Submitted:
11 July 2023
Posted:
11 July 2023
You are already at the latest version
Abstract
Neuroendocrine tumors (NETs) of duodenal origin are an unusual subset among all NETs, comprising only about 3% of this neoplasm class. In general, NETs are characterized by overexpression of somatostatin receptors and carry an excellent prognosis with early diagnosis and intervention. Chromogranin A (CgA), a protein originating in secretory vesicles of neurons and endocrine cells, has gained wide usage in NET diagnosis and surveillance. Lanreotide is a synthetic octapeptide somatostatin analog with potent anti-proliferative action which has been approved by the FDA (U.S.) and EMA (E.U.) for NET treatment. It is known for its inhibitory effects on growth hormone, serotonin, CgA, and other markers. Here we describe a 56yr-old female with functional NET of duodenal origin, where serum CgA was successfully reduced from 3636 to <100 ng/mL after multidose lanreotide within five months. Of note, no metastatic spread was identified on positron emission tomography/computed tomography with 64Cu-labeled somatostatin analog tracer. Surgical resection of distal antrum, pylorus, and proximal duodenum followed without complication. Histology revealed several foci of well-differentiated tumor cells with characteristic neuroendocrine features and clear surgical margins; low proliferation index (2%) was noted on Ki-67 staining. While select laboratory and imaging modalities are available for diagnosis and monitoring of duodenal NET, this is the first reported therapeutic use of lanreotide in this NET setting. The observed serum CgA attenuation, even before surgery, supports its effectiveness in management of primary nonmetastatic duodenal NET.
Keywords:
neuroendocrine tumor
; duodenum
; chromogranin A
; lanreotide
; surgery
1. Introduction
Neuroendocrine tumors (NETs) are malignancies of endocrine origin with an incidence perhaps as low as 2:100,000 [1]. These lesions derive from neuroendocrine cells which may potentially arise anywhere in the body; detection is difficult due to long periods of quiescence. NET cells overexpress surface somatostatin receptors (SSTRs) which are therapeutic targets for synthetic somatostatin analogs (e.g., octreotide & lanreotide). NET diagnosis can be assisted by a variety of positron emission tomography/CT radiopharmaceuticals, including 64Cu-dotatate [2].
2. Clinical Presentation
A 56yr old non-smoking Caucasian female in good general health presented for abdominal discomfort and chronic reflux. Evaluation included upper endoscopy for direct visualization to the descending duodenum. Esophageal and stomach survey was unremarkable although a polypoid structure was noted at the duodenal bulb mucosa (Figure 1). Snare cautery was used to remove this lesion, retrieved via Roth Net® (Steris Healthcare, Dublin IRL). Histology showed clear deep margins of the sampled tissue with no necrosis and low mitotic activity at <2 mitoses/2 mm2 field. Immunohistochemical staining was positive for synaptophysin with a Ki-67 proliferation index of 2% (Figure 2). These findings were consistent with a provisional diagnosis of well-differentiated neuroendocrine tumor (Grade 1), with imaging studies and laboratory tests scheduled to refine the treatment approach.
While electrolytes and CBC were essentially normal, serum Chromogranin A (CgA) was markedly elevated at 3636 ng/mL (normal <311 ng/mL); serotonin was undetectable (<10 ng/mL). CBC showed neutrophil/lymphocyte ratio at 2.38 (normal <3) and for platelet/lymphocyte this was 12.88 (normal <150) (1). The aberrant CgA value supported prompt chemotherapy with 120mg lanreotide (Depot Somatuline®, Ipsen PharmaBiotech; Signes, FR) and three doses were administered before surgery. Contemporaneous CgA measurements confirmed an adequate tissue response (Figure 3). Positron emission tomography/CT images obtained from mid-skull through proximal femur after i.v. administration of 3.87mCi of 64Cu-dotatate (Detectnet®, Curium US LLC; Maryland Heights, MO) revealed physiologic distribution of radiotracer, with no pathologic foci or scatter to suggest metastatic disease (Figure 3). Next, exploratory laparotomy, resection of distal antrum, pylorus and first portion of the duodenum was performed after private insurance approval four months later. Multiple fluoroscopy images confirmed patency and integrity of the gastrointestinal tract during the procedure, and the postoperative recovery was unremarkable.
