Submitted:
15 August 2023
Posted:
16 August 2023
You are already at the latest version
Abstract
Increasingly small, non-palpable testicular incidentalomas <1cm are discovered in the clinical practice. The ESUR Scrotal and Penile Imaging Working Group suggests active surveillance with US, and surgery only for nodules that grow. This approach, however, requires validation.
A consecutive series of 127 incidentalomas were initially followed-up and operated if they were growing (n=28), or because of preference of the patient and of the referring urologist (n=11). For the lesions that were growing specific growth rate (SGR) and doubling time (DT) were calculated assuming an exponential grow. Also, the velocity of increase of the average diameter (∆Dav) and of the maximum diameter (∆Dmax) were calculated. Of the 127 nodules which were initially followed-up, 6 disappeared, 8 reduced in size, 85 were stable, and 28 increased in size. All 18 malignant tumours, 8/9 benign tumours, and 2/12 surgically proved non-neoplastic lesions were growing. The best cut-off values of the growth indicators to differentiate between malignant and non-malignant histology were 3.47x10-3 %volume/day, ≤179 days, >10x10-3 mm/day, and >5x10-3 mm/day for SGR, DT, ∆Dmax, ∆Dav, respectively.
A conservative approach of non-growing small incidentalomas is safe. Malignant and non-malignant small incidentalomas can be effectively differentiated based on growing parameters, even though superimposition exists.
Keywords:
testicular incidentaloma
; imaging
; non‐palpable testicular tumours
; Testis lesion
; growth rate
; incidental testicular tumour
; histology
1. Introduction
Small (<1cm), asymptomatic lesions are often discovered incidentally during a scrotal US investigation performed for other purpose. Only about 30% of these lesions are malignant, while the others are either benign tumours, or non-neoplastic lesions [1]. The smaller the lesion, the lower is the chance of being malignant. Virtually all lesions <3 mm are benign, while lesions <5mm are benign in 87% of cases [1].
According to the current release of the EAU Guidelines on Testicular Cancer, testis sparing surgery (TSS) together with frozen section examination can be offered in patients with a high likelihood of having a benign testicular tumour, which is exactly the case for these patients, but orchidectomy is still considered the treatment of choice in patients with solid testicular nodules, and lesion follow-up is not recommended [2]. However, urological practice is evolving towards a less aggressive approach in which serial US monitoring is also used [3,4].
Since also very small lesions may actually be a malignant tumour, the main issue of this less aggressive approach is to differentiate lesions that can be safely followed-up from those which require surgery, either TSS or orchidectomy. Then, the growth rate of a lesion is used to indicate malignancy, be it associated or not with positive tumour markers [4]. Testicular tumours are usually considered fast-growing lesions; on the contrary, benign tumours and/or non-neoplastic lesions grow slowly or remain stable, reduce in size, or even disappear during the follow-up. This is commonly observed in clinical practice; however, there are not firm data in the literature, and the reported fast doubling times (ranging from 10 to 30 days) of testicular neoplasms regard the growing characteristics of metastatic lymph nodes, not those of the primary tumour [5].
Since the growth rate of small testicular tumours is unknown, no thresholds have been established to distinguish between benign and malignant lesion. As a consequence, differentiation based on growing speed remains unreliable.
In our clinical practice, testis sparing surgery is recommended for lesions ≥1cm and for lesions <1cm which are growing [6]. By convention, an overall increase in the greater diameter ≥1mm during two consecutive follow-up investigations is considered unequivocal growth.
In this study, a series of 127 small (<10mm), incidentally detected non-palpable testicular lesions with negative tumour markers has been retrospectively investigated. The lesions were initially followed up, and a minority of them (n=39) were operated because they were growing (n=28), or due to patient and/or urologist preference (n=11). The aim was threefold: a) to substantiate whether small, incidentally detected testicular lesions can be safely followed up; b) to assess the growth rate of surgically proven benign, malignant and non-neoplastic lesions; c) to investigate whether a threshold could be identified for a reliable differentiation between benign/non neoplastic lesions and malignant tumours based on growth characteristics.
2. Material and methods
This research study was conducted retrospectively from data obtained for clinical purposes. All the procedures performed were part of the routine care. Approval was granted by the Ethics Committee of the institution of the corresponding author (verb128 27/02/2023, available at: https://www2.units.it/comitatoetico/verbali21_23/). All patients verbally consented to scrotal sonographic evaluation. Data were processed without any patient-identifying information.
From October 2001 to November 2021, in seven diagnostic centers,127 consecutive patients (median age, 38 years; range, 16–78 years) with incidentally detected, nonpalpable testicular lesions <1cm of maximum diameter were initially scheduled for active surveillance. All patients had negative tumour markers. Cysts were excluded. Different high-end US equipment was used, with high-frequency, broadband probes. In 37/127 patients who had multiple small lesions the largest was considered for the purpose of this study. The other 90 patients had a single lesion. In the majority of cases (98/127, 77%) the follow-up was carried out following ESUR recommendations [7] and patients were monitored every three months for 12 months and then annually. In the remaining 29 patients one or more examinations were missed during the follow-up. In our series, surgery was scheduled during the follow-up for 39/127 lesions because the lesion was growing (n=28), or because of preference of the patient and of the referring urologist (n=11).
