
Submitted:
26 July 2023
Posted:
27 July 2023
You are already at the latest version
Abstract
Introduction: The aim of the present systematic review was to evaluate the clinical and radiographic success of partial pulpotomies in deep caries processes or post-eruptive defects in young, vital permanent teeth. Methods: Electronic databases, PubMed, Scopus, and Embase, were searched, followed by a manual search. Randomized controlled trials evaluating partial pulpo-tomy with a follow-up period of ≥12 months were included. Meta-analyses using a random effect model were performed. Results: A total of 3.127 articles were retrieved, and after duplicate re-moval, 2.642 were screened by title and abstract; 1 additional article was found during the manual search in the reference lists, and 79 were identified. Finally, 6 papers were included in the review. Regardless of the partial pulpotomy modalities or material used, there were no signifi-cant differences between clinical and radiographic success rates (cumulative success rate 91,8%-92,3%, respectively). Five studies were included in the meta-analysis that did not indicate any statistically significant differences in success rates when Mineral Trioxide Aggregate was compared to other materials (95% CI 0,239 to 1,016 p=0.055). Conclusion: This research system-atically evaluates the evidence and summarises the available data on partial pulpotomy in young permanent teeth. Given its high clinical and radiographic success rate, partial pulpotomy should be considered when vital pulpal therapy needs to be performed in highly damaged young per-manent teeth, as this procedure provides a biological benefit and allows more invasive endodon-tic treatments to be postponed.
Keywords:
Partial pulpotomy
; Minimal invasive endodontics
; Caries
; Molar Incisor Hypomineralization
1. Introduction
Avoiding irreversible dental treatments such as pulpectomy or extractions whenever possible is mandatory, especially in young patients. With the current state of knowledge, the emergence of new materials, and the increased consideration for minimally invasive treatments, partial pulpotomy (PP) is becoming a viable option that clinicians should consider when treating young patients [1,2,3].
Severe caries and enamel defects such as Molar Incisor Hypomineralization (MIH) affect many children worldwide: the prevalence of early childhood caries is around 48%, while it is 15% for MIH [1,2]. First, molars are particularly affected by caries as they are in a very vulnerable state, erupting at 6 years of age when brushing skills are often inadequate [4,5]. With regard to the pulp of teeth with MIH, a histological difference has been found compared to sound teeth: the presence of leucocytes is more significant, and innervation is altered due to the expression of neuropeptides and ion channels, resulting in peripheral sensitization [6]. Due to the hypomineralized enamel, an overlay of a carious process on MIH teeth is frequent, and if undetected, this can rapidly progress to the pulp [7]. Adopting the most conservative and least invasive treatments is necessary to maintain these teeth and all others affected as long as possible [8,9].
Considering this scenario, partial pulpotomy may represent a therapeutic option. The first reference to the term 'partial pulpotomy' in the dental literature was made by Cvek in 1978. The author reported that 96% of teeth with crown fractures healed after surgical amputation of 2-3 mm of inflamed pulp tissue [3]. Nowadays, partial pulpotomy is one of the vital pulpal treatments that allows physiological root development in young teeth with an open apex, avoiding root treatment or extraction [8,10]. PP is performed in cases of dental trauma and symptomatic deep caries in the dentin or when the tooth is severely damaged due to an enamel development defect [11,12].
Partial pulpotomy differs from total pulpotomy because the entire coronal pulp is removed in the latter procedure, and a drug is applied directly to the root canal orifices. It also differs from direct pulp cupping because the exposed pulp is only covered with dental material to facilitate the formation of a protective barrier [13]. In the case of PP, the recommended extent for removal of the inflamed pulp varies from 2 to 4 mm in different works [14]. All authors agree on the need to preserve as much of the pulp rich in coronal cells; this strategy increases the chances of healing due to physiological dentin deposition in the amputated area. Hemostasis, in the case of healthy pulp, should occur within 4-10 minutes, although different times are reported in the literature; if hemostasis is not achieved, more invasive treatment may be necessary [14,15,16].
Emerging materials and techniques that provide a good seal and better biocompatibility allow partial pulpotomy to be performed with less uncertainty [17,18]. Calcium hydroxide (CH) is a widely used alkaline material with a pH of up to 12.5, producing a bactericidal effect and allowing hard tissue formation [19,20]. However, concerns have been raised about its toxicity due to its caustic effect, inability to adhere to dentin, degradation over time, and tunnel defects in the restorative dentin bridge [21,22,23]. In recent years, searching for better materials has led Mineral Trioxide Aggregate (MTA) to be considered the gold standard for vital pulp therapies [24]. Already 20 years ago, Aeinehci et al. stated that a thicker dentinal bridge and a more evident odontoblastic layer were present in human teeth treated with MTA compared to those treated with CH [25]. Several studies have reported good physical and biocompatibility characteristics of MTA; the material allows satisfactory sealing, optimal marginal adaptation, and maintains a high pH for a long time [26,27,28]. In addition, it cannot be inhibited by blood or moisture and has low solubility [29,30].
Another material to consider for partial pulpotomy is Biodentine (BD), a calcium silicate cement (CSC) widely used for vital pulpal therapy [31,32]. The physical properties of BD compared to MTA are a reduced setting time and the replacement of bismuth oxide with zirconium oxide as a radio pacifier [33]. Biodentine has good biocompatibility and bioactivity, homogeneity, sealing ability, and high compressive strength [33]. Furthermore, BD has been reported to cause less coronal discoloration than MTA [34]. Finally, laser therapy could be considered an auxiliary tool for vital pulp therapy, as it can be used to achieve hemostasis and coagulation [35,36].
For the above reasons and current knowledge, partial pulpotomy is a viable treatment option. However, it is still unclear which of the numerous pulp capping materials provides the best clinical efficacy and tooth survival rate when used for the partial pulpotomy technique.
The present review and meta-analysis were planned to assess whether, in the presence of a correct diagnosis, a partial pulpotomy may be an appropriate treatment in young teeth, avoiding more invasive and complex techniques, such as abiogenesis, specification, or regenerative endodontics. In detail, this study aimed to systematically evaluate the evidence regarding the clinical and radiographic success and pathological outcomes of the techniques and materials used for partial pulpotomy. This meta-analysis included deep cariogenic processes and post-eruptive defects in young viable permanent teeth.
