
Submitted:
24 July 2023
Posted:
26 July 2023
You are already at the latest version
Abstract
Amyotrophic lateral sclerosis (ALS) is a neurodegenerative disease with a complex genetic architecture, showing monogenic, oligogenic, and polygenic inheritance. In this study, we describe the case of a 71 years-old man diagnosed with ALS with an atypical phenotype, due to the presence of a progressive ocular ptosis. Genetic analyses revealed two variants in SOD1 and TBK1 genes respectively and the LHON-associated m.14484T>C variant in the mitochondrial DNA (mtDNA). We discuss how all these variants may synergically impinge on mitochondrial function, contributing to the pathogenic mechanisms which might ultimately lead to the neurodegenerative process, possibly influencing the clinical ALS phenotype.
Keywords:
SOD1
; amyotrophic lateral sclerosis
; TBK1
; mitochondrial DNA
; oligogenic inheritance.
1. Introduction
Amyotrophic lateral sclerosis (ALS) is a fatal neurodegenerative disease conventionally classified as familial or sporadic. However, besides this simple subdivision, the genetic architecture underlying the disease’s pathogenesis is highly complex, showing monogenic, oligogenic, and polygenic inheritance, with variable gene penetrance and heritability [1].
Monogenic familial amyotrophic lateral sclerosis accounts for 10–15% of affected individuals, albeit with incomplete penetrance [2]. In the remaining 85%, large genome-wide association studies (GWAS) have been useful to identify rare or private variants that might act as risk factors and/or disease modifiers, thus modulating phenotypic presentation [2].
Nowadays, ALS’ pathogenesis is considered as a multi-step disease process, where multiple hits, both genetic and environmental, are needed to develop the disease [3]. Furthermore, several observations proved that the burden of multiple genetic rare variants might trigger the degenerative process, modulating also the clinical phenotype [4].
Recently, a large study on ALS [5] pointed to the burden of multiple risk factors disclosed in the nuclear genome but missed to consider the impact of mitochondrial DNA (mtDNA) variation, which is frequently neglected but may contribute to the pathogenesis or modulate the phenotype also in ALS. As an example, we reported the unique association of ALS and Leber’s hereditary optic neuropathy (LHON) in two unrelated patients who had a late onset ALS with rapid diseases course, speculating that mtDNA might have contributed as a possible risk factor or disease modifier in ALS [6].
Here we report a new case of a SOD1 patient carrying an additional variant in TBK1 gene and the LHON-associated m.14484T>C variant in the mtDNA. This case supports the oligogenic nature of ALS and further rises questions on the possible contributory role of mtDNA variation in the ALS pathogenesis and clinical expression.
2. Case presentation
A 71-years-old man came to our attention for the progressive onset of weakness in his legs, started three years before, and worsened in the past year, leading to the use of aids in walking. Since the age of 58, he also reported progressive bilateral eyelid droop, without clear daily fluctuation.
His past history was relevant for hypertension under pharmacological treatment. From the age of 54, he also suffered from a progressive hearing loss, interpreted as mixed (transmissive and sensory) and partially related to otosclerosis, for which he underwent surgery, without any improvement.
In his family history, he had a brother with progressive hearing loss (started at 55 years), and unspecified gait disturbances associated with increased creatin kinase (CK) levels. The patient did not report any other neurological disease recurring in his family.
The neurological examination revealed bilateral severe ocular ptosis without deficits in ocular movements, bilateral hypoacusia, hyposthenia and hypotrophy in the lower limbs, especially in the distal compartment on the right side. Deep tendon reflexes were diffusely reduced. Gait showed right drop foot with steppage. Exacerbation of ptosis after effort or repeated closing of the eyes was not noted.
Due to the association of hypoacusia and bilateral ptosis, a mitochondrial disorder was suspected.
Routine blood exams only showed an increase of CK (367 U/L, n.v. < 170). Antibodies against acetylcholine receptor were negative.
Brain Magnetic Resonance revealed bilateral fronto-parietal atrophy and mild signs of microangiopathy. FLAIR-T2-weighted sequence displayed hyperintensity of the cortico-spinal tracts (Figure 1a,b). Spectroscopy did not reveal pathological lactate in ventricles.
The optic coherence tomography (OCT) showed normal findings.
Similarly, the cerebrospinal fluid analysis revealed normal proteins and cells levels.
Electromyography (EMG) showed the presence of subacute neurogenic changes in the lower limbs (right > left), in particular in right vastus medialis, left gastrocnemius and bilateral tibialis anterior muscles. Genioglossus, right biceps brachialis and left first dorsal interosseous were normal.
These findings raised the suspicion of a motor neuron disease.