2.1. Data analysis
Images obtained during the follow-up studies were retrieved for retrospective review. Patients’ ages at the time of the first examinations and histologic results of the operated lesions were also retrieved from the archives. Retrospective review of images was performed on a per-patient basis by a radiologist with 10-years’ experience in US imaging (IC) who was not aware of the histology of the lesion. If the patient had multiple testicular lesions, the largest was considered. The reviewer was asked to measure the lesions during the follow-up, and to assess whether they were stable, shrinking, growing or they disappeared.
For the purpose of the study, testicular lesions were labelled as stable when their maximum diameter increased/decreased less than 1mm during two consecutive follow-up investigations, as shrinking when their maximum diameter decreased more than 1mm, or as growing when an overall increase in greater diameter of 1mm or more was observed during two consecutive follow-up investigations.
For the lesions that were growing, the three diameters of the target nodules were measured and volume calculated applying the ellipsoid formula. Then, the specific growth rate (SGR) and doubling time (DT) were calculated as previously described, assuming an exponential growth of the lesion [8]. SGR (%volume/day) is defined as percentage volume increase per unit of time. DT (in days) is defined as the amount of time it takes for the lesion to double in size. Since the uncertainty of volume estimation can be high for millimetric nodules [9], also the velocity of increase of the average diameter (∆Dav) and of the maximum diameter (∆Dmax) of the nodules were calculated. The formulas used for measuring these parameters are reported in Table 1.
2.2. Reference procedure
The lesions which reduced in size or were stable during a follow-up of 1 year or more were considered presumably benign. As regards the 28 growing lesions, final diagnosis was obtained histologically, as well as in 11 non-growing lesions which were operated according with patient’s or urologist’s decision.
2.3. Statistical Analysis
Statistical analyses were performed using MedCalc for Windows, version 19.3.1 (MedCalc Software, Ostend, Belgium).
Size differences of the malignant and of non-malignant nodules when first identified at ultrasonography, and differences among the growth indicators were assessed using the Student’s t-test. The sensitivity, specificity, and predictive values to assess malignancy for different growth indicators were tested using a receiver operating characteristic (ROC) curve analysis. The Youden’s index was applied to identify the cutoff values that maximize both sensitivity and specificity.
3. Results
Of the 127 testicular lesions which were initially followed-up, 6 disappeared, 8 reduced in size, 85 were stable, and 28 increased in size. The duration of the follow-up in non-operated lesions ranged from 1 to 22 years. Histology was available for 39 operated lesions, 11 stable, and 28 growing. Among the 11 stable lesions there were 1 benign tumour and 10 non-neoplastic lesions (Table 2). When only the 28 growing lesions were considered, 18 were malignant tumours (Figure 1), 8 were benign tumours (Figure 2), and 2 were non-neoplastic lesions. The initial volume of malignant and of non-malignant lesions was not statistically different (Student’s t-test, p=0.53). On the countrary, SGR (Figure 3), ∆Dmax and ∆Dav were significantly higher for malignant tumours (11.4x10-3 vs 3.47x10-3 %volume/day, 31x10-3 vs. 9x10-3 mm/day, and 24x10-3 vs. 7x10-3 mm/day, respectively). There was a trend toward a higher DT for malignant tumours, but differences with non-malignant lesions were not statistically significant (Table 3).
The best cut-off values of the growth indicators to differentiate between malignant and non-malignant histology were 3.47x10-3 %volume/day, ≤179 days, >10x10-3 mm/day, and >5x10-3 mm/day for SGR, DT, ∆Dmax, ∆Dav, respectively (ROC curve analysis, Youden index J) (Table 4). All malignant tumours were removed within 18 months after discovery. They were all stage IA lesions.
4. Discussion
Even if the EAU Guidelines on Testicular Cancer recommend surgery for all incidentally detected testicular lesions there is increasing evidence that this approach constitutes an overtreatment [10], causing adverse fertility, hormonal, and mental health adverse outcomes [11,12]. Several investigations show that the majority of small testicular incidentalomas are benign or non-neoplastic lesions. Bieniek et al. found six malignant lesions in 120 sub-centimetric testicular incidentalomas [3]. All malignant lesions were >5mm on initial imaging. Scandura et al. investigated a series of 81 testicular incidentalomas <1cm and found that two third of them, and all those <5mm were benign [10]. She concludes that patients who undergo an orchidectomy for lesions <5 mm are “Victims of Modern Imaging Technology“. In a recent systematic review, virtually all lesions <3 mm and 86.6% of lesions <5 mm were non-malignant [1]. In spite of this, even very small incidentalomas can actually be a small cancer. The smallest malignant tumour in our series was identified with a volume of 176 mm3 and a maximum diameter of 4mm.
