Submitted:
03 August 2023
Posted:
04 August 2023
You are already at the latest version
Abstract
Aortic valve stenosis and malignancy frequently coexist and share the same risk factors as atherosclerotic disease. Data reporting the prognosis of patients with severe aortic stenosis and cancer are limited. Tailoring the correct and most optimal care for cancer patients with severe aortic stenosis is complex. Cancer patients may be further disadvantaged by aortic stenosis if it interferes with their treatment by increasing the risk associated with oncologic surgery and compounding the risks associated with cardiotoxicity and heart failure (HF). Nowadays, several therapeutic options are available for aortic valve stenosis (surgical valve replacement , transcatheter valve implantation, balloon valvuloplasty, or medical therapy), but in presence of malignancy, the use of one of these versus the others should be decided on a case-by-case approach, depending on cancer stage and associated treatment, expected outcome, comorbidities and after an accurate physical examination and Doppler-echocardiography which are the key tools for diagnosing and evaluating aortic stenosis. The current review considers the available data on the association between aortic stenosis and cancer, and therapeutic options.
Keywords:
aortic stenosis
; cancer
; valve replacement
; cardio-oncology
; transcatheter valve implantation
; radiation therapy
1. Introduction
The coexistence of cancer and calcific aortic valve stenosis (AS) is a common medical scenario, especially in the elderly, due to sharing risk factors (i.e. hypertension, obesity, diabetes, smoking, dyslipidemia), the inflammatory state associated with malignancies, and/or cardiotoxic effects of cancer therapy [1]. As reported in studies listed in Table 1, the prevalence of cancer in patients with severe AS varies between 5.4 and 37.8% [2,3,4]. Data reporting the prognosis of patients with severe AS and cancer are limited. In a 10-year single-center retrospective study, cancer patients with severe AS (mean aortic valve area 1.0 ± 0.3 cm2) had a 5-year mortality of 48%; 59% deaths were due to cancer progression, 31% were due to heart failure (HF) and stroke[5]. Minamino-Muta et al. in a Japanese retrospective study of 3815 patients in a multicenter AS registry, found that outcomes are worse not only in patients with active cancer but also in those with a previous history of malignancy[6]. Mortality was mainly cancer-related, with comparable aortic valve–related deaths between cancer and no-cancer patients. Despite the increasing prevalence in AS and cancer, death rates have been steadily declining with the introduction of novel therapies[7], but at present optimal strategy for management of severe AS in patients with an active cancer is unclear. Cancer patients are routinely excluded from clinical trials because of poor long-term prognosis. Active malignancy often hinders the decision to proceed with invasive procedures such as cardiac surgery. Furthermore, cancer patients have additional risks and subsequent co-morbidities related to their cancer and therapy, such as prior exposure to potentially cardiotoxic chemotherapy, prior chest radiation, immunocompromised state, and increased risk of both bleeding and thromboembolic disease[8]. In patients with cancer, AS may interfere with optimal antineoplastic management (i.e., high-risk oncological surgery or potentially cardiotoxic chemotherapies). Symptomatic AS is occasionally diagnosed in cancer patients undergoing cardiovascular evaluation; likewise, cancer is often recognized during assessment preceding aortic valve interventions. In these complex cases, physicians face difficult treatment decision. Khrais et al found [9] that AS can be seen as a prognostic risk factor in patients with colorectal cancer for adverse outcomes due to higher rates of lower gastrointestinal bleeding and resulting iron-deficiency anemia.
Severe symptomatic AS in patients with cancer requires a careful assessment in order to select the appropriate therapeutic choices and their timing (i.e. valve-treatment first versus cancer-treatment first). Echocardiography is key to confirming the diagnosis and severity of AS, assessing valve abnormalities, left ventricular (LV) hypertrophy and function, detecting other valve disease or aortic pathology, and providing prognostic information. These echocardiographic findings must be considered together with coronary/vascular diseases and cardiovascular medications. LV systolic dysfunction represents an important prognostic factor and is included in the current operative risk scores[10]. It can be due to long-standing pressure-overload, to associated aortic regurgitation or mitral valve disease, coronary artery disease, but also to cardiotoxicity induced by cancer treatment (especially anthracyclines and targeted therapies such as tyrosine kinase inhibitor, antihuman epidermal growth factor receptor 2, anti-vascular endothelial growth factor, proteasome inhibitors) [11]. Ezaz and colleagues[12] developed a risk factor–scoring tool for patients on trastuzumab to help identify those at highest risk of developing HF or cardiomyopathy. A 7-factor risk (age, adjuvant chemotherapy, coronary artery disease-CAD, atrial fibrillation or flutter, diabetes mellitus, hypertension, and renal failure) score was derived and validated. Low (0–3points), medium (4–5 points), and high (= 6 points) risk strata had 3-year rates of HF or LV dysfunction of 16.2%,26%, and 39.5%, respectively. LV dysfunction can remain asymptomatic for a long time[13], but once symptomatic, the prognosis is among the worst in the HF population[14]. Moreover, chest radiation and cardiotoxic drugs (i.e. anthracyclines) have been noted to produce de-novo AS via valve leaflet thickening, fibrosis, retraction and calcification [15], but at the present the impact that they may have on AS progression has not been studied. Bravo-Jaimes at al have found that patients with mild or moderate AS and cancer are more likely to die before having AS progression, which is in turn associated with CAD and prevalent cyclophosphamide use[16].
Several therapeutic options are currently available for aortic valve stenosis, such surgical valve replacement (SAVR), transcatheter valve replacement (TAVR), balloon valvuloplasty, or medical therapy. Use of one of these versus the others should be decided on a case-by-case approach, depending on cancer stage and associated treatment, expected outcome, comorbidities[17]. However, cancer survivors patients with a confirmed remitted malignancy and evidence of severe AS, after an accurate multidisciplinary team evaluation with oncologists, interventional cardiologist, heart surgeon, can be considered similar candidates to patients with non-previous cancer history in terms of eligibility for aortic valve replacement .
