Submitted:
19 July 2023
Posted:
19 July 2023
Read the latest preprint version here
Abstract
Data show that preschoolers consume few vegetables, fruits, whole grains, and nuts. We investigated whether a properly planned kindergarten menu can contribute to optimized daily intake of healthy foods. In this cross-sectional experimental study, we designed a 5-day prototype kindergarten menu with consistently followed dietary guidelines and randomly divided six invited kindergartens into a prototype group that received the prototype menu (PG, n=4) and a control group that used their regular menu (CG, n=2). From the participating kindergartens, we invited healthy 5-6-year-old children to participate. Outside of kindergarten, participants ate as usual. All completed a 7-day dietary record of foods consumed inside and outside of kindergarten. We used the Dietary Assessment Tool OPEN to analyze the average daily intake of seven food groups and compare it to the dietary guidelines. Fifty-seven participants completed the study, 40 from PG and 17 from CG. The average daily intake of vegetables (54% vs. 28%), whole grains (100% vs. 47%), and nuts (104% vs. 4%) was significantly higher (p<0.05) in participants from PG compared with guideline recommendations than in participants from CG. Average daily intake of fruits, meats, dairy products, and refined grains did not differ significantly between study groups. Only kindergarten diet made a significant contribution, as intake outside of kindergarten did not show significant differences. The study demonstrates the importance of a well-planned menu in kindergartens and can serve as a basis for future interventions aimed at improving the nutritional environment in childcare facilities.
Keywords:
child nutrition
; dietary record
; food groups
; food intake
; recommendations
; dietary guidelines
; kindergarten
1. Introduction
According to the most recent Global Burden of Disease study [1], one in five premature deaths worldwide can be attributed to unhealthy diets. The relationship between nutrients, foods, and dietary patterns has important implications, particularly for the prevention and development of chronic non-communicable diseases (NCDs) such as cardiovascular disease, cancer, and diabetes [2,3]. The preschool years are a time of intense growth and development and a critical period for the development of lifelong eating habits that can help reduce the burden of NCDs later in life [4]. Although the home environment is a key factor in shaping eating habits [5], more than 80% of preschool children in high-income countries are enrolled in pre-primary education [6,7], where they may spend up to 251 days/year and up to 9 hours/day [7]. During these hours, at least three meals per day (breakfast, lunch, and snack) and often an additional snack, are consumed, which should meet more than 60% of children's daily nutritional and energy needs. This high figure suggests that meals in kindergartens can influence children's health, either to their advantage or disadvantage.
In the last decade, many European countries have implemented various measures to improve food environment in kindergartens and schools [8]. However, the recent report of EFSA Comprehensive European Food Consumption Database [9] shows, that European children consume very low amounts of vegetables and nuts, while fruit intake is slightly better, but still too low. Nutrition in Slovenian kindergartens is well organized, as all children have access to the high-quality food, regardless of their socioeconomic status. Nevertheless, a Slovenian survey shows that only 30% of toddlers eat vegetables daily, 60% eat fruit and 59% of Slovenian toddlers do not eat nuts at all [10].
Most kindergartens in Slovenia are municipal (public) and provide three to four meals daily (breakfast, lunch and 1-2 snacks). The menus are prepared by a qualified staff member who is obliged to follow the national Guidelines for Healthy Eating in Educational Institutions (Guidelines) [11]. All meals are cooked and prepared in kitchens of the kindergartens or, to a small percentage, supplied by external food providers. Children in groups of up to 22 take all meals in classrooms with one to two teachers. Guidelines are well established, but allow for some simplifications, most notably reflected in inadequate supply of vegetables, whole grains and nuts [12]. A low supply of whole grain products, fruits and vegetables in kindergarten diets is also reported in several other studies [13,14,15], and nuts are rarely mentioned, despite the positive health effects and the known contribution of inadequate intake of the above food groups to the economic burden [16,17,18,19].
Some studies have described the contribution of kindergarten nutrition to a daily intake of food groups in children [14,15,20,21], but, to our knowledge, this is the first study to compare the contribution of kindergarten menus, within the same country, with same mandatory Guidelines, to the recommended daily intake of selected food groups in children. Our objective was to determine whether a properly planned kindergarten menu can contribute to a more adequate daily intake of healthy food groups and, consequently, to a more adequate nutrient intake in children. Therefore, our study had three main objectives: 1) to create a prototype 5-day kindergarten menu in strict adherence to the Guidelines and evaluate the average supply of foods from seven food groups (fruits, vegetables, whole grains, refined grains and potatoes, nuts, meat and meat substitutes and milk and dairy products) compared to the supply of a regular (simplified) 5-day kindergarten menus. 2) Comparison of the contribution of the prototype menu to the daily intake of the above food groups among participants in the prototype group (PG) with the contribution of the regular (control) menu to the daily intake of food groups among participants in the control group (CG). 3) To compare the food intake of participants in both research groups on weekdays and the weekend, with the Recommended Daily Food Intakes (RDFI) in the Guidelines [11].
We hypothesized that the prototype kindergarten menu would significantly contribute to a more adequate daily intake of vegetables, fruits, whole grains, and nuts with respect to the RDFI compared with regular kindergarten menus. The second hypothesis states that food group intakes among participants of PG and CG would be more consistent with the RDFI on weekdays than on the weekend.
2. Materials and Methods
2.1. Study design
Our cross-sectional experimental study of the contribution of kindergarten nutrition to the daily intake of seven food groups, with emphasis on vegetables, fruits, whole grains, and nuts, in 5-6-year-old children was part of a larger study registered at ClinicalTrials.gov (NCT04252105). Ethical approval was granted by the Medical Ethics Committee of the Republic of Slovenia (No. 0120-66/2019/8). Two terms are used in this study: Daily menu and daily meals. The daily menu contains a list of foods and dishes to be prepared daily for each meal. Daily meals include all individual foods and dishes in the menu in the quantities (g) actually offered to a child per kindergarten day.
2.2. Participants and Settings
In order to avoid the bias of the environment in which the food was prepared and served, 6 kindergartens from two Slovenian regions were invited to participate in the study. Prior to participation in the study, written consent was obtained from the kindergarten directors. After approval, the invited kindergartens were randomly divided into two groups: the prototype group (PG), which included two kindergartens from each region (n=4), and the control group (CG), which included one kindergarten from each region (n=2). Randomization was performed in Excel using the RANDBETWEEN function to select the control kindergarten in each region. The VLOOKUP function was used to determine the name of the randomized kindergarten. PG was given a 5-day prototype menu plan (Thursday to Wednesday, no weekends) (Supplementary Table S1), whereas CG used menus from the same period of the previous year to avoid bias caused by kindergartens knowing about their participation in the study (Supplementary Tables S2 and S3). All menus were designed in accordance with the Guidelines [11], with the only difference being that the prototype menus strictly followed the detailed recommendations, whereas the regular menus followed only the general recommendations of the Guidelines. Briefly, the Guidelines specify in detailed instructions the exact amounts of each food group that should be offered in the kindergarten diet for children, e.g., at age 4-6 years, 220 g of vegetables, 150 g of fruits, 86 g of whole grains, 86 g of refined grains, 8 g of nuts, etc. (Table 2). On the other hand, the general recommendation states that fresh fruits and/or vegetables, as many whole grains as possible, occasional nuts, etc. should be offered at every meal.