Management strategies to reduce non-necessary surgery of small incidentally found testicular nodules include on one side improvement of lesions’ characterization at multiparametric US and magnetic resonance imaging (MRI) [13,14,15,16,17] and, on the other side, different management based on the growth characteristics of the lesion at US. The Scrotal and Penile Imaging Working Group (SPIWG) of the European Society of Urogenital Radiology (ESUR), in particular, suggests to resort to active surveillance in these lesions, with US examinations every three months in the first year and then annually [7]. The World Federation of Ultrasound in Medicine and Biology (WFUMB) recommends surgery for lesions that grow or display increasing vascularity on interval imaging, while stable lesions can be managed conservatively [18]. There are no recommendations as regards the duration of the follow-up [18].
Even though this approach for testicular incidentaloma is considered oncologically safe in appropriately selected cases, and is successfully applied in several centers, its theoretical basis needs to be substantiated. To the best of our knowledge, growth rate of testicular tumours has not been previously investigated. Doubling times of testicular tumours tissue have been reported ranging from 10 to 30 days, but these data regard growth characteristics of metastatic lymph nodes, not of the primary tumour itself [5].
A consecutive series of 127 patients is herein retrospectively investigated in whom small, non-palpable testicular tumours with negative tumour markers were initially followed-up, and only the growing ones were operated. Our data confirm that a conservative approach is effective in reducing non-necessary operation. In our series, in fact, surgery was avoided in 88/127 (69%) lesions.
In our series, 11 non-growing lesions were eventually operated due to patient and/or referring urologist preference. 10/11 of them were non-neoplastic lesions, one was a benign tumour. Similarly, in the series of Toren et al. six non-growing lesions were operated; four were non-neoplastic lesions, 2 were benign tumour [4]. These data show that even though non-growing small incidentalomas are virtually all benign, leaving a small testicular lesion in place is still cause of concern, both among the urologists, and among the patient, which results in overtreatment. It is therefore advisable to train the urologists on this issue and, most important, to reassure the patient about the safety of the follow-up.
Although, in principle, it cannot be excluded that any of these non-operated incidentalomas were actually a malignant tumour, this is unlikely. In fact, 11 patients who were operated even if the lesion was stable during the follow-up had all benign tumours or non-neoplastic lesions. On the other hand, 18/28 (64%) growing lesions were malignant, and evaluation of growth indicators helped identification of malignant tumours.
Our data suggest that malignant small, non-palpable incidentalomas are mostly seminomas (17/18 in our series, 94%). All were identified and removed within 18 months after discovery, and all were stage IA tumours.
In clinical stage I seminoma tumour size has a bearing for risk of tumour recurrence [19]. Therefore, it could be argued that a delay in the operation could be detrimental for the patient, since a larger tumour is removed. For small tumours, however, increased risk of tumour recurrence is minimum. According with Chung et al. increase in size from 1cm to 2cm it increases recurrence risk from 9% to 11% [20]. Therefore, the follow-up period should not affect the patient prognosis.
In our series, only two patients had lesion >2cm in diameter when operated. They were a benign leydigoma, and a seminoma in a monorchid patient, who refused operation until the lesions reached a maximum diameter of 28mm. After the operation the patient did not receive further treatment and is free from relapse after a surveillance of 10 years.
We believe that based on these data and disease prevalence, a non-aggressive management of small testicular incidentalomas is justified, and should be considered safe when follow-up is associated to self-examination and tumour marker assessment, in order to reduce the risk of interval tumour growth [7].
Slow-growing seminomas can be encountered which cannot be distinguished from benign tumours based on growth characteristics [21]. This could have an effect on the choice of the surgical approach. In our series, a slow growing seminoma was encountered (SGR 2x10-3 %/day, DT 316 days). The lesion was stable during the first six months of the follow-up and then began to increase in size. The patient was initially resistant to surgery, but was eventually operated. He could have been eligible for testis sparing surgery, but orchidectomy was performed because of patient’s and urologist’s preference. Testis sparing surgery, however is safe if a careful surgical technique is used [22].
In our series, SGR, ∆Dmax, and ∆Dav, were significantly different for malignant and non-malignant lesions, while DT did not reach a statistical significance. The limitations of DT for quantifying tumour growth have been already underlined for pulmonary nodules [23].
The variability of DT is much larger than that for SGR, making the latter a more suitable measure of volume change. In particular, it has been shown that DT largely overestimates the difference in growth rate of slowly growing tumors and underestimates the difference in growth rate of rapidly growing tumors, while SGR uniformly indicates the difference between growth rates throughout all ranges [8,24]. As a consequence, the growth rate of testicular incidentalomas should be expressed by SGR, or percentage volume increase per unit time, when technically feasible. In our clinical practice, however, an overall increase in the greater diameter ≥1mm during two consecutive follow-up investigations was considered an unequivocal growth. Serial evaluations are necessary due to the large intrinsic errors in the measurement of the diameters of subcentimetric nodules.
