
Submitted:
28 June 2023
Posted:
29 June 2023
You are already at the latest version
Abstract
Background Coronary artery disease (CAD) is a widely recognized cardiovascular disease that is considered the leading cause of death worldwide, affecting people on a global scale. Percutaneous coronary intervention (PCI), which involves procedures such as balloon angioplasty or stenting, plays an important role in opening blocked arteries and minimizing damage to the cardiac muscle. While the use of drug-eluting stents (DESs) has significantly reduced the occurrence of coronary restenosis, the problem of in-stent restenosis (ISR) continues to pose a significant clinical challenge. Gaining a deeper understanding of the clinical predictors associated with ISR is vital for early detection and appropriate treatment. Hence, this study aimed to evaluate the clinical predictors of ISR specifically in Taiwanese patients. Methods We conducted a single-center, retrospective case-control study, enrolling 517 CAD patients undergoing previous coronary stenting and stable angina with positive stress test or acute coronary syndrome (ACS) during follow-up between January 2019 and December 2022 at National Taiwan University Hospital. The patients were categorized into two groups: the ISR group, consisting of individuals who received drug-coated balloon (DCB) treatment (n=177), and the non-ISR group, comprising patients who did not receive DCB treatment (n=340). To gather relevant data, we meticulously reviewed the medical records and analyzed the findings from coronary angiography to assess the clinical characteristics of the patients. Results Patients with three-vessel disease (3VD) exhibited a higher prevalence of underlying diseases and were more likely to be taking aspirin and clopidogrel. Moreover, our analysis revealed that age (adjusted odds ratio [aOR] 1.02, 95% confidence interval [CI] 1.00 - 1.04, p = 0.037) and the presence of 3VD (adjusted odds ratio [aOR] 2.15, 95% confidence interval [CI] 1.03 - 4.46, p = 0.039) were significantly associated with an increased risk of coronary ISR. Conclusions Older age and 3VD were the independent predictors of coronary ISR in CAD patients receiving coronary stent implantation.
Keywords:
coronary artery disease
; drug-coated balloon
; in-stent restenosis
; predictors
1. Introduction
Coronary artery disease (CAD) is one of the major cardiovascular diseases which has been known as the leading cause of death affecting the global human population. Percutaneous coronary intervention (PCI), a procedure aimed at opening blocked arteries and reducing damage to the myocardium, encompasses various techniques such as percutaneous transluminal coronary angioplasty (PTCA), stent implantation, and the use of drug-coated balloons (DCBs). Back in the early 1970s, stents were not yet available, and PTCA was the sole method used in PCI to address coronary artery stenosis. However, the occurrence of restenosis within six months postoperatively was alarmingly high, reaching approximately 50% [1]. In the 1980s, the introduction of bare-metal stents (BMSs) managed to reduce the six-month restenosis rate to 30% [2]. Over the past decade, the advent of new-generation drug-eluting stents (DESs) incorporating antiproliferative drugs like zotarolimus or everolimus has further decreased the occurrence of in-stent restenosis (ISR) to less than 10% [3]. Additionally, fully bioresorbable vascular scaffolds (BVSs), constructed from naturally occurring and synthetic biodegradable polymers, have emerged as a novel type of stent. These scaffolds provide similar drug delivery capabilities to metallic DESs for a period of six to twelve months after stenting, followed by gradual bioresorption [4]. Through advancements in PCI techniques and the development of innovative stents, the management of CAD has witnessed significant progress, resulting in reduced rates of restenosis and improved patient outcomes.
ISR refers to post-stenting coronary arterial damage followed by neointimal tissue proliferation ≥ 50% of the lumen diameter [5]. The clinical manifestations of ISR can vary widely, ranging from silent ischemia to acute myocardial infarction (AMI). Acute coronary syndrome (ACS), which includes unstable angina (UA), non-ST-segment elevation myocardial infarction (NSTEMI), and ST-segment elevation myocardial infarction (STEMI), accounts for more than half of all cases of ISR. Moreover, the presence of ACS in conjunction with ISR independently increases the risk of major adverse cardiac events (MACE) [6]. The significant incidence of severe ISR presentations emphasizes the importance of modifying ISR-related risk factors for secondary prevention.
The mechanisms of ISR arise from vascular injury caused by stent implantation, involving inflammation, proliferation, and matrix remodeling. The inflammatory responses to mechanical stretch, endothelial denudation, and subintimal hemorrhage triggered cascades of proliferative process, including vascular smooth muscle cell (VSMC) proliferation and migration, extracellular matrix synthesis, and resulted in formation of neointimal hyperplasia [7]. In fact, ISR is influenced by multiple factors. Firstly, patient characteristics such as age and comorbid conditions play a role. Secondly, biological factors, including drug resistance, systemic inflammation, neoatherosclerosis, and the presence of calcified nodules, contribute to ISR. Thirdly, genetic factors are associated with the development of neointimal tissue. Fourthly, mechanical factors, such as stent under-expansion, over-dilatation of an undersized stent, and stent fracture, can also contribute to ISR. Lastly, technical factors, including barotrauma outside the stented segment, the presence of residual uncovered atherosclerotic plaques, and stent gaps, may influence the occurrence of ISR [8]. Despite the significant decrease in the incidence of coronary restenosis following stenting, the adoption of stent implantation on a large scale highlights that ISR remains a significant clinical challenge. The average time for ISR to occur is approximately 12 months with DESs and 6 months with BMSs [5,9]. In recent years, several predictors for ISR have been proposed; however, the results have been inconsistent and not yet fully clarified. Consequently, we conducted a single-center, retrospective cohort study to evaluate the clinical predictors of ISR in Taiwanese patients with CAD.
2. Materials and Methods
2.1. Study Design
We conducted a single-center, retrospective case-control study, enrolling 517 CAD patients undergoing previous coronary stenting and stable angina with positive stress test or acute coronary syndrome during follow-up between January 2019 and December 2022 at National Taiwan University Hospital. The patients were divided into two groups: the ISR group, consisting of patients who received drug-coated balloon (DCB) treatment for ISR (n=177), and the non-ISR group, comprising patients who did not receive DCB treatment and did not develop ISR (n=340). The inclusion criteria for the study were as follows: 1) patients above 20 years old, 2) patients who had experienced ISR after coronary stenting with BMSs, DESs, or BVSs and were subsequently treated with DCBs, referred as the ISR group, and 3) patients who had undergone coronary stenting with BMSs, DESs, or BVSs but did not develop ISR as confirmed by angiographic diagnosis, referred as the non-ISR group. The medical records and coronary angiographic findings of the patients were reviewed to assess their clinical characteristics.