In each kindergarten, two classrooms with children aged 5-6 years (n=40-44) were invited to participate in the study. The participation criteria were as follows: a healthy child aged 5-6 years, who must have participated in all meals in the kindergarten (breakfast, lunch, two snacks) during the period of 5 days (study duration), while gender was not a factor. The exclusion criteria were: all food allergies and chronic diseases. During the initial meetings with parents (from August to the end of September 2019), we explained the purpose of the study and obtained written informed consent from parents. The study was planned to take place between the end of February 2020 and the end of April 2020.
2.3. Anthropometric measurements
To avoid bias due to a possibly individually higher food requirement, we needed data on the body weight and height of all participants. These were collected from participants' pediatricians who performed a regular medical examination between March and June 2020, before school enrollment. Height was measured to the nearest 100 millimeters using a stadiometer, and body weight was measured to the nearest 100 grams using an electronic scale. Participants wore light underwear and no shoes. BMI was calculated, and weight status was defined using the International Working Group on Obesity–sex- and age-specific cut-offs for children [22].
2.4. Assessment of food groups offered in kindergarten menus/meals
We obtained weighed recipes (n=129) from all six kindergartens with portion sizes per child and brands of all foods and beverages used to prepare daily kindergarten meals. We entered all recipes obtained into the OPEN dietary assessment tool [23], and the dishes were classified into seven food groups (milk and dairy products, meat and substitutes, fruits, vegetables, nuts, whole grains, and refined foods and potatoes). It is currently not possible to divide starchy foods into whole grains and refined using the tool OPEN, so the classification of starchy foods was done manually. Foods containing cereals were classified as whole grain if they contained at least 27 g of whole grain per 100 g of product or more than 6 g of dietary fiber /100 g [24]. Potatoes were classified as refined foods due to their low dietary fiber content (≤ 6 g) [25]. Legumes were not treated separately; they were classified as vegetables. In addition, we treated nuts separately in our study, mainly because of their very low intake in children [10] and their beneficial effects on health [18]. Food groups with high fat or sugar content were not the subject of this part of the study. The classification of mixed dishes from kindergartens into food groups is shown in Supplementary Table S4.
2.4. Dietary intake in kindergartens
Kindergarten teachers received detailed verbal and written instructions from a trained dietitian on how to complete the 5-day dietary record during the study. The design of dietary record followed EFSA recommended guidelines [26]. Each teacher received printed, 5-day close-ended forms with all foods included on the menu and a digital household scale to weigh the amount of food served and the amount of leftovers after each meal. Before the official start of the study, we performed a trial recording to rule out possible dilemmas. A total of 5 consecutive daily meals (from Thursday to Wednesday, excluding weekends) were observed in 12 classrooms in 6 kindergartens. Teachers recorded only beverages consumed as part of the meal. Beverages (water and unsweetened tea) consumed by participants outside of meals were not included in our study. Participants were allowed to eat as much as they wanted; they were neither restricted nor forced to eat certain foods.
2.5. Dietary intake outside kindergartens
Participants' parents were asked to report food intake outside of kindergarten, that is, on the same days as recorded by kindergarten teachers, and on weekends, using the weighing technique or the estimated food intake technique. They were given 7 consecutive days of preprinted, open-ended daily forms on which dietary record was organized according to the usual meal plan-breakfast, snack, lunch, snack, dinner, and space for additional snacks. It also contained sufficient space to record product (brand) names, ingredients, and amounts in grams. We included detailed written instructions. In addition, parents were given a national picture book with household measures to determine the amount of food intake (https://nijz.si/publikacije/slikovno-gradivo-s-prikazom-velikosti-porcij/), which was developed for the needs of the EU Menu Study and prepared according to the guidelines of PANCAKE [27]. The picture book contains 46 different foods or simple recipes presented with a series of pictures. Each food contains six different portion sizes that were used to evaluate not only the food pictured but also other foods with similar density, size, and shape. We encouraged parents to be as accurate as possible and to write down foods and beverages immediately after children consumed them.
2.6. Dietary intake data processing
After completion of the study, we entered all data from a 7-day dietary record for each participant into the OPEN dietary assessment tool [23]. Dietary records were reviewed for incomplete or conflicting information, and the dietitian obtained any missing data from parents, teachers, or cooks by telephone within a week of study completion. Final data on the amount of the seven food groups consumed by each participant (in grams) were estimated using OPEN and, in the case of whole grains, manually by the dietitian, who reviewed the declarations and recipes of all starchy foods and mixed kindergarten dishes. Energy and macronutrient intake data (total fat, protein, carbohydrate, dietary fiber, and sodium) were also estimated using OPEN. All data collected were classified at either PG or CG, and the mean values of each variable were compared - with respect to both groups and with respect to RDFI.
2.6. Statistical methods
We calculated descriptive statistics, including means and standard deviations for all measurements. The Welch t-test was used to compare several outcome measures between PG and CG (amount of food groups served in kindergartens, food groups intake in kindergartens, food groups intake in kindergartens during the week and on weekend, and leftovers-difference between food served and consumed in kindergartens). In addition, the total amount of food group intake per weekday and weekend was determined, comparing weekday and weekend intake within a group and between the two groups relative to the RDFI. We tested the hypotheses for normal distribution by plotting each parameter with histograms, and it was found that the distribution was not always normal. Nevertheless, we used the Welch t-test, as the most appropriate to test the hypothesis of equal means even when the distribution is not normal, the variance is different, and the sample size is relatively small [29]. Analyses were performed separately for the different food groups. We used the Bonferroni correction for multiple comparisons. We performed all analyses using R version 4.0.2(29), with the statistical significance level set at 0.05.
3. Results
3.1. Participants and settings
We obtained 94 written informed consents from parents, but because of the COVID -19 epidemic, a total of 57 healthy participants completed the study (61% response rate), whereas other participants (n=37) did not return to kindergartens and were excluded from the study. For the same reason, the study was completed in only one kindergarten in March 2020, while it was conducted in the other five kindergartens in May and June 2020. It was not possible to extend the study further because participants entered elementary school immediately after summer holiday in July and August. Figure 1 illustrates kindergarten enrollment, randomization into PG and CG, the number of participants from each kindergarten, participants lost to follow-up, and the number of participants who completed the study.
3.2. Anthropometric measurements
All participants were Caucasian, and the mean values in the PG and CG groups were as follows: Body height 118.1±4.7 cm vs. 117.8±3.4 cm, body weight 22.2±3.6 kg vs. 21.5±3.7 kg, and BMI 15.9±1.8 vs. 16.4±2.6 kg/m2, all p˃0.05. Considering the nonsignificant differences in all anthropometric measurements, we conclude that participants in the two study groups have similar quantitative dietary intake requirements.
3.3. Food groups offered in kindergartens
Thirty daily meals were analyzed (20 according to the prototype 5-day menu and 10 according to the regular 5-day menu), and all foods and composite dishes (e.g., risottos, stews, pastas, soups) were classified into seven food groups (Supplementary Table S4). The proportion of vegetables in composite dishes obtained from weighed recipes from PG ranged from 7-74%, with the largest range for tuna in tomato sauce (7-49%), followed by vegetable soups (13-45%). The proportion of vegetables in composite dishes ranged from 12-70% at CG. Fruits were mostly offered in raw form, while vegetables were offered in raw and cooked forms. Different amounts of the food groups used in the same dishes of the prototype menu were also found in most other composite dishes. Figure 2 shows that the offer in PG kindergartens is more in line with the Recommended Daily Food Offer (RDFO) than the offer in CG kindergartens. In fact, it is recommended that the supply be consistent with the recommended daily food intake. The consistency in the design of the prototype menu contributed to a more appropriate relationship between the amounts of food groups offered and the achievement of the RDFO in the PG kindergarten menu. In contrast, the high proportion of fruit, refined foods, and potatoes on the CG kindergarten menus already met the RDFO, which prevented additional offerings of vegetables and whole grains. This should be considered when planning kindergarten menus in the future and the ratio optimized in favor of vegetables and whole grains.