2. Pathophysiology
Clinical risk factors associated with AS development and progression mirror those associated with atherosclerosis, and because many are shared by cancer (advanced age, smoking, hypertension, hypercholesterolemia, obesity, metabolic syndrome, diabetes, and elevated lipoprotein (a) levels) prevalence and incidence rates of both disorders are rising simultaneously [18,19]. These common conditions together with microbial and viral infections, allergen exposure, radiation, toxic chemicals, alcohol consumption, tobacco use, and other chronic and autoimmune diseases induce inflammation[20]. It is now known that inflammation mediates all atherosclerosis stages, from initiation to progression and, ultimately, plaque unstabilization and thrombosis. Conditions such as hypertension, smoking, dyslipidemia, and insulin resistance all appear to trigger atherosclerosis, in promoting the expression of adhesion molecules by endothelial cells, allowing leukocyte attachment to blood vessel walls that normally resist their attachment. In recent decades, extensive factual and circumstantial evidence has shown several cancer types to be induced by infection or chronic inflammatory disease (eg, human papillomavirus and cervical cancer, Helicobacter pylori and stomach cancer, Epstein-Barr virus and lymphoma)[21]. As stated by Koene et al. [20] , controlling cardiovascular disease risk factors can help reduce the risk of cancer. There is an urgent need to improve the health status of the population to reduce the prevalence of both diseases.
Although chronic inflammation is an indispensable feature of the pathogenesis and progression of both cardiovascular disease and cancer, additional mechanisms can be found at their intersection such as non-modifiable risk factors, including age, sex, and race/ethnicity, which are uncontrollable. There are obvious differences between male and female organs and hormonal fluctuations that influence both cardiovascular disease and cancer progression. Of all non-modifiable risk factors, age is a steady independent variable with regard to cardiovascular disease and cancer, yet the associations between age and disease onset can be highly influenced by lifestyle parameters, such as diet, physical activity, body mass index and smoking.
3. Treatment
Currently, optimal strategy for management of severe AS in patients with an active cancer is still unclear. Tailoring the correct and most optimal care for cancer patients with severe AS is complex. Asymptomatic patients with severe AS, in absence of adverse prognostic features such as reduced LV ejection fraction, or symptoms appearance during exercise stress test, are recommended for a watchful waiting approach, with regular and frequent follow-up and prompt intervention in case of clinical progression (i.e. symptoms ). In this way, asymptomatic patients can proceed with their antineoplastic therapy without interruptions or delays. Medical treatment of hypertension and hyperlipidemia, according to current international guidelines, is recommended for patients with severe AS. According to the 2020 American College of Cardiology Foundation / American Heart Association guidelines, adult patients with symptomatic severe AS (stage D), or with asymptomatic severe AS with LVEF <50% or need of other cardiac surgery have an indication for aortic valve replacement (AVR). If the risk for a SAVR is high or prohibitive, decision-making focuses on TAVR or palliative care, depending on the life expectancy[22]. In the 2021 European Society of Cardiology Guidelines for The Management of Valvular Heart Disease, AVR is indicated in patients with symptomatic severe AS, except for those in whom intervention is unlikely to improve quality of life or survival (due to severe comorbidities) or for those with concomitant conditions associated with survival <1 year [23]. In the past years, in patients with severe AS, priority was given to the treatment of the neoplastic disease rather than the treatment of the severe valvular disease. However, patients undergoing SAVR have shown markedly better survival, due to better resilience to anemia, infection/sepsis, and rapid volume changes from chemotherapy regimens or hypotension/volume loss during surgical procedures, not uncommon during cancer treatment. It must be said, anyway, that patients with severe AS are not excellent candidates for surgery mainly due to comorbidities that increase the estimated periprocedural morbidity and mortality[2]. Conflicting results come from reports where SAVR is performed before cancer surgery[24]. A fundamental problem of SAVR in cancer patients, is that open surgery requires extracorporeal circulation. Among various other systemic effects, cardiopulmonary bypass can cause immunosuppression, increase inflammation (as demonstrated by a significant increase in TNF-alpha, Il-10, Il-6, Il-1 and TGF-beta) and worsen cancer outcomes. So precisely because of the immunosuppressive effects, patients with hematologic cancers are at risk of having worse outcomes than those with solid tumors and better immune system. However, the relationship between the use of extracorporeal circulation and cancer progression has not yet been clearly demonstrated. Among the comorbidities, we should also consider the vascular fragility that patients with active cancer can develop, and which can sometimes be caused by anticancer drugs or radiotherapy. In addition, cardiac surgery recovery times are longer, and this could lead to a delay and lengthening of the antineoplastic therapy times.
Even if is mandatory to consider each case individually (SAVR vs TAVR), it is reasonable to conclude that TAVR, for cancer patients with severe AS, can more frequently be the best clinical choice by avoiding cardiopulmonary bypass and all its consequences. One of the biggest advantages of TAVR is its minimal invasiveness and so, shorter recovery time. Moreover, thanks to the increasing access of cancer patients to TAVR, delays in cancer treatment have been significantly reduced from about 2 months after cardiac surgery to 2 weeks[25]. TAVR does not require a median sternotomy or cardiopulmonary bypass and can be performed under local anesthesia, which reduces the overall time required to complete the procedure, which benefits patients with malignancies. Manger et al. and Landes et al. reported that TAVR periprocedural mortality and major complication rates were equivalent in patients with and without active cancer[3]. Kojima et al. reported no difference in terms of complications between patients undergoing TAVR with and without active cancer[26]. However, despite technical difficulties for open surgery may be overcome by TAVR, major comorbidities may influence post-TAVR prognosis just as with SAVR[27]. To be eligible for TAVR, as mentioned before, cancer patients should have a prognosis of 1 year or greater. However, precise estimation of prognosis has always been very difficult in these patients, and even more so lately, thanks to the rapid expansion of new and innovative cancer therapies. A fundamental element to consider in choosing the most suitable type of intervention for the patient, in addition to the prognosis, is the stage of the neoplastic pathology . Patients with history of cancer, who are judged in remission by the oncology team, are usually eligible for TAVR. Patients with early cancer stages, who can safely receive oncologic treatment could be easily considered for TAVR as soon as remission is confirmed. In other cases, performing TAVR before cancer treatment, allows for radical oncologic treatment shortly after valve intervention [28]. Patients with AS and a localized cancer can be stabilized and TAVR can be considered after exclusion of metastatic disease. Patients with advanced disease stage, metastases, multiple comorbidities, and very short estimated survival may be candidates for balloon valvuloplasty as a "bridge to destination" surgery[29].