2. Materials and Methods
2.1. Protocol and Registration
This review was registered in the International Register of Systematic Reviews (PROSPERO) in March 2023 (CRD42023408988). The writing of this systematic review follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Supplementary Table S1).
2.2. Eligibility Criteria
The research question was formulated based on PICO and aimed to answer the following question: what is the success rate of partial pulpotomy in vital permanent teeth of children and young adults with severe caries lesions or developmental defects at 12 months? The following inclusion criteria were adopted: studies that included paediatric and young populations (age <24 years) with vital permanent teeth with caries and/or severe enamel defects treated with a partial pulpotomy. The age threshold of 24 years was chosen because, according to the literature, the cell signalling pathways associated with bacterial inflammation are weaker in the pulp of children and young adults, which could explain the better endodontic results [37,38]. Furthermore, the World Health Organization's definition of "young" covers the age range of 10 to 24 years [39]. The comparators considered were teeth treated by partial pulpotomy with different materials: MTA, Calcium hydroxide and Biodentine, used alone or in combination with other materials/devices; teeth treated with other pulpal therapies were not considered. No sex or health condition limitations were indicated. Only randomized clinical trials written in English and published between 2012 and 2022 were considered. Exclusion criteria were studies that included participants with teeth treated only with other vital pulp therapies, such as complete pulpotomy and direct or indirect pulp capping, traumatized teeth, or partial pulpotomies with a follow-up of less than 12 months.
2.3. Search Strategy
The electronic search was conducted using three databases: PubMed (National Library of Medicine), Embase (Elsevier), and Scopus (Elsevier). The search was performed from 15th October to 31st December 2022. A search on grey literature (Google Scholar) was made in March 2023. All the references were uploaded onto Endnote® software for duplicate management and study selection. The search strategy for each database is displayed in the supplementary file (Supplementary Table S2). Finally, the reference lists of the studies included were hand searched to identify additional records.
2.4. Study Selection and Data Extraction
After the exclusion of duplicates, two independent authors (NC and MGC) screened the papers according to title and abstract; in case of doubt, the opinion of a third author (GC) was sought. After full-text evaluation, selected articles were uploaded onto a Microsoft Office Excel® spreadsheet (Supplementary Table S3). Data extraction was performed in duplicate (NC and MEO), including a description of the study design, outcome, variables assessed, and results. Every effort was made to obtain the original data from the Authors, who e-mail and/or ResearchGate® contacted. Cohen's kappa value for reviewer agreement was performed for abstracts and full texts.
2.5. Risk of Bias
The risk of bias in the included studies was assessed by the ROB-2 tool [40]. The bias evaluated were confounding, selection of participants, classification of interventions, deviation from intended interventions, missing data, measurement of outcomes, and selection of reported results. Two reviewers (NC and MCG) conducted the assessments, and the discussion resolved divergences.
2.6. Outcome Measures
The primary outcome of this review was the clinical success rate assessed as the absence of pain, swelling, mobility, abscess, percussion tenderness, and/or the radiographic success rate considered as the absence of periapical radiolucency and periodontal ligament enlargement. Secondary outcomes were the restoration type and oral health-related quality of life as measured by standardized questionnaires.
2.7. Heterogeneity
The heterogeneity was evaluated for correspondence between subjects’ characteristics, interventions, and outcomes. The Random Effect analysis was applied, and statistical heterogeneity was performed using I2 statistic; values over 50% indicated heterogeneity and significance was present at p<0.1.
2.8. Synthesis of the Results
The MedCalc® package was employed for the analysis. A meta-analysis was considered appropriate and conducted in the presence of studies with comparable data, i.e., reporting the same outcome, interventions, and same follow-up time (NC and GC). The total number of treated subjects with events was analyzed and compared for dichotomous data. The confidence interval was calculated at 95%.
3. Results
A total of 3.127 articles were retrieved, and after duplicate removal, 2.642 were screened by title and abstract and 2564 were excluded (Supplementary Table S4); 78 papers were identified, and 1 additional article was found during the search in the study's reference lists. After full-text evaluation, 73 papers were discharged (Supplementary Table S5) and 6 studies were included in the systematic review, of which 5 in the meta-analysis [3,41,42,44,46]. The search strategy can be seen in the PRISMA flowchart (Figure 1). Cohen's kappa value for the inter-reviewer agreement was 0.58 at the title and abstract screening (95.6% agreement) and 0.83 at full-text screening (96.2% agreement).
3.1. Study Characteristics
All included studies were parallel RCTs published between 2014 and 2022 and can be found on PubMed, Embase and Scopus. General characteristics of the included studies are reported in Table 1. All the studies were carried out in university/college settings and received university grants, except two [3,42].
Table 2 shows the main characteristics of the six studies included. The sample sizes ranged from 50 [6] to 105 [42] patients, with a corresponding number of teeth ranging between 50 [6] and 119 [42]; the age of the participants ranged from 6 [43,44] to 15 [44]. Regarding interventions, all the studies evaluated the success rate of partial pulpotomy at 12 months; the other follow-ups were done at different time points at 1 [44], 3 [3,6,42,44], 6 [3,6,42,43,44,45] and 24 months [3,6,43,45]. The most common dental material used for pulp therapy was MTA, while the final restoration was performed with many different techniques: composite resin [43,44,45], stainless steel crown [6,42,46], glass ionomer cement [6,44,45], prosthetic crown [45], and amalgam [3]. All the studies considered success based on clinical and radiographical outcomes. Clinical failure was declared in case of pain, swelling, mobility, abscess, and tenderness to percussion. Radiographical failure was instead considered in periapical radiolucency cases and periodontal ligament widening in all studies.
One study, not included in the meta-analysis, compared partial pulpotomy with other viable pulpal therapies [6]: indirect pulpal treatment, partial, cervical, and total pulpotomy. The study was the only one to treat teeth with MIH and showed a higher clinical and radiographic success rate at 24 months with indirect pulp treatment (95,8%), but the results were not statistically significant if compared to the success rate of partial or cervical pulpotomy (85,7% for both).