Significantly higher (p<0.05) average daily amounts of vegetables (188 vs. 103g), whole grains (137 vs. 54g), and nuts (14 vs. 0g) were offered in PG kindergartens compared to CG kindergartens, while higher amounts of refined foods and potatoes (74 vs. 169g) and fruits (143 vs. 198g) were offered in CG kindergartens. While PG meals on average contained an adequate daily quantity of nuts (14g), CG menu did not include nuts. The availability of milk and dairy products as well as meat and meat substitutes were similar in PG and CG kindergartens. Since most children in Slovenia spend 9 hours per day in kindergarten, according to the Guidelines, 75% of daily energy and nutrient needs should be covered by the daily kindergarten menu. All quantitative offerings of food groups in PG and CG kindergartens compared to the recommendations of the guidelines are shown in Table 1.
3.4. Energy, macronutrient and sodium content in kindergarten meals
Table 2 shows that prototype kindergarten meals had a significantly (p<0.05) higher and more adequate energy, total fat and dietary fiber content than regular kindergarten meals, while there was no significant difference between protein and carbohydrates content. Considering the reference values set in Guidelines [11] for energy and nutrient intake, kindergarten meals provided participants from PG compared with those from CG with an average of 72% and 57% of the Dietary Reference Intake (DRI) for energy. Meals from PG kindergartens contained an adequate amount of total fat (72% of mean DRI value), while meals from CG kindergartens did not meet the minimum DRI value for kindergarten offer (64%). The protein content was adequate in all kindergarten meals, while the carbohydrate content was slightly too low in meals from PG (74% DRI) and even lower in meals from CG (66% DRI). The content of dietary fibre was adequate in all kindergarten meals, however meals from PG contained significantly more. The analysis also showed that the kindergarten meals from PG contained 5 g of salt and the kindergarten meals from CG contained 4 g of salt, which was above the limit for maximum allowable daily intake for all meals; these findings require immediate action.
3.5. Food intakes in kindergartens and outside kindergartens on weekdays in PG and CG participants
PG and CG participants’ 7-day food intakes (in grams) in kindergartens and outside kindergartens on weekdays and the weekend are shown in Table 1. Mean daily intake of food groups on weekdays among participants from PG compared with intake on weekdays among participants from CG was significantly higher (p<0.05) among participants from PG for each comparison: 56% vs. 31% RDFI for vegetables, 100% vs. 47% RDFI for whole grains, and 100% vs. 0% RDFI for nuts. Fruit consumption did not differ significantly among days of the week, reaching 100% RDFI among participants from PG and 108% RDFI among participants from CG. Daily intake of refined grains and potatoes was significantly higher (p<0.05) in participants from CG and averaged 171% RDFI, while intake was 111% RDFI in participants from PG. The results in Table 1 clearly show that only the kindergarten diet contributed to the significant differences in total weekday intakes of food groups, as intakes outside kindergartens did not differ significantly.
Comparison between intakes of food groups inside and outside kindergarten (Figure 2) shows that in kindergartens, PG participants on average consumed 80% of their total daily intake of vegetables, 92% of whole grains and 96% of nuts, while CG participants on average consumed, in kindergartens 63% of their total daily intake of vegetables and 91% of whole grains. In comparison with PG participants, CG participants consumed in kindergartens significantly higher amounts of refined foods and potatoes (57% vs 103% of RDFI) and higher, but not significantly higher, amounts of fruit (56% vs 67% RDFI). There were no significant differences between PG and CG participants regarding the intake of milk and dairy products or meat and substitutes in kindergartens, although daily intake was higher in PG participants (72% vs 55%, and 54% vs 45% of RDFI). There were also no significant differences in the amount of food leftover at kindergarten meals between participants from PG and CG (Supplementary Table S5).
Our results reveal that an adequate offer of healthy food groups in the kindergarten meals is very important, since the intake of these foods (vegetables, whole grain foods, nuts) outside the kindergarten is very low.
3.6. Weekend food intake among participants of PG and CG and comparison with weekday intake
During the weekend, intakes of all food groups did not differ significantly between participants from PG and CG and were inadequate for all food groups except meat and its substitutes, and refined foods and potatoes (Table 1). The greatest deviation from the RDFI was found in the intake of vegetables, whole grains, and nuts in both study groups, as their average daily intake did not even reach 20%. The average intake of milk and dairy products and fruit was slightly more adequate, corresponding to 91% and 77% of the RDFI, respectively, in participants from PG and 97% and 66% of the RDFI, respectively, in participants from CG.
A comparison of weekday and weekend intakes showed that participants from PG consumed a significantly higher (p<0.05) and at the same time more adequate amount of vegetables, whole grains, and nuts during the week, which was fully covered by the kindergarten meals. There was no significant difference between intakes of other food groups among participants from PG.
Although the total intake of whole grain products was low during the week among participants of CG, it was still significantly higher than the intake during the weekend (43% vs. 11% of RDFI), to which the kindergarten meals contributed. Average intakes of all other food groups among CG participants were not significantly different when comparing weekdays to weekends.
4. Discussion
This cross-sectional experimental study is, to the best of our knowledge, the first study that comparing the contribution of the prototype and regular 5-day kindergarten menu in the same country with obligatory national dietary Guidelines, to average daily intake of food groups in 5-6-year-old participants.
We confirmed our hypothesis that kindergarten menus designed by strictly following nutritional guidelines can significantly contribute to a more adequate daily intake of vegetables, fruits whole grains and nuts in PG participants during weekdays. Results also confirmed our second hypothesis that compared to the nutrition provided outside kindergartens, kindergarten nutrition in both research groups contributed to a more optimal intake of healthy food groups; however, the contribution of the prototype menu was superior. Despite the fact that Slovenian educational institutions are obligated to prepare meals in accordance with national Guidelines, our previous study revealed that kindergarten meals can significantly differ, both in terms of offered food groups as well in terms of the content of macronutrients, minerals and antioxidants [31].
There are only few studies examining the daily intake of food groups and/or nutrients in preschool children (under 6 years of age), some of them examining the contribution of daily nutrition inside and outside kindergartens [14,15,32], others only individual meals, either at home or in kindergartens or at both places [21,33,34,35]. They all report similar outcomes, namely that organized kindergarten nutrition is on average of higher quality than nutrition outside kindergartens, which was also confirmed in our study.
Since the main goal of our study was to clarify the contribution of kindergarten nutrition to daily nutrition in participants, we focused mainly on the offer and intake of food groups in kindergartens. All menus in PG and CG kindergartens were planned in accordance with the Guidelines, which was reflected in the similar offer of all main food groups, including total offer of combined fruit and vegetables groups (331 g vs. 301 g) and combined whole grains and refined grains plus potatoes (211 vs. 223 g). However, there were significant differences in the ratio of offered vegetables and fruits, whole grains and refined grains with potatoes and offered nuts on the PG vs CG menus (Table 1), mainly due to the greater diversity of offered foods. Namely, PG menu contained on average 14 different dishes/day, while CG menu comprised on average 10 dishes/day. The more diverse offer in PG was reflected in a significantly higher intake of vegetables, whole grains and nuts in PG kindergarten participants, corroborating the results of a recent meta-analysis which reports that food intake can be increased in the presence of variety [36]. The results of our study are also consistent with the findings of Roe et al. [37] that children eat more vegetables when offered a variety of different types of familiar vegetables compared to being offered a single vegetable snack. A recent study on portion sizes of vegetables and fruits shows that serving larger portions results in increased daily consumption of vegetables and fruits in children [38], however, these foods were also wasted in bigger amounts. This was not confirmed in our study, as the amount of waste in PG kindergartens was not significantly higher than in CG kindergartens (Supplementary Table S5), as prototype menu included dishes that children were familiar with and which comprised more vegetables, whole grains and nuts. The effectiveness of incorporating vegetables into multiple main dishes as strategies to increase vegetables intake was also confirmed in some other studies [39].