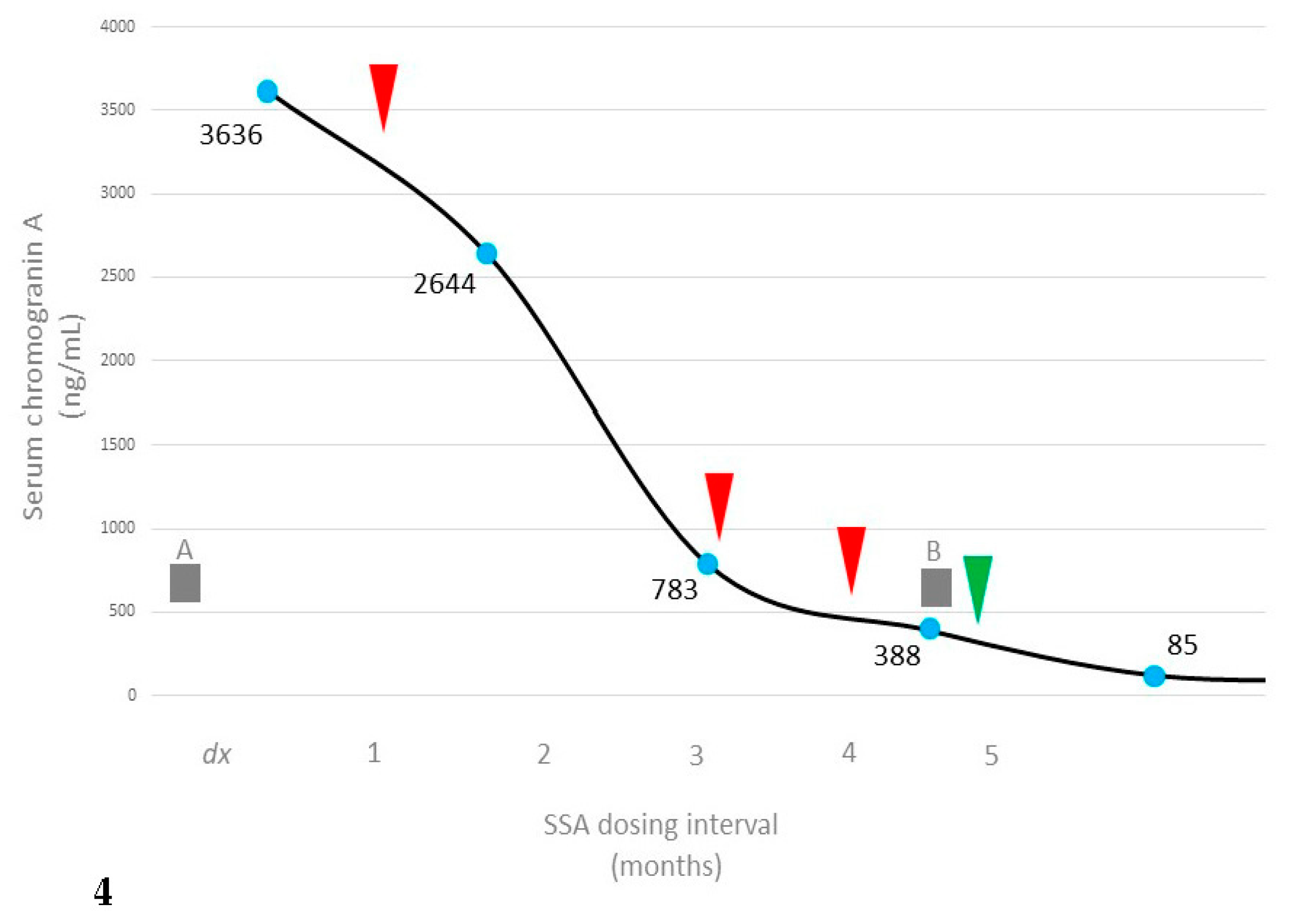
Microscopic exam of surgical specimens agreed with earlier biopsy findings, showing four local nests of well-differentiated neuroendocrine tumor cells involving lamina propria and submucosa at the gastroduodenal junction. Mitotic activity was <1 per hpf, without necrosis. Paraffin immunohistochemistry confirmed cytokeratin AE1/AE3+, synaptophysin+ staining with Ki-67 proliferation index of 2%. One additional lanreotide dose was given post-operatively, then discontinued due to satisfactory normalization of serum CgA (Figure 4).