For the same reason, SGR and DT are not routinely evaluated at the time of the examination, since errors in calculating the diameters are multiplied. In this study it has been shown that linear parameters such as Dmax, and ∆Dav, which are immediately derived from the measurement of the diameters, are effective in providing a rough estimation of tumour growth, sensitive enough for prompt identification of fast-growing lesions.
Use of high-end equipment and higher frequency probes improve spatial and contrast resolution. It could improve the accuracy of the measurements, and make prompt identification of slow-growing lesions easier. Also, 3D imaging with automatic volume calculation could be an option to reduce variability.
This study has several limitations. The most important are its retrospective design and the relatively small number of operated patients. The timing of the follow-up was not the same in all patients, since in 29 of them one or more examinations were missed during the follow-up. As it is commonly accepted for small tumours, in this study an exponential growth has been postulated for calculating SGR and DT [8], but this assumption requires confirmation with large prospective studies.
Another limitation of this study is that only one lesion was a non-seminomatous tumour, and only two non-neoplastic lesions were growing. This likely reflect the real prevalence of disease, suggesting that, among small nonpalpable incidentalomas with negative tumour markers that are growing, benign and malignant tumours prevail, malignancy is more frequent (64% in our series), and most malignant tumours are seminomas (94% in our series).
The very low incidence of non-seminomatous tumours in this series is difficult to explain, since the overall prevalence of seminomas is approximately 55%-60% [25]. However, about 85% of seminomas are diagnosed as clinical stage I disease as compared with about 60% among non-seminomas [26,27]. This has been temptatively explained with a faster progression of non-seminomatous tumour [28]. Our findings may have a similar explanation. If non-seminomatous tumours grow faster, it could be unlikely to identify them when they are non-palpable, <1cm lesions. Moreover, since about 58% of clinical stage I non-seminomatous tumours have positive tumour markers [26], some of these lesions could also have been excluded for this reason.
In conclusion, This retrospective study represents the first attempt to estimate the growth rate of testicular incidentalomas, to identify thresholds to differentiate surgical from non-surgical lesions, and benign from malignant lesions. We found that benign and malignant lesions can be effectively differentiated based on growing parameters, even though superimposition exists. These results are promising, but the strength of the evidence suffers from the retrospective design of the study. Prospective multicenter studies with a larger number of lesions are necessary to substantiate them, leading to an evidence-based paradigm shift in the management of small testicular incidentalomas.
References
- Bertolotto, M.; Campo, I.; Pavan, N.; Buoite Stella, A.; Cantisani, V.; Drudi, F.M.; et al. What Is the Malignant Potential of Small (<2 cm), Nonpalpable Testicular Incidentalomas in Adults? A Systematic Review. Eur Urol Focus.
- Nicol, D.; Berney, D.; Algaba, F.; Boormans, J.L.; di Nardo, D.; Fankhauser, C.D.; et al. EAU Guidelines on Testicular Cancer. Arnhem, The Netherlands: EAU Guidelines Office; 2023.
- Bieniek, J.M.; Juvet, T.; Margolis, M.; Grober, E.D.; Lo, K.C.; Jarvi, K.A. Prevalence and Management of Incidental Small Testicular Masses Discovered on Ultrasonographic Evaluation of Male Infertility. J Urol. 2018, 199, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Toren, P.J.; Roberts, M.; Lecker, I.; Grober, E.D.; Jarvi, K.; Lo, K.C. Small incidentally discovered testicular masses in infertile men--is active surveillance the new standard of care? J Urol. 2010, 183, 1373–1377. [Google Scholar] [CrossRef] [PubMed]
- Mazrani, W.; O’Malley, M.E.; Chung, P.W.; Warde, P.; Vesprini, D.; Panzarella, T. Lymph node growth rate in testicular germ cell tumours: implications for computed tomography surveillance frequency. Clin Oncol (R Coll Radiol). 2011, 23, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Connolly, S.S.; D’Arcy, F.T.; Gough, N.; McCarthy, P.; Bredin, H.C.; Corcoran, M.O. Carefully selected intratesticular lesions can be safely managed with serial ultrasonography. BJU Int. 2006, 98, 1005–1007. [Google Scholar] [CrossRef] [PubMed]
- Rocher, L.; Ramchandani, P.; Belfield, J.; Bertolotto, M.; Derchi, L.E.; Correas, J.M.; et al. Incidentally detected non-palpable testicular tumours in adults at scrotal ultrasound: impact of radiological findings on management Radiologic review and recommendations of the ESUR scrotal imaging subcommittee. Eur Radiol. 2016, 26, 2268–2278. [Google Scholar] [CrossRef]
- Mehrara, E.; Forssell-Aronsson, E.; Ahlman, H.; Bernhardt, P. Specific growth rate versus doubling time for quantitative characterization of tumor growth rate. Cancer Res. 2007, 67, 3970–3975. [Google Scholar] [CrossRef]