In the final stages of the neoplastic disease, a more conservative approach aimed at improving the quality of life during palliative treatment is preferred. A recent expert consensus issued by the Society for Cardiovascular Angiography and Interventions, recommends aortic balloon valvuloplasty or TAVR for cancer patients with AS as either a palliative or cure for valvular disease, to improve quality of life or to facilitate appropriate treatment of cancer therapy. Unfortunately, due to the characteristics of advanced stage cancer patients, it is difficult to conduct large studies, limiting the quality of data to support this approach [29]. A small study from Schechter et al of 65 cancer patients with severe AS found that valve replacement improves survival, regardless of the type of cancer or anti-cancer therapy, with TAVR being the most effective [25]. Nowadays the majority of cancer patients diagnosed with severe AS undergo valve replacement before cancer treatment, with the large majority receiving TAVR more than SAVR. Despite the lower risk of TAVR complications, the literature is not univocal about what are the peri-procedural complications of TAVR that could cause a delay in cancer treatment and modified overall survival. A meta-analysis of Marmagkiolis et al. demonstrates a favorable post-TAVR short-term mortality and remarkable safety, with improved stroke and acute kidney injury (AKI) rates without increased bleeding and need for new pacemaker implantation in cancer patients compared to controls[7]. Conversely, a meta-analysis from Bendary et al., reported higher rates of postprocedural pacemaker, without no difference in short-term mortality[30]. In a systematic review of Arocutipa et al., AKI occurred more frequently in patients with active cancer[31]. AKI is a very common complication of TAVR and can rates up to 50% of procedures. Its origin is multifactorial: in addition to the iodinated contrast, bleeding and anemia, volume depletion, micro embolisms, hypotension, or nephrotoxic drugs also contribute. Importantly, tumor type also plays a role in the risk of post-TAVR AKI. Thus, the decision to ultimately pursue TAVR is not an easy choice and involves a multidisciplinary and holistic approach in assessing the appropriateness of intervention.Recently, also in light of the study of Ullah et al [32],which highlighted different outcomes between SAVR and TAVR based on the tumor location, our group proposed a detailed specific decision-making algorithm for the management of symptomatic severe AS in cancer patients, both active and in remission[33] .Specifically, in the case of active cancer, once it is ascertained that cancer related life expectancy is >1 year, that cancer treatment is not feasible before AS treatment, and that cancer treatment can be delayed for at least 2 months, the decision-making process is comparable to cancer in remission. In this case, evaluation for the presence of high-risk features for SAVR and/or clinical conditions favoring TAVI is suggested. Where such conditions are not present, the choice between TAVR and SAVR rests in the judgment of the heart team, including consideration that tumor site can influence management strategy and of personal patient choice (Figure 1).
3.1. Radiation therapy and Aortic stenosis treatment
An issue that should not be forgotten in the field of AS and cancer disease, is the impact of radiotherapy on these patients. Chest radiation (C-XRT) is part of standard treatment protocols in various malignancies including lymphoma and breast, lung, and esophagus cancer. Fibrosis and calcification of the mitral and aortic valves, especially at the leaflet base and the aorto-mitral curtain” [34], have been noted in patients who underwent C-XRT. A dose dependent toxic effect on the heart has been previously demonstrated, and immunobiological studies have shown specifically a dose-dependent effect of aortic valve fibrosis. It has been suggested that> 30 Gy is considered a high dose of mediastinal radiation[35]. In terms of screening, the International Cardio-Oncology Society recommends obtaining routine transthoracic echocardiogram in all patients who are planned to undergo thoracic radiation and every 5 years thereafter to screen for radiation-induced valvulopathy[36]. However, this recommendation has yet to be integrated into routine clinical practice. In a retrospective study of Hodgkin disease survivors with and without prior chest radiation, 6 of 49 (12%) patients who underwent C-XRT developed moderate or severe aortic regurgitation, mitral regurgitation, or AS, whereas only 1 of 29 patients without prior chest radiation developed more than mild AS, and 1 more than mild aortic regurgitation [37]. This patient group is plagued by a high mortality and presents unique challenges in surveillance and in balancing risks and benefit of treatment[38]. Donnellan et al.[39] compared AS patients with prior exposure to C-XRT to a group with similar AS at baseline but no history of irradiation. Although progression of AS was similar in both groups, significantly more patients in the C-XRT group underwent AVR for development of symptoms (80% vs 50%, p < 0.001) during a mean follow-up of 3.6 ± 2 years. Despite that, the C-XRT group had significantly higher long-term mortality than the comparison group. The decision-making of treatment modality for radiation-induced AS should be a multidisciplinary decision that is targeted for the patient’s specific characteristics and needs taking in account the complexity of anatomy and disease history. Patients with a prior history of radiation to the chest are considered to be at high risk for surgery for numerous reasons: the ascending aorta can be markedly calcified (‘porcelain aorta’) making cross-clamping difficult, the frequent need for associated mitral and coronary surgery, presence of pulmonary fibrosis which correlate directly with mortality postoperatively[35]. Therefore, history of prior chest radiation is now included in the STS risk score before a cardiac surgery given its significant effect on surgical mortality[40]. A recent matched cohort study found that radiation was associated with a statistically significant increase in in-hospital mortality and 6-year mortality after SAVR compared with patients without a radiation history[41]. However, 61% of patients were undergoing SAVR with another concomitant procedure. Isolated SAVR has been shown to have better 5-year survival than combined procedures in patients with radiation-induced AS[42]. TAVR is an increasingly performed procedure and may be an important treatment avenue for patients with radiation-induced AS taking in account potential complications, such as fistulization and tissue rupture.
