Submitted:
11 August 2023
Posted:
14 August 2023
You are already at the latest version
Abstract
Background: Ovarian cancer is the leading cause of death from gynecological malignancies with serous carcinoma being the most common histopathologic subtype. Epithelial-Mesenchymal Transition (EMT) correlates with an increased metastatic potential, whereas the transcription factor SOX11 is overexpressed in diverse malignancies. Methods: In the present study, we aim to evaluate the potential role of the immunohistochemical expression of SOX11 in 30 serous ovarian carcinomas in association with E-cadherin and Vimentin expression as well as with patients’ clinicopathological data. Results: Most of the examined cases showed concurrent expression of E-cadherin and Vimentin, whereas SOX11 was expressed in a minority of the cases (26,7%). Interestingly, the positive cases had more frequently a metastatic disease at the time of diagnosis compared to the negative cases (p=0.09), an association, however, of marginal significance. Moreover, there was a negative correlation between E-Cadherin and SOX11 expression (p=0,0077) and a positive correlation between Vimentin and SOX11 expression (p=0,0130). Conclusions: The present work, for the first time, provides preliminary evidence SOX11 overexpression alongside E-cadherin loss in the promotion of EMT in serous ovarian cancer, thereby endorsing tumor metastasis.
Keywords:
SOX11
; epithelial-mesenchymal
; transition
; E-cadherin
; vimentin
; ovarian
; cancer
; metastasis
; survival
Introduction
The fifth most frequent tumor-related cause of death for women in the United States is ovarian cancer, which is the most common cause of death from malignancies of the female genital tract[1]. The American Cancer Society predicts that in the United States in 2023, there will be about 19,710 new cases of ovarian cancer diagnosed and about 13,270 women will pass away from ovarian cancer[1]. Ovarian cancer comes in a variety of histological forms. The majority of ovarian cancers are epithelial carcinomas, with high-grade serous ovarian cancer being the most prevalent morphological subtype[2]. Given the lack of specific symptoms in the early stages of the disease, ovarian cancer is typically discovered when the tumor is at an advanced stage and after metastasis has taken place[3,4]. When a distant metastasis is present, the 5-year survival rate for women with invasive epithelial ovarian cancer falls to 31%[5]. A histologic examination of the tumor mass is necessary for a conclusive diagnosis; this is typically done after the tumor has been surgically removed[6].
The Epithelial-Mesenchymal Transition (EMT) is a biological process that enables a polarized epithelial cell to undergo numerous biochemical changes that allow it to assume a mesenchymal cell phenotype, which includes enhanced migratory capacity, invasiveness, elevated resistance to apoptosis, and significantly increased production of extracellular matrix components[7]. Normally, this cell interacts with the basement membrane via its basal surface. The breakdown of the underlying basement membrane and the development of a cell with a mesenchymal phenotype that can move away from the epithelial layer in which it originated are signs that an EMT has occurred[8]. EMT requires a number of various molecular processes to be activated. These consist of the induction of ECM-degrading enzymes, the activation of transcription factors, the expression of particular microRNAs, changes in the expression of specific cell-surface proteins, and reorganization and expression of cytoskeletal proteins. These contributing factors are frequently used as biomarkers to show that a cell has undergone EMT[8]. α-Smooth muscle actin (α-SMA), Fibroblast-Specific Protein 1 (FSP1), vimentin, and desmin are examples of mesenchymal markers that carcinoma cells can express[9]. These cells are frequently present at the invasive front of primary tumors and are thought to be those that eventually progress through the subsequent stages of the invasion-metastasis cascade, including intravasation, transport through the circulation, extravasation, the formation of micrometastases, and finally the development of small colonies into macroscopic metastases[10,11,12].
The SOX family is a group of transcription factors that play significant roles in determining cell fate, which includes the transcription factor SOX11, mapping to chromosome 2p25.3[13]. SOX11 has the N- and C-terminal transactivation domains as its functional domains[14]. It has been discovered that SOX11 functions downstream of proneural basic helix-loop-helix (bHLH) proteins, which commit progenitor cells to a neurogenic program to create a neuronal phenotype. Its functional relevance to neurogenesis was further confirmed by the discovery of SOX11 expression in medulloblastoma[15]. Moreover, SOX11 shows normal expression in the developing central nervous system of the embryo, keratinocytes, and several other epithelial tissues[16]. Interestingly, SOX11 has been shown to be expressed in a number of malignancies, such as mantel cell lymphomas, pancreatic solid pseudo-papillary tumors, brain tumors and breast carcinomas[17,18,19,20]. Recently, SOX11 was also implicated to play a significant role in mesenchymal state and embryonic cellular phenotypes in breast cancer[21].
In view of these considerations, the present study aims to investigate the potential role of SOX11 in metastatic serous ovarian cancer as a marker of EMT, as well as its influence on patients’ clinico-pathological characteristics including survival.