- Larici, A.R.; Farchione, A.; Franchi, P.; Ciliberto, M.; Cicchetti, G.; Calandriello, L.; et al. Lung nodules: size still matters. Eur Respir Rev. 2017, 26. [Google Scholar] [CrossRef]
- Scandura, G.; Verrill, C.; Protheroe, A.; Joseph, J.; Ansell, W.; Sahdev, A.; et al. Incidentally detected testicular lesions <10 mm in diameter: can orchidectomy be avoided? BJU Int. 2018, 121, 575–582. [Google Scholar]
- Huddart RA, Norman A, Moynihan C, Horwich A, Parker C, Nicholls E, et al. Fertility, gonadal and sexual function in survivors of testicular cancer. Br J Cancer. 2005, 93, 200–207. [Google Scholar] [CrossRef]
- Tuinman, M.A.; Hoekstra, H.J.; Fleer, J.; Sleijfer, D.T.; Hoekstra-Weebers, J.E. Self-esteem, social support, and mental health in survivors of testicular cancer: a comparison based on relationship status. Urol Oncol. 2006, 24, 279–286. [Google Scholar] [CrossRef]
- Tsili, A.C.; Bertolotto, M.; Rocher, L.; Turgut, A.T.; Dogra, V.; Secil, M.; et al. Sonographically indeterminate scrotal masses: how MRI helps in characterization. Diagn Interv Radiol. 2018, 24, 225–236. [Google Scholar] [CrossRef] [PubMed]
- Konstantatou, E.; Fang, C.; Romanos, O.; Derchi, L.E.; Bertolotto, M.; Valentino, M.; et al. Evaluation of Intratesticular Lesions With Strain Elastography Using Strain Ratio and Color Map Visual Grading: Differentiation of Neoplastic and Nonneoplastic Lesions. J Ultrasound Med. 2019, 38, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Cantisani, V.; Di Leo, N.; Bertolotto, M.; Fresilli, D.; Granata, A.; Polti, G.; et al. Role of multiparametric ultrasound in testicular focal lesions and diffuse pathology evaluation, with particular regard to elastography: Review of literature. Andrology. 2021, 9, 1356–1368. [Google Scholar] [CrossRef]
- Bertolotto, M.; Muca, M.; Curro, F.; Bucci, S.; Rocher, L.; Cova, M.A. Multiparametric US for scrotal diseases. Abdom Radiol (NY). 2018, 43, 899–917. [Google Scholar] [CrossRef] [PubMed]
- Drudi, F.M.; Valentino, M.; Bertolotto, M.; Malpassini, F.; Maghella, F.; Cantisani, V.; et al. CEUS Time Intensity Curves in the Differentiation Between Leydig Cell Carcinoma and Seminoma: A Multicenter Study. Ultraschall Med. 2016, 37, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Lewicki, A.; Freeman, S.; Jedrzejczyk, M.; Dobruch, J.; Dong, Y.; Bertolotto, M.; et al. Incidental Findings and How to Manage Them: Testis- A WFUMB Position Paper. Ultrasound Med Biol. 2021, 47, 2787–2802. [Google Scholar] [CrossRef] [PubMed]
- Zengerling, F.; Kunath, F.; Jensen, K.; Ruf, C.; Schmidt, S.; Spek, A. Prognostic factors for tumor recurrence in patients with clinical stage I seminoma undergoing surveillance-A systematic review. Urol Oncol. 2018, 36, 448–458. [Google Scholar] [CrossRef]
- Chung, P.; Daugaard, G.; Tyldesley, S.; Atenafu, E.G.; Panzarella, T.; Kollmannsberger, C.; et al. Evaluation of a prognostic model for risk of relapse in stage I seminoma surveillance. Cancer Med. 2015, 4, 155–160. [Google Scholar] [CrossRef]
- Moore, N.; Laurila, T.; Jarrard, D.F. Sonographically documented stable seminoma: a case report. Int Urol Nephrol. 2007, 39, 1163–1165. [Google Scholar] [CrossRef]
- Giannarini, G.; Dieckmann, K.P.; Albers, P.; Heidenreich, A.; Pizzocaro, G. Organ-sparing surgery for adult testicular tumours: a systematic review of the literature. Eur Urol. 2010, 57, 780–790. [Google Scholar] [CrossRef]
- Reeves, A.P.; Chan, A.B.; Yankelevitz, D.F.; Henschke, C.I.; Kressler, B.; Kostis, W.J. On measuring the change in size of pulmonary nodules. IEEE Trans Med Imaging. 2006, 25, 435–450. [Google Scholar] [CrossRef] [PubMed]
- Mehrara, E.; Forssell-Aronsson, E.; Ahlman, H.; Bernhardt, P. Quantitative analysis of tumor growth rate and changes in tumor marker level: specific growth rate versus doubling time. Acta Oncol. 2009, 48, 591–597. [Google Scholar] [CrossRef] [PubMed]
- Rajpert-De Meyts, E.; McGlynn, K.A.; Okamoto, K.; Jewett, M.A.; Bokemeyer, C. Testicular germ cell tumours. Lancet. 2016, 387, 1762–1774. [Google Scholar] [CrossRef] [PubMed]
- Klepp, O.; Flodgren, P.; Maartman-Moe, H.; Lindholm, C.E.; Unsgaard, B.; Teigum, H.; et al. Early clinical stages (CS1, CS1Mk+ and CS2A) of non-seminomatous testis cancer. Value of pre- and post-orchiectomy serum tumor marker information in prediction of retroperitoneal lymph node metastases. Swedish-Norwegian Testicular Cancer Project (SWENOTECA). Ann Oncol. 1990, 1, 281–288. [Google Scholar]
- Verhoeven, R.H.; Karim-Kos, H.E.; Coebergh, J.W.; Brink, M.; Horenblas, S.; de Wit, R.; et al. Markedly increased incidence and improved survival of testicular cancer in the Netherlands. Acta Oncol. 2014, 53, 342–350. [Google Scholar] [CrossRef]
- Oldenburg, J.; Berney, D.M.; Bokemeyer, C.; Climent, M.A.; Daugaard, G.; Gietema, J.A.; et al. Testicular seminoma and non-seminoma: ESMO-EURACAN Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2022, 33, 362–375. [Google Scholar] [CrossRef]
Figure 1.