An accurate analysis with computed tomography angiography (CTA) evaluating aortic valve characteristics and size, access route and degree of aortic calcifications for optimal TAVR planning is always mandatory, especially in this very high risk setting[43]. Zafar et al[44] showed in a 2020 systematic review and meta-analysis that TAVR was a safe option for patients with radiation-induced AS. Although current guidelines do not recommend TAVR in patients with a life expectancy of less than 1 year, many cancer survivors do not meet this timeline, and even those on active therapy, are experiencing continued improvement in survival. There will therefore be a growing need to revisit the option and benefit of TAVR in cancer patients[7].
3.2. Aortic stenosis, coronary artery disease (CAD) and mitral regurgitation
Concomitant cardiovascular problems, such as CAD or mitral regurgitation (MR) should be promptly assessed before the treatment of AS. Surgical approach with combined valvular intervention and coronary revascularization may represent an extreme high risk setting in fragile patients such as cancer ones. Therefore, a percutaneous approach is reasonably the best option to adopt. As reported above, CTA of the aorta and the iliofemoral arteries is crucial for pre-procedural planning and the combination of coronary computed tomography angiography (CCTA) may be useful for the exclusion of concomitant CAD in order to minimize invasive procedures in this high risk patients[45]. In case of concomitant significant CAD, American guidelines[22] recommend percutaneous coronary interventions (PCI) before TAVR in the case of left main disease and significant proximal CAD. Instead, European guidelines[46] do not recommend specific timing for coronary revascularization but suggest to base a decision according to the clinical presentation, coronary anatomy, and extent of myocardial at risk. PCI in concomitant with TAVR is recommended in patients at high risk of coronary obstruction by the prosthetic aortic valve (e.g. ostial lesion, low left main height, or a valve-in-valve implantation) or in patients in whom it is desirable to minimize dual antiplatelet therapy (DAPT) due to bleeding risk[47]. Regarding antithrombotic therapy, the standard treatment after TAVR is aspirin while patients with an indication for oral anticoagulation therapy or DAPT should receive the specific treatment according to the pre-existent clinical indication without any concern to the valve procedure. This represents a concrete advantage especially in patients with higher bleeding risk such as cancer patients[48]. Furthermore, the progressive younger age of patient candidates for TAVR makes the possibility of re-accessing the coronary arteries increasingly important. Thus, further studies on increasing coronary re-access after TAVR and best timing of percutaneous coronary interventions in relation to TAVR are necessary.
The reported prevalence of moderate or severe mitral regurgitation (MR) in AS patients eventually undergoing SAVR or TAVR ranged between 19% and 33%[47,49]. Ruel et al. have found that AS patients with function MR ≥2+ and a left atrial diameter >5 cm, preoperative peak aortic valve gradient <60 mm Hg, or atrial fibrillation have a significantly higher risk of cardiac HF and persistent mitral regurgitation after AVR than other AS patients. Waisbren et al.[50] in their work support a conservative, tailored approach to concomitant mitral surgery in patients presenting for correction of AS who demonstrate functional regurgitation. Finally, in patients with severe MR, there is not enough experience to make recommendations about surgery versus combined or sequential TAVR and percutaneous mitral edge-to-edge repair. Currently no consistent data is available about the coexistence of AS and MR and the related treatment in the subgroup of cancer patients.
3.3. Aortic stenosis and cardiac Amyloidosis
The prevalence of calcific AS and cardiac amyloidosis (CA) increases with age, and their association is, as expected, not uncommon in the elderly. Deposition of amyloid substance, especially transthyretin, can involve any cardiovascular structure, including aortic valve, myocardial walls and it may contribute to the initiation and progression of AS, as well as progressive myocardial dysfunction. Until now, there is no recommendation or consensus on whether patients with AS should be systematically screened for CA[51]. In patients with coexisting CA, AS severity should be assessed according to current guidelines[52]. Approximately 50% of patients with confirmed CA have a severe low-flow low-gradient AS with preserved LV ejection fraction, ( the so called “ paradoxical low-flow, low-gradient pattern”)[53], characterized by severe LV concentric remodeling, impairment of diastolic filling, left atrial remodeling and dysfunction, markedly reduced LV global longitudinal strain function and right ventricular remodeling and dysfunction [4,24]. The assessment of AS severity is more challenging in patients with low-flow, low gradient AS, and additional imaging tests are required to differentiate a true-severe versus a pseudo-severe AS. Dobutamine stress echocardiography may be used to confirm AS severity. The quantitation of aortic valve calcium burden using non-contrast computed tomography appears to be the most appropriate imaging modality to confirm AS severity in patients with CA. Until now, there is no randomized trial and no expert consensus that determines the best management of CA in patients with AS. There are very few data on the outcome and therapeutic management of patients with AS and concomitant CA. Most studies reported a high risk of mortality and non-improvement in functional status following AVR in patients with severe AS and CA [53,54,55]. One study in a small number of patients (n<30) suggest that outcome of patients with AS and CA may be better with TAVR versus SAVR(53).
4. Conclusions
The cardio-oncology patient population has been increasing in recent years, requiring appropriate management strategies to improve quality of life and survival rate. The coexistence of significant aortic valve stenosis and cancer is relatively common and poses diagnostic and therapeutic dilemmas . Collaboration between cardiologists and oncologists is of primary importance to select the best treatment approach and optimize the timing of intervention. Further clinical trial and registry studies are needed to better appreciate outcomes in this complex setting.
Author Contributions
Conceptualization, P.F.; writing—original draft preparation, G.S., S.M.,L.B.,A.F., review and editing P.F; visualization, P.F., S.C..; supervision, P.F., S.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Acknowledgments
None.
Disclosure of Conflict of Interests
The authors state that they have no conflict of interest.