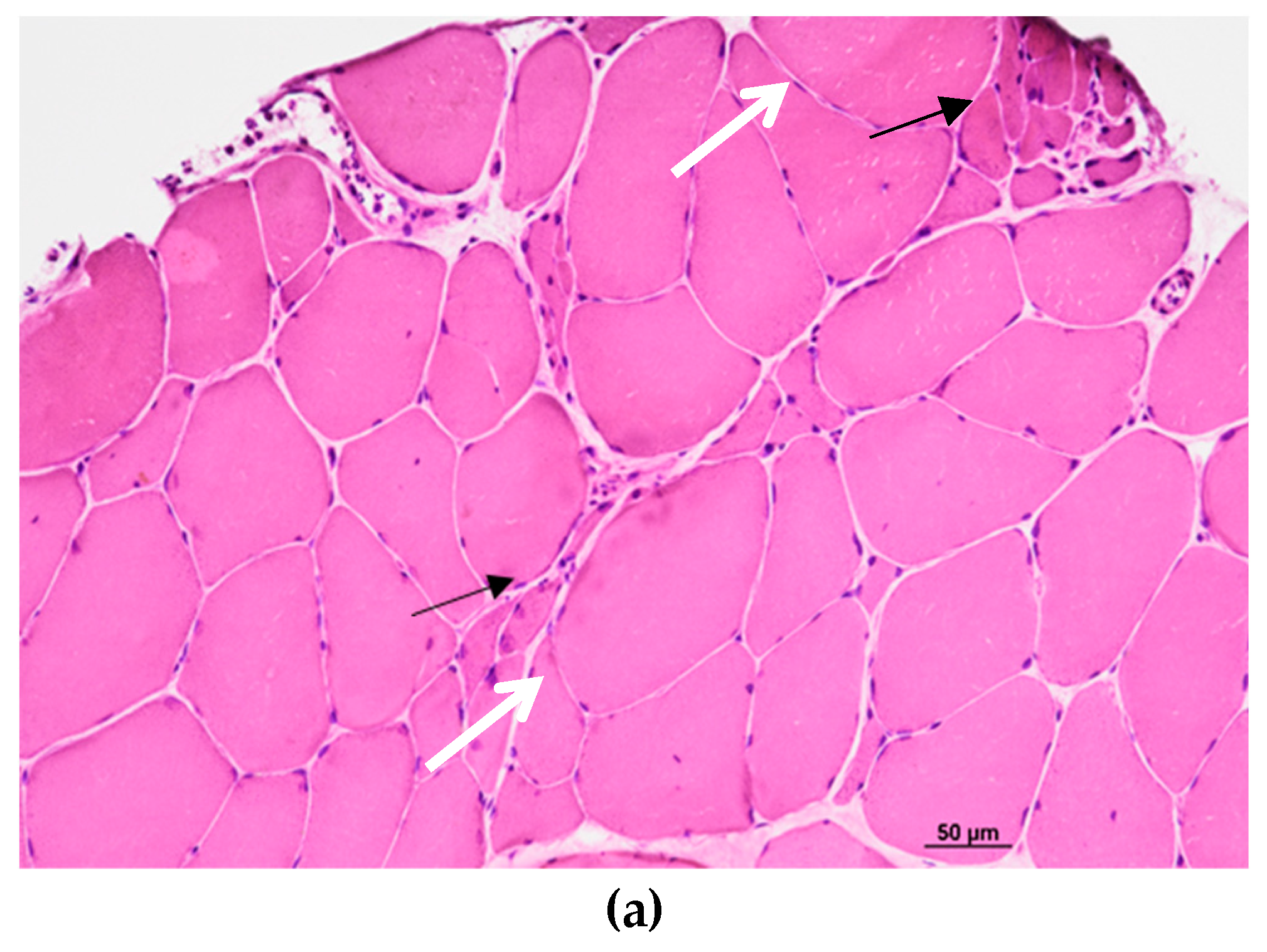
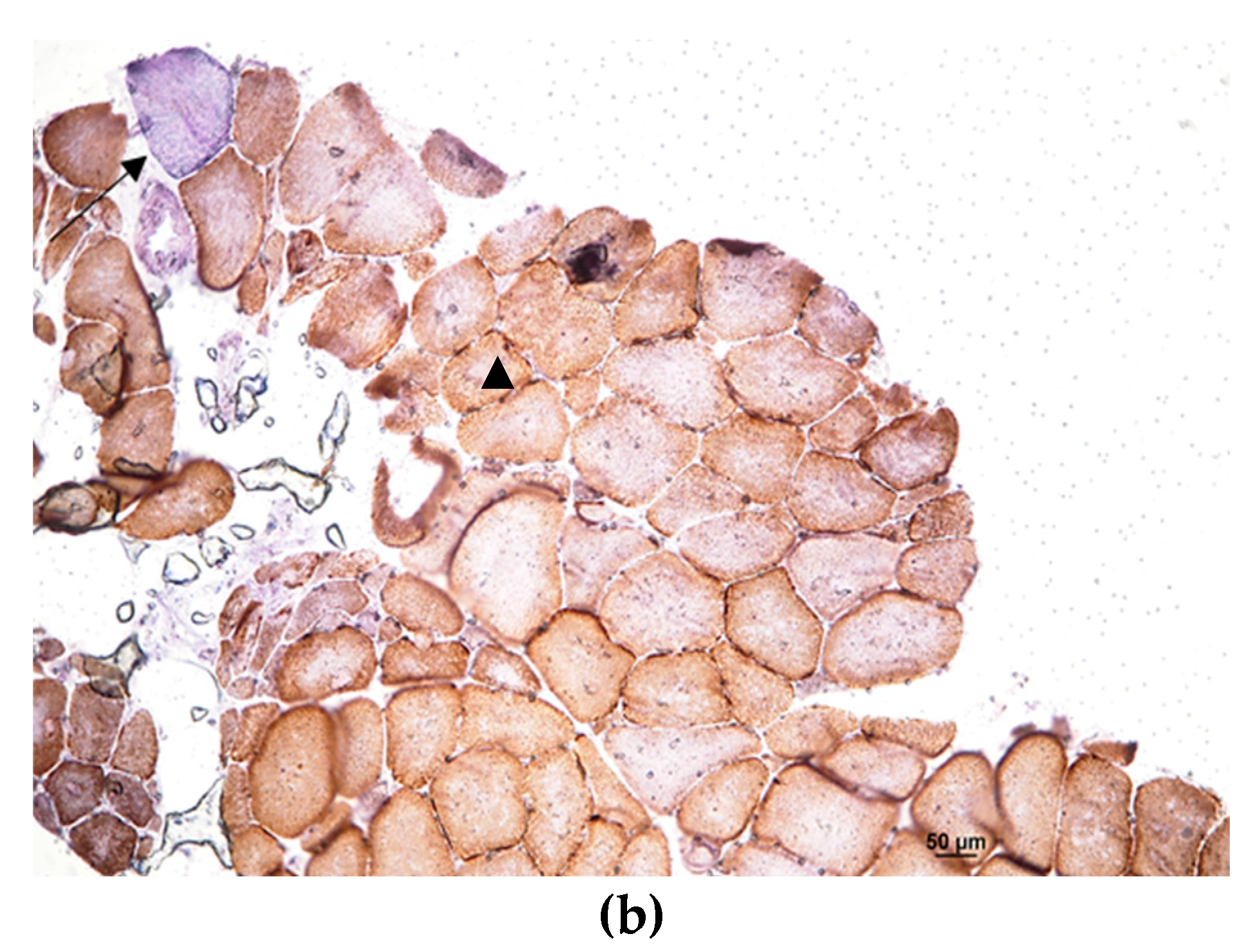
The tibialis anterior muscle biopsy confirmed the presence of neurogenic changes (Figure 2a), without clear signs of a primary mitochondrial disease, except for a few fibers displaying subsarcolemmal enhancement and a single COX negative fiber observed with the double COX/SDH staining, both probably due to a secondary defect (Figure 2b).