The five studies included in the meta-analysis compared the success rate of partial pulpotomy with MTA with that of other materials/device: Chailertvanitkul et al. [3] and Ozgur et al. [43] with Calcium hydroxide, Uyar et al. [42] with calcium hydroxide and Biodentine, Uesrichai et al. [46] with Biodentine and Tozar et al. [44] with MTA plus Erbium CrYGG laser.
The data in Table 2 were calculated using the proportions for dropouts and overall success; each data was found in the tables of the selected manuscripts.
3.2. Risk of Bias Assessment
Figure 2 presents the main results of the risk of bias assessment of the included studies. In three studies [42,44,46], a certain risk of bias was found, while in the other four, a low risk of bias was found [3,6,43,45]. The randomization process for patient allocation and deviations from the intended interventions were judged to be at low risk for all selected studies. The studies were rated at a low risk of attrition bias because dropouts were low. Outcome measurement was clearly stated in most studies, as was information on methods and standardization of procedures.
3.3. Qualitative Synthesis
The overall success rate considering clinical and radiographic success of partial pulpotomy at 12-month follow-up was greater than 85% in all studies. In the studies considered for the meta-analysis, partial pulpotomy with Calcium hydroxide, Biodentine, MTA plus laser had a cumulative success rate of 91,8%. In comparison, partial pulpotomy with MTA had a cumulative success rate of 92,3%. Saline or hypochlorite solution did not significantly affect the outcomes [43]. The Er: CrYSGG laser did not show significantly better results when applied before MTA [44].
Concerning secondary outcomes, none of the included studies compared treatments to the amount of pulp removed, type of restoration, or oral health-related quality of life using standardized questionnaires.
3.4. Quantitative Synthesis
Quantitative synthesis was achieved by combining 5 papers that compared the success rate of partial pulpotomy using MTA compared to other materials such as calcium hydroxide, Biodentine, or MTA + laser Er [3,42,43,44,46]. Random-effect model showed no statistical significance in the success rate: p=0,055, 95%CI 0,239 to 1,016. The heterogeneity among studies was low I2 (inconsistency) =0%. The resulting forest plot is shown in Figure 2.
Statistical analysis of publication bias was not performed as fewer than 10 studies were included.
4. Discussion
To the authors' knowledge, this systematic review is the first to have performed a meta-analysis of the available studies on the clinical/radiographic effectiveness of partial pulpotomy using different materials in children and young adults. There are not yet many RCTs on PP, but those identified are of good quality and generally agree that this vital pulp therapy has a high clinical and radiographic success rate, exceeding 85% at 12 months follow-up. These results agree with those described in another systematic review on partial pulpotomy which found a clinical success rate of 93% at 12 months [47]. An umbrella analysis found overall success rates for complete and partial pulpotomies of 88.5% and 90.6%, respectively [48]. At the same time, viable direct pulp capping techniques appear to have a lower success rate, above 75% at 12 months [13]. No evidence of the superiority of Mineral Trioxide Aggregate over other materials was found in the present study. The material used on the amputated pulp does not influence the success rate. The results indicate that all materials examined, i.e., MTA, Calcium hydroxide, Biodentine, and MTA + Erbium (Er) laser, produced satisfactory clinical performance. However, concerns may arise regarding the relatively short follow-up period (12 months) of the included studies, as treatment stability over time may also depend on the performance of the pulpotomy material used. Therefore, in the state of the art and knowledge, further well-designed randomized clinical trials are needed to assess which material is most effective for long-term partial pulpotomy. Especially when newly erupted teeth are treated, adequate follow-ups are necessary to evaluate the success of therapy and apical closure. In the latter cases, it is essential to preserve pulpal viability as long as possible to increase the longevity of the treated tooth.
Although the actual pulp status can only be determined histologically [46], a 96.6% correlation has been found between reversible pulpitis's clinical and histological status [49]. The key to the success of partial pulpotomy lies in the following factors: accurate pre-treatment diagnosis (reversible pulpitis), correct isolation of the tooth, adequate removal of the infected pulp, a reasonable choice of materials, and congruent restoration. Bleeding control is also crucial in the success of PP: hemostasis should be achieved within 2-4 minutes if proper pulpal removal has been performed [6]. This review has not identified a restorative material or technique superior in the success of PP; however, in endodontics, the importance of an excellent marginal seal that prevents further invasion of microorganisms is well known [50].
This review considered studies in which PP had been performed for deep carious lesions (ICDAS 4,5,6) and post-eruptive breakdown, as the latter is often superimposed on a carious lesion, such as in cases of severe MIH [51]. The site of exposure of the tooth could influence the success rate [45]; more failures have been found with axial than occlusal exposures. Occlusal exposures have a more favorable prognosis because the more permeable cervical third is preserved, and tooth isolation is easier [45,52]. Including post-eruptive lesions adds value to this work, as treating this type of lesion is a daily activity for many pediatric dentists worldwide. Due to the scarcity of selected studies, it was impossible to compare the success of partial pulpotomy performed in decayed teeth or with MIH. However, this could be a target for future studies, as knowing which technique or material works best would be vital in improving clinical outcomes of this very prevalent enamel development defect.
Further studies on pulp treatments for MIH-affected teeth are needed, especially now that classification systems such as the MIH severity scoring system (MIH-SSS) are becoming popular among pediatric dentists [53]. Awareness of the MIH-SSS should be disseminated among general dentists, as it could be assumed that many MIH teeth are included in clinical research considered as decayed teeth. Indeed, studies confirm the lack of knowledge of the developmental defects of enamel among general dentists [54,55,56].
The American Association of Endodontics and the European Society of Endodontology guidelines support vital pulp techniques, even on teeth with closed apex or mature pulp [57,58]. The new clinical trend is to avoid or at least delay invasive treatments, as the possibility of maintaining part of the pulp vital now that materials and techniques are highly specialized is important; dissemination of the vital pulp therapies among clinicians should be recommended. Future treatment directions should focus on clear and standardized indications to guide clinicians in the extent of pulp removal to make it easier for dentists to include partial pulpotomy in their everyday practice.
