Submitted:
15 August 2023
Posted:
18 August 2023
You are already at the latest version
Abstract
Diffuse cavernous hemangioma of the rectum (DCHR) is a rare benign lesion of vascular malformation. According to previous studies, the most reported major symptoms of DCHR are recurrent painless rectal bleeding or iron deficiency anemia[1][2][3][4][5][6]. We present a case of an 8Y11M boy who was diagnosed with DCHR by MRI. The patient underwent Laparoscopic-assisted transanal distal sigmoidectomy and sigmoido-anal anastomosis(Laparoscopic Swenson Procedure), and recovered well. After the operation, the child had short-term fecal incontinence and loose stools, which returned to normal after half a year. Regardless of age and symptoms, early and correct diagnosis and treatment of DCHR and postoperative restoration of normal anal function are necessary. Laparoscopic Swenson procedure may be a good option for the treatment of DCHR.
Keywords:
diffuse cavernous hemangioma
; rectum
; Laparoscopic Swenson
; children
1. INTRODUCTION
Diffuse cavernous hemangioma of the rectum (DCHR) is relatively rare,the most common symptoms are recurrent painless rectal bleeding or iron-deficiency anemia,some patients were misdiagnosed as internal hemorrhoids or treated as ulcerative colitis or Crohn’s disease [7,8]. Current diagnostic modalities are abdominal X-ray, CT, MRI, endoscopic ultrasonography, and colonoscopy, all of which have their own advantages. Compared with the high recurrence rate of palliative care, surgical treatment is the first choice [9,10]. Laparoscopic Swenson Procedure has been used to treat Hirschsprung’s disease and its related diseases. However, this approach has not been evaluated in the treatment of patients with DCHR.
2. CASE PRESENTATION
This case reports a boy aged 8 years and 11 months who first presented with recurrent painless rectal bleeding 7 years ago. In early childhood, bleeding symptoms were thought to be due to anal floss, and three colonoscopies performed 2 years earlier in the gastroenterology department showed no significant abnormal lesions in the rectum. The patient was admitted to our hospital with recurrent hematochezia. He had no significant medical or family history.
His laboratory tests revealed a hemoglobin level of 10.2 g/dL. Three colonoscopies showed no apparent abnormal lesions. Abdominal MRI revealed the possibility of vascular malformations in the rectum wall and around the rectum (Figure 1).
The patient was diagnosed with DCHR and underwent laparoscopic-assisted transanal distal rectosigmoid resection and sigmoidal-anal anastomosis (Laparoscopic Swenson Procedure).
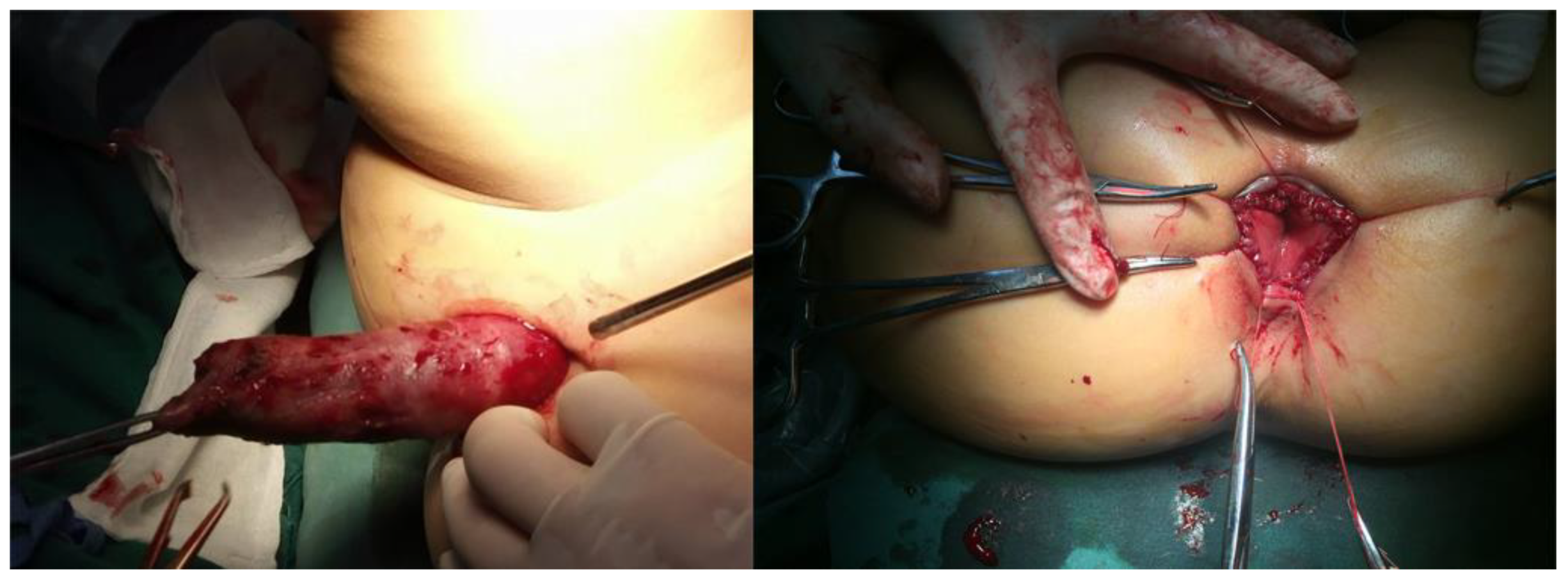
