
Submitted:
19 July 2023
Posted:
21 July 2023
You are already at the latest version
Abstract
Background: Trans-septal endocardial left ventricle lead placement is an alternative technique used capture the left ventricular endocardially but it is use is limited due lack of evidence, practice uptake and clinical trials. we evaluated the efficiency of the procedure, post procedural complication rate, rate of thromboembolic events as well as changes in echocardiographic parameters, brain natriuretic peptide (BNP) level and the New York Heart Association (NYHA) class.
Results: TSLV lead implant is safe, improves ejection fraction, LVEDV, LVESV, LVIDd. Significantly reduces NTproBNP levels and NYHA class. Stroke rate was reported only in one patient (9%), noticeably, this particular patient was on DOAC rather than anti-vitamin K antagonists. In this group, patients, who were on Warfarin , were not reported to have any thrombo-embolic events.
Discussion:
Trans-septal endocardial LV lead implant in patients with a failed CS approach remains a viable alternative however, there is a higher risk of stroke amongst these patients, as well as more procedure related risk of complications compared to conventional CRT.
The data analysis demonstrates that patients undergoing a TSLV lead implant due to a failed trans-venous approach have more advanced heart failure, defined by their higher NYHA class compared to conventional trans-venous CRT implant groups. Their pre TSLV implant, echocardiographic parameters are also worse compared to trans-venous CRT implant group
Keywords:
Cardiac resynchronisation therapy
; trans-septal LV lead
; Heart Failure
; Quality of life
Introduction
Cardiac resynchronisation therapy (CRT) implantation has significantly improved quality of life and reduced overall mortality due to heart failure (1-6). The conventional method of CRT implantation is implanting a left ventricle (LV) lead into a side branch of the coronary sinus tributary to pace the epicardial surface and capture the LV. This is safe, well tolerated with high success rate (7). The rate of failure to place an LV lead has decreased over time. In a large study by Gamble et al., involving 29503 patients, the overall rate of failed LV lead placement was 3.6%, these include inability to cannulate the coronary sinus (CS), unsuitable target vein and phrenic nerve stimulation (8). The extent of myocardial scar and viability could also lead to high capture thresholds or non-response to CRT (9).
Alternative methods largely used in this group of patients is implanting a surgical epicardial LV lead. Although efficient, it requires surgical assessment of the patients and often are deemed to be high risk understandably due to their multiple co-morbidities and majority of the time in NYHA class III-IV, other methods which have been tried are physiological pacing.
Trans-septal endocardial left ventricle lead placement is an alternative technique used capture the left ventricular endocardially but it is use is limited due lack of evidence, practice uptake and clinical trials. There has been a paucity of retrospective studies which evaluate the risk of complications, safety and efficacy of this procedure as well as long term complications. Laszlo et al. studied 44 patients who underwent trans-septal LV endocardial lead implantation with a median of 29 months follow up. Here it was demonstrated that, even though an effective approach, it was associated with a higher rate of thromboembolic cerebrovascular accident (CVA) of 7% compared to general background rate (10, 11). On the other hand, in an another study by Berry et al., a trans septal LV lead implantation was successful in 9 out of ten patients with stable stimulation threshold and no thromboembolic events on appropriate anticoagulation (12).
Neuhoff et al. reported 4 patients with no thrombo-embolic events, haemorrhage or infection and follow up transthoracic echocardiogram showed improvement in left ventricle ejection fraction (LVEF) and overall improvement in their functional status (13).
Since these patients are in heart failure and dependent on device therapy, an alternative approach is considered for those with a failed trans-venous LV lead implant (14).
In this single tertiary centre, retrospective study, we evaluated the efficiency of the procedure, post procedural complication rate, rate of thromboembolic events as well as changes in echocardiographic parameters, brain natriuretic peptide (BNP) level and the New York Heart Association (NYHA) class.
Study design
This was a single tertiary centre retrospective study involving 14 patients from 2008 to 2021 with failed CS approach left ventricle lead that ended up having a trans-septal endocardial lead implant. Three participants were excluded from the study due to incomplete investigations both before and after the procedure.
There were 7 cardiac resynchronisation therapy- defibrillator (CRT-D) and 4 cardiac resynchronisation therapy- pacemaker (CRT-P). 7 patients were in NYHA class IV and 4 in NYHA class III.
This study was part of an audit at Plymouth University NHS Trust, Derriford Hospital, under the registration number: CA_2022-23-283 and CA_2022-23-281 and CA_2022-23-282.
Patient selection and sample size
All 11 participants in this study had their echocardiographic assessment performed by British Society of Echocardiography -accredited physiologists, an echocardiogram before the upgrade and after the upgrade were necessary for the participants to be included in the study, out of 14 patients, 3 were left out of the study due to absence of a repeat echocardiogram post endocardial LV lead implantation. Parameters, such as LVEF by Simpson’s biplane, left ventricle end diastolic volume (LVEDV), left ventricle end systolic volume (LVESV) and left ventricle internal dimension in diastole (LVIDd) were analysed before and after an endocardial LV lead implantation; device interrogations and optimisation were performed by a British Heart Rhythm Society-accredited physiologist, all of the participants reviewed in this study had a pre-upgrade pacemaker/ICD interrogation showing the percentage of RV pacing. Physical notes were analysed in those without electronic records to obtain the necessary information. A post-implant CRT interrogation was performed in all patients showing percentage BiV pacing.
