Submitted:
08 August 2023
Posted:
09 August 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
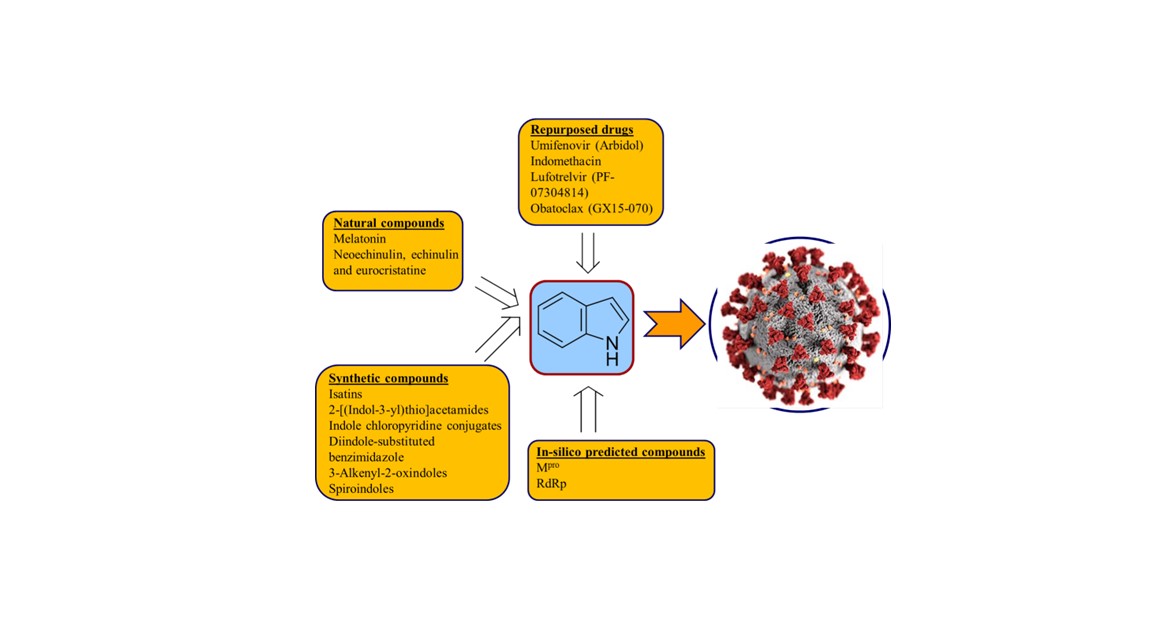
The COVID-19 pandemic has posed a significant threat to society in recent times, endangering human health, life, and economic well-being. The disease spreads quickly due to the highly infectious SARS-CoV-2 virus, which has undergone numerous mutations. Despite intense research efforts by the scientific community since its emergence in 2019, no effective therapeutics have been discovered yet. While some repurposed drugs have been used to control the global outbreak and save lives, none have proven universally effective, particularly for severely infected patients. Although the spread of the disease is generally under control, anti-SARS-CoV-2 agents are still needed to combat current and future infections. This study reviews some of the most promising repurposed drugs containing indolyl heterocycle, which is an essential scaffold of many alkaloids with diverse bio-properties in various biological fields. The study also discusses natural and synthetic indole-containing compounds with anti-SARS-CoV-2 properties, as well as computer-aided drug design (in-silico studies) for optimizing anti-SARS-CoV-2 hits/leads.
Keywords:
Indole
; COVID-19
; SARS-CoV-2
; Alkaloids
; Natural
; Synthetic
; In-silico
1. Introduction
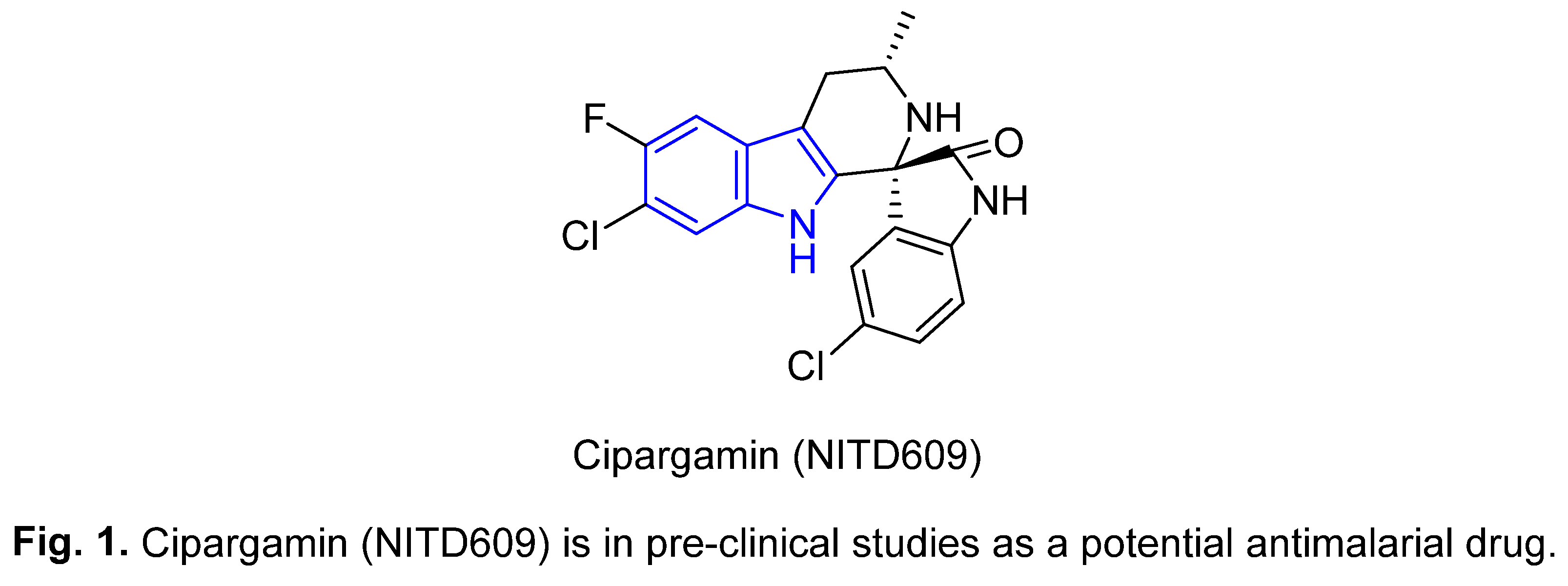
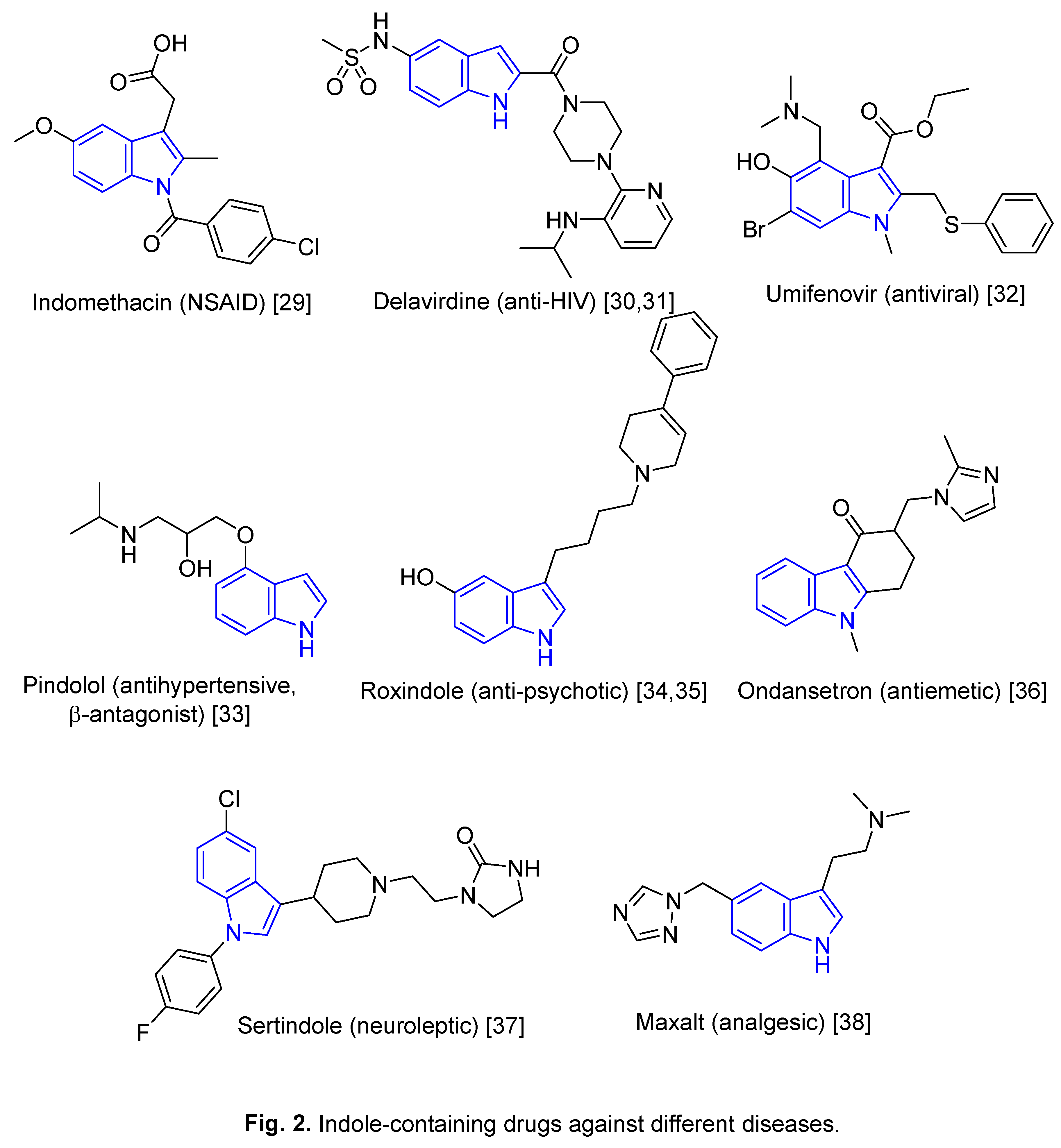
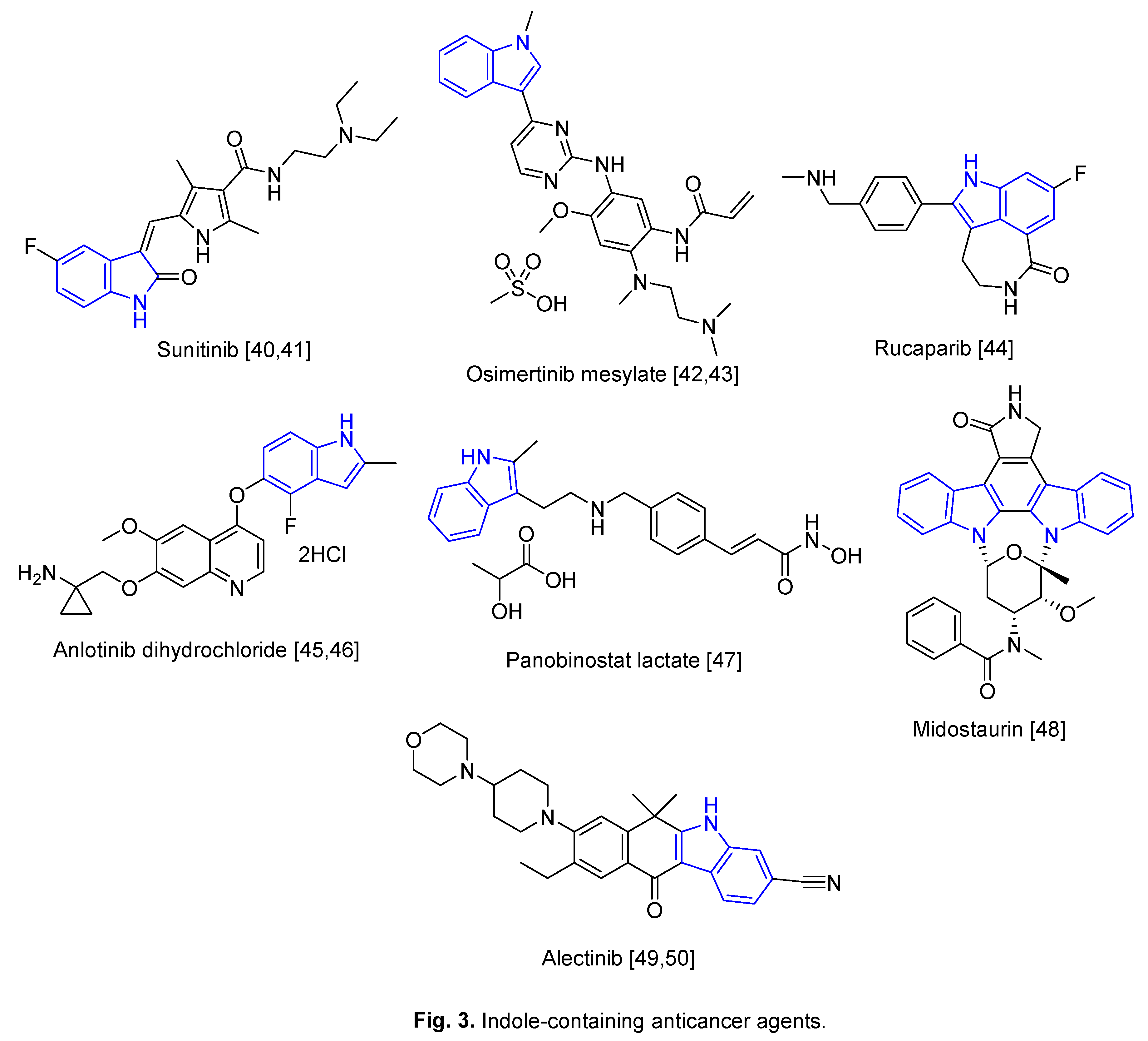
The indole moiety is one of the most privileged scaffolds in the alkaloid category. Indole-containing compounds are widely distributed in plants, animals, and microorganisms and represent important pharmacophores that can bind with receptors controlling bio-properties [1]. Diverse biological properties have been exhibited by natural and synthetic indole-containing analogs, including anti-microorganism activities such as antimicrobial [2‒5], antifungal [6‒8], antiviral [9‒14], and mycobacterial [15] action. Cipargamin (Figure 1), which has an indolyl scaffold, has been identified as a potent inhibitor of protein synthesis in Plasmodium falciparum and has subsequently progressed to pre-clinical trials as a potential antimalarial drug [16]. A range of other potential antimalarial candidates with the indolyl scaffold have additionally been reported [17‒20]. Anti-diabetic [21,22] and anti-inflammatory [23‒27] properties have also been observed for indole derivatives. Figure 2 presents some of the indole-containing drugs approved for the treatment of a range of conditions [1,2,28]. Indole-based anticancer drugs and potent agents [28,39] are illustrated in Figure 3 and many indolyl analogs identified as antitumor-active candidates have also been reported [51‒57].
The coronavirus disease 2019 (COVID-19) has proved to be one of the most serious crises facing human health in recorded history. The disease is caused by the fast-spreading infectious virus, SARS-CoV-2 (severe acute respiratory syndrome coronavirus-2) transmitted between humans, and threatened human life worldwide. Until 2019, the virus strain had not been reported as being invasive among humans [58]. The first infection was initially linked to a fish and wild animal market in Wuhan City, China at the end of 2019 before the disease spread dramatically, within a few weeks, to almost all countries of the world affecting millions of people [59]. The World Health Organization (WHO) declared a global severe emergency and pandemic in March 2020 [60]. To date (July 5, 2023) WHO statistics indicate officially counted/confirmed 767.7 million infected patients with 6.949 million deaths globally [61].
The symptoms of COVID-19 are similar to many other conditions and seasonal diseases (flu is an example) and include cough, runny nose, mild fever, and headache. Breathing difficulties, chest pain, and hypertension occur in severe infections that require hospitalization in intensive care and oxygen supply [62,63]. The pandemic placed many countries under unprecedented economic pressure due to the curtailment of normal social activities that affected a significant amount of the global population. The wide scientific community, including research institutes, universities, and pharmaceutical companies devoted considerable resources to the study of the cell biology of SARS-CoV-2, the identification of diagnostic agents, and the optimization of effective therapeutics [64].
SARS-CoV-2 is a zoonotic virus of single-strand RNA (ssRNA(+)), covered by glycoprotein spikes and belonging to the Coronaviridae family. It is mostly found in bats but, for unknown reasons, was transmitted to the human species leading to the global pandemic. The viral RNA genetic material is capable of acting directly as viral messenger RNA producing the viral protein inside the host cell [65‒68]. Numerous waves of viral mutations were detected, potentially affecting transmissibility and severity in humans. Delta (B.1.617) and Delta plus (B.1.617.2) are more deadly and infectious than the other mutations (for example, Alpha, B.1.1.7; Beta, B.1.351; or Gamma, P.1) [62]. Omicron is more extensively mutated and was detected in November 2021 with the viral wave spreading widely around the world. Although it has a higher risk of infection/reinfection, it has milder symptoms and lower fatality in vaccinated people. This may be a factor in the pandemic transitioning to an epidemic [69].
Vaccination is one of the most important means for controlling the development of a pandemic and saving human lives. The neutralizing antibodies formed due to vaccination can provide protection against viral infection or at least result in milder/weaker symptoms upon infection. In the case of COVID-19, BNT162b2 (Pfizer/BioNTech), mRNA-1273 (Moderna), and AZD1222 (University of Oxford & AstraZeneca) have been the most prominent vaccines discovered and used globally [60,69]. Herd immunity is the aim of large-scale vaccination and it may limit the extent of infection and terminate a global pandemic. In the case of COVID-19, evidence for the acquired immunity in recovered patients was limited, thereby raising questions about the herd immunity hypothesis. Consequently, the acquired immunity due to vaccination antibodies is not certain against infection/re-infection [59,70].
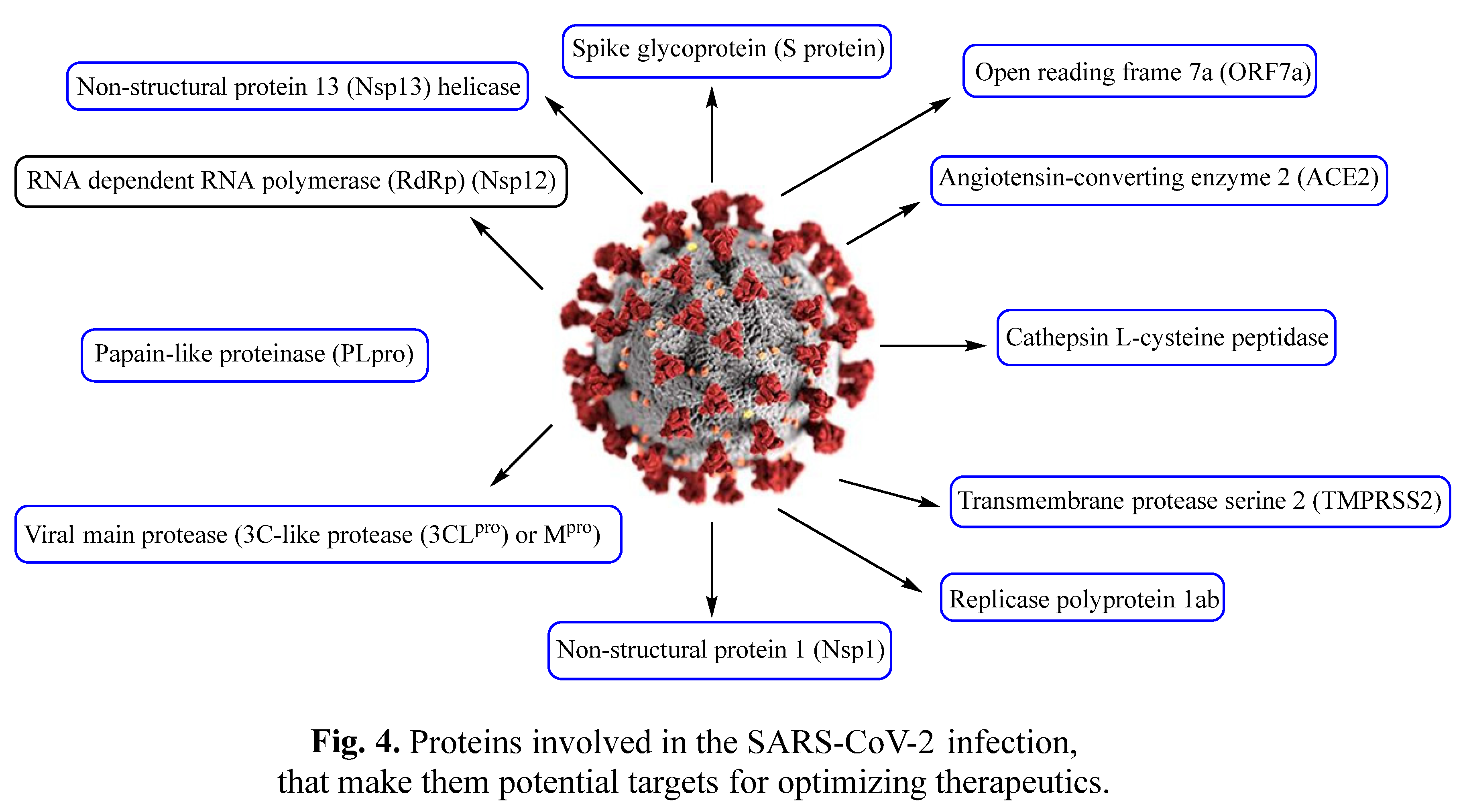
Biochemical studies have identified some proteins involved in SARS-CoV-2 infections (Figure 4 summarizes some) [71] and thus are potential targets for controlling the infection and optimizing potential therapeutics.
The emerging healthcare crisis due to the global outbreak due to the pathogenic SARS-CoV-2 virus united the scientific community and the pharmaceutical industry in a race against time in the search and optimization of any medicinal entity/device/therapeutic capable of controlling the spread of COVID-19 and bringing back normality [72]. De-novo drug development usually follows several successive steps. The first is the discovery of potent and safe agents from among many candidates. Preclinical studies support the biochemical mode of action and applicability of the agents as potentially therapeutic. Clinical trials are essential for the assessment of success and identification of side effects. The post-marketing safety monitoring step is necessary for the continuation of the new therapeutics as one of the available medications. Drug development is therefore time-consuming and costly, requiring about 10‒15 years and millions of dollars to progress from pre-identification of the potent/lead compound through to the medical store. Only about 10% of the potential agents are successful ]73‒75].
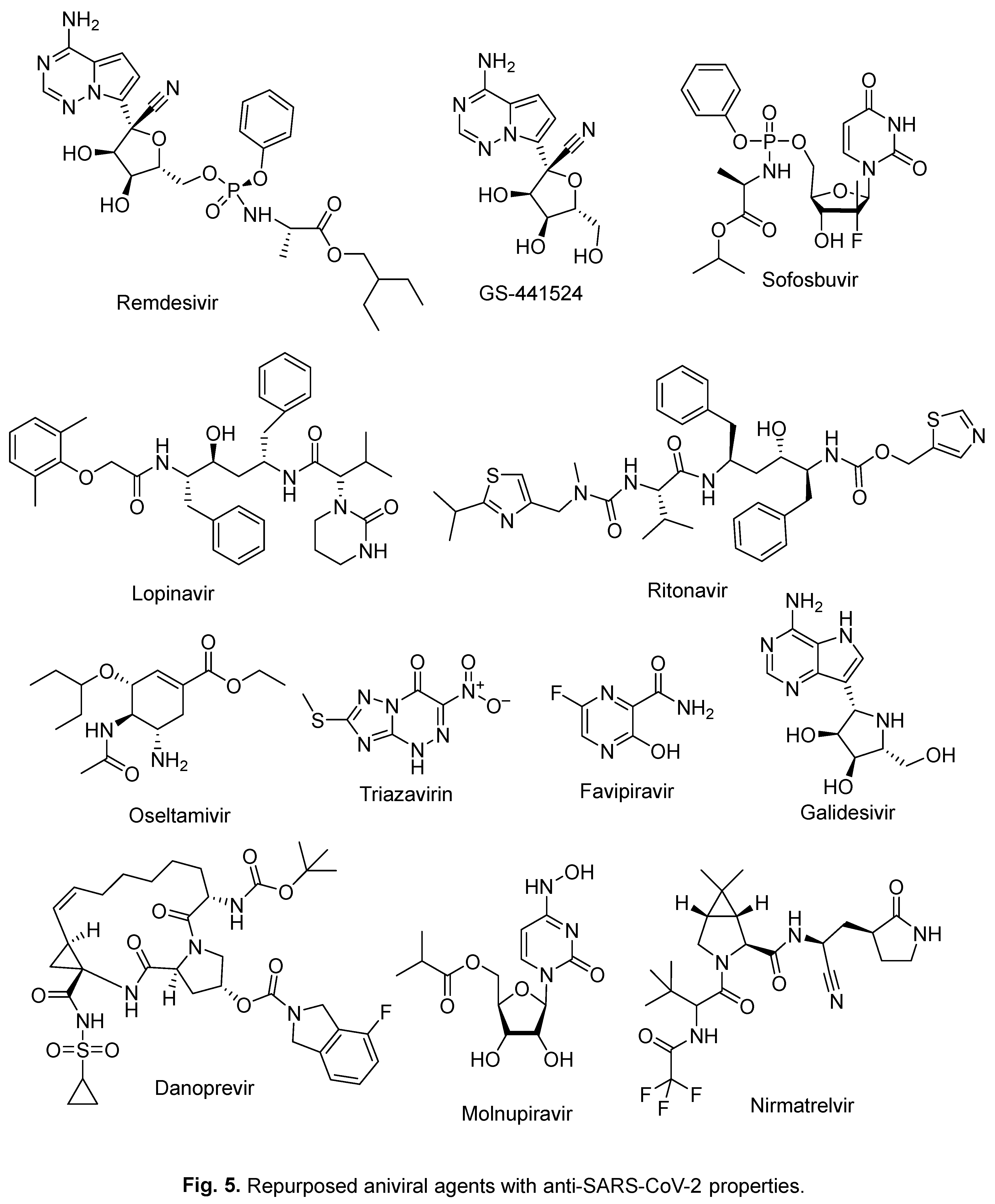
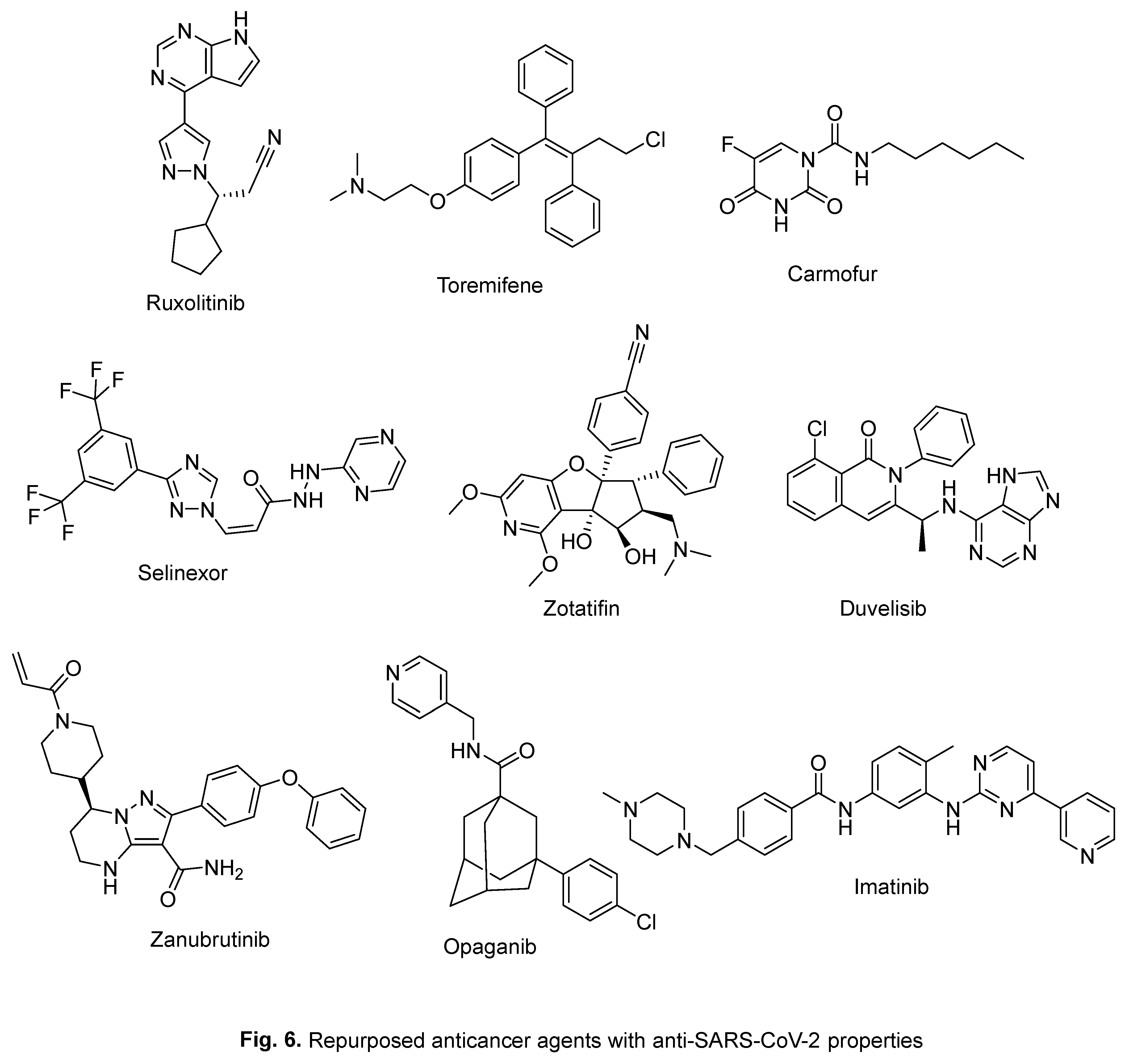
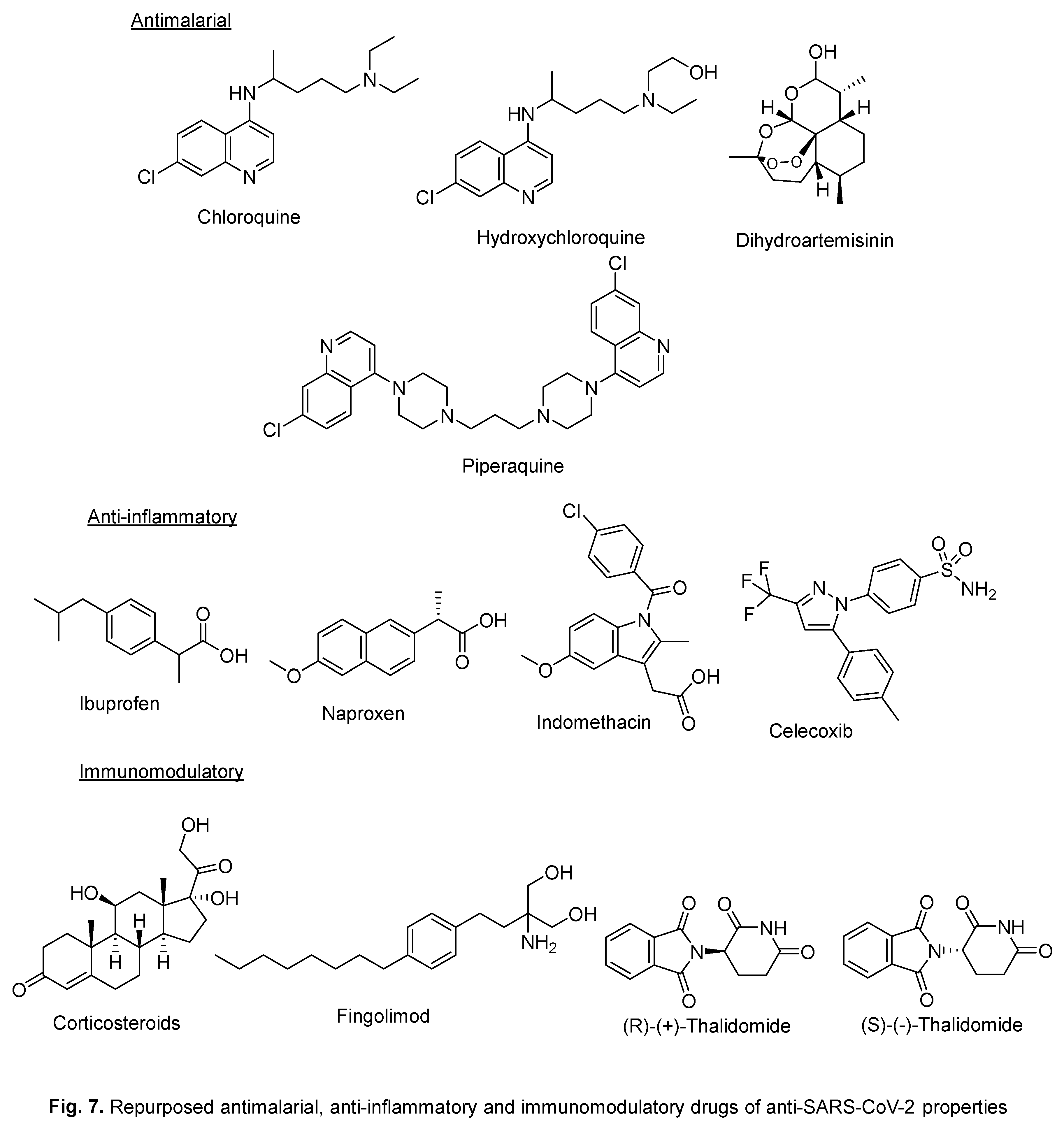
In-silico studies utilizing various techniques/software can assist in assigning anti-SARS-CoV-2 agents. This may shorten the time needed for identifying potential entities to be submitted for in-vitro/in-vivo testing followed by the clinical trial(s) phases. In other words, in-silico studies are a shortcut to attaining the final targeted therapeutics, saving the time and money required [76,77]. Additionally, drug repurposing/re-profiling, a strategy that considers the use of approved or investigated drugs for use outside the original therapeutic application, can shorten the period needed due to the well-established safety profile and understood side effects/drawbacks. This approach has many advantages over the development of entirely novel therapeutics, including cost reduction and lower risk [78‒80]. Several antiviral, anticancer, antimalarial, anti-inflammatory, and immunomodulatory active agents/drugs have been repurposed for anti-SARS-CoV-2 application (Figure 5, Figure 6 and Figure 7 mentioned some of them) [63,81,82,83,84,85].
Remdesivir (Figure 5) is a broad-spectrum antiviral agent. It was the first therapeutic granted approval under emergency-use authorization by the Food and Drug Administration (FDA) [9,59,73]. It was originally developed by Gilead Sciences as an anti-Ebola virus agent. It was approved as a COVID-19 therapeutic with RNA-dependent RNA polymerase (RdRp) inhibitory properties due to its ability to be metabolized in the infected/host cell analogs to a nucleoside triphosphate. It is capable of terminating viral replication through RdRp action via integration in the RNA viral chain [9,86]. Molnupiravir (Lagevrio) (Figure 5) was awarded FDA approval in December 2021 [87,88]. It also exerts its anti-SARS-CoV-2 activity via RdRp inhibition [9]. Paxlovid, which is a combination of Nirmatrelvir and Ritonavir (Figure 5), was awarded FDA approval in December 2021 [89]. Ritonavir/Pf-07321332 acts against SARS-CoV-2 through main protease (Mpro) inhibition [83].
Our current discussion builds upon our previous work, which aimed to explore materials with anti-SARS-CoV-2 properties that could potentially aid in identifying agents against COVID-19 [9,66,90‒93]. Specifically, we are examining indole-containing compounds, whether they are naturally occurring or artificially created, that may possess anti-SARS-CoV-2 properties.