3. Discussion
Primary duodenal NET has a favorable overall prognosis, and recent published experience in this subgroup shares some features with our case. For example, a 61yr old female in Japan was found to have a 15mm nodule at the descending duodenum confirmed as NET after endoscopic biopsy. Serum testing was normal and the lesion was classified as nonfunctional; the patient underwent subtotal stomach-preserving pancreaticoduodenectomy with good results [3]. In China, NET was reported in a 55yr-old female with a palpable non-tender upper abdominal mass. Ultrasound-guided abdominal biopsy obtained tissue for histologic analysis where cells positive for chromogranin A, synaptophysin, and cytokeratin were identified; partial duodenal resection followed without complication [4].
Certainly uncommon now, NET was once encountered even less often—A fivefold increase for this diagnosis was noted between 1973 and 2004 [5]. The upward trend is likely attributed to better detection from endoscopy, as well as improved imaging and laboratory techniques. Some 60% of NETs have either a pancreatic or gastrointestinal primary source (i.e., appendix, colon, intestine, rectum, stomach), collectively termed gastroenteropancreatic NETs [6]. Approximately 30% of NETs are functionally secretory, producing bioactive peptides and neuroamines which can cause fatigue, abdominal discomfort, muscle weakness, or dermal flushing/cutaneous vasodilation [7]. Among all NETs, those of duodenal origin comprise only 1-3% with clinical manifestations similar to other digestive tract tumors, resulting in nonspecific and variable clinical symptoms [8]. Most NETs develop sporadically, with no recognized causes or identifiable risk factors.
Chromogranin A (CgA) testing offers a noninvasive approach for detection and management of NET, as several neuroendocrine cell types express it. However, misleading results are possible among patients with chronic non-NET conditions or with certain medications (e.g., omeprazole, losartan, aspirin, paracetamol, and others) so a careful history is needed to interpret CgA values accurately [9]. In metastatic NET, CgA levels are typically far higher than for local NET [10] yet the order-of-magnitude elevation above reference range (with no metastatic spread) observed in this case highlights the variability of this parameter. Ki-67 is considered a proxy marker for mitosis/proliferative index, as it a nuclear protein expressed throughout the active cell cycle except in G0 (i.e., absent in resting cells). Another widely used marker in NET assessment is synaptophysin, a synaptic vesicle glycoprotein present in neuroendocrine cells and in virtually all brain and spinal cord neurons.
Highly specific radiotracers have encouraged a trend away from conventional scintigraphy to positron emission tomography/CT. The drive to enhance cell target specificity includes using 64copper-labeled [1,4,7,10-tetraazacyclododecane-N,N′,N″,N‴-tetraacetic acid]-D-Phe1, Tyr3-octreotate radiotracer (64Cu-dotatate), which preferentially seeks the G-protein-coupled receptor somatostatin receptor subtype-2 [2]. 64Cu has a low maximal positron energy (0.653 MeV) resulting in a shorter mean positron range compared to 68Ga. Moreover, 64Cu has a longer t1/2 than gadolinium-based radiotracers (12.7h vs. 68min) which favors the copper reagent by prolonging its use time [11]. While 64Cu-dotatate has been broadly used to diagnose somatostatin receptor-positive NET [12], this is among the first to describe its application specifically for duodenal NET.
Because native somatostatin has a circulatory half-life of ≤3min, its therapeutic use to inhibit dysfunctional neuroendocrine output has been overtaken by long-acting synthetic analogs [13]. Lanreotide is in this category, with approval for use in refractory acromegaly, gastroenteropancreatic NET, and adult carcinoid syndrome [14]. Here the sharp CgA decreases measured in response to lanreotide, even before surgery, illustrate its efficacy for duodenal NET. While lanreotide has been used for other neuroendocrine tumors, this is the first description of its successful application in isolated, primary duodenal NET. Periodic monitoring is planned, and it is anticipated that our case will provide another successful nonrecurrence.
Author Contributions
ESS and SHW organized manuscript drafts; ESS, SHW, SLT and DMI reviewed the literature and developed revisions; all authors read and approved the final manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Written informed consent was obtained from the patient for publication this paper.