Although the weekdays intake of vegetables was not adequate even in PG participants, their average daily weekday’s intake was significantly more optimal than average weekend intakes and weekdays intakes in CG participants whom were offered too low amount of vegetables in kindergarten. Low amounts of vegetables contained in daily kindergarten meals, only around 20% of RDFI, are also reported by some other studies from Finland [15] and the US [14,38].
The prototype kindergarten menu also contributed to a more adequate daily intake of whole grains on weekdays in PG participants, while the intake of whole grains in CG participants was low during the weekdays, but still significantly higher than during the weekends. Our results strongly encourage a greater supply of whole grains in kindergartens as we revealed that replacing refined grains with whole grains can contribute to the recommended daily intake, considering that intake outside kindergarten is low. Additionally, as a result of significantly higher amount of offered vegetables and whole grains in PG kindergarten meals it is necessary to highlighted the significantly higher content of dietary fiber in meals, which was also confirmed by chemical analysis our kindergarten meals [31]. Providing a sufficient amount of dietary fiber is very important, as the recent study states that a higher fiber intake is associated with better glucose tolerance levels and lower cardiovascular risk in children [40]. Unfortunately, the OPEN analysis and also the chemical analysis of our kindergarten meals [31] showed, that too much sodium/salt is used in kindergarten food preparation, which calls for immediate action, especially in terms of educating the kitchen staff.
Participants in both study groups during weekdays were consumed the recommended fruit intake, but not during the weekend, which was in the first case due to the implementation of the Slovenian national guidelines [11] which have been mandatory in all educational institutions since 2010, and in second case due to poor eating habits among Slovenian [10].
Our study was also focused on offer and intake of nuts, as we did not find any study that addressed the inclusion of nuts in the kindergarten diet. The EFSA report state that European children, on average has low intake or no consumption of nuts [9], but we demonstrate in our study that we can contribute, with kindergarten nutrition only, to an adequate daily intake. In addition to their broad health benefits [18,41] nuts also improve overall diet quality [42] therefore they should be more specifically addressed in dietary guidelines. It is to be pointed out that care should be taken when providing nuts to children in kindergartens, as there is a risk of suffocation, which must be considered when preparing and serving this food group. In addition, tree nut allergies are among the eight most common food allergies that may cause severe reactions [43]. Despite all the risks, the benefits of eating nuts may exceed the possible disadvantages; therefore, nuts could be included in kindergarten menus, providing that all safety precautions are maintained.
Considering that the children are expected to consume more than 60% of their daily energy and nutritional needs (in Slovenia and some other countries even up to 75%) in kindergartens, we observed that offer in the prototype menu satisfied RDFI requirements with regard to almost all parameters, while the regular menu did not. Besides that, the 7-day participants dietary record showed that diet outside the kindergarten contained very low amounts of vegetables, whole grains and nuts, which is in accordance with EFSA report, which shows that intakes of healthy food groups are inadequate [9]. By comparing the average amounts of food groups consumed during the week and during the weekend, when only parents take care for children’s nutrition, we can clearly distinguish the positive contribution of kindergarten nutrition, especially in providing an adequate amount of vegetables, fruits, whole grains and nuts. This contribution was also revealed in CG participants, although their weekday’s nutrition was less adequate than nutrition in PG participants. Based on results, we recommend designing kindergarten meals by strictly following the Guidelines, without simplifying. Although some healthy foods are not well accepted by children, we should try different strategies for increasing their consumption, rather than stop offering them [44].
The results of our study coincide with the findings of several other studies [13,14,21], as they show that kindergarten nutrition contributes to a more adequate daily intake of vegetables, fruits, and whole grains in the participants from both study groups. However, with our study we also revealed that by consistently following the dietary guidelines in the design of kindergarten menus, we can contribute to a significantly more adequate daily intake of vegetables, fruit, whole grains and nuts, compared to a simplified menu design, which should lead to more effective supervision of the implementation of the nutritional guidelines in kindergartens. As illustrated in Supplementary Table S4, differences in offered food groups were seen even between dishes prepared in PG kindergartens with the same menu, as cooks including different amounts of food groups, the biggest differences being in the use of vegetables and whole grains.
Kindergarten nutrition depends on several factors, one of the most important being the ability and educational level of nutritionists and cooks who should be able to design menus and prepare healthy meals in accordance with the guidelines of healthy eating. Additional studies and national measures are needed to achieve these goals.
The main strength of our study was that we compared differently designed kindergarten menus within the same country, with the same dietary guidelines, which, to the best of our knowledge, has not been studied yet. Additionally, strength is represented by the 7-day weighted dietary record, which also includes weekends, providing a solid insight into the average amount of food groups’ intakes in 5-6-year-old children. All mixed dishes were carefully disaggregated according to weighted recipes to obtain accurate data on the content of individual food groups. Due to the relatively small number of participants, we were able to daily interact with their parents, teachers and cooks, which additionally prevented errors in filling dietary records. Data are presented in grams, which allows for the most accurate comparison with other studies. As there are no national data on the average daily intake of food groups for 5-6 years old children, our results filled the gap on missing data, although they were not representative. Furthermore, the 5- day prototype menu can be helpful for designing new menus and can be easily transferred to other kindergarten environments.
The findings of this study need to be interpreted in the light of its limitations. Since the OPEN tool does not provide discrimination between whole grain and refined starchy food products, the classification was performed manually. This could lead to a difference between the results of other studies, as the methodology for calculating whole grain foods is not yet unified. Besides relatively small number of participants, limitations is also, due to COVID-19 epidemic, a relatively short observational period.
In the last decade, many European countries have implemented various measures to improve food environment in kindergartens and schools [8], but still, recent national surveys [9] indicate that children do not consume a sufficient amount of food groups, which are recognized as beneficial for health. We believe that with our study, we have opened a new field of future research that should look for more sustainable ways for the most optimal intakes of recommended food groups in kindergartens.
5. Conclusions
To our knowledge, this is the first study to demonstrate the important value of a well-planned kindergarten menu in improving daily intake of vegetables, whole grains, and nuts in 5-6-year-old children. The results highlight the need for additional strategies to avoid simplification in planning kindergarten menus and the important contribution of kindergarten meals to adequate daily nutrition. Our study also highlighted participants' excessive salt consumption, which was attributed to the overuse of salt in kindergartens and home kitchens. The findings may serve as a basis for future interventions to improve the nutritional environment in child care settings.
Supplementary Materials
The following supporting information can be downloaded at: www.mdpi.com/xxx/s1, Table S1: Prototype 5-day kindergarten menu, including the recommended serving portions (g/child) and approximate energy intakes by individual meals; Table S2: Regular 5-day kindergarten menu from Zasavje region including the recommended serving portions (g/child) and approximate energy intakes by individual meals; Table S3: Regular 5-day kindergarten menu from Central Slovenia region including the recommended serving portions (g/child) and approximate energy intakes by individual meals; Table S4: Classification of foods and mixed dishes from 5-day kindergarten menus into food groups; Table S5: Leftovers in PG kindergartens and CG kindergartens.