Specific surgical procedures: A Trocar with a diameter of 10mm was placed at the umbilical margin, pneumoperitoneum was established by pneumoperitoneum needle puncture (12mmHg), the main vision lens was inserted, and a Trocar with a diameter of 5mm was placed in the right lower abdomen and the right upper abdomen. Exploration revealed a diffuse distribution of intestinal wall hemangioma in the distal rectum and sigmoid colon, with prominent anterior wall, and a distribution of vascular malformations in the pelvic soft tissues (Figure 2). The distal mesentery of sigmoid colon and mesorectum were removed and separated to the pelvic floor under the premise of retaining the corresponding vascular arch with forceps and ultrasonic scalpel respectively. After changing to lithotomy position. The colon was pulled out of the anus with a tissue clamp over the peritoneal reflex. The bowel was cut open in a circular way, and about 15cm of the bowel was pulled out. The edge of the rectum to the dentate line was resected, 1.5cm of the anterior wall and 0.5cm of the posterior wall of the rectum were retained, and the sigmoid colon was cut in the reverse oblique, and then the end-to-end heart-shaped anastomosis was performed with the rectum. After examination for no active bleeding, anastomotic stenosis and leakage, an anal canal was placed (Figure 3).
The operation time was 170 minutes, blood loss was 20ml, intraoperative blood transfusion was not required, and the patient recovered well after the operation. The gastric tube was removed on the 3rd postoperative day, and oral administration was started on the 5th postoperative day. The anal canal was removed on the 8th postoperative day and the patient was discharged on the 14th postoperative day. The patient was followed up for 1 week /1 month /3 months /6 months /13 months /24 months and no obvious signs of recurrence were found by ultrasound. After the operation, the child had short-term fecal incontinence and loose stools, which returned to normal after half a year.
3. DISCUSSION
DCHR is a rare benign vascular lesion. It originates from the submucosal blood vessels and is caused by the abnormal development of embryonic mesodermal tissue, accounting for 80% of rectal hemangiomas [11]. Since the first case of rectal hemangioma was reported by Phillips in 1839, about 350 cases have been reported worldwide [5]. It is more common in children and young adults, and the male to female ratio is generally 2:1 [12]. According to previous studies, the most commonly reported main symptoms of DCHR are recurrent painless rectal bleeding or iron deficiency anemia [1,2,3,4,5,6], Some patients are misdiagnosed with internal hemorrhoids or treated for ulcerative colitis and Crohn’s disease [7,8], Of course, there are other symptoms including lower abdominal pain, low bowel obstruction and constipation.