Materials and Methods
Patient Collective
This is a study of archival histopathological material from 30 patients with a serous ovarian carcinoma diagnosed during 2017–2018 at the Department of Pathology, in Klinikum Nuremberg, Germany, for whom medical records were available. All patients underwent a surgical resection and none of them had received any kind of neoadjuvant radio- or chemotherapy prior to surgery. Our cohort was based on the random selection of 15 patients with the presence of metastasis and 15 patients with no evidence of metastasis at the time of diagnosis. Other histological subtypes, borderline tumors as well as mixed carcinomas were excluded from our analysis. Patients were assigned a clinical stage according to the International Federation of Obstetrics and Gynecology (FIGO) standards[22]. Surgical and pathological findings and postoperative abdominopelvic computerized tomography scans were used to determine the FIGO stage for the ovarian adenocarcinomas and the residual disease after initial surgery. The study was conducted in accordance with the Declaration of Helsinki and was approved by the Bioethics Committee of the Paracelsus University, Nuremberg, Germany. Due to the retrospective nature of the studies, as well as the lack of impact on the treatment of patients, it was not necessary to obtain informed consent.
Immunohistochemical analysis
Immunohistochemistry (IHC) for E-cadherin, Vimentin and SOX11 was performed on formalin-fixed, paraffin-embedded tissue sections using the following antibodies: mouse monoclonal anti-SOX11 (clone MR-58, Firma Cell Marque), mouse monoclonal anti-E-cadherin (NCH-38, Dako) and mouse monoclonal Vimentin (clone V9, DAKO). Envision Flex+ Mouse (K8021, DAKO) was used as a detection system. For each antibody, suitable negative and positive controls were used as appropriate. IHC evaluation was performed by counting by an experienced pathologist, blinded to clinical information.
Statistical analysis
Statistical analysis was performed by a MSc biostatistician. The association between the IHC expression of E-cadherin, Vimentin, and SOX11, and clinicopathological characteristics was examined using non-parametric tests with correction for multiple comparisons, as appropriate. Survival analysis was performed using Kaplan–Meier survival curves and the differences between the curves were compared with log-rank test. A p-value of <0.05 was considered statistically significant. A p-value of > 0.05 but lower of < 0.10 was considered of marginal significance. The analysis was performed with the statistical package STATA 11.0/SE for Windows.
Results
Patients’ characteristics
The patients’ characteristics are shown in Table 1. The median age was 61,5 (range 46-79 years). Tumor stage according to FIGO was as follows: 23% has a FIGO-stage I, 10% a FIGO-stage II, 67% a FIGO-stage III and 30% a FIGO-stage IV. Five patients had a low grade (LG) and 25 a high grade (HG) carcinoma. Follow-up information was available in 21 patients, six of whom died of their disease within a period of 3,4-35 months. From the 15 patients with metastatic disease at diagnosis 6 of them had a lymph node metastasis, 3 a lymph node and a liver metastasis, 4 a pleura metastasis, one a liver metastasis and one a skin metastasis.
Immunohistochemical expression of E-Cadherin in ovarian serous carcinoma
E-cadherin expression was observed in 29/30 ovarian serous carcinomas with a median value of 92,5% (range 0-100%, Figure 1 A, D). There was no variety in the staining intensity, which was considered moderate to high. The LG ovarian serous carcinomas showed an increased expression of E-cadherin when compared to the HG carcinomas, but this association was of marginal significance (Mann Whitney U Test, p=0,06). Moreover, the carcinomas with metastasis at the time of diagnosis showed a lower E-cadherin expression compared to the ones without a metastatic disease (Mann Whitney U Test, p=0,0063) (Figure 1). There was no significant association with the FIGO-stage (Kruskal Wallis ANOVA, p>0,10) or the patients’ survival (log rank test, p>0,10).
Immunohistochemical expression of Vimentin in ovarian serous carcinoma
Vimentin expression was observed in 22/30 cases, showing a median value of 15% (range 0-90%, Figure 1C, F). There was no variety in the staining intensity, which was considered moderate to high. No significant association was detected in terms of FIGO-stage, tumor grade, presence of metastasis or patients’ survival (Kruskal Wallis ANOVA, Mann Whitney U Test, and log-rank test, p>0,10).
Immunohistochemical expression of SOX11 in ovarian serous carcinoma
SOX11 was negative in the majority of the cases and was observed only in 8/30 cases (26,7%, median value 0, range 0-90%, Figure 1 B, E). These eight positive cases had more frequently a metastatic disease at the time of diagnosis compared to the negative cases (75% versus 41%, Chi-square Test, p=0.09, Figure 3). This association was, however, of marginal significance. There was no significant correlation with FIGO-stage, tumor grade, or patients’ survival (Kruskal Wallis ANOVA, Mann Whitney U Test, and log-rank test, p>0,10).
Associations between the examined molecules
There was a negative correlation between E-Cadherin and SOX11 expression (Spearman correlation coefficient R= -0,4773, p=0,0077) and a positive correlation between Vimentin and SOX11 expression (Spearman correlation coefficient R= 0,4480, p=0,0130). In particular, the one case in our cohort which was negative for E-cadherin displayed an increased expression of SOX11, calculated as 70%.