2.2. Patients and Clinical Characteristics
This research involved gathering patients' demographic information, including age, gender, body mass index, and underlying diseases such as hypertension, type II diabetes mellitus, peripheral artery occlusive disease, chronic kidney disease, end-stage renal disease, atrial fibrillation or atrial flutter, heart failure with reduced ejection fraction, and a history of coronary artery bypass graft. Additionally, we analyzed the current cardiovascular medications used by all participants in the study, including antiplatelet drugs, anticoagulants, statins, beta blockers, angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers, and angiotensin receptor-neprilysin inhibitors. The baseline characteristics of these factors were compared to the coronary vessel disease (VD) group, which included one-vessel disease (1VD), two-vessel disease (2VD), and three-vessel disease (3VD). In the population with coronary ISR, we classified the clinical manifestations into silent ischemia, stable angina, and acute coronary syndrome (ACS) for further analysis.
2.3. Coronary Angiographic Analysis
Coronary ISR was defined as the occurrence of post-stenting coronary arterial damage followed by neointimal tissue proliferation that resulted in a reduction of the lumen diameter by at least 50%. The coronary angiographic diagnoses were categorized into different types: one vessel disease (1VD), two vessel disease (2VD), three vessel disease (3VD), and left main (LM) disease. LM disease was defined as ≥ 50% angiographic narrowing of the LM coronary artery, either with or without multi-vessel coronary artery disease (CAD). Furthermore, chronic total occlusion (CTO) was identified as the total occlusion of a coronary artery lasting for at least 3 months based on angiography. CTO represents a particularly complex coronary lesion. The vessels affected by ISR could be the LM coronary artery, left anterior descending artery (LAD), left circumflex artery (LCX), right coronary artery (RCA), ramus intermedius artery (RI), or involve multiple vessels. In our analysis, we examined the number of ISR lesions among patients with ISR and assessed the type of stents used in all study participants.
2.4. Statistical Methods
This research study was divided into three groups: the one vessel disease (1VD), two vessel disease (2VD), and three vessel disease (3VD) groups. A comparison of the VD groups was conducted using the Chi-square test for categorical variables. Baseline characteristics were presented as numbers and percentages (n (%)). Continuous variables were analyzed using one-way analysis of variance (ANOVA), and the results were reported as means and standard deviations (mean ± SD). Logistic regression models were employed in this study to estimate the odds ratio (OR) and 95% confidence interval (CI) to assess the risk associated with all the baseline variables. Potential confounding variables were taken into account, and adjusted odds ratios (aORs) were computed to consider their impact on the relationship between the ISR group and the non-ISR group. A significance level of p ≤ 0.05 was utilized for the statistical tests, and two-tailed p-values were considered significant. All statistical analyses were performed using the SAS System for Windows version 9.4 (SAS Institute Inc., Cary, North Carolina, USA).
3. Results
3.1. Baseline Characteristics
The results of the study indicated significant differences among the one vessel disease (1VD) group (n=55), two vessel disease (2VD) group (n=144), and three vessel disease (3VD) group (n=318) in terms of age, underlying diseases, and cardiovascular medications. In relation to gender, the percentage of males in the 1VD group was 70.91%, in the 2VD group was 79.86%, and in the 3VD group was 84.28% (p=0.036). Among the mentioned factors, the 3VD group exhibited the highest proportion of underlying diseases, including hypertension, type II diabetes mellitus, dyslipidemia, chronic kidney disease, end-stage renal disease, and a history of coronary artery bypass graft. Additionally, the use of cardiovascular medications such as aspirin and clopidogrel was more prevalent in the 3VD group (Table 1). Among all the patients with coronary ISR, stable angina (n=125, 71%) accounted for the majority of clinical manifestations, followed by ACS (n=28, 16%), and silent ischemia (n=24, 13%) (Figure 1).
3.2. Independent Clinical Predictors of Coronary ISR
In Table 2, we performed adjustments for age, BMI, and sex in Model 1. Subsequently, in Model 2, we further adjusted for underlying diseases in addition to age, BMI, and sex. The results of Model 1 showed that patients with three vessel disease (3VD) had a higher risk of coronary ISR compared to the reference group, with an adjusted odds ratio (aOR) of 2.58 (95% confidence interval [CI] 1.30 - 5.13, p = 0.006). Model 2 also demonstrated a significant association between 3VD and increased risk of coronary ISR, with an aOR of 2.34 (95% CI 1.14 - 4.79, p = 0.020), after adjusting for all the specified variables. Furthermore, in Model 3 (Table 3), where adjustments were made for all variables, including age, BMI, sex, and underlying diseases, the analysis revealed that within the age group, there was a significant association between increasing age and the risk of coronary ISR, with an aOR of 1.02 (95% CI 1.00 - 1.04, p = 0.037). Specifically, within the VD group, the 3VD subgroup was found to have a significantly higher risk of coronary ISR, with an aOR of 2.15 (95% CI 1.03 - 4.46, p = 0.039). These findings highlight that both age and the presence of three vessel disease (3VD) are independently associated with an increased risk of coronary ISR.
3.3. Coronary Angiography and Lesion Characteristics
When considering the previous stent type, there was no statistically significant difference observed between the coronary ISR group and the non-ISR group for both BMS and DES (Figure 2). In terms of the coronary lesions, the results of coronary angiography showed significant differences between the ISR group and the non-ISR group. The ISR group had a higher percentage of patients with left main (LM) disease (22% versus 12%, p=0.002), three vessel disease (3VD) (75% versus 55%, p<0.001), and chronic total occlusion (CTO) (44% versus 23%, p<0.001) compared to the non-ISR group (Figure 3). Regarding the location of the coronary ISR, the left anterior descending artery (LAD) accounted for the majority of the affected vessels, with 80 cases (44%). This was followed by the right coronary artery (RCA) with 47 cases (26%), and the left circumflex artery (LCX) with 30 cases (17%) (Figure 4).