Acknowledgments
The authors are grateful to Norma M. Edwards, MD and Guy E. Nichols, MD PhD (Knoxville, TN) for their expert contributions to surgery and histology, and to Robin T. Pitt (Jonesboro, AR) for assistance in patient coordination.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Armentano DPD, Monteiro MR, Aguiar PN Jr, Tsukamoto JS, Pio RB, Arakelian R, et al. Laboratory variables as predictors of progression in gastroenteropancreatic neuroendocrine tumors in different lines of antineoplastic treatments. Einstein (Sao Paulo) 2022;20:eAO6985. [CrossRef]
- Zobel EH, Ripa RS, von Scholten BJ, Curovic VR, Diaz LJ, Hansen TW, et al. Effect of liraglutide on vascular inflammation evaluated by [64Cu]DOTATATE. Diagnostics (Basel) 2021;11(8):1431. [CrossRef]
- Aoyama N, Wada M, Taniguchi Y, Inokuma T, Nakanishi Y, Fukuda A, et al. A case of neuroendocrine neoplasm of the minor duodenal papilla. Clin J Gastroenterol 2022;Dec 21. [CrossRef]
- Wang X, Wu Y, Cao X, Zhang X, Cheng Y, Kong L. Duodenal neuroendocrine tumor: A rare case report. Medicine (Baltimore) 2021;100(6):e24635. [CrossRef]
- Yao JC, Hassan M, Phan A, Dagohoy C, Leary C, Mares JE, et al. One hundred years after "carcinoid": Epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J Clin Oncol 2008;26(18):3063-72. [CrossRef]
- Khatri W, Spiro E, Henderson A, Rowe SP, Solnes LB (2023). Gastroenteropancreatic tumors: FDG positron emission tomography/computed tomography. PET Clin 2023;S1556-8598(22)00094-3. [CrossRef]
- Paulson S, Ray D, Aranha S, Scales A, Wang Y, Liu E. Lanreotide depot to treat gastroenteropancreatic neuroendocrine tumors in a U.S. community oncology setting: A prospective, observational study. Oncol Ther 2022;10(2):463-79. [CrossRef]
- Gaiani F, de’Angelis N, Minelli R, Kayali S, Carra MC, de’Angelis GL. Pediatric gastroenteropancreatic neuroendocrine tumor: A case report and review of the literature. Medicine (Baltimore) 2019;98(37):e17154. [CrossRef]
- Al-Risi ES, Al-Essry FS, Mula-Abed WS (2017). Chromogranin A as a biochemical marker for neuroendocrine tumors: A single center experience at Royal Hospital, Oman. Oman Med J 2017;32(5):365-70. [CrossRef]
- Qiao XW, Qiu L, Chen YJ, Meng CT, Sun Z, Bai CM, et al. Chromogranin A is a reliable serum diagnostic biomarker for pancreatic neuroendocrine tumors but not for insulinomas. BMC Endocr Disord 2014;14:64. [CrossRef]
- Loft M, Carlsen EA, Johnbeck CB, Johannesen HH, Binderup T, Pfeifer A, et al. 64Cu-DOTATATE PET in patients with neuroendocrine neoplasms: Prospective, head-to-head comparison of imaging at 1 hour and 3 hours after injection. J Nucl Med 2021;62(1):73-80. [CrossRef]
- Delpassand ES, Ranganathan D, Wagh N, Shafie A, Gaber A, Abbasi A, et al. 64Cu-Dotatate PET/CT for imaging patients with known or suspected somatostatin receptor-positive neuroendocrine tumors: Results of the first U.S. prospective, reader-masked clinical trial. J Nucl Med 2020;61(6):890-6. [CrossRef]
- Simonenko VB, Dulin PA, Makanin MA. Somatostatin analogues in treatment of gastrointestinal and pancreatic neuroendocrine tumors. Klin Med (Mosk) 2006;84(4):4-8.
- Kehoe, TE. NDA approval notification [letter to InvaGen Pharmaceuticals]. U.S. FDA Reference ID: 4906945; Silver Spring MD, 17 December 2021:1-5.
Figure 1.
Pre-resection view of duodenal neuroendocrine tumor polyp (arrow). Bar = 1mm.