Genetic analysis, through Whole Exome Sequencing (WES) with an in silico panel analysis, was initially focused on the fronto-temporal dementia (FTD)-ALS related genes (SOD1, FUS, TARBP, SEXT, ANXA11, CHCHD10, DTCN1, FIG4, HNRNPA1, KIF5A, MATR3, NEK1, OPTN, PFN1, SIGMAR1, SPG11, SQSTM1, TUBA4A, UBQLN2, VAPB, VCP), and revealed the presence of the heterozygous variant c.412A>G (p.Thr138Ala) in the SOD1 gene (NM_000454.5), and the heterozygous variant c.422T>C (p.Ile141Thr) in the TBK1 gene (NM_013254.4). The presence of expanded alleles in the C9Orf72 gene was also excluded.
The heterozygous p.Thr138Ala variant in the SOD1 gene (OMIM*147450), which was not reported in the gnomAD v.2.1.1 database, was classified as pathogenic (PP5, PP3, PM2, PM5, PM1, PP2 criteria) according to the American College of Medical Genetics (ACMG) guidelines (Richards et al., 2015). Relevantly, the p.Thr138Ala could be a likely founder variant, since it was reported in three other Italian patients with ALS, supporting its pathogenic role [7-9].
The heterozygous p.Ile141Thr in the TBK1 gene (OMIM*604834) was a very rare variant (1/250,400 alleles in gnomAD) and was classified as hot VUS (PP3, PM2) according to the ACMG guidelines. This gene has been associated to ALS and/or frontotemporal dementia with an autosomal dominant inheritance (MIM#616439).
Therefore, a diagnosis of motor neuron disease with a selective involvement of lower motor neurons (progressive muscular atrophy, PMA) was made.
Due to the progressive bilateral ptosis, atypical for a motor neuron disease, we also screened a panel of genes associated to chronic progressive external ophthalmoplegia (CPEO) (ABAT, AFG3L2, C10orf2, DGUOK, DNA2, DNM1L, FBXL4, GFER, MFN2, MGME1, MPV17, OPA1, POLG, POLG2, RNASEH1, RRM2B, SLC25A10, SPG7, SUCLA2, SUCLG1, TFAM, TK2, TOP3A, TYMP) that resulted negative as well as a panel of 176 genes associated with non-syndromic hearing loss and deafness (data not shown).
Finally, to further investigate the CPEO phenotype, we analyzed the mtDNA extracted from skeletal muscle. Quantitative testing for pathologic accumulation of single/multiple macrodeletions was normal and the mtDNA copy number assessment showed an increase of around 30% compared to controls. The complete mtDNA sequencing revealed the presence of the Leber’s hereditary optic neuropathy (LHON) associated homoplasmic variant m.14484T>C/MT-ND6 on a H1a3c haplogroup background.
Neurofilament light chain levels in the CSF were also investigated and were significantly increased (5822 pg/ml, v.n. 340-650).
The patient’s clinical conditions continued to progress over the years: at a 2-years follow-up he was not able to stand or walk autonomously anymore, and he also showed a moderate hypotrophy and weakness in the upper limbs with functional deficits; no bulbar involvement was detected.
3. Discussion
Ocular ptosis is not a classic symptom of ALS, although it has been rarely reported [10-12]. Intriguingly, De Marchi et al. reported two siblings with a history of progressive ptosis without ocular movement impairment, diagnosed with a bulbar ALS with rapid progression [12]. Thus, notwithstanding the rarity, our case is not unprecedented. To disclose the possible genetic cause, we first aimed at screening the major genes associated with ALS and FTD, as well as searching for expansion in C9Orf72, revealing a combination of two different genetic variants of interest.
To further refine the genetic investigation, in consideration of the ptosis and sensorineural deafness affecting our patient pointing to a possible mitochondrial disease, we also screened mtDNA extracted from the muscle biopsy. Analyses for mtDNA single/multiple deletions was within normal range. Sequencing the entire mtDNA revealed as incidental finding the homoplasmic pathogenic variant m.14484T>C/MT-ND6, on a haplotype H1a3c background. The copy number was higher than control range, in agreement with the compensatory mechanism already described in patients carrying LHON pathogenic variants [13] and congruently to the occasional subsarcolemmal increase of COX/SDH staining. The m.14484T>C/MT-ND6 variant is causative of LHON, but was never described in CPEO phenotypes, and therefore cannot explain by itself the ocular ptosis of our patient. Furthermore, our patient did not show any signs of optic neuropathy, and his family history was negative for cases suggestive of LHON on the maternal lineage. This is not surprising, as is well established that the m.14484T>C/MT-ND6 variant expresses the LHON phenotype principally in the context of the haplogroup J [14] and has been frequently found in population screenings without being linked to LHON [15]. In fact, as recently highlighted, the LHON m.11778G>A/MT-ND4 and m.14484T>C/MT-ND6 variants have been both found to be present in 1 every 800-1000 individuals from normal populations, associated with low penetrance mtDNA backgrounds such as haplogroups H and U [16,17], thus reinforcing the idea that deleterious mtDNA variants may be incidentally found when investigating patients for a neurodegenerative disorder.