4. Discussion
The risk factors associated with coronary ISR have not been completely elucidated. Proposed risk factors for coronary ISR include hypertension, diabetes, dyslipidemia, heart failure, chronic kidney disease, a history of previous coronary artery bypass graft, and multi-vessel disease [10,11,12,13,14]. Our study revealed that the group with three-vessel disease (3VD) had the highest prevalence of underlying conditions such as hypertension, diabetes, dyslipidemia, chronic kidney disease, end-stage renal disease, and a history of coronary artery bypass graft. These individuals also had a higher usage of cardiovascular medications like aspirin and clopidogrel. However, only older age and the presence of 3VD were identified as independent clinical predictors of coronary ISR. The complexity of CAD with diffuse lesions may contribute to an increased risk of atherosclerosis progression and ISR following coronary stenting [15]. Multi-vessel CAD is often accompanied by various comorbidities and is characterized by smaller vessel size, longer and more diffuse lesions. This poses challenges in selecting an appropriate stent size and length to cover the entire lesion. Consequently, there is a potential for geographical miss during PCI, leading to an increased risk of ISR development [16,17]. Pathological studies have indicated that calcified atherosclerotic lesions can be classified into microcalcification and macrocalcification. Microcalcification is more prevalent in younger patients and is associated with endothelial inflammation and plaque instability, potentially leading to ACS. On the other hand, macrocalcification occurs predominantly in older patients with multi-vessel CAD, making revascularization during PCI more difficult [18,19]. Interestingly, although diabetes has long been considered a major risk factor for coronary ISR [20,21], our study did not demonstrate an increased risk. In the era of DES, the high efficacy of these stents may have mitigated the vulnerability of diabetic patients to stent injury and neointimal proliferation [14].
The incidence of coronary ISR has significantly decreased with the advancements in stent technology and improvements in interventional procedures. New generation DESs have been developed to address the concerns of coronary ISR and enhance the long-term effectiveness of PCI when compared to BMSs [22,23]. Despite these advancements, BMSs continue to be extensively utilized worldwide, with an average adoption rate of approximately 20% [24,25]. When it comes to the likelihood of developing ISR, larger coronary arteries, which are defined as vessels with a lumen diameter greater than 3-3.5 mm, are less prone to this complication than smaller arteries. Consequently, BMSs are often preferred for larger vessels as they provide sufficient space to accommodate neointimal hyperplasia. As a result, the use of BMSs is primarily associated with a higher incidence of aggressive restenosis in cases involving longer lesions or smaller vessels [26,27,28,29]. Morice MC et al. also proposed that BMS use might not take higher risk of coronary ISR and need for repeated revascularization in patients with larger coronary vessels [30]. Similarly, in our study, we observed that coronary ISR did not occur more frequently in patients with BMSs compared to those with DESs. This finding emphasizes that in carefully selected patients with larger coronary vessel diameter, there may not be a necessity to preferentially implant a DES to reduce the risk of future ISR, which substantially decreases the medical costs. Currently, the treatment for CAD is well optimized, including use of dual antiplatelet, renin-angiotensin system blockage and high-strength statins. These treatments may substantially decrease the occurrence of coronary ISR, even in cases involving BMSs.
The clinical presentation of coronary ISR can vary, but it often manifests similarly to CAD, including silent ischemia, angina pectoris, and recurrent cardiac events (unstable angina or ACS). Previous studies have provided insights into the clinical presentations of coronary ISR in patients with BMSs and DESs. It has been found that unstable angina is the most common presentation of BMS ISR, accounting for a range of 26% to 53% of cases, followed by AMI, which occurs in approximately 3.5% to 20% of patients. Similarly, DES ISR is characterized by unstable angina in approximately 16% to 66% of cases and AMI in 1% to 20% of cases [5,31,32]. However, our study yielded unexpected results. We observed that stable angina accompanied by stress-induced myocardial ischemia, as evidenced by myocardial perfusion imaging (MPI), was the predominant clinical presentation of coronary ISR, accounting for 71% of cases. This finding highlights the significance of identifying stress-induced myocardial ischemia through MPI in patients with angina or angina-equivalent symptoms, particularly those at high risk for coronary ISR. It is important to note that the risk of coronary ISR is highest within the first year after stent placement, and gradually decreasing over time. Therefore, regular follow-up tests, including stress tests, electrocardiograms (ECGs), or imaging studies, are recommended for high risk patients to monitor their condition and detect any signs of ischemia. In summary, our study highlight the prevalence of stable angina with stress-induced myocardial ischemia as the main presentation of coronary ISR. Timely identification of ischemia through MPI testing in patients at high risk for ISR may play a crucial role in reducing the incidence of ACS.
In our study, we observed that the left anterior descending (LAD) coronary artery had the highest incidence of ISR among all the study populations, accounting for 44% of all ISR lesions. From an anatomical perspective, the LAD coronary artery differs from the LCX and RCA in several ways. It possesses two sets of branches known as septal branches and diagonal branches. The septal branches perforate the interventricular septum to supply the anterior two-thirds of the septum, while the diagonal branches supply the anterior left ventricle. Coronary ISR can occur in arteries of different sizes, but it is more likely to occur in smaller arteries. Several possible mechanisms may support this hypothesis. Firstly, smaller arteries have a greater density of smooth muscle cells (SMCs) compared to larger arteries. SMCs play a crucial role in the development of coronary ISR as they can proliferate and migrate to the site of injury caused by stent placement. The excessive proliferation of SMCs contributes to the narrowing of the vessel and the development of ISR [33]. Secondly, although DES use can significantly reduce the incidence of ISR, in smaller arteries, there is less surface area available for drug deposition, leading to reduced efficacy in preventing restenosis. Thirdly, smaller arteries are subjected to relatively higher mechanical stresses such as compression, expansion, and flexion while stent placement. These mechanical stresses can cause stent struts to recoil or induce arterial injury, contributing to a higher incidence of ISR [34]. Lastly, smaller coronary arteries poses more challenges to achieve optimal stent expansion and apposition during stent deployment. Inadequate stent expansion or incomplete coverage of the lesion segment may contribute to the development of ISR [8,35].
Limitations
This study had several limitations that need to be acknowledged. Firstly, it was a retrospective study, which means that the results may have been influenced by various confounding factors. Secondly, the study did not compare the treatment modalities of PCI with DCB or new stenting in the population with coronary ISR, which may provide valuable insights into the effectiveness of different interventions. Thirdly, the analysis of short-term and long-term coronary ISR was hindered by a substantial amount of missing data, potentially limiting the overall conclusions that can be drawn. Lastly, the sample size utilized in the study was relatively small, indicating the need for further validation of the findings in larger populations or among different ethnic groups. By recognizing these limitations, future studies can focus on addressing these issues to enhance the validity and generalizability of the findings.