Abbreviations:
| AKI: | acute kidney injury |
| AS: | aortic stenosis |
| CA: | cardiac amyloidosis |
| CAD: | coronary artery disease |
| CCTA: | coronary computed tomography angiography |
| CTA: | computed tomography angiography |
| C-XRT: | chest radiation therapy |
| DAPT: | dual antiplatelet therapy |
| HF: | heart failure |
| LV: | left ventricular |
| MR: | mitral regurgitation |
| PCI: | percutaneous coronary interventions |
| SAVR: | surgical valve replacement |
| TAVR: | transcatheter valve replacement |
References
- Giza, D.E.; Iliescu, G.; Hassan, S.; Marmagkiolis, K.; Iliescu, C. Cancer as a Risk Factor for Cardiovascular Disease. Curr. Oncol. Rep. 2017, 19, 39. [Google Scholar] [CrossRef]
- Faggiano, P.; Frattini, S.; Zilioli, V.; Rossi, A.; Nistri, S.; Dini, F.L.; Lorusso, R.; Tomasi, C.; Cas, L.D. Prevalence of comorbidities and associated cardiac diseases in patients with valve aortic stenosis. Potential implications for the decision-making process. Int. J. Cardiol. 2012, 159, 94–99. [Google Scholar] [CrossRef]
- Mangner, N.; Woitek, F.J.; Haussig, S.; Holzhey, D.; Stachel, G.; Schlotter, F.; Höllriegel, R.; Mohr, F.W.; Schuler, G.; Linke, A. Impact of active cancer disease on the outcome of patients undergoing transcatheter aortic valve replacement. J. Interv. Cardiol. 2018, 31, 188–196. [Google Scholar] [CrossRef]
- Guha, A.; Dey, A.K.; Arora, S.; Cavender, M.A.; Vavalle, J.P.; Sabik, J.F., III; Jimenez, E.; Jneid, H.; Addison, D. Contemporary Trends and Outcomes of Percutaneous and Surgical Aortic Valve Replacement in Patients With Cancer. J. Am. Hear. Assoc. 2020, 9, e014248. [Google Scholar] [CrossRef]
- Okura, Y.; Ishigaki, S.; Sakakibara, S.; Yumoto, C.; Hashitate, M.; Sekine, C.; Fujita, T.; Takayama, T.; Ozaki, K.; Sato, N.; et al. Prognosis of Cancer Patients with Aortic Stenosis Under Optimal Cancer Therapies and Conservative Cardiac Treatments. Int. Hear. J. 2018, 59, 750–758. [Google Scholar] [CrossRef] [PubMed]
- Minamino-Muta, E.; Kato, T.; Morimoto, T.; Taniguchi, T.; Nakatsuma, K.; Kimura, Y.; Inoko, M.; Shirai, S.; Kanamori, N.; Murata, K.; et al. Malignant disease as a comorbidity in patients with severe aortic stenosis: clinical presentation, outcomes, and management. Eur. Hear. J. - Qual. Care Clin. Outcomes 2018, 4, 180–188. [Google Scholar] [CrossRef] [PubMed]
- Marmagkiolis, K.; Monlezun, D.J.; Cilingiroglu, M.; Grines, C.; Herrmann, J.; Toutouzas, K.P.; Ates, I.; Iliescu, C. TAVR in Cancer Patients: Comprehensive Review, Meta-Analysis, and Meta-Regression. Front. Cardiovasc. Med. 2021, 8. [Google Scholar] [CrossRef]
- Yusuf, S.W.; Sarfaraz, A.; Durand, J.-B.; Swafford, J.; Daher, I.N. Management and outcomes of severe aortic stenosis in cancer patients. Am. Hear. J. 2011, 161, 1125–1132. [Google Scholar] [CrossRef] [PubMed]
- Khrais, A.; Gilani, N.; Sapin, J.; Abboud, Y.; Kahlam, A.; Le, A.; Shah, M.; Palani, A.; Javed, J. Differential Rates of Lower Gastrointestinal Bleeding and Other Outcomes in Colorectal Cancer Patients With Aortic Stenosis. Cureus 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Nashef, S.A.; Roques, F.; Sharples, L.D.; Nilsson, J.; Smith, C.; Goldstone, A.R.; Lockowandt, U. EuroSCORE II. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2012, 41, 734–745. [Google Scholar] [CrossRef]
- Zamorano JL, Lancellotti P, Rodriguez Munoz D, Aboyans V, Asteggiano R, Galderisi M, et al. 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: The Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur J Heart Fail 2017, 19, 9–42.