The decision to implant an endocardial LV lead was made by a multi-disciplinary team and the participants had at least one failed attempt to implant a trans-venous LV lead. Failed trans-venous LV lead were; one case due to persistent phrenic nerve stimulation, 3 cases due to high pacing thresholds, one case post LV lead extraction and 6 other cases were, either due to difficulty cannulating the coronary sinus or inability to identify a suitable CS tributary side branch.
All of the participants already had, either a conventional pacemaker or an implantable cardioverter defibrillator (ICD), hence, an endocardial LV lead implantation was classified as an upgrade procedure.
Statistical analysis
Statistical analysis was performed using Microsoft Excel (Microsoft Corp., Redmond, WA, USA), together with the XLSTAT add-on for MS Excel (Addinsoft SARL, Paris, France). The descriptive analysis of the study group was performed with Excel, while normality tests (Anderson–Darling) and complex statistical tests (chi squared, Wilcoxon) were performed using XLSTAT.
Because most of the numerical variables recorded in our study did not have a normal (Gaussian) distribution, the nonparametric Kruskal-Wallis test was primarily used to detect significant differences between the values in the compared data series for patient groups, while Wilcoxon test for paired samples was used to compare pre- and post-procedure values.
Results
Analysis of trans-septal endocardial LV lead (TSLV)
A total of 11 patients were successfully implanted with a TSLV, the sex ratio was 81% in favour of male patients (9 male and 2 female). The median age was (76±9). There were 7 patients (63.64%) with >40% RVP and 4 (36.36%) patients with <40% RVP. Post-upgrade BiV pacing was >90 % in all of the participants. The distribution of patients based on aetiology of cardiomyopathy, medication history and associated comorbidities are listed in “Table 1”.
The mean pre TSLV implant QRS duration was 170±20ms, compared to 114±18ms after upgrade, showing a narrower QRS duration of at least (57±11) ms, which was a statistically significant difference with a P value (<0.0038). The pre TSLV implant LVESV was 160±50 ml and after implant, it was 131±64 ml with a post implant decrease in LVESV of (29.73±40ml); P value of (0.0459) showing significant statistical difference. The pre implant LVIDd measured in 2M-mode was 6.15±0.5 cm compared to 5.64±0.8cm after, showing a decrease in LVIDd of (0.51±0.45cm) with a P value of 0.0095. The pre implant mean LVEDV was 224±63 ml and post implant LVEDV was 185±85 ml, with a median decrease in LVEDV of (38.91±58.46 ml) and P value of 0.0453, showing a statistically significant difference, illustrated in “Figure 1”. The mean LVEF before TSLV was 20±9% and 32±15% after implant, showing an increase in LVEF of (11.91±14.63%), which was statistically significant with a P value of 0.0119, The mean NYHA class before implant was 3.6±0.5 compared to 2.18±0.6 post implant, showing at least a one-grade classification decrease in NYHA class, which was statistically significant with a P value of 0.0049.
Pre TSLV implant NTpro BNP mean level was 2799±2961 compared to post TSLV implant which was 2068 ±2160, with a median reduction of -731.45±1638 post TSLV implant which was statistically significant with a P value of 0.0082, illustrated in “Figure 2”.
5 (45.45%) patients were on direct oral anticoagulants (DOACs) and 6 (53.55%) on Warfarin with a target INR of 2.5-3.5. only one of the 11 patients (9.09%) was admitted with a presumed thromboembolic CVA; this patient was anticoagulated with a DOACs, none of the patients on Warfarin had a documented CVA post TSLV implant.
Analysis of TSLV compared to trans-venous CRT upgrade
Since we demonstrated that TSLV implant improves both clinical and echocardiographic parameters, we then compared these parameters with those who had a trans-venous cardiac resynchronisation therapy (CRT) upgrade either from a conventional pacemaker to CRT-P or an ICD to a CRT-D. 151 (93 CRT-P and 58 CRT-D) patient’s clinical and echocardiographic parameters were analysed to facilitate this comparative analysis. Table 2 and Table 3 show, descriptive analysis of, trans-venous group.
All the groups had statistically significant reduction in QRS duration following an LV lead implant. Mean pre TSLV implant LVESV was greater than trans-venous CRT upgrades (160±50ml compared to 121±33mls in CRT-P upgrade groups and 151±47mls in CRT-D upgrade group) which was statistically significant, however post LV lead implant reduction in LVESV were statistically similar in all the groups with a P value of 0.0584. LVEDV was also greater in TSLV group before implant (224±63mls versus 170±50 in CRT-P upgrade patients and 219±69mls in CRT-D), post LV lead implant reduction in LVEDV was statistically similar in all the groups with a p value of 0.69 showing no significant statistical significance illustrated in “Figure 3”. Mean ejection fraction (EF) before TSLV implant was statistically lower in TSLV group compared to those with a trans-venous CRT upgrade (20±9 % versus 30.5±9.7 in CRT-P group and 23.88±11 in CRT-D group), post LV lead implant increase in EF was similar in all groups. Patients in TSLV group had a greater NYHA class pre TSLV implant (3.64±0.5 versus 2.88±0.55 in CRT-P group and 3.10±0.7 in CRT-D group) which was significant but not statistically significant in NYHA class reduction between the groups post an LV lead implant, illustrated in “Figure 4”.