Discussion
Given its high prevalence and mortality, ovarian cancer has long attracted the interest of diverse international study groups with a view to identifying and determining trustworthy biomarkers in the context of tumor metastasis and patient survival. Despite the therapeutic advancements over the past 20 years, which have undoubtedly revolutionized the anti-ovarian-cancer therapy, 5-year relative survival rates amount to only 31% for invasive epithelial ovarian cancer in a distant Surveillance, Epidemiology, and End Results (SEER) stage[5]. Recently, Huh et al. tried to uncover novel diagnostic biomarkers for HG serous ovarian cancer by data-independent acquisition mass spectrometry and succeeded in identifying a total of four potential biomarkers (Fibrinogen-A, von-Willebrand factor, Rho GDP dissociation inhibitor beta and Serpin family F member) that might play a significant role in HG serous ovarian cancer cell proliferation and migration[23]. Similarly, Atallah et al. proved that both bikunin and creatine kinase b represent useful biomarkers concerning ovarian cancer survival and prognosis, while osteopontin seems to correlate with ovarian cancer progression and metastasis[24].
In general, the decrease of E-cadherin as a marker of the epithelial phenotype has been suggested to indicate the progression of EMT[25]. Evidence has also shown the correlation between loss of E-cadherin expression by tumor cells and the progression of EMT in the cell[8]. However, the complete conduction of EMT and the subsequent acquisition of a pure mesenchymal phenotype is not always necessary for metastasis[26], which is in alignment with the results of this project. Of the total 30 cases, there was only one case with complete loss of E-cadherin expression and high vimentin expression, implicating a loss of the epithelial phenotype. All the other cases possessed either a hybrid phenotype, co-expressing both E-cadherin and Vimentin or an epithelial phenotype, expressing only E-cadherin. Interestingly, 21 of 30 cases displayed concurrent E-cadherin and vimentin expression. This high proportion of cases positive for both E-cadherin and vimentin is also reported in the literature in the serous subtype of ovarian carcinomas[27].
As far as SOX11 is concerned, only four study groups have to date examined the role of SOX11 as an epithelial ovarian cancer biomarker in terms of tumor metastasis and patient survival. In 2009, Brennan et al. were the first to describe SOX11 as a prognostic factor for enhanced recurrence-free survival in epithelial ovarian cancer after controlling for tumor stage and grade, with the loss of SOX11 correlating with a diminished recurrence-free survival as well as a more aggressive phenotype[28]. Two years later, Sernbo et al. reported that SOX11 expression accounts for an improved survival of patients with high grade epithelial ovarian cancer, depending on cancer stage[29]. Davidson et al. could not, however, identify SOX11 as a marker of longer survival in serous ovarian cancer effusions[30]. Last but not least, Fang et al. suggested that ovarian cancer cell proliferation and invasion were inhibited by SOX11 overexpression, indicating that miR-223-3p controls ovarian cancer cell growth and invasion by specifically targeting SOX11 expression[31].
In the present study, we were able to show that SOX11 seems to positively correlate with a metastatic disease at the time of diagnosis, but not with FIGO-stage, tumor grade, or patients’ survival. Moreover, a negative correlation was noted between E-Cadherin and SOX11 expression, and a positive correlation between Vimentin and SOX11 expression. In this regard, the results of our study for the first time highlight the fact that SOX11 overexpression could play a role in the promotion of EMT in serous ovarian cancer, hence stimulating tumor metastasis. A similar observation has been reportedly made in breast cancer, in which SOX11 seems to promote epithelial/mesenchymal hybrid state and alter tropism of invasive breast cancer cells, also enhancing tamoxifen resistance[21,32]. The hybrid EMT state gives tumor cells the advantage of acquiring the mesenchymal characteristics without the complete loss of epithelial characteristics. Thus, the tumor cells can attach to the ECM with increased connectivity[33], which is why cells in partial EMT states exhibit greater metastatic competence than cells that have an epithelial or mesenchymal phenotype. This relationship was also observed in this project with the association between low expression of E-cadherin and positive expression of SOX11 with the presence of metastasis. There is evidence that the hybrid states of EMT may be triggered by calcium signaling[34]. In addition, tumor cells in the partial EMT state are thought to not only enhance the invasive properties of the cell, but also generate circulating tumor cells and cancer stem cells, as well as promote anticancer drug resistance. The phenotypic changes that allow cells to adopt a hybrid EMT state are regulated by extracellular matrix components, exosomes, and soluble factors. These in turn regulate multiple EMT transcription factors[33]. These previous assumptions and findings about EMT highlight the complexity of the topic.