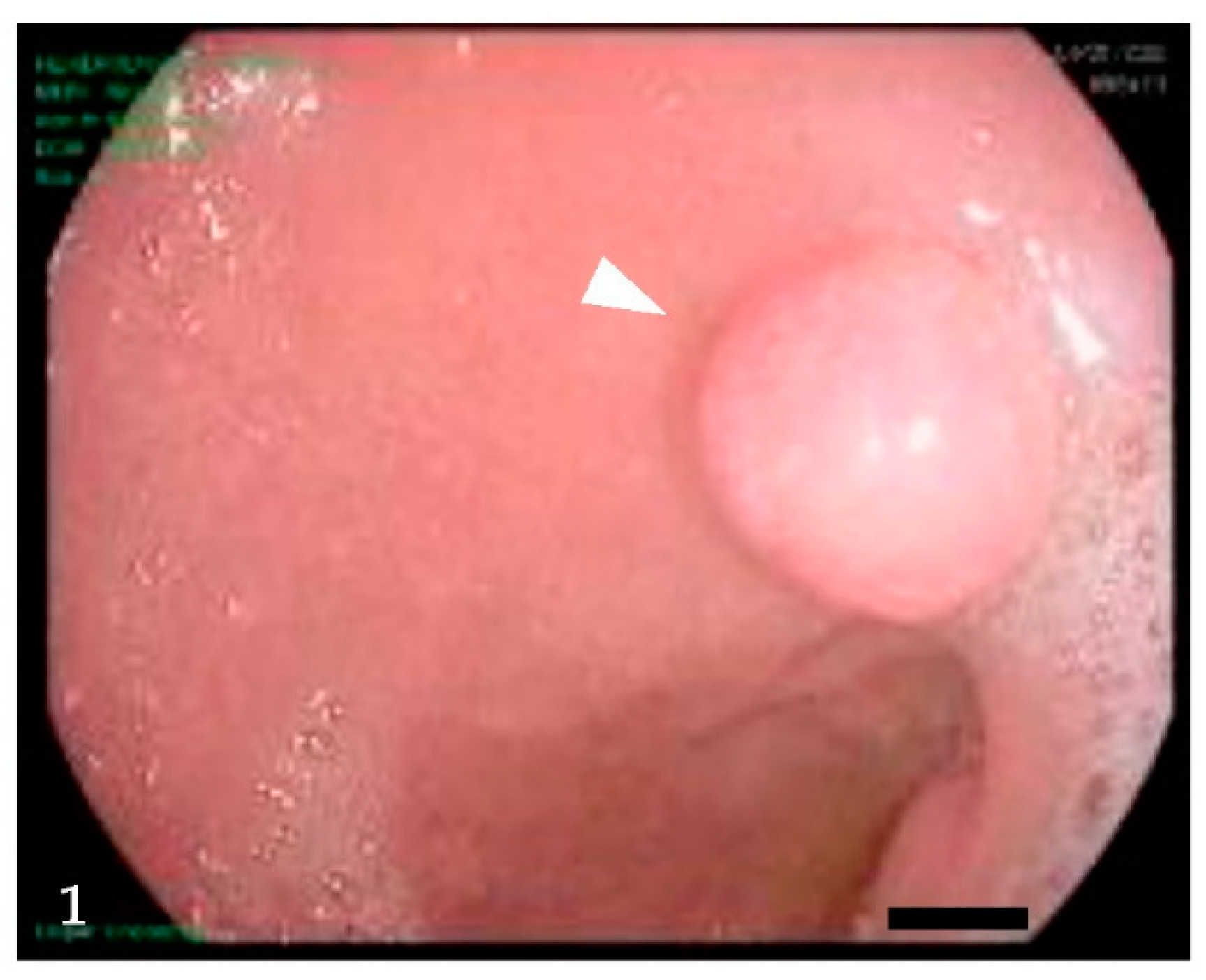
Figure 2.
For this duodenal NET, 2% proliferation index was noted on paraffin immunohistochemistry Ki-67 nuclear staining (red circles). Multiple nested organoid proliferations of well-differentiated cells with typical neuroendocrine features were noted at the gastroduodenal junction. Bar = 100μ (original magnification 400x).
Figure 2.
For this duodenal NET, 2% proliferation index was noted on paraffin immunohistochemistry Ki-67 nuclear staining (red circles). Multiple nested organoid proliferations of well-differentiated cells with typical neuroendocrine features were noted at the gastroduodenal junction. Bar = 100μ (original magnification 400x).