Discussion
TSLV lead implant is safe, improves ejection fraction, LVEDV, LVESV, LVIDd. Significantly reduces NTproBNP levels and NYHA class. These were also demonstrated in multiple other studies (15-20).
Stroke rate was reported only in one patient (9%), noticeably, this particular patient was on DOAC rather than anti-vitamin K antagonists. In this group, patients, who were on Warfarin , were not reported to have any thrombo-embolic events.
The data analysis demonstrates that patients undergoing a TSLV lead implant due to a failed trans-venous approach have more advanced heart failure, defined by their higher NYHA class compared to conventional trans-venous CRT implant groups. Their pre TSLV implant, echocardiographic parameters are also worse compared to trans-venous CRT implant group. One could assume that, these patients are high risk for a surgical approach to implant an LV lead, both, due to their significance of heart failure as well as poor echocardiographic parameters. Although, multiple studies demonstrate, the overall safety and effectiveness of a surgically placed epicardial LV lead (21-23). In a study by Miller et al., mortality rate amongst patient undergoing surgical LV implant was higher compared to trans-venous CRT implant (24).
On the other hand, conduction system pacing has demonstrated promising outcomes in patients with heart failure. In a study by Barbara-pinchado et al., it was demonstrated that his bundle pacing (HBP) can be alternative to CRT in those patients where trans-venous approach is not feasible (25). In another study by Lustgarten et al., HBP was found to have an equivalent CRT response (26). These go in line with multiple other studies demonstrating that, conduction system pacing is an effective and feasible approach and can have similar outcomes as in CRT (27-31).
Conclusions
Trans-septal endocardial LV lead implant in patients with a failed CS approach remains a viable alternative however, there is a higher risk of stroke amongst these patients, as well as more procedure related risk of complications compared to conventional CRT. TSLV lead implant is safe, improves ejection fraction, LVEDV, LVESV, LVIDd. Significantly reduces NTproBNP levels and NYHA class. It is interesting to look to the future with the emergence of conduction system pacing, as safe and feasible alternative technique due to the fact that, although these patients get extraordinary electrical parameters and post LV lead implant improvement in both, clinical and echocardiographic parameters; high rate of stroke and complexity of device extraction in case of infected device as well as systemic implication, makes it less attractive. This builds a case for ongoing trials comparing conduction system pacing with CRT as a better alternative for this group of patients.
Multidisciplinary approach and patient selection are very important in this group of patients.
Author Contributions
Conceptualization, Arsalan Farhangee and Ion Mindrila; methodology, Arsalan Farhangee, Mark Davies and Ion Minrila.; software, Arsalan Farhangee.; validation, Mark Davies, Ion Mindrila, Mihai Mesina; formal analysis, Arsalan Farhangee, Ion Mindrila, Mihai Mesina; investigation, Arsalan Farhangee.; resources, Arsalan Farhangee.; data curation, Arsalan Farhangee; writing—original draft preparation, Arsalan Farhangee, Mihai Mesina; writing—review and editing, Arsalan Farhangee, Mark Davies and Ion Mindrila.; visualization, Arsalan Farhangee.; supervision, Ion Mindrila.; project administration, Arsalan Farhangee; All authors have read and agreed to the published version of the manuscript.
Funding
The Article Processing Charges were funded by the University of Medicine and Pharmacy of Craiova, Romania.
Institutional Review Board Statement
This was part of a multicentre national audit with the following registration numbers: CA_2022-23-283, CA_2022-23-281 and CA_2022-23-282.
Informed Consent Statement
Patient consent was waived due to making part of a national audit.
Acknowledgments
We are grateful to the contributions made by the physiologist from Derriford Hospital, Lincoln County Hospital and Milton Keynes University Hospital.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| TSLV | Trans septal left ventricle |
| TV | Trans-venous |
| CRT | Cardiac resynchronisation therapy |
| CRTD | Cardiac resynchronisation therapy Defibrillator |
| CRTP | Cardiac resynchronisation therapy Pacemaker |
| PPM | Permanent Pacemaker |
| ICD | implantable cardioverter defibrillator |
| LV | Left ventricle |
| LVSD | Left ventricle systolic dysfunction |
| LBBB | Left bundle branch block |
| HF | Heart Failure |
| CKD | Chronic Kidney disease |
| EF | Ejection fraction |
| LVEF | Left ventricle ejection fraction |
| LVIDd | Left ventricle internal diameter in diastole |
| LVEDV | Left ventricle end diastolic volume |
| LVESV | left ventricle end systolic volume |
| NYHA | New York heart association |