5. Conclusions
Patients with CAD who are older in age and have three-vessel disease are at a higher risk of developing coronary ISR. Therefore, it is crucial to arrange close follow-up after PCI in these patients. Monitoring and regular check-ups are necessary to detect any potential signs of ISR early and intervene promptly to ensure optimal patient outcomes.
Author Contributions
Conceptualization, Yu-An Chen and Chia-Ti Tsai.; methodology, Yen-Chun Huang.; software, Yen-Chun Huang.; formal analysis, Yen-Chun Huang.; investigation, Yu-An Chen.; resources, Cho-Kai Wu, Juey-Jen Hwang, Yi-Chih Wang, Jiun-Yang Chiang, and Chia-Ti Tsai; data curation, Yu-An Chen; writing—original draft preparation, Yu-An Chen; writing—review and editing, Cho-Kai Wu, and Chia-Ti Tsai ; supervision, Cho-Kai Wu, Juey-Jen Hwang, Yi-Chih Wang, Jiun-Yang Chiang, and Chia-Ti Tsai. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
202007135RINC.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
No new data were created.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Nobuyoshi M, Kimura T, Nosaka H et al, Restenosis after successful percutaneous transluminal coronary angioplasty: serial angiographic follow-up of 229 patients. J Am Coll Cardiol 1988, 12, 616–623. [CrossRef]
- Fischman DL, Leon MB, Baim DS, et al. A randomized comparison of coronarystent placement and balloon angioplasty in the treatment of coronary artery disease. Stent Restenosis Study Investigators. N Engl J Med 1994, 331, 496–501. [Google Scholar] [CrossRef]
- Taniwaki M, Stefanini GG, Silber S, et al. 4-Year clinical outcomes and predictors of repeat revascularization in patients treated with new-generation drug-eluting stents. J Am Coll Cardiol 2014, 63, 1617–1625. [Google Scholar] [CrossRef]
- Kereiakes DJ, Onuma Y, Serruys PW, et al. Bioresorbable vascular scaffolds for coronary revascularization. Circulation. 2016, 134, 168–182. [Google Scholar] [CrossRef]
- Dangas GD, Claessen BE, Caixeta A, et al. In-stent restenosis in the drug-eluting stent era. J Am Coll Cardiol 2010, 56, 1897–1907. [Google Scholar] [CrossRef]
- Magalhaes MA, Minha S, Chen F, et al. Clinical presentation and outcomes of coronary in-stent restenosis across 3-stent generations. Circ Cardiovasc Interv 2014, 7, 768–776. [Google Scholar] [CrossRef] [PubMed]
- Jukema JW, Verschuren JJ, Ahmed TA, et al. Restenosis after PCI. Part 1: pathophysiology and risk factors. Nat Rev Cardiol 2011, 9, 53–62. [Google Scholar]
- 8. Aoki J, Tanabe K. Mechanisms of drug-eluting stent restenosis. Cardiovasc Interv Ther.
- Zhang DM, Chen S. In-stent restenosis and a drug-coated balloon: insights from a clinical therapeutic strategy on coronary artery diseases. Cardiol Res Pract 2020, 20, 8104939. [Google Scholar]
- Singh M, Gersh BJ, McClelland RL, et al. Clinical and angiographic predictors of restenosis after percutaneous coronary intervention: insights from the Prevention of Restenosis with Tranilast and Its Outcomes (PRESTO) trial. Circulation 2004, 109, 2727–2731. [Google Scholar] [CrossRef]
- Byrne RA, Joner M, Kastrati A. Stent thrombosis and restenosis: what have we learned and where are we going? The Andreas Gruntzig Lecture ESC 2014. Eur Heart J 2015, 36, 3320–3331.
- Cassese S, Byrne RA, Tada T, et al. Incidence and predictors of restenosis after coronary stenting in 10 004 patients with surveillance angiography. Heart 2014, 100, 153–159. [Google Scholar] [CrossRef]
- Aoyama Y, Hirayama H, Ishii H, et al. Impact of chronic kidney disease on a re-percutaneous coronary intervention for sirolimus-eluting stent restenosis. Coron Artery Dis 2012, 23, 528–532. [Google Scholar] [CrossRef] [PubMed]
- Kastrati A, Dibra A, Mehilli J, et al. Predictive factors of restenosis after coronary implantation of sirolimus- or paclitaxel-eluting stents. Circulation 2006, 113, 2293–2300. [Google Scholar] [CrossRef] [PubMed]
- Wang JL, Qin Z, Wang ZJ et al. New predictors of in-stent restenosis in patients with diabetes mellitus undergoing percutaneous coronary intervention with drug-eluting stent. J Geriatr Cardiol 2018, 15, 137–145. [Google Scholar]