2. Repurposed indole-containing drugs
2.1. Umifenovir (Arbidol)
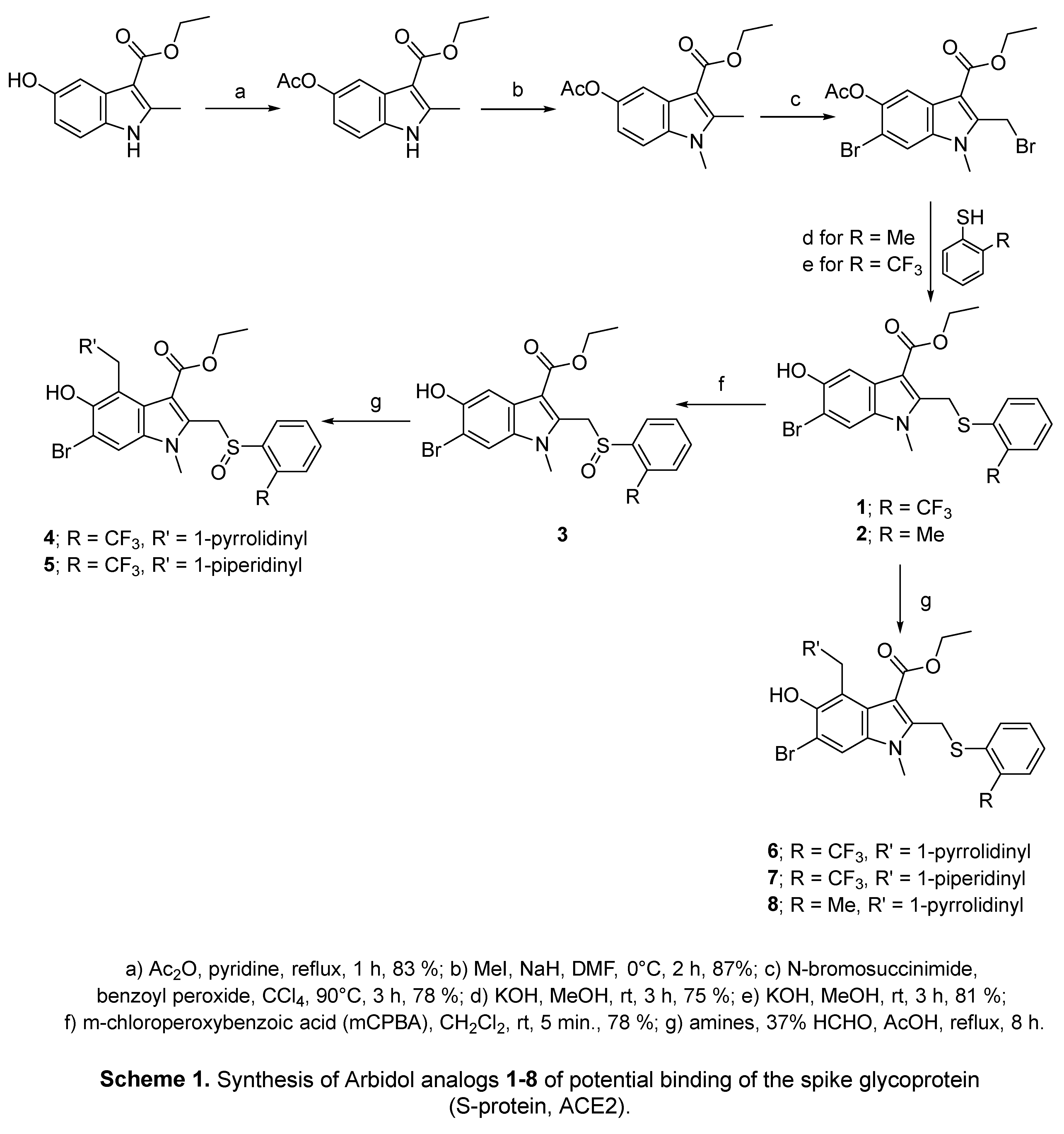
Umifenovir (Arbidol) (Figure 8) is a broad-spectrum antiviral drug with inhibitory properties against both RNA and DNA viruses such as Zika, influenza, hepatitis (HBV, HCV), ebola, West Nile and herpes viruses.94,95 It is one of the drugs that has been repurposed against COVID-19 and has IC50 = 4.11 μM against SARS-CoV-2 [96]. It acts through inhibition of the lipid envelope thereby limiting contact and hence the fusion of the viral cell (membrane fusion inhibitor) with the host/human cell (targeting S-protein/ACE2 “angiotensin-converting enzyme 2”) [97‒100]. Computational studies including molecular docking (PDB ID: 6LZG) [101] and molecular dynamics [102,103] support the mode of action. Antioxidant properties of Arbidol have also been reported to be attributed to its ability to react with free radicals. This may indicate that the anti-SARS-CoV-2 bio-properties of Arbidol are arising from several biochemical pathways [94]. Clinical studies have confirmed the suitability of Arbidol as a monotherapy or in combination with other therapeutics for COVID-19 patients [104‒114]. Some countries (e.g., Russia, China, and Iran [95]), have awarded licenses to Arbidol for the prevention or treatment of COVID-19 [115].

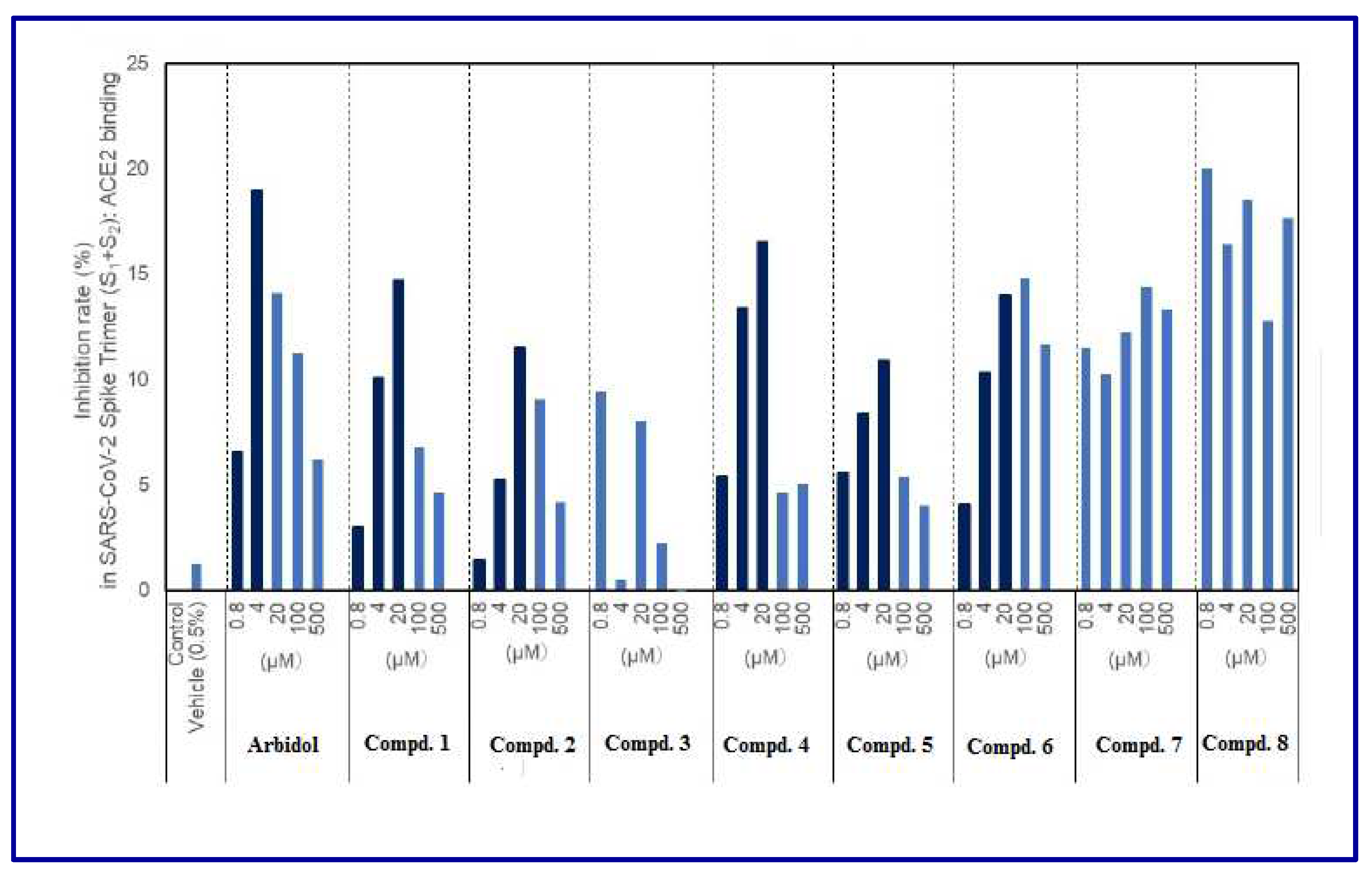
A series of Arbidol analogs 1‒8 have been synthesized starting from 5-hydroxy-2-methylindole-3-carboxylate (Scheme 1). Potential binding of the compounds with the spike glycoprotein (S-protein, ACE2 binding) was determined (Figure 9) revealing no inhibition rates greater than 20%. Some inhibitory properties at low concentrations were higher than others but this can be explained in terms of the low solubility of the compounds in aqueous medium [96].
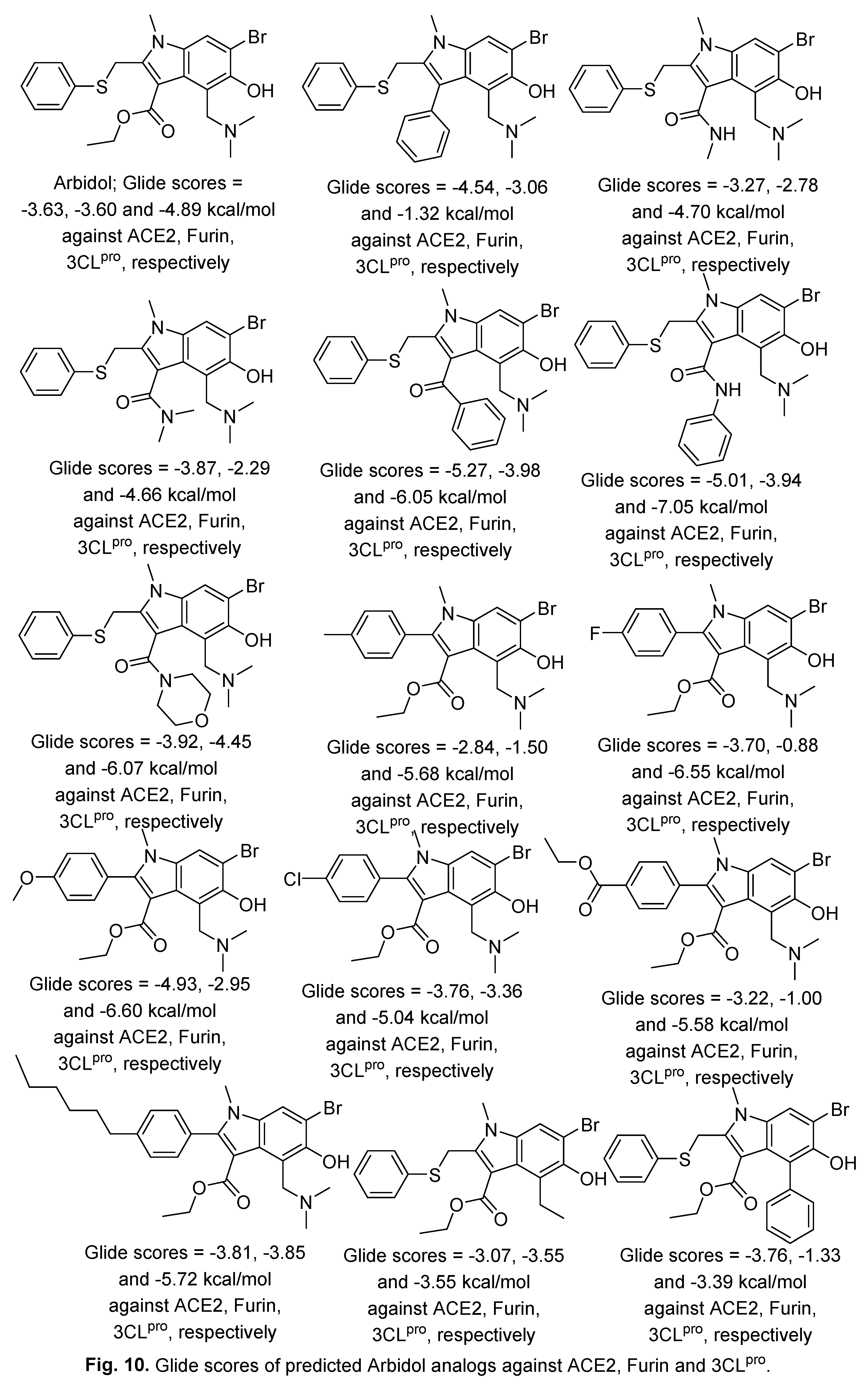
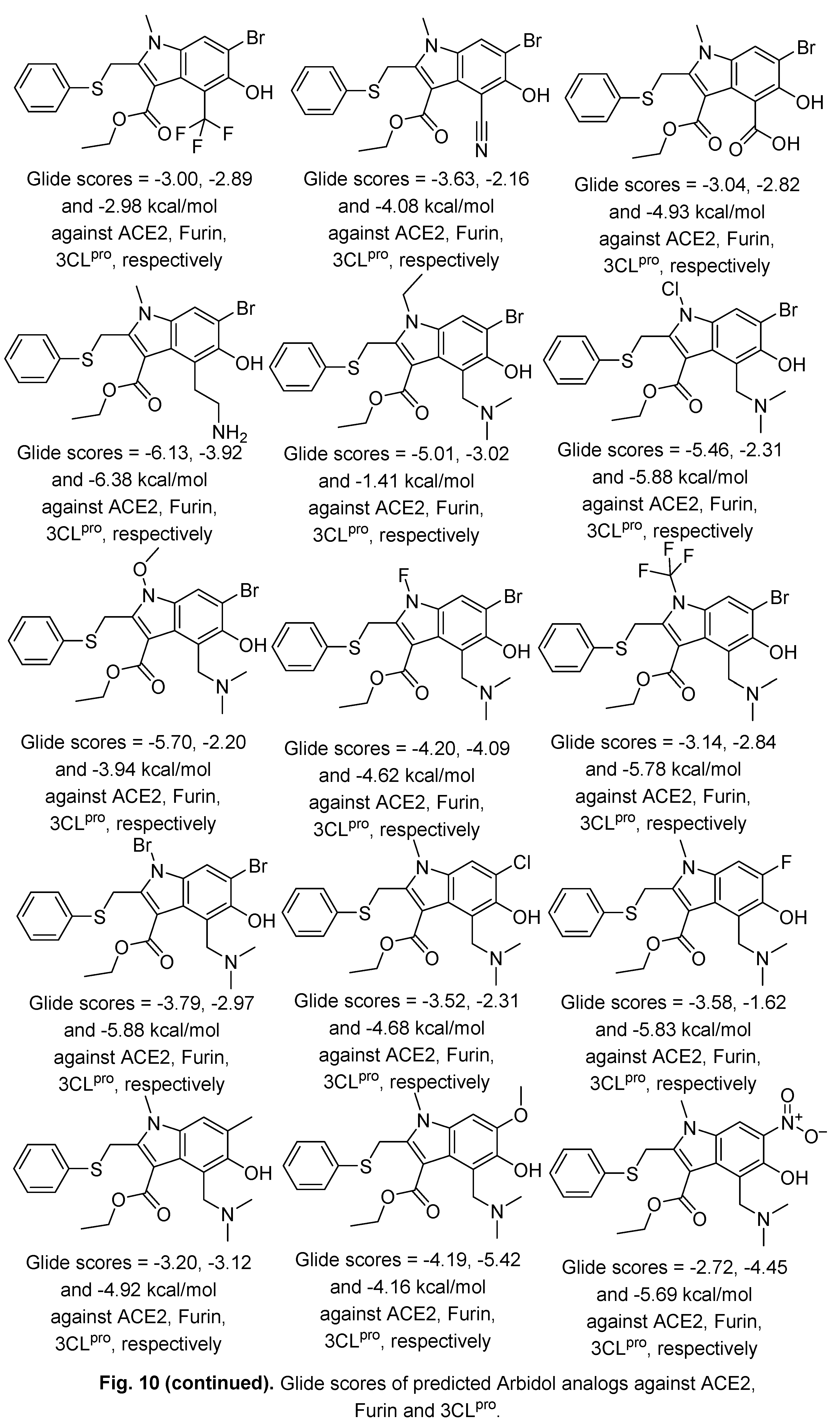
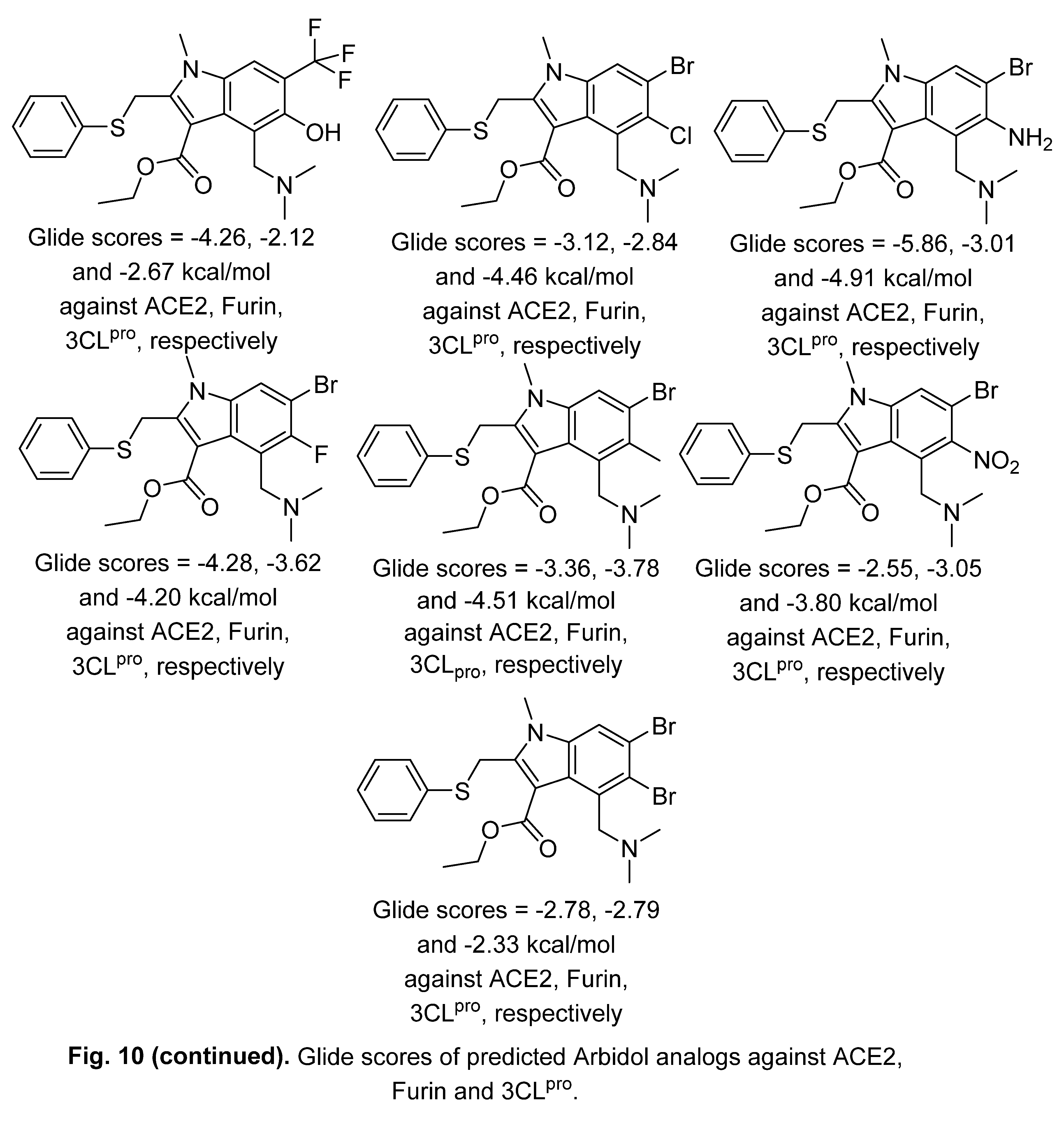
Arbidol analogs have also been designed, through in-silico studies using Schrodinger software, as inhibitors of ACE2, which is the key receptor that facilitates the entrance of the SARS-CoV-2 virus into the host cell (PDB ID: 6LZG) in addition to the proteases like furin (PDB ID: 5MIM), TMPRSS2 (transmembrane protease serine 2), TMPS2 human and 3CLpro (3 chymotrypsin-like protease, PDB ID: 6LU7) which are essential for the viral replication. This approach may enable the optimization of multi-targeted inhibitor agents with potential efficacy against COVID-19, but the lack of experimental bio-properties data limits the progress [116] (Figure 10).
Figure 9.
Inhibitory properties of Arbidol analogs 1‒8.
2.2. Indomethacin
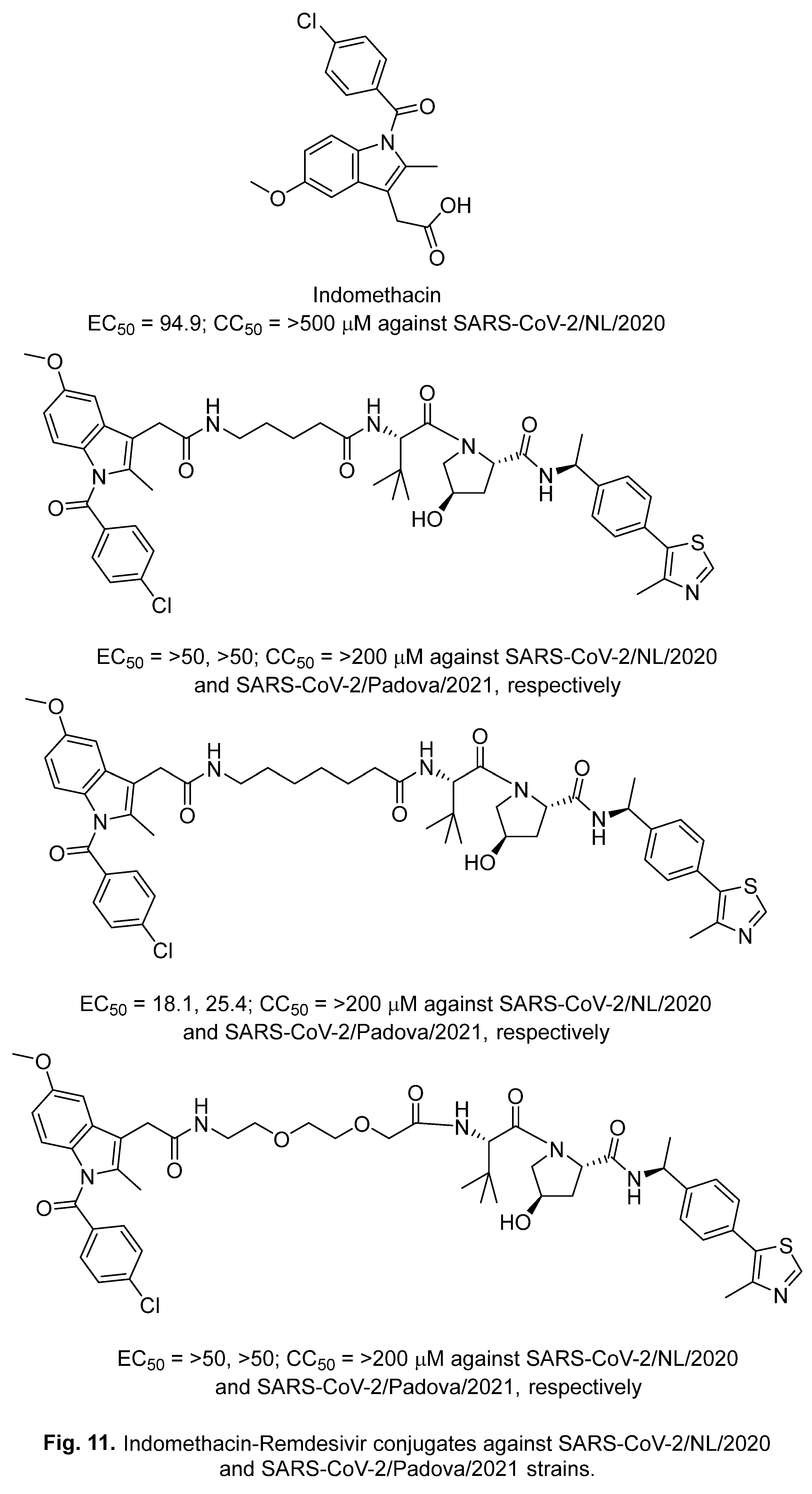
Indomethacin (Figure 7) is a (non-steroidal anti-inflammatory (NSAID), and analgesic drug used globally.29,117,118 It works through non-selective inhibition of cyclooxygenase (COX), which is the key enzyme to produce prostaglandin from arachidonic acid. Prostaglandin is responsible for inflammation and pain [119]. Inflammation is a natural response of the human body due to harmful effects. It is associated with many diseases, including microorganism (bacterial/viral) infections, cancers, and asthma [90].
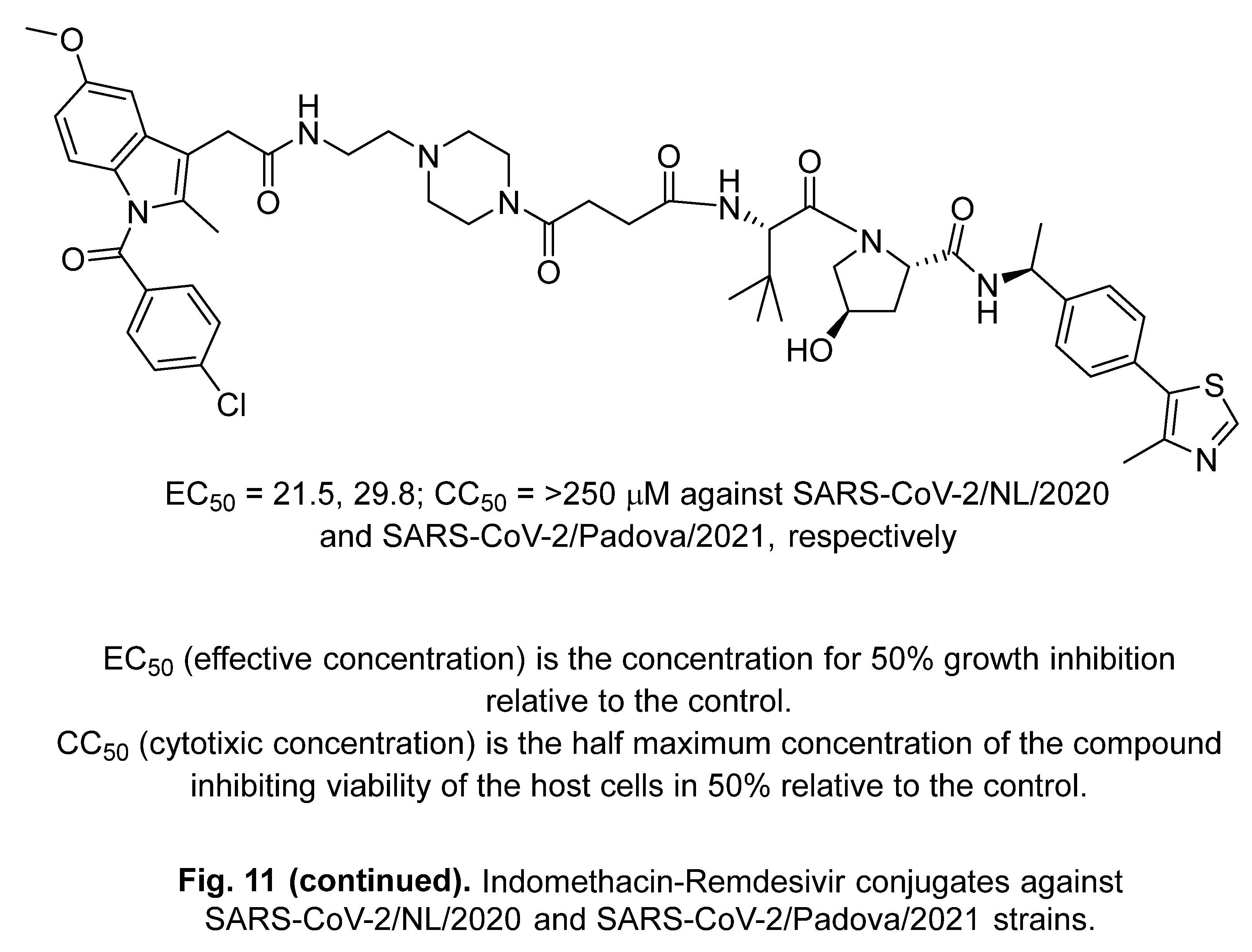
Although indomethacin does not inhibit replication of SARS-CoV-2 (infected Vero E6 bio-assay), studies have reported its potential as a co-treatment for COVID-19 patients due to its potent efficacy against symptoms associated with the disease [120‒124]. Some Indomethacin-Remdesivir conjugates-based proteolysis-targeting chimeras (PROTAC) have been reported with enhanced properties against SARS-CoV-2/NL/2020 and SARS-CoV-2/Padova/2021 strains relative to the parent indomethacin [121] (Figure 11). Conjugation between these mentioned drugs, or any other similar agents, can be a useful approach for optimizing promising hits/leads against SARS-CoV-2.
2.3. Lufotrelvir (PF-07304814)
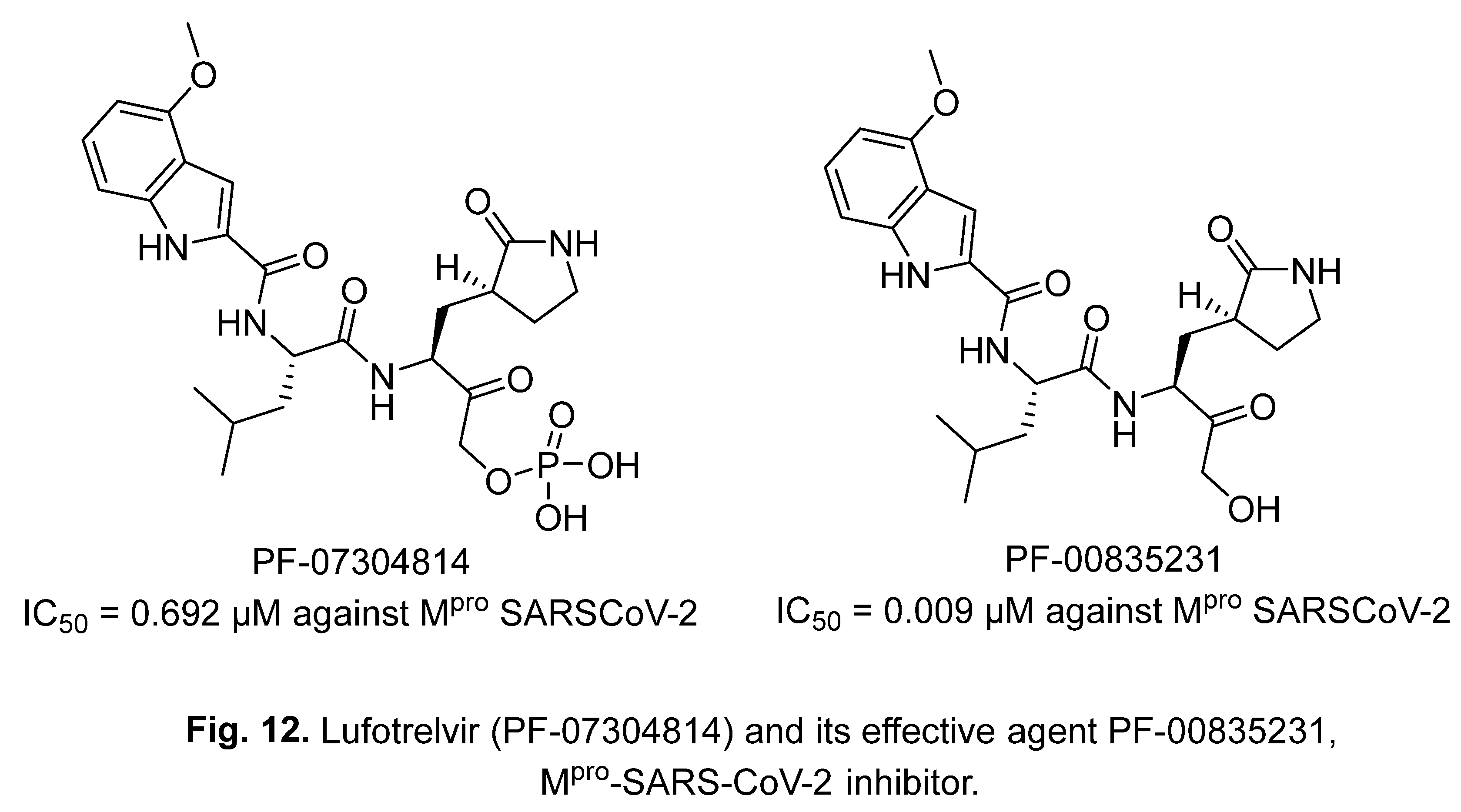
Lufotrelvir (PF-07304814) (Figure 12) is a SARS-CoV-2 main protease (Mpro) inhibitor developed by Pfizer for intravenous application. The phosphate group is cleaved in-vivo liberating PF-00835231, the effective agent against various viral strains [125].
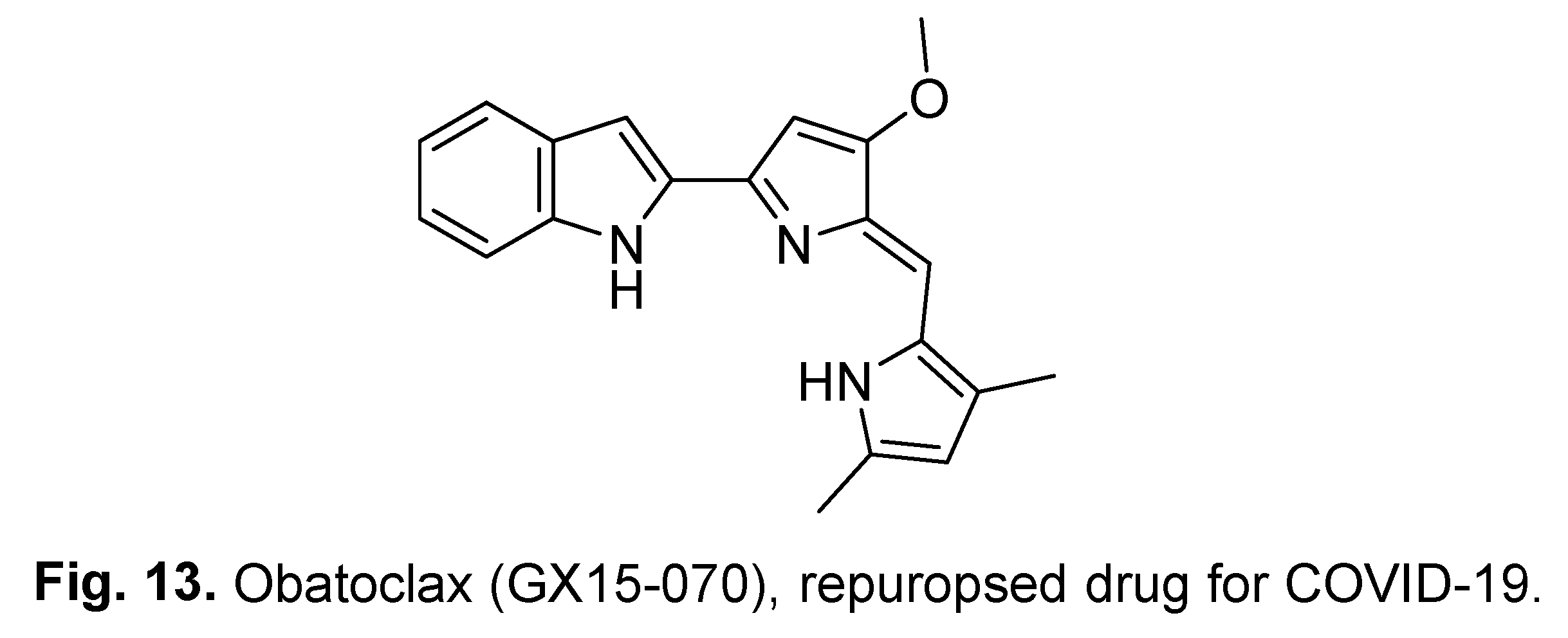
2.4. Obatoclax (GX15-070)
Obatoclax (GX15-070) (Figure 13) is an antitumor agent (leukemia, lymphoma, and lung) via BCL-2 protein inhibition inducing mitochondrial apoptosis and has been subjected to Phase II clinical trials. It was repurposed for COVID-19 due to its promising properties against ACE2 thereby blocking cellular entry by the infectious virus [126].