Author Contributions
MB participated in the design of the study, collected and analyzed the data and writing—original draft preparation; TB co-designed the study, supervised data interpretation, writing—review and editing and critically revised and compiled the manuscript; MK co- designed the study, supervised methodology, writing—review and editing, critically revised and compiled the manuscript. All authors have read and approved this version of the manuscript.
Funding
The study was supported by the Slovenian Research Agency (Program P3-0395 and I0-0035).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Committee for Medical Ethics of the Republic of Slovenia (No.0120-66/2019/8), 18 June 2019).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
Authors gratefully acknowledge for the cooperation to all parents of the participants and cooperation and support of the principals, of all six kindergartens (Barbara Novinec, Anita Čretnik, Majda Fajdiga, Darja Rakovič, Daša Bokal, Maja Petan Majcen), to nutritionists (Branka Strah, Sara Goršek Bobek, Natalija Benko, Ana Mulej, Dunja Volavšek) and to all the teachers and kitchen staff who actively participated in this study.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
OPEN – national dietary assessment tool; PG – prototype group; CG – control group; SD – Standard Deviation; DRI – Dietary Reference Intake; RDFI – Recommended Daily Food Intake; RDFO – Recommended Daily Food Offer.
References
- GBD 2016. Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar] [CrossRef] [PubMed]
- Bowen KJ, Sullivan VK, Kris-Etherton PM, Petersen KS. Nutrition and cardiovascular disease—an update. Curr Atheroscler Rep 2018, 20:8. [CrossRef]
- World Health Organization. Noncommunicable diseases progress monitor 2020. Available online: https://www.who.int/publications/i/item/9789240000490 (accessed on 15 September 2022).
- Fernandez-Jimenez R, Al-Kazaz M, Jaslow R, Carvajal I, Fuster V. Children present a window of opportunity for promoting health: JACC review topic of the week. J Am Coll Cardiol 2018, 72, 3310–3319. [CrossRef]
- 5. Scaglioni S, Arrizza C, Vecchi F, Tedeschi S. Determinants of children's eating behavior. Am J Clin Nutr, 2006. [CrossRef]
- UNICEF. A World Ready to Learn: Prioritizing quality early childhood education. 2019. Available online: https://uni.cf/world-ready-to-learn-data (accessed on 8 July 2023).
- European Commission/EACEA/Eurydice. Eurydice Brief: Key Data on Early Childhood Education and Care in Europe. Luxembourg: Publications Office of the European Union 2019, 1-24. [CrossRef]
- Kovacs VA, Messing S, Sandu P, Nardone P, Pizzi E, Hassapidou M, Brukalo K, Tecklenburg E, Abu-Omar K. Improving the food environment in kindergartens and schools: an overview of policies and policy opportunities in Europe. Food Policy 2020, 96: 101848. [CrossRef]
- EFSA. Food consumption data. 2022. Available online: https://www.efsa.europa.eu/en/data-report/food-consumption-data (accessed on 3 January 2023).
- NIJZ. Različni vidiki prehranjevanja prebivalcev Slovenije: v starosti od 3 mesecev do 74 let. 2019. Available online: https://nijz.si/wp-content/uploads/2022/07/razlicni_vidiki_prehranjevanja_prebivalcev_slovenije.pdf (accessed on 3 January 2023).
- Gabrijelčič Blenkuš M, Pograjc L, Gregorčič M, Adamič M, Čampa A. Smernice zdravega prehranjevanja v vzgojno-izobraževalnih ustanovah (od prvega leta starosti naprej). Ministry of Health 2005. Available online: https://nijz.si/wp-content/uploads/2022/07/smernice_zdravega_prehranjevanja_v_viu.pdf (accessed on 15 September 2022).
- NIJZ. Strokovno spremljanje prehrane s svetovanjem v vzgojno-izobraževalnih zavodih v letu 2018. 2018. Available online: https://nijz.si/wp-content/uploads/2017/05/porocilo_spremljanja_pehrane_v_viz_2018_gn_0.pdf NIJZ (accessed on 15 September 2022).
- Tugault-Lafleur CN, Black JL. Lunch on school days in Canada: examining contributions to nutrient and food group intake and differences across eating locations. J Acad Nutr Diet 2020, 120, 1484–1497. [Google Scholar] [CrossRef] [PubMed]
- Luecking CT, Mazzucca S, Vaughn AE, Ward DS. Contributions of early care and education programs to diet quality in children aged 3 to 4 years in central North Carolina. J Acad Nutr Diet 2020, 120, 386–394. [Google Scholar] [CrossRef]
- 15. Korkalo L, Nissinen K, Skaffari E, Vepsäläinen H, Lehto R, Kaukonen R, Koivusilta L, Sajaniemi N, Roos E, Erkkola M. The contribution of preschool meals to the diet of Finnish preschoolers. Nutrients. [CrossRef]
- Benjamin EJ, Virani SS, Callaway CW et al. Heart disease and stroke statistics-2018 update: a report from the American heart association. Circulation 2018, 137, 67–492. [Google Scholar] [CrossRef]
- Reynolds A, Mann J, Cummings J, Winter N, Mete E, Te Morenga L (2019) Carbohydrate quality and human health: a series of systematic reviews and meta-analyses. Lancet 393:434-445. [CrossRef]
- Ros, E. Eat nuts, live longer. J Am Coll Cardiol 2017, 70, 2533–2535. [Google Scholar] [CrossRef]
- Lieffers JRL, Ekwaru JP, Ohinmaa A, Veugelers PJ. The economic burden of not meeting food recommendations in Canada: the cost of doing nothing. PLoS One 2018, 13, 0196333. [Google Scholar] [CrossRef]
- Hasnin S, Dev DA, Tovar A. Participation in the CACFP ensures availability but not intake of nutritious foods at lunch in preschool children in child-care centers. J Acad Nutr Diet 2020, 120, 1722–1729. [Google Scholar] [CrossRef]
- 21. Sisson SB, Kiger AC, Anundson KC, Rasbold AH, Krampe M, Campbell J, Degrace B, Hoffman L. Differences in preschool-age children's dietary intake between meals consumed at childcare and at home. Prev Med Rep. [CrossRef]
- Cole TJ, Lobstein T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr Obes 2012, 7, 284–294. [Google Scholar] [CrossRef]
- Korošec M, Golob T, Bertoncelj J, Stibilj V, Seljak BK (2013) The Slovenian food composition database. Food Chem 2013, 140, 495–499. [CrossRef]
- Ross AB, van der Kamp JW, King R, Lê KA, Mejborn H, Seal CJ, Thielecke F, Healthgrain Forum. Perspective: a definition for whole-grain food products-recommendations from the healthgrain forum. Adv Nutr 2017, 8, 525–531. [Google Scholar] [CrossRef] [PubMed]
- 25. Jones JM, García CG, Braun HJ. Perspective: whole and refined grains and health-evidence supporting "Make half your grains whole". Adv Nutr. [CrossRef]
- EFSA. General principles for the collection of national food consumption data in the view of a pan-European dietary survey. EFSA Journal 2009, 7, 1435. [Google Scholar] [CrossRef]
- NIJZ. Slikovno gradivo za določanje vnosa živil. 2017; Available online: Artboard 1 (nijz.si) (accessed 20 September 2022). [Google Scholar]
- Fagerland MW, Sandvik L. Performance of five two-sample location tests for skewed distributions with unequal variances. Contemp Clin Trials 2009, 30, 490–496. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: a language and environment for statistical computing. R Foundation for Statistical Computing. 2018. Available online: 2019https://www.gbif.org/tool/81287/r-a-language-and-environment-for-statistical-computing. (accessed on 1 October 2022).