Overall, the PMA phenotype, classically characterized by a prevalent dysfunction of the lower motor neuron, and the quite long disease duration of our case could be mainly explained by the SOD1 variant, already found in patients with a spinal onset, absence of bulbar involvement and a slow disease progression, with a variable age at onset (mean 53 years, ranging from 35 to 73 years) [7-9]. On the other hand, the co-occurrence of another variant in an ALS-FTD gene, the TBK1 gene, is consistent with the oligogenic and complex background underlying both sporadic and familial ALS [1]. TBK1 has been reported to contribute to around 1.3% ALS, 3%–4% ALS-FTD, and <1% FTD with TDP-43 pathology [18]. Among the patients with TBK1 mutations, over 50% patients were diagnosed as ALS, as well as 18% FTD, 14% FTD-ALS, and 1.3% AD [19]. The clinical manifestations are highly heterogeneous, and intrafamilial and interfamilial heterogeneity were also reported in patients carrying the same variants [20]. The most common initial symptoms included limb weakness, cognitive deficits, and bulbar signs. This extreme heterogeneity makes genetic-phenotype correlations quite challenging.
Furthermore, this case, in particular the uncertain role of the mtDNA m.14484T>C/MT-ND6 pathogenic variant, deserves a few more comments. We previously reported the unprecedented occurrence in two unrelated patients with ALS of another LHON homoplasmic mutation, the most common m.11778G>A/MT-ND4 change, associated with optic atrophy in only one of the two patients. We speculated that the mtDNA could have played a role as disease modifier in these patients, as they were characterized by late-onset ALS and rapid course to death [6]. Our current findings in this other patient remark that mtDNA variants in ALS are probably more frequent than expected and deserve to be systematically explored in conjunction with the nuclear genome analysis, to better evaluate their possible role in the disease pathogenesis, penetrance and clinical evolution. In support, rare cases of ALS patients with causative mtDNA mutations and clear signs of mitochondrial disease have been also reported [21].
Remarkably, all genes found in our patient are known to play an essential role in mitochondrial function. First, the Cu/Zn superoxide dismutase 1 protein (SOD1) is an abundantly expressed antioxidant enzyme that exists as a homodimer and localizes to the cytosol, but also in the intermembrane mitochondrial space, whereas the manganese superoxide dismutase 2 (SOD2) is in the mitochondrial matrix [22]. Besides the antioxidant properties, it has been implicated in signal transduction, and both its wild-type and mutant forms are prone to misfolding [23,24]. Therefore, dysfunctional SOD1 may lead to increased reactive oxygen species (ROS) levels, but also to the formation of insoluble aggregates, associated with the mitochondrial outer membrane, of both perturbated and wild-type forms. It is already known that in the SOD1-G93A mouse model mitochondria appeared with dilated and disorganized cristae, both in the axons and dendrites of motor neurons at onset of disease [25]. Changes in mitochondrial morphology, such as swelling or enlargement, were also found in soma, proximal axons and motor nerve terminals in tissue from ALS patients [26], which result in an impairment of their axonal transport in motor neurons [27]. Since morphological abnormalities in mice appeared before the onset of symptoms of motor neuron degeneration, it has been postulated that mitochondria impairment may play a key role in starting motor neuron degeneration in ALS, although the exact pathological mechanism remains unclear.
On the other hand, the NF-kappa-B-activating kinase encoded by the TBK1 gene plays a critical role in several cellular pathways, including selective clearance of mitochondria and regulation of inflammation. Indeed, this kinase binds to and phosphorylates a number of proteins involved in innate immunity and autophagy, including optineurin (OPTN) and p62, both of which have been implicated in ALS. In details, TBK1-OPTN axis targets damaged mitochondria for degradation via PINK1/parkin-mediated mitophagy [28]. Functional studies revealed that mutations disrupting the structure of the protein impair the recruitment of TBK1 to damaged mitochondria, inhibiting the mitophagy process [29]. Moreover, primary neurons expressing TBK1 mutations demonstrated higher baseline levels of mitochondrial stress and an inability to manage induced oxidative damage, both of which may contribute to neurodegeneration [30].
To conclude, as primary mtDNA defects such as the m.14484T>C/MT-ND6 variant are well known to impair the activity of complex I, leading to a decrease in ATP synthesis and an increasing generation of ROS [31,32], we propose as plausible that all variants identified in this patient may contribute to mitochondrial dysfunction and motor neuron degeneration, possibly leading to the atypical phenotype of our patient. This case illustrates how multiple nuclear and mitochondrial variants may ultimately contribute to the neurodegenerative process, with a leading role for mitochondrial dysfunction in ALS pathogenesis. A systematic parallel analysis of nuclear encoded risk factors for ALS in conjunction with mtDNA sequence analysis is warranted in large cohort studies to fully clarify this possible missing genetic contribution to ALS pathogenesis.
Author Contributions
Conceptualization, V.V., R.L. and V.C.; methodology, F.P., D.O., C.F., L.C., M.L.V., S.C. and V.C.; investigation, V.V., F.P., D.O., C.F., A.F., L.C., A.M., M.L.V., S.C., R.L. and V.C.; data curation, V.V., F.P., D.O., C.F., A.F., L.C., A.M., M.L., S.C., R.L.; writing—original draft preparation, V.V., F.P., and V.C.; writing—review and editing, D.O., C.F., A.F., L.C., A.M., M.L.V., S.C., R.L. and V.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Area Vasta Emilia Romagna (CE-AVEC -17151-17152).