3. Natural indole-containing compounds
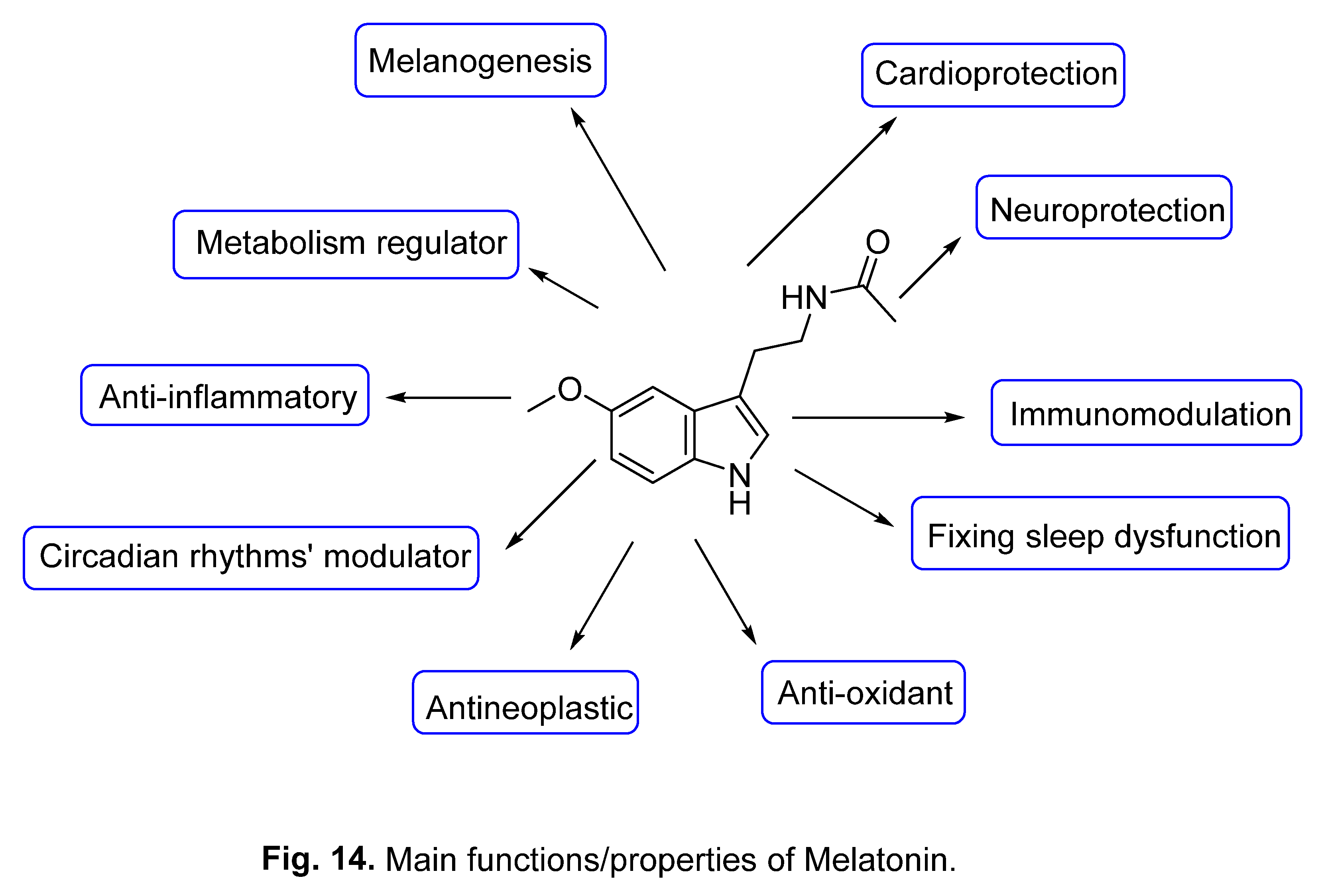
3.1. Melatonin
Melatonin is a natural hormone biosynthesized from tryptophan primarily by the pinealocytes of the pineal gland in the brain in the dark (hormone of darkness) and transferred by blood to the body organ from the cerebrospinal fluid. It exerts several biological properties [127‒131] (Figure 14). The correlation between the COVID-19 fatalities in the elderly with the decrease in melatonin secretion rate drew attention to a possible application of the hormone for treatment [132]. The ability of melatonin as an anti-oxidant and anti-inflammation also suggested a potential role as an anti-SARS-CoV-2 [133]. Due to its safety profile and diverse bio-properties, numerous reports have considered the role for melatonin in the prevention and treatment of COVID-19 [134‒139]. Clinical studies/observations have supported its ability to reduce the severity of the disease, shorten the hospitalization period or lead to complete recovery upon administration, either as a mono-therapeutic [137‒139] or with other therapeutics, for COVID-19 infected patients [134‒136].
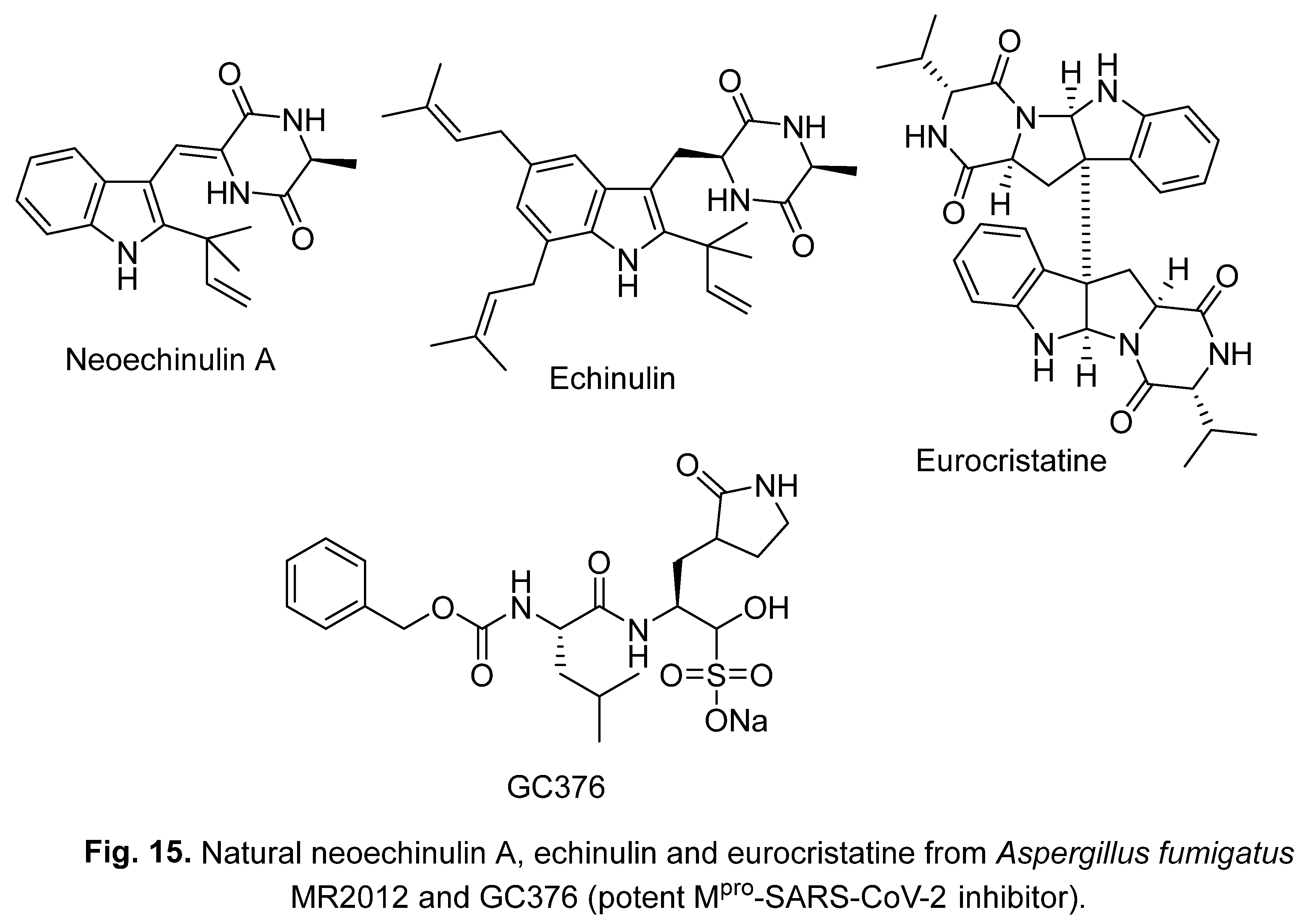
3.2. Neoechinulin A, echinulin and eurocristatine
The natural compounds neoechinulin A, echinulin, and eurocristatine (Figure 15) can be obtained from organisms such as Aspergillus fumigatus MR2012. Neoechinulin A and echinulin have Mpro-SARS-CoV-2 inhibitory properties (IC50 = 0.47, 3.90 μM, respectively) [140]. For comparison, the value is (IC50 = 0.36 μM) for GC376 which is a potent Mpro-SARS-CoV-2 inhibitor [141].
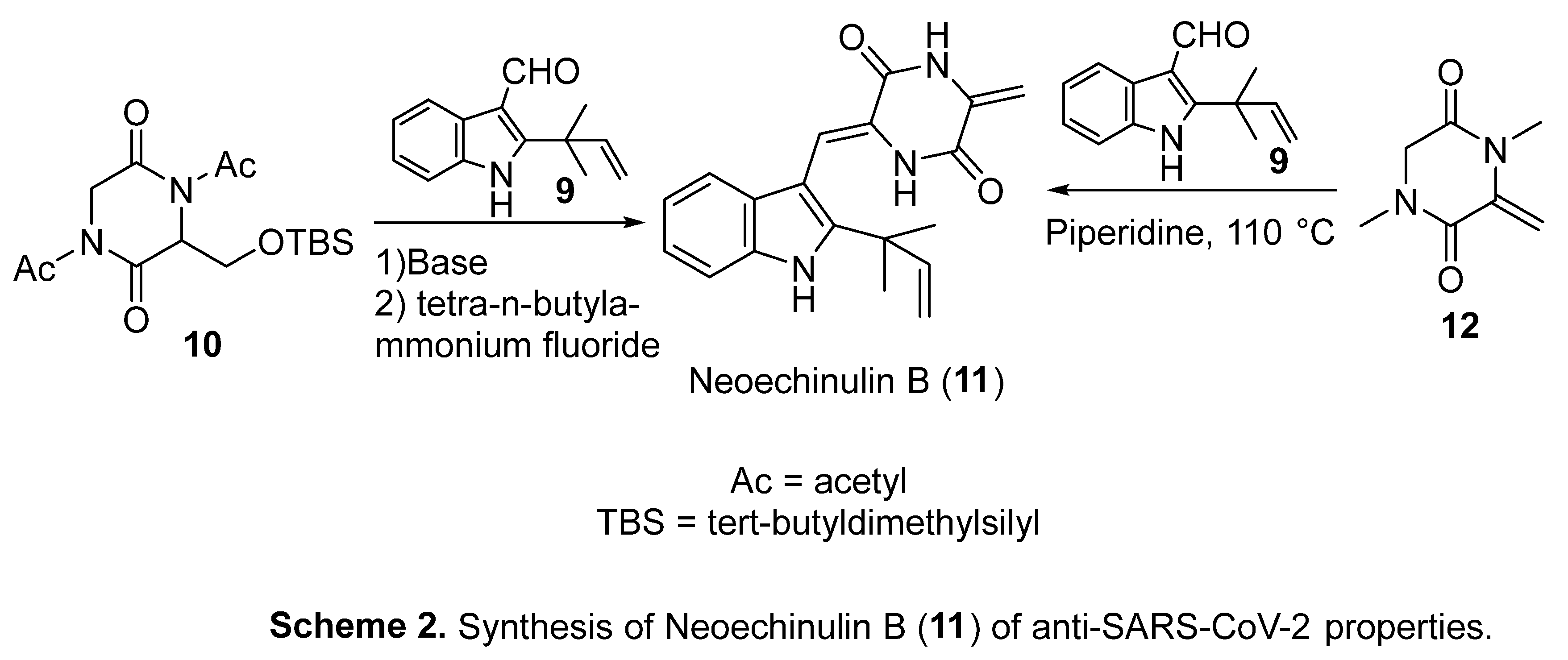
Neoechinulin B 11 can be extracted from Eurotium rubrum Hiji025. It has been synthesized in a two-step reaction involving the 2-indole aldehyde 9 and the appropriate 2,5-piperazinedione 10 in basic conditions followed by tetra-n-butylammonium fluoride. Alternatively, 11 could be obtained from the aldehyde 9 and 2,5-piperazinedione 12 in the presence of piperidine at 110 °C (Scheme 2). Neoechinulin B 11 has anti-SARS-CoV-2 properties (Vero E6, assay, IC50 = 32.9, CC50 = >70 μM) [142].
4. Synthetic indole-containing compounds
4.1. Isatins
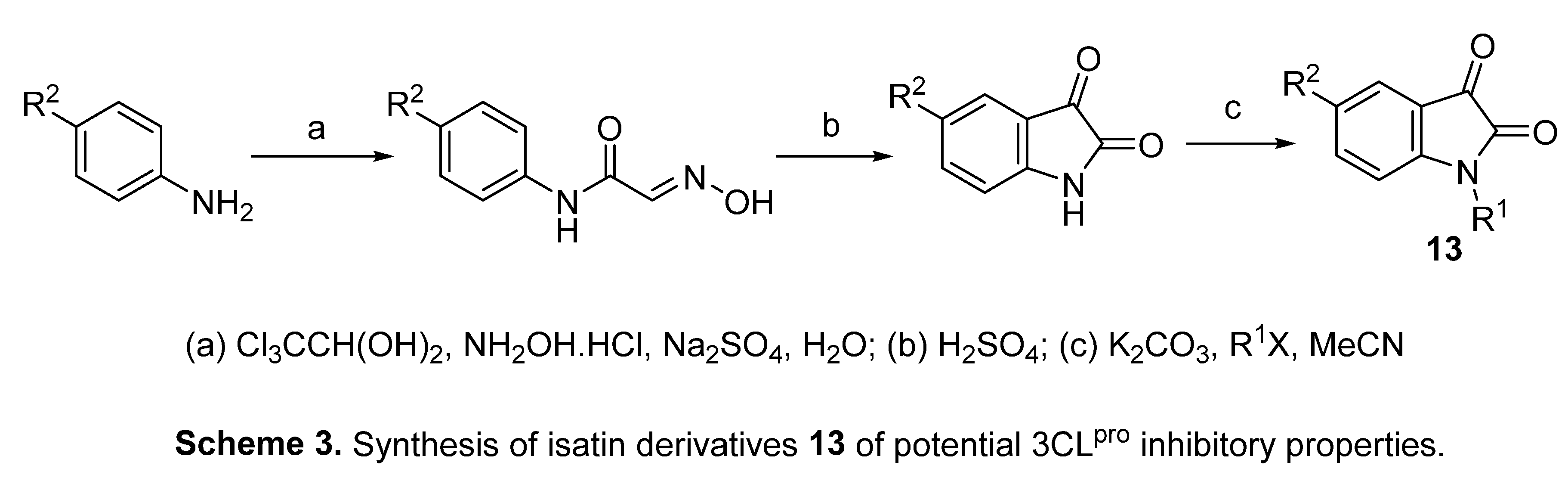
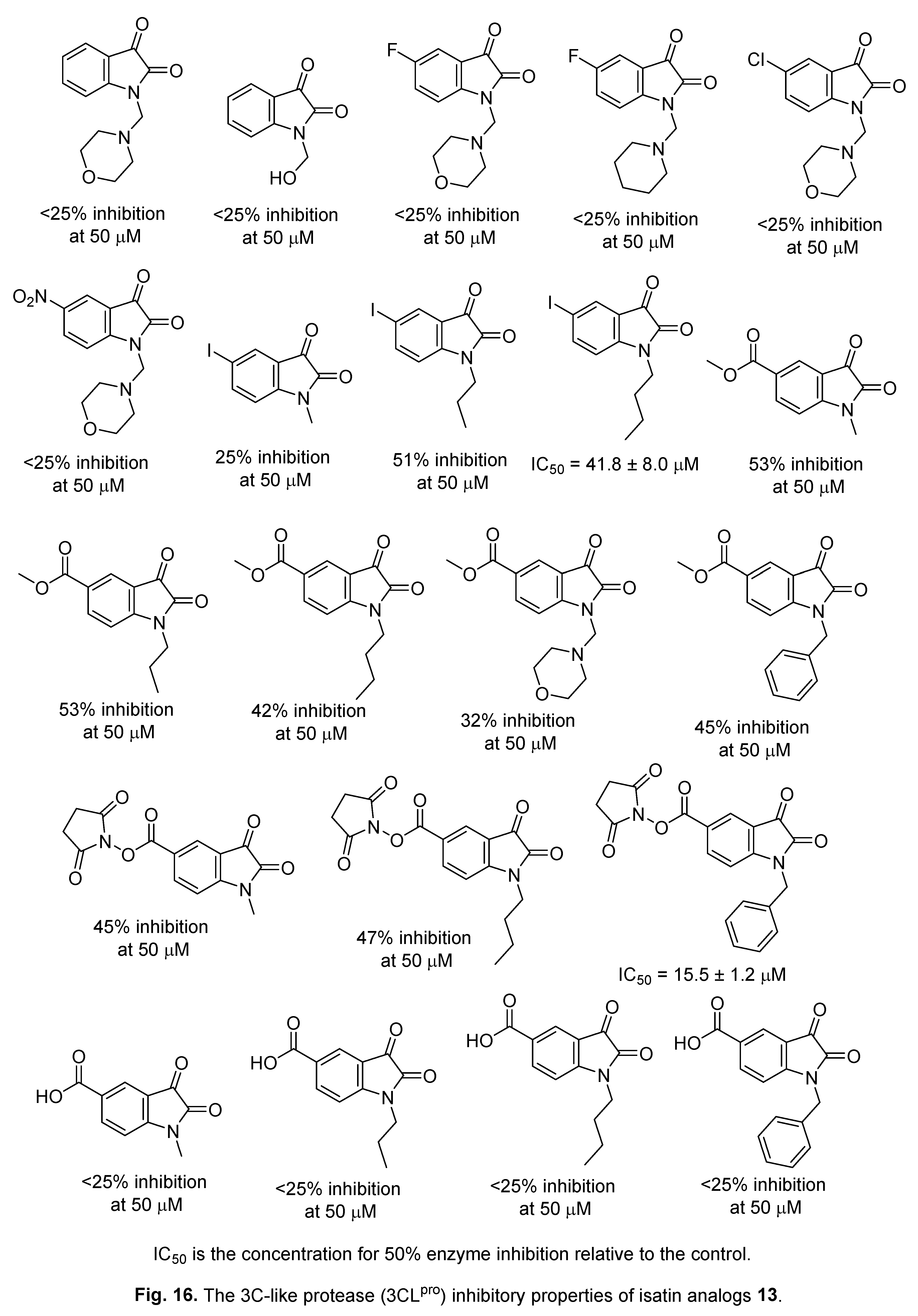
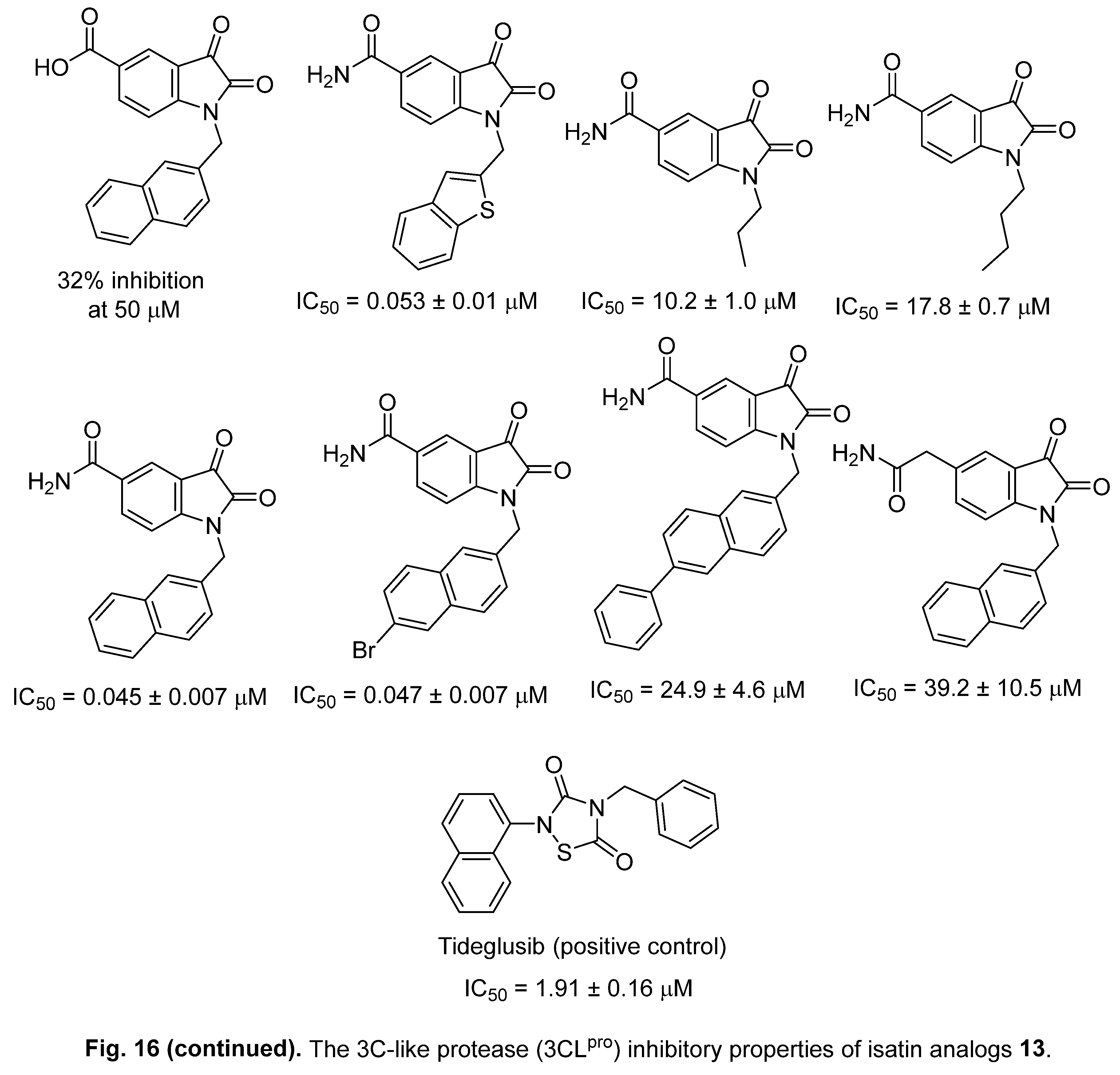
A series of isatin derivatives 13 have been synthesized through the reaction of aromatic amines with hydroxylamine hydrochloride (NH2OH.HCl) and chloral hydrate [Cl3CCH(OH)2] followed by cyclization with concentrated sulfuric acid (H2SO4) at 90 °C and alkylation (Scheme 3). Some of the synthesized isatin analogs 13 revealed 3C-like protease (3CLpro) [or main protease (Mpro)] SARS-CoV-2 inhibitory properties relative to Tideglusib (positive control) [143] (Figure 16).
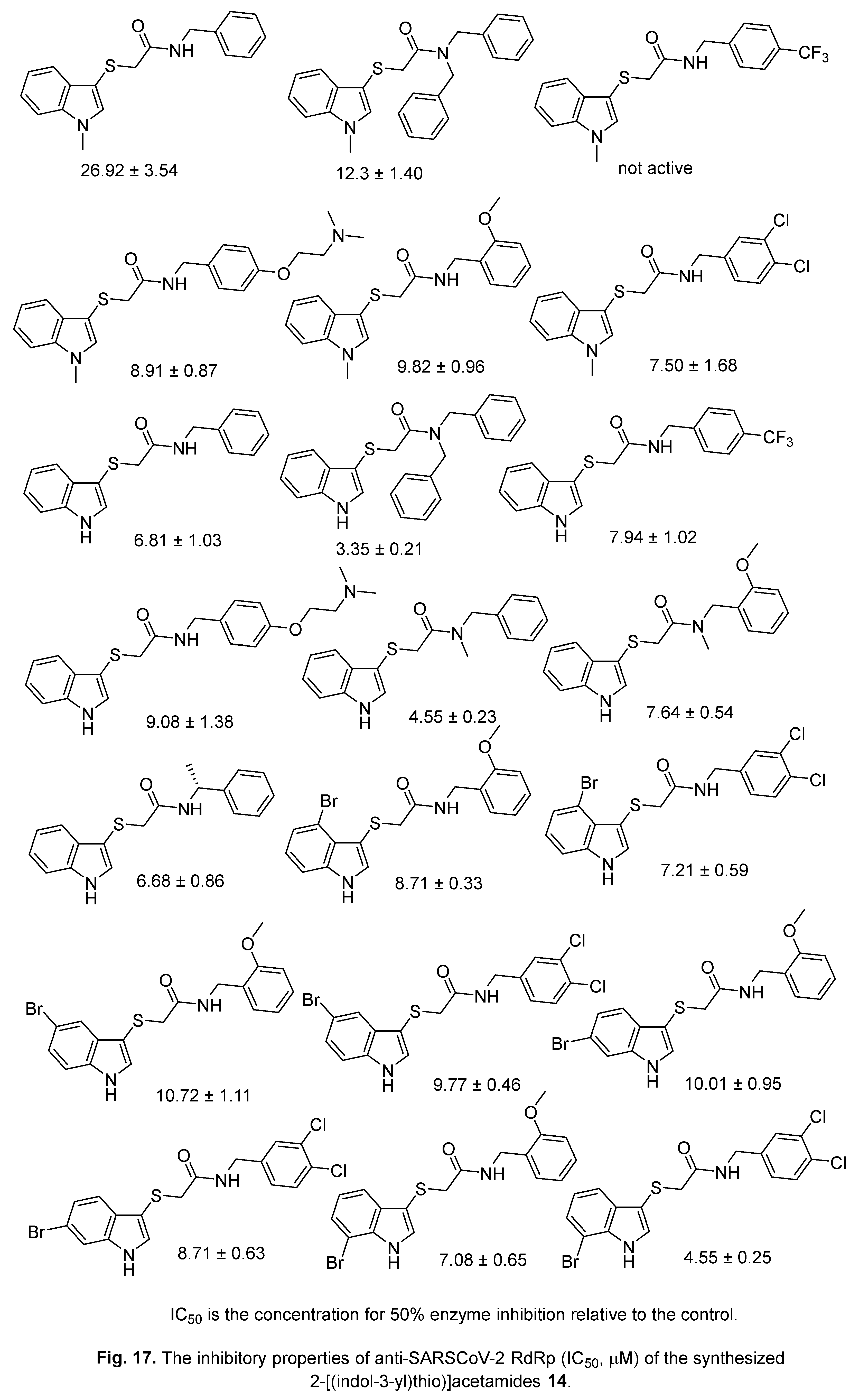
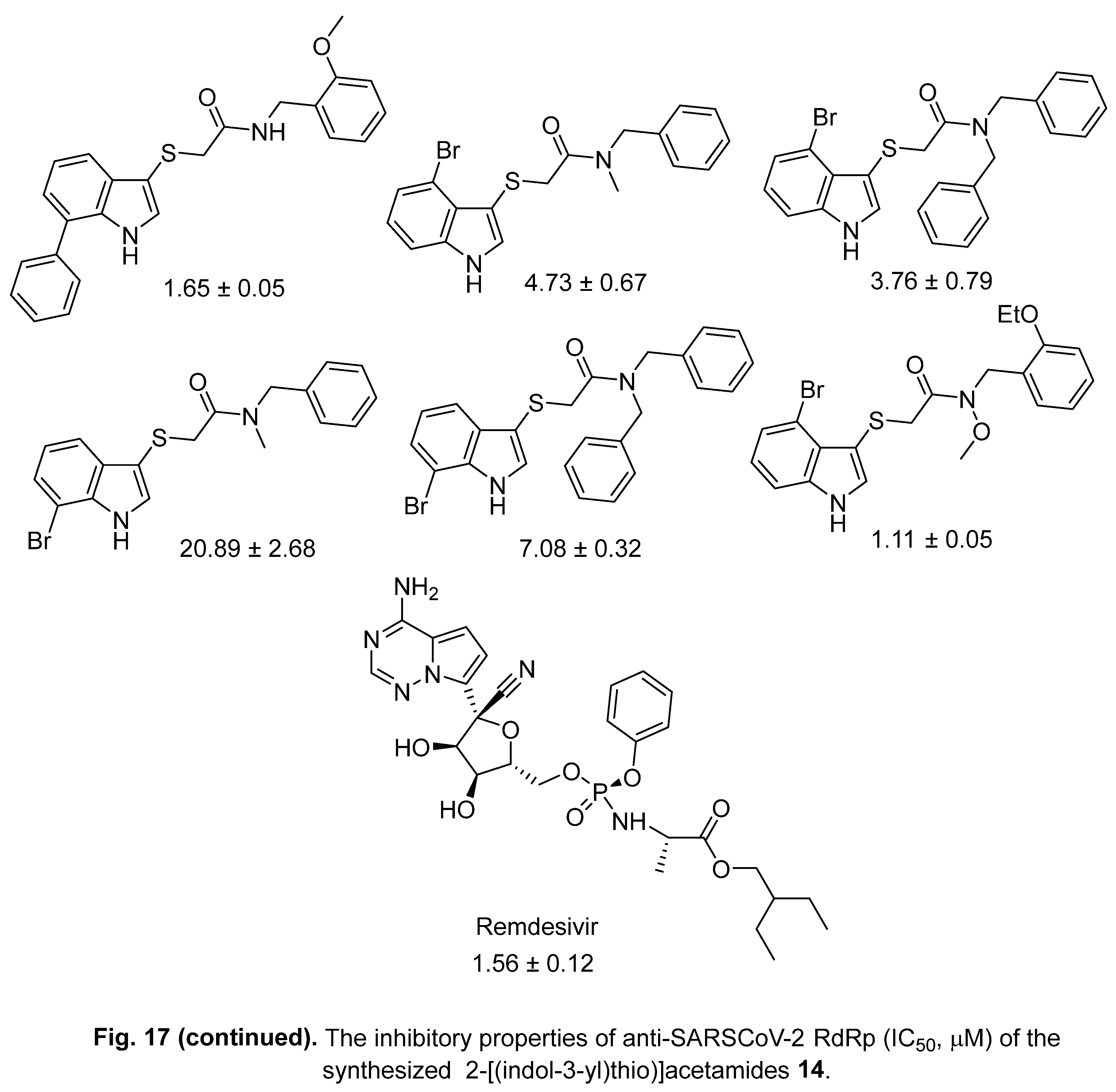
4.2. 2-[(Indol-3-yl)thio]acetamides
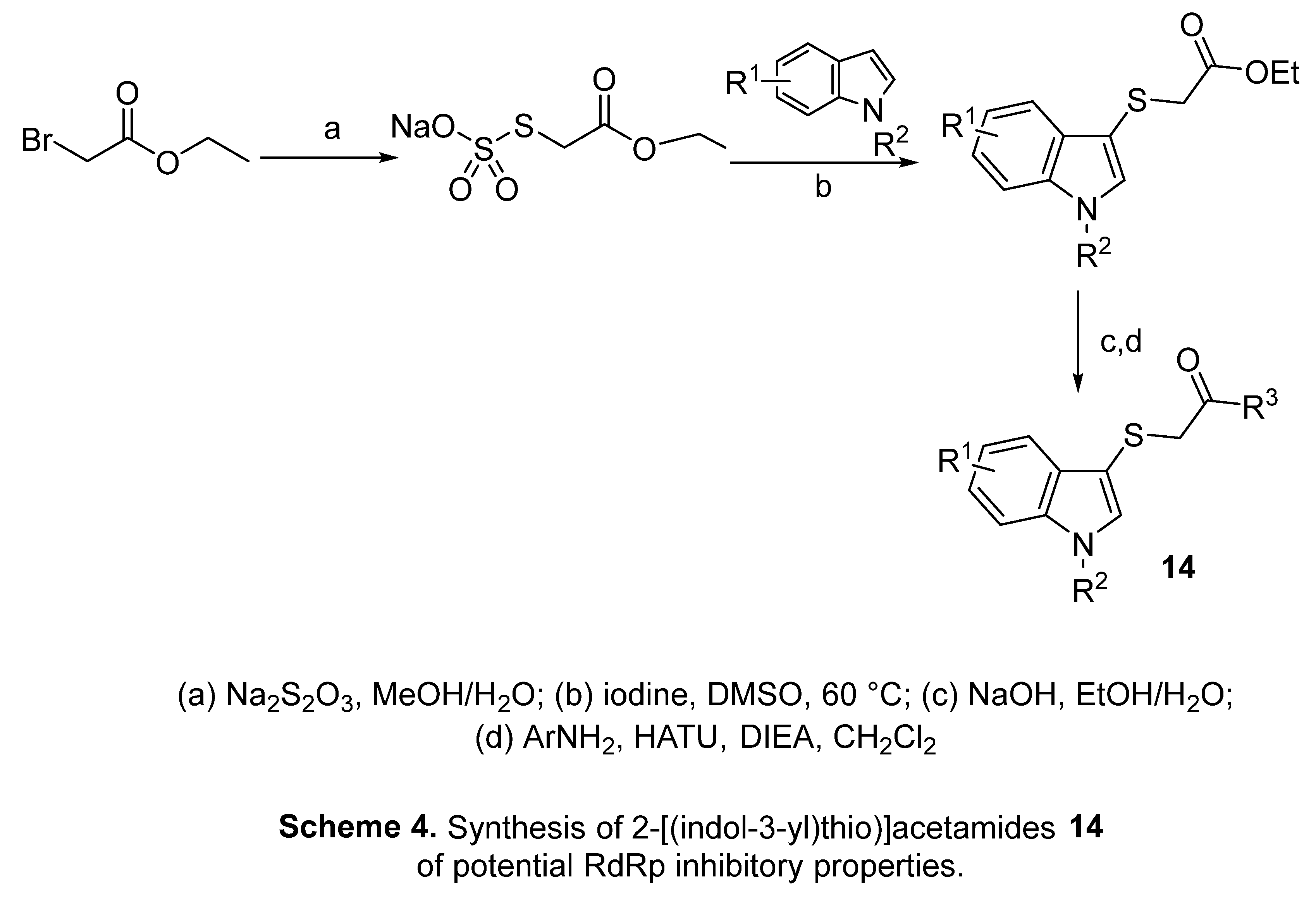
2-[(Indol-3-yl)thio)acetamides 14 were synthesized through the reaction of indole derivatives with Bunte salt ethyl acetate-2-sodium thiosulfate in iodine/DMSO at 60 °C followed by hydrolysis (NaOH, EtOH/H2O) and coupling with the appropriate amine (Scheme 4). Some of the synthesized agents exhibited RdRp inhibitory properties relative to Remdesivir [144] (Figure 17). Considering these observations (Figure 17) and those mentioned in Figure 16, it can be concluded that the substituent attached to the indolyl heterocycle plays a circular role in the mode of action. Compounds of Figure 16 exhibited 3CLpro inhibitory properties. However, those of Figure 17 revealed RdRp inhibitory properties. So, the mutual mode of action may be optimized by manipulating the substitution of indolyl heterocycle for assigning potent anti-SARS-CoV-2 agents.