- Deon V, Del Bo' C, Guaraldi F, Abello F, Belviso S, Porrini M, Riso P, Guardamagna O. Effect of hazelnut on serum lipid profile and fatty acid composition of erythrocyte phospholipids in children and adolescents with primary hyperlipidemia: a randomized controlled trial. Clin Nutr 2018, 37, 1193–1201. [Google Scholar] [CrossRef]
- 31. Berlic M, Jug U, Battelino T, Levart A, Dimitrovska I, Alberht A, Koročec M. Antioxidant-rich foods and nutritional value in daily kindergarten menu: a randomized controlled evaluation executed in Slovenia. Food Chem, 1345. [CrossRef]
- Bernardi JR, Cezaro CD, Fisberg RM, Fisberg M, Vitolo MR. Estimation of energy and macronutrient intake at home and in the kindergarten programs in preschool children. J Pediat 2010, 86, 59–64. [Google Scholar] [CrossRef]
- Andreyeva T, Kenney EL, O'Connell M, Sun X, Henderson KE. Predictors of nutrition quality in early child education settings in Connecticut. J Nutr Educ Behav 2018, 50(5, :458-467. [CrossRef]
- Romo-Palafox MJ, Ranjit N, Sweitzer SJ, Roberts-Gray C, Byrd-Williams CE, Briley ME, Hoelscher DM. Adequacy of parent-packed lunches and preschooler's consumption compared to dietary reference intake recommendations. J Am Coll Nutr 2017, 36, 169–176. [CrossRef]
- Robson SM, Khoury JC, Kalkwarf HJ, Copeland K. Dietary intake of children attending full-time child care: What are they eating away from the child-care center? J Acad Nutr Diet 2015, 115, 1472–1478. [Google Scholar] [CrossRef]
- Embling R, Pink AE, Gatzemeier J, Price M, D Lee M, Wilkinson LL. Effect of food variety on intake of a meal: a systematic review and meta-analysis. Am J Clin Nutr 2021, 113, 716–741. [Google Scholar] [CrossRef]
- Roe LS, Meengs JS, Birch LL, Rolls BJ. Serving a variety of vegetables and fruit as a snack increased intake in preschool children. Am J Clin Nutr 2013, 98, 693–699. [Google Scholar] [CrossRef]
- Roe LS, Sanchez CE, Smethers AD, Keller KL, Rolls BJ. Portion size can be used strategically to increase intake of vegetables and fruits in young children over multiple days: a cluster-randomized crossover trial. Am J Clin Nutr 2022, 115, 272–283. [Google Scholar] [CrossRef]
- Spill MK, Birch LL, Roe LS, Rolls BJ. Hiding vegetables to reduce energy density: an effective strategy to increase children's vegetable intake and reduce energy intake. Am J Clin Nutr 2011, 94, 735–741. [Google Scholar] [CrossRef] [PubMed]
- Larrosa S, Luque V, Grote V, Closa-Monasterolo R, Ferré N, Koletzko B, Verduci E, Gruszfeld D, Xhonneux A, Escribano J. Fibre Intake Is Associated with Cardiovascular Health in European Children. Nutrients 2020, 13, 12. [Google Scholar] [CrossRef]
- Feng Y, Bi Y, Tang X, Zhang P, Tong J, Peng X, Tian J, Liang X. Protective effects of appropriate amount of nuts intake on childhood blood pressure level: a cross-sectional study. Front Med (Lausanne) 2022, 8, 793672. [Google Scholar] [CrossRef]
- Mead LC, Hill AM, Carter S, Coates AM. The effect of nut consumption on diet quality, cardiometabolic and gastrointestinal health in children: a systematic review of randomized controlled trials. Int J Env Res Pub He 2021, 18, 454. [Google Scholar] [CrossRef] [PubMed]
- Weinberger T, Sicherer S. Current perspectives on tree nut allergy: a review. J Asthma Allergy 2018, 11, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Taylor CM, Emmett PM. Picky eating in children: causes and consequences. Proc Nutr Soc 2019, 78, 161–169. [Google Scholar] [CrossRef]
Figure 1.
Flowchart of the study showing the enrollment process of participants, assignment to the two study groups, losses to follow-up, and the number of participants completing the study. Note: K, kindergarten; PK, prototype kindergarten; CK, control kindergarten; n, number of participants.
Figure 1.
Flowchart of the study showing the enrollment process of participants, assignment to the two study groups, losses to follow-up, and the number of participants completing the study. Note: K, kindergarten; PK, prototype kindergarten; CK, control kindergarten; n, number of participants.
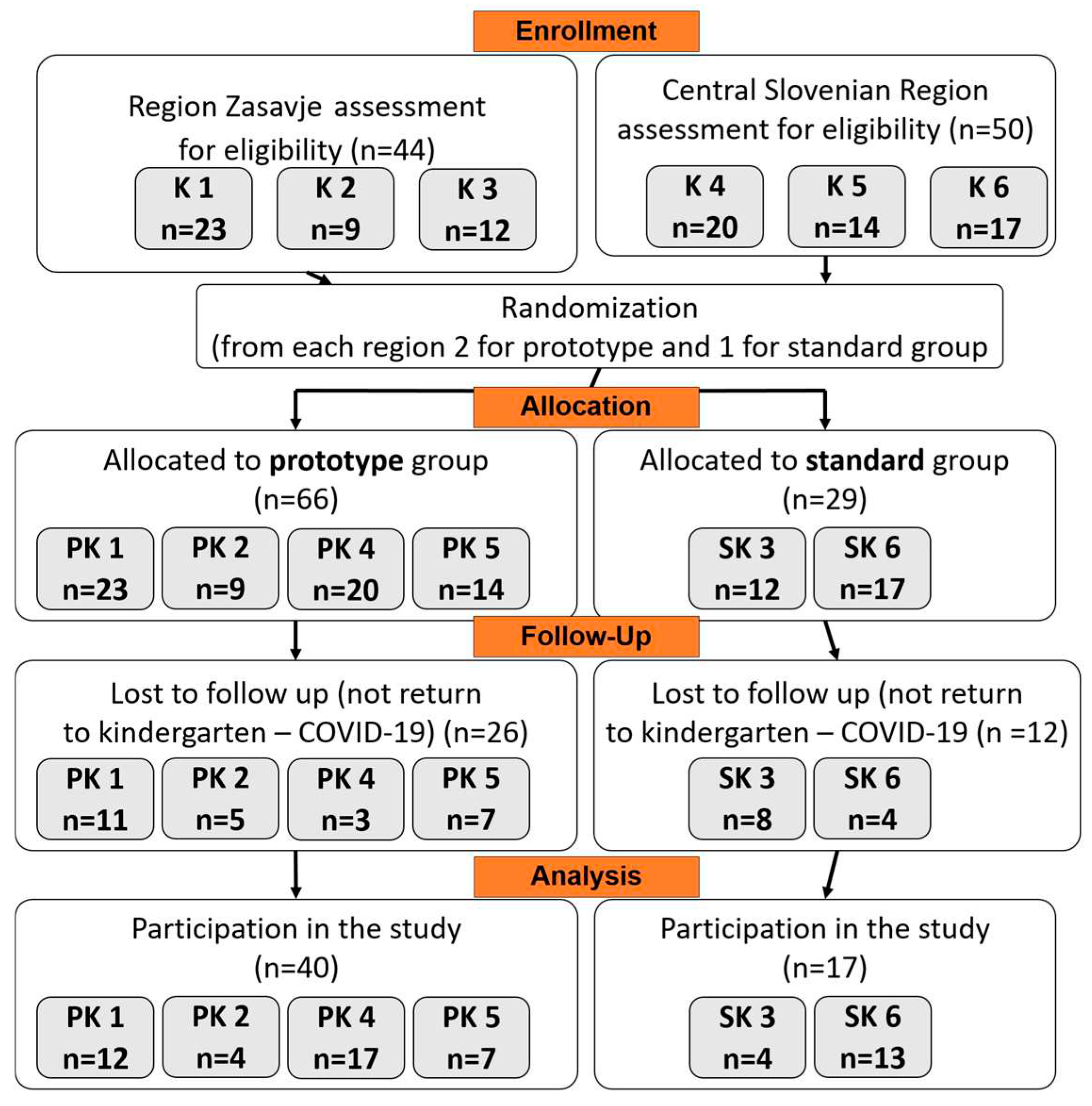
Figure 2.