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article
Acknowledgments
We are thankful to the patient for agreeing to this publication. Palombo F. and Carelli V. were supported by the Italian Ministry of Health with the “Ricerca Corrente” funding. Vacchiano V., M.L. Valentino, Liguori R and Carelli V. are members of ERN-NMD.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Goutman, S.A.; Hardiman, O.; Al-Chalabi, A.; Chió, A.; Savelieff, M.G.; Kiernan, M.C.; Feldman, E.L. Emerging insights into the complex genetics and pathophysiology of amyotrophic lateral sclerosis. Lancet Neurol. 2022, 21, 465–479. [Google Scholar] [CrossRef]
- Ryan, M.; Heverin, M.; McLaughlin, R.L.; Hardiman, O. Lifetime Risk and Heritability of Amyotrophic Lateral Sclerosis. JAMA Neurol. 2019, 76, 1367–1374. [Google Scholar] [CrossRef]
- Al-Chalabi, A.; Calvo, A.; Chio, A.; Colville, S.; Ellis, C.M.; Hardiman, O.; Heverin, M.; Howard, R.S.; Huisman MHB, Keren, N. ; Leigh, P.N.; Mazzini, L.; Mora, G.; Orrell, R.W.; Rooney, J.; Scott, K.M.; Scotton, W.J.; Seelen, M.; Shaw, C.E.; Sidle, K.S.; Swingler, R.; Tsuda, M.; Veldink, J.H.; Visser, A.E.; van den Berg, L.H.; Pearce, N. Analysis of amyotrophic lateral sclerosis as a multistep process: a population-based modelling study. Lancet Neurol. 2014, 13, 1108–1113. [Google Scholar] [CrossRef]
- van Blitterswijk, M.; van Es, M.A.; Hennekam, E.A.; Dooijes, D.; van Rheenen, W.; Medic, J.; Bourque, P.R.; Schelhaas, H.J.; van der Kooi, A.J.; de Visser, M.; de Bakker, P.I.; Veldink, J.H.; van den Berg, L.H. Evidence for an oligogenic basis of amyotrophic lateral sclerosis. Hum Mol Genet. 2012, 21, 3776–3784. [Google Scholar] [CrossRef]
- van Rheenen, W.; van der Spek RAA, Bakker MK et al (2021) Common and rare variant association analyses in amyotrophic lateral sclerosis identify 15 risk loci with distinct genetic architectures and neuron-specifc biology. Nat Genet 53, 1636–1648. [CrossRef]
- Amore, G.; Vacchiano, V.; La Morgia, C.; Valentino, M.L.; Caporali, L.; Fiorini, C.; Ormanbekova, D.; Salvi, F.; Bartoletti-Stella, A.; Capellari, S.; Liguori, R.; Carelli, V. Co-occurrence of amyotrophic lateral sclerosis and Leber's hereditary optic neuropathy: is mitochondrial dysfunction a modifier? J Neurol. 2023, 270, 559–564. [Google Scholar] [CrossRef]
- Zhang, M.; Xi, Z.; Ghani, M.; Jia, P.; Pal, M.; Werynska, K.; Moreno, D.; Sato, C.; Liang, Y.; Robertson, J.; Petronis, A.; Zinman, L.; Rogaeva, E. Genetic and epigenetic study of ALS-discordant identical twins with double mutations in SOD1 and ARHGEF28. J Neurol Neurosurg Psychiatry. 2016, 87, 1268–1270. [Google Scholar] [CrossRef]
- Visani, M.; de Biase, D.; Bartolomei, I.; Plasmati, R.; Morandi, L.; Cenacchi, G.; Salvi, F.; Pession, A. A novel T137A SOD1 mutation in an Italian family with two subjects affected by amyotrophic lateral sclerosis. Amyotroph Lateral Scler. 2011, 12, 385–388. [Google Scholar] [CrossRef]