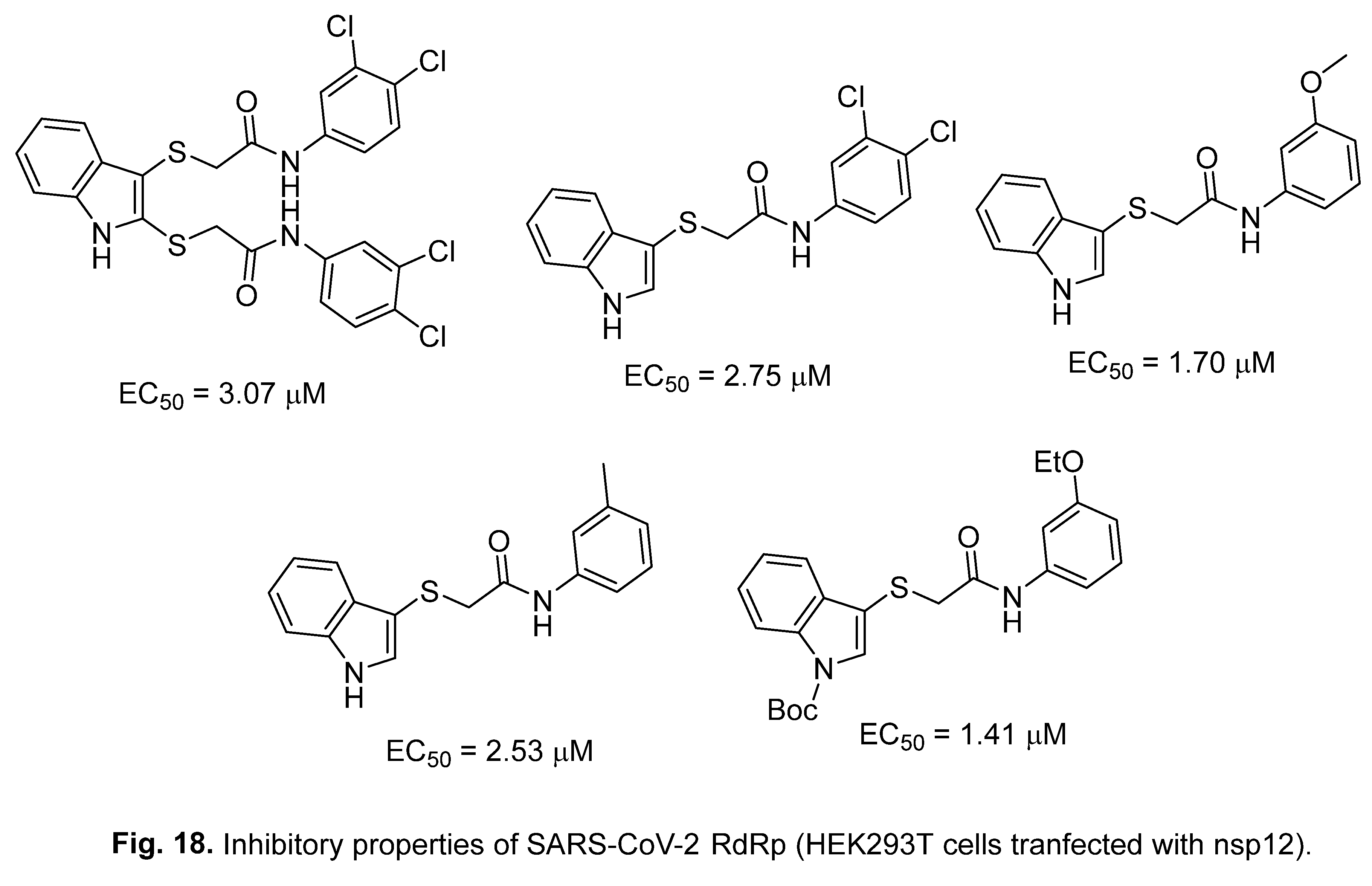
A set of acetamide-containing indoles with possible RdRp SARS-CoV-2 inhibitory properties have been explored. The efficacy of the most promising agents was comparable to that of Remdesivir (EC50 = 1.05 μM) [145] (Figure 18).
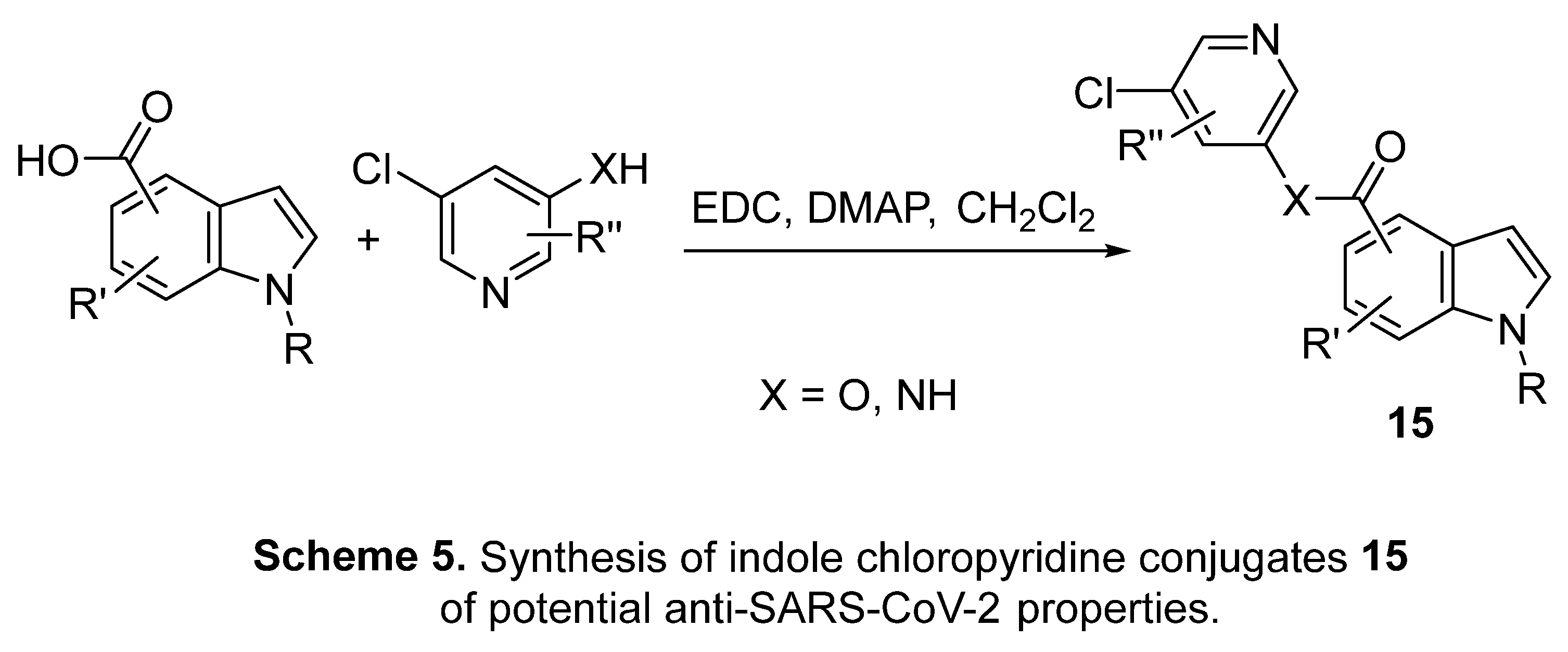
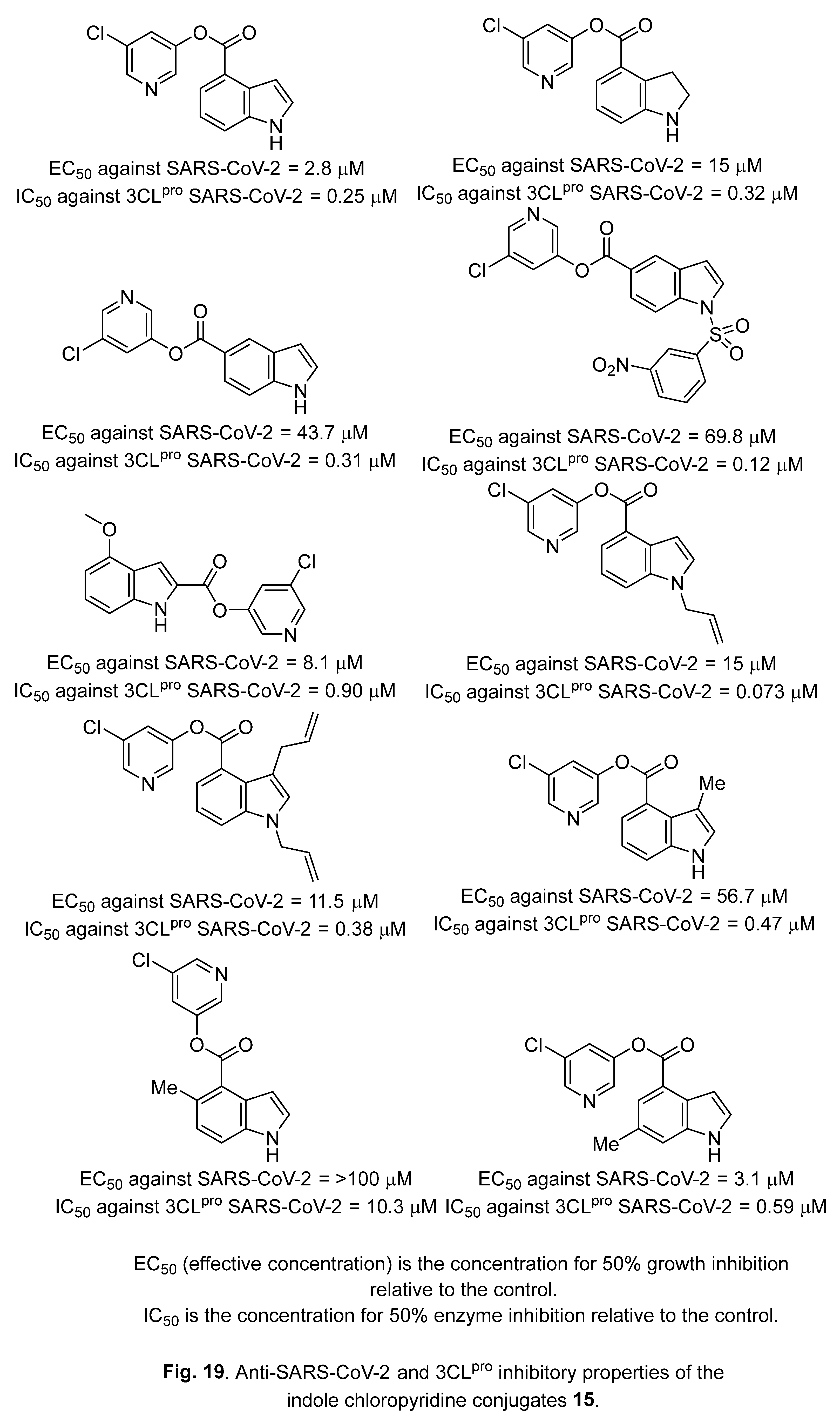
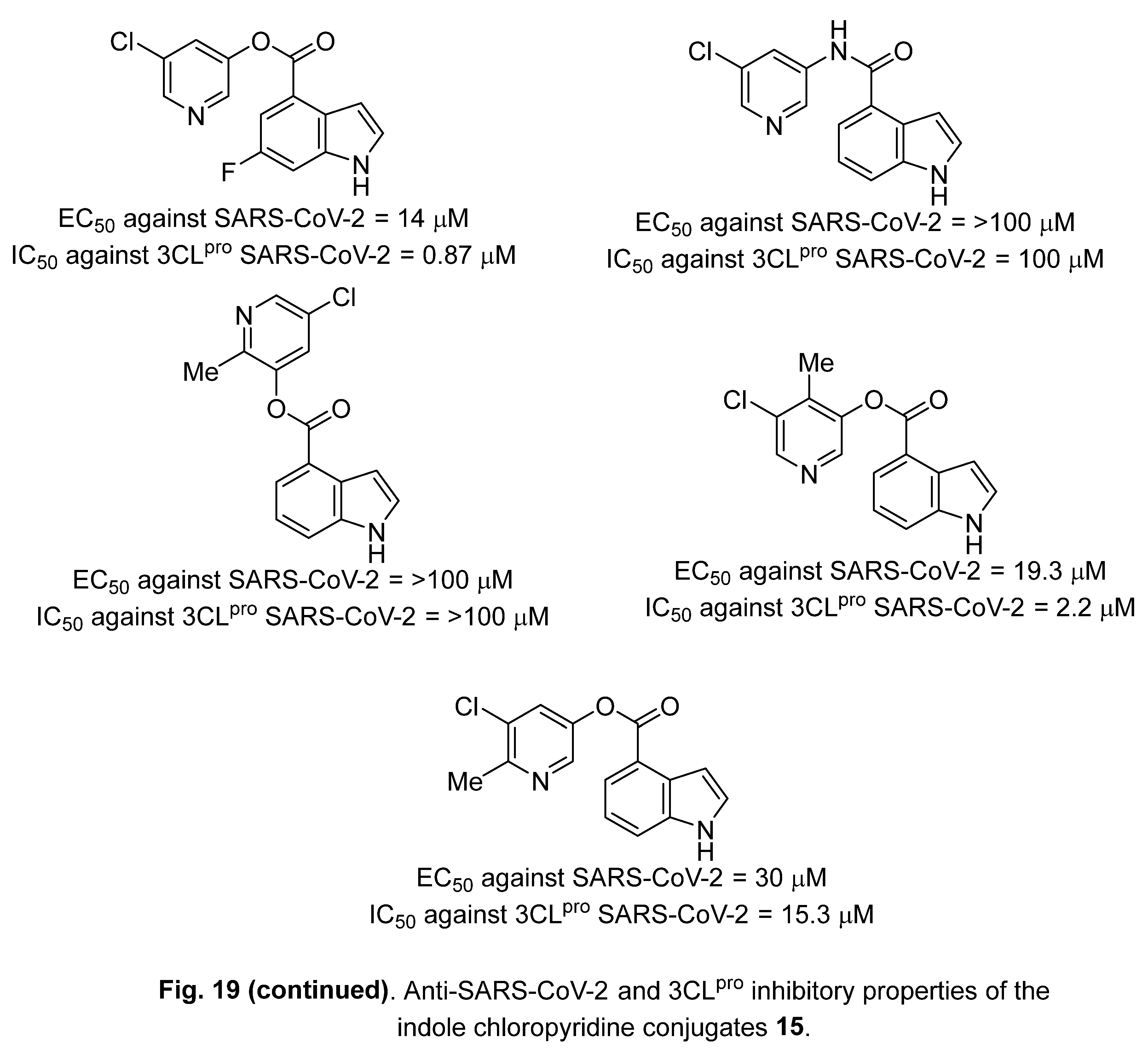
4.3. Indole chloropyridine conjugates
A variety of indole chloropyridine conjugates 15 were synthesized via reaction of the appropriate indolecarboxylic acid with 3-chloropyridin-5-ols or 5-amino-3-chloropyridines using 1-ethyl-3-(3-dimethylaminopropyl)carbodiimide (EDC) and dimethylaminopyridine (DMAP) in methylene chloride (CH2Cl2) (Scheme 5). Anti-SARS-CoV-2 activities (Vero E6 assay) with 3CLpro inhibitory properties were observed for some of the synthesized agents [59] (Figure 19).
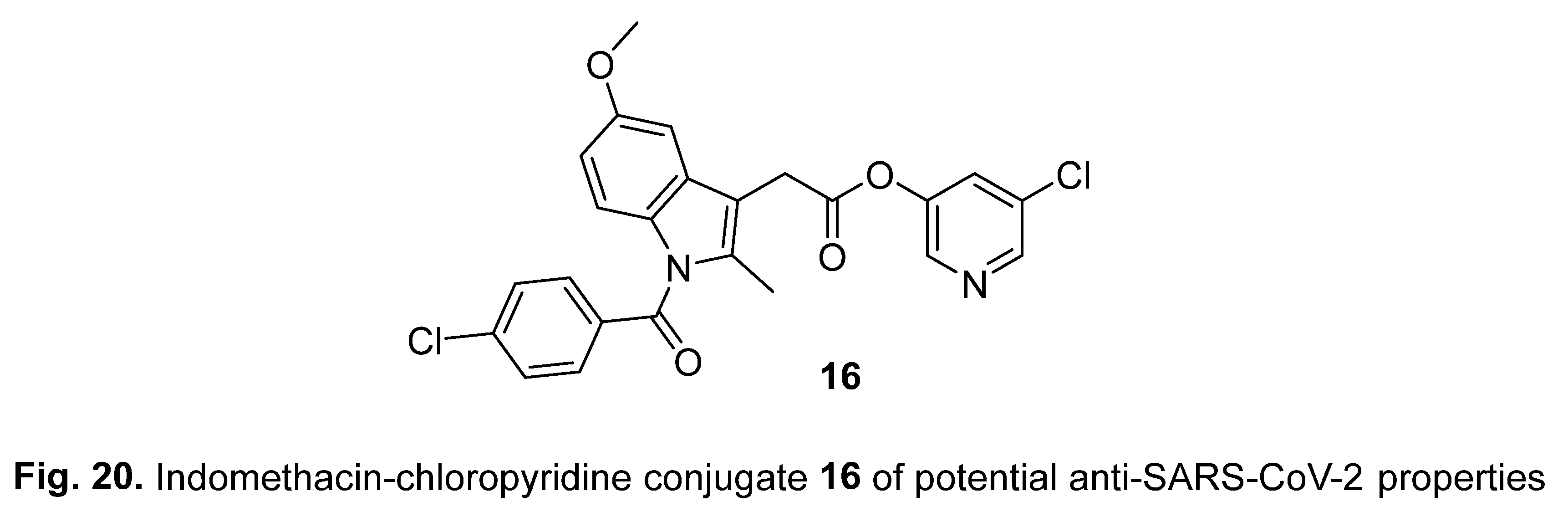
Indomethacin-chloropyridine conjugate 16 (Figure 20) is also possible by utilizing the same reaction conditions (EDC and DMAP in CH2Cl2, 53% yield). Anti-SARS-CoV-2 activity was observed for the compound (EC50 against SARS-CoV-2 = 30.2 μM, IC50 against 3CLpro SARS-CoV-2 = 5.32 μM) [146].
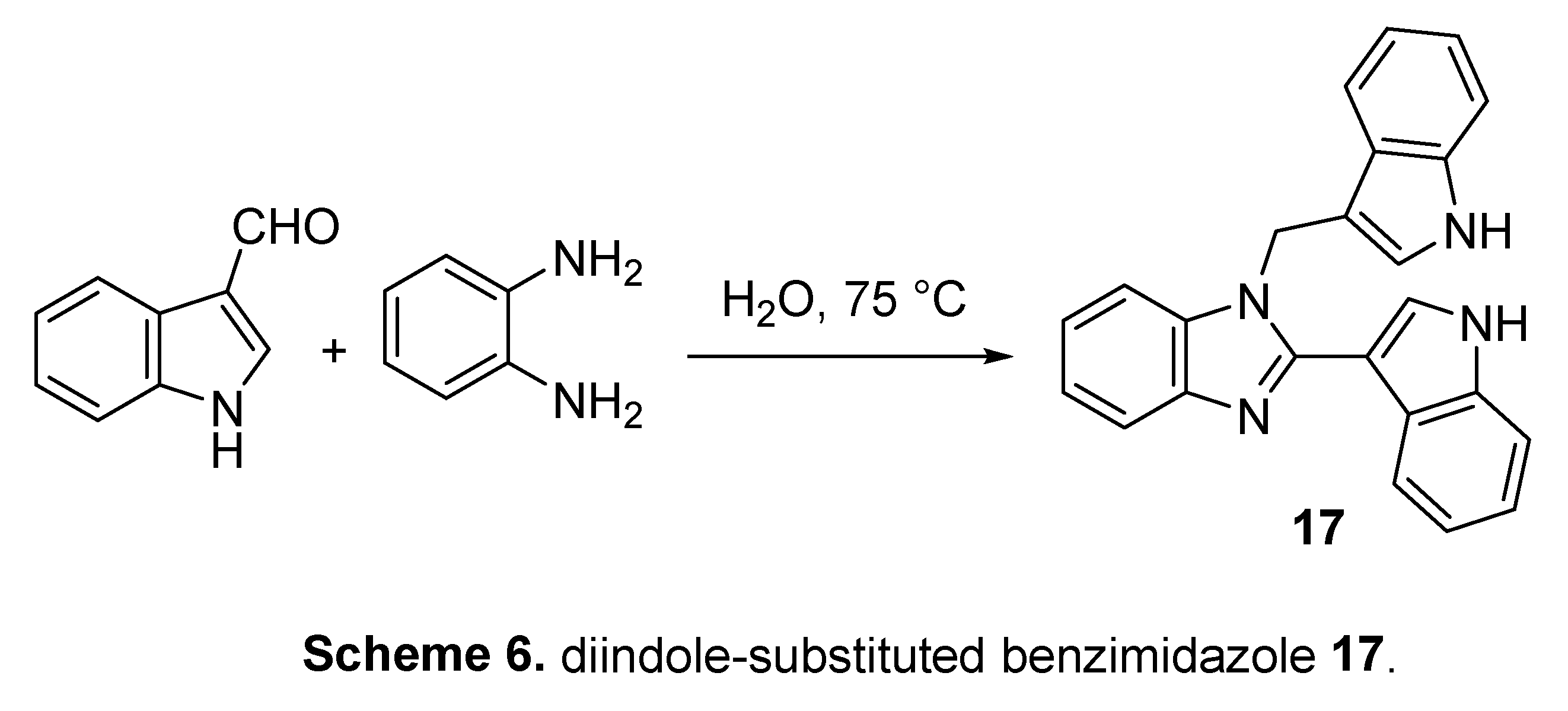
4.4. Diindole-substituted benzimidazole
Condensation of 3-indolealdehyde with o-phenylenediamine under green conditions (in water at 75 °C) in a 2:1 molar ratio afforded the corresponding diindole-substituted benzimidazole 17 (Scheme 6). The synthesized agent revealed 92.4 % cell viability (Verso E6) at 9.0 μM concentration in comparison to 99.23% for Remdesivir at 10 μM. The antiviral properties of 17 were supported by the immunofluorescence assay [147].
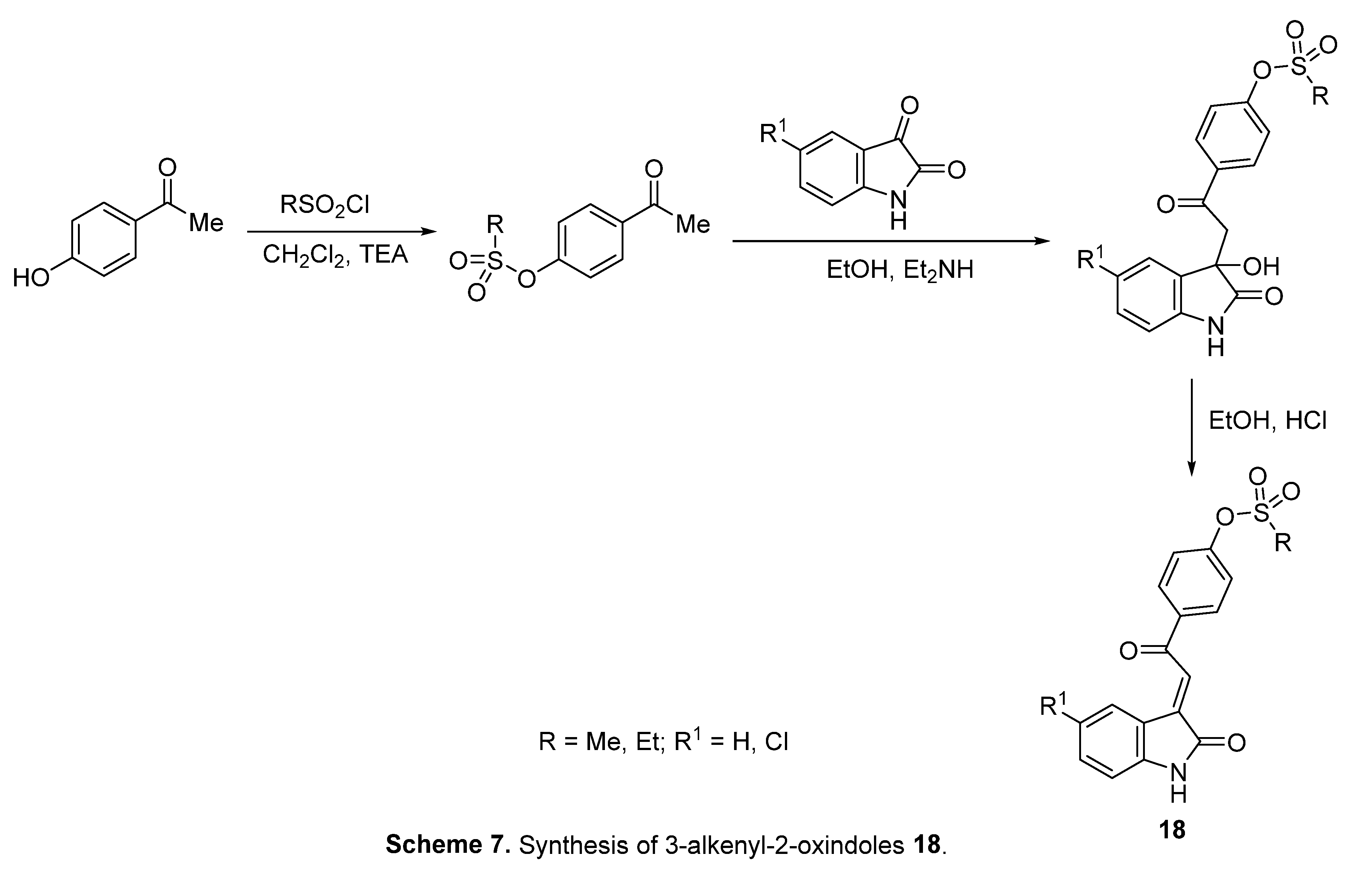
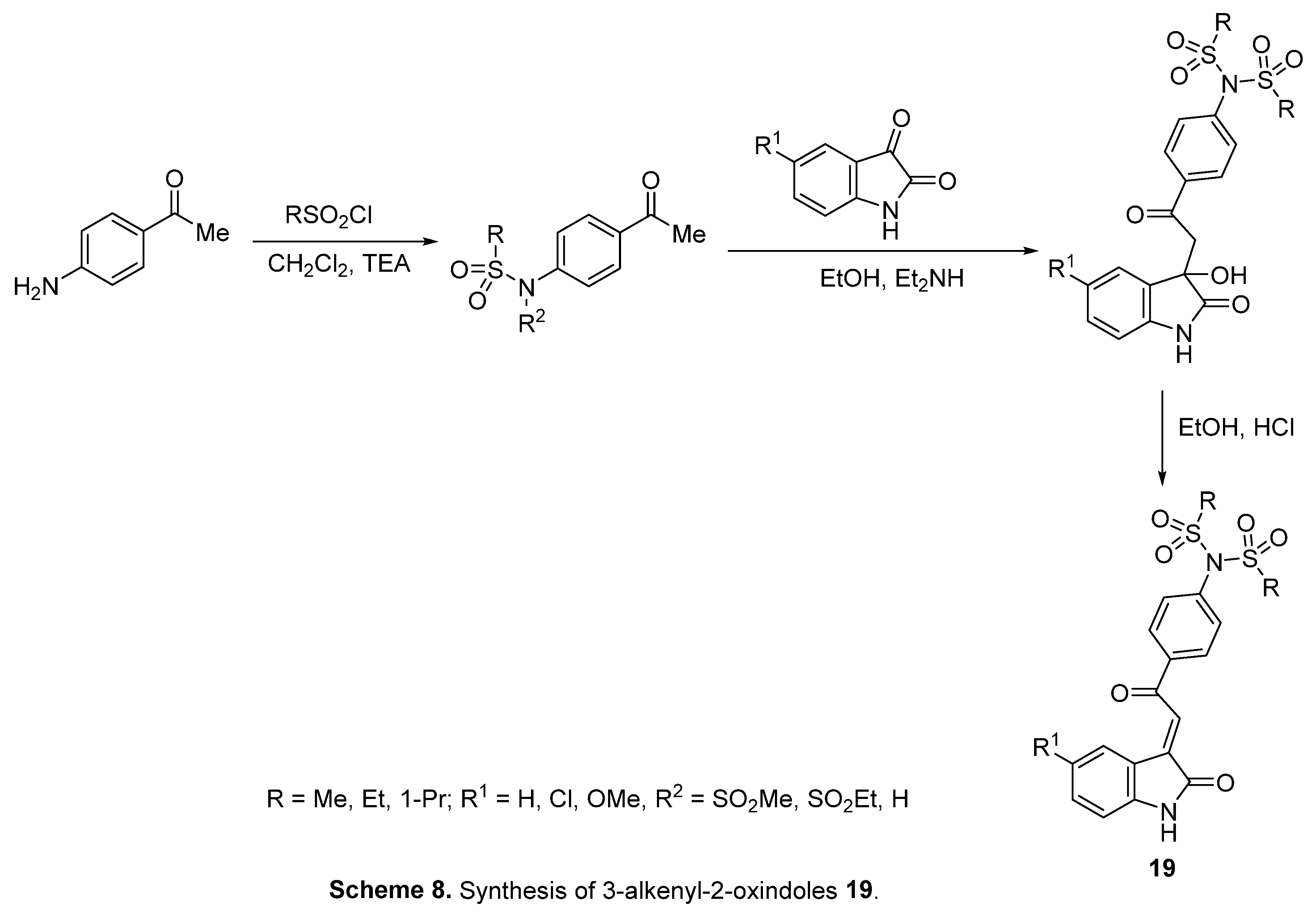
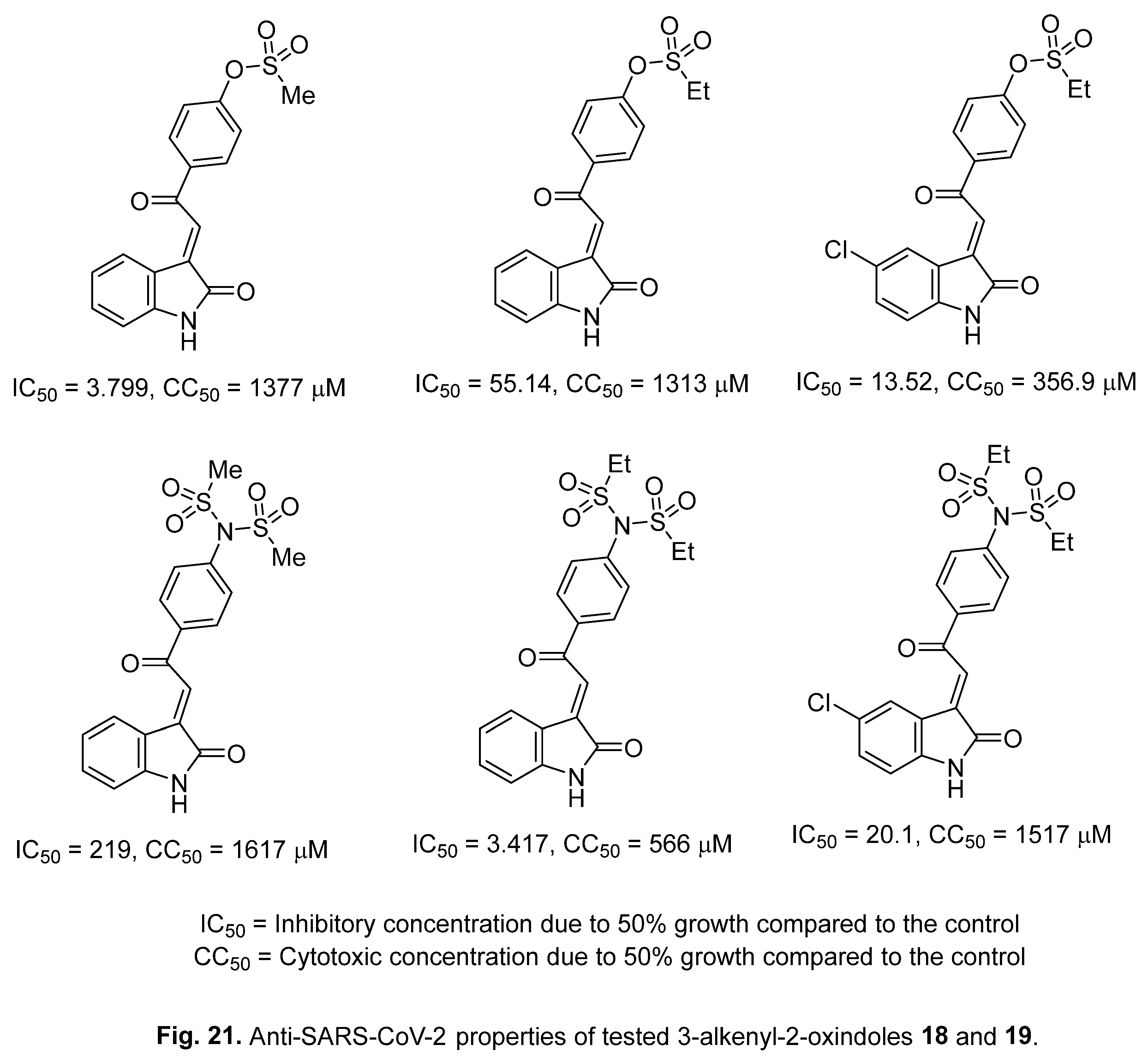
4.5. 3-Alkenyl-2-oxindoles
Anti-SARS-CoV-2 3-alkenyl-2-oxindoles 18 and 19 were obtained through acidic dehydration (HCl/EtOH) from the corresponding 3-hydroxy analogs (Schemes 7,8). Some of the synthesized agents showed potent anti-SARS-CoV-2 properties (Figure 21) relative to the standards (IC50 = 29.25, 19.78, 1382, CC50 = 356.4, 377.7, 2633 μM for Hydroxychloroquine, Chloroquine, and Favipiravir, respectively) in the Vero E6 assay [148].