An average amount of served food groups from prototype 5-day and regular kindergarten daily meals (breakfast, lunch, 2 snacks) compared to RDFI (orange line) and 75% RDFI (red line); and contribution of kindergartens daily diet (breakfast, lunch, 2 snacks) and diet outside kindergartens to daily intakes of food groups in PG participants (n=40) and CG participants (n=17), compared to RDFI (orange line) and 75% RDFI (red line). Note: RDFI, Recommended Daily Food Intake set in dietary Guidelines for healthy eating in educational institutions.
Figure 2.
An average amount of served food groups from prototype 5-day and regular kindergarten daily meals (breakfast, lunch, 2 snacks) compared to RDFI (orange line) and 75% RDFI (red line); and contribution of kindergartens daily diet (breakfast, lunch, 2 snacks) and diet outside kindergartens to daily intakes of food groups in PG participants (n=40) and CG participants (n=17), compared to RDFI (orange line) and 75% RDFI (red line). Note: RDFI, Recommended Daily Food Intake set in dietary Guidelines for healthy eating in educational institutions.
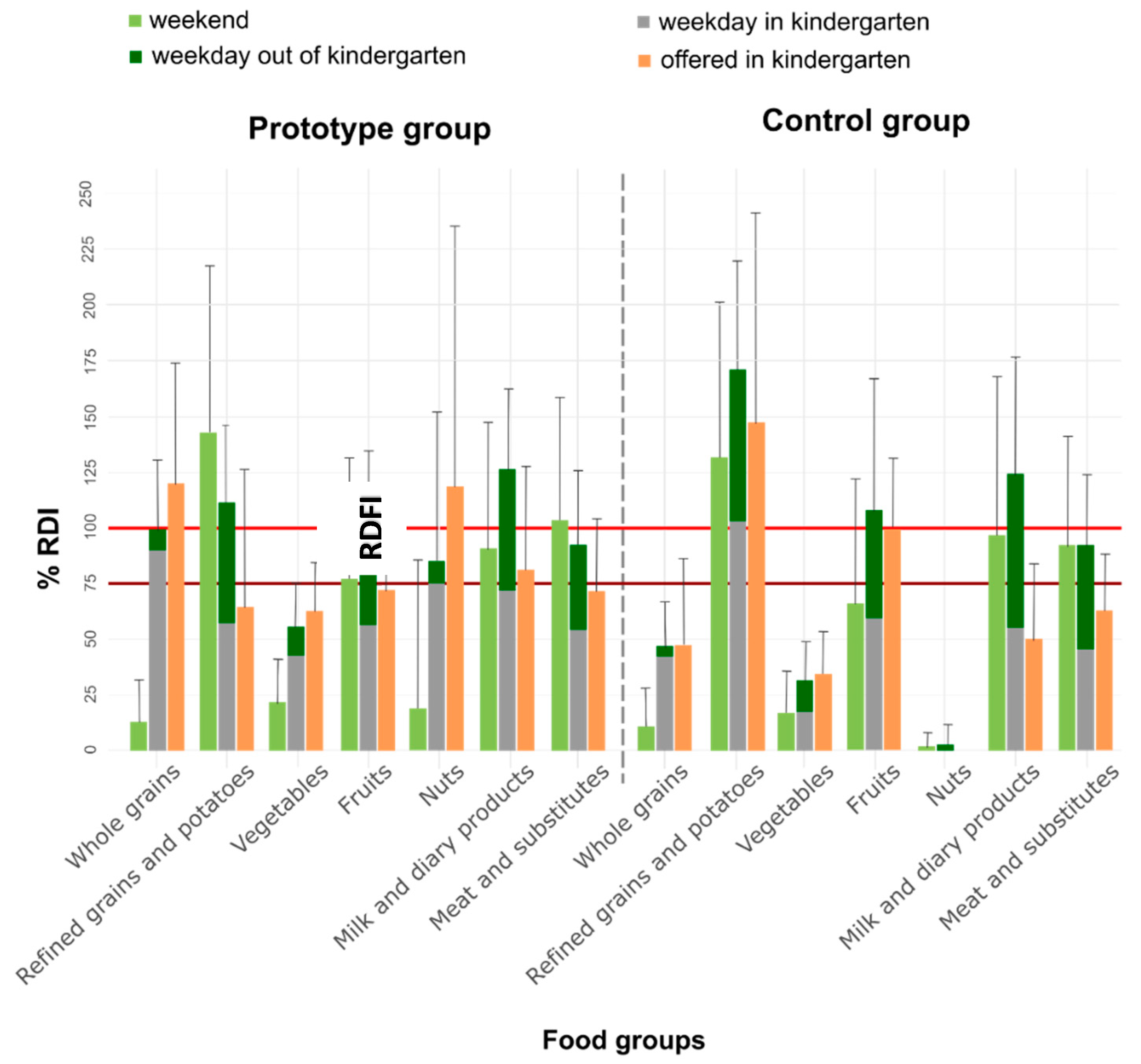

Table 1.
An average 5-day offer of food groups in PG kindergartens (n=4) and CG kindergartens (n=2) and 5/7-day intake of food groups in 5-6 years old participants (n=57), divided into prototype group (n=40) and control group (n=17), according to meal location. The data were obtained from consecutive 7-day dietary record inside and outside kindergartens.
Table 1.
An average 5-day offer of food groups in PG kindergartens (n=4) and CG kindergartens (n=2) and 5/7-day intake of food groups in 5-6 years old participants (n=57), divided into prototype group (n=40) and control group (n=17), according to meal location. The data were obtained from consecutive 7-day dietary record inside and outside kindergartens.