Notably, our observations are contradictory to the aforementioned results of the previous studies in ovarian cancer[28,29,30,31]. Brennan et al. used an in silico transcriptomic screen and evaluated SOX11 expression using IHC and automated algorithms in 76 epithelial ovarian cancer cases, hence concluding that SOX11 loss correlates with a decreased recurrence-free survival and a more aggressive phenotype[28]. Sernbo et al. compared SOX11 expression and clinicopathological data in a cohort of 154 primary invasive epithelial ovarian cancer cases of several histological types, including mucinous and endometrial carcinoma, and suggested that SOX11 expression was associated with an improved survival of patients with high grade epithelial ovarian cancer, depending on cancer stage[29]. Furthermore, Davidson et al. assessed the expression of E-cadherin, vimentin and SOX11 in 100 advanced-stage serous ovarian carcinoma effusions using IHC and reported that only vimentin expression was significantly related to poor chemotherapy response at diagnosis[30]. Last but not least, Fang et al. highlighted that the SOX11 mRNA expression is significantly lower in the ovarian cancer cell lines SKOV3, OVCAR3, A2780, and ES2, compared to the HOSE normal ovarian cell line, and that the SOX11 mRNA expression is also significantly downregulated in ovarian cancer than in normal tissues[31]. This discrepancy might be attributed to the different study populations (cell lines vs. patients, size of patient collectives, absence of control group, histopathological ovarian cancer subtype), the employed study methods (IHC vs. Western Blot) and/or the preferred statistical testing methods.
The results of our study are only preliminary and, by no means, allow for generalized conclusions on the role of SOX11 as a biomarker for serous ovarian carcinoma. Given the small patient number, our findings undoubtedly represent an interesting observation concerning the role of SOX11 as a potential biomarker for metastatic serous ovarian cancer, but still need to be studied in larger study populations in order to be further verified and avoid statistical errors due to study sample size.
In summary, we report, for the first time, the potential role of E-cadherin and SOX11 as biomarkers for serous ovarian cancer with a special focus on EMT and distant metastasis. Our findings may, hence, pave the way for the identification of novel biomarkers in the context of advanced (serous) ovarian cancer diagnosis and treatment.
Author Contributions
I.P. Writing—Original Draft Preparation J.I.S. Investigation, Resources; D. A. Investigation (Data collection); D. B. Investigation, Resources; G. L. Conceptualization, Investigation, Writing—Review and Editing, Formal analysis, Supervision. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and it was approved by the Bioethics Committee of the Paracelsus medical University (April 2022).
Informed Consent Statement
Not applicable. Due to the retrospective nature of the studies and the lack of impact on the treatment of patients, it was not necessary to obtain informed consent.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Society AC. Key Statistics for Ovarian Cancer: American Cancer Society 2023 [Available from: https://www.cancer.org/cancer/types/ovarian-cancer/about/key-statistics.html.
- Prat J. Ovarian carcinomas: five distinct diseases with different origins, genetic alterations, and clinicopathological features. Virchows Arch. 2012;460(3):237-49.
- Seebacher V, Reinthaller A, Koelbl H, Concin N, Nehoda R, Polterauer S. The Impact of the Duration of Adjuvant Chemotherapy on Survival in Patients with Epithelial Ovarian Cancer - A Retrospective Study. PLoS One. 2017;12(1):e0169272.
- Psilopatis I, Sykaras AG, Mandrakis G, Vrettou K, Theocharis S. Patient-Derived Organoids: The Beginning of a New Era in Ovarian Cancer Disease Modeling and Drug Sensitivity Testing. Biomedicines. 2022;11(1).
- Society AC. Survival Rates for Ovarian Cancer: American Cancer Society 2023 [Available from: https://www.cancer.org/cancer/types/ovarian-cancer/detection-diagnosis-staging/survival-rates.html.
- Society AC. Tests for Ovarian Cancer: American Cancer Society; 2022 [Available from: https://www.cancer.org/cancer/types/ovarian-cancer/detection-diagnosis-staging/how-diagnosed.html.
- Kalluri R, Neilson EG. Epithelial-mesenchymal transition and its implications for fibrosis. J Clin Invest. 2003;112(12):1776-84.
- Kalluri R, Weinberg RA. The basics of epithelial-mesenchymal transition. J Clin Invest. 2009;119(6):1420-8.
- Yang J, Weinberg RA. Epithelial-mesenchymal transition: at the crossroads of development and tumor metastasis. Dev Cell. 2008;14(6):818-29.
- Brabletz T, Jung A, Reu S, Porzner M, Hlubek F, Kunz-Schughart LA, Knuechel R, Kirchner T. Variable beta-catenin expression in colorectal cancers indicates tumor progression driven by the tumor environment. Proc Natl Acad Sci U S A. 2001;98(18):10356-61.
- Fidler IJ, Poste G. The "seed and soil" hypothesis revisited. Lancet Oncol. 2008;9(8):808.
- Thiery JP. Epithelial-mesenchymal transitions in tumour progression. Nat Rev Cancer. 2002;2(6):442-54.
- Lefebvre V, Dumitriu B, Penzo-Mendez A, Han Y, Pallavi B. Control of cell fate and differentiation by Sry-related high-mobility-group box (Sox) transcription factors. Int J Biochem Cell Biol. 2007;39(12):2195-214.