Minimally invasive dental techniques, such as partial pulpotomy, should also be taught in dental schools and among specialists in pediatric dentistry and endodontics [59,60].
Anyhow the evidence of the interventions under investigation in this review is not strong enough to support any clinical recommendations. One of the limitations of this meta-analysis is that in the clinical trials included, it was impossible to blind the operators to the material used. Moreover, the low number of studies included reduces the level of evidence. This difficulty in finding eligible studies was mainly related to methodological discrepancies in sample/teeth selection and the absence of a precise definition of partial pulpotomy. In particular, some studies were not included in this review as they include patients with a wide age range and do not provide results according to age. Indeed, some articles were excluded because there was no clear distinction between partial pulpotomy, direct pulp capping, and complete pulpotomy. Another weakness of the study is that aiming to extract as much information as possible about PP studies without clear distinction on the age groups that were included but not used for the meta-analysis. In addition, there is a lack of data assessing how the success of the therapy affects the quality of life, which can be significantly impaired by pain or functional limitations in chewing. As previously suggested [13], future research should involve rigorously defined methodology and standardization of specific criteria for the techniques used and the variables considered. In a general scenario in which minimal invasive dentistry is encouraged by scientific evidence, this review, and others on a similar topic, underline that choosing conservative treatments should be preferable. Given the reduced evidence from this review, eminent guidelines such as those of the American Association of Endodontics or the European Society of Endodontology might be encouraged [57,58].
5. Conclusions
This systematic literature review demonstrates that Partial pulpotomy is a successful dental procedure when vital pulpal therapy is required in highly damaged young permanent teeth. Comparable clinical and radiological success was found for all materials used, i.e. Mineral Trioxide Aggregate, MTA+laser, Calcium Hydroxide and Biodentine. The biological sparing of partial pulpotomy is an important result that allows more invasive endodontic treatments to be postponed.
Supplementary Materials
The following supporting information can be downloaded at: www.mdpi.com/xxx/s1 Table S1. Prisma check-list; Table S2. Search string; Table S3. Extraction form; Table S4. Papers discarded after title and abstract evaluation; Table S5. Papers discarded after full text evaluation.
Author Contributions
Conceptualization, NC. and GC.; methodology, GC.; software, MGC.; validation, MEO., NC., and GC.; formal analysis, SC.; investigation, GC.; resources, SC.; data curation, NC and MGC.; writing—original draft preparation, NC and CG.; writing—review and editing, MEO.; visualization, SC.; supervision, GC.; project administration, MGC; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Uribe, S.E.; Innes, N.; Maldupa, I. The global prevalence of early childhood caries: A systematic review with meta-analysis using the WHO diagnostic criteria. Int J Paediatr Dent 2021, 31, 817–830. [Google Scholar] [CrossRef] [PubMed]
- Zhao, D.; Dong, B.; Yu, D.; Ren, Q.; Sun, Y. The prevalence of molar incisor hypomineralization: evidence from 70 studies. Int J Paediatr Dent 2018, 28, 170–179. [Google Scholar] [CrossRef] [PubMed]
- Chailertvanitkul, P.; Paphangkorakit, J.; Sooksantisakoonchai, N.; Pumas, N.; Pairojamornyoot, W.; Leela-Apiradee, N.; Abbott, P.V. Randomized control trial comparing calcium hydroxide and mineral trioxide aggregate for partial pulpotomies in cariously exposed pulps of permanent molars. Int Endod J 2014, 47, 835–842. [Google Scholar] [CrossRef] [PubMed]
- Pujar, P.; Subbareddy, V.V. Evaluation of the tooth brushing skills in children aged 6-12 years. Eur Arch Paediatr Dent 2013, 14, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Boustedt, K.; Dahlgren, J.; Twetman, S.; Roswall, J. Tooth brushing habits and prevalence of early childhood caries: a prospective cohort study. Eur Arch Paediatr Dent 2020, 21, 155–159. [Google Scholar] [CrossRef]
- Al-Batayneh, O.B.; Abdelghani, I.M. Outcome of vital pulp therapy in deeply carious molars affected with molar incisor hypomineralisation (MIH) defects: a randomized clinical trial. European Archives of pediatric dentistry : official journal of the European Academy of Paediatric Dentistry 2022, 23, 587–599. [Google Scholar] [CrossRef] [PubMed]
- Ghanim, A.M.; Manton, D.J.; Morgan, M.V.; Marino, R.J.; Bailey, D.L. Trends of oral health care and dental treatment needs in relation to molar incisor hypomineralisation defects: a study amongst a group of Iraqi schoolchildren. Eur Arch Paediatr Dent 2012, 13, 171–178. [Google Scholar] [CrossRef]
- Ricucci, D.; Siqueira, J.F.; Li, Y.; Tay, F.R. Vital pulp therapy: histopathology and histobacteriology-based guidelines to treat teeth with deep caries and pulp exposure. Journal of Dentistry 2019, 86, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Leong, D.J.X.; Yap, A.U. Vital pulp therapy in carious pulp-exposed permanent teeth: an umbrella review. Clin Oral Investig 2021, 25, 6743–6756. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.M.; Ricucci, D.; Saoud, T.M.; Sigurdsson, A.; Kahler, B. Vital pulp therapy of mature permanent teeth with irreversible pulpitis from the perspective of pulp biology. Aust Endod J 2020, 46, 154–166. [Google Scholar] [CrossRef]