- Paramasivam G, Devasia T, Jayaram A, et al. In-stent restenosis of drug-eluting stents in patients with diabetes mellitus: clinical presentation, angiographic features, and outcomes. Anatol J Cardiol 2020, 23, 28–34. [Google Scholar]
- Her AY, Shin ES, Kim S, et al. Drug-coated balloon-based versus drug-eluting stent-only revascularization in patients with diabetes and multivessel coronary artery disease. Cardiovasc Diabetol 2023, 22, 120. [Google Scholar] [CrossRef]
- Mori H, Torii S, Kutyna M, et al. Coronary artery calcificationand its progression: What does it really mean? J Am Coll Cardiol Img 2018, 11, 127–142. [Google Scholar]
- Sarnak MJ, Amann K, Bangalore S, et al. Chronic kidney disease and coronary artery disease: JACC state-of-the-art review. J Am Coll Cardiol 2019, 74, 1823–1838. [Google Scholar] [CrossRef] [PubMed]
- Elezi S, Kastrati A, Pache J, et al. Diabetes mellitus and the clinical and angiographic outcome after coronary stent placement. J Am Coll Cardiol 1998, 32, 1866–1873. [Google Scholar] [CrossRef]
- Carrozza JP Jr, Kuntz RE, Fishman RF, et al. Restenosis after arterial injury caused by coronary stenting in patients with diabetes mellitus. Ann Intern Med 1993, 118, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Stefanini GG, Holmes DR. Drug-eluting coronary-artery stents. N Engl J Med 2013, 368, 254–265. [Google Scholar] [CrossRef]
- Piccolo R, Bonaa KH, Efthimiou O, et al. Drug-eluting or bare-metal stents for percutaneous coronary intervention: a systematic review and individual patient data meta-analysis of randomised clinical trials. Lancet 2019, 393, 2503–2510. [Google Scholar] [CrossRef]
- Biswas S, Duffy SJ, Lefkovits J, et al. Australian trends in procedural characteristics and outcomes in patients undergoing percutaneous coronary intervention for ST-elevation myocardial infarction. Am J Cardiol 2018, 121, 279–288. [Google Scholar] [CrossRef]
- Rymer JA, Harrison RW, Dai D, et al. Trends in bare-metal stent use in the united states in patients Aged >/=65 Years (from the CathPCI Registry). Am J Cardiol 2016, 118, 959–966. [Google Scholar] [CrossRef]
- Colombo A, Giannini F, Briguori C. Should we still have bare-metal stents available in our catheterization laboratory? J Am Coll Cardiol 2017, 70, 607–619. [Google Scholar] [CrossRef]
- Elezi S, Kastrati A, Neumann FJ, et al. Vessel size and long-term outcome after coronary stent placement. Circulation 1998, 98, 1875–1880. [Google Scholar] [CrossRef]
- Cutlip DE, Chauhan MS, Baim DS, et al. Clinical restenosis after coronary stenting: perspectives from multicenter clinical trials. J Am Coll Cardiol 2002, 40, 2082–2089. [Google Scholar] [CrossRef]
- Changal KH, Mir T, Khan S, et al. Drug-eluting stents versus bare-metal stents in large coronary artery revascularization: Systematic review and meta-analysis. Cardiovasc Revasc Med 2021, 23, 42–49. [Google Scholar] [CrossRef]
- Morice MC, Urban P, Greene S, et al. Why are we still using coronary bare-metal stents? J Am Coll Cardiol 2013, 61, 1122–1123. [Google Scholar] [CrossRef]
- Bossi I, Klersy C, Black AJ, et al. In-stent restenosis: long-term outcome and predictors of subsequent target lesion revascularization after repeat balloon angioplasty. J Am Coll Cardiol 2000, 35, 1569–1576. [Google Scholar] [CrossRef]
- Chen MS, John JM, Chew DP, et al. Bare metal stent restenosis is not a benign clinical entity. Am Heart J 2006, 151, 1260–1264. [Google Scholar] [CrossRef]
- Marx SO, Totary-Jain H, Marks AR. Vascular smooth muscle cell proliferation in restenosis. Circ Cardiovasc Interv 2011, 4, 104–111. [Google Scholar] [CrossRef]
- Bedoya J, Meyer CA, Timmins LH, et al. Effects of stent design parameters on normal artery wall mechanics. J Biomech Eng 2006, 128, 757–765. [Google Scholar] [CrossRef]
- Wang P, Qiao H, Wang R, et al. The characteristics and risk factors of in-stent restenosis in patients with percutaneous coronary intervention: what can we do. BMC Cardiovasc Disord 2020, 20, 510. [Google Scholar]
Figure 1.
Clinical manifestations of coronary ISR. ACS: acute coronary syndrome.
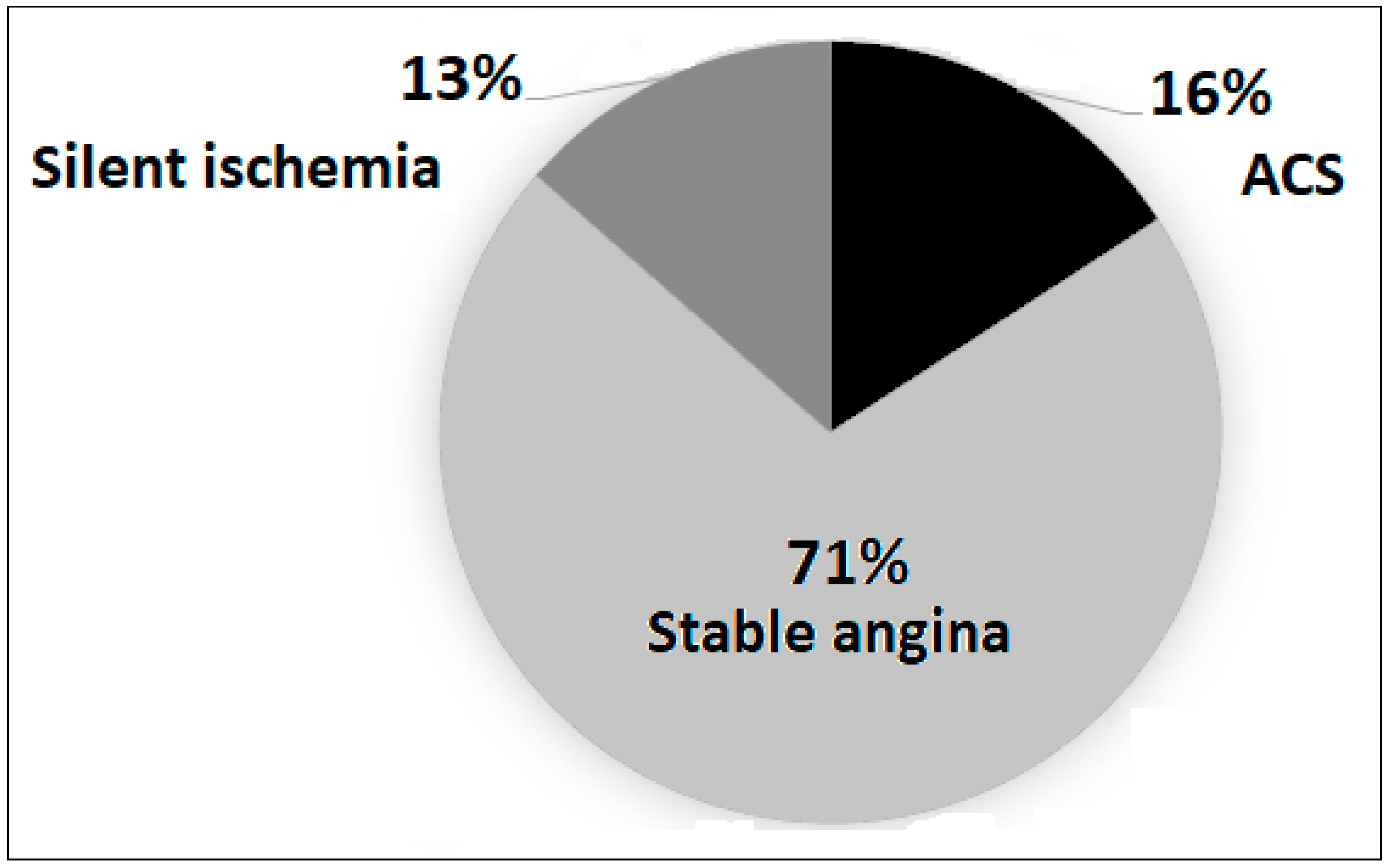
Figure 2.