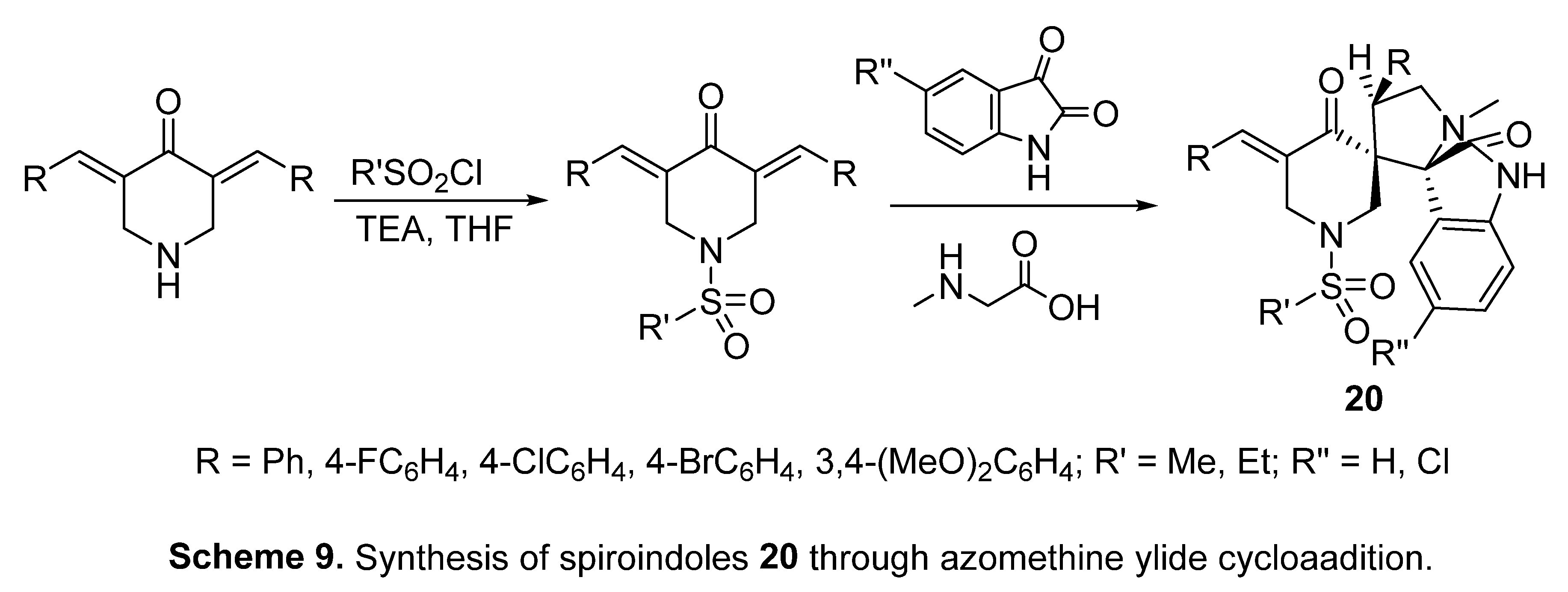
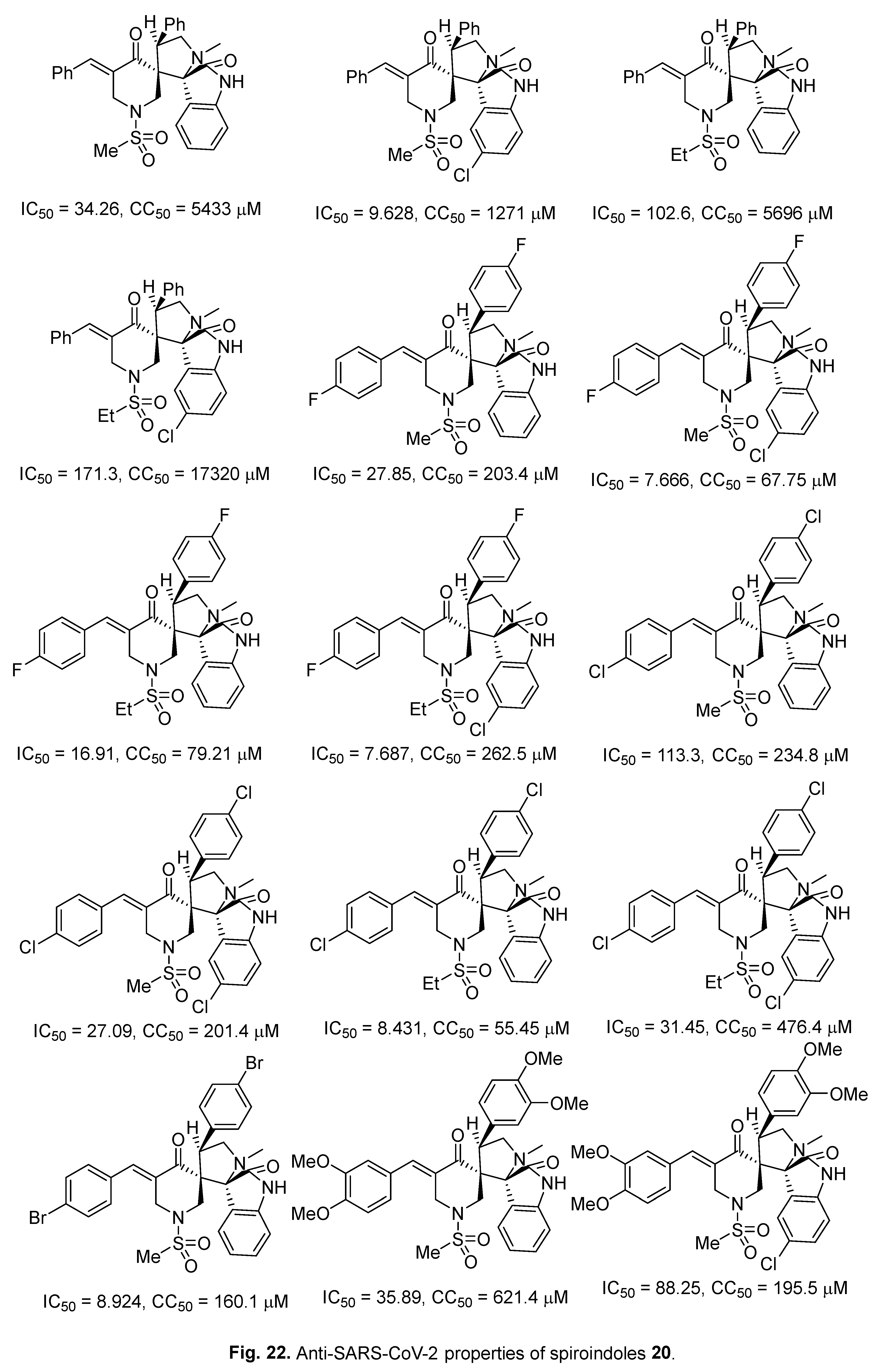
4.6. Spiroindoles
Spiroindoles 20 were synthesized through cycloaddition of azomethine ylide (obtained from sarcosine and isatins) with 3,5-diylidene-4-piperidones (Scheme 9). Promising anti-SARS-CoV-2 properties were shown by some of the synthesized agents in the Vero E6 assay relative to the standards Hydroxychloroquine, Chloroquine, and Favipiravir [149] (Figure 22).
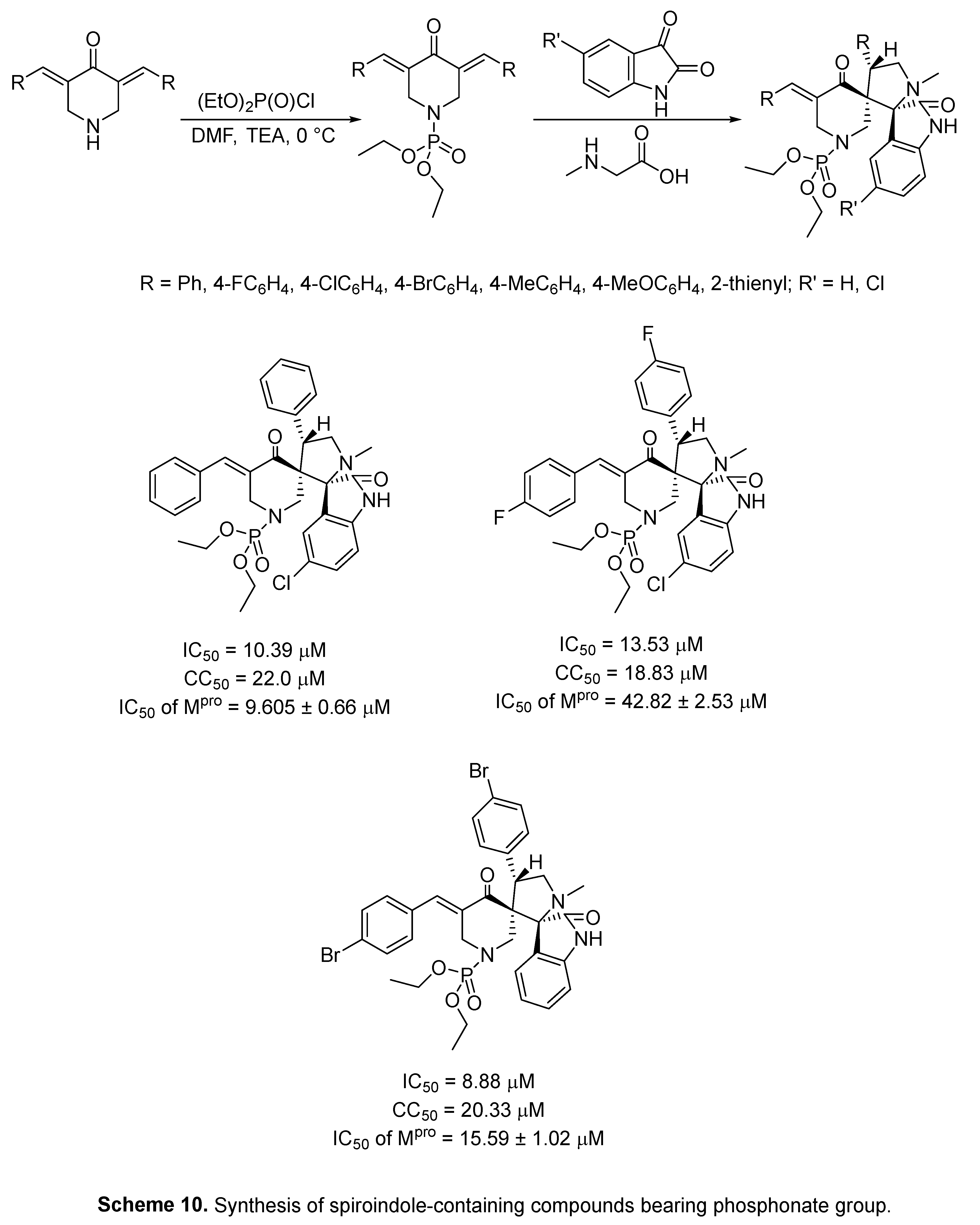
Anti-SARS-CoV-2 spiroindole-containing compounds bearing phosphonate group were recently reported with potential Mpro inhibitory properties, synthesized through azomethine (generated from the reaction of isatin and sarcosine) reaction with the appropriate 3,5-bis((E)-ylidene)-1-phosphonate-4-piperidone [150] (Scheme 10).
It has been noticed through this report (Scheme 10) that the spiroindoles with sulfonyl group (Figure 22) are more promising anti-SARS-CoV-2 agents relative to those with phosphonate group.
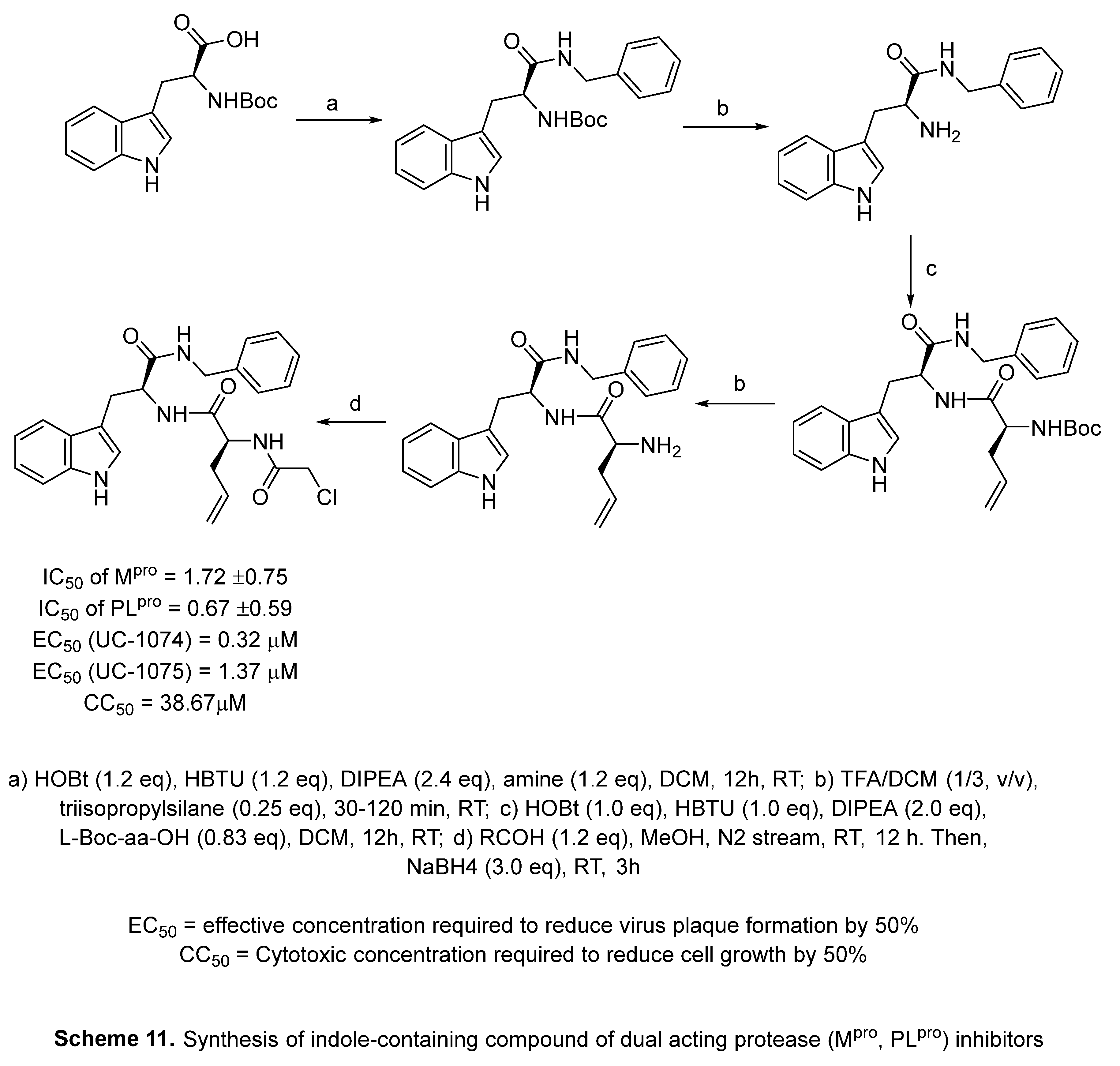
4.7. Indole with dual acting proteases inhibitor
Di Sarno [151] reported synthesis of indole-containing compound with potential SARS-CoV-2 protease (Mpro “main protease” and PLpro “papain like protease”) inhibitory properties (Scheme 11).
5. In-silico predicted anti-SARS-CoV-2 indoles
The use of computational techniques is an accessible approach to identifying effective hits/leads and accelerating the drug discovery program directed towards the development of anti-SARS-CoV-2, either through repurposing or de novo drug design. Virtual screening can reduce the time and cost needed for establishing possible bioactive agents. However, the agents identified by in-silico studies still require supporting experimental bio-properties investigations to realize the benefits of these studies [152,153].
5.1. SARS-CoV-2 (main protease, Mpro) inhibitor
SARS-CoV-2 main protease (Mpro or 3CLpro) controls many essential viral processes including maturation, replication, and transcription. This makes it a potential target for optimizing therapeutics against COVID-19 [154,155]. Paxlovid is a prominent protease inhibitor approved by the FDA at the end of 2021 for mild and moderately effected patients. It is a combination of two therapeutics, Nirmatrelvir (3CL protease inhibitor) and Ritonavir (protease inhibitor, therapeutic against HIV/AIDS). Paxlovid is effective at reducing the hospitalization period when administrated at the beginning of COVID-19 symptoms [156‒158].
In this section, representative examples of computationally predicted Mpro SARS-CoV-2 inhibitors will be highlighted. Jayabal et al. reported the synthesis of 3-substituted indoles 21 through a multi-component green synthetic approach via reaction of nitroketene S,S-acetal, diamine-containing compound, 3-formylchromone, and indole in the presence of In(OTf)3 as a catalyst in refluxing ethanol [62] (Scheme 12). Computationally, some of the synthesized agents showed inhibitory properties for SARS-COV-2 Mpro (PDB: 6LU7) and spike glycoprotein (PDB: 7NX7) utilizing Auto Dock-Vina software (v. 1.1.2). For comparison, Remdesivir binding energy = -7.7, -6.5 kcal/mol is against main protease 6LU7 and spike glycoprotein 7NX7, respectively [62] (Figures 23,24).
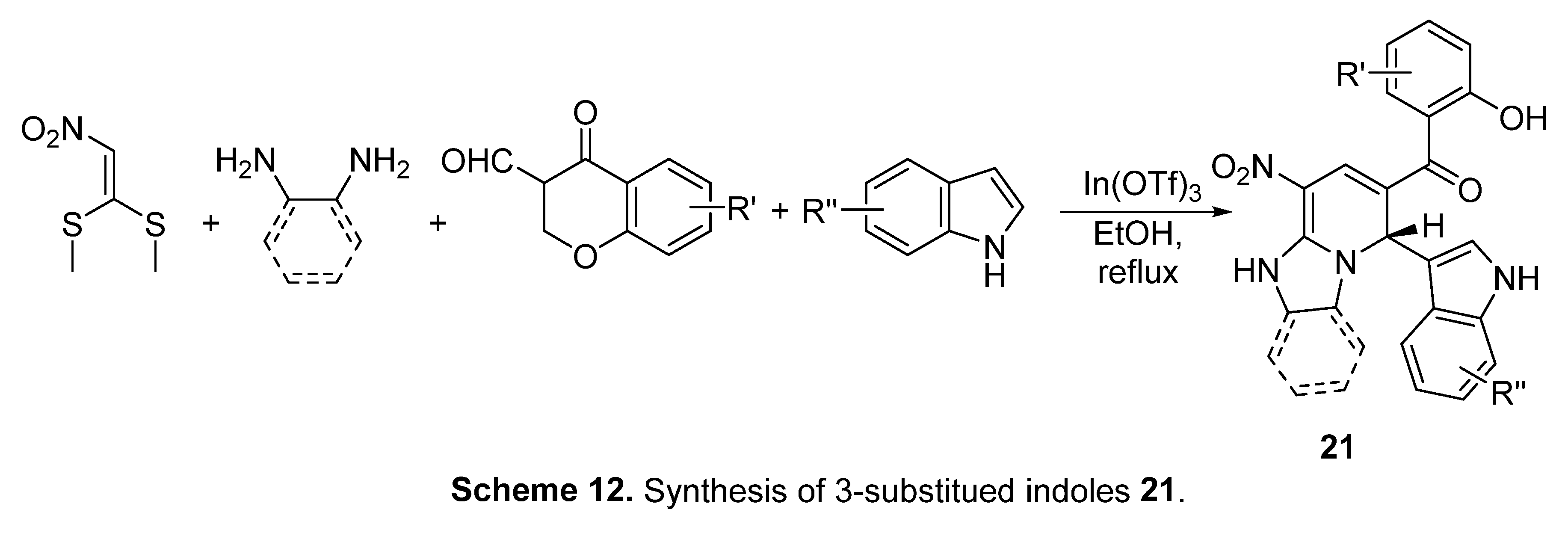
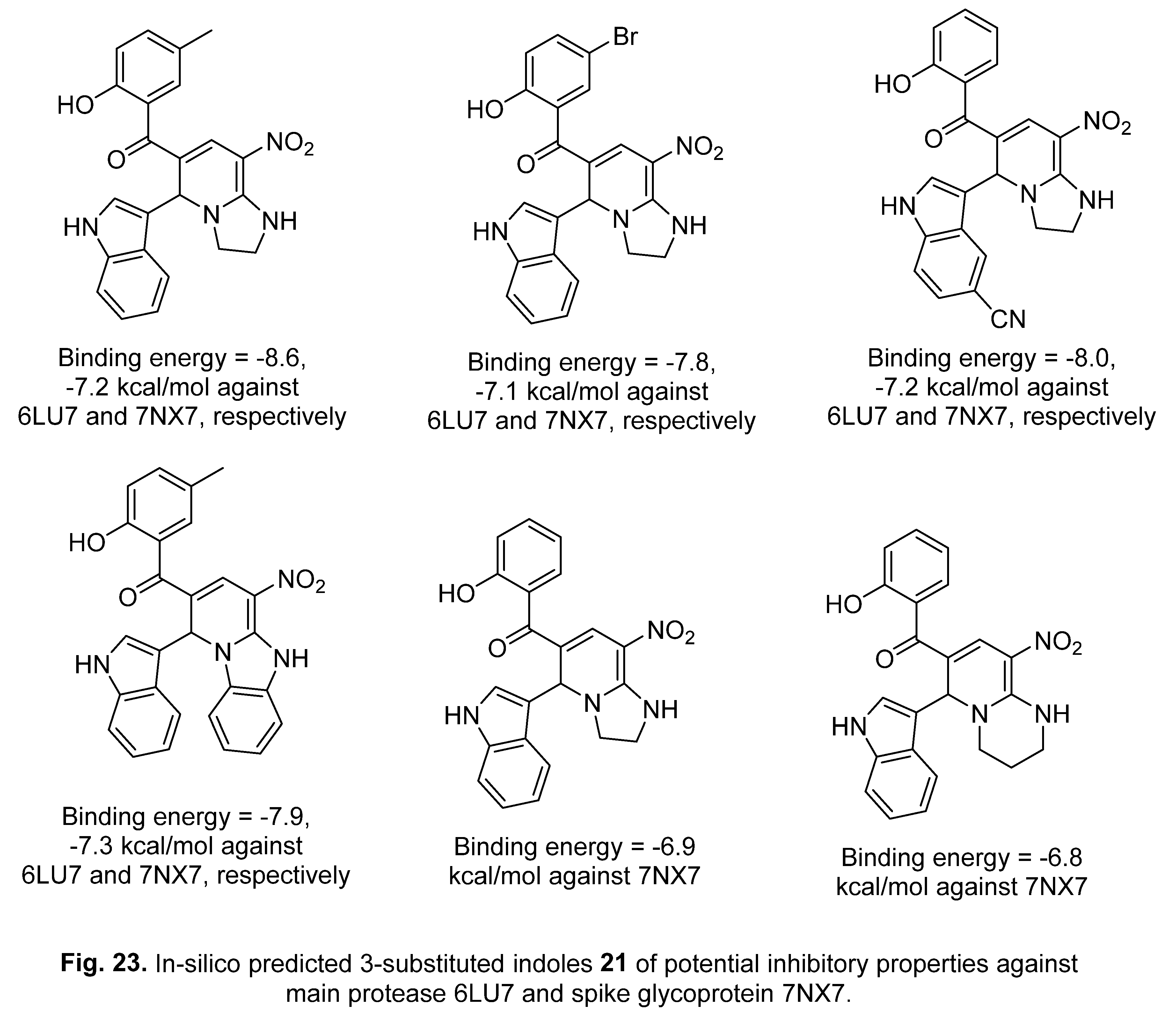
Figure 24.
Representation of Remdesivir and predicted 3-substituted indoles 21 revealing potential properties against 6LU7.
Figure 24.
Representation of Remdesivir and predicted 3-substituted indoles 21 revealing potential properties against 6LU7.
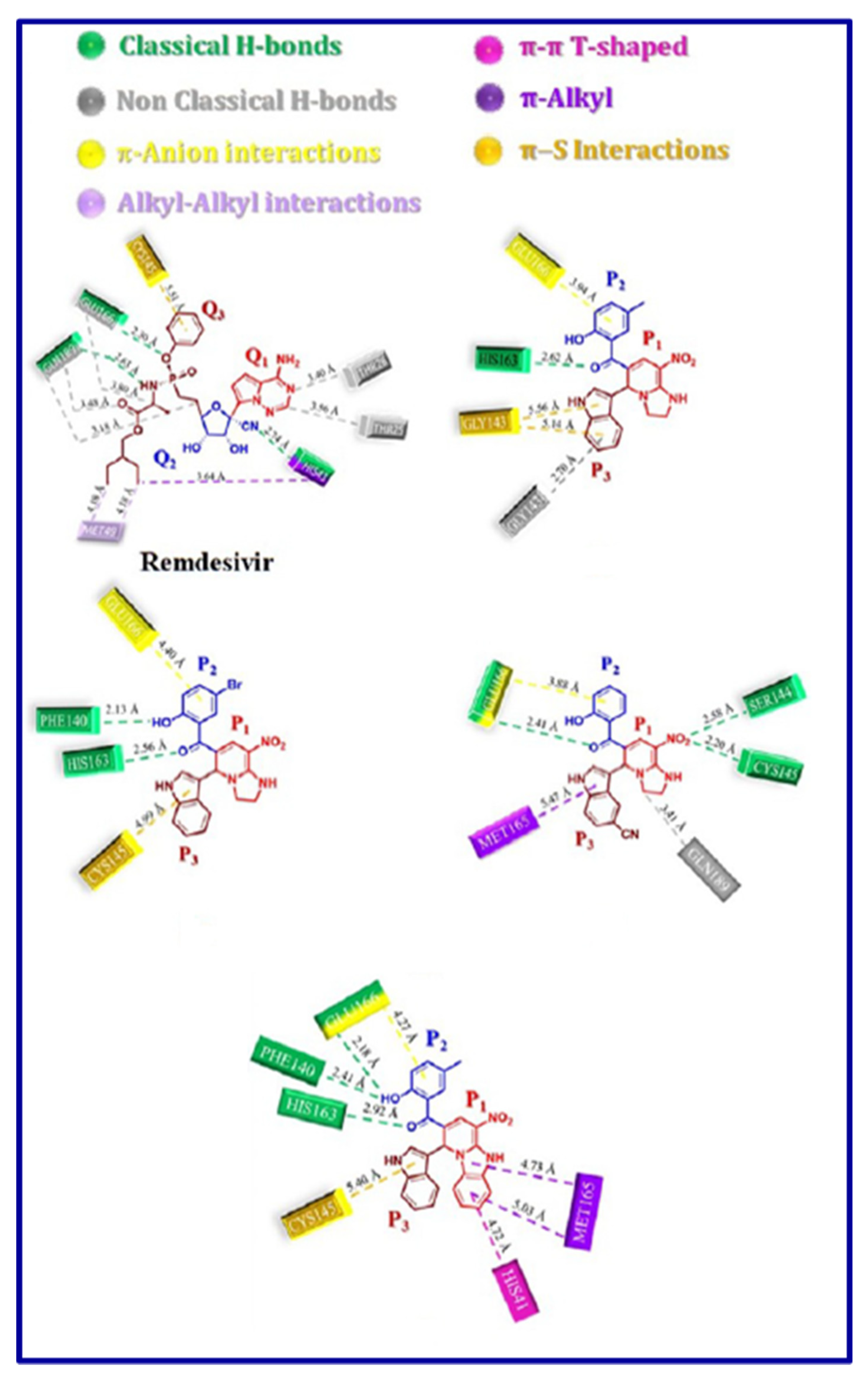
Figure 24.
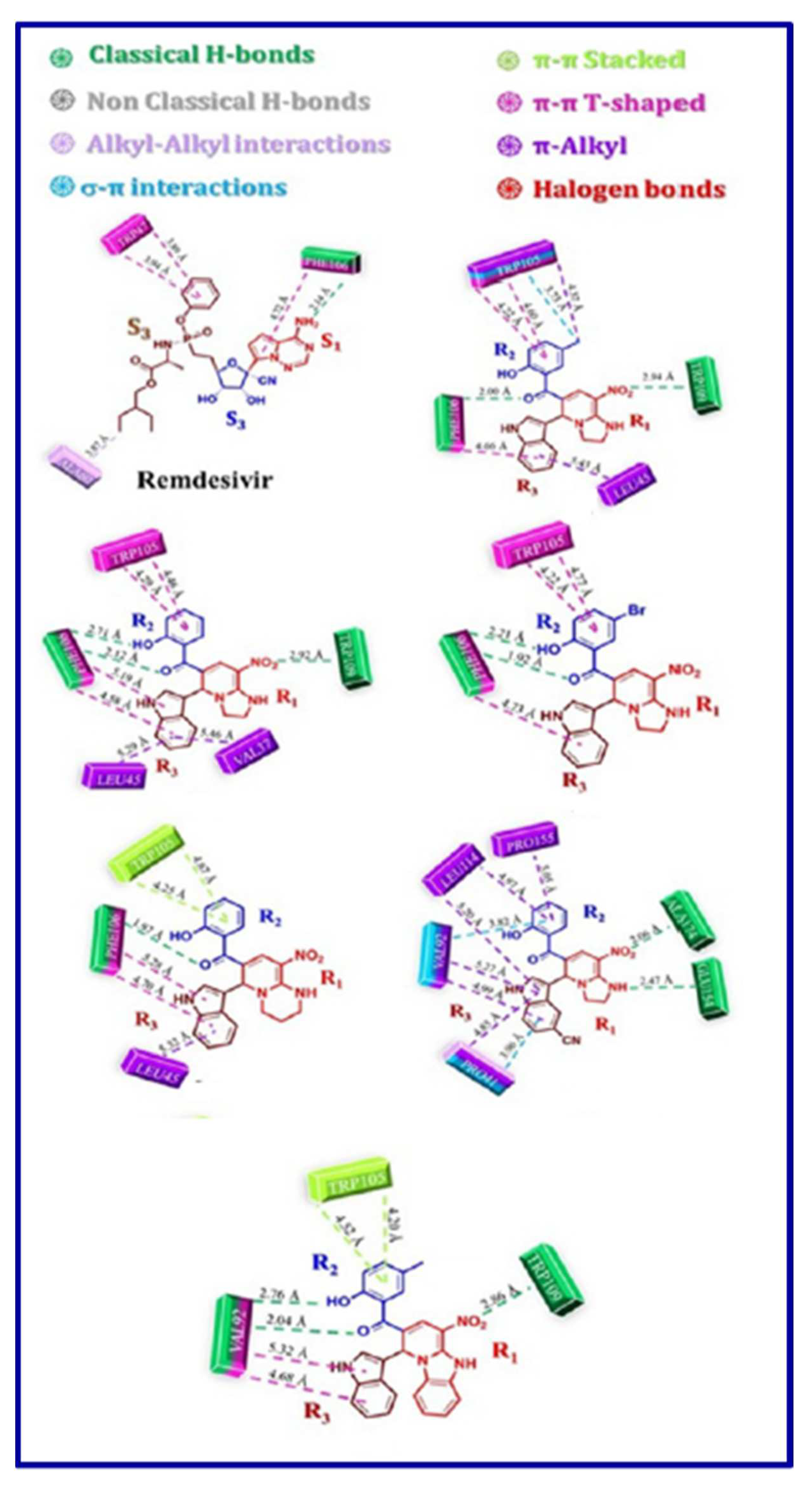
(continued). Representation of Remdesivir and predicted 3-substituted indoles 21 revealing potential properties against 7NX7.
Figure 24.
(continued). Representation of Remdesivir and predicted 3-substituted indoles 21 revealing potential properties against 7NX7.
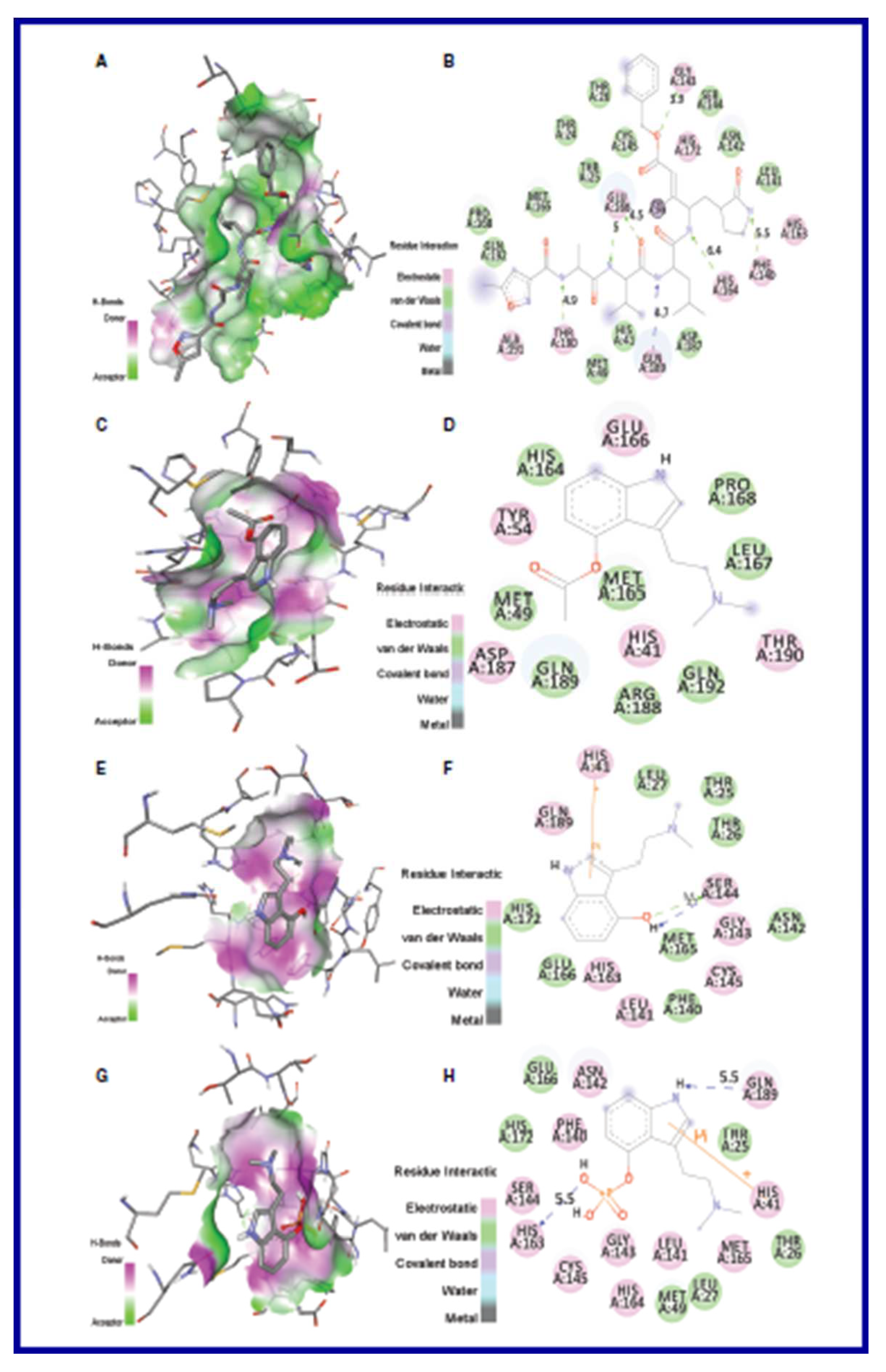
Many mushroom metabolites have potential biological activities. Psilacetin, psilocin, and psilocybine, which are psilocybin-mushroom components, have been subjected to Mpro SARS-CoV-2 docking studies (PDB: 6LU7) utilizing AutoDock and AutoDock vina software. They reveal considerable binding affinity in the protein active site (interaction docking scores = -6.0, -5.4, -5.8 kcal/mol for psilacetin, psilocin, and psilocybine, respectively) [159] (Figures 25,26).
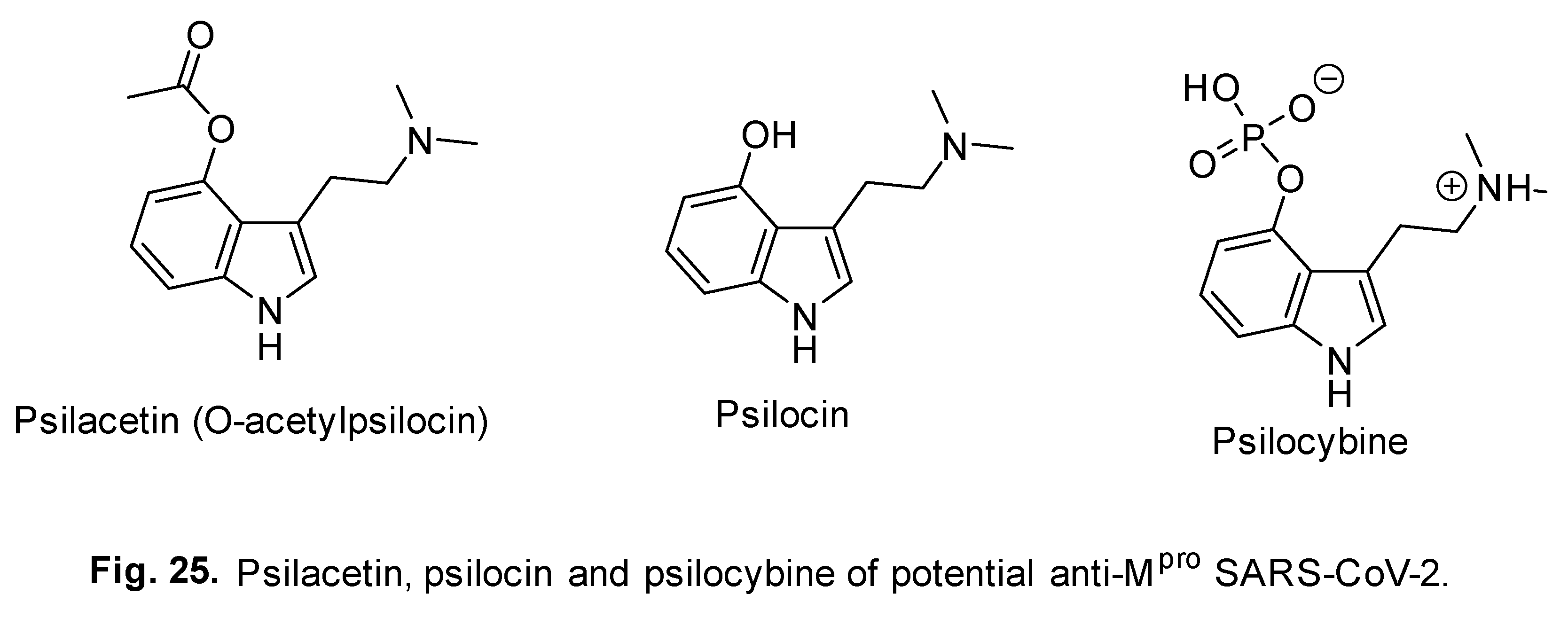
Figure 26.