- Origone, P.; Caponnetto, C.; Verdiani, S.; Mantero, V.; Cichero, E.; Fossa, P.; Bellone, E.; Mancardi, G.; Mandich, P. T137A variant is a pathogenetic SOD1 mutation associated with a slowly progressive ALS phenotype. Amyotroph Lateral Scler. 2012, 13, 398–399. [Google Scholar] [CrossRef] [PubMed]
- Pinto, S.; de Carvalho, M. Amyotrophic lateral sclerosis patients and ocular ptosis. Clin Neurol Neurosurg. 2008, 110, 168–170. [Google Scholar] [CrossRef]
- Shindo, K.; Satake, A.; Fukao, T.; Ichinose, Y.; Takiyama, Y. Palpebral ptosis as the initial symptom of amyotrophic lateral sclerosis. Neurol Sci. 2020, 41, 211–212. [Google Scholar] [CrossRef] [PubMed]
- De Marchi, F.; Corrado, L.; Bersano, E.; Sarnelli, M.F.; Solara, V.; D'Alfonso, S.; Cantello, R.; Mazzini, L. Ptosis and bulbar onset: an unusual phenotype of familial ALS? Neurol Sci. 2018, 39, 377–378. [Google Scholar] [CrossRef] [PubMed]
- Giordano, C.; Iommarini, L.; Giordano, L.; Maresca, A.; Pisano, A.; Valentino, M.L.; Caporali, L.; Liguori, R.; Deceglie, S.; Roberti, M.; Fanelli, F.; Fracasso, F.; Ross-Cisneros, F.N.; D'Adamo, P.; Hudson, G.; Pyle, A.; Yu-Wai-Man, P.; Chinnery, P.F.; Zeviani, M.; Salomao, S.R.; Berezovsky, A.; Belfort, R., Jr.; Ventura, D.F.; Moraes, M.; Moraes Filho, M.; Barboni, P.; Sadun, F.; De Negri, A.; Sadun, A.A.; Tancredi, A.; Mancini, M.; d'Amati, G.; Loguercio Polosa, P.; Cantatore, P.; Carelli, V. Efficient mitochondrial biogenesis drives incomplete penetrance in Leber's hereditary optic neuropathy. Brain 2014, 137 Pt 2, 335–353. [Google Scholar] [CrossRef]
- Hudson, G.; Carelli, V.; Spruijt, L.; Gerards, M.; Mowbray, C.; Achilli, A.; Pyle, A.; Elson, J.; Howell, N.; La Morgia, C.; Valentino, M.L.; Huoponen, K.; Savontaus, M.L.; Nikoskelainen, E.; Sadun, A.A.; Salomao, S.R.; Belfort, R., Jr.; Griffiths, P.; Yu-Wai-Man, P.; de Coo, R.F.; Horvath, R.; Zeviani, M.; Smeets, H.J.; Torroni, A.; Chinnery, P.F. Clinical expression of Leber hereditary optic neuropathy is affected by the mitochondrial DNA-haplogroup background. Am J Hum Genet. 2007, 81, 228–233. [Google Scholar] [CrossRef]
- Bolze, A., Mendez, F., White, S., Tanudjaja, F., Isaksson, M., Rashkin, M., Bowes, J. er al. Selective constraints and pathogenicity of mitochondrial DNA variants inferred from a novel database of 196, 554 unrelated individuals. bioRxiv. 2019; (Preprint at) https://doi.org/10.1101/798264. [CrossRef]
- Watson, E.C.; Davis, R.L.; Ravishankar, S.; Copty, J.; Kummerfeld, S.; Sue, C.M. Low disease risk and penetrance in Leber hereditary optic neuropathy. Am J Hum Genet. 2023, 110, 166–169. [Google Scholar] [CrossRef]