Previous stent types. BMS: bare-metal stent, DES: drug-eluting stent, BVS: bioresorbable vascular scaffold, ISR: in-stent restenosis.
Figure 2.
Previous stent types. BMS: bare-metal stent, DES: drug-eluting stent, BVS: bioresorbable vascular scaffold, ISR: in-stent restenosis.
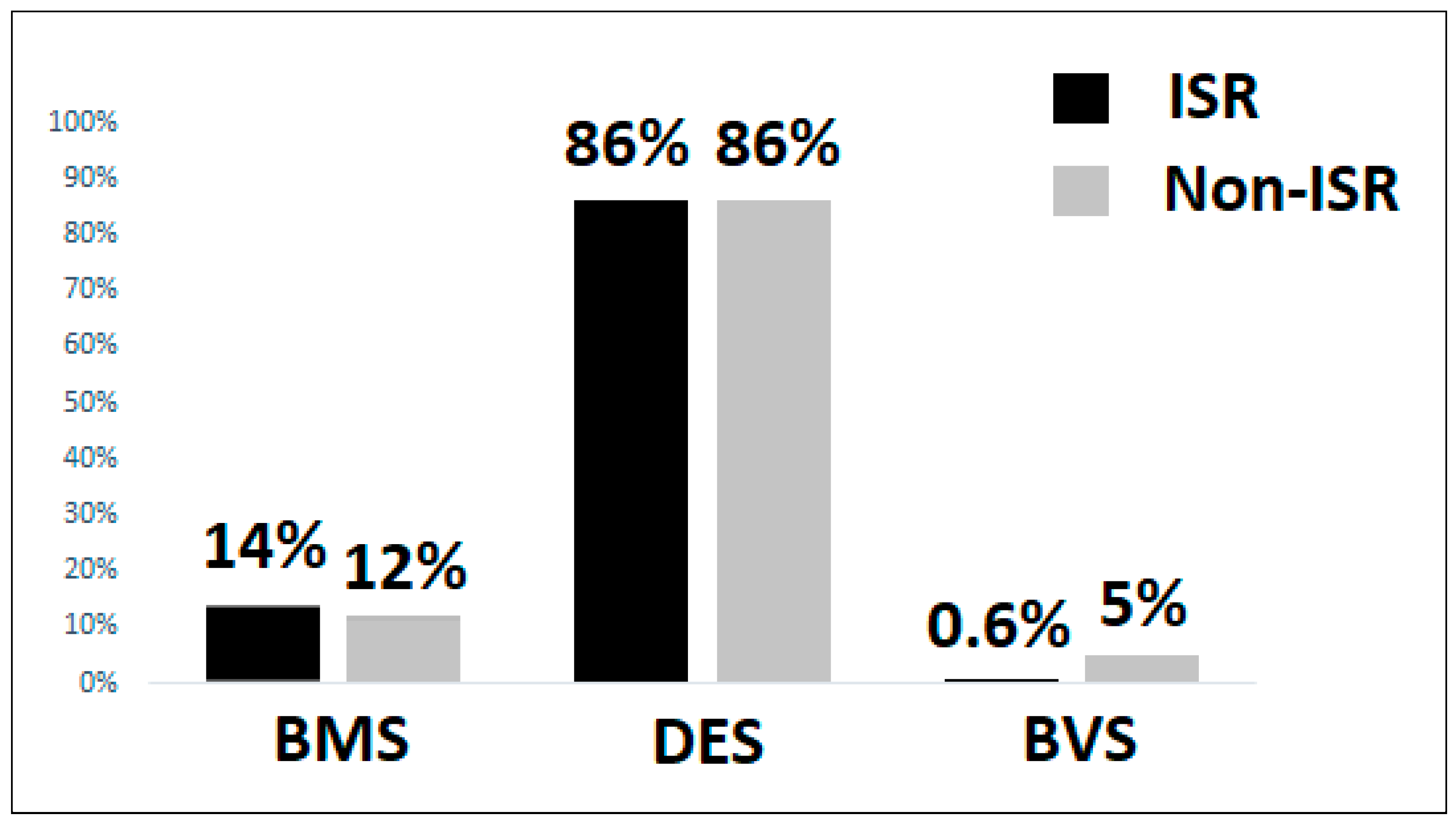
Figure 3.
Severity of coronary artery disease. LM: left main coronary artery, CTO: chronic total occlusion.
Figure 3.
Severity of coronary artery disease. LM: left main coronary artery, CTO: chronic total occlusion.