2D- and 3D-docking interactions of A/B, N3 inhibitor; C/D, psilacetin; E/F, psilocin; and G/H, psilocybine in the active pocket of Mpro SARS-CoV-2 (PDB: 6LU7).
Figure 26.
2D- and 3D-docking interactions of A/B, N3 inhibitor; C/D, psilacetin; E/F, psilocin; and G/H, psilocybine in the active pocket of Mpro SARS-CoV-2 (PDB: 6LU7).
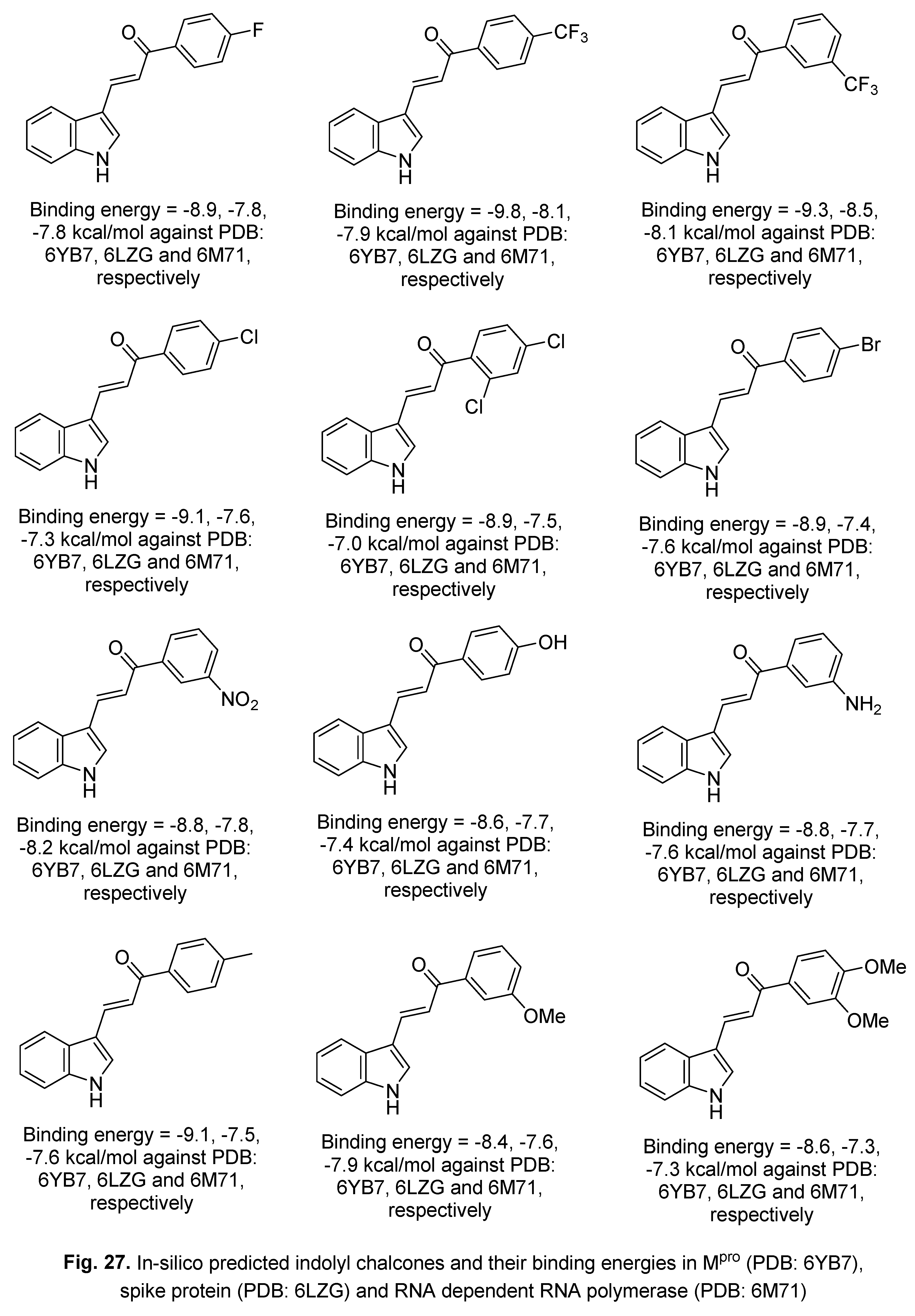
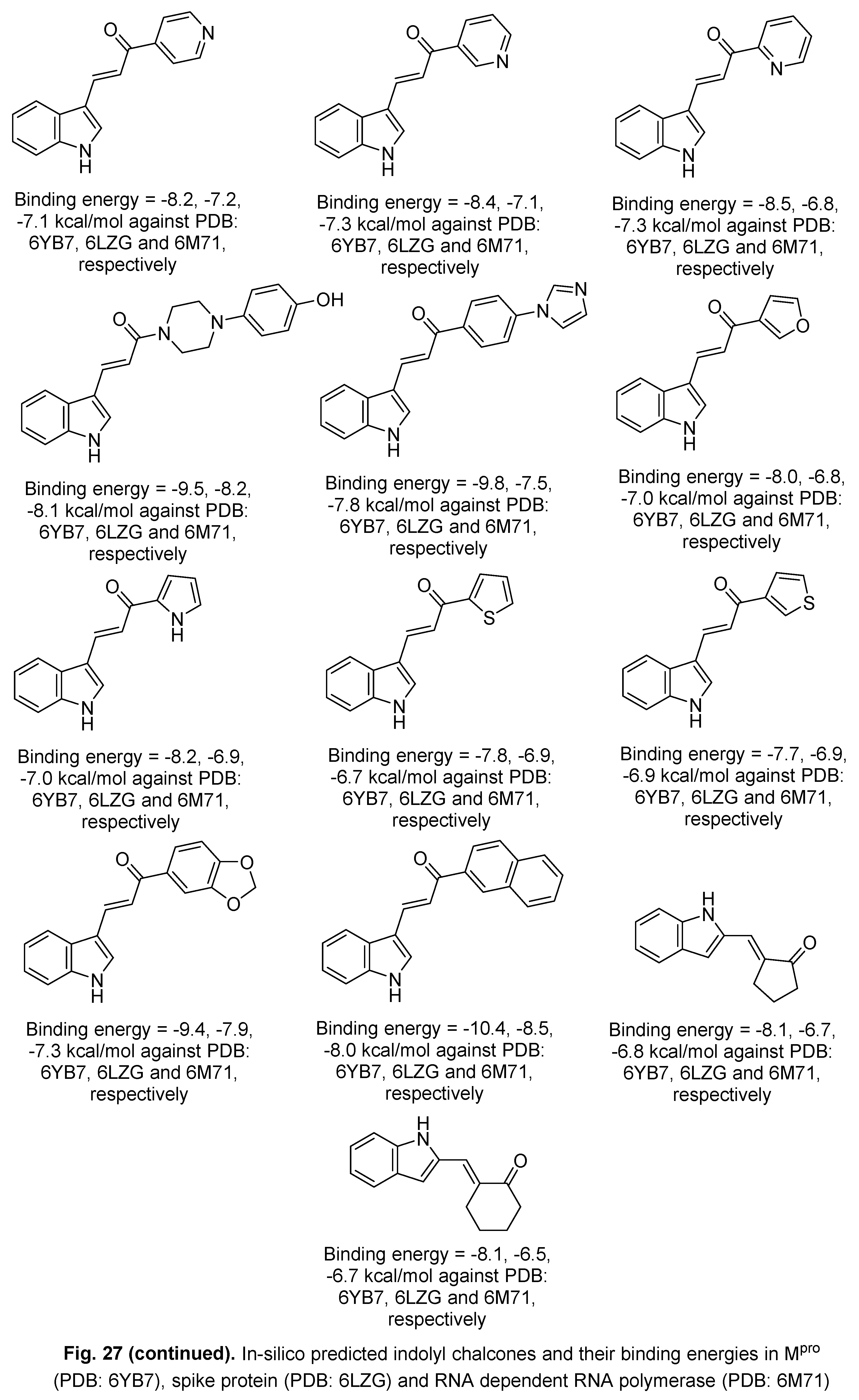
A series of indolyl chalcones have also been explored against Mpro (PDB: 6YB7), spike protein (PDB: 6LZG) and RNA dependent RNA polymerase (PDB: 6M71) in-silico by the blind docking technique utilizing AutoDock Vina v.1.1.2. Some of the results suggested promising inhibitory properties that may help narrow the search for anti-SARS-CoV-2 candidates [160] (Figure 27).
The Schiff bases formed from the condensation of isatin and 2-(1-aminobenzyl)benzimidazole revealed in-silico possible Mpro SARS-CoV-2 inhibitory properties (3CL protease, PDB: 6LU7, AutoDock 4.2 software). The 5-bromo-substituted analog of bis-Schiff base 22 formed from the condensation of 2-(1-aminobenzyl)benzimidazole and the corresponding bis-isatin in ethanol containing a few drops of AcOH at room temperature (Scheme 13) is the most promising [161] (Figure 28).
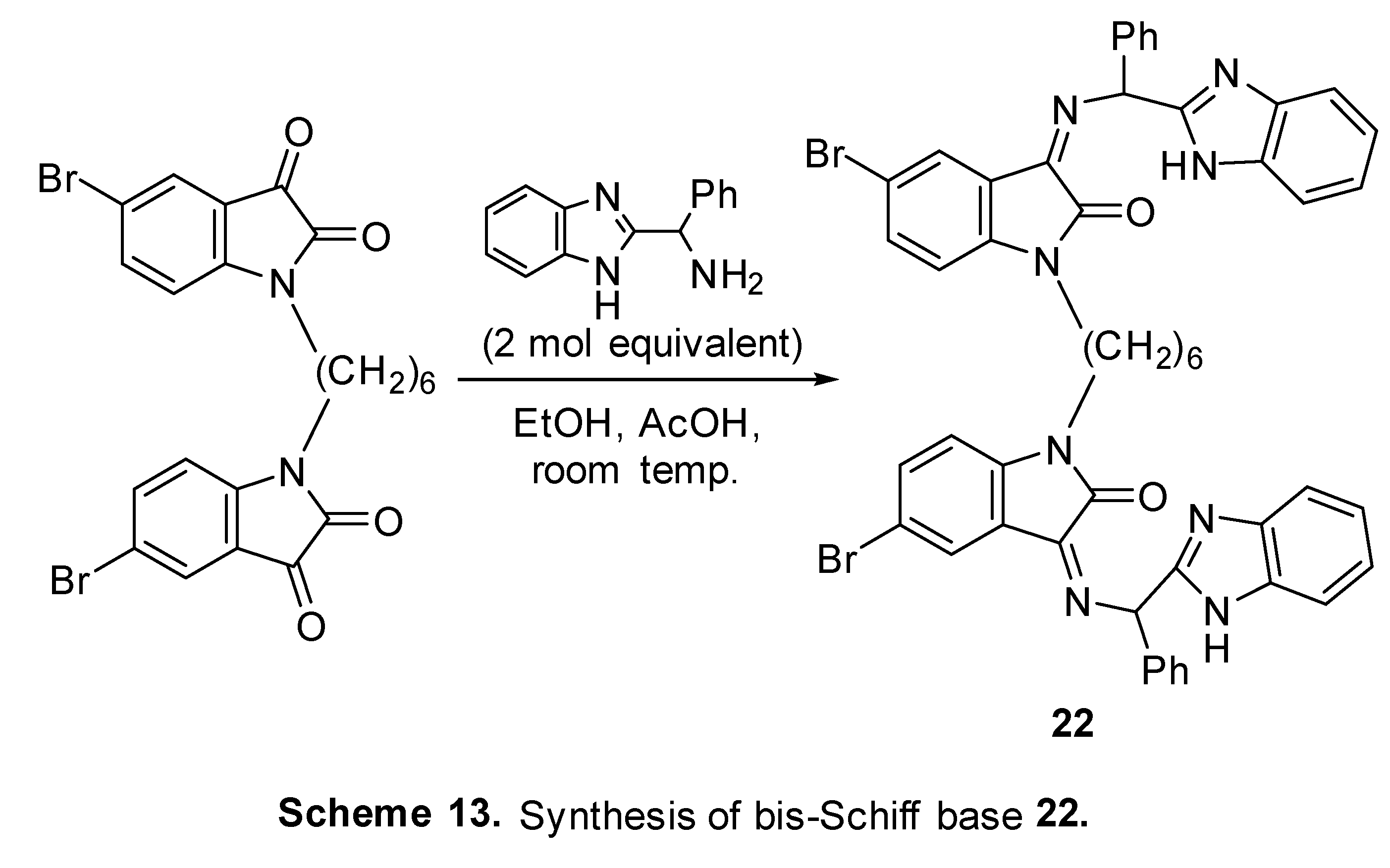
Figure 28.
2D-docking interaction of Schiff bases and N3 in the active site of Mpro SARS-CoV-2 (PDB: 6LU7).
Figure 28.
2D-docking interaction of Schiff bases and N3 in the active site of Mpro SARS-CoV-2 (PDB: 6LU7).
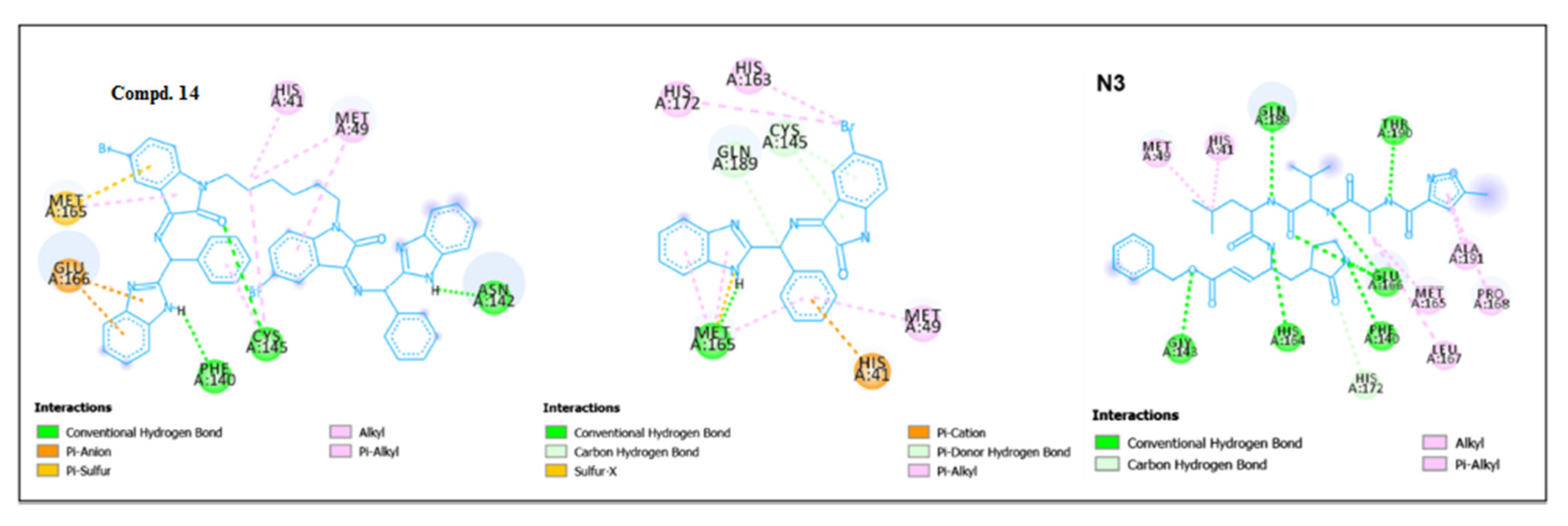
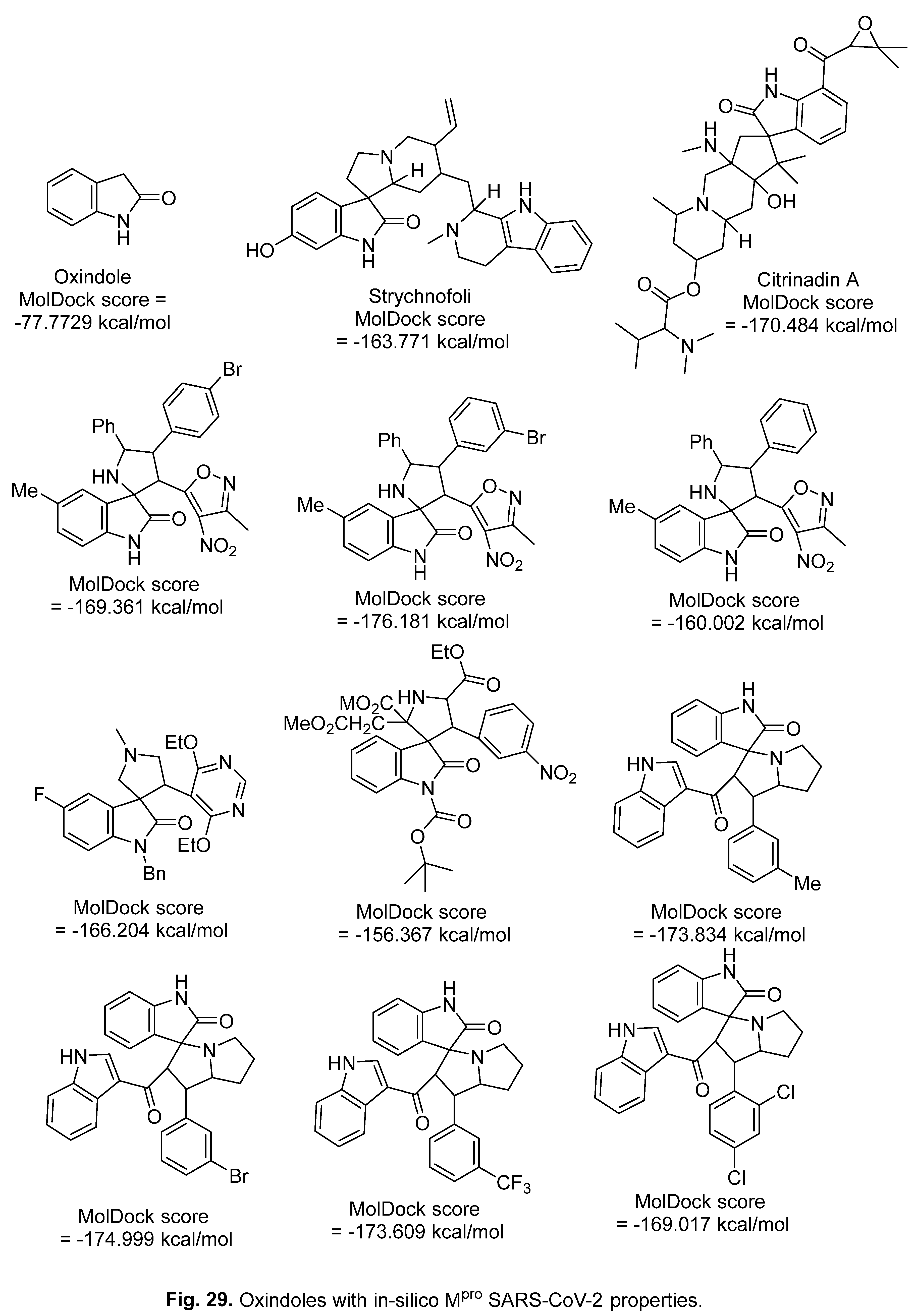
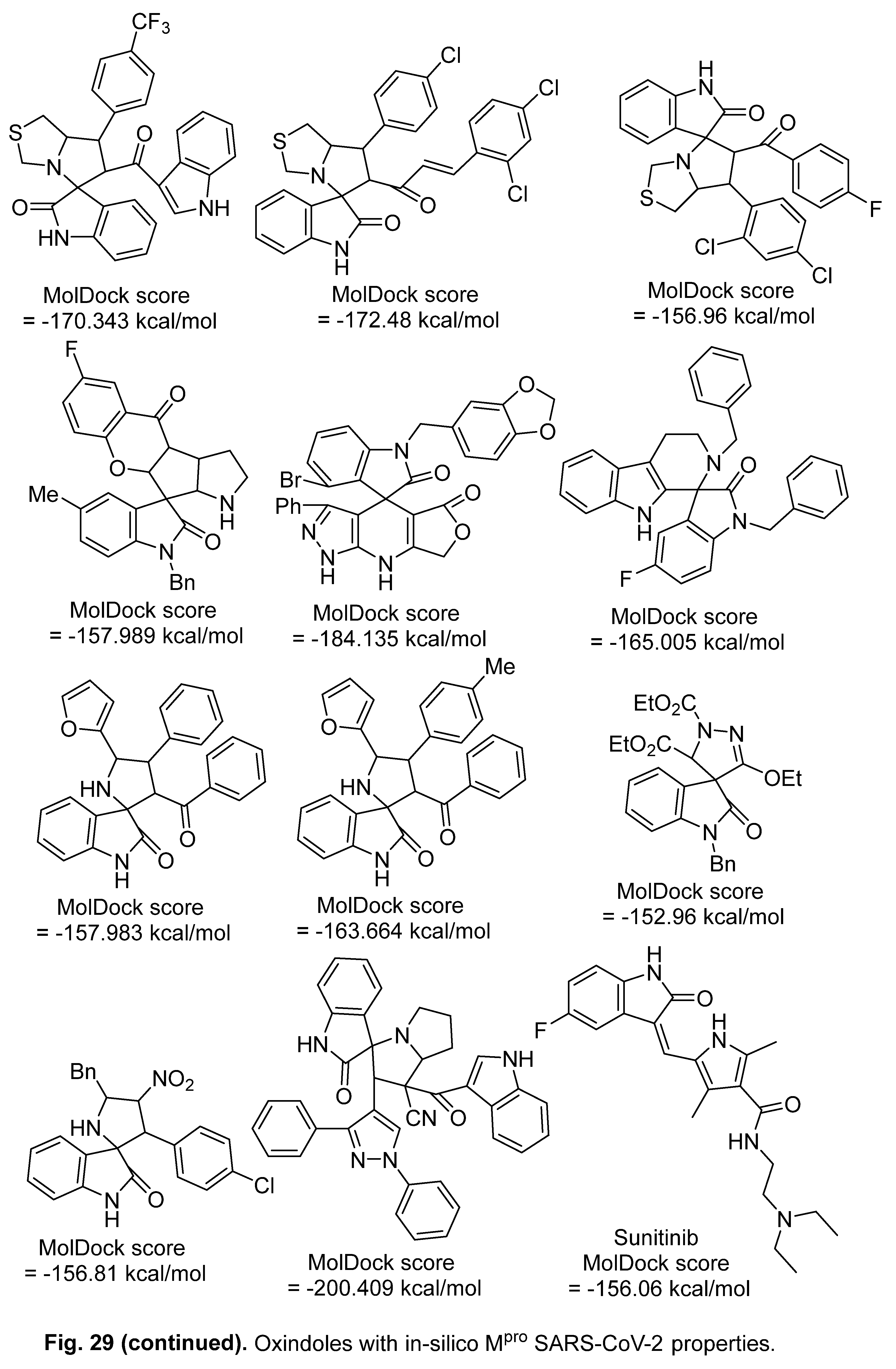
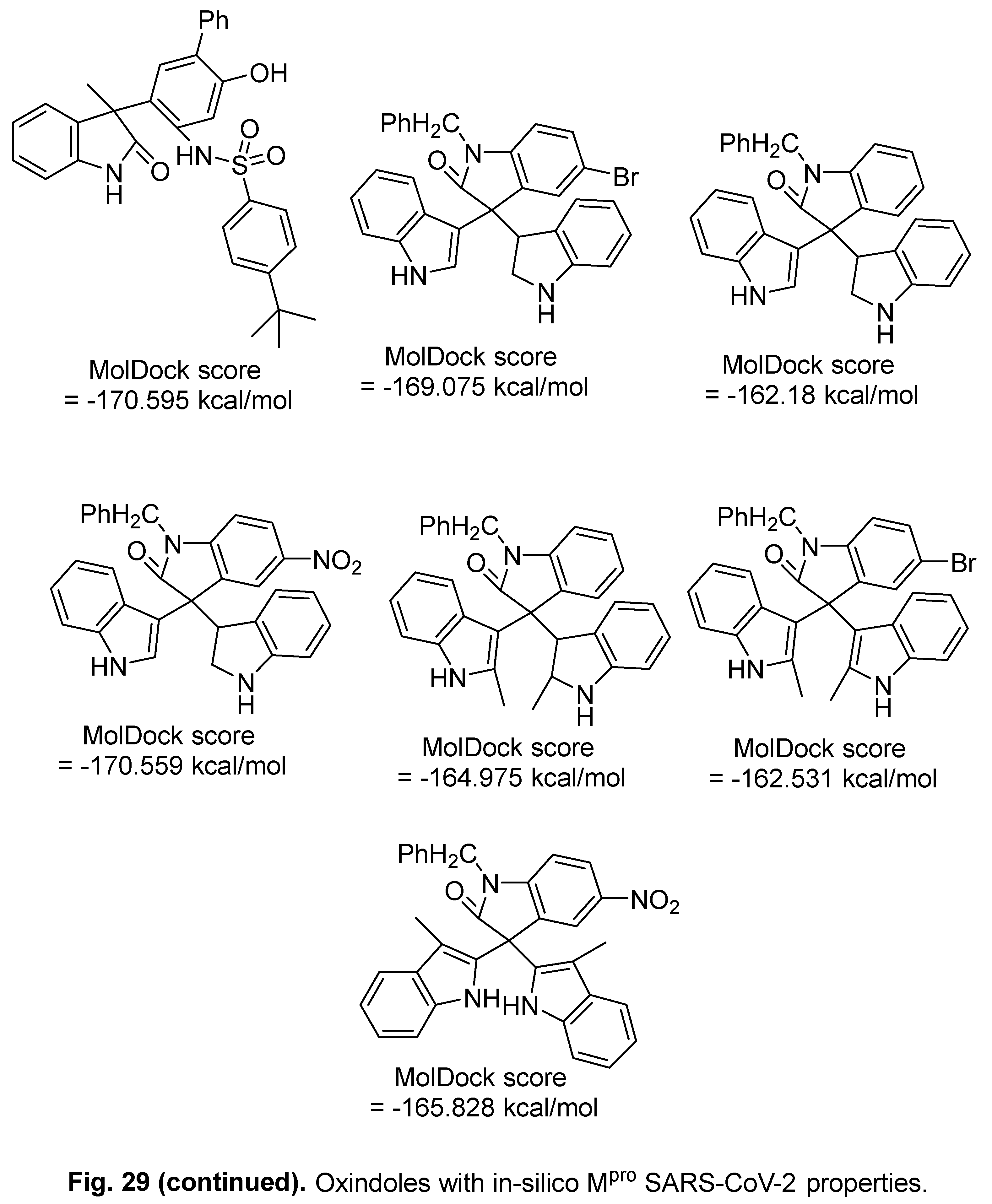
A set of 2-oxindole derivatives with in-silico Mpro SARS-CoV-2 inhibitory properties were mentioned (PDB ID: 6LU7, Molegro Virtual Docker version 7.0.0 Software, MVD) [162] (Figure 29).
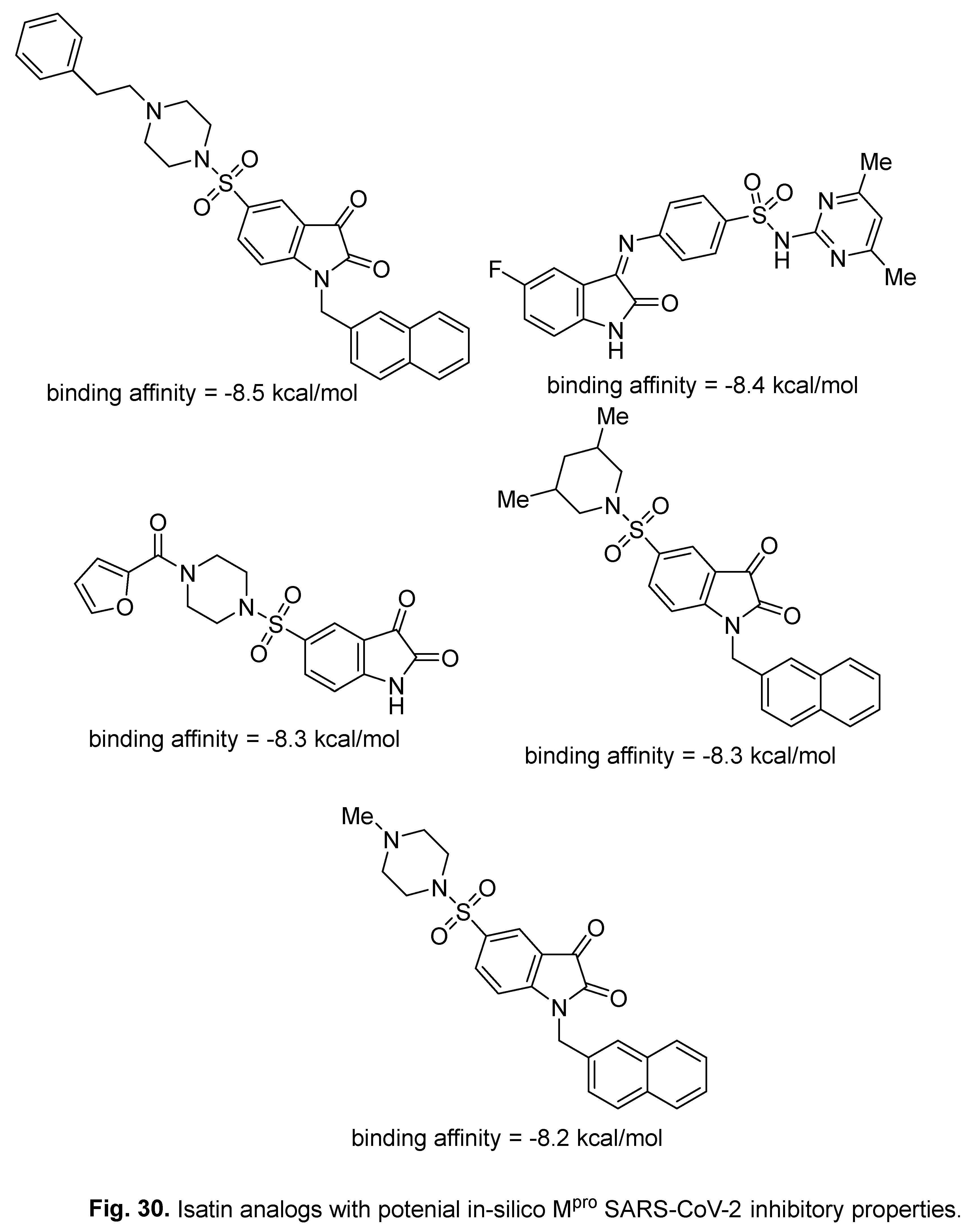
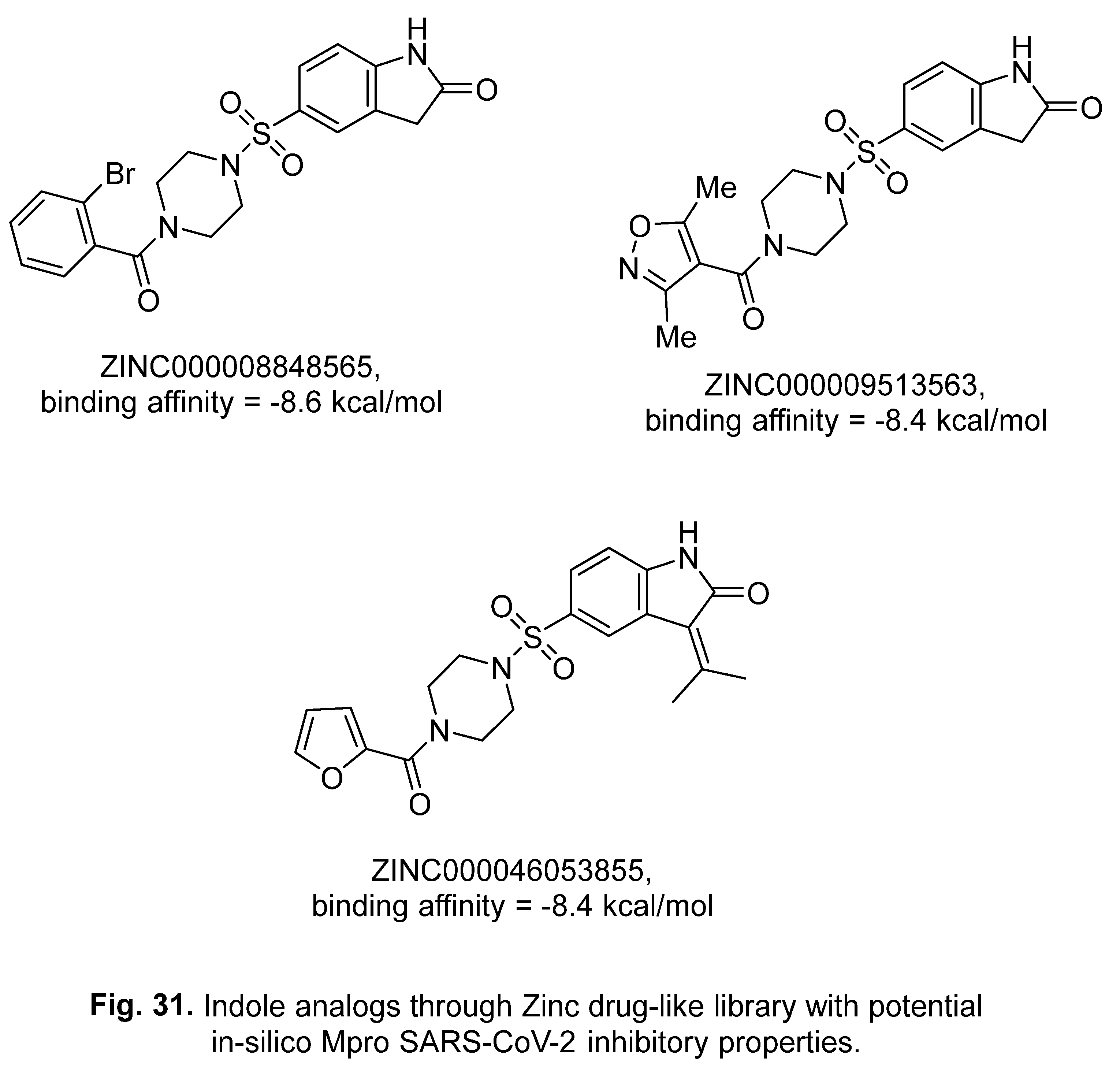
A set of isatin based protease inhibitors were collected from previous publications followed by in-silico high throughput screening in the active pocket of Mpro SARS-CoV-2 (chain-A, PDB: 6M03). The most promising agents were identified based on the observed binding affinities (Figure 30). Searching the Zinc drug-like library for similar analogs followed by virtual screening (AutoDock Vina), identified indole analogs with potential inhibitory properties against Mpro SARS-CoV-2 [72] (Figure 31).