- Penzo-Mendez AI. Critical roles for SoxC transcription factors in development and cancer. Int J Biochem Cell Biol. 2010;42(3):425-8.
- de Bont JM, Kros JM, Passier MM, Reddingius RE, Sillevis Smitt PA, Luider TM, den Boer ML, Pieters R. Differential expression and prognostic significance of SOX genes in pediatric medulloblastoma and ependymoma identified by microarray analysis. Neuro Oncol. 2008;10(5):648-60.
- Jay P, Goze C, Marsollier C, Taviaux S, Hardelin JP, Koopman P, Berta P. The human SOX11 gene: cloning, chromosomal assignment and tissue expression. Genomics. 1995;29(2):541-5.
- Harrison G, Hemmerich A, Guy C, Perkinson K, Fleming D, McCall S, Cardona D, Zhang X. Overexpression of SOX11 and TFE3 in Solid-Pseudopapillary Neoplasms of the Pancreas. Am J Clin Pathol. 2017;149(1):67-75.
- Weigle B, Ebner R, Temme A, Schwind S, Schmitz M, Kiessling A, Rieger MA, Schackert G, Schackert HK, Rieber EP. Highly specific overexpression of the transcription factor SOX11 in human malignant gliomas. Oncol Rep. 2005;13(1):139-44.
- Zhang LN, Cao X, Lu TX, Fan L, Wang L, Xu J, Zhang R, Zou ZJ, Wu JZ, Li JY, et al. Polyclonal antibody targeting SOX11 cannot differentiate mantle cell lymphoma from B-cell non-Hodgkin lymphomas. Am J Clin Pathol. 2013;140(6):795-800.
- Shepherd JH, Uray IP, Mazumdar A, Tsimelzon A, Savage M, Hilsenbeck SG, Brown PH. The SOX11 transcription factor is a critical regulator of basal-like breast cancer growth, invasion, and basal-like gene expression. Oncotarget. 2016;7(11):13106-21.
- Oliemuller E, Newman R, Tsang SM, Foo S, Muirhead G, Noor F, Haider S, Aurrekoetxea-Rodriguez I, Vivanco MD, Howard BA. SOX11 promotes epithelial/mesenchymal hybrid state and alters tropism of invasive breast cancer cells. Elife. 2020;9.
- Meinhold-Heerlein I, Fotopoulou C, Harter P, Kurzeder C, Mustea A, Wimberger P, Hauptmann S, Sehouli J, Kommission Ovar of the AGO. Statement by the Kommission Ovar of the AGO: The New FIGO and WHO Classifications of Ovarian, Fallopian Tube and Primary Peritoneal Cancer. Geburtshilfe Frauenheilkd. 2015;75(10):1021-7.
- Huh S, Kang C, Park JE, Nam D, Kim SI, Seol A, Choi K, Hwang D, Yu MH, Chung HH, et al. Novel Diagnostic Biomarkers for High-Grade Serous Ovarian Cancer Uncovered by Data-Independent Acquisition Mass Spectrometry. J Proteome Res. 2022;21(9):2146-59.
- Atallah GA, Abd Aziz NH, Teik CK, Shafiee MN, Kampan NC. New Predictive Biomarkers for Ovarian Cancer. Diagnostics (Basel). 2021;11(3).
- Loh CY, Chai JY, Tang TF, Wong WF, Sethi G, Shanmugam MK, Chong PP, Looi CY. The E-Cadherin and N-Cadherin Switch in Epithelial-to-Mesenchymal Transition: Signaling, Therapeutic Implications, and Challenges. Cells. 2019;8(10).
- Na TY, Schecterson L, Mendonsa AM, Gumbiner BM. The functional activity of E-cadherin controls tumor cell metastasis at multiple steps. Proc Natl Acad Sci U S A. 2020;117(11):5931-7.
- Loret N, Denys H, Tummers P, Berx G. The Role of Epithelial-to-Mesenchymal Plasticity in Ovarian Cancer Progression and Therapy Resistance. Cancers (Basel). 2019;11(6).
- Brennan DJ, Ek S, Doyle E, Drew T, Foley M, Flannelly G, O'Connor DP, Gallagher WM, Kilpinen S, Kallioniemi OP, et al. The transcription factor Sox11 is a prognostic factor for improved recurrence-free survival in epithelial ovarian cancer. Eur J Cancer. 2009;45(8):1510-7.
- Sernbo S, Gustavsson E, Brennan DJ, Gallagher WM, Rexhepaj E, Rydnert F, Jirstrom K, Borrebaeck CA, Ek S. The tumour suppressor SOX11 is associated with improved survival among high grade epithelial ovarian cancers and is regulated by reversible promoter methylation. BMC Cancer. 2011;11:405.
- Davidson B, Holth A, Hellesylt E, Tan TZ, Huang RY, Trope C, Nesland JM, Thiery JP. The clinical role of epithelial-mesenchymal transition and stem cell markers in advanced-stage ovarian serous carcinoma effusions. Hum Pathol. 2015;46(1):1-8.