Non-palpable, incidentally detected testicular lesion which displayed a rapid growth during the follow-up. In the first examination (A) the lesion had a maximum diameter of 4mm, while the diameter was 6mm and 14mm after 3 months (B) and 6 months (C). A seminoma was found at surgery (D).
Figure 1.
Non-palpable, incidentally detected testicular lesion which displayed a rapid growth during the follow-up. In the first examination (A) the lesion had a maximum diameter of 4mm, while the diameter was 6mm and 14mm after 3 months (B) and 6 months (C). A seminoma was found at surgery (D).
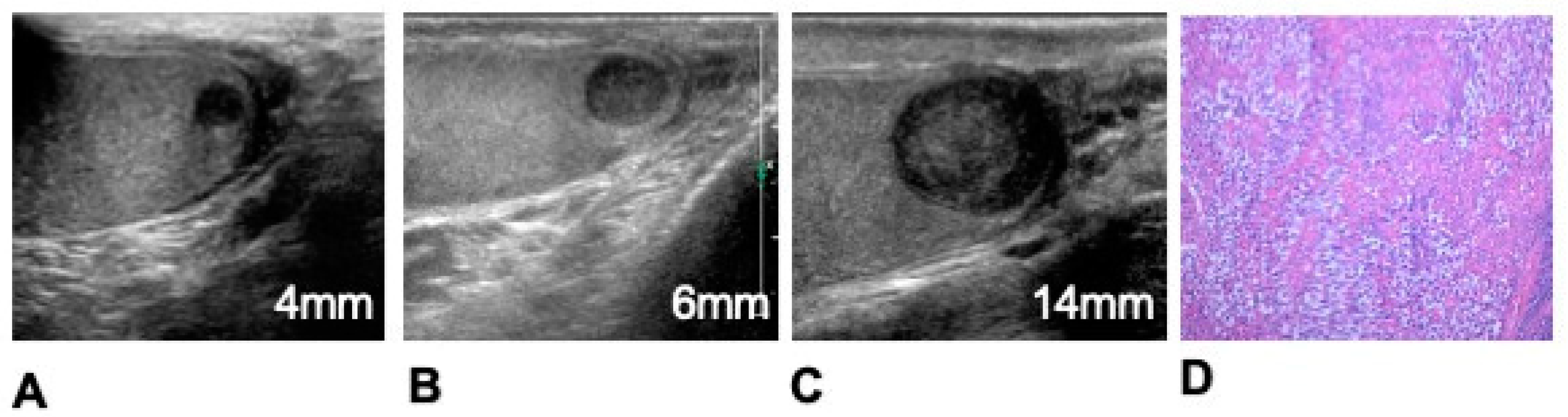
Figure 2.
Non-palpable, incidentally detected testicular lesion which displayed a slow growth during the follow-up. In the first examination (A) the lesion had a maximum diameter of 2mm, while the diameter was 2.2mm and 2.5mm after 3 months (B) and 6 months (C) during the follow-up. A leydigoma was found at surgery (D).
Figure 2.
Non-palpable, incidentally detected testicular lesion which displayed a slow growth during the follow-up. In the first examination (A) the lesion had a maximum diameter of 2mm, while the diameter was 2.2mm and 2.5mm after 3 months (B) and 6 months (C) during the follow-up. A leydigoma was found at surgery (D).