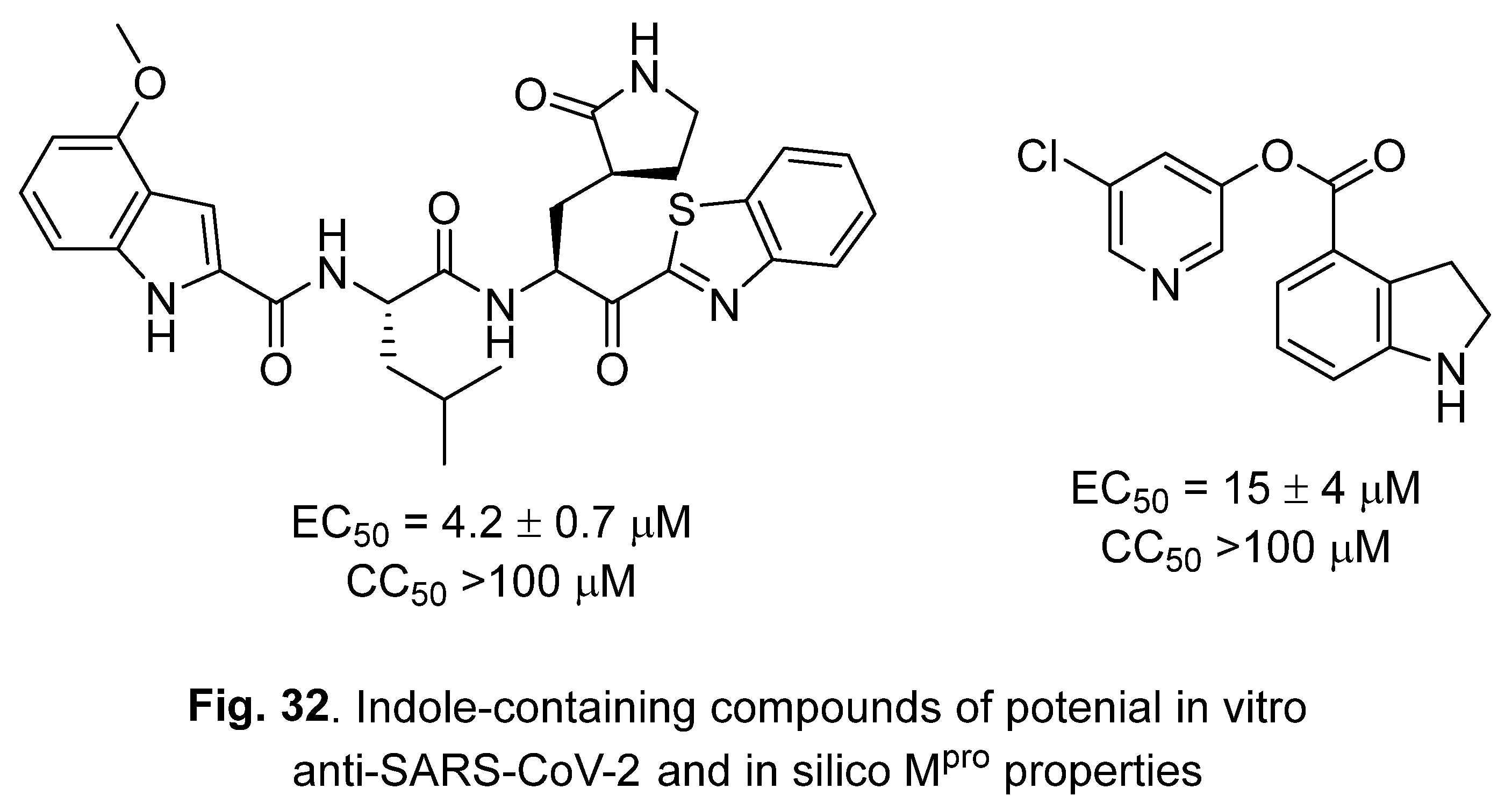
Hattori et al. have also reported the in-silico Mpro SARS-CoV-2 properties (PDB: 6Y2F, Maestro Version 10.7.015) in addition to the in vitro activity (Vero E6 assay) of indole-containing compounds [163] (Figure 32).
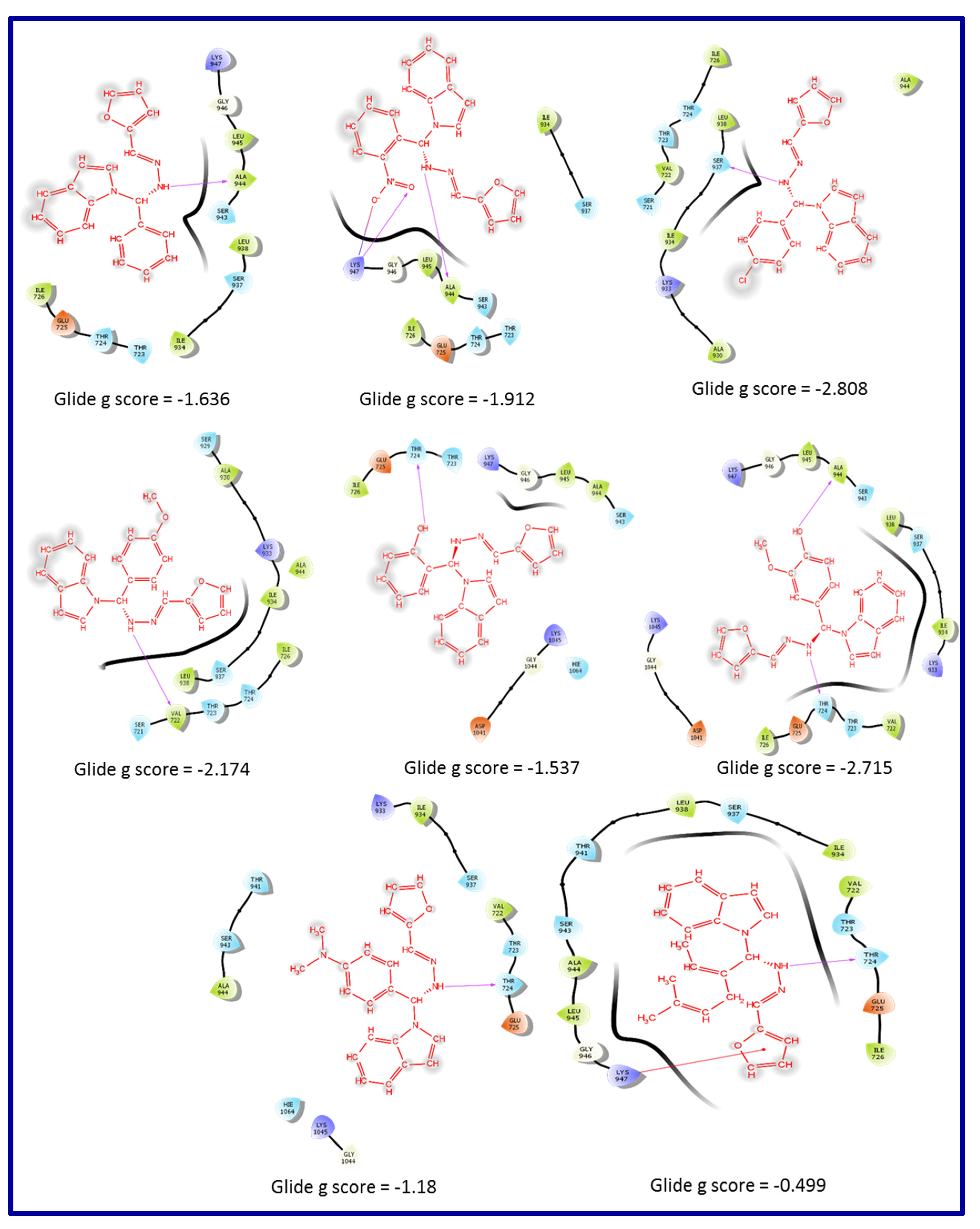
2-Indole-containing compounds 23 were obtained through the reaction of indole, furan-2-ylmethylenehydrazine, and appropriate aldehyde in ethanol (Scheme 14). Considerable activity against SARS-CoV-2 spike glycoprotein (PDB: 6WPT, Schrodinger 12.4 software) was observed for some of the synthesized agents [164] (Figure 33).
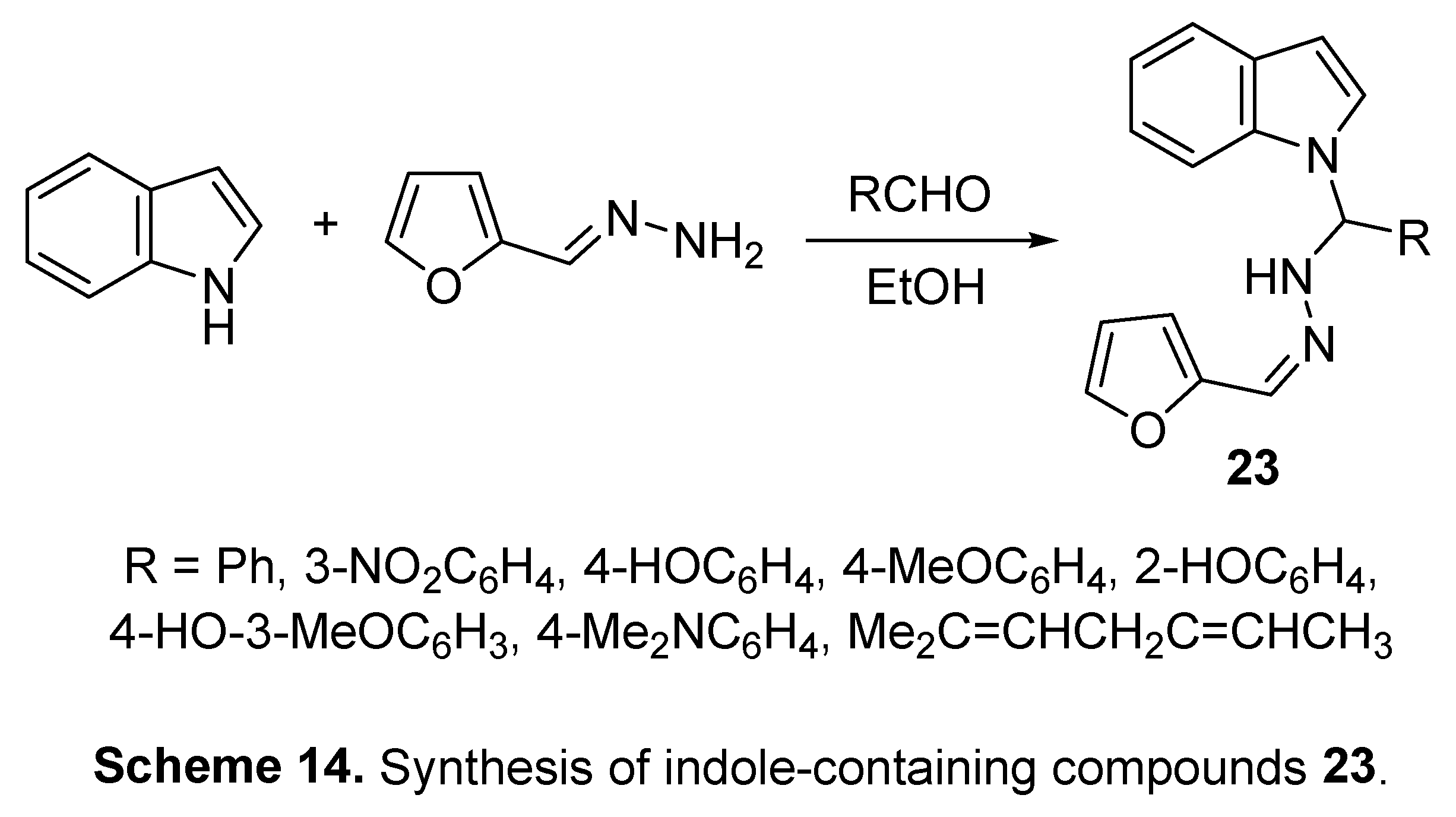
Figure 33.
2D- docking interaction of indole-containing compounds 23 in the active site of SARS-CoV-2 spike glycoprotein (PDB: 6WPT).
Figure 33.
2D- docking interaction of indole-containing compounds 23 in the active site of SARS-CoV-2 spike glycoprotein (PDB: 6WPT).
5.2. RdRp (RNA-dependent RNA polymerase) inhibitor
The RdRp enzyme is one of the most reliable targets for optimizing potent antiviral therapeutics. This is attributed to its ability to terminate the viral RNA replication in addition to the lack of any similar RdRp in the host cell, thus minimizing off-target effects [9,165].
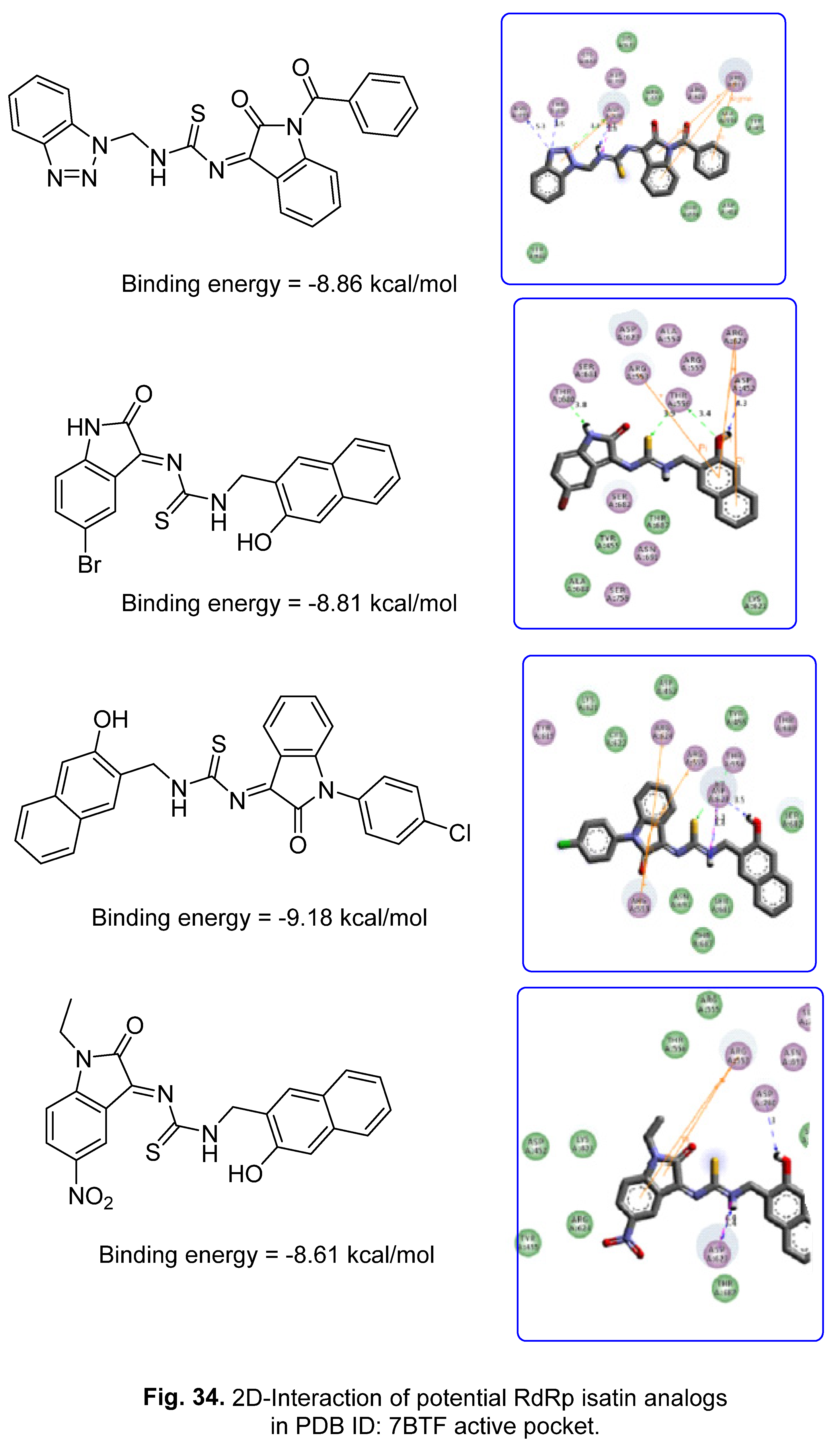
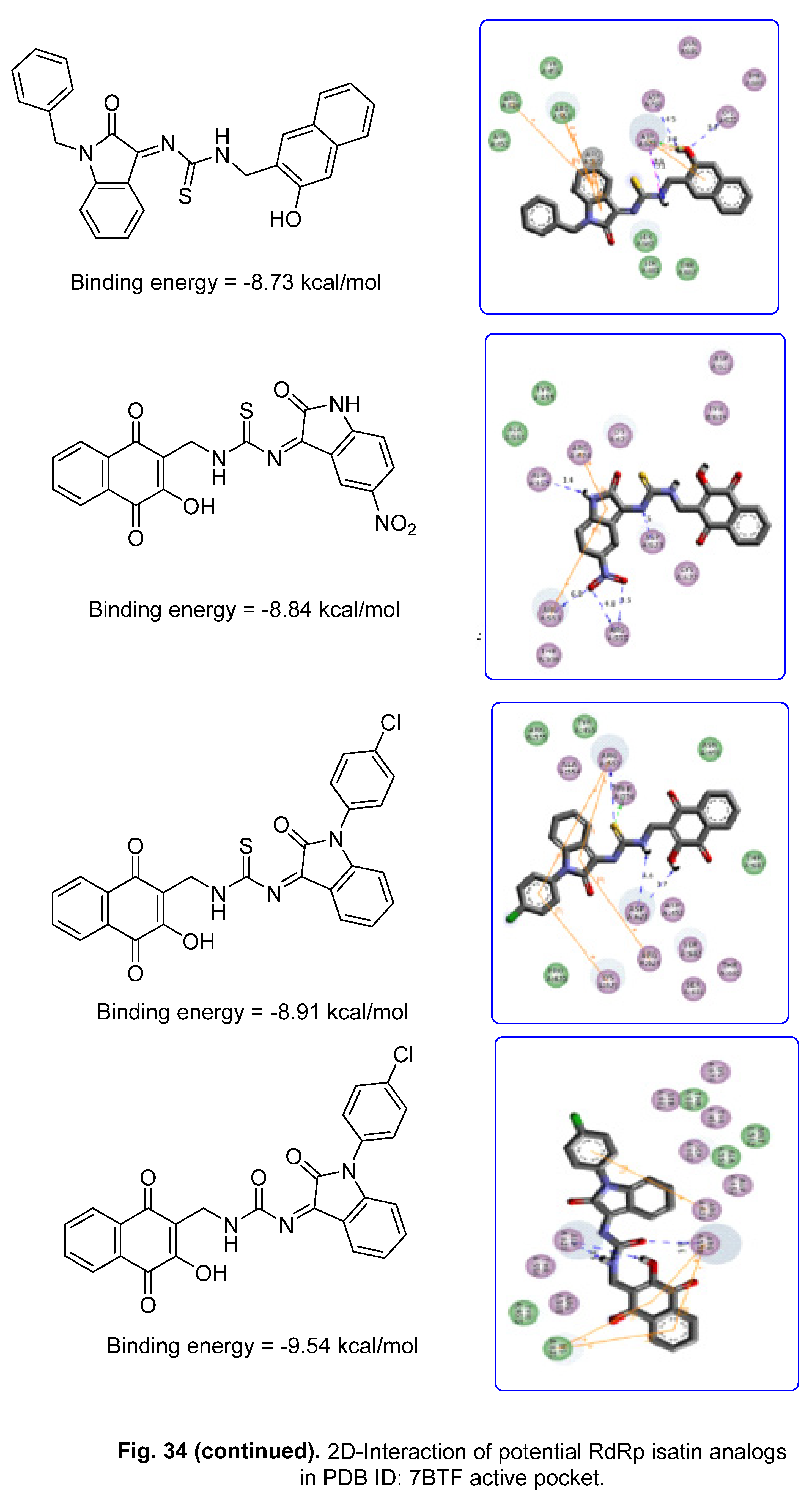
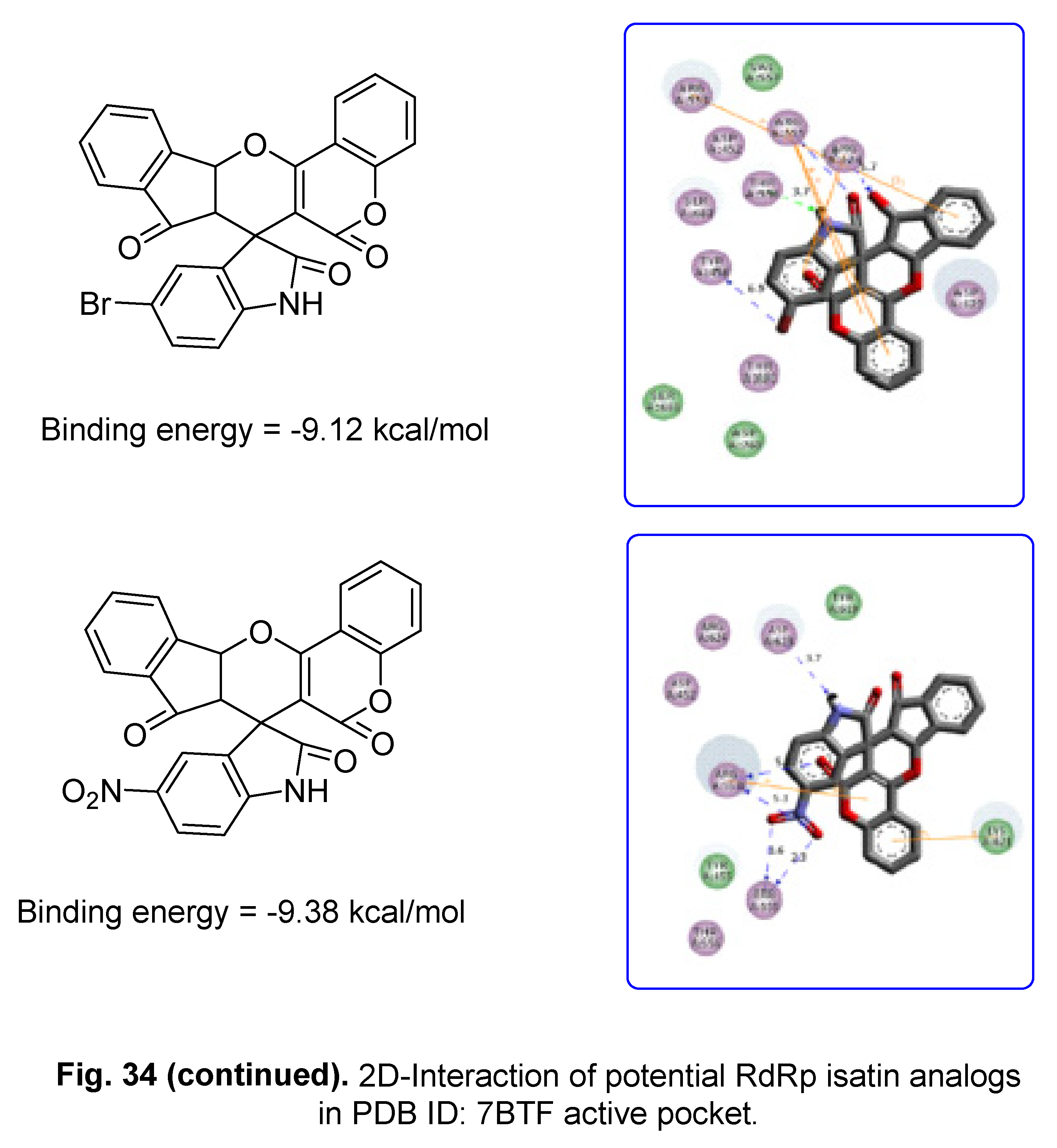
A computational study has also explored isatin analogs for the identification of promising RdRp SARS-CoV-2 inhibitor agents (PDB ID: 7BTF, AutoDock), and the most promising compounds discovered are exhibited in Figure 34 [166].
6. Conclusion
COVID-19 has proven to be one of the most serious crises facing human health in recorded history. The scientific community has been working tirelessly to optimize effective therapeutics, and while vaccination has been successful in controlling the pandemic, research into effective treatment of current and future mutants remains crucial. One area of focus has been on the indole scaffold, which includes many alkaloid categories and has shown promise in the fight against COVID-19. Repurposed indole-containing drugs as well as various natural and synthetic indole analogues have been investigated for anti-SARS-CoV-2 efficacy. In-silico studies utilized to assist in generating new hits and optimizing leads against SARS-CoV-2. 3-Alkenyl-2-oxindoles and spiroindoles also seem to be important anti-SARS-CoV-2 agents that can be synthesized in a regio-selective approach. From all the cited reports, it can be concluded that indole-containing compounds are important lead molecules and can be further optimized for development of potential agents against SARS-CoV-2.
Acknowledgments
This work was supported financially by National Research Centre, Egypt, project ID: 13060103.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
- N. George, M. J. Akhtar, K. A. Al Balushi, S. A. Khan, Rational drug design strategies for the development of promising multi-target directed indole hybrids as anti-Alzheimer agents, Bioorg. Chem. 127 (2022) 105941. [CrossRef]
- H.-L. Qin, J. Liu, W.-Y. Fang, L. Ravindar, K. P. Rakesh, Indole-based derivatives as potential antibacterial activity against methicillin-resistance Staphylococcus aureus (MRSA), Eur. J. Med. Chem. 194 (2020) 112245. [CrossRef]
- A. Ramkissoon, M. Seepersaud, A. Maxwell, J. Jayaraman, A. Ramsubhag, Isolation and antibacterial activity of indole alkaloids from Pseudomonas aeruginosa UWI-1, Molecules 25 (2020) 3744. [CrossRef]
- Y. Liu, Y. Cui, L. Lu, Y. Gong, W. Han, G. Piao, Natural indole-containing alkaloids and their antibacterial activities, Arch Pharm. 353 (2020) e2000120. [CrossRef]
- T. Meng, Y. Hou, C. Shang, J. Zhang, B. Zhang, Recent advances in indole dimers and hybrids with antibacterial activity against methicillin-resistant Staphylococcus aureus, Arch Pharm. 354 (2021) e2000266. [CrossRef]
- J. Ma, Y. Jiang, X. Zhuang, H. Chen, Y. Shen, Z. Mao, G. Rao, R. Wang, Discovery of novel indole and indoline derivatives against Candida albicans as potent antifungal agents, Bioorg. Med. Chem. Lett. 71 (2022) 128826. [CrossRef]
- M. Bolous, N. Arumugam, A. I. Almansour, R. S. Kumar, K. Maruoka, V. C. Antharam, S. Thangamani, Broad-spectrum antifungal activity of spirooxindolo-pyrrolidine tethered indole/imidazole hybrid heterocycles against fungal pathogens, Bioorg. Med. Chem. Lett. 29 (2019) 2059–2063. [CrossRef]
- M.-L. Yang J. Chen, M. Sun, D.-B. Zhang, K. Gao, Antifungal indole alkaloids from Winchia calophylla, Planta Med. 82 (2016) 712‒716. /: 82 (2016) 712‒716, https. [CrossRef]
- M. S. Bekheit, S. S. Panda, A. S. Girgis, Potential RNA-dependent RNA polymerase (RdRp) inhibitors as prospective drug candidates for SARS-CoV-2, Eur. J. Med. Chem. 252 (2023) 115292. [CrossRef]
- S. Nie, J. Zhao, X. Wu, Y. Yao, F. Wu, Y.-L. Lin, X. Li, A. R. Kneubehl, M. B. Vogt, R. Rico-Hesse, Y. Song, Synthesis, structure-activity relationship and antiviral activity of indole-containing inhibitors of Flavivirus NS2B-NS3 protease, Eur. J. Med. Chem. 225 (2021) 113767. /: 225 (2021) 113767, https. [CrossRef]
- C. Wei, L. Zhao, Z. Sun, D. Hu, B. Song, Discovery of novel indole derivatives containing dithioacetal as potential antiviral agents for plants, Pestic. Biochem. Physiol. 166 (2020) 104568. [CrossRef]
- M.-Z. Zhang, Q. Chen, G.-F. Yang, A review on recent developments of indole-containing antiviral agents, Eur. J. Med. Chem. 89 (2015) 421‒441. 2015. [CrossRef]
- J. Blaising, S. J. Polyak, E.-I. Pecheur, Arbidol as a broad-spectrum antiviral: An update, Antiviral Res. 107 (2014) 84–94. [CrossRef]
- M. Giampieri, A. Balbi, M. Mazzei, P. La Collab, C. Ibba, R. Loddo, Antiviral activity of indole derivatives, Antiviral Res. 3 (2009) 179–185. /. [CrossRef]
- V. Mashayekhi, K. H. M. E. Tehrani, P. Azerang, S. Sardari, F. Kobarfard, Synthesis, antimycobacterial and anticancer activity of novel indole-based thiosemicarbazones, Arch. Pharm. Res. 44 (2021) 764–776. /. [CrossRef]
- B. Yu, D.-Q. Yu. H.-M. Liu, Spirooxindoles: Promising scaffolds for anticancer agents, Eur. J. Med. Chem. 97 (2015) 673‒698. [CrossRef]
- M. Chauhan, A. Saxena, B. Saha, An insight in the anti-malarial potential of indole scaffold: A review, Eur. J. Med. Chem. 218 (2021) 113400. [CrossRef]
- A. S. Surur, S. A. Huluka, M. L. Mitku, K. Asres, Indole: The after next scaffold of antiplasmodial agents?, Drug Des. Devel. Ther. 14 (2020) 4855–4867. /. [CrossRef]
- J.-Y. Li, X.-F. Sun, J.-J. Li, F. Yu, Y. Zhang, X.-J. Huang, F.-X. Jiang, The antimalarial activity of indole alkaloids and hybrids, Arch Pharm. 353 (2020) e2000131. [CrossRef]
- S. N. S. Vasconcelos, K. A. Meissner, W. R. Ferraz, G. H. G. Trossini, C. Wrenger, H. A. Stefani, Indole-3-glyoxyl tyrosine: synthesis and antimalarial activity against Plasmodium falciparum, Future Med. Chem. 11 (2019) 525–538. /, 2019. [CrossRef]
- Y. Tamura, I. Morita, Y. Hinata, E. Kojima, H. Ozasa, H. Ikemoto, M. Asano, T. Wada, Y. Hayasaki-Kajiwara, T. Iwasaki, K. Matsumura, Identification of novel indole derivatives as highly potent AMPK activators with anti-diabetic profiles, Bioorg. Med. Chem. Lett. 68 (2022) 128769. [CrossRef]
- M. Nazir, M. A. Abbasi, Aziz-ur-Rehman, S. Z. Siddiqui, K. M. Khan, Kanwal, U. Salar, M. Shahid, M. Ashraf, M. A. Lodhi, F. A. Khan, New indole based hybrid oxadiazole scaffolds with N-substituted acetamides: As potent anti-diabetic agents, Bioorg. Chem. 81 (2018) 253–263. [CrossRef]
- A. Kumari, R. K. Singh, Synthesis, molecular docking and biological evaluation of N-substituted indole derivatives as potential anti-inflammatory and antioxidant agents, Chem. Biodivers. 19 (2022) e202200290. [CrossRef]
- Ì. T. T. Jacob, F. O. S. Gomes, M. D. S. de Miranda, S. M. V. de Almeida, I. J. da Cruz-Filho, C. A. Peixoto, T. G. da Silva, D. R. M. Moreira, C. M. L. de Melo, J. F. de Oliveira, M. C. A. de Lima, Anti-inflammatory activity of novel thiosemicarbazone compounds indole-based as COX inhibitors, Pharmacol. Rep. 73 (2021) 907‒925. [CrossRef]
- L.-L. Song, Y.-L. Mu, H.-C. Zhang, G.-Y. Wu, J.-Y. Sun, A new indole alkaloid with anti-inflammatory from the branches of Nauclea officinalis, Nat. Prod. Res. 34 (2020) 2283‒2288. [CrossRef]
- S. Sharma, D. Kumar, G. Singh, V. Monga, B. Kumar, Recent advancements in the development of heterocyclic anti-inflammatory agents, Eur. J. Med. Chem. 200 (2020) 112438.
- L. Jiang, H. Pu, X. Qin, J. Liu, Z. Wen, Y. Huang, J. Xiang, Y. Xiang, J. Ju, Y. Duan, Y. Huang, Syn-2, 3-diols and anti-inflammatory indole derivatives from Streptomyces sp. CB09001. Nat. Prod. Res. 35 (2021) 144‒151. [CrossRef]
- Y. Hong, Y.-Y. Zhu, Q. He, S.-X. Gu, Indole derivatives as tubulin polymerization inhibitors for the development of promising anticancer agents, Bioorg. Med. Chem. 55 (2022) 116597. 116597. [CrossRef]
- https://www.drugs.com/history/tivorbex.html (accessed on , 2023). 6 July.
- G. Li, Y. Wang, E. De Clercq, Approved HIV reverse transcriptase inhibitors in the past decade, Acta Pharm. Sin. B 12 (2022) 1567‒1590. [CrossRef]
- https://pubmed.ncbi.nlm.nih.gov/11364363/ (accessed on , 2023). 6 July.
- https://go.drugbank.com/drugs/DB13609 (accessed on , 2023). 6 July.
- https://www.accessdata.fda.gov/drugsatfda_docs/label/2007/018285s034lbl.pdf (accessed on , 2023). 6 July.
- W. J. Cronenwett, Schizophrenia pharmacology: Past, present, and future targets for intervention, Focus 14 (2016) 308–314. [CrossRef]
- R. B. Mailman, V. Murthy, Third generation antipsychotic drugs: partial agonism or receptor functional selectivity?, Curr Pharm Des. 16 (2010) 488–501. /: 16 (2010) 488–501, https. [CrossRef]
- https://www.drugs.com/history/zuplenz.html (accessed on , 2023). 6 July.
- https://www.drugs.com/history/serdolect.html (accessed on , 2023). 6 July.
- https://www.thepharmaletter.com/article/merck-s-maxalt-approved-in-usa (accessed on , 2023). 6 July.
- Y. Han, W. Dong, Q. Guo, X. Li, L. Huang, The importance of indole and azaindole scaffold in the development of antitumor agents, Eur. J. Med. Chem. 203 (2020) 112506. [CrossRef]
- https://www.drugs.com/history/sutent.html (accessed on , 2023). 6 July.
- https://www.cancer.gov/about-cancer/treatment/drugs/sunitinibmalate (accessed on , 2023). 6 July.
- https://www.drugs.com/history/tagrisso.html (accessed on , 2023). 6 July.
- https://www.cancer.gov/about-cancer/treatment/drugs/osimertinib (accessed on , 2023). 6 July.
- https://www.cancer.gov/about-cancer/treatment/drugs/rucaparibcamsylate (accessed on , 2023). 6 July.
- S. Li, Anlotinib: A novel targeted drug for bone and soft tissue sarcoma, Front. Oncol. 11 (2021) 664853. [CrossRef]
- Y. Y. Syed, Anlotinib: First global approval, Drugs 78 (2018) 1057–1062. [CrossRef]
- https://www.drugs.com/history/farydak.html (accessed on , 2023). 6 July.
- https://www.drugs.com/history/rydapt.html (accessed on , 2023). 6 July.
- https://www.drugs.com/history/alecensa.html (accessed on , 2023). 6 July.
- https://www.cancer.gov/about-cancer/treatment/drugs/alectinib (accessed on , 2023). 6 July.