- Ezaz G, Long JB, Gross CP, Chen J. Risk Prediction Model for Heart Failure and Cardiomyopathy After Adjuvant Trastuzumab Therapy for Breast Cancer. J. Am. Hear. Assoc. 2014, 3, e000472. [CrossRef] [PubMed]
- Lenihan, D.J.; Oliva, S.; Chow, E.J.; Cardinale, D. Cardiac toxicity in cancer survivors. Cancer 2013, 119 (Suppl. 11), 2131–2142. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, D.; Colombo, A.; Lamantia, G.; Colombo, N.; Civelli, M.; De Giacomi, G.; Rubino, M.; Veglia, F.; Fiorentini, C.; Cipolla, C.M. Anthracycline-Induced Cardiomyopathy: Clinical Relevance and Response to Pharmacologic Therapy. J. Am. Coll. Cardiol. 2010, 55, 213–220. [Google Scholar] [CrossRef]
- Murbraech K, Wethal T, Smeland KB, Holte H, Loge JH, Holte E, et al. Valvular Dysfunction in Lymphoma Survivors Treated With Autologous Stem Cell Transplantation: A National Cross-Sectional Study. JACC Cardiovasc Imaging 2016, 9, 230–239. [Google Scholar] [CrossRef]
- Bravo-Jaimes, K.; Palaskas, N.L.; Banchs, J.; Abelhad, N.I.; Altaf, A.; Gouni, S.; Song, J.; Hassan, S.A.; Iliescu, C.; Deswal, A.; et al. Rate of Progression of Aortic Stenosis in Patients With Cancer. Front. Cardiovasc. Med. 2021, 8. [Google Scholar] [CrossRef]
- Balanescu SM, Balanescu DV, Donisan T, Yang EH, Palaskas N, Lopez-Mattei J, et al. The Onco-cardiologist Dilemma: to Implant, to Defer, or to Avoid Transcatheter Aortic Valve Replacement in Cancer Patients with Aortic Stenosis? Curr Cardiol Rep. 2019, 21, 83. [Google Scholar] [CrossRef]
- Masoudkabir, F.; Sarrafzadegan, N.; Gotay, C.; Ignaszewski, A.; Krahn, A.D.; Davis, M.K.; Franco, C.; Mani, A. Cardiovascular disease and cancer: Evidence for shared disease pathways and pharmacologic prevention. Atherosclerosis 2017, 263, 343–351. [Google Scholar] [CrossRef]
- Paris, S.; Tarantini, L.; Navazio, A.; Faggiano, P. Cardio-oncology: the new frontier of clinical and preventive cardiology. Monaldi Arch. Chest Dis. 2020, 90. [Google Scholar] [CrossRef]
- Koene RJ, Prizment AE, Blaes A, Konety SH. Shared Risk Factors in Cardiovascular Disease and Cancer. Circulation 2016, 133, 1104–1114. [CrossRef]
- Kamp, D.W.; Shacter, E.; A Weitzman, S. Chronic inflammation and cancer: the role of the mitochondria. Oncology 2011, 25, 400–410. [Google Scholar] [PubMed]
- Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, 3rd, Gentile F, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 143, e72–e227. [Google Scholar]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease: Developed by the Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Revista espanola de cardiologia 2022, 75, 524. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.Y.; Kim, S.M.; Lee, K.S.; Park, S.W.; Chung, M.J.; Cho, H.; Jung, J.I.; Jang, H.W.; Jung, S.-H.; Goo, J. Quantification of Aortic Valve Calcifications Detected During Lung Cancer-Screening CT Helps Stratify Subjects Necessitating Echocardiography for Aortic Stenosis Diagnosis. Medicine 2016, 95, e3710–e3710. [Google Scholar] [CrossRef] [PubMed]
- Schechter, M.; Balanescu, D.V.; Donisan, T.; Dayah, T.J.; Kar, B.; Gregoric, I.; Giza, D.E.; Song, J.; Lopez-Mattei, J.; Kim, P.; et al. An update on the management and outcomes of cancer patients with severe aortic stenosis. Catheter. Cardiovasc. Interv. 2019, 94, 438–445. [Google Scholar] [CrossRef]
- Kojima, Y.; Higuchi, R.; Hagiya, K.; Saji, M.; Takamisawa, I.; Iguchi, N.; Takanashi, S.; Doi, S.; Okazaki, S.; Sato, K.; et al. Prognosis of patients with active cancer undergoing transcatheter aortic valve implantation: An insight from Japanese multicenter registry. IJC Hear. Vasc. 2022, 40, 101045. [Google Scholar] [CrossRef]
- Mack MJ, Leon MB, Thourani VH, Makkar R, Kodali SK, Russo M, et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N Engl J Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef]
- Sakai, T.; Yahagi, K.; Miura, S.; Hoshino, T.; Yokota, T.; Tanabe, K.; Ikeda, S. Transcatheter aortic valve implantation for patients with lung cancer and aortic valve stenosis. J. Thorac. Dis. 2018, 10, E387–E390. [Google Scholar] [CrossRef]
- Iliescu, C.A.; Grines, C.L.; Herrmann, J.; Yang, E.H.; Cilingiroglu, M.; Charitakis, K.; Hakeem, A.; Toutouzas, K.P.; Leesar, M.A.; Marmagkiolis, K. SCAI Expert consensus statement: Evaluation, management, and special considerations of cardio-oncology patients in the cardiac catheterization laboratory (endorsed by the cardiological society of india, and sociedad Latino Americana de Cardiologıa intervencionista). Catheter. Cardiovasc. Interv. Off. J. Soc. Card. Angiogr. Interv. 2016, 87, E202–E223. [Google Scholar]
- Bendary, A.; Ramzy, A.; Bendary, M.; Salem, M. Transcatheter aortic valve replacement in patients with severe aortic stenosis and active cancer: a systematic review and meta-analysis. Open Heart 2020, 7, e001131. [Google Scholar] [CrossRef]
- Diaz-Arocutipa, C.; Torres-Valencia, J.; Zavaleta-Camacho, G.; Vicent, L. Association Between Previous or Active Cancer and Clinical Outcomes in TAVR Patients: A Systematic Review and Meta-Analysis of 255,840 Patients. Front. Cardiovasc. Med. 2021, 8, 763557. [Google Scholar] [CrossRef] [PubMed]
- Ullah, W.; Thalambedu, N.; Zahid, S.; Muhammadzai, H.Z.U.; Sandhyavenu, H.; Kumar, A.; Alraies, M.C.; Vishnevsky, A.; Ruggiero, N.J.; Mamas, M.A.; et al. Trends and Outcomes of TAVI and SAVR in Cancer and Noncancer Patients. JACC Adv. 2023, 2, 100167. [Google Scholar] [CrossRef]
- Faggiano, P.; Lorusso, R.; Carugo, S.; Faggiano, A. Heart Valve Team Conundrum. JACC: Adv. 2023, 2. [Google Scholar] [CrossRef]
- Desai, M.Y.; Wu, W.; Masri, A.; Popovic, Z.B.; Agarwal, S.; Smedira, N.G.; Lytle, B.W.; Griffin, B.P. Increased Aorto-Mitral Curtain Thickness Independently Predicts Mortality in Patients With Radiation-Associated Cardiac Disease Undergoing Cardiac Surgery. Ann. Thorac. Surg. 2014, 97, 1348–1355. [Google Scholar] [CrossRef] [PubMed]