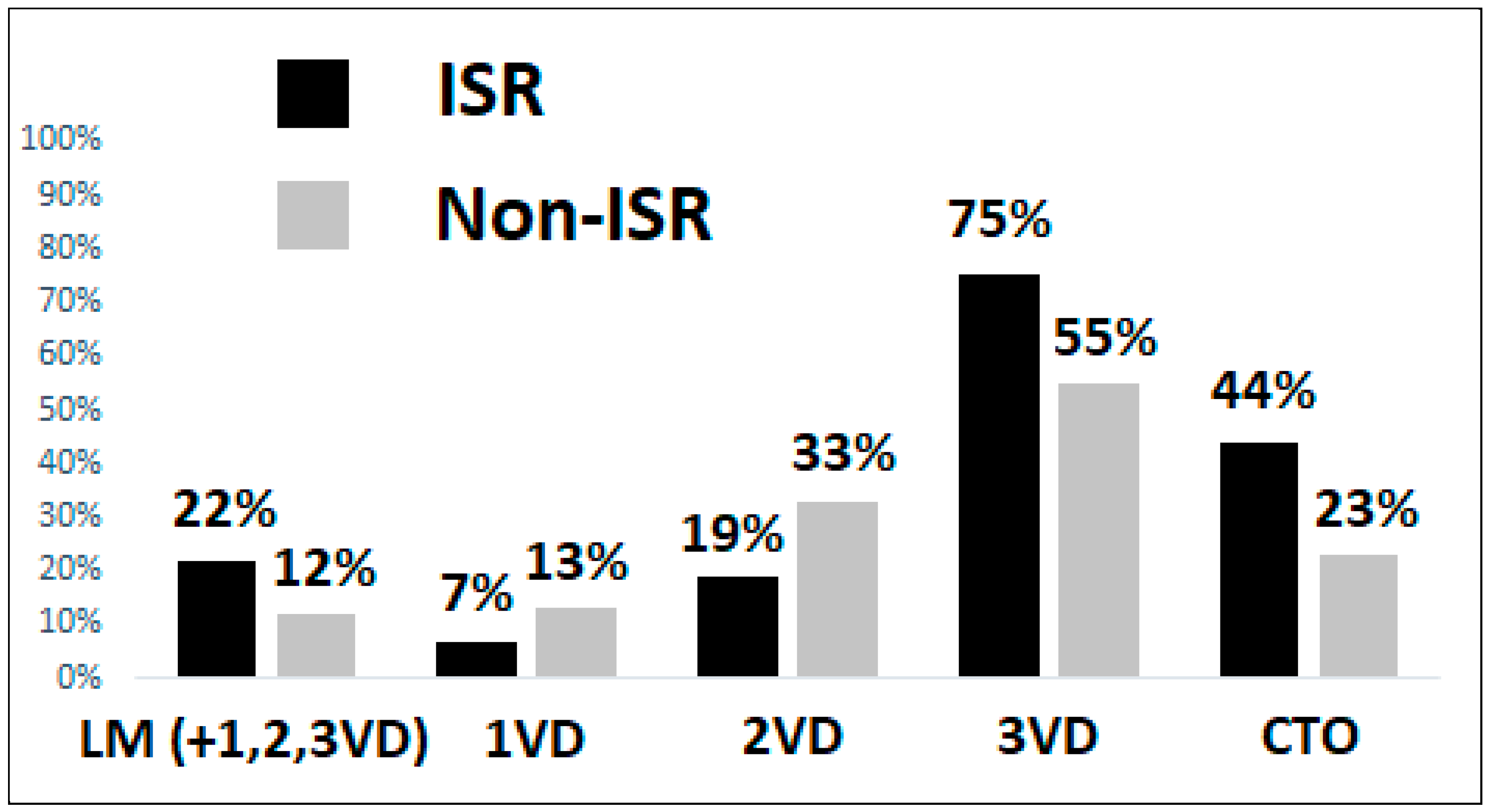
Figure 4.
Coronary ISR vessel.
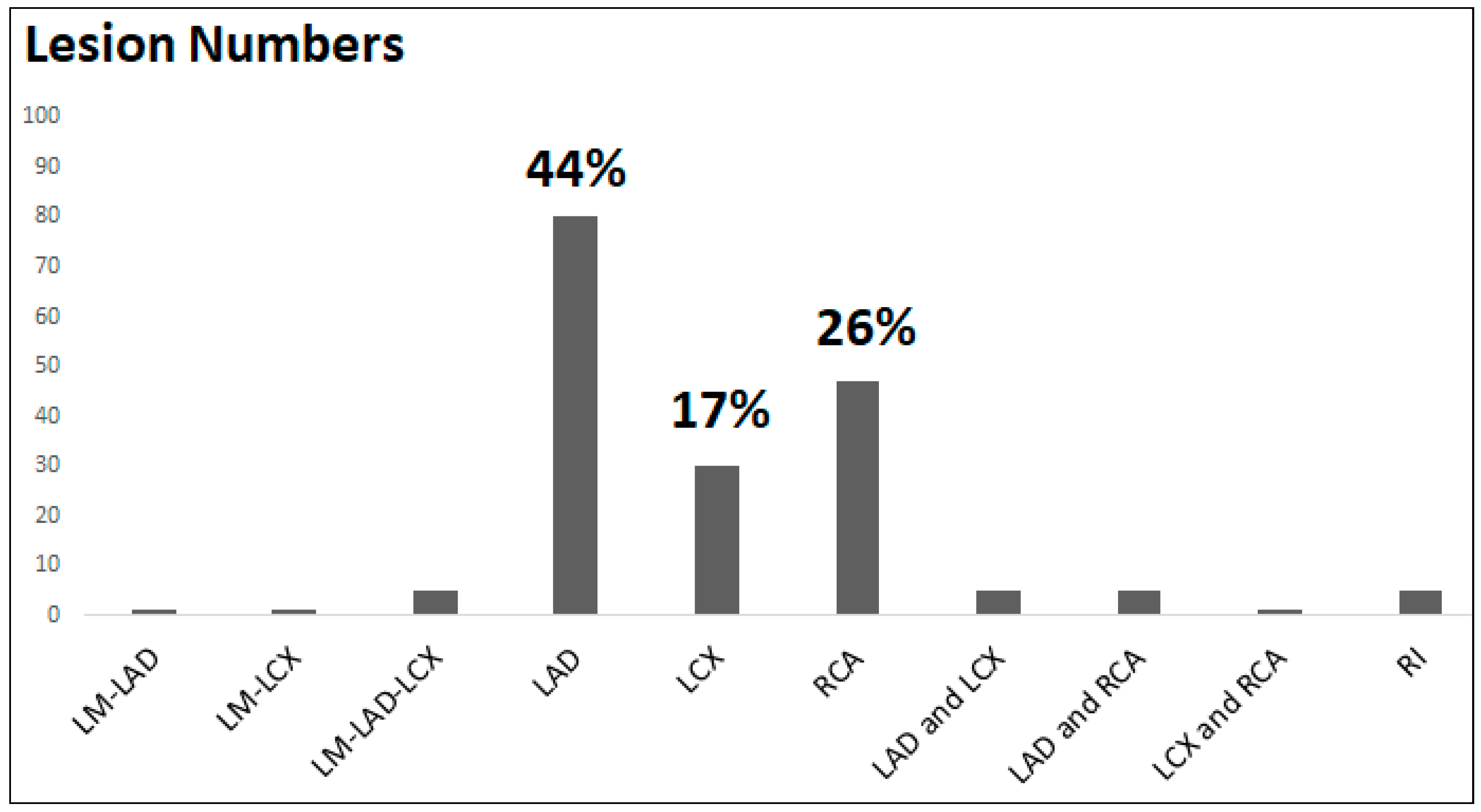

Table 1.