- Fang G, Liu J, Wang Q, Huang X, Yang R, Pang Y, Yang M. MicroRNA-223-3p Regulates Ovarian Cancer Cell Proliferation and Invasion by Targeting SOX11 Expression. Int J Mol Sci. 2017;18(6).
- Xiao Y, Xie Q, Qin Q, Liang Y, Lin H, Zeng D. Upregulation of SOX11 enhances tamoxifen resistance and promotes epithelial-to-mesenchymal transition via slug in MCF-7 breast cancer cells. J Cell Physiol. 2020;235(10):7295-308.
- Saitoh M. Involvement of partial EMT in cancer progression. J Biochem. 2018;164(4):257-64.
- Norgard RJ, Pitarresi JR, Maddipati R, Aiello-Couzo NM, Balli D, Li J, Yamazoe T, Wengyn MD, Millstein ID, Folkert IW, et al. Calcium signaling induces a partial EMT. EMBO Rep. 2021;22(9):e51872.
Figure 1.
E-Cadherin, SOX11 and Vimentin expression in ovarian serous caricnomas. (A, B, C) A high grade serous carcinoma with loss of E-Cadherin (A, x400) and increased expression of SOX11 (B, x400) and Vimentin (C, x400), (D-F) A high grade serous carcinoma with expression of E-Cadherin (D, x200), SOX11 (E, x200) and Vimentin (F, 400).
Figure 1.
E-Cadherin, SOX11 and Vimentin expression in ovarian serous caricnomas. (A, B, C) A high grade serous carcinoma with loss of E-Cadherin (A, x400) and increased expression of SOX11 (B, x400) and Vimentin (C, x400), (D-F) A high grade serous carcinoma with expression of E-Cadherin (D, x200), SOX11 (E, x200) and Vimentin (F, 400).
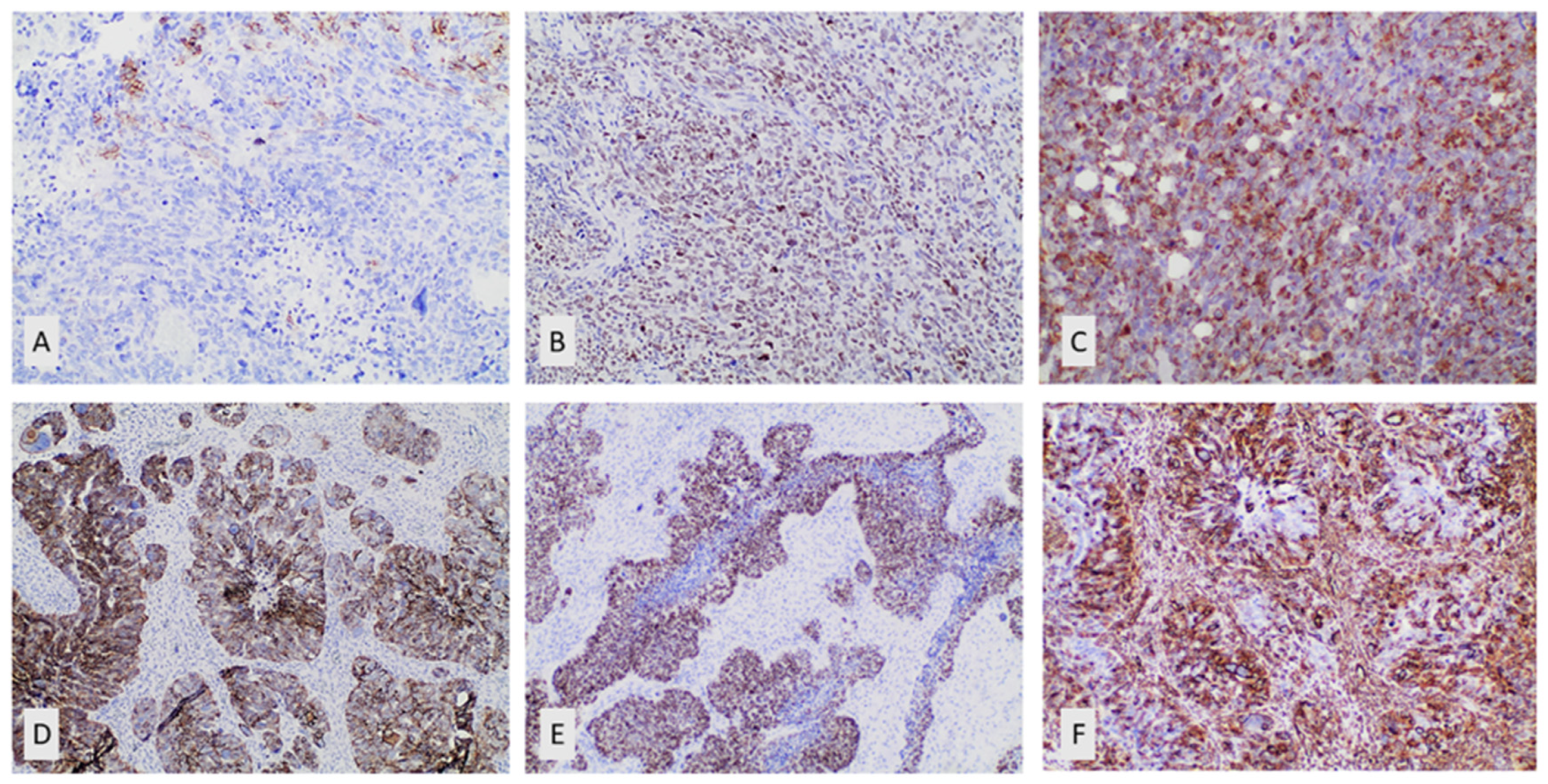
Figure 2.