The clinical manifestations of DCHR are non-specific symptoms. However, auxiliary examinations have their own characteristics.In the abdominal X-ray findings, closely packed venules were seen in some cases [13]. With the development of colonoscopy, CT, rectal ultrasound, and MRI, abdominal radiography has been replaced by them. Colonoscopy is an important examination to visually observe rectal hemangioma and its lesion length. The typical findings on colonoscopy are congestion and swelling of the rectal mucosa, with soft, distorted, enlarged blue-red or dark-red submucosal vascular lesions [14,15]. CT is another important examination for the diagnosis of rectal hemangioma. Typical CT findings are thickening of the rectal wall, serpentine enlargement of blood vessels around the rectum, and sometimes multiple calcifications in the pelvic region [16]. MRI is superior to CT because of its ability to produce high-resolution and multidimensional soft tissue images [16]. Therefore, it can provide accurate information on the exact size of the rectal hemangioma, the involvement of the sphincter, and the involvement of adjacent structures.
At present, the treatment of DCHR is generally divided into palliative treatment and surgical treatment. The common palliative treatment is low-dose radiation therapy, cryotherapy, vascular ligation therapy, sclerotherapy, and interventional angiography occlusion [5,6,16,17]. Palliative treatment can reduce the amount and frequency of rectal bleeding, but it is prone to recurrence. Therefore, non-surgical treatment of rectal hemangioma is not recommended [9,10].
Surgical treatment is the first option for DCHR. Among them, endoscopic surgery is widely recommended because of its short operation time and small surgical injury. The selection of endoscopic surgery is also controversial. It is thought that the main advantage of EFTR (endoscopic full-thickness resection), as compared with endoscopic mucosal resection and ESD (endoscopic submucosal dissection), is the lower risk of residual or recurrent hemangioma because hemangiomas sometimes invade into or completely exceed the muscular layer. EFTR (endoscopic full-thickness resection) may be a better treatment option for colorectal cavernous hemangioma involving the muscularis propria layer [4,18,19]. However, the scope of endoscopic surgery is small, and it may not be able to do anything for DCHR cases that spread to the pelvis.
Therefore, the disadvantages of traditional surgery are undoubtedly obvious. Among the traditional surgical options, compared with TME (total mesorectal excision), it is difficult to completely remove the distal rectal lesions, TaTME (transanal total mesorectal excision) can directly remove the lesions deep to the dentate line, which has more advantages [1,20].
So far, there are few reports about laparoscopic surgery as a further improvement of traditional surgery. Leal et al. reported 2 cases of laparoscopy-assisted bowel resection for DCHR, after which the children returned to normal without abnormal defecation and bloody stools [2]. Fujii et al. introduced robot-assisted surgery and suggested that robotic surgery has certain advantages over laparoscopic surgery, including three-dimensional imaging, no vibration, dexterity in motion scaling, and minimal bleeding. But robotic surgery requires a longer operation time [21].
In this case, due to the child’s young age and small operable space at pelvic floor and anus, laparoscopic surgery was innovatively combined with TaTME, and Laparoscopic Swenson’s operation in Hirschsprung’s disease surgery was used for reference. This is the first report on the treatment of DCHR by laparoscopic-assisted transanal distal sigmoidorectal resection and sigmoidoanal canal anastomosis.
The amount of bleeding during the operation was less and the patient recovered satisfactorily. Although the defecation function was abnormal in a short time after operation, the long-term defecation function was good. Based on the susceptibility age of DCHR, this result is acceptable. This experience suggests that the Laparoscopic Swenson procedure may be a new option for the treatment of DCHR, especially in children.
References
- Wang, H.T. et al. (2010). Diagnosis and treatment of diffuse cavernous hemangioma of the rectum: Report of 17 cases. World Journal of Surgery. [CrossRef]
- Leal, R.F. et al. (2011). Laparoscopic-assisted bowel resection with construction of a colonic reservoir for cavernous hemangioma of the rectum: Report of two cases. Techniques in Coloproctology. [CrossRef]
- Sood, R. et al. (2013). Chronic haematochezia caused by diffuse cavernous haemangioma of the rectum. Journal of Gastrointestinal and Liver Diseases.