| ESC | European society of cardiology |
| AV | Atrioventricular |
| ARNi | angiotensin receptor-neprilysin inhibitor |
| MRA | Mineral receptor antagonists |
| SGLT-2 | Sodium-glucose transport protein 2 inhibitors |
References
- Moss, A.J.; Hall, W.J.; Cannom, D.S.; Klein, H.; Brown, M.W.; Daubert, J.P.; et al. Cardiac-resynchronization therapy for the prevention of heart-failure events. N Engl J Med 2009, 361, 1329–1338. [Google Scholar] [CrossRef] [PubMed]
- Abraham, W.T.; Fisher, W.G.; Smith, A.L.; Delurgio, D.B.; Leon, A.R.; Loh, E.; et al. Multicenter InSync randomized clinical evaluation. Cardiac resynchronization in chronic heart failure. N Engl J Med 2002, 346, 1845–1853. [Google Scholar] [CrossRef] [PubMed]
- Higgins, S.L.; Hummel, J.D.; Niazi, I.K.; Giudici, M.C.; Worley, S.J.; Saxon, L.A.; et al. Cardiac resynchronization therapy for the treatment of heart failure in patients with intraventricular conduction delay and malignant ventricular tachyarrhythmias. J Am Coll Cardiol 2003, 42, 1454–1459. [Google Scholar] [CrossRef] [PubMed]
- Abraham, W.T.; Young, J.B.; León, A.R.; Adler, S.; Bank, A.J.; Hall, S.A.; et al. Effects of cardiac resynchronization on disease progression in patients with left ventricular systolic dysfunction, an indication for an implantable cardioverter-defibrillator, and mildly symptomatic chronic heart failure. Circulation 2004, 110, 2864–2868. [Google Scholar] [CrossRef] [PubMed]
- Dewhurst, M.J.; Linker, N.J. Current evidence and recommendations for cardiac resynchronization therapy. Arrhythm Electrophysiol Rev 2014, 3, 9–14. [Google Scholar] [CrossRef]
- Kosztin, A.; Vamos, M.; Aradi, D.; Schwertner, W.R.; Kovacs, A.; Nagy, K.V.; et al. De novo implantation vs. upgrade cardiac resynchronization therapy: a systematic review and meta-analysis. Heart Fail Rev 2018, 23, 15–26. [Google Scholar] [CrossRef] [PubMed]
- León, A.R.; Abraham, W.T.; Curtis, A.B.; Daubert, J.P.; Fisher, W.G.; Gurley, J.; Hayes, D.L.; Lieberman, R.; Petersen-Stejskal, S.; Wheelan, K.; MIRACLE Study Program. Safety of transvenous cardiac resynchronization system implantation in patients with chronic heart failure: combined results of over 2, 000 patients from a multicenter study program. J Am Coll Cardiol. 2005, 46, 2348–2356. [Google Scholar] [CrossRef] [PubMed]
- Gamble, J.H.P.; Herring, N.; Ginks, M.; Rajappan, K.; Bashir, Y.; Betts, T.R. Procedural success of left ventricular lead placement for cardiac resynchronization therapy: A meta-analysis. JACC Clin Electrophysiol. 2016, 2, 69–77. [Google Scholar] [CrossRef]
- Ypenburg, C.; Schalij, M.J.; Bleeker, G.B.; Steendijk, P.; Boersma, E.; Dibbets-Schneider, P.; Stokkel, M.P.; van der Wall, E.E.; Bax, J.J. Impact of viability and scar tissue on response to cardiac resynchronization therapy in ischaemic heart failure patients. Eur Heart J. 2007, 28, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Gellér, L.; Salló, Z.; Molnár, L.; Tahin, T.; Özcan, E.E.; Kutyifa, V.; Osztheimer, I.; Szilágyi, S.; Szegedi, N.; Ábrahám, P.; Apor, A.; Nagy, K.V.; Kosztin, A.; Becker, D.; Herczeg, S.; Zima, E.; Merkely, B. Long-term single-centre large volume experience with transseptal endocardial left ventricular lead implantation. Europace. 2019; 21, 1237–1245. [Google Scholar] [CrossRef]
- Rademakers, L.M.; Van Gelder, B.M.; Scheffer, M.G.; Bracke, F.A. Mid-term follow up of thromboembolic complications in left ventricular endocardial cardiac resynchronization therapy. Hear Rhythm. 2014, 11, 609–613. [Google Scholar] [CrossRef] [PubMed]
- van Gelder, B.M.; Scheffer, M.G.; Meijer, A.; Bracke, F.A. Transseptal endocardial left ventricular pacing: an alternative technique for coronary sinus lead placement in cardiac resynchronization therapy. Heart Rhythm. 2007, 4, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Morgan, J.M.; Biffi, M.; Gellér, L.; Leclercq, C.; Ruffa, F.; Tung, S.; et al. ALternate Site Cardiac ResYNChronization (ALSYNC): a prospective and 355 multicentre study of left ventricular endocardial pacing for cardiac resynchronization therapy. Eur Heart J 2016, ehv723. [Google Scholar] [CrossRef]
- Moriña-Vázquez, P.; Roa-Garrido, J.; Fernández-Gómez, J.M.; Venegas-Gamero, J.; Pichardo, R.B.; Carranza, M.H. Direct left ventricular endocardial pacing: An alternative when traditional resynchronization via coronary sinus is not feasible or effective. PACE - Pacing Clin Electrophysiol. 2013, 36, 699–706. [Google Scholar] [CrossRef]
- Patel, M.B.; Worley, S.J. Snare coupling of the pre-pectoral pacing lead delivery catheter to the femoral transseptal apparatus for endocardial cardiac resynchronization therapy: Mid-term results. J Interv Card Electrophysiol. 2013, 36, 209–216. [Google Scholar] [CrossRef]
- Geller L, Molnar L, Szilagyi S., Zima E, Szeplaki G, Osztheimer I, et al. Long term efficacy and safety of transseptal endocardial left ventricular lead implantation after left ventricular lead implantations. Eur Heart J. 2014, 35, P525.