Schematic representation of the association between E-cadherin expression and presence of metastasis.
Figure 2.
Schematic representation of the association between E-cadherin expression and presence of metastasis.
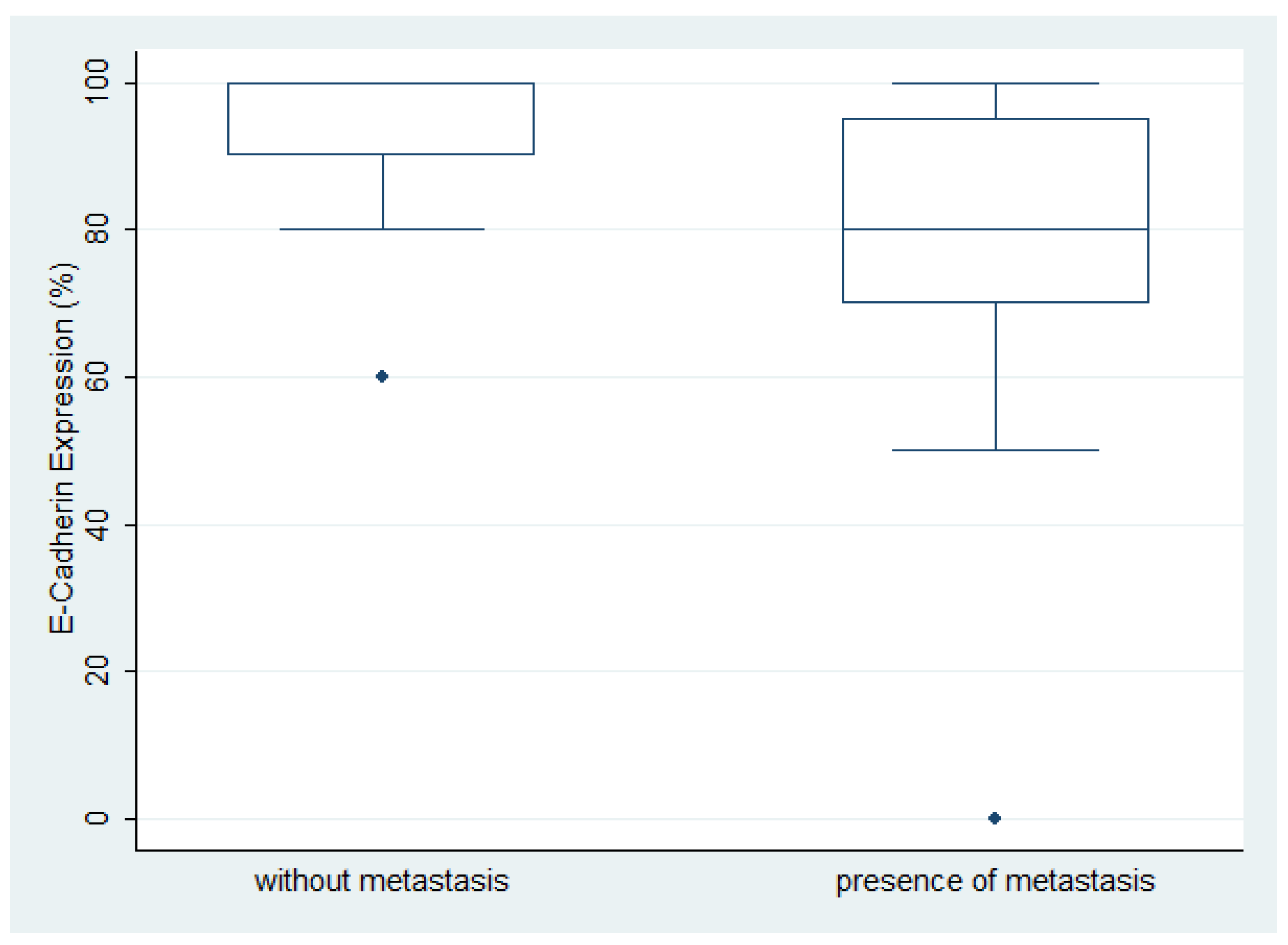
Figure 3.