- Andrade, P. et al. (2015). Diffuse cavernous hemangioma of the rectum: case report and literature review. International Journal of Colorectal Disease. [CrossRef]
- Kimura, S. et al. (2007). Cavernous hemangioma in the ascending colon treated by endoscopic mucosal resection. Journal of Gastroenterology and Hepatology (Australia). [CrossRef]
- Fujikawa, H. et al. (2014). Sphincter-saving resection of rectal hemangioma based on Doppler transrectal ultrasonography findings: report of a case. International surgery. [CrossRef]
- Amarapurkar, D.N. et al. (1998). Cavernous hemangiomas of the rectum: Report of three cases. American Journal of Gastroenterology. [CrossRef]
- Wang, H.T. et al. (2005). Diffuse cavernous hemangioma of the rectosigmoid colon. Techniques in Coloproctology. [CrossRef]
- Yang, G.Z. et al. (2013). Giant mesenteric hemangioma of cavernous and venous mixed type: A rare case report. BMC Surgery. [CrossRef]
- Amati, A.L. et al. (2014). A hemangioma of the sigmoid colon mesentery presenting as a retroperitonealtumor: A case report and review. World Journal of Surgical Oncology. [CrossRef]
- Lyon, D.T. and Mantia, A.G. (1984). Large-bowel hemangiomas. Diseases of the Colon & Rectum. [CrossRef]
- Cunningham, J.A. et al. (1989). Diffuse cavernous rectal hemangioma-Sphincter-sparing approach to therapy - Report of a case. Diseases of the Colon & Rectum. [CrossRef]
- Dachman, H.; et al. Colorectal Hemangloma : Radlologic Findings. Pathology 1987. [Google Scholar]
- Wang, A.Y. and Ahmad, N.A. (2007). Diffuse Cavernous Hemangioma of the Colon and Rectum. Clinical Gastroenterology and Hepatology. [CrossRef]
- Londono-Schimmer, E.E. et al. (1994). Coloanal sleeve anastomosis in the treatment of diffuse cavernous haemangioma of the rectum: Long-term results. British Journal of Surgery. [CrossRef]
- Hervías, D. et al. (2004). Diffuse cavernous hemangioma of the rectum: an atypical cause of rectal bleeding. Revista Española de Enfermedades Digestivas. [CrossRef]
- Gottlieb, K.; et al. Massive hemorrhage in pregnancy caused by a diffuse cavernous hemangioma of the rectum - EUS as imaging modality of choice. MedGenMed Medscape General Medicine 2008. [Google Scholar]
- Chen, K. et al. (2019). Successful endoscopic submucosal dissection of a large cavernous hemangioma in the colon. Endoscopy. [CrossRef]
- Liu, W. et al. (2023). Successful resection of a cavernous hemangioma involving the rectal muscularis propria layer by endoscopic full-thickness resection. Endoscopy. [CrossRef]
- Deijen, C.L. et al. (2016). COLOR III: a multicentre randomised clinical trial comparing transanal TME versus laparoscopic TME for mid and low rectal cancer. Surgical Endoscopy. [CrossRef]
- Fujii, Y. et al. (2020). Robotic surgical procedure for diffuse cavernous hemangioma of the rectum: A case report. Asian journal of endoscopic surgery. [CrossRef]
Figure 1.
Abdominal MRI revealed the possibility of vascular malformations in the rectum wall and around the rectum.
Figure 1.
Abdominal MRI revealed the possibility of vascular malformations in the rectum wall and around the rectum.