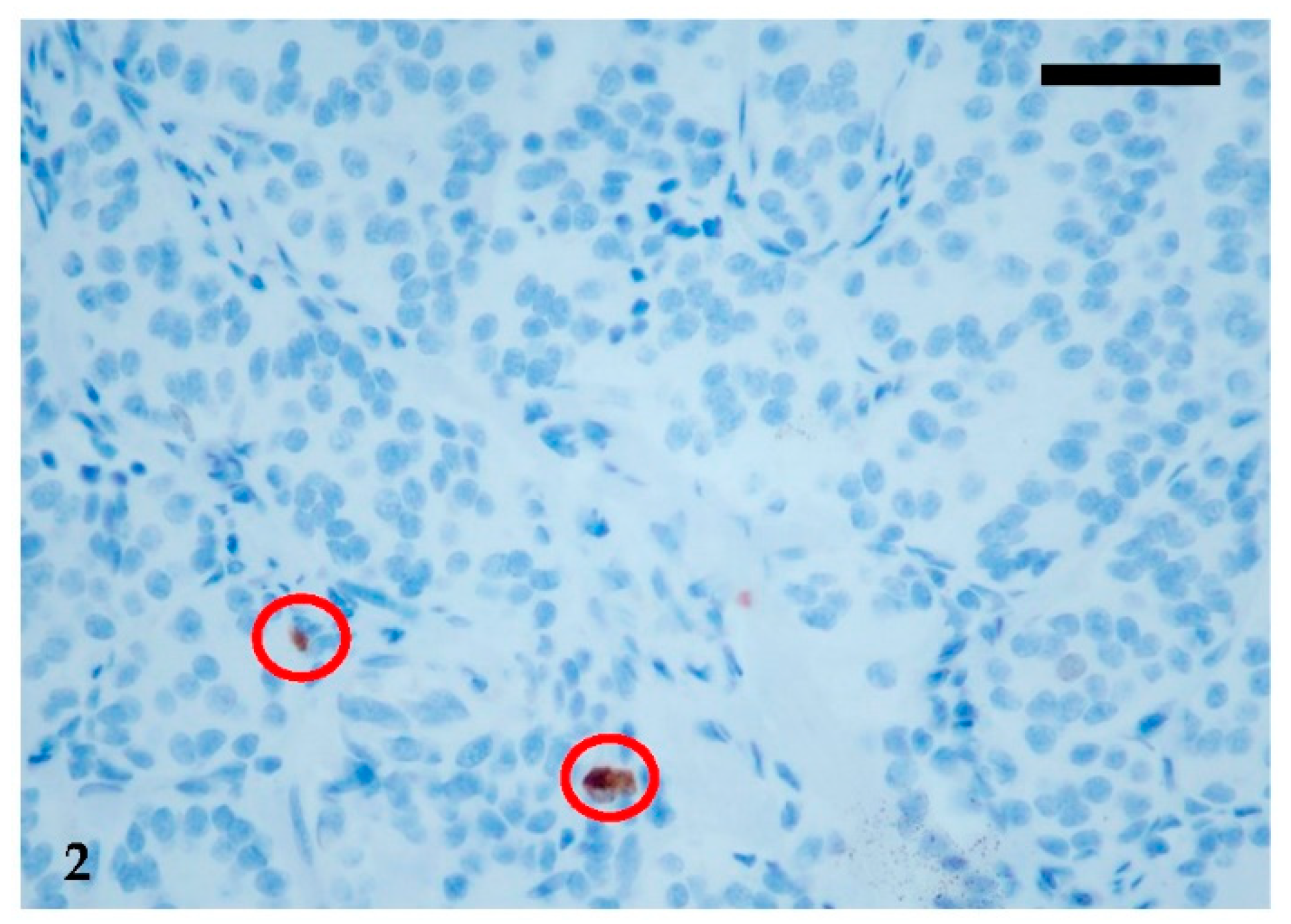
Figure 3.
Representative positron emission tomography/CT image obtained before surgery with i.v. 64Cu-dotatate (dose=3.87 mCi), showing radiotracer uptake near the duodenal bulb. No evidence of distant metastatic disease, no ascites, pulmonary nodularity or adnexal mass were apparent on CT.
Figure 3.
Representative positron emission tomography/CT image obtained before surgery with i.v. 64Cu-dotatate (dose=3.87 mCi), showing radiotracer uptake near the duodenal bulb. No evidence of distant metastatic disease, no ascites, pulmonary nodularity or adnexal mass were apparent on CT.