- S. Dadashpour, S. Emami, Indole in the target-based design of anticancer agents: A versatile scaffold with diverse mechanisms, Eur. J. Med. Chem. 150 (2018) 9‒29. [CrossRef]
- R. Patil, S. A. Patil, K. D. Beaman, S. A. Patil, Indole molecules as inhibitors of tubulin polymerization: potential new anticancer agents, an update (2013–2015), Future Med. Chem. 8 (2016) 1291–1316. /: 8 (2016) 1291–1316, https. [CrossRef]
- S. A. Patil, R. Pati D. D. Miller, Indole molecules as inhibitors of tubulin polymerization: potential new anticancer agents, Future Med. Chem. 4 (2012) 2085–2115. [CrossRef]
- A. Ahmad, W. A. Sakr, K. M. W. Rahman, Anticancer properties of indole compounds: Mechanism of apoptosis induction and role in chemotherapy, Curr. Drug Targets 11 (2010) 652‒666. /. [CrossRef]
- S. S. Panda, A. S. Girgis, M. N. Aziz, M. S. Bekheit, Spirooxindole: A versatile biologically active heterocyclic scaffold, Molecules 28 (2023) 618. [CrossRef]
- I. A. Seliem, S. S. Panda, A. S. Girgis, Q. L. Tran, M. F. Said, M. S. Bekheit, A. Abdelnaser, S. Nasr, W. Fayad, A. A. F. Soliman, R. Sakhuja, T. S. Ibrahim, Z. K. M. Abdel-Samii, A. M. M. Al-Mahmoudy, Development of isatin-based Schiff bases targeting VEGFR-2 inhibition: Synthesis, characterization, antiproliferative properties, and QSAR studies, ChemMedChem 17 (2022) e202200164. [CrossRef]
- A. S. Girgis, S. S. Panda, M. N. Aziz, P. J. Steel, C. D. Hall, A. R. Katritzky, Rational design, synthesis, and 2D-QSAR study of anti-oncological alkaloids against hepatoma and cervical carcinoma, RSC Adv. 5 (2015) 28554–28569. [CrossRef]
- Y. Y. Lee, H. H. Park, W. Park, H. Kim, J. G. Jang, K. S. Hong, J.-Y. Lee, H. S. Seo, D. H. Na, T.-H. Kim, Y. B. Choy, J. H. Ahn, W. Lee, C. G. Park, Long-acting nanoparticulate DNase-1 for effective suppression of SARS-CoV-2-mediated neutrophil activities and cytokine storm, Biomaterials 267 (2021) 120389. [CrossRef]
- A. K. Ghosh, J. Raghavaiah, D. Shahabi, M. Yadav, B. J. Anson, E. K. Lendy, S.-i. Hattori, N. Higashi-Kuwata, H. Mitsuya, A. D. Mesecar, Indole chloropyridinyl ester-derived SARS-CoV-2 3CLpro Inhibitors: Enzyme inhibition, antiviral efficacy, structure‒activity relationship, and X-ray structural studies, J. Med. Chem. 64 (2021) 14702–14714. [CrossRef]
- S. K. Mishra, T. Tripathi, One year update on the COVID-19 pandemic: Where are we now?, Acta Tropica 214 (2021) 105778. 2021. [CrossRef]
- https://covid19.who.int/ (accessed on , 2023). 5 July.
- K. Jayabal, D. Elumalai, S. Leelakrishnan, S. Bhattacharya, V. Rengarajan, T. Kannan, S.-C. Chuang, Green and regioselective approach for the synthesis of3-substituted indole based 1,2-dihydropyridine and azaxanthone derivatives as a potential lead for SARS-CoV-2 and delta plus mutant virus: DFT and docking studies, ACS Omega 7 (2022) 43856−43876. [CrossRef]
- Shagufta, I. Ahmad, The race to treat COVID-19: Potential therapeutic agents for the prevention and treatment of SARS-CoV-2, Eur. J. Med. Chem. 213 (2021) 113157. [CrossRef]
- J. M. Sanders, M. L. Monogue, T. Z. Jodlowski, J. B. Cutrell, Pharmacologic treatments for coronavirus disease 2019 (COVID-19), A Review, JAMA 323 (2020) 1824‒1836. [CrossRef]
- L. Zheng, L. Zhang, J. Huang, K.S. Nandakumar, S. Liu, K. Cheng, Potential treatment methods targeting 2019-nCoV infection, Eur. J. Med. Chem. 205 (2020) 112687. [CrossRef]
- I. A. Seliem, S. S. Panda, A. S. Girgis, Y. Moatasim, A. Kandeil, A. Mostafa, M. A. Ali, E. S. Nossier, F. Rasslan, A. M. Srour, R. Sakhuja, T. S. Ibrahim, Z. K. M. Abdel-samii, A. M. M. Al-Mahmoudy, New quinoline-triazole conjugates: Synthesis, and antiviral properties against SARS-CoV-2, Bioorg. Chem. 114 (2021) 105117. [CrossRef]
- P. Zhou, X.-L. Yang, X.-G. Wang, B. Hu, L. Zhang, W. Zhang, H.-R. Si, Y. Zhu, B. Li, C.-L. Huang, H.-D. Chen, J. Chen, Y. Luo, H. Guo, R.-D. Jiang, M.-Q. Liu, Y. Chen, X.-R. Shen, X. Wang, X.-S. Zheng, K. Zhao, Q.-J. Chen, F. Deng, L.-L. Liu, B. Yan, F.-X. Zhan, Y.-Y. Wang, G.-F. Xiao, Z.-L. Shi, A pneumonia outbreak associated with a new coronavirus of probable bat origin, Nature 579 (2020) 270–273. [CrossRef]
- R. Banerjee, L. Perera, L. M. V. Tillekeratne, Potential SARS-CoV-2 main protease inhibitors, Drug Discov. Today, 26 (2021) 804‒816. [CrossRef]
- Y. Araf, F. Akter, Y.-d. Tang, R. Fatemi, S. A. Parvez, C. Zheng, G. Hossain, Omicron variant of SARS-CoV-2: Genomics, transmissibility, and responses to current COVID-19 vaccines, J. Med. Virol. 94 (2022) 1825–1832. [CrossRef]
- M. He, Y. Huang, Y. Wang, J. Liu, M. Han, Y. Xiao, N. Zhang, H. Gui, H. Qiu, L. Cao, W. Jia, S. Huang, Metabolomics-based investigation of SARS-CoV-2 vaccination (Sinovac) reveals an immune-dependent metabolite biomarker, Front. Immunol. 13 (2022) 954801. [CrossRef]
- R. Yapasert, P. Khaw-on, R. Banjerdpongchai, Coronavirus infection-associated cell death signaling and potential therapeutic targets, Molecules 26 (2021) 7459. [CrossRef]
- V. Varadharajan, G. S. Arumugam, S. Shanmugam, Isatin-based virtual high throughput screening, molecular docking, DFT, QM/MM, MD and MM-PBSA study of novel inhibitors of SARS-CoV-2 main protease, J. Biomol. Struct. Dyn. 40 (2022) 7852–7867. [CrossRef]
- Y. Hua, X. Dai, Y. Xu, G. Xing, H. Liu, T. Lu, Y. Chen, Y. Zhang, Drug repositioning: Progress and challenges in drug discovery for various diseases, Eur. J. Med. Chem. 234 (2022) 114239. [CrossRef]
- T. Pillaiyar, S. Meenakshisundaram, M. Manickam. M. Sankaranarayanan, A medicinal chemistry perspective of drug repositioning: Recent advances and challenges in drug discovery, Eur. J. Med. Chem. 195 (2020) 112275. [CrossRef]
- S. Kumar, S. Kovalenko, S. Bhardwaj, A. Sethi, N. Y. Gorobets, S. M. Desenko, Poonam, B. Rathi, Drug repurposing against SARS-CoV-2 using computational approaches, Drug Discov. Today 27 (2022) 2015‒2027. [CrossRef]
- K. Mohamed, N. Yazdanpanah, A. Saghazadeh, N. Rezaei, Computational drug discovery and repurposing for the treatment of COVID-19: A systematic review, Bioorg. Chem. 106 (2021) 104490. [CrossRef]
- W.-C. Chiou, M.-S. Hsu, Y.-T. Chen, J.-M. Yang, Y.-G. Tsay, H.-C. Huang, C. Huang, Repurposing existing drugs: identification of SARS-CoV-2 3C-like protease inhibitors, J. Enzyme Inhib. Med. Chem. 36 (2021) 147–153. [CrossRef]
- T. Asselah, D. Durantel, E. Pasmant, G. Lau, R. F. Schinazi, COVID-19: Discovery, diagnostics and drug development, J. Hepatology 74 (2021) 168–184. [CrossRef]
- A. Sarkar, K. Mandal, Repurposing an antiviral drug against SARS-CoV-2 main protease, Angew. Chem. Int. Ed. 60 (2021) 23492–23494. [CrossRef]
- P. N. Batalha, L. S. M. Forezi, C. G. S. Lima, F. P. Pauli, F. C. S. Boechat, M. C. B. V. de Souza, A. C. Cunha, V. F. Ferreira, F. d. C. da Silva, Drug repurposing for the treatment of COVID-19: Pharmacological aspects and synthetic approaches, Bioorg. Chem. 106 (2021) 104488. [CrossRef]
- J. Dowarah, B. N. Marak, U. C. S. Yadav, V. P. Singh, Potential drug development and therapeutic approaches for clinical intervention in COVID-19, Bioorg. Chem. 114 (2021) 105016. [CrossRef]
- N. Trivedi, A. Verna, D. Kumar, Possible treatment and strategies for COVID-19: review and assessment, Eur. Rev. Med. Pharmacol. Sci. 24 (2020) 12593‒12608. [CrossRef]
- N. A. Ashour, A. A. Elmaaty, A. A. Sarhan, E. B. Elkaeed, A. M. Moussa, I. A. Erfan, A. A. Al-Karmalawy, A systematic review of the global intervention for SARS-CoV-2 combating: From drugs repurposing to Molnupiravir approval, Drug Des. Devel. Ther. 16 (2022) 685–715. [CrossRef]
- J. Santos, S. Brierley, M. J. Gandhi, M. A. Cohen, P. C. Moschella, A. B. L. Declan, Repurposing therapeutics for potential treatment of SARS-CoV-2: A review, Viruses 12 (2020) 705. [CrossRef]
- X. Zhang, Y. Yang, M. Grimstein, G. Liu, E. Kitabi, J. Fan, Y.-H. Wang, J. Earp, J. L. Weaver, H. Zhu, J. Liu, K. S. Reynolds, S.-M. Huang, Y. Wang, Anti–SARS-CoV-2 repurposing drug database: Clinical pharmacology considerations, CPT Pharmacometrics Syst. Pharmacol. 10 (2021) 973–982. [CrossRef]
- A. Simonis, S. J. Theobald, G. Fätkenheuer, J. Rybniker, J. J. Malin, A comparative analysis of remdesivir and other repurposed antivirals against SARS-CoV-2, EMBO Mol. Med. 13 (2021) e13105. [CrossRef]
- https://go.drugbank.com/drugs/DB15661 (accessed on , 2023). 6 July.
- https://www.drugs.com/history/molnupiravir.html (accessed on , 2023). 6 July.
- https://www.drugs.com/history/paxlovid.html (accessed on , 2023). 6 July.
- A. M. Srour, S. S. Panda, A. Mostafa, W. Fayad, M. A. El-Manawaty, A. A. F. Soliman, Y. Moatasim, A. El Taweel, M. F. Abdelhameed, M. S. Bekheit, M. A. Ali, A. S. Girgis, Synthesis of aspirin-curcumin mimic conjugates of potential antitumor and anti-SARS-CoV-2 properties, Bioorg. Chem. 117 (2021) 105466. [CrossRef]
- I. A. Seliem, A. S. Girgis, Y. Moatasim, A. Kandeil, A. Mostafa, M. A. Ali, M. S. Bekheit, S. S. Panda, New pyrazine conjugates: Synthesis, computational studies, and antiviral properties against SARS-CoV-2, ChemMedChem 16 (2021) 3418–3427. [CrossRef]
- M. A. Youssef, S. S. Panda, D. R. Aboshouk, M. F. Said, A. El Taweel, M. GabAllah, W. Fayad, A. A. F. Soliman, A. Mostafa, N. G. Fawzy, A. S. Girgis, Novel curcumin mimics: Design, synthesis, biological properties and computational studies of piperidone-piperazine conjugates, ChemistrySelect 7 (2022) e202201406. [CrossRef]
- K. A. Wyman, A. S. Girgis, P. S. Surapaneni, J. M. Moore, N. M. Abo Shama, S. H. Mahmoud, A. Mostafa, R. F. Barghash, Z. Juan, R. D. Dobaria, A. J. Almalki, T. S. Ibrahim, S. S. Panda, Synthesis of potential antiviral agents for SARS-CoV-2 using molecular hybridization approach, Molecules 27 (2022) 5923. [CrossRef]
- C. Li, L. Wang, L. Ren, Antiviral mechanisms of candidate chemical medicines and traditional Chinese medicines for SARS-CoV-2 infection, Virus Res. 286 (2020) 198073. [CrossRef]
- I. Leneva, N. Kartashova, A. Poromov, A. Gracheva, E. Korchevaya, E. Glubokova, O. Borisova, A. Shtro, S. Loginova, V. Shchukina, R. Khamitov, E. Faizuloev, Antiviral activity of Umifenovir in vitro against a broad spectrum of coronaviruses, including the novel SARS-CoV-2 Virus, Viruses 13 (2021) 1665. [CrossRef]
- H. Tanaka, S. Miyagi, Y. Yoshida, J. S. Lamb, C. N. Chick, L. P. Luhata, M. Shibata, E. Tanaka, Y. Suzuki, T. Usuki, Synthesis and biological evaluation of Umifenovir analogues as anti-SARS-CoV-2 agents, ChemistrySelect 7 (2022) e202202097. [CrossRef]
- A. Shuster, D. Pechalrieu, C. B. Jackson, D. Abegg, H. Choe, A. Adibekian, Clinical antiviral drug Arbidol inhibits infection by SARS-CoV-2 and variants through direct binding to the spike protein, ACS Chem. Biol. 16 (2021) 2845–2851. [CrossRef]
- A. K. Yadav, S. Wen, X. Xu, L. Yu, Antiviral treatment in COVID-19: which is the most promising? - a narrative review, Ann. Palliat. Med. 10 (2021) 707‒720. [CrossRef]
- X. Pan, L. Dong, L. Yang, D. Chen, C. Peng, Potential drugs for the treatment of the novel coronavirus pneumonia (COVID-19) in China, Virus Res. 286 (2020) 198057. [CrossRef]
- D. Wang, Z. Li, Y. Liu, An overview of the safety, clinical application and antiviral research of the COVID-19 therapeutics, J. Infect. Public Health 13 (2020) 1405–1414. [CrossRef]
- A. K. Padhi, A. Seal, J. M. Khan, M. Ahamed, T. Tripathi, Unraveling the mechanism of arbidol binding and inhibition of SARS-CoV-2: Insights from atomistic simulations, Eur. J. Pharmacol. 894 (2021) 173836. [CrossRef]
- S. S. Borisevich, E. M. Khamitov, M. A. Gureev, O. I. Yarovaya, N. B. Rudometova, A. V. Zybkina, E. D. Mordvinova, D. N. Shcherbakov, R. A. Maksyutov, N. F. Salakhutdinov, Simulation of molecular dynamics of SARS-CoV-2 S-protein in the presence of multiple Arbidol molecules: Interactions and binding mode insights, Viruses 14 (2022) 119. [CrossRef]
- N. Vankadari, Arbidol: A potential antiviral drug for the treatment of SARS-CoV-2 by blocking trimerization of the spike glycoprotein, Int. J. Antimicrob. Agents 56 (2020) 105998. [CrossRef]
- Z. Zhu, Z. Lu, T. Xu, C. Chen, G. Yang, T. Zha, J. Lu, Y. Xue, Arbidol monotherapy is superior to lopinavir/ritonavir in treating COVID-19, J. Infection 81 (2020) e21–e23. [CrossRef]
- M. Nojomi, Z. Yassin, H. Keyvani, M. J. Makiani, M. Roham, A. Laali, N. Dehghan, M. Navaei, M. Ranjbar, Effect of Arbidol (Umifenovir) on COVID-19: a randomized controlled trial, BMC Infectious Diseases 20 (2020) 954. [CrossRef]
- Y. Li, Z. Xie, W. Lin, W. Cai, C. Wen, Y. Guan, X. Mo, J. Wang, Y. Wang, P. Peng, X. Chen, W. Hong, G. Xiao, J. Liu, L. Zhang, F. Hu, F. Li, F. Zhang, Efficacy and safety of Lopinavir/Ritonavir or Arbidol in adult patients with mild/moderate COVID-19: An exploratory randomized controlled trial, Med. 1 (2020) 105‒113. [CrossRef]
- Z. Wang, B, Yang, Q. Li, L. Wen, R. Zhang, Clinical features of 69 cases with coronavirus disease 2019 in Wuhan, China, Clin. Infect. Dis. 71 (2020) 769‒777. . [CrossRef]
- Z. Zhu, Z. Lu, T. Xu, C. Chen, G. Yang, T. Zha, J. Lu, Y. Xue, Arbidol monotherapy is superior to lopinavir/ritonavir in treating COVID-19, J. Infect. 81 (2020) e21‒23. [CrossRef]
- Z. Wang, X. Chen, Y. Lu, F. Chen, W. Zhang, Clinical characteristics and therapeutic procedure for four cases with 2019 novel coronavirus pneumonia receiving combined Chinese and Western medicine treatment, Biosci. Trends 14 (2020) 64‒68. [CrossRef]
- R. Ramachandran, V. Bhosale, H. Reddy, V. Atam, M. M. A. Faridi, J. Fatima, V. Shukla, Z. A. Khan, H. Khan, V. Singh, M. P. S. Negi, M. Srivastava, A. K. Srivastava, C. B. Tripathi, N. Ghosh, N. Majumdar, R. K. Tripathi, S. K. Rath, P. R. Mishra, S. Sharma, T. K. Kundu, Phase III, randomized, double-blind, Placebo controlled trial of efficacy, safety and tolerability of antiviral drug Umifenovir vs standard care of therapy in non-severe COVID-19 patients, Int. J. Infect. Dis. 115 (2022) 62–69. [CrossRef]
- M. Yu, D.-C. Wang, S. Li, Y.-H. Lei, J. Wei, L.-Y. Huang, Meta-analysis of arbidol versus lopinavir/ritonavir in the treatment of coronavirus disease 2019, J. Med. Virol. 94 (2022) 1513–1522. [CrossRef]
- C. Yang, C. Ke, D. Yue, W. Li, Z. Hu, W. Liu, S. Hu, S. Wang, J. Liu, Effectiveness of Arbidol for COVID-19 prevention in health professionals, Front. Public Health 8 (2020) 249. [CrossRef]
- M. Li, T. Yu, J. Zhu, Y. Wang, Y. Yang, K. Zhao, Y. Yi, J. He, C. Li, J. He, Comparison of the antiviral effect of Arbidol and Chloroquine in treating COVID-19, Ann. Palliat. Med. 10 (2021) 3307‒3312. [CrossRef]
- X.-L He, Y.-Y. Zhou, W. Fu, Y. Xue, M.-Y. Liang, B.-H. Yang, W.-I. Ma, Q. Zhou, L. Chen, J.-C. Zhang, X.-R. Wang, Prolonged SARS-CoV-2 viral shedding in patients with COVID-19 was associated with delayed initiation of Arbidol treatment and consulting doctor later: A retrospective cohort study, Curr. Med. Sci. 41 (2021) 1096‒1104. [CrossRef]
- N. V. Ul’yanovskii, D. S. Kosyakov, S. A. Sypalov, I. S. Varsegov, I. S. Shavrina, A. T. Lebedev, Antiviral drug Umifenovir (Arbidol) in municipal wastewater during the COVID-19 pandemic: Estimated levels and transformation, Sci. Total Environ. 805 (2022) 150380. [CrossRef]
- S. Choudhary, O. Silakari, Scaffold morphing of arbidol (umifenovir) in search of multi-targeting therapy halting the interaction of SARS-CoV-2 with ACE2 and other proteases involved in COVID-19, Virus Res. 289 (2020) 198146. [CrossRef]
- F. D. Hart, P. L. Boardman, Indomethacin: A new non-steroid anti-inflammatory agent, British Medical J. (1963) 965–970. /. [CrossRef]
- A. M. Ghanim, A. S. Girgis, B. M. Kariuki, N. Samir, M. F. Said, A. Abdelnaser, S. Nasr, M. S. Bekheit, M. F. Abdelhameed, A. J. Almalki, T. S. Ibrahim, S. S. Panda, Design and synthesis of ibuprofen-quinoline conjugates as potential anti-inflammatory and analgesic drug candidates, Bioorg. Chem. 119 (2022) 105557. [CrossRef]
- R. M. Bokhtia, S. S. Panda, A. S. Girgis, N. Samir, M. F. Said, A. Abdelnaser, S. Nasr, M. S. Bekheit, A. S. Dawood, H. Sharma, M. Wade, S. K. Sharma, A. M. Ghanim, New NSAID conjugates as potent and selective COX-2 inhibitors: Synthesis, molecular modeling and biological investigation, Molecules 28 (2023) 1945. [CrossRef]
- R. Ravichandran, S. K. Mohan, S. K. Sukumaran, D. Kamaraj, S. S. Daivasuga, S. O. A. S. Ravi, S. Vijayaraghavalu, R. K. Kumar, An open label randomized clinical trial of Indomethacin for mild and moderate hospitalized Covid-19 patients, Sci. Rep. 12 (2022) 6413. [CrossRef]
- J. Desantis, B. Mercorelli, M. Celegato, F. Croci, A. Bazzacco, M. Baroni, L. Siragusa, G. Cruciani, A. Loregian, L. Goracci, Indomethacin-based PROTACs as pan-coronavirus antiviral agents, Eur. J. Med. Chem. 226 (2021) 113814. [CrossRef]
- R. Gomeni, T. Xu, X. Gao, F. Bressolle-Gomeni, Model based approach for estimating the dosage regimen of indomethacin a potential antiviral treatment of patients infected with SARS CoV-2, J. Pharmacokinet. Pharmacodyn. 47 (2020) 189–198. [CrossRef]
- A. V. Krymchantowski, R. P. Silva-Néto, C. Jevoux, A. G. Krymchantowski, Indomethacin for refractory COVID or post-COVID headache: a retrospective study, Acta Neurol. Belg. 122 (2022) 465–469. [CrossRef]
- N. Shekhar, H. Kaur, P. Sarma , A. Prakash, B. Medhi, Indomethacin: an exploratory study of antiviral mechanism and host-pathogen interaction in COVID-19, Expert Rev. Anti-infect. Ther. 20 (2022) 383‒390. [CrossRef]
- J. Li, C. Lin, X. Zhou, F. Zhong, P. Zeng, P. J. McCormick, H. Jiang, J. Zhang, Structural basis of main proteases of coronavirus bound to drug candidate PF-07304814, J. Mol. Biol. 434 (2022) 167706. [CrossRef]
- B. Mao, V. T. K. Le-Trilling, K. Wang, D. Mennerich, J. Hu, Z. Zhao, J. Zheng, Y. Deng, B. Katschinski, S. Xu, G. Zhang, X. Cai, Y. Hu, J. Wang, M. Lu, A. Huang, N. Tang, M. Trilling, Y. Lin, Obatoclax inhibits SARS-CoV-2 entry by altered endosomal acidification and impaired cathepsin and furin activity in vitro, Emerg. Microbes Infect. 11 (2022) 483‒497. [CrossRef]
- R. Begum, A. N. M. Mamun-Or-Rashid, T. T. Lucy, K. Pramanik, B. K. Sil, N. Mukerjee, P. Tagde, M. Yagi, Y. Yonei, Potential therapeutic approach of melatonin against omicron and some other variants of SARS-CoV-2, Molecules 27 (2022) 6934. [CrossRef]
- M. Vlachou, A. Siamidi, A. Dedeloudi, S. K. Konstantinidou, I. P. Papanastasiou, Pineal hormone melatonin as an adjuvant treatment for COVID-19 (Review), Int. J. Mol. Med. 47 (2021) 47. /. [CrossRef]
- H. Parlakpinar, S. Polat, H. A. Acet, Pharmacological agents under investigation in the treatment of coronavirus disease 2019 and the importance of melatonin, Fundam. Clin. Pharmacol. 35 (2021) 62–75. [CrossRef]
- E. L. Feitosa, F. T. D. S. S. Júnior, J. A. D. Neto, L. F. L. Matos, M. H. D. Moura, T. O. Rosales, G. B. L. De Freitas, COVID-19: Rational discovery of the therapeutic potential of Melatonin as a SARS-CoV-2 main protease inhibitor, Int. J. Med. Sci. 17 (2020) 2133-2146. [CrossRef]
- R. Zhang, X. Wang, L. Ni, X. Di, B. Ma, S. Niu, C. Liu, R. J. Reiter, COVID-19: Melatonin as a potential adjuvant treatment, Life Sci. 250 (2020) 117583. [CrossRef]
- G. Öztűrk, K. G. Akbulut, Ş. Gűney, Melatonin, aging, and COVID-19: Could melatonin be beneficial for COVID-19 treatment in the elderly?, Turk. J. Med. Sci. 50 (2020) 1504‒1512. /: 50 (2020) 1504‒1512, https. [CrossRef]
- A. Wichniak, A. Kania, M. Siemiński, W. J. Cubała, Melatonin as a potential adjuvant treatment for COVID-19 beyond sleep disorders, Int. J. Mol. Sci. 22 (2021) 8623. [CrossRef]
- R. J. Reiter, R. Sharma, F. Simko, A. Dominguez-Rodriguez, J. Tesarik, R. L. Neel, A. T. Slominski, K. Kleszczynski, V. M. Martin-Gimenez, W. Manucha, D. P. Cardinali, Melatonin: highlighting its use as a potential treatment for SARS-CoV-2 infection, Cell. Mol. Life Sci. 79 (2022) 143. [CrossRef]
- I. G. García, M. Rodriguez-Rubio, A. R. Mariblanca, L. M. de Soto, L. D. García, J. M. Villatoro, J. Q. Parada, E. S. Meseguer, M. J. Rosales, J. González, J. R. Arribas, A. J. Carcas, P. de la Oliva, A. M. Borobia, A randomized multicenter clinical trial to evaluate the efficacy of melatonin in the prophylaxis of SARS-CoV-2 infection in high-risk contacts (MeCOVID Trial): A structured summary of a study protocol for a randomised controlled trial, Trials 21(2020) 466. [CrossRef]
- Z. T. Hasan, M. Q. Y. M. A. Al Atrakji, A. K. Mehuaiden, The effect of Melatonin on thrombosis, sepsis and mortality rate in COVID-19 patients, Int. J. Infect. Dis. 114 (2022) 79–84. [CrossRef]
- S.-H. Lan, H.-Z. Lee, C.-M. Chao, S.-P. Chang, L.-C. Lu, C.-C. Lai, Efficacy of melatonin in the treatment of patients with COVID-19: A systematic review and meta-analysis of randomized controlled trials, J. Med. Virol. 94 (2022) 2102–2107. [CrossRef]
- G. Farnoosh, M. Akbariqomi, T. Badri, M. Bagheri, M. Izadi, A. Saeedi-Boroujeni, E. Rezaie, H. E. G. Ghaleh, H. Aghamollaei, M. Fasihi-ramandi, K. Hassanpour, G. Alishiri, Efficacy of a low dose of melatonin as an adjunctive therapy in hospitalized patients with COVID-19: A randomized, double-blind clinical trial, Arch. Med. Res. 53 (2022) 79–85. [CrossRef]
- A. Ziaei, P. Davoodian, H. Dadvand, O. Safa, S. Hassanipour, M. Omidi, M. Masjedi, F. Mahmoudikia, B. Rafiee, M. Fathalipour, Evaluation of the efficacy and safety of Melatonin in moderately ill patients with COVID-19: A structured summary of a study protocol for a randomized controlled trial, Trials 21 (2020) 882. [CrossRef]
- H. A. Alhadrami, G. Burgio, B. Thissera, R. Orfali, S. E. Jiffri, M. Yaseen, A. M. Sayed, M. E. Rateb, Neoechinulin A as a promising SARS-CoV-2Mpro inhibitor: In vitro and in silico study showing the ability of simulations in discerning active from inactive enzyme inhibitors, Mar. Drugs 20 (2022) 163. [CrossRef]
- W. Vuong, M. B. Khan, C. Fischer, E. Arutyunova, T. Lamer, J. Shields, H. A. Saffran, R. T.McKay, M. J. van Belkum, M. A. Joyce, H. S. Young, D. L. Tyrrell, J. C. Vederas, M. J. Lemieux, Feline coronavirus drug inhibits the main protease of SARS-CoV-2 and blocks virus replication, Nat. Commun. 11 (2020) 4282. [CrossRef]
- K. Nishiuchi, H. Ohashi, K. Nishioka, M. Yamasaki, M. Furuta, T. Mashiko, S. Tomoshige, K. Ohgane, S. Kamisuki, K. Watashi, K. Kuramochi, Synthesis and antiviral activities of Neoechinulin B and its derivatives, J. Nat. Prod. 85 (2022) 284−291. [CrossRef]
- P. Liu, H. Liu, Q. Sun, H. Liang, C. Li, X. Deng, Y. Liu, L. Lai, Potent inhibitors of SARS-CoV-2 3C-like protease derived from N-substituted isatin compounds, Eur. J. Med. Chem. 206 (2020) 112702. [CrossRef]
- G.-N. Zhang, J. Zhao, Q. Li, M. Wang, M. Zhu, J. Wang, S. Cen, Y. Wang, Discovery and optimization of 2-((1H-indol-3-yl)thio)-N-benzyl-acetamides as novel SARS-CoV-2 RdRp inhibitors, Eur. J. Med. Chem. 223 (2021) 113622. [CrossRef]
- J. Zhao, G. Zhang, Y. Zhang, D. Yi, Q. Li, L. Ma, S. Guo, X. Li, F. Guo, R. Lin, G. Luu, Z. Liu, Y. Wang, S. Cen, 2-((1H-indol-3-yl)thio)-N-phenyl-acetamides: SARS-CoV-2 RNA-dependent RNA polymerase inhibitors, Antiviral Res. 196 (2021) 105209. [CrossRef]
- A. K. Ghosh , D. Shahabi, M. Yadav, S. Kovela, B. J. Anson, E. K. Lendy, C. Bonham, D. Sirohi, C. A. Brito-Sierra, S-i. Hattori, R. Kuhn, H. Mitsuya, A. D. Mesecar, Chloropyridinyl esters of nonsteroidal anti-inflammatory agents and related derivatives as potent SARS-CoV-2 3CL protease inhibitors, Molecules 26 (2021) 5782. [CrossRef]
- P. K. Mudi, A. K. Mahanty, M. Kotakonda, S. Prasad, S. Bhattacharyya, B. Biswas, A benzimidazole scaffold as a promising inhibitor against SARS-CoV-2, J. Biomol. Struct. Dyn. 41 (2023) 1798–1810. [CrossRef]
- A. S. Girgis, S. S. Panda, A. M. Srour, A. Abdelnaser, S. Nasr, Y. Moatasim, O. Kutkat, A. El Taweel, A. Kandeil, A. Mostafa, M. A. Ali, N. G. Fawzy, M. S. Bekheit, E. M. Shalaby, L. Gigli, W. Fayad, A. A. F. Soliman, 3-Alkenyl-2-oxindoles: Synthesis, antiproliferative and antiviral properties against SARS-CoV-2, Bioorg. Chem. 114 (2021) 105131. [CrossRef]
- N. G. Fawazy, S. S. Panda, A. Mostafa, B. M. Kariuki, M. S. Bekheit, Y. Moatasim, O. Kutkat, W. Fayad, M. A. El-Manawaty, A. A. F. Soliman, R. A. El-Shiekh, A. M. Srour, R. F. Barghash, A. S. Girgis, Development of spiro-3-indolin-2-one containing compounds of antiproliferative and ant-SARS-CoV-2 properties, Sci. Rep. 12 (2022) 13880. [CrossRef]
- M. S. Bekheit, S. S. Panda, B. M. Kariuki, S. H. Mahmoud, A. Mostafa, A. S. Girgis, Spiroindole-containing compounds bearing phosphonate group of potential Mpro-SARS-CoV-2 inhibitory properties, Eur. J. Med. Chem. 258 (2023) 115563. [CrossRef]
- V. Di Sarno, G. Lauro, S. Musella, T. Ciaglia, V. Vestuto, M. Sala, M. C. Scala, G. Smaldone, F. Di Matteo, S. Novi, M. F. Tecce, O. Moltedo, G. Bifulco, P. Campiglia, I. M. Gomez-Monterrey, R. Snoeck, G. Andrei, C. Ostacolo, A. Bertamino, Identification of a dual acting SARS-CoV-2 proteases inhibitor through in silico design and step-by-step biological characterization, Eur. J. Med. Chem. 226 (2021) 113863. [CrossRef]
- A. Serra, M. Fratello, A. Federico, R. Ojha, R. Provenzani, E. Tasnadi, L. Cattelani, G. del Giudice, P. A. S. Kinaret, L. A. Saarimäki, A. Pavel, S. Kuivanen, V. Cerullo, O. Vapalahti, P. Horvath, A. Di Lieto, J. Yli-Kauhaluoma, G. Balistreri, D. Greco, Computationally prioritized drugs inhibit SARS-CoV-2 infection and syncytia formation, Brief. Bioinfor. 23 (2022) 1–20. [CrossRef]
- S. S. Panda, A. S. Girgis, S. J. Thomas, J. E. Capito, R. F. George, A. Salman, M. A. El-Manawaty, A. Samir, Synthesis, pharmacological profile and 2D-QSAR studies of curcumin-amino acid conjugates as potential drug candidates, Eur. J. Med. Chem. 196 (2020) 112293. [CrossRef]
- M. Mohseni, H. Bahrami, B. Farajmand, F. S. Hosseini, M. Amanlou, H. Salehabadi, Indole alkaloids as potential candidates against COVID-19: an in silico study, J. Mol. Model. 28 (2022) 144. [CrossRef]
- V. Raj, J.-H. Lee, J.-J. Shim, J. Lee, Antiviral activities of 4H-chromen-4-one scaffold-containing flavonoids against SARS–CoV–2 using computational and in vitro approaches, J. Mol. Liq. 353 (2022) 118775. [CrossRef]
- https://www.drugs.com/history/paxlovid.html (accessed on , 2023). 6 July.
- https://go.drugbank.com/unearth/q?utf8=%E2%9C%93&searcher=drugs&query=Paxlovid (accessed on , 2023). 6 July.
- J. Reina, C. Iglesias, Nirmatrelvir más ritonavir (Paxlovid) una potente combinación inhibidora de la proteasa 3CLpro del SARS-CoV-2, Rev. Esp. Quimioter 35 (2022) 236‒240. [CrossRef]
- F. I. Khan, F. Hassan, D. Lai, In silico studies on psilocybin drug derivatives against SARS-CoV-2 and cytokine storm of human interleukin-6 receptor, Front. Immunol. 12 (2022) 794780. [CrossRef]
- B. G. Vijayakumar, D. Ramesh, A. Joji, J. J. prakasan, T. Kannan, In silico pharmacokinetic and molecular docking studies of natural flavonoids and synthetic indole chalcones against essential proteins of SARS-CoV-2, Eur. J. Pharm. 886 (2020) 173448. [CrossRef]
- S. Singhal, P. Khanna, L. Khanna, Synthesis, comparative in vitro antibacterial, antioxidant and UV fluorescence studies of bis indole Schiff bases and molecular docking with ct-DNA and SARS-CoV-2 Mpro, Luminescence 36 (2021) 1531–1543. [CrossRef]
- V. R. Shah, J. D. Bhaliya, G. M. Patel, In silico approach: docking study of oxindole derivatives against the main protease of COVID-19 and its comparison with existing therapeutic agents, J. Basic Clin. Physiol. Pharmacol. 32 (2021) 197–214. [CrossRef]
- S.-i. Hattori, N. Higashi-Kuwata, H. Hayashi, S. R. Allu, J. Raghavaiah, H. Bulut, D. Das, B. J. Anson, E. K. Lendy, Y. Takamatsu, N. Takamune, N. Kishimoto, K. Murayama, K. Hasegawa, M. Li, D. A. Davis, E. N. Kodama, R. Yarchoan, A. Wlodawer, S. Misumi, A. D. Mesecar, A. K. Ghosh, H. Mitsuya, A small molecule compound with an indole moiety inhibits the main protease of SARS-CoV-2 and blocks virus replication, Nat. Commun. 12 (2021) 668. [CrossRef]
- P. Gobinath, P. Packialakshmi, K. Vijayakumar, M. H. Abdellattif, M. Shahbaaz, A. Idhayadhulla, R. Surendrakumar, Synthesis and cytotoxic activity of novel indole derivatives and their in silico screening on spike glycoprotein of SARS-CoV-2, Front. Mol. Biosci. 8 (2021) 637989. [CrossRef]
- X. Xu, Y. Chen, X. Lu, W. Zhang, W. Fang, L. Yuan, X. Wang, An update on inhibitors targeting RNA-dependent RNA polymerase for COVID-19 treatment: promises and challenges, Biochem. Pharmacol. 205 (2022) 115279. [CrossRef]
- R. Kumar M., D. A. Gideon, R. Mariadasse, V. Nirusimhan, S. Rosita A., J. C. Edward, J. Jeyaraman, V. Dhayabaran, In silico evaluation of isatin-based derivatives with RNA-dependent RNA polymerase of the novel coronavirus SARS-CoV-2, J. Biomol. Struct. Dyn. 40 (2022) 6710–6724. 2022. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