Schematic representation of the association between SOX11 positivity and the presence of metastasis.
Figure 3.
Schematic representation of the association between SOX11 positivity and the presence of metastasis.
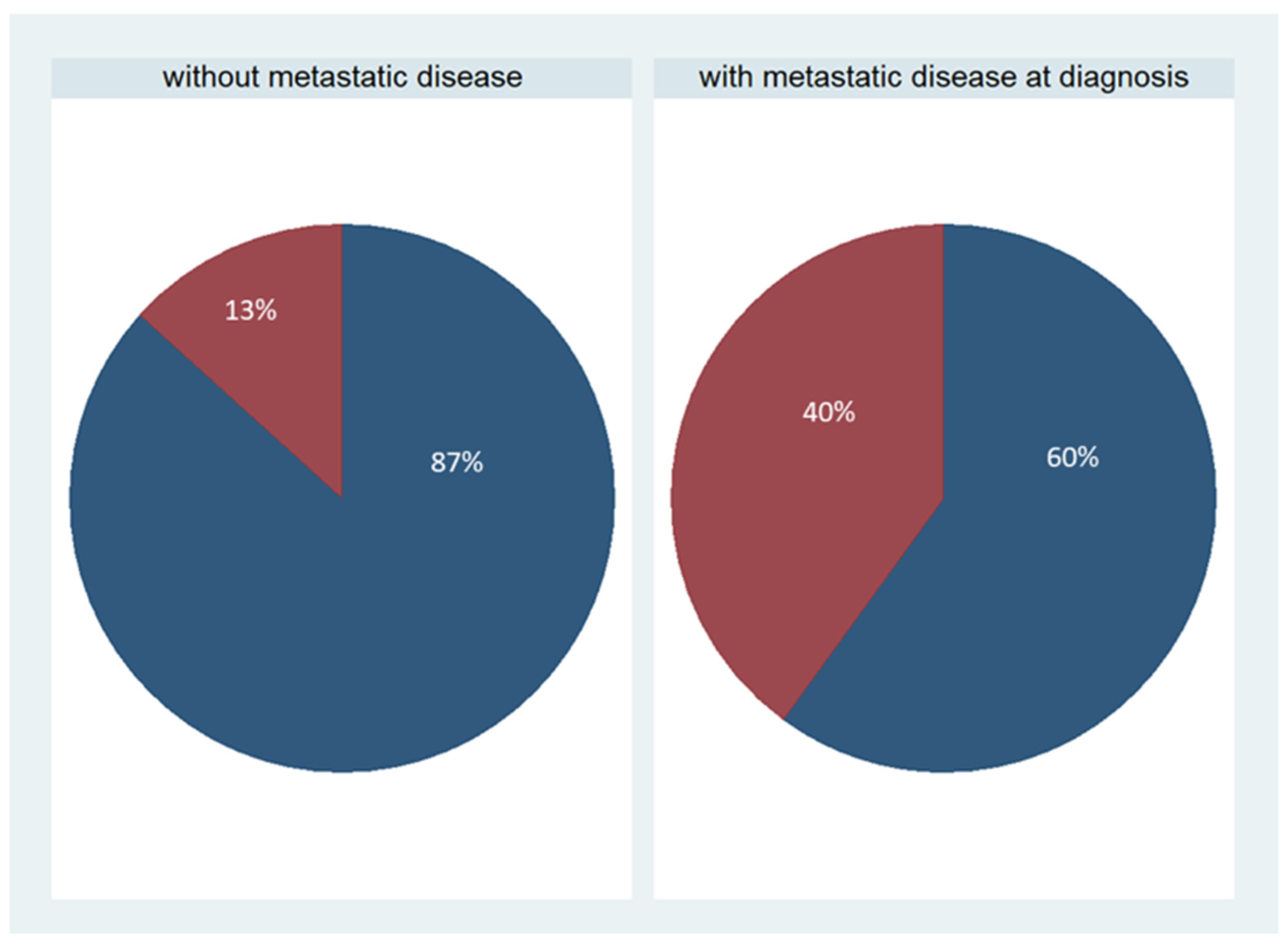

Table 1.
Patients’ characteristics.
| Patients’ characteristics | Median value | Value range |
|---|---|---|
| Age (in years) | 61,5 | 46-92 |
| FIGO stadium | Number of patients | Percentage |
| I | 7 | 23% |
| II | 3 | 10% |
| III | 11 | 37% |
| IV | 9 | 30% |
| Tumor grade | Number of patients | Percentage |
| Low grade | 5 | 17% |
| High grade | 25 | 83% |
| Metastasis | Number of patients | Percentage |
| Metastatic cancer | 15 | 50% |
| Non-metastatic cancer | 15 | 50% |
| Residual disease | ||
| None/minimal | 25 | 83% |
| >2cm | 5 | 17% |
| Event | Number of patients | Percentage |
| Death of disease | 6/21 (follow-up: 3,4-35 months) | 28% |
| Censored | 15/21 (follow-up: 5-68 months) | 71% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