- Alqaderi, H.E.; Al-Mutawa, S.A.; Qudeimat, M.A. MTA pulpotomy as an alternative to root canal treatment in children's permanent teeth in a dental public health setting. J Dent 2014, 42, 1390–1395. [Google Scholar] [CrossRef]
- Rodd, H.D.; Boissonade, F.M.; Day, P.F. Pulpal status of hypomineralized permanent molars. Pediatr Dent 2007, 29, 514–520. [Google Scholar]
- Tong, H.J.; Seremidi, K.; Stratigaki, E.; Kloukos, D.; Duggal, M.; Gizani, S. Deep dentine caries management of immature permanent posterior teeth with vital pulp: A systematic review and meta-analysis. J Dent 2022, 124, 104214. [Google Scholar] [CrossRef] [PubMed]
- Ghoddusi, J.; Forghani, M.; Parisay, I. New approaches in vital pulp therapy in permanent teeth. Iran Endod J 2014, 9, 15–22. [Google Scholar] [PubMed]
- Baume, L.J.; Holz, J. Long-term clinical assessment of direct pulp capping. Int Dent J 1981, 31, 251–260. [Google Scholar] [PubMed]
- Fong, C.D.; Davis, M.J. Partial pulpotomy for immature permanent teeth, its present and future. Pediatr Dent 2002, 24, 29–32. [Google Scholar]
- Witherspoon, D.E. Vital pulp therapy with new materials: new directions and treatment perspectives--permanent teeth. J Endod 2008, 34, S25–28. [Google Scholar] [CrossRef]
- Witherspoon, D.E.; Small, J.C.; Harris, G.Z. Mineral trioxide aggregate pulpotomies: a case series outcomes assessment. J Am Dent Assoc 2006, 137, 610–618. [Google Scholar] [CrossRef]
- Bogen, G.; Kim, J.S.; Bakland, L.K. Direct pulp capping with mineral trioxide aggregate: an observational study. J Am Dent Assoc 2008, 139, 305–315, quiz 305-315. [Google Scholar] [CrossRef]
- Cox, C.F.; Suzuki, S. Re-evaluating pulp protection: calcium hydroxide liners vs. cohesive hybridization. J Am Dent Assoc 1994, 125, 823–831. [Google Scholar] [CrossRef]
- Cox, C.F.; Subay, R.K.; Ostro, E.; Suzuki, S.; Suzuki, S.H. Tunnel defects in dentin bridges: their formation following direct pulp capping. Oper Dent 1996, 21, 4–11. [Google Scholar] [PubMed]
- Stanley, H.R. Pulp capping: conserving the dental pulp--can it be done? Is it worth it? Oral Surg Oral Med Oral Pathol 1989, 68, 628–639. [Google Scholar] [CrossRef] [PubMed]
- Schuurs, A.H.; Gruythuysen, R.J.; Wesselink, P.R. Pulp capping with adhesive resin-based composite vs. calcium hydroxide: a review. Endod Dent Traumatol 2000, 16, 240–250. [Google Scholar] [CrossRef]
- Palczewska-Komsa, M.; Kaczor-Wiankowska, K.; Nowicka, A. New Bioactive Calcium Silicate Cement Mineral Trioxide Aggregate Repair High Plasticity (MTA HP)-A Systematic Review. Materials (Basel) 2021, 14. [Google Scholar] [CrossRef]
- Aeinehchi, M.; Eslami, B.; Ghanbariha, M.; Saffar, A.S. Mineral trioxide aggregate (MTA) and calcium hydroxide as pulp-capping agents in human teeth: a preliminary report. Int Endod J 2003, 36, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Moghaddame-Jafari, S.; Mantellini, M.G.; Botero, T.M.; McDonald, N.J.; Nor, J.E. Effect of ProRoot MTA on pulp cell apoptosis and proliferation in vitro. J Endod 2005, 31, 387–391. [Google Scholar] [CrossRef]
- Torabinejad, M.; Parirokh, M.; Dummer, P.M.H. Mineral trioxide aggregate and other bioactive endodontic cements: an updated overview - part II: other clinical applications and complications. Int Endod J 2018, 51, 284–317. [Google Scholar] [CrossRef]
- Parirokh, M.; Torabinejad, M.; Dummer, P.M.H. Mineral trioxide aggregate and other bioactive endodontic cements: an updated overview - part I: vital pulp therapy. Int Endod J 2018, 51, 177–205. [Google Scholar] [CrossRef]
- Vanderweele, R.A.; Schwartz, S.A.; Beeson, T.J. Effect of blood contamination on retention characteristics of MTA when mixed with different liquids. J Endod 2006, 32, 421–424. [Google Scholar] [CrossRef]
- Torabinejad, M.; Hong, C.U.; McDonald, F.; Pitt Ford, T.R. Physical and chemical properties of a new root-end filling material. J Endod 1995, 21, 349–353. [Google Scholar] [CrossRef]
- Katge, F.A.; Patil, D.P. Comparative Analysis of 2 Calcium Silicate-based Cements (Biodentine and Mineral Trioxide Aggregate) as Direct Pulp-capping Agent in Young Permanent Molars: A Split Mouth Study. J Endod 2017, 43, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Slaboseviciute, M.; Vasiliauskaite, N.; Drukteinis, S.; Martens, L.; Rajasekharan, S. Discoloration Potential of Biodentine: A Systematic Review. Materials (Basel) 2021, 14. [Google Scholar] [CrossRef] [PubMed]
- Kaur, M.; Singh, H.; Dhillon, J.S.; Batra, M.; Saini, M. MTA versus Biodentine: Review of Literature with a Comparative Analysis. J Clin Diagn Res 2017, 11, ZG01–ZG05. [Google Scholar] [CrossRef]
- Al-Hiyasat, A.S.; Ahmad, D.M.; Khader, Y.S. The effect of different calcium silicate-based pulp capping materials on tooth discoloration: an in vitro study. BMC Oral Health 2021, 21, 330. [Google Scholar] [CrossRef] [PubMed]
- Toomarian, L.; Fekrazad, R.; Sharifi, D.; Baghaei, M.; Rahimi, H.; Eslami, B. Histopathological evaluation of pulpotomy with Er,Cr:YSGG laser vs formocresol. Lasers Med Sci 2008, 23, 443–450. [Google Scholar] [CrossRef] [PubMed]
- Marx, I.; Op't Hof, J. The Er,Cr:YSGG hydrokinetic laser system for dentistry--clinical applications. SADJ 2002, 57, 323–326. [Google Scholar]
- Aslantas, E.E.; Buzoglu, H.D.; Karapinar, S.P.; Cehreli, Z.C.; Muftuoglu, S.; Atilla, P.; Aksoy, Y. Age-related Changes in the Alkaline Phosphatase Activity of Healthy and Inflamed Human Dental Pulp. J Endod 2016, 42, 131–134. [Google Scholar] [CrossRef]
- Aslantas, E.E.; Buzoglu, H.D.; Muftuoglu, S.F.; Atilla, P.; Karapinar, S.P.; Aksoy, Y. Effects of aging and inflammation on catalase activity in human dental pulp. Arch Oral Biol 2022, 141, 105482. [Google Scholar] [CrossRef]
- WHO. SIXTY-FOURTH WORLD HEALTH ASSEMBLY - Youth and health risks 2011.