| Food Groups 1 |
Meat and substitutes (g) | Milk and dairy products (g) |
Fruits (g) |
Vegetables (g) | Nuts (g) |
Whole grains (g) | Refined grains and potatoes (g) | |
|---|---|---|---|---|---|---|---|---|
| Variable of interest | RDFI 2 4-6y (75% RDFI) 3 |
110 (82.5) | 400 4 (300) |
200 (150) |
300 (225) |
11 5 (8) |
115 6 (86) |
115 6 (86) |
| Offered in kindergarten Mean (SD) 7 | PG | 78 (36) | 325 (162) | 143 (61) | 188 (66) | 14 (13) | 137 (62) | 74 (71) |
| CG | 69 (28) | 200 (136) | 198 (64) | 103 (58) | 0 | 54 (45) | 169 (108) | |
| p value | 1 | 0.231 | 0.233 | 0.011* | <0.001* | 0.002* | 0.152* | |
| Weekday in kindergartens Mean (SD) 8 | PG | 59 (23) | 289 (94) | 112 (34) | 136 (48) | 8 (6) | 106 (35) | 66 (23) |
| CG | 50 (24) | 220 (101) | 134 (74) | 60 (51) | 0 | 49 (26) | 119 (48) | |
| p value | 1 | 0.137 | 1 | <0.001* | <0.001* | <0.001* | 0.002* | |
| Weekdays outside kindergartens Mean (SD) 9 | PG | 42 (28) | 216 (111) | 88 (65) | 33 (31) | 0.8 (3) | 9 (13) | 62 (39) |
| CG | 51 (29) | 275 (199) | 82 (64) | 35 (36) | 0.3 (1) | 5 (10) | 78 (39) | |
| p value | 1 | 1 | 1 | 1 | 1 | 1 | 1 | |
| Total weekdays Mean (SD) |
PG | 101 (37) | 505 (145) | 200 (80) | 169 (59) | 8.3 (7) | 115 (36) | 128 (40) |
| CG | 101 (35) | 495 (210) | 216 (118) | 95 (53) | 0.3 (1) | 54 (23) | 197 (56) | |
| p value | 1 | 1 | 1 | <0.001* | <0.001* | <0.001* | 0.005* | |
| Total weekends Mean (SD) 10 |
PG | 113 (61) | 365 (227) | 153 (109) | 66 (58) | 2 (7) | 13 (22) | 164 (86) |
| CG | 101 (54) | 388 (285) | 131 (112) | 52 (57) | 0.2 (0.7) | 13 (20) | 152 (80) | |
| p value | 1 | 1 | 1 | 1 | 0.288 | 1 | 1 |
PG, prototype group; CG, control group; SD, Standard Deviation; RDFI, Recommended Daily Food Intake; RDFO, Recommended Daily Food Offer. 1 The food groups represent the groups used in dietary assessment tool OPEN; starchy foods were separated into whole grains and refined grains and potatoes. 2 RDFI for 4-6-year-old children set in Guidelines [11]. 3 75% RDFI/O recommended food intake/offer in kindergarten. 4 RDFI for milk and dairy products is 2 units, of which 1 unit represents: 200 ml of milk or yogurt or 30 g of soft cheese (cottage cheese, cheese spread) or 15 g of hard cheese (parmesan, edam, gouda, etc.) [11]. Based on the recipes, we converted milk and dairy units to g as follows: milk and yogurt as actual intake, soft cheese = (amount*200)/30 hard cheese=(amount*200)/15. 5 RDFI was calculated based on the doses recommended for adults, adjusted to children’s body weight (on average 0.43 g/kg of body weight [30]. 6 RDFI for starchy foods is 9 units, of which 1 unit represents 20-30 g of starchy foods, at least half of them should be whole grain (11). 7 Mean (SD) Mean values of offered PG and CG kindergartens meals, based on weighed recipes and analysed with OPKP. 8 Mean (SD) Mean values of 5-consecutive days (without weekends) intake of food groups in kindergartens, in PG participants (n=40) and CG participants (n=17), obtained from 5-day kindergarten weighed dietary record completed by participants’ teachers. 9 Mean (SD) Mean values of 5- weekday (without weekend) intake of food groups outside kindergarten, in PG participants (n=40) and CG participants (n=17), obtained from 7-day weighed or estimated dietary record, completed by participants’ parents. 10 Mean (SD) Mean weekend (2-day) intake of food groups in PG participants (n=40) and CG participants (n=17), obtained from 7-day weighed or estimated dietary record, completed by participants’ parents. *Values of average offer /intake amounts in the same column are significantly different between PG and CG (p<0.05).
Table 2.
An average 5-day energy content and approximate composition of meals prepared by kindergartens within the prototype (n=4) and regular (n=2) menu and average 5/7-day energy content and approximate composition of meals, consumed according to eating locations, separately for PG participants (n=40) and CG participants (n=17).
Table 2.
An average 5-day energy content and approximate composition of meals prepared by kindergartens within the prototype (n=4) and regular (n=2) menu and average 5/7-day energy content and approximate composition of meals, consumed according to eating locations, separately for PG participants (n=40) and CG participants (n=17).
| Energy (kcal) |
Total fat (g) |
Protein (g) |
CH (g) |
DF (g) |
Na (mg) |
||
|---|---|---|---|---|---|---|---|
| Variable of interest | DRI1 4-6 y. (75% DRI)2 |
1550 (1162) |
52–60 (39-45) |
39-58 (29-44) |
˃194 ˃146 | ˃ 15 (˃ 11) |
<1180 (880) |
| Offered in kindergartens Mean (SD)3 |
PG | 1115 (221) | 43 (12) | 39 (7) | 143 (31) | 20 (5) | 1983 (1148) |
| CG | 883 (178) | 25 (12) | 35 (8) | 128 (30) | 14 (5) | 1605 (718) | |
| p value | 0.031* | <0.001* | 1 | 1 | 0.017* | 1 | |
| Weekday in kindergartens Mean (SD)4 |
PG | 830 (176) | 30 (8) | 29 (6) | 112 (23) | 15 (3) | 1478 (400) |
| CG | 664 (239) | 20 (8) | 28 (11) | 94 (34) | 10 (4) | 1126 (521) | |
| p value | 0.097 | <0.001* | 1 | 0.334 | <0.001* | 0.196 | |
| Weekdays outside kindergartens Mean (SD)5 | PG | 660 (206) | 25 (9) | 22 (8) | 87 (30) | 6 (2) | 687 (286) |
| CG | 799 (289) | 32 (15) | 27 (8) | 101 (37) | 6 (3) | 757 (366) | |
| p value | 0.508 | 0.587 | 0.227 | 0.956 | 1 | 1 | |
| Total weekdays Mean (SD) |
PG | 1486 (250) | 55 (12) | 50 (10) | 198 (35) | 21 (4) | 2154 (463) |
| CG | 1462 (317) | 52 (16) | 54 (11) | 195 (46) | 16 (5) | 1910 (517) | |
| p value | 1 | 1 | 1 | 1 | 0.01* | 0.627 | |
| Total weekends Mean (SD)6 |
PG | 1336 (374) | 50 (17) | 48 (14) | 173 (56) | 11 (5) | 1648 (852) |
| CG | 1440 (289) | 57 (15) | 48 (8) | 183 (44) | 12 (3) | 1519 (527) | |
| p value | 1 | 0.808 | 1 | 1 | 1 | 1 |
PG, prototype group; CG, control group; SD, Standard Deviation; CH, Carbohydrates; DF, dietary fibre; Na, sodium. 1DRI – Dietary Reference Intake per day for 4-6 years old children with PAL (Physical Activity Level) 1.6 (Moderately Active) [11]. 2 75% – DRI for time spent in kindergarten. 3 Mean (SD) Mean values of offered PG and CG kindergartens meals, based on weighed recipes and analysed with OPKP. 4 Mean (SD) Mean values of 5-weekdays (without weekend) intake energy, macronutrient and sodium consumed in kindergartens by PG and CG participants. 5 Mean (SD) Mean values of 5-weekdays (without weekends) intake energy, macronutrient and sodium consumed outside kindergartens by PG and CG participants. 6 Mean (SD) Mean values of weekend (2-day) intake energy, macronutrient and sodium consumed by PG and CG participants. *Values in the same column of average offer /intake amounts are significantly different between PG and CG participants (p<0.05).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