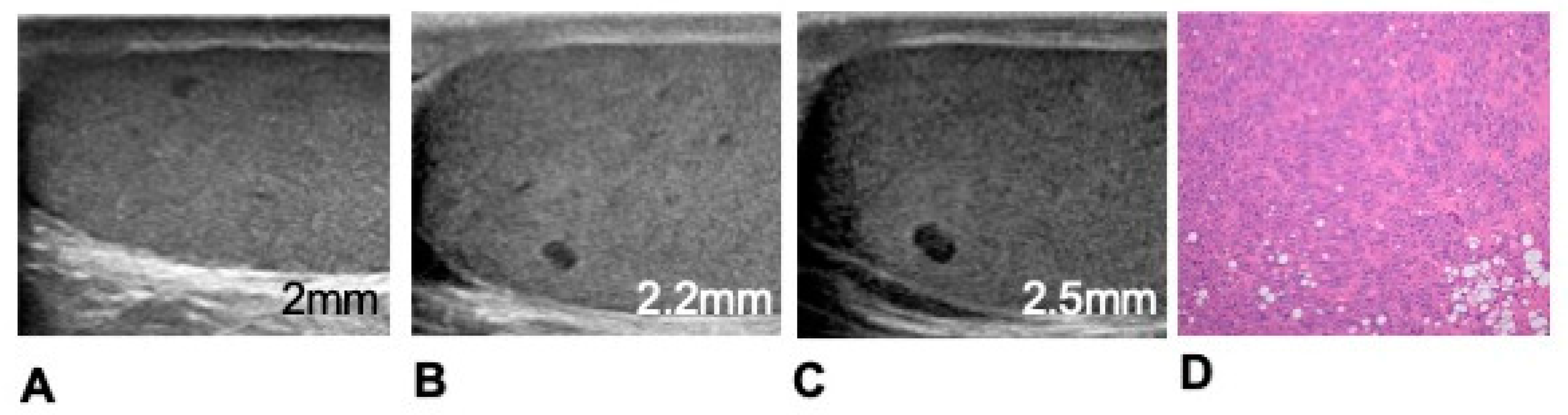
Figure 3.
Specific growth rate (SGR, %/day), doubling time (DT, days), velocity of increase of the maximum diameter (∆Dmax, mm/day) and of the average diameter (∆Dav, mm/day) of malignant and non-malignant growing testicular incidentalomas.
Figure 3.
Specific growth rate (SGR, %/day), doubling time (DT, days), velocity of increase of the maximum diameter (∆Dmax, mm/day) and of the average diameter (∆Dav, mm/day) of malignant and non-malignant growing testicular incidentalomas.
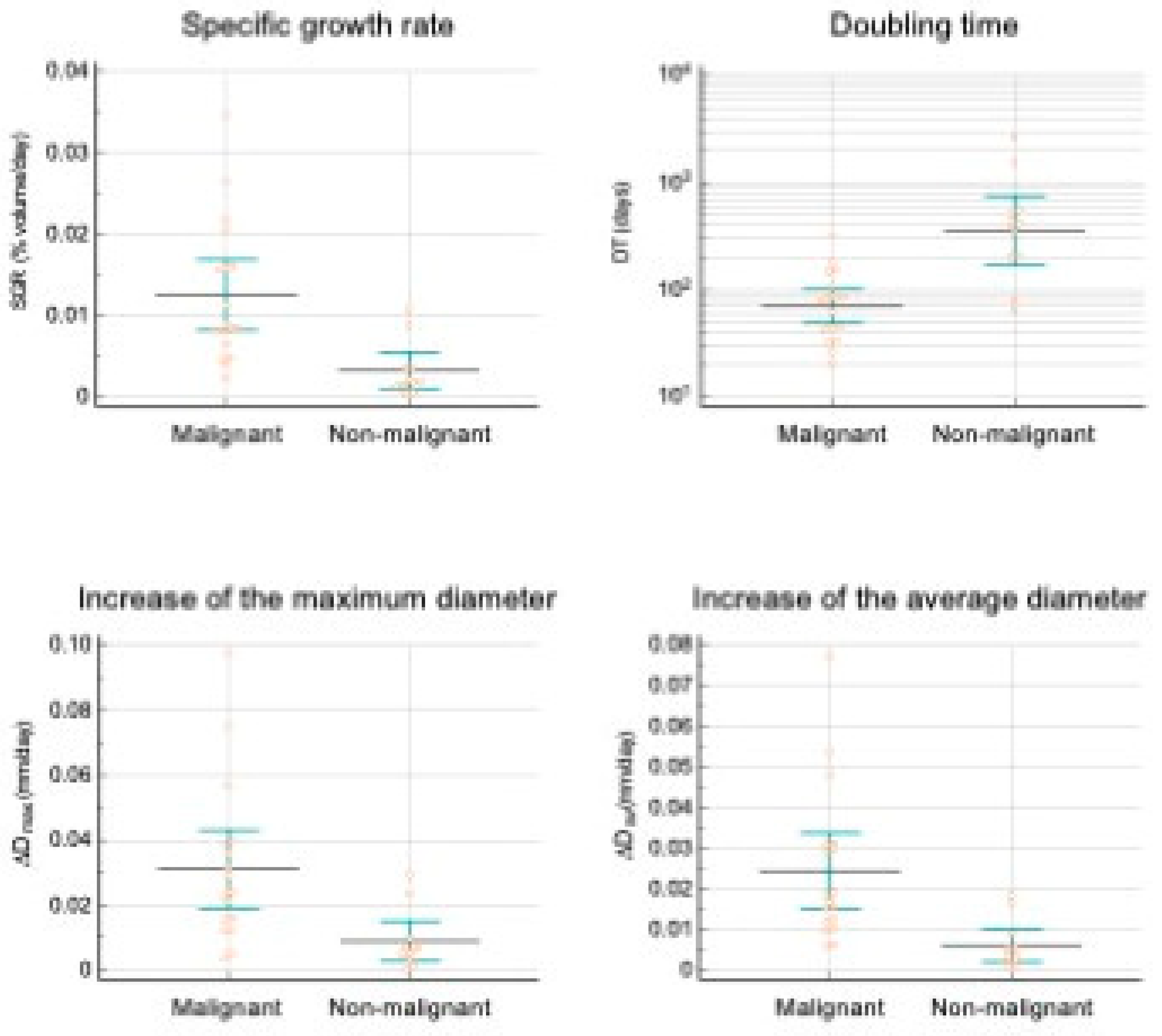

Table 1.