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. Rob 2: a revised tool for assessing the risk of bias in randomized trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Özgür, B.; Kargın, S.T.; Ölmez, M.S. Clinical evaluation of giomer- and resin-based fissure sealants on permanent molars affected by molar-incisor hypomineralization: a randomized clinical trial. BMC Oral Health 2022, 22, 275. [Google Scholar] [CrossRef]
- Uyar, D.S.; Alacam, A. Evaluation of partial pulpotomy treatment in cariously exposed immature permanent molars: Randomized controlled trial. Niger J Clin Pract 2021, 24, 1511–1519. [Google Scholar] [CrossRef]
- Özgür, B.; Uysal, S.; Güngör, H.C. Partial Pulpotomy in Immature Permanent Molars After Carious Exposures Using Different Hemorrhage Control and Capping Materials. Pediatric dentistry 2017, 39, 364–370. [Google Scholar]
- Tozar, K.N.; Erkmen Almaz, M. Evaluation of the Efficacy of Erbium, Chromium-doped Yttrium, Scandium, Gallium, and Garnet Laser in Partial Pulpotomy in Permanent Immature Molars: A Randomized Controlled Trial. Journal of Endodontics 2020, 46, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Kang, C.M.; Kim, S.H.; Shin, Y.; Lee, H.S.; Lee, J.H.; Kim, G.T.; Song, J.S. A randomized controlled trial of ProRoot MTA, OrthoMTA and RetroMTA for pulpotomy in primary molars. Oral Dis 2015, 21, 785–791. [Google Scholar] [CrossRef] [PubMed]
- Uesrichai, N.; Nirunsittirat, A.; Chuveera, P.; Srisuwan, T.; Sastraruji, T.; Chompu-inwai, P. Partial pulpotomy with two bioactive cements in permanent teeth of 6- to 18-year-old patients with signs and symptoms indicative of irreversible pulpitis: a noninferiority randomized controlled trial. International Endodontic Journal 2019, 52, 749–759. [Google Scholar] [CrossRef]
- Albaiti, S.S.; Albishri, R.F.; Alhowig, M.T.; Tayyar, W.I.; Alqurashi, N.F.; Alghamdi, F.T. Partial Pulpotomy as an Applicable Treatment Option for Cariously Exposed Posterior Permanent Teeth: A Systematic Review of Randomized Clinical Trials. Cureus 2022, 14, e26573. [Google Scholar] [CrossRef]
- Lin, G.S.S.; Yew, Y.Q.; Lee, H.Y.; Low, T.; Pillai, M.P.M.; Laer, T.S.; Wafa, S. Is pulpotomy a promising modality in treating permanent teeth? An umbrella review. Odontology 2022, 110, 393–409. [Google Scholar] [CrossRef]
- Ricucci, D.; Loghin, S.; Siqueira, J.F., Jr. Correlation between clinical and histologic pulp diagnoses. J Endod 2014, 40, 1932–1939. [Google Scholar] [CrossRef] [PubMed]
- Muliyar, S.; Shameem, K.A.; Thankachan, R.P.; Francis, P.G.; Jayapalan, C.S.; Hafiz, K.A. Microleakage in endodontics. J Int Oral Health 2014, 6, 99–104. [Google Scholar]
- Goel, N.; Jha, S.; Bhol, S.; Dash, B.P.; Sarangal, H.; Namdev, R. Molar Incisor Hypomineralization: Clinical Characteristics with Special Emphasis on Etiological Criteria. J Pharm Bioallied Sci 2021, 13, S651–S655. [Google Scholar] [CrossRef]
- Cho, S.Y.; Seo, D.G.; Lee, S.J.; Lee, J.; Lee, S.J.; Jung, I.Y. Prognostic factors for clinical outcomes according to time after direct pulp capping. J Endod 2013, 39, 327–331. [Google Scholar] [CrossRef]
- Cabral, R.N.; Nyvad, B.; Soviero, V.; Freitas, E.; Leal, S.C. Reliability and validity of a new classification of MIH based on severity. Clin Oral Investig 2020, 24, 727–734. [Google Scholar] [CrossRef]
- Alanzi, A.; Faridoun, A.; Kavvadia, K.; Ghanim, A. Dentists' perception, knowledge, and clinical management of molar-incisor-hypomineralisation in Kuwait: a cross-sectional study. BMC Oral Health 2018, 18, 34. [Google Scholar] [CrossRef]
- Delgado, R.M.; Botelho, J.; Machado, V.; Mendes, J.J.; Lopes, L.B. Knowledge, perception, and clinical experiences on molar incisor hypomineralization amongst Portuguese dentists. BMC Oral Health 2022, 22, 250. [Google Scholar] [CrossRef]
- Gamboa, G.C.S.; Lee, G.H.M.; Ekambaram, M.; Yiu, C.K.Y. Knowledge, perceptions, and clinical experiences on molar incisor hypomineralization among dental care providers in Hong Kong. BMC Oral Health 2018, 18, 217. [Google Scholar] [CrossRef]
- European Society of Endodontology developed, b.; Duncan, H.F.; Galler, K.M.; Tomson, P.L.; Simon, S.; El-Karim, I.; Kundzina, R.; Krastl, G.; Dammaschke, T.; Fransson, H.; et al. European Society of Endodontology position statement: Management of deep caries and the exposed pulp. Int Endod J 2019, 52, 923–934. [Google Scholar] [CrossRef]
- Therapy, A.A.o.E.S.C.o.V.P. AAE Position Statement on Vital Pulp Therapy. Guidelines & Position Statements AAE 2021.