- Garrigue, S.; Jaïs, P.; Espil, G.; Labeque, J.N.; Hocini, M.; Shah, D.C.; et al. Comparison of chronic biventricular pacing between epicardial and 395 endocardial left ventricular stimulation using Doppler tissue imaging in patients with heart failure. Am J Cardiol. 2001, 88, 858–862. [Google Scholar] [CrossRef] [PubMed]
- Scott, P.A.; Yue, A.M.; Watts, E.; Zeb, M.; Roberts, P.R.; Morgan, J.M. Transseptal left ventricular endocardial pacing reduces dispersion of ventricular repolarization. PACE - Pacing Clin Electrophysiol. 2011, 34, 1258–1266. [Google Scholar] [CrossRef]
- Hugo, J.; Gamble, P.; Herring, N.; Ginks, M.; Rajappan, K.; Bashir, Y.; et al. Endocardial left ventricular pacing for cardiac resynchronization: systematic review and meta-analysis. Europace [Internet]. 2017, 1–9. [Google Scholar]
- Kim, H.R.; Lim, K.; Park, S.J.; Park, J.S.; Kim, J.Y.; Chung, S.; Jung, D.S.; Park, K.M.; On, Y.K.; Kim, J.S. Thoracoscopic Implantation of Epicardial Left Ventricular Lead for Cardiac Resynchronization Therapy. J Cardiovasc Dev Dis. 2022, 9, 160. [Google Scholar] [CrossRef]
- Navia, J.L.; Atik, F.A.; Grimm, R.A.; Garcia, M.; Vega, P.R.; Myhre, U.; Starling, R.C.; Wilkoff, B.L.; Martin, D.; Houghtaling, P.L.; Blackstone, E.H.; Cosgrove, D.M. Minimally invasive left ventricular epicardial lead placement: surgical techniques for heart failure resynchronization therapy. Ann Thorac Surg. 2005, 79, 1536–1544; discussion 1536-44. [Google Scholar] [CrossRef] [PubMed]
- Nelson, K.E.; Bates, M.G.; Turley, A.J.; Linker, N.J.; Owens, W.A. Video-assisted thoracoscopic left ventricular pacing in patients with and without previous sternotomy. Ann Thorac Surg. 2013, 95, 907–913. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.L.; Kramer, D.B.; Lewis, E.F.; Koplan, B.; Epstein, L.M.; Tedrow, U. Event-free survival following CRT with surgically implanted LV leads versus standard transvenous approach. Pacing Clin Electrophysiol. 2011, 34, 490–500. [Google Scholar] [CrossRef]
- Barba-Pichardo, R.; Manovel Sanchez, A.; Fernandez-Gomez, J.M.; et al. Ventricular resynchronization therapy by direct His-bundle pacing using an internal cardioverter defibrillator. Europace. 2013, 15, 83–88. [Google Scholar] [CrossRef]
- Lustgarten, D.L.; Crespo, E.M.; Arkhipova-Jenkins, I.; Lobel, R.; Winget, J.; Koehler, J.; Liberman, E.; Sheldon, T. His-bundle pacing versus biventricular pacing in cardiac resynchronization therapy patients: A crossover design comparison. Heart Rhythm. 2015, 12, 1548–1557. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Su, L.; Wu, S.; et al. Long-term outcomes of His bundle pacing in patients with heart failure with left bundle branch block. Heart. 2019, 105, 137–143. [Google Scholar] [CrossRef]
- Vijayaraman, P.; Subzposh, F.A.; Naperkowski, A.; et al. Prospective evaluation of feasibility, electrophysiologic and echocardiographic characteristics of left bundle branch area pacing. Heart Rhythm. 2019, 16, 1774–1782. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Su, L.; Vijayaraman, P.; et al. Left bundle branch pacing for cardiac resynchronization therapy: nonrandomized on-treatment comparison with His bundle pacing and biventricular pacing. Can J Cardiol. 2021, 37, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Vijayaraman, P.; Ponnusamy, S.S.; Cano, O.; et al. Left bundle branch pacing for cardiac resynchronization therapy: results from International LBBP Collaborative Study Group. JACC Clin Electrophysiol. 2021, 7, 135–147. [Google Scholar] [CrossRef]
- Vijayaraman, P.; Herweg, B.; Ellenbogen, K.A.; et al. His-optimized cardiac resynchronization therapy to maximize electrical resynchronization. Circ Arrhythm Electrophysiol. 2019, 12, e006934. [Google Scholar] [CrossRef]
Figure 1.
LVESV, LVEDV and LVIDd, significantly improved post TSLV implant with a p value of <0.05.