Definition of the parameters used for quantification of lesion growth rate.
| Parameter | Equation | Definition |
|---|---|---|
| Specific growth rate (SGR) | ln(V2/V1)/(t2-t1) (%volume/day) | percentage volume increase per unit of time |
| Doubling time (DT) | ln(2)/SGR (Days) | amount of time it takes for the lesion to double in volume |
| velocity of increase of the maximum diameter (∆Dmax) | (Dmax2-Dmax1)/(t2-t1) (mm/days) | velocity of increase of the maximum diameter |
| velocity of increase of the average diameter (∆Dav) | (Dav2-Dav1)/(t2-t1)(mm/days) | velocity of increase of the average diameter |
V1, Dmax1, Dav1, lesion volume, maximum diameter and average diameter at time t1; V2, lesion volume, maximum diameter and average diameter at time t2.
Table 2.
Histology of the 38 operated lesions.
| Malignant tumours (n=18) | Growing (n=18) | Seminoma (n=17) Non-seminoma (n=1) |
|---|---|---|
| Benign tumours (n=9) | Stable (n=1) | Leydigoma (n=1) |
| Growing (n=8) | Leydigoma (n=7) Capillary haemangioma (n=1) |
|
| Non-neoplastic lesions (n=12) | Stable (n=10) | Leydig cell hyperplasia (n=6) Fibrosis (n=3) Granulomatous orchitis (n=1) |
| Growing (n=2) | Leydig cell hyperplasia (n=2) |
Table 3.
Differences in growth indicators between surgically proved malignant vs. non-malignant lesions.
Table 3.
Differences in growth indicators between surgically proved malignant vs. non-malignant lesions.
| Growth indicator | Malignant lesions* | Non malignant lesions* | P |
|---|---|---|---|
| SGR (%volume/day) | 11.4±2.11x10-3 | 3.47±1.1x10-3 | <0.003 |
| DT (days) | 90±17 | 535±236 | 0.093 |
| ∆Dmax | 31±6 x10-3 | 9±3 x10-3 | <0.003 |
| ∆Dav | 24±4 x10-3 | 7±2 x10-3 | <0.002 |
*data reported as average ± standard error of the mean; SGR: Specific growth rate (%volume/day); DT: Doubling time (days); ∆Dmax: velocity of increase of the maximum diameter (mm/day); (∆Dav: velocity of increase of the average diameter (mm/day).
Table 4.
Area under the ROC curve (AUC) and cutoff values of the growth indicators that maximize both sensitivity and specificity to differentiate between surgically proved malignant vs. non-malignant testicular lesions.
Table 4.
Area under the ROC curve (AUC) and cutoff values of the growth indicators that maximize both sensitivity and specificity to differentiate between surgically proved malignant vs. non-malignant testicular lesions.
| Growth indicator | AUC* | Associated criterion (Youden index J) | Sensitivity | Specificity |
|---|---|---|---|---|
| SGR (%/day) | 0.883±0.075 | >3.47x10-3 | 94.44 | 80.00 |
| DT (days) | 0.883±0.075 | ≤179 | 94.44 | 80.00 |
| ∆Dmax | 0.839±0.082 | >10 x10-3 | 88.89 | 80.00 |
| ∆Dav | 0.889±0.071 | >5 x10-3 | 100.00 | 70.00 |
SGR: Specific growth rate (%/day); DT: Doubling time (days); ∆Dmax: velocity of increase of the maximum diameter (mm/day); (∆Dav: velocity of increase of the average diameter (mm/day); *AUC ± standard error.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