- Mackey, D.A.; Ong, J.S.; MacGregor, S.; Whiteman, D.C.; Craig, J.E.; Lopez Sanchez MIG, Kearns, L. S.; Staffieri, S.E.; Clarke, L.; McGuinness, M.B.; Meteoukki, W.; Samuel, S.; Ruddle, J.B.; Chen, C.; Fraser, C.L.; Harrison, J.; Howell, N.; Hewitt, A.W. Is the disease risk and penetrance in Leber hereditary optic neuropathy actually low? Am J Hum Genet. 2023, 110, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.P.; Van Broeckhoven, C.; van der Zee, J. ALS Genes in the Genomic Era and their Implications for FTD. Trends Genet. 2018, 34, 404–423. [Google Scholar] [CrossRef]
- Yu, H.; Yu, W.; Luo, S.S.; Yang, Y.J.; Liu, F.T.; Zhang, Y.; Chen, Y.; Sun, Y.M.; Wu, J.J. Association of the TBK1 mutation p.Ile334Thr with frontotemporal dementia and literature review. Mol Genet Genomic Med. 2019, 7, e547. [Google Scholar] [CrossRef]
- Freischmidt, A.; Wieland, T.; Richter, B.; Ruf, W.; Schaeffer, V.; Müller, K.; Marroquin, N.; Nordin, F.; Hübers, A.; Weydt, P.; Pinto, S.; Press, R.; Millecamps, S.; Molko, N.; Bernard, E.; Desnuelle, C.; Soriani, M.H.; Dorst, J.; Graf, E.; Nordström, U.; Feiler, M.S.; Putz, S.; Boeckers, T.M.; Meyer, T.; Winkler, A.S.; Winkelman, J.; de Carvalho, M.; Thal, D.R.; Otto, M.; Brännström, T.; Volk, A.E.; Kursula, P.; Danzer, K.M.; Lichtner, P.; Dikic, I.; Meitinger, T.; Ludolph, A.C.; Strom, T.M.; Andersen, P.M.; Weishaupt, J.H. Haploinsufficiency of TBK1 causes familial ALS and fronto-temporal dementia. Nat Neurosci. 2015, 18, 631–636. [Google Scholar] [CrossRef]
- Hirano, M.; Angelini, C.; Montagna, P.; Hays, A.P.; Tanji, K.; Mitsumoto, H.; Gordon, P.H.; Naini, A.B.; DiMauro, S.; Rowland, L.P. Amyotrophic lateral sclerosis with ragged-red fibers. Arch Neurol. 2008, 65, 403–406. [Google Scholar] [CrossRef]
- Vijayvergiya, C.; Beal, M.F.; Buck, J.; Manfredi, G. Mutant superoxide dismutase 1 forms aggregates in the brain mitochondrial matrix of amyotrophic lateral sclerosis mice. J Neurosci. 2005, 25, 2463–2470. [Google Scholar] [CrossRef] [PubMed]
- Pasinelli, P.; Belford, M.E.; Lennon, N.; Bacskai, B.J.; Hyman, B.T.; Trotti, D.; Brown RH, Jr. Amyotrophic lateral sclerosis-associated SOD1 mutant proteins bind and aggregate with Bcl-2 in spinal cord mitochondria. Neuron 2004, 43, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Bille, A.; Jónsson, S.Æ.; Akke, M.; Irbäck, A. Local unfolding and aggregation mechanisms of SOD1: a Monte Carlo exploration. J Phys Chem B. 2013, 117, 9194–9202. [Google Scholar] [CrossRef] [PubMed]
- Vande Velde, C.; McDonald, K.K.; Boukhedimi, Y.; McAlonis-Downes, M.; Lobsiger, C.S.; Bel Hadj, S.; Zandona, A.; Julien, J.P.; Shah, S.B.; Cleveland, D.W. Misfolded SOD1 associated with motor neuron mitochondria alters mitochondrial shape and distribution prior to clinical onset. PLoS One 2011, 6, e22031. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, S.; Iwata, M. Mitochondrial alterations in the spinal cord of patients with sporadic amyotrophic lateral sclerosis. J Neuropathol Exp Neurol. 2007, 66, 10–16. [Google Scholar] [CrossRef]