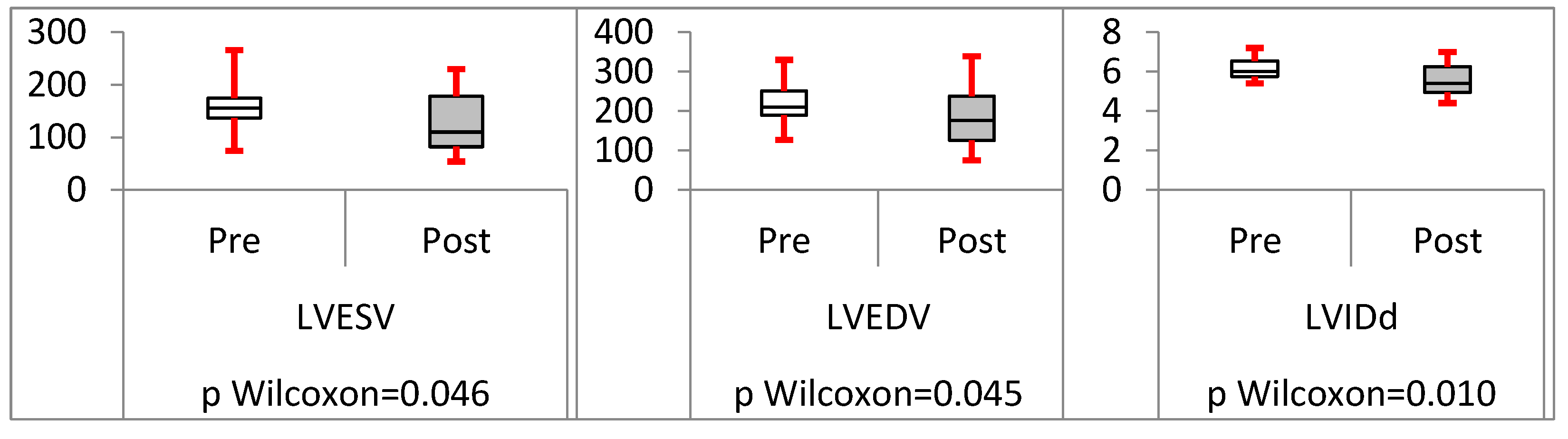
Figure 2.
NYHA class, ProBNP and EF improved significantly following TSLV implant, p value < 0.05 amongst all.
Figure 2.
NYHA class, ProBNP and EF improved significantly following TSLV implant, p value < 0.05 amongst all.
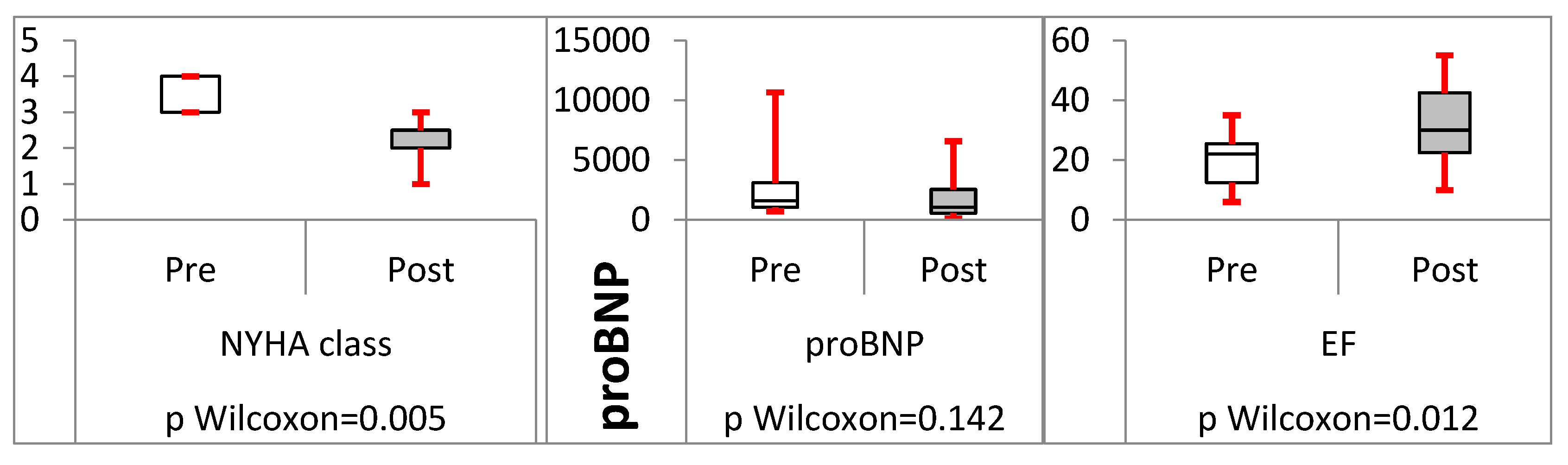
Figure 3.
LVEDV and LVESV significantly reduced post LV lead implant; this was statistically significant in all three groups. However, the degree of significance, comparing the groups were not statistically significant, proving that TSLV is equally beneficial as a conventional upgrade.
Figure 3.
LVEDV and LVESV significantly reduced post LV lead implant; this was statistically significant in all three groups. However, the degree of significance, comparing the groups were not statistically significant, proving that TSLV is equally beneficial as a conventional upgrade.