- Belzile-Dugas, E.; Michel, C.; Morin, J.-F.; Eisenberg, M.J. The Heart-Team Approach for the Treatment of Radiation-Induced Aortic Stenosis and Coronary Artery Disease: A Case Report. CJC Open 2021, 3, 1388–1391. [Google Scholar] [CrossRef] [PubMed]
- Mitchell JD, Cehic DA, Morgia M, Bergom C, Toohey J, Guerrero PA, et al. Cardiovascular Manifestations From Therapeutic Radiation: A Multidisciplinary Expert Consensus Statement From the International Cardio-Oncology Society. JACC CardioOncol. 2021, 3, 360–380. [Google Scholar] [CrossRef] [PubMed]
- Bijl JM, Roos MM, van Leeuwen-Segarceanu EM, Vos JM, Bos WW, Biesma DH, et al. Assessment of Valvular Disorders in Survivors of Hodgkin's Lymphoma Treated by Mediastinal Radiotherapy +/- Chemotherapy. Am J Cardiol. 2016, 117, 691–696. [Google Scholar] [CrossRef]
- Wu W, Masri A, Popovic ZB, Smedira NG, Lytle BW, Marwick TH, et al. Long-term survival of patients with radiation heart disease undergoing cardiac surgery: a cohort study. Circulation 2013, 127, 1476–1485. [Google Scholar] [CrossRef]
- Donnellan E, Griffin BP, Johnston DR, Popovic ZB, Alashi A, Kapadia SR, et al. Rate of Progression of Aortic Stenosis and its Impact on Outcomes in Patients With Radiation-Associated Cardiac Disease: A Matched Cohort Study. JACC Cardiovasc Imaging 2018, 11, 1072–1080. [Google Scholar] [CrossRef]
- Shahian DM, Jacobs JP, Badhwar V, Kurlansky PA, Furnary AP, Cleveland JC, Jr. , et al. The Society of Thoracic Surgeons 2018 Adult Cardiac Surgery Risk Models: Part 1-Background, Design Considerations, and Model Development. Ann Thorac Surg. 2018, 105, 1411–1418. [Google Scholar] [CrossRef]
- Donnellan, E.; Masri, A.; Johnston, D.R.; Pettersson, G.B.; Rodriguez, L.L.; Popovic, Z.B.; Roselli, E.E.; Smedira, N.G.; Svensson, L.G.; Griffin, B.P.; et al. Long-Term Outcomes of Patients With Mediastinal Radiation–Associated Severe Aortic Stenosis and Subsequent Surgical Aortic Valve Replacement: A Matched Cohort Study. J. Am. Hear. Assoc. 2017, 6, e005396. [Google Scholar] [CrossRef]
- Ghoneim, A.; Bouhout, I.; Perrault, L.P.; Bouchard, D.; Pellerin, M.; Lamarche, Y.; Demers, P.; Carrier, M.; Cartier, R.; El-Hamamsy, I. Reexamining the Role of Surgical Aortic Valve Replacement After Mediastinal Radiation Therapy. Ann. Thorac. Surg. 2017, 104, 485–492. [Google Scholar] [CrossRef] [PubMed]
- Renker, M.; Schoepf, U.J.; Kim, W.K. Combined CT Coronary Artery Assessment and TAVI Planning. Diagnostics 2023, 13, 1327. [Google Scholar] [CrossRef] [PubMed]
- Zafar, M.R.; Mustafa, S.F.; Miller, T.W.; Alkhawlani, T.; Sharma, U.C. Outcomes after transcatheter aortic valve replacement in cancer survivors with prior chest radiation therapy: a systematic review and meta-analysis. Cardio-Oncology 2020, 6, 8. [Google Scholar] [CrossRef] [PubMed]
- Boyer, J.; Bartoli, A.; Deharo, P.; Vaillier, A.; Ferrara, J.; Barral, P.-A.; Jaussaud, N.; Morera, P.; Porto, A.; Collart, F.; et al. Feasibility of Non-Invasive Coronary Artery Disease Screening with Coronary CT Angiography before Transcatheter Aortic Valve Implantation. J. Clin. Med. 2023, 12, 2285. [Google Scholar] [CrossRef]
- Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2021.
- Mack, M.J.; Brennan, J.M.; Brindis, R.; Carroll, J.; Edwards, F.; Grover, F.; Shahian, D.; Tuzcu, E.M.; Peterson, E.D.; Rumsfeld, J.S.; et al. Outcomes Following Transcatheter Aortic Valve Replacement in the United States. JAMA 2013, 310, 2069–2077. [Google Scholar] [CrossRef]
- Tarantini, G.; Tang, G.; Fovino, L.N.; Blackman, D.; Van Mieghem, N.M.; Kim, W.-K.; Karam, N.; Carrilho-Ferreira, P.; Fournier, S.; Pręgowski, J.; et al. Management of coronary artery disease in patients undergoing transcatheter aortic valve implantation. A clinical consensus statement from the European Association of Percutaneous Cardiovascular Interventions in collaboration with the ESC Working Group on Cardiovascular Surgery. EuroIntervention 2023, 19, 37–52. [Google Scholar] [CrossRef]
- Leon MB, Smith CR, Mack M, Miller DC, Moses JW, Svensson LG, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010, 363, 1597–1607. [Google Scholar] [CrossRef]
- Waisbren, E.C.; Stevens, L.-M.; Avery, E.G.; Picard, M.H.; Vlahakes, G.J.; Agnihotri, A.K. Changes in Mitral Regurgitation After Replacement of the Stenotic Aortic Valve. Ann. Thorac. Surg. 2008, 86, 56–62. [Google Scholar] [CrossRef]
- Ternacle J, Krapf L, Mohty D, Magne J, Nguyen A, Galat A, et al. Aortic Stenosis and Cardiac Amyloidosis: JACC Review Topic of the Week. J Am Coll Cardiol. 2019, 74, 2638–2651. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ, et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2017, 38, 2739–2791. [Google Scholar] [CrossRef] [PubMed]
- Galat A, Guellich A, Bodez D, Slama M, Dijos M, Zeitoun DM, et al. Aortic stenosis and transthyretin cardiac amyloidosis: the chicken or the egg? Eur Heart J. 2016, 37, 3525–3531. [Google Scholar] [CrossRef]
- Java AP, Greason KL, Dispenzieri A, Grogan M, King KS, Maleszewski JJ, et al. Aortic valve replacement in patients with amyloidosis. J Thorac Cardiovasc Surg. 2018, 156, 98–103. [Google Scholar] [CrossRef]
- Cavalcante JL RS, Abdelkarim I, et al. Cardiac amyloidosis is prevalent in older patients with aortic stenosis and carries worse prognosis. J Cardiovasc Magn Reson 2017, 19, 98. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Proposed decision-making algorithm for the management of patients with severe aortic stenosis and cancer. Modified from Faggiano et Al, JACC Advances 2023. AS: aortic valve stenosis; SAVR: surgical aortic valve replacement; TAVR : transcatheter aortic valve replacement.