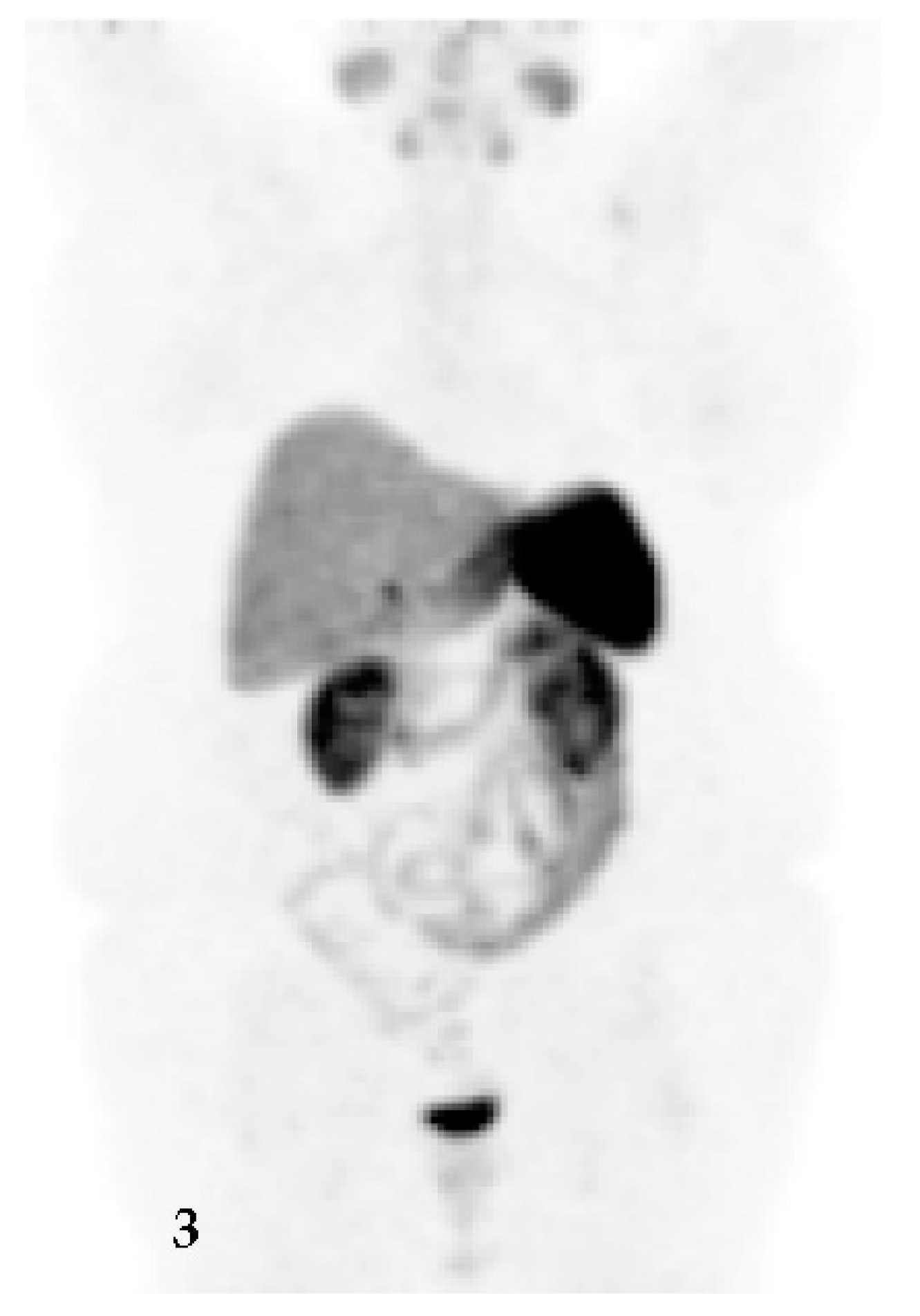
Figure 4.
Diagnosis (dx) by endoscopic biopsy (A) and subsequent resection (B) for duodenal neuroendocrine tumor is shown with CgA measurements (blue), responsive to preoperative synthetic somatostatin analog (SSA) lanreotide (red arrows). Only one SSA dose was given postoperatively (green arrow) as CgA normalized.
Figure 4.
Diagnosis (dx) by endoscopic biopsy (A) and subsequent resection (B) for duodenal neuroendocrine tumor is shown with CgA measurements (blue), responsive to preoperative synthetic somatostatin analog (SSA) lanreotide (red arrows). Only one SSA dose was given postoperatively (green arrow) as CgA normalized.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