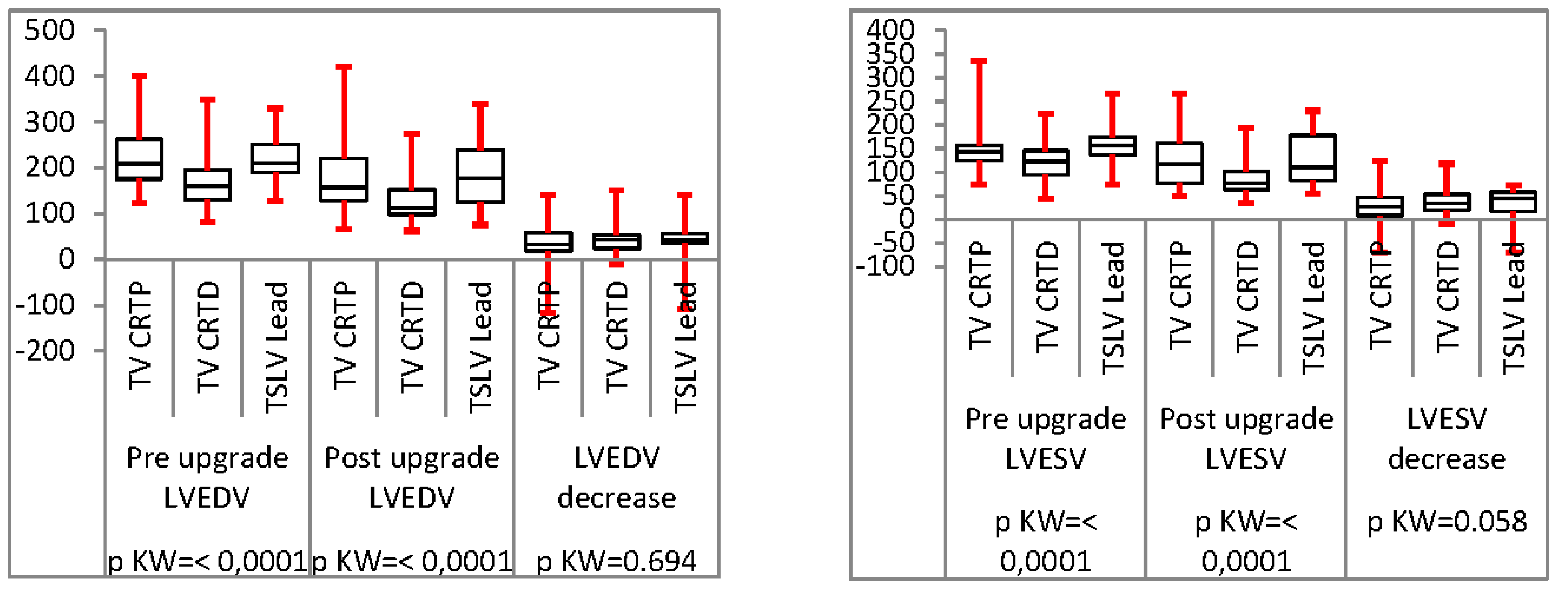
Figure 4.
NYHA class and EF, both improved, significantly in all three categories. Similar to other parameters, the change in NYHA and EF were not significantly different between the groups, again, suggesting that, TSLV lead implantation is equally beneficial as in conventional upgrades.
Figure 4.
NYHA class and EF, both improved, significantly in all three categories. Similar to other parameters, the change in NYHA and EF were not significantly different between the groups, again, suggesting that, TSLV lead implantation is equally beneficial as in conventional upgrades.
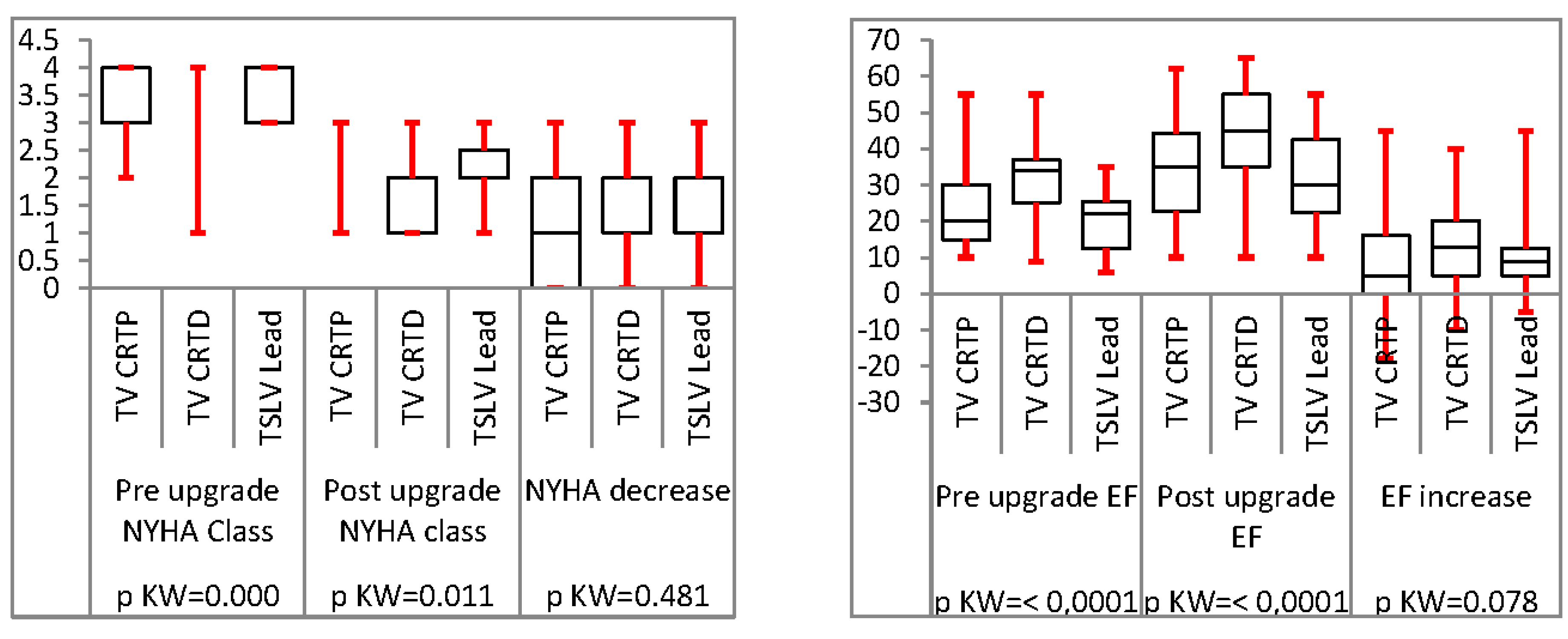

Table 1.