- Chevalier, V.; Le Fur Bonnabesse, A.; Duncan, H.F. Frightened of the pulp? A qualitative analysis of undergraduate student confidence and stress during the management of deep caries and the exposed pulp. Int Endod J 2021, 54, 130–146. [Google Scholar] [CrossRef]
- Duncan, H.F. Present status and future directions-Vital pulp treatment and pulp preservation strategies. Int Endod J 2022, 55 Suppl 3, 497–511. [Google Scholar] [CrossRef]
Figure 1.
Prisma flow chart.
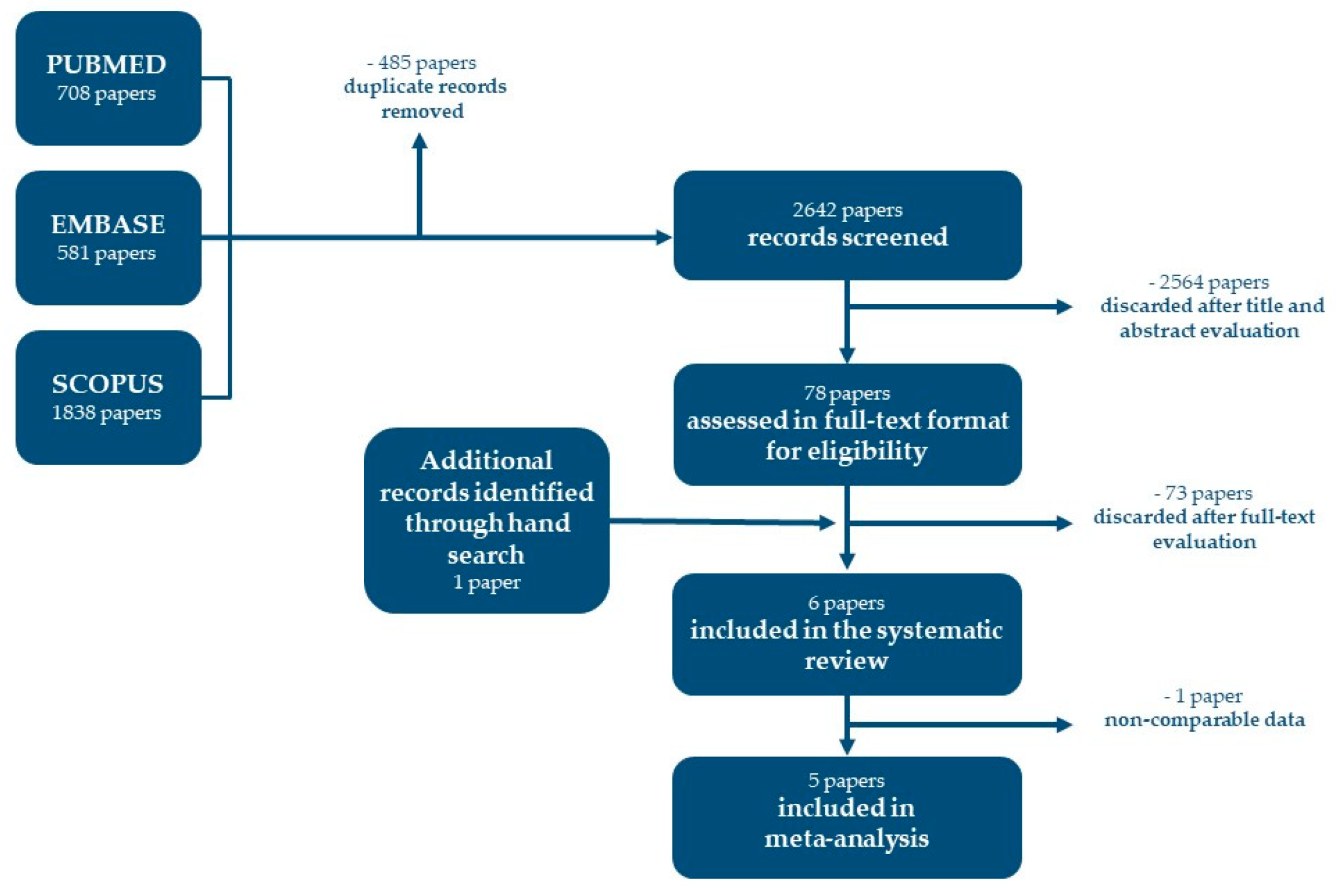
Figure 2.
Risk of Bias assessment.