- De Vos, K.J.; Chapman, A.L.; Tennant, M.E.; Manser, C.; Tudor, E.L.; Lau, K.F.; Brownlees, J.; Ackerley, S.; Shaw, P.J.; McLoughlin, D.M.; Shaw, C.E.; Leigh, P.N.; Miller CCJ, Grierson, A. J. Familial amyotrophic lateral sclerosis-linked SOD1 mutants perturb fast axonal transport to reduce axonal mitochondria content. Hum Mol Genet. 2007, 16, 2720–2728. [Google Scholar] [CrossRef]
- He, L.; Chen, L.; Li, L. The TBK1-OPTN Axis Mediates Crosstalk Between Mitophagy and the Innate Immune Response: A Potential Therapeutic Target for Neurodegenerative Diseases. Neurosci Bull. 2017, 33, 354–356. [Google Scholar] [CrossRef]
- Richter, B.; Sliter, D.A.; Herhaus, L.; Stolz, A.; Wang, C.; Beli, P.; Zaffagnini, G.; Wild, P.; Martens, S.; Wagner, S.A.; Youle, R.J.; Dikic, I. Phosphorylation of OPTN by TBK1 enhances its binding to Ub chains and promotes selective autophagy of damaged mitochondria. Proc Natl Acad Sci U S A. 2016, 113, 4039–4044. [Google Scholar] [CrossRef]
- Harding, O.; Evans, C.S.; Ye, J.; Cheung, J.; Maniatis, T.; Holzbaur ELF. ALS- and FTD-associated missense mutations in TBK1 differentially disrupt mitophagy. Proc Natl Acad Sci U S A. 2021, 118, e2025053118. [Google Scholar] [CrossRef]
- Carelli, V.; Ghelli, A.; Bucchi, L.; Montagna, P.; De Negri, A.; Leuzzi, V.; Carducci, C.; Lenaz, G.; Lugaresi, E.; Degli Esposti, M. Biochemical features of mtDNA 14484 (ND6/M64V) point mutation associated with Leber's hereditary optic neuropathy. Ann Neurol. 1999, 45, 320–328. [Google Scholar] [CrossRef] [PubMed]
- Baracca, A.; Solaini, G.; Sgarbi, G.; Lenaz, G.; Baruzzi, A.; Schapira, A.H.; Martinuzzi, A.; Carelli, V. Severe impairment of complex I-driven adenosine triphosphate synthesis in leber hereditary optic neuropathy cybrids. Arch Neurol. 2005, 62, 730–736. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Brain Magnetic Resonance revealed bilateral fronto-parietal atrophy; coronal (a) and axial (b) FLAIR-T2-weighted sequences displayed hyperintensity of the cortico-spinal tracts (arrows).
Figure 1.
Brain Magnetic Resonance revealed bilateral fronto-parietal atrophy; coronal (a) and axial (b) FLAIR-T2-weighted sequences displayed hyperintensity of the cortico-spinal tracts (arrows).
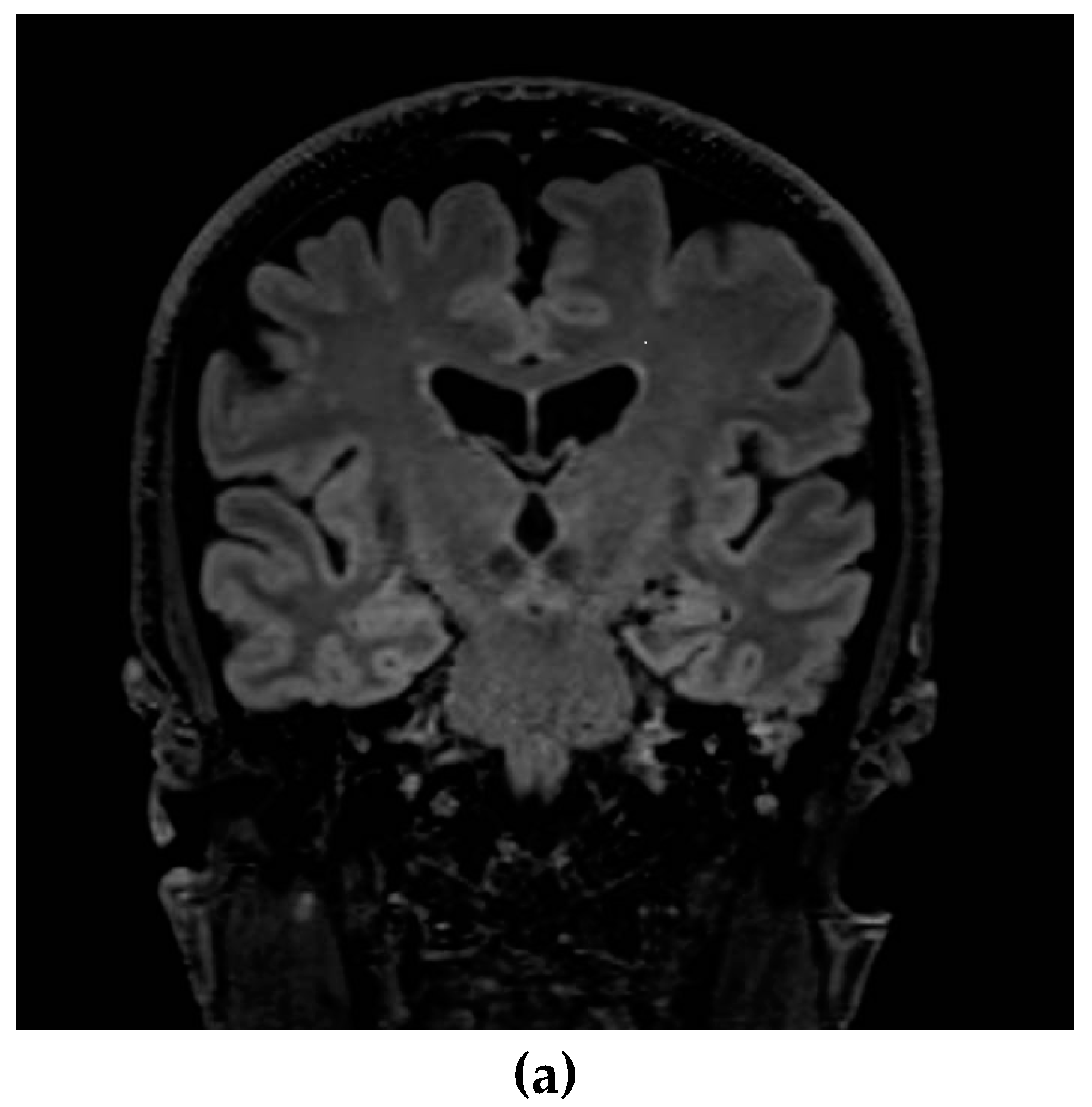
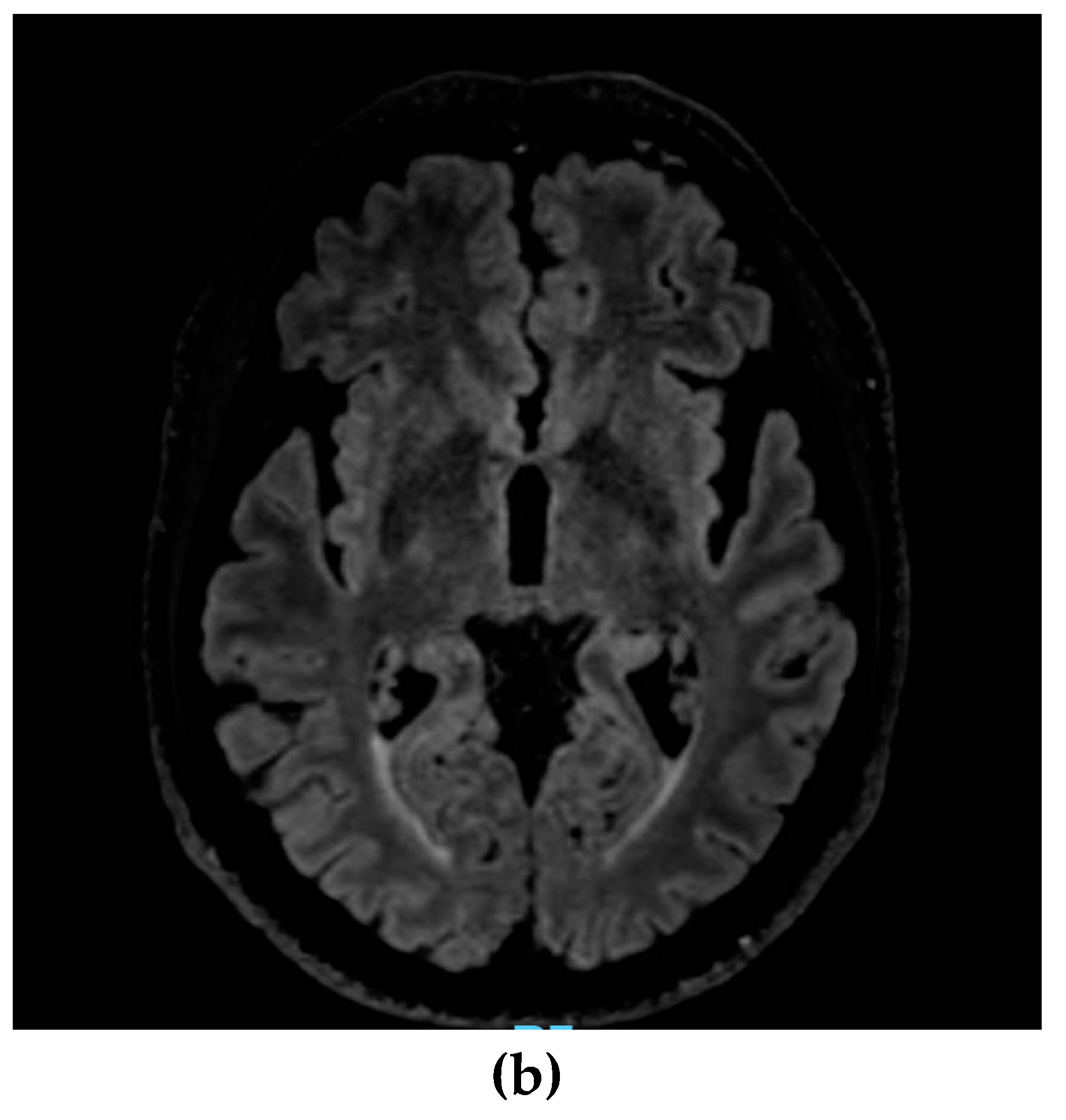
Figure 2.
Hematoxilin Eosin staining (a) showed neurogenic changes with small groups of atrophic fibers (arrows). Cytochrome C Oxidase/Succinate dehydrogenase double staining (b) showed a few fibers displaying subsarcolemmal enhancement (head of arrow) and a single COX negative fiber (arrow).
Figure 2.
Hematoxilin Eosin staining (a) showed neurogenic changes with small groups of atrophic fibers (arrows). Cytochrome C Oxidase/Succinate dehydrogenase double staining (b) showed a few fibers displaying subsarcolemmal enhancement (head of arrow) and a single COX negative fiber (arrow).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



