) | ||
| 1 | 51 | Citology: Persistent Borderline smears | Pelvic Pain, Postcoital Bleeding | 3 | Laparoscopy: Normal | Past: Nil | ||
| 1 | 43 | Pelvic Pain, Postcoital Bleeding | 3 | Laparoscopy: Endometriosis in the pouch of douglas | Past: LLETZ;Previous cervical cautery | |||
| 1 | 46 | Mild tomoderatedyskaryosis | Intermenstrual Bleeding,Post-coital Bleeding | 2 | Laparoscopy: Endometriosis on both utero-sacral ligaments | Past: LLETZ;Previous Cervical Cryocautery | ||
| 1 | 36 | Persistent borderline smears | Intermenstrual Bleeding | 3 | Laparoscopy: Normal | Past: LLETZ |
* NS – not specified.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