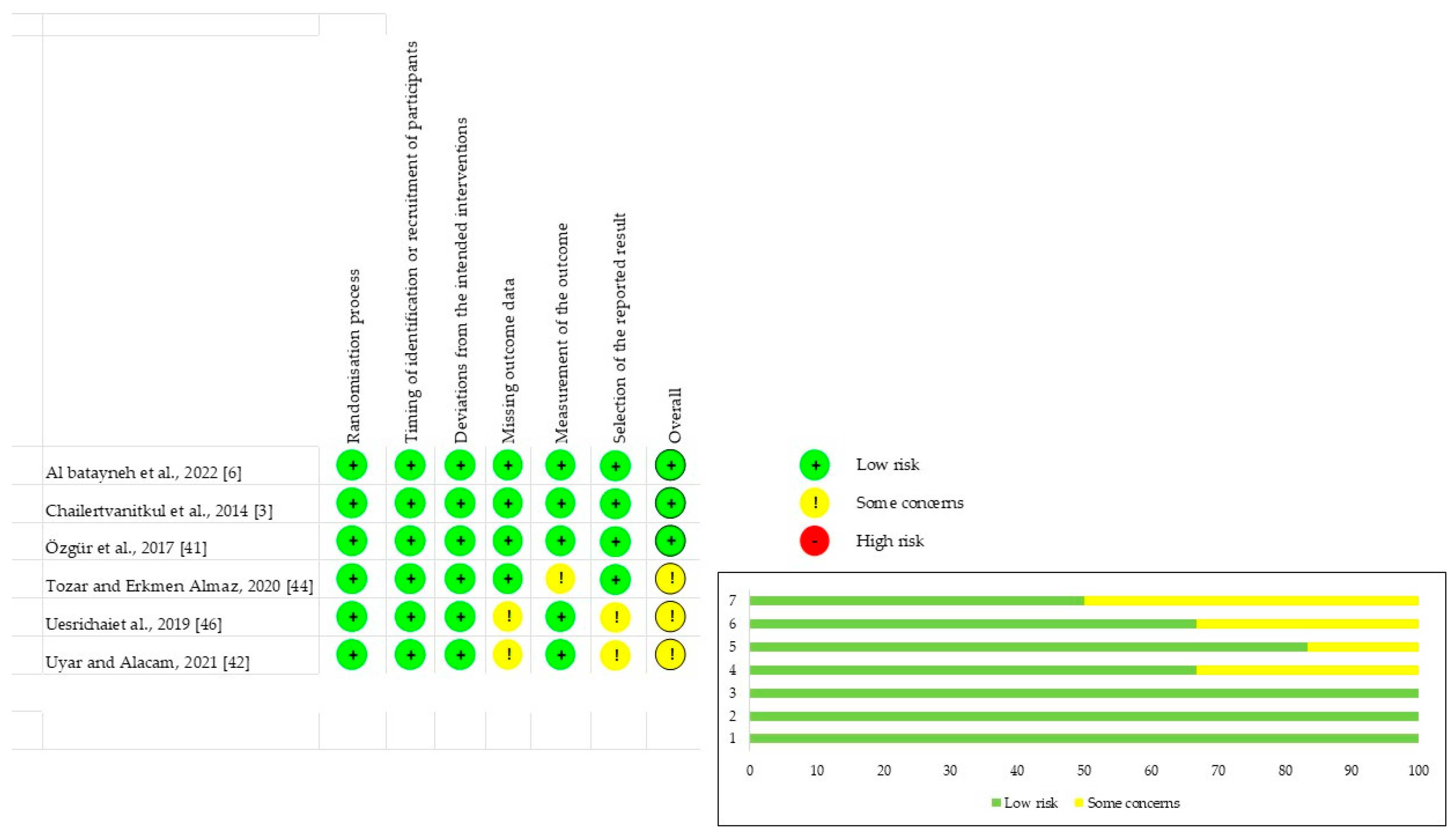
Figure 3.
Forest plot - Success of partial pulpotomy using MTA vs CH, BD and MTA+laser.


Table 1.
General characteristics of the included studies.
| First Author (year) | Source | Location | Funding source |
|---|---|---|---|
| Al-batayneh et al., 2022 [6] | Eur Arch Paed Dent | Jordan | University grant |
| Chailertvanitkul et al., 2014 [3] | Int Endod J | Thailand | Not reported |
| Özgür et al., 2017 [41] | BMC Oral Health | Turkey | University grant |
| Tozar and Erkmen Almaz, 2020 [44] | J Endod | Turkey | University grant |
| Uesrichaiet al., 2019 [46] | Int Endod J | Thailand | University grant |
| Uyar and Alacam, 2021 [42] | Niger J Clin Pract | Turkey | None |
Table 2.
Table 2. Main characteristics of the included studies.
| Study | Age (Rage or Mean) | Patients (n) | Teeth (n) | Drop-Out of Teeth n (%) | Study Design | Final Restoration | Follow-Up (mo.) | Overall Success Rate at 12 mo. (n/total) | Conclusion | |
|---|---|---|---|---|---|---|---|---|---|---|
| Test | Control | |||||||||
| Al-batayneh et al., 2022 [6]* | 11±3.2 yy | 50 | 50 | 3/50 (6.0%) | PP vs IPC or FP | GIC, SSC | 3, 6, 12, 24 | PP 11/12 | IPC 2/25 | VTP is a valid option in severe carious lesions of permanent first molars with MIH over 24 mo. IPC had a higher success rate (95.8%) than PP or CP (85.7% for both). |
| FP 2/11 | ||||||||||
| Chailertvanitkul et al., 2014 [3] | 7-10 yy | 80 | 84 | 8/84 (9.5%) | MTA vs CH | Amalgam | 3, 6, 12, 24 | MTA 41/44 | CH 37/40 | PP using MTA or CH resulted in favourable treatment outcomes. Unfavorable outcomes increase for pulp exposure >5 mm |
| Özgür et al., 2017 [43] | 6-13 yy | 63 | 80 | 4/80 (5.0%) | MTA vs CH | CR | 6, 12, 18, 24 | MTA/SH 19/20 | CH/SH 19/20 | PP with MTA or CH produces comparable and favorable results in immature permanent teeth. |
| MTA/SS 20/20 | CH/SS 19/19 | |||||||||
| Tozar and Erkmen Almaz, 2020 [44] | 6-15 yy | 90 | 90 | 3/90 (3.3%) | MTA vs MTA + Laser Er, Cr: YSGG | GIC, CR | 1, 3, 6, 12 | MTA 40/45 | MTA+Laser 43/45 | The use of the laser did not contribute to the success rate compared to MTA alone. |
| Uesrichaiet al., 2019 [46] | 10 yy | 69 | 69 | 2/67 (3.0%) | MTA vs BD | C, SSC | 32.2±17.9 | MTA 34/37 | BD 26/30 | Permanent teeth with signs and symptoms of irreversible pulpitis were successfully treated with PP using MTA and BD. |
| Uyar and Alacam, 2021 [42] | 7.9 yy | 105 | 119 | 0/54 (0.0%) | MTA vs CH or BD | SSC | 3, 6, 12 | MTA 17/18 | CH 13/18 | PP treatment is a good option and has high success rates at 12 months with CH, MTA and BD. |
| BD 17/18 | ||||||||||
N: number; yy: years; mo.: moths; PP: partial pulpotomy; CP: cervical pulpotomy; FP: full pulpotomy; VPT: vital pulp therapy; MTA: Mineral Trioxide Aggregate; BD: Biodentine; CH: Calcium hydroxide; CR: Composite resin; GIC: glass ionomer cement; SSC: stainless steel crown; DCP: direct pulp capping; IPC: indirect pulp capping; SH: sodium hypochlorite; SS: sterile saline *Not included in meta-analysis.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