Description of the categorical variables recorded for TSLV group.
| Demographics | |
| 1.Male | 9 (81%) |
| 2.Female | 2 (18%) |
| Underlying Rhythm | |
| 1.Sinus | 8(72.7 %) |
| 2.Atrial arrhythmia | 3 (27.3 %) |
| Age | 76 ± 9 years old |
| Aetiology | |
| 1.Ischaemic cardiomyopathy | 8(72.7 %) |
| 2.Non-ischaemic cardiomyopathy | 3 (27.3 %) |
| 3.Inherited Cardiac Conditions | 1 (9%) |
| 4.Valvular heart disease | 2 (18%) |
| Medication History | |
| 1.Beta-Blockers | 11 (100%) |
| 2.Mineral receptor antagonists (MRA) | 10 (90.9%) |
| 3.Angiotensin receptor-neprilysin Inhibitors ( ARNi) | 7 (63.4%) |
| 4.Sodium-glucose transport protein 2 inhibitors ( SGLT-2) | 7 (63.4%) |
| Comorbidities | |
| 1.Diabetes | 5 (45.4%) |
| 2.CKD stage | |
| 2.1: CKD Stage II | 2(27.7%) |
| 2.2: CKD stage IIIa | 4 (36.36%) |
| 2.3: CKD stage IIIb | 2(18.18%) |
| 2.4 CKD stage IV | 2 (18.18%) |
| 2.5 CKD Stage V | - |
| 3.Hypertension | 11 (100%) |
Table 2.
Description of the categorical variables recorded for recorded for the CRT-P group.
| Dermographics | |
| 3.Male | 64 (69%) |
| 4.Female | 29 (31%) |
| Underlying Ryhthm | |
| 3.Sinus | 62 (66%) |
| 4.Atrial arryhthmia | 31 (34%) |
| Age | 82±10 years old |
| Aetiology | |
| 5.Ischaemic cardiomyopathy | 35 (37%) |
| 6.Non-ischaemic cardiomyopathy | 56 (60%) |
| 7.Inherited Cardiac Conditions | 5 (5.38%) |
| 8.Valvular heart disease | 14 (15%) |
| Medication History | |
| 5.Beta-Blockers | 93 (100%) |
| 6.Mineral receptor antagonists (MRA) | 79 (85%) |
| 7.Angiotensin receptor-neprilysin Inhibitors ( ARNi) | 46 (49.4%) |
| 8.Sodium-glucose transport protein 2 inhibitors ( SGLT-2) | 43 (46%) |
| Comorbidities | |
| 4.Diabetes | 33 (35.4%) |
| 5. CKD stage | |
| 2.1: CKD Stage II | 42 (45.16%) |
| 2.2: CKD stage IIIa | 34 (36.5%) |
| 2.3: CKD stage IIIb | 4 (4.3%) |
| 2.4 CKD stage IV | 6 (6.45%) |
| 2.5 CKD Stage V | - |
| 6.Hypertension | 83 (89.5%) |
Table 3.
Description of the categorical variables the CRT-D group.
| Dermographics | |
| 5.Male | 42 (73%) |
| 6.Female | 16 (27%) |
| Underlying Ryhthm | |
| 5.Sinus | 42 (73%) |
| 6.Atrial arryhthmia | 16 (33%) |
| Age | 76±10 years old |
| Aetiology | |
| 9.Ischaemic cardiomyopathy | 42 (72.4%) |
| 10.Non-ischaemic cardiomyopathy | 11 (18.9%) |
| 11.Inherited Cardiac Conditions | 9 (15.5%) |
| 12.Valvular heart disease | 3 (5.17%) |
| Medication History | |
| 9.Beta-Blockers | 58 (100%) |
| 10.Mineral receptor antagonists (MRA) | 44 (75.8%) |
| 11.Angiotensin receptor-neprilysin Inhibitors ( ARNi) | 36 (62%) |
| 12.Sodium-glucose transport protein 2 inhibitors ( SGLT-2) | 33 (57%) |
| Comorbidities | |
| 7.Diabetes | 29 (50%) |
| 8.CKD stage | |
| 2.1: CKD Stage II | 23 (39.6%) |
| 2.2: CKD stage IIIa | 19 (32.7%) |
| 2.3: CKD stage IIIb | 8 (13.8%) |
| 2.4 CKD stage IV | 6 (10.34%) |
| 2.5 CKD Stage V | - |
| 9.Hypertension | 49 (84.5%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