Figure 1.
Proposed decision-making algorithm for the management of patients with severe aortic stenosis and cancer. Modified from Faggiano et Al, JACC Advances 2023. AS: aortic valve stenosis; SAVR: surgical aortic valve replacement; TAVR : transcatheter aortic valve replacement.
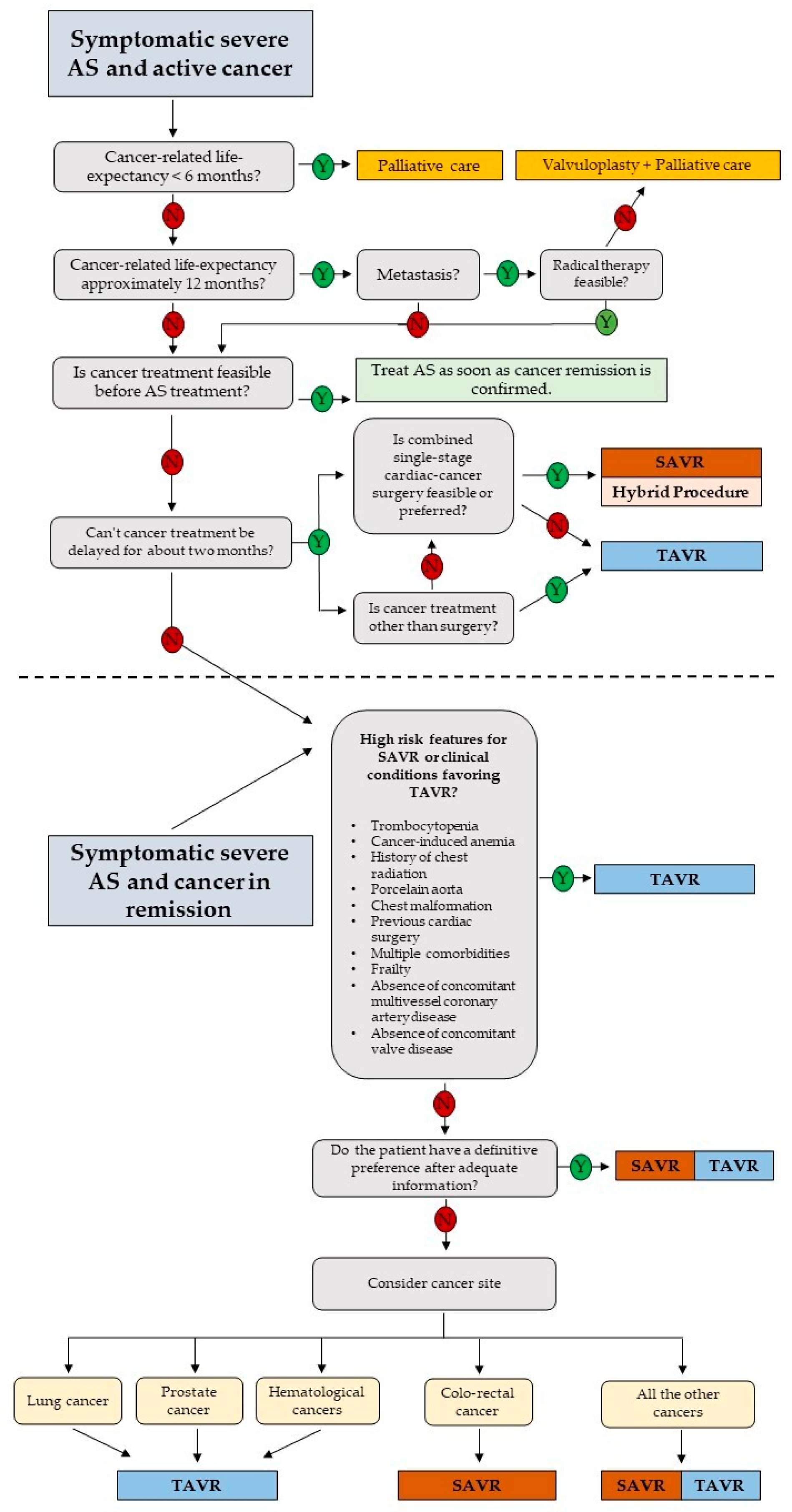

Table 1.
Prevalence of cancer in patients with severe aortic stenosis according to available studies.
Table 1.
Prevalence of cancer in patients with severe aortic stenosis according to available studies.
| Author | Reference | All population, n | Cancer, n (%) |
|---|---|---|---|
| Faggiano et al. | Int J Cardiol.2012;159(2):94-9 | 240 | 64(26.6%) |
| Mangner et al. | J Interv Cardiol. 2018;31(2):188-96 | 1821 | 99(5.4%) |
| Minamino-Muta et al. | Eur Heart J Qual Care Clin Outcomes. 2018;4(3):180-8. | 3815 | 513 (13.4%) |
| Okura et al. | Int Heart J. 2018;59(4):750-8. | 26325 | 111(0.42%) |
| Guha et al. | J Am Heart Assoc. 2020;9(2):e014248 | 47295 | 27960 (37.8%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