Demographic and clinical characteristics.
| Variables | 1VD (n = 55) | 2VD(n = 144) | 3VD(n = 318) | P value |
|---|---|---|---|---|
| Age | 66.80 ± 11.28 | 68.10 ± 11.98 | 67.77 ± 10.78 | 0.762 |
| Gender (Male) | 39 (70.91) | 116 (80.56) | 270 (84.91) | 0.036 |
| BMI (kg/m2) | 25.95 ± 3.79 | 25.94 ± 3.58 | 26.23 ± 3.62 | 0.685 |
| Underlying diseases | ||||
| HTN | 37 (67.27) | 115 (79.86) | 268 (84.28) | 0.010 |
| T2DM | 15 (27.27) | 60 (41.67) | 179 (56.29) | <0.001 |
| DLP | 35 (63.64) | 116 (80.56) | 229 (72.01) | 0.033 |
| PAOD | 1 (1.82) | 6 (4.17) | 15 (4.72) | 0.615 |
| CKD | 3 (5.45) | 10 (6.94) | 53 (16.67) | 0.003 |
| ESRD | 2 (3.64) | 5 (3.47) | 35 (11.01) | 0.010 |
| AF/AFL | 10 (18.18) | 17 (11.81) | 27 (8.49) | 0.078 |
| HFrEF | 5 (9.09) | 22 (15.28) | 47 (14.78) | 0.499 |
| History of CABG | 0 (0) | 2 (1.39) | 25 (7.86) | 0.002 |
| Medications | ||||
| Aspirin | 27 (49.09) | 99 (68.75) | 228 (71.70) | 0.003 |
| Clopidogrel | 21 (38.18) | 53 (36.81) | 158 (49.69) | 0.020 |
| Ticagrelor | 1 (1.82) | 5 (3.47) | 20 (6.29) | 0.030 |
| Prasugrel | 2 (3.64) | 5 (3.47) | 13 (4.09) | 0.946 |
| NOAC | 7 (12.73) | 9 (6.25) | 19 (5.97) | 0.176 |
| Statin | 35 (63.64) | 102 (70.83) | 235 (73.90) | 0.276 |
| ACEi /ARB | 17 (30.91) | 59 (40.97) | 133 (41.82) | 0.309 |
| Beta blockers | 30 (54.55) | 75 (52.08) | 180 (56.60) | 0.661 |
| ARNI | 0 (0) | 5 (3.47) | 13 (4.09) | 0.311 |
| Previous stent type | ||||
| BMS | 6 (10.91) | 17 (11.81) | 43 (31.52) | 0.797 |
| DES | 43 (78.18) | 120 (83.33) | 280 (88.05) | 0.099 |
| BVS | 6 (10.91) | 10 (6.94) | 1 (0.31) | - |
| Primary outcome | ||||
| ISR | 12 (21.82) | 33 (22.92) | 132 (41.51) | <0.001 |
BMI: body mass index, HTN: hypertension, T2DM: type II diabetes mellitus, DLP: dyslipidemia, PAOD: peripheral artery occlusive disease, CKD: chronic kidney disease, ESRD: end stage renal disease, AF: atrial fibrillation, AFL: atrial flutter, HFrEF: heart failure with reduced ejection fraction, CABG: coronary artery bypass graft, NOAC: non-vitamin K antagonist oral anticoagulant, ACEi: angiotensin converting enzyme inhibitor, ARB: angiotensin II receptor blocker, ARNI: angiotensin receptor-neprilysin inhibitor, ISR: in-stent restenosis, 1VD: one-vessel disease, 2VD: two-vessel disease, 3VD: three-vessel disease.
Table 2.
Independent clinical predictors of coronary ISR.
| Variables | Model 1 | P value | Model 2 | P value | |
|---|---|---|---|---|---|
| aOR (95% CI) | aOR (95% CI) | ||||
| Group of VD | 1VD (ref) | 1 | 1 | ||
| 2VD | 1.05 (0.49 – 2.24) | 0.889 | 1.04 (0.48 – 2.25) | 0.917 | |
| 3VD | 2.58 (1.30 – 5.13) | 0.006 | 2.34 (1.14 – 4.79) | 0.020 | |
Model 1: adjusted sex, age, and BMI; Model 2: adjust sex, age, BMI, and underlying diseases.
Table 3.
Independent clinical predictors of coronary ISR.
| Variables | Model 3 | P value | |
|---|---|---|---|
| aOR (95% CI) | |||
| Group of VD | 1VD (ref) | 1 | |
| 2VD | 0.96 (0.44 – 2.10) | 0.934 | |
| 3VD | 2.15 (1.03 – 4.46) | 0.039 | |
| Age | 1.02 (1.00 – 1.04) | 0.037 | |
| Gender | Female (ref) | 1 | |
| Male | 1.00 (0.59 – 1.71) | 0.976 | |
| BMI (kg/m2) | 0.99 (0.94 – 1.05) | 0.920 | |
| Underlying diseases | |||
| HTN | 0.68 (0.40 – 1.17) | 0.169 | |
| T2DM | 1.42 (0.93 – 2.16) | 0.100 | |
| DLP | 0.75 (0.47 – 1.21) | 0.254 | |
| PAOD | 1.42 (0.55 – 3.63) | 0.643 | |
| CKD | 0.91 (0.50 - 1.66) | 0.761 | |
| ESRD | 1.45 (0.68 – 3.08) | 0.328 | |
| AF/AFL | 1.53 (0.67 – 3.47) | 0.308 | |
| HFrEF | 1.28 (0.70 – 2.34) | 0.407 | |
| History of CABG | 1.69 (0.73 – 3.98) | 0.218 | |
| Medications | |||
| Aspirin | 1.39 (0.87 – 2.23) | 0.165 | |
| Clopidogrel | 1.04 (0.67 – 1.62) | 0.838 | |
| Ticagrelor | 0.92 (0.37 – 2.30) | 0.867 | |
| Prasugrel | 0.80 (0.28 – 2.28) | 0.681 | |
| NOAC | 0.74 (0.26 – 2.06) | 0.565 | |
| Statin | 1.29 (0.80 – 2.07) | 0.288 | |
| ACEi /ARB | 1.03 (0.68 – 1.55) | 0.887 | |
| Beta blockers | 1.07 (0.72 – 1.60) | 0.707 | |
| ARNI | 0.69 (0.21 – 2.22) | 0.540 | |
Model 3: adjust sex, age, BMI , underlying diseases, and medications.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