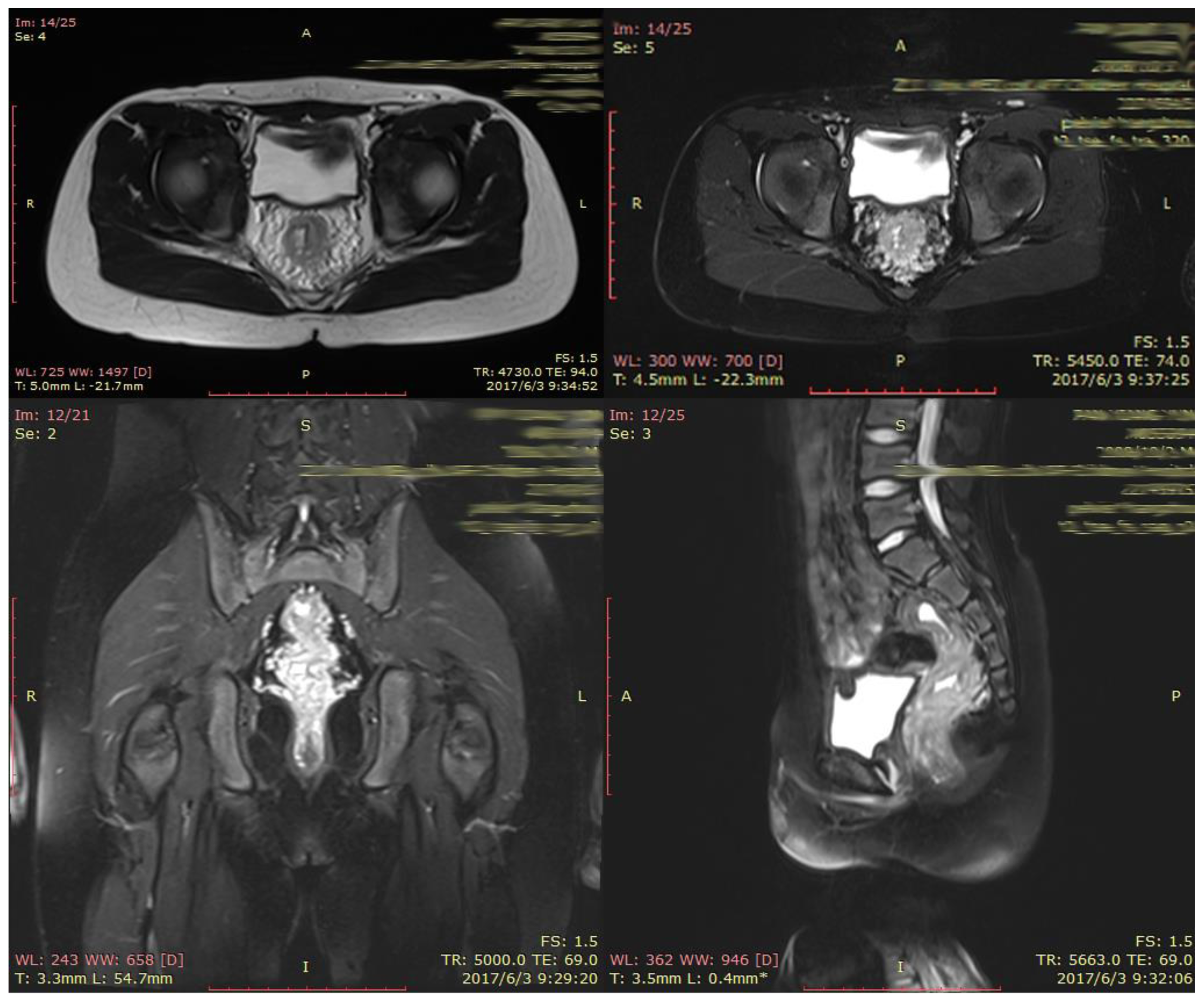
Figure 2.
A diffuse distribution of intestinal wall hemangioma in the distal rectum and sigmoid colon, with prominent anterior wall, and a distribution of vascular malformations in the pelvic soft tissues.
Figure 2.
A diffuse distribution of intestinal wall hemangioma in the distal rectum and sigmoid colon, with prominent anterior wall, and a distribution of vascular malformations in the pelvic soft tissues.
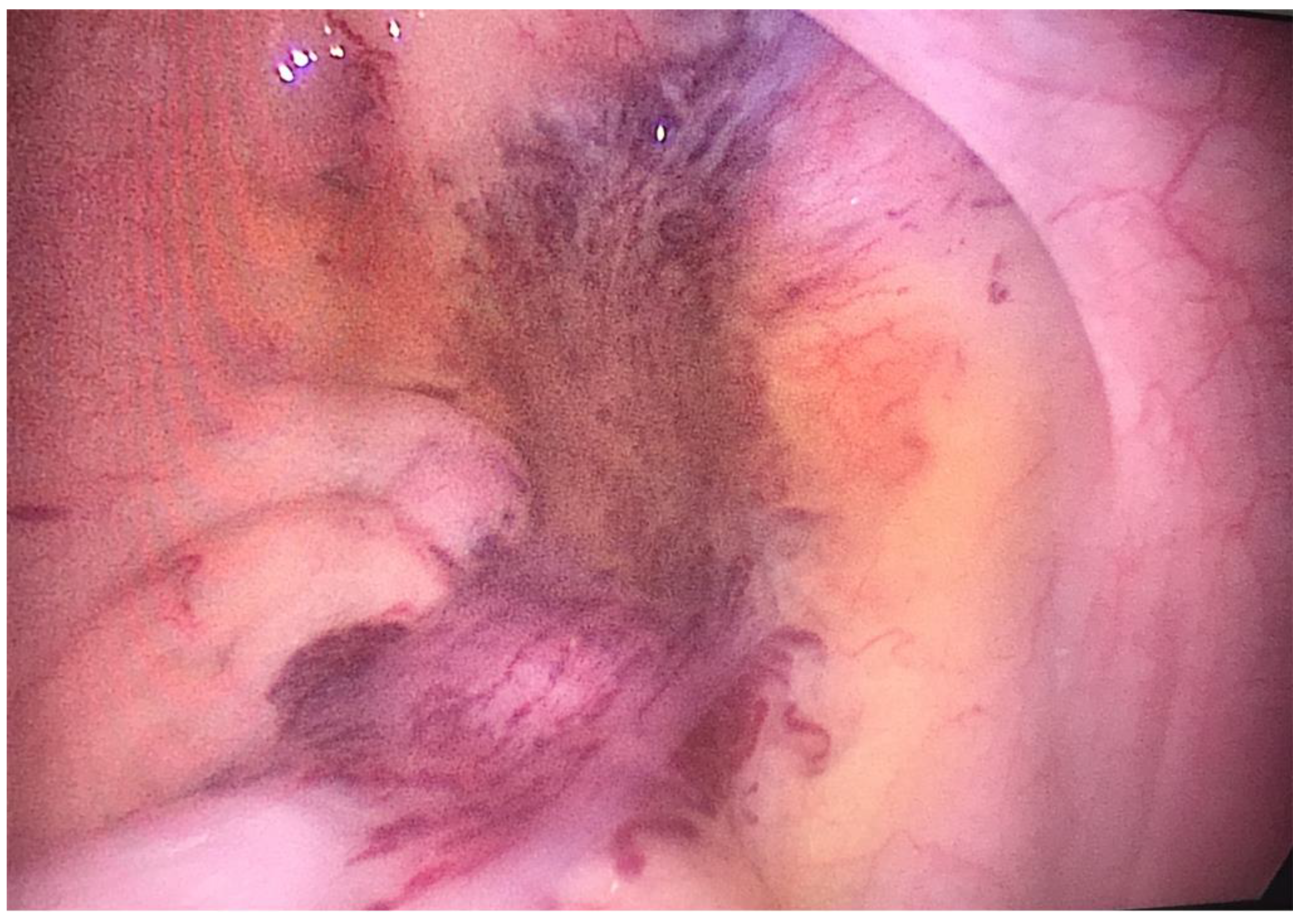
Figure 3.
After changing to lithotomy position. The colon was pulled out of the anus . The edge of the rectum to the dentate line was resected, 1.5cm of the anterior wall and 0.5cm of the posterior wall of the rectum were retained, and the sigmoid colon was cut in the reverse oblique, and then the end-to-end heart-shaped anastomosis was performed with the rectum. .
Figure 3.
After changing to lithotomy position. The colon was pulled out of the anus . The edge of the rectum to the dentate line was resected, 1.5cm of the anterior wall and 0.5cm of the posterior wall of the rectum were retained, and the sigmoid colon was cut in the reverse oblique, and then the end-to-end heart-shaped anastomosis was performed with the rectum. .
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



